Article Text

Abstract
Background Mast cell activation is thought to be involved in visceral hypersensitivity, one of the main characteristics of the irritable bowel syndrome (IBS). A study was therefore undertaken to investigate the effect of the mast cell stabiliser ketotifen on rectal sensitivity and symptoms in patients with IBS.
Methods 60 patients with IBS underwent a barostat study to assess rectal sensitivity before and after 8 weeks of treatment. After the initial barostat, patients were randomised to receive ketotifen or placebo. IBS symptoms and health-related quality of life were scored. In addition, mast cells were quantified and spontaneous release of tryptase and histamine was determined in rectal biopsies and compared with biopsies from 22 age- and gender-matched healthy volunteers.
Results Ketotifen but not placebo increased the threshold for discomfort in patients with IBS with visceral hypersensitivity. This effect was not observed in normosensitive patients with IBS. Ketotifen significantly decreased abdominal pain and other IBS symptoms and improved quality of life. The number of mast cells in rectal biopsies and spontaneous release of tryptase were lower in patients with IBS than in healthy volunteers. Spontaneous release of histamine was mostly undetectable but was slightly increased in patients with IBS compared with healthy volunteers. Histamine and tryptase release were not altered by ketotifen.
Conclusions This study shows that ketotifen increases the threshold for discomfort in patients with IBS with visceral hypersensitivity, reduces IBS symptoms and improves health-related quality of life. Whether this effect is secondary to the mast cell stabilising properties of ketotifen or H1 receptor antagonism remains to be further investigated.
Trial Registration Number NTR39, ISRCTN22504486.
- Irritable bowel syndrome
- visceral hypersensitivity
- mast cell
- tryptase
- histamine
- ketotifen
- functional bowel disorder
Statistics from Altmetric.com
- Irritable bowel syndrome
- visceral hypersensitivity
- mast cell
- tryptase
- histamine
- ketotifen
- functional bowel disorder
Significance of this study
What is already known about this subject?
Visceral hypersensitivity is recognised as an important mechanism in irritable bowel syndrome (IBS).
There is growing evidence for an important role of mast cells in IBS.
In animal studies mast cell stabilisers decrease visceral perception.
Ketotifen is a mast cell stabiliser and an H1 receptor antagonist.
What are the new findings?
Ketotifen increased the threshold of discomfort in patients with IBS with visceral hypersensitivity.
Ketotifen improved IBS symptoms and quality of life.
There was, however, no relation between mast cell number, visceral perception and clinical outcome.
How might it impact on clinical practice in the foreseeable future?
Mast cell stabilisers and/or H1 receptor antagonists should be considered and further explored as a therapeutic approach in the treatment of patients with IBS.
Introduction
Visceral hypersensitivity or enhanced perceptual responses to controlled distension of the colon and rectosigmoid is recognised as an important mechanism in inflammatory bowel syndrome (IBS) and is present in 21–65% of patients with IBS.1 2 Although both central and peripheral factors may be involved, the exact pathophysiology of visceral hypersensitivity is not fully understood. There is, however, growing evidence that mast cells have an important role.3 The number of colonic mast cells is increased in animal models of visceral hypersensitivity. Similarly, in patients with IBS, an increased number of mast cells is found in the small intestine,4 large intestine5 6 and rectum.7 Second, the number of mucosal mast cells and proximity to sensory nerves in colonic tissue is positively correlated to abdominal pain.6 Third, mast cell activity measured as spontaneous release of histamine and tryptase is enhanced in the jejunal fluid4 and supernatant of colonic biopsies of patients with IBS.6 8 It should be emphasised, however, that the release of mediators into the supernatant may be non-physiological and could simply be a reflection of trauma to the biopsy. Fourth, exposure to the supernatant obtained from colonic biopsies of patients with IBS but not from healthy controls increases the excitability of rat mesenteric sensory nerves and induces visceral hypersensitivity in mice.8 9 Finally, in animal models, administration of the mast cell stabiliser doxantrazole prevents stress-induced and acetic acid-induced visceral hypersensitivity.10 To what extent findings in animal models apply to the human situation is, however, unclear. It therefore remains to be studied whether mast cells are indeed involved in visceral hypersensitivity to distension in man.
Activation of the mast cell occurs by cross-linking of immunoglobulin E (IgE) receptors or by non-IgE-related substances like cytokines, neuropeptides and complement components.11 When activated, mast cells degranulate by rapidly releasing mediators pre-stored in vesicles such as tryptase, histamine and several cytokines, thereby inducing an inflammatory response. Degranulation of mast cells is blocked by membrane stabilisers such as chromones (sodium cromoglycate) and ketotifen. At present, only a limited number of mast cell stabilisers is available for human use, including ketotifen. This drug is mainly used as an anti-asthmatic drug but is also reported to be effective in preventing mucosal damage and mast cell hyperplasia in a rat model of colitis12 and inducing clinical improvement in a subset of patients with inflammatory bowel disease.13 Accepting that mast cells may represent an important target, mast cell stabilisation could be a therapeutic approach to improve abnormal visceral perception. We designed a double-blind placebo controlled study to assess the effect of ketotifen on rectal sensitivity to distension, spontaneous mucosal tryptase release and IBS symptoms in patients fulfilling the Rome II criteria of IBS. The primary objective of the study was to evaluate the effect of mast cell stabilisation with ketotifen on visceral perception to rectal distension in hypersensitive patients with IBS. We also investigated whether the presence of an increased number of mast cells and/or increased spontaneous mucosal tryptase release is associated with visceral hypersensitivity to rectal distension and whether improvement in visceral perception results from alterations in these parameters. In addition, abdominal symptoms were monitored to evaluate the potential therapeutic benefit of mast cell stabilisation in patients with IBS.
Methods
Study subjects
Between January 2005 and December 2007, 108 patients from the gastrointestinal motility unit at the Academic Medical Centre, a tertiary referral centre, were assessed for eligibility. Of these, 60 patients with IBS (72% women, mean±SD age 36±2 years, range 19–65 years) were enrolled in the study. Twenty-two patients were excluded for not meeting the inclusion criteria, 25 refused to participate and one did not attend the first visit. Selection criteria included a positive diagnosis by the Rome II criteria of IBS. A minimum investigation to exclude organic disease included a careful history, normal physical examination, normal sigmoidoscopy, normal thyroid stimulating hormone levels, normal blood counts and negative stool examinations. Patients had to be free of concomitant diseases such as diabetes and cardiovascular disorders, including psychiatric disorders. Celiac disease was excluded in those patients with diarrhoea-predominant IBS by antibodies to anti-tissue transglutaminase and antibodies to anti-endomysium or duodenal biopsies. Biopsies of normal colonic tissue were routinely taken to exclude microscopic colitis. Medication likely to interfere with gastrointestinal function or analgesics was discontinued at least 7 days before entering the study. The use of histamine antagonists was an exclusion criterion for participation. Before the treatment period, biopsies of the descending colon were obtained during colonoscopy in 29 patients with IBS.
Twenty-two healthy volunteers (68% women, mean±SD age 30±3 years, range 20–61 years) free of abdominal symptoms were recruited by public advertisement and were invited to undergo a barostat study to assess rectal sensitivity. Rectal biopsies were taken at the same session. Fifteen of these healthy volunteers also underwent a colonoscopy on a separate occasion to obtain biopsies from the descending colon.
Study design
The patients with IBS were included in a placebo controlled double-blind randomised trial consisting of 2 weeks of screening, 8 weeks of treatment and 2 weeks of follow-up. After an initial barostat, hypersensitive and normosensitive patients14 were separately randomised 1:1 for either treatment with a daily dose of ketotifen or placebo. Patients were included and randomised by TKK. The randomisation code was generated by the pharmacy and stored there until the study was completed. Both the investigators and the patients were blinded to the treatment. All patients randomised to receive ketotifen started with 2 mg twice daily for 2 weeks, after which the dose was increased to 4 mg twice daily for another 2 weeks to reach a final dose of 6 mg twice daily during the last 4 weeks of the study. The number of pills was similarly increased in those patients randomised to receive placebo. After 8 weeks of treatment a second rectal barostat study was performed to assess the effect of treatment on rectal sensitivity. In addition, before and after treatment four rectal biopsies were collected, two for mast cell counts and two to determine the spontaneous release of tryptase.
Barostat studies
Rectal sensitivity to distension was assessed using an electronic barostat which automatically corrected for the compressibility of air (Distender Series II, G&J Electronics, Toronto, Ontario, Canada). The barostat was connected to a 500 ml polyethylene bag (maximal diameter 9 cm) tightly wrapped on the distal end of a double lumen polyvinyl tube (Salem Sump tube 14 Ch; Sherwood Medical, St Louis, Missouri, USA) introduced into the rectum.14 The barostat protocol is described in detail elsewhere.15 Briefly, subjects scored the perception of sensation evoked by rectal distension using a 6-point scale with verbal descriptors (0=no sensation; 1=first sensation; 2=first urge to defaecate; 3=normal urge to defaecate; 4=severe urge to defaecate; 5=discomfort/pain).
Immunohistochemistry: mast cell counts
For mast cell quantification, rectal and descending colon biopsies were fixed in formaldehyde immediately after collection and subsequently embedded in paraffin. Immunohistochemical staining was performed on 4 μm deparaffined sections. For antigen retrieval, the CD117 sections were heated for 10 min in TRIS-EDTA (pH 9). Sections were incubated with a primary monoclonal antibody directed against human mast cell tryptase (anti-human tryptase, Chemicon, Temecula, California, USA, mab1222) or a polyclonal antibody directed against human CD117 (anti-human C-kit/CD117, Dako, Glosturp, Denmark) for 1 h (concentration 1/900 for tryptase and 1/50 for CD117). The tryptase sections were reincubated with a secondary biotinylated anti-goat/anti-mouse immunoglobulin (Dako, 30 min) followed by ABC kit (Dako) for 30 min. The CD117 sections were reincubated with Powervision (poly-HRP anti-rabbit, Immunologic, Duiven, The Netherlands) for 30 min. Specific staining for both tryptase and CD117 was performed with AEC (Sigma, St Louis, Missouri, USA) for 10 min. Sections were counterstained with haematoxylin (Sigma) for 1 min. Negative controls were included and did not contain any specific staining. Tryptase and C-kit positive mast cells were subsequently quantified in 18 high power fields of each section by computer-assisted image analysis (Qwin Analysis System; Leica, Cambridge, UK) and expressed as mean number/mm2 mucosal tissue.
Histamine and tryptase release
To evaluate the spontaneous release of the mast cell mediators tryptase and histamine from rectal mucosal biopsies, we adapted a previously described method from Barbara and colleagues.6 Directly after sampling, two biopsies of the rectum were weighed and then immersed in 2 ml Hanks' solution (37°C) continuously oxygenated (95% O2/5% CO2). After 25 min of incubation, the solution was removed and centrifuged at 1700 rpm for 5 min. After centrifugation, the supernatant was aliquoted and stored at −80°C until analysis. Histamine release was measured by ELISA (IBL International GmbH, Hamburg, Germany) according to the manufacturer's instructions. The lower limit of detection of the assay is 4 ng/ml. Tryptase concentrations were assessed at the routine Laboratory of Allergy and Pulomonary Diseases, University Medical Center Groningen, Groningen, The Netherlands. Tryptase (α-protryptase and β-tryptase) was measured using a commercial fluoroenzyme immunoassay (FEIA) (Phadia AB, Uppsala, Sweden) with a lower limit of detection of 1 μg/l. This method shows high specificity and reproducibility in measuring the concentration of tryptase.16 In a pilot study we compared the release of tryptase and histamine from biopsy samples taken from the rectum and descending colon and did not find any difference.
Symptom assessment
Before entering the study, patients were asked to indicate whether their IBS symptoms were stress-related, food-related and/or whether they had any diagnosed allergies. The severity of IBS symptoms was scored before and after 8 weeks of treatment with the validated Gastrointestinal Symptom Rating Scale (GSRS) in which the intensities of the symptoms are scored on a 7-graded Likert scale with descriptive anchors (0=no symptoms at all; 1=minimal symptoms; 2=mild symptoms; 3=moderate symptoms; 4=rather serious symptoms; 5=serious symptoms and 6=very severe symptoms).17 Abdominal pain was assessed by the validated Subject's Global Assessment (SGA) of Abdominal Pain and Discomfort. In addition, weekly symptom relief was monitored by the SGA of Relief. Finally, health-related quality of life was measured by the IBS-QOL.
Data analysis
The primary end point was the effect of ketotifen on the threshold for discomfort during rectal distension in patients with IBS with hypersensitivity. Based on the 10th percentile of previously performed barostat studies in healthy volunteers, patients were considered hypersensitive to rectal distension if the thresholds for discomfort were lower than 24 mm Hg above intra-abdominal pressure.14 Secondary end points were the effect on spontaneous tryptase release, global symptom relief, abdominal pain scores and gastrointestinal symptoms. Symptom relief is expressed as the weekly percentage of patients reporting considerable to complete relief of symptoms. The cut-off level of significant symptoms obtained by the GSRS questionnaire was set at 4 (at least rather serious symptoms).
Rectal compliance was calculated as the slope of the steepest part of the pressure–volume curve during phasic distension obtained by measuring the mean intrabag volumes over the last 60 s of the first four distension steps and plotting it against the corresponding distending pressure.18
Statistics
Based on data derived from a previous study,18 we considered 6 mm Hg a relevant detectable difference in the threshold of discomfort (primary outcome measure). Given a standard deviation of 5 mm Hg, it was calculated that the sample size had to be at least 12 to detect a difference in means of 6 mm Hg using a two group t test with a two-sided significance level of 0.05 and 90% power. To compensate for potential dropouts we invited a total of 60 patients to participate in the study protocol.
Statistical analysis was performed using commercially available software (SPSS Version 12.0.1). Continuous data were compared using the Student t test for independent samples and the paired t test for related samples. Sensory thresholds, mast cell number and the concentration of mast cell mediators were not normally distributed and therefore analysed by the Mann–Whitney U test or Kruskal–Wallis test for independent samples and the Wilcoxon signed rank test for related samples. Comparison of proportions was performed using χ2 testing. Differences were considered significant at the 5% level. Multiple testing was corrected using the Holm–Bonferroni method.
Results
Study subjects
Table 1 summarises the demographic characteristics of the patients with IBS and the control group (healthy volunteers). Of the patients with IBS, 22% indicated that symptoms started following an episode of acute gastroenteritis, in 10% symptom onset was associated with stress and almost two-third of patients were unable to identify disease triggers. These different subgroups of patients were equally distributed between the two treatment arms. All but one participating patient with IBS completed the study medication and two patients (one receiving placebo and one receiving ketotifen) declined to undergo the second rectal sensitivity measurement at the end of the study.
Baseline characteristics of study subjects
Side effects
Side effects were reported equally by participants receiving ketotifen (77%) and placebo (67%, p=0.30). Fatigue (47% vs 27%, p=0.11), dry mouth (27% vs 23%, p=0.77), dizziness (20% vs 27%, 0.54), decreased awareness (0% vs 10%, p=0.08), nervousness (3% vs 3%, p=1.0) and headache (0% vs 3%, p=0.31) were not significantly different between participants receiving ketotifen and those receiving placebo. Eight participants gained weight (2–5 kg, self-reported) during the treatment period: seven of these were treated with ketotifen and one was treated with placebo (p=0.02).
Effects of ketotifen in patients with IBS
After assessment of visceral sensitivity, hypersensitive and normosensitive patients were separately randomised to receive ketotifen or placebo.
Hypersensitive patients with IBS
The minimal distending pressure was not affected by ketotifen (before 9±1 mm Hg, after 9±1 mm Hg) or placebo (before 7±1 mm Hg, after 7±1 mm Hg).
Pressure sensitivity
At baseline the thresholds were comparable between the ketotifen and placebo groups (data not shown). The thresholds for first sensation and urge to defaecate were not affected by ketotifen or placebo. In contrast, ketotifen but not placebo significantly increased the threshold of discomfort (figure 1). A similar but non-significant trend was observed when the effect of treatment on threshold for discomfort was expressed as the percentage change compared with baseline (ketotifen 41±14% vs placebo 9±11%, p=0.08).

Individual thresholds for discomfort/pain during rectal distension before and after 8 weeks of treatment with placebo or ketotifen in (A) hypersensitive patients and (B) normosensitive patients. The horizontal lines represent the mean thresholds for discomfort. *p=0.015, **p=0.024 vs before treatment.
Rectal compliance
Compared with baseline, 8 weeks of treatment with either ketotifen or placebo did not significantly alter compliance (ketotifen 10±1 to 9±1 ml/mm Hg; placebo 14±1 to 15±2 ml/mm Hg, NS).
Normosensitive patients with IBS
Pressure sensitivity
At baseline, no differences were found in baseline visceral sensitivity (data not shown). After 8 weeks of treatment, no changes in thresholds of first sensation or urge were observed. The threshold of discomfort significantly decreased during placebo whereas ketotifen had no effect (figure 1).
Rectal compliance
At baseline, rectal compliance was 12±1 ml/mm Hg and 12±1 ml/mm Hg, respectively, in the ketotifen and placebo groups. The compliance measured after 8 weeks of treatment was not affected by ketotifen (14±1 ml/mm Hg, NS) or placebo (12±1 ml/mm Hg, NS).
Mast cell counts
At baseline, both normosensitive and hypersensitive patients with IBS had a lower number of tryptase-positive mucosal mast cells in rectal and descending colon biopsies than healthy volunteers (figure 2). Compared with healthy volunteers, the number of CD117-positive rectal mucosal mast cells was lower in normosensitive (p=0.001) and hypersensitive patients but did not reach statistical significance in hypersensitive patients with IBS (p=0.06). There was no effect of treatment with either placebo or ketotifen on the number of tryptase- or CD117-positive cells (table 2). A representative picture of CD117-positive immunolabelling in patients with IBS and healthy volunteers is shown in the online supplement.
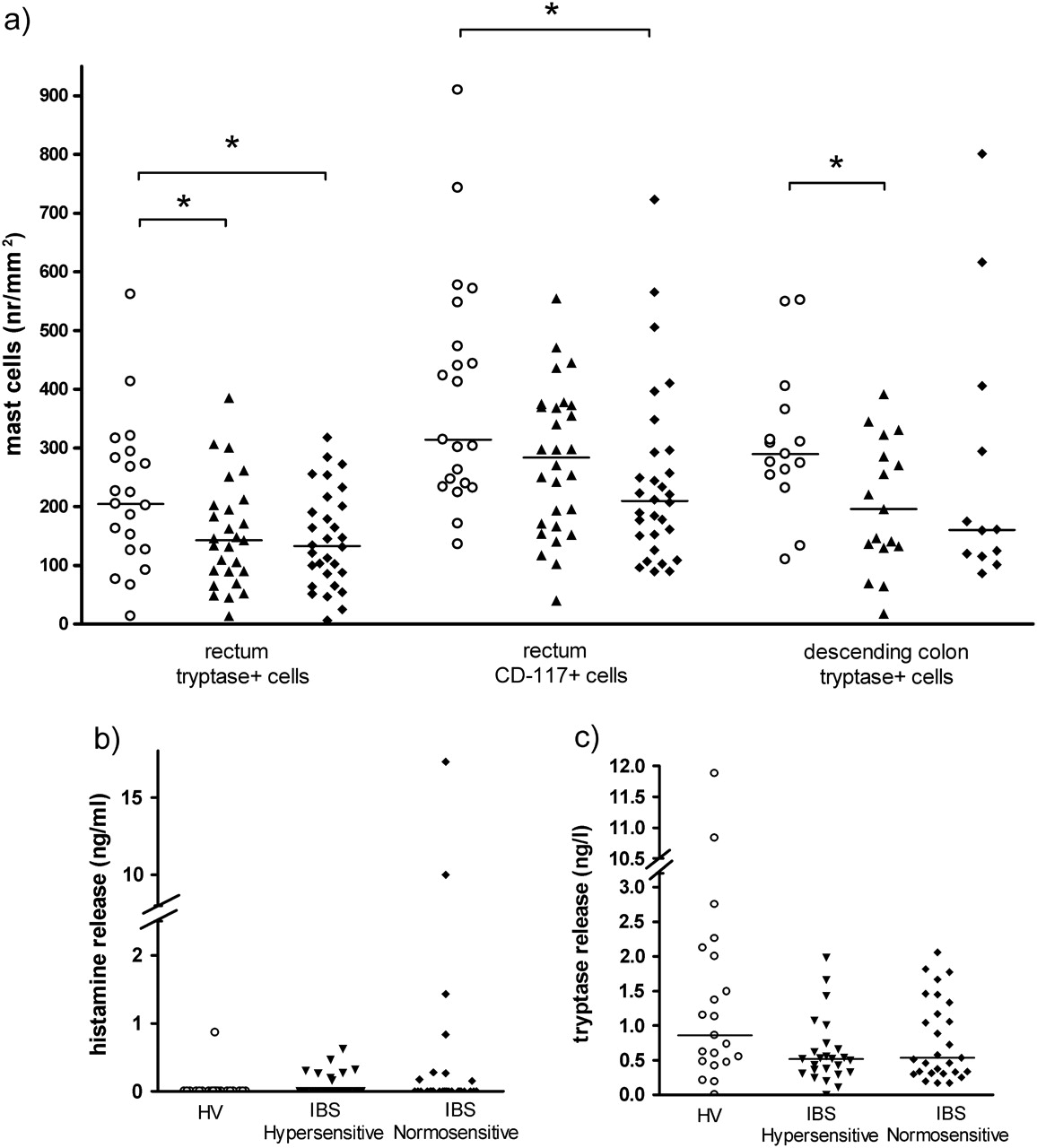
(A) Individual rectal mucosal mast cell numbers identified using tryptase and CD-117 immunostaining counted by digital image analysis (expressed as number of cells/mm2). Spontaneous release of (B) histamine and (C) tryptase measured in the supernatant of two rectal biopsies corrected for biopsy weight. Note the segmented y-axis and the two upper outliers in spontaneous tryptase release and histamine release. Circles represent healthy volunteers (HV); triangles represent patients with irritable bowel syndrome (IBS) with visceral hypersensitivity; and diamonds represent patients with IBS with visceral normosensitivity. Horizontal lines represent median values. *p<0.05.
Rectal mucosal mast cell counts (number/mm2) and spontaneous release of tryptase (μg/l) and histamine (μg/ml) in hypersensitive and normosensitive patients with irritable bowel syndrome (IBS) at baseline and after treatment with placebo or ketotifen
Histamine and tryptase release
To evaluate whether mast cell activation contributes to visceral hypersensitivity or affects therapeutic outcome, spontaneous histamine and tryptase release was measured in the supernatant of rectal biopsies before and after treatment. Kruskal–Wallis analysis revealed that histamine (p=0.10) and tryptase release (p=0.076) were not significantly different between patients with IBS with visceral hypersensitivity, patients with IBS with visceral normosensitivity and healthy volunteers. Histamine release in all patients with IBS (both visceral hypersensitive and normosensitive) was significantly increased compared with healthy volunteers (p=0.04), whereas spontaneous release of tryptase in patients with IBS was lower than in healthy volunteers (p=0.04). Treatment with placebo or ketotifen did not affect the release of histamine or tryptase (table 2). To evaluate whether spontaneous tryptase release can be blocked by mast cell stabilisers, biopsies from healthy volunteers were incubated in vitro with high concentrations of ketotifen (1 μM, n=11) and another mast cell stabiliser, doxantrazole (1 mM, n=11). However, incubation with these agents did not reduce basal tryptase release (data not shown).
Symptoms
The study is not sufficiently powered to reliably examine the differences in clinical outcome between hypersensitive and normosensitive patients with IBS. Therefore, as no significant differences were detected in clinical symptoms at baseline (data not shown) or after treatment, data from hypersensitive and normosensitive patients were pooled to evaluate the effect of ketotifen on symptoms. The data of hypersensitive and normosensitive patients with IBS are, however, separately inserted in each figure.
Global relief
After 8 weeks of treatment 20% reported at least considerable relief of symptoms when treated with ketotifen compared with 10% of those treated with placebo (NS, figure 3). The percentage of patients reporting improvement fell in both groups to a comparable level in the follow-up period.

Weekly effect of placebo (n=30) and ketotifen (n=30) on global symptom relief; percentage of patients reporting at least considerable relief of symptoms. There was no significant difference between placebo and ketotifen.
Gastrointestinal symptoms
At baseline there were no significant differences in gastrointestinal symptoms between the two groups. After 8 weeks of treatment the percentage of patients with abdominal pain (p=0.02), bloating (p=0.02), flatulence (p=0.04), diarrhoea (p=0.05) and incomplete evacuation (p=0.04) was lower with ketotifen than with placebo (figure 4). When corrected for multiple testing with Holm–Bonferroni, however, these differences were not significant.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Percentage of patients reporting severe complaints of abdominal pain at day 1 and after 8 weeks of treatment; *p<0.05. (B)Percentage of patients reporting at least rather serious complaints of irritable bowel syndrome (IBS) symptoms (score 4–6) obtained by Gastrointestinal Symptom Rating Scale questionnaire after treatment with placebo (n=28) or ketotifen (n=27). *p<0.05 ketotifen vs placebo; **p<0.05 vs baseline. When corrected for multiple testing with Holm-Bonferroni there were no significant differences between patients with IBS and healthy volunteers. Inc evac, incomplete evacuation.
Health-related quality of life
At baseline, quality of life measured by the IBS-QOL was comparable between placebo and ketotifen except for the mean score of sexual relations which was significantly higher in patients randomised to ketotifen (placebo 50±6, ketotifen 67±5, p=0.04). Compared with placebo, after 8 weeks of treatment with ketotifen patients had a higher score in all subscales with a significant difference in sleep (placebo 71±5, ketotifen 87±4, p=0.01), diet (placebo 61±4, ketotifen 83±3, p<0.001) and sexual functioning (placebo 56±6, ketotifen 87±4, p<0.01). When corrected for multiple testing, the differences in diet and sexual functioning remained statistically significant.
The effect of ketotifen on quality of life was comparable between hypersensitive and normosensitive patients.
Relationship between perception thresholds, mast cell counts, histamine release, tryptase release and clinical symptoms/response
At baseline the severity of abdominal pain was not correlated with the number of CD117-positive (p=1.0, r=0.01) or tryptase-positive (p=0.9, r=0.03) mast cells, nor was there a correlation between abdominal pain and spontaneous histamine release (p=0.9, r=0.02) or tryptase release (p=0.5, r=−0.09). We did not observe a significant relationship between abdominal pain and the threshold of discomfort (p=0.08, r=−0.2).
The number of CD117- and tryptase-positive mast cells, spontaneous release of histamine and tryptase and the threshold of discomfort at baseline did not predict the response to treatment with ketotifen. Moreover, changes in mast cell number were not correlated with treatment response to ketotifen in terms of threshold of discomfort, global relief or abdominal pain, nor were alterations in histamine or tryptase release associated with clinical outcome. In hypersensitive patients there was no correlation between changes in the threshold of discomfort and changes in abdominal pain scores after treatment with either placebo or ketotifen.
Discussion
In this study we evaluated the effect of 8 weeks of treatment with ketotifen, a mast cell stabilising agent with H1 receptor antagonistic properties, in patients with IBS. Ketotifen treatment (up to 6 mg twice daily) increased the threshold of discomfort in patients with IBS with visceral hypersensitivity, improved abdominal pain and other IBS symptoms such as bloating, flatulence, diarrhoea and incomplete evacuation, and was accompanied by an improvement in health-related quality of life. However, no effect on the release of tryptase and histamine from rectal biopsies could be demonstrated, suggesting that mechanisms other than mast cell stabilisation—most likely H1 receptor antagonism—may be involved. Based on our findings, we conclude that mast cell stabilisers and/or H1 receptor antagonists should be further explored as a potential new therapeutic approach for IBS.
To date, abundant evidence favouring an important role for mast cells in the pathophysiology of IBS has been reported. Several studies have shown that the number of mast cells and/or spontaneous release of mediators such as proteases, serotonin and histamine are increased in patients with IBS.4–7 19 Also, the number of mast cells in proximity to nerve fibres seems to correlate with the severity of abdominal pain perception in IBS.6 Although these findings strongly point towards an important role for mast cells in IBS, their role in abnormal visceral perception in man has not been properly studied. As visceral hypersensitivity is currently considered an important therapeutic target,1 we anticipated that patients with visceral hypersensitivity may react differently to treatment. In fact, this subgroup of patients may preferentially benefit from agents aiming to normalise visceral perception.14 We therefore carefully assessed visceral perception to rectal distension before randomisation to ketotifen or placebo. Our study showed that treatment with ketotifen increased the threshold for discomfort in patients with IBS with visceral hypersensitivity. In contrast, visceral perception was not affected in patients with a normal threshold for discomfort, suggesting that ketotifen has no visceral analgesic properties per se. Similar findings were previously reported with l-NMMA, an inhibitor of nitric oxide synthase, where the threshold for discomfort was only increased in patients with IBS with visceral hypersensitivity but not in healthy volunteers.20 The degree of improvement observed in our study is comparable to previous studies evaluating other drugs such as l-NMMA,20 alosetron21 and fedotozine,22 of which alosetron has proved to be clinically efficient in patients with IBS.23
Accepting that visceral hypersensitivity is an important mechanism involved in the generation of IBS symptoms, one would anticipate that normalisation or improvement of visceral perception is an important prerequisite for clinical efficacy. Although our study was not powered to evaluate clinical efficacy or differences in clinical outcome between normosensitive and hypersensitive patients with IBS, we did show improvement in IBS symptoms and health-related quality of life for the entire group after treatment with ketotifen. In contrast, no differences were seen in side effects between ketotifen and placebo except for a gain in weight. Weight gain may, however, also be explained by a positive effect of the drug on symptoms allowing patients to eat more. Severe abdominal pain significantly decreased from 31% to 7% after treatment with ketotifen. Likewise, ketotifen effectively reduced complaints of abdominal pain, diarrhoea, bloating, flatulence and incomplete evacuation, most likely all contributing to the increase in global relief. Furthermore, after withdrawal of ketotifen, abdominal complaints returned to baseline levels, further pointing to a beneficial effect of treatment with ketotifen. It should be emphasised, however, that we observed similar results in normosensitive and hypersensitive patients (figure 4) and that neither baseline nor changes in thresholds of discomfort were able to predict clinical outcome. Moreover, no correlation was demonstrated between improvement in visceral sensation and clinical outcome after treatment with ketotifen in hypersensitive patients. It therefore remains questionable to what extent improvement in the threshold for discomfort is a good predictor of clinical response, especially in view of the increasing evidence that this parameter is susceptible to habituation and subjectivity.24 Furthermore, in accordance with our findings, other studies investigating a range of different classes of therapeutic agents in patients with IBS show little predictability between symptom improvement and changes in visceral sensory thresholds (reviewed by Mayer1). Based on these considerations, the reliability of visceral hypersensitivity measured by barostat as a biomarker remains questionable, whereas the proof of concept that visceral hypersensitivity is indeed an important pathophysiological mechanism in IBS is in fact still lacking. Nevertheless, similar to our study, previous clinical studies showed clinical improvement of gastrointestinal symptoms using other mast cell stabilisers. In an unblinded uncontrolled study, treatment with disodium cromoglycate for 1 month was evaluated in 428 patients with diarrhoea-predominant IBS. Mast cell stabilisation resulted in a reduction in IBS symptoms and was equally effective as an elimination diet.25 Another study in patients with persistent diarrhoea of unknown aetiology showed that disodium cromoglycate reduced stool frequency.26 Moreover, disodium cromoglycate improved abdominal pain, distension and diarrhoea in patients with food intolerance.27 Taken together, although these studies were partly uncontrolled and unblinded, these data support the concept that mast cells could be an interesting target for treatment in patients with IBS.
To further explore the role of mast cells in IBS (and visceral hypersensitivity in particular), we evaluated mast cell numbers and mast cell mediator release from mucosal biopsies. No differences in the mast cell markers tryptase or CD117 were observed between normosensitive and hypersensitive patients with IBS. The number of mast cells was even lower in patients with IBS than in age-matched controls. The latter data are in contrast with the study by Barbara et al which showed increased mast cell numbers in colonic biopsies from patients with IBS.6 A possible explanation for this discrepancy could be differences in patient population or the anatomical region studied. However, Cenac and colleagues8 observed no differences in mast cell numbers between rectal and colonic biopsies and, comparable to our data, did not find an increased number of mast cells. We were also unable to detect increased release of tryptase in the supernatant of rectal biopsies. It should be stressed that we determined the total tryptase concentration (α-protryptase and β-tryptase) using a commercial fluoroenzyme immunoassay specific for human tryptase,28 whereas others have measured tryptase levels indirectly by assessing proteolytic activity.6 8 This technique is, however, not specific for mast cell activation as proteases from, for example, commensal bacteria and the intestinal epithelium may all contribute to the increased proteolytic activity observed in the supernatant. In contrast to tryptase, we observed that, on average, histamine release was slightly increased in patients with IBS but could only be detected in 16 of the 54 samples. Our findings are similar to those recently published by Buhner et al.19 As for protease activity, histamine can also be produced by commensal bacteria,29 indicating that sources other than mast cells should be considered. As mast cell numbers are not increased and there is no evidence for increased release of mast cell mediators, our data fail to confirm mast cell activation in IBS.
How then can the effect of ketotifen on visceral perception and IBS symptoms be explained? First, although ketotifen has well-established mast cell stabilising properties,30 it is also recognised as a relatively selective non-competitive H1 receptor antagonist.31 H1 receptors are expressed by several cell types such as smooth muscle cells, neurons and immune cells including mast cells.32 33 In the gastrointestinal tract, H1 receptors are expressed in the muscularis, mucosa and submucosa and, interestingly, are more expressed in the colonic mucosa of patients with IBS.34 Furthermore, excitation of rat sensory neurons by colonic supernatant derived from patients with IBS was inhibited by H1 receptor blockade.9 In addition to peripheral H1 receptors, H1 receptors are also widely expressed in the brain, mediating nociception, arousal, locomotor activity and appetite control,35 36 which may have contributed to the improvement in quality of life in the subscales of sleep, diet and energy. Future studies evaluating the effect of H1 receptor antagonism in patients with IBS are therefore warranted.
Second, the number of mast cells present in the mucosa and/or the mediators detected in the supernatant may be unreliable biomarkers for mast cell activation. Spontaneous release of mast cell mediators may indeed be the wrong biomarker to evaluate the role of mast cells in IBS. For example, although stress-induced visceral hypersensitivity in rats is mediated by mast cells,10 no differences in spontaneous mast cell release were observed between hypersensitive (stressed) and normosensitive animals. Only when activated by IgE crosslinking did mast cells derived from stressed animals release more histamine than those from non-stressed controls.37 Several attempts to trigger mast cell activation in rectal and colonic biopsies using corticotrophin-releasing hormone, substance P or ionomycin have, however, failed (data not shown). Moreover, a recent study in patients with inflammatory bowel disorders showed that, whereas the number was not affected, colonic mast cells expressed an altered receptor profile and a different response to activation.38 Hence, despite a reduction in total number, theoretically the mast cell stabiliser ketotifen still may alter visceral hypersensitivity by inhibiting the activated release of mast cell mediators. Finally, in order to be considered as a biomarker for IBS or visceral hypersensitivity, symptoms, barostat findings or treatment outcome should be correlated or associated with changes in the release of the mediator under study. Neither tryptase nor histamine release correlated with barostat findings or predicted clinical outcome. We therefore seriously question whether the amount of mediators released in the supernatant is a good indicator of mast cell activation.
In conclusion, our study demonstrates that ketotifen reduced visceral hypersensitivity and IBS symptoms and improved quality of life. The number of mast cells in colonic mucosal biopsies and the release of tryptase were, however, not increased and the release of mediators in the supernatant from rectal biopsies was not reduced by ketotifen treatment. Other mechanisms of action such as H1 receptor blockade may therefore explain the beneficial effect of ketotifen treatment, indicating that mast cell stabilisation and also H1 receptor blockade should be further explored as potential new treatments for IBS.
References
Footnotes
Funding TKK is supported by a grant from the Netherlands Digestive Diseases Foundation (MLDS) grant number MWO 05-42 and by a grant from Johnson and Johnson. GEB is funded by the European Seventh Framework Programme Theme (Health-2007-2.4.5-2, IPODD) and by a grant from the Flemish Government (Odysseus program, Fonds Wetenschappelijk Onderzoek (FWO), grant G.0905.08). The funders had no influence on the study design or on the collection, analysis, interpretation of data; on the writing of the report; or on the decision to submit the paper for publication.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Medical Ethics Committee of the Academic Medical Center Amsterdam.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Digest