Article Text

Abstract
Background and aims: Mutations in BRAF have been linked with colorectal cancers (CRC) showing high level microsatellite instability (MSI-H). However, the distribution of BRAF mutations in MSI-H cancers remains to be clarified with respect to precursor lesions and the CpG island methylator phenotype (CIMP).
Methods: Forty three hyperplastic polyps (HP), nine mixed polyps (MP), five serrated adenomas (SA), 28 conventional adenomas (AD), 18 hereditary non-polyposis colorectal cancers (HNPCC), and 127 sporadic CRC (46 MSI-H and 81 non-MSI-H) were collected from patients undergoing colectomy for either CRC or hyperplastic polyposis. Twenty five of 57 serrated lesions were derived from four patients with hyperplastic polyposis. HP were further subdivided according to recently documented morphological criteria into 27 classical HP and 16 variant lesions described as “sessile serrated adenoma” (SSA). All tumours were screened for BRAF activating mutations.
Results: The BRAF mutation was more frequent in SSA (75%) and MP (89%) than in classical HP (19%), SA (20%), and AD (0%) (p<0.0001), and also in sporadic MSI-H cancers (76%) compared with HNPCC (0%) and sporadic non-MSI-H cancers (9%) (p<0.0001). The BRAF mutation was identified more often in CIMP-high serrated polyps (72%) and CIMP-high CRC (77%) than in CIMP-low (30%) and CIMP-negative (13%) polyps (p = 0.002) as well as CIMP-low (18%) and CIMP-negative (0%) CRC (p<0.0001).
Conclusions: The BRAF mutation was frequently seen in SSA and in sporadic MSI-H CRC, both of which were associated with DNA methylation. Sporadic MSI-H cancers may originate in SSA and not adenomas, and BRAF mutation and DNA methylation are early events in this “serrated” pathway.
- AD, conventional adenoma (tubular adenoma and tubulovillous adenoma)
- CIMP, CpG island methylator phenotype
- CRC, colorectal cancer
- dHPLC, denaturing high performance liquid chromatography
- FAP, familial adenomatous polyposis
- HNPCC, hereditary non-polyposis colorectal cancer
- HP, hyperplastic polyp
- MMR, mismatch repair
- MP, mixed polyp
- MSI, microsatellite instability
- MSI-H, high level MSI
- RFLP, restriction fragment length polymorphism
- SA, serrated adenoma
- SSA, sessile serrated adenoma
- BRAF
- colorectal cancer
- serrated pathway
- CpG island methylator phenotype
- microsatellite instability
Statistics from Altmetric.com
- AD, conventional adenoma (tubular adenoma and tubulovillous adenoma)
- CIMP, CpG island methylator phenotype
- CRC, colorectal cancer
- dHPLC, denaturing high performance liquid chromatography
- FAP, familial adenomatous polyposis
- HNPCC, hereditary non-polyposis colorectal cancer
- HP, hyperplastic polyp
- MMR, mismatch repair
- MP, mixed polyp
- MSI, microsatellite instability
- MSI-H, high level MSI
- RFLP, restriction fragment length polymorphism
- SA, serrated adenoma
- SSA, sessile serrated adenoma
Colorectal cancer (CRC) is one of the leading causes of cancer mortality in the Western world and is considered to be a heterogeneous disease.1–3 Approximately 5% of cases are attributable to familial cancer syndromes (hereditary non-polyposis colorectal cancers (HNPCC) and familial adenomatous polyposis (FAP)) while the remainder arises sporadically.1,2 HNPCC is due to a germline mutation of DNA mismatch repair (MMR) genes, and cancers occurring in this condition show high level DNA microsatellite instability (MSI-H). Approximately 15% of sporadic CRC are also characterised by high level MSI due to somatic inactivation of a MMR gene.2 While the evolution of the majority of non-MSI-H cancers is consistent with the accepted adenoma-carcinoma model,4 initiation and pathogenic progression of sporadic MSI-H cancers remains controversial.3,5,6
For many years, hyperplastic polyps (HP) have been regarded as colorectal lesions with little neoplastic potential and therefore of no pathogenic consequence.7 However, this view has recently been challenged by the proposal that a subset of HP predisposes to sporadic MSI-H cancers and may progress through a “serrated neoplastic pathway”.3,8 Lesions with serrated architecture (serrated polyps) include classical HP and the much rarer mixed polyps (MP), and serrated adenomas (SA).7,9 SA are composed of adenomatous (dysplastic) epithelium that nevertheless show the architectural serration that is characteristic of HP while MP are combined lesions that include separate hyperplastic and adenomatous components.10 Based on multiple microscopic features, classical or harmless HP have recently been distinguished from large, often right sided, HP which are more likely to have malignant potential.9,11–13
An important molecular feature frequently associated with, but not exclusive to, sporadic MSI-H cancers is the CpG island methylator phenotype (CIMP) which is characterised by methylation of multiple CpG islands located within the promoter region of genes.14–18 CpG islands are seen in approximately 50% of human genes and consist of dense regions of cytosine-guanosine dinucleotides that are susceptible to methylation of the cytosine residues resulting in gene silencing. Within the context of CRC, hypermethylation of CpG islands provides an epigenetic mechanism for the transcriptional repression of genes which are known to be important in neoplastic development, such as p16, MGMT, and the MMR gene hMLH1.14,19–21 It has been postulated that aberrant methylation in association with other genetic alterations is the mechanism by which the “serrated neoplastic pathway” to CRC is initiated.3,22
BRAF, a member of the RAF family of serine/threonine kinases, mediates cellular responses to growth signals through the RAS-RAF-MAP kinase pathway.23,24 Activating mutations in BRAF have recently been identified in 70% of malignant melanomas and 5–15% of CRCs.25–27 In all of the human cancers surveyed, the most common mutation identified was a V599E amino acid substitution that mimics phosphorylation at T598 and S601 and results in constitutive kinase activation.25,28 Furthermore, it has been demonstrated that the BRAF mutation is strongly associated with MMR deficient CRC and inversely correlated with mutation of the K-ras oncogene.25–27 Based on this evidence it was postulated that BRAF and K-ras mutations are equivalent in their tumorigenic effects and that both MMR deficient and proficient tumour types progress through the same biochemical pathways.26
In this study, we evaluated the frequency of the BRAF mutation in 85 colorectal polyps, and in 145 CRC stratified by MSI and/or CIMP status. Our findings showed that the oncogenic BRAF mutation had a striking association with both CIMP-high sporadic MSI-H cancers and a subset of HP showing CIMP-high, thereby providing strong evidence that sporadic MSI-H cancers evolve from these lesions and not from adenomas. These results suggest that the BRAF mutation and DNA methylation are key genetic events in initiation of the serrated neoplastic pathway in the development of CRC.
MATERIALS AND METHODS
Tissue samples
The study was performed on fresh frozen tissue samples obtained from patients undergoing colectomy for neoplasia at the Royal Brisbane Hospital. Patients provided written informed consent and the study was approved by the Human Research Ethics Committee of the Queensland Institute of Medical Research. All samples were dissected macroscopically by a pathologist to ensure that they contained predominantly neoplastic tissue. The study group consisted of 85 colorectal polyps and 145 cancers, both with matching normal mucosa. Age at operation and sex of the patient were noted. Cases were selected for study from a large consecutive series of operative specimens on the basis of MSI status or evidence of HNPCC (cancers) and overall histological appearance (polyps).
The colorectal cancer group was enriched for MSI-H cancers as BRAF activating mutations had been specifically associated with this tumour type,26 and included 64 MSI-H cancers (46 sporadic and 18 HNPCC). Sporadic MSI-H cancers comprised cancers derived from patients over 56 years of age with no family history of CRC. HNPCC tumours had been characterised in a prior study.29 MSI status for each tumour was determined by examining a panel of 10 microsatellite markers (BAT-26, BAT-25, BAT-40, BAT-34C4, MYCL, D10S197, D18S55, D5S346, D17S250, and ACTC) using previously described techniques.30–33 Cancers with instability in at least four (40%) of the markers were classified as MSI-H with the remainder classified as non-MSI-H.31 For all MSI-H cancers, immunohistochemical staining of hMLH1 and hMSH2 was performed and all sporadic MSI-H cancers showed loss of hMLH1 protein expression.29 Information regarding mucinous histology, histological grade, clinicopathological staging, and tumour infiltrating lymphocytes was available on a subset of cancers which had been examined for these features in previous reports.16,29,30
Fresh frozen polyp samples were selected to enrich the cohort for “serrated pathway” lesions as a recent report had shown that BRAF activating mutations were highly associated with these polyp types.34 Half of each bisected polyp was placed in liquid nitrogen after resection for subsequent DNA analysis while the remaining half was submitted for histological diagnosis. Eighty five polyps were classified: 43 HP, nine MP, five SA and 28 AD (tubular or tubulovillous adenoma) using WHO criteria.10,35 Of the 57 serrated polyps, 25 (15 HP, eight MP, and two SA) were derived from four patients with hyperplastic polyposis36 and the remaining 32 were obtained from 14 patients undergoing surgery for CRC.37 Twenty eight AD were derived from 11 patients undergoing surgery for CRC.
Histological evaluation
Sections (4 μm) were cut from formalin fixed paraffin embedded blocks and stained with haematoxylin and eosin. Polyp cases were reviewed by two independent observers (JRJ and TH). The purpose of this review was to identify HP showing atypical histological features that have been associated with the recently documented HP variant described as “sessile serrated adenoma” (SSA).11–13 Features that were assessed included: (1) exaggerated serration, papillarity, or villosity, including serration in the lower crypt; (2) crypt irregularity, including pronounced budding, branching, or horizontally arranged crypts; (3) crypt dilatation; (4) increased crypt epithelium to stroma ratio; (5) mitoses in the upper half of crypts; (6) vesicular nuclei with prominent nucleoli in the upper half of crypts; and (7) increased production of intracellular and/or luminal mucin.11–13 HP were defined as “atypical” if four or more of these features were present. Rare discrepant findings between the two observers were resolved by consensus. HP were also partitioned for size into: (a) lesions 5 mm or less in size and (b) those greater than 5 mm. The site of the polyps in the colon was also noted.
Mutation analysis
Genomic DNA was extracted using standard methods and amplified using previously described polymerase chain reaction primers.25,38 Samples were screened for mutations in BRAF (exon 15) and K-ras (codons 12 and 13) by restriction fragment length polymorphism (RFLP)32,38–40 and in BRAF (exons 11 and 15) by denaturing high performance liquid chromatography (dHPLC).25,41 All products showing positive results from RFLP or dHPLC analysis were purified and sequenced manually using AmpliCycle Sequencing Kit (Applied Biosystems, Branchburg, New Jersey, USA) or automatically using Big Dye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems, Foster City, California, USA) and analysed on a ABI 3100 Genetic Analyzer.
Methylation analysis
Bisulfite modification of genomic DNA was performed as previously described.16,17 The COBRA method was used to examine the methylation status of the four CpG islands (MINT1, MINT2, MINT12, and MINT31) used to determine CIMP status.16,17,37 Cancers and serrated polyps were classified as CIMP-high (3–4 markers methylated), CIMP-low (1–2 markers methylated), and CIMP-negative (no marker methylated).16,37hMLH1 promoter methylation data were obtained from previous studies.16,29,37
Statistical analysis
Differences in frequency were assessed by Pearson’s χ2 test, Fisher’s exact test (extended), or the Student’s t test, and all p values were two sided. Multiple regression analysis was carried out using the STATISTICA 6 software package (Statsoft Corporation). A p value of <0.05 was considered significant.
RESULTS
Mutually exclusive relationship between BRAF and K-ras mutations in colorectal polyps and cancers
We performed BRAF and K-ras mutation analysis on 85 colorectal polyps comprising 43 HP, nine MP, five SA, and 28 AD, and on 145 CRC, comprising 64 MSI-H cancers (18 HNPCC and 46 sporadic) and 81 non-MSI-H cancers. In total, 26 polyps and 42 cancers containing BRAF mutations were identified in 230 samples studied (tables 1, 2). All BRAF mutations showed the same thymine to adenine transversion at nucleotide 1796, resulting in a valine to glutamine substitution at codon 599 (V599E) (fig 1). K-ras mutations were also found in 20 polyps and 43 cancers (tables 1, 2). In our study, neither polyps nor cancers simultaneously harboured both BRAF and K-ras mutations.
BRAF and K-ras mutations in colorectal cancers
BRAF and K-ras mutations in colorectal polyps
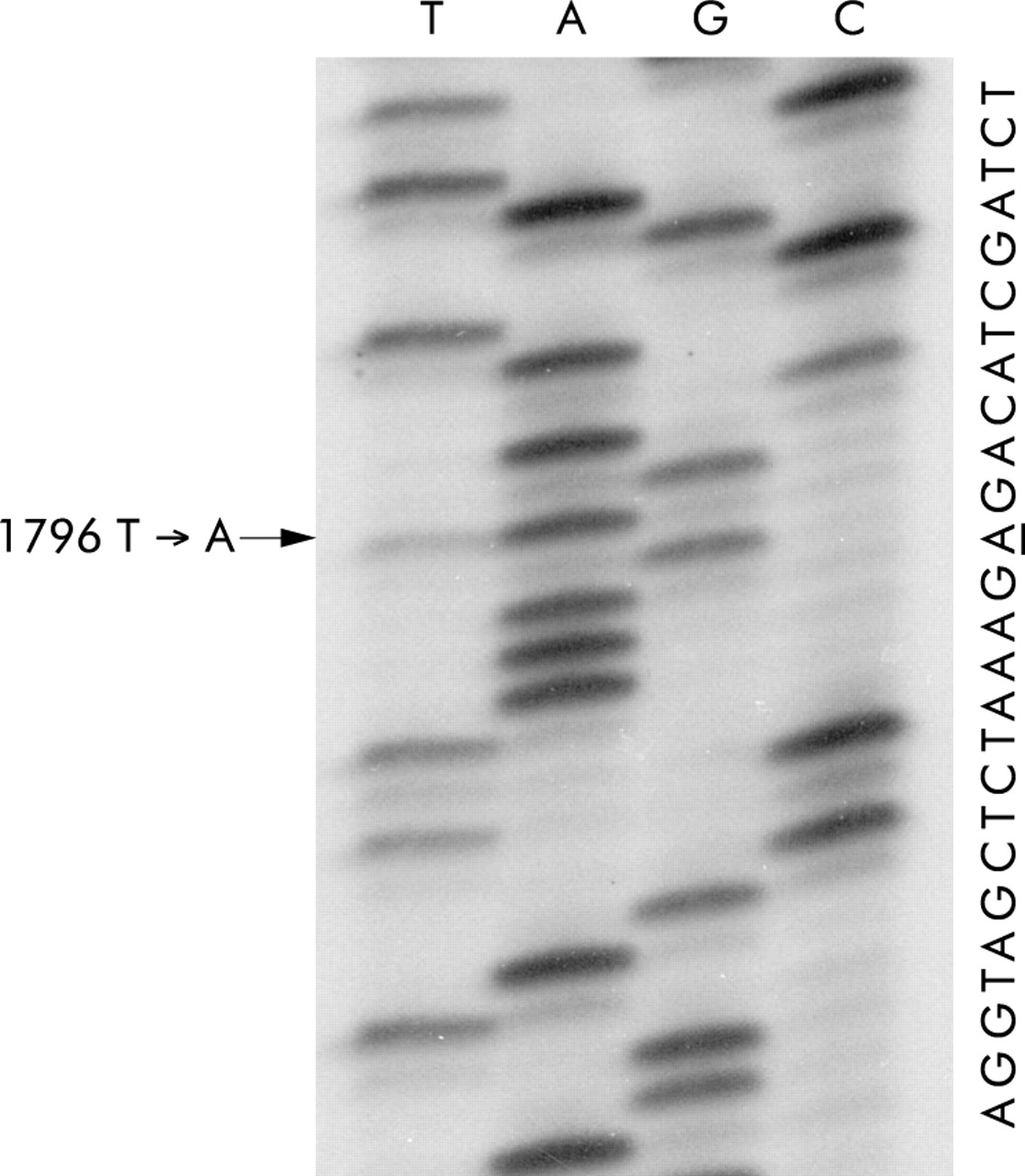
Representative sequence showing the BRAF V599E (T1796A) mutation.
Relationship between BRAF and K-ras mutation and MSI-status in CRC
The oncogenic V599E mutation was identified 35 of 46 (76%) sporadic MSI-H, seven of 81 (9%) non-MSI-H, and in 0 of 18 (0%) familial (HNPCC) cancers (table 1). These observations demonstrated a highly significant association between BRAF mutation and sporadic MSI-H cancers compared with non-MSI-H and HNPCC cancers (p<0.0001 and p<0.0001, respectively). Conversely, K-ras mutation was detected in six of 18 (33%) CRC in HNPCC, 36 of 81 (44%) sporadic non-MSI-H cancers, and in only one of 46 (2%) sporadic MSI-H cancer (table 1). In addition, CRCs with the BRAF mutation were associated with typical features of sporadic MSI-H CRC; older age (p<0.0001), female sex (p = 0.006), right sided anatomical location (p<0.0001), high tumour grade (p<0.0001), and mucinous histology (p<0.0001), compared with CRC without BRAF mutations (table 3). The clinicopathological stage of the cancer and the presence of tumour infiltrating lymphocytes showed no significant relationships with BRAF mutation.
Patient demographics and characteristics of colorectal cancers evaluated for BRAF mutations
Association between BRAF mutation and histopathology of polyps
The BRAF V599E mutation was identified in 17 of 43 (40%) HP, eight of nine (89%) MP, one of five (20%) SA, and 0 of 28 (0%) AD (p<0.0001) (table 2). Among the 43 HP, 16 showed atypical features found in SSA, as described by Torlakovic et al and Goldstein et al (fig 2).11,13 The V599E mutation was identified in 12 of 16 (75%) HP with atypical features (SSA) and in all of eight MP showing atypical features within the hyperplastic component. Therefore, the BRAF mutation segregated with a total of 20 of 24 (83%) HP and MP having the atypical features used to define the HP variant termed SSA.11,13 In contrast, the BRAF mutation occurred in only five of 28 (18%) polyps (27 HP and the single MP) lacking these atypical features (p<0.0001). When size of lesions with serrated architecture was considered in 55 serrated polyps (43 HP, nine MP, and three SA), the BRAF mutation was more frequently seen in polyps larger than 5 mm (p<0.02). In addition, 12 of 15 (80%) large polyps (6 mm or more) had the atypical features, contrasting with 12 of 37 (32%) small polyps (5 mm or less) (p<0.01). When location in the colon was analysed, the BRAF mutation was more highly represented in right sided serrated polyps (HP, MP, and SA) than left sided polyps (p<0.01). The origin of serrated polyps was also considered. In hyperplastic polyposis patients, 22 of 25 (88%) polyps (two of two classical HP, 11 of 13 variant HP, eight of eight MP with atypical architecture, and one of two SA) harboured the BRAF mutation, while four of 32 (13%) sporadic polyps (three of 25 classical HP, one of three variant HP, 0 of one MP without serrated architecture, and 0 of three SA) had the BRAF mutation (p<0.0001). However, multiple regression analysis carried out on the four characteristics strongly associated with BRAF mutation (atypical histology, size, location, and origin of polyps) revealed origin within hyperplastic polyposis to be the only independent predictor of BRAF mutation (p<0.001).

Haematoxylin and eosin stains of two hyperplastic polyps (HP) showing the atypical features described as sessile serrated adenoma (SSA) by Torlakovic et al and Goldstein et al.11,13 (A) Low power view of a variant HP in which there is a hypermucinous epithelium showing crypt dilatation and horizontal extension of crypts immediately above the muscularis mucosae. (B) Medium power magnification of a variant HP showing exaggerated serration, crypt dilatation, and crypt branching, but no definite evidence of dysplasia.
Relationship between BRAF mutation and DNA methylation in serrated polyps and CRC
To determine if there was any relationship between BRAF mutation and DNA methylation, we investigated the frequency of the BRAF (V599E) mutation in CIMP-high, CIMP-low, and CIMP-negative sporadic CRC and serrated polyps. A highly significant association was found with BRAF mutations identified in 20 of 26 CIMP-high cancers (77%), while eight of 44 CIMP-low (18%) and 0 of 34 CIMP-negative cancers (0%) carried this mutation (p<0.0001) (table 1). Notably, when sporadic MSI-H cancers were further stratified by CIMP status, we found an even greater association. In sporadic MSI-H cases, 16 of 17 (94%) CIMP-high cancers harboured the V599E mutation while five of nine (56%) CIMP-low and 0 of two (0%) CIMP-negative cancers had the V599 mutation (p = 0.004) (fig 3). For sporadic non-MSI-H cases, four of nine (44%) CIMP-high cancers had the V599E mutation in contrast with three of 35 (9%) CIMP-low and 0 of 32 CIMP-negative cancers (p = 0.0008). When hMLH1 promoter methylation was considered, it was seen in 16 of 24 cancers (66%) with the BRAF mutation and in only four of 74 (5%) without (p<0.0001). Of the four tumours with hMLH1 promoter methylation but no BRAF mutation, two cases were HNPCC patient and the remaining two cases were sporadic non-CIMP-high cancers that were MSI-H. None of 18 serrated lesions tested showed hMLH1 promoter methylation.

{kind=link}
{kind=link}
{kind=link}
Histogram showing the frequency of the BRAF (V599E) mutation in hereditary non-polyposis colorectal cancer (HNPCC), sporadic high level microsatellite instability (MSI-H) cancer, and non-MSI-H cancers stratified according to CpG island methylator phenotype (CIMP) status. The percentage of BRAF mutation in each group of cancers is indicated and the frequency of the mutation is represented in black. Indicated are p values comparing CIMP-high, CIMP-low, and CIMP-negative cancers within sporadic MSI-H and non-MSI-H cases.
Although 22 of 25 serrated polyps obtained from subjects with hyperplastic polyposis showed BRAF mutations, there was an overall significant association between BRAF mutation and DNA methylation across the 56 serrated polyps tested in the study, with 18 of 25 CIMP-high (72%), seven of 23 CIMP-low (30%), and one of eight CIMP-negative (13%) polyps (p = 0.002) (table 2). Of note, four HP with the BRAF mutation were observed outside the setting of hyperplastic polyposis, as defined by Burt and Jass,36 and one of these HP showed both atypical histology and CIMP-high.
DISCUSSION
In this study we showed that activating BRAF mutations were strongly associated with sporadic MSI-H cancers where somatic inactivation of hMLH1 occurs but were not found in MSI-H cancers arising in the inherited syndrome HNPCC. Several previous studies have examined the relationship between MSI status and BRAF mutation. Yuen et al found no significant association between MSI status and BRAF mutation27 but only a limited number of MSI-H cancers were examined. In the study of Rajagopalan et al, an association between MMR and BRAF mutation was reported26 but sporadic and inherited (HNPCC) cancers were not considered separately. Our results show clearly that inherited MSI-H cancers, which also have MMR deficiency, do not harbour BRAF mutations. Rather, BRAF mutation appears to be associated with sporadic CRC, in particular those with methylation of multiple CpG islands, including in some cases the promoter of hMLH1. This finding is in agreement with current reports.42–44 When CIMP status was determined using five markers (four MINTs and p16), this trend did not change (data not shown). The BRAF mutation was also associated with the characteristics of sporadic MSI-H cancers such as female sex, mucinous histology, and advanced age at diagnosis but not with tumour infiltrating lymphocytes, a feature shared with cancers arising in HNPCC.29,30 In contrast, hMLH1 methylation was rare in tumours without BRAF mutations (four cases). In each of these cases, methylation of multiple promoters was not a concomitant feature.
The BRAF mutation was also commonly seen in CIMP-high non-MSI-H cancers (44%) although at a lower frequency than in CIMP-high MSI-H cancers (94%). As four of nine (44%) of CIMP-high non-MSI-high cancers also harboured the K-ras mutation, nearly 90% of all CIMP-high cancers had either BRAF or K-ras mutations. These observations were confirmed by our findings in serrated polyps in which hMLH1 methylation had not occurred.37 Methylation of hMLH1 is a late event that leads to dysplasia within polyps. Our data indicate that the BRAF mutation is very closely linked with DNA methylation and not specifically with hMLH1 methylation. These results suggest that a shared environmental factor or selection pressure lead to both DNA methylation and BRAF mutation. For example, sporadic MSI-H cancers are associated with cigarette smoking and occur predominantly in the environment of the proximal colon.45 The BRAF (V599E) mutation is frequent in tumour types prone to RAS mutation and our results agree with the concept that these are alternative ways of activating the RAS/RAF/MAP-kinase pathway.25–27 In agreement with others, we found a reciprocal association between this BRAF mutation and the K-ras mutation.26,27
The second major implication of our study is that sporadic MSI-H cancers develop from a subtype of HP and not from conventional adenomas. We found no BRAF mutation in 28 adenomas investigated. This is unlikely to be due to technical considerations such as dilution of the sample with normal DNA as all samples in this study were macroscopically dissected. Furthermore, the denaturing HPLC technique used to screen for BRAF mutations is highly sensitive across a broad range of genes.41,46–48 In addition, others have reported the BRAF mutation at a very low frequency in adenomas.26,27 Our data are similar to those of Chan and colleagues34 in that we associated BRAF mutation with colorectal polyps with epithelial serration. However, we further demonstrated that BRAF mutations were associated with the variant HP described as SSA within the setting of hyperplastic polyposis.11,13 In extraintestinal tumours, BRAF mutations also appear to occur early in tumorigenesis, for example in naevi,49 and in specific subgroups, for example serous borderline tumours which are precursors of low grade ovarian serous carcinomas.40 Activated BRAF signals through RAS/RAF/MEK/ERK/MAP-kinase to promote proliferation but it is also known to have an antiapoptotic role. BRAF knockout mice die in utero due to increased apoptosis of differentiated endothelial cells24 and BRAF overexpression leads to protection against apoptosis by inactivating caspases after cytochrome C release.28 One hypothesis to explain the role of BRAF in colorectal tumorigenesis would be that apoptosis evasion due to BRAF activation leads to accumulation of differentiated colonocytes that characterises atypical HP and that later, when cells acquire other mutations, the effect of activated BRAF is to drive proliferation.
The very high frequency (94%) of BRAF mutations in both CRC with MSI and/or extensive DNA methylation, and in colorectal polyps with serrated morphology showing extensive DNA methylation and atypical features, strongly supports earlier work linking the development of sporadic MSI-H CRC through an alternative “serrated” pathway and suggest that BRAF mutation and DNA methylation occur as early events in this pathway.5,8,22,29,50 The subset of HP with atypical histological features and described as SSA are likely to be the principal precursors of MSI-H CRC.11–13 These polyps have been found with increased frequency in the colon of patients who have sporadic MSI-H CRC and also in subjects with hyperplastic polyposis.5,11,13 Such polyps frequently show CIMP.6,37 Cancers developing in patients with the condition hyperplastic polyposis in which there are large numbers of variant HP are more likely to be MSI-H.51 Methylation is related to tissue aging.18 Given the biological link between tissue aging and apoptosis and the suggestion that HP are caused by inhibition of apoptosis,3 it is conceivable that age related methylation becomes exaggerated within these polyps and serves as the basis for CIMP.
Although most of our variant HP with BRAF mutations were obtained from subjects diagnosed with hyperplastic polyposis, HP with BRAF mutations, including a variant HP or SSA with both BRAF mutation and CIMP-high, were found outside the context of hyperplastic polyposis in this study, suggesting that such lesions may also arise sporadically. We would stress also that 22 of 32 of the HP occurring outside the context of hyperplastic polyposis in this study were from the distal colorectum and therefore one might not expect to find within the sporadic subset many variant HP with BRAF mutations. In fact, the BRAF mutation was found in only one of 10 sporadic HP obtained from the proximal colon. This may indicate that only a fraction of proximal HP serve as precursors of CRC with BRAF mutations. In contrast, there is little evidence implicating conventional adenomas in the evolution of sporadic MSI-H CRC,3 although adenomas are the precursors to cancer in HNPCC.52 The absence of BRAF mutations in inherited MSI-H CRC, as well as in adenomas, is consistent with the suggestion that BRAF mutations do not occur as a consequence of MMR deficiency.43,44
In this study we have shown that the BRAF mutation segregates with a variant HP described by others as sessile serrated adenoma (SSA),11,13 at least within the setting of hyperplastic polyposis. We have also shown, in agreement with others,43,44 that the BRAF mutation segregates with sporadic MSI-H CRC showing DNA methylation. Such tumours are relatively frequent in subjects with hyperplastic polyposis, and in this syndrome we have a model for the progression of the serrated precursor lesion to CRC which is analogous to the adenoma-carcinoma model in the inherited syndrome FAP.4,53 Although most of our variant HP with BRAF mutation were obtained from subjects diagnosed with hyperplastic polyposis, there were also some instances of BRAF mutations in sporadic HP. Therefore, our data not only provide confirmation of the hypothesis that MSI-H CRC which arises in hyperplastic polyposis develops from variant serrated polyps,3 but also suggest that sporadic MSI-H cancers may arise from these lesions. In summary, our conclusions are based on the finding that MSI-H CRC has been linked with both hyperplastic polyposis and sporadic hyperplastic polyps,3 the fact that sessile serrated adenomas occur frequently not only in hyperplastic polyposis12 but also sporadically in the proximal colon,11,13 and finally the fact that there are no data indicating biological differences between SSA that occur sporadically or in the context of hyperplastic polyposis.
The present study has several clinical implications. It provides a novel mechanistic basis to the clinical observation that large proximal hyperplastic-like polyps have malignant potential and may require removal when discovered during colonoscopy. Furthermore, the BRAF mutation may be employed to distinguish HNPCC from sporadic MSI-H cancers. Because it is relatively simple to detect a known single base substitution, BRAF mutations could be developed as a faecal marker of CRC. In the future, BRAF may be an attractive target for therapeutic drugs, especially as conventional adjuvant chemotherapy has recently been shown to be ineffective in the treatment of sporadic MSI-H cancer.54
Acknowledgments
We would like to thank Ron Buttenshaw for expert technical assistance. This work was supported in part by the Royal Brisbane and Women’s Hospital Research Foundation, the Australian National Health and Medical Research Council, the US National Institutes of Health (UO1-CA74778), and the Walter Paulson Memorial Tumor Bank. The Queensland Institute of Medical Research has approved the use of previously collected stored tissue samples, which remain anonymous to protect individuals’ confidentiality.
REFERENCES
Footnotes
-
↵* T Kambara and L A Simms contributed equally to this work.