Article Text

Abstract
Objective Patients with non-erosive reflux disease (NERD) have impaired oesophageal mucosal integrity (dilated intercellular spaces). Oesophageal mucosal integrity reflects the balance between repeated reflux damage and mucosal recovery. The relationship between mucosal integrity and acid sensitivity is unclear. Oesophageal impedance may be used for in vivo mucosal integrity measurement. We studied acid-induced changes in oesophageal mucosal integrity and acid perception in patients with heartburn.
Design 50 patients with heartburn whithout oesophagitis underwent impedance monitoring before, during and after 10 min oesophageal perfusion with neutral (pH6.5) and acid solutions (pH1). Symptoms and impedance were recorded during perfusion. Impedance recovery was assessed for 2 h post-perfusion in ambulatory conditions followed by 24-h impedance-pH study.
Results Reflux monitoring discriminated 20 NERD and 30 functional heartburn (FH) patients. Neutral perfusion caused impedance fall that recovered within 10 min. Acid perfusion caused impedance fall with slow recovery: 6.5 Ω/min (IQR 3.3-12.0 Ω/min). Patients with slow recovery (<25th percentile) had lower baseline impedance (1273 Ω ±208 Ω vs. 3220 Ω ±275 Ω ±, p < 0.01) and more frequent acid sensitivity (10/12 vs. 4/12, p = 0.04) than those with fast (>75th percentile) recovery. Patients with NERD had lower baseline impedance (1669 ± 182 Ω vs. 2384 ± 211 Ω, p = 0.02) and slower impedance recovery (6.0 ± 0.9 Ω/min vs. 10.7 ± 1.6 Ω/min, p = 0.03) than patients with FH.
Conclusion Impaired mucosal integrity might be the consequence of repeated reflux episodes with slow recovery. Mucosal integrity, recovery capacity and symptom perception are linked. Low basal impedance and slow recovery after acid challenge are associated with increased acid sensitivity.
- Gastro-oesophageal reflux disease
- oesophageal mucosa
- oesophageal impedance
- oesophageal reflux
- oesophageal physiology
- endoscopic ultrasonography
- acid-related diseases
- adenocarcinoma
- anti-reflux therapy
- Barrett's oesophagus
- gastrointestinal motility
- dysphagia
- erosive oesophagitis
- mucosal barrier
- neurogastroenterology
Statistics from Altmetric.com
- Gastro-oesophageal reflux disease
- oesophageal mucosa
- oesophageal impedance
- oesophageal reflux
- oesophageal physiology
- endoscopic ultrasonography
- acid-related diseases
- adenocarcinoma
- anti-reflux therapy
- Barrett's oesophagus
- gastrointestinal motility
- dysphagia
- erosive oesophagitis
- mucosal barrier
- neurogastroenterology
Significance of this study
What is already known about this subject?
-
The oesophagus, in non-erosive reflux disease, has microscopic abnormalities not seen on endoscopy (dilated intercellular spaces).
-
Patients with functional heartburn have no microscopic abnormalities.
-
Baseline oesophageal impedance appears to represent oesophageal mucosal integrity, and is lower in patients with NERD than in healthy controls.
-
Oesophageal acid perfusion causes a long-lasting fall in impedance.
What are the new findings?
-
In patients with heartburn, the fall in impedance after a standard acid challenge and its recovery shows significant inter-individual variability.
-
The mucosal phenotype susceptible to acid perception is that of low baseline impedance, and slow recovery of impedance after acid challenge.
-
Patients with NERD have a lower baseline impedance and slower post-acid impedance recovery than patients with FH.
-
The study suggests that increased acid perception is associated with a ‘vulnerable’ mucosal integrity maintained by repetitive acid exposures with slow mucosal recovery.
How might it impact on clinical practice in the foreseeable future?
-
An understanding of the pathophysiological characteristics of the oesophageal mucosa in NERD can identify novel therapeutic targets for refractory disease.
Introduction
Almost 70% of patients with gastro-oesophageal reflux symptoms have no macroscopic evidence of oesophageal mucosal damage, and are termed as having either non-erosive reflux disease (NERD) or functional heartburn (FH).1 ,2 In NERD, typical reflux symptoms (heartburn, regurgitation) are caused by the reflux of gastric contents (including acid, weak acid and bile acids)3–6 into the oesophagus. In FH, these symptoms do not appear to be related temporally to reflux events, a lack of association that can be established with 24 h reflux monitoring.7
In erosive eoesophagitis, enhanced perception of acid reflux is thought to be due to breach of the mucosal barrier and permeation of luminal contents, followed by nociceptor activation. In NERD, where there is much less inflammation and no mucosal erosions, the pathophysiology is less well understood. Although patients with NERD do not have endoscopic-visible erosions, their mucosa is not completely normal. Compared with healthy subjects, the oesophageal mucosal epithelium in NERD shows (under light and electron microscopy) dilated intercellular spaces (DIS).8 DIS is not found in patients with FH.9 Such disruption in mucosal integrity, for example, dilated intercellular spaces, is not only apparent morphologically, but can also be expressed in functional terms. From in vitro animal and human experiments, we know that exposure of oesophageal mucosa to solutions representative of gastric refluxates is able to induce a reduction of transepithelial electrical resistance (TER) and increased permeability to small molecules.10 ,11 Theoretically, such changes in mucosal barrier function may allow alterations in pH and permeation of noxious or sensitising substances into the epithelial intercellular spaces, and may facilitate submucosal nociceptor activation.12
Until recently, oesophageal mucosal integrity has been studied in animal tissue or human biopsies that allowed measurement of intercellular spaces, or changes in permeability. However, these techniques did not allow characterisation of dynamic changes of oesophageal mucosa integrity over time.
Multichannel oesophageal intraluminal impedance is a technique that has been developed to complement measurements of pH in reflux studies.13 It has recently been highlighted as a potential surrogate tool for in vivo assessment of oesophageal mucosal integrity.14 The impedance measures changes in conductivity to an alternating electric current between a pair of electrodes mounted on a catheter. The current is passed between these electrodes through the adjacent material that connects them: during a reflux event, this may be liquid refluxate, but in the case of the empty oesophagus it is the mucosa that lies in close contact and offers the resistance (in Ohms) to direct current. A study that included animal and human data showed that there was a positive correlation between in vivo baseline impedance and in vitro TER measurements.14 It is known that the baseline impedance of the distal oesophageal mucosa is lower in patients with NERD than in healthy subjects,15 and decreases further in patients with erosive oesophagitis, or Barrett's oesophagus.16
When oesophageal biopsies are exposed to acid in Ussing Chambers, there is a fall in TER, followed by a slow recovery to baseline.11 Similarly, when the oesophagus was infused with acid in healthy subjects, a drop in impedance was observed, followed by a slow recovery to baseline.14 Thus far, such dynamic properties of mucosal integrity in patients with reflux symptoms have not been studied. Oesophageal mucosal integrity, as expressed by baseline impedance, is probably a dynamic process reflecting (1) the damaging effect of repeated acid reflux events and (2) the mucosal capacity to recover integrity.
We hypothesise that there is a relationship between slow recovery of mucosal integrity after acid exposure, mucosal vulnerability (low baseline impedance) and increased perception of reflux episodes.
We aimed to study dynamic properties of oesophageal mucosal integrity and symptom perception in patients with NERD and FH.
Materials and methods
Subjects
Fifty (median age 45, range 20–81; 27 females) consecutive patients attended the Upper Gastrointestinal Physiology Unit of the Royal London Hospital for investigation of typical reflux symptoms. In all cases, the reflux symptoms had not responded sufficiently to PPI therapy, and this was the reason for referral. All patients had been off PPI therapy for a minimum of 7 days. All had an upper gastrointestinal endoscopy demonstrating the absence of erosive oesophagitis, or Barrett's oesophagus, (during the last 3 months). All patients had high-resolution oesophageal manometry prior to reflux studies, and patients with major abnormalities (ie, achalasia, oesophago gastric junction (OGJ) outflow obstruction, nutcracker/jackhammer oesophagus, diffuse oesophageal spasm, absent peristalsis) were excluded.
Oesophageal reflux monitoring and acid sensitivity test were performed in patients as part of their clinical assessment. All subjects gave written informed consent.
Experimental protocol
All subjects underwent an oesophageal acid perfusion challenge followed by a 24-h reflux monitoring with pH-impedance recordings.
An intraluminal pH-impedance catheter (Sandhill Scientific, Highlands Ranch, Colorado, USA) incorporating a single perfusion lumen was positioned transnasally into the oesophagus such that the oesophageal pH sensor was located 5 cm above the manometrically defined lower oesophageal sphincter (LES), with the perfusion point 10 cm above the LES. Mucosal impedance was continuously measured in the most distal impedance segment located 3 cm above the LES (ie, 7 cm below the perfusion point). Data was recorded on a portable digital data logger (Sandhill Scientific).
The study protocol is outlined in figure 1. After placement of the catheter, the subject remained in a seated position. Distal oesophageal impedance was recorded in basal conditions for 15 min. Impedance recording continued throughout the remainder of the study. Next, an oesophageal perfusion of a neutral solution (NaCl 0.9% buffered at pH 6.5) was performed at 10 ml/min for 10 min. This was followed by a 10-min rest period with no perfusion. Then, intra-oesophageal perfusion of acidic solution (HCl at pH 1.0) was performed over 10 min at 10 ml/min. Subjects were not aware of which perfusion was being carried out. Subjects recorded their symptoms during the perfusions using a Likert scale (0–10: 0=no pain; 10=worst imaginable pain).

Study scheme.
After the perfusion period, subjects were free to ambulate, but were asked not to eat or drink anything, and to remain upright during the next 120 min. Patients subsequently completed their clinical 24-h pH-impedance reflux study. During this reflux study, patients were asked to press buttons on the recorder to indicate mealtimes, body positions and symptom episodes.
Data analysis
Baseline impedance was measured as a mean impedance value between minutes 5 and 15 of the baseline period (the first 5 min were excluded to allow for frequent artefact, as the subjects acclimatised themselves to the catheter). We calculated the mean impedance value over the perfusion periods. Reflux events, but not swallows, were excluded from this calculation (swallow-induced quick impedance changes provoked little effect on mean baseline-impedance measurements).
Thereafter, impedance was measured every 10 min for 120 min. At the same time-points, mean oesophageal pH was also recorded.
The impedance recovery after perfusion was calculated as follows. We measured the rate (Ω/min) of impedance increase between minutes 5 and 90 after cessation of the acid perfusion. Minutes 0–5 were not considered in order to allow for complete acid bolus clearance from the distal oesophagus. We chose to measure the rate of impedance recovery between 5 and 90 min because preliminary experiments revealed this to be the most linear part of the recovery process. We also calculated the rate of impedance recovery as a percentage of baseline impedance increase per minute. The subsequent reflux monitoring study was analysed as follows. The first 3 h of the recording (corresponding to the perfusion and recovery phase of the study protocol) were excluded from analysis. Pathological oesophageal acid exposure was considered as over 4.2%. Reflux-symptom correlation was calculated using the symptom index17 and symptom-associated probability.18
Patients were defined as having NERD if the 24-h oesophageal acid exposure was >4.2%, and/or there was a positive correlation between reflux (acid or weakly acidic reflux) and symptom episodes (both symptom index >50% and symptom-associated probability >95% had to be positive). A diagnosis of FH was made if there was no pathological reflux and no reflux-symptom correlation.19
The analysis of impedance changes during and after perfusions was performed by one of the investigators (PW) blinded to the results of the 24-h reflux monitoring and patient classification.
Statistics
All data are expressed as mean±SEM unless otherwise stated. Single comparisons were made with an unpaired Student's t test (parametric data) or Mann–Whitney U test (nonparametric data) wherever appropriate. Multiple comparisons were made with ANOVA followed by Bonferroni's or Dunn's multiple comparison test. Correlations were tested using the Spearman and Pearson tests wherever appropriate. Fisher's exact test was used to test proportional differences. Significance was declared at p<0.05.
Results
Twenty-four-hour clinical reflux monitoring
Mean oesophageal acid exposure time for all patients was 4.02% (range 0–20%). Twenty patients were classified as NERD (15 with increased acid exposure, 5 with only positive reflux-symptom association). Thirty patients had physiological oesophageal acid exposure and negative reflux-symptom association, and were diagnosed with FH.
Acid sensitivity
No subjects reported discomfort during the neutral perfusion.
31 of 50 patients (62%) perceived heartburn, with a median pain score of 8 in those perceiving pain. All patients completed 10 min acid perfusion.
Baseline oesophageal mucosal impedance
In all patients, baseline impedance at 3 cm above the LES was 2098 Ω (IQR 1155–2770 Ω). There was a weak but significant correlation between baseline impedance and 24-h oesophageal acid exposure time (r=−0.36, p<0.01), and no correlation between baseline impedance and acid clearance time.
Low baseline impedance (<1155 Ω ie, lower than 25th percentile) was more often associated with a positive acid sensitivity test than high baseline impedance (>2770 Ω) (Fisher test p<0.01). In other words, baseline impedance was lower in those subjects with a positive acid sensitivity test than in those with a negative sensitivity test (1736±139 vs 2741±296, p<0.01, figure 2). This was true even when only patients with FH were considered (1927±210 vs 3018±354, p=0.01).
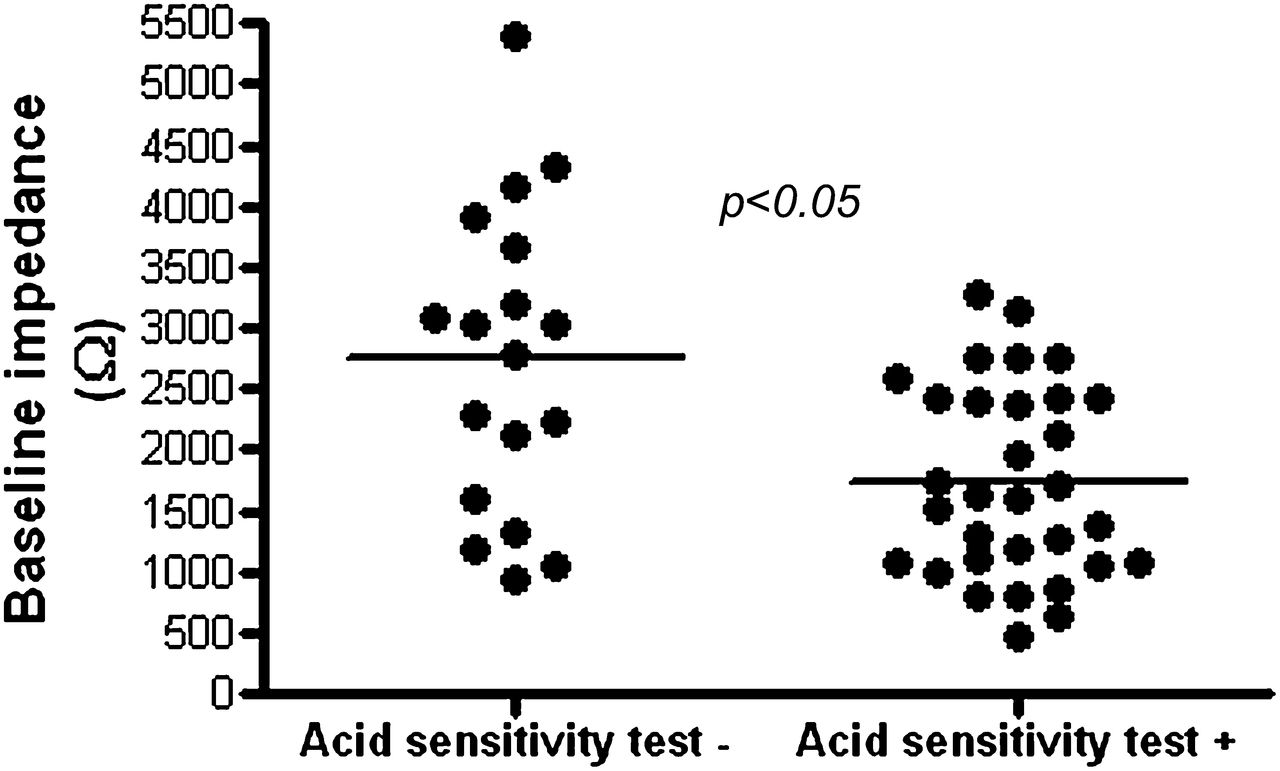
Baseline oesophageal mucosal impedance in patients according to acid sensitivity result. A positive test implies heartburn was perceived. A negative test implies no heartburn perception.
Perfusion with neutral solution
Perfusion with neutral solution provoked a fall in impedance to 675±53 Ω in all patients. No heartburn was perceived in all subjects during neutral perfusion. After perfusion, there was a very fast recovery of impedance to baseline (within 10 min impedance was 98±4% of baseline, mean increase rate 203.7±11.8 Ω/min).
Perfusion with acidic solution
Perfusion with acidic solution provoked a fall in impedance to 349±20 Ω in all patients.
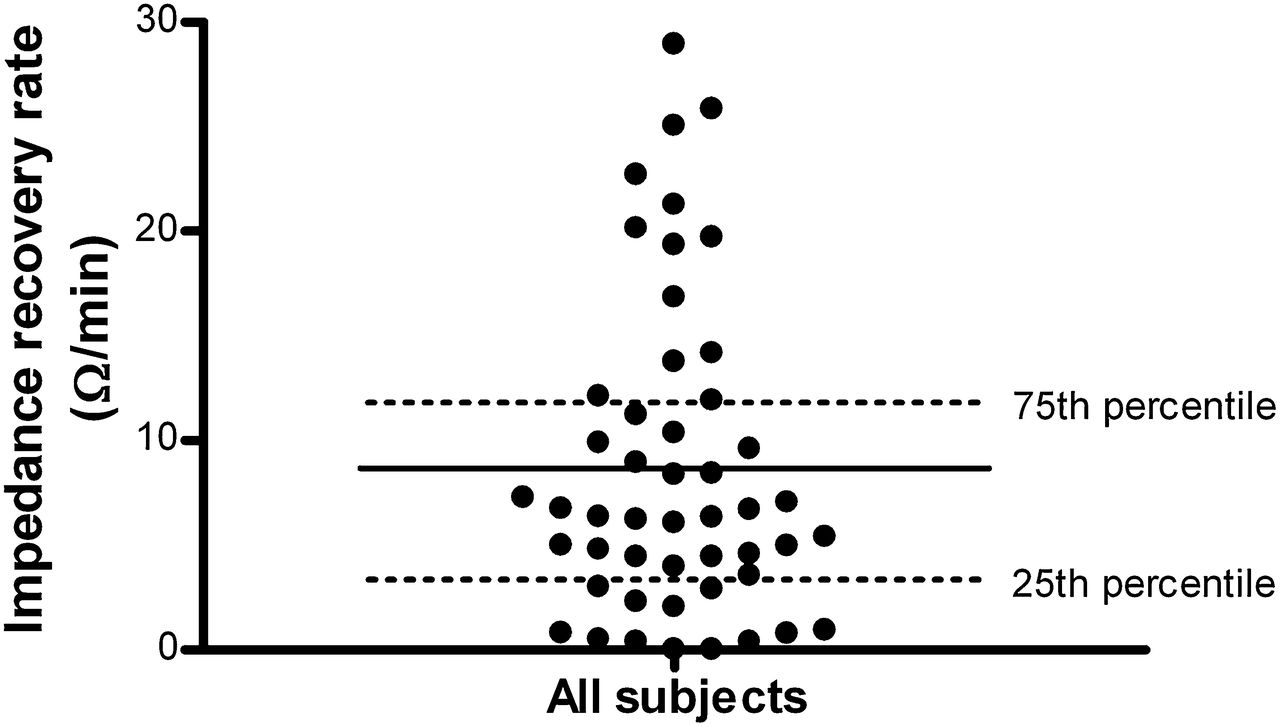
After acid perfusion, there was a much slower recovery of impedance compared with the recovery post-neutral perfusion. The median impedance recovery rate was 6.5 Ω/min (25th–75th percentile=3.3–12.0, figure 3). The mean percentage of baseline increase rate was 0.4%/min. Impedance recovery expressed as absolute values (Ω/min), or as per cent baseline increase (% baseline/min), showed a significant positive correlation (r=0.73, p<0.01). At 90 min after perfusion, the median impedance was 73% (IQR 67%–92%) of baseline. Baseline impedance correlated well with post-perfusion impedance recovery rate (r=0.7, p<0.01, figure 4). There was no correlation between impedance recovery rate and acid clearance time on 24-h reflux monitoring.

Inter-individual variability of impedance recovery post-acid perfusion in patients with reflux symptoms.

Correlation between post-acid perfusion impedance recovery rate and baseline impedance.
Patients with slower impedance recovery (<3.3 Ω/min, ie,<25th percentile, n=12) had lower basal impedance (1273 Ω±208 vs 3220 Ω±275, p<0.01), more often acid sensitivity (10/12 vs 4/12, p=0.03), and higher 24-h acid exposure (4.3%±1.2 vs 1.7%±0.4, p=0.04) than those with quicker impedance recovery (>12.0 Ω/min, ie, >75th percentile, n=12).
Comparison of NERD versus FH
In the 24-h reflux monitoring, patients with NERD had significantly higher acid exposure, greater percentage of acid reflux events and longer acid clearance time than patients with FH (table 1).
Comparison of 24-h pH-impedance data in patients with FH and patients with NERD
In patients with NERD, baseline impedance was significantly lower than those with FH (1669±182 Ω vs 2384±211 Ω, p=0.02, figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Baseline oesophageal mucosal impedance in patients according to phenotype (NERD vs FH).
Patients with NERD had a slower rate of impedance recovery compared with patients with FH (6.0±0.9 Ω vs 10.7±1.6 Ω, p=0.03). The reason for the different rates of impedance recovery between patients with NERD and patients with FH was not due to differences in acid exposure or number of swallows needed to clear the acid during the recovery period. The 120-min acid exposure (pH<4) in FH and NERD groups was 9.4%±1.7% and 13.4%±2.7%, respectively (not significant). The number of swallows needed to clear acid after perfusion was 5.0±0.5 and 5.5±0.7, respectively (not significant).
Patients with NERD showed a trend towards increased acid sensitivity compared with patients with FH (16 of 21 vs 16 of 29), but this was not statistically significant (p=0.1).
Discussion
We tested the hypothesis that there is a relationship between slow recovery of oesophageal mucosal integrity after acid exposure, mucosal vulnerability (low baseline impedance) and increased perception of reflux episodes.
We assessed the dynamic impedance changes that occur before, during and after an intraluminal acid challenge in patients with reflux symptoms.
Our study results show (1) a distal oesophageal acid challenge in patients with reflux symptoms causes an abrupt fall in impedance that recovers slowly, displaying a significant inter-individual variability; (2) there is a relationship between rate of impedance recovery and baseline impedance, that is, the slower the recovery, the lower the baseline impedance; (3) patients with low baseline impedance were more sensitive to acid exposure; (4) a group of subjects who display slow recovery of impedance after acid perfusion, low baseline impedance, high 24-h acid exposure and high acid sensitivity can be identified; (5) compared with FH, patients with NERD have slower recovery of mucosal integrity after acid perfusion, lower baseline impedance, but not a significant difference in acid sensitivity.
In contrast with the rest of the gastrointestinal tract, the oesophageal mucosa is characterised by tightly apposed non-keratinised stratified squamous epithelium. Under physiological conditions, the oesophageal epithelium forms an effective barrier against the passage of noxious substances, such as acid, from the oesophageal lumen into the submucosa.20 In vivo and in vitro experimental mucosal exposure to acid impairs the barrier properties, as assessed by morphological and permeability studies.8 ,10 ,12 ,21 This failure of normal barrier function may allow the passage of acid or other noxious components of the refluxates (eg, pepsin or bile acid) such that they can stimulate submucosal nociceptors and provoke symptoms in the absence of macroscopic erosions.22 In vitro studies do not allow characterisation of dynamic changes of oesophageal mucosa integrity over time.
Assessment of baseline oesophageal impedance is currently suggested as a surrogate technique to study the integrity of the oesophageal mucosa. Baseline impedance in relation to 24-h acid exposure has been investigated,15 but the dynamic response of the oesophageal mucosal integrity to acid exposure has not been characterised in patients with reflux symptoms. It is likely that the baseline integrity of the mucosa is a function of its restoration capacity after repeated acid exposure. In vivo oesophageal impedance enabled us to evaluate dynamic properties of oesophageal mucosal integrity in patients during and after a standardised acid challenge.
The fall in impedance that occurs during acid perfusion is predominantly due to the conductance of the acid solution itself lying in contact with the impedance segment. However, this study confirms that low impedance persists for a long time after the clearance of this acid. This impairment of integrity seen is in accordance with in vitro findings when human oesophageal mucosal biopsies are exposed to acid.11 The long-lasting fall of the impedance implies that the barrier property of the mucosa is impaired for some time after an acid exposure. We see that the recovery of the impedance displays a significant inter-individual variability. This observation is of interest since it appears that patients with acid-induced mucosal damage do not reconstitute their mucosal integrity at the same rate. As such, one can hypothesise that patients with a slower recovery of integrity will be more likely to have long-lasting vulnerability of their mucosa. Indeed, we found a close association between slow recovery of integrity after acid challenge, and a low baseline impedance value. It is therefore possible that low baseline impedance is partly a consequence of the impaired ability of the mucosa to rapidly reconstitute its barrier function. Supporting this theory is our finding that patients with low baseline impedance (more impaired integrity) have more sensitivity to acid perfusion than those with high baseline impedance. This is true even when only patients with FH are included in the calculation.
In our study, we did not use the spontaneous reflux-symptom association (during 24-h reflux monitoring) to assess acid sensitivity. Instead, we used perception of a standard acid challenge. Although the first method seems to be more physiological, most studies on oesophageal chemosensitivity rely on standard acid perfusion techniques due to large inter-individual and day-to-day variability in symptom perception during ambulatory reflux monitoring.
Patients with a slow impedance recovery had a lower baseline impedance and more acid sensitivity than patients with a quick impedance recovery. The slower recovery group also had higher 24-h acid exposure than the quicker recovery group. This is important, as one can consider the following paradigm: if a patient has a reflux episode, the oesophageal mucosal integrity is impaired. This mucosal integrity recovers slowly. During this time of low integrity, the patient is more vulnerable to symptoms from reflux episodes. As more reflux events (and more oesophageal acid exposure) occur, the integrity is further impaired, and further delays the adequate reconstitution of barrier function, rendering the patient yet more vulnerable to reflux perception. A clinical correlate of this has previously been documented, whereby it was noted that a reflux event is more likely to be perceived if there was a previous burden of acid exposure.23 ,24
When we compare patients with FH and those with NERD, we see that patients with NERD have a lower baseline impedance. This would be in keeping with previous observations of morphological changes (DIS) in the distal oesophagus of patients with NERD, but not in patients with FH.9 According to our paradigm, the low baseline impedance in NERD compared with FH would be more likely to occur if the recovery of impedance is slower in patients with NERD, and indeed, this is the case. We did not see increased acid sensitivity in patients with NERD compared with patients with FH. This may be a limitation of the power of the study, since there was a non-significant trend towards increased perception in the NERD group.
The mechanism of symptom perception in FH is unclear. We already know that patients with FH (who by definition do not have reflux-induced symptoms) display a high ‘positive’ rate when the acid sensitivity test is used as a diagnostic tool.25 Within our FH group, patients who perceived acid perfusion had lower baseline impedance than those who did not, suggesting that peripheral factors may still play a role in their acid perception. Indeed, one can identify a subgroup of patients with FH who, despite having a normal reflux study, have a mucosal integrity behaviour phenotype that is very similar to patients with NERD.
The mechanisms underlying acid-induced impairment of mucosal integrity and heartburn are not completely understood. Acid (and, perhaps, other constituents of the refluxate) is able to cause change in paracellular permeability of the epithelium via disruption of normal tight-junction morphology. Acute acid injury is able to cause cleavage of the junction protein, e-cadherin,26 and there are notable changes in claudins that occur in gastro-oesophageal reflux disease (GORD).26–28 Such disruption could conceivably be via an inflammatory mechanism. Within the oesophageal epithelium are acid-sensitive receptors, such as transient receptor potential channel and vanilloid subfamily member 1 (TRPV1).29 These respond to HCl and capsaicin by producing a platelet-activating factor, an important inflammatory mediator involved in the chemo-attraction and activation of immune cells, particularly eosinophils. Further evidence for a putative inflammatory mechanism in NERD was demonstrated by Kandulski et al,30 who showed increased IL-8 expression in patients with GORD compared with controls. This inflammatory secretion appeared to be associated with an increased expression of PAR-2, potentially suggesting that changes in gene expression could lead to increased susceptibility to local inflammation. Differences in inflammatory mediators between patients with NERD and patients with FH are currently under investigation.
We measure acid sensitivity to a 10-min acid perfusion in all our patients who do not respond adequately to PPI therapy. We do not yet suggest building acid perfusion into clinical testing in all reflux-monitoring studies. The clinical relevance of impedance-recovery measurements is not yet established, and will require outcome studies to determine its role. We believe the current study is more valuable as a physiological investigation into mucosal integrity and behaviour in gastro-oesophageal reflux disease, and we believe it provides a novel insight into mucosal pathophysiology.
An accurate power calculation for this study was difficult since we were measuring new variables on which there was no previous data. We did, however, use an assumption based on retrospective analysis of impedance recovery after non-experimental clinical acid sensitivity testing in previous patients. Here, we assumed that the NERD group would have mucosa that recovered 25% slower than in the FH group. This gave a suggested sample size of 36. In reality, the difference in mean recovery between FH and NERD was greater than 25%, and as such, we are confident that a sample of 50 is sufficiently powered to show a difference.
A limitation of our study is that impedance recovery was only measured for 2 h post-acid perfusion. Ideally, this period should be longer since most subjects had not re-attained baseline levels over 2 h. Food and drink were not permitted during this recovery period as this creates a significant impedance artefact. As such, the 2-h timeframe was considered a satisfactory compromise, since a recovery rate can be reasonably calculated in this time period without the need for patients to undergo an even longer period of uncomfortable fasting.
It is possible that our classification of patients with NERD was not completely accurate. The reason for this is that patients had their endoscopy as part of their clinical evaluation for refractory reflux symptoms. Some patients may previously have erosive oesophagitis that was ‘converted’ to NERD by PPI therapy. However, all our patients had ongoing symptoms despite normal endoscopic mucosa, and we are interested in the physiological properties of this non-eroded mucosa in generation of persistent symptoms.
The use of widened intercellular spaces on electron microscopy could have been considered in order to improve our phenotyping, however, the only study describing this showed overlap between individuals with NERD and individuals with FH.9
We performed perfusions before knowing the patient phenotype (FH or NERD). We believe that for the objective of the study it was not necessary to know the phenotype prior to the test. Indeed, it ensured blinding of the investigator during the acid sensitivity test.
A further limitation of the study is that corresponding in vitro assessment of mucosal integrity by analysing oesophageal biopsies in Ussing Chambers was not carried out. An experiment, whereby serial endoscopic biopsy over a 90-min period to confirm our findings would be desirable, but would be unfeasible and distressing for the participant. However, we know from previous animal studies that in vitro measures of mucosal permeability do correlate well with in vivo impedance measurements.14 As such, we were confident in the use of MII in this role.
In summary, this study indicates that impaired mucosal integrity can be induced by acid, and maintenance of this impaired status can be promoted by slow reconstitution after acid exposure. This situation appears to favour symptomatic acid perception. These findings give us a greater insight into the pathophysiological attributes of the oesophageal mucosa that contribute to NERD.
References
Footnotes
-
Funding Grant support: DS receives a grant from the Medical Research Council for Translational Research in Neurogastroenterology; grant number: MGAB1A7R. DS receives a research grant from Sandhill Scientific, USA.
-
Competing interests Philip Woodland, Mohannad Al-Zinaty and Etsuro Yazaki have no conflicts of interest to declare. Daniel Sifrim receives a research grant from Sandhill Scientific, USA.
-
Provenance and peer review Not commissioned; externally peer reviewed.