Article Text

Abstract
Objective Eosinophilic oesophagitis (EoE) and gastro-oesophageal reflux disease (GORD) can have similar clinical and histological features. Proton pump inhibitors (PPIs) are used to distinguish the disorders, with the assumption that only GORD can respond to PPIs. Oesophageal expression of eotaxin-3 stimulated by Th2 cytokines might contribute to oesophageal eosinophilia in EoE. Th2 cytokine effects on the oesophagus in GORD are not known. The objective of the authors was to explore the molecular mechanisms of Th2 cytokines on eotaxin-3 expression by oesophageal squamous cells from patients with GORD and EoE, and the effects of omeprazole on that eotaxin-3 expression.
Design Using telomerase-immortalised and primary cultures of oesophageal squamous cells from GORD and EoE patients, the authors measured eotaxin-3 protein secretion stimulated by Th2 cytokines (interleukin (IL)-4 and IL-13). Eotaxin-3 promoter constructs were used to study transcriptional regulation. Cytokine-induced eotaxin-3 mRNA and protein expression were measured in the presence or absence of omeprazole.
Results There were no significant differences between EoE and GORD primary cells in cytokine-stimulated eotaxin-3 protein secretion levels. In EoE and GORD cell lines, IL-4 and IL-13 activated the eotaxin-3 promoter, and significantly increased eotaxin-3 mRNA and protein expression. Omeprazole blocked the cytokine-stimulated increase in eotaxin-3 mRNA and protein expression in EoE and GORD cell lines.
Conclusion Oesophageal squamous cells from GORD and EoE patients express similar levels of eotaxin-3 when stimulated by Th2 cytokines, and omeprazole blocks that eotaxin-3 expression. These findings suggest that PPIs might have eosinophil-reducing effects independent of effects on acid reflux and that response to PPIs might not distinguish EoE from GORD.
- Eosinophilic oesophagitis
- GORD
- proton pump inhibitors
- Th2 cytokines
- eotaxin-3
- fibrogenesis
- epithelial cells
- dysphagia
- epithelial barrier
- Barrett's metaplasia
- gastro-oesphageal junction
- molecular carcinogenesis
- Barrett's carcinoma
- Barrett's oesophagus
- ACID
- molecular biology
- acid-related diseases
Statistics from Altmetric.com
- Eosinophilic oesophagitis
- GORD
- proton pump inhibitors
- Th2 cytokines
- eotaxin-3
- fibrogenesis
- epithelial cells
- dysphagia
- epithelial barrier
- Barrett's metaplasia
- gastro-oesphageal junction
- molecular carcinogenesis
- Barrett's carcinoma
- Barrett's oesophagus
- ACID
- molecular biology
- acid-related diseases
Significance of this study
What is already known on this subject?
-
Eosinophilic oesophagitis (EoE) and gastro-oesophageal reflux disease (GORD) can share clinical and histological features, including oesophageal eosinophilia, and it is sometimes difficult to distinguish the two disorders.
-
It has been proposed that EoE can be distinguished from GORD by the response to proton pump inhibitor therapy.
-
Patients with EoE exhibit greater oesophageal expression of eotaxin-3 (a potent eosinophil chemoattractant) than patients with GORD, but it is not known if this is because the oesophagus of EoE patients constitutively overexpresses eotaxin-3 or if oesophageal eotaxin-3 overexpression is acquired as the result of stimulation by cytokines or other factors.
-
The Th2 cytokines interleukin (IL)-13 and IL-4, which are overproduced in allergic disorders, can stimulate oesophageal expression of eotaxin-3.
What are the new findings?
-
Cultures of oesophageal squamous cells from gastro-oesophageal reflux disease (GORD) and eosinophilic oesophagitis (EoE) patients express similar levels of eotaxin-3 at baseline and when stimulated by Th2 cytokines.
-
Omeprazole blocks Th2 cytokine-stimulated eotaxin-3 expression in cultures of oesophageal squamous cells from GORD and EoE patients.
How might it impact on clinical practice in the foreseeable future?
-
In both gastro-oesophageal reflux disease (GORD) and eosinophilic oesophagitis (EoE), proton pump inhibitors (PPIs) might have eosinophil-reducing effects that are independent of their effects on gastric acid secretion.
-
A response to PPI therapy might not distinguish EoE from GORD.
Introduction
Eosinophil predominant oesophageal inflammation is the key histological feature of eosinophilic oesophagitis (EoE), a chronic, immune/antigen-mediated disease that causes oesophageal symptoms such as dysphagia and chest pain.1 Eosinophils also can infiltrate the oesophagus in gastro-oesophageal reflux disease (GORD), a chronic, acid-peptic condition in which refluxed stomach contents cause oesophageal damage and symptoms, which often include dysphagia and chest pain.2 In some patients, therefore, it can be difficult to distinguish EoE from GORD. Furthermore, it has been suggested that there is a complex interaction between EoE and GORD, and that the notion of establishing a clear distinction between the disorders might be too simplistic.3
The mechanisms underlying oesophageal eosinophilia in EoE and GORD are not clear. In EoE, one proposed mechanism involves oesophageal expression of eotaxin-3, a potent eosinophil chemoattractant. RNA microarray expression analyses have shown that oesophageal squamous mucosal biopsy specimens from children with EoE exhibit profound upregulation of the eotaxin-3 gene.4 Patients with EoE also have greater oesophageal mucosal expression of eotaxin-3 mRNA than patients with GORD.5 However, it is not clear whether those increased eotaxin-3 expression levels result from constitutive overexpression of eoxtaxin-3 in the oesophagus of EoE patients, or whether that overproduction is acquired as a consequence of oesophageal stimulation by allergic cytokines or other factors. In addition, oesophageal mucosal biopsy specimens are comprised of diverse cell types (eg, epithelial, inflammatory, stromal cells), and available studies do not establish which of those cell types are responsible for the increased eotaxin-3 expression.
In a number of different cell types, the expression of eotaxin-3 is stimulated by T helper (Th)2 cytokines such as interleukin (IL)-4 and IL-13, whose overproduction is characteristic of allergic disorders. IL-4 and IL-13 are known to activate the signal transducer and activator of transcription (STAT)6 signalling pathway.6–8 In some GORD patients, it is conceivable that Th2 cytokines activate oesophageal STAT6 signalling to induce eotaxin-3 production, thereby causing oesophageal eosinophilia. Presently, few data are available on Th2 cytokine effects on the oesophagus of patients with GORD.
It has been proposed that EoE can be distinguished from GORD by the patient's response to proton pump inhibitors (PPIs).9 ,10 The premise is that reduced gastric acid secretion is the only important effect of PPIs and, therefore, only an acid-peptic disorder like GORD can respond to PPIs. Challenging this premise is the recent identification of patients whose oesophageal symptoms and eosinophilia respond to PPIs even though they have no evidence of GORD by endoscopy or oesophageal pH monitoring.1 ,11 The mechanism underlying this ‘PPI-responsive oesophageal eosinophilia’ is not known. It is conceivable that these patients simply have GORD that is not detectible by endoscopy and pH monitoring, but that responds to PPIs nevertheless. However, it is also possible that these patients are responding to anti-inflammatory effects of PPIs independent of their effects on gastric acid secretion, and a number of putative anti-inflammatory effects of PPIs have been described.12
The objective of our study was to determine the effects of Th2 cytokines (IL-13 and IL-4) on transcriptional regulation and secretion of eotaxin-3 in oesophageal squamous cells from patients with EoE or GORD. To do so, we established primary cultures of oesophageal squamous cells from EoE and GORD patients, and we immortalised oesophageal squamous cells from patients with EoE through stable incorporation of human telomerase reverse transcriptase (hTERT). In addition, we explored whether the PPI omeprazole could block the effects of Th2 cytokines on eotaxin-3 expression by oesophageal squamous cells.
Materials and methods
Patients
These studies were approved by the institutional review board of the Dallas VA Medical Center. Nine adult patients with EoE (all male subjects, average age 44±4.9 SEM years) and six adult patients with GORD (five male subjects, average age 56.4±4.6 years) had biopsy specimens taken from the squamous-lined oesophagus to establish primary cell cultures (supplemental materials).
Isolation and culture of oesophageal squamous cells
Oesophageal squamous cell cultures were established from oesophageal biopsy specimens as previously described (supplemental materials).13–15 We also used two previously characterised, telomerase-immortalised, non-neoplastic oesophageal squamous cell lines established from patients with GORD (NES-B10T and NES-G4T).16 All cell lines exhibited a squamous phenotype and were used at population doubling (PD) 50–90 unless otherwise indicated.
Human telomerase retroviral infection
The oesophageal squamous cells from two EoE patients were retrovirally infected with hTERT as previously described (supplemental materials) to create two telomerase-immortalised cell lines (EoE1-T and EoE2-T).13
Contact inhibition and anchorage-dependent cell growth assays
For EoE1-T and EoE2-T, 1×106 cells were plated in six-well plates, harvested at multiple time points ranging from 1 to 20 days, and counted using the Coulter Z1 particle counter (Beckman Coulter, Brea, California, USA). For EoE1-T and EoE2-T, 5×105 cells were plated in triplicate in soft agar as previously described; OE33 oesophageal adenocarcinoma cells (Sigma) served as a positive control.16 Plates were examined daily for 3 weeks. Cells were imaged using a Bio-Rad Molecular Imager (Bio-Rad, Hercules, California, USA).
Western blotting
Proteins were separated by SDS-polyacrylamide gel electrophoresis, transferred to nitrocellulose membranes and incubated with primary antibodies to cytokeratins 4 and 14, p53, p21, β-tubulin and β-actin (supplemental materials). All blots were performed in duplicate.
UV-B irradiation
EoE1-T and EoE2-T cells were cultured overnight in 100 mm plates, rinsed several times with 1× PBS, and exposed to 200 J/m2 ultraviolet-B (UV-B) irradiation as previously described.13 Protein was harvested at 24, 48, and 72 h after irradiation. Non-irradiated cells served as controls. MCF-7 cells treated with doxorubicin (0.2 μg/ml) served as a positive control for p53 and p21 expression.
Cytokine stimulation of oesophageal squamous cells and omeprazole treatment
Cells were stimulated with 0–100 ng/ml of IL-13 or IL-4 (R&D Systems, Minneapolis, Minnesota, USA) for 48 h. For PPI studies, omeprazole (Sigma) was acid-activated in medium with pH 5.5 for 30 min.17 Cells were then pretreated for 2 h with omeprazole 50 μM in medium with pH 7.4 prior to the addition of cytokines. Omeprazole remained in the media throughout the period of cytokine stimulation.
ELISA for eotaxin-3
We performed ELISA of conditioned media, using commercially available ELISA kits (R&D Systems) to assess the production of eotaxin-3 by oesophageal cells (supplemental materials). All assays were performed in duplicate.
Semiquantitative and quantitative real-time PCR
Semiquantitative and real-time PCR were performed for eotaxin-3, IL-13Rα1 and IL-4Rα mRNAs in all four cell lines (supplemental materials). All PCR assays were performed in triplicate in at least two separate experiments.
Eotaxin-3 promoter activity
Plasmid constructs containing the proximal 800 bp of the eotaxin-3 promoter cloned into pGL3 upstream of a luciferase reporter (EO 1), and EO 1 containing point mutations in the distal (−693), proximal (−89) or both STAT6 binding sites were used for transfection studies; renilla reporter pHRL-TK was used to equalise for transfection efficiency (all plasmids were the generous gift of Dr Marc Rothenberg, Cincinnati Children's Hospital, Cincinnati, Ohio, USA).6 Data were expressed as relative light units for firefly luciferase normalised to renilla luciferase (supplemental materials). All assays were performed in at least three separate experiments.
Statistical analyses
Quantitative data are expressed as mean±SEM. Statistical analyses were performed using a paired or unpaired Student t test with the Instat for Windows statistical software package (GraphPad Software, San Diego, California, USA). For multiple comparisons, ANOVA and Student–Newman–Keuls multiple-comparisons test were performed. p Values ≤0.05 were considered significant for all analyses.
Results
IL-13 and IL-4 stimulate eotaxin-3 protein secretion to similar mean levels in primary oesophageal squamous cells from EoE and GORD patients, with substantial variation among individuals
Oesophageal mucosal biopsy specimens from EoE patients express greater levels of eotaxin-3 mRNA than GORD patients or normal controls,4 ,5 but mucosal biopsy specimens comprise diverse cell types. To isolate the contribution of epithelial cells, we studied Th2 cytokine-stimulated eotaxin-3 secretion in primary oesophageal squamous cell cultures from nine patients with EoE and six patients with GORD (figure 1). At baseline, both groups exhibited minimal secretion of eotaxin-3 protein. Stimulation with IL-13 or IL-4 for 48 h caused a marked increase in eotaxin-3 protein secretion in both the EoE and GORD cell cultures. However, there were no significant differences between EoE and GORD cells in their mean levels of Th2 cytokine-stimulated eotaxin-3 protein secretion. In figure 1, note the wide scatter of stimulated cell data points indicating substantial differences among cells from individual EoE and GORD patients in their levels of stimulated protein secretion.

Baseline and Th2 cytokine-stimulated eotaxin-3 protein secretion in primary oesophageal squamous cells from nine patients with eosinophilic oesophagitis (EoE) and six patients with gastro-oesophageal reflux disease (GORD). Cells were stimulated for 48 h with interleukin (IL)-13 (10 ng/ml) or IL-4 (1 ng/ml). Data are the mean±SEM of two separate experiments. *p≤0.05 compared with unstimulated (baseline) control.
Establishment of telomerase-immortalised oesophageal squamous cell lines from patients with EoE
Growth of the uninfected parental cells, EoE1 and EoE2, stopped at PD ∼30 and ∼20, respectively, while hTERT-infected cells continue to grow after more than 100 PDs (supplemental figure 1A–D). The PD times of EoE1-T and EoE2-T are approximately 41 and 36 h, respectively. The TRAP-eze detection kit demonstrates substantial telomerase activity after the introduction of hTERT (supplemental figure 1E). In addition, EoE1-T and EoE2-T cells express cytokeratins 4 and 14 (markers of oesophageal squamous cell differentiation) (supplemental figure 1F).18 ,19
EoE1-T and EoE2-T cells are not transformed and express p53 and p21 cell cycle checkpoint proteins appropriately after UV-B irradiation
Unlike transformed cells,20 EoE1-T and EoE2-T cells demonstrate cell–cell contact inhibition (supplemental figure 2A–B). In addition, EoE1-T and EoE2-T cells show no growth in soft agar after 3 weeks, unlike the OE33 oesophageal adenocarcinoma cells, which exhibit anchorage-independent growth evidenced by numerous colonies in soft agar (supplemental figure 2C). These in vitro assays suggest that EoE1-T and EoE2-T cells, although immortalised, are not transformed.
Immortalisation of human cells using viral oncoproteins commonly disrupts normal growth control mechanisms like the p53 cell-cycle checkpoint.21 In contrast, telomerase-immortalised cell lines usually maintain appropriate p53 responses.13–15 We determined whether our EoE1-T and EoE2-T cells maintain an appropriate p53 response to UV-induced DNA damage (supplemental figure 2D). We found that UV-B exposure (200 J/m2) increased expression levels of p53 protein and its downstream effector protein p21 within 24 h, and levels of both remained elevated at 48 and 72 h.
IL-13 and IL-4 stimulate eotaxin-3 protein secretion in oesophageal squamous cell lines from EoE and GORD patients
We found that Th2 cytokines stimulate primary oesophageal squamous cells from EoE and GORD patients to secrete similar mean levels of eotaxin-3 protein. Using our telomerase-immortalised cell lines, we explored mechanisms underlying this cytokine-stimulated eotaxin-3 production. As in our primary cell cultures, we found minimal baseline secretion of eotaxin-3 in all four cell lines, with no significant differences in baseline levels among the lines (figures 2A–D and 3A–D). Stimulation with IL-13 (figure 2A–D) and IL-4 (figure 3A–D) caused significant increases in eotaxin-3 secretion in all four cell lines. In figures 2 and 3, note the different scales on the y-axes indicating substantial differences among cell lines from individual EoE and GORD patients in their levels of stimulated protein secretion. After reviewing these data, we selected to use IL-13 at a dose of 10 ng/ml and IL-4 at a dose of 1 ng/ml for subsequent experiments.

Baseline and interleukin (IL)-13-stimulated eotaxin-3 protein secretion in (A) EoE1-T, (B) EoE2-T, (C) NES-G4T and (D) NES-B10T cells. Cells were stimulated for 48 h with IL-13 at doses of 1, 10 and 100 ng/ml. Data are the mean±SEM of two separate experiments. *p≤0.05 compared with unstimulated (baseline) control; **p≤0.01 compared with unstimulated (baseline) control; ***p≤0.001 compared with unstimulated (baseline) control.

Baseline and interleukin (IL)-4-stimulated eotaxin-3 protein secretion in (A) EoE1-T, (B) EoE2-T, (C) NES-G4T and (D) NES-B10T cells. Cells were stimulated for 48 h with IL-4 at doses of 1, 10 and 100 ng/ml. Data are the mean±SEM of two separate experiments. *p≤0.05 compared with unstimulated (baseline) control; **p≤0.01 compared with unstimulated (baseline) control; ***p≤0.001 compared with unstimulated (baseline) control.
IL-13 and IL-4 induce expression of eotaxin-3 mRNA in EoE and GORD cell lines
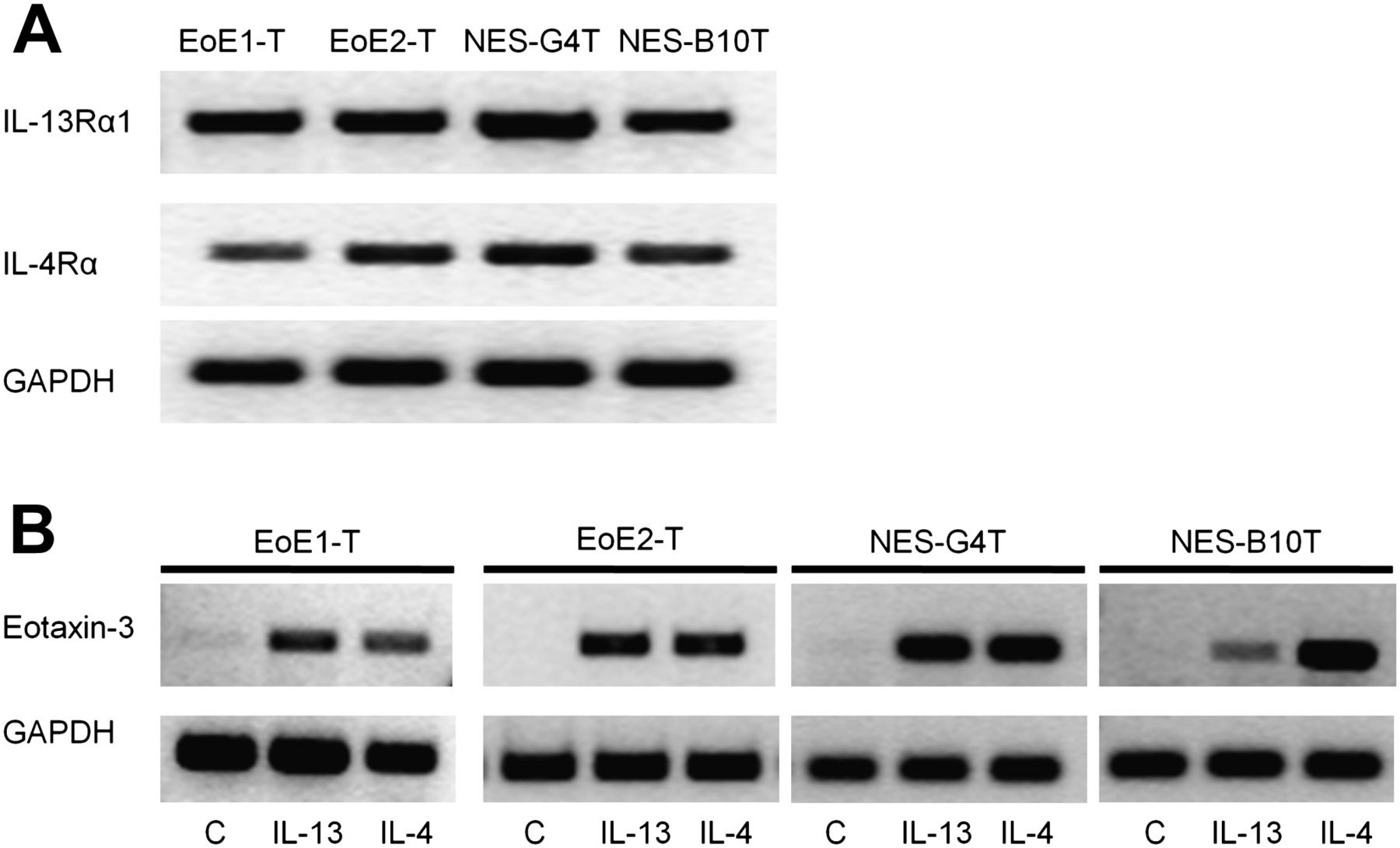
To determine whether the increase in transcriptional regulation might be due to upregulation of cytokine receptors, we assessed mRNA expression levels for the IL-13 receptor IL-13Rα1, and the IL-4 receptor IL-4Rα. There were no substantial differences in mRNA expression levels for IL-13Rα1 or IL-4Rα among the cell lines (figure 4A). We next determined whether cytokine-stimulated eotaxin-3 protein secretion might be due to increased transcriptional regulation. Using RT-PCR, we found that all four cell lines increased eotaxin-3 mRNA expression following stimulation with IL-13 or IL-4 for 48 h (figure 4B).
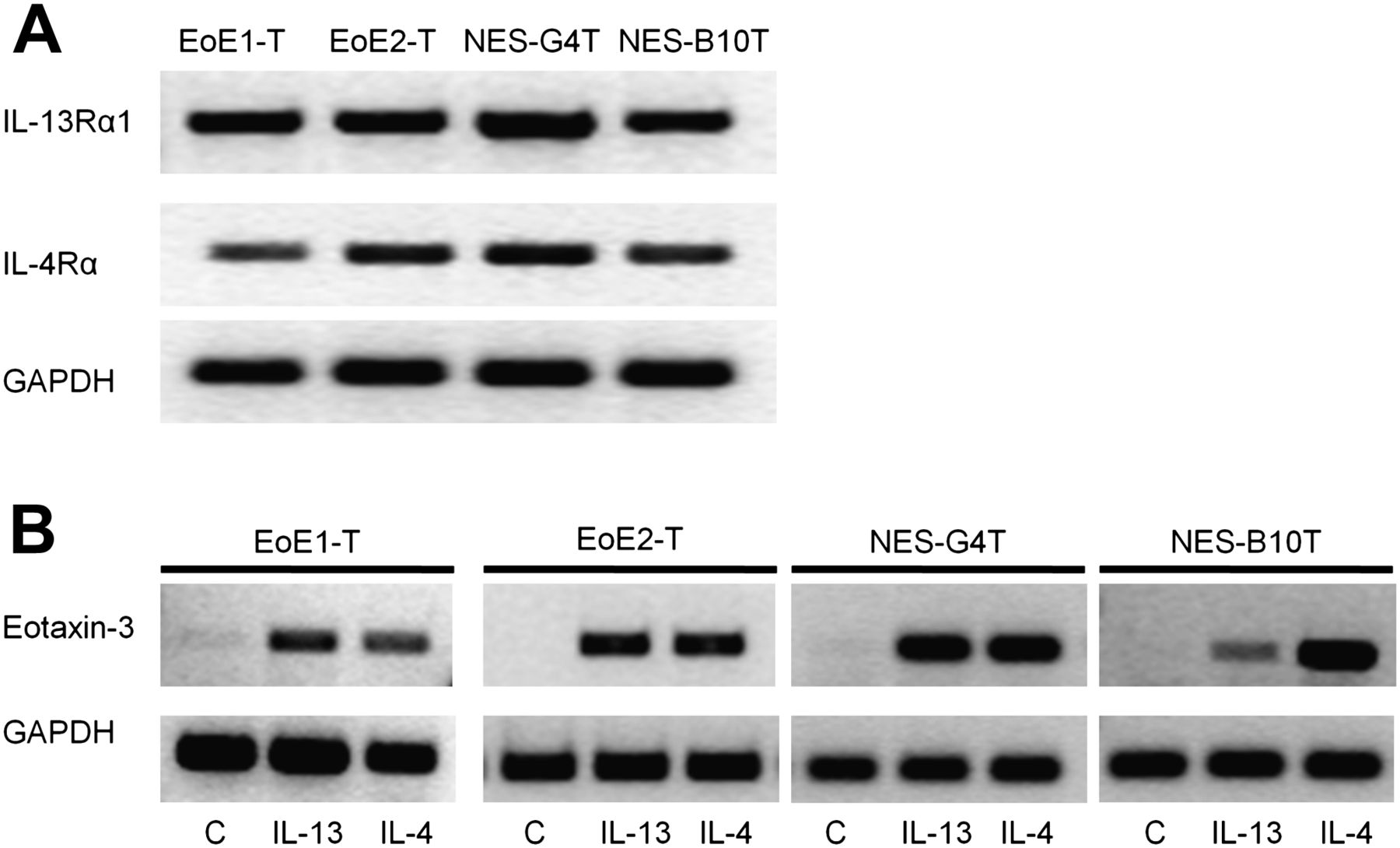
(A) Baseline interleukin (IL)-13 and IL-4 receptors mRNA expression in EoE1-T, EoE2-T, NES-G4T and NES-B10T. Depicted is one of three separate experiments. (B) Eotaxin-3 mRNA expression levels after 48 h of stimulation with IL-13 or IL-4 in EoE1-T, EoE2-T, NES-G4T and NES-B10T. Depicted is one of three separate experiments.
IL-13 and IL-4 activate the eotaxin-3 promoter in oesophageal squamous cells from EoE and GORD patients
We next determined whether IL-13 and IL-4 activate the eotaxin-3 promoter in primary oesophageal squamous cells. We transiently transfected the cells using the EO 1 promoter (−800 bp). After stimulation with IL-13 (10 ng/ml) or IL-4 (1 ng/ml) for 24 h, both EoE and GORD cells exhibited significantly increased eotaxin-3 promoter activity (figure 5A). There were no significant differences in the degree of promoter activation between the groups.

(A) Th2 cytokine stimulation increases eotaxin-3 promoter activity in primary oesophageal squamous cells from patients with eosinophilic oesophagitis and gastro-oesophageal reflux disease. (B–E) The sequence and location of each consensus signal transducer and activator of transcription (STAT)6 site upstream of the luciferase reporter are detailed. X depicts the mutated sites. Cell lines were treated with interleukin (IL)-13 (10 ng/ml) or IL-4 (1 ng/ml) for 24 h. (B) Full length EO 1 promoter (−800 bp); (C) EO 1 promoter with mutations in both STAT6 binding sites; (D) EO 1 promoter with mutation in the distal (−693) STAT6 binding site; and (E) EO 1 promoter with mutation in the proximal (−89) STAT6 binding site. Data are the mean±SEM of at least three separate experiments. *p≤0.05; **p≤0.01; ***p≤0.001.
To determine the relevant STAT6 DNA binding site, we transfected EoE and GORD cell lines with EO 1 promoter and its promoter mutation constructs, and stimulated the cells with IL-13 and IL-4 (figure 5B–E). With mutations of both the proximal and distal STAT6 binding sites, cytokine-stimulated eotaxin-3 promoter activation was abolished in all four cell lines (figure 5C). Mutation of the proximal (figure 5E) but not the distal (figure 5D) STAT6 binding site abolished cytokine-stimulated eotaxin-3 promoter activation. These findings show that the proximal STAT6 DNA binding site is the relevant one in both EoE and GORD cells.
Omeprazole blocks the IL-13- and IL-4-induced increase in eotaxin-3 protein secretion
We next explored whether omeprazole could block the IL-13- and IL-4-induced increase in eotaxin-3 protein secretion. We treated the four cell lines with IL-13 (50 ng/ml) or IL-4 (10 ng/ml) for 48 h in the presence or absence of omeprazole 50 μM (figure 6). Omeprazole alone had no effect on eotaxin-3 secretion. IL-13 and IL-4 caused significant increases in the secretion of eotaxin-3 in all four cell lines, as expected. In the presence of omeprazole, however, the cytokine-induced increase in eotaxin-3 secretion was significantly reduced.

Omeprazole (OME) blocks cytokine-stimulated eotaxin-3 protein secretion. (A) EoE1-T, (B) EoE2-T, (C) NES-G4T and (D) NES-B10T were stimulated for 48 h with either IL-13 (50 ng/ml) or IL-4 (10 ng/ml) in the presence or absence of omeprazole (50 μM). Data are the mean±SEM of two separate experiments. *p≤0.05 compared with unstimulated (baseline) control; **p≤0.01 compared with control; ***p≤0.001 compared with control; #p≤0.05 compared with corresponding Th2 cytokine stimulation alone; ##p≤0.01 compared with corresponding Th2 cytokine stimulation alone; ###p≤0.001 compared with corresponding Th2 cytokine stimulation alone.
Omeprazole decreases IL-13- and IL-4-induced eotaxin-3 mRNA expression
To determine whether omeprazole affected Th2 cytokine-induced eotaxin-3 transcriptional regulation, RT-PCR and real-time PCR were performed to evaluate Th2 cytokine-induced eotaxin-3 mRNA expression in the presence or absence of omeprazole. We treated cells with IL-13 (50 ng/ml) or IL-4 (10 ng/ml) for 1.5 h and found that omeprazole decreased IL-13- and IL-4-induced eotaxin-3 mRNA expression (figure 7A–D). Omeprazole alone had no effect on baseline eotaxin-3 mRNA expression.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cytokine-induced eotaxin-3 mRNA expression levels in the presence or absence of omeprazole (50 μM) in (A) EoE1-T, (B) EoE2-T, (C) NES-G4T and (D) NES-B10T determined by conventional PCR and quantitative real-time PCR. Depicted is one of two separate experiments. ***p≤0.001 compared with control; ###p≤0.001 compared with corresponding Th2 cytokine stimulation alone.
Discussion
In telomerase-immortalised oesophageal squamous cell lines from patients with EoE and GORD, we have shown that Th2 cytokines (IL-4 and IL-13) activate the eotaxin-3 promoter via its proximal STAT6 binding site, and significantly increase eotaxin-3 mRNA expression and protein secretion. We also have demonstrated that there are no significant differences between primary oesophageal squamous cells from EoE and GORD patients in the degree of activation of eotaxin-3 promoter or in the level of eotaxin-3 protein secretion stimulated by those Th2 cytokines. Finally, we have shown that omeprazole can block the cytokine-stimulated increase in eotaxin-3 mRNA expression and protein secretion in oesophageal squamous cell lines from patients with GORD or EoE.
Oesophageal biopsy specimens from EoE patients have exhibited profound increases in eotaxin-3 mRNA expression levels compared with specimens from patients with GORD.4 ,5 However, it has not been clear whether those increased eotaxin-3 levels are due to constitutive oesophageal overproduction of eotaxin-3 in EoE patients or whether that overproduction is an acquired phenomenon. In addition, mucosal biopsies comprise a number of different cell types, and it has not been clear which of those types are responsible for the increased eotaxin-3 expression observed in mucosal biopsy specimens. Our EoE and GORD primary squamous cell cultures both exhibited similar low levels of eotaxin-3 protein secretion at baseline. In primary cultures, furthermore, we observed that mean levels of cytokine-stimulated eotaxin-3 protein secretion did not differ significantly between EoE and GORD cells. These observations suggest that the increased eotaxin-3 expression observed in biopsy specimens from EoE patients compared with GORD patients is not due to a fundamental genetic difference in the capacity of the oesophageal squamous cells to produce eotaxin-3. Rather, our observations that both EoE and GORD cells produce low levels of eotaxin-3 protein at baseline and that Th2 cytokines stimulate both to secrete similar levels of eotaxin-3 protein suggest that the higher eotaxin-3 levels found in EoE patients may be acquired as the result of stimulation by another, presumably allergic, disorder. It is important to appreciate that, although our cell culture systems enabled us to focus on Th2 cytokine effects on squamous epithelial cells, those systems provided no information on any other cell type. Our studies suggest that squamous epithelial cells contribute to the elevated eotaxin-3 levels found in oesophageal biopsy specimens from EoE patients, but it remains possible that other cell types (eg, inflammatory, stromal cells) also contribute to those elevated levels.
Primary oesophageal squamous cell cultures are established by placing oesophageal biopsy specimens essentially unaltered into culture medium. The lack of genetic alteration is considered desirable for studies on cellular and molecular mechanisms. Unfortunately, primary cell cultures have a very limited lifespan, which limits their utility for extended studies. Such studies typically are conducted in immortal cell lines, which can replicate in culture indefinitely. Earlier studies used oesophageal squamous carcinoma cell lines to investigate molecular mechanisms involved in Th2 cytokine-induced eotaxin-3 expression.22 However, cancer cells contain numerous, poorly characterised genetic abnormalities that might alter cellular responses to cytokines. Therefore, we established telomerase-immortalised oesophageal squamous cell lines as preferable in vitro models for mechanistic molecular analyses. Telomerase immortalisation enables cells to replicate without limit while maintaining otherwise normal cell features, and we have shown that our EoE cell lines exhibit a number of properties of normal, non-neoplastic cells. For example, they maintain morphological and protein expression characteristics of normal oesophageal squamous cells, including the expression of squamous cell markers like cytokeratins 4 and 14.18 ,19 Unlike transformed cells, EoE1-T and EoE2-T cells maintain growth inhibition with cell-to-cell contact, demonstrate anchorage-dependent growth and have an intact p53 cell-cycle checkpoint. Thus, our cell lines appear to be valid models for studying cell signalling in EoE.
Although our primary cell cultures showed no significant differences between EoE and GORD cells in their mean levels of cytokine-stimulated eotaxin-3 protein secretion, our two EoE cell lines exhibited higher eotaxin-3 secretion levels than our two GORD cell lines. It is possible that this difference was an artefact resulting from the telomerase-immortalisation process, but we think it is more likely that the difference is spurious. Figure 1 shows a wide scatter of data points indicating substantial differences among cells from individual EoE and GORD patients in their levels of cytokine-stimulated protein secretion. With such a wide variation among patients, significant differences between small numbers of individual cell lines might occur readily by chance alone.
We found that EoE and GORD oesophageal cell lines have similar molecular mechanisms for Th2 cytokine induction of eotaxin-3. There were no apparent differences in mRNA expression levels for IL-13Rα1 or IL-4Rα among the lines. We found that all four cell lines increased eotaxin-3 mRNA expression and promoter activation following Th2 cytokine stimulation. This finding was confirmed in primary cells. Using the eotaxin-3 promoter and its promoter mutation constructs, all four cell lines demonstrated that the proximal STAT6 DNA binding site was the main regulatory site for eotaxin-3 transcription. These findings on Th2 cytokine effects in our non-neoplastic oesophageal cells are in agreement with earlier studies using oesophageal squamous cancer cell lines, dermal fibroblasts, kidney and bronchial cells.7 ,8 ,22 ,23 We show that Th2 cytokine-induced STAT6 signalling can cause increased eotaxin-3 expression by oesophageal squamous epithelial cells, but it is possible that Th2 cytokines stimulate other signalling pathways that also might contribute to increase eotaxin-3 production.
The unclear distinction between EoE and GORD in some patients continues to pose a clinical challenge. Histologically, both EoE and GORD demonstrate eosinophilic infiltration, but the degree of eosinophilic infiltration usually is more pronounced in EoE. However, Rodrigo et al reported that EoE could not be distinguished from GORD solely on the basis of maximum eosinophil count in oesophageal biopsy specimens.24 Indeed, some GORD patients had eosinophil counts exceeding 100 per high power field. Our finding that EoE and GORD cells exhibit similar increases in eotaxin-3 mRNA expression and protein secretion upon stimulation with Th2 cytokines provides a potential molecular explanation for this clinical observation.
EoE is widely regarded as a manifestation of food allergy, but it has not been clear why a food allergy should cause eosinophils to accumulate in the oesophagus primarily. Oesophageal production of eotaxin-3 appears to play a key role in attracting eosinophils to the oesophagus. If a food allergen triggers a Th2 immune response, then our studies suggest that oesophageal squamous cells will respond to that Th2 cytokine stimulation by increasing eotaxin-3 expression, which would draw eosinophils to the oesophagus. This is a potential mechanism whereby a food allergy could cause eosinophils to home to the oesophagus.
GORD is associated with oesophageal eosinophilia through mechanisms that are not clear. Research in this area has focused primarily on the role of refluxed acid. For example, acid causes human oesophageal microvascular endothelial cells to express adhesion molecules recognised by ligands on the eosinophil.25 Acid also causes the oesophageal mucosa to release platelet-activating factor, which can attract eosinophils.26 In our experiments, we have demonstrated that primary oesophageal squamous cells from GORD patients increase their expression of eotaxin-3 when stimulated by IL-4 and IL-13 to a similar degree as cells from EoE patients. These findings suggest that the release of Th2 cytokines conceivably might contribute to oesophageal eosinophilia in GORD.
Although GORD is not an allergic disorder, it has been suggested that GORD might contribute to the development of an allergic oesophagitis.3 Most recognised food allergens are glycoproteins with molecular weights between 3 and 90 kD.27 ,28 The normal oesophageal epithelium is highly impermeable to such large molecules. For example, the normal rabbit oesophagus is virtually impermeable to epidermal growth factor, a 6 kD peptide and to dextrans with a molecular weight of 4 kD.29 After exposure to acid and pepsin, however, oesophagus becomes permeable to epidermal growth factor and to dextrans as large as 20 kD. Thus, GORD-induced epithelial damage could result in exposure of deep layers of oesophageal epithelium to food allergens, which might trigger a systemic or local Th2 immune response that stimulates oesophageal eotaxin-3 production. Proof for this speculation requires further studies.
The response of an oesophageal disease to an empirical trial of PPIs has been regarded as evidence for an underlying acid-peptic disorder, based on the assumption that reduced gastric acid secretion is the only important effect of PPIs. Recent clinical observations have called this assumption into question, however. As mentioned, patients with PPI-responsive oesophageal eosinophilia have no evidence of GORD by endoscopy or pH monitoring.1 ,11 In one recent study, 30 patients with clinical and histological evidence of EoE were randomly assigned to treatment with either esomeprazole or fluticasone.30 After 8 weeks of treatment, there were no significant differences between the groups in the rates of clinical and histological remission, and baseline oesophageal pH monitoring results were not useful for predicting response to either drug. These observations suggest that PPIs might have anti-inflammatory effects independent of effects on gastric acid secretion, and a number of potential anti-inflammatory effects of PPIs have been described.12
We found that treatment with omeprazole blocks Th2 cytokine-induced eotaxin-3 mRNA expression and protein secretion in both GORD and EoE cell lines. These are cells in cultures in vitro and, therefore, any omeprazole effects must be independent of the effects on gastric acid production. These findings suggest that a clinicopathological response to PPI therapy might not distinguish EoE from GORD. Our study was not designed to investigate the mechanisms underlying omeprazole's effects on the transcriptional regulation of eotaxin-3. However, we have shown that Th2 cytokine-stimulated eotaxin-3 expression in oesophageal squamous cells is mediated by STAT6 signalling and, in other epithelial cell types, PPIs have been found to inhibit STAT6 phosphorylation.17
In conclusion, we have shown that oesophageal squamous cells from patients with EoE and GORD secrete low levels of eotaxin-3 at baseline. In both EoE and GORD oesophageal squamous cells, Th2 cytokines activate the eotaxin-3 promoter through STAT6, causing similar significant increases in expression of eotaxin-3 mRNA and in secretion of eotaxin-3 protein. We have also shown that treatment with omeprazole reduces Th2 cytokine-stimulated eotaxin-3 mRNA expression and protein secretion in GORD and EoE oesophageal squamous cell lines. These findings suggest that, in both GORD and EoE, PPIs might have eosinophil-reducing effects that are independent of their effects on gastric acid production. Thus, a response to PPI therapy may not distinguish EoE from GORD, and our findings provide a rationale for the use of PPIs in the management of EoE, irrespective of the presence of GORD.
Acknowledgments
The authors would like to thank Dr Marc E Rothenberg for contributing the eotaxin-3 promoter constructs.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
-
Funding This work was supported by the Office of Medical Research, Departments of Veterans Affairs (RFS, SJS, DHW), the National Institutes of Health (R01-DK63621 to RFS, R01-CA134571 to RFS and SJS, T32 DK007745-14 to EC, K12 HD-068369-01 to EC) and the American Gastroenterological Association Institute (Fellow to Faculty Transition Award to EC).
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the institutional review board on human studies at the Dallas VA Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.