Article Text

Abstract
Data on the natural history of elderly-onset inflammatory bowel disease (IBD) are scarce.
Methods In a French population-based cohort we identified 841 IBD patients >60 years of age at diagnosis from 1988 to 2006, including 367 Crohn's disease (CD) and 472 ulcerative colitis (UC).
Results Median age at diagnosis was similar for CD (70 years (IQR: 65–76)) and UC (69 years (64–74)). Median follow-up was 6 years (2–11) for both diseases. At diagnosis, in CD, pure colonic disease (65%) and inflammatory behaviour (78%) were the most frequent phenotype. At maximal follow-up digestive extension and complicated behaviour occurred in 8% and 9%, respectively. In UC, 29% of patients had proctitis, 45% left-sided and 26% extensive colitis without extension during follow-up in 84%. In CD cumulative probabilities of receiving corticosteroids (CSs), immunosuppressants (ISs) and anti tumor necrosis factor therapy were respectively 47%, 27% and 9% at 10 years. In UC cumulative probabilities of receiving CS and IS were 40% and 15%, respectively at 10 years. Cumulative probabilities of surgery at 1 year and 10 years were 18% and 32%, respectively in CD and 4% and 8%, respectively in UC. In CD complicated behaviour at diagnosis (HR: 2.6; 95% CI 1.5 to 4.6) was associated with an increased risk for surgery while CS was associated with a decreased risk (HR: 0.5; 0.3 to 0.8). In UC CS was associated with an increased risk (HR: 2.2; 1.1 to 4.6) for colectomy.
Conclusions Clinical course is mild in elderly-onset IBD patients. This information would need to be taken into account by physicians when therapeutic strategies are established.
- Inflammatory Bowel Disease
- Elderly
- Epidemiology
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
-
The prevalence of inflammatory bowel disease (IBD) is increasing worldwide and the ageing of the population makes elderly-onset IBD a rising problem.
-
There are still uncertainties regarding clinical presentation, disease course and impact of treatments in elderly-onset IBD.
-
Better knowledge of natural history and current prescribing patterns is needed as a first step in improving quality of care delivered to elderly patients with IBD.
What are the new findings?
-
In this largest population-based study of elderly-onset IBD reported to date, 1/20 incident cases of Crohn's disease and 1/8 incident cases of ulcerative colitis occurred in people >60 years of age.
-
The clinical presentation at diagnosis and the course of IBD in elderly-onset patients was mild as compared with younger-onset IBD patients.
-
Taken together, the natural history of elderly-onset IBD is less aggressive than in younger patients.
How might it impact on clinical practice in the foreseeable future?
-
This information challenging previous statements mostly coming from referral centres or small series would need to be taken into account when discussing risk/benefit ratios of therapeutic strategies in elderly-onset patients with IBD.
Introduction
The incidence of inflammatory bowel disease (IBD) is increasing worldwide and the ageing of the population makes elderly-onset IBD a rising problem.1 ,2 The official world census estimated the proportion of elderly patients presently at 4% to 28% of the population.3–5 Uncertainties regarding clinical presentation of IBD, disease course and impact of treatments in the elderly still exist because data are scarce at a population level and are mainly coming from referral centres and/or small-size series.6–11 In addition, in most studies there was no distinction between elderly-onset IBD and elderly patients with disease starting at a younger age. Moreover data from clinical trials cannot be extrapolated to this particular population since in the great majority of them (notably those with biologicals) patients >75 years of age are not eligible. Meanwhile physicians caring for elderly patients are faced with several specific problems such as misdiagnoses, risk/benefit appreciation of medical12 ,13 and surgical therapies and need for concurrent management of significant comorbidities.14 Thus a better knowledge of natural history is strongly needed as a first step in improving quality of care delivered to elderly patients.6–11
The population-based study EPIMAD in northern France provides access to a large cohort of patients with IBD since 1988. The aims of the present study were to describe IBD phenotypes at diagnosis and during follow-up in diagnosed patients >60 years of age and to compare them with younger populations. We also looked at their therapeutic management and outcomes and focused on risk factors for surgery.
Patients and methods
Patient population
Cases included all patients >60 years of age diagnosed with IBD recorded in the EPIMAD registry from January 1988 to December 2006. Study area was northern France with 5 841 156 inhabitants according to the 2008 national population census and was divided into four administrative areas: Nord (2 564 959 inhabitants), Pas-de-Calais (1 459 531), Somme (568 086) and Seine-Maritime (1 248 580). Only patients who had been resident in the defined study area at the time of diagnosis of their disease were included.
Methodology of the EPIMAD registry was previously described in detail.15 Briefly, eight interviewer practitioners collected data of all incident IBD patients diagnosed by all gastroenterologists (GEs) of the area practicing in the private or public sector (n=262). Only patients who had been resident in the defined study area at the time of diagnosis were included. Each GE reported on all patients first consulting for symptoms compatible with IBD. The interviewer practitioners visited the GE's consulting office and collected data from the charts in a standardised questionnaire for each new case. The main data collected were age, gender, year of diagnosis, interval between onset of symptoms and diagnosis, and clinical, radiological, endoscopic and histological findings at the time of diagnosis. Final diagnosis of Crohn's disease (CD) and ulcerative colitis (UC) was made by two expert gastroenterologists and was recorded as definite, probable or possible, according to validated and previously published criteria.15 For the purpose of this study, only patients with definite or probable CD, UC and follow-up ≥2 years were considered.
Additional data collection for the present study
Data were extracted from files of GE and from hospital medical records, and were collected in standardised questionnaires specifically designed for the study. All records were reviewed for accuracy and completeness and validated by the investigator responsible (CC).
Description of variables
Data retrospectively collected at diagnosis and maximal follow-up included age, gender, date of IBD diagnosis, time between the onset of symptoms and diagnosis, IBD localisation and disease behaviour according to the Montreal classification.16 Regarding CD, L1 was ileal disease, L2 colonic and L3 ileocolonic disease (L1 with caecal involvement was considered as L3) and L4 was upper gastrointestinal disease (which could be associated to L1, L2 or L3). Perianal lesions included abscesses and/or fistulae. CD behaviour B1 was inflammatory (non-stricturing non-penetrating), B2 was stricturing and B3 was penetrating disease. B2 (stricturing) and B3 (penetrating) were pooled and defined as ‘complicated behaviour’. The ‘p’ index could be added to B1, B2 or B3 when concomitant perianal disease was present. Regarding UC, proctitis (E1) was defined as a proximal extent of inflammation distal to the rectosigmoid junction, E2 as limited to the colorectum distal to the splenic flexure and E3 as extending proximally to the splenic flexure. Extraintestinal manifestations (EIMs) included joints, skin, and ocular and hepatobiliary manifestations.
The following medications were recorded: 5-aminosalicylic acid (5-ASA; oral or topical); corticosteroids (CSs, oral, topical or intravenous); immunosuppressants (ISs) (azathioprine/6-mercaptopurin and/or methotrexate) and anti tumor necrosis factor (anti-TNF)α including infliximab (IFX), adalimumab (ADA) and certolizumab pegol. Patients were considered as exposed if the medication (at least one prescription) was started at diagnosis or during follow-up and cumulative duration was recorded. CS dependency was defined as continued therapy caused by relapse upon reduction, impeding discontinuation of CS and resistance as the absence of regression of clinical symptoms.
Surgery was restricted to intestinal resection defined as small bowel resection, partial or total colectomy which could be either subtotal colectomy with ileorectal anastomosis or with ileoanal anastomosis (IAA). Definitive stoma was also recorded. Appendectomy, stricturoplasty and elective surgical treatment of anoperineal lesions were excluded.
This study followed the regulations and instructions set up by the Comité National des Registres (approval no 97107 and No 983792).
Statistical analysis
Qualitative variables were given as percentages. Quantitative variables were calculated as medians with IQR (first quartile–third quartile). In order to compare characteristics of patients > 60 years at diagnosis with other groups of age, three additional groups were extracted from the EPIMAD database: 892 IBD patients (689 CD and 203 UC) <17 years at diagnosis, 7112 (4678 CD and 2434 UC) between 17 years and 39 years at diagnosis and 2364 (1175 CD and 1189 UC) between 40 years and 59 years at diagnosis. Global comparison according to age at diagnosis was performed using the χ2 test for qualitative variables and by a Kruskal-Wallis test for quantitative variables. For the comparison of IBD localisation and CD behaviour at diagnosis and at maximal follow-up, a McNemar's χ2 test for symmetry was performed.
Cumulative probabilities (CP) and the 95% CIs of each treatment and surgery were calculated using the Kaplan-Meier method. Risk factors for surgery were searched for using bivariate Cox proportional hazards models. HR and its 95% CI (CI, lower–upper) were used to quantify risk for surgery. For assessing the effect of each treatment on the risk of surgery, we used a propensity score method to adjust analyses for observable differences between treated and not treated patients. Parameters with a p value <0.2 in bivariate analyses were introduced into Cox proportional hazards multivariable regression with backward selection at level 0.2. Data were analysed with SAS software V.9.2 (SAS, Chicago, Illinois, USA). Statistical significance was considered p≤0.05.
Results
Demographic information
From 1988 to 2006, 11 724 patients were diagnosed with IBD, 1058 (9%) being >60 years at diagnosis and representing 5% and 11% of all incident CD and UC cases, respectively. Among the >60 years cohort, 447 had CD (42%) including 367 with a follow-up ≥2 years, 561 had UC (53%) including 474 with a follow-up ≥2 years, and 50 (5%) had IBD unclassified. The recruitment of incident cases was stable over time in different age groups except in patients <17 years at CD diagnosis: in this age group, the incidence increased from 6.5 to 11.1/105 inhabitants from 1988 to 2007.17
Among all IBD patients, the proportion of CD was lower in elderly-onset patients than in younger adults (47% vs 62%; p<10−4) while the proportion of UC was higher (63% vs 42%, respectively; p<10−4). The elderly-onset CD and UC mean annual incidences standardised on sex were 2.6/105 inhabitants (2.4–2.8) and 3.1/105 (2.9–3.4), respectively.
Clinical presentation at diagnosis
Main clinical characteristics of elderly-onset CD and UC patients in comparison with younger patients are displayed in tables 1 and 2. At diagnosis, median age was 70 (65–76) years in CD and 69 (64–73) in UC. There was a female predominance (62%) in CD and a male predominance (62%) in UC. In CD, median time from symptoms onset to diagnosis was shorter than in younger patients (p=0.0005) whereas there was no difference in UC. A family history of IBD was less frequent (7% and 3% of CD and UC) than in other age groups (p<10−4). The median follow-up was 6 (2–11) years. When compared with younger patients, elderly-onset CD patients had less diarrhoea, abdominal pain and systemic symptoms, but more rectal bleeding and anal fistulas (table 1) while elderly-onset UC patients had less rectal bleeding and abdominal pain (table 2).
Sociodemographic and clinical characteristics at diagnosis according to age of 6909 patients with Crohn's disease in a population-based study from northern France
Sociodemographic and clinical characteristics at diagnosis according to age of 4310 patients with ulcerative colitis in a population-based study from northern France
Extraintestinal manifestations
EIMs were present in 5% (n=41) at diagnosis and 9% (n=72) at maximal follow-up including axial or peripheral arthropathies in 37%, skin manifestations in 57% (with erythema nodosum in 47%) and uveitis in 2% of patients. Three cases of primary sclerosing cholangitis (4% of all EIMs) were all diagnosed in UC patients (0.6% of the 474 UC patients).
IBD localisation at diagnosis and at maximal follow-up
A complete examination of the colon was performed in 696/841 (83%) patients and of the small bowel in 54% and 17% of CD and UC patients, respectively. An upper gastrointestinal endoscopy was performed in 121/367 (33%) CD patients.
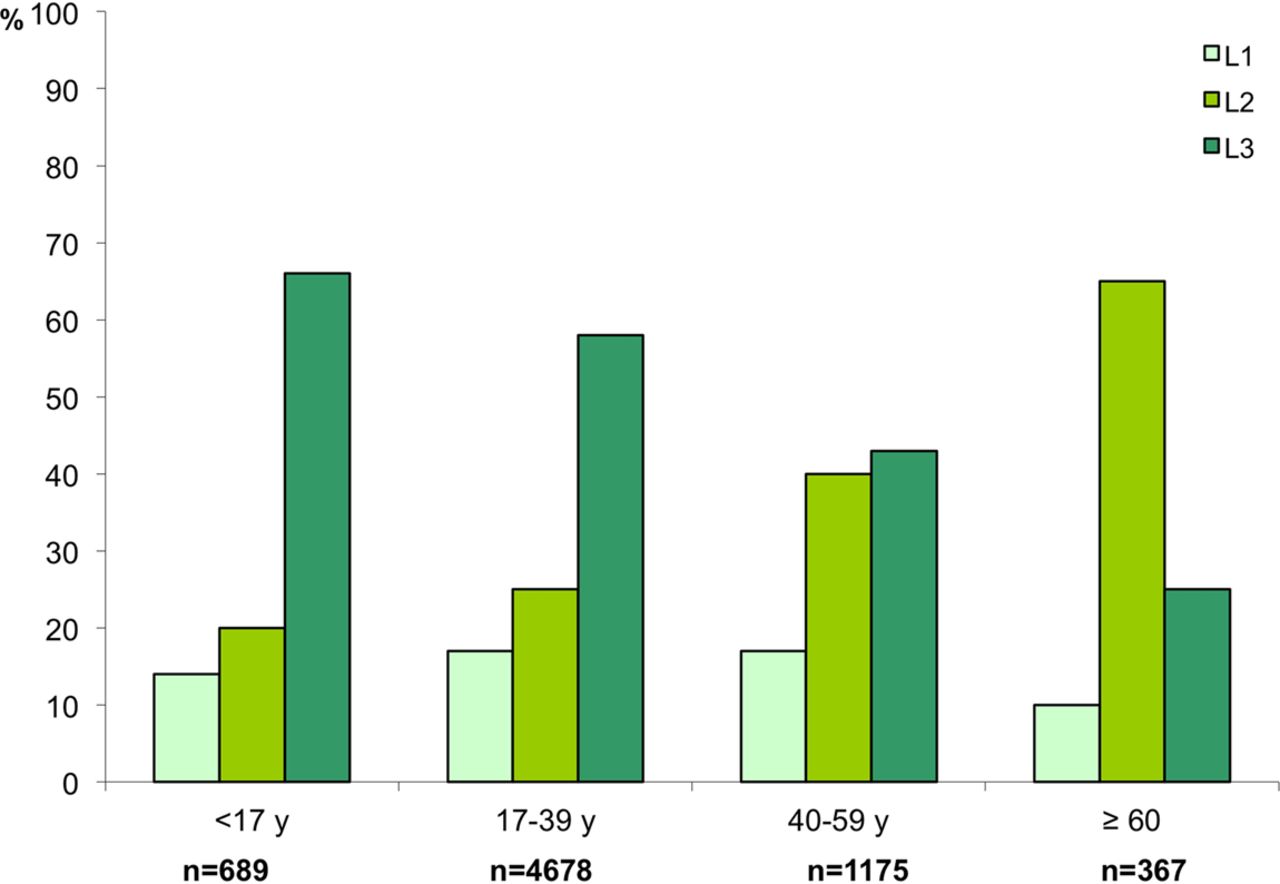
In CD, colonic localisation (L2+L3) was more frequent than in other age groups at diagnosis and maximal follow-up (p=0.002) (figure 1) while involvement of the upper gastrointestinal tract (L4) was found in only 22 (6%) patients and remained stable at maximal follow-up. All together, CD localisation remained stable at maximal follow-up in 92% of patients.
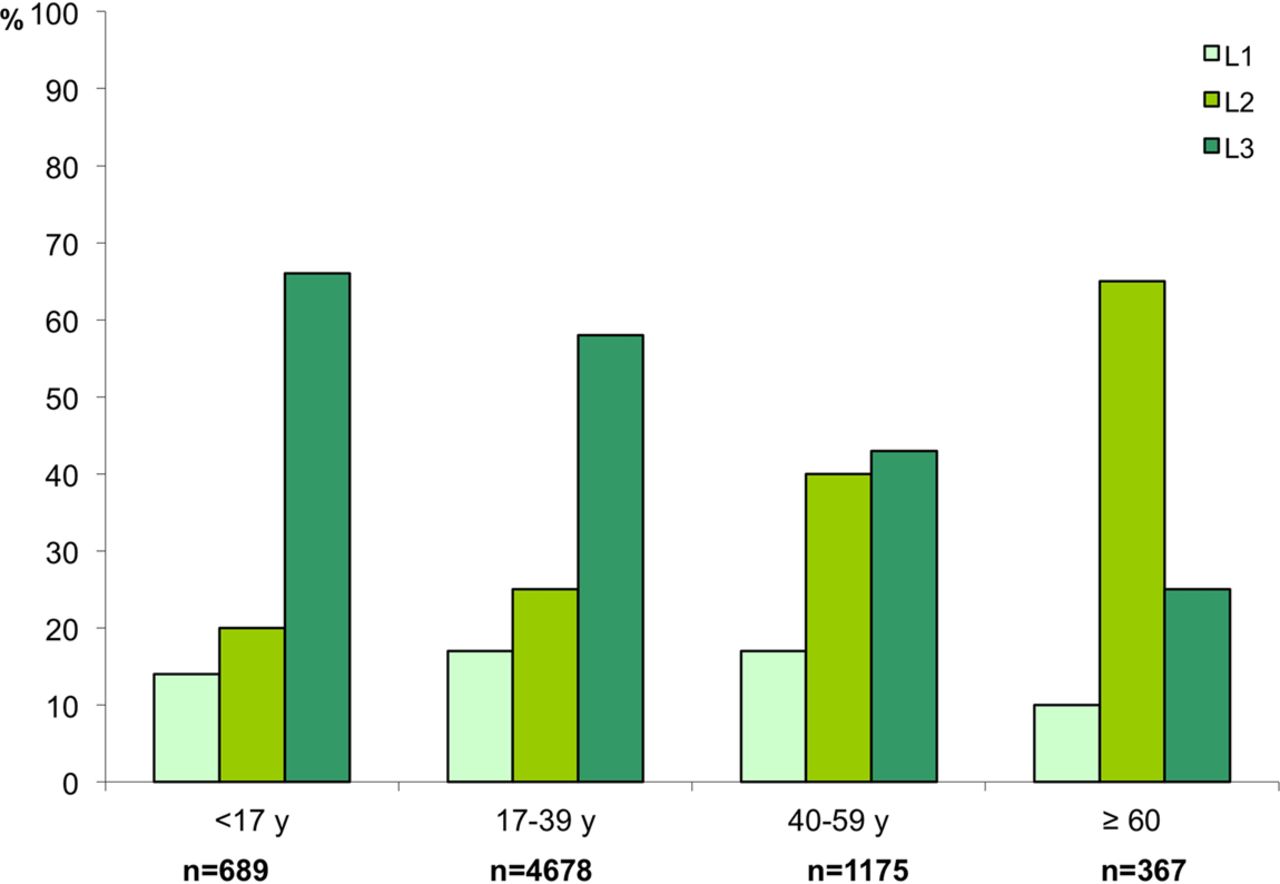
Crohn's disease localisation at diagnosis according to age in 367 elderly-onset patients (>60 years) compared with 689 paediatric-onset patients (<17 years), 4678 patients 17–39 years old and 1175 patients 40–59 years (p=0.002). Disease site was recorded according to Montreal classification with a slight modification (ileal localisation with caecal involvement was considered as a L3 localisation). Pure colonic (L2) and ileocolonic (L3) localisations have been pooled to show the frequency of colonic localisation. Access the article online to view this figure in colour.
In UC, proctitis (E1) was less frequent than in other age groups (p<10−4) (figure 2). Among patients with E1 at diagnosis, 8% progressed to E2 (n=31) and 3% to E3 (n=11) at maximal follow-up and among patients with E2 at diagnosis, 5% progressed to E3 (n=22). All together, UC localisation remained stable at maximal follow-up in 84% of patients.

Ulcerative colitis localisation at diagnosis according to age in 474 elderly-onset patients (>60 years) compared with 213 paediatric-onset patients (<17 years), 2342 patients 17–39 years old and 1189 patients 40–59 years from a population-based study in northern France (p<10−4). Disease site was recorded according to Montreal classification. Ulcerative proctitis (E1) defined as involvement limited to the rectum (ie, proximal extent of inflammation distal to the rectosigmoid junction); left-sided colitis (E2) defined as involvement limited to the portion of the colon distal to the splenic flexure and extensive colitis (E3) defined as involvement extending proximally to the splenic flexure. Access the article online to view this figure in colour.
CD behaviour at diagnosis and at maximal follow-up
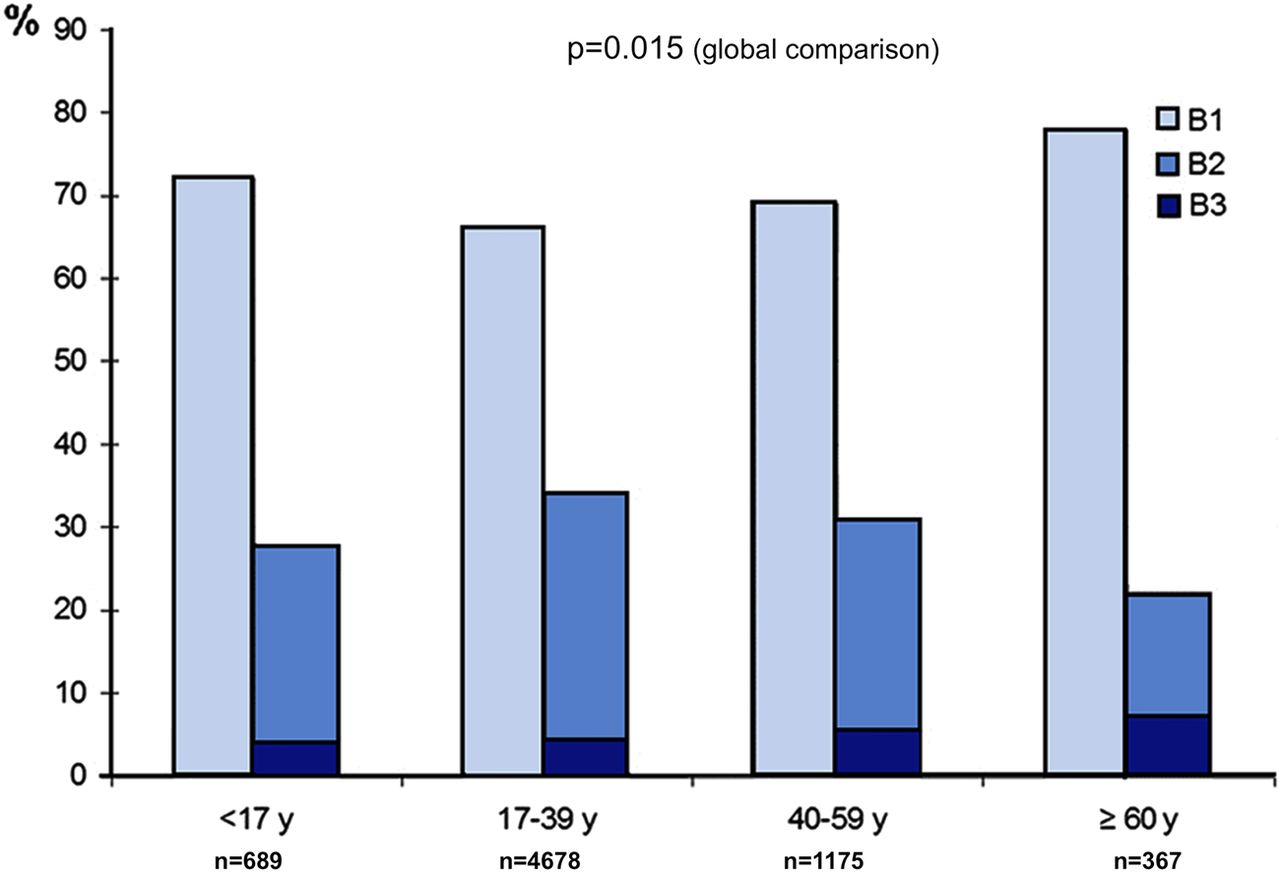
The initial behaviour of elderly-onset CD patients was B1 in 78%, B2 in 17% and B3 in 5% with less complicated behaviour (B2 and B3) than in younger patients (figure 3) (p=0.01). Perianal lesions were present in 8% of patients as compared with 7%, 5% and 6% in the <17, 17–39 and 40–59 years groups, respectively (p=0.015 for global comparison). At final follow-up, behaviour was B1 in 69%, B2 in 19% and B3 in 12% of patients and 17% had perianal lesions. Although this was significantly different (p<10−4) when compared with diagnosis, disease behaviour at follow-up was thus stable in most patients with a progression from uncomplicated to complicated disease in only 9% (figure 4).
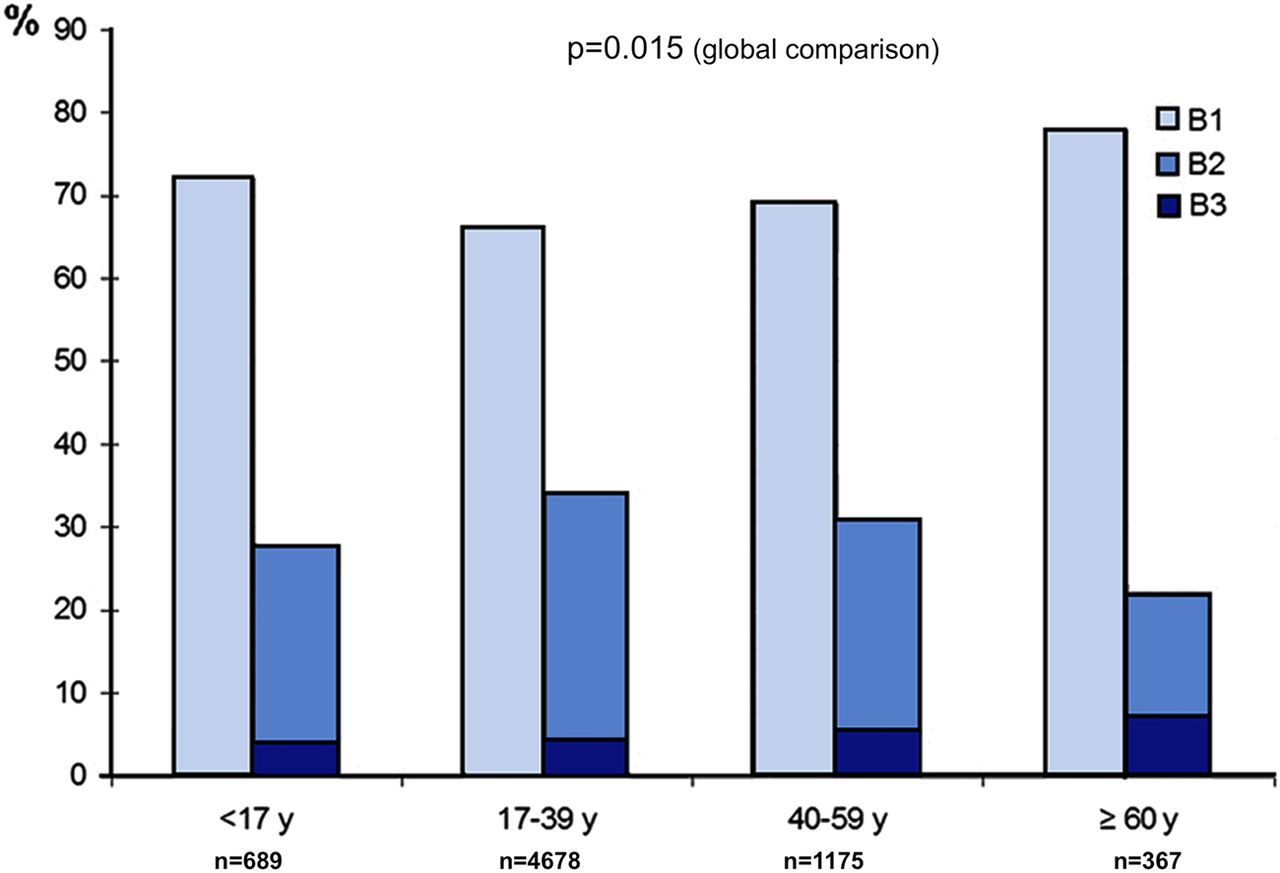
Crohn's disease behaviour at diagnosis according to age in 367 elderly-onset patients (>60 years) compared with 689 paediatric-onset patients (<17 years), 4678 patients 17–39 years old and 1175 patients 40–59 years (p=0.015). Behaviour was recorded according to Montreal classification. Stricturing (B2) and penetrating (B3) behaviours have been pooled to show the frequency of complicated behaviours. Access the article online to view this figure in colour.

Modification of Crohn's disease behaviour after a 15-year duration in 367 elderly-onset patients (>60 years). The disease behaviour was stable in proportion of disease behaviour subgroups with a progression from uncomplicated to complicated disease in only 9% of patients. Access the article online to view this figure in colour.
Medications
5-ASA treatments were given to 628/841 (75%) patients with a similar CP in CD and UC: 68% (95% CI 63% to 73%) at 1 year, 77% (72% to 82%) at 5 years and 80% (75% to 85%) at 10 years in CD and 65% (61% to 70%) at 1 year, 78% (74% to 82%) at 5 years and 84% (80% to 88%) at 10 years in UC (figure 5A).
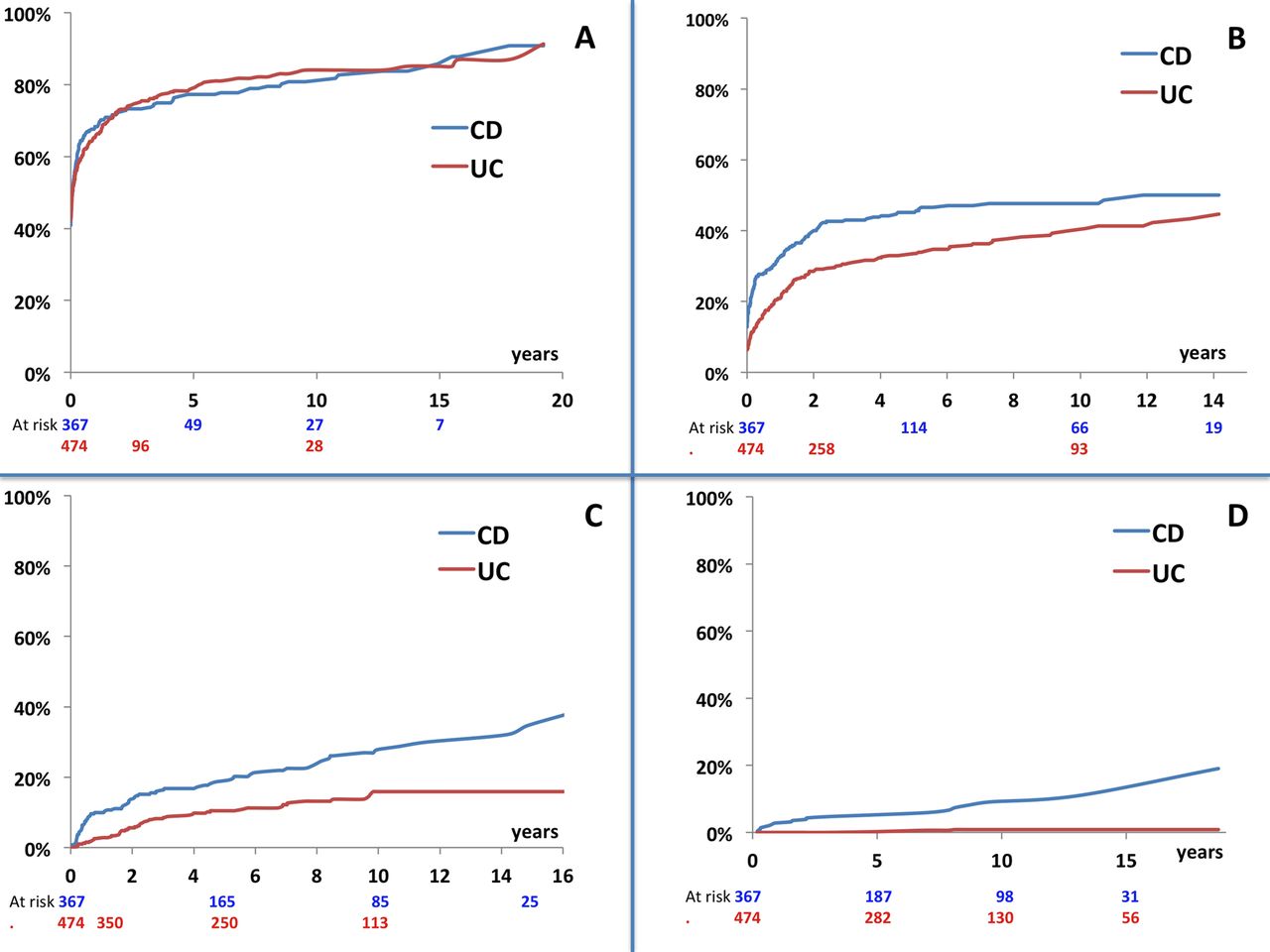
Cumulative risk of receiving different medical treatments in 367 elderly-onset patients with Crohn's disease and 474 elderly-onset patients with ulcerative colitis (UC). (A) In Crohn's disease (CD), cumulative probability of receiving 5-aminosalicylic acid (5-ASA) or sulfasalazine was 0.68 (95% CI 0.63 to 0.73) at 1 year, 0.77 (0.72 to 0.82) at 5 years and 0.80 (0.75 to 0.85) at 10 years from time of diagnosis. In UC, cumulative probability of receiving 5-ASA or sulfasalazine was 0.65 (95% CI 0.61 to 0.70) at 1 year, 0.78 (0.74 to 0.82) at 5 years and 0.84 (0.80 to 0.88) at 10 years from time of diagnosis. (B) In CD, cumulative probability of receiving systemic steroid was 0.32 (95% CI 0.28 to 0.38) at 1 year, 0.45 (95% CI 0.39 to 0.51) at 5 years and 0.47 (95% CI 0.43 to 0.52) at 10 years from time of diagnosis. In UC, cumulative probability of receiving systemic steroid was 0.21 (0.17 to 0.25) at 1 year, 0.34 (0.29 to 0.38) at 5 years and 0.40 (0.35 to 0.45) at 10 years from time of diagnosis. (C) In CD, cumulative probability of receiving immunosuppressants (IS) was 0.10 (95% CI 0.07 to 0.14) at 1 year, 0.45 (95% CI 0.39 to 0.51) at 5 years and 0.47 (95% CI 0.43 to 0.52) at 10 years from time of diagnosis. In UC, cumulative probability of receiving IS was 0.025 (0.01 to 0.04) at 1 year, 0.10 (0.07 to 0.14) at 5 years and 0.15 (0.11 to 0.20) at 10 years from time of diagnosis. (D) In CD, cumulative probability of receiving anti-TNFα therapy was 0.03 (95% CI 0.01 to 0.05) at 1 year, 0.05 (95% CI 0.03 to 0.08) at 5 years and 0.09 (95% CI 0.06 to 0.14) at 10 years from time of diagnosis. In UC, cumulative probability of receiving anti-TNFα therapy was 0.0 at 1 year, 0.004 (0.001 to 0.006) at 5 years and 0.02 (0.01 to 0.03) at 10 years from time of diagnosis. Access the article online to view this figure in colour.
CS therapy was given to 258/841 (31%) patients (41% in CD and 33% in UC). The CP of receiving CS in CD was 32% at 1 year (95% CI 28% to 38%), 45% (39% to 51%) at 5 years and 47% (43% to 54%) at 10 years (figure 5B). The CP in UC was 21% (17% to 25%) at 1 year, 34% (29% to 38%) at 5 years and 40% (35% to 45%) at 10 years (figure 5B). The median duration of CS exposure was 5.5 months (3–13) in CD and 4.6 months (2.6–9.5) in UC. Forty-six (18%) patients became CS-dependent (9% in CD and 20% in UC) and 23 (9%) were CS-resistant at 1 year (6% in CD and 9% in UC).
ISs were given to 133/841 (16%) patients (23% in CD and 10% UC), predominantly azathioprine (n=128) and less often methotrexate (n=18). The CP of receiving IS in CD was 10% (7% to 14%) at 1 year, 18% (14% to 24%) at 5 years and 27% (21% to 33%) at 10 years (figure 5C). The CP in UC was 2.5% (1% to 4%) at 1 year, 10% (7% to 14%) at 5 years and 15% (11.5% to 20%) at 10 years (figure 5C). The median time from IBD diagnosis to IS start was 1.9 (0.4–5) years and cumulative duration of treatment was 19 (5–58) months.
Anti-TNFα therapy was given to 26 CD patients (7%) with a CP of 3% (1% to 5%) at 1 year, 5% (3% to 8%) at 5 years and 9% (6% to 14%) at 10 years (figure 5D). The median time from CD diagnosis to anti-TNFα start was 2 (1–8) years; 24 patients (6%) received IFX and four adalimumab. In UC only four patients received IFX with a median time from diagnosis to start of 6 (5–8) years.
Surgery
IBD diagnosis was made during surgery in 55/841 (6.5%) patients, 48 (13%) in CD and 7 (1.4%) in UC. At least one intestinal resection was performed in 103/367(28%) CD patients of whom 24/367 (7%) had a definitive stoma at the same time as the first intestinal resection. The CP of surgery was 18% (14% to 23%) at 1 year, 27% (23% to 32%) at 5 years and 32% (27% to 38%) at 10 years (figure 6). In UC, colectomy was performed in 34 (7%) patients: 14 had a subtotal colectomy with ileorectal anastomosis, three a coloprotectomy with IAA and 17 (50%) a definitive stoma. The CP of colectomy was 4% (2% to 6%) at 1 year, 8% (5% to 11%) at 5 years and 8% (6% to 12%) at 10 years (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative risk of surgery in 367 elderly-onset patients with Crohn's disease and 474 elderly-onset patients with ulcerative colitis. In Crohn's disease, cumulative probability of first intestinal resection was 0.18 (95% CI 0.14 to 0.23) at 1 year, 0.27 (95% CI 0.23 to 0.32) at 5 years and 0.32 (95% CI 0.27 to 0.38) at 10 years from time of diagnosis. In UC, cumulative probability of colectomy was 0.04 (0.02 to 0.06) at 1 year, 0.08 (0.05 to 0.11) at 5 years and 0.08 (0.06 to 0.12) at 10 years from time of diagnosis. Access the article online to view this figure in colour.
At a 10-year follow-up, 54% of CD and 66% of UC patients were never exposed to any CS, IS or anti-TNF-therapy nor operated on while those percentages were 32% and 52% in paediatric-onset CD (p=0.0025) and UC (p=0.0049), respectively (see online supplementary figures S1 and S2).
Risk factors for surgery
L1 and L3 localisations and B2 and B3 behaviour at diagnosis of CD were associated with an increased risk of intestinal resection while the use of CS was associated with a decreased risk. Age, gender, EIMs, perianal lesions and use of IS did not influence this risk. In the multivariate analysis, a complicated behaviour (B2 or B3) was the only risk factor for intestinal resection (2.7 (1.6–4.8); p<0.001) while CS use was associated with a reduced risk (0.5 (0.3–0.8); p=0.005) (table 3).
Bivariate and multivariate analysis of variables associated with the risk of first intestinal resection in 367 elderly-onset patients with Crohn's disease
Disease localisation at UC diagnosis and exposure to CS were associated with an increased risk of colectomy. Age, gender, EIMs and use of IS did not influence this risk (table 4). In the multivariate analysis CS use was the only factor associated with an increased risk of colectomy (HR: 2.2 (1.1 to 4.6); p=0.03).
Bivariate and multivariate analyses of variables associated with the risk of colectomy in 474 elderly-onset patients with ulcerative colitis
Discussion
This is to our knowledge the largest population-based study of elderly-onset IBD reported to date. One out of 20 incident cases of CD and one out of eight incident cases of UC occurred in people aged >60 years in our geographical area of northern France. Elderly-onset CD was characterised by the predominance of colonic localisation often associated with perianal disease, and an uncomplicated behaviour with less progression over time than in younger patients. Elderly-onset UC was characterised by the predominance of left-sided and extensive colitis at diagnosis and rare disease extension at follow-up. As for medical therapies, almost all elderly IBD patients received 5-ASA, approximately 40% received systemic steroids, less than 20% IS and 2% anti-TNFα therapy. Only 16% of elderly-onset patients were operated on at 10 years from diagnosis. Taken together, the course of elderly-onset IBD seems less aggressive than is usually reported in younger patients: more than half of the patients were never exposed to any drug except 5-ASA nor were they operated on.
A major strength of the study was the availability of data from a large population of >60 -year-old (median age of 70 years in CD and 69 years in UC) patients diagnosed with IBD according to well-defined criteria.15 This allowed us to properly exclude various clinical situations such as diverticulitis and ischaemic colitis that may hinder the diagnosis of IBD in this age bracket. In addition, median follow-up was 6 years, and 80% were followed for at least 2 years, so that our data accurately portrayed the course of IBD in elderly patients in a period of time where access to IS and anti-TNF therapies was widespread in our region.
Incidence of elderly-onset IBD (2.6/105 inhabitants in CD and 3.1 in UC) is similar in our region to other European studies.11 ,18–28 Incident cases of IBD occurring at >60 years of age represented 9% of our whole population-based IBD cohort confirming the rarity of the diagnosis.8 Even though northern France is characterised by a higher overall incidence of CD than UC, UC was prominent in the elderly population as consistently observed in population-based studies.25 ,29–31 One hypothesis may be the influence of smoking cessation in the elderly as a prevention of cardiovascular events. This hypothesis could be reinforced by the fact that UC localisation at diagnosis was strikingly similar between the elderly-onset and young age-onset groups with proctitis representing only one-third of the population as compared with more than 50% in the middle age groups. This more extensive phenotype may again reflect the influence of no smoking or smoking cessation in the extreme ages. This will require further investigation.32
Clinical presentation of IBD was different in the elderly people and in younger age groups. There were less diarrhoea, abdominal pain, EIM, weight loss and fever, and more rectal bleeding in CD; the frequent colonic localisation may account in part for these findings. There were less rectal bleeding, abdominal pain and systemic symptoms in UC. This atypical presentation that may impose for other clinical conditions, including rectal or colonic cancer, may well explain an early referral to endoscopy and the short interval between symptoms and diagnosis that was observed as well as the striking percentage (6.5%) of patients in whom the diagnosis was made at surgery. The process of IBD diagnosis can be separated into three different phases: the time between the occurrence of first symptoms and the consultation with the general practitioner; the time between this first consultation and referral to a gastroenterologist; the time required by the gastroenterologist to make the diagnosis. Wagtmans et al33 have shown that the two first steps were actually shorter in patients over 40 years of age than in younger patients. The fear of cancer, the greater impact of digestive symptoms including rectal syndrome and urgency in a patient with another debilitating condition may explain an early awareness and referral despite a less typical clinical presentation.
Phenotypes of CD at diagnosis in elderly-onset CD are quite consistent with the literature, with colonic CD being more common than small bowel or ileocolonic disease and with a greater proportion of inflammatory, uncomplicated behaviour.6–10 34–42 Disease localisation was stable over time as observed in adults, but one important finding in our study was the relative rarity of behaviour progression which looks quite unique to this population. At final follow-up only 30% of patients had B2/B3 behaviour as compared with more than 50% in younger patients. In UC disease localisation was stable with only 16% of patients with progression over time which is similar to the rate reported by Langholz et al43 (17% at 6 years) in a Danish population and in sharp contrast with the 49% rate of extension that we reported in our paediatric population.44 This less aggressive course of IBD in the elderly would need to be taken into account when discussing therapeutic strategies.33 ,45 ,46 A note of caution in interpreting this data is that the frequency of total colonoscopy performed during the period of follow-up in the paediatric and elderly population was not registered in the database.
The wide use of 5-ASA among patients with CD is in agreement with other population-based cohorts,47 thus suggesting a possible role for these compounds in patients with mild CD. However, evidence indicates that 5-ASA is minimally effective as compared with placebo in CD.48 Still, this was by far the most prescribed treatment in elderly patients likely because of its perceived favourable side profile. On the other side, not surprisingly and in accordance with guidelines 49 the vast majority of UC patients were exposed to 5-aminosalicylates which also likely reflects their perceived safety in this fragile population. Even though systemic steroids were the drugs most often prescribed, the cumulative exposure (45% and 33% at 5 years in CD and UC, respectively) in elderly IBD people was actually less than in previous population-based studies in which rates of 43% at 1 year 46 and almost 75% at 5 years have been reported.50–52 The rates of steroid dependence and resistance were also similar to other adult populations. There has been an increase in the use of IS and biologicals in patients with IBD in the recent years. Remarkably in our elderly-onset cohort, only 27% of CD patients and 16% of UC patients received IS at a 10-year follow-up which is half of what has been described in the whole IBD population and only 3% were exposed to anti-TNF therapy. These small percentages, also observed in previous studies from USA and Europe, may not be surprising given the low percentage of steroid dependence and the fear of side effects in elderly people.6–11 Recent literature actually confirmed that ageing is a risk factor for lymphoma and skin cancer in patients exposed to IS 12 ,53 and of serious infections in those receiving IFX.13
Several observations related to surgery look quite unique to this population. First, while the cumulative incidence of surgery was in the low percentiles of the literature, more than half of patients were operated on either at diagnosis or during the first year after diagnosis. In a study by Lakatos et al9 old age was also a predictive factor for an early resort to surgery in CD. This may reflect fear of misdiagnosis and reluctance for prescribing immunosuppressive drugs when surgery is a reasonable alternative. In UC colectomy rate was in accordance with previously published data with percentages varying from 3% to 6% at 1 year,54–56 3% to 8% at 5 years 55–58 and 10% at 10 years.56 However two major differences were noted: first, the maximal rate of colectomy was already observed at 5 years suggesting an earlier resort to surgery than in younger adults, as already suggested by Wagtmans et al33; second, coloprotectomy with IAA was performed in less than 10% of patients most likely because worse pouch survival, functional outcome and quality of life have been reported in elderly UC patients.59 ,60 In our IBD cohort, a definitive stoma was performed in 5% of patients in the whole cohort. The risk for permanent stoma is not well documented in IBD population. It was estimated at 0.23% per year 61 in a Swedish CD population-based study. This procedure may be more acceptable in elderly than in younger patients.
When looking at risk factors for surgery in CD, B2 and B3 behaviours were risk factors as consistently reported,62–64 but quite strikingly exposure to systemic steroid was associated with a strong reduced risk. This is in sharp contrast with our paediatric data and the study performed in Olmsted County where treatment with systemic steroid was associated with an increased risk for surgery.44 ,63 It has been repeatedly shown that systemic steroids do not alter the natural course of CD and may actually increase the risk of complications. The situation may be different in old patients where most of the patients had an inflammatory form responding well to systemic steroids with no progression towards a complicated behaviour.
In conclusion, the patterns of phenotypic presentation, disease progression, medical and surgical treatments look quite unique in elderly-onset patients with IBD at a population level. Several observations from this study that challenge previous statements mostly coming from referral centres or small series would need to be taken into account by clinicians when discussing risk/benefit ratios of therapeutic strategies in these patients.
Acknowledgments
The authors wish to thank the interviewing practitioners who collected data: N Guillon, I Rousseau, A Pétillon, B Turck, P Fosse, S Auzou, M Leconte, C Le Gallo, D Rime. The authors thank all adult and paediatric gastroenterologists who participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure 1
- Data supplement 2 - Online figure 2
Footnotes
-
Contributors CC: generation, collection, assembly and interpretation of data; drafting of the manuscript. JS: study design; analysis and interpretation of data; statistical analysis; drafting and critical revision of the manuscript and approval of the final version of the manuscript. GS: concept and study design; interpretation of data; drafting and critical revision of the manuscript and approval of the final version of the manuscript. MF: acquisition of data; interpretation of data. VM: acquisition of data. J-EL: acquisition of data. FV: interpretation of data. J-LD: concept and study design; interpretation of data; critical revision of the manuscript. AC: concept and study design; interpretation of data; critical revision of the manuscript. LD: concept and study design; interpretation of data. LP-B: concept and study design; interpretation of data. EL: concept and study design; interpretation of data; critical revision of the manuscript. J-FC: concept and study design; interpretation of data; drafting and critical revision of the manuscript and approval of the final version of the manuscript. CG-R: concept and study design; acquisition of data, interpretation of data; drafting and critical revision of the manuscript and approval of the final version of the manuscript.
-
Funding EPIMAD is organised under an agreement between the Institut National de la Santé et de la Recherche Médicale (INSERM) and the Institut de Veille Sanitaire (InVS) and also received financial support from the François Aupetit Association, the Lion's Club of Northwestern France, Ferring Laboratories, the Société Nationale Française de Gastroentérologie, Lille, Amiens and Rouen University Hospital. This study was supported by a grant from the French Ministry of Health (PHRC I 2010–n°13–20) and by Astra-Zeneca Company (IRMAD Grant). This work was presented in part at the American Gastroenterology Association meeting held in San Diego in 2012.
-
Competing interests None.
-
Ethics approval French Health Minister.
-
Provenance and peer review Not commissioned; externally peer reviewed.