Article Text

Abstract
Objective Non-alcoholic fatty liver disease (NAFLD) is a frequent complication of morbid obesity, but its severity varies greatly and thus there is a strong need to better define its natural history in these patients.
Design Liver biopsies were systematically performed in 798 consecutive patients with severe obesity undergoing bariatric surgery. Histology was compared with clinical, biological, anthropometrical and body composition characteristics.
Results Patients with presumably normal liver (n=179, 22%) were significantly younger at bariatric surgery than patients with NAFLD (37.0 vs 44.4 years, p<0.0001). However, both groups showed quite similar obesity duration, since patients with presumably normal liver reported the onset of obesity at a significantly younger age than those with NAFLD (14.8 vs 20.0 year, p<0.0001). The trunk/limb fat mass ratio increased according to liver disease severity (presumably normal liver: 1.00, steatosis: 1.21, non-alcoholic steatohepatitis (NASH): 1.34, p<0.0001), although the total body fat mass decreased (presumably normal liver: 50%, steatosis: 49.1%, NASH: 47.4%, p<0.0001). The volume of subcutaneous adipocytes increased according to severity of liver disease but only in female patients (presumably normal liver: 8543 picolitres, steatosis: 9156 picolitres, NASH: 9996 picolitres).
Conclusions These results suggest that young adults are more prone to store fat in subcutaneous tissue and reach the threshold of bariatric surgery indication before their liver is damaged. A shift of fat storage from subcutaneous to visceral adipose tissue compartment is associated with liver damages. Liver might also be targeted by subcutaneous hypertrophic adipocytes in females since hypertrophic adipocytes are more exposed to lipolysis and to the production of inflammatory mediators.
- MORBID OBESITY
- LIVER BIOPSY
- FATTY LIVER
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Obesity is associated with an increasing risk of non-alcoholic fatty liver disease (NAFLD).
A large body of literature is on histology of liver lesions in patients with severe obesity.
Visceral fat is involved in liver disease through release of free fatty acid and adipokines.
What are the new findings?
Young patients with obesity reach the threshold of bariatric surgery before developing liver disease because of a greater expandability of subcutaneous adipose tissue.
Severity of liver disease is correlated with the ratio between trunk and extremity fat mass.
Hypertrophy of subcutaneous adipocyte in female, not in male, might contribute to severity of liver disease.
Histological lesions of NAFLD in patients with severe obesity cover a continuous spectrum of features that cannot be easily classified using the usual classification per category (NAFLD vs non-alcoholic steatohepatitis).
How might it impact on clinical practice in the foreseeable future?
Evaluation of fat distribution in patients who are morbidly obese may contribute to predict severity of liver disease.
A histological score such the steatosis, activity and fibrosis score may better describe the complexity of liver histology in patients who are morbidly obese.
Introduction
The incidence of obesity has dramatically increased over recent decades (WHO: The World Health Report 2002—Reducing Risks, Promoting Healthy Life 2009; Available from: http://www.who.int/whr/2002/en/) and constitutes a serious worldwide issue mainly because of its association with type 2 diabetes mellitus, coronary heart disease and non-alcoholic fatty liver disease (NAFLD).1 NAFLD consists of a wide histological spectrum of lesions including steatosis, inflammation, hepatocellular injury and fibrosis. These lesions are present in various combinations and of varying severity. Following the seminal description by Ludwig et al2 in 1980, patients with NAFLD have been divided into two main categories: non-alcoholic fatty liver (NAFL) and non-alcoholic steatohepatitis (NASH). This segregation was supported by large epidemiological studies showing significant differences in prognosis. Patients with NASH displayed higher risks of fibrosis progression, as well as both overall and liver-related mortality, compared with patients with NAFL.3–5 Therefore, patient eligibility in NAFLD clinical trials is mainly been based on histological NASH diagnosis.6
However, this dual classification has several limitations since both NAFL and NASH categories cover a heterogeneous group of diseases. To circumvent this limitation, several scoring systems have been proposed. The NASH Clinical Research Network within the National Institute of Diabetes and Digestive and Kidney Diseases proposed the NAFLD Activity Score (NAS), comprising the unweighted sum of semi-quantitative measures of steatosis, hepatocellular ballooning and lobular inflammation.7 Recently, the Fatty Liver Inhibition of Progression (FLIP) European pathology consortium proposed independent scoring of steatosis (S), activity (A) and fibrosis (F) within the SAF score.8 The SAF score has shown to be highly reproducible between pathologists, either between expert ones or general practicing pathologists after a short training period.9
We herein took advantage of our large prospective database of liver biopsies in patients with severe obesity, which were systematically obtained during bariatric surgery, and accompanied detailed phenotypical and histopathological characterisation. This study highlighted new correlations between liver histology and clinical, biological, demographic, anthropometrical and body composition characteristics that may further clarify the natural history of NAFLD in severe obesity.
Materials and methods
Patients
The study enrolled 798 obese subjects included in a bariatric surgery programme, prospectively and consecutively recruited by the Nutrition Department from Hotel-Dieu and Pitié-Salpêtrière Hospitals (reference centres for medical and surgical care of obesity in Paris, France). All patients had undergone surgical liver biopsy during the bariatric intervention. Subjects were aged >18 years, and fit the criteria for obesity surgery according to current guidelines, that is, body mass index (BMI) ≥40 or ≥35 kg/m2 and at least one comorbidity (hypertension, type 2 diabetes mellitus, dyslipidemia or obstructive sleep apnoea syndrome). Preoperative evaluation included detailed medical history, physical examination and nutritional, metabolic, cardiopulmonary and psychological assessments. Exclusion criteria included autoimmune, inflammatory or infectious diseases, viral hepatitis, cancer, known alcohol consumption (>20 g/day) or kidney diseases. All subjects gave written informed consent. The local ethics committee approved the present clinical investigations.
Clinical and laboratory assessment
Body weight was measured to the nearest 0.1 kg with subjects in indoor clothing and no shoes. BMI was calculated as weight divided by height squared. Body composition was estimated by whole-body fan-beam dual-emission X-ray absorptiometry (DXA) scanning (Hologic Discovery W, software V.12.6, 2; Hologic, Bedford, Massachusetts, USA), as previously described.10 Body regions (eg, arms, legs, trunk) were delineated with the use of specific anatomical landmarks as described elsewhere.11 Analysed DXA variables were total, trunk and appendicular (limbs) fat mass (kg). Relative body fat content was expressed as percent body fat (total fat mass (kg)/body weight (kg)×100). In agreement with American Diabetic Association criteria, diabetes was defined according to a glycaemia >7 or >11 mM 2 hours after oral glucose tolerance test or the use of antidiabetic drugs. Hypertension and dyslipidemia was identified according to new metabolic syndrome definition cut-offs from the International Diabetes Federation (http://www.idf.org/webdata/docs/MetS_def_update2006.pdf).
Sera were collected from venous blood following an overnight fast. Serum glucose, triglycerides, total cholesterol and high-density lipoprotein cholesterol, alanine aminotransferase (ALT), aspartate aminotransferase (AST) and γ-glutamyl transpeptidase were measured. Serum insulin concentrations were determined by Bi-INSULIN IRMA (CisBio International, Gif-sur-Yvette, France) as previously described.12
During the preoperative evaluation, adipose tissue samples were taken by needle aspiration from the abdominal subcutaneous fat depot in 668 patients. After adipocyte isolation and collagenase digestion, adipocyte diameter was measured as previously described.13 ,14 The mean fat cell volume was computed according to the formula by Hirsch and Gallian.15 Patients whose adipocyte measurement could not be performed did not differ significantly from those with adipocyte measurement regarding clinical data and liver lesions.
Liver biopsy
Surgical liver biopsies of the left lobe were systemically performed during bariatric surgery using the same standardised procedure with a scalpel blade. Each liver fragment measured at least 1 cm2 on cut section. Tissue samples were formalin-fixed and paraffin-embedded. Serial sections were stained with H&E, picrosirius red and Perls' iron stain. All biopsies were reviewed by a single liver pathologist. Evaluations were performed either using the category classification, NAS and SAF scores as previously described.8 ,9 SAF scoring independently assesses the steatosis grade (S), the activity grade (A) and the fibrosis stage (F), the latter staged according to the NASH Clinical Research Network definition.7 Categorical classification (either normal liver, NAFL or NASH) used the FLIP algorithm, which relies on a combination of elementary lesions to diagnose or exclude NASH.8 The SAF activity score (from A0 to A4) was calculated by adding grades of hepatocellular ballooning and lobular inflammation. Ballooning was graded from 0 to 2 (0: normal hepatocytes with cuboidal shape, sharp angles and pink eosinophilic cytoplasm; 1: presence of hepatocyte clusters with a rounded shape and pale cytoplasm, usually reticulated, where sizes are similar to normal hepatocytes even though the shape is different; 2: as for grade 1, but where there were also at least one enlarged ballooned hepatocyte—at least a twofold size increase compared with normal cells—within a grade 1 ballooning hepatocyte cluster). Lobular inflammation was defined as a focus of two or more inflammatory cells within the lobule, either organised as microgranulomas or located within the sinusoids. Foci were counted at 20× magnification (grade 0: none; 1:<2 foci per lobule; 2: >2 foci per lobule).
Statistics
Bioclinical variables are reported as mean and 95% CI or frequency, as appropriate. Distributions of continuous variables were examined for skewness and kurtosis and were logarithmically transformed where appropriate. The χ2 test was used for categorical variables and the Student's t-test or analysis of variance (ANOVA) for continuous variables, where appropriate, to evaluate statistical significance.
Results
Histology and correlation with clinicobiological variables
Baseline characteristics of the 798 patients are shown in table 1. Most patients were female (78%) and of Caucasian origin (73.5%). Mean BMI was 47.5 kg/m2. Diabetes was detected in 39%, high blood pressure in 48%, dyslipidemia in 50% and sleep apnoea in 32% of the cohort.
Cohort baseline characteristics including 798 patients who are morbidly obese before bariatric surgery
Among the 619 patients with NAFLD, 340 (55%) had NAFL and 279 (45%) had NASH. The number of patients according to their component SAF scores and disease category is provided in table 2. Severe steatosis (S3), marked activity (A3 or A4) and advanced fibrosis (F3 or F4) were observed in 177 (22%), 143 (18%) and 59 (7%) of all patients, respectively.
Distribution of SAF score per disease category
Within the cohort, 141 patients had strictly normal liver via histological analysis (SAF score: S0A0F0) and 38 patients had no steatosis but mild lesions, either mild activity (S0A1F0; hepatocyte clarification/ballooning, n=2; or lobular inflammation, n=9), or mild fibrosis (S0A0F1, n=25 and S0A0F2, n=3) with one patient having combined mild activity and mild fibrosis (S0A1F1). Since we did not observe any significant differences in clinical or biological parameters between patients with histologically normal livers or those with no steatosis but minimal lesions (see online supplementary table S1), these patients were then grouped into a single group called ‘presumably normal liver’. Patients with severe obesity and presumably normal liver were significantly younger, more often female, of non-Caucasian origin, and had fewer obesity comorbidities than those with NAFLD (table 3). Indeed, 153 patients (85%) with presumably normal liver had either no or only one comorbidity (type 2 diabetes mellitus, hypertension, dyslipidemia), while 26 patients (15%) had more than one associated comorbidity, a distribution that was significantly different from the NAFLD group (0 or 1 cofactor: n=338, 55% vs ≥2 associated cofactors: n=281, 45%, p<0.0001).
supplementary tables
Comparison of baseline characteristics of patients with presumably normal liver and NAFLD
NAFL was observed in 340 patients. This group included patients with obesity with steatosis alone, or steatosis with mild lesions but not NASH. Within this group, steatosis was grade 1 in 48% of cases (n=166), grade 2 in 33% of cases (n=112) and grade 3 in 19% of cases (n=62). Only 87 individuals (26%) had pure steatosis. Others had steatosis either associated with mild activity (grade 1 lobular inflammation, n=69 or ballooning, n=98) and/or mild fibrosis (F1; n=145, F2; n=42). A further 18 cases had grade 2 activity (either inflammation only but grade 2, n=10 cases; or grade 2 ballooning without inflammation, n=8 cases). Septal fibrosis was identified in 10 cases (F3). This group of patients with steatosis and associated lesions but no NASH had significantly higher ALT (p<0.001), more dyslipidemia (p<0.05), higher fasting insulin levels (p<0.01) than those with steatosis alone (see online supplementary table S2).
NASH was confirmed in 279 patients as defined by the FLIP algorithm. A steatosis grade ≥2 or a fibrosis stage ≥2 was more common in biopsies with NASH than in those with NAFL (S ≥ 2, 88% in NASH vs 54% in NAFL, p<0.0001, F ≥ 2, 48% in NASH vs 15% in NAFL, p<0.0001).
Among patients with NASH, 136 (49%) had an activity score graded to 2, and 143 (51%) had a score >2. Patients with SAF activity scores >2 were significantly less often of Caucasian origin (p<0.05), often had more type 2 diabetes mellitus (p<0.05), higher ALT (p<0.001) and insulin levels (p<0.001) than those with A=2 (see online supplementary table S3).
When dividing liver disease into five subgroups (healthy liver, pure steatosis, steatosis with mild associated lesions, NASH with activity score=2 and NASH with activity score >2), AST and ALT progressively increased (ANOVA p<0.01 for ALT and AST) (figure 1A, B). Accordingly, the prevalence of type 2 diabetes mellitus, hypertension and dyslipidemia significantly increased with the severity of liver disease (figure 1E, F).
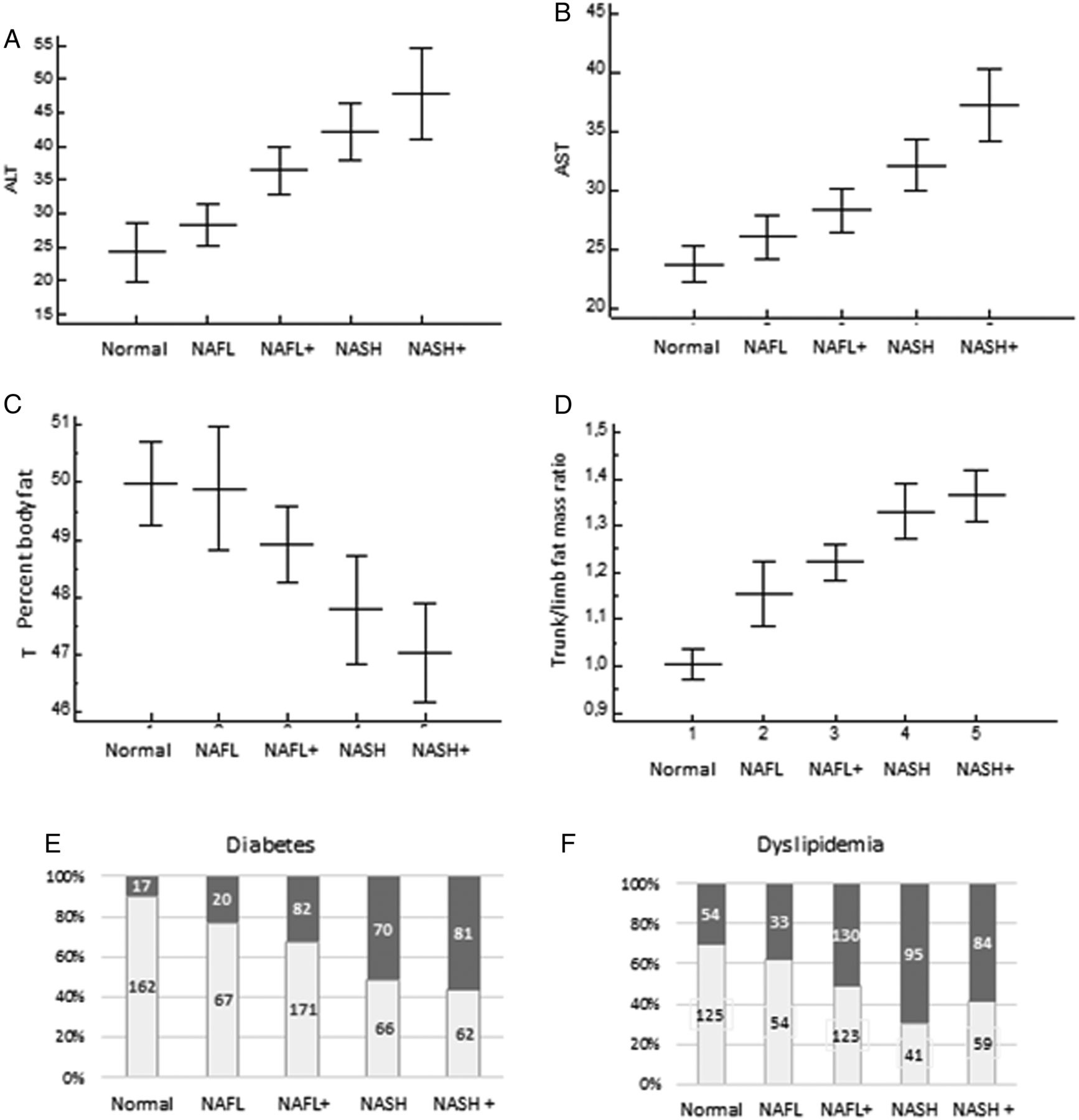
Correlation between subgroups of liver diseases with alanine aminotransferase (ALT) (A), aspartate aminotransferase (AST) (B), percentage body fat mass (C), trunk/limb fat mass ratio (D), percentage of type 2 diabetes mellitus (E, in grey) or dyslipidemia (F, in grey). NAFL, non-alcoholic fatty liver; NASH, non-alcoholic steatohepatitis.
Natural history
Patients with presumably normal liver were significantly younger than the overall NAFLD group (presumably normal liver: 37.0 years (35.3 to 38.7); NAFLD: 44,4 years (43.5 to 45.3), p<0.0001) (table 3). Interestingly, the younger age of patients with presumably normal liver at bariatric surgery was not related to shorter obesity duration but to an earlier onset of obesity. Indeed, for 445 patients with documented obesity onset, obesity was diagnosed at a mean age of 14.8 years (12.6 to 16.9) in patients with histologically presumably normal liver at bariatric surgery, significantly earlier than in those with NAFLD (20.0 years (18.8 to 21.2), p<0.0001). Therefore, the duration of obesity exposure was not significantly different between the group with presumably normal liver and those with NAFLD (presumably normal liver: 22.1 years (20.0 to 24.2), NAFLD: 24.0 years (22.9 to 25.0), not significant (ns)).
Compared with patients with NAFL, patients with NASH were older at the time of bariatric surgery (46.3 years (44.9 to 47.6) for NASH vs 42.9 years (41.7 to 44.1) for NAFL, p<0.001, table 4). In the 243 patients for whom the age of obesity onset was known, there was no significant difference between patients with NAFL and those with NASH (obesity onset: 20.0 years (18.3 to 21.6) in NAFL vs 20.8 years (18.8 to 22.8) in NASH, ns). Since patients with NASH were significantly older at bariatric surgery than those with NAFL, it follows that NASH develops after a longer exposure to obesity than NAFL (duration of obesity: 22.9 years (21.6 to 24.2) in NAFL vs 26.2 years in NASH (24.5 to 27.9), p<0.001).
Baseline characteristics of patients who are morbidly obese with NAFL and NASH
Relationship between liver disease and adipose tissue
In the whole cohort, the percentage of DXA-measured total body fat decreased progressively with increasing steatosis grade (S0: 50% (49.2% to 50.7%); S1: 49.4% (48.7% to 50.1%); S2: 48.2% (47.5% to 48.9%); S3: 47.5% (46.6% to 48.3%), ANOVA p<0.001, figure 2A). Fat mass distribution was also significantly different according to steatosis grade. Indeed, the trunk/limb fat mass ratio (figure 2B) increased significantly with the steatosis grade (ANOVA p<0.001). These results suggest that liver steatosis is associated with a change in fat repartition towards ectopic storage in the liver, rather than a simultaneous increase of fat depots both in adipose tissue and in the liver. Similarly, patients with NASH had lower percentages of total body fat mass (47.4% (46.8% to 48.0%)) than those with NAFL (49.1% (48.6% to 49.7%), p<0.0001) or those with presumably normal liver (50.0 (49.2 to 50.7), p<0.0001).

Correlation between steatosis grade and (A) percent of body fat (B) trunk/limb fat mass ratio (*p<0.05, **p<0.01, ***p<0.001).
Conversely, the trunk/limb fat mass ratio increased progressively from healthy liver (1.00 (0.97 to 1.04)) to NAFL (1.21 (1.17 to 1.24), p<0.0001) when comparing with presumably normal liver, and to NASH (1.34 (1.31 to 1.39), p<0.0001 in comparison with NAFL) (table 4). When dividing liver disease into five subgroups (healthy liver, pure steatosis, steatosis with mild associated lesions, NASH with activity score=2 and NASH with activity score >2), the percentage body fat decreased (ANOVA p<0.01) while trunk/limb fat ratio increased (ANOVA p<0.01, figure 1C, D).
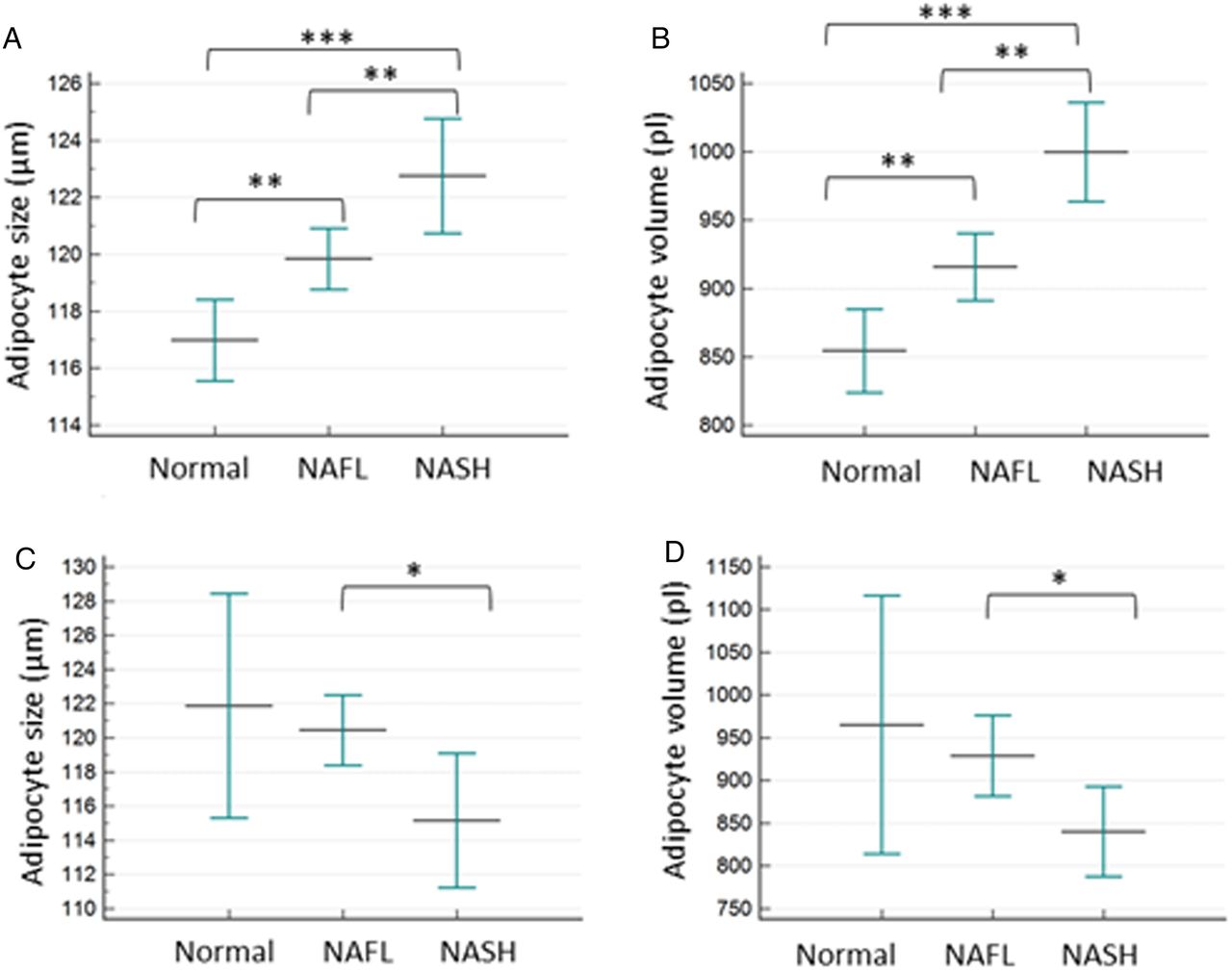
Size and volume of adipocytes from the subcutaneous tissue were compared according to liver status. Diameter and volume significantly increased with severity of liver disease but only in females (size: 1170 µm (1155 to 1184) in presumably normal liver, 1198 µm (1187 to 1209) in NAFL (p<0.01 vs presumably normal liver), 1227 µm (1207 to 1247) in NASH (p<0.01 vs NAFL); volume: 8543 pl (8237 to 8848) in presumably normal liver, 9156 pl (8911 to 9402) in NAFL, p<0.01, 9996 pl (9633 to 10 360) in NASH. Such correlations were not found in male patients but the number of male distributed in each liver category was also lower (figure 3). No significant correlation was found between size or volume of adipocytes and age of patients at bariatric surgery (data not shown).
{kind=link}
{kind=link}
{kind=link}
Correlation between severity of liver disease and adipocyte size (A and C), adipocyte volume (B and D) within female (A and B) and male patients (C and D). *p<0.05, **p<0.01, ***p<0.001. NAFL, non-alcoholic fatty liver; NASH, non-alcoholic steatohepatitis.
Discussion
The clinical condition of severe obesity has continued to progress worldwide, however, bariatric surgery has proven to be efficient in reducing mortality, cardiometabolic risks and liver lesions.16 In this French cohort, liver biopsies were systematically prospectively performed during bariatric surgery—independent of clinical or biological liver symptoms—in a large number of well-phenotyped patients with severe obesity.
Since bariatric surgery was performed according to the same standardised international guidelines throughout the study, this cohort constitutes an unbiased overview of liver lesions in patients with severe obesity, who are candidates for obesity surgery. Furthermore, a single experienced liver pathologist performed all histological evaluation according to a validated and detailed systematic histological analysis using category classifications, NAS and SAF scores. Since a previous study has shown a low interobserver variation and a minimal intraobserver variation in assessing the SAF score components, we assume that this approach guarantees strong reliable histological assessment throughout the duration of the study. Finally, sampling error due to superficial fragments (as often seen with needle biopsy) was limited as much as possible, as biopsies were collected by experienced surgeons well aware of surgical biopsy constraints for their interpretation.
Our results initially indicated that among patients with severe obesity, 22% had histologically presumably normal liver.
The reported percentage of normal liver in the patients who are morbidly obese is highly variable in the literature, a difference that might be related to variability in patient recruitment.17–23 Since this population was exclusively recruited through the same obesity clinic and the same bariatric surgery programme over a number of years, it differs from other cohorts of patients recruited through hepatology departments, and thus may reflect a more unbiased spectrum of liver lesions in severe or morbid obesity. To some extent, severe obesity with normal liver is comparable to metabolically healthy patients with obesity, which were described some 15 years ago, and whose prevalence rates have been reported to vary between 10% and 34% in patients with obesity.24 ,25
In some patients although there was no visible steatosis, there were occasional foci of inflammation or fibrosis. In the absence of steatosis, the prognostic value of these findings is uncertain and most probably benign, hence the term ‘presumably normal’ when describing these livers. However, long-term follow-up of these patients will be necessary to rule out a theoretical progression of liver injury in spite of the absence of steatosis—a scenario that would be at odds with the current pathogenic paradigms of NAFLD/NASH.
Our study showed that the patients with presumably normal liver were younger at the time of bariatric surgery than patients with NAFLD, and more often tended to be women. However, patients with presumably normal liver reported obesity onset significantly earlier than those with NAFLD and, as a consequence, patients with presumably normal liver and NAFLD show similar obesity durations, but differ in age. Altogether, these results suggest that young adults are more prone to reach the threshold of bariatric surgery indication before liver damage occurs. This might be related to the ‘adipose-tissue expandability hypothesis’ which proposes that the storage capacity of subcutaneous adipose tissue is limited and when the threshold is reached, the flux of excess lipids is sent to ectopic sites, thus promoting metabolic complications.26 Younger patients may have higher subcutaneous adipose tissue expandability, with better ability to trap and retain free fatty acids in their subcutaneous adipose tissue. Indeed, lipid storage in the liver (steatosis) was rare in younger individuals with severe obesity, while it was more common in older individuals. This suggests that adipose tissue's ‘buffering capacity’ to store excessive fat may be progressively lost with increasing age. However, in other populations (ie, patients who are not morbidly obese), young patients may have NASH and even advanced NASH or cirrhosis.27 Therefore, it is highly likely that age is not the only determinant of adipose tissue dysfunction, and that predisposed young individuals can still exhibit reduced adipose tissue storage capacity.
The progressive increase in trunk/limb fat ratio from presumably normal liver to advanced NAFLD and its correlation with steatosis grade may support the hypothesis that fat storage shifts from subcutaneous to other compartments such as the visceral adipose tissue and the liver. However, we did not directly measure the abundance of visceral fat and trunk/limb ratio is an indirect estimate.26 Expansion of visceral adipose tissue and an increased flux of free fatty acids to the liver through the portal blood flow might connect visceral adipose tissue expansion to NAFLD development.28 Accumulation of inflammatory cells in visceral tissue is associated with NAFLD severity in morbid obesity. This also suggests a potential contribution of visceral fat to inflammation and fibrosis in the liver through lipotoxicity and the release of bioactive molecules including hormones, cytokines and adipokines into portal blood.29 ,30 Similarly, a recent study has shown links between phospholipid profiling, particularly glycerophosphoglycerols, and NASH signatures in morbid obesity.31
In patients with obesity, fat mass can expand by increasing the average fat cell volume (hypertrophy) and/or the number of adipocytes (hyperplasia). While adipocyte hyperplasia is considered an adaptive mechanism, adipocyte hypertrophy per se is seen as a key detrimental event associated with in vitro and in vivo loss of insulin sensitivity in both lean and obese conditions compared with adipocyte hyperplasia.32–34 Subjects with larger adipocytes have a higher incidence of lipolysis and elevated levels of pro-inflammatory factors including leptin, interleukin (IL)-6 and IL-8, and reduced levels of adiponectin.35 Furthermore, hypertrophic adipocytes in both subcutaneous and abdominal fat compartments are characterised by expression of genes coding for proteins involved in adipocyte metabolism or inflammation.36 Interestingly, our study showed significant increases in both size and volume of subcutaneous adipocytes (hypertrophy) in female patients with NASH compared with those with NAFL and healthy liver. Therefore, our study is the first to demonstrate a potential link between adipocyte hypertrophy in the subcutaneous areas and the severity of liver disease, where adipocyte hypertrophy seems thus associated with a deleterious effect on liver parenchyma in obese female patients. Evaluation of visceral adipocyte size may strengthen this hypothesis.
Classification of NAFLD by categories (presumably normal liver, NAFL and NASH) is obviously a very reductive approach since this study demonstrates that each of these three categories were heterogeneous, both in terms of histology and regarding clinical and biological phenotypes. Indeed, within the NAFL group, only a minority (26%) had pure steatosis while most had associated but mild lesions (activity and/or fibrosis). Interestingly, some clinical and biological parameters were significantly different when comparing patients with pure steatosis to those with steatosis and activity and/or fibrosis but no NASH. This supports the notion that NAFL is rarely pure steatosis but is actually a highly clinicopathologically heterogeneous group with different lesions, and that can be fully histologically described using the SAF score. Similarly, the NASH category contains both patients with bona fide NASH but relatively mild activity (A=2 with ballooning=1 and inflammation=1) and a group with more severe disease (A>2) also with some clinical and biological differences.
Altogether, this raises the question whether it is still relevant to split NAFLD into NAFL and NASH, whereas histological, clinicobiological patterns and anthropometric data clearly show a continuum within the NAFLD group. The SAF may help to more accurately describe the spectrum of lesions within the NAFLD group of patients. This tool would certainly facilitate follow-up evaluation of histological lesions, especially in the context of clinical trials and repeated biopsies.
Our study demonstrates that NAFLD is a very heterogeneous disease in a large representative cohort of patients with severe obesity and patients who are morbidly obese. We herein point at the importance of body fat repartition linked to the severity of the diseases. Furthermore, adipose tissue characteristics (ie, adipocyte size and volume) also seem to be associated with NAFLD severity.
Acknowledgments
We thank Patricia Bonjour and Nathalie Colnot for their assistance with the histological studies. We thank Florence Marchelli for the construction and maintenance of the database, and Valentine Lemoine for patient recruitment and follow-up.
References
Footnotes
Contributors PB, JT, KC conceived and designed the study. PB drafted the manuscript. JT, JAW, CP, J-MO collected the patients clinical and laboratory data. PB, JT, KC contributed to the analysis of the data. VP and VR contributed to the writing of the manuscript. AT and J-LB operated the patients. All authors critically revised the manuscript and approved its final version.
Funding The study was supported by the Assistance Publique-Hôpitaux de Paris, and the Direction of Clinical Research (CRC) for clinical investigation (PHRC 02076 to KC, CRC P050318 to CP and CRCCRCCRC-FIBROTA to JAW and KC), as well as the Fondation pour la Recherche Médicale, Horizon 2020 EPoS project, grant 634413, and the National Agency of Research (ANR Adipofib, and the national programme ‘Investissements d'Avenir’ with the reference ANR-10-IAHU-05).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The local ethics committee of University Pierre and Marie Curie.
Provenance and peer review Not commissioned; externally peer reviewed.