Article Text

Abstract
Background Previous studies examining the incidence of colorectal cancer after polypectomy have provided discordant findings. The aim of this study was to compare the risk of colorectal cancer after adenoma removal in routine clinical practice with the risk in the general population.
Design Cohort study based on detailed data from a population-based registry that has collected all cases of both colorectal cancers and adenomas diagnosed in a clearly-defined population since 1976.
Setting French administrative area of Côte-d'Or (Burgundy).
Methods Residents of the area diagnosed for the first time with colorectal adenoma between 1990 and 1999 were included (n=5779). Initial and follow-up data until December 2003 were used to calculate the colorectal cancer standardised incidence ratio (SIR) and cumulative probabilities after adenoma removal.
Results After a median follow-up of 7.7 years, 87 invasive colorectal cancers were diagnosed whereas 69 cases were expected. Compared with the general population, the overall SIR was 1.26 (95% CI 1.01 to 1.56). The risk of colorectal cancer depended on the characteristics of the initial adenoma (SIR 2.23 (95% CI 1.67 to 2.92) for advanced adenomas and 0.68 (95% CI 0.44 to 0.99) for non-advanced adenomas). In cases of advanced adenomas, the SIR was 1.10 (95% CI 0.62 to 1.82) in patients with colonoscopic follow-up and 4.26 (95% CI 2.89 to 6.04) in those without. The 10-year cumulative probabilities of colorectal cancer were, respectively, 2.05% (95% CI 1.14% to 3.64%) and 6.22% (95% CI 4.26% to 9.02%).
Conclusions In routine practice, the risk of colorectal cancer after adenoma removal remains high and depends both on initial adenoma features and on colonoscopy surveillance practices. Gastroenterologists should encourage patients to comply with long-term colonoscopic surveillance.
- Colorectal cancer risk
- colorectal adenomas
- polypectomy
- colonoscopic surveillance
- population-based registry
- cancer epidemiology
- dietary - colon cancer
- cancer registries
- colonoscopy
- adenoma
- cancer
- cancer prevention
- colorectal cancer
- dietary factors
- epidemiology
Statistics from Altmetric.com
- Colorectal cancer risk
- colorectal adenomas
- polypectomy
- colonoscopic surveillance
- population-based registry
- cancer epidemiology
- dietary - colon cancer
- cancer registries
- colonoscopy
- adenoma
- cancer
- cancer prevention
- colorectal cancer
- dietary factors
- epidemiology
Significance of this study
What is already known about this subject?
Previous prospective studies suggest a marked decrease in the risk of colorectal cancer after adenoma removal.
Such studies were conducted under highly standardised conditions among selected patients.
The effectiveness of endoscopic adenoma removal is less clear in population-based studies.
What are the new findings?
In routine clinical practice, the risk of colorectal cancer after advanced adenoma removal remained higher than in the general population, but the risk was reduced after non-advanced adenoma.
Follow-up colonoscopy seems to be effective in reducing the risk of colorectal cancer among patients with adenoma from the general population.
Compliance with colonoscopic surveillance has to be improved among patients with adenoma.
How might it impact on clinical practice in the foreseeable future?
This study reinforces the importance of careful and long-term surveillance, particularly among patients with advanced adenoma.
Improving the compliance of adenoma patients with guidelines on colonoscopic surveillance is a major challenge for general practitioners and gastroenterologists.
Background
In France, as in other European countries and in North America, colorectal cancer is the second most common cancer with an estimated 37 400 new cases in 2005, and the second most common cause of death by cancer.1 ,2 There is indirect evidence that most cancers arise from an adenoma, a very common lesion, in a multistep process. Adenomas >10 mm in diameter with high-grade dysplasia or a villous component have a high potential for malignant transformation.3
Although colonoscopy is the most sensitive method for detecting and removing colorectal adenomas, it carries some risks for the patient, it is costly for society and its acceptability is sometimes low. Thus, in France, as in many countries, colonoscopy is only used in symptomatic patients, individuals with positive faecal occult blood tests or those at high risk, particularly with a family or personal history of colorectal cancer.4 Surveillance colonoscopy is also recommended in individuals who have had one or more adenomas removed at colonoscopy because of their increased risk of developing metachronous colorectal neoplasms.4 ,5 National guidelines on post-polypectomy surveillance were produced in 1998 by the French National Consensus Conference.6 However, before this date, professional societies and experts published recommendations which were similar to those published in 1998 and used by most gastroenterologists.7 ,8 A recent pooled analysis of eight prospective studies with scheduled surveillance colonoscopies showed that, during a median follow-up period of 47.2 months, 11.2% of patients with adenoma were diagnosed with advanced colorectal adenomas at surveillance colonoscopy, and 0.6% with invasive cancer.9
Previous studies that examined the risk of colorectal cancer after adenoma removal provided discordant findings, largely explained by differences in study design, in studied populations, or in reference groups.10–22 Moreover, some of these studies performed under highly standardised conditions did not reflect the reality of routine adenoma removal and follow-up practices. We hypothesise that, given current colonoscopic practices, the long-term incidence of colorectal cancer could be higher than expected in adenoma patients within the general population, and that the excess risk may depend on the initial characteristics of the removed adenomas and on compliance with follow-up colonoscopy. This hypothesis is partly supported by the results of the only recent population-based study on the topic which suggested that Dutch patients with adenoma were at increased risk of colorectal cancer compared with the general population.11 However, this study did not provide detailed data on initial adenoma characteristics nor information on colonoscopic surveillance practices in the general population. The advantage of the population-based Registry of Côte-d'Or is that it has collected detailed data on all cases of both colorectal cancers and adenomas diagnosed in a well-defined population. Based on these data, the aim of this study was to estimate the risk of colorectal cancer in patients with adenoma within the general population followed-up in routine practice, both overall and according to the initial characteristics of the patients and adenomas and to colonoscopic follow-up practices.
Methods
Study design
Patients were identified from the population-based registry of colorectal polyps in Côte-d'Or (Burgundy, France), which includes data on all cases of colorectal adenomas diagnosed since 1976. There were 506 755 residents in the area covered by the registry, according to the 1999 census.
The study population comprised all residents of Côte-d'Or diagnosed for the first time with a colorectal adenoma between 1 January 1990 and 31 December 1999 (n=7043).
As shown in figure 1, we excluded patients with known familial polyposis or hereditary non-polyposis colorectal cancer syndrome, inflammatory bowel disease, a personal history of adenoma or colorectal cancer, or with synchronous colorectal cancer (n=770). Colorectal cancer or adenomas diagnosed within 1 year of the initial colonoscopy were assumed to have been present during the initial investigation. Thus, these lesions were considered as being present at the first colonoscopy. This strategy resulted in the exclusion of 42 patients who developed colorectal cancer during the first year after adenoma diagnosis, and patients who died or were followed-up for <1 year (n=452). The final analysis included 5779 patients.

Study flow diagram.
Information on adenoma cases is routinely obtained from all public and private pathology laboratories in the area. Pathology reports were used to classify adenomas according to histological architecture, grade of dysplasia, size and location. For patients with multiple adenomas, the most severe adenoma was used for classification. Advanced adenomas were defined as adenomas with a diameter ≥10 mm and/or a villous component and/or high-grade dysplasia (severe dysplasia or intramucosal carcinoma). Adenoma location was defined according to the 10th International Classification of Diseases for Oncology23 and classified into: proximal colon (caecum, ascending colon, hepatic flexure and transverse colon), distal colon (splenic flexure, descending colon and sigmoid) and rectum (rectosigmoid junction and rectum ampulla).
In France, colonoscopies are performed only by trained gastroenterologists in public or private hospital endoscopic units. The medical records of the gastroenterologists were reviewed to obtain missing information such as age, sex, family history of colorectal tumours, adenoma size and adenoma location. For the present study, all follow-up colonoscopies were collected and their findings recorded until the study end-point date (31 December 2003) or the last known follow-up date. A follow-up colonoscopy was defined as an examination performed between 1 year after first adenoma removal and the end-point date or the date of cancer diagnosis. The colonoscopy that detected colorectal cancer was considered as a follow-up colonoscopy only if the patient was asymptomatic and if the reason for colonoscopy was clearly stated as surveillance of previous colorectal lesions. The vital status of adenoma patients was obtained from multiple sources including national mortality files (National Register for the Identification of Physical Persons), gastroenterologists and general practitioners' medical records, and hospital discharge files. Follow-up information was obtained for 96.4% of the patients with adenoma included in the present study.
In addition, the cancer registry collects all cases of digestive cancers including colorectal cancers. Data are regularly collected from public and private pathology laboratories, university and local hospitals, the Comprehensive Cancer Centre, private specialists (gastroenterologists, surgeons, oncologists, radiotherapists), general practitioners, as well as from the French National Health Service and the monthly review of death certificates. The quality and comprehensiveness of registration is certified every 4 years by an audit of the National Institute for Health and Medical Research (INSERM) and of the National Public Health Institute (InVS). Cancer registry activities were approved by the Burgundy Medical Ethics Committee and the National Commission for Data Processing and Liberties (CNIL). Data from the cancer registry were used to identify patients with adenoma who developed metachronous cancer and to provide reference incidence data in the Côte-d'Or population. The registry also allows patients with a history of colorectal cancer or synchronous colorectal cancer to be identified. Only invasive colorectal cancers were considered.
Statistical analysis
Person-time was calculated for patients with adenoma over a period beginning 1 year after the date of diagnosis of first adenoma until the date of invasive colorectal cancer diagnosis or the date of death or the last available medical follow-up or the end-point date (December 2003), whichever came first. The number of person-years was calculated by sex and 5-year age group. The sex and age-specific colorectal cancer incidence rates in the general population were obtained from the cancer registry. The expected number of colorectal cancers was calculated by multiplying incidence rates in the general population by the observed sex and age-specific number of person-years at risk in the study population. The ratio of observed to expected cases of colorectal cancer was reported as a standardised incidence ratio (SIR). The calculation of 95% CIs was based on the exact Poisson distribution.24 Cumulative colorectal cancer probabilities were calculated using the Kaplan–Meier method and expressed with 95% CI.
Statistical analyses were performed using STATA V.10.0 (Stata Corporation).
Results
Study population
Between 1990 and 1999, a total of 5779 patients from Côte-d'Or who underwent adenoma removal for the first time were included. Their mean (SD) age was 61.1 (12.9) years in men and 62.2 (13.6) years in women (p<0.001). A family history of colorectal cancer was reported in 9.8% of patients (table 1). During the initial colonoscopy, advanced adenomas were removed in 32.9% of patients and multiple adenomas in 25.9% of patients. For patients with available information on completeness of colonoscopy, the examination reached the caecum in 86.9% of patients. Among the 3842 patients for whom the reason for initial colonoscopy was known, the colonoscopy was performed because of symptoms in 3364 patients (87.6%), a family history of colorectal cancer in 263 (6.8%), a positive faecal occult blood test in 155 (4.0%) and individual screening in 60 (1.6%).
Characteristics of patients and their adenomas upon initial examination
Overall risk of colorectal cancer after first adenoma removal
The median follow-up was 7.7 years (interquartile range (IQR) 5.2–10.5) after diagnosis of the adenoma. After exclusion of the first year following adenoma removal, the total number of person-years at risk was 39 712. During follow-up, 87 invasive colorectal cancers were diagnosed in the study population whereas 69.0 cases were expected. Thus, compared with the general population, the risk of colorectal cancer was significantly increased after first adenoma removal (SIR 1.26 (95% CI 1.01 to 1.56)). The median time period between first resection of adenoma and diagnosis of invasive colorectal cancer was 4.8 years (IQR 2.8–7.7). The distribution of TNM stages in cancer patients was 55 with stages I or II (63.2%) and 32 with stages III, IV or unclassified (36.8%).
Risk of colorectal cancer after resection of advanced and non-advanced adenoma
At initial colonoscopy, 1899 patients had initial advanced adenomas and 3236 had only non-advanced adenomas (figure 1). As indicated in table 2, among the 53 cancers diagnosed after initial advanced adenoma, 18 (34.0%) were diagnosed 12–36 months after adenoma removal. Among patients with non-advanced adenoma, four of 26 (15.4%) were diagnosed between 12 and 36 months.
Standardised incidence ratio (SIR) of colorectal cancer after first adenoma removal according to characteristics of patients and adenomas
As shown in table 2, the SIRs were noticeably different between patients with an advanced adenoma (SIR 2.23 (95% CI 1.67 to 2.92)) and those with a non-advanced adenoma (SIR 0.68 (95% CI 0.44 to 0.99)). In patients with an advanced adenoma, the SIRs were significantly increased regardless of sex, age, number or location of adenomas and the time period since adenoma diagnosis. In patients with a non-advanced adenoma, the SIRs were consistently <1 regardless of the studied group, even though they did not reach the significance level.
Colonoscopic follow-up
As shown in figure 1, information on colonoscopic follow-up was available for 4881 patients (84.5%). These patients were younger and more often had a family history of colorectal cancer and an advanced adenoma at the baseline colonoscopy than patients without information on colonoscopic follow-up. Among these 4881 patients, 2834 (58.1%) had had at least one follow-up colonoscopy. The follow-up colonoscopies revealed that 1071 patients (37.8%) had no polyps, 636 (22.5%) had only non-adenomatous polyps, 286 (10.1%) had developed new advanced adenomas, 838 (29.6%) had non-advanced adenomas and 3 (0.1%) had an invasive colorectal cancer.
Table 3 shows that colonoscopic follow-up had a marked effect on the risk of colorectal cancer, especially in patients with an advanced adenoma. The risk fell to that found within the general population if patients with an advanced adenoma had at least one follow-up colonoscopy (SIR 1.10 (95% CI 0.62 to 1.82)), while this risk was more than four times higher in patients without follow-up colonoscopy (SIR 4.26 (95% CI 2.89 to 6.04)). After resection of non-advanced adenomas, the risk of colorectal cancer tended to be lower than that found within the general population, especially when patients had at least one follow-up colonoscopy (SIR 0.60 (95% CI 0.30 to 1.07)), even if the SIR did not reach the significance level.
Standardised incidence ratio (SIR) of colorectal cancer after first adenoma removal according to colonoscopic follow-up
As detailed in table 4, the overall proportion of advanced TNM stage cancers (TNM III/IV/unclassified) tended to be higher among patients without colonoscopic follow-up than in the other groups. This trend was mainly due to patients with an initial advanced adenoma; the proportion of advanced stage cancers was 28.3% among patients with advanced adenoma without colonoscopic follow-up and 7.5% among those with a known colonoscopic follow-up.
Proportion of advanced TNM stage colorectal cancers according to the initial features of first adenomas removed and colonoscopic follow-up
Cumulative probabilities of colorectal cancer
Overall, the cumulative probabilities of developing colorectal cancer after adenoma removal were 0.83% (95% CI 0.62% to 1.12%) at 5 years and 1.89% (95% CI 1.49% to 2.39%) at 10 years. Corresponding figures were, respectively, 1.94% (95% CI 1.39% to 2.70%) and 3.95% (95% CI 2.91% to 5.36%) in patients with advanced adenomas, and 0.26% (95% CI 0.13% to 0.53%) and 0.90% (95% CI 0.58% to 1.40%) in patients with non-advanced adenomas.
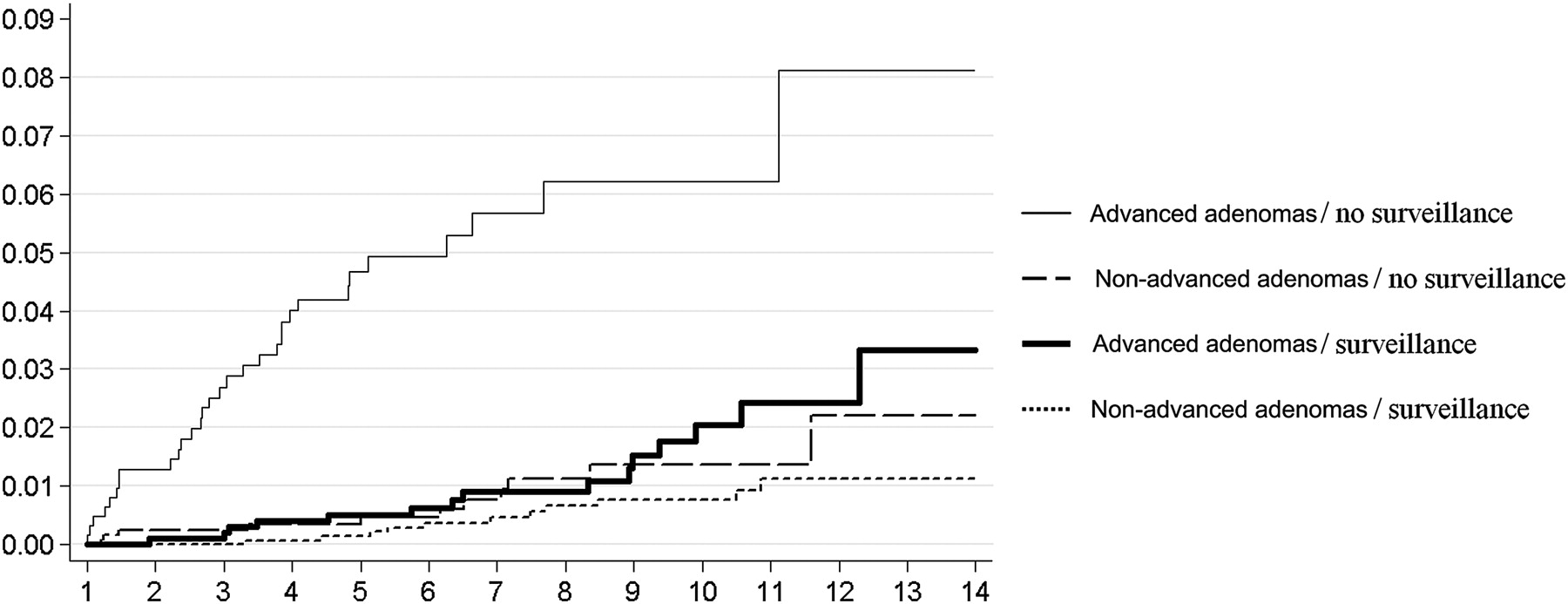
As indicated in Figure 2, the 10-year cumulative probability of colorectal cancer in patients with an initial advanced adenoma was 2.05% (95% CI 1.14% to 3.64%) for patients with at least one follow-up colonoscopy, and 6.22% (95% CI 4.26% to 9.02%) for those without. Corresponding figures in patients with non-advanced adenomas were respectively 0.76% (95% CI 0.39% to 1.48%) and 1.37% (95% CI 0.70% to 2.65%).
{kind=link}
{kind=link}
Cumulative probabilities of colorectal cancer according to whether the first adenoma is advanced or non-advanced and the presence or absence of surveillance.
Discussion
This study showed that, given the usual conditions of polypectomy and colonoscopic follow-up, the long-term risk of colorectal cancer remained higher in patients diagnosed for the first time with adenomas than in the general population. Our study highlighted that both initial adenoma features and the conditions of colonoscopic surveillance in routine practice strongly affected the cancer risk. Compared with the general population, the risk of developing colorectal cancer after polypectomy only remained high in patients with advanced adenomas and without follow-up colonoscopy. However, patients with initial advanced adenomas could largely benefit from colonoscopic surveillance, since the risk of cancer was similar to that in the general population when at least one follow-up colonoscopy was performed. The cancer risk was low in patients with non-advanced adenomas in comparison with the general population.
The advantage of this registry study is that it is based on a large population of unselected patients with a long duration of follow-up, so that it provided unbiased and accurate estimates of colorectal cancer risk, even in subgroups. Registration in the same area of both colorectal cancers and adenomas was performed by the same staff during the study period, which guaranteed standardised data recording. This also allowed us to use reference data from the same population to calculate SIRs. Furthermore, the study population lived in an area of France where the incidence of colorectal cancer and facilities fall within the national average,1 and patients underwent colonoscopies in university or general hospitals as well as in private hospitals. Our results can therefore be broadly extrapolated to overall clinical practice in France.
However, our study has some limitations. First, it is an observational study that did not allow for any causal relationship as a randomised controlled trial to be drawn. The purpose of the present population-based study was to describe the reality of routine clinical practice where patients are not always properly prepared for colonoscopy, complete resection is not always performed and patients do not systematically undergo surveillance colonoscopy. No data were available on the quality of the colonoscopic preparation or on withdrawal time during the endoscopic examination. In contrast to some previous studies which included only subjects with total colonoscopy, in our study the proportion of incomplete colonoscopy at baseline was estimated to be 13.1% among patients with available information on completeness of colonoscopy. In order to consider that all diagnosed polyps had been completely removed, data from the repeated colonoscopy performed within the year following diagnosis were included with the baseline data. The legitimacy of our strategy, though imperfect, is consolidated by the results of the Dutch study showing a SIR as high as 7.9 overall, which dropped to 1.5 after exclusion of the first year.11 In our study the SIR was 1.66 (95% CI 1.38 to 1.97) for the overall period and 1.26 (95% CI 1.01 to 1.56) after exclusion of the first year.
Several studies have examined the risk of colorectal cancer after polypectomy and provided discordant results. Some of them found either no change15 ,18 ,19 or an increased risk of colorectal cancer after polypectomy.12 ,20 In contrast, most prospective studies13 ,16 ,17 ,21 ,22 and one retrospective study14 performed in selected patients enrolled in scheduled surveillance programmes found a significant reduction in the risk of colorectal cancer compared with the general population, with SIRs ranging from 0.24 in the National Polyp study22 to 0.65 in a Danish study.16 These studies were sometimes based on small hospital series or on short follow-up periods. Expected incidences were calculated from external populations which is not the case in population-based studies. In the National Polyp study22 and the Italian study,14 patients with very large adenomas at baseline were excluded. The high risk of recurrence in such patients is well recognised and constitutes one of the key elements behind the current recommendations for post-polypectomy surveillance worldwide.25 ,26 Atkin et al showed that the risk of rectal cancer or colon cancer was confined to patients with advanced adenomas at baseline, whereas patients with non-advanced adenomas had no increased risk.12 However, in this study, as well as in the Telemark Polyp study, the first detection of adenoma was based on rectosigmoidoscopy.12 ,21 Whatever the results yielded by these studies of varying quality, they do not reflect the usual conditions of colonoscopic practice and surveillance in the general population and thus the actual risk incurred by patients with adenoma.
To our knowledge, only two previous population-based studies have provided results on the topic, and both showed an excess of colorectal cancer after adenoma removal.10 ,11 After exclusion of the first year following adenoma removal, the SIR reported was 1.77 (95% CI 1.3 to 2.2) in the Swiss study10 and 1.5 (95% CI 1.4 to 1.6) in the Dutch study.11 Our study extended the above findings in several ways. First, we demonstrated that the characteristics of adenomas diagnosed for the first time in patients from the general population had a major impact on the subsequent risk of cancer. Clearly, the overall risk of colorectal cancer in populations with adenomas is largely dependent on the proportion of patients with advanced adenomas. Such detailed information was not available in the Swiss and Dutch studies and may partially account for the slightly higher risk of colorectal cancer reported.10 ,11
Second, our study suggested that a family history of colorectal cancer may increase the risk of subsequent colorectal cancer in patients with advanced adenomas but not in those with non-advanced adenomas. The SIR was almost twice as high in patients with advanced adenoma with a positive family history compared with those with a negative history. This finding is in line with previous reports from our group suggesting that first-degree relatives of patients with large adenomas or of patients with cancer had an increased risk of developing both large adenomas and cancer.27 ,28
Last, our findings suggest that the benefit of colonoscopic surveillance, demonstrated in randomised trials, could also be observed under the usual conditions of colonoscopic practice, especially in patients with advanced adenomas. Clearly, such patients are intrinsically at a high risk of colorectal cancer, probably because of an unfavourable genetic, lifestyle or environmental background. The reduction in the SIR from 4.26 without any follow-up colonoscopy to 1.10 with follow-up colonoscopy justifies the great benefit of colonoscopic surveillance among these patients. Moreover, the proportion of advanced TNM stage cancers tended to be lower if patients with advanced adenomas at baseline had had a follow-up colonoscopy (7.5% vs 28.3%). For patients with non-advanced adenomas at baseline, their risk of colorectal cancer was similar to or lower than that observed in the general population, with only marginal variations due to follow-up colonoscopy.
Owing to the benefit of colonoscopic surveillance, the low rate of colonoscopy among patients with a previous adenoma is worrying. This is not specific to the area since this low compliance with screening colonoscopy has already been reported in studies performed all over the country.28 ,29 According to current guidelines, surveillance colonoscopy is recommended at 3 years for an advanced adenoma and at 5 years for a non-advanced adenoma. In the present study, when analysis was restricted to patients with advanced adenoma with at least 3 years of follow-up, only 50.6% of patients had had at least one colonoscopy within the 3 years (+6 months) following adenoma removal (data not shown). Among patients with non-advanced adenomas and at least 5 years of follow-up, 47.7% had had a follow-up colonoscopy within the 5 years (+6 months) following adenoma removal. In France, the cost of colonoscopy to the patient is not an explanation since the examination is almost totally reimbursed by the French health insurance system covering 98% of the population. Further studies are needed to understand why patients do not follow the recommendations of their gastroenterologist after removal of the first adenoma, and thus to develop appropriate strategies to improve the acceptability of colonoscopy. It is possible that these patients did not perceive themselves as being at risk of colorectal cancer. A thorough evaluation of sociological and psychological barriers would be necessary to understand the resistance of these patients to colonoscopic follow-up and to increase their awareness of the incurred risks and benefits of surveillance.
In conclusion, this study shows that, given the usual conditions of colonoscopic practice and surveillance in the general population, the risk of colorectal cancer after removal of an adenoma remains higher than expected. The risk pattern in patients with advanced and non-advanced adenomas reinforces the importance of careful and long-term surveillance, particularly among high-risk patients. Improving the compliance of patients with adenoma to guidelines on colonoscopic surveillance is a major challenge for general practitioners and gastroenterologists.
Acknowledgments
The authors are grateful to the pathologists and the gastroenterologists of Côte-d'Or. They also thank I Dasseux, P Demasson, J Durier, E Lanier, M L Poillot and G Viénot for their technical assistance.
References
Footnotes
Funding This work was supported in part by the French Ministry of Health (PHRC), the National Institute of Medical Research (INSERM), the Regional Council of Burgundy and the ‘Fondation de France’.
Competing interests None.
Ethics approval Ethics approval was provided by Burgundy Medical Ethics Committee and the National Commission for Data Processing and Liberties (CNIL).
Provenance and peer review Not commissioned; externally peer reviewed.