Article Text

Statistics from Altmetric.com
Introduction
The objective of this review is to address three questions based on data almost exclusively acquired in humans: what does the ‘leaky gut’ mean? Should clinicians diagnose leaky gut and, if so, how can it be diagnosed? Is the leaky gut treatable? There are vast numbers of papers that link ‘leaky gut’ with altered microbiota in disease models in experimental animals, from allergy to non-alcoholic steatohepatitis to depression and amyotrophic lateral sclerosis. This review focuses almost exclusively on the evidence from human studies, since the clinicians need to address the three questions in the context of their patients. In addition, it focuses on the evidence of leaky gut in non-GI diseases, which are the focus of many diseases or disorders in which leaky gut and microbiota are considered to be aetiopathologically important mechanisms.
There is much folklore about the leaky gut and its relationship to microbial balance within the gut. One of the first ‘hits’ in searching information on leaky gut on the internet provides comprehensive advice, contrasting what happens when the balance is ‘right’ and when ‘out of whack’, and advice on how to get the gut microbes back into balance (box 1).
Leaky gut
Balance: when the microbial balance in your gut is right, your whole body functions the way it is supposed to. But when that balance gets out of whack—say because of chronic stress, chronic constipation, exposure to environmental toxins like pesticides, eating a poor diet or taking an antibiotic that wipes out a lot those microbes—the ‘bad’ bacteria cut holes in the fence and some of them, along with food particles and toxins, leak into the bloodstream. When your immune system sees organisms where they do not belong, it attacks, causing irritation and inflammation.
Causes: leaky gut has so many possible causes, so many possibly symptoms
Consequences: ‘The leakage in leaky gut may be responsible for a huge variety of health issues, ranging from minor (bloating, cramps, fatigue, food allergies and sensitivities, gas, and headaches) to ‘bigger things’: autoimmune conditions, depression and other mood disorders, diabetes, inflammatory bowel disease, and multiple sclerosis’.
Treatment: ‘Functional medicine’: get gut microbes back into balance: multistep programme
Remove foods that create problems for example, gluten, sugar and dairy.
Replace with foods less likely to irritate gut: fermented foods, for example, sauerkraut, kimchi, yoghourt, kefir, and pickles, are healing foods.
Repair the damage with supplements: L-glutamine (heal the intestinal lining), vitamin D, zinc and omega-3 fatty acids (such as fish oil).
Repopulate your good gut bacteria: probiotics or get a transplant from another person.
One of the biggest leaky gut red flags is having issues with a variety of foods.
Talk with your healthcare provider: you might have leaky gut syndrome.
Do not, however, try to treat it yourself.
There is no controversy regarding barrier dysfunction in diseases resulting in intestinal inflammation and damage such as coeliac or Crohn’s disease, or ulceration from non-steroidal anti-inflammatory drugs (NSAIDs) resulting in structural abnormalities of the epithelium. The ‘leaky gut’ is a simplistic term reflecting intestinal permeability, a function that was extensively studied in these diseases and reported in the scientific literature from 1970 to 1990.1–3
There may be several reasons for this resurgence of interest in the ‘leaky gut’. First, there is frustration about the lack of perceived advances in the management of common GI symptoms such as pain, diarrhoea and bloating; thus, a cause, such as leaky gut, is sought. Second, the scientific literature has promulgated ‘dysbiosis’ in diverse states, from obesity to autism, despite evidence that this documented parabiosis4 does not necessarily result in any metabolic or other changes in mucosal functions, including barrier function, or the role in pathogenesis of these diseases.5 Third, there is scientific research using diverse methods that documents alterations in human intestinal barrier function in disorders such as IBS or food allergy. However, there is no current gold standard with clear performance characteristics of the tests for barrier function, the diverse methods available actually measure very different endpoints and the clinical significance and relevance are unclear. Fourth, as explained by Quigley,6 there are popular perceptions of the barrier as a single cell thick, the epithelial layer having disruptions of intercellular connections leading to increased permeability and consequent access to the blood stream for various noxious chemicals, intact bacteria and a host of dietary and microbial components and designation as the primary abnormality in diverse diseases such as food intolerance, fibromyalgia, chronic fatigue syndrome and autism (all unsupported by any data).
Despite the recommendation to not self-treat, there are many resources, books and articles with recommendations on restoring the ‘healthy balance’ including eating dirt, curing with candida and education about the microbiome, the ‘human super organism’ and ‘the good gut’.
Given the current perceptions on ‘leaky gut’ that appear informed mostly by folklore or overreaching conclusions based on limited data, it is important to provide a balanced view of the scientific data to facilitate the role of clinicians in addressing the nature, diagnosis and treatment of abnormal intestinal barrier function in humans. To address this, it is important to characterise the intestinal barrier, the pathways between and through epithelial cells and measurement of intestinal permeability in humans. This provides the basis for examination of non-intestinal diseases characterised as ‘stress’ can really break the barrier and to review possible treatments including diet, natural substances and medications.
The intestinal barrier
The intestinal barrier is a dynamic entity interacting with and responding to various stimuli. It consists of multiple elements. In the lumen, there is degradation of bacteria and antigens by bile, gastric acid and pancreatic juice, and commensal bacteria that inhibit the colonisation of pathogens by production of antimicrobial substances. The next element of the barrier is the microclimate consisting of the unstirred water layer, glycocalyx and mucus layer that prevent bacterial adhesion by immunoglobulin A (IgA) secretion and by the physical barrier provided by the glycocalyx and mucus. Epithelial cells, connected by apical junctional complexes, have the ability to transport luminal content, but they also react to noxious stimuli by secretion of chloride and antimicrobial peptides. The Paneth cells in the epithelial layer, where they are most numerous in the crypts, also produce high quantities of defensins and several other antibiotic peptides and proteins when exposed to Gram positive and negative bacteria or bacterial products such as lipopolysaccharide. Beyond the epithelium, the lamina propria provides defence based on innate and acquired immunity cells secreting IgA, cytokines, chemokines and mast cell proteases, as well as endocrine and secretomotor mechanisms mediated by the enteric nervous system, which result in intestinal propulsive motility.7 Some of the important transmitters are serotonin (5-HT), histamine and cannabinoids.
The mucus layer consists of two components: an inner firmly adherent layer where bacteria are sparse and secreted peptides are protective with antibacterial functions (eg, defensins and lysozyme) and a thicker and loosely adherent outer layer where bacteria and bacterial products are abundant. The mucus layer is thicker in the colon than in the small bowel and may reach a depth of over 800 microns, which is not much less than the height of an entire villus (range 500–1600 microns). There is regional variation in the barrier along the gut; in the small intestine, pore size increases from 4 Å to 5 Å at the villus tip to over 20 Å at the base of the crypt. In addition, the microbiota influences the barrier and elements of the barrier impact the microbiota.6 There are several examples in the literature demonstrating diverse effects of bacteria and their products on intestinal barrier structure or function. Thus, Bifidobacteria enhance barrier function in experimental necrotising enterocolitis in mice,8 the yeast Saccharomyces boulardii has beneficial effects on altered intestinal microbiota and epithelial barrier defects in different pathologies,9 and different strains of Escherichia coli have opposite effects on the barrier: E. coli Nissle 1917 stimulates the tight junction protein ZO-2,10 11 whereas a prototypic translocating bacterium, E. coli strain C25, increases permeability.12 Products of the bacteria such as bacterial toxins, or bacterial dehydroxylation producing secondary bile acids and short-chain fatty acids produced by bacterial fermentation protect against bacteria or enhance the barrier function.13–15
At the level of the epithelial cells, from the apical to the basal domains of enterocytes, there are three sets of intercellular junctions: tight junction (zonula occludens (ZO)), adherens junction (zonula adherens) and desmosome. Together they comprise the apical junctional complex, which supports the dense microvillus brush border and regulates epithelial barrier function and intercellular transport.16 The anatomy and composition of the mucosal barrier and its intercellular junctions are shown in figure 1.17
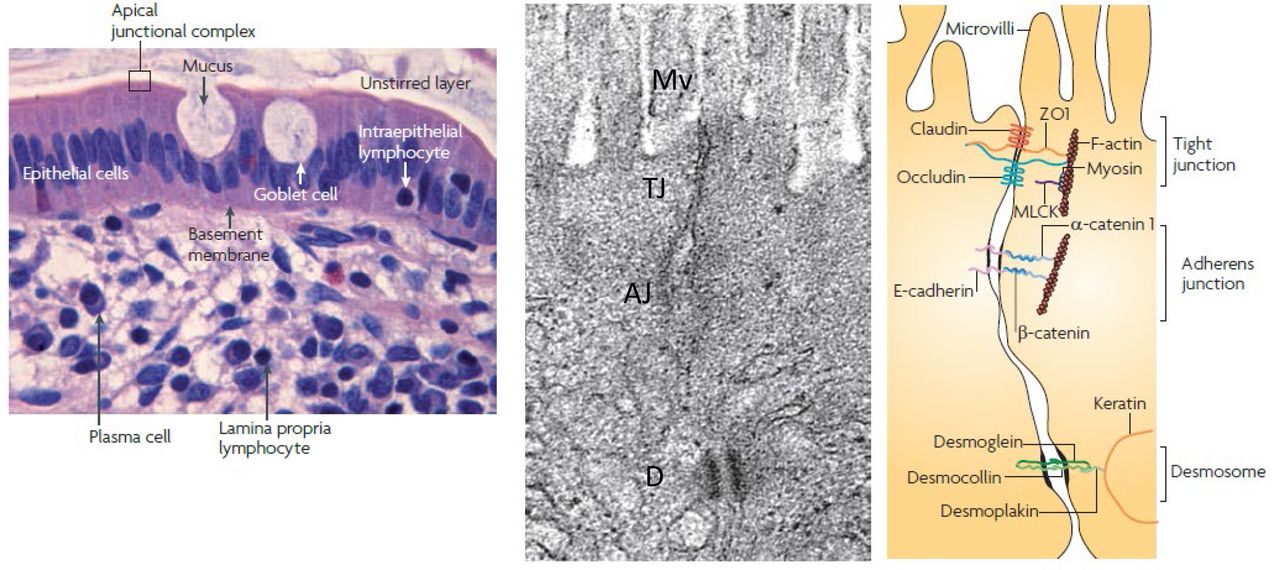
Anatomy of the mucosal barrier. Left panel: in the human intestinal mucosa, composed of columnar epithelial cells, lamina propria (with its immune cells) and muscular mucosa, the goblet cells synthesise and release mucin, and the unstirred layer is immediately above the epithelial cells. The tight junction (TJ) is a component of the apical junctional complex, and it seals paracellular spaces between epithelial cells. Middle and right panels show an electron micrograph and the corresponding line drawing of the junctional complex of an intestinal epithelial cell. The key elements of the TJ are the zona occludens and zona adherens, each of which is made up of different components. Just below the base of the microvilli (Mv), the plasma membranes of adjacent cells seem to fuse at the TJ, where claudins, zonula occludens 1 (ZO1), occludin and F–actin interact. E-cadherin, α-catenin 1, β-catenin, catenin δ1 (also known as p120 catenin; not shown) and Factin interact to form the adherens junction (AJ). Myosin light chain kinase (MLCK) is associated with the perijunctional actomyosin ring. Desmosomes, located beneath the apical junctional complex, are formed by interactions between desmoglein, desmocollin, desmoplakin and keratin filaments. In general, diffusion through claudins and occludin within the membrane is energy independent, whereas ZO-1 facilitates exchange between TJ and cytosolic pools through energy-dependent mechanisms. Reproduced from ref. 17.
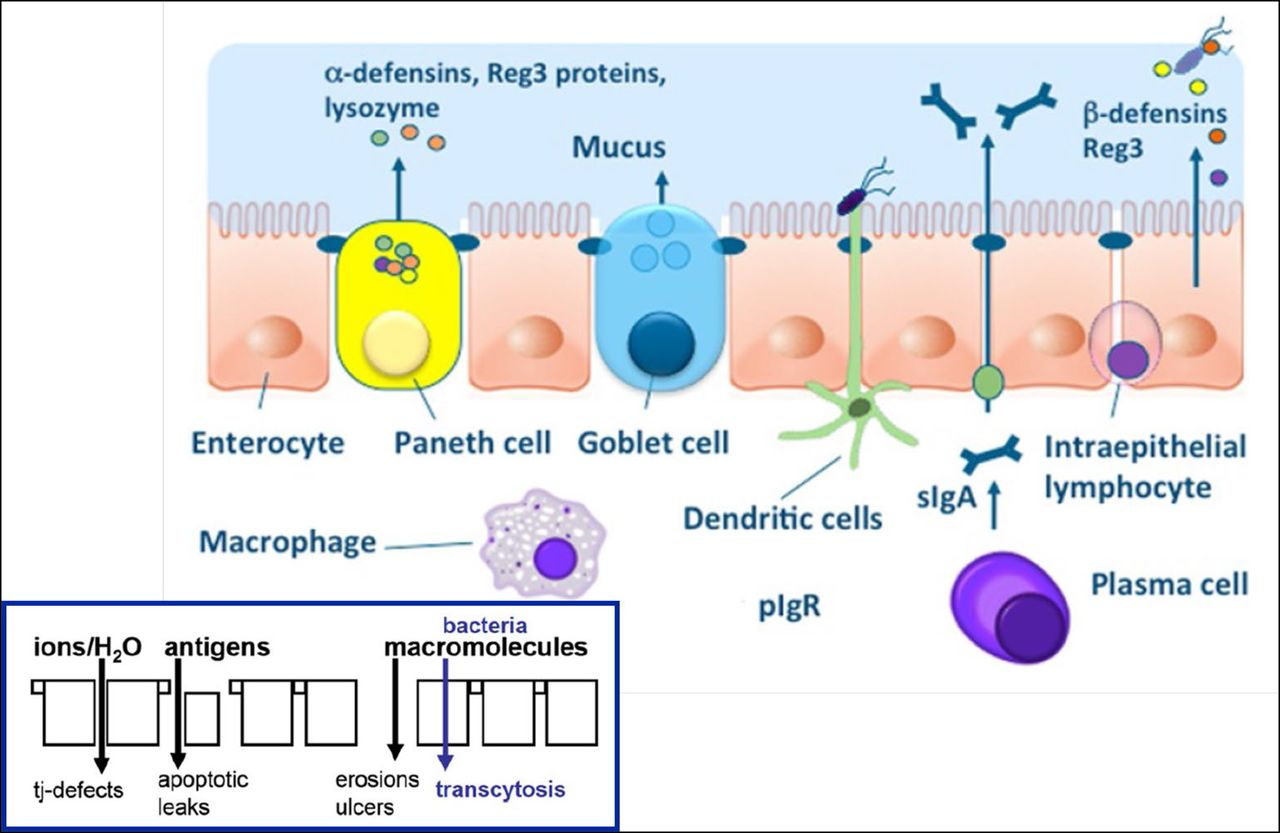
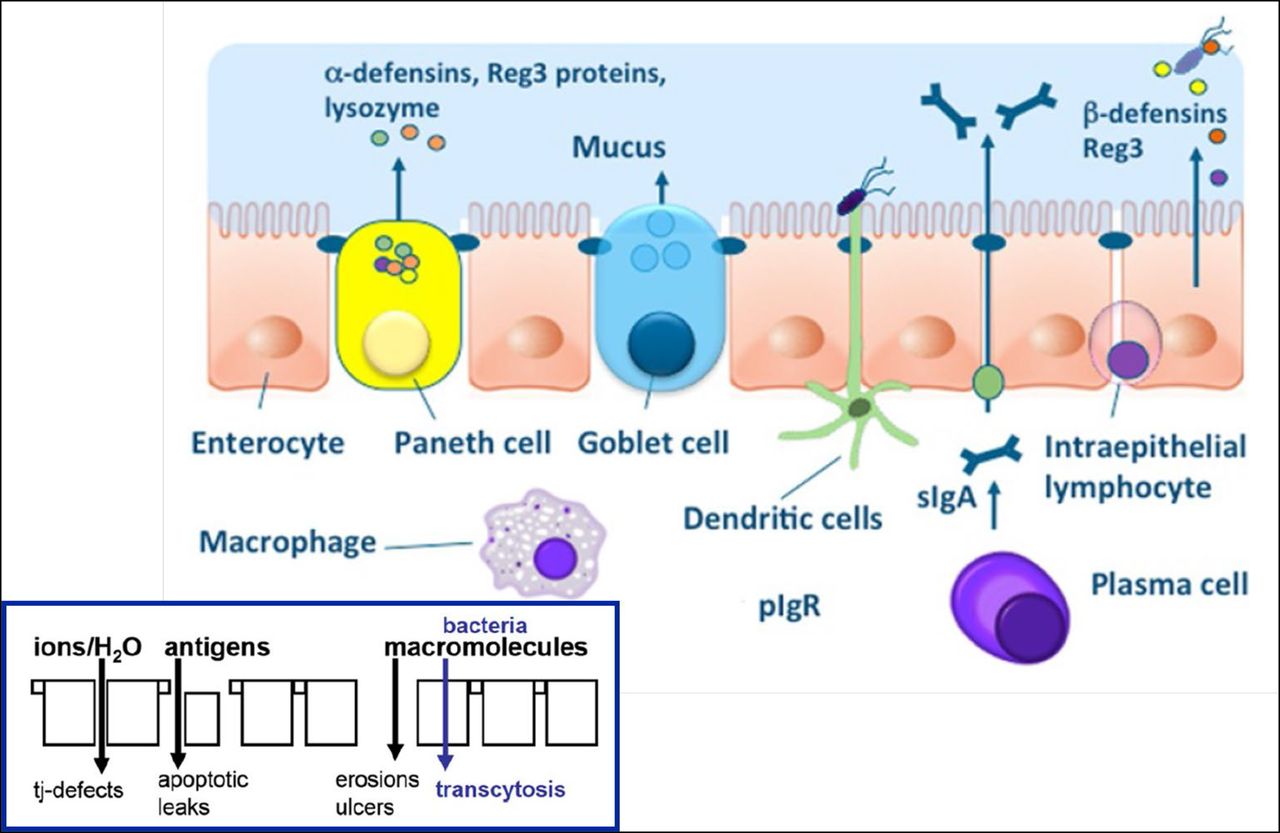
In general, it is recognised that there are three distinct paracellular epithelial permeability pathways: ‘leak’ and ‘pore’ pathways, which are regulated by tight junctions and define intestinal permeability; and an ‘unrestricted’ pathway, which is associated with apoptotic leaks in pathological states, is independent of tight junctions and provides access of luminal antigens to the lamina propria. In the presence of erosions or ulcers, bacteria gain access to the mucosa (figure 2).16 18
{kind=link}
{kind=link}
Intestinal barrier and its dysfunctions. The intestinal barrier includes the mucus layer preventing bacterial adhesion by secretion of chemicals such as α-defensins and IgA secretion, epithelial cells, connected at the tight junctions (TJ) by junctional complexes, having the ability to transport luminal content and react to noxious stimuli by secretion of chloride and antimicrobial peptides, and the lamina propria innate and acquired immunity cells secreting Ig and cytokines. Intestinal permeability measurements are determined by the marker molecules used for measurement, since the type of molecules that pass the intestinal barrier depends on the type of lesion. Reproduced from ref. 18.
The importance of the mucus component of the barrier
Mucus is secreted by the goblet cells and serves as the first physical defense in the barrier, preventing antigens, toxins and bacteria from directly contacting the epithelial cells. The elements of the mucus layer are highly glycosylated mucin proteins with a central protein core (abundant in serine, threonine and proline (Pro) amino acid residues) and O-glycosylation with hexoses and hexosamines oriented almost perpendicular to the protein core like a bottle brush, forming a gel-like sieve overlying the intestinal epithelium.19
In the small and large intestine, mucin 2 (MUC2) is the most abundant mucus protein secreted by goblet cells. Intestinal epithelial cells (IECs) also express transmembrane mucins (MUC1, MUC3, MUC4, MUC12, MUC13 and MUC17) that remain attached to the apical surface and form the glycocalyx together with glycolipids. Other major mucus proteins secreted by goblet cells are chloride channel regulator, calcium-activated-1, Fc globulin-binding protein, which covalently binds and cross-links mucus proteins, zymogen granule protein 16 (ZG16, a small lectin-like protein that binds to Gram+organisms), and antibodies, especially IgA. Secreted mucus mixes with Paneth cell secretions containing antibacterial peptides, lysozyme, deleted in malignant brain tumours 1, and also MUC2.19
Immune regulators, such as antimicrobial proteins and IgA molecules, are released in the mucus gel in a gradient from the epithelium to the lumen, thereby reinforcing the defence against the luminal microbes.20 The composition of the mucus layer can affect the microbiota in the gut, while the microbiota also determines the properties of the mucus gel.21 Muc2 knockout mice spontaneously develop colitis.22
Surfactants, including bile salts (chenodeoxycholate (10 mM) and hyodeoxycholate (10 mM), but not cholate (10 mM), ursodeoxycholate (10 mM) or Tween-20] induce secretion of mucus.23 In fact, bile salts impact the ability of mucus to serve as a barrier to hydrophilic and lipophilic compounds.24 Secretion of mucus is a prelude to the epithelial damage that leads to colonic secretion by the secretagogue bile acids, chenodeoxycholic acid25 26 and deoxycholic acid,27 28 and these effects can be partly inhibited by prostaglandins. Intra-arterial prostaglandin E2 (PGE2) evokes the secretion of intestinal mucus,29 and PGE2 reverses NSAID enteropathy, in part, by inducing mucus secretion.30 Other goblet cell secretagogues are cholinergic agonists, histamine, peptide tyrosine tyrosine (peptide YY) and serotonin. Overall, there is a role for the enteric nervous system, the enteroendocrine cells and resident immune cells in mediation of colonic mucus release.31 Cholinergic inhibition of mucin secretion with intra-arterial atropine reduced the epithelial damage and fluid secretion secondary to 5 mM sodium chenodeoxycholate in the rabbit colon in vivo.32
Dietary emulsifiers, like bile acids, are amphipathic, that is, they are molecules with hydrophilic and lipophilic sections that maintain fat molecules in liquid suspension or water-soluble components in a hydrophobic environment. Dietary emulsifiers interact with the multilayered endogenous mucus secretions that coat the luminal surfaces of the intestinal tract and may compromise the ability of human mucus to prevent contact between micro-organisms and IECs.33 Numerous synthetic surfactant food additives (anionic, cationic or non-ionic) are used in the food industry (such as mono- and diglycerides or esters of fatty acids (E471, E473 and E475)), as reviewed elsewhere.34 35 Some of these have been shown to increase intestinal permeability through paracellular and/or transcellular mechanisms, and some of them were also shown to inhibit P-glycoprotein or have mucolytic activity, such as the two emulsifiers, carboxymethylcellulose and polysorbate 80 (Tween).36
Additionally, based on the general characteristics of surfactants, it can be predicted that they decrease the hydrophobicity of the mucus layer, which has also been shown to be associated with increased intestinal permeability.34 Dietary emulsifiers may interact with gut microbiota and altered mucus thickness to promote colitis in Il10 and Tlr5 knockout mice, which are predisposed to development of spontaneous colitis37 and increase translocation of E. coli across IECs.38
Example of increased transcellular permeability
The examples provided above focused predominantly on the intercellular barrier and mucus barrier. However, there is evidence that there may be altered expression of cellular transport mechanisms that may ultimately lead to intercellular barrier dysfunction and systemic inflammation. An excellent example of the potential impact of increased transcellular permeability without apoptosis or intestinal ulceration is provided by the demonstration, in mouse models of obesity and diabetes, that hyperglycaemia drives intestinal barrier permeability through glucose transporter 2-dependent transcriptional reprogramming of IECs and alteration of tight and adherence junction integrity.39 These findings were demonstrated by reduced ZO-1 expression and increased fluorescein isothiocyanate (FITC)-dextran in serum after oral administration, indicating increased intestinal permeability, as well as an increased short-circuit current measured across the epithelial layer in Ussing chambers. There were also increased intestinal bacteria at systemic sites. Control experiments showed that these effects were due to hyperglycaemia rather than obesity or alterations in leptin signalling.
Intestinal permeability: pathophysiological mechanisms and methods of analysis
In this section, diverse methods of measurement and analysis are discussed, and the strengths and weaknesses are addressed. It is also important to note that intestinal permeability is influenced by several factors, which are not always considered in the publications, including the circadian cycle40 and stress.41
Orally administered probe molecules
Intestinal permeability is most commonly measured indirectly in humans by the fractional urinary excretion of orally ingested probes that cross the intestinal epithelium by the paracellular pathway, enter the bloodstream, are filtered by the glomerulus and excreted in the urine without active reabsorption in the kidney.42 Fractional urinary excretion can, therefore, be used as an indirect measure of intestinal permeability.
The most commonly used probe molecules are saccharides. Although regional differences for preferred absorption sites have been suggested,43 it is important to note that sucrose is only useful in the first hour postingestion, as it is rapidly metabolised (to glucose and fructose) and, therefore, at best, provides information about gastric and duodenal permeability. Moreover, other monosaccharides, such as mannitol and rhamnose, and disaccharides, such as lactulose and sucralose, are all absorbed in the small bowel and colon, and the timing of urinary excretion provides the best way to differentiate regional analyses: 0–2 hours reflects predominantly small intestinal permeability and 8–24 hours reflects almost exclusively colonic permeability.44 Also, among these saccharides, sucralose is the one not metabolised by colonic bacteria; similarly, polyethylene glycol 400 and radioactive chromium complexed with ethylene diamine tetracetic acid (51Cr-EDTA) are not degraded by colonic bacteria. However, the utility of these probe molecules is somewhat compromised by the ‘background’ ingestion of some of the sugars, particularly mannitol and sucralose.
Until relatively recently, interpretation of permeability tests was based on the following assumptions. Lactulose is a relatively large molecule, can only cross via the leak pathway or at sites of epithelial damage and is considered a marker of barrier integrity. Mannitol, which is reputedly one-third as large as lactulose, is assumed to cross the pore pathway, which allows passage of sodium ions, water and small solutes; therefore, mannitol and other monosaccharides such as rhamnose used to be regarded as measures of surface area.42 The inference was that the lactulose:mannitol ratio might measure the sum of leak pathway permeability and epithelial damage normalised to surface area. However, a review of the molecular sizes of the sugar probe molecules (table 1) suggests that there is no relevant difference in the reported or estimated molecular diameters and, therefore, it appears unlikely that they traverse the epithelium through different pathways.
Molecular sizes of the sugar and other probe molecules
In fact, the mass of saccharides that is absorbed during 1 hour in the healthy gut following ingestion orally is typically up to 2% of rhamnose and 0.07% of lactulose administered in children in USA.45 In healthy adults, the fractional excretion over 24 hours is 31.2%±3.4% (SEM) for 13C-mannitol and 0.32%±0.03% for lactulose.46 Therefore, despite the similarity in molecular diameters, there is a 100-fold difference in the per cent of recovery of the monosaccharides and disaccharides; however, if the larger molecule traverses the ‘leak’ pathway, the latter might also allow passage of the small molecule, and there is no compelling evidence that the different sugars actually traverse the intestinal barrier via different pathways.
Other factors, such as tertiary molecular structure, are likely relevant to explain the marked difference in absorption ratios of monosaccharides and disaccharides which is 30–100-fold for the monosaccharide, mannitol, compared with the disaccharide, lactulose. In practice, modern methods of assay based on liquid chromatography-mass spectrometry accurately measure the saccharides, and the most commonly used combinations are therefore lactulose or sucralose (as disaccharides) with mannitol or rhamnose (as monosaccharides). Because of potential ‘contamination’ by environmental exposures to mannitol and sucralose, the lactulose and rhamnose or 13C-mannitol saccharides are increasingly used for in vivo permeability measurements. In addition, as indicated above, 0–2 hour urine collection reflects predominantly small intestinal permeability and 8–24 hour collection almost exclusively colonic permeability.
Overall, these tests still have limited validity based on uncertainty of the normal values, lack of standardisation of test procedure and lack of validation including responsiveness of a standardised test to treatment.
In vitro or tissue measurements of intestinal barrier
Several methods are used to assess intestinal permeability on biopsies taken from the human gut and measured by the transfer of probe molecules across mucosal biopsies in Ussing chambers (in association with measurements of transepithelial resistance and short circuit current measurements). Other approaches quantitate the tight junction proteins in the mucosal biopsies, or they assess the faecal supernatant in cellular monolayers or rat or mouse colonic mucosa in vitro.
There are differences in in vivo compared with in vitro measurements of barrier functions. The molecular size of probe molecules that can cross the epithelial barrier in humans in vivo is at least 10-fold smaller than in vitro, which shows that molecules of approximately 4–40 kDa (eg, dextran 4 or 40) easily traverse the intestinal mucosa in a Ussing chamber in vitro. There are also differences that may reflect additional functional barriers in vivo that are excluded in the in vitro studies, including the lamina propria, innervation by submucosal neurons and permeability of end capillaries that constitute other potential barriers impeding passage of the probe molecules into the circulation in vivo. For example, intercellular complexes are under neurohumoural control, such as from vasoactive intestinal peptide (VIP) and cholinergic neurons, from the submucosal plexus,47 48 and these are lost in biopsied mucosa.
Endoscopic measurements of intestinal barriers in humans
Two techniques are available: first, confocal endomicroscopy, which shows leaks of intravenously administered fluorescein into the gut lumen during endoscopy49 (eg, in response to food-associated changes in the intestinal mucosa of patients with diarrhoea-predominant IBS); and second, endoscopic mucosal impedance, in which a 2 mm diameter catheter is passed through an endoscope and placed in contact with the duodenal mucosa under direct visualisation, and two circumferential sensors, placed 2 mm apart on the mucosa for 0.10 s, in the four quadrants of the duodenum with a decompressed lumen, and all fluid aspirated.50 The studies of food-associated changes during these challenge tests provide some evidence that there can be barrier changes that may indeed support the concept of transient ‘leakiness’ of the gut.
Abnormal barrier function in intestinal disease states
It is clear that inflammatory or ulcerating diseases result in abnormal intestinal barrier function. However, this is not the category of disease that is being associated with leaky gut, as discussed in the next section. The abnormal barrier function is well described for conditions such as IBD, as well as in first degree relatives of patients with IBD,3 51 coeliac disease and gluten sensitivity without overt coeliac disease in patients with HLA-DQ2/8 (genotype associated with coeliac disease,52 53 intestinal graft versus host disease, enteric infections and infestations and HIV infection and AIDS).42 There is also extensive literature54 documenting abnormal intestinal permeability in IBS and the association of abnormal permeability with pain in IBS, although the degree of altered barrier function is clearly lower than in inflammatory bowel or coeliac diseases. Longitudinal studies in patients with IBD suggest that increased intestinal permeability preceded relapsed of Crohn’s disease,55 suggesting a pathogenetic role of the epithelial barrier in the pathogenesis of gut inflammation; in addition, IBS is highly prevalent in first degree relatives of IBD patients,56 suggesting that intestinal permeability could be a relevant factor in the determination of symptoms.
Several other non-GI diseases have been associated with leaky gut, based on limited or no supporting data,6 42 including asthma, autism, Parkinson’s disease, multiple sclerosis, eczema, psoriasis, eosinophilic oesophagitis, environmental enteropathy, kwashiorkor, fibromyalgia, depression, chronic fatigue syndrome, multiorgan failure syndrome (shock, burns and trauma), non-alcoholic fatty liver disease (NAFLD), alcoholic cirrhosis, obesity, metabolic syndrome, pancreatitis and rheumatoid arthritis. Two separate groups independently studied small bowel permeability in patients with eosinophilic oesophagitis; one group documented increased small bowel permeability, though the mechanism whereby this results in the eosinophilic infiltration of the oesophagus is unclear57; the second group did not document increased small bowel permeability, but they reported improvement in the eosinophilic oesophagitis with an elemental diet.58 All of these diseases and disorders associated with possibly altered intestinal barrier function are pathological diseases, not what is usually associated with non-specific ‘leaky gut’.
Leaky gut: the pro arguments
The concept of a leaky gut in non-GI diseases is supported by evidence of dysfunctional gut mucosal barrier in stress-associated conditions and the response of the altered barrier to non-drug interventions; associations of disease states with altered intestinal permeability and microbiome; and alterations in intestinal permeability as a result of gut-directed therapy in diverse conditions including healthy people or diverse groups of children in central African countries.
Dysfunctional gut mucosal barrier due to endurance exercise and effects of non-drug intervention
Table 2 summarises the literature on two types of conditions that result in stress to the intestinal barrier, with documented effects on intestinal permeability or biochemical evidence of mucosal damage, and restoration with a dietary, non-pharmacological intervention. These studies suggest that there are ‘stress’ states in which there is documentation of altered barrier function and examples of normalisation that would support the concept of a transient leakiness of the gut barrier. There is also recent evidence suggesting that changes in intestinal microbiota composition (characterised by increased α-diversity and changes in the relative abundance of >50% of identified genera, including increased abundance of less dominant taxa at the expense of more dominant taxa such as Bacteroides) and metabolism (reduced serum interleukin-6 and reduced stool cysteine) coincide with increased intestinal permeability (documented by increased sucralose excretion in urine after oral load) in young adults under prolonged physiological stress in the form of a 4-day cross-country ski march.59 Discussion of the role of the microbiota in intestinal barrier function is beyond the scope of the current article. Further studies are required to explore the hypothesis that epithelial barrier dysfunction associated with mucosal enrichment of specific bacterial strains may predispose to a shift to disease-associated microbiota that eventually leads to pathological consequences such as IBD in individuals with genetic predisposition.60
Summary of the literature on conditions that result in stress to the intestinal barrier, with documented effects on intestinal permeability or biochemical evidence of mucosal damage, and restoration with a dietary, non-pharmacological intervention
Associations of disease states with altered intestinal permeability and microbiome
From a detailed review of the literature, it is clear that animal models of disease have documented a three-point relationship: disease phenotype, barrier change and altered microbiota. As exemplified best with chronic liver disease, the directionality of the relationship is controversial, even from animal studies. For example, one hypothesis argues that increased endogenous production of ethanol by gut bacteria (eg, E. coli) caused by small intestinal bacterial overgrowth results in increased intestinal permeability, bacterial translocation and hepatic inflammation due to the translocated bacteria or their products.61 An alternative hypothesis is that the liver disease causes a systemic inflammatory response that leads to increased intestinal permeability, with bacterial translocation and further hepatic damage.62 63
In many studies in the literature, particularly in human studies, the three focal points of the relationship are not all examined, and ‘triangulation’ is therefore based on hypothesis or inference based on the association between two of these three factors. Table 3 summarises information garnered from studies in ageing, food allergy, liver disease, parenteral nutrition (or enteral exclusion) and neuropsychiatric diseases in humans or in animal models where there are no human data available. In general, the data should be regarded as hypothesis generating, that is, the leaky gut may be a cause or an effect of the disease (as in the case of liver disease), and there may be either normal or dysbiotic microbiota that lead to inflammatory or other consequences that have impact on the disease. In some situations, alteration of the microbiota may result in reduced severity of the disease in humans, as demonstrated with hepatic cirrhosis in response to treatment with Lactobacillus casei strain Shirota or VSL#3, which contains eight lyophilised bacterial strains.64
Summary of diseases or disorders with increased intestinal permeability and altered microbiota
Alterations in intestinal permeability as a result of gut-directed therapy
A third proargument is provided by examples from the literature of in vivo human studies showing alterations in intestinal permeability as a result of gut-directed therapy, as summarised in table 4. One study worthy of specific comment is the randomised, placebo-controlled trial of oral glutamine in about 100 patients showing normalisation of LMR in association with improvement in the IBS-symptom severity score, stool frequency and consistency.65 However, most of the other studies are small, used different nutrients and diverse methods and require replication.
Examples from the literature of in vivo human studies showing alterations in intestinal permeability as a result of gut-directed therapy with nutrient, supplement or fibre
There is also hope that probiotics or commensal organisms improve intestinal barrier function66; however, the evidence to date is sparse, often based on animal models rather than human studies, the beneficial effect may be through the effects of butyrate and the documented effects have been reported for the organism Akkermansia municiphila.67 There is a microintegral membrane protein (MIMP) that is the smallest domain of surface layer protein from Lactobacillus plantarum. MIMP had a significant anti-inflammatory effect in an experimental model of dextran sodium sulfate (DSS)-induced colitis.68 This was achieved through multiple mechanisms: regulating the gut barrier (appearance of FITC-dextran in serum after oral gavage, as well as upregulation of the expression of junctional adhesion molecule-1, occludin and ZO-1 in the colon tissues), microbiota (increased richness and diversity, including increased Leuconostocaceae and Leuconostoc, instead of Firmicutes and Clostridia, which were abundant in the DSS group) and inflammatory cytokines through the Toll-like receptor 4-related pathway.68
These cumulated observations suggest that there are non-pathological situations that may be associated with increased permeability, and these relatively minor perturbations can be reversed with dietary, non-pharmacological approaches. Further studies of such approaches, including prebiotics and probiotics, are eagerly awaited.
Leaky gut: the con arguments
As indicated by other authors,6 16 there are, however, important pitfalls that need to be considered and precautions to be taken in attributing biological or clinical relevance to ‘leakiness’ of the barrier. First, altered permeability may be an epiphenomenon. For example, any inflammatory process may impair barrier integrity, and other factors such as dietary components or intraluminal factors such as bile acids can independently influence barrier function. Second, although allergens, stress and physical activity may indeed alter intestinal barrier function, it is unclear how this predisposes to clinical consequences. Third, impaired barrier function (eg, genetically determined defects in barrier components) does not, in isolation, lead to disease phenotype in experimental animal models of disease. Fourth, increased permeability is not necessarily deleterious, and there is no convincing evidence that an intervention that restores or improves barrier function in humans can alter the natural history of disease. Thus, for example, whereas antitumour necrosis factor-α therapy reduces mucosal inflammation and restores intestinal permeability in patients with IBD, and butyrate, zinc and some probiotics also ameliorate mucosal barrier dysfunction, it is still unproven that permeability manipulation should be considered as a therapeutic target in IBD.69
Conclusions
Although the ultrastructure and function of the epithelial barrier have been well characterised, the role of and interactions with other components of the barrier, especially the mucus layer and its perturbation, remain unclear. The role of gut barrier function is deemed to be important, but there are many unresolved questions as there are no validated clinical diagnostic tests. Although chemicals, nutrients, prebiotics and even plant extracts (eg, indigo naturalis) improve barrier function, there are no validated drug treatments yet, and the impact of restoring barrier function to ameliorate clinical manifestations in local GI disease or systemic diseases is as yet unproven. Clinicians should be aware of the potential of barrier dysfunction in GI diseases and the potential as a target for future therapy.
Acknowledgments
The author would like to thank Mrs Cindy Stanislav for excellent secretarial assistance.
References
Footnotes
Contributors MC: authorship of manuscript.
Funding MC is supported by grants R01-DK67071 and R01-DK115950 from National Institutes of Health.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Patient consent for publication Not required.