Article Text

Abstract
Objective To gain mechanistic insights, we compared effects of low fermentable oligosaccharides, disaccharides and monosaccharides and polyols (FODMAP) and high FODMAP diets on symptoms, the metabolome and the microbiome of patients with IBS.
Design We performed a controlled, single blind study of patients with IBS (Rome III criteria) randomised to a low (n=20) or high (n=20) FODMAP diet for 3 weeks. Symptoms were assessed using the IBS symptom severity scoring (IBS-SSS). The metabolome was evaluated using the lactulose breath test (LBT) and metabolic profiling in urine using mass spectrometry. Stool microbiota composition was analysed by 16S rRNA gene profiling.
Results Thirty-seven patients (19 low FODMAP; 18 high FODMAP) completed the 3-week diet. The IBS-SSS was reduced in the low FODMAP diet group (p<0.001) but not the high FODMAP group. LBTs showed a minor decrease in H2 production in the low FODMAP compared with the high FODMAP group. Metabolic profiling of urine showed groups of patients with IBS differed significantly after the diet (p<0.01), with three metabolites (histamine, p-hydroxybenzoic acid, azelaic acid) being primarily responsible for discrimination between the two groups. Histamine, a measure of immune activation, was reduced eightfold in the low FODMAP group (p<0.05). Low FODMAP diet increased Actinobacteria richness and diversity, and high FODMAP diet decreased the relative abundance of bacteria involved in gas consumption.
Conclusions IBS symptoms are linked to FODMAP content and associated with alterations in the metabolome. In subsets of patients, FODMAPs modulate histamine levels and the microbiota, both of which could alter symptoms.
Trial registration number NCT01829932.
- IRRITABLE BOWEL SYNDROME
- HISTAMINE
- CARBOHYDRATES
- COLONIC MICROFLORA
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Meals trigger symptoms in many patients with IBS and specific diets can improve symptoms.
Low fermentable oligosaccharides, disaccharides and monosaccharides and polyols (FODMAP) diets appear to improve symptoms but the specific role of FODMAPs is unclear.
Metabolomics can identify metabolites of the host-microbial interactions and provide mechanistic insights.
What are the new findings?
Metabolic profiling of urine showed diets caused significant separation of metabolome.
There was an eightfold reduction in urinary histamine in the low FODMAP group.
Low FODMAP diet increased Actinobacteria richness and diversity and high FODMAP diet decreased the relative abundance of bacteria involved in gas consumption, likely contributing to symptoms.
The lactulose breath test did not predict responders of a low FODMAP diet.
How might this impact on clinical practice in the foreseeable future?
Low FODMAP diets have a specific action that is beneficial in patients with IBS but further studies are needed to identify the specific FODMAPs that produce this benefit.
There is evidence that FODMAPs modulate immune activation in subsets of patients and histamine may be an important pathophysiological mediator.
Changes in gut microbiota may play a role in symptom generation in a subset of patients with IBS; however, a low FODMAP diet might induce potential ‘unhealthy’ changes at the microbial level but requires long-term studies.
Introduction
There is increasing evidence that interactions between food components and the microbiota could provide mechanistic insights into the pathophysiology of IBS.1–3 In particular, a number of studies suggest that fermentable oligosaccharides, disaccharides and monosaccharides and polyols (FODMAPs) can induce IBS symptoms.3–8 Dietary interventions using low FODMAP diets showed marked improvement in symptoms, benefiting up to 70% of patients in some studies.3 Furthermore, a recent study suggested that the reduction of FODMAPs in a gluten-free diet could explain, at least in part, the benefit observed with gluten avoidance in patients with IBS who do not have coeliac disease.4 Despite this growing enthusiasm for the low FODMAP diet, mechanisms underlying the diet are unclear. Furthermore, there are concerns regarding the magnitude of the response as the controls in some studies may not negate a placebo effect2 ,9 and a recent study suggests that FODMAP reduction may not confer a benefit over traditional IBS diet recommendations.8 Together, these observations raise questions about whether FODMAPs have a specific mechanism that explains their ability to alter IBS symptoms.
The mechanism by which reducing FODMAP could decrease IBS symptoms could be multifactorial. The most widely cited action linked with FODMAPs is distention caused by both the osmotic effect of FODMAPs and gas production resulting from fermentation in the colon.5 ,10 This distention could activate nociceptors and enteric reflexes leading to increased symptoms. This would be worsened in those with underlying visceral hypersensitivity,10 a common feature in IBS. Other observations however suggest additional mechanisms could also be involved.1 For example, the beneficial effects of low FODMAP diets seem to extend to patients with either diarrhoea or constipation, suggesting more than just a simple osmotic action.10 Other studies suggest FODMAPs may improve global symptoms such as depression.11 ,12 Given that depression has also been linked to low grade inflammation in IBS,13 this could imply an interaction between the immune system and FODMAPs. Finally, given the pivotal role in the microbiota in fermenting FODMAPs,14 the metabolic response of the patient's microbiota to FODMAPs might also be important in understanding underlying mechanisms.
Metabolomic measurements are increasingly recognised as a valuable tool to understand the impact of diet on the host15 and dietary interventions may provide important insights into the pathophysiology of disorders, including IBS. To examine the impact of FODMAPs on the metabolome, we evaluated three measures, (1) a 5 h lactulose breath test (LBT), (2) metabolic profiling in urine using direct infusion and gas chromatography mass spectrometry and (3) partial 16s rRNA gene profiling (Illumina) to analyse stool microbiota composition, at baseline and following the diet intervention. We chose to compare low and high FODMAP diets in a blinded fashion to minimise the placebo and nocebo effects of altering diets on symptoms and obtain a measure of the specific impact of FODMAP content.
Materials and methods
Subjects
In this prospective, randomised, single blind parallel study comparing the effect of a low-FODMAP versus high-FODMAP diet in patients with IBS (figure 1), subjects were recruited from adult outpatient clinics at a single-centre academic teaching hospital in Kingston, Ontario, Canada between June 2013 and November 2014. Patients were eligible for the study if they were 18 years or older and met the Rome III criteria for IBS of any subtype including IBS with constipation (IBS-C), IBS with diarrhoea (IBS-D), mixed type IBS (IBS-M) or unsubtyped IBS (IBS-U) and had symptoms for greater than 6 months. The study protocol was approved by the Health Sciences Research Ethics Board at Queen's University (DMED-1443-11) and was registered with the USA National Library of Medicine clinical trials registry ClinicalTrials.gov (NCT01829932).

Schematic drawing of the study design. FODMAP, fermentable oligosaccharides, disaccharides and monosaccharides and polyols, IBS-SSS, IBS symptom severity scoring.
Study design
Visit 1: screening
Patients received verbal and written information about the study and gave informed consent (figure 1). Patients were advised that the purpose of the study was to ‘assess whether changing the amount of certain foods in the diet affects symptoms of IBS by altering how bacteria interact with the gut’. Patients were excluded if they had a history of gastric, small bowel or colonic surgery, active IBD, coeliac disease, were pregnant or were unable to come off the following medications: antibiotics (including use within past 4 weeks), stool bulking agents, narcotic analgesics or lactulose. No patients reported taking probiotics. Patients were also excluded if they recorded on a written checklist they were on one of the following special diets: Palaeolithic diet, gluten-free diet, low FODMAP diet or Atkins diet. They were not told what type of diet they were being assigned or that one diet might be superior to the other, and the concept of FODMAPs was never mentioned during the study.
Visit 2 (day 0): randomisation
Patients completed the IBS symptom severity questionnaire, underwent a baseline 5 h LBT and provided a urine and stool sample. They were then randomised by the hospital statistician using a computer generated randomisation programme to either diet 1 (a high FODMAP content diet) or diet 2 (a low FODMAP content diet) which was contained in a sealed envelope. They were also provided a dietary log booklet and asked to record their daily food intake for the 3-week study period.
Visit 3 (day 21); end of diet treatment
Patients completed a final IBS symptom severity questionnaire, provided a urine and stool sample and repeated the LBT. This data, and the corresponding baseline data were collected by a study administrator who was blinded to the intervention. The dietician, who was not blinded to the intervention, then collected their diet diaries and reviewed their compliance with the diets. Following completion of the study, the dietician scored FODMAP content in the diet logs in a blinded fashion using a scoring system specifically designed for this study (see online supplementary table S1 and methods).
Supplementary table 1
Intervention
During visit 2, each subject met individually for 30–60 min with the GI dietician to review the components of their assigned diet and to obtain advice on sample menus. The randomisation envelope also contained a dietary booklet specifically designed for this study that described five sample meals for breakfast, lunch, dinner and snacks and specified foods either high or low in FODMAP content, depending on their assignment. They were free to pick the specific foods that they consumed but were not allowed to be on antibiotics, fibre supplements or lactulose during the 3-week study period.
Outcome assessments
Symptoms. Changes in symptoms were assessed using the previously validated IBS symptom severity system (IBS-SSS).16 The maximum score is 500 and is summed from five individual scores; abdominal pain (severity and days of pain), distension, dissatisfaction with bowel habit and a quality of life measure.
Lactulose Breath Test. Patients fasted for 10 h overnight and after providing a baseline breath sample they ingested the test meal consisting of a packet of Kristalose. Breath samples were then obtained every 15 min for 5 h (see supplementary methods for details).
Supplemental material
Urine Mass Spectrometry Analysis of Metabolome. Urine samples were assayed using a combined direct infusion (DI-)/liquid chromatography (LC-) tandem mass spectrometry (MS/MS) (AbsolutIDQ p180 kit, Biocrates Life Sciences AG, Innsbruck, Austria), and gas-chromatography (GC-) MS assays at The Metabolomics Innovation Center (Edmonton, AB) to identify and quantify metabolites, as previously described.17
Deep sequencing analysis of 16S rRNA with Illumina. The V3 region of the 16S rRNA gene was amplified as previously described.18 Custom inhouse Perl scripts were developed to process the sequences after Illumina sequencing18 with Cutadapt to trim any over-read; paired-end sequences were aligned with PANDAseq19 with a 0.7 quality threshold. If there was a mismatch in the assembly of a specific set of paired-end sequences, or any sequences with ambiguous base calls, they were discarded. Operational taxonomic units (OTUs) were picked using AbundantOTU+,20 and sequences were clustered to 97% sequence identity. Taxonomy was assigned at a 0.8 threshold using the Ribosomal Database Project (RDP)19 classifier V.2.2 trained against the Greengenes small subunit (SSU) database (2013 release). The obtained OTU table was filtered excluding ‘Root’ and any sequence that was not present at least three times across the entire data set. Calculations of within-community diversity (α-diversity), between-community diversity (β-diversity), significant OTU presence and correlations with FODMAP scores were run using QIIME.21
Statistical analysis
Continuous data were analysed using paired and unpaired t test reporting, two-tailed p values after the normality of the distribution had been demonstrated with the D'Agostino and Pearson omnibus test; p<0.05 was considered to be statistically significant. The LBT (area under the curve, AUC) was the primary end point as previous studies suggested the difference in hydrogen production between patients with IBS consuming a low FODMAP diet versus a standard diet was greater than the SD of hydrogen production within groups.5 Based on this assumption, we calculated 16 patients were needed per arm to have 80% power to detect a difference between groups of >1 within-group SD of hydrogen production using an unpaired t test with a two-sided α of 0.05.
Metabolite concentrations (μmol/L) were normalised to creatine (mmol/L) and reported as the ratio (μmol/mmol). The MetaboAnalyst 3.0 was used for metabolomic related statistical analysis.22 (see supplementary methods for details).
The 16s RNA sequencing analysis was performed using SPSS V.20.0 software for Windows (SPSS, Chicago, Illinois, USA) or QIIME scripts. Statistical comparisons were performed using Kruskal–Wallis tests, Mann–Whitney tests, Spearman's correlations and linear regressions, where appropriate. False discovery rate correction was applied for multiple comparisons.
Results
Patient characteristics
The study enrolled 40 patients with IBS, 2 withdrew from the low FODMAP group (1 from difficulty following the diet plus increased symptoms and 1 did not report at visit 2 despite multiple attempts to contact patient) and 1 from the high FODMAP group (did not report at visit 2 despite multiple attempts to contact patient). Most patients were IBS-D or IBS-M. Patients were well matched for age, gender, medications, body mass index and IBS subtype between groups (table 1).
Comparison of subject demographics between low FODMAP and high FODMAP cohorts
Symptom scores
Baseline IBS-SSS were not different between the two groups (289.6±19.17 vs 279.8±18.36, p=0.48). Patients in the low FODMAP group had a mean decrease in global symptom scores of 28% compared with baseline following the 3 week diet intervention (p<0.001), whereas the high FODMAP group patients reported a mean increase of 7% in symptoms (not significantly different from baseline) (table 2 and figure 2A). Comparison of the postdiet scores between the two groups showed a statistically significant difference (p=0.01) and the proportion of patients defined as responders (IBS symptom reduction ≥5016) was significantly greater in the low FODMAP group (72%; 13/18) compared with the high FODMAP group (21%; 4/19) (p<0.009).
Comparison of IBS symptom response to diet interventions
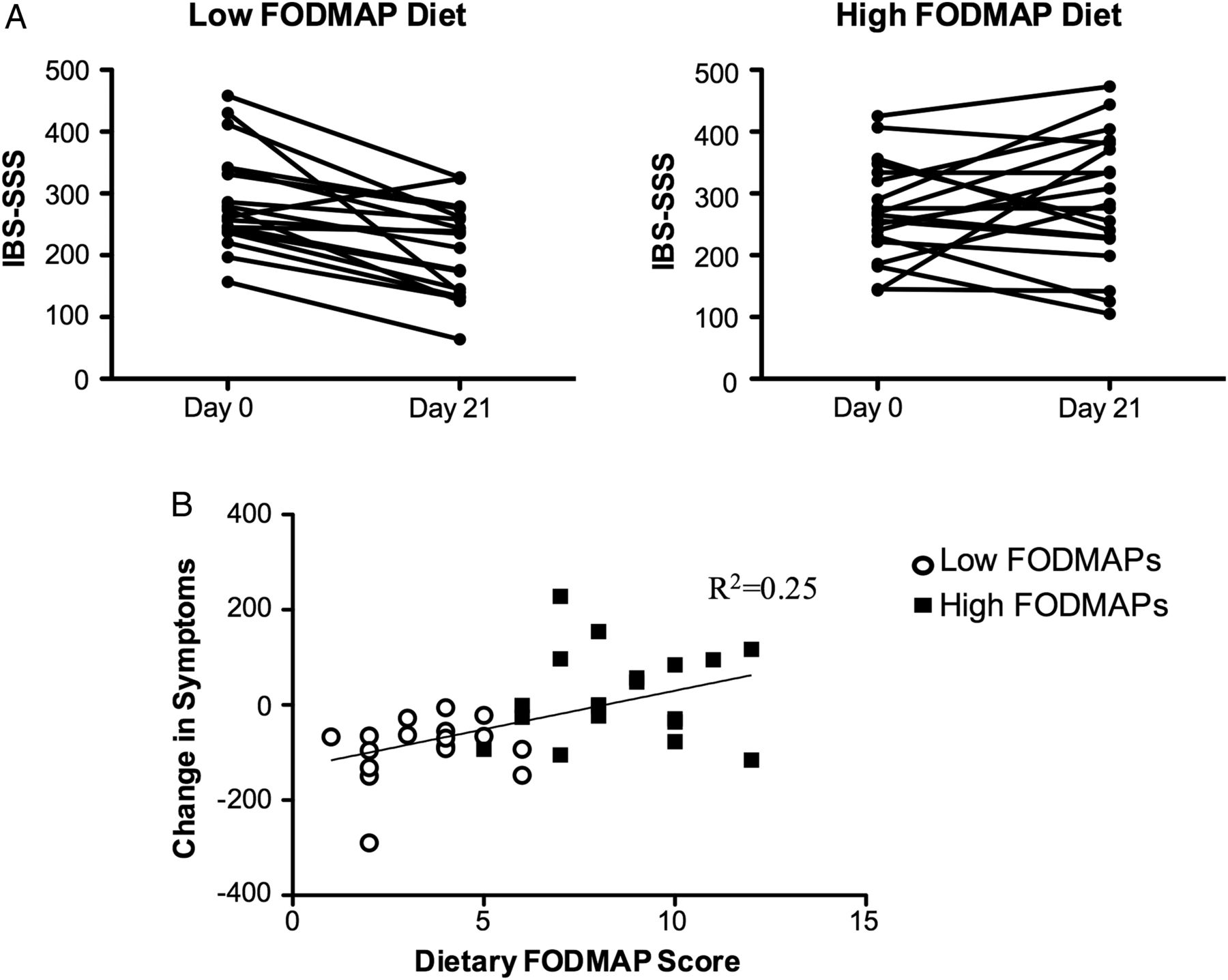
Global IBS symptoms improved on a low fermentable oligosaccharides, disaccharides and monosaccharides and polyols (FODMAP) diet but not a high FODMAP diet. (A) Individual scores showing almost all patients improved in the low FODMAP group whereas most patients in the high FODMAP group were unchanged or worse. (B) Increases in dietary FODMAP content based on a FODMAP scoring system (see text and supplementary table S1), independent of diet assignment, positively correlated with increasing symptoms in patients with IBS. IBS-SSS, IBS symptom severity scoring.
Examination of components of the IBS-SSS revealed a marked decrease in abdominal pain scores in the low FODMAP group (52% reduction; p<0.01) (table 2). In contrast, patients in the high FODMAP group reported significantly more days of pain (table 2; p<0.05). Patients in the low FODMAP group also reported a trend towards a reduction in abdominal distention (table 2; p=0.08). When asked whether they were satisfied with the intervention, only those in the low FODMAP group reported a significant increase in satisfaction (table 2).
To provide an independent measure of the relationship between FODMAP consumption and IBS symptoms, patient diaries for the 3rd week of the diet were reviewed in a blinded fashion by the dietician and scored using a 14-point scoring system (see online supplementary table S1). The scores ranged from 1 to 6 (mean=3.5±0.34) in the low FODMAP group and from 5 to 12 (mean=8.6±0.46) in the high FODMAPs group (p<0.0001 between groups), suggesting good compliance with the diets. We correlated the FODMAP diet diary scores (independent of their diet assignment) and global IBS symptom scores and found a positive correlation between IBS symptom severity and their level of FODMAP consumption (figure 2B; p=0.002, R2=0.25).
There was no significant change in body weight in either group following the 3 week diet (pre low FODMAP=75.7±20.5 kg, post=75.3±20.4 kg; pre high FODMAPs=75.2±14.9 kg, post=75.2±13.9 kg).
Lactulose breath test
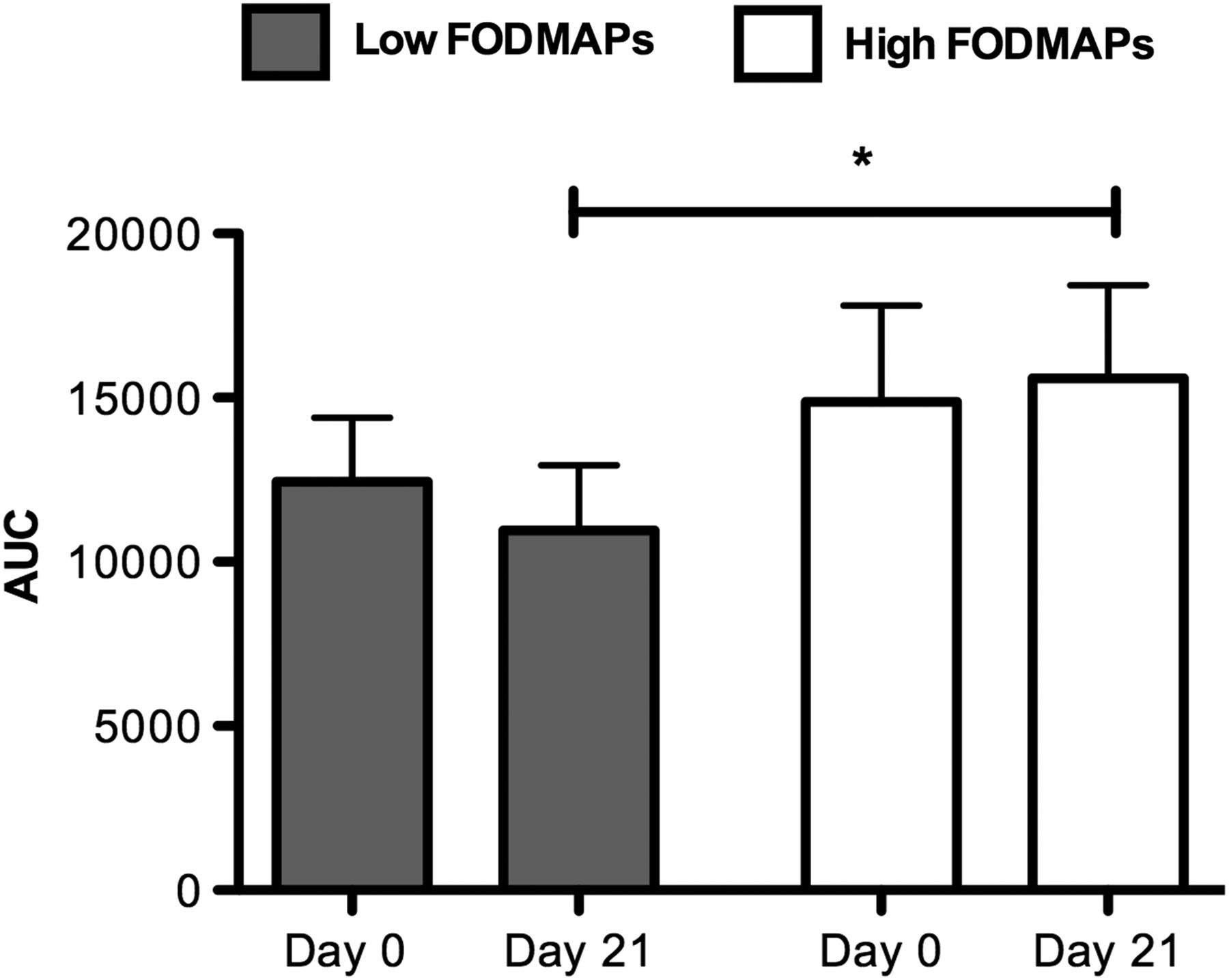
Small differences in H2 AUC were observed in the post LBTs in the high FODMAP group compared with the low FODMAP group (figure 3) (p<0.05, corrected for baseline differences between groups). The baseline H2 responses to lactulose, the relative change in post-test levels compared with baseline and the absolute post-test levels did not correlate with overall symptom response (data not shown). No differences were observed in the methane measurements between the two diet groups (data not shown).

Effect of fermentable oligosaccharides, disaccharides and monosaccharides and polyols (FODMAP) diets on lactulose breath test. Following the diet interventions, small differences were observed in the area under the curve (AUC) between the H2 response to lactulose ingestion in the low FODMAP versus the high FODMAP diet group. (*p<0.05, corrected for baseline differences).
Urinary metabolomic evaluation
Using DI-MS, GC-MS and LC-MS techniques on urine samples (n=15 low FODMAP group; n=18 high FODMAP group) we could quantify 75, 37 and 41 metabolites, respectively. Using univariate analysis, 29 candidate metabolites were selected for further analysis using partial least squares discriminant analysis (PLS-DA). Baseline metabolomic profiles of patients in the two diet groups were not different from each other (figure 4A, p=0.77, R2=0.13 and Q2=−0.62). However, following dietary intervention there was a significant separation in metabolomic profiles of patients with IBS in the two diet groups (figure 4B). The observed separation was found to be statistically significant using permutation testing (p=0.001). The R2 and Q2 of the model was 0.63 and 0.33, respectively. The variable importance in projection (VIP) values of three metabolites (histamine, p-hydroxybenzoic acid (pHBA) and azelaic acid) were above 1.5, indicative of their significant role in the discrimination between metabolomic profiles of subjects in the two groups after the dietary intervention. The VIP values of these three metabolites as well as their mean levels in each diet group before and after the intervention are presented (table 3). In the low FODMAP diet group, urinary histamine level decreased significantly after the intervention (figure 5), while in the high FODMAP group a marginally significant increase in urinary levels of pHBA was seen. In addition, when comparing the postdiet effects, the means of these metabolites were statistically different (p<0.05) between the two diet groups when adjusting for their baseline values.
Concentrations (µmol/mmol creatine) of the three major urinary metabolites that discriminate between the two diets

Changing the fermentable oligosaccharides, disaccharides and monosaccharides and polyols (FODMAP) content is associated with alterations in the metabolome. (A) Principal component analysis of the urine metabolome demonstrated that both groups were similar on day 0 (p=0.77, R2=0.13, Q2=−0.62). (B) Urine metabolomic profile on day 21 showed significant separation of patients on a low FODMAP diet compared with patients on a high FODMAP diet (p=0.001, R2=0.63, Q2=0.33).

Low fermentable oligosaccharides, disaccharides and monosaccharides and polyols (FODMAP) diet significantly decreases urine histamine levels. (A) Urine histamine levels remained unchanged after 21 days of a high FODMAP diet (normalised to creatine) whereas there was a significant reduction in urine histamine in the low FODMAP group. *p<0.05. B. Individual patients that had elevated urine histamine (normalised to creatine) on day 0, day 21 or both in the high FODMAP group (left panel) and the low FODMAP group (right panel).
16s RNA profiling of colonic microbiome
A total of 20 990 056 reads before quality filtering (an average of 333 175 reads per sample with a range of 266 694–417 572), 8 346 208 reads after quality filtering (an average of 139 103.467 reads per sample with a range of 111 067–173 213) and 3602 OTUs (an average of 578.15 OTUs per sample with a range of 235–961 OTUs per sample, after quality filtering) were obtained from the 60 samples sequenced.
There was no difference in α-diversity (within-community, species diversity and richness) or β-diversity (between-community) between samples from before and after high or low FODMAP diets and the results were similar across all types of IBS (IBS-D, IBS-C, IBS-M and IBS-U). However, when analysing only the samples after 3 weeks of a high FODMAP or a low FODMAP diet, faecal samples from the low FODMAP group showed higher Actinobacteria richness and diversity (corrected p=0.046 and 0.02, respectively) compared with the high FODMAP group. Analysing only the samples of patients with IBS-M and IBS-D (excluding two IBS-C and one IBS-U to create a more uniform group, all with some diarrhoea) we observed higher bacterial richness (corrected p=0.047) in the low FODMAP group compared with the high FODMAP group (figure 6A). Specifically, Firmicutes, Clostridiales and Actinobacteria richness was higher (all corrected p=0.029, 0.023 and 0.029, respectively), and Actinobacteria bacterial diversity was increased (corrected p=0.013). Analysis of the taxonomic composition at the highest assigned taxonomic level (genus level) revealed that bacteria from the genus Adlercreutzia (Coriobacteriaceae), Dorea (Lachnospiraceae) and the family of Actinomycetaceae were lower after a high FODMAP diet (uncorrected p=0.02, 0.05 and 0.044, respectively) (figure 6B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Colonic microbiota composition of patients with IBS after 3 weeks of low or high fermentable oligosaccharides, disaccharides and monosaccharides and polyols (FODMAP) diet. α-diversity analysis of bacterial communities in faeces of patients with IBS after high (closed circle) or low (open circle) FODMAP diet (A). The richness estimator Chao 1 reveals a significant reduction in species richness in patients that followed a high FODMAP diet in comparison to those following a low FODMAP diet. From left: Total bacterial richness, Firmicutes richness, and Actinobacteria richness, here measured as number of observed species. Significantly different families and genera across the three sample groups (B). The P value shown in the graph is that of the pairwise comparison from the Kruskal–Wallis test. Significant linear regressions observed in faecal samples from patients with IBS after a high (closed circle) FODMAP diet between relative abundance of unclassified (Uncl.) Ruminococcaceae, Roseburia and Bilophila with symptoms (Δ of P1—P0), H2 production (Δ of P1—P0) and histamine concentration (Δ of P1—P0), respectively (C). Significant linear regressions observed in faecal samples from patients with IBS after a low (open circle) FODMAP diet between relative abundance of Bacteroidetes, Akkermansia muciniphila and Adlercreutzia with symptoms (Δ of P1—P0), H2 production (Δ of P1—P0) and p-hydroxybenzoic acid concentration (Δ of P1—P0), respectively (D). In each plot is included the linear regression line and statistical details, matched for age, gender, medications, body mass index (BMI) and IBS subtype between groups (table 1).
When analysing the paired data, we observed that Propionibacteriaceae (Actinomycetales) decreased (uncorrected p=0.043) while unclassified genera within the Clostridiales family XIII Incertae sedis (uncorrected p=0.008) and Porphyromonas (uncorrected p=0.01) increased after the low FODMAP diet. Interestingly, the high FODMAP diet induced more changes as several bacterial groups decreased after the high FODMAP diet, but the family Bifidobacteriaceae (uncorrected p=0.041) and unclassified genera within the family Lachnospiraceae increased (uncorrected p=0.036).
Correlating microbial changes with diet, symptoms and metabolome
Several abundant genera were negatively correlated with increasing FODMAP dietary content, including two genera belonging to the Lachnospiraceae family (Clostridium and Roseburia) (R=0.369, p=0.045; R=−0.381, p=0.038, respectively), as well as some low abundant genera such as Olsenella (Coriobacteriaceae) (R=−0.384, p=0.036), Shuttleworthia (Lachnospiraceae) (R=0.402, p=0.027) and unclassified Veillonellaceae (R=−0.430, p=0.018). On the other hand, the low abundant genus Enterococcus positively correlated with FODMAP dietary content (R=0.385, p=0.036). Moreover, we observed several significant correlations between bacterial relative abundance and symptoms, H2 production and urine metabolome (figure 6C, D, table 4 and online supplementary table S2). Specifically, in the high FODMAP group, the relative abundance of unclassified Ruminococcaceae accounted for 5.5% of the explained variability in symptoms, and the Roseburia spp accounted for 7.2% of the explained variability in H2 production. We also found that Odoribacter, Parabacteroides, Prevotella, Bilophila and Lachnobacterium accounted for 11.7%, 5.1%, 8.7%, 6.5% and 6.9%, respectively, of the explained variability in urinary histamine concentration, while Lactococcus accounted for 5.0% of the explained variability in pHBA concentration.
Supplementary table 2
Significant correlations between bacterial genera and symptoms, H2 production and urine metabolome in faecal samples from patients with IBS after high or low FODMAP diet (Δ(P1−P0))
In the low FODMAP group, Bacteroidetes accounted for 6.5% of the explained variability in symptoms, and Akkermansia accounted for 5.4% of the explained variability in H2 production. Urinary histamine levels positively correlated with the relative abundance of unclassified Porphyromonadaceae spp. Moreover, we observed that Adlercreutzia, Firmicutes and Actinomyces accounted for 5.8%, 5.1% and 9.9% of the explained variability in urinary pHBA and azelaic acid concentration. In addition, testing the data with MaAsLin (multivariate analysis with linear modelling)23 ,24 showed that the relative abundance of unclassified Porphyromonadaceae was strongly associated with urinary histamine concentration (corrected p value=0.04).
Discussion
This study has shown that FODMAP content is linked to IBS symptoms. We found that patients with IBS randomised to a low FODMAP diet had improved IBS symptoms, whereas most patients randomised to the high FODMAP diet had either no improvement or worsening of symptoms. Our study design blinded patients to the nature of the dietary intervention and attendant consequences and used diets that should have opposing actions, thereby mitigating the placebo and potential nocebo bias. Our study also provided an independent assessment of the impact of FODMAPs on IBS symptoms by correlating a quantitative measure of FODMAP content consumption with symptoms, regardless of diet assignment. This also showed significant correlation between symptoms and FODMAP content, further attesting to the conclusion that FODMAPs are linked to IBS symptoms.
There is rapidly growing interest in the study of food metabolomics to understand the complex interaction between diet and patients.15 This metabolome has two different fractions, endogenous metabolome and food metabolome, and are derived from the digestion of food, their absorption and biotransformation by the human donor and the microbiota. Our study identified major changes in specific metabolites and associations between these metabolites and the microbiota in response to the dietary interventions, as shown in table 4. These reflect changes in both the endogenous and food metabolome and while the full significance of these changes has yet to be elucidated, the implications of our metabolomic data are that multiple pathways could lead to symptoms in IBS. For example, this could include signalling by active and inert (eg, gases) metabolites due to fermentation and degradation by specific bacteria. Furthermore, dietary modulation of the microbiota could either increase the abundance of specific bacteria or their metabolites, thereby amplifying abnormal signalling by these pathways.
Our analysis of the urinary metabolome identified three specific metabolites that were altered by the diet, histamine, pHBA and azelaic acid. The reduction in histamine in the low FODMAP group and increase in the high FODMAP group in subsets of patients is of immediate interest given the strong evidence that histamine is an important signalling molecule underlying IBS symptoms. It is widely recognised that histamine is increased in the mucosa of many patients with IBS,25–27 is associated with increased mast cell activation, and sensitises nociceptive and enteric neurons.28–30 The mast cell stabiliser ketotifen increased threshold for patients with discomfort IBS with visceral hypersensitivity as well as improved IBS symptoms.31 Furthermore, in preliminary studies, histamine blockade with H1 antagonists improves IBS symptoms.32 Although the mechanism(s) causing elevation of histamine was not directly determined in our study, there are several pathways that warrant further study. One pathway involves short-chain fatty acid (SCFA)33 signalling to mast cells given the evidence that fermentation of FODMAPs increases these metabolites in the colon and that SCFAs can modulate mast cells.34–36 The other is mechanically induced mast cell degranulation. This may occur because fermentation of FODMAPs could lead to distention of the intestine, and mechanical forces are also known to degranulate mast cells.37 In contrast to the histamine changes, the other two metabolites, pHBA and azelaic acid, showed a relative increase in the low FODMAP group compared with the high FODMAP group. pHBA is an organic acid and a phenolic derivative of benzoic acid. Significant amounts of benzoic acid have been found in most berries. In addition, benzoic acid is a byproduct of phenylalanine metabolism in bacteria and is produced when gut bacteria process polyphenols from plant sources.38 Azelaic acid, a C9 linear α,ω-dicarboxylic acid, is found in whole grains specifically wheat, rye, barley, oat seeds and sorghum39 and has anti-inflammatory properties.40 Although dietary intake of patients was not assessed at baseline, the observed increase in urinary azelaic acid concentration following the FODMAP diet may be related to an increase in the consumption of oat seeds and sorghum intake in the low FODMAP group. However, further adequately powered studies are needed to understand the variability of the expression of these metabolites in patients with IBS and patients without IBS, and their relationship with symptoms.
FODMAPs are prebiotics for selective microbial species and consequently diet-induced changes in the colonic microbiota potentially amplify signalling molecules underlying IBS symptoms. We did not observe a distinct clustering in microbiota profiles between the patients on low and high FODMAP diets, which might be due to other environmental factors, including their long-term diet or medications. However, we did observe changes at the taxonomical level of several bacterial families and genera. These changes were reflected in the higher bacterial richness and diversity in the faecal samples of patients after a low FODMAP diet. Our results are in agreement with previous studies that showed a decrease in Bifidobacteria41 in patients with IBS on the low FODMAP diet. Interestingly, despite a decrease in Bifidobacteria relative abundance after the low FODMAP diet, Actinobacteria richness and diversity was still higher in these patients in comparison to those on the high FODMAP diet. However, we also observed that the shift caused by the low FODMAP diet to the microbial community left a niche open to potentially harmful bacteria, such as Porphyromonadaceae,42 ,43 which we found to be strongly associated with urinary histamine levels.
Levels of SCFA producers (members of Clostridiales, Bacteroides, Prevotella and Bifidobacteria), which are generally considered to be important for intestinal health,44 were altered by changes in FODMAP content. Interestingly, the relative abundance of lactate producers Bifidobacteria were increased after the high FODMAP diet as previously described,41 but that of butyrate producers Roseburia and Ruminococcus was lower after the high FODMAP diet. Indeed, examining levels of H2 as an indirect measure of fermentation, we observed a lower relative abundance of the butyrate producers Roseburia spp in patients with higher H2 levels. Patients on the low FODMAP diet, instead, had higher relative abundance of Adlercreutzia, a bacterium that consumes H2 for equol production and can thus decrease gas formation, such as hydrogen sulfide and methane.45 ,46 It is possible that this contributed to the reduced pain and bloating reported by our patients. Moreover, we have observed that despite presenting with similar relative abundance on low or high FODMAP diets, Akkermansia muciniphila abundance inversely correlated with H2 production in both groups. This bacterium has been reported to have beneficial effects on host metabolism and immune homoeostasis.44 ,47
Several limitations of the study design were identified. First, we did not conduct a careful analysis of dietary intake at baseline prior to the baseline measurements and the dietary intervention. This could have impacted on the initial baseline measurements including the breath-test results and potentially diluted the impact of the dietary interventions. Second, the adequacy of the blinding was not formally monitored. Patients were only advised at their enrolment visit that diet can potentially affect symptoms but no clues were offered as to the specific nature of the diet and what the potential outcome might be on their symptoms. Most patients were enrolled before the FODMAP diet was routinely used in our clinics and a large number enquired at their final visit with the dietician about the nature of their diet, suggesting their blinding was intact. Nonetheless, we cannot exclude the possibility that some patients may have deduced the nature of their diet.
In summary, we found that patients with IBS who consumed a low FODMAP diet had a significant improvement in symptoms and changes in their metabolome suggesting that immune signalling and alterations in the microbiota could be important mechanistic pathways in subsets of patients with IBS. Metabolic profiling of urine samples from patients with IBS provides a practical means of testing and this study sets the stage for larger trials designed to examine how changes in histamine and possibly other metabolites correlate with symptoms and whether they provide important biomarkers for enriching clinical studies. Breath tests may have the potential to identify patients who will benefit from the reduction of FODMAPs if measurements could detect individuals who have an exaggerated response to a FODMAP, such as lactulose. However, our study suggests that lactulose alone is not sufficient and further studies are needed to examine whether a combination of specific FODMAPs would be predictive. We also found evidence however that low FODMAP diets could potentially have long-term negative consequences, as reported by others. The current recommendation at most centres is that a strict restriction of FODMAPs is not the long-term goal of the diet. Thus identifying the one or more offending FODMAPs in specific patients and examining whether less restrictive reductions mitigate the negative impact on the microbiota will be important.
Acknowledgments
The authors thank Dr Oscar Cruz Pereria for his input in study design.
References
Footnotes
Contributors KM and SV contributed to the design of the study. KM, SV and DER contributed to analysis of patient symptoms and metabolome; TS analysed patient diets. FD analysed patient characteristics. AHK and KM analysed urinary metabolites. GDP and PB analysed the microbiome and correlated with urinary metabolites. All authors contributed to writing of the manuscript.
Funding GDP was supported by an Actavis-CAG-CIHR postdoctoral fellowship. SV was supported by a CIHR operating grant.
Competing interests None declared.
Ethics approval Health Sciences Research Ethics Board at Queen’s University.
Provenance and peer review Not commissioned; externally peer reviewed.