Article Text

Abstract
Background: Exposure to acid and duodeno-gastro-oesophageal reflux (DGOR) both increase with oesophageal lesions in gastro-oesophageal reflux disease (GORD). It is unknown whether DGOR exposure is an independent risk factor for oesophageal lesions. A multivariate analysis was performed on the relationship between oesophageal lesions and demographics and acid and DGOR exposure.
Methods: In 422 patients with suspected GORD, upper endoscopy, oesophageal manometry, and pH and DGOR monitoring were performed. Stepwise logistic regression was used to identify factors associated with the presence of oesophagitis, severity of oesophagitis and the presence of Barrett’s oesophagus. ORs and 95% CIs were computed at different cut-offs.
Results: 54% of the patients had no oesophagitis, 36% had grade A–B oesophagitis, 3% had grade C–D oesophagitis and 7% had Barrett’s oesophagus. In multivariate analysis, oesophagitis was associated with hiatal hernia (OR 3.621, 95% CI 2.263 to 5.794) and DGOR exposure (OR up to 2.236, 95% CI 1.356–3.685), while a low body mass index (BMI) seemed protective (OR for BMI >first quartile 2.245, 95% CI 1.371 to 3.677). Severity of oesophagitis was only associated with acid exposure (OR up to 5.038, 95% CI 1.452 to 17.480). The presence of Barrett’s oesophagus was associated with male sex (OR 3.621, 95% CI 2.263 to 5.794), DGOR (OR up to 5.017, 95% CI 2.051 to 12.274) and acid exposure (OR up to 3.031, 95% CI 1.216 to 7.556).
Conclusions: Several independent factors are associated with oesophageal lesions in GORD. The risk of oesophagitis is associated with hiatal hernia, BMI and DGOR exposure; severity of oesophagitis depends on acid exposure; and Barrett’s oesophagus is associated with male sex and exposure to both acid and DGOR.
Statistics from Altmetric.com
Gastro-oesophageal reflux disease (GORD) is one of the most common disorders affecting the gastrointestinal tract. GORD is defined by the presence of symptoms and/or lesions that can be attributed to the reflux of gastric contents into the oesophagus. The most typical clinical symptoms are heartburn and regurgitation, but GORD can manifest itself through a variety of other oesophageal and extra-oesophageal symptoms. Peptic oesophagitis and Barrett’s oesophagus are the specific lesions associated with GORD, but a large proportion of patients with typical GORD symptoms do not have endoscopic evidence of oesophagitis.1–4
GORD symptoms and lesions are classically attributed to reflux of the acid component of gastric content into the oesophagus. However, although oesophageal acid exposure increases with increasing severity of oesophagitis and is highest in Barrett’s oesophagus, the presence or severity of lesions cannot be explained by acid exposure alone.3 5 A number of observations support the concept that non-acidic reflux may also contribute to symptoms and lesions. Reflux of duodenal contents into the stomach is a physiological phenomenon, mainly occurring postprandially.6 Hence, it is not unusual for gastro-oesophageal refluxate to contain duodenal secretions, pancreatic secretions and bile.3 5 Animal studies have indicated that the oesophageal mucosa is relatively resistant to reflux of acid alone, unless the exposure occurs at very high concentrations (pH<1.0). Addition of pepsin at low concentrations induces oesophageal lesions at pH values below 2.3 7–10 Bile acids, especially when conjugated, are injurious to the rabbit oesophageal mucosa at acidic pH,9 and unconjugated bile acids are injurious at neutral pH.10
Aspiration studies demonstrated the presence of bile and pancreatic enzymes in oesophageal aspirates from GORD patients.11–13 Bilitec 2000, a fibreoptic spectrophotometric probe developed to quantify duodeno-gastro-oesophageal reflux (DGOR) in an ambulatory fashion, uses light absorption in the bilirubin spectrum as a marker for the presence of duodenal contents. Validation studies have reported a good correlation between Bilitec measurements and bile acid concentrations.14–16 Ambulatory aspiration studies found a significant correlation between the bilirubin concentration of aspirated samples and the fibreoptic reading.16 Moreover, a good correlation was found between total bilirubin content and the concentrations of pancreatic enzymes in the refluxate, suggesting that bilirubin is a good marker for the entire DGOR.
The pathological role of duodenal contents, consisting of bilirubin, bile acids and pancreatic enzymes, has been suggested in patients developing oesophagitis after total gastrectomy and in patients with achlorhydria.17 18 Similar to pH monitoring, several studies have demonstrated a progressive increase in DGOR across the spectrum of GORD, with a particularly high prevalence in patients with Barrett’s oesophagus and complications.5 19–23 Combined Bilitec and pH studies showed that simultaneous exposure to both acid and DGOR is the most prevalent reflux pattern and that the majority of DGOR episodes occur in an acidic environment.5 23 24 These studies suggest that a synergistic activity of acid reflux and DGOR may contribute to the occurrence and severity of oesophageal lesions in GORD.3 17 25 It is unknown whether the higher DGOR exposure in higher grade lesions merely reflects increased reflux events, as indicated by the higher acid exposure, or whether this is an independent factor contributing to the development of oesophageal lesions. The purpose of the present study, therefore, was to evaluate which factors are involved in the pathophysiology of oesophageal lesions in GORD, by means of multivariate analysis.
MATERIALS AND METHODS
Patients
Over a 2.5-year period, 637 patients underwent evaluation of suspected GORD. The main inclusion criteria were typical GORD symptoms (heartburn and/or regurgitation) and a normal serum bilirubin level.
Exclusion criteria were: peptic ulcer disease, previous oesophageal, gastric or biliary surgery; previous abdominal or thoracic radiotherapy; active gastrointestinal bleeding; oesophageal or fundic varices; diabetes mellitus; Zollinger–Ellison syndrome; connective tissue diseases; neurological disorders; Crohn’s disease; infectious oesophagitis; or active neoplastic disease. At the time of the investigations, access to proton pump inhibitors (PPIs) in Belgium was limited to patients with erosive oesophagitis and restricted to 1 year. Patients were also required to be off PPIs for at least 4 weeks. After these exclusions, 422 patients (66%) were eligible for the study.
Study protocol
The Ethics Committee of the hospital approved the study protocol. Patients were asked to fill out a detailed questionnaire about symptoms, smoking and drinking habits, weight and height, and underwent an ambulatory 24 h oesophageal pH and Bilitec monitoring. All drugs potentially affecting gastrointestinal motility and gastrointestinal secretion were discontinued at least 4 weeks prior to the study.
Probes for assessing acid and DGOR were introduced via a nasal orifice into the oesophagus 5 cm proximal to the lower oesophageal sphincter (LOS), previously defined by stationary oesophageal manometry. The probes were then attached with adhesive tape to the subject’s nose and cheek. In addition, appropriate positioning in the oesophagus was confirmed by fluoroscopy.
Data collection devices were connected to the probes and worn in a belt on the patient’s waist. Registration of acid or DGOR lasted for approximately 22 h, after which the probes were removed and the data transferred to a personal computer for analysis. Patients recorded the time of liquid food or fluid consumption and posture changes on a diary card. They were instructed to stay upright during the daytime. During the recording time, only a free amount of liquid meals (200 ml Nutridrink; 300 kcal: 13% proteins, 48% carbohydrates and 39% lipids; Nutricia, Belgium) was used.19 Patients were asked preferably to drink water and to avoid coffee, tea and fruit juices during the recording.
Upper gastrointestinal endoscopy
Before ambulatory testing for acid reflux and DGOR, all subjects underwent an upper gastrointestinal endoscopy. If necessary, they were sedated by intravenous administration of diazepam (up to 10 mg). During endoscopy, the presence of oesophagitis was noted and graded according to the Los Angeles classification.26 The presence and extent of Barrett’s oesophagus, defined as an extension of columnar lined epithelium of at least 1 cm into the tubular oesophagus, was also noted, and biopsy specimens were obtained in all patients suspected to have Barrett’s oesophagus to diagnose intestinal metaplasia. Gastric biopsies were taken to determine the Helicobacter pylori status. In those who had been on a PPI, the original oesophagitis grade prior to PPI therapy was used as a reference.
Stationary oesophageal manometry
Patients also underwent a manometry before the introduction of the pH and Bilitec probe after an overnight fast using an 8-lumen manometric assembly incorporating a sleeve sensor.19 25 Side-holes 1 cm beyond the distal margin of the sleeve, at the proximal sleeve margin and at 4, 8, 12 and 16 cm more proximally, recorded pressures in the stomach and the oesophageal body, and a side-hole in the pharynx monitored swallowing. The sleeve, gastric and oesophageal side-holes were perfused with distilled water at a rate of 0.6 ml/min using a low compliance pneumohydraulic capillary infusion system. The pharyngeal side-hole was perfused at a rate of 0.3 ml/min, in order to obtain an accurate indication of swallowing but minimise the effect of the assembly on the swallow rate. Each lumen was connected to external pressure transducers (pvb, Medizintechnik, Germany). With the sleeve adequately positioned across the gastro-oesophageal junction, 10 wet swallows (5 ml of water) were administered at 30 s intervals.
Basal LOS pressure was measured at end expiration and referenced to intragastric pressure. The amplitude of oesophageal contractions was obtained by averaging the amplitudes from the two most distal channels during the 10 wet swallows.
Ambulatory pH monitoring
Ambulatory oesophageal pH monitoring was performed using an antimony pH electrode with a separate skin reference electrode (Synectics Medical, Stockholm, Sweden). The data were stored on a portable digital recorder (Digitrapper Mk III, Synectics Medical, Stockholm, Sweden). Before each study, the pH probe was calibrated in buffer solutions of pH 7 and 1. An episode of acid reflux was defined as a decrease in oesophageal pH to <4 for more than 10 s.19 25
The ambulatory recording data were analysed with the aid of commercially available software (Gastrosoft, Synectics Medical, Irvine, Texas, USA). Acid reflux was quantified with the following variables obtained from computerised analysis: number of reflux episodes, number of reflux episodes lasting longer than 5 min/h and percentage of time with pH⩽4. The recording was divided into meal, postprandial (2 h after a meal), interdigestive, upright and supine periods.
Measurement of DGOR
The fibreoptic spectrophotometer Bilitec 2000 (Synectics, Stockholm, Sweden) was used to quantify DGOR. The data were stored on a portable digital recorder, loaded into a personal computer and analysed with dedicated software (Synectics Medical, Stockholm, Sweden). Before each study, the probe was calibrated in water. An episode of DGOR was defined as an increase in oesophageal bilirubin absorbance >0.14 for more than 10 s.19 25
The ambulatory recording data were analysed with the aid of commercially available software (Gastrosoft). Duodenal reflux was quantified with the following variables obtained from computerised analysis: number of reflux episodes, number of reflux episodes lasting longer than 5 min/h and percentage of time with bilirubin absorbance ⩾0.14. The recording was divided into meal, postprandial (2 h after a meal), interdigestive, upright and supine periods.
Statistical analysis
Values are expressed as mean and SEM for parametric data, and median and interquartile range for non-parametric data. Results were compared using Student t test, Mann–Whitney U test or χ2 test wherever appropriate. p Values were considered to be significant if <0.05.
For the univariate analysis, 33 factors were analysed: gender, age, body mass index (BMI), H pylori status, hiatus hernia, smoking, alcohol use, LOS pressure and oesophageal contraction amplitude, as well as all parameters obtained from the reflux measurements. These included for both acid reflux and DGOR the total number of reflux episodes, number of reflux episodes longer than 5 min and the percentage of time at pH⩽4 or absorbance ⩾0.14. These parameters were assessed both for the total time, and for the upright and the supine position period.
To define the risk factors associated with oesophagitis, patients without and with oesophagitis, excluding Barrett’s oesophagus, were compared. To define risk factors for severe lesions, patients with Los Angeles grade A or B were compared with those with grade C or D lesions, excluding Barrett’s oesophagus. Finally, we compared patients with and without Barrett’s oesophagus.
Parameters differing significantly according to the univariate analysis (p<0.05) between the six groups were included in a multivariate logistic regression analysis. Acid and DGOR exposure were used as continuous variables. Independent significant parameters were identified using an ascending selection procedure (Proc Logistic Regression, SAS 6.08, Cary, North Carolina, USA). p Values of 0.05 and 0.1 were chosen as cut-off points to enter and exit the stepwise procedure. Odds ratios (ORs) and 95% CIs were calculated.
From the independent variables determined by multivariate logistic regression analysis, a second analysis was performed using different cut-offs for these variables. Cut-off levels were chosen at the first, second and third quartile. ORs and 95% CIs were computed for each of these cut-offs.
RESULTS
Patient characteristics
A total of 422 patients (201 men (48%), mean age 46.8 (0.7) years) were recruited for the study: 103 patients (24%) were active smokers and 125 (30%) patients drank alcohol regularly. The mean weight was 73.0 (0.7) kg, the mean height 170 (0.4) cm and the mean BMI 25.2 (0.2) kg/m2. Manometry showed normal amplitude peristalsis in 83% of the patients. Low amplitude (<30 mm Hg) peristalsis in the distal oesophagus occurred in 16%, and in two patients contractions were absent in the distal oesophagus.
Endoscopy
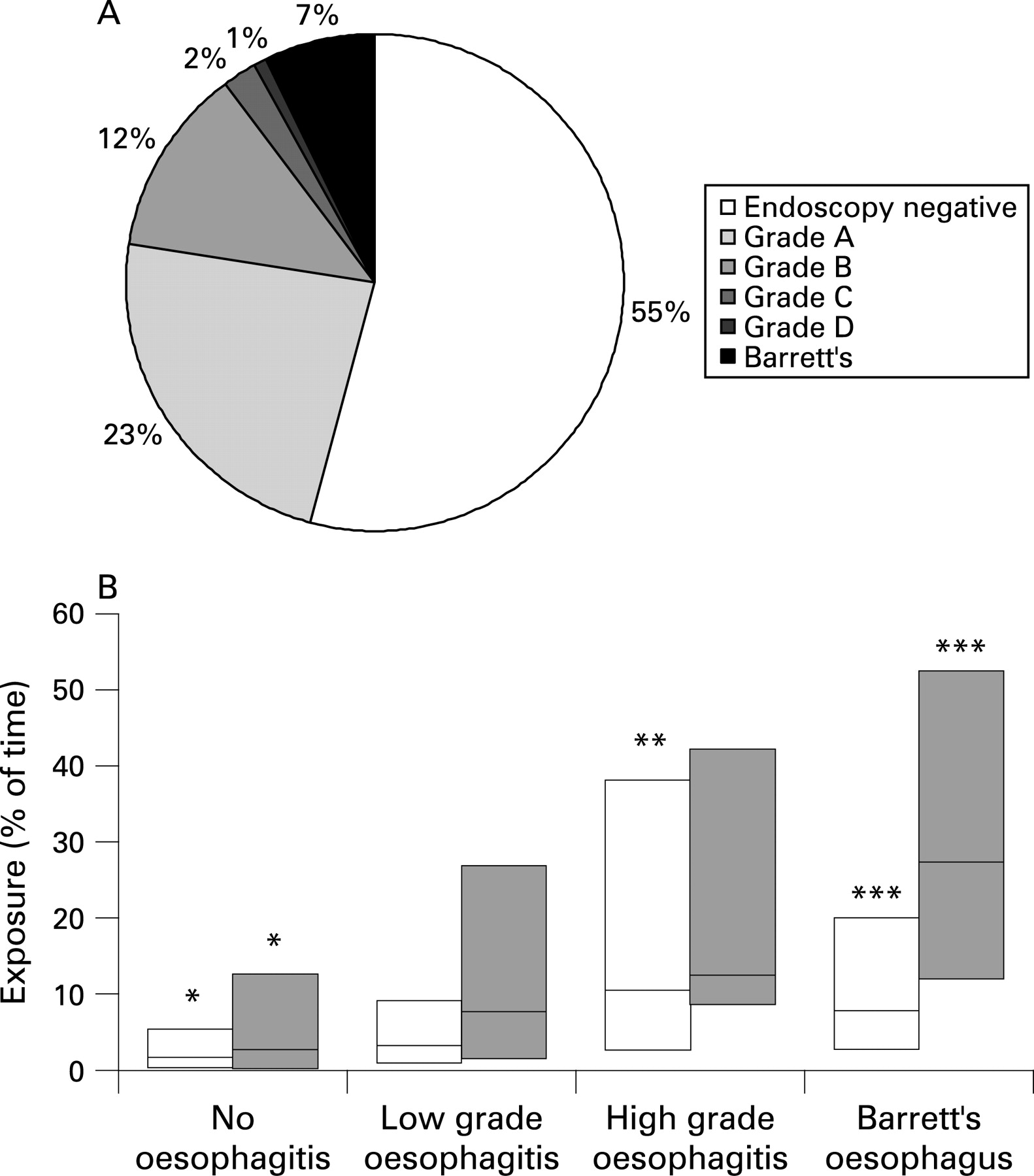
All 422 patients underwent an endoscopic examination before the 24 h measurements. In 228 patients (54.0%) no oesophageal lesions were found. According to the Los Angeles classification, oesophagitis grade A was found in 99 (23.5%), grade B in 52 (12.3%), grade C in 9 (2.1%) and 4 (1.2%) had grade D. Thirty patients (7.1%) had a Barrett’s oesophagus with a mean length of 4.0 (0.3) cm (fig 1A). A hiatus hernia with a mean length of 5.5 (0.2) cm was found in 154 patients (36.5%). Seventy-seven patients (18.4%) were H pylori positive, and no H pylori result was available in three patients.

Bilitec and pH measurements
The mean duration of the combined pH and Bilitec measurement was 21.2 (1.6) h. Table 1 summarises acid and DGOR reflux findings for the total recording time and for the upright and supine recording times. According to previously established normal values,27 155 patients had pathological acid exposure (37%; 35% upright and 24% supine) and 215 patients had pathological DGOR exposure (51%; 44% upright and 46% supine). Acid exposure and DGOR increased with increasing severity of lesions (fig 1B).
Factors associated with the presence of erosive oesophagitis
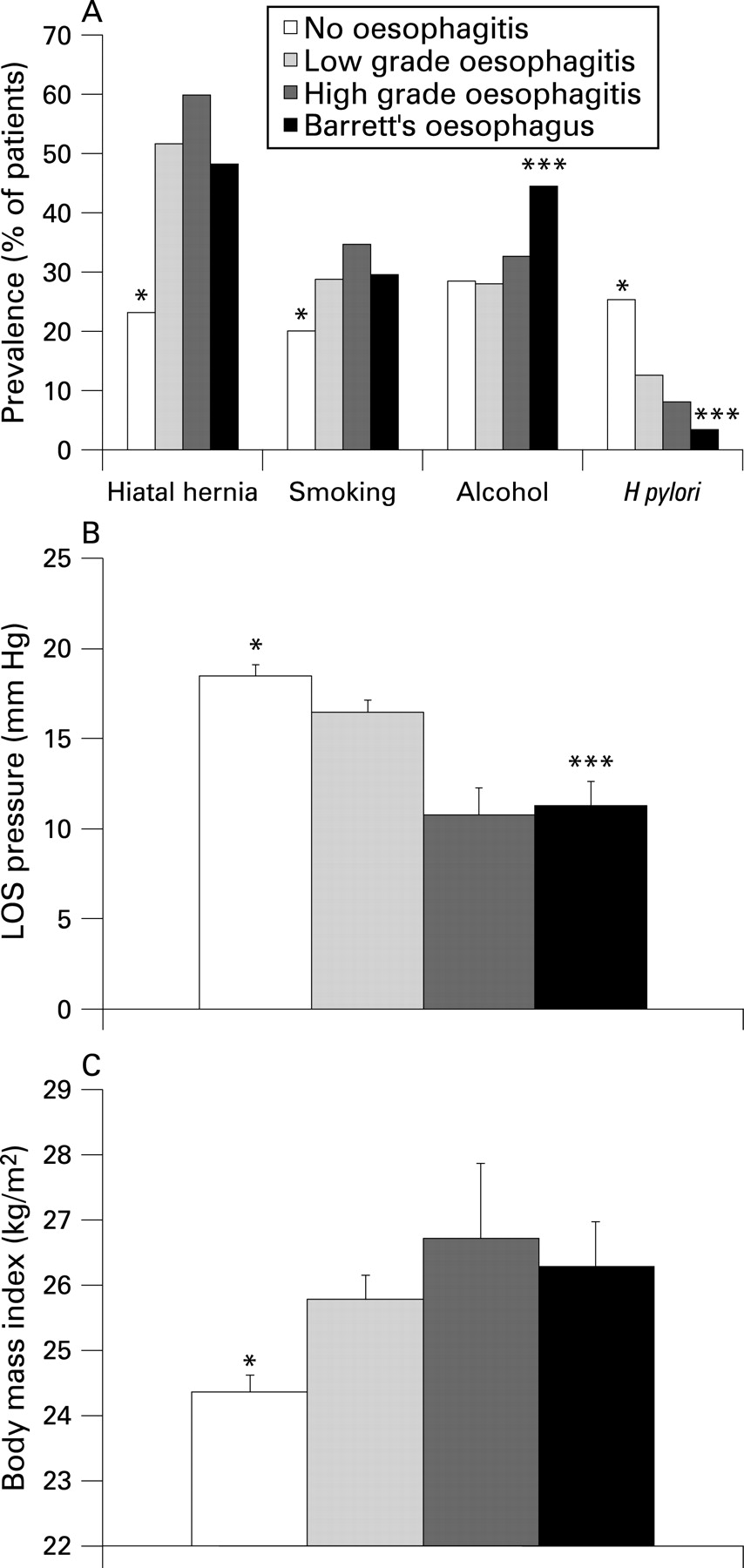
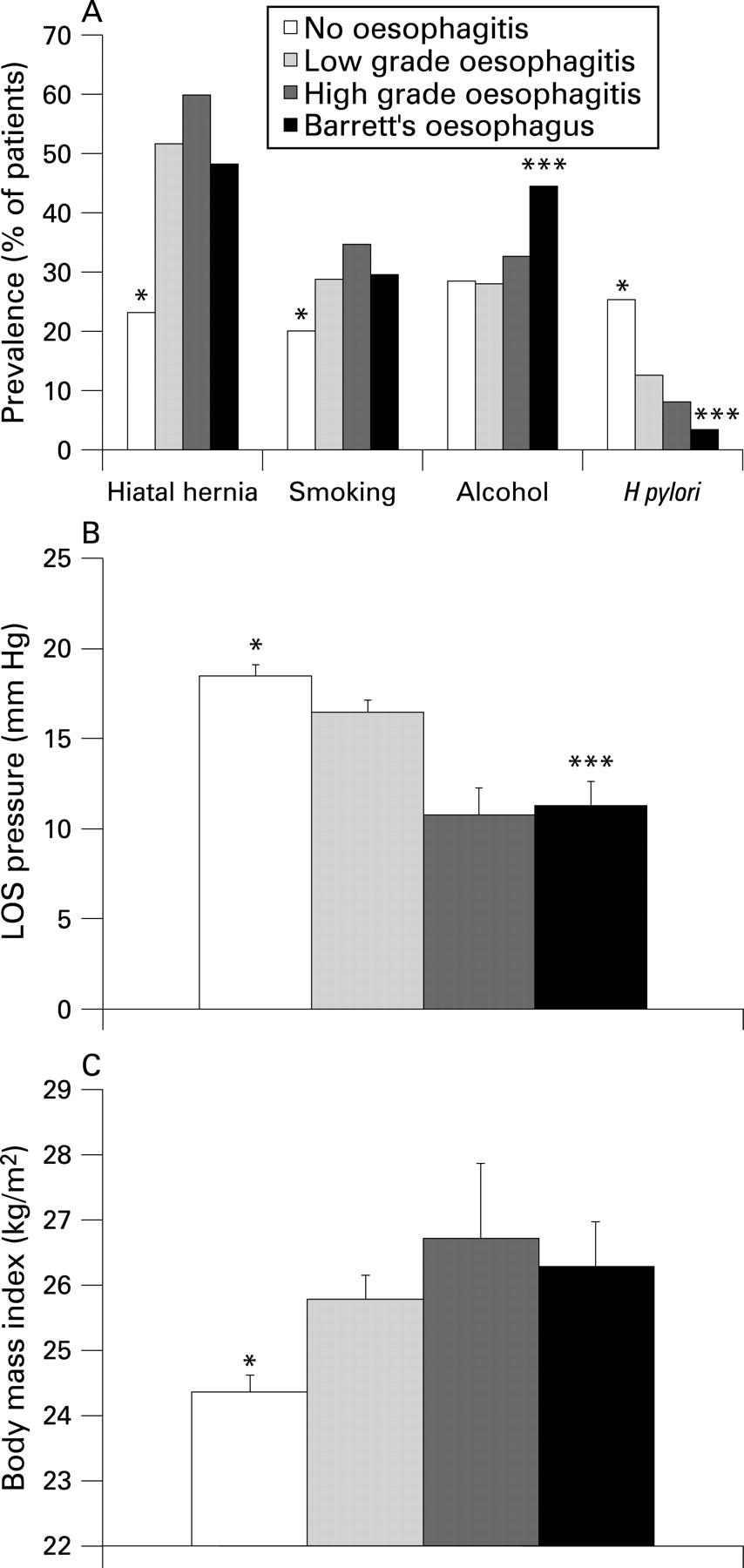
The comparison between patients with and without oesophagitis, excluding Barrett’s, is summarised in table 2. In the univariate analysis, oesophagitis patients had a significantly higher BMI, a lower prevalence of H pylori infection and a lower LOS pressure. All acid reflux and DGOR parameters were higher in oesophagitis patients, for total as well as upright and supine times. No relationship was found between alcohol intake and oesophagitis, but smoking was significantly more prevalent in oesophagitis patients (table 2) (fig 2A–C).
{kind=link}
{kind=link}
The multivariate logistic regression analysis identified the presence of a hiatus hernia (HH), BMI and DGOR exposure (B%T) as independent risk factors for the presence of oesophagitis. The model (y = −2.5178 + 0.0599 × BMI + 1.2844 × HH + 0.0117 × B%T) explained 70.3% of the variance. The results of the multivariate analysis, at different cut-offs for continuous variables, are shown in table 3. Cut-offs at the first, second and third quartile were 0.6%, 4.4% and 17.0% of time, respectively, for DGOR, and 22, 25 and 28 kg/m2 respectively for BMI. When total acid or DGOR exposure were removed, the analysis revealed that supine, and not upright, DGOR exposure was an independent risk factor for the presence of oesophagitis. The increase in OR with increasing cut-offs was almost absent for total DGOR exposure, and showed a modest increase for supine DGOR from 2.245 at the first quartile to 2.820 at the third quartile cut-off. It is possible that the association of DGOR with oesophagitis reflects a threshold factor rather than a progressively increasing quantitative factor. With increasing BMI cut-offs, decreasing OR for an association of oesophagitis with high BMI was found. This secondary analysis suggests that a low BMI is protective against reflux oesophagitis, rather than a higher BMI predisposing to oesophagitis.
Factors associated with the severity of oesophagitis
Table 4 summarises the comparison of patients with low (grades A, B) and high (grades C, D) grade oesophagitis, excluding Barrett’s oesophagus. Patients with higher oesophagitis grades had a lower LOS pressure, a higher total acid exposure and a higher number of DGOR episodes (fig 2A–C).
The multivariate analysis identified only increasing acid exposure (A%D) as an independent risk factor for the severity of oesophagitis. The model (y = −2.8959+0.0339×A%T) explained 59.2% of the variance. The results of the multivariate analysis, at different cut-offs for acid exposure, are shown in table 5. Cut-offs at the first, second and third quartile for acid exposure were 0.6%, 2.2% and 7.1% of time, respectively. Analysis for upright and supine revealed that only upright acid exposure was a borderline significant risk factor for severity of oesophagitis.
Factors associated with Barrett’s oesophagus
Table 6 summarises the comparison between patients with and without Barrett’s oesophagus. In univariate analysis, Barrett’s patients were more likely to be men, and had a lower LOS pressure compared with patients without Barrett’s oesophagus. All acid reflux and DGOR parameters were higher in Barrett’s patients, for total as well as upright and supine times. No relationship was found between smoking and Barrett’s oesophagus, but alcohol intake was significantly more prevalent in patients with Barrett’s (table 6) (fig 2A–C).
The multivariate logistic regression analysis identified male sex (MS), increasing acid exposure (A%T) and increasing DGOR exposure (B%T) as independent risk factors for the presence of Barrett’s oesophagus. The model (y = −3.7558 + 0.8420 × MS + 0.0195 × A%T+0.0248 × B%T) explained 75.0% of the variance. The results of the multivariate analysis, at different cut-offs for continuous variables, are shown in table 7. Cut-offs at the first, second and third quartile were 0.6%, 4.9% and 20.1% of time, respectively, for DGOR, and 0.6%, 2.4% and 7.5% of time, respectively, for acid exposure. Refining the analysis revealed that upright acid exposure, upright DGOR exposure and the number of long-lasting acid or DGOR reflux episodes were independent risk factors for the presence of Barrett’s oesophagus. However, unlike for upright acid exposure, the ORd did not clearly increase with increasing cut-offs for upright DGOR exposure. Smoking or alcohol intake did not present as independent risk factors in the multivariate analysis.
DISCUSSION
In the present study, we evaluated combined pH and Bilitec measurements, demographic, endoscopic and manometric characteristics in a large group of GORD patients to identify factors associated with the presence of oesophagitis, the severity of oesophagitis and the presence of Barrett’s oesophagus. The prevalence of oesophageal lesions and of hiatal hernia seen during endoscopy are comparable with those in previous reports.28–31 A summary of the independent risk factors is provided in table 8.
Traditionally, acid reflux is believed to be the most important factor contributing to GORD symptoms and lesions. In a multivariate analysis of 78 patients, impaired oesophageal acid clearance, hypotonic LOS and the level of acid secretion were identified as independent risk factors for oesophagitis.32 Wilson et al showed in a multiple regression analysis that BMI was associated with oesophagitis and found an association between the presence of a hiatal hernia and BMI.33
In these studies, DGOR and its role in the occurrence of oesophageal lesions were not assessed. However, animal studies suggest that the normal oesophagus mucosa is relatively resistant to luminal acid in normal concentrations, and that acid is caustic only at very low pH values.34–38 In similar in vitro studies, the addition of pepsin allows lesions to occur at higher pH ranges.8 39–43 The role of duodenal contents, which amongst others contain bilirubin, bile salts, lysolecithin and pancreatic enzymes such as trypsin, in inducing oesophageal mucosal lesions is still incompletely elucidated. The observation of oesophagitis in patients with achlorhydria and after total gastrectomy does suggest a potential damaging effect of DGOR on oesophageal mucosa in man.17 18 44 A number of studies suggest involvement of DGOR in oesophagitis that occurs or persists in spite of acid-suppressive therapy.27 45
In the present study, we observed that GORD patients with oesophagitis, compared with GORD patients without lesions, not only had significantly higher oesophageal acid exposure, but also had higher oesophageal DGOR exposure. Furthermore, oesophagitis patients also had a higher BMI, a hiatus hernia, a lower LOS pressure and were more likely to smoke compared with patients without oesophagitis. In the multivariate analysis, only the presence of a hiatus hernia, a higher BMI and DGOR exposure were independent factors associated with the risk of oesophagitis. In particular, DGOR exposure in the supine position was a risk factor for the presence of oesophagitis. The presence of a hiatus hernia with a lowered LOS pressure represents a major defect in the anatomic antireflux barrier. A previous analysis suggested that BMI was a risk factor for oesophagitis, probably through a higher prevalence of hiatus hernia.33 In the present study, a low BMI seemed to be a factor that protected against oesophagitis, as the OR for erosive oesophagitis did not continue to increase with a rising BMI. Surprisingly, oesophageal acid exposure was not an independent risk factor associated with the occurrence of erosive oesophagitis. These data suggest that reflux of duodenal contents may be an important cofactor in the induction of oesophageal lesions in GORD.
We also studied the factors associated with the severity of oesophagitis, by distinguishing high grade from low grade oesophagitis lesions, with the exclusion of patients with Barrett’s oesophagus. In the univariate analysis, high grade oesophagitis was associated with lower LOS pressure, higher oesophageal acid exposure and higher number of DGOR episodes. However, in the multivariate analysis, only oesophageal acid exposure, mainly in the upright position, was an independent risk factor for severe oesophagitis. Taken together, these data suggest that DGOR is an important risk factor for the occurrence of oesophagitis, perhaps by acting as a barrier disrupter, but when oesophageal lesions occur acid exposure is the principal factor determining their severity. The findings are in agreement with animal studies that demonstrate a synergistic effect of bile and acid in inducing oesophageal lesions.8 39–43
A final analysis, comparing patients with and without Barrett’s oesophagus, revealed Barrett’s patients to have a higher prevalence of male sex and alcohol consumption, a lower LOS pressure, a lower rate of Helicobacter infection, higher oesophageal acid exposure and higher oesophageal DGOR exposure. In the multivariate analysis, male sex and both oesophageal acid exposure and DGOR exposure were identified as independent risk factors for Barrett’s oesophagus. In contrast to the risk for the presence of oesophagitis, the presence of Barrett’s oesophagus was mainly associated with the number of long-lasting acid reflux episodes and long-lasting DGOR reflux episodes in the upright position. Several previous studies have demonstrated increased oesophageal acid and DGOR exposure in Barrett’s patients,19–24 thereby suggesting a synergistic activity of acid and bile in inducing Barrett’s mucosa. The findings are also consistent with the results of a multivariate analysis in a surgical cohort of patients, where, besides male sex, both abnormal bile reflux and long-lasting acid reflux episodes were independent risk factors for Barrett’s oesophagus.46 That study also identified the presence of a hiatal hernia, hypotensive LOS, oesophageal hypocontractility and long-standing GORD symptoms as independent risk factors for Barrett’s oesophagus,46 but these factors were not retained in the present cohort of patients. Alcohol consumption was a significant factor in the univariate analysis, but was not an independent factor. Involvement of lifestyle factors in the development of a Barrett’s oesophagus to oesophageal cancer have traditionally been suspected, but smoking and alcohol consumption could not be identified as independent factors in different studies.47–49 Recent in vitro studies support the synergistic action of acid and bile reflux in the pathogenesis of Barrett’s complications, as upregulation of the protein product of the c-myc oncogene and induction of cyclooxygenase 2 were induced by acidified bile in biopsies from patients with Barrett’s oesophagus.51–53
We found a low prevalence of H pylori infection, but this prevalence was significantly higher in patients without oesophagitis, and lower in patients with Barrett’s oesophagus. These findings are consistent with previous observations suggestive of a protective effect of Helicobacter infection against GORD lesions and complications.54–56 However, Helicobacter infection was never identified as an independent factor in the multivariate analyses, but the overall infection rates were low in the population that was studied.
In summary, we identified independent risk factors associated with the presence of oesophageal lesions in GORD. Besides the presence of a hiatal hernia, we found that DGOR, especially supine DGOR exposure, was an independent risk factor for the presence of oesophagitis, while a low BMI was a protective factor. In the case of oesophagitis, acid exposure was the main risk factor for high grade lesions. Male sex, long-lasting acid exposure and DGOR exposure were all independent risk factors associated with Barrett’s oesophagus. This study confirms that multiple factors are involved in the pathogenesis of oesophageal lesions in GORD.
REFERENCES
Supplementary materials
web only appendix 57/8/1056
Files in this Data Supplement:
Footnotes
Competing interests: Declared. The declaration can be viewed online only at http://gut.bmj.content/vol57/issue8
Ethics approval: The Ethics Committee of the University Hospital Gasthuisberg approved the study protocol.
Linked Articles
- Digest