Article Text

Abstract
Objective: Assessment of disease extension and activity is crucial to guide treatment in Crohn’s disease. The objective of the current cross-sectional study was to determine the accuracy of MR for this assessment.
Design: 50 patients with clinically active (n = 35) or inactive (n = 15) Crohn’s disease underwent ileocolonoscopy (reference standard) and MR. T2-weighted and precontrast and postcontrast-enhanced T1-weighted sequences were acquired. Endoscopic activity was evaluated by CDEIS (Crohn’s Disease Endoscopic Index of Severity); in addition endoscopic lesions were classified as absent, mild (inflammation without ulcers) or severe (presence of ulceration).
Results: The comparison of intestinal segments with absent, mild and severe inflammation demonstrated a progressive and significant (p<0.001) increase in the following MR parameters: wall thickness, postcontrast wall signal intensity, relative contrast enhancement, presence of oedema, ulcers, pseudopolyps and lymph node enlargement. Independent predictors for CDEIS in a segment were wall thickness (p = 0.007), relative contrast enhancement (p = 0.01), presence of oedema (p = 0.02) and presence of ulcers at MR (p = 0.003). There was a significant correlation (r = 0.82, p<0.001) between the CDEIS of the segment and the MR index calculated according to the logistic regression analysis coefficients. The MR index had a high accuracy for the detection of disease activity (area under the receiver operating characteristic (ROC) curve 0.891, sensitivity 0.81, specificity 0.89) and for the detection of ulcerative lesions (area under the ROC curve 0.978, sensitivity 0.95, specificity 0.91) in the colon and terminal ileum.
Conclusion: The accuracy of MR for detecting disease activity and assessing severity brings about the possibility of using MR as an alternative to endoscopy in the evaluation of ileocolonic Crohn’s disease.
Statistics from Altmetric.com
Assessment of disease extension and activity is crucial in patients with Crohn’s disease (CD) to determine the therapeutic strategy, and has important prognostic implications. This assessment usually relies on endoscopy.1 However, endoscopy cannot always be complete, and there are several drawbacks related to the invasiveness, procedure-related discomfort, risk of bowel perforation and relatively poor patient acceptance. This fact has led to the search for alternative techniques to assess disease extension and severity in inflammatory bowel disease (IBD) including sonography and CT.2 Exposure to ionising radiation is a relevant limitation of the latter, especially in light of the patients’ young age.3 We and others have proposed the use of sonography for evaluation of IBD activity as an alternative to endoscopy, but assessment of the intestine by this technique is frequently incomplete due to gas interposition.4
Magnetic resonance (MR) has the potential to overcome these limitations. It is characterised by a very high soft tissue contrast, lack of ionising radiation and lower incidence of adverse events related to the intravenous contrast employed compared with CT. Although several MR characteristics of the bowel have been described in patients with CD, no studies have specifically addressed the relative usefulness of each of these MR signs in the assessment of inflammatory activity and severity, and most protocols relied only on measurement of wall thickness and degree of enhancement after administration of paramagnetic contrast. Using the latter parameters, some previous reports5–9 produced controversial results, and methodological differences make comparisons difficult. Despite its potential usefulness, a major drawback to the routine use of MR in the assessment of CD is the lack of precise criteria to define bowel involvement by CD, and quantify the severity of inflammatory lesions.
Therefore, the aims of this cross-sectional study were to characterise the MR patterns of the colon and the terminal ileum in patients with active and inactive CD; to establish the MR changes indicative of mild and severe intestinal lesions; and to provide a quantitative index of disease activity based on MR findings.
PATIENTS AND METHODS
Patients and examinations
Between June 2007 and April 2008, 50 patients with an established diagnosis of CD of at least 6 months duration, with or without clinical symptoms of activity, were prospectively studied at a single centre. During the same period, two patients refused to participate in the study because of personal reasons: one patient preferred to avoid MR exploration due to claustrophobia, and in another patient MR examination could not be completed due to intolerance of the enema. Patients underwent complete clinical assessment, had blood samples obtained for cell blood counts and C-reactive protein (CRP) measurements, and underwent conventional ileocolonoscopy and MR examination within 2 days. Clinical disease activity was assessed using the Harvey–Bradshaw score.10 Investigators performing ileocolonoscopy or MR were unaware of clinical data or of the results of other examinations. All patients gave their informed consent to participate in the study after approval of the project by the ethics committee of the Hospital Clínic of Barcelona.
Endoscopic data collection
Ileocolonoscopy was considered the reference standard for the evaluation of IBD extension and severity. All patients underwent endoscopy 4–24 h before or after the MR examination. Patients followed a bowel cleansing protocol with oral ingestion of 3000–4000 ml of an iso-osmotic polyethylene glycol (PEG) and electrolyte solution (Bohm laboratories, Fuenlabrada, Spain) on the evening before examination. Endoscopies were performed under anaesthesia with propofol (Mayne Pharma, Madrid, Spain) and remifetanyl (GlaxoSmithKline, Madrid, Spain). The severity and extent of inflammatory lesions were evaluated using the Crohn’s Disease Endoscopic Index of Severity (CDEIS).1 For CDEIS calculation, the endoscopic variables were as originally defined: deep ulcers and superficial ulcers (presence or absence), ulcerated surface and affected surface (evaluated on a 10 cm linear analogue scale), and ulcerated and non-ulcerated stenosis. These variables were evaluated in the terminal ileum, ascending colon, transverse colon, descending and sigmoid colon, and the rectum.
For comparison of endoscopic and MR findings in each segment, a calculation of endoscopic activity of the segment was performed by dividing the colon into five segments instead of four as for the conventional CDEIS calculation (ascending colon, transverse colon, descending colon, sigmoid colon and rectum) and scoring the CDEIS variables in each of these segments and the terminal ileum. The score of ulcerated or non-ulcerated stenosis was imputed to the affected segment. In addition, a classification of lesion severity of each segment was performed by considering three categories: (1) absence of lesions; (2) presence of inflammatory lesions without ulceration, including erythema, oedema, pseudopolyps and aphtae; and (3) presence of superficial or deep ulcerations.
The endoscopist completed an endoscopic scoring sheet immediately after colonoscopy. All procedures were performed by two gastroenterologists with >10 years experience in conventional colonoscopy using standard equipment (CFQ 140 L; Olympus, Japan), and after a period of joint training for CDEIS scoring.
MR acquisition
In most cases MR and ileocolonoscopy were performed on the same day, under the bowel cleansing protocol described previously, without any additional preparation for MR. In the few instances that the two techniques were not performed on the same day bowel cleansing with 1000–2000 ml of PEG solution was given 4 h before performing MR.
All MR examinations were performed using a 3.0 T MR unit (TrioTim; Siemens Medical Solutions, Erlangen, Germany). Patients were placed in the supine position in the MR imager. This position is more comfortable for patients. A combination of two surface coils was used for signal reception to allow coverage of the whole abdominal area. To reduce bowel peristalsis, 40 mg of hyoscine butylbromide (Buscapina; Boehringer Ingelheim, Sant Cugat, Spain) were injected intravenously.
To achieve an adequate distension of the distal ileum, 45 min before the MR each patient was required to drink 1500 ml of iso-osmotic PEG and electrolyte solution. Saline was retrogradly instilled into the colon through a flexible rectal balloon catheter (Silkolater Teleflex Medical, Alicante, Spain). The volume of warm water was adjusted for each patient to avoid abdominal pain or discomfort, ranging from 1000 to 2000 ml. The procedure was well tolerated.
Initially a true fast imaging with a steady precession sequence was acquired in the coronal plane to ensure optimal colon distension. Then, the acquisition protocol outlined in table 1 was performed. VIBE (volumetric interpolated breath-hold examination) sequences were acquired before and 70 s after intravenous administration of 0.2 ml/kg body weight of gadolinium chelate (gadodiamide 0.5 mmol/l Ominscan-Amersham, Madrid, Spain) at a rate of 2 ml/s.
MR image analysis
To establish disease extension by MR, we used the same division into six segments as was used in colonoscopy (distal ileum, ascending, transverse, descending, sigmoid colon and rectum). Image analysis was performed using a dedicated postprocessing workstation (Leonardo; Siemens AG Medical Solutions). The following were studied by MR in each colonic segment and in the terminal ileum: bowel wall thickness (mm), presence of mucosal ulceration (defined as deep depressions in the mucosal surface), presence of mural oedema (hyperintesity on T2-wedged sequences of the colon wall relative to the signal of the psoas muscle), presence of pseudopolyps in the lumen, enlarged (>1 cm) regional mesenteric lymph nodes, quantitative measurement of wall signal intensity (WSI) before and after intravenous contrast administration measured in VIBE sequences, and relative contrast enhancement (RCE) of the intestinal wall. Quantitative measurements of WSI were obtained from the areas with the greatest thickening. WSI corresponds to the average of three WSI measurements. RCE was calculated according the following formula: RCE = ((WSI postgadolinium–WSI pregadolinium)/(WSI pregadolinium))×100×(SD noise pregadolinium/SD noise postgadolinium), where SD noise pregadolinium corresponds to the average of three SDs of the signal intensity measured outside of the body before gadolinium injection, and SD noise postgadolinium corresponds to the SD of the same noise after gadolinium administration.11
Statistical analysis
Differences in qualitative MR findings were tested with the χ2 test; differences in quantitative measures were tested using analysis of variance (ANOVA) followed by the Bonferroni posthoc test. Correlations between the CDEIS, Harvey–Bradshaw index, CRP and MR index scores were measured by the Spearman rank coefficient.
For defining the MR findings that were independent predictors of disease activity, a binary logistic regression was used with the presence of an endoscopic lesion (of any type) as the dependent variable, and with the presence of oedema, ulcerations, pseudopolyps, wall thickness and RCE in MR as independent variables. For defining the independent predictors of the presence of ulcerations at endoscopy, a binary logistic regression was used, with this endoscopic finding as dependent variable, and the same MR variables listed above as independent variables. The multivariate procedures were validated by bootstrap bagging with 1000 samples. Development of an MR index of disease activity was based on the findings of the individual segments. Since distribution of the values for CEDEIS was not normal, with 60% of segments having no significant lesions, a tobit regression model was applied. In that model, the calculated CDEIS per segment was used as the dependent variable, and again the presence of oedema, ulcerations, pseudopolyps, wall thickness and RCE in MR were introduced as independent variables. The accuracy of the scores determined by MR for the prediction of the presence of active disease and the presence of severe lesions was assessed by calculating receiver operating characteristic (ROC) curves.
Interobserver agreement between paired evaluations of MR by two radiologists (JR and SR) was performed through kappa statistics12 for comparisons of qualitative variables (presence of oedema, ulcers, pseudopolyps and lymph nodes), and through the intraclass correlation coefficient13 for assessing the reproducibility level of quantitative MR measurements (wall thickness, basal signal intensity, contrast signal intensity and RCE).
Statistical power
We estimated that by studying 50 patients at least 200 colonic segments and 40 ileal segments would be available for examination (colonoscopy completed in 90% and ileoscopy in 80%). Of those 50% would be normal, 25% would have non-ulcerative lesions and 25% would have ulcerative lesions. This number provides the ability to detect differences of 20% for the presence of activity, and 25% for the presence of ulcerations among those with disease activity with an alpha risk of 0.05 and beta of 0.1.
A p value of <0.05 was considered significant. Calculations were done with the SPSS package version 15 (SPSS, 1989–2006, Chicago, Illinois, USA).
RESULTS
Patients
Clinical and biological characteristics of the 50 patients included in the study are provided in table 2. According to the Harvey–Bradshaw index, 15 patients were in clinical remission (index ⩽4) and 35 patients had active disease (index >4). CRP was elevated relative to reference values (normal ⩽8 mg/l) in 35 patients. Complete endoscopic evaluation of the colon with intubation of the ileum through the ileocecal valve or an ileocolonic anastomosis was achieved in 36 patients (72%). Reasons for incomplete ileocolonoscopy were disease severity (n = 3), stenosis (n = 3) or technical impossibility (n = 8). The total number of colonic segments examined, considering the extension of examinations and previous resection surgery, was 213. Of these, 130 were without lesions, 43 had mild lesions including erythema, oedema, pseudopolyps or aphtoid ulcers, and 40 segments had severe lesions with superficial and/or deep ulcers. Tolerance of MR examination was in general very good. The average duration of the entire MR examination within the MR imaging unit was ∼25 min. Only three patients, all with severe rectal lesions, complained of tenesmus upon instillation of the enema that did not preclude completion of the examination.
MR findings according to endoscopic lesion severity
As shown in table 3 and fig 1, the majority of MR findings had a close correlation with the severity of endoscopic lesions. Oedema on MR examination was present in 77.5% of colonic segments with ulcers at endoscopy, was significantly less frequent in segments with inflammatory lesions without ulcers (20.9%) and absent in endoscopically normal segments. Ulcers were identified by MR in 65% of patients with ulcers at endoscopy, were very rare in segments with mild inflammation (7.0%) and were never observed in endoscopically normal mucosa. The presence of enlarged lymph nodes and pseudopolyps was less prevalent, but also significantly more frequent in patients with ulcers compared with the other groups of patients (table 3). The kappa measure of agreement between endoscopy and MR for identification of ulcers was 0.71, and for pseudopolyps 0.86, although the sensitivity of MR for the detection of segments with ulcerative lesions was markedly increased when not only direct identification of ulcers, but also wall thickening and REC were considered (see below).

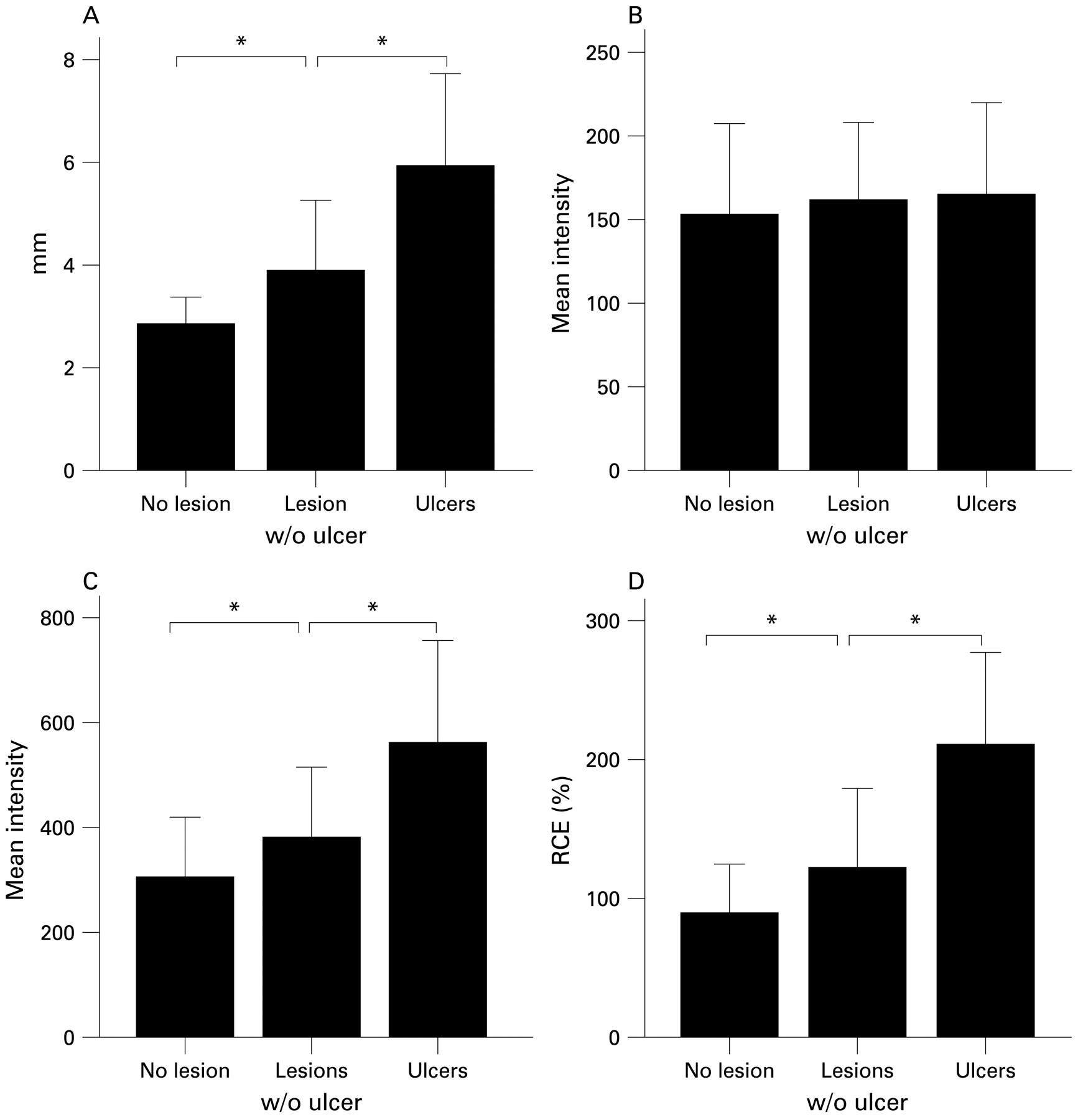
Changes in quantitative magnetic resonance (MR) parameters according to endoscopic severity of colonic lesions. Wall thickness (A), post-ontrast wall signal intensity (C) and relative contrast enhancement (D) were significantly increased in parallel with the severity of endoscopic lesions. Basal signal intensity (B) was not influenced by inflammatory lesions. *p<0.01. w/o, without.
Figure 1 depicts the changes in quantitative MR parameters according to endoscopic severity of colonic lesions. The increase in wall thickness paralleled the endoscopic severity of lesions, with a significant increase in segments with inflammatory lesions without ulcers compared with those with normal mucosa, and again significantly increased in segments with ulcers compared with non-ulcerative inflammatory lesions. In contrast, basal signal intensity was similar in all groups. After intravenous injection of contrast, WSI was markedly elevated in segments with ulceration relative to segments with inflammation without ulcers, and also in the latter compared with normal segments. RCE also paralleled the severity of endoscopic lesions with significant differences between segments with normal mucosa, segments with mild lesions and segments with ulcers.
MR changes were similar in all colonic segments, with the exception of lymph node enlargement that was predominantly associated with the presence of severe endoscopic lesions in terminal ileum, ascending colon and rectal regions. The characteristics and magnitude of MR changes in the ileum were similar to those of the colon, with significant (p<0.05) increases in the proportion of patients having oedema, ulcers identified at MR, and lymph nodes in the ileocecal region, as the severity of endoscopic lesions increased from normal to presence of any lesion, and from non-ulcerative lesions to presence of ulcers. Pseudopolyps were not identified in the ileum. Also a significant increase in wall thickness, WSI and RCE (all p<0.05 by ANOVA test), but not basal signal intensity, was observed in the ileum that paralleled the severity of endoscopic lesions. Examples of MR alterations associated with the presence of active inflammation are shown in figs 2 and 3.
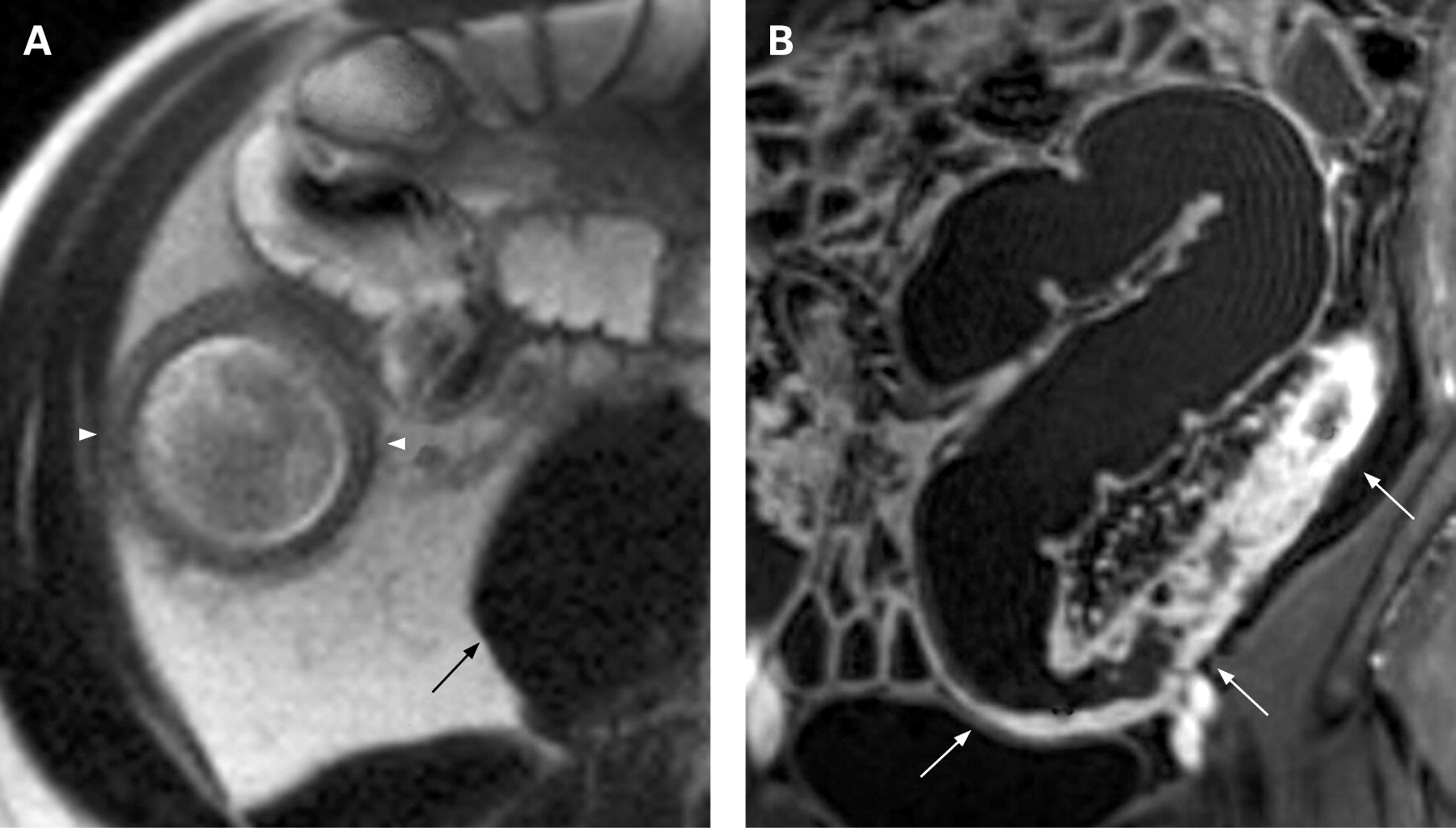
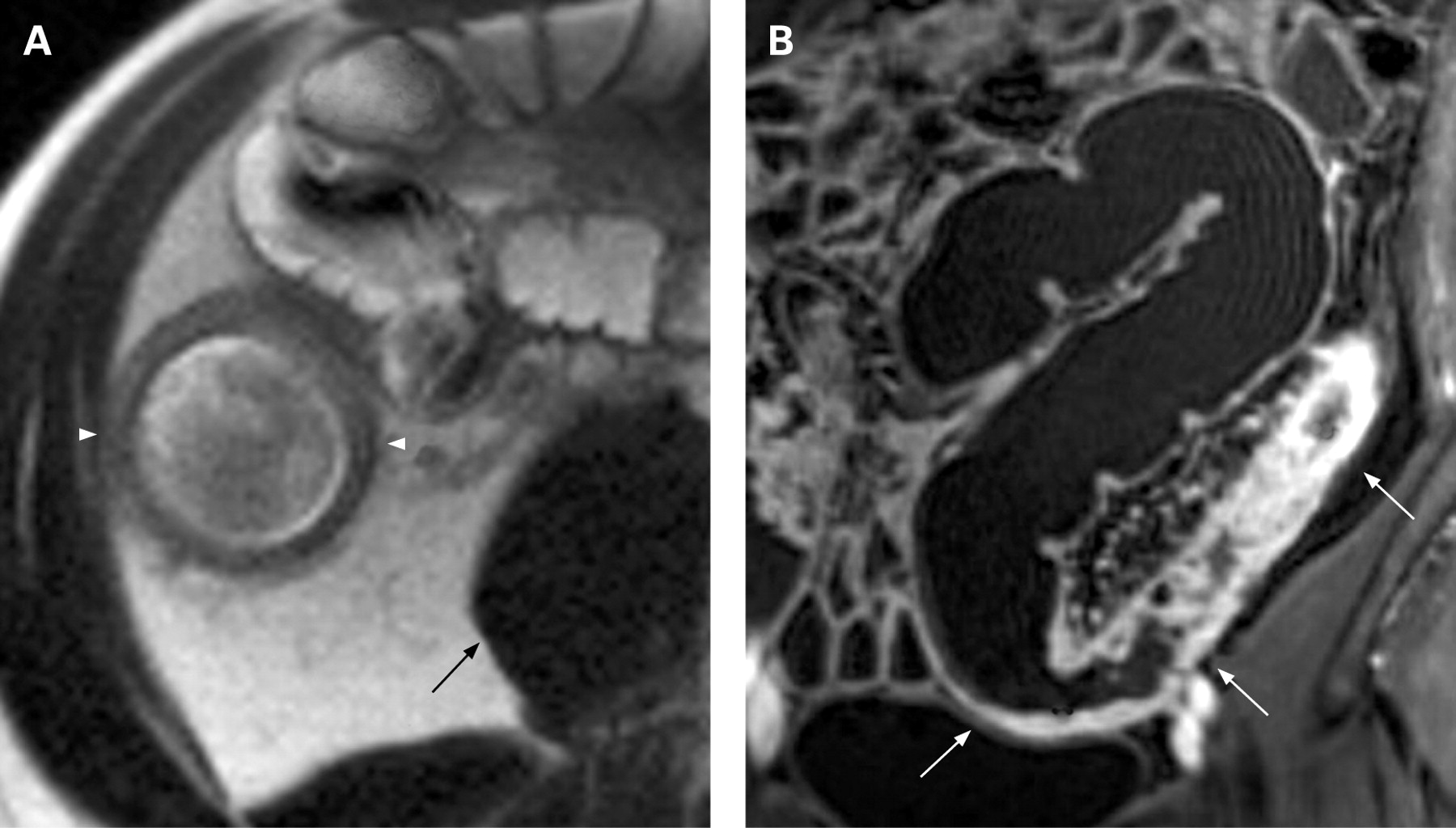
(A) Magnetic resonance axial T2-wedged depicts moderate wall thickening of the ascending colon (arrowheads) that also has a hypersignal relative to the psoas muscle (arrow) indicating the presence of oedema. (B) Coronal T1-VIBE (volumetric interpolated breath-hold examination) after intravenous contrast administration. Marked enhancement of the sigmoid colon and descending colon (arrows) relative to the remaining colon can be seen. Also note the presence of the irregularity of the mucosal surface showing ulcers and inflammatory pseudopolyps.
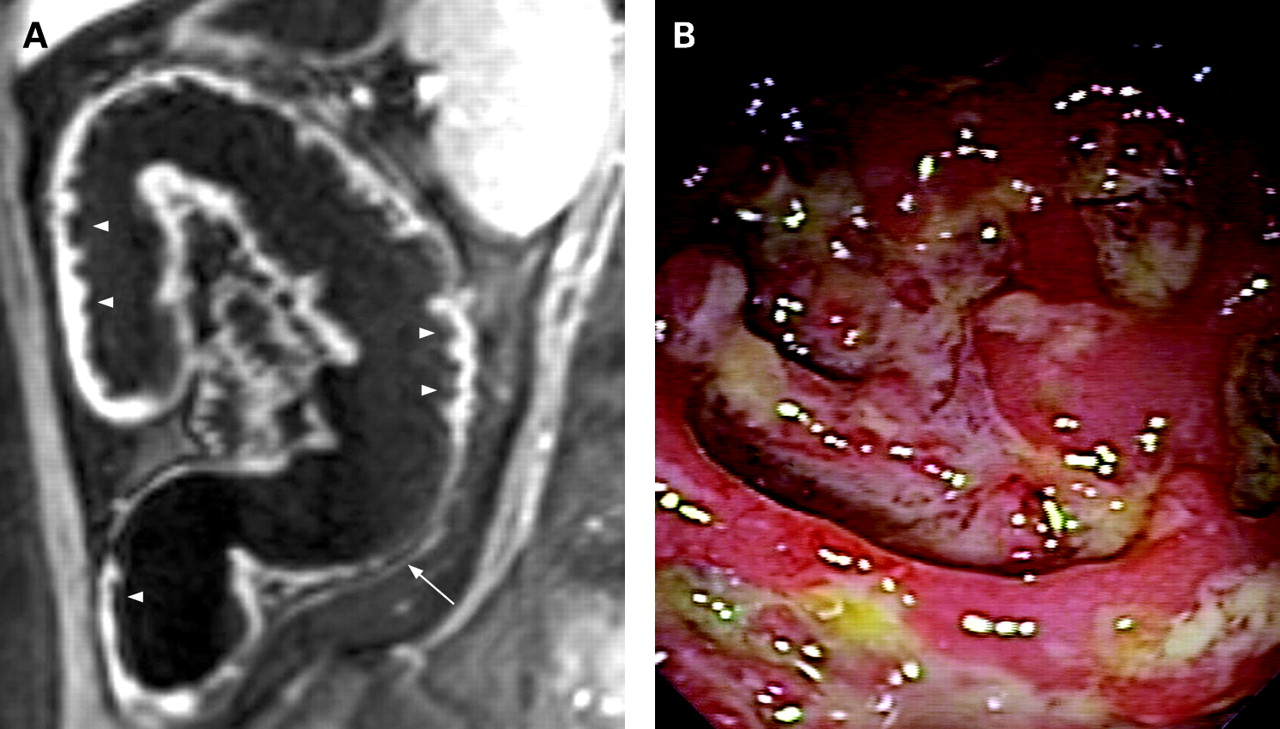
Sagital T1-VIBE (volumetric interpolated breath-hold examination) after intravenous contrast administration of the descending colon and splenic flexure showing discontinuous lesions with segmental thickening of the colon wall and deep ulcers (arrowheads) alternating with a segment without inflammatory changes (arrow) (A); colonoscopy of the same segment shows the presence of deep ulcers in the mucosa (B).
Interobserver agreement in the evaluation of MR changes was very high. The kappa index was 0.96 (p<0.001) for the presence of oedema, 0.87 (p<0.001) for ulcers, 0.92 (p<0.001) for lymph nodes and 0.85 (p<0.001) for pseudopolyps. The intraclass correlation coefficients were 0.91 (p<0.001) for wall thickness, 0.73 (p<0.001) for basal signal intensity and 0.93 (p<0.001) for contrast signal intensity.
Predictors of disease activity and severity in MR
To determine which of the MR findings had an independent predictive value for the presence of disease activity at endoscopy, the presence of ulcers at endoscopy or to predict the quantitative CDEIS value for a particular segment, the variable presence of lymph nodes was not introduced in the regression analyses, because this finding is not uniform in all anatomical locations. Since there was a highly significant correlation between contrast signal intensity and RCE, and the latter may be less influenced by technical characteristics of the MR equipment, only RCE was introduced in the regression analyses.
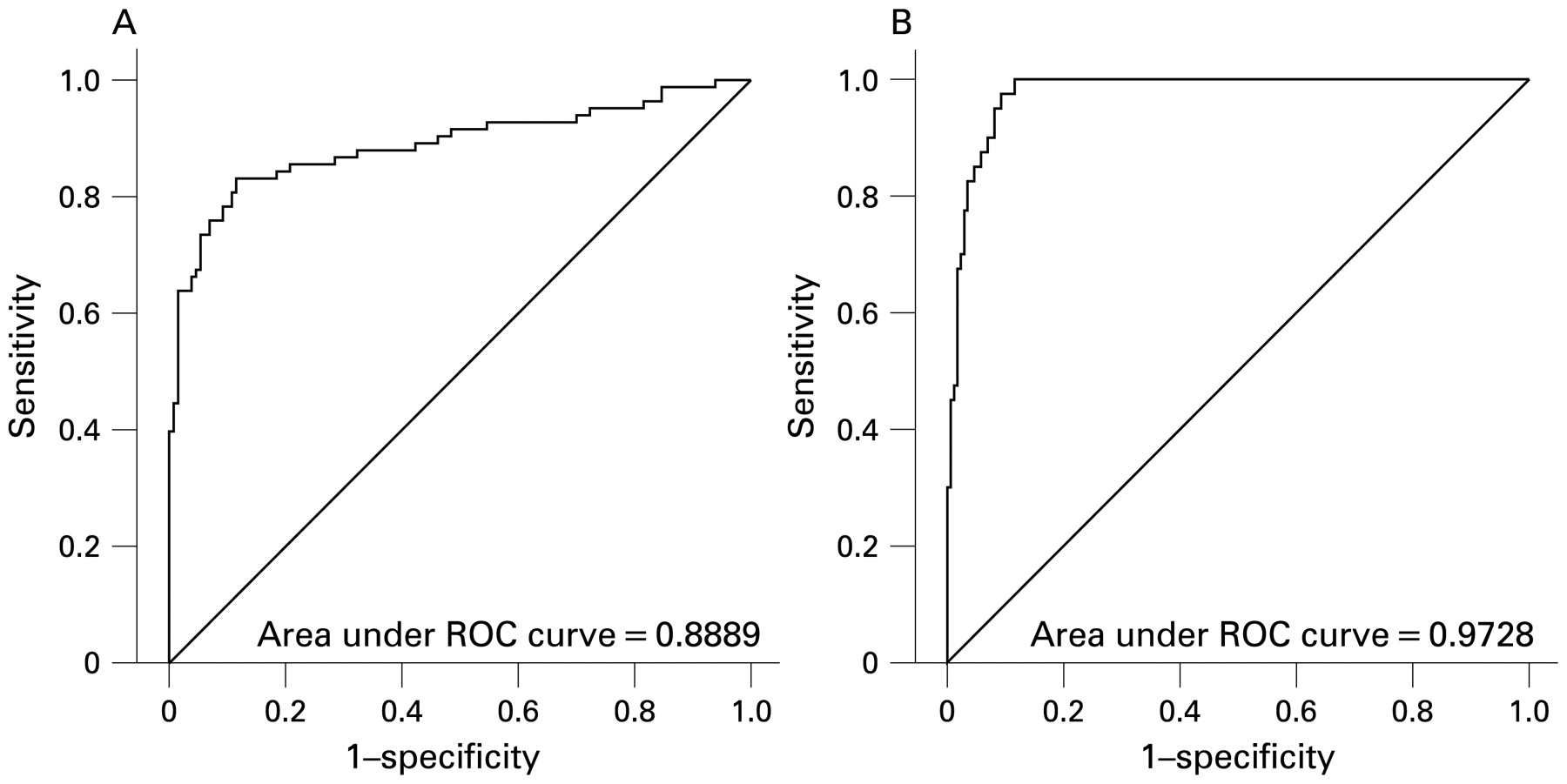
The only MR findings that were independent predictors of the presence of active disease at endoscopy, with either mild or severe lesions, were wall thickness (p<0.001) and RCE (p = 0.013). The accuracy of a score based on these variables to predict active disease was high, with an area under the ROC curve of 0.89 (fig 4A), and sensitivity and specificity >0.8. We performed an internal validation of the model by bootstrapping, and in 997 replications of random sampling the frequency of occurrence of wall thickness as a predictor was 100% and that of RCE 54%.
Logistic regression analysis showed that independent predictors of the presence of ulcers at endoscopy were wall thickness (p<0.001), RCE (p = 0.03) and identification of ulcers at MR (p = 0.003). The accuracy of a score based on these variables to predict the presence of ulcerations at endoscopy was high, with an area under the ROC curve of 0.97 (fig 4B), sensitivity of 0.9 and specificity of 0.94. Bootstrapping analysis showed that the predictors were robust, confirming all the variables from logistic regression, with wall thickness appearing in 91%, presence of ulcer at MR in 73% and RCE in 57% of the replications.

Receiver operating characteristic (ROC) curves, of a magnetic resonance-based index to predict presence of active disease (A) and presence of ulcerative lesions (B) in Crohn’s disease.
Since data distribution for CDEIS of segments was not normal, with 60% of segments having no significant lesions, a tobit regression analysis was applied. This analysis demonstrated that independent predictors for CDEIS are wall thickness (p = 0.007), RCE (p = 0.01), presence of oedema (p = 0.02) and presence of ulcers at MR (p = 0.003). There was a high and significant correlation coefficient between the CDEIS of the segment and the MR index calculated according to the logistic regression analysis coefficients (r = 0.82, p<0.001).
From the latter analysis we derived a simplified score (Magnetic Resonance Index of Activity) to quantify disease activity based on MR findings in each segment as follows:
MRIA (segment) = 1.5×wall thickness (mm)+0.02×RCE+5×oedema+10×ulceration.
The calculated simplified MRIA index also has a high (r = 0.81) and significant (p<0.001) correlation with the CEDEIS of the corresponding segment. The simplified MRIA in fact had a high correlation (r = 0.997) with the index calculated directly from the truncated logistic regression. MRIA range was 3.4–35.0; the index has a high accuracy for the detection of disease activity (area under the ROC curve 0.891, sensitivity 0.81, specificity 0.89, using a cut-off point of 7.3) and for the detection of ulcerative lesions (area under the ROC curve 0.978, sensitivity 0.95, specificity 0.91, using a cut-off point of 9.6) in the colon and terminal ileum.
Comparison of MR and other measures of disease activity
A global MRIA was calculated by adding the values of rectum, sigmoid, descending, transverse and ascending colon and ileum. A significant correlation of the global MRAI index was observed with CDEIS (r = 0.78, p<0.001) (fig 5), Harvey–Bradshaw index (r = 0.56, p<0.001) and CRP (r = 0.53, p<0.001). Correlations of CDEIS with the Harvey–Bradshaw index (r = 0.59, p<0.001) and CRP (r = 0.42, p<0.01) were of similar magnitude to those of the MRAI index.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between the Crohn’s Disease Endoscopic Index of Severity (CDEIS) and the global Magnetic Resonance Index of Activity (MRIA).
DISCUSSION
In this prospective study we provide evidence that the magnitude of quantitative MR changes such as wall thickening, contrast signal intensity and RCE closely parallel the severity of endoscopic lesions; and also the presence of oedema, ulcers, enlarged lymph nodes and pseudopolyps is significantly more prevalent in intestinal segments with more severe endoscopic lesions. This allowed the creation of an MR index of activity composed of the factors with independent predictive value that has a high accuracy for the detection of disease activity and presence of ulceration and is highly correlated with CDEIS.
MR technical advances including ultra-high-field strength body MR, capability of providing fast multiplanar images with excellent soft tissue contrast, requirement for minimally invasive procedures, and lack of radiation exposure allowing repeated assessments over time render MR a potentially valuable technique for evaluation of patients with CD.14–17 Previous studies in patients with CD have predominantly evaluated the diagnostic potential of MR for small bowel lesions, showing promising results. However, data regarding the diagnostic accuracy of MR for colonic lesions are so far scarce and controversial. Whereas results reported by Narin et al9 and Ajaj et al5 provide an acceptable concordance of findings between MR and endoscopy for the detection of disease activity (sensitivity of 87–89% and specificity of 85–100%), Schreyer et al8 and Dintel et al6 reported only discrete results (sensitivity of 32–64% and specificity of 81–100%), suggesting that the technique may not be adequate for evaluation of CD lesions. Discrepancy between these results can be partially explained on the basis of technical aspects. The study of Schreyer et al employed the “bright lumen” MR technique, using a rectal enema of gadolinium that produces a hypersignal on both T1 and T2 sequences and can partially mask the enhancement and mural thickening of the colonic wall. More recently, “dark lumen” MR is increasingly applied, as we did in the current study. Using a water rectal enema produces intraluminal hypointensity on T1 sequences, achieving a high contrast with a bright bowel wall after intravenous contrast administration. In two studies, Dintel et al6 and Langhorst et al7 evaluated the inflammatory changes in the colon using “dark lumen” MR but without bowel cleansing; this can hamper the identification of inflammatory changes due to difficulties in establishing precise measurements of wall thickness and obscuring the presence of ulcerations. Similar to our study, Narin et al9 and Ajaj et al5 applied “dark lumen” MR with bowel cleansing to evaluate the colon in CD, showing in both cases a high accuracy of MR for the detection of lesions. However, both trials included a relatively small number of patients, and made only a qualitative analysis of MR findings. Considering our results together with previous evidence, we suggest that dark lumen MR with bowel cleansing is probably the current best choice to evaluate inflammatory changes in the colon using this imaging modality. The optimal timing of data acquisition for MR colonography is somewhat controversial. We begin the acquisition 70 s after the initiation of the bolus, based on previously reported studies.5 18 This phase allows assessment of mucosal and mural enhancement as well as visualisation of abdominal viscera. Others have suggested an enterography phase (∼45 s after bolus injection) for better detection of mucosal enhancement, but it seems that this provides no contribution to the assessment of CD activity.19
An aspect that may have contributed to the high diagnostic accuracy in our study is the use of a 3.0 T MR unit. The images obtained with 3.0 T have a better signal and higher spatial resolution than those obtained with 1.5 T, contributing to increasing the sensitivity for lesion detection.17 20 Some artefacts are associated with the use of a 3.0 T MR unit, in particular magnetic susceptibility artefacts that appear on T2 sequences in the presence of paramagnetic objects (eg, surgical suture in ileocolic anastomosis). Nevertheless, these artefacts do not usually represent a limitation for evaluation of potential inflammatory changes because the extension of the inflammatory tissue is larger than the artefact. Also, an additional measure to reduce susceptibility artefacts is the use of fast turbo spin-echo T2 sequences (eg, HASTE).21
Both MR and CT techniques emerge as excellent techniques to assess inflammatory activity and detection of extraintestinal complications in CD.2 14 22–24 CT provides a better spatial resolution than MR, has greater availability and is less time consuming. However, MR provides better soft tissue contrast and uses non-ionising radiation. It has been estimated that CT examinations account for most of the irradiation exposure in patients with IBD.3 25The long-term cumulative effect of this radiation in combination with co-exposure to potentially synergistic agents such as methotrexate may increase the risk of neoplasia in these patients.25 Finally, as for MR, studies on the accuracy of CT in the evaluation of CD focused on the detection of lesions in the small bowel. The only prospective study evaluating the value of CT for the characterisation of inflammatory lesions in the colon suggests a limited sensitivity of CT, although only the mucosal alterations, and not wall thickness and contrast enhancement, were considered.26
Doppler ultrasonography represents another non-ionising imaging technique which may provide information about disease activity.27 28 However, the difficulty of visualisation of deep bowel segments and high interobserver variability represent significant drawbacks. Finally, 99mTc hexamethyl-propylamine-oxim leucocyte scintigraphy is a non-invasive technique, but radiation exposure and limited sensitivity, especially in patients receiving steroid treatment, are leading to a reduced used of this technique.29
MR examination of the small bowel requires oral luminal contrast to achieve adequate distension. MR enteroclysis allows better small bowel distention than MR follow-through. However, nasojejunal tube placement entails radiation exposure and produces discomfort, and consequently movement artefacts are more frequent. The only study comparing both modalities concluded that bowel distension was inferior in MR follow-through, but diagnostic accuracy was similar in both methods.30 In our study, oral ingestion of the luminal contrast provided adequate distension of the distal ileum, the segment we compared with endoscopy. MR enteroclysis might be necessary in selected cases in which upper CD lesions are suspected and adequate distension is not achieved with oral administration of the luminal contrast.
Because the location of CD lesions in the intestine has a characteristic skip pattern, in which segments with severe ulcerative lesions can be adjacent to others with normal mucosa, we evaluated the MR findings associated with lesions of different endoscopic severity in a segment by segment analysis as in previous studies4 8 24 and also as a global MR index of activity. MR changes found to be associated with disease activity and severity in the current study include oedema, presence of ulcers, wall thickening and RCE. In our study, these four parameters were independent predictors of the presence and severity of disease activity. This finding is in keeping with previous studies focused mainly on the small intestine.5 14 31 32 Mural oedema is a characteristic feature of active inflammation of the bowel wall, and can be detected as an increase of signal on T2-wedged sequences. In severe involvement, odema can extend to the mesentery. Mural thickening is well correlated with the presence of activity and with severity. Using a three-dimensional VIBE sequence, wall thickening can be evaluated at any plane of space. Based on both bowel wall thickening and RCE, inflammatory changes can be detected with great accuracy and played a dominant role in the detection of bowel inflammation.
Other parameters previously related to inflammatory changes include enlarged mesenteric lymph nodes and loss of haustra folds.4 5 We did not include haustra length in our analysis because of its variability between the proximal and distal colon. Also, long-standing CD can induce shortening of colonic haustra secondary to fibrosis in the submucosa.33 The presence of enlarged lymph nodes has great variability depending on the anatomic location and patient age (more frequent in the young population).34 Additionally, prevalence of enlarged lymph nodes in our series was low.
Demonstration of the high accuracy of MR in detecting the presence of disease activity and differentiating the presence or absence of ulcers is of considerable clinical relevance given the prognostic implications of the presence or persistence of ulcerative lesions in terms of disease course and surgical requirements.35 The MRIA we propose in the current study may be useful to categorise disease severity in a given patient, and to monitor responses to therapeutic interventions both in the clinical setting and in therapeutic trials.
One of the limitations of the current study is the lack of validation of the results in an independent cohort. While these results are not available, we provide an internal validation of the results using bootstrapping. The variables that were independent predictors of the presence of disease activity or the presence of ulcerations were validated by this approach. Also, the magnitude of changes in MRIA in response to treatment and their correlation with changes in the CDEIS need to be characterised in future studies. Furthermore, development of an effective tagging method will probably improve the patient acceptance of MR since one of the main drawbacks of the technique is the need for bowel cleansing.
Overall, the results provided in the current study lead to the suggestion that MR may be considered as an alternative to endoscopy in cases with an established diagnosis of ileocolonic CD in which biopsy samples are not necessary. MR has significant advantages over colonoscopy, including the ability provide a complete assessment of the ileocolonic region in all patients, as compared with 72% of complete ileocolonoscopies in our series, a proportion very similar to previous observations. As performed in our study, administration of oral contrast and an enema for MR may produce slight discomfort in some patients, but anaesthesia is not required as for ileocolonoscopy. The possibility of identifying inflammatory lesions in all locations of the gastrointestinal tract, and also extraluminal complications, in just one examination represents a clear advantage of MR over colonoscopy for evaluation of CD.
Acknowledgments
This work has been supported by grant PI07/90253 from the Ministerio de Sanidad, Spain.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: The ethics committee of the Hospital Clínic of Barcelona approved the project
Linked Articles
- Digest