Article Text

Abstract
Objective Several genetic risk factors have been identified for non-alcoholic chronic pancreatitis (NACP). A genome-wide association study reported an association of chronic pancreatitis (CP) with variants in PRSS1–PRSS2 (rs10273639; near the gene encoding cationic trypsinogen) and CLDN2–MORC4 loci (rs7057398 in RIPPLY1 and rs12688220 in MORC4). We aimed to refine these findings in a large European cohort.
Design We studied 3062 patients with alcohol-related CP (ACP) or NACP and 5107 controls. Also, 1559 German patients with alcohol-associated cirrhosis or alcohol dependence were included for comparison. We performed several meta-analyses to examine genotype–phenotype relationships.
Results Association with ACP was found for rs10273639 (OR, 0.63; 95% CI 0.55 to 0.72). ACP was also associated with variants rs7057398 and rs12688220 in men (OR, 2.26; 95% CI 1.94 to 2.63 and OR, 2.66; 95% CI 2.21 to 3.21, respectively) and in women (OR, 1.57; 95% CI 1.14 to 2.18 and OR 1.71; 95% CI 1.41 to 2.07, respectively). Similar results were obtained when German patients with ACP were compared with those with alcohol-associated cirrhosis or alcohol dependence. In the overall population of patients with NACP, association with rs10273639 was absent (OR, 0.93; 95% CI 0.79 to 1.01), whereas rs7057398 of the X chromosomal single nucleotide polymorphisms was associated with NACP in women only (OR, 1.32; 95% CI 1.15 to 1.51).
Conclusions The single-nucleotide polymorphisms rs10273639 at the PRSS1–PRSS2 locus and rs7057398 and rs12688220 at the CLDN2–MORC4 locus are associated with CP and strongly associate with ACP, but only rs7057398 with NACP in female patients.
- CHRONIC PANCREATITIS
- GENETIC POLYMORPHISMS
- PANCREATITIS
- TRYPSINOGEN
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Genetic associations for non-alcoholic chronic pancreatitis (NACP) in PRSS1, PRSS2, CFTR, SPINK1, CTRC and CPA1, as well as a gene-dosage effect of PRSS1-PRSS2 locus have been identified.
Alcohol misuse is the predominant cause of chronic pancreatitis (CP); however, only 3%–5% of alcohol misusers develop the disease. This implicates genetic susceptibility factors, which have not been elucidated so far.
A recent genome-wide association study (GWAS) reported PRSS1–PRSS2 and CLDN2–MORC4 locus variants that affect risk for CP, and the data have not been replicated up to now.
What are the new findings?
This study in a large European cohort replicates and refines the impact of PRSS1-PRSS2 and CLDN2-MORC4 locus variants as susceptibility factors predominantly in ACP.
Variants at both loci are susceptibility factors for ACP and not alcohol misuse per se according to our comparison with alcohol-dependent and patients with alcoholic liver cirrhosis.
Risk increase for the X chromosomal CLDN2-MORC4 locus is comparable in men and women. As such this factor does not explain any sex differences in disease susceptibility.
How might it impact on clinical practice in the foreseeable future?
The replication and refinement of the recently identified susceptibility variants justifies further studies on their functional properties.
By the identification of new pathways, new strategies for influencing the clinical picture of NACP and ACP might be developed in the long term.
Introduction
The genetic susceptibility to chronic pancreatitis (CP) is best illustrated by the discovery of cationic trypsinogen mutations (PRSS1 HGNC:9475) in families with autosomal-dominant inherited pancreatitis.1 There is also strong evidence that genetic variants contribute to cases of CP without a clear inheritance pattern. Indeed, idiopathic CP (ICP) is associated with genetic alterations in CFTR (HGNC:1884), SPINK1 (HGNC:11244), PRSS2 (HGNC:9483), CTRC (HGNC:2523) and CPA1 (HGNC:2296).2–7 The association of genetic variants and disease susceptibility is less clear for alcohol-related CP (ACP). There is a low enrichment of SPINK1 (p.N34S) and CTRC (p.R254W) alleles in ACP populations, and no other consistent genetic risk contributors have been described.5 ,8 Similar to ICP, the PRSS2 p.G191R variant protects against ACP development.2 All these associations have been discovered through candidate-driven genetic association studies.
A recent paper described a different approach and reported novel risk and protecting loci for CP identified through a genome-wide association study (GWAS). A number of variants in the PRSS1–PRSS2 but also the CLDN2–MORC4 locus (Claudin 2; HGNC:2041; RIPPLY1, ripply transcriptional repressor 1, HGNC:25117; MORC4, MORC family CW-type zinc finger 4, HGNC:23485) were captured as risk factors for CP.9 This study investigated patients with different types of CP as well as recurrent acute pancreatitis (RAP) and stratified individuals into alcohol-related and alcohol-unrelated pancreatitis groups. In a first screening cohort, three single nucleotide polymorphisms (SNPs) rs10273639 (in the PRSS1–PRSS2 locus on chromosome 7, in perfect linkage disequilibrium with rs2011216 in intron 1 and rs6667 in exon 5 of PRSS1), rs7057398 and rs12688220 (both in a new locus, CLDN2–MORC4 on the X chromosome) reached genome-wide significance. After scrutiny, the PRSS1–PRSS2 rs10273639 T allele appeared to protect against CP, whereas RIPPLY1 rs7057398 C allele and MORC4 rs12688220 T allele increased disease susceptibility.9 There is some biological plausibility for the association with the PRSS1–PRSS2 locus as it may disturb the balance of pancreatic proteases and antiproteases in favour of the former.10 ,11 Claudin 2 represents a tight junction protein involved in low-resistance cation-selective ion and water transport between endothelial cells.12 ,13 One might speculate that CLDN2–MORC4 locus variants lead to miss-localisation of pancreatic CLDN2 that hampers its biological function. However, this speculation warrants further experimental support.
Prior to the design of experimental studies that focus on the biological role of these variants, it is crucial that GWAS results are replicated. This is needed to prove that results are valid and reliable to determine generalisability and to better judge the effect size of the discovered association.14 We investigated the association of PRSS1–PRSS2 and CLDN2–MORC4 locus variants in a large European cohort of ACP and non-alcoholic CP (NACP) to confirm the former finding. In order to assess the effect of alcohol consumption, we further refined our analyses by including cohorts of patients with alcohol-associated cirrhosis (ALC) as well as with alcohol dependence (AD) without hepatic or pancreatic disease.
Materials and methods
Study subjects
The respective medical ethical review committees of all participating centres approved the study protocol and all patients gave written informed consent. The diagnosis of CP was based on two or more of the following findings: (a) presence of a typical history of recurrent pancreatitis or (b) recurrent abdominal pain typical for CP, (c) calcifications and/or (d) pancreatic ductal irregularities revealed by imaging of the pancreas.15 ACP was diagnosed in patients who had consumed at least 80 g ethanol per day for at least 2 years in men or 60 g per day for women. We labelled patients with NACP in the absence of exogenous factors such as alcohol.
ALC was diagnosed by a history of habitual ethanol intake (see ACP diagnosis above, duration at least 10 years), typical findings in liver biopsy or clinical and laboratory findings indicative for liver disease. Such laboratory and clinical findings included abnormal levels of aminotransferases, gamma glutamyl transpeptidase, coagulation tests, serum albumin concentration, platelet count, complications related to liver cirrhosis such as oesophageal varices, ascites, hepatic encephalopathy and typical liver morphology in imaging studies. Other aetiologies of liver cirrhosis were excluded by standard laboratory tests.
Patients with AD were recruited from psychiatric and addiction medicine departments in different cities across southern and central Germany. AD was diagnosed per DSM-IV criteria by consensus of two clinical psychiatrists. All patients were of self-reported German ancestry and did not suffer from CP or ALC.16
The study included 1866 patients (male, n=1567) with ACP and 1196 patients (male, n=596) with NACP from different European countries. In addition, we enrolled 5107 controls (male, n=2287), 661 German patients with ALC (male, n=480) and 898 Germans with AD (male, n=797). Characteristics of the patients and controls are summarised in table 1. More details of the controls are summarised in online supplementary table S1.
Characteristics of patients and controls
Genotyping
Details of the methods used for genotyping are summarised in the online supplementary material. As quality controls, 3% of all samples were genotyped in duplicates blinded to the investigator. The concordance rate was >98%. Call rates for rs10273639, rs7057398 and rs12688220 in the European samples were 99.1% (9641/9730), 99% (9636/9730) and 98.8% (9609/9730), respectively.
Statistical analysis
Quality of SNP genotypes was assessed by study-wise call rate and exact test for Hardy–Weinberg equilibrium in controls (female controls only for the X chromosomal SNPs). We also calculated overall statistics and performed stratified tests of Hardy–Weinberg equilibrium according to Troendle and Yu.17 According to these measures, genotype qualities were excellent throughout. Study-wise genetic effects were determined by logistic regression analysis assuming an additive model of inheritance. For X chromosomal SNPs, we analysed the subgroups of men and women separately. Following the approach of Loley et al,18 we also determined combined effects by either assuming a model of complete X inactivation (XIA) or no X inactivation (nXIA) at all. The major purpose of our study is to compare allele frequencies of risk variants between different subgroups of patients (ACP, NACP) and controls (healthy, alcohol dependent, patients with cirrhosis). Corresponding contrasts of interest are listed in online supplementary table S2. Study-wise effects were pooled by standard meta-analysis techniques as implemented in the package ‘meta’ of the statistical software ‘R 3.0.1’ (ww.r-project.org). Heterogeneity between studies was assessed using Q-statistics. Due to occasionally observed study heterogeneity, we calculated random-effect models throughout. For the purpose of model diagnostics, we analysed and compared likelihoods of XIA, nXIA and sex interaction. In figures 1, 2A, B, 3, 4A, B and 5, we present forest plots of our meta-analysis results as well as other features. Finally, we performed a stratified analysis regarding age of onset in the German population. Forest plots were generated using GraphPad Prism (V.6.0a) (San Diego). p Values <0.05 were considered statistically significant. Online supplementary figures S1a, b and S2a, b display the results of X chromosomal analysis assuming models of complete or no X inactivation.
Results
PRSS1–PRSS2 locus (rs10273639)
In meta-analysis, rs10273639 showed the strongest association with ACP (OR 0.63, 95% CI 0.55 to 0.72, p value 8.5×10−11). No association was observed for NACP (OR 0.93, 95% CI 0.79 to 1.08, p value 0.3). An association was also observed for the comparison between German patients with ACP and patients with ALC (OR 0.58, 95% CI 0.50 to 0.66, p value 2.6×10−12). The association was also found in comparison of German patients with ACP with German patients with AD (OR 0.55, 95% CI 0.47 to 0.63, p value 2.3×10−16). Similar frequencies of the SNP were observed in AD, ALC and healthy controls.
For patients with ACP coming from individual European countries, an association was apparent for Germany, France, the Netherlands, Hungary, Italy, Romania and the UK (Germany OR 0.59, 95% CI 0.52 to 0.66, p value 2.9×10−19; France OR 0.64, 95% CI 0.47 to 0.88, p value 0.007; the Netherlands OR 0.56, 95% CI 0.43 to 0.72, p value 6.3×10−6; Hungary OR 0.43, 95% CI 0.18 to 0.94, p value 0.04; Italy OR 0.77, 95% CI 0.60 to 0.97, p value 0.03; Romania OR 0.41, 95% CI 0.23 to 0.69, p value 0.001; the UK OR 0.53, 95% CI 0.30 to 0.91, p value 0.02). The logistic regression and meta-analysis results of rs10273639 are summarised in figure 1, while the genotype frequencies for the groups are given in online supplementary tables S3 and S4. The TT genotype was underrepresented in all European patients with ACP (all patients 9.5% vs all controls 18.1%, p value 9.6×10−33, except for the samples from Poland (12.9% patients vs 12.4% controls, p value 0.99)). In the NACP cohorts, this underrepresentation was found only in German patients (patients 13.8% vs controls 17.9%, p value 0.01).
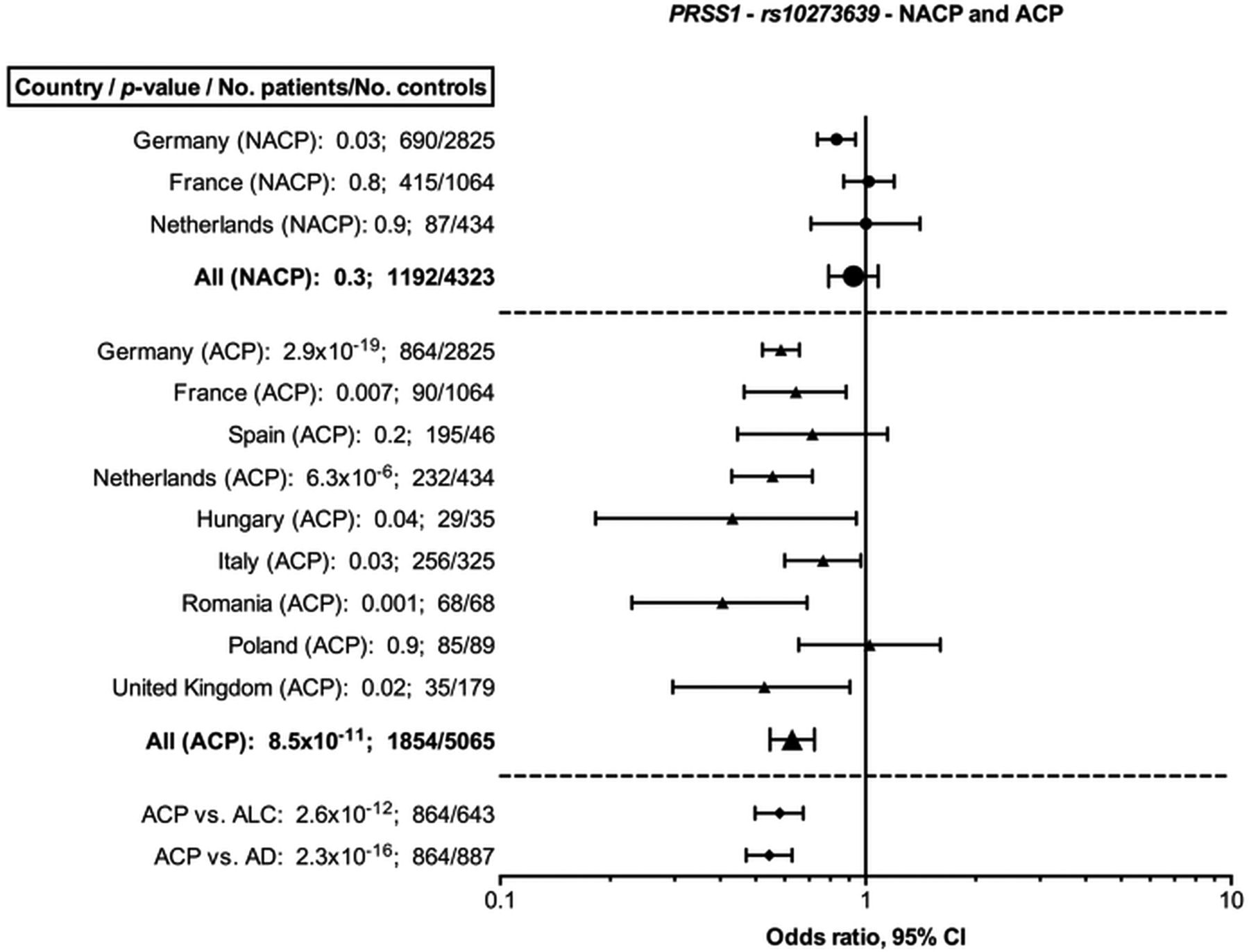
Meta-analysis results for rs10273639 (PRSS1–PRSS2) in patients with non-alcoholic chronic pancreatitis (NACP), alcohol-related chronic pancreatitis (ACP) and comparison of German ACP patients with alcohol-associated cirrhosis (ALC) and with alcohol-dependent (AD) patients. Results are presented in a semi-log scale.
RIPPLY1 (rs7057398)
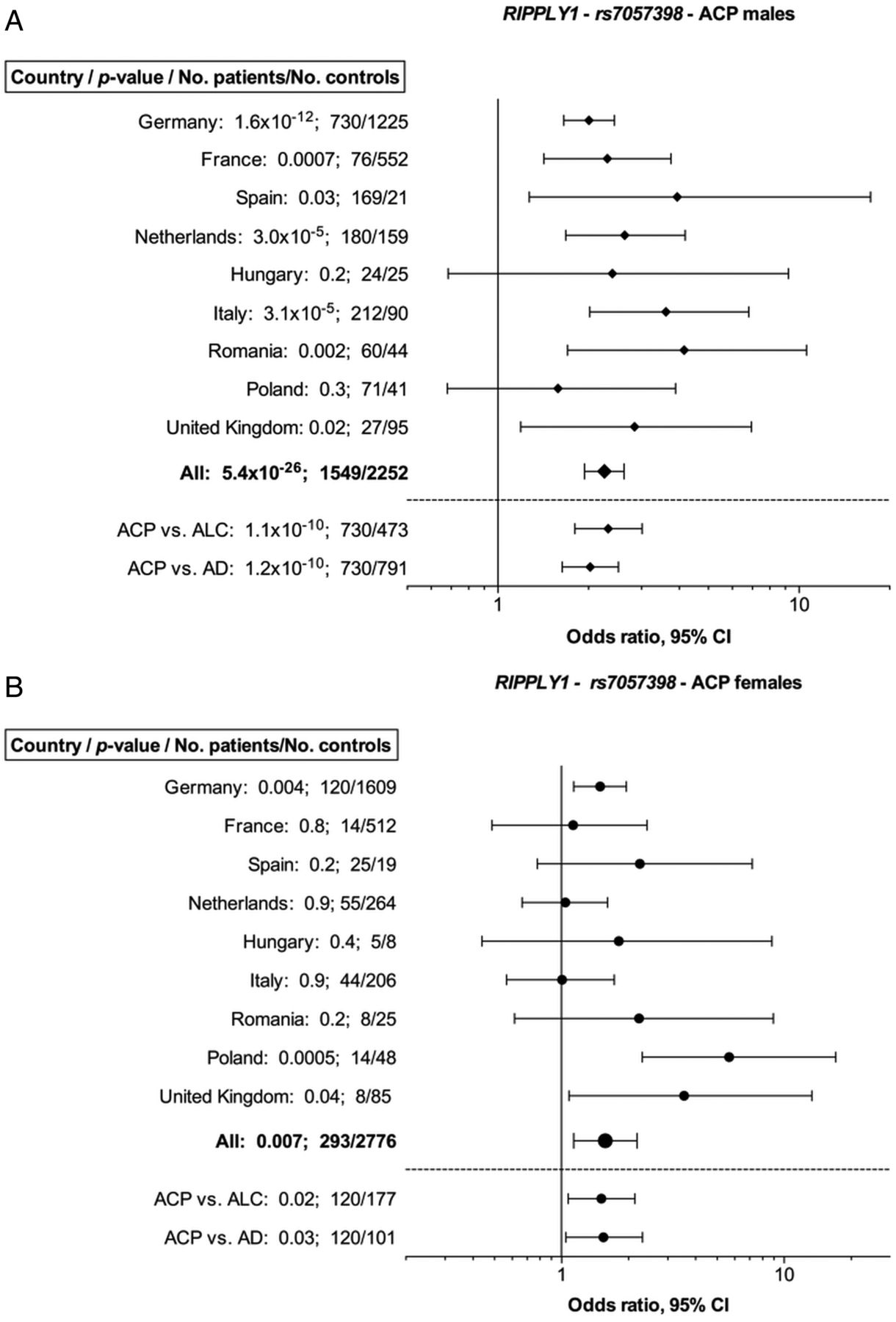
In meta-analysis, significant associations were found for rs7057398 in male patients with ACP (OR 2.26, 95% CI 1.94 to 2.63, p value 5.4×10−26) and in female patients (OR 1.57, 95% CI 1.14 to 2.18, p value 0.007). Upon stratification by countries, we detected a significant association with male patients with ACP originating from Germany, France, Spain, the Netherlands, Italy, Romania and the UK (p values 1.6×10−12, 0.0007, 0.03, 3.0×10−5, 3.1×10−5, 0.002 and 0.02, respectively). We obtained similar results for female patients with ACP from Germany, Poland and the UK (p value 0.004, 0.0005 and 0.04). We then assessed the strength of the association by comparison of the results obtained from patients with ALC and AD. Indeed, rs7057398 was overrepresented in ACP relative to other alcohol-related disorders. This was especially apparent for the cohort of male German patients with ACP in comparison with ALC (OR 2.32, 95% CI 1.80 to 3.01, p value 1.1×10−10) as well as with AD (OR 2.03, 95% CI 1.64 to 2.51, p value 1.2×10−10). In addition, the SNP is not associated with risk of cirrhosis or AD, neither for men nor for women. Figure 2A, B summarises the results of the meta-analysis of rs7057398 in patients with ACP. Results of XiA and nXiA are summarised in online supplementary figure S1a, b.

(A and B) Meta-analysis results for rs7057398 (RIPPLY1) in patients with alcohol-related chronic pancreatitis (ACP) and comparison of German ACP patients with alcohol-associated cirrhosis (ALC) and with alcohol-dependent (AD) patients. Results are presented in a semi-log scale.
The genotype and allele frequencies of rs7057398 in patients with ACP are presented in online supplementary tables S5 and S6. The C allele was more frequent in male patients with ACP from all European countries investigated (43.8% vs controls 27.5%, p value 10×10−25) and the C allele was significantly overrepresented (p value 0.0001) in female patients with ACP (35.2%) compared with controls (27.3%).
We detected a significant association for rs7057398 with NACP upon logistic regression in female patients (OR 1.30, 95% CI 1.14 to 1.49, p value 1.3×10−4), but not in male patients (figure 3). Estimated genetic effect sizes are always smaller than for ACP. As shown in Supplementary tables S7 and S8, the C allele was slightly overrepresented in male patients with NACP (all patients: 32.6% vs 28.3%, p value 0.04; German patients: 33.3% vs 27.1%, p value 0.03). Subgroup analyses revealed that in German women and in the overall female patients with NACP there was an overrepresentation of CC genotype (patients 10.1% vs controls 7.8%, p value 2.6×10−4; patients 10.3% vs controls 8.6%, p value 4.2×10−5).

Meta-analysis results for rs7057398 (RIPPLY1) in patients with non-alcoholic chronic pancreatitis (NACP). Results are presented in a semi-log scale. Y-axis intersects x-axis at 1.
MORC4 (rs12688220)
Similar to the results obtained for rs7057398 in ACP, rs12688220 was significantly associated in male (OR 2.66, 95% CI 2.21 to 3.21, p value 1.1×10−24) and female patients (OR 1.71, 95% CI 1.41 to 2.07, p value 3.3×10−8) with ACP (figure 4A, B). The association was also statistically significant in individual male cohorts from Germany, France, Spain, the Netherlands, Italy and Romania (p value 1.2×10−16, 8.4×10−6, 0.02, 2.5×10−6, 5.4×10−6 and 0.001, respectively), as well as in the female cohorts from Germany, Poland and the UK (p value 0.0003, 0.003 and 0.03). Results of XiA and nXiA are summarised in online supplementary figure S2a, b.
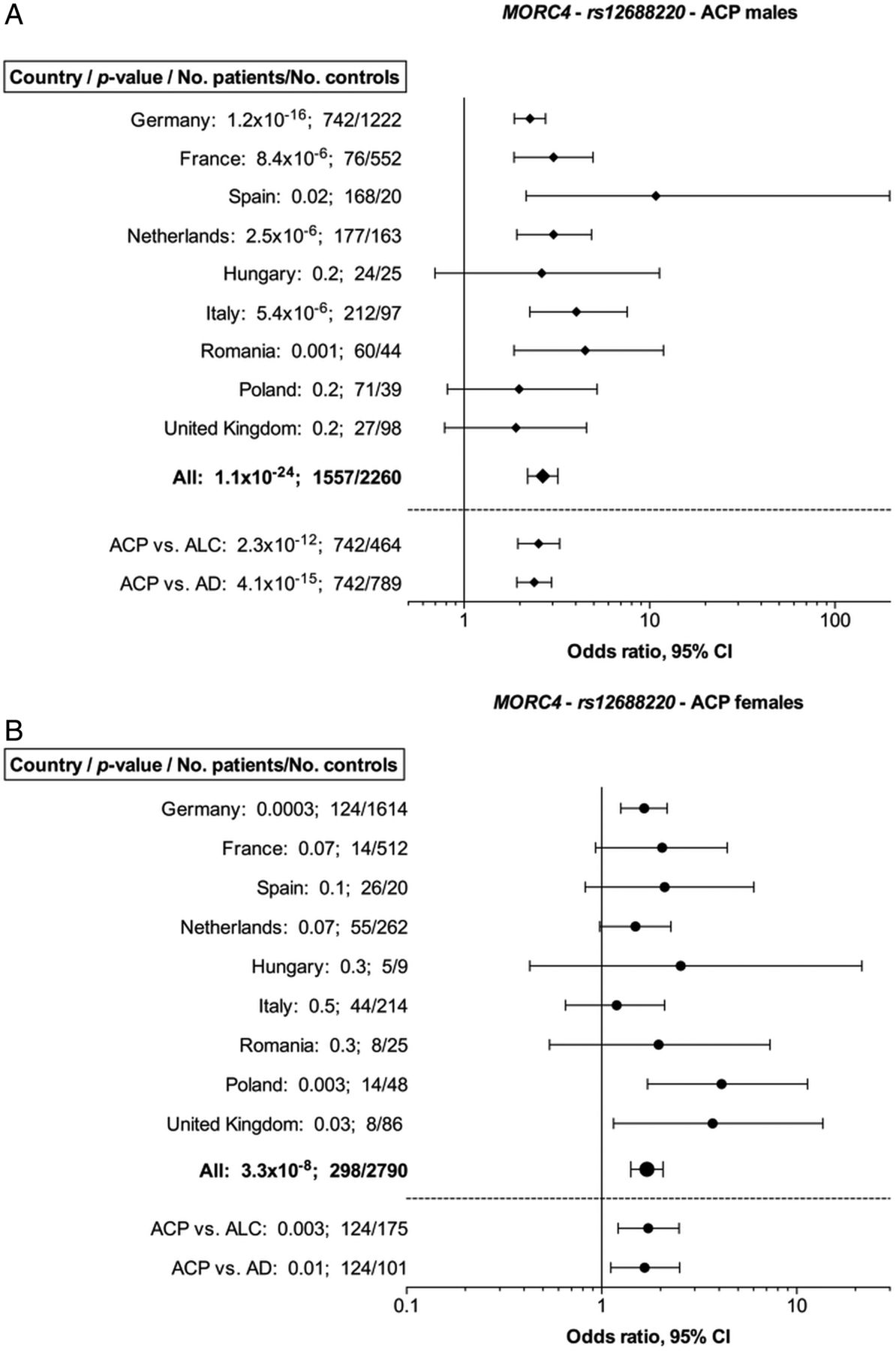
(A and B) Meta-analysis results for rs12688220 (MORC4) in patients with alcohol-related chronic pancreatitis (ACP) and comparison of German ACP patients with alcohol-associated cirrhosis (ALC) and with alcohol-dependent (AD) patients. Results are presented in a semi-log scale.
Online supplementary tables S9 and S10 summarise the genotype and allele distribution of rs12688220 in ACP. The T allele was overrepresented in all European male cohorts (men: all patients 43.9% vs all controls 25.1%, p value 4.6×10−33), while in female ACP cohorts from Germany, Poland and the UK as well as in the overall female group the overrepresentation of the TT genotype was statistically significant (women: all patients 10.4% vs all controls 6.7%, p value 2.4×10−7).
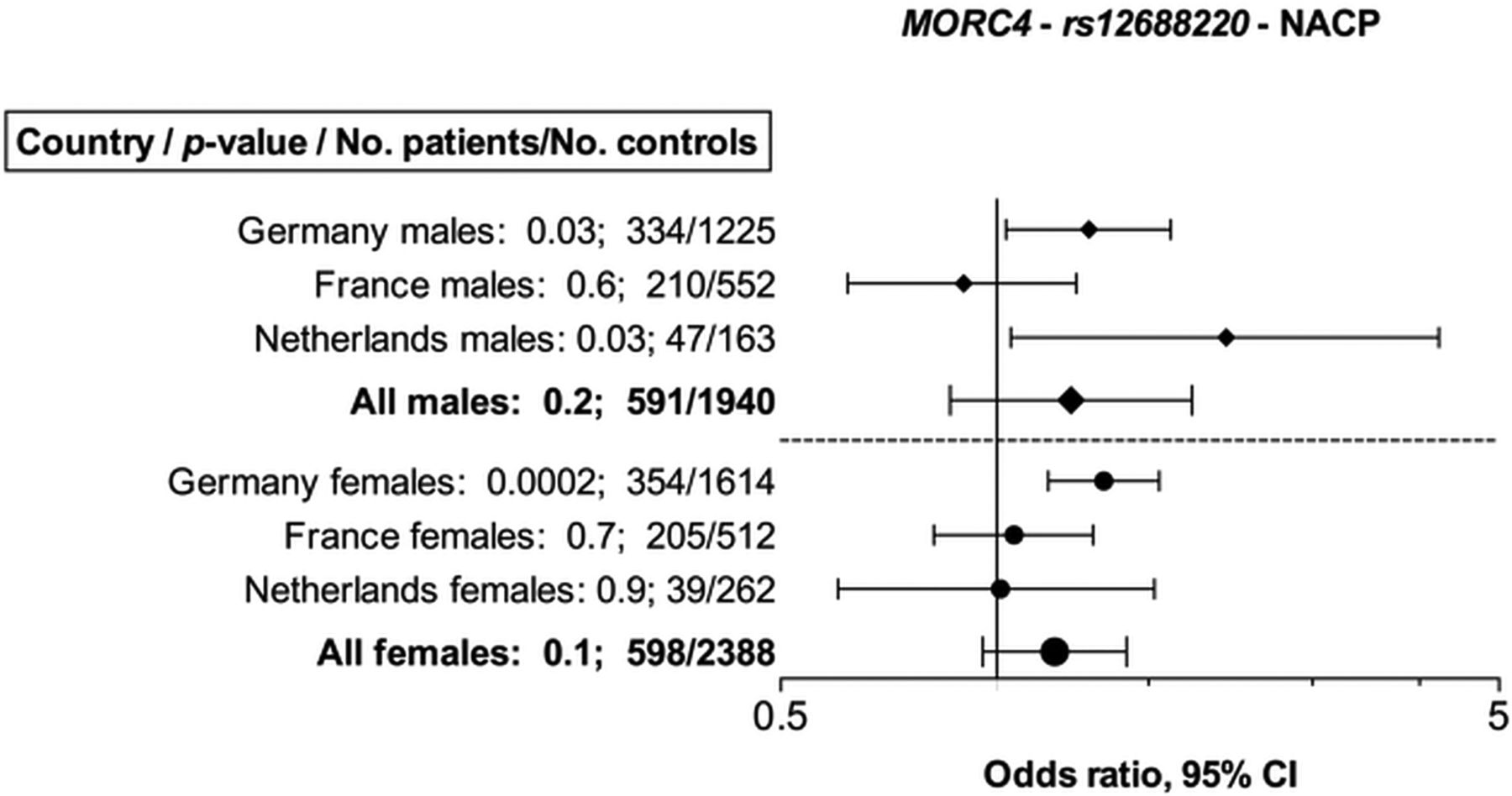
In the meta-analysis, we detected no significant association in the overall male and female NACP group (p value 0.2 and 0.1). Again, genetic effect sizes are clearly smaller than for ACP. In single-study analyses, significant differences were found in the German NACP female group (OR 1.41, 95% CI 1.18 to 1.68, p value 0.0002) and in the male NACP groups from Germany (OR 1.34, 95% CI 1.03 to 1.75, p value 0.03) and the Netherlands (OR 2.09, 95% CI 1.05 to 4.12, p value 0.03) (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analysis results for rs12688220 (MORC4) in patients with non-alcoholic chronic pancreatitis (NACP). Results are presented in a semi-log scale. Y-axis intersects x-axis at 1.
Again, no differences were observed between the three control groups. Genotype and allele distributions of this variant can be found in online supplementary tables S11 and S12.
Additional analyses
We pooled our cases and control groups in order to compare our results with the analysis published by Whitcomb et al. Results are summarised in online supplementary table S13 for all SNPs. Strong associations were observed for all variants, that is, the results of Whitcomb et al are clearly replicated.
To analyse whether effect sizes of X chromosomal variants are different between male and female patients, we performed sex-interaction analysis but interaction terms were not significant throughout (results not shown). We also compared the models of XIA and nXIA and observed a non-significant trend that XIA is more likely.
Finally, in order to better understand the lack of associations for NACP, we performed a stratified analysis of the German cohort regarding age of onset. Interestingly, we observed a trend towards higher genetic effect sizes in groups of later age of onset. This could explain, for example, the lack of associations in the French cohort in which the age range is 1–20 years (see online supplementary table S14).
Discussion
This case–control study replicates and refines a robust association between a PRSS1–PRSS2 locus variant (rs10273639) and CP. This is particularly strong in ACP and not apparent in NACP. The effect is independent from alcohol consumption as the difference in allele frequency remained upon comparison with other alcohol-related disorders (ALC and AD). The risk reduction by rs10273639 was higher in our overall ACP cohort (OR 0.63, CI 0.55 to 0.72) compared with the overall GWAS data (OR 0.73, seOR 0.029), which might be explained by the mixture of different aetiologies of patients with CP and RAP in the recent publication.9 When using a comparable analysis strategy, similar results were obtained (see online supplementary table S13; OR 0.71, CI 0.61 to 0.84). Thus, the T allele confers protection against the development of ACP, but not against NACP. The protective effect of the T allele was observed for all single studies except for the samples from Poland. Genetic effect sizes vary between OR=0.41 (Romania) to OR=1.0 (Poland). However, this can be explained by small sample sizes rather than ethnic differences.
What is the biological background of our findings? The PRSS1–PRSS2 locus SNP rs10273639 (c.−408T>C) is located 408 nucleotides upstream of the ATG start codon of PRSS1 and as such might influence PRSS1 expression. Indeed, the SNP seems to correlate with PRSS1 mRNA levels in 69 pancreas tissue samples pointing towards its role in the regulation of PRSS1 expression.9 Trypsinogen expression was lowest in TT genotypes, which suggests that this genotype might protect against pancreatitis development. However, the normalised gene expression data from pancreatic tissue had high SEs and a p value of 0.01 after removal of two outliers and, therefore, probably warrant further evidence to support this assumption.9 In addition, SNPs rs2011216 and rs6667 were found to be in linkage disequilibrium with rs10273639 and as such the biological effect might be related to those or even other SNPs.
We obtained similar results for the CLDN2–MORC4 locus SNPs. We discovered that an association of both the RIPPLY1 and the MORC4 SNP with ACP was present in men and in women. Genetic effect sizes in men were somewhat higher than in women (OR=2.66 compared with OR=1.71 for MORC4 and OR=2.27 compared with OR=1.56 for RIPPLY1), but no significant SNP–sex interactions were found. The associations with NACP were weaker throughout and not significant except for the RIPPLY1 variant in female patients.
In older epidemiological studies, it was shown that women developed ACP at an earlier age and after consumption of a lower total amount of alcohol than men.19 ,20 It is a matter of debate whether genetic effects at chromosome X can explain this observation. However, in our study, the genetic effect sizes of men and women were not significantly different for the variants considered. Moreover, by comparing models with and without assuming X inactivation, we did not receive a clear preference towards one of these assumptions. In view of these results, the X chromosomal CLDN2-MORC4 locus variants do not even partly explain the higher ACP risk in men.
The role of CLDN2/RIPPLY1/MORC4 in pancreatitis is less clear. As a tight junction protein CLDN2 is involved in low-resistance cation-selective ion and water transport between endothelial cells.12 ,13 The functional consequence of each investigated SNP is rather unclear so far. The recent paper proposed an atypical localisation of CLDN2 in acinar cells and an increase of CLDN2 expression in one investigated CP pancreas specimen (cDNA expression level) as well as in Western blot analyses from 19 pancreas specimens with different genotypes. Both for MORC4 and RIPPLY1 as well as for TBC1D8B, another gene within the CLDN2 locus, the recent paper proposed no relevance for CP development.
For the X chromosomal variants, the effect sizes were smaller in a recently published GWAS.9 Again, this can be explained by the markedly observed stronger genetic effect sizes of ACP compared with NACP.
The aetiology of AD involves environmental and genetic factors. Its heritability is estimated at ∼50%.21 Since patients with ACP were compared with controls without defined alcohol consumption in our study as well as in the published GWAS, the described SNPs might represent markers for alcoholism and not for ACP. However, when data of patients with ACP were compared with patients with alcohol-associated liver cirrhosis and alcohol dependence in our study, the association of all investigated SNPs was replicated with similar effect sizes. Therefore, we conclude that the association of the three SNPs is specific for ACP and is unrelated to AD or alcohol-related liver disease.
In summary, our data refine the results of the recently published GWAS. The PRSS1–PRSS2 rs10273639 T allele protects against development of ACP but not NACP. The X chromosomal RIPPLY1 and MORC4 SNPs showed strong association with ACP. For NACP, the associations are weaker and only significant for the RIPPLY1 SNP in women. The variants are not associated with the risk of AD or liver cirrhosis. The observed differences in SNP effects between ACP and NACP could be due to interactions of variants with alcohol consumption, which would amplify the risk, or they could result from differences in the pathophysiology of the two forms of CP. These hypotheses warrant future functional investigations.
Acknowledgments
The authors thank all individuals who have participated in this study. We also thank Knut Krohn, Kathleen Schön and Birgit Oelzner (IZKF core unit DNA technologies, Leipzig) for excellent technical assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
↵*Members of the PanEuropean Working group on Alcoholic Chronic Pancreatitis.
†Names and affiliations of the rest of the co-authors are listed at the end of the manuscript.
MHD, PK, MS, EM, CF, JPHD and HW contributed equally.
Correction notice The order of the author list in HTML version has been corrected since published Online First. The structure of the author list in PDF version is slightly different from the online version but this difference does not affect the content of this paper.
Further authors list Hana Algül,13 Thomas Berg,14 Hans Bödeker,15 Matthias Blüher,2 Marco J Bruno,16 Stephan Buch,17 Peter Bugert,18 Halina Cichoz-Lach,19 Andrzej Dabrowski,20 Antoni Farré,21 Josef Frank,22 Anita Gasiorowska,23 Andrea Geisz,24 Elisabetta Goni,11 Johannes Grothaus,25 Robert Grützmann,26 Stephan Haas,27 Jochen Hampe,17 Claus Hellerbrand,28 Peter Hegyi,24 Dominik Huster,29 Mihai Ioana,30 Sevastitia Iordache,31 Grazyna Jurkowska,20 Volker Keim,9 Olfert Landt,32 Milena Di Leo,11 Markus M Lerch,33 Philippe Lévy,34 Matthias J Löhr,27 Milan Macek,35 Nuria Malats,36 Ewa Malecka-Panas,23 Alberto Mariani,11 Davide Martorana,37 Julia Mayerle,33 Josefina Mora,38 Joachim Mössner,9 Sebastian Müller,39 Johann Ockenga,40 Jana Paderova,35 Sergio Pedrazzoli,41 Stephen P Pereira,42 Roland Pfützer,43 Francisco X Real,44 Vinciane Rebours,34 Monika Ridinger,28 Marcella Rietschel,22 Kerstin Rohde,9 Stephan Sack,45 Adrian Saftoiu,31 Alexander Schneider,46 Hans-Ulrich Schulz,47 Michael Soyka,48 Peter Simon,33 James Skipworth,49 Felix Stickel,50 Michael Stumvoll,2, 51 Pier Alberto Testoni,11 Anke Tönjes,2, 51 Matthias Treiber,13 Frank Ulrich Weiss,33 Jens Werner,52 Norbert Wodarz28
13II. Medizinische Klinik, Klinikum rechts der Isar of the Technical University Munich, Munich, Germany
14Department of Internal Medicine, Neurology and Dermatology, Clinic of Gastroenterology and Rheumatology, Division of Hepatology, University of Leipzig, Leipzig, Germany
15Hospital Freiberg, Academic Hospital of the Technical University Dresden, Clinic for Internal Medicine, Freiberg, Germany
16Department of Gastroenterology & Hepatology, Erasmus Medical Centre, University Medical Centre Rotterdam, Rotterdam, The Netherlands
17Medical Department I, University Hospital Dresden, TU Dresden, Dresden, Germany
18Institute of Transfusion Medicine and Immunology, Medical Faculty of Mannheim University of Heidelberg, German Red Cross Blood Service of Baden-Württemberg-Hessen, Mannheim, Germany
19Department of Gastroenterology, Medical University of Lublin, Lublin, Poland
20Department of Gastroenterology and Internal Medicine, Medical University Bialystok, Bialystok, Poland
21Department of Gastroenterology, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
22Department of Genetic Epidemiology in Psychiatry, Central Institute of Mental Health, University of Heidelberg, Heidelberg, Germany
23Department of Digestive Tract Diseases, Medical University of Lodz, Lodz, Poland
24First Department of Medicine, University of Szeged, Szeged, Hungary
25Department of Medicine I, Altona General Hospital, Hamburg, Germany
26Department of General, Thoracic and Vascular Surgery, University Hospital Carl Gustav Carus, Technical University Dresden, Dresden, Germany
27Gastrocentrum, Karolinska Institutet CLINTEC, Stockholm, Sweden
28Department of Internal Medicine I, University Hospital Regensburg, Regensburg, Germany
29Evangelisches Diakonissenkrankenhaus Leipzig, Academic Hospital of the University of Leipzig, Leipzig, Germany
30Molecular and Cellular Biology Department, University of Medicine and Pharmacy Craiova, Craiova, Romania
31Department of Internal Medicine and Gastroenterology, University of Medicine and Pharmacy, Craiova, Romania
32TIB MOLBIOL, Berlin, Germany
33Department of Medicine A, University Medicine Greifswald, Greifswald, Germany
34Pôle des Maladies de l'Appareil Digestif, Service de Gastroentérologie-Pancréatologie, Hôpital Beaujon, AP-HP, Clichy, France
35Department of Biology and Medical Genetics, University Hospital Motol and 2nd Faculty of Medicine, Charles University, Prague, Czech Republic
36Grupo de Epidemiología Genética y Molecular Programa de Genética del Cáncer Humano Centro Nacional de Investigaciones Oncológicas (CNIO), Madrid, Spain
37Unit of Molecular Genetics, University Hospital of Parma, Parma, Italy
38Department of Biochemistry, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
39Department of Internal Medicine, Salem Medical Centre and Centre for Alcohol Research, University of Heidelberg, Heidelberg, Germany
40Medical Clinic II, Internal Medicine, Gastroenterology, Endocrinology and Nutritional Medicine, Klinikum Links der Weser, Klinikum Bremen Mitte, Bremen, Germany
41IV Surgical Clinic, Department of Medical and Surgical Sciences, University of Padua, Padua, Italy
42UCL Institute for Liver and Digesive Health, Division of Medicine, University College London, London, UK
43Clinic for Internal Medicine, Hospital Döbeln, Döbeln, Germany
44Epithelial Carcinogenesis Group, Molecular Pathology Programme, Centro Nacional de Investigaciones Oncológicas, Madrid, Spain
45Clinic for Internal Medicine II, Ev. Klinikum Paul-Gerhardt-Stift, Paul-Gerhardt-Diakonie Hospital and Care GmbH, Lutherstadt Wittenberg, Germany
46Department of Gastroenterology, Hepatology, Infectious Diseases, Medical Faculty of Mannheim University of Heidelberg, Mannheim, Germany
47Department of Surgery, Otto-von-Guericke University Magdeburg, Magdeburg, Germany
48Psychiatric Hospital, University of Munich, Munich, Germany
49Department of Surgery and Interventional Science, University College London, London, UK
50Department of Visceral Surgery and Medicine, Inselspital Bern, Berne, Switzerland
51Department of Internal Medicine, Neurology and Dermatology, Division of Endocrinology, University of Leipzig, Leipzig, Germany
52Department of General Surgery, University of Heidelberg, Heidelberg, Germany
Contributors MHD, PK, MS and JR conceived, designed and directed the study. MHD, PK, MS, EM, CR, and JR designed, performed and interpreted genetic analyses with significant contributions from JPHD, CF, and HW. MHD, PK, JR wrote the manuscript with significant contributions from MS, EM, J-MC, CF, JPHD, and HW. OL provided oligonucleotides. All other coauthors recruited study subjects, collected clinical data and provided genomic DNA samples. All authors approved the final manuscript and contributed critical revisions to its intellectual content.
Funding This work was supported by the Deutsche Forschungsgemeinschaft (DFG) grants RO 3929/1-1 & RO 3939/2-1 (to JR), Wi 2036/2-2 & Wi 2036/2-3 (to HW), and SFB 1052 (to MB, MS, AT, PK), by the Boehringer Ingelheim Foundation (to KR), by a grant of the Colora Stiftung gGmbH (to JR), the Else Kröner-Fresenius-Foundation (EKFS) (to HW), by CZ.2.16/3.1.00/24022OPPK and "Conceptual development project of research organization #00064203" (University Hospital Motol, Prague) from the Czech Ministry of Health, Norway Grants PDP3 (to MM), the Institut National de la Santé et de la Recherche Médicale (INSERM; to CF), the Programme Hospitalier de Recherche Clinique (PHRC R 08-04; to CF), the French Association des Pancréatites Chroniques Héréditaires (to CF), the Council of Scientific and Industrial Research (CSIR) (to CF).
Competing interests None.
Ethics approval Ethical Committee of the University Leipzig.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are included in the manuscript.