Article Text

Abstract
Objective Depression is associated with IBD, but the effect of antidepressants on IBD has been sparsely studied. We assessed the impact of depression and antidepressant therapies on the development of IBD.
Design The Health Improvement Network (THIN) was used to identify a cohort of patients with new-onset depression from 1986 to 2012. THIN patients who did not meet the defining criteria for depression were part of the referent group. The outcome was incident Crohn’s disease (CD) or ulcerative colitis (UC). Cox proportional hazards modelling was performed to evaluate the rate of Crohn’s disease or UC development among patients with an exposure of depression after controlling for age, sex, socioeconomic status, comorbid conditions, smoking, anxiety and antidepressant use including atypical antidepressants, mirtazapine, monoamine oxidase inhibitors (MAOI), serotonin norepinephrine reuptake inhibitors (SNRI), selective serotonin reuptake inhibitors (SSRI), serotonin modulators; and tricyclic antidepressants (TCA).
Results We identified 403 665 (7.05%) patients with incident depression. Individuals with depression had a significantly greater risk of developing CD (adjusted HR=2.11, 95% CI 1.65 to 2.70) and UC (adjusted HR=2.23, 95% CI 1.92 to 2.60) after controlling for demographic and clinical covariates. SSRI and TCA were protective against CD, whereas mirtazapine, SNRI, SSRI, serotonin modulators and TCA were protective for UC.
Conclusion Patients with a history of depression were more likely to be diagnosed with IBD. In contrast, antidepressant treatments were selectively protective for Crohn’s disease and UC. These results may impact counselling and management of depression and IBD.
- Crohn’s disease
- ulcerative colitis
- inflammatory bowel disease
- epidemiology
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Depression is a prevalent disorder associated with immune activation and cytokine release.
Antidepressants can attenuate inflammation in depression.
Depression is associated with IBD, but the temporal association between depression and IBD, and the role of antidepressants are not known.
What are the new findings?
In a large and robust cohort, depression increases the risk of developing both Crohn’s disease and UC.
The use of selective serotonin reuptake inhibitors and tricyclic antidepressants protects against Crohn’s disease.
Mirtazapine, serotonin norepinephrine reuptake inhibitor, selective serotonin reuptake inhibitors, serotonin modulators and tricyclic antidepressants protect against UC.
How might it impact on clinical practice in the foreseeable future?
Diagnosis of depression increases the risk of IBD, and this effect may be mitigated through treating depression with antidepressants.
In individuals with depression and GI symptoms, there should be a high index of suspicion for IBD.
Antidepressants may play a role in attenuating peripheral inflammation in IBD and other autoimmune diseases.
Background
Depression is a highly prevalent multifactorial disorder that has been strongly linked to activation of the immune system and cytokine release.1 2 Approximately 5%–10% of primary care patients have depression.3 Recent studies have demonstrated that the use of antidepressants can improve depression while attenuating inflammatory cytokine production.2 4–6
Inflammatory bowel disease (IBD), which consists of Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic immune-mediated disease resulting in inflammation of gut mucosal tissues, with an increasing prevalence worldwide.7–9 Several studies have demonstrated that patients with IBD are more likely to experience depression, and that depression worsens the prognosis of IBD.10–13 A recent systematic review identified studies exploring whether depression can influence the development of IBD.14 In one prospective cohort study, depression was associated with an increased risk of CD, but not UC.15 However, no prior study has evaluated the temporal association between depression and the subsequent diagnosis of IBD, while also investigating the effect of antidepressant use on this risk.
Therefore, we used a large representative database with robust pharmacological records to assess whether a diagnosis of depression increases the likelihood of developing IBD after controlling for antidepressant use.
Methods
Study design and patient data source
We performed a retrospective cohort study using UK-based electronic medical records database, The Health Improvement Network (THIN).16 THIN provides anonymised primary care data for more than 12 million individuals who are nationally and regionally representative of the general UK population.17 18 THIN provides demographic data, medical diagnoses (in the form of Read codes), prescriptions (using the Multilex system) and laboratory data.19 Additionally, every practice in THIN has an Acceptable Mortality Reporting date, which ensures that the practice properly records patient deaths and therefore helps to avoid potential immortal time bias.
Study population
THIN was used to identify an inception cohort of physician-diagnosed, clinical depression cases and a referent group studied between 1986 and 2012. The depression and control cohorts were followed to first diagnosis of CD or UC. Individuals were eligible for participation if they (1) were between 10 and 90 years of age at their start date in THIN; and (2) had at least 1 year of records following their start date in THIN (which is the latter of the registration date or practice’s Acceptable Mortality Reporting date).20
Primary exposure and outcome
The primary exposure of interest was incident depression. Incident cases of depression were defined as individuals who (1) met the case definition for depression (ie, at least one code for a depressive disorder, excluding individuals with a record of any bipolar disorder code in their lifetime, as defined previously21 22); and (2) did not have a diagnosis of depression in the 1 year following their start date in THIN. Depression was evaluated as a time-dependent exposure, such that all patients who developed depression first contributed unexposed person-time and were counted in the referent group until the first depression code that appeared in THIN following the inclusion criteria. This marked the start of exposed time. The partitioning of person-time was done to avoid potential immortal time bias.23 The referent group (unexposed) was defined as anyone who did not meet the case definition for depression.
The primary outcome of interest was a diagnosis of CD or UC. External validation studies conducted on the General Practice Research Database (GPRD)—the precursor to the THIN database—have confirmed its reliability in the study of IBD.24 Studies of GPRD and THIN demonstrate that both databases have similar validity in data recording.25 Incident cases of IBD were defined as individuals who (1) had at least 3 years of data in THIN following their start date in THIN and prior to their CD or UC diagnosis; and (2) met the case definition for IBD (ie, more than one code for IBD recorded, separated by a time interval of at least 4 weeks).20 26 A washout period of 3 years was used to separate incident from prevalent cases of IBD. Patients who were recorded for both CD and UC, and those who had prevalent IBD prior to the study start, were excluded from the study. Patients were followed until the earliest of CD or UC diagnosis, migration out of practice, death, or the last date of collection up to 31 May 2012, for up to 26 years of follow-up.
Covariates
Potential confounders that were controlled for were age, sex, socioeconomic status, comorbid conditions, smoking status, anxiety and antidepressant use. Age was explored as a categorical variable and defined as under the age of 50 or over the age of 50 at baseline (ie, start date in THIN), as this age provides a meaningful distinction in the manifestation of depressive disorders.27 Socioeconomic status at baseline was stratified by quintiles (1 being the least deprived and 5 being the most deprived), and estimated using postcode level indicators generated from the Townsend Deprivation Index.28 The Charlson Comorbidity Index was used to identify comorbid conditions within 3 years of enrolment in a THIN practice and defined based on the presence of validated Read codes and associated weights.29
Smoking status at baseline (within 1 year prior to the index date) was defined as (1) never smoker; (2) ex-smoker; (3) current smoker; and (4) unclassifiable as those who did not have smoking information available. Anxiety diagnosis was based on the presence of Read codes corresponding to an anxiety disorder within 1 year of the index date. Antidepressant medication use at baseline was stratified according to the following categories (online supplementary appendix A): (1) atypical antidepressants; (2) monoamine oxidase inhibitors (MAOI); (3) serotonin norepinephrine reuptake inhibitors (SNRI); (4) selective serotonin reuptake inhibitors (SSRI); (5) serotonin modulators; and (6) tricyclic antidepressants (TCA). Mirtazapine was further separated and given its own category based on a recent study noting its protective effect in another autoimmune disease, primary biliary cholangitis.30
Supplementary file 1
Data analysis
Characteristics of patients, stratified by depression status, were summarised descriptively. Χ2 test and Wilcoxon rank-sum test were used to identify differences between the exposure groups at baseline. Cox proportional hazards models were used to identify the time from depression to either CD or UC diagnosis. Both crude and analyses adjusted for age, sex, socioeconomic status, comorbidities, smoking status, anxiety diagnosis and antidepressant medication were performed. Effect modification was explored for age and sex using a likelihood ratio test. Estimates were reported as HRs and accompanying 95% CIs. Sensitivity analyses were done to examine the robustness of findings, specifically to determine the impact of (1) restricting observations to have at least 6 months between depression and CD diagnosis or depression and UC diagnosis, and (2) changing the initial washout period from 1 year to 5 years for depression. An additional sensitivity analysis was performed to determine the nature of the relationship between antidepressant use and the development of CD and UC. We identified the proportion of patients in the depression cohort who developed CD or UC among those who used versus those who did not use antidepressants. This was compared with the proportion of patients in the general population who developed CD or UC among users and non-users of antidepressants.
All analyses were performed using Stata-MP V.13.1 with a predetermined alpha of 0.05.
Results
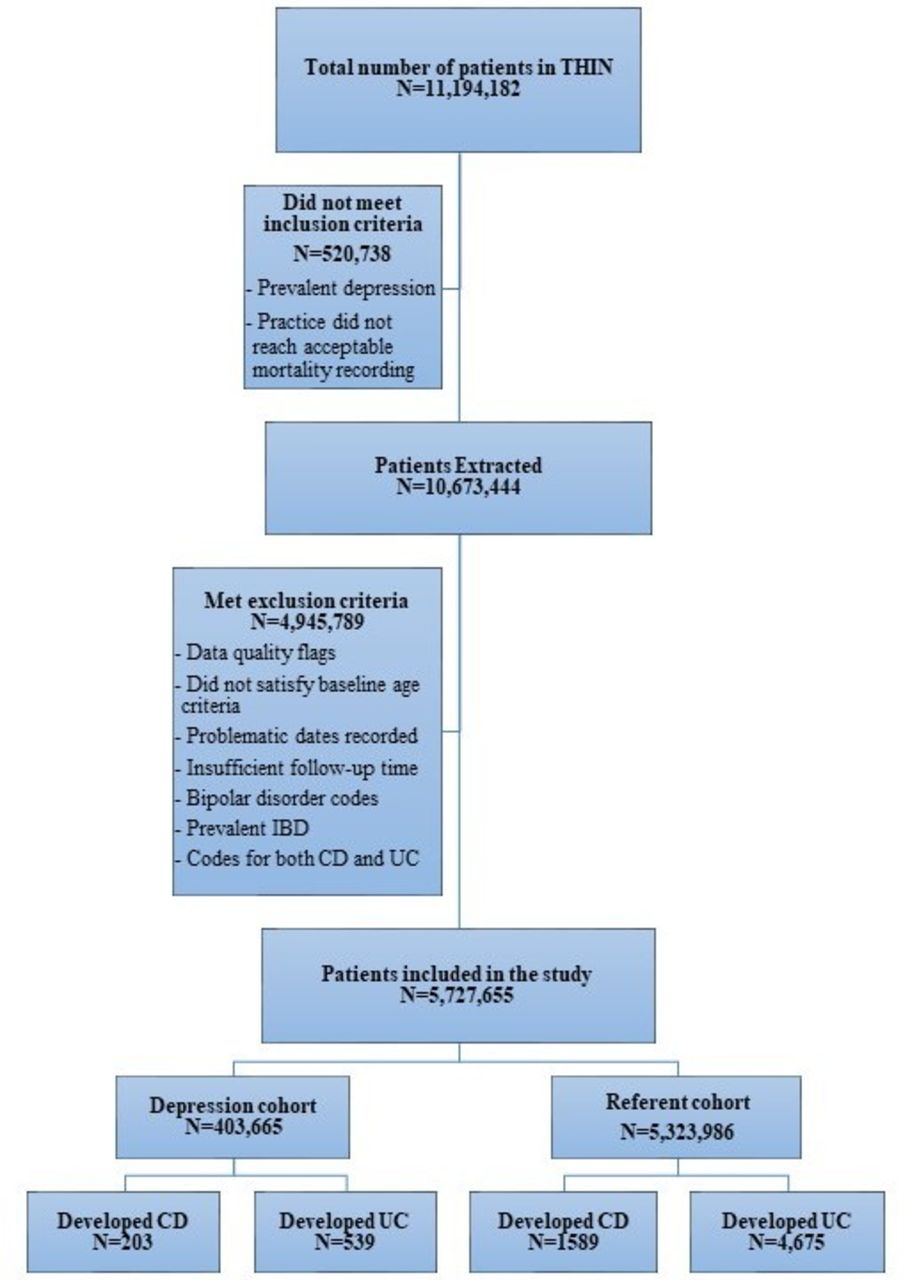
We identified 403 665 cases of depression and 5 323 986 individuals without a history of depression between 1986 and 2012 (figure 1). Median follow-up per individual was 6.7 years (IQR: 9.3). The patient characteristics are summarised in table 1. Approximately 65% of the depression cases were female compared with just 50% of the referent group (p<0.0001). During follow-up, 203 (0.05%) patients with depression and 1589 (0.03%) referent patients developed CD (p<0.0001); 539 (0.13%) of patients with depression and 4675 (0.09%) of the referent patients developed UC (p<0.0001).
{kind=link}
Flow diagram of patients in The Health Improvement Network (THIN) included in the depression to IBD analysis. CD, Crohn’s disease; UC, ulcerative colitis.
Baseline characteristics stratified by depression status
Crohn’s disease
The unadjusted hazard of developing CD among those with depression was increased 67% compared with those without depression (HR 1.67; 95% CI 1.44 to 1.93) (table 2). No evidence of effect modification was detected by age or sex (p=0.3303). After adjustment for all covariates including age, sex, socioeconomic status, comorbidities, obesity, smoking status, anxiety and the antidepressant medications, the relationship between depression and CD remained significantly elevated (HR=2.11; 95% CI 1.65 to 2.70). Current smokers had an increased rate of CD development compared with never smokers (HR 1.64; 95% CI 1.41 to 1.92). Use of SSRI (HR 0.63; 95% CI 0.50 to 0.78) and TCA (HR 0.77; 95% CI 0.61 to 0.97) was protective against CD (table 2).
HRs for the risk of Crohn’s disease or UC associated with depression in unadjusted and adjusted models
In the sensitivity analysis used to restrict observations to have at least 6 months between depression and CD diagnosis, the fully adjusted model yielded an HR of 1.89 (95% CI 1.47 to 2.44), which was similar to the fully adjusted model reported in table 2 without this restriction. Similarly, a sensitivity analysis examining a change in the initial washout period from 1 year to 5 years produced an adjusted HR of 1.99 (95% CI 1.39 to 2.84) which was comparable to the fully adjusted model reported in table 2. In a sensitivity analysis used to examine the relationship between antidepressant use and CD, the risk of CD among the depression cohort was lowest in patients treated with antidepressants (0.05%) compared with 0.07% patients developing CD among those with depression who did not use antidepressants. In the general population cohort, this risk was slightly higher among those using antidepressants with 0.04% being diagnosed with CD versus 0.03% among those who did not use antidepressants (table 3).
Proportion of patients who were prescribed an antidepressant by depression status and developed Crohn’s disease or UC compared with those who did not use antidepressants and developed Crohn’s disease or UC
Ulcerative colitis
The unadjusted hazard estimate for developing UC in those with depression was increased 41% compared with those without depression (HR 1.41; 95% CI 1.29 to 1.55) (table 2). Effect modification was not identified by age or sex (p=0.4381). After adjustment for age, sex, socioeconomic status, comorbidities, obesity, smoking status, anxiety and the antidepressant medications, the hazard of developing UC in patients with depression was 2.23 times the hazard for patients without depression (95% CI 1.92 to 2.60). Former smokers had a greater risk of disease development (HR 1.48; 95% CI 1.32 to 1.66). Use of mirtazapine (HR 0.34; 95% CI 0.15 to 0.77), SNRI (HR 0.46; 95% CI 0.25 to 0.83), SSRI (HR 0.48; 95% CI 0.42 to 0.55), serotonin modulators (HR 0.46; 95% CI 0.23 to 0.92) and TCA (HR 0.59; 95% CI 0.51 to 0.68) was protective against UC.
When restricting observations to have at least 6 months between depression and a UC diagnosis in a sensitivity analysis, the adjusted HR was 2.11 (95% CI 1.81 to 2.46), which was not substantially different from the HR that did not restrict these observations. Furthermore, a change in the initial washout period of depression to 5 years with the outcome of a UC diagnosis resulted in an HR of 2.18 (95% CI 1.75 to 2.72), which did not result in a discernable difference from the fully adjusted model using a 1 year washout. The results of a sensitivity analysis used to examine the relationship between antidepressant use and UC development revealed that the risk of UC was lowest among those with depression treated with antidepressants (0.12% vs 0.20% in non-users of antidepressants). In the general population, the risk of UC was the same between those using (0.09%) and not using antidepressant (0.09%) medications (table 3).
Discussion
Overall, we found that depression increased the rate of diagnosis of CD and UC. This is the first study to explore the temporal relationship between depression and IBD while accounting for use of antidepressants. The association between depression and IBD remained significant after adjustment of covariates and through sensitivity analyses. Treatment of depression with SSRI and TCA significantly protected against CD, whereas mirtazapine, SNRI, SSRI, serotonin modulators and TCA treatment of depression was protective for UC. Depression increases the risk of developing IBD, which may be mitigated by the use of antidepressants in the treatment of depression.
An association between depression and inflammation is well established.2 28 31 32 A recent study noted the bidirectionality between peripheral inflammation—like that in IBD—is associated with proinflammatory cytokine production and release, including tumour necrosis factor (TNF)-α, interleukin (IL)-1β and IL-6.33 34 These cytokines can activate receptors expressed on vagus nerve afferents, which in turn can alter central neurotransmitter release and behaviour.35 Administration of cytokines to healthy volunteers and animals can result in depressed mood and sickness behaviour through this mechanism.36–43 Subsequent treatment with cytokine antagonists, such as anti-TNF therapy as given in IBD, can improve disease-associated depressed behaviour.42 44
Depression is classically associated with activation of the hypothalamic-pituitary-adrenal (HPA) axis and increased circulating cortisol levels.45 46 Prolonged activation of the HPA axis, as occurs in the setting of chronic stress, or during chronic inflammation including IBD, causes chronic cortisol elevation leading to reduced sensitivity to glucocorticoid receptors.47 48 Reduced glucocorticoid receptor sensitivity can enhance immunological responses and augment inflammation, effects that in turn can increase inflammatory responses and potentially drive the expression of clinically overt IBD in patients who are at risk.49 50 This mechanism may explain, at least in part, our current observations.
Our results support findings from a recent study noting the bidirectionality of IBD and mood disorders.51 Further, our results highlight a novel impact of antidepressants in reducing the risk of patients developing IBD. Specifically, our findings indicate that SSRI use is associated with a reduced risk of developing both CD and UC. A recent systematic review identified that antidepressant therapy may indeed be beneficial in IBD, improving prognosis through both somatic symptom control and anti-inflammatory effects.52 Human studies indicate that inflamed mucosa of individuals with CD and UC has decreased colonic norepinephrine and serotonin content compared with non-diseased controls.53 54 Therefore, an increase in tissue levels of norepinephrine and serotonin induced by SSRIs and SNRIs may potentially explain how SSRIs could be protective in both CD and UC. Further, murine models have demonstrated that colonic inflammation, associated with increased tissue concentration of both TNF-α and IL-1β, is worsened by depression-like behaviour induced by reserpine-mediated monoamine depletion.55
Administration of TCAs to these murine models attenuates intestinal inflammation.55 Similarly, our study identified that TCAs are also protective against IBD. Interestingly, we found that SNRIs, serotonin modulators and mirtazapine were all protective against UC, but not CD. These differences suggest that neurotransmitter-related immune modulatory responses in these two diseases differ, however the mechanism underlying this observation remains unexplained and awaits future mechanistic studies in relevant animal models of IBD. It is likely that disease-related differences in mucosal immunity and barrier homeostasis between CD and UC play an important role in this differential response to antidepressant effects.56 57 Further, the direction of the HRs for antidepressant use and IBD was nearly all less than 1 (with the exception of MAOI that had a very low usage frequency of <0.1%). In future studies with a larger sample of individuals exposed to antidepressants, these associations could become more precise.
Unique to our study, we explored whether the effects of using antidepressants on IBD development were independent of the diagnosis of depression. We conducted a subanalysis among the general population not diagnosed with depression, but exposed to antidepressants for indications other than depression. Among the referent population the risk of CD (0.04% vs 0.03%) and UC (0.09% vs 0.09%) was similar among those exposed to antidepressants and those not exposed to antidepressants, respectively. In contrast, among individuals with a diagnosis of depression, the risk of UC was lower in those treated with antidepressants (0.12%) as compared with those not treated with antidepressants (0.2%). These data suggest that a diagnosis of depression increases the risk of IBD, and this effect may be mitigated through treating depression with antidepressants, particularly for UC. The effect of depression and treating depression on the development of IBD should be evaluated in future studies that can elucidate whether treating depression can reduce the incidence of IBD.
This study has several strengths including a large sample size allowing for powered analyses, comprehensive data on important risk factors such as anxiety, smoking, socioeconomic status and obesity. Additionally, we were able to select population-based cases that are representative of the general population.58
Despite these strengths, several limitations should be considered. First, it is possible that patients with depression or IBD may have been misclassified.59 We defined incident IBD cases using a case definition used in other studies of incident IBD in THIN,19 60 and our results remained consistent with sensitivity analyses. The case definition used for depression has been used previously21 22 and excluded individuals with a coding for bipolar depression, thereby decreasing the likelihood of misclassification. Second, our study analysed the influence of antidepressant medication, but was not able to explore the role of alternative depression therapies such as cognitive–behavioural or electroconvulsive therapy. Further, we were not able to identify the role of other important potential prognostic factors in depression such as social support.61 Third, we were not able to ascertain the severity of depression using valid tools such as the Patient Health Questionnaire-9.62 Therefore, we encourage replication of our findings in other depression data sources that are able to stratify by disease severity.
In conclusion, we have shown that depression increases the rate of diagnosis of both CD and UC. Moreover, we have found that antidepressant therapies such as TCAs, mirtazapine and SSRIs can attenuate that risk. Though the absolute risk is low, based on our findings, we recommend increasing the index of suspicion for a diagnosis of IBD in patient’s with depression and GI symptoms, and considering introduction of antidepressants.
Acknowledgments
GGK is a CIHR Embedded Clinician Research chair.
References
Footnotes
ADF and IAV contributed equally.
Contributors Study concept and design: ADF, IV, AAS, SP, GGK. Acquisition of data: ADF, IV, ML, SP, GGK. Analysis of data: ADF, IV, ML, SP, GGK. Interpretation of data: ADF, IV, AAS, ML, MGS, CB, SP, GGK. Drafting of the manuscript: ADF, IV, GGK. Critical revision of the manuscript for intellectual content: AAS, ML, MGS, CB, SP.
Funding This work was funded through a Canadian Institutes of Health Research Team Grant in Inflammation in Chronic Disease. Grant ID: THC –135231.
Competing interests MGS, AAS and GGK share a patent: TREATMENT OF INFLAMMATORY DISORDERS, AUTOIMMUNE DISEASE, AND PBC. UTI Limited Partnership, assignee. Patent 62/555,397. 7 September 2017. GGK has served as a speaker for Janssen, AbbVie and Pfizer, and has received research support from Janssen, AbbVie, GlaxoSmithKline and Shire.
Ethics approval The Conjoint Health Research Ethics Board at the University of Calgary (ID: 24423) and the UK’s IMS Health Scientific Review Committee approved the study protocol (ID: 16THIN052).
Provenance and peer review Not commissioned; externally peer reviewed.