Article Text

Abstract
Objective To present results of the Kyoto Global Consensus Meeting, which was convened to develop global consensus on (1) classification of chronic gastritis and duodenitis, (2) clinical distinction of dyspepsia caused by Helicobacter pylori from functional dyspepsia, (3) appropriate diagnostic assessment of gastritis and (4) when, whom and how to treat H. pylori gastritis.
Design Twenty-three clinical questions addressing the above-mentioned four domains were drafted for which expert panels were asked to formulate relevant statements. A Delphi method using an anonymous electronic system was adopted to develop the consensus, the level of which was predefined as ≥80%. Final modifications of clinical questions and consensus were achieved at the face-to-face meeting in Kyoto.
Results All 24 statements for 22 clinical questions after extensive modifications and omission of one clinical question were achieved with a consensus level of >80%. To better organise classification of gastritis and duodenitis based on aetiology, a new classification of gastritis and duodenitis is recommended for the 11th international classification. A new category of H. pylori-associated dyspepsia together with a diagnostic algorithm was proposed. The adoption of grading systems for gastric cancer risk stratification, and modern image-enhancing endoscopy for the diagnosis of gastritis, were recommended. Treatment to eradicate H. pylori infection before preneoplastic changes develop, if feasible, was recommended to minimise the risk of more serious complications of the infection.
Conclusions A global consensus for gastritis was developed for the first time, which will be the basis for an international classification system and for further research on the subject.
- GASTRIC CANCER
- FUNCTIONAL DYSPEPSIA
- HELICOBACTER PYLORI - GASTRITIS
- HELICOBACTER PYLORI - TREATMENT
- GASTRITIS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- GASTRIC CANCER
- FUNCTIONAL DYSPEPSIA
- HELICOBACTER PYLORI - GASTRITIS
- HELICOBACTER PYLORI - TREATMENT
- GASTRITIS
Introduction
For decades endoscopic ‘gastritis,’ gastric erosions and even histological findings of gastric inflammation have failed to attract much attention from clinicians as the majority of patients with these findings remain asymptomatic. Although gastritis is often used to describe dyspeptic symptoms, the presence of such symptoms correlates poorly with histological or endoscopic gastritis. Although the term ‘gastritis’ is still used as a concept to explain dyspeptic symptoms, gastritis as a term refers to gastric inflammation, often accompanying structural mucosal changes.1 This gastric inflammation (gastritis) has long been associated with peptic ulcer, gastric cancer and pernicious anaemia, but the cause or causes of gastritis remain poorly understood. The discovery that Helicobacter pylori (H. pylori) was a cause of gastritis2 focused attention on the aetiology, natural history and prognosis of gastritis.
Worldwide the most common cause of chronic gastritis is infection with H. pylori. H. pylori causes progressive damage to the gastric mucosa and is now accepted as playing a causative role in a number of important diseases, including duodenal ulcer disease, gastric ulcer disease, gastric adenocarcinoma and gastric mucosa-associated lymphoid tissue (MALT) lymphoma.3–5 Indeed, H. pylori–induced gastritis is considered as the most important risk factor for peptic ulcer and its complications as well as for gastric cancer.5
The current International Statistical Classification of Diseases and Related Health Problems (ICD-10), issued in 1989 by the International Conference for the Tenth Revision of the ICD was endorsed by WHO at the 43rd general assembly in 1990 and has been used for disease statistics since 1994 among member countries of WHO. In the ICD-10, all the digestive diseases are classified under K code with different two-digit numbers.6 However, H. pylori was not integrated into gastritis classification in the gastritis section (K29) of ICD-10, even though H. pylori gastritis is the predominant type of gastritis and clinically by far the most relevant because of its predisposing role of severe gastroduodenal complications.3–5 Moreover, the current ICD-10 classification of gastritis is not organised according to aetiology but is merely a mixture of phenotype and aetiology and also includes duodenitis (box 1). Therefore, a revision of the gastritis and duodenitis classification based on all the possible aetiologies was proposed after the working group meeting for the ICD-11 revision held in Tokyo in 2010 and submitted as the ICD11 β foundation component. However, in the ICD11 β foundation classification (box 2), the original plan was changed. In an attempt to gather broader opinions on the rationale of the new classification system originally proposed to ICD-11, we devoted one section to this important issue at this meeting.
Current International Statistical Classification of Diseases and Related Health Problems (ICD-10) classification of gastritis (K29 code) http://apps.who.int/classifications/icd10/browse/2015/en#/K29
K29 Gastritis and duodenitis
Excl: eosinophilic gastritis or gastroenteritis (K52.8)
Zollinger–Ellison syndrome (E16.4)
K29.0 Acute haemorrhagic gastritis
Incl: Acute (erosive) gastritis with haemorrhage
Excl: erosion (acute) of stomach (K25.–)
K29.1 Other acute gastritis
K29.2 Alcoholic gastritis
K29.3 Chronic superficial gastritis
K29.4 Chronic atrophic gastritis
Incl: Gastric atrophy
K29.5 Chronic gastritis, unspecified
Incl: Chronic gastritis
Antral
Fundal
K29.6 Other gastritis
Incl: Giant hypertrophic gastritis
Granulomatous gastritis
Ménétrier disease
K29.7 Gastritis, unspecified
K29.8 Duodenitis
K29.9 Gastroduodenitis, unspecified
Excl, exclusion criteria; Incl, inclusion criteria.
Classification of gastritis (2A) and duodenitis (2B) in the foundation component of International Statistical Classification of Diseases and Related Health Problems (ICD11 β) (as accessed at 20 January 2015) http://apps.who.int/classifications/icd11/browse/f/en#/
Please note that this classification is continuously updated and hence is subject to change. This classification is not authorised by WHO.
2A Classification of gastritis at the foundation layer of ICD11 β
Helicobacter pylori-induced gastritis
Drug-induced gastritis
Autoimmune gastritis
Stress-induced gastritis
Special forms of gastritis
Allergic gastritis
Gastritis due to biliary reflux
Lymphocytic gastritis
Ménétrier disease
Eosinophilic gastritis
Infectious gastritis
Gastric phlegmone
Bacterial gastritis
H. pylori-induced gastritis
Enterococcal gastritis
Mycobacterial gastritis
Tuberculous gastritis
Non-tuberculous mycobacterial gastritis
Mycobacterium avium-intracellulare gastritis
Gastritis due to other specified non-tuberculous mycobacteria
Secondary syphilitic gastritis
Viral gastritis
Cytomegaloviral gastritis
Enteroviral gastritis
Fungal gastritis
Gastritis due to mucoromycosis
Gastric candidiasis
Gastric histoplasmosis
Parasitic gastritis
Gastric anisakiasis
Cryptosporidium gastritis
Gastric strongyloides stercoralis
Gastritis due to other diseases classified elsewhere
Gastritis due to Crohn's disease
Gastritis due to sarcoidosis
Gastritis due to vasculitis
Gastritis due to external causes
Alcoholic gastritis
Radiation gastritis
Chemical gastritis
Gastritis due to other specified external causes
Gastritis of unknown aetiology with specific endoscopic or pathological features
Superficial gastritis
Acute superficial gastritis
Chronic superficial gastritis
Acute haemorrhagic gastritis
Chronic atrophic gastritis
Mild to moderate gastric atrophy
Severe gastric atrophy
Metaplastic gastritis
Granulomatous gastritis
Hypertrophic gastritis
Other gastritis
Chronic gastritis, not elsewhere classified
Acute gastritis, not elsewhere classified
2B Classification of duodenitis at the foundation layer
Helicobacter pylori-induced duodenitis
Stress-induced duodenitis
Duodenitis due to external causes
Alcoholic duodenitis
Chemical duodenitis
Radiation duodenitis
Duodenitis due to other external causes
Drug-induced duodenitis
Special forms of duodenitis
Allergic duodenitis
Eosinophilic duodenitis
Lymphocytic duodenitis
Infectious duodenitis
Duodenal phlegmone
Bacterial duodenitis
Mycobacterial duodenitis
Non-tuberculous mycobacterial duodenitis
Tuberculous duodenitis
Duodenitis due to Whipple's disease
Fungal duodenitis
Duodenal candidiasis
Parasitic duodenitis
Ancylostomiasis duodenitis
Duodenal anisakiasis
Duodenitis due to Giardia lamblia
Strongyloides duodenitis
Viral duodenitis
Cytomegaloviral duodenitis
Herpetic duodenitis
Duodenitis due to other diseases, classified elsewhere
Duodenitis due to coeliac disease
Duodenitis due to Crohn's disease
Duodenitis due to sarcoidosis
Duodenitis due to vasculitis
Duodenitis due to IgA vasculitis
Duodenitis due to Whipple's disease
Duodenitis of unknown aetiology with specific endoscopic or pathological features
Acute haemorrhagic duodenitis
Granulomatous duodenitis
As stated above, if H. pylori gastritis is categorised as an infectious disease, the inclusion of H. pylori gastritis-associated dyspeptic symptoms as a ‘functional disease’ entity poses a special challenge,7 ,8 despite it being implicated in the pathogenesis of functional dyspepsia (FD) symptoms.9 Despite the definition given by Rome III,9 a conceptual ambiguity on how to deal with H. pylori gastritis-associated dyspeptic symptoms in the context of the clinical assessment of FD still remains.5 ,10–12 Accordingly, guidelines and meta-analyses that included dyspepsia associated with H. pylori under the umbrella of ‘functional dyspepsia’5 ,10–12 would require reconsideration in accordance with advances made in the area of H. pylori gastritis.
Third, there has been significant technical progress in diagnostic tools for GI diseases. Advanced endoscopy with image-enhanced modalities and magnification allows diagnosis of gastritis with a high degree of accuracy, even before histological confirmation.13–15 Furthermore, non-invasive diagnostic tests such as the [13C]-urea breath test, faecal antigen test and serological parameters serve as surrogate markers of H. pylori gastritis and indicators of gastritis severity.5 Classification systems for grading gastritis such as the Operative Link for Gastritis Assessment (OLGA) and Operative Link for Gastric Intestinal Metaplasia Assessment (OLGIM) have also been proposed,16–18 in addition to the internationally accepted Sydney System,19 ,20 and their utility needs to be evaluated and agreed upon.
In 2013, the Japanese government insurance policy approved eradication therapy for H. pylori-positive gastritis after endoscopic examination, to exclude more serious diseases such as ulcer and cancer, in line with the Japanese guidelines for H. pylori management.11 However, no global consensus has been published on when to recommend eradication therapy for H. pylori gastritis and how to follow up after eradication.
Since the global awareness of gastritis is still confounded by a number of controversial issues as described above, a meeting was set up in Kyoto to achieve global consensus on H. pylori gastritis; to attempt conceptual changes in gastritis classification in general; to agree diagnosis and management strategies with special reference to FD and cancer prevention.
Method
Consensus development process
Four major topics were chosen by core members of the organising committee (KS, NU and PM). Drafts of clinical questions (CQs) about each topic were prepared by the ad hoc committee of the Japanese Society of Gastroenterology (JSGE) and were further revised by core members (KS, PM and EME-O). Altogether, 23 CQs were selected for the first round of voting.
Faculty members were selected from members of the JSGE, European Helicobacter Study Group, Asian Pacific Association of Gastroenterology, Healthy Stomach Initiative and the working group members of gastroenterology for ICD-11. These members were assigned to one of the four subgroups by core members (KS, NU and PM) based on their expertise and two members from each subgroup were invited to serve as moderators. The faculty members of each group were assigned one or two CQs for which they were asked to prepare statements and supporting evidence. These statements were edited by moderators and core members and uploaded to the electronic voting system developed by JSGE.
The Delphi method was used for consensus development, and voting by each faculty member was done anonymously through the electronic system. Each faculty member was asked to indicate one of the following levels of agreement: strongly agree, agree with minor reservation, agree with major reservation, disagree with minor reservation, disagree with major reservation and strongly disagree. If the member’s vote was other than strongly agree or agree with minor reservation, they were asked to give the reasons for reservation or disagreement.
Consensus level was predefined as ≥80% of the sum of the votes of strongly agree plus agree with minor reservation. After the first round of voting, moderators in each subgroup initiated further discussion about the statements which had failed to reach consensus. After this discussion, the revised statements were uploaded to the electronic voting system for a second round of voting. This process resulted in several CQs being modified for improved understanding and to better fit the statements. At the second round of voting, faculty members were asked to provide recommendation as to the grade of evidence and the levels of supporting evidence for the statements. Recommendation grade and evidence level were based on the GRADE system21 ,22 (see online supplementary table S1 and S2). Electronic reminders were automatically sent to all faculty members twice (3 days and 1 day before the closing dates). Voting rates of 100% were achieved in the two voting sessions.
The second round of voting was followed by a face-to-face meeting in Kyoto on 31 January to 1 February 2014. On the first day, preliminary plenary voting was conducted since faculty members had hitherto been blinded to the voting results in other sections. This process identified several statements which failed to achieve consensus of ≥80%. Each group then met to resolve disagreements and better reflect opinions from all group members. On the second day, the revised statements were presented at plenary discussions with all group members. Voting for each statement was done using a key pad system with the levels of agreements being shown on the screen in real time. Statements that failed to reach consensus were discussed, revised if considered necessary and voted on again. Finalised statements were summarised by moderators assigned to each group.
The five colleagues who could not attend the face-to-face meeting or missed the final voting were invited later to give their votes for all the finalised statements without notification of the plenary voting results. The impact of their votes is discussed below.
For management of conflict of interest (COI), each member was asked to present COI status according to the JSGE guidelines. If a relevant COI had existed, that person would have been asked not to vote, in accordance with the recent consensus,23 but no such case was encountered. The majority of the funding was provided by JSGE with a hand-reach support from industries, which were otherwise not involved in the planning, organisation or manuscript writing and did not join in the discussions.
Process and results
At the first round of voting 16 CQs achieved the predefined consensus level of ≥80%. Six statements failed to reach consensus and each section met to modify their assigned statements based on the comments and opinions received. This led to some questions being split into two or being combined, resulting in 24 CQs, including 25 statements which were subjected to the second round of voting within their assigned group. The results of the second round of voting were disclosed on the first day of the face-to-face meeting in Kyoto. At this stage, all statements except one had achieved consensus. To facilitate further discussion in the break-out sessions, preliminary plenary voting was done to enable the respective section members to consider the opinions of all group members.
On the second day, the finalised CQs and accompanying statements were presented for plenary voting. If consensus levels were not reached, open discussions ensued to modify the statements, followed by voting. All the finalised CQs and statements are shown in the four consensus sections. Levels of recommendation and evidence are shown together with the voting results. For CQ1 to CQ8A, 39 members voted, while 38 voted for CQ8B to CQ14A and 37 voted for CQ14B to CQ23. During the plenary voting, one subdivided CQ (CQ19) was recombined, while another CQ (CQ21) was deleted because of redundancy, resulting in 22 CQs and 24 statements. All voting during the plenary session was done anonymously by an electronic voting system with key pads distributed to each faculty member. The five faculty members who missed the plenary voting session were asked to vote later for the finalised CQs and statements without knowledge of the plenary voting results. Their voting results were almost identical with the plenary voting results. They agreed on all the CQs with the only exception being CQ11, showing 80% (one out of five) agreement. Since there was no inconsistency between the plenary voting and voting by the absentees, combining the two sets of results did not influence the outcome. The entire consensus results are shown below.
CONSENSUS STATEMENT
Section 1. Classification of gastritis in relation to ICD-11
CQ1. Is the current ICD-10 classification for gastritis appropriate?
Statement 1
The current ICD-10 classification for gastritis is obsolete in view of the discovery of H. pylori.
Grade of recommendation: strong
Evidence level: high
Consensus level: 100%
Comment
The ICD-10 classification of gastritis was formulated in 1989 and is still in effect in most countries. At the time of formulation, the ICD-10 classification of gastritis and duodenitis (K29) was rudimentary as it was based on macroscopic and histomorphological criteria; the only aetiological factor assigned was alcohol6 (box 1). The histological classification of gastritis considered mainly aspects of atrophy and autoimmunity.1
The discovery of H. pylori had not been taken into account, possibly because even though release came after the discovery of Campylobacter pylori (H. pylori), the role of H. pylori in disease was still controversial. The recognition of H. pylori infection as the primary cause of chronic gastritis proved to be a breakthrough that reopened the chapter on gastritis and its role in disease.2 ,24 ,25 At present, no classification of gastritis would be complete without including H. pylori as the aetiological cause.
CQ2. Is the proposed ICD-11 classification for gastritis appropriate?
Statement 2
The newly proposed classification of gastritis in the ICD11 β version is an improvement because it is based on aetiological factors.
Grade of recommendation: strong
Evidence level: moderate
Consensus level: 100%
Comment
Although the ICD-10 has been updated regularly to accommodate new diseases and concepts, WHO recognised the necessity of overall systematic changes in the ICD and decided to revise the current ICD-10 to ICD-11 in 2007. As the intermediate process for this revision, the ICD11 β version was formulated with input from various scientific advisory groups. This version was open to the public so that opinions from various interest groups and a broader range of medical specialists could be reflected before compiling the ICD-11. ICD11 β foundation component consists of the core of the ICD-11 classification from which mortality and morbidity classifications will derive. However, it remains a draft and can be changed from time to time before finalisation of ICD-11 (for more details, please visit http://www.who.int/classifications/icd/revision/betaexpectations/en/).
In the ICD11 β foundation component of the gastritis section, classification of gastritis was principally based on aetiological factors with consideration of their specific pathophysiological principles (box 2). Accordingly, H. pylori gastritis is categorised as a specific nosological entity.
The assessment of gastritis based on histopathological criteria was completely changed after recognition of H. pylori as the most common cause of chronic gastritis. The Sydney System was developed as a consequence and has been integrated into clinical practice. The Sydney classification of gastritis combined histological parameters of activity, chronicity, atrophy, intestinal metaplasia, topographical distribution and aetiopathogenic information for reporting the pathology of gastritis in endoscopic biopsies.19 ,20
As described above, classification of gastritis in the foundation component of ICD11 β version is principally based on causative factors, in order to cover the three most important and best defined categories of gastritis—namely, (a) H. pylori-induced, (b) drug-induced and (c) autoimmune gastritis. A specific diagnosis among these different categories of gastritis is required to direct specific management and treatment strategies. The diagnosis of H. pylori-induced gastritis has major implications for life-long healthcare. H. pylori gastritis may cause dyspeptic symptoms26 ,27 and result in gastroduodenal pathologies, including peptic ulcer disease (PUD) and gastric cancer. The recognised role of H. pylori as a carcinogen makes eradication of H. pylori infection the preferred strategy for the prevention of gastric cancer.5 ,11 ,28 There is more to learn about aetiologies other than H. pylori in gastritis and this is dealt with as ‘H. pylori-negative or idiopathic gastritis’.29
The proposed aetiology-based classification for gastritis in the foundation component of ICD11 β version was further refined by this consensus meeting (box 3). Clinical validation is needed to further define and confirm the usefulness of the new classification.
Aetiology-based classification of gastritis (3A) and duodenitis (3B). A proposal according to the consensus at the Kyoto consensus conference
3A Proposed classification of gastritis in the Kyoto consensus conference
Autoimmune gastritis
Infectious gastritis
Helicobacter pylori-induced gastritis
Bacterial gastritis other than H. pylori
Helicobacter heilmannii gastritis
Enterococcus gastritis
Mycobacteria gastritis
Secondary syphilitic gastritis
Gastric phlegmone
Viral gastritis
Enteroviral gastritis
Cytomegalovirus gastritis
Fungal gastritis
Gastritis due to mucormycosis
Gastric candidiasis
Gastric histoplasmosis
Parasitic gastritis
Cryptosporidium gastritis
Gastric strongyloides stercorale
Gastric anisakiasis
Gastritis due to external causes
Drug-induced gastritis
Alcoholic gastritis
Radiation gastritis
Chemical gastritis
Gastritis due to duodenal reflux
Gastritis due to other specified external cause
Gastritis due to specified causes
Lymphocytic gastritis
Ménétrier disease
Allergic gastritis
Eosinophilic gastritis
Gastritis due to other diseases classified elsewhere
Gastritis due to sarcoidosis
Gastritis due to vasculitis
Gastritis due to Crohn's disease
3B Proposed classification of duodenitis in the Kyoto consensus conference
Infectious duodenitis
H. pylori-induced duodenitis
Bacterial duodenitis other than H. pylori
Mycobacterial duodenitis
Duodenitis due to Tropheryma whipplei (Whipple's disease)
Duodenal phlegmone
Fungal duodenitis
Duodenal candidiasis
Parasitic duodenitis
Ancylostomasis (hookworm) duodenitis
Duodenal anisakiasis
Duodenitis due to Giardia lamblia
Strongyloides duodenitis
Viral duodenitis
Cytomegaloviral duodenitis
Herpetic duodenitis
Duodenitis due to external causes
Alcoholic duodenitis
Chemical duodenitis
Radiation duodenitis
Duodenitis due to other external causes
Drug-induced duodenitis
Duodenitis due to specified causes
Allergic duodenitis
Eosinophilic duodenitis
Lymphocytic duodenitis
Duodenitis due to other diseases classified elsewhere
Duodenitis due to Crohn's disease
Duodenitis due to sarcoidosis
Duodenitis due to vasculitis
Duodenitis due to Henoch–Schönlein purpura
Duodenitis due to coeliac disease
Furthermore, duodenitis, which was in the gastritis section in ICD-10, is now categorised in an independent section in the foundation component. It should be noted that the Joint Linearisation of Mortality and Morbidity of ICD11 β version is now publicly available (see online supplementary table S3) and differs significantly from the foundation component (box 2) or aetiology-based classification proposed in this paper (box 3). This linearisation did not adopt the principle of aetiology-based classification, thus requiring further revision.
CQ3. Is it necessary to categorise gastritis according to gastric subsite?
Statement 3
It is useful to categorise H. pylori-induced gastritis according to gastric subsites, because the risks of gastric cancer and peptic ulcer are affected by the patterns of gastritis.
Grade of recommendation: strong
Evidence level: high
Consensus level: 97.4%
Comment
The categorisation of H. pylori gastritis according to gastritis subsites together with the assessment of gastritis severity allows prediction of an individual’s risk of developing severe gastroduodenal complications and, in particular, gastric cancer.30–32
Depending on the gastric subsites involved, gastric function and, in particular, gastric acid secretion may be profoundly affected, resulting in gastric acid hypersecretion, hyposecretion or even achlorhydria.33–35
Subsite characterisation of gastritis is also critically important for identifying those patients who remain at high risk after H. pylori eradication and thus are candidates for regular endoscopic and histological follow-up.36 Patients with severe atrophic gastritis (with or without intestinal metaplasia) in the corpus or with severe corpus predominant gastritis are those at highest risk for progression to gastric cancer of the intestinal type31 ,37 and for diffuse-type gastric cancer. In diffuse-type gastric cancer the prevalence of antral atrophic gastritis is almost identical to that seen in the intestinal type but is slightly less with corpus atrophic gastritis than with intestinal type gastric cancer.38
CQ4. Is it necessary to categorise gastritis according to histology (severity) and/or endoscopy?
Statement 4
It is advisable to categorise gastritis according to histology, because the risk of development of gastric cancer in H. pylori gastritis varies according to the extent and severity of inflammation and atrophy.
Grade of recommendation: strong
Evidence level: high
Consensus level: 100%
Comment
The updated Sydney System has been globally implemented into clinical practice and requires proper assessment of all the relevant characteristics of H. pylori gastritis including atrophy and intestinal metaplasia at different gastric subsites.19 ,20 Categorising gastritis is clinically relevant because the ‘phenotype’ of H. pylori gastritis determines the risk of progression to gastroduodenal complications.
Severity and extent of atrophic gastritis and intestinal metaplasia are well established as indicators of the increased risk for developing gastric cancer.31 ,39 ,40 Similarly, severe H. pylori-induced corpus gastritis is associated with an increased risk for gastric cancer.31 ,41 New staging systems for the characterisation of gastritis have been introduced to assess the gastric cancer risk. They are used in clinical practice and are either based on the severity of atrophy in various gastric subsites (OLGA)16 ,17 or on intestinal metaplasia (OLGIM).18 Both systems, discussed further in section 3, are reported to have a positive impact on patient management.
CQ5. How should we classify gastric erosions in the context of chronic gastritis?
Statement 5
Gastric erosions should be reported separately from gastritis. The natural history and clinical significance of gastroduodenal erosions depend on aetiology and need further clarification.
Grade of recommendation: strong
Evidence level: low
Consensus level: 100%
Comment
Gastric erosions are defined as superficial mucosal breaks with a diameter of <3 mm or <5 mm.42 This small size makes it less likely to confound erosions with peptic ulcers which, by definition, penetrate the muscularis mucosae.3
Gastric erosions can be detected in the context of H. pylori infection but are more frequently caused by intake of mucosal damaging drugs—in particular, aspirin and non-steroidal anti-inflammatory drugs (NSAIDs).43 ,44
Furthermore, several different morphological forms were noted after eradication of H. pylori as (a) flat, (b) raised, (c) haemorrhagic and (d) appearing as bleeding spots with localisation in the antrum in the absence of drugs,45 possibly owing to hyperacidity after eradication therapy.46 ,47
From a clinical perspective, the most relevant aspect of erosions is that patients taking NSAIDs and having numerous erosions in the stomach are at increased risk of developing ulcers subsequently.48
Few studies on the clinical significance or natural history of gastric or duodenal erosions have been reported. Thus, it is important to conduct a prospective research in which erosions in the stomach and duodenum are separately reported in conjunction with the category of gastritis, which is needed to better understand the natural history of gastric erosions and their potential to progress to ulceration and bleeding. Validated scores for reporting erosions for research purposes should be used.49
CQ6. Is H. pylori gastritis an infectious disease irrespective of symptom and complications?
Statement 6
H. pylori gastritis should be defined as an infectious disease, even when patients have no symptoms and irrespective of complications such as peptic ulcers and gastric cancer.
Grade of recommendation: strong
Evidence level: high
Consensus level: 100%
Comment
H. pylori gastritis is an infectious disease and leads to chronic active gastritis of varying severity in virtually all infected subjects.50
There is a significant variability in the interindividual expressions of gastric mucosal structural damage and accordingly the associated physiological perturbations also vary.30 ,35 H. pylori gastritis may remain clinically unapparent or evolve into severe complications. The rate of progression is unpredictable. The most severe clinical expression is gastric cancer, which is often incurable by the time of diagnosis.
Cure of H. pylori infection leads to healing of the inflamed gastric mucosa, which may return to normal. H. pylori eradication may improve or resolve dyspeptic symptoms and usually cures PUD. H. pylori gastritis is a disease which can be cured and thus prevent severe complications. If H. pylori gastritis has progressed to more severe forms of gastritis, including atrophic gastritis with or without intestinal metaplasia, or severe corpus predominant gastritis, the risk of gastric cancer is increased and eradication of the infection at this stage needs to be integrated with a follow-up strategy.5 ,11 ,28 ,31 ,36 ,40
Section 2 Dyspepsia associated with H. pylori infection
CQ7. Does H. pylori gastritis cause dyspepsia?
Statement 7
H. pylori gastritis is the cause of dyspepsia in a subset of patients.
Grade of recommendation: strong
Evidence level: high
Consensus level: 100%
Comment
A large number of observations support the conclusion that H. pylori infection may be a cause of symptoms in a proportion of patients presenting with dyspepsia.26 ,27 First, acute iatrogenic or self-administered infection with H. pylori can induce acute dyspeptic symptoms.24 ,25 However, while persistent colonisation virtually always leads to chronic gastritis,48 in the majority of individuals severe dyspeptic symptoms are transient.24 ,25 ,51 Second, most but not all, epidemiological studies show associations between H. pylori infection and (uninvestigated) dyspeptic symptoms.52–55 The most convincing evidence can be derived from H. pylori eradication studies in infected patients with uninvestigated or FD.12 ,56–61 In these studies, eradication is associated with a small but statistically significant benefit for symptom control over no eradication; the estimated number needed to treat is 1412 and in a more recent study the number was 8.61 At present there are no criteria to predict whether a patient with dyspeptic symptoms will respond to eradication therapy or not. Therefore, the only way in clinical practice is to eradicate the H. pylori infection and see whether symptoms resolve or whether additional treatments will be required. The symptomatic gain takes at least 6 months to become significant over no eradication and this has been attributed to the time it takes for gastritis to recover.12 ,59–61
CQ8. Should we categorise H. pylori-associated dyspepsia as a specific entity?
Statement 8A
In H. pylori-infected patients with dyspepsia, symptoms can be attributed to H. pylori gastritis if successful eradication therapy is followed by sustained symptom remission.
Grade of recommendation: strong
Evidence level: high
Consensus level: 97.4%
Statement 8B
H. pylori-associated dyspepsia (as in statement 8A) is a distinct entity.
Grade of recommendation: strong
Evidence level: moderate
Consensus level: 92.1%
Comment
Based on the Rome III consensus,9 ,62 FD is defined as “the presence of chronic dyspeptic symptoms (postprandial fullness, early satiation, epigastric pain or burning) without evidence of structural disease (including at upper endoscopy) that is likely to explain the symptoms” (figure 1). This group was contrasted with those in whom chronic dyspeptic symptoms have an identified organic or metabolic cause, where elimination of that cause or improvement of the disease leads to resolution or improvement of symptoms.9

Diagnostic algorithm of Helicobacter pylori-associated dyspepsia. Patients with dyspeptic symptoms after negative routine laboratory and upper gastrointestinal endoscopy except for positive H. pylori tests, should undergo eradication therapy. If sustained symptomatic relief is obtained, their dyspeptic symptoms are considered as H. pylori-associated dyspepsia. On the other hand, if dyspeptic symptoms do not resolve or recur after eradication therapy, they are judged to have functional dyspepsia. EGD, oesophagastroduodenoscopy.
The Rome III consensus mentions a subset of patients with H. pylori gastritis as representative of organic dyspepsia if they respond to eradication. Patients with H. pylori gastritis in whom symptoms persist despite eradication therapy eliminating the infection were identified as having FD.9 As mentioned above, eradication therapy studies showed that a subset of H. pylori-infected patients with FD derive symptomatic benefit from eradication, with a delay of at least 6 months from cure of the infection.12 ,59–61
Based on these considerations, sustained symptom control after successful eradication identifies H. pylori as the organic cause of the symptoms in these patients and provides the rationale to consider H. pylori-associated dyspepsia as a separate clinical entity. H. pylori-infected patients with chronic dyspeptic symptoms and negative endoscopy are now treated and labelled depending on their treatment response as outlined in figure 1.
CQ9. Is eradication of H. pylori infection first-line treatment for improving dyspeptic symptoms?
Statement 9
Eradication of H. pylori is first-line treatment for H. pylori-infected dyspeptic patients.
Grade of recommendation: strong
Evidence level: high
Consensus level: 94.7%
Comment
As is apparent from statement 8, there is a group of patients with FD for whom H. pylori is considered the cause of their symptoms, and this can be established if eradication is associated with sustained symptom benefit.9 ,59–61 This scenario is the only one where patients with chronic dyspeptic symptoms and a negative endoscopy can be ‘cured’, albeit with some delay after successful eradication therapy.12 ,59–61 Moreover, very few effective alternative therapeutic approaches have been proved to have substantial and sustained benefit in FD.63 Finally, eradication therapy is a short treatment, with acceptable cost–benefit for controlling dyspeptic symptoms, and with other potential benefits for prevention of peptic ulcer and gastric cancer.5 Based on these considerations, eradication therapy can be proposed as first-line treatment for H. pylori-infected dyspeptic patients, which is in line with a recent management algorithm by the Rome foundation.64
CQ10. How effective is H. pylori eradication on dyspeptic symptoms—in the short and long term—and how does it compare with other treatments (such as proton pump inhibitors (PPIs))?
Statement 10
In H. pylori-infected dyspeptic patients, eradication therapy for dyspeptic symptoms is better than placebo and is the preferred option.
Grade of recommendation: strong
Evidence level: high
Consensus level: 97.4%
Comment
Eradication therapy studies have confirmed that a subset of H. pylori-infected patients with FD is relieved of dyspeptic symptoms by eradication therapy.12 ,56–61 To date, only a limited number of studies have directly compared eradication therapy with other treatments that are used for FD, such as PPIs or prokinetic therapy.57 ,60 ,61 Hence, although the symptomatic gain takes at least 6 months,57 ,60 ,61 eradication is the preferred treatment. Future trials should compare eradication with treatment modalities other than placebo in H pylori-infected patients with chronic dyspeptic symptoms and a negative endoscopy.
CQ11. Should patients who remain dyspeptic after successful H. pylori eradication be considered to have FD?
Statement 11
Patients who remain symptomatic after successful H. pylori eradication should be considered to have FD.
Grade of recommendation: weak
Evidence level: moderate
Consensus level: 97.4%
Comment
As indicated in statements 8A and 8B and in agreement with the Rome III criteria,9 ,62 H. pylori infected dyspeptic patients with negative endoscopy who experience sustained symptom control are labelled as having H. pylori-associated dyspepsia. Conversely, when symptoms do not benefit in the long term from successful eradication, this indicates that H. pylori gastritis did not cause the symptoms in these patients. Consequently, they can keep the label ‘functional dyspepsia’ (figure 1).
Section 3 Diagnosis of gastritis
CQ12. Is it possible to make a diagnosis of atrophy and/or intestinal metaplasia by endoscopy?
Statement 12
Atrophic mucosa and intestinal metaplasia can be accurately detected by image-enhanced endoscopy, after appropriate training. Grade of recommendation: strong
Evidence level: high
Consensus level: 84.2%
Comment
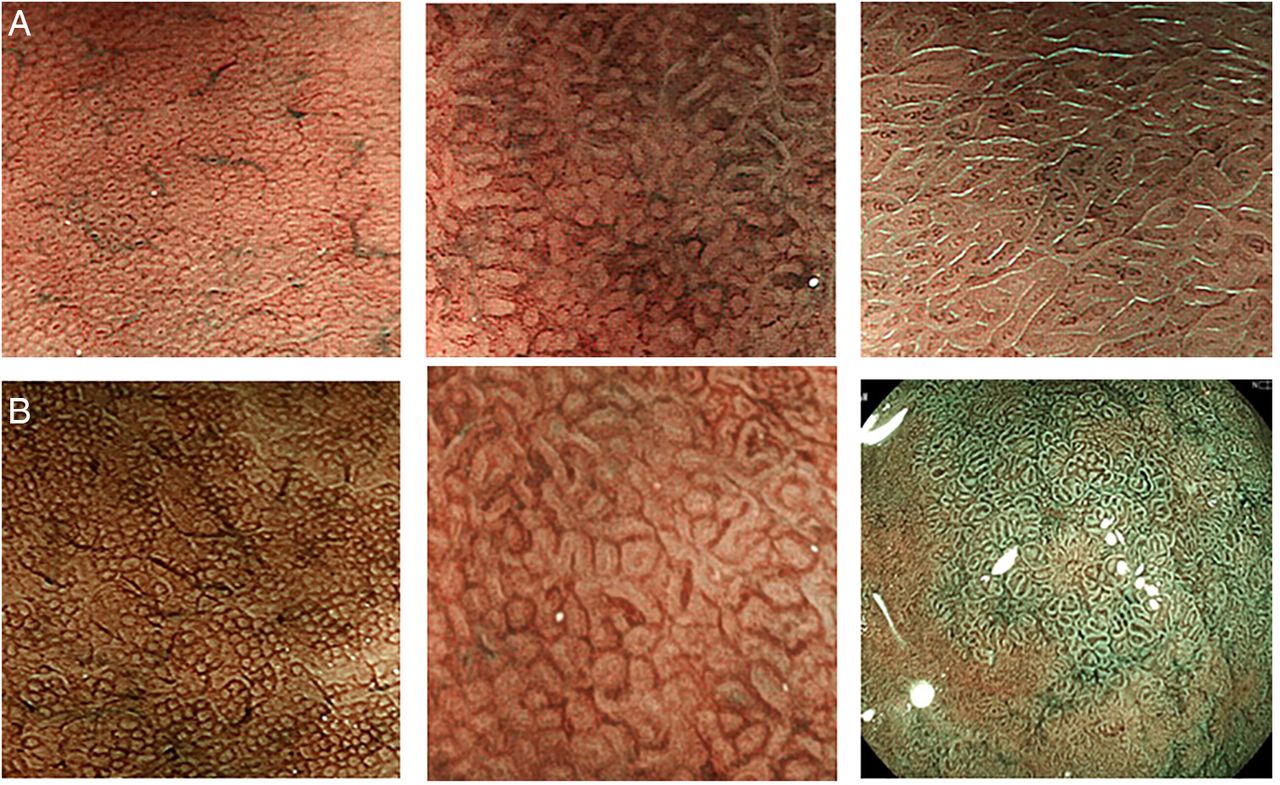
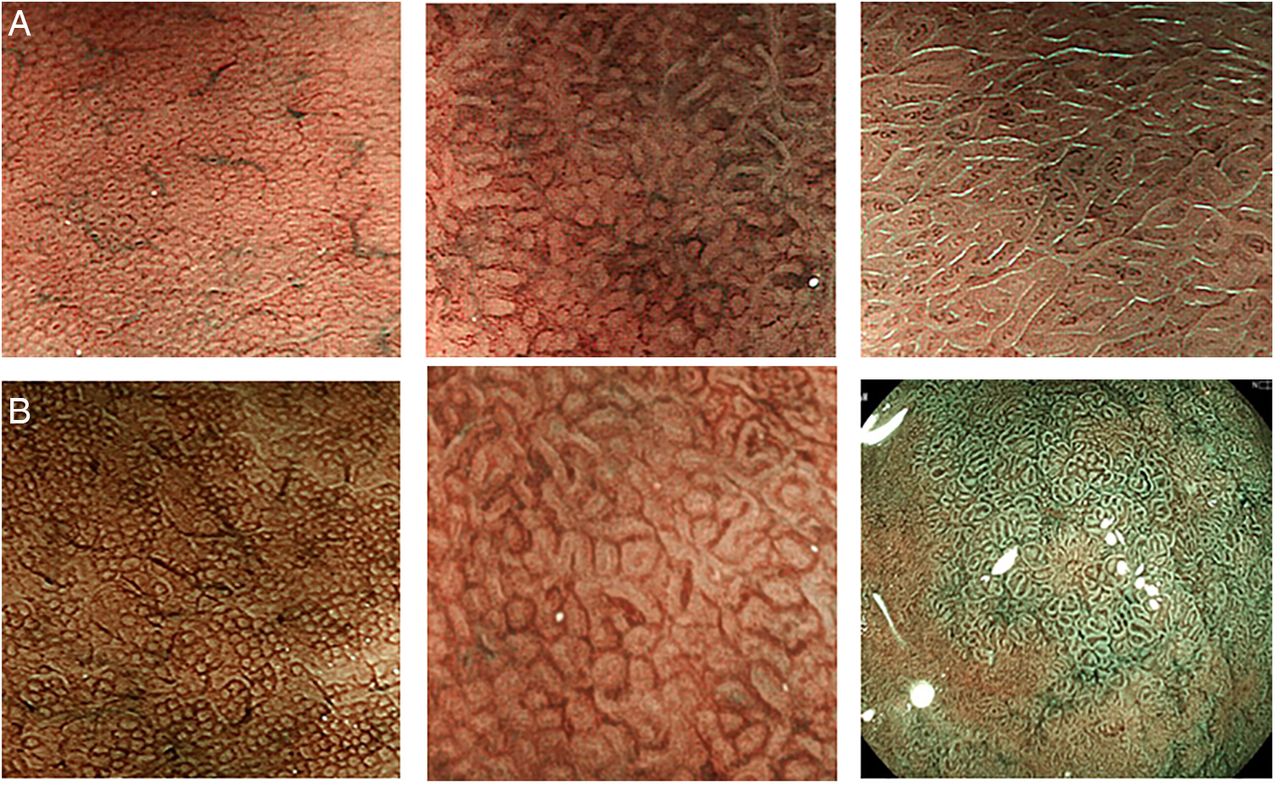
Conventional endoscopy is, in most hands, an inadequate tool for diagnosing atrophy and intestinal metaplasia and therefore it remains mandatory that a biopsy is carried out, allowing histomorphological assessment of the gastric mucosa according to the Sydney classification.19 ,20 However, image-enhanced endoscopy has improved the accuracy and reproducibility of endoscopic diagnosis of premalignant gastric lesions. This includes chromoendoscopy,65 high-resolution magnification endoscopy66 ,67 and image-enhanced endoscopy combined with magnification15 ,68–72 (figure 2). These methods are now routinely available in Japan and will be increasingly used worldwide. Adequate evaluation of the stomach mucosa with each of these methods requires appropriate training66 and offers the advantage of targeted biopsies.
{kind=link}
{kind=link}
Image enhanced endoscopy. (A) Narrow band imaging (NBI) of the gastric mucosa. Round homogeneous sized pits with regularly arranged collecting venules are shown (left). This pattern (regular arrangement of collecting venules) named ‘RAC’ pattern in the corpus mucosa highly indicates a Helicobacter pylori negative state.13 In the H. pylori-infected mucosa with inflammation, pit patterns are elongated, varied in sizes and shapes with spaces between them. Collecting venules are obscured owing to inflammation (centre).14 When intestinal metaplasia develops, the pit pattern is further elongated with light blue lines (light blue crest sign) decorating the pits margins (right).66 The images were provided by Dr Kazuyoshi Yagi. (B) Blue laser imaging (BLI) of the gastric mucosa. BLI is a new modality of image enhancement.70 The BLI-bright mode can easily obtain lower magnification images, similar to the NBI images in (A) (left). With BLI-magnification mode, further mucosal details including periglandular capillary networks (red coloured circles surrounding the pits) are seen (centre). BLI endoscopy is useful for identifying the area of intestinal metaplasia where greenish coloured elongated pit patterns predominate (right). The images were provided by Dr Hiroyuki Osawa, Jichi Medical University.
CQ13. Is the updated Sydney System appropriate for histological diagnosis of gastritis?
Statement 13
Accurate histological assessment of gastritis requires biopsy sampling of both antrum and corpus.
Grade of recommendation: strong
Evidence level: high
Consensus level: 92.1%
Comment
Premalignant lesions of the stomach may be unevenly distributed. Therefore, accurate histological assessment of gastritis requires biopsy sampling of both antrum and corpus. This may facilitate the classification and grading of preneoplastic gastric lesions.73 Various studies have shown that more extensive biopsy sampling increases the diagnostic yield for identifying patients with premalignant lesions and provides a better overview of the severity and distribution of these lesions.74–76 This also has practical limitations, which led to the updated Sydney System. This provides guidance on the methods of sampling and the histopathological grading of individual abnormalities—in particular, inflammation, gland loss and metaplasia.20 The Sydney System recommends routine sampling of five gastric biopsy specimens: antrum greater and lesser curvature, incisura and corpus greater and lesser curvature. Specimens need to be put into separate vials and grouped for each site or lesion. The system is widely used; the most common modification being to leave out the separate incisura sample.36 It is of key importance that separate specimens are obtained from endoscopically visible lesions. The accuracy of image-enhanced endoscopy in trained hands further increases the yield of targeted biopsies.66 ,77 ,78
CQ14. Are grading systems such as OLGA and OLGIM useful for risk stratification?
Statement 14A
Gastric cancer risk correlates with the severity and extent of atrophic gastritis. Grade of recommendation: strong
Evidence level: high
Consensus level: 94.7%
Statement 14B
Histological staging systems such as OLGA and OLGIM are useful for risk stratification.
Grade of recommendation: strong
Evidence level: low
Consensus level: 97.3%
Comment
Most gastric cancers are triggered by longstanding gastritis, primarily due to H. pylori infection. This can occur via a multistep pathway of precancerous lesions—in particular, atrophic gastritis, intestinal metaplasia and dysplasia/intraepithelial neoplasia. Various studies confirm an increased gastric cancer risk in patients with premalignant gastric lesions. For instance, a nationwide study from the Netherlands including approximately 98 000 patients with premalignant gastric lesions reported, on average, a 2–3% gastric cancer risk over 10 years.79 This risk varied with the baseline stage of premalignant lesions, being 0.8%, 1.8%, 3.9% and 32.7% for patients with atrophic gastritis, intestinal metaplasia, mild-to-moderate dysplasia and severe dysplasia, respectively.79
These data confirmed the association between presence of premalignant gastric lesions and development of gastric cancer, yet also showed that the risk for developing gastric cancer in an individual with premalignant lesions is nevertheless small (2–6 per 1000 people per year). This necessitates the use of risk stratification methods.
Gastric biopsy sampling can be used to provide the most important information for risk classification. This led to the OLGA staging system.16 ,17 This histological staging system grades patients with gastritis into stages with corresponding gastric cancer risk. Further studies showed that this staging system provides relevant clinical information.80–82 Based on the high prevalence of atrophic gastritis in at-risk populations and the limited reproducibility and high interobserver variability in histological diagnosis of atrophic gastritis, a further proposal was made for the OLGIM system based on diagnosis and distribution of intestinal metaplasia.18
The interobserver reproducibility was improved for intestinal metaplasia compared with atrophic gastritis, and the correlation between the severities of gastritis remained at least as strong.18 Subsequent studies with both the OLGA and OLGIM systems showed a higher gastric cancer risk in patients in stage III or IV of OLGA or OLGIM.82–84 As a result, upper gastrointestinal surveillance endoscopy should be offered to patients in these subcategories.
CQ15. Are serological tests (pepsinogen I, II, I/II, H. pylori antibody) useful for risk stratification?
Statement 15
Serological tests (pepsinogen I and II and H. pylori antibody) are useful for identifying individuals at increased risk for gastric cancer. Grade of recommendation: strong
Evidence level: high
Consensus level: 91.9%
Comment
Serological tests for the diagnosis of chronic gastritis and gastric atrophy have been in use for more than 25 years. These include H. pylori serology (crude antigen with or without additional determination of anti-CagA antibodies) for the diagnosis of gastritis, and serum pepsinogen I and II and gastrin for the diagnosis of gland loss resulting in hypoacidity.85 These tests are usually applied in panels of multiple tests and have been shown to be a useful non-invasive diagnostic tool in an individual patient, and as a population screening and surveillance tool.86 ,87 A Japanese cohort of 9293 screenees underwent serological assessment by means of H. pylori serology and pepsinogen I and II measurement.86 The annual progression to gastric cancer was very low in subjects with normal pepsinogens, irrespective of H. pylori status. The annual progression to gastric cancer was substantially higher (3.5–6 per 1000 per year) in individuals with low serum pepsinogen levels, compatible with presence of atrophic gastritis.86 In the latter group, the incidence of gastric cancer was higher among those with negative H. pylori serology than among those with positive H. pylori serology, which is indicative of progressive and widespread atrophy and metaplasia impairing further H. pylori colonisation. Similar findings were obtained in other studies.88 ,89
CQ16. When is it appropriate to search and screen for H. pylori gastritis?
Statement 16
Depending on the epidemiological context, it is appropriate to search and screen for H. pylori gastritis at an age before development of atrophic gastritis and intestinal metaplasia.
Grade of recommendation: strong
Evidence level: moderate
Consensus level: 97.3%
Comment
H. pylori infection is mainly acquired in childhood, up to the age of 12 years, in developed countries mostly by intrafamilial transmission.90–92 The bacterium and associated gastritis persist lifelong, unless treated by eradication therapy, or unless end-stage widespread atrophic gastritis and intestinal metaplasia occur. The risk for gastric cancer depends on the grade of gastric atrophy and intestinal metaplasia.31 ,82–84 ,86 H. pylori eradication can reduce the risk for cancer, but this effect is largely confined to patients without atrophy and metaplasia.93–95 In patients with these lesions, H. pylori eradication reduces gastritis, but may not stop further progression to cancer. As a result, cancer can occur more than 10 years after H. pylori eradication treatment.96 Against this background, it is appropriate to search and screen for H. pylori gastritis at an age when new infections become less likely (>12 years) and before development of atrophic gastritis and intestinal metaplasia. This all depends on the geographical location and epidemiological context, taking into account the prevalence of infection and age-related cancer incidence.97
Section 4 Management of gastritis
CQ17. Should all H. pylori-positive individuals receive eradication therapy?
Statement 17
H. pylori infected individuals should be offered eradication therapy, unless there are competing considerations.
Grade of recommendation strong
Evidence level: high
Consensus level: 100%
Comment
H. pylori is a major human pathogen that causes chronic and progressive gastric mucosal damage and is aetiologically related to peptic ulcer, gastric cancer and gastric atrophy. It is also closely associated with gastric MALT lymphoma, dyspepsia, hyperplastic gastric polyps and idiopathic thrombocytopenic purpura.5 ,12 ,46 ,47 ,61 ,98–104 H. pylori-positive individuals are also the major reservoir for transmission of the infection.
The decision to eradicate a chronic infection in a society should be based on quantitative data regarding the outcome of untreated infections. H. pylori causes a chronic infection, similar, for example, to asymptomatic syphilis or tuberculosis, and the final outcome for any individual cannot be predicted.105 H. pylori infection differs from many other chronic infectious diseases because it is always transmissible, thus putting others at risk. Because the gastric damage is progressive, the lack of an obvious clinical manifestation at diagnosis has no predictive value for life-time risk to an individual patient, their family or to the community. Benefits of H. pylori eradication for an individual depend in part on the degree and extent of damage that has already occurred and the reversibility of that damage. Potential benefits of eradication include stopping the progression of mucosal damage, stabilisation or reduction in risk of developing gastric cancer, resolution of mucosal inflammation, stabilisation or improvement of gastric mucosal function, return of the normal mechanisms governing acid secretion, cure of H. pylori-related PUD, reduction in risk of gastrointestinal complications of NSAID therapy and prevention of future development of H. pylori-related peptic ulcer.2 ,5 ,11 ,28 ,46 ,47 ,106–115
For society, the benefits include reduction of the reservoir of infected individuals capable of transmitting the infection to others, and avoidance of the costs associated with diagnosis, management and outcomes of H. pylori-related diseases that are prevented. Thus, H. pylori-infected patients should be offered eradication therapy unless there are competing considerations such as comorbidities, re-infection rates in their communities, competing health priorities of society and financial cost. It has to be remembered, however, that there are concerns about the negative impact of eradication therapies on human health, such as increase in allergy or obesity and perturbation of microbiota.116 ,117
CQ18. What is the optimal timing for H. pylori eradication in asymptomatic subjects?
Statement 18
The maximum benefit of H. pylori eradication is obtained if it is done while the mucosal damage is still non-atrophic.
Grade of recommendation: strong
Evidence level: high
Consensus level: 100%
Comment
H. pylori eradication always confers a benefit by halting progression of gastric mucosal damage, reducing the reservoir of infected individuals and reducing or preventing H. pylori-associated diseases. The maximum benefit of eradication for an individual is obtained if eradication is done while the H. pylori-induced mucosal damage has not progressed beyond the non-atrophic stage. This population is found in countries where gastric cancer is still prevalent and is concentrated in the younger generation. H. pylori eradication of adolescents and young adults has an additional advantage of reducing or preventing transmission of the infection to their children.
As noted above (Section 3), the risk for development of gastric cancer correlates with the extent and severity of atrophic gastritis. It is impossible to define the risk for an individual based on age. Cancer risk in any population relates to the rate of progression of gastric mucosal damage, which is high in populations at high risk of cancer and low in H. pylori-infected populations with a low cancer risk. Thus, while it is possible to identify an average age at which the transition from non-atrophic to atrophic phenotype occurs for any population, one should expect that any age group will contain individuals with a wide range of damage, ranging from uninfected (normal) to advanced atrophy. This emphasises the need for risk stratification based on objective parameters including a validated histological staging system rather than on age, to identify whether one eradication treatment is needed or whether the patient might require surveillance.
The incidence of gastric cancer increases with age, which is a surrogate marker for the time required for progression of atrophic gastritis. When atrophic gastritis becomes extensive and severe, the risk increases exponentially. Cancer is the culmination of a multistep process of genetic instability, with cancer cells possessing mutations in coding regions, somatic gene rearrangements and epigenetic changes such as methylation. Current data are consistent with the notion that H. pylori eradication halts the progression of damage and reduces or eliminates the H. pylori-associated events that increase genetic instability in the gastric mucosa. These include infection-associated DNA double-strand breaks,118 impaired DNA mismatch repair,119 aberrant activation-induced cytidine deaminase expression, which induces nucleotide alterations involved in DNA mutations,120 aberrant methylation in a number of gene promoters in the gastric mucosa, including cell growth-related genes, DNA-repair genes, tumour-suppressor genes, the cell adherence gene E-cadherin and CpG islands of microRNA genes121–123 and aberrant microRNA expression.124 H. pylori infection also causes an inflammatory response with mucosal infiltration of acute and chronic inflammatory cells. Cancer risk is increased in relation to the ability of the infecting strain to cause inflammation (eg, those possessing the Cag pathogenicity island). However, all strains cause inflammation, and gastric cancer is associated with infections lacking putative virulence factors. Thus all H. pylori infections should be considered pathogenic and should be eradicated.
Because of the damage and premalignant changes, H. pylori eradication cannot ‘reset the clock’ to zero (ie, no risk) but can stop the progression of risk and stabilise or decrease the subsequent risk.
CQ19. Do we need to adopt eradication regimens according to the geographical area?
Statement 19
Eradication regimens should be based on the best locally effective regimen, ideally using individual susceptibility testing or community antibiotic susceptibility, or antibiotic consumption data and clinical outcome data. The agents available differ in different regions and this, in part, dictates what regimens are possible.
Grade of recommendation: strong
Evidence level: high
Consensus level: 100%
Comment
The success of a proven successful H. pylori eradication regimen depends on the pattern of resistance in the population and on the common host genotypes of drug metabolising enzymes in the population. The prevalence of H. pylori resistance to commonly used antimicrobial agents greatly varies geographically and is linked to consumption of antibiotics in the region,125 so the preferred eradication regimen often differs between regions. Ideally, treatment regimens should be chosen based on susceptibility testing. Within any region, only regimens that reliably produce eradication rates of ≥90% in that population should be used for empirical treatment.5 ,126–129
CQ20. Does eradication of H. pylori prevent gastric cancer?
Statement 20
Eradication of H. pylori reduces the risk of gastric cancer. The degree of risk reduction depends on the presence, severity and extent of atrophic damage at the time of eradication.
Grade of recommendation: strong
Evidence level: high
Consensus level: 100%
Comment
H. pylori infection is the most important cause of gastric cancer as it is estimated that 89% of non-cardia gastric cancer, representing 78% of all cases of gastric cancer, can be attributed to chronic H. pylori infection.130 Prevention of H. pylori infections removes the primary cause of gastric cancer and will thus reduce the incidence of gastric cancer in that population. The effectiveness of H. pylori eradication for prevention of gastric cancer depends on the severity and extent of atrophic damage at the time of eradication and ranges from essentially complete prevention for those with non-atrophic gastritis to stabilisation or reduction of risk in those with established atrophic changes.94 ,95 As noted in Section 3, risk can be stratified using a variety of approaches, such as one of the validated histological stratification systems (eg, OLGA or OLGIM),16–18 and H. pylori eradication can stabilise risk and halt the progression of risk.28 ,94 Prevention of acquisition of H. pylori infections and eradication of the infection before the development of atrophic changes are forms of primary prevention. Secondary prevention involves identification and surveillance of those at risk in order to remove intraepithelial lesions and early gastric cancer(s) before they become invasive.5 ,71 ,72 ,77 ,131 There may be also a role for cancer immunotherapy to treat premalignant lesions and halt their progression to more advanced lesions.132
CQ21. Should the outcome of eradication therapy always be assessed (ie, test for cure)?
Statement 21
The outcome of eradication therapy should always be assessed, preferably non-invasively.
Grade of recommendation: strong
Evidence level: high
Consensus level: 100%
Comment
Failure of eradication is common and allows the mucosal damage to progress, and so eradication should always be confirmed, preferably using a non-invasive test such as a urea breath test or a validated monoclonal-based stool antigen test.5 For patients requiring endoscopic follow-up, such as after endoscopic removal of a gastric adenoma, histological assessment can be used. Confirmation of cure also provides an early warning system for the increasing antibiotic resistance in a population that will manifest as increasing rates of treatment failure.125 ,128 ,129
CQ22. Which patients need long-term follow-up after eradication?
Statement 22
H. pylori eradication may not completely eliminate the risk of gastric cancer. Patients who remain at risk, as defined by the extent and severity of atrophy, should be offered endoscopic and histological surveillance.
Grade of recommendation: strong
Evidence level: high
Consensus level: 97.3%
Comment
Long-term follow-up such as regular endoscopic surveillance should be based on estimating the risk of developing gastric cancer after H. pylori eradication (ie, risk stratification).95 ,133 Cancer risk correlates with the extent and severity of atrophic gastritis and risk stratification should be confirmed using a validated histological risk scoring systems such as OLGA or OLGIM.16–18 In areas with proven expertise in endoscopic scoring, a system such as that of Kimura and Takemoto can be used initially, although histological confirmation is still recommended.134 ,135 Patients whose H. pylori infection was diagnosed non-invasively (eg, urea breath test or stool antigen) should be considered for histological assessment. These patients should include those within the age range in which atrophic changes are common in that population and those with a history of gastric ulcer as well as those with a pretreatment serum pepsinogen I of ≤70 ng/mL and a pepsinogen I:II ratio ≤3.136–138 All those at especially high risk, including those at risk for intraepithelial neoplasia (dysplasia) or early gastric cancer, are candidates for regular endoscopic surveillance.
Discussion
The global consensus meeting on H. pylori gastritis has set a new landmark for gastritis, which has continued to be an ill-conceived clinical entity placed between a histological picture and upper abdominal symptoms.
In spite of the fact that gastritis had been long recognised as an important clinical entity, generations of gastroenterologists have neglected the importance of treatment of this nosological entity. Rudolf Schindler described chronic gastritis as a serious disease and a precursor of gastric cancer and considered their relationship as being of outstanding importance in the fight against gastric cancer.139
The discovery of H. pylori has revolutionised the pre-existing concepts of gastritis by assigning a specific aetiology to this entity underlying PUD and gastric cancer. The majority of these serious conditions are manifestations developed on the background of chronic gastritis caused by a unique infectious agent, H. pylori. For PUD, guidelines unanimously recommend eradication as the primary treatment for those with positive H. pylori tests. However, there has been no consensus on how and when to manage individuals with H. pylori gastritis itself, which is crucial to the efficiency of gastric cancer prevention because most patients with chronic gastritis may remain asymptomatic until the appearance of severe complications. Furthermore, both gastritis and duodenitis were recognised as important causes of upper gastrointestinal bleeding,140 encouraging our attention to these conditions now that anti-thrombotic therapies are increasingly being used.
To further compromise the concept of gastritis as a significant clinical entity, the term ‘gastritis’ has historically, but wrongly, been used as a substitute for a clinical diagnosis of FD. Historical studies, however, failed to demonstrate a significant association between histological findings of gastritis and the dyspeptic symptom complex.141 ,142 Hence, a potential pathogenetic role for H. pylori in causing dyspeptic symptoms was initially considered doubtful and its eradication in FD controversial.143 ,144 Meta-analysis of a large number of controlled trials with longer follow-up confirmed that eradication of H. pylori in patients with FD conveys a small but statistically significant benefit.12 Consequently, dyspepsia attributable to H. pylori gastritis involves an underlying organic cause and should be excluded from the FD category. Additionally, ‘dyspeptic’ patients should not automatically be labelled as having ‘gastritis’ without any histological confirmation.
Diagnostic assessment of gastritis has been advanced by the recent introduction of high-resolution endoscopy with image-enhanced modalities, and magnification is now used routinely in major hospitals in Japan. This endoscopic technology allows the identification of mucosal changes (for targeted biopsies) more precisely, leading to more accurate evaluation of cancer risks such as preneoplastic changes. Wider use of this new endoscopic system outside Japan may be limited at present.
The Kyoto consensus meeting focused attention on gastritis in all its clinical expression and dealt with four main topics: classification of gastritis in relation to ongoing ICD revision, FD and H. pylori infection, diagnosis of gastritis and the management of gastritis. The methodology of the meeting adopted all modern means for reaching consensus and included an internet-based Delphi method with full access to published data in a completely ‘neutral’ environment.
In summary, The Kyoto meeting proposed an aetiology-based classification for gastritis and concluded that H. pylori gastritis is an infectious disease. As such, H. pylori gastritis requires treatment whether or not it is associated with symptoms because it represents a condition that may evolve towards serious complications, including peptic ulcer and gastric neoplasia.
Consensus was reached on the existence of a separate category of patients with dyspeptic symptoms that are due to H. pylori gastritis. In these patients, eradication therapy is the recommended first-line treatment. Because of the diagnostic problems related to ‘gastritis’, these patients should be labelled as having H. pylori-associated dyspepsia and are identified by sustained dyspeptic symptom relief after eradication.
For the diagnosis of gastritis, it was agreed that risk stratification systems such as OLGA and OLGIM are useful as are the serological markers. In view of recent technological advancements, image-enhanced endoscopy should be encouraged for identifying mucosal changes which carry a high risk of developing into gastric neoplasia. Finally, it was recommended that early eradication therapy, ideally before preneoplastic changes occur, should be undertaken. However, the feasibility of implementing this strategy should be regionally tailored. As eradication therapy does not guarantee elimination of the risk of gastric cancer, follow-up should be considered for patients who have preneoplastic conditions.
Although there are still many remaining areas to be discussed, we believe the outcome of the Kyoto consensus meeting presented in this report will improve patient care and will provide a cornerstone for further refinement and research in the area of gastritis.
Acknowledgments
We thank the Japanese Society of Gastroenterology (JSGE) for providing financial support, enabling this global consensus meeting. Technical support by Omura Publishing Co Ltd and Mr Osamu Iimura of the JSGE is greatly appreciated. We also thank Japan Convention Service Co Ltd for their excellent management of the conference.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
- Data supplement 3 - Online table 3
Footnotes
Correction notice This article has been corrected since it published Online First. Hidekazu Suzuki has been added to the collaborators list.
Collaborators List of faculty members and affiliations (alphabetical order of family names): Takeshi Azuma, Department of Gastroenterology, Kobe University; Franco Bazzoli, Department of Gastroenterology, University of Bologna; Francis Ka-Leung Chan, Department of Medicine and Therapeutics, The Chinese University of Hong Kong; Minhu Chen, Department of Gastroenterology, The first affiliated hospital, SunYat-sen University; Naoki Chiba, McMaster University; Tsutomu Chiba, Department of Gastroenterology, Kyoto University; Luiz Gonzaga Vas Coelho, Department of Internal Medicine, Faculty of Medicine, Federal University of Minas Gerais; Francesco Di Mario, Department of Clinical Experimental Medicine, University of Parma; Kwong Ming Fock, Department of Gastroenterology, Changi General Hospital; Yasuhiro Fukuda, Sasayama Medical Center, Hyogo College of Medicine; Takahisa Furuta, Center for Clinical Research, Hamamatsu University School of Medicine; Robert Maximilian Genta, Department of Pathology, Miraca Life Sciences Research Institute and University of Texas Southwestern; Khean-Lee Goh, Division of Gastroenterology and Hepatology, Department of Medicine, University of Malaya; Masanori Ito, Department of Gastroenterology and Metabolism, Hiroshima University, Tomonori Kamada, Department of Internal Medicine, Kawasaki Medical School; Peter Harry Katelaris, Department of Gastroenterology, Concord Hospital, University of Sidney; Mototsugu Kato, Division of Endoscopy, Hokkaido University Hospital; Takashi Kawai, Endoscopy Center, Tokyo Medical University Hospital; Nayoung Kim, Department of Internal Medicine, Seoul National University Bundang Hospital; Ryuji Kushima, Department of Pathology, Shiga University of Medical Science; Varocha Mahachai, Division of Gastroenterology, Chulalongkorn University Hospital; Takeshi Matsuhisa, Nippon Medical School Tama Nagayama Hospital; Francis Mégraud, INSERM U853 and Department of Bacteriology; Hiroto Miwa, Department of Gastroenterology, Hyogo College of Medicine; Kazunari Murakami, Department of Gastroenterology, Oita University; Colm Antoine O'Morain, Faculty of Health Sciences, Trinity College; Massimo Rugge, Department of Pathology, Padova University; Kiichi Sato, International University of Health and Welfare; Tadashi Shimoyama, Department of Gastroenterology and Hepatology, Hirosaki University; Akiko Shiotani, Department of Internal Medicine, Kawasaki Medical College; Toshiro Sugiyama, Department of Internal Medicine, Toyama University; Hidekazu Suzuki, Department of Gastroenterology, Keio University; Kazuyoshi Yagi, Department of Medicine, Niigata Prefectural Yoshida Hospital; Ming-Shiang Wu, Department of Internal Medicine, National Taiwan University.
Contributors KS, NU, EME-O and PM planned the meeting and prepared the clinical questions. KS, JT, EJK, EME-O, DYG and PM wrote the manuscipt. SM, KH and MA helped to summarise the voting results of sections 1, 3 and 4, respectively. All other faculty members contributed to formulating one or two statements for each clinical question, participated in the meeting and voted. They also read and approved the manuscript.
Competing interests KS has received research grants from Eisai, Daiichi Sankyo and Takeda. He has also received lecture fees from Astellas, Fuji Film and Takeda. JT has provided scientific advice to AlfaWassermann, Almirall, AstraZeneca, Danone, GI Dynamics, GlaxoSmithKline, Ironwood, Janssen, Menarini, Novartis, Rhythm, Shire, Sucampo, Takeda, Theravance, Tsumura, Will-Pharma, Yuhan and Zeria. He has also served on speaker bureaus for Abbott, Almirall, AstraZeneca, Danone, Janssen, Menarini, MMS, Novartis, Shire, Takeda and Zeria. He has received research grants from Novartis, Shire and Zeria. DYG is a consultant for RedHill Biopharma and has received research support. He is also a consultant for Otsuka Pharmaceuticals and for BioGaia. KH has received lecture fees from Astellas, AstraZeneca, Daiich Sankyo, Dainippon Sumitomo, Eisai, Otsuka, Takeda and Zeria. He has also received research funds from Astellas, Daiichi Sankyo, Eisai and Takeda. MA belongs to the department funded by Eizai Co Ltd at Hokkaido University Graduate School of Medicine. NU has received lecture fees from Astellas, AstraZeneca, Eisai and Takeda. PM has received speaker's fee from Abbvie, Aptalis, AstraZeneca and Takeda.
Provenance and peer review Not commissioned; externally peer reviewed.