Article Text

Abstract
Background: Twenty four hour oesophageal pH monitoring is frequently used to quantify the association between a patient’s symptom and gastro-oesophageal reflux. Three indices (symptom association probability (SAP), symptom index (SI), and symptom sensitivity index (SSI)) are used to quantify and establish this relation.
Aims: The aim of the present study was to compare these indices against the omeprazole test (OT) as an objective indicator of reflux induced symptoms.
Methods: Fifty two patients with a predominant symptom of heartburn were enrolled from gastroenterology and primary care clinics. Baseline symptom score was calculated at the fist visit. All patients underwent 24 hour oesophageal pH monitoring, and symptom-reflux association indices were calculated. All patients were placed on high dose omeprazole (40 mg in the morning, 20 mg at night) after completion of pH monitoring and symptom score was recorded again after one week.
Results: Thirty eight patients completed the study. All three indices were significantly related to each other (p<0.001). SAP and SSI (with a new cut off of 1.3, but not with the commonly used 5%) had statistically significant relations with OT (p<0.05 for both). SSI had the highest positive and negative predictive values and sensitivity. The specificity of SSI and SAP was equal and lower than SI. Areas under the receiver operating characteristic (ROC) curve for the three indices were not significantly different from each other or from a hypothetical non-discriminating test. Per cent time pH <4, sex, and age had no relation to OT and no effect on its correlation with association indices. No cut off point could be found at which the results of SI could be related significantly to the OT results.
Conclusion: SAP and SSI are significantly related to symptomatic response to high dose omeprazole; however, they are far from perfect, with a significant number of discordant cases as well as relatively small areas under the ROC curves. We suggest that the new cut off of 1.3 be used for SSI in the future. Further research is needed to identify possible methods to improve the discrimination power of these indices or to identify possible patient characteristics that may affect this relation.
- GOR, gastro-oesophageal reflux
- GORD, gastro-oesophageal reflux disease
- OT, omeprazole test
- SAP, symptom association probability
- SI, symptom index
- SSI, symptom sensitivity index
- ROC, receiver operating characteristic
- PPI, proton pump inhibitor
- gastro-oesophageal reflux
- heartburn
- symptom index
- symptom association probability
- symptom sensitivity index
Statistics from Altmetric.com
- GOR, gastro-oesophageal reflux
- GORD, gastro-oesophageal reflux disease
- OT, omeprazole test
- SAP, symptom association probability
- SI, symptom index
- SSI, symptom sensitivity index
- ROC, receiver operating characteristic
- PPI, proton pump inhibitor
- gastro-oesophageal reflux
- heartburn
- symptom index
- symptom association probability
- symptom sensitivity index
Ambulatory 24 hour pH monitoring is no longer universally accepted as “the gold standard”1,2 for diagnosis of gastro-oesophageal reflux (GOR) but it is routinely used for assessment of the possible associations between symptoms and reflux.2–4
Three measures (symptom sensitivity index (SSI), symptom index (SI), and symptom association probability (SAP)) were proposed as numerical scales to quantify the symptom-reflux association, and therefore help to decide whether symptom episodes that occurred during the recording were related to GOR.2–6
SI is defined as the percentage of reflux related symptom episodes6 and SSI the percentage of symptom related reflux episodes.3
These two indices however have common weak points: firstly, they have arbitrary cut off points,1 and secondly, they focus on the frequency of simultaneous occurrence of reflux and symptoms while ignoring the frequency of “non-associated” reflux and symptom episodes.7
In order to circumvent these shortcomings, a new index (SAP), based on statistical analysis (cross tabulation) of a contingency table consisting of four possible combinations of reflux and symptoms, was suggested as a more statistically meaningful way of investigating this association3,6–8 and the p value of <0.05 (Fisher’s exact test) proposed as its cut off point.2,4,7
Despite the apparent progress in sophistication, none of the above mentioned indices have been prospectively validated against an independent criterion of diagnostic accuracy, such as symptomatic response to antireflux therapy.2 In fact, the major problem is lack of an objective and reliable gold standard test—independent of pH monitoring—to which these indices can be compared.8,9
A number of studies suggest a short course of a high dose of a proton pump inhibitor (PPI) such as omeprazole as a practical, non-invasive, and relatively reliable test in establishing a cause and effect relation between GOR and symptoms.1,10–12 Although these “PPI tests” are far from ideal for diagnosing gastro-oesophageal reflux disease (GORD),8,9 they are the only available objective independent measures against which these indices can be tested. It also should be noted that the final purpose of an association index is to select those patients whose symptoms are related to acid reflux and therefore should be responsive to acid reduction therapy.
The aim of the present study was to prospectively validate SAP, SI, and SSI against symptomatic response to a PPI trial (omeprazole test (OT)).
MATERIALS AND METHODS
Patients
Fifty two consecutive patients with a predominant symptom of typical heartburn were initially enrolled in the study from gastroenterology and primary care clinics affiliated to Shiraz University of Medical Sciences. All patients consented to the protocol procedure.
Heartburn was defined as a burning sensation behind the sternum with radiation from the epigastrium towards the mouth. Inclusion was limited to patients with a history of at least three episodes of heartburn per week in the one month period prior to entry. Exclusion criteria were a history of peptic ulcer disease, gastrointestinal surgery, malignancy, use of PPIs in the previous four weeks, or H2 blockers and promotility agents in the previous week, and use of prescription non-steroidal anti-inflammatory drugs. Medication for other illnesses continued at constant doses when possible.
Study protocol
At entrance to the study a questionnaire, including demographic and upper endoscopy data and a heartburn severity and frequency score,10–12 was completed. Total heartburn score was calculated by multiplying grades of severity and frequency (table 1).
Grading of severity and frequency of heartburn
Endoscopy data were not used in the final analysis because the reliability of the initial data could not be confirmed, and 60% of patients did not consent to repeat endoscopy. Later, all patients underwent ambulatory oesophageal pH monitoring and then a trial of high dose omeprazole (generic omeprazole; Exir Pharmaceutical Company, formerly Lorestan Pharmaceutical Company, Lorestan, Iran, copied from UQUIFA Pharmaceutical Company Spain), 40 mg in the morning, 20 mg at night, for seven days.
The same questionnaire was completed again at the end of the omeprazole trial by one of the investigators, unaware of the pH monitoring results. A reduction of >50% in the heartburn score or reaching zero from any previous score was considered a positive OT.1,11
Ambulatory 24 hour pH monitoring
After an overnight fast, the pH probe (Zinetics 24 ME; Medtronic Functional Diagnostics, Tonsbakken, Denmark) was positioned transnasally 5 cm above the manometrically determined lower oesophageal sphincter and secured to the nose and cheek. A reference electrode was attached to the chest skin. The pH electrode was calibrated before and after the recording using pH 7 and 1 buffer solutions.
Patients registered periods of eating, supine position, and heartburn using a written diary as well as pressing buttons on the data logger. Medtronic μdigitrapper 4Mb flash series (Synetics Medical AB, Stockholm, Sweden) was used as the data logger. Patients were encouraged to pursue their usual everyday activities and diet. After completion of the study, recorded data were transferred to a computer and analysed using dedicated software (Multigram, GI edition, version 6.31, Gastrosoft Inc). All tracings were reviewed by one of the investigators to reveal any technical difficulties.

Distribution of symptom sensitivity index in the study population.
Data analysis
SI and SSI were calculated as described by Wiener and colleagues6 and Breumelhof and colleagues,3 respectively. For calculation of SAP, consecutive two minute periods of pH recording were analysed for the presence of reflux and symptoms. A symptom episode was considered as reflux positive if either of the two minute periods preceding or following the start of the symptom was reflux positive (pH <4 for ⩾5 seconds). A contingency table was constructed and Fisher’s exact test was used to calculate the p value according to Weusten and colleagues.4 SAP was calculated as (1.0−P)×100%.
Values >1.3 (based on the findings of the current study), ⩾50%, and >95% were considered as indicators of significant symptom-reflux association for SSI, SI, and SAP, respectively.4 Cross tabulation and the χ2 test were used to identify any significant relationships between the results of the OT (responder, non-responder) and each association parameter (reflux associated, non-reflux associated).
Statistical analyses were done by SPSS statistical software package(version 11.5.0 SPSS Inc, 1989–2002). Comparison of receiver operating characteristic (ROC) curves was performed using MedCalc statistical software package (version 7.6.0.0, 1993–2004).
RESULTS
Fifty two patients were initially enrolled into the study. Fourteen had to be withdrawn from further analysis for various protocol violations: seven due to lack of symptoms during the pH recording period, six due to unacceptable quality of recorded data (significant error in post test calibration of pH electrode in three and electrical interferences, presumably due to loosening of the external reference electrode, in three), and one patient could not tolerate the catheter for more than six hours. Patient’s characteristics are summarised in table 2.
Characteristics of the 38 patients who completed the study
A total number of 4589 reflux episodes and 141 symptom episodes were registered in the 38 patients who completed the study. Table 3 shows the statistical characteristics of the registered reflux and symptom episodes.
Statistical characteristics of the registered reflux and symptom episodes
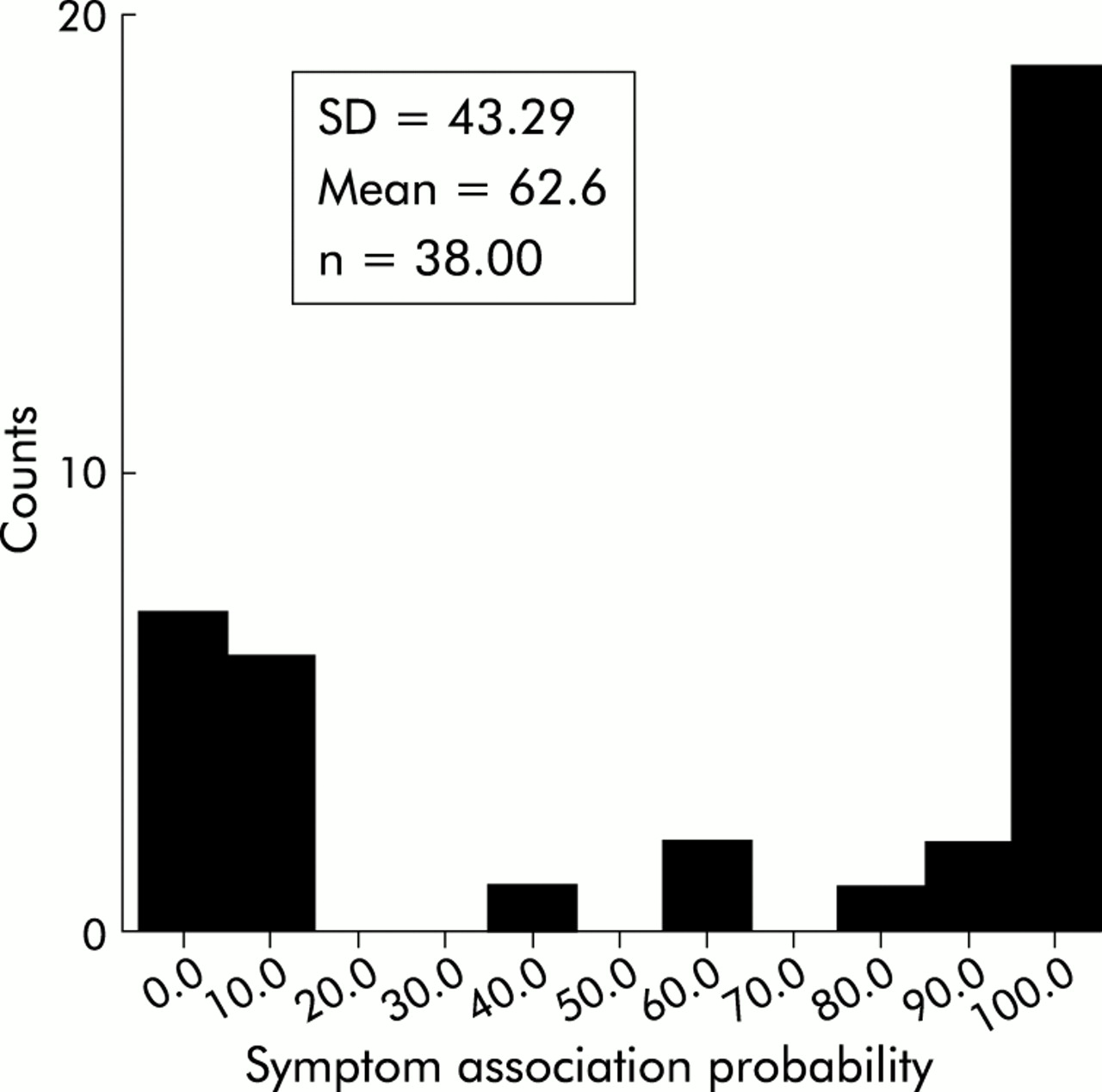
Mean acid exposure time (pH <4) in the studied groups was 128.1 minutes (4–1444). Mean per cent time during ambulatory pH monitoring in which pH was <4 was 9.1% (SD 2.37; range 0.1–53.7%): 42.1% of patients had pH <4 for more than 4% of the recoded time. Figures 1–3 show the distribution of SI, SSI, and SAP in these patients.

Distribution of symptom index in the study population.
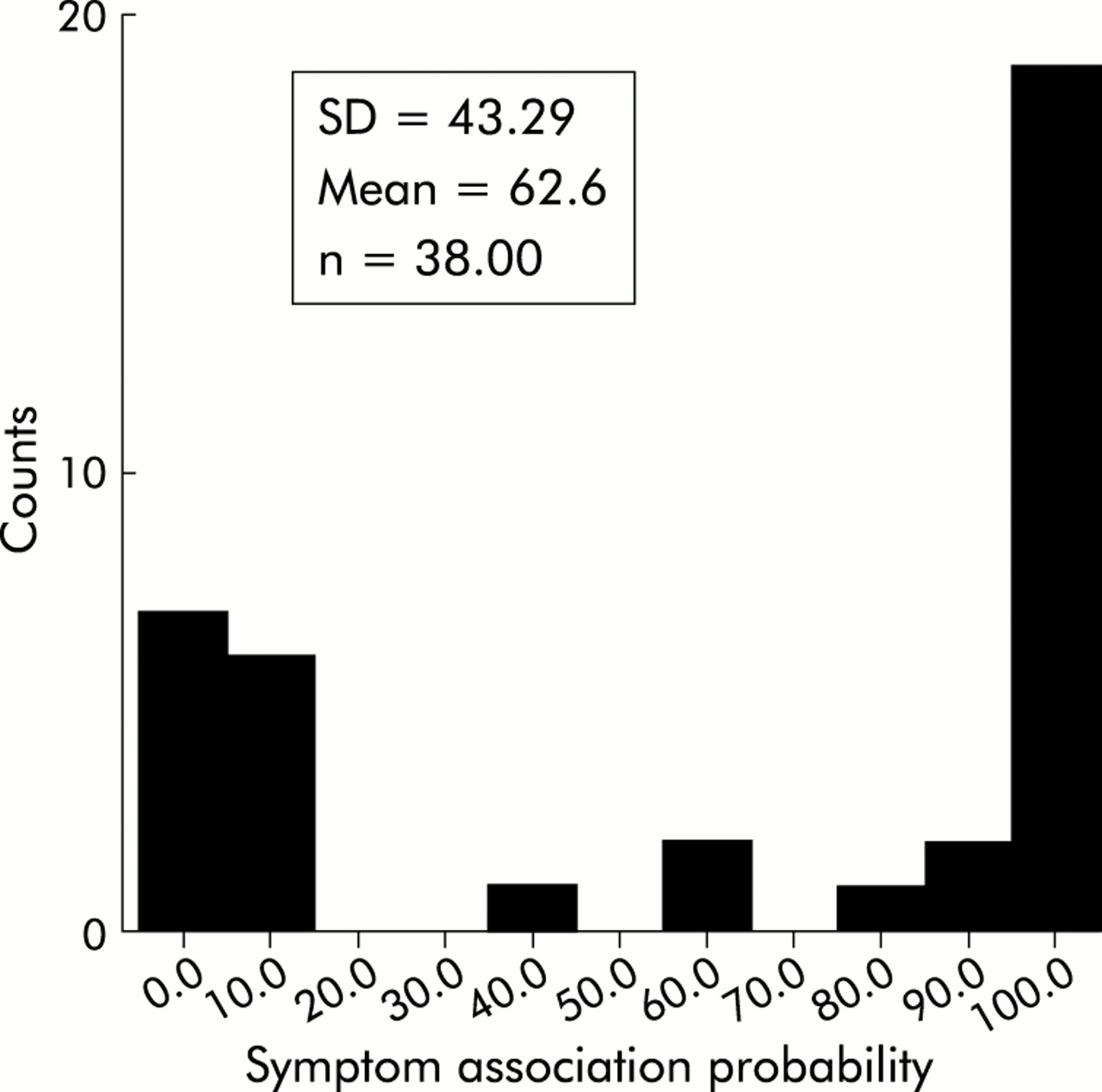
Distribution of symptom association probability in the study population.
The OT was positive in 23 patients (51.1%). In the OT positive group, 13 (56.52%) had complete disappearance of symptoms and 10 (43.48%) had more than 50% improvement in symptom score. Of those patients with a negative test, nine (60%) had less than 50% improvement and six (40%) had no change in the symptom score. No age or sex differences were demonstrated between omeprazole responders and non-responders (p values 0.611 and 0.214, respectively). There were also no significant differences between OT positive versus negative groups in total time pH <4 (p = 0.497, Komolgorov-Smirnov test).
Although there were more patients with abnormal pH monitoring results in the omeprazole responder versus non-responder group (52.2% v 36.3%), the difference was not statistically significant (Pearson χ2 = 2.423, p = 0.182).
A statistically significant association was found between the OT results and SAP (Pearson χ2 = 5.397, two sided significance = 0.02, Fisher’s exact test 0.045 and 0.022 for two and one sided significance, respectively). No significant relation was found between OT and SSI (using cut offs of 5% and 10%) (Pearson χ2 2.42 and 1.54 and p values 0.12 and 0.22, respectively). However, the relation was significant when a level of more than 1.3 (the most suitable point on the ROC curve) was used as the cut off (Pearson χ2 = 8.19, p<0.05).There was no significant relation between SI and the results of the OT using significance levels of 10, 15, 20, 25, 30, 35, 40, 45, 50, 55, 60, 65, 70, 75, 80, 85, 90, and 95 (p value >0.05, Pearson χ2). Figure 4 shows the concordance rate of each of the association indices with OT.

Per cent concordance of symptom sensitivity index (SSI), symptom association probability (SAP), and symptom index (SI) with the omeprazole test.
Although SSI had the highest concordance rate with OT, it was unable to predict its results in 26.3% of patients. There were no differences in sex, age, or level of acid exposure between the concordant versus discordant groups for either SAP or SSI. SSI also had the highest sensitivity and negative predictive value for OT (table 4). It should be noted that with the commonly used level of >5%, SSI had lower concordance, sensitivity, and predictive values than SAP. The specificity of SSI and SAP was equal and less than SI (table 4).
Comparison of predictive values, sensitivity, and specificities for the symptom association probability (SAP), symptom sensitivity index (SSI), and symptom index (SI)
Statistically significant associations were found between SAP and the two other variables (SI and SSI) using bivariate correlation (Spearman’s rho 0.793 and 0.604 and p value 0.000 for both). SI and SSI were also significantly related (Spearman’s rho = 0.677 and p value = 0.000). Mean SSI was significantly higher in the OT positive versus the OT negative group (Komolgorov-Smirnov test Z = 1.424, p = 0.035) but the difference for the two other indices was not statistically significant.
Comparison of mean numbers of symptom episodes in the group with a positive OT and negative SAP with both concordant groups and the group with a negative OT and a positive SAP showed significantly lower numbers of symptom episodes in the first group (Kruskall-Wallis non-parametric test, p<0.05 for both relations). The same was also true for the mean number of symptom episodes and SSI (Kruskall-Wallis non-parametric test, p<0.05 for both relations) (table 5). No difference was found for the number of reflux episodes between these groups.
Comparison of mean number of symptom episodes in the three groups classified on the basis of correlations between the omeprazole test (OT) and symptom association probability (SAP) or symptom sensitivity index (SSI)
Construction of ROC (receiver operating characteristic) curves for the three association indices showed that although SSI had the largest area under the curve, none of the indices had enough discrimination power to be significantly different from a hypothetical non-discriminating test in prediction of the results of OT (fig 5). There were no statistically significant differences between area under the ROC curve for each of the above mentioned indices (p>0.05 for all, Hanley and McNeil method).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of receiver operating characteristic (ROC) curves for symptom association probability (SAP), symptom index (SI), and symptom sensitivity index (SSI).
DISCUSSION
In our study, SI had the poorest performance of all association indices, with the highest discordance rate as well as absence of any cut off point at which the relation of its results with OT could reach a statistically significant level. Considering the fact that the final purpose of an association index is to provide a yes or no answer to the question of reflux-symptom association, absence of an objective meaningful cut off point makes SI almost useless.
SAP and SSI (with the new cut off point) had statistically significant associations with the results of the OT but their associations were far from ideal, with discordance rates of 32% and 26%, respectively. SSI had the highest positive and negative predictive values, sensitivity, and concordance for the results of OT.
As SAP is a statistical parameter showing the presence or absence of a non-random relation between acid exposure (measured on the basis of the selected threshold) and perceived symptoms, the presence of discordance between SAP and OT reveals major defects in our understanding of the symptom production process in GORD. The superior performance of SSI in terms of sensitivity, concordance, and predictive values compared with SAP, despite the more statistically sound basis for calculation of the latter, also cannot be explained easily and may be related to the same defects. Theses defects may include inability of the present indices to take into account the possible role of non-acid reflux and application of an identical threshold in different patients with different symptoms and (most likely) different levels of visceral sensitivity. It should be noted that the imperfect nature of OT as a gold standard may also affect these relations. Also, the areas under the ROC curves for these indices were not significantly different from each other and therefore the possible practical importance of the modest differences observed between their sensitivities, specificities, and predictive values will be minimal.
With all three indices, the number of discordant cases with a positive OT and a negative association index was higher than discordant cases with the reverse situation (21% v 10.5% for SAP). For 21% with a positive OT but a negative SAP, placebo response to omeprazole with no real reflux induced symptom is one of the possibilities which can be tested in a double blind placebo controlled study. On the other hand, this group had a significantly lower number of symptom episodes compared with the two other groups (concordant group and those with a negative OT and positive SAP). It is noteworthy that the same relation was found between SSI and number of symptom episodes (table 5). A possible explanation is that these association indices may have lower sensitivities for detection of symptom-reflux associations in patients with lower numbers of symptoms during pH recordings and may require modifications in this group.
For the group with a negative OT and positive SAP, repeat pH monitoring while receiving omeprazole may show whether this combination is due to the ineffectiveness of omeprazole in suppressing acid reflux, or whether symptoms are induced by factors other than acid reflux. The relatively low percentage of patients with significant acid reflux in our study population—all suffering from symptoms that are considered typical of GOR—was also reported in other recent articles13 and may be related to differences in perception of constant stimuli between different patients.14
Contrary to previous studies4 in which SAP had a significant relation only with SI, in our study, all of these indices were significantly related to each other. Failure of the association indices to predict the results of OT better than a hypothetical non-discriminating test, as shown by the ROC curves, may be related to their inherent shortcomings—which may not be able to account for all of the factors involved in symptom production in GOR—as well as the inability of the OT to serve as the gold standard for discrimination of reflux related symptoms. However, it is apparent that these indices are unable to predict the response of the one of the most typical symptoms of GOR (heartburn) to one of the most effective medical treatments available.
It should be noted that the precision of the estimates of sensitivity, specificity, significance of the relations, and results of ROC curves are dependent on the number of subjects studied and future studies with more patients are needed to document the results of the present investigation.
Acknowledgments
We are indebted to the staff of the Nemazee Hospital Endoscopy Unit. This study was supported by a grant from the research council of the Shiraz University of Medical Sciences.
REFERENCES
Footnotes
-
Published online first 21 April 2005
-
Conflict of interest: None declared.