Article Text

Abstract
Objective To evaluate the risk and predictors of hepatocellular carcinoma (HCC) in HBeAg-negative chronic hepatitis B patients of the large HEPNET.Greece cohort study who received long-term oral antivirals starting with lamivudine monotherapy.
Design Retrospective analysis of HCC incidence in HBeAg-negative chronic hepatitis B patients from a retrospective–prospective cohort who were treated with nucleos(t)ide analogue(s) starting with lamivudine monotherapy for ≥12 months.
Setting A nationwide network of liver centres.
Patients 818 patients were included: 517 with chronic hepatitis B only; 160 with compensated cirrhosis; 56 with decompensated cirrhosis; 85 with unclassified disease severity.
Interventions All patients were treated with nucleos(t)ide analogue(s) starting with lamivudine monotherapy.
Main outcome measures Development of HCC.
Results During a median follow-up of 4.7 years, HCC developed in 49 (6.0%) patients. The 5-year cumulative incidence of HCC was higher in patients with cirrhosis than in those with chronic hepatitis B only (11.5% vs 3.2%, respectively; p<0.001). HCC developed in 0.7%, 6.7% and 11.7% of patients <50, 50–60 and >60 years old, respectively (p<0.001). Virological on-therapy remission did not significantly affect the incidence of HCC in all patients or those with cirrhosis, but it showed a trend for lower HCC incidence in patients with chronic hepatitis B only (p=0.076). In multivariate analysis, age, gender and cirrhosis were independently associated with HCC risk regardless of virological remission.
Conclusions Long-term therapy with nucleos(t)ide analogue(s) starting with lamivudine monotherapy does not eliminate HCC risk in HBeAg-negative chronic hepatitis B. The risk of HCC is particularly high in patients with cirrhosis, who should remain under HCC surveillance even during effective therapy. Older age and male gender remain independent risk factors for HCC, while virological on-therapy remission does not seem to significantly reduce the overall incidence of HCC.
- Hepatocellular carcinoma
- chronic hepatitis B
- cirrhosis
- nucleos(t)ide analogues
- lamivudine
- virological remission
- antiviral therapy
- cirrhosis
- hepatitis B
- hepatocellular carcinoma
Statistics from Altmetric.com
- Hepatocellular carcinoma
- chronic hepatitis B
- cirrhosis
- nucleos(t)ide analogues
- lamivudine
- virological remission
- antiviral therapy
- cirrhosis
- hepatitis B
- hepatocellular carcinoma
Significance of this study
What is already known about this subject?
Chronic hepatitis B is still the most common underlying cause of hepatocellular carcinoma (HCC).
Treatment of chronic hepatitis B has dramatically improved over the last decade due to the introduction of nucleos(t)ide analogues.
Long-term therapy with nucleos(t)ide analogue(s) has improved the overall outcome of chronic hepatitis B, but its effect on the incidence of HCC has not been adequately studied, particularly in large ‘real-life’ cohorts.
What are the new findings?
Long-term therapy with nucleos(t)ide analogue(s) starting with lamivudine monotherapy does not eliminate the risk of HCC in HBeAg-negative chronic hepatitis B.
Older age, male gender and presence of cirrhosis remain independent risk factors for HCC even under nucleos(t)ide analogue(s).
Virological on-therapy remission does not seem to significantly reduce the overall incidence of HCC.
How might it impact on clinical practice in the foreseeable future?
All HBeAg-negative chronic hepatitis B patients with cirrhosis should remain under HCC surveillance even when they are effectively treated with nucleos(t)ide analogue(s).
Treatment of chronic hepatitis B (CHB) has dramatically improved over the last decade,1–3 but chronic hepatitis B virus (HBV) infection is still the most common underlying cause of hepatocellular carcinoma (HCC), which remains one of the most common cancers worldwide.4 Since both cirrhosis and persistently high viraemia are very important HCC risk factors in CHB,4–6 antiviral therapy could theoretically prevent HCC by inhibiting HBV replication and preventing the development of, or even reversing, cirrhosis.1–3 7–10
The current therapeutic options for CHB may be summarised as treatment with standard or pegylated interferon α (IFNα), a drug with antiviral, immunomodulatory and perhaps antitumoral activities, and treatment with oral pure antivirals.1–3 Several studies and meta-analyses suggest that IFNα may decrease the HCC incidence, with a more marked effect in sustained responders, particularly in Asian cohorts.11–16 However, most patients with CHB are currently treated with oral nucleos(t)ide analogues (NUCs). These agents are usually the preferred first choice of treatment because of the expected low efficiency, possible contraindications or poor tolerance of IFNα or they are given as a subsequent treatment when IFNα fails to achieve a sustained response.1–3
Long-term therapy with NUCs has improved the overall outcome of CHB and resulted in a substantial reduction in the need for liver transplantation,1–3 17 but its effect on HCC incidence has not been adequately studied, particularly in large ‘real-life’ cohorts. Moreover, HCC risk factors in patients with CHB receiving long-term NUC therapy have not been clarified.
In 2003, the HEPNET.Greece network was established to collect data from tertiary liver centres throughout the country and evaluate the current epidemiology and course of chronic HBV and hepatitis C virus (HCV) infection in Greece.18 19 This ongoing nationwide HEPNET.Greece cohort study has a retrospective–prospective design, with the recording of data initiated in 1997 for all patients with chronic HBV and HCV infection followed in the participating centres. The study is sponsored by the Greek government, approved and conducted through the Hellenic Center for Disease Control and Prevention (HCDCP, KEELPNO, Greece).
The aim of this study was to evaluate the risk and predictors of HCC in the patients with CHB of the HEPNET.Greece cohort who were treated with NUCs for ≥12 months. In order to have a homogeneous group, we decided to include only HBeAg-negative patients who started with lamivudine monotherapy, as they represented the vast majority of treated patients with CHB in this cohort.
Patients and methods
Patient population
All patients with HBeAg-negative CHB from the HEPNET.Greece cohort were included in this study if they were ≥16 years old and had received treatment with NUCs starting with lamivudine monotherapy for ≥12 months until November 2008. Patients with or without cirrhosis of any severity were included, while patients with HCC diagnosed before or within the first 6 months of treatment and patients with coinfection with hepatitis D, hepatitis C or HIV were excluded. Patients with HCC diagnosed between the 6th and 12th month of therapy who remained on NUCs for ≥12 months were included.
Follow-up
All patients were treated and followed at the participating centres according to the Greek guidelines of HCDCP for the treatment of chronic viral hepatitis (http://www.keelpno.gr/). In particular, the most recent (2008) Greek guidelines recommend that all patients with HBeAg-negative CHB and compensated liver disease (see next section for definition) should be treated with IFNα (preferably pegylated-IFNα) therapy for 48 weeks or with long-term NUC monotherapy, while all patients with HBV decompensated cirrhosis should be treated with NUCs if they have detectable HBV DNA. Patients with CHB treated with NUCs were expected to have a clinical examination and routine laboratory tests at least every 3 months and determination of serum HBV DNA concentrations at least every 6 months (preferably every 3 months for patients with cirrhosis) and on any biochemical breakthrough, as reported previously.20 HBV DNA concentrations were determined by various assays (in-house real-time PCR assays with sensitivity 45–80 IU/ml in 60% of samples and commercially available tests from Roche Diagnostics in 40% of samples (Amplicor HBV Monitor tests with sensitivity 80–200 IU/ml: 25%; Cobas Amplicor HBV Monitor test with sensitivity 60 IU/ml: 12.5%; Cobas TaqMan HBV test with sensitivity 15 IU/ml: 2.5%)) at the laboratory of each centre but were expressed in IU/ml after the appropriate transformation.21 In patients with cirrhosis, ultrasonography and measurement of α-fetoprotein (AFP) concentrations were performed as HCC surveillance at least every 6 months.
A structured case record form (CRF) was used for the collection of data for the HEPNET.Greece cohort study. Data were prospectively updated twice a year. In 2004, the written CRF was replaced by an electronic data form. All CRFs were submitted to the statistical and data management centre. Data quality controls were performed for detection of possible duplications, logical errors, missing values or unacceptable values, and data queries were generated and sent to the respective centre. Since 2005, the data have been reported directly to a properly set up electronic database.
Definitions
HBeAg-negative CHB was diagnosed in patients with positive HBsAg and negative HBeAg for ≥6 months and two of the following three criteria: abnormal alanine aminotransferase; HBV DNA >2000 IU/ml; liver histological lesions compatible with CHB. CHB patients were classified into cases with (a) CHB only (without cirrhosis) if they had a pretreatment liver biopsy without lesions of cirrhosis, (b) compensated cirrhosis if they had histological and/or ultrasonographic (nodules in the hepatic parenchyma, spleen >12 cm, portal vein >16 mm) and/or endoscopic (varices, portal gastropathy) findings compatible with cirrhosis, or (c) decompensated cirrhosis if they had developed ascites, variceal bleeding, encephalopathy and/or non-obstructive jaundice (bilirubin >3 mg/dl). Patients without a pretreatment liver biopsy and without any other sign of cirrhosis were classified as cases of unclassified disease severity.
Virological remission was diagnosed in patients who achieved and maintained HBV DNA undetectability (defined as concentrations <200 IU/ml) throughout therapy, virological breakthrough under therapy in patients with detectable HBV DNA after initial undetectability, and virological no response in patients who never achieved HBV DNA undetectability. Virological no remission was defined as either virological breakthrough or virological no response. Only responses to the initial therapy were taken into account in our analyses, unless otherwise stated.
The diagnosis of HCC was based on histological findings or compatible radiological findings and serum AFP >400 ng/ml.22
Entry into the study was defined as the date of lamivudine onset. Follow-up was the time interval between study entry and the last available clinical information or until December 2009. Analysis time was the time interval between study entry and HCC diagnosis or end of follow-up in the absence of HCC development.
Statistical analysis
All data were entered into, and analysed using, the statistical package Stata V.10.1. For continuous variables, median values and IQR are presented. The non-parametric Kruskal–Wallis test or the two-sided Fisher exact test was used for comparisons. Cumulative probabilities of HCC occurrence in different subgroups were estimated using the Kaplan–Meier method and compared using the log rank test. Univariable Cox proportional hazards regression models were used to estimate the effect of various variables on the hazard of HCC occurrence. Multivariable Cox proportional hazards regression analysis included all variables used in the univariable analyses. HRs with 95% CIs and p values from the Wald test are presented. p<0.05 was considered to be significant.
Results
Patient characteristics
Up until November 2008, the HEPNET.Greece cohort included 4552 adult patients with chronic HBV infection without any other viral coinfection. Of these, 3734 patients were excluded: 3386 did not fulfil the diagnosis of CHB and/or never received NUCs, 178 had received NUCs for <12 months, 72 had HBeAg-positive CHB, 66 did not start treatment with lamivudine monotherapy, and 32 had HCC diagnosed before or within the first 6 months of therapy. Thus, a total of 818 patients were included; 517 (63.2%) had CHB only, 160 (19.6%) had compensated cirrhosis, and 56 (6.9%) had decompensated cirrhosis, while the disease severity remained unclassified in 85 (10.4%). The diagnosis of compensated cirrhosis was based on histological lesions in 80 (50%) patients and on radiological and/or endoscopic findings in the remaining 80. In the latter, the diagnosis of cirrhosis was based on two or more radiological and/or endoscopic findings in 70 cases and on only one radiological finding in 10 cases. The main baseline characteristics of the 818 patients in relation to their disease severity are presented in table 1.
Main baseline characteristics of 818 patients with HBeAg-negative chronic hepatitis B treated with nucleos(t)ide analogue therapy starting with lamivudine monotherapy in relation to the severity of the liver disease
Virological remission during lamivudine monotherapy was maintained in 228 (27.9%), while virological no remission was observed in 578 (70.7%) patients. Virological response could not be determined in 12 (1.5%) cases. During follow-up, lamivudine monotherapy changed to a combination or another NUC therapy in 402 (49.1%) patients. Rescue therapy (adefovir and lamivudine, 68%; adefovir alone, 27.5%; entecavir, 3%; entecavir and adefovir, 1.5%) was started at a median of 1.4 (0.3–2.5) years after breakthrough detection in patients with virological breakthrough or after lamivudine onset in patients with virological no response.
Regarding the major outcomes, three patients with baseline compensated cirrhosis and virological no response developed decompensated cirrhosis (HCC developed in one of them), while 33 patients died and one patient with baseline decompensated cirrhosis underwent liver transplantation. Patients with baseline cirrhosis were more likely than those without to die from liver-related causes (12/216 (5.6%) vs 9/517 (1.7%), p=0.013) or from HCC only (6/216 (2.8%) vs 4/517 (0.8%), p=0.072), whereas death rates from causes unrelated to the liver were similar in the two groups (2/216 (0.9%) vs 6/517 (1.2%), p=0.660). In total, 180 (22%) patients were lost to follow-up, as no information was available for them during the last ≥1.5 years of the study period.
Risk factors for HCC
During a median follow-up of 4.7 years, HCC was diagnosed in 49 (6.0%) of the 818 patients (CHB only, 20/517 (3.9%); cirrhosis, 22/216 (5.6%); p=0.001). The cumulative HCC incidence was 0.7%, 2.1%, 3.8% and 5.6% at 1, 2, 3 and 5 years, respectively, being significantly higher in patients with cirrhosis than in those without (p<0.001) (figure 1) and tending to be higher in patients with decompensated cirrhosis than in those with compensated cirrhosis than in those with CHB only (p=0.097) (table 2).

Cumulative incidence of hepatocellular carcinoma (HCC) in 818 patients with HBeAg-negative chronic hepatitis B (CHB) with or without cirrhosis treated with nucleos(t)ide analogue(s) starting with lamivudine monotherapy in relation to disease severity. The HCC incidence was significantly higher in patients with cirrhosis than in those without (p<0.001, log rank test).
Development of hepatocellular carcinoma (HCC) in 818 patients with HBeAg-negative chronic hepatitis B treated with nucleos(t)ide analogue(s) therapy starting with lamivudine monotherapy in relation to the severity of the liver disease
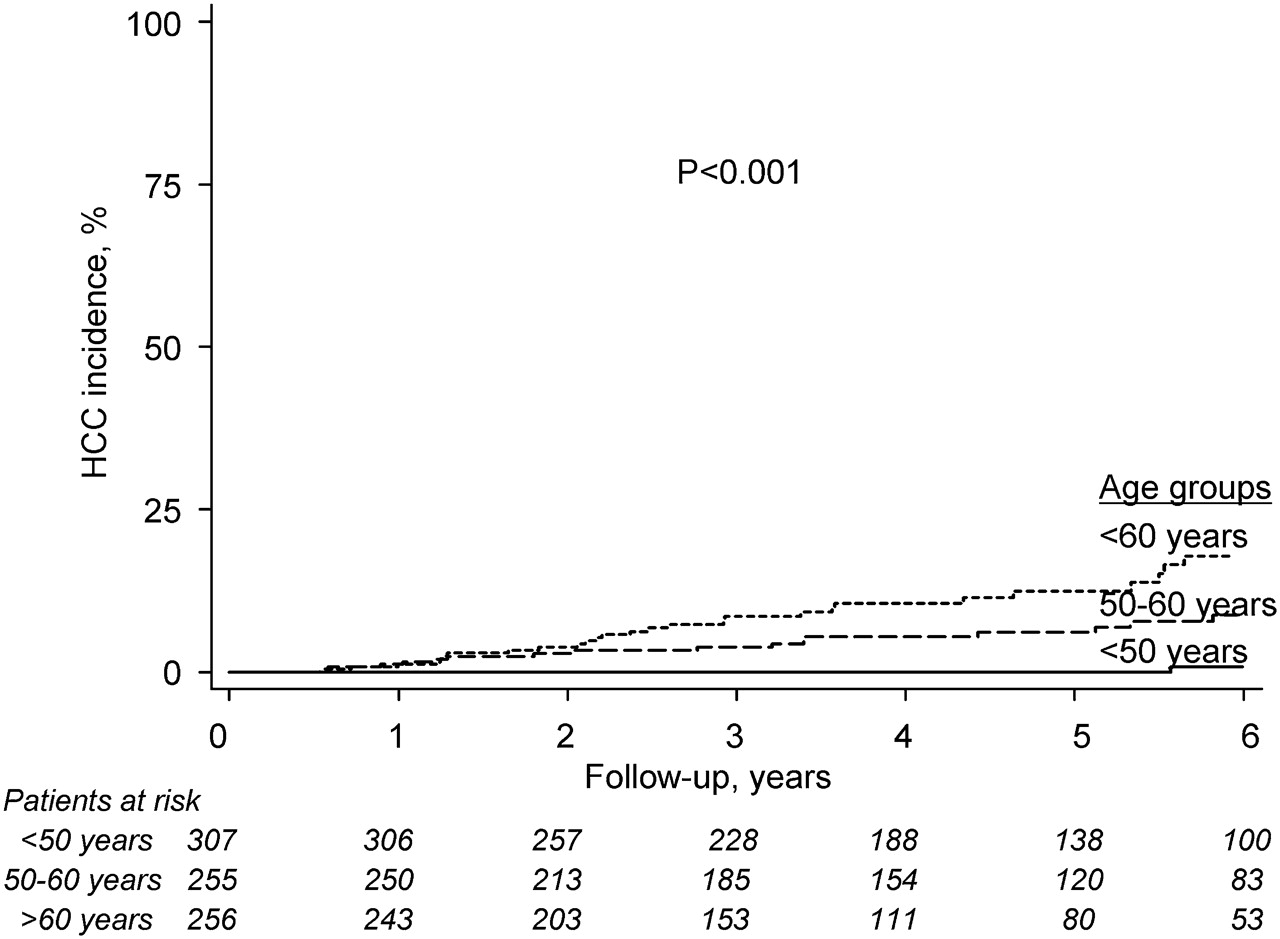
In univariable Cox regression analyses, the HCC risk was significantly higher in patients with cirrhosis (p<0.001), older age (p<0.001), lower albumin concentrations (p=0.044), lower haemoglobin concentrations (p=0.001) and lower platelet counts (p=0.039), while male patients tended to develop HCC more frequently (p=0.076) (table 3). Regarding age, HCC developed in only 0.7% (2/304) of patients younger than 50 years, 6.7% (17/254) of patients aged 50–60 years, and 11.8% (30/255) of patients over 60 years (p<0.001, log rank test) (figure 2). Older age and lower platelet counts were also found to increase the HCC risk in patients with CHB only, while older age and lower haemoglobin concentrations were found to increase the HCC risk in cirrhotic patients (table 3).
Risk factors for the development of hepatocellular carcinoma (HCC) in 818 patients with HBeAg-negative chronic hepatitis B treated with nucleos(t)ide analogue(s) therapy starting with lamivudine monotherapy. Results of univariable Cox regression analyses

Cumulative incidence of hepatocellular carcinoma (HCC) in 818 patients with HBeAg-negative chronic hepatitis B with or without cirrhosis treated with nucleos(t)ide analogue(s) starting with lamivudine monotherapy in relation to age group. The HCC incidence was significantly higher in patients over 60 years than in those between 50 and 60 years than in those younger than 50 years (p<0.001, log rank test).
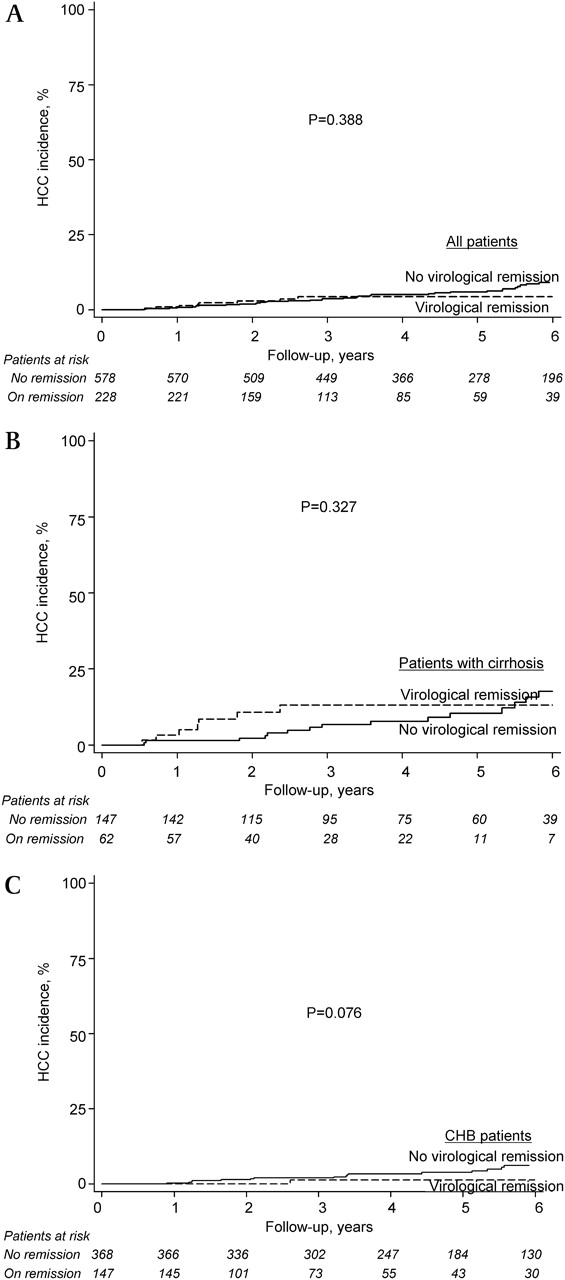
HCC was diagnosed in 3.6% (8/228) of patients with virological remission and 7.1% (41/578) of patients without virological remission during lamivudine monotherapy (p=0.388, log rank test). In the eight patients with virological remission, HCC was diagnosed at a median of 15 (range 7–30) months after the start of lamivudine treatment or 8 (1–25) months after the induction of virological remission. Of these eight patients, seven had cirrhosis (decompensated: five) and one severe fibrosis (Ishak's stage: four) at baseline. In 12 patients with no virological response, HCC was diagnosed at a median of 22 (8–60) months after the start of lamivudine treatment. In 29 patients with virological breakthrough, HCC was diagnosed in six cases at a median of 2 (0–4) months before, and in 23 cases at a median of 18 (2–68) months after, the detection of virological breakthrough. In univariable Cox regression analysis, the HCC risk did not differ significantly between patients with and without virological remission under lamivudine monotherapy (HR 0.49; 95% CI 0.12 to 2.03; p=0.322) (table 3). Ten patients with HCC and no virological remission under lamivudine treatment received rescue therapy at a median of 12 (range 4–40) months after the onset of lamivudine or virological breakthrough. After the onset of rescue therapy, HCC developed at a median of 4 (2–8) months in six patients who had not achieved virological remission, at 22 and 50 months in two who had an initial virological response and subsequent breakthrough before HCC diagnosis, and at 24 and 32 months in two remaining in virological remission for 36 and 12 months. Among the 402 patients who received rescue therapy, virological response to rescue therapy was not found to have a significant effect on HCC incidence (HR 0.41; 95% CI 0.03 to 1.53; p=0.123).
There was a marginally significant interaction between cirrhosis status and virological response (p=0.056). HCC developed in 0.7% (1/147) and 5.2% (19/368) of non-cirrhotic patients with CHB with or without virological remission (p=0.020) as well as in 11.3% (7/62) and 10.2% (15/147) of cirrhotic patients with or without virological remission under lamivudine monotherapy (p=0.990), respectively. A trend for a higher HCC incidence was observed in non-cirrhotic patients with CHB without virological on-therapy remission than those with (p=0.076, log rank test), while virological remission did not have a significant effect on HCC incidence in cirrhotic patients (p=0.327 for all cirrhotics, p=0.600 for compensated cirrhotics, p=0.094 for decompensated cirrhotics) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Cumulative incidence of hepatocellular carcinoma (HCC) in 818 patients with HBeAg-negative chronic hepatitis B (CHB) with or without cirrhosis treated with nucleos(t)ide analogue(s) starting with lamivudine monotherapy in relation to their virological response. Maintenance of on-therapy virological remission did not significantly affect the HCC incidence in all patients (p=0.388, log rank test) (A) or in patients with compensated or decompensated cirrhosis (p=0.327, log rank test) (B), but it showed a trend for lower HCC incidence in patients with CHB without cirrhosis (p=0.076, log rank test) (C).
The effect of virological remission under lamivudine monotherapy on HCC incidence did not significantly change when patients with HCC diagnosed between the 6th and 12th month of therapy were not taken into account (p=0.292). However, when HCC cases diagnosed between the 6th and 24th month were omitted, the HCC incidence was found to be marginally non-significantly lower in patients with virological remission than in those without (p=0.062, log rank test).
Multivariable Cox regression analysis including all variables that appear in table 3 showed that only baseline age, gender and presence of cirrhosis were independently associated with the HCC risk (table 4). In patients with cirrhosis, baseline age, but not gender, remained an independent significant HCC risk factor, while the severity of cirrhosis showed a trend but did not reach statistical significance. In non-cirrhotic patients, both age and gender remained independent significant HCC risk factors, while virological on-therapy remission showed a trend to being an independent risk factor (p=0.076) (table 4). Moreover, in the non-cirrhotic patients, virological on-therapy remission was significantly associated with lower HCC risk (adjusted HR 0.12; 95% CI 0.01 to 0.93; p=0.042) when age was included in the model as a continuous variable.
Independent risk factors for the development of hepatocellular carcinoma (HCC) in 818 patients with HBeAg-negative chronic hepatitis B treated with nucleos(t)ide analogue(s) therapy starting with lamivudine monotherapy. Results of multivariable Cox regression analyses
When the effect of age was evaluated in combination with other HCC risk factors, no significant interactions between age and gender (p=0.712 in univariate analysis and p=0.696 when adjusted for all other factors presenting in table 4) or between age and liver disease severity (p=0.437 and p=0.234, respectively) were found. However, there were some indications that the age effect might differentiate according to virological remission (p=0.118 and p=0.121, respectively). In particular, the age effect remained significant in subjects without virological remission (p<0.001, log rank test), but not in those maintaining on-therapy virological remission (p=0.535). The event rates by age group and gender, liver disease severity and virological remission under therapy are presented in table 5. The highest HCC rates were observed in patients older than 60 years who were male (14.6%) or cirrhotic (14.9%) or without virological remission (15.6%), while the HCC rate in patients above 60 years who maintained virological remission was only 5.5%.
Development of hepatocellular carcinoma (HCC) in 818 patients with HBeAg-negative chronic hepatitis B treated with nucleos(t)ide analogue(s) therapy starting with lamivudine monotherapy in relation to their age and other risk factors
Discussion
Our findings show that HBeAg-negative patients with CHB treated with long-term NUCs starting with lamivudine monotherapy remain at risk of developing HCC. Whether the incidence of HCC would have been higher if such patients had remained untreated cannot be answered by our data, as there were no untreated controls. In a previous cohort study from Greece, including untreated historical controls, and in a large randomised placebo-controlled study from Asia, lamivudine therapy was shown to reduce the incidence of HCC in patients with CHB with or without compensated cirrhosis.17 20 In fact, the beneficial effects of lamivudine monotherapy, compared with placebo, on liver disease progression and even on HCC development observed in the Asian trial not only resulted in the early termination of the study but also made unethical the future design of placebo-controlled studies including patients with CHB.17 So, more specific questions, such as the effect of antiviral therapy on survival, the detection of patient subgroups who can obtain the greatest therapeutic benefit, or the effect of response to initial and/or rescue therapy on the patient outcome, can no longer be answered by placebo-controlled trials and can be evaluated only in large cohort studies. In any case, long-term therapy with NUCs may reduce, but does not definitely eliminate, the risk of HCC in patients with CHB.
The severity of liver disease was found to significantly affect the HCC risk. The cumulative HCC incidence was highest in our patients with decompensated cirrhosis (approaching 20% at 5 years), but high even in patients with compensated cirrhosis (approaching 10% at 5 years), compared with patients without cirrhosis (<4% at 5 years). Cirrhosis is a well-known strong risk factor for HCC among untreated chronic HBV patients,4 5 23 while previous data have shown that the HCC risk remains high in cirrhotic patients receiving lamivudine. In particular in two previous large studies with cirrhotic patients receiving lamivudine, HCC was diagnosed in 8.3% (38/458) of patients with compensated cirrhosis and only 0.8% (4/529) of non-cirrhotic patients with CHB followed for a median of 24–32 months,17 24 rates that are comparable to those observed in our cohort. The strong effect of baseline cirrhosis on HCC risk during NUC therapy was also confirmed in a recent systematic review including 3287 patients with CHB.25 Only cirrhotic patients underwent HCC surveillance in our study, and such a different follow-up strategy may have affected the higher and/or earlier HCC incidence in the cirrhotic patients. On the other hand, the cirrhosis effect may have been underestimated, as some of the initially non-cirrhotic patients with virological no response or breakthrough could have developed HCC after progressing to cirrhosis during therapy, which was not diagnosed without a new liver biopsy. In any case, the high HCC risk in HBV cirrhosis of any severity despite the long-term NUC therapy supports the recommendations for close HCC surveillance in such patients even under treatment.
Older age and male gender, which are also well-known HCC risk factors in untreated patients,4 5 23 were found to be independent factors associated with higher HCC incidence in our patients receiving long-term NUC therapy. In particular, the HCC rates were extremely high in specific subgroups of patients, with more than one risk factor being highest (15%–16%) in male patients, or cirrhotic patients, or patients without virological remission who were older than 60 years. In a recent large, long-term cohort study, older age, cirrhosis, low albumin, high bilirubin and high serum HBV DNA concentrations were found to represent independent HCC risk factors even after adjustment for antiviral therapy.26 Low albumin concentrations were also found to be HCC risk factors in all our patients, but only in the univariable analyses (table 3), while bilirubin and HBV DNA concentrations were not among the HCC risk factors in our cohort. The results of the two studies, however, cannot be easily compared, as few of our patients had low albumin and high bilirubin concentrations, while no conclusion can be reliably drawn on the possible predictive effect of HBV DNA concentration at the onset of treatment with NUCs in the Yang et al study.26
The induction and maintenance of on-therapy virological remission was not observed to significantly reduce the overall HCC incidence in our patients. The absence of a universal HBV DNA assay represents a limitation of our study, but the use of one common HBV DNA test is almost impossible in such a long-term multicentre, ‘real-life’ cohort study. Moreover, we do not think that the use of different HBV DNA assays, but with close sensitivities, substantially affected our findings. The absence of an association between virological remission and the overall HCC incidence seems to be in contrast with the well-known association between high levels of HBV replication and increased HCC risk,6 but there may be some explanations. First, viral suppression may decrease, but cannot eliminate, the HCC risk in patients with chronic HBV,17 20 24 because HBV DNA may have already integrated into the host genome before the onset of treatment and may have already resulted in genomic alterations and/or chromosomal instability.27 28 In addition, some of the tumours may already have developed before the start of treatment, but not detected at baseline by our routine HCC screening methods. This hypothesis is in agreement with the finding that the maintenance of virological on-therapy remission approached statistical significance for reduction of HCC incidence when HCC cases diagnosed within the first 24 months of therapy were excluded from the analysis (p=0.062).
The absence of an association between virological remission and the overall HCC incidence in our study seems to be in contrast with the findings of a recent systematic review.25 Differences in the patients' baseline characteristics may be responsible for this seemingly contradictory finding. In fact, a large proportion of patients in the systematic review were HBeAg positive (49%) and/or Asians (48%) and relatively young (mean age <50 years in five of the 16 studies with NUC-naive patients), while only HBeAg-negative Caucasian patients with a mean age of 54 years were included in our study. Moreover, the possible different effect of virological remission on the HCC risk in relation to the severity of liver disease may also be responsible for this discrepancy. Virological on-therapy remission under lamivudine monotherapy had no effect on the incidence of HCC in our patients with cirrhosis, but showed a trend for reduced incidence of HCC in our non-cirrhotic patients (p=0.076), which remained close to, or reached, statistical significance in multivariable analysis models (p=0.076 or p=0.042). Interestingly, this differentiated effect of virological remission persisted even after other predictor factors were controlled for (p for interaction: 0.031). In fact, HCC developed in only one (<1%) of our 147 non-cirrhotic patients remaining in virological remission compared with 5.2% (19/368) of those without maintained virological response (p=0.020). The beneficial effect of virological remission in non-cirrhotic patients is in agreement with the findings of the systematic review,25 but caution is required in interpreting the results for cirrhotic patients. Only two relatively small studies (22 and 59 patients) included in the systematic review provided clear data for the effect of virological remission on HCC incidence among cirrhotic patients.29 30 In these 81 cirrhotic patients, who were younger (mean age 53 vs 59 years) and had more active liver disease (higher baseline alanine aminotransferase and HBV DNA) compared with our 216 cirrhotic patients, HCC was reported to develop in 8.3% of those remaining in virological remission and 37.8% of those without virological remission (11.3% and 10.2% in our study, respectively). If our study had been published earlier and included in the systematic review, virological on-therapy remission would not have been found to decrease the HCC incidence in cirrhotic patients (10/98 (10.2%) vs 32/192 (16.7%), p=0.193).
The latter findings suggest that the potential for malignant transformation of hepatocytes remains in cirrhotic patients even in the absence of HBV replication,4 5 23 while persistent viral replication appears to be critical for HCC development in non-cirrhotic patients with CHB. Thus, the HCC risk appears to remain high in HBeAg-negative patients with established cirrhosis even under effective NUC therapy, which has been reported to reverse the histological lesions of cirrhosis in some cases.3 9 10
In conclusion, long-term therapy with NUCs starting with lamivudine monotherapy does not eliminate the HCC risk in HBeAg-negative patients with CHB, especially those with pre-existing cirrhosis. Older age and male gender remain independent HCC risk factors among patients with CHB receiving NUC treatment. The induction and maintenance of virological on-therapy remission does not seem to significantly reduce the overall HCC incidence. However, virological on-therapy remission has a trend for a protective effect in patients with HBeAg-negative CHB without cirrhosis, but no effect on the high HCC risk in patients with established cirrhosis, who should remain under HCC surveillance even when they are under an effective antiviral regimen.
Acknowledgments
We thank the Hellenic Center for Disease Control and Prevention (HCDCP, KEELPNO, Greece) for sponsoring the HEPNET.Greece network.
References
Footnotes
See Commentary, p 1025
Linked article 236521.
Funding Hellenic Center for Disease Control and Prevention (HCDCP, KEELPNO, Greece).
Competing interests GVP: Advisory Board and/or Speaker for Bristol-Myers Squibb, Gilead, Novartis Pharmaceuticals, Roche, Schering-Plough; Research grants from Bristol-Myers Squibb, Gilead, Roche. SM: Advisory Board and/or Speaker for Bristol-Myers Squibb, Gilead, Novartis Pharmaceuticals, Roche, Schering-Plough. TV: Advisory Board for Gilead, Roche. KM: Advisory Board for Bristol-Myers Squibb, Schering-Plough; Research grants from, Gilead, Novartis Pharmaceuticals, Roche. EKM: Speaker for Bristol-Myers Squibb; Research grants from Gilead, Roche. The remaining authors have no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.