Article Text

Abstract
Introduction Benefits of immunosuppressive therapy in Crohn's disease have been demonstrated in controlled trials; however, it is unclear whether these drugs alter the longer-term natural history of this condition.
Aims and Methods To assess changes in disease outcomes in a population-based cohort of patients diagnosed in Cardiff from 1986 to 2003. Case notes from Crohn's disease incidence studies in Cardiff were reviewed retrospectively for disease characteristics and follow-up information on drug therapy, and the need for surgery for Crohn's disease. The study population was divided into three groups by year of diagnosis (Group A=1986–1991, Group B=1992–1997 and Group C=1998–2003).
Results 341 patients were included. Kaplan–Meier (KM) analysis showed increasing use of immunosuppressants over time. At 5 years after diagnosis this was 11% in Group A, 28% in Group B, and 45% in Group C (p=0.001) and the median time to start of thiopurines was 77, 21 and 11 months in Group A, B and C respectively. There was a significant reduction in long-term steroid use at 5 years post diagnosis: 45 (44%), 31 (31%) and 24 (19%) patients in Group A, B and C respectively (p=0.001). KM analysis showed a significant reduction in the cumulative probability of intestinal surgery: At 5 years this was 59% (Group A), 37% (Group B) and 25% (Group C) (p=0.001). In a multivariate Cox analysis, year of diagnosis, disease location, oral corticosteroids within 3 months of diagnosis and early thiopurine use (within the first year of diagnosis) were all independent factors affecting likelihood of intestinal surgery.
Conclusion This population-based cohort shows marked changes in rates of surgery, and the reduction is independently associated with year of diagnosis, and associated temporally with increased and earlier thiopurine use.
- 6-mercaptopurine
- azathioprine
- Crohn's disease
- IBD clinical
- surgical resection
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Medical therapy for Crohn's disease has changed dramatically over the past 20 years with increasing use of immunosuppressive drugs
It has been difficult to demonstrate an association between increased azathioprine use and decreased Crohn's disease surgical resection rates
What are the new findings?
Resection rates for Crohn's disease have fallen significantly in Cardiff from 1986 to 2003
Overall use and early (within 1 year of diagnosis) use of thiopurines have increased, and long-term corticosteroid use (more than 1 year) have reduced significantly during this time
Multivariate analysis shows that early thiopurine use, colonic disease location, and more recent diagnosis are associated with lower rates of intestinal surgery
Multivariate analysis shows that early corticosteroids (within 3 months of diagnosis) and stricturing behaviour at diagnosis are associated with higher rates of intestinal surgery
How might it impact on clinical practice in the foreseeable future?
Patients should be advised that the likelihood of surgery for Crohn's disease is much lower than it was in the past
The association between early thiopurine use and reduced intestinal surgery rates merits further investigation
Background
Crohn's disease is an inflammatory bowel disease with a chronic, potentially debilitating clinical course. Information on disease outcomes, including the likelihood of surgery, and the results of drug therapy, are important for patients, and for planning health resources. As surgery is not curative in Crohn's disease, bowel resection is highly significant, and stoma formation a life-changing event for patients. Numerous reports on disease outcomes in Crohn's disease have been published, but many are from referral centres, and there are relatively few population-based studies. The British Society of Gastroenterology guidelines state that at least 50% of patients are likely to require surgical treatment in the first 10 years of disease and approximately 70–80% will require surgery in their lifetime.1 Surgical resection rates over time vary widely amongst published studies, ranging from 25% to 61% at 5 years in a recent review,2 which concluded that there was little evidence that disease outcomes for Crohn's disease had changed over the past four decades. Jess et al3 showed that early surgery (within 1 year of diagnosis) has fallen from 35% (1962–1987) to 12% (2003–2004). Medical therapy for Crohn's disease has changed markedly over the past 25 years. Immunosuppressive therapy has increased during this time with azathioprine and 6-mercaptopurine being the most widely used, and the efficacy of these drugs in Crohn's disease has been shown in clinical trials (maximum 2 years).4–8 It has been more difficult, however, to show that early and widespread use of these drugs have reduced surgical rates in routine practice, or altered the long-term outcomes. A recent study from France9 10 did not show a reduction in the need for intestinal surgery in spite of increasing use of immunosuppressants. Anti-tumour necrosis factor therapies are now becoming widespread, but most centres are not routinely using these drugs, and thiopurines at present remain the most widely used immunosuppressive therapy.
Data on incidence of Crohn's disease in the city of Cardiff has been collected over many years with data available up to 2005. This well-defined population-based cohort gave an opportunity to evaluate changes in natural history. The aims of the study were to evaluate rates of surgery and drug therapy in patients diagnosed between 1986 and 2003 during which time there was a large increase in the use of immunosuppressant therapy, particularly azathioprine.
Methods
Study design
The study included all patients diagnosed with Crohn's disease who were residents in the city of Cardiff between 1986 and 2003, to give at least 5 years of post-diagnosis follow-up information, which was collected to December 2008. Patients were those detailed in the Cardiff Crohn's disease incidence studies (1986–2005),11–13 and as previously described, the diagnosis of Crohn's disease was based on the Lennard-Jones diagnostic criteria.14 Patients had been identified from records of weekly histopathology meetings, the pathology database, hospital patient administration system, (recording diagnosis for inpatients), and from clinic letters in the Department of Gastroenterology and Paediatrics at the University Hospital of Wales and Llandough hospital. Patients who were not resident in the city of Cardiff, but who were tertiary referrals, or who had moved after diagnosis elsewhere had been excluded to give a population-based cohort. Where information was not available from the medical records and those who were lost to follow-up, we contacted the general practitioners and some of the patients with a follow-up questionnaire. Patients were divided into three 6-year periods (hexiles): Group A=1986–1991, Group B=1992–1997, and Group C=1998–2003 based on the year of diagnosis.
The medical records were reviewed retrospectively for patient demographics, disease characteristics, drug treatments and information on any surgical procedures and resections. Patient demographics included age at diagnosis, year of diagnosis, sex, smoking status at diagnosis and whether they were lost to follow-up. Disease characteristics included disease distribution (as documented by any investigations within the first year of diagnosis) based on the Montreal classification (L1=terminal ileum, L2=colonic, L3=ileo-colonic, L4=upper GI).15 Peri-anal disease was defined as such if specific therapy was required (abscess drainage, insertion of setons, or antibiotic or drug therapy). Information on medication use was collected, including corticosteroid therapy (prednisolone or budesonide, time to commencement, initial dose and duration of corticosteroid treatment, long-term steroid use). Long-term corticosteroid use was defined as 1 year or more of therapy during which there was no more than 8 weeks break before restarting. Early corticosteroid use was defined as treatment starting within 3 months of diagnosis. Details of immunomodulator therapy (including azathioprine and 6-mercaptopurine, methotrexate and infliximab) included time to commencement, maximum dose tolerated, side-effects, and duration. During this time, thiopurine therapy was used as second-line therapy, much as described in the European Crohn's and Colitis Organisation (ECCO) guidelines,16 with azathioprine generally used initially, but occasional first-line 6-mercaptupurine. Target doses were generally 2 mg/kg for azathioprine, 1 mg/kg for 6-mercaptopurine (unless limited by side-effects) but lower doses were often used prior to 1995. Methotrexate was occasionally used for thiopurine intolerance or failure. Infliximab was only used for refractory disease, and use has increased slowly since 2000. Details of all surgical procedures and resections performed for Crohn's disease were collected, including time to surgery. Operations were classified as intestinal surgery if there was resection of bowel, stricturoplasty or defunctioning stoma formation. Other operations included abscess drainage, examination under anaesthetic, and insertion of setons for perianal fistulae. Analysis was performed for intestinal surgery, for any surgical procedure, and for stoma formation. Information on mortality from all causes during follow-up was recorded.
Statistics
Continuous variables are presented as median and ranges. Comparison of groups was made by the Kruskal–Wallis test. Categorical variables are presented as percentages and comparison of frequencies was made by the χ2 test. Outcomes up to 5 years from diagnosis are presented, except where stated otherwise. Kaplan–Meier analysis was used to estimate the cumulative probability of receiving oral corticosteroids, thiopurine therapy (azathioprine or 6-mercaptopurine) or of undergoing surgery. Kaplan–Meier curves were compared by log rank (Mantel–Cox) test, both overall and pairwise. Factors that may affect the likelihood of intestinal surgery over time were investigated using Cox proportional hazard regression models. Univariate analysis was performed and results presented as hazard ratios (HRs). Multivariate analysis was performed in a stepwise analysis (using variables that were significant in the univariate analysis) to assess factors independently influencing likelihood of intestinal surgery. Data was analysed by SPSS software (version 16.0). A p value of ≤0.05 was considered significant.
Results
Three hundred and forty-one residents in the city of Cardiff were diagnosed with Crohn's disease in the 18-year period from 1986 to 2003. There were 105 patients in Group A (diagnosed 1986–1991), 99 in Group B (diagnosed 1992–1997) and 137 in Group C (diagnosed 1998–2003). Follow-up information was collected where available up to December 2008. The median length of follow-up overall was 92 months (range 41–261 months). Median (range) follow-up for Group A was 168 (49–261) months, for Group B 111 (60–244) months and for Group C 73 (41–100) months, p<0.001, with an overall 3171 patient-years of follow-up. Five-year follow-up information was available in 330 (97%) patients. Of those with 5 year follow-up, the data was obtained from hospital case notes in 307 patients, and for those who had moved or been discharged, from general practitioners (17 patients) and direct contact with six patients by telephone questionnaire. The patient characteristics at diagnosis in the three groups are shown in table 1. There was a female predominance (female to male ratio 1.66:1), as documented in previous incidence studies.13 In Group A, 49% were smokers at time of diagnosis, and this was lower in Group B (39%) and Group C (41%), but this was not statistically significant. The median age at diagnosis was 30 (range 4 to 86 years). There was a trend towards more ileocolonic and colonic disease distribution at diagnosis in groups B and C, with less terminal ileal distribution but these differences were not statistically significant. Isolated colonic disease (45%) was the commonest disease distribution at diagnosis in the entire cohort. Disease behaviour at diagnosis is also shown, along with behaviour at the end of follow-up. Because the length of follow-up differed between the groups, statistical analysis was not performed using final disease behaviour data.
Patient details at diagnosis
Corticosteroid therapy
Oral corticosteroids were used in 272 (80%) patients at any time during follow-up. In 216 (63%) patients corticosteroids were started within 3 months of diagnosis (table 2). At 5 years, 259 (76%) had received corticosteroids. Only 13 patients received their first corticosteroid therapy later than 5 years from diagnosis. Most received prednisolone initially (n=233) with the rest receiving budesonide (n=39). The proportion using corticosteroids at any time, or within 3 months of diagnosis did not differ significantly between the three groups (table 2), but there was a significant reduction in long-term corticosteroid use within the first 5 years of diagnosis over time, with 45 (44%), 31 (31%) and 24 (19%) patients in Groups A, B and C, respectively, receiving corticosteroids for more than 1 year, with no more than 2 months break during that time (p=0.001). Most on long-term corticosteroids were on prednisolone (98) with only two on budesonide.
Drug therapy 1986–2003: number (percentage)
Immunosuppressant therapy
Thiopurines were commenced in 129 patients (38%) overall (azathioprine in 117, 6–mercaptopurine in 12). Median dose was 100 mg for azathioprine (range 25–200 mg) and 100 mg for 6-mercaptopurine (range 75–125 mg). The median azathioprine dose rose from 75 mg (group A) to 100 mg (group B) and 125 mg (Group C), p<0.001. Between 1986 and 2003 there was a significant increase in the early and overall use of thiopurines. Early use (within 1 year of diagnosis) increased from 3% in Group A to 12% in Group B and 25% in Group C (p=0.001). Five years after diagnosis, thiopurines had been used in 11% of Group A, 28% Group B, and 45% Group C as shown in table 2 (p=0.001). Kaplan–Meier curves for time to start of thiopurines are shown in figure 1. The median time to start of thiopurines was 77, 21 and 11 months in Group A, B and C respectively (figure 2) and differences between the three groups were highly significant (p=0.001). The median duration of thiopurine treatment during the 5 years from diagnosis was 19 months overall, rising from a median of 14 months in Group A, and 16 months in Group B, to 23 months in Group C (p=0.001). Overall, toxicity occurred in 28/129 patients (21.7%). This included 14 with nausea and/or vomiting, six with headache, four with neutropenia, two with flu-like illness, one malignant melanoma and one with portal pyaemia. The thiopurines were stopped in 22, and continued in reduced dose in six.

Kaplan–Meier curve showing time from diagnosis to start of thiopurine therapy in the three hexiles. Group A versus B p<0.001; Group A versus C p<0.001; Group B versus C p=0.021.

Box-and-whisker plot showing time from diagnosis to start of thiopurines in the three hexiles. p=0.001 overall.
There was a small number of patients treated with methotrexate (n=9), all after failure or intolerance of thiopurines. Infliximab was used in 22 patients, all in Group C (16%), and all were receiving concomitant thiopurine or methotrexate treatment. The median time to start of infliximab was 20 months from diagnosis.
Surgical therapy
There were a total of 148 (43%) patients who had intestinal surgery. A further 18 (5%) had other surgical procedures. Details of first intestinal surgery are shown in table 3. Twenty patients had two intestinal surgeries, seven had three, and four patients had four operations for Crohn's disease during follow-up. Ileocaecal resection was the commonest procedure overall. The commonest second resection was defunctioning ileostomy (n=6), followed by left hemicolectomy (n=5), stricturoplasty (n=4) followed by one each of subtotal colectomy, left hemicolectomy, completion proctectomy, defunctioning colostomy and a right hemicolectomy. Thirty-one patients had a surgical intervention at diagnosis and 26 of these were resections. The time to first intestinal surgery is shown by Kaplan–Meier curve in figure 3. There was a significant increase in time to first surgery between the three groups (p=0.001). At 1 year, the proportions having intestinal surgery did not differ (table 4), but at 5 years the proportion was significantly less in the later groups (59%, 37% and 25%, respectively, in Group A, B and C, p=0.001). There was also a significant reduction in patients having any surgical procedure (intestinal surgery or surgery for perianal disease) in the later groups and this was 60% in Group A, 42% in Group B and 35% in Group C at 5 years post diagnosis (p=0.017). There was a reduction in the number of patients having ileostomy or colostomy within 5 years of diagnosis, with eight patients in group A, and one each in group B and C (p=0.007). The 18 non-resection operations were all drainage of perianal abscess or examination under anaesthetic with insertion of setons for fistulising perianal disease (2, 5 and 11 in Group A, B and C, respectively, p=0.1).
Details of first intestinal surgery for Crohn's disease (at any time during follow-up)
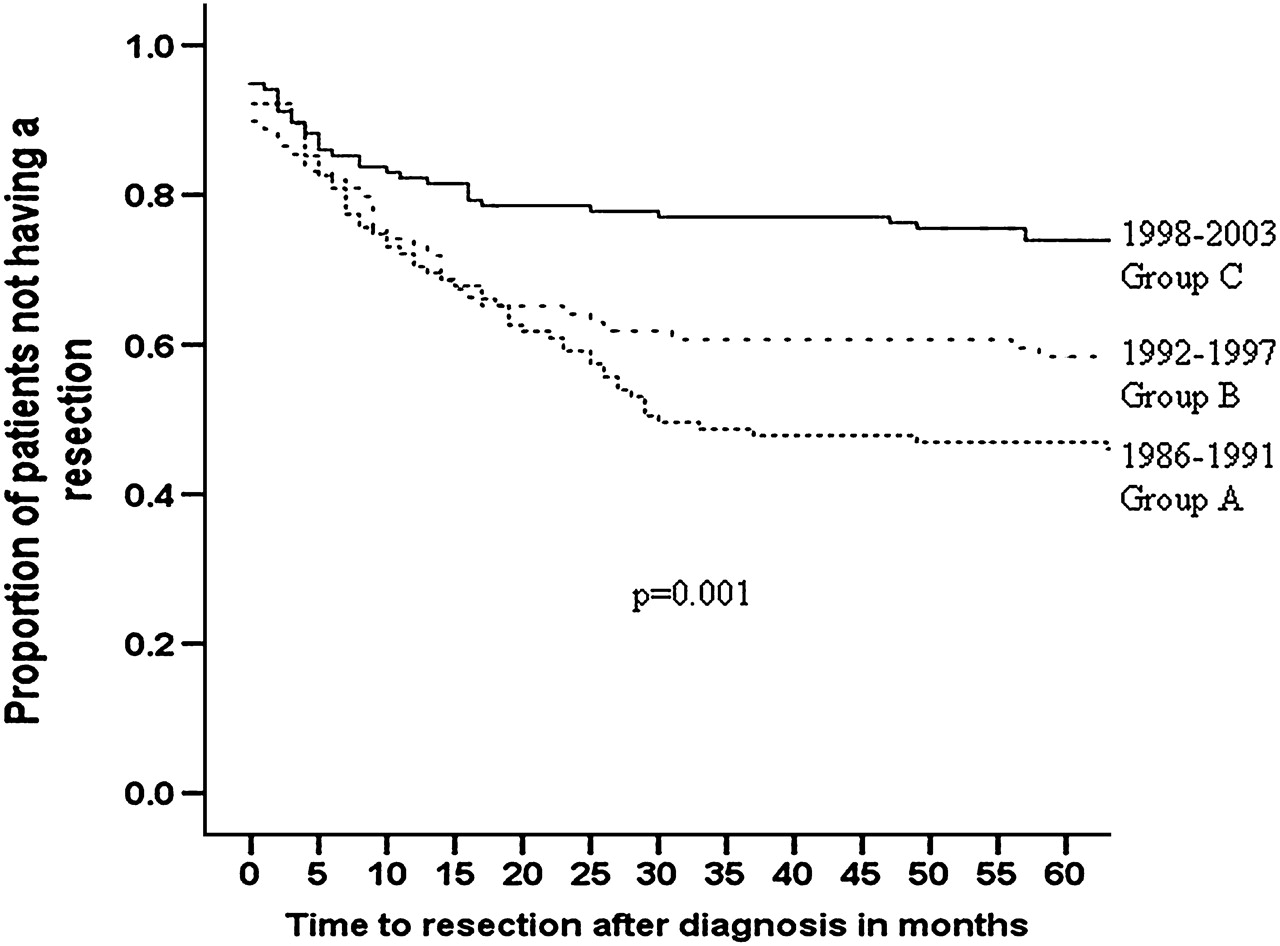
Kaplan–Meier curve showing time from diagnosis to first intestinal surgery in the three hexiles. Group A versus B p= not significant; Group A versus C p<0.001; Group B versus C p=0.007.
Number of patients with intestinal surgery for Crohn's disease at diagnosis and follow-up
Factors influencing intestinal surgery
Patients with terminal ileal disease at diagnosis (L1) had increased likelihood of intestinal surgery, and colonic or ileocolonic distribution had reduced likelihood of surgery, as shown in figure 4. In a univariate Cox regression analysis, early use of thiopurines (within the first year of diagnosis), year of diagnosis and isolated colonic involvement at diagnosis were associated with decreased risk of intestinal surgery. Oral corticosteroid use within 3 months of diagnosis, terminal ileal distribution, and stricturing disease at diagnosis were associated with increased risk of intestinal surgery, as was young age at diagnosis (table 5). Disease behaviour at follow-up was also associated with likelihood of resection, increasing with both stricturing disease (HR 2.3 (95% CI 1.6 to 3.3), p<0.001) and penetrating disease at follow-up (HR 1.7 (1.1–2.6), p=0.02). In a multivariate Cox analysis, year of diagnosis, disease location, oral corticosteroid therapy within 3 months of diagnosis and early use of thiopurines (within the first year of diagnosis) were all independent factors affecting likelihood of intestinal surgery (table 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier curve showing time from diagnosis to first intestinal surgery according to disease location at diagnosis (Montreal classification). L1 versus L2 p<0.001; L1 versus L3 and L1 versus L4 p=not significant; L2 versus L3 p=0.002; L2 versus L4 and L3 versus L4 p=not significant.
Univariate Cox analysis showing hazard ratios (HRs) for variables affecting risk of intestinal surgery
Stepwise multivariate Cox model showing hazard ratios (HRs) for variables affecting risk of intestinal surgery
Mortality and malignancies
There were 16 deaths during the 3171 patient years of follow-up. There were four, six and six deaths in Group A, B and C, respectively. Among these patients six were current or previous smokers. Two patients in Group A and Group C died from metastatic lung cancer (neither on immunosuppressants). There was one patient with terminal ileal Crohn's disease on azathioprine diagnosed in 1992 who had developed metastatic colorectal cancer. One patient developed malignant melanoma after 3 years on azathioprine, which was removed surgically, with no recurrence. There was no other malignancy, opportunistic infections or serious toxicities related to immunosuppressive therapy during follow-up, and in particular, no lymphoma diagnosed in this cohort.
Discussion
The Cardiff population has well documented incidence of Crohn's disease extending back to the 1930s.13 The incidence in Cardiff was 66.4/106/year (95% CI 57.9 to 76.1) in the period 1996–2005.13 The study period of the present paper, 1986–2003, corresponds to major changes in the use of immunosuppressive therapy, with much wider usage and early use of azathioprine particularly, such that 45% in the most recent hexile (1998–2003) used the drug, with 25% receiving it within 1 year of diagnosis. Even in the most recent hexile, patients in this study were treated with thiopurine drugs as second-line therapy, as in the ECCO guidelines.16 The levels of thiopurine use fits with that quoted in other studies, such as that from Paris,9 showing a rise from 4% using immunosuppressives in 1978–1982, to 63% in 1998–2002, although this is in a referral population, and may therefore have a higher proportion with more severe disease. Early use of thiopurines has increased, particularly in paediatric Crohn's following the study by Markowitz et al,17 with 61% of Crohn's disease patients under 17 at diagnosis receiving thiopurines at any time, in the EPIMAD registry from north to west France.18
This study does have some limitations. By its nature, as an observational study, we can only identify associations between increasing thiopurine use and decreased surgery rates, but of course many other changes have occurred during the study period. These include considerable changes in surgical practice, as discussed below. The reduction in smoking rates at diagnosis, although not statistically significant, is likely to have an impact, and we have incomplete data on numbers of patients who gave up smoking during follow-up. There have been far more aggressive smoking cessation interventions in our unit over the past 10 years. Differences in disease distribution over time are also a major factor in likelihood of surgery. Multivariate analysis has limitations in showing independent associations. Data was gathered retrospectively, and we had no accurate measure of disease severity. This could only be inferred from drug use and surgical interventions. There is likely to be a confounding effect of immunosuppressive therapy being used for more severe disease, making it more difficult to demonstrate any protective effect. Overall thiopurine use was not used as a variable, because many patients started thiopurines after surgery. Of the 49 patients receiving early thiopurines, only one started after intestinal surgery. We focused predominantly on first intestinal surgery, and first use of immunosuppressive drugs. The number of subsequent resections was smaller, and so analysis of preventative effects of immunosuppressive therapy was not possible. Our data does have strengths, however. The population-based cohort means that tertiary referral effects are eliminated, and the results are representative of the UK Crohn's population generally. Five-year follow-up is also nearly complete with only 3% lost to follow-up.
The rates of intestinal surgery decreased during the study period from 59% at 5 years, to 25%. There is a wide variation in reported rates of surgery in the literature. Older population-based studies quote higher rates, such as the Danish population described by Munkholm et al19 with 47% at 5 years, rising to 61% after 10 years and 82% at 20 years. Rates of 61% at 5 years were reported from Stockholm County in a population cohort from 1955 to 1989.20 Surgical rates were lower (approximately 37%) in the National Cooperative Crohn's Disease Study from the USA in the 1970s.21 A more recent cohort diagnosed in 1990–1993 (the IBSEN study from Norway) reported 28% surgery at 5 years.22 An American non-population-based study showed a 3 year surgery rate of 24% in patients diagnosed in 1991–1997.23
During the study period 1986–2003, much has changed that could potentially affect rates of surgery for Crohn's disease. The availability of diagnostic tests has altered, surgical techniques, particularly use of laparoscopy have developed, and there is less use of defunctioning ileostomy formation in routine management of Crohn's disease. Segmental resections and stricturoplasty are more widely used than in the past. Clinical features of the disease may also have changed. The proportion of patients with colonic disease has slowly increased, with a fall in the number with isolated terminal ileal disease,13 although the differences in distribution did not differ significantly between our three groups in this study. The proportion with colonic disease in the Cardiff population is somewhat higher than in other studies, and remains unexplained. We also documented a trend towards a fall in the number of cigarette smokers at diagnosis across the three hexiles from 49% to 41%. Unlike other studies,23 we could not show an association between smoking and risk of resection. Our data was incomplete, however, for numbers of patients who gave up smoking after diagnosis, or after resection, and this number is likely to be considerable. Univariate analysis did show significant reduction in risk of intestinal surgery for patients with colonic disease at diagnosis, and increase in risk for those with terminal ileal disease, and stricturing disease behaviour. We had no way of assessing disease severity in this retrospective study, apart from the use of corticosteroids, and there was a significant increase in risk of intestinal surgery for those receiving corticosteroids within 3 months of diagnosis. An alternative explanation for the positive association between early corticosteroids and surgery is that these drugs adversely affect the natural history. This remains contentious. Thiopurine use within the first year was associated with a significantly reduced risk of operation. In the multivariate Cox model of risk factors for intestinal surgery, four factors remained independently predictive of surgery. These were early use of thiopurines, corticosteroids within 3 months, year of diagnosis and disease location. Other studies have found it difficult to show that increased use of thiopurines have reduced likelihood of surgery. The French study from Cosnes et al has been widely quoted as failing to show a reduced rate of surgery in successive cohorts of patients over time, in spite of the increased use of thiopurines.9 The reasons why this study differs in this respect to our study are many. They include data on both a locally diagnosed, and referral group; less complete follow-up (31% lost to follow-up), and many in the locally diagnosed group had early surgery (43%), or before receiving more than 3 months of immunosuppression.There was no change in surgical rates in three further studies,24–26 perhaps because they covered a shorter period (7–12 years), were non-population-based, coming from referral centres24 25 or a US nationwide inpatient survey,26 and largely covered a period where azathioprine use was already starting to plateau, although infliximab use was rising significantly. One study only evaluated small bowel resection.25 However, the EPIMAD study of paediatric Crohn's disease18 was able to demonstrate a protective association of the use of azathioprine on risk of surgery in a Cox multivariate model, and showed that the time to the commencement of azathioprine was shorter in non-surgical patients than in those requiring resection. It is possible that early use of azathioprine was much more widespread in these paediatric patients than in the Cosnes study.
In addition to changes in surgical resection rates, we have also shown a reduction in patients requiring ileostomy or colostomy over time. Numbers were too small for statistical assessment of association with immunosuppressive use. The impact of other changes over time, including changes in surgical practice (more segmental resections) and changes in disease distribution over time, may also be relevant. Although numbers of resections have fallen significantly, there was an increase in the number of surgical procedures for perianal Crohn's disease. Numbers of these operations rose from two in the earliest group, to 11 in the latest, and is likely directly related to a more conservative management approach in conjunction with medical therapy. Whilst overall corticosteroid use, and early use, did not differ over time, there was a fall in long-term corticosteroid use over 1 year or more, (allowing up to an 8 week gap for patients who relapsed after a tapering course and then restart). The strong temporal association suggests that this is a benefit of more widespread immunosuppressant usage.
The changes in intestinal surgery rates, stoma formation, and long-term corticosteroid are likely also to have been influenced by the introduction of infliximab. However, infliximab was only used in patients in the most recent hexile, (22/137 (16%), at a median of 20 months after diagnosis), and has remained a therapy for those with refractory disease failing other immunosuppressants. While we cannot separate out the effects of different immunosuppressants in this retrospective study, it is clear that many of the changes were evident between the first and second hexiles, and the association with early thiopurine use remains strong. There is a great deal of evidence that early infliximab use reduces hospitalisations and surgery,27 and it is likely that the continuing increase in early use of more aggressive immunosuppressive therapy will further alter the natural history of Crohn's.
Despite increased immunosuppressant use, we did not notice any direct medication related toxicity. No serious opportunistic infection, or leucopenia requiring hospital admission was noted. There were no lymphomas, but one adolescent patient developed a melanoma while on azathioprine. Our study is too small to give any accurate estimate of lymphoma or malignancy risk of immunosuppressants.
In summary, this population-based study has demonstrated marked and significant changes to the natural history of Crohn's over an 18-year period, with reduced rates of surgery, and reduction in long-term corticosteroids. A number of factors are likely to have resulted in falling intestinal surgery rates during this time. Although this study cannot prove causality, our data show an association with the earlier and more widespread use of immunosuppressive therapy.
Acknowledgments
We are grateful for statistical support in this study from Dr Angela Casbard, Cardiff University.
References
Footnotes
Competing interests ABH has served as a speaker and advisory board member for Schering Plough and has received research funding from Schering Plough.
Ethics approval Ethics approval was obtained from the South-East Wales Research Ethics Committee, and Cardiff and Vale NHS Trust Research and Development Committee.
Provenance and peer review Not commissioned; externally peer reviewed.