Article Text

Abstract
Background The National Health Service Bowel Cancer Screening Programme (BCSP) in England uses a guaiac-based faecal occult blood test (gFOBt). A quantitative faecal immunochemical test (FIT) for haemoglobin (Hb) has many advantages, including being specific for human blood, detecting Hb at a much lower concentration with a single faecal sample and improved uptake.
Methods In 2014, a large comparative pilot study was performed within BCSP to establish the acceptability and diagnostic performance of FIT. Over a 6-month period, 40 930 (1 in 28) subjects were sent a FIT (OC-SENSOR) instead of a gFOBt. A bespoke FIT package was used to mail FIT sampling devices to and from FIT subjects. All participants positive with either gFOBt or FIT (cut-off 20 µg Hb/g faeces) were referred for follow-up. Subgroup analysis included cut-off concentrations, age, sex, screening history and deprivation quintile.
Results While overall uptake increased by over 7 percentage points with FIT (66.4% vs 59.3%, OR 1.35, 95% CI 1.33 to 1.38), uptake by previous non-responders almost doubled (FIT 23.9% vs gFOBt 12.5%, OR 2.20, 95% CI 2.10 to 2.29). The increase in overall uptake was significantly higher in men than women and was observed across all deprivation quintiles. With the conventional 20 µg/g cut-off, FIT positivity was 7.8% and ranged from 5.7% in 59–64-year-old women to 11.1% in 70–75-year-old men. Cancer detection increased twofold and that for advanced adenomas nearly fivefold. Detection rates remained higher with FIT for advanced adenomas, even at 180 µg Hb/g.
Conclusions Markedly improved participation rates were achieved in a mature gFOBt-based national screening programme and disparities between men and women were reduced. High positivity rates, particularly in men and previous non-respondents, challenge the available colonoscopy resource, but improvements in neoplasia detection are still achievable within this limited resource.
- COLORECTAL CANCER SCREENING
- EPIDEMIOLOGY
- COLORECTAL NEOPLASIA
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Guaiac-based faecal occult blood test (gFOBt) screening for bowel cancer reduces bowel cancer mortality in those screened by 25%.
Uptake of gFOBt in the National Health Service (NHS) Bowel Cancer Screening Programme (BCSP) was 58.2% in the fiscal year 2014/2015 and was lower in men, the deprived population and in previous non-responders.
The faecal immunochemical test (FIT) for haemoglobin is recommended in the European Guidelines on colorectal cancer screening.
FIT measures human haemoglobin and at lower concentrations than gFOBt. Using an automated technique, FIT provides a quantitative result that enables users to determine an acceptable positivity rate.
Studies have shown increased uptake of FIT compared with gFOBt.
What are the new findings?
FIT can enable marked improvements in uptake and clinical outcomes in a well-established screening programme where subjects have received up to seven previous invitations to screening.
The adoption of an innovative package for mailing and returning the FIT device may have contributed to improved uptake.
Uptake increased from 59.3% with gFOBt to 66.4% with FIT, an increase greater than has been reported previously in an established screening programme.
The increase in uptake was greatest in previous non-responders (FIT 23.9% vs gFOBt 12.5%) and was higher in men than in women. This effect has not been reported previously.
Uptake was increased across all deprivation quintiles (6.6 percentage points in the least deprived and 7.8 percentage points in the most deprived).
FIT cut-off concentrations up to 40 μg Hb/g faeces achieved increased detection rates of cancer and up to 180 μg Hb/g faeces increased detection of advanced adenomas.
How might it impact on clinical practice in the foreseeable future?
Replacement of gFOBt with FIT in the NHS BCSP would result in a markedly increased uptake, particularly and importantly in some ‘hard-to-reach’ groups.
The increase in uptake due to FIT has to be considered alongside FIT positivity when determining a cut-off concentration appropriate for the available colonoscopy resource.
The design of packages used to distribute and return FIT devices should be considered by programme organisers.
Data on the clinical effect of different cut-off concentrations in population subgroups will help maximise the clinical benefit within a prescribed colonoscopy resource in existing screening programmes.
Improved clinical outcomes can still be achieved at high cut-off concentrations.
Development of a screening algorithm that combines FIT concentrations with other risk indicators (age, sex, screening history, deprivation) may enable improved clinical outcomes within the same colonoscopy resource.
Background
Randomised controlled trials have shown that screening using a guaiac-based faecal occult blood test (gFOBt) can reduce mortality from bowel cancer.1–5 The National Health Service (NHS) Bowel Cancer Screening Programme (BCSP) in England currently uses a gFOBt and invites men and women aged 60–74 (inclusive) for screening every two years. The programme was rolled out across England in 2006 and had achieved national coverage for 60–74 year olds in 2015. While the uptake of gFOBt-based screening in the UK compares well with that in most other countries, it is low relative to the uptake among women in population-based breast or cervical screening programmes.6 ,7 The uptake of gFOBt in England is higher in women than men, increases with age from 60 to 69 years and decreases with increasing levels of deprivation.8
Reported reasons for non-participation include low perceived relevance of screening and avoiding or delaying decision-making, but also having some degree of intention to take part but failing to do so because of practicalities.7 ,9 ,10 The gFOBt adopted by the NHS BCSP requires six faecal samples, two from each of three separate bowel motions, and the partially completed kit must be stored by the participant until all three bowel motions have been sampled. It is likely that the gFOBt sampling method and the screening algorithm used in England, whereby up to three gFOBt kits may be required to achieve a definitive screening test result,6 are important deterrents to bowel cancer screening.11
An alternative faecal occult blood test, the ‘faecal immunochemical test’ (FIT) for haemoglobin (Hb), has many advantages including requiring a single faecal sample and being specific for human blood, which it can detect at much lower concentrations than is possible with gFOBt. The collection of the faecal sample is much simpler, using a stick that is reinserted and hygienically sealed into a small tube containing a preservative buffer solution. The automated FIT analysers have the advantage of providing an objective quantitative faecal Hb concentration and enable colonoscopy referral to be based on a locally selected FIT cut-off concentration, whereas the determination of a positive gFOBt result is by subjective visual interpretation and has a single, manufacturer-determined, cut-off concentration. FIT kits and the cost of mailing are, however, marginally more expensive than for gFOBt.
Many studies have shown higher uptake of FIT compared with gFOBt in average-risk populations.12–19 FIT has been adopted for organised population-based screening in Italy, Slovenia, Australia, the Netherlands, France, Malta and Southern Ireland,11 and in February 2015 the Scottish government announced plans to change from gFOBt to FIT screening.20
In 2014, the NHS BCSP performed a pilot study to examine the acceptability and diagnostic performance of using FIT in an established screening programme in England. The aims of the epidemiological evaluation of the pilot were to compare FIT and gFOBt in terms of uptake and the proportion of tests that are positive (positivity), both overall and within demographic subgroups, together with the uptake of colonoscopy in test-positive subjects, and detection rates and positive predictive values (PPVs) for cancer, adenoma and advanced adenoma. As a pilot for a change to a national programme, the study also explored other practical issues pertinent to the adoption of FIT. The application of a low FIT cut-off concentration of 20 µg Hb/g faeces with a relatively high positivity enabled assessment of the effect of a range of higher cut-off concentrations on screening outcomes, with positivity rates below and above that currently observed in the gFOBt-based programme.
Methods
The study used the routine screening population invited by either of two of the five English BCSP Hubs (the Midlands and North West and the Southern Hub). Each of these Hubs covers a large area of England and invites 1.1–1.2 million subjects for gFOBt screening each year. The study population was therefore drawn from over half of the eligible population in England. Participants with positive FIT or gFOBt results were managed according to the usual BCSP protocol and given a clinic appointment for follow-up in their local Screening Centre (18 Centres in the Southern Hub, 15 Centres in the Midlands and North West Hub). The sample size of the pilot was determined to provide 80% power to detect a difference between 60% and 62% uptake at the 5% significance level in subgroups of the population by age and sex.
The FIT system used for the pilot was the OC-SENSOR sampling tube (third-generation buffer) and OC-SENSOR Diana analyser (Eiken Chemical, Japan, supplied by Mast Diagnostics, Bootle, UK) and the gFOBt was Hema-Screen (Immunostics, New Jersey, USA, supplied by Alpha Laboratories, Eastleigh UK). A sensitive FIT cut-off concentration of 20 µg Hb/g faeces (equivalent to 100 ng Hb/mL buffer with the OC-SENSOR sampling tube) was applied by the Hub laboratories to enable the pilot to explore the practical and clinical implications of applying a wide range of FIT screening sensitivities. To minimise the impact upon the colonoscopy workload of using a more sensitive test regime than that of gFOBt, the BCSP's call/recall system was modified to ensure that only the first in every 28 routine invitations would be FIT. This regime was applied strictly to each Screening Centre throughout the period of the pilot. The order of invitations for each Centre is produced by the Bowel Cancer Screening System (BCSS) and is not influenced by subject demographics. This protocol ensured that assignment to either a FIT or gFOBt invitation was not influenced by age, sex, screening history or index of deprivation, making the assignment of subjects effectively random. All subjects are sent the routine pre-invitation letter 8 days before being sent a test kit. The pre-invitation letters for gFOBt and FIT were similar in content; the gFOBt group received the usual gFOBt information leaflet21 with the pre-invitation, while the FIT group received a version of the information leaflet appropriate for FIT with a single information sheet explaining that the individual had been invited as part of the FIT pilot and the rationale for study. No subjects allocated to one test type were subsequently offered or allowed to transfer to the other test.
FIT pre-invitations were distributed between 7 April and 10 October 2014. Each FIT device carried a unique subject-assigned barcode and was secured in a bespoke delivery box (figure 1) on which the instructions for use were printed and that, when resealed, enabled the used kit to be returned to the Hub for analysis. The box was designed to make the screening experience more attractive, with simple instructions for use on the box itself with no additional correspondence or packaging. To facilitate easier comparison of performance between OC-SENSOR and other FIT systems, Hb concentrations are reported in the World Endoscopy Organization recommended units µg Hb/g faeces.22

Faecal immunochemical test packing used in pilot study.
Data collection
All data required for the epidemiological evaluation were recorded on the BCSS database. Individual anonymised data for both FIT and gFOBt were provided to the Centre for Cancer Prevention, Queen Mary University of London; this paper includes data recorded on the BCSS database as at early April 2015 (26 weeks after the last pilot screening invitation).
All subjects served by either of the two Hubs were included in the analysis. Age was defined as the subject's age in years at the date of pre-invitation. Data were restricted to subjects aged 59–75 years, inclusive. A few subjects (82) who were <59 (n=45) or >75 years old (n=37) were excluded from the study (post-invitation corrections to subject's date of birth may account for these discrepancies). Subjects aged 59 (n=7352) or 75 years (n=83) were included because the date that pre-invitations were prepared and posted deviated by a few days from the birthday due to weekend birthdays and to routine measures designed to reduce random daily fluctuation in the rate of invitations. Uptake is reported by sex and age group, by socio-economic status and by screening history (prevalent first-time invitees (mostly 60-year-old subjects), prevalent previous non-responders and incident (previous responders)).
Uptake was calculated as the proportion of subjects sent the pre-invitation letter that were ‘adequately’ screened. Subjects who are sent pre-invitations and then advise the programme that they do not wish to be screened are not excluded from the calculation. Adequate screening is defined by the BCSP as having either a definitive negative (normal) or definitive positive (abnormal) test result and the uptake calculation includes in the numerator only subjects returning a first kit within 182 days of pre-invitation. Subjects recorded as not having returned a first test kit or failing to reach a definitive test result by not returning a repeat kit following a weak positive, spoilt kit or technical error, are defined as having not been adequately screened.
Positivity was calculated as the proportion of adequately screened subjects who had a definitive positive result. Colonoscopy uptake was calculated as the proportion of subjects with a positive test result who had a colonoscopy outcome/episode outcome recorded. (This included a small number of subjects who had an alternative diagnostic test such as flexible sigmoidoscopy or CT colonography).
Subjects with high-risk adenomas (≥5 adenomas or ≥3 adenomas at least one of which was ≥1 cm) or intermediate-risk adenomas (3–4 small adenomas or at least one ≥1 cm) were defined as having advanced adenomas.23 Detection rates were calculated using number of subjects adequately screened as the denominator and PPV calculations used the number of subjects with a definitive colonoscopy outcome as the denominator.
A composite indicator of area-based socio-economic deprivation for each subject according to their postcode of residence (index of multiple deprivation (IMD)) was derived using the English Indices of Deprivation 2010.24 The indices use census-derived indicators of income, education, employment, environment, health and housing at small-area (lower layer super output areas) level to generate a scale from 0 (least deprived) to 83.33 (most deprived). IMD quintiles were based on the recorded IMD scores for all subjects invited by either Hub during the pilot study. The IMD quintiles were Q1: 0.61–7.38; Q2: 7.39–11.77; Q3: 11.78–17.41; Q4: 17.42–27.97; Q5: 27.98–83.33. The IMD score was assigned and supplied by the Health and Social Care Information Centre based on subject postcode of residence.
The Southern Hub and the Midlands and North West Hub have distinct demographic differences as evidenced by their IMD profile,6 and the Midlands and North West Hub completed three rounds of biennial gFOBt screening of a small proportion of its population in a pilot programme prior to commencement of the National programme in July 2006,25 meaning that subjects will have received up to seven previous invitations.
Logistic regression was used to compare uptake, positivity and detection rates according to type of test kit in a univariate analysis, in subgroups stratified by age group, sex, Hub, screening episode and IMD quintile, and in a multivariate analysis adjusting for these factors. Interaction terms were included to assess the differential effect of kit type between subgroups. A p value <0.05 was used to define statistically significant findings.
Results
During the 6-month FIT pilot period, 40 930 subjects were invited to complete a FIT and 1 126 087 subjects were invited to complete a gFOBt. Table 1 gives the breakdown of subjects invited by screening episode, age group, sex, Hub and IMD quintile; the demographic and screening history profiles of the two groups were very similar.
Characteristics of populations invited
Uptake
The overall uptake was 66.4% for FIT compared with 59.3% for gFOBt (OR 1.35, 95% CI 1.33 to 1.38, p<0.001) (table 2). Uptake of both FIT and gFOBt was slightly higher in the Southern Hub, but the increase from gFOBt to FIT was similar in both Hubs. A total of 2.15% FIT invitees (881/40 930) and 2.17% gFOBt invitees (24 431/1 126 087) requested not to receive a kit after the pre-invitation and before mailing the kit.
Uptake of FIT and gFOBt by Hub and screening episode
The most marked difference in uptake between FIT and gFOBt was seen in the prevalent (previous non-responder) episodes (FIT 23.9% vs gFOBt 12.5%; OR 2.20, 95% CI 2.10 to 2.29) (table 2). The prevalent first-time invitees also showed a marked increase (61.2% vs 50.4%; OR 1.55, 95% CI 1.48 to 1.63) and in the ‘compliant’ population (those with incident episodes) uptake increased to 90.1% (90.1% vs 85.8%; OR 1.50, 95% CI 1.43 to 1.57).
The increase in uptake was significantly greater in men (absolute difference 8.1% (FIT 64.5% vs gFOBt 56.4%; OR 1.41, 95% CI 1.36 to 1.45)) than women (absolute difference 6.0% (68.1% vs 62.1; OR 1.31, 95% CI 1.27 to 1.34)) (figure 2). The differential uptake between men and women was reduced from 5.7 percentage points with gFOBt to 3.6 percentage points with FIT. In men aged 59–64 years, there was an absolute difference of 10.6% (60.7% vs 50.1%, OR 1.54 (95% CI 1.47 to 1.61)), although that age group has a large proportion of prevalent first-time invitees and the increase in uptake did not vary significantly by age group in the multivariate analysis (p value for interaction 0.22).
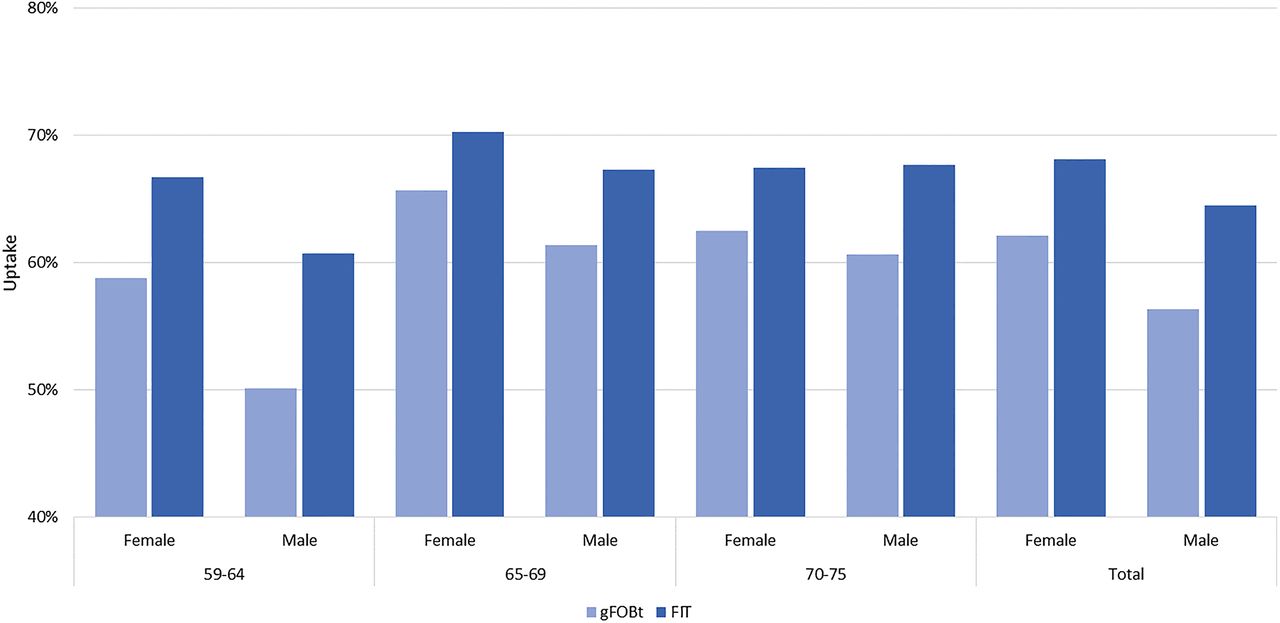
Uptake of faecal immunochemical test (FIT) and guaiac-based faecal occult blood test (gFOBt) by age group and sex.
| 59–64 | 65–69 | 70–75 | Total | |||||
|---|---|---|---|---|---|---|---|---|
| Female | Male | Female | Male | Female | Male | Female | Male | |
| OR (FIT vs gFOBt) | 1.40 | 1.54 | 1.23 | 1.30 | 1.24 | 1.36 | 1.31 | 1.41 |
| 95% CI | 1.34 to 1.47 | 1.47 to 1.61 | 1.17 to 1.30 | 1.23 to 1.37 | 1.17 to 1.32 | 1.27 to 1.45 | 1.27 to 1.34 | 1.36 to 1.45 |
Uptake with both FIT and gFOBt showed the expected inverse relationship with deprivation8 (figure 3). The increase in uptake with FIT versus gFOBt in IMD quintile 5 (most deprived) was 7.8 percentage points, 54.3% vs 46.5% (OR 1.37, 95% CI 1.31 to 1.43), and that in quintile 1 (least deprived) was 6.6 percentage points, 73.5% vs 66.9% (OR 1.37, 95% CI 1.30 to 1.44); the difference across quintiles was not significant.
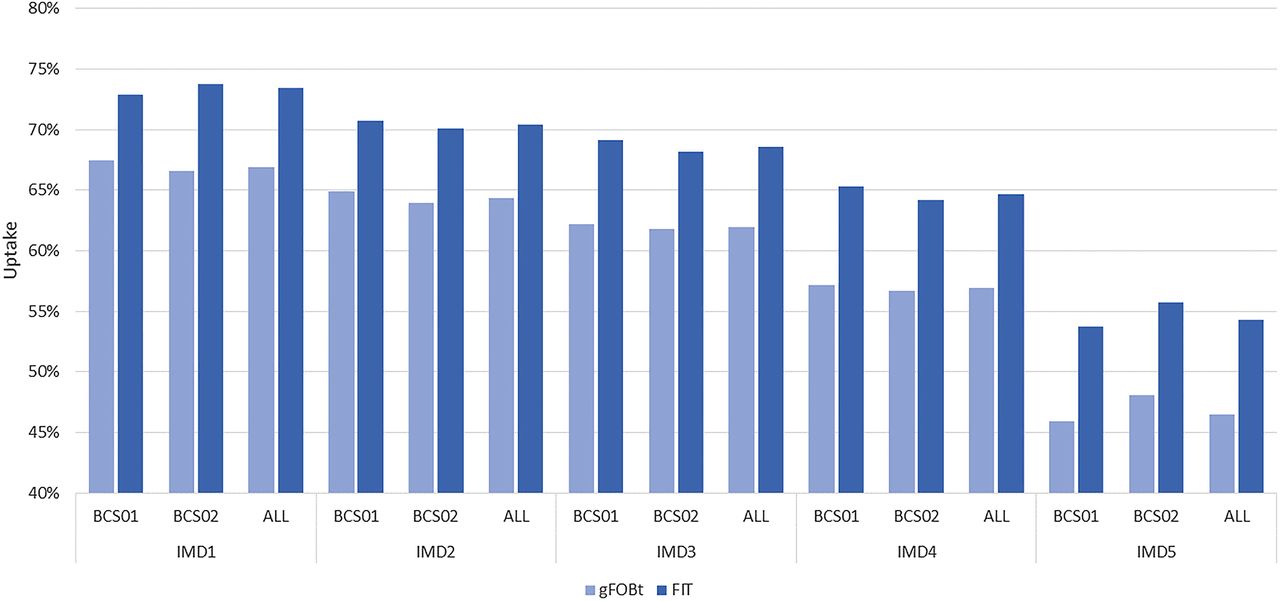
Uptake of faecal immunochemical test (FIT) and guaiac-based faecal occult blood test (gFOBt) by index of multiple deprivation (IMD) quintile and screening Hub.
| IMD1 (least deprived) | IMD2 | IMD3 | IMD4 | IMD5 | Total | |
|---|---|---|---|---|---|---|
| OR (total) (FIT vs gFOBt) | 1.37 | 1.31 | 1.34 | 1.39 | 1.37 | 1.35 |
| 95% CI | 1.30 to 1.44 | 1.25 to 1.38 | 1.24 to 1.41 | 1.33 to 1.45 | 1.31 to 1.43 | 1.33 to 1.38 |
Adjusted for all other variables (age, Hub, sex, deprivation and screening episode), the ORadj for uptake with FIT versus gFOBt was 1.74 (95% CI 1.70 to 1.79) (table 3). The increased OR after adjustment compared with the univariate analysis (OR 1.35) is due mainly to the effect of screening episode, with the largest increase in uptake observed in the prevalent (previous non-responder) episode, which has the lowest overall uptake.
Results of multivariate analyses of uptake and positivity
Positivity
The overall positivity for FIT with a 20 μg Hb/g faeces cut-off concentration was 7.8%, and for gFOBt was 1.7% (OR 4.82, 95% CI 4.59 to 5.05) (table 4). The increased positivity of FIT compared with gFOBt was significantly higher in the Midlands and North West Hub (8.7% positive with FIT vs 1.6% with gFOBt, OR 5.68, 95% CI 5.30 to 6.08) than in the Southern Hub (7.1% positive with FIT vs 1.8% with gFOBt, OR 4.16, 95% CI 3.89 to 4.45); the positivity with gFOBt was higher in the Southern Hub.
Positivity of FIT (cut-off 20 µg Hb/g faeces) and gFOBt by screening episode and Hub
Overall positivity for both FIT and gFOBt was highest in prevalent (previous non-responder) screening episodes (table 4). The increase in positivity with FIT was significant in all screening episodes, with the greatest increase observed in the incidence episodes (OR 5.06, 95% CI 4.79 to 5.35).
Positivity for both tests was higher in men than women, but the increase with FIT was similar (table 5). The increase in FIT positivity increased significantly with age, from an OR of 4.40 (95% CI 4.06 to 4.76) at 59–64 years to an OR of 5.21 (95% CI 4.76 to 5.70) at 70–75 years. Positivity increased with increasing level of deprivation, but the increase in positivity was similar across IMD quintiles (both overall and in the individual Hubs) (table 6).
Positivity of FIT (cut-off 20 µg Hb/g faeces) and gFOBt by age and sex
Positivity of FIT (cut-off 20 µg Hb/g faeces) and gFOBt by IMD quintile
FIT positivity decreased steadily with increasing cut-off concentration, from 7.83% at 20 µg Hb/g faeces to 1.52% at 180 µg Hb/g faeces (table 7). A similar pattern of reduced FIT positivity with increasing cut-off was evident for all screening episodes (figure 4) and IMD quintiles (figure 5).
PPVs and detection rates by sex, with different FIT cut-off concentrations (µg Hb/g faeces)
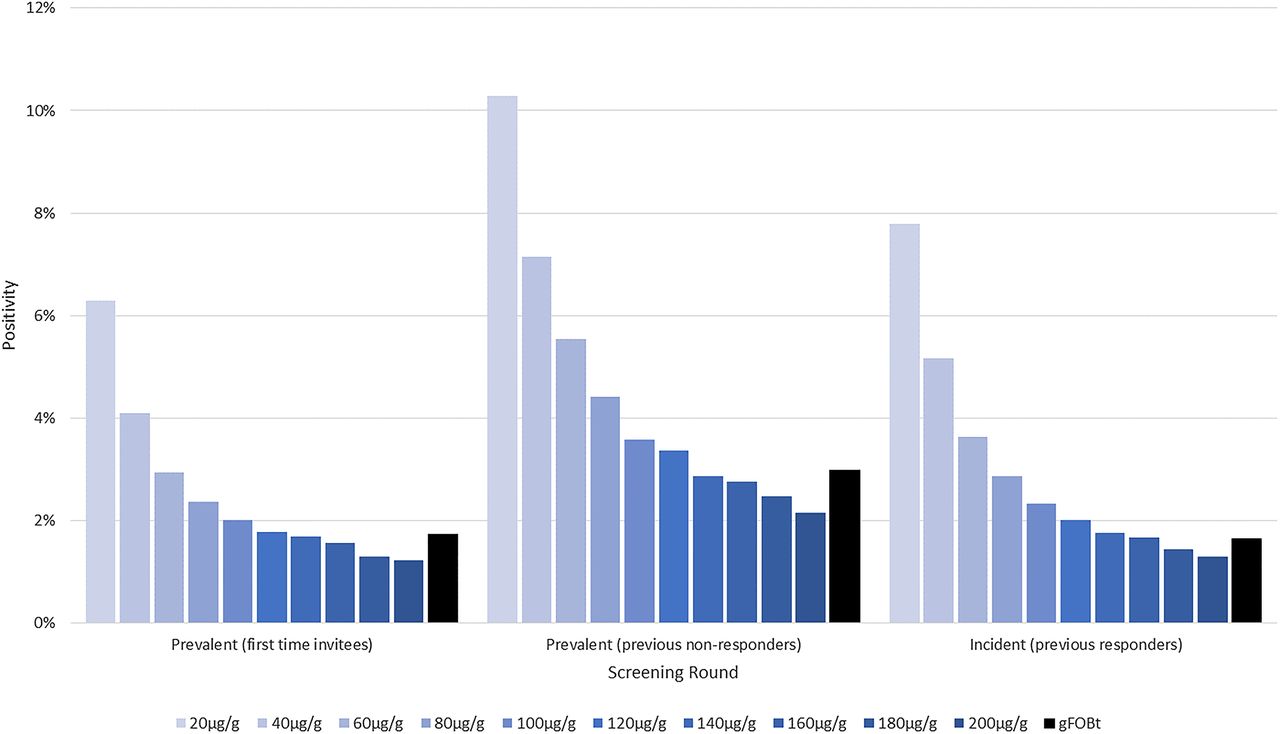
Positivity of faecal immunochemical test (FIT) and guaiac-based faecal occult blood test (gFOBt) by screening episode using varying FIT cut-off concentrations (µg Hb/g faeces). Hb, haemoglobin.

Positivity of faecal immunochemical test (FIT) and guaiac-based faecal occult blood test (gFOBt) by index of multiple deprivation (IMD) quintile using varying FIT cut-off concentrations (µg Hb/g faeces). Hb, haemoglobin.
In the multivariate analysis, the adjusted OR (ORadj) for FIT positivity (using cut-off concentration 20 µg/g) was 4.70 (95% CI 4.48 to 4.94). The increase in positivity with FIT differed significantly with age group and by screening episode, but not between males and females or between IMD quintiles. The difference in the increase in positivity between Hubs remained significant (table 3).
Uptake of colonoscopy
Overall colonoscopy uptake was 85.7% in FIT-positive subjects and 85.0% in gFOBt-positive subjects (table 7).
Detection rates
Using the cut-off concentration of 20 μg Hb/g, the cancer detection rate was 0.27% with FIT compared with 0.12% for gFOBt (OR 2.20, 95% CI 1.73 to 2.79, p<0.001) (table 7). Detection rates of advanced adenoma were 1.73% with FIT and 0.35% with gFOBt (OR 4.97, 95% CI 4.50 to 5.49, p<0.001). The detection rates for all neoplasms including low-risk adenomas were 3.74% and 0.76%, respectively (OR 5.05, 95% CI 4.72 to 5.41, p<0.001) (data not shown). Rates of detection of both cancers and adenomas fell with increasing cut-off concentration.
The cancer detection rate was no longer significantly higher with FIT at concentrations >40 µg Hb/g faeces. At a concentration of 180 µg Hb/g faeces, the cancer detection rate was only slightly higher than that for gFOBt, but the detection rate of advanced adenomas remained higher (0.43% vs 0.35%, OR 1.21 (95% CI 1.00 to 1.46, p<0.05)).
The detection rates of CRC and of advanced adenomas were more than twice as high in men as in women with both FIT at 20 µg Hb/g and gFOBt (table 7), but there was no significant difference in the increase with FIT between sexes. The increase in detection of advanced adenomas was highest in the oldest age group, and the Midlands and North West Hub (with higher positivity) had higher detection rates of advanced adenomas and all neoplasms than the Southern Hub (data not shown).
For advanced adenomas, there was a significant difference in the increased detection with FIT between screening episode types at the cut-off concentration of 20 μg Hb/g. The greatest increase was observed in incident screens where the detection of advanced adenomas increased from 0.33% to 1.71% (table 8) (OR 5.31, 95% CI 4.73 to 5.96, p<0.001). The detection of advanced adenomas fell more steeply with increasing cut-off concentration in subjects screened in the incident episode (figure 6).
PPVs and detection rates by screening episode type, with different FIT cut-off concentrations (µg Hb/g faeces)

Detection rates for advanced adenoma by screening episode with different faecal immunochemical test (FIT) cut-off concentrations (µg Hb/g faeces). gFOBt, guaiac-based faecal occult blood test; Hb, haemoglobin.
There were no significant differences in the increase in detection rates between IMD quintiles (data not shown).
Positive predictive value
The PPV of FIT at 20 µg Hb/g for cancer was significantly lower than for gFOBt (4.0% vs 8.3%, OR 0.47, 95% CI 0.37 to 0.60, p<0.001), but the PPVs for advanced adenoma were similar between tests (25.8% vs 24.0%, OR 1.10, 95% CI 0.98 to 1.23, p=0.1) (table 7), and for cancer plus advanced adenoma the PPV of FIT was non-significantly lower (OR 0.90, 95% CI (0.82 to 1.01)). For all neoplasms including low-risk adenomas, the PPV was higher for FIT; 55.6% vs 51.8% (OR 1.17, 95% CI 1.06 to 1.29, p=0.003) (data not shown).
The PPV of FIT for cancer increased with increasing cut-off concentration, from 4.0% to 10.6% (table 7); the PPV for advanced adenoma increased with increasing cut-off up to 100 µg Hb/g faeces, but not further.
Even after increasing the FIT cut-off concentration from 150 to 180 µg Hb/g to reduce positivity and allow for the increased uptake (ensuring similar colonoscopy requirements to that for gFOBt), FIT had a significantly higher detection rate and higher PPV for advanced adenomas and a higher PPV for all neoplasms than gFOBt (table 7).
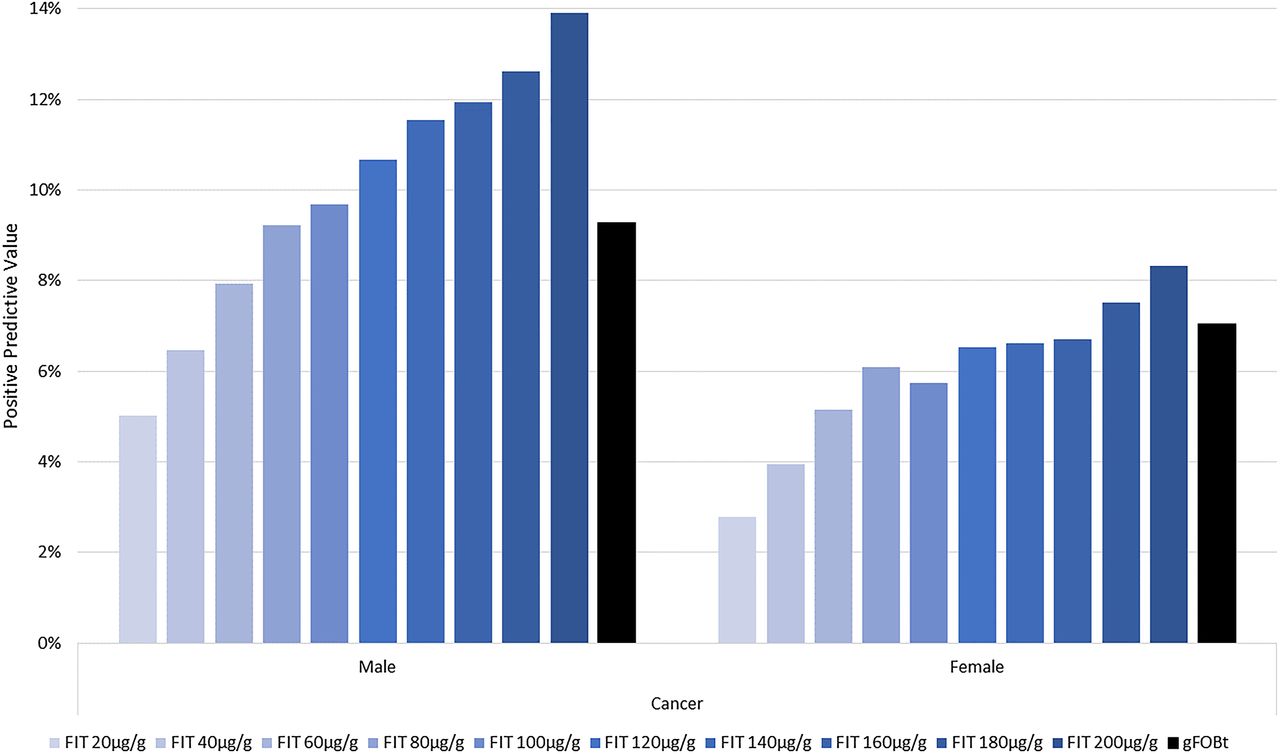
Trends in PPVs with increasing cut-off concentration by sex were similar to those for all subjects (table 7, figures 7 and 8). The proportion of cancers that would have been missed with an increased cut-off from 20 to 180 µg Hb/g faeces did not differ significantly by sex or screening episode, but the proportion of advanced adenomas that would have been missed was significantly higher in the incident episode (78.5% compared with 66.1% and 66.7% in the prevalent first-time invitees and prevalent (previous non-responders) respectively, p=0.03) (table 8).

Positive predictive value for cancer by sex with different faecal immunochemical test (FIT) cut-off concentrations (µg Hb/g faeces). gFOBt, guaiac-based faecal occult blood test; Hb, haemoglobin.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Positive predictive value for advanced adenoma by sex with different faecal immunochemical test (FIT) cut-off concentrations (µg Hb/g faeces). gFOBt, guaiac-based faecal occult blood test; Hb, haemoglobin.
Discussion
The FIT pilot in England has demonstrated a significant and marked increase in uptake of the FIT kit compared with the gFOBt kit currently in use in the NHS BCSP. Organised population-based biennial colorectal cancer screening commenced in England in July 2006 and the screening device and screening algorithm have not changed since then. While the national average uptake has gradually increased from 50.9% in 2006/2007 to 58.2% in 2014/2015, it remains poor compared with the other NHS cancer screening programmes in spite of both local and national initiatives to improve it. Uptake is poor at first invitation, particularly among men and among the deprived population, characterising the challenge that has faced the programme since its inception. The FIT pilot provided an opportunity to begin to address these issues, and considerable efforts were made to make the invitation process, including presentation of test kit and instructions for use, as simple as possible. The resulting increase in uptake was larger than that obtained by most other intervention studies in established programmes,26–29 perhaps reflecting these efforts. A study in Australia has reported a similar OR for the effect of general practitioner endorsement on uptake, although with a lower baseline uptake of 32%.26 Importantly, the differential uptake between men and women was reduced with FIT, with the absolute difference falling from 5.7% to 3.6%. Although we did not observe a significant decrease in the trend of decreasing uptake with increasing level of deprivation, an increase in uptake was observed across all quintiles of deprivation, with an absolute increase of nearly 8% in the most deprived quintile. Analysis using IMD quintiles based on the national distribution of scores, rather than those in the pilot population, did not alter our findings. Of particular importance is the marked increase in uptake observed in previous non-responders. The increase among first-time invitees is likely to be sustained in subsequent screening episodes since numerous studies have shown that previous participation is a strong predictor of future compliance.7 ,25–28 ,30–32
The increase in uptake reported here is greater than that observed in most studies elsewhere, although a meta-analysis of five studies found a risk ratio of 1.16 (95% CI 1.03 to 1.31) for compliance with FIT versus gFOBt.33 The meta-analysis included one study34 in which subjects were first required to collect the kit from a clinic; the proportion of subjects invited who collected a kit was lower in the FIT arm, but once the kits had been dispensed participation was higher with FIT. The other four studies in the meta-analysis showed risk ratios for uptake with FIT ranging from 1.19 to 1.27.13–15 ,35 Of these, the two largest studies, both in the Netherlands, which found uptake to increase from 46.9% or 49.5% with gFOBt to 59.6% or 61.5% with FIT, were both conducted in previously unscreened populations.13 ,15 A study in Scotland has reported overall uptake of 58.7% with FIT compared with 53.9% for gFOBt, with higher uptake in all age and deprivation quintiles for both men and women.18 ,19 However, in the Scottish study FIT uptake and clinical outcomes in two evaluation NHS boards were compared with results obtained contemporaneously in two other similar NHS boards and before and after the evaluation of FIT. The present study was conducted in the setting of a national population-based screening programme and, while it was not a formal randomised study, the selection of 1 in 28 subjects to receive a FIT, as described, led to a similar distribution of characteristics in the two groups of subjects, and thus to a more robust comparison than was possible in the study in Scotland. Our results show similar increases in uptake in the first screening episode to those reported in the Dutch studies. Ours is the only study, however, to show a significant increase in uptake in previous non-responders, which has important implications for improving uptake overall. On the basis of these results, the introduction of FIT in England would initially result in approximately 290 000 additional subjects being screened each year. As stated above, uptake is likely to continue to increase as those responding in the first screening episode continue to participate in later episodes.
Differing demographics lead to regional variations in uptake and the introduction of FIT in the national programme is likely to result in greater increases in uptake (and colonoscopy workload) in some areas. The impact of FIT in the London region with its diverse population and current poor uptake6 is particularly difficult to predict. The use of a single cut-off concentration may result in different positivity in different Hubs due to differing demographic profiles; in the pilot study, the increase in positivity with FIT differed between the two Hubs, but positivity increased across all IMD quintiles.
The detection of cancers and advanced adenomas was greatly increased with the relatively low FIT cut-off concentration used in the pilot, and the PPV for advanced adenoma was similar to that for gFOBt, even at this low cut-off. In particular, it is noteworthy that the greatest increase in detection of advanced adenomas was seen in subjects previously screened. Detection rates of CRC and advanced adenomas (high and intermediate risk) fell with increasing FIT cut-off concentrations. The PPVs for cancer increased, but those for advanced adenomas did not alter greatly for cut-off concentrations >100 μg Hb/g faeces. Other studies using the same cut-off of 20 μg Hb/g faeces have reported similar increases in cancer detection;13 ,15 ,36 the observed detection rates will vary according to population characteristics and, for advanced adenoma, with the definition used.
An increase in uptake has implications for colonoscopy workload; the cut-off concentration for FIT used in the pilot was deliberately set at a low level to enable outcomes across a range of important cut-off concentrations to be studied. FIT positivity with this low cut-off was markedly higher than the current BCSP gFOBt positivity of about 1.7%. There is a relatively small resource of trained and accredited endoscopists in England; initially, it will be necessary to select a FIT cut-off concentration with a positivity (allowing for the marked increase in screening uptake), which delivers a colonoscopy referral rate similar to that currently experienced with gFOBt screening.
In our study, using a FIT cut-off concentration of 180 µg Hb/g faeces, and allowing for the marked increase in uptake, the number of subjects referred to colonoscopy with a positive FIT would be similar to that with gFOBt, but would still result in a significantly higher detection rate and higher PPV for advanced adenomas and all neoplasms compared with gFOBt. It is likely that positivity at a fixed cut-off will fall with repeat screening as subjects with adenomas are removed from the population and this will provide the programme with an opportunity to adjust the cut-off concentration and make the test more sensitive to the detection of neoplasia while maintaining the colonoscopy referral rate.
The use of different cut-off concentrations according to sex or other population characteristics (including screening history) has been proposed.37 ,38 The determination of such cut-offs will vary according to whether the aim is to maximise detection rates, PPV or other outcomes. With the need to maintain a positivity similar to that of the current programme, it is difficult to determine subgroup-specific cut-offs based on our data, but ongoing data collection should provide further information to enable such calculations.
In conclusion, this study illustrates a means by which new screening tests or screening protocols can be piloted within a ‘live’ screening programme. The method adopted enabled reliable comparison to be made between an existing and proposed biomarker in the screening population. The marked increase in uptake with FIT, its effect in reducing existing disparities (between men and women and between screening episodes) and the near doubling in uptake of the population previously resistant to screening all support the case for a swift transition to using FIT as the primary screening test in the NHS BCSP. While improving the clinical benefits of screening, the full potential of FIT will be realised only by exploiting the use of FIT concentration in a risk algorithm within an increased colonoscopy resource.
Acknowledgments
The authors are grateful to the following BCSP staff who contributed to the execution of the pilot: Carole Burtonwood, Carolyn Piggott, Sheena Pearson, Katy Reed (Southern BCSP Hub); Angela Ryder, Lisa Morgan and Julie Low (Midlands and North West BCSP Hub); Phil McCorry, Richard Winder, Suzanne Wright (NHS Cancer Screening National Office). The authors also acknowledge Tony McCann, Penny Aitchison, Helen Thomas, Jim Summers and Andrew Stockley (Health and Social Care Information Centre) for their important contribution and Iain McElarney (Mast Diagnostics UK) and Richard Sargent (REAL Digital International) who facilitated the design of the FIT postal package.
References
Footnotes
Contributors SM, SS, SPH and TJD contributed to the design of the study; all authors contributed to the analysis or interpretation of the data. SM, SPH and CM drafted the manuscript, and all authors were responsible for revising it critically for important intellectual content. All authors gave final approval of the version published.
Funding The funding for the evaluation of the pilot was provided by the National Office of the NHS Cancer Screening Programmes (now part of Public Health England).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.