Article Text

Abstract
Objective Intestinal permeability and psychological stress have been implicated in the pathophysiology of IBD and IBS. Studies in animals suggest that stress increases permeability via corticotropin-releasing hormone (CRH)-mediated mast cell activation. Our aim was to investigate the effect of stress on intestinal permeability in humans and its underlying mechanisms.
Design Small intestinal permeability was quantified by a 2 h lactulose–mannitol urinary excretion test. In a first study, 23 healthy volunteers were subjected to four different conditions: control; indomethacin; public speech and anticipation of electroshocks. In a second study, five test conditions were investigated in 13 volunteers: control; after pretreatment with disodium cromoglycate (DSCG); administration of CRH; DSCG+CRH and DSCG+public speech.
Results Indomethacin, as a positive comparator (0.071±0.040 vs 0.030±0.022; p<0.0001), and public speech (0.059±0.040; p<0.01), but not the shock protocol increased intestinal permeability. Similarly, salivary cortisol was only increased after public speech. Subgroup analysis demonstrated that the effect of public speech on permeability was only present in subjects with a significant elevation of cortisol. CRH increased the lactulose–mannitol ratio (0.042±0.021 vs 0.028±0.009; p=0.02), which was inhibited by the mast cell stabiliser DSCG. Finally, intestinal permeability was unaltered by public speech with DSCG pretreatment.
Conclusions Acute psychological stress increases small intestinal permeability in humans. Peripheral CRH reproduces the effect of stress and DSCG blocks the effect of both stress and CRH, suggesting the involvement of mast cells. These findings provide new insight into the complex interplay between the central nervous system and GI function in man.
- Stress
- Epithelial Barrier
- Mast Cells
- Inflammatory Bowel Disease
- Irritable Bowel Syndrome
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
Psychological stress influences the disease course of IBD and functional GI disorders.
-
In rodents, psychological stress increases small intestinal permeability and leads to an inflammatory response.
-
Mast cells and peripheral corticotropin-releasing hormone (CRH) are critical players in stress-induced elevated intestinal permeability in rodents.
What are the new findings?
-
Public speech leads to increased mucosal-to-serosal, paracellular intestinal permeability in healthy humans who display sufficient activation of the hypothalamic–pituitary–adrenal axis.
-
Peripheral administration of CRH reproduces stress-induced hyperpermeability in man.
-
The enhanced intestinal permeability following public speech and exogenous CRH seems to depend on mast cells since it was blocked by sodium cromoglycate.
How might it impact on clinical practice in the foreseeable future?
-
Stabilisation of mast cells and CRH receptor antagonists are attractive options for the treatment or prevention of stress-related exacerbations of functional and organic GI disorders.
Introduction
The study of the interaction between psychological states and GI function is a complex and developing field. The bidirectional neurohumoral communication system between the brain and the gut (‘brain–gut axis’, BGA), mediating the effects of stress on the GI tract, has been considered a pivotal player in the pathogenesis of ‘functional’ GI disorders like IBS and functional dyspepsia for many years.1
Psychosocial stress and psychiatric comorbidity are common in IBS, can influence the onset of symptoms and predict the clinical outcome.2–4 However, the exact mechanisms through which stress exerts its role in IBS remain unclear. More recently, the importance of psychosocial stressors and the BGA has also been recognised in overt organic GI disease, such as IBD. Emerging evidence (reviewed in Ref. 5) suggests that a bidirectional brain–gut interplay exists in IBD, where psychological stress can result from active disease but can also contribute to triggering or exacerbating intestinal symptoms and inflammation.
Increased intestinal permeability has been demonstrated in both functional and organic GI diseases.6–8 Mucosal inflammation is the key feature of IBD, but low-grade inflammation has also been implicated in symptom generation in IBS.9 Studies in animal models have identified increased intestinal permeability as the potential link between psychological stress and the activation of a mucosal immune response via enhanced penetration of luminal antigens.10–12 In rodents, psychological stressors like water-avoidance stress,11 ,13 ,14 restraint stress13 ,15 and crowding stress10 induced intestinal hyperpermeability in a corticotropin-releasing hormone (CRH) and mast cell-dependent fashion. However, the effect of psychological stressors on human intestinal permeability is unclear and mechanistic data in humans are lacking. The available data are limited to the effect of artificial stressors like hand immersion in cold water which resulted in increased secretion of albumin in the intestinal lumen.16 ,17 However, the relevance of this type of stressors in daily life is debatable. Moreover, it is unclear how albumin secretion relates to lumen-to-blood permeability. Recently, increased intestinal permeability quantified by a lactulose–mannitol excretion test was reported in troops after a 4 -week combat training,18 but due to the nature of the training programme, it is impossible to separate the effects of psychological from physical stress.
The aim of the present study was to investigate the effect of acute psychological stress on small intestinal permeability in healthy humans and to unravel the underlying mechanism. Based on the available evidence in animals, we hypothesised that acute psychosocial stress would increase intestinal permeability in healthy humans and that this effect can be blocked with mast cell stabilisation. We also hypothesised that exogenous CRH would reproduce the effect of stress on small intestinal permeability.
Materials and methods
Subjects
For both studies, healthy undergraduate students were recruited at the biomedical and pharmaceutical school of the University of Leuven. Exclusion criteria were chronic GI disorders or symptoms, diabetes mellitus (type 1 or 2), psychiatric disease, smoking, coeliac disease, food allergy, atopy (eczema, asthma, allergic rhinoconjunctivitis), allergy to non-steroidal anti-inflammatory drugs (NSAID) or intolerance and first-degree relatives with IBD, coeliac disease or type 1 diabetes mellitus. During the last 2 weeks before the study, the volunteers were not taking medication except for oral contraceptive drugs. During the 3 days before a test, participants were instructed to refrain from drinking alcohol and on the day before the test lactose-containing products were to be avoided. The study protocol was in accordance with the Declaration of Helsinki and approved by the ethics committee of the University of Leuven before initiation of the study (approval numbers ML6425 and ML8291). All volunteers provided written informed consent before the first test.
In vivo permeability testing
All tests, with the exception of the speech condition, started at 14:00 to reduce diurnal variation. Because of the nature of the public speech (scheduled exam, cf. infra), this condition started between 12:00 and 16:00. A non-lactose-containing breakfast was allowed until 6 h before the test. After this, only water ad libitum was allowed until the end of the experiment except from 30 min before the start until 30 min after drinking the test solution. The in vivo permeability test was a standard differential urinary sugar excretion test.7 ,19 The test solution consisted of 5 g of lactulose (Eurogenerics, Brussels, Belgium) and 2 g of mannitol (ABC Chemicals, Mississauga, Ontario, Canada) dissolved in 150 mL of water. Both sugars are not metabolised and renally eliminated after absorption. The solution was ingested within 1 min in the lab in the presence of an investigator and within 5 min after voiding the urinary bladder. In the first study (cf. test conditions), urine was collected at 0–2 h, 2–4 h and 4–6 h in containers with 750 mg of neomycin to avoid bacterial infection. In the second study, urine was collected for 2 h only because of logistic reasons and new data indicating that the 0–2 h collection most accurately reflects the small intestinal phase.20 ,21 The lactulose–mannitol ratio (LMR) in the urine collection of the first 2 h is a measure for small intestinal permeability.19–21
Test conditions
In the first study, the volunteers all underwent four conditions: (1) control, (2) indomethacin, (3) public speech and (4) shock. The order of the test conditions was random. Volunteers were asked to schedule the tests, except for the speech condition, in weeks without anticipated unusual stressors and on days without intense physical activity. The minimal interval for the next test was 4 days after a control test, 1 week for the speech and shock condition and 2 weeks for the indomethacin condition. For the indomethacin condition, volunteers were instructed to take 75 mg of indomethacin at 22:00 on the evening before the test (ie, 16 h before drinking the test solution) and 50 mg at 10:00 on the day of the test (ie, 4 h before the test). The public speech condition was a scheduled oral presentation (bachelor or master thesis) in English in front of an examination jury followed by questions with a total duration between 30 and 45 min. The volunteers drank the test solution just prior to entering the room in which the exam took place. The shock condition was a laboratory-based stress protocol involving anticipation of painful electroshocks at the non-dominant upper arm in a darkened room. One ‘shock’ consisted of 50 2 ms stimuli of 15 mA at a 200 Hz rate. Over the course of 30 min, the possibility of a shock was announced 20 times by an auditory (headphones) and visual (computer screen) countdown at randomised time intervals. Half of these countdown sequences were immediately followed by an electric shock in a randomised fashion. Subjects were told that the intensity of the shock could vary during the test. During the 30 min test, the volunteers were instructed to look at the screen at all times. The test solution was administered immediately before the start of the test.
In the second study, the volunteers were subjected to five conditions: (1) control; (2) after oral treatment with disodium cromoglycate (DSCG) (Nalcrom, kindly provided free of charge by Italchimici SpA, Rome, Italy) 200 mg qid for 2 weeks; (3) after intravenous bolus injection of 100 µg CRH (CRH Ferring, Ferring Pharmaceuticals, Hoofddorp, The Netherlands); (4) after injection of CRH with DSCG pretreatment during 2 weeks and (5) public speech condition similar as in the first study with DSCG pretreatment during 2 weeks. No side effects of CRH or DSCG administration were noted besides mild transient facial flushing in 75% of volunteers during the first 30 min after CRH injection.
Evaluation of stress symptoms and hormones
The intensity of stress symptoms was evaluated by the state version of the validated Spielberger State-Trait Anxiety Inventory (STAI) Questionnaire right before drinking the test solution at each test, 1 h before and immediately after the public speech and immediately after the shock protocol.22 A total STAI score was calculated according to the instructions of the questionnaire. Background stress levels during the last 6 months were evaluated by the Perceived Stress Questionnaire (PSQ).23 Salivary samples were collected (Salivette, Sarstedt, Nümbrecht, Germany) for determination of cortisol by ELISA (DRG Diagnostics, Marburg, Germany) according to the manufacturer's instructions.
Sample preparation and determination of lactulose and mannitol concentration
After collection, the total urine volume was noted and 1.5 mL sample aliquots were filtered with 450 nm filters (Merck Millipore, Billerica, Massachusetts, USA) and stored at −20°C until further analysis. All the samples were coded without reference to the test condition. The measurements were performed and the chromatograms were analysed by a lab technician (EH) who was blinded to the test condition. For analysis, the internal standard cellobiose was added to the sample. Twenty microlitres of the samples was analysed by a high performance liquid chromatography (HPLC) set-up (Alliance 2695, Waters, Zellik, Belgium), which was equipped with a Prevail Carbohydrate column (250 mm×4.6 mm, 5 µm particle size; Grace, Deerfield, Massachusetts, USA). The chromatographic separation was carried out isocratically with 75% acetonitrile/25% MilliQ water for 16 min. The effluent was analysed in an evaporative light scattering detector (ELSD) (ELSD 3300, Grace) with a N2 flow of 1.5 L/min at 40°C. Data were processed using Empower V.2.0 (Waters). Because of interfering peaks in the chromatogram, the lactulose or mannitol concentration could not be determined in nine and six samples in the first study and second study, respectively. The limits of detection were 1.2 mg/L and 1 mg/L for mannitol and lactulose, respectively.
Data analysis and statistical analysis
For each test condition, the LMR was calculated as the lactulose concentration divided by the mannitol concentration and the fractional excretion (FE) of both sugars was determined. For the speech and shock condition, the salivary cortisol concentrations immediately after the stressors were used. The STAI scores immediately before the public speech and after the shock were used, since these reflected the highest stress scores for the respective conditions.
For both studies, multilevel models (mixed models) were constructed for the different dependent variables: LMR, FE of lactulose and mannitol, salivary cortisol and STAI score. The main effect of ‘test condition’ (within-subject categorical variable) was tested to compare the different conditions of interest in both studies, with post hoc t tests and Bonferroni correction for multiple testing. To test the post hoc hypothesis that the effect of ‘stress condition’ on LMR is mediated by cortisol, cortisol was added to the model of the first study as a continuous between-subject variable. Level of statistical significance was set at 0.05. Data are presented as mean±SD. All statistical analyses were performed using SAS for Microsoft Windows, V.9.2 (SAS Institute Inc., Cary, North Carolina, USA).
Results
Acute psychological stress increases small intestinal permeability
In the first study, 23 healthy university students (12 men, 21±1.5 years; body mass index (BMI) 21.3±3.1 kg/m2) were included to investigate the effect of acute psychological stress on intestinal permeability. Two separate stress paradigms were applied. The first condition was a ‘naturalistic’ public speech test, which consisted of the presentation of scientific results followed by questions by a jury (‘speech’). The second condition was an experimental paradigm, in which stress was elicited through the anticipation of painful electroshocks at randomised intervals during 30 min (‘shock’).
Both stress protocols were effective at the behavioural level, as demonstrated by significantly elevated state anxiety scores on the STAI (figure 1A). However, only the speech condition resulted in elevated salivary cortisol levels, a marker of activation of the hypothalamic–pituitary–adrenal (HPA) axis (figure 1B). Salivary cortisol levels were already elevated 1 h before and immediately before the exam in comparison with baseline (12.4±4.3 and 12.5±5.63 vs 9.4±5.4 ng/mL; p<0.01 1 h before vs baseline and p<0.001 immediately before vs baseline), indicating anticipation stress. In contrast, salivary cortisol before the shock condition was similar to baseline (9.3±3.2 vs 9.4±5.4 ng/mL; p=0.50).

Behavioural and hormonal effects of the stress protocols. (A) Both the ‘speech’ and the ‘shock’ condition resulted in elevated anxiety scores evaluated by the STAI-state score. (B) Only the public speech condition increased salivary cortisol levels, indicating activation of the HPA axis. ***p<0.0001 compared with the control condition. HPA, hypothalamic–pituitary–adrenal; STAI, State-Trait Anxiety Inventory state subscale. Mean and SD are indicated on the graph.
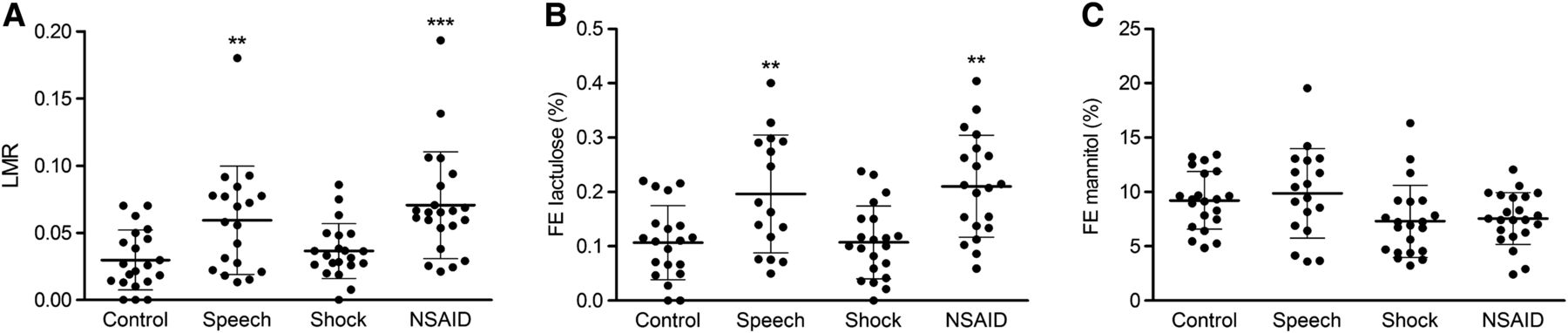
The LMR in the urine collection of the first 2 h after ingestion of the respective sugars was used to quantify small intestinal permeability.19–21 The LMR after two oral doses of indomethacin, which is known to impair intestinal permeability,24 served as a validation of our analysis methodology. As expected, indomethacin significantly increased the LMR compared with the control test situation (0.071±0.040 vs 0.030±0.022; p<0.0001). The FE of mannitol was similar after indomethacin compared with the control test (7.6±2.4 vs 9.2±2.7; p>0.05) in contrast to a twofold higher FE of lactulose (0.20±0.10 vs 0.11±0.07%; p<0.01). The speech (0.059±0.040 vs 0.030±0.022; p<0.01) but not the shock (0.036±0.020; p=0.97) condition resulted in an elevated LMR (figure 2A), indicating a stress-induced rise in small intestinal permeability, as hypothesised. The increased LMR resulted from the increased excretion of lactulose, while the excretion of mannitol was not influenced by the test condition (figure 2B,C). Analysis of the 2–4 h and 4–6 h collections demonstrated an increased LMR after indomethacin in the 4–6 h collection only (see online supplementary table S1).

Small intestinal permeability during psychological stress conditions. (A) The LMR was significantly increased in the public speech condition. Similarly, the fractional excretion (FE) of lactulose (B) was elevated in the speech condition in contrast to the FE of mannitol (C), which was similar across the different test conditions. **p<0.01 compared with the control condition. ***p<0.0001 compared with the control condition. LMR, lactulose–mannitol ratio. Mean and SD are indicated on the graph.
Stress-induced elevation of permeability depends on activation of the ‘stress axis’
The fact that only public speech and not anticipation of electroshocks increased the LMR in combination with elevated salivary cortisol levels led us to hypothesise that coordinated activation of the ‘stress axis’ (HPA axis, autonomic nervous system) plays a key role in the stress-induced permeability changes. In support of this hypothesis, we found in a post hoc analysis that the statistical effect of ‘test condition’ on LMR was mediated by cortisol levels (as a readout for stress axis activation): including both cortisol and the ‘test condition’ (control, speech or shock) in the multilevel model rendered the effect of the ‘stress condition’ non-significant (p=0.22), with a significant cortisol main effect (p=0.02) (figure 3).25 Similarly, the speech condition had no effect on intestinal permeability in those volunteers with a cortisol level below the 90th centile (P90) of the control condition (15.25 ng/mL) during the public speech (LMR 0.042±0.028 vs 0.032±0.022 during the speech and control condition, respectively; p=0.80) (n=12/23). In contrast, there was a significant increase in LMR (0.075±0.047 vs 0.034±0.030; p<0.01) in subjects with a cortisol above the P90 of the control condition during public speech (n=11/23). Similar results were obtained when using mean+2SD of the control condition (18.52 ng/mL) as the cut-off value (LMR 0.051±0.050 vs 0.028±0.022 in volunteers with cortisol below the cut-off; p=0.20 (n=15) and 0.075±0.016 vs 0.031±0.026 in those with cortisol above the cut-off; p<0.01 (n=8)).
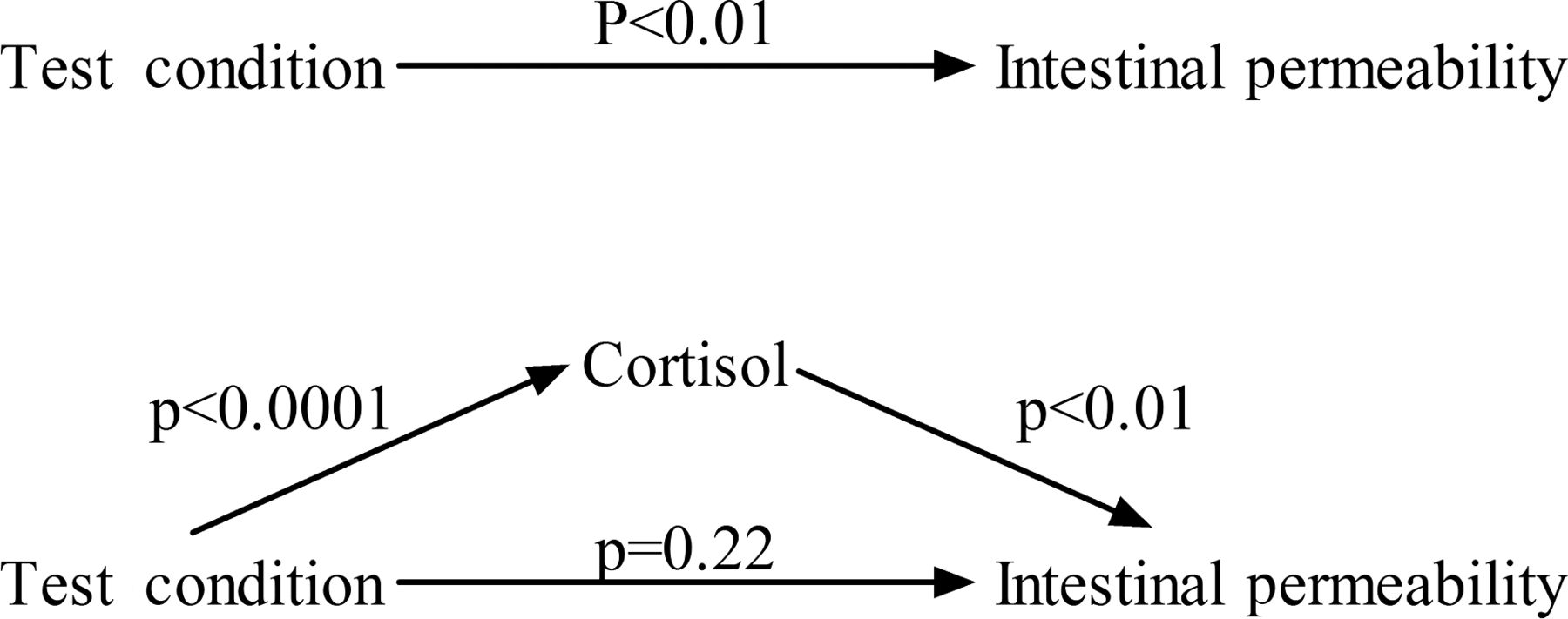
The effect of the test condition on intestinal permeability is mediated by cortisol. (A) The test condition was a significant predictor for intestinal permeability when included as the only independent variable in the model. However, adding the salivary cortisol levels to the model (B) led to loss of significance of the effect of the test condition.
Gender, BMI and background stress levels during the last 6 months, evaluated by the PSQ, were not associated with LMR (all p>0.34), nor did they change the effect of ‘stress condition’ when controlled for in the model.
CRH increases intestinal permeability in a mast cell-dependent way
In a second study, we investigated the effect of CRH and mast cells on intestinal barrier function. Thirteen healthy volunteers (four men, 22±1.4 years; BMI 22.3±2.5 kg/m2) underwent five different test conditions: (1) control; (2) after oral treatment with the mast cell stabiliser DSCG 200 mg qid for 2 weeks (‘DSCG’); (3) after intravenous bolus injection of 100 µg CRH (‘CRH’); (4) after injection of CRH with DSCG pretreatment (‘CRH+DSCG’) and (5) similar public speech condition as in the first study with DSCG pretreatment (‘Speech+DSCG’).
‘CRH’, ‘CRH+DSCG’ and ‘speech+DSCG’ all resulted in elevated salivary cortisol levels (figure 4B), but only in the case of public speech this was accompanied by subjective stress as reflected by higher STAI scores (figure 4A). Exogenous CRH increased the LMR compared with the control condition (0.042±0.021 vs 0.028±0.009; p=0.02) and this increase was abolished by mast cell stabilisation (0.025±0.008; p>0.5) (figure 4C). DSCG had no effects on intestinal permeability by itself (0.029±0.008; p>0.5). Finally, public speech did not alter the intestinal barrier function after DSCG pretreatment (0.027±0.010; p>0.5) (figure 4C), also when considering only those volunteers who had a salivary cortisol above the P90 of the control condition (n=9/13).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of corticotropin-releasing hormone (CRH) administration and mast cell stabilisation on intestinal permeability. (A) Public speech was the only test condition that elevated the STAI score. (B) CRH with and without DSCG and public speech all increased salivary cortisol. (C) CRH administration increased intestinal permeability, which could be blocked by DSCG pretreatment. Public speech had no effect on intestinal permeability after pretreatment with the mast cell stabiliser DSCG. ***p<0.0001; *p<0.05 compared with the control condition. CRH, corticotropin-releasing hormone; DSCG, disodium cromoglycate; STAI, State-Trait Anxiety Inventory; LMR, lactulose–mannitol ratio. Mean and SD are indicated on the graph.
Discussion
In the current study, we have demonstrated that public speech, a naturalistic psychosocial stressor, increases small intestinal permeability in healthy volunteers, and showed this effect to be mediated by activation of the stress axis, reflected by increased cortisol levels. This response was also dependent on the activation of mast cells since pretreatment with the mast cell stabiliser DSCG blocked stress-induced hyperpermeability. Finally, administration of exogenous CRH reproduced stress-dependent permeability changes, again in a mast cell-dependent fashion.
In clinical practice, psychological stress is often suspected to adversely affect the course of organic and functional GI disorders. This observation is supported by longitudinal follow-up studies in IBD patients in clinical remission, showing that stress increases the risk of disease relapse.26–28 In IBS patients, chronic life stress is a powerful predictor of subsequent symptom intensity and outcome,4 although others reported that the magnitude of this correlation is relatively small, indicating that stress is only one of the multiple factors that contributes to symptoms and symptom reporting.29 It is unclear how stress exactly triggers GI symptoms and inflammation, but one plausible mechanism may be its negative effect on intestinal barrier function.5 This hypothesis originates from animal research, demonstrating increased paracellular and transcellular passage of macromolecules in the small intestine and colon of rodents in several models of psychological stress.10–15 Penetration of foreign antigens across the defective intestinal barrier may incite an inflammatory reaction10 ,11 and contribute to GI disease activity. However, translational studies in humans demonstrating increased intestinal permeation of luminal substances in acute stress conditions are lacking.
Previous studies in healthy volunteers have demonstrated increased jejunal albumin secretion and water and salt output during cold pain stress16 ,17 or after dichotomous listening.30 However, it is controversial whether these alterations truly reflect intestinal permeability since albumin in the jejunal perfusate represents a reverse flux from the intravascular to the luminal compartment.16 ,17 In contrast, our study has directly demonstrated an increased transepithelial passage of luminal molecules quantified by the urinary LMR. Separating the LMR into its two components, the mannitol excretion was unaltered, contrary to increased lactulose permeation. These findings are in line with the principle of the method: the smaller mannitol molecule crosses the intestinal epithelium via the paracellular pathway in villus and crypt regions, while the larger lactulose has very limited paracellular permeation in normal conditions restricted to the crypt regions. In case of impaired intestinal barrier function, the passage of lactulose will increase contrary to the unaltered excretion of mannitol, resulting in a higher LMR.7 ,19 It has been suggested that the FE of mannitol may suffice as a measure for small intestinal permeability.20 ,21 However, since psychological stress influences gastric emptying and intestinal transit, the FE of a single sugar may not adequately reflect intestinal permeability.31 Moreover, in the current study we demonstrated that the FE of mannitol was unaltered in the positive control condition, that is, after administration of indomethacin, arguing against the use of a single sugar to assess small intestinal permeability. Recent studies have highlighted the importance of restricting the urine collection to the first 2 h after ingestion of the sugars, since later collections may partially reflect colonic permeability.7 ,21 In the current study, analysis of the 2–4 h and 4–6 h collections demonstrated increased LMR after indomethacin in the 4–6 h collection only, but without differences in the FE of lactulose and mannitol. The doses of the sugars used were based on the available literature.32–37 Some groups have used higher doses (up to 10 g) of lactulose.38–40 However, increasing the dose of lactulose reduces sensitivity of the test because of intraluminal fluid retention.19 ,41
Besides the methodology used to study intestinal barrier function, another strength of the current study is the use of a real-life psychosocial stressor in contrast to more artificial pain stressors. We also compared the effects of the naturalistic stressor to a laboratory-based experimental stress protocol. Only the public speech in the exam situation but not anticipation of electroshocks increased salivary cortisol and impaired the intestinal barrier function. Several factors may account for this difference, for example, the multidimensional nature of the stress induced by the public speech (delivering the speech per se, worrying about the consequences of failing the test, etc.) and the fact that anticipatory stress is already present before the actual exam in the public speech situation as indicated by the increased cortisol levels before the exam.
In the current study, we did not investigate how long the effect of the public speech on intestinal permeability persisted. This relevant question was beyond the scope of our study since it would require postponing the ingestion of the permeability probe to later time points after the stressor in a similar group of volunteers undergoing the same stress situation. Determination of the duration of the barrier defect is relevant to gain more insight into the mechanism of induction of symptoms and inflammation by stress and should be addressed in follow-up studies. Recently, Wilder-Smith and colleagues reported increased LMR in a subgroup of soldiers after 4 weeks of combat training.18 However, interpretation of this study is hampered by several factors. Urine was collected over 5 h in this study, which allows a significant fraction of the sugars to pass through the colon with partial bacterial degradation of lactulose and mannitol.21 The LMR, but not the FEs of lactulose and mannitol, was elevated only in soldiers who developed IBS-like symptoms. However, increased intestinal permeability in IBS has been reported before,7 and it is unclear whether the claimed permeability defect is related just to the development of IBS or due to the stress situation. Finally, combat training represents a combined physical and psychological stressor and it is difficult to distinguish whether the elevated permeability is caused by physical exertion, as has previously been reported,42 by the psychological stress or by the combination.
An important observation in our study was the fact that the public speech condition did not alter intestinal permeability when the volunteers were pretreated with the mast cell stabiliser DSCG. This finding translates animal data to human pathophysiology and encourages the evaluation of mast cell stabilisers in stress-sensitive GI disorders. In a placebo-controlled trial, Klooker et al43 recently reported improvement of abdominal pain and other symptoms in IBS patients by the mast cell stabiliser ketotifen. The number of mast cells and ex vivo mediator release in rectal biopsies were not influenced by the drug, but this may be an inappropriate readout to confirm in vivo stabilisation, as mentioned by the authors. In future studies of mast cell stabilisers in IBS, intestinal permeability and perceived stress levels should be taken into account. Early studies on exercise-induced asthma in children demonstrated that DSCG has a rapid onset of its prophylactic action,44 suggesting that short treatment regimens or even acute administration may be useful in stress-induced symptoms in IBS. Moreover, the evaluation of mast cell stabilisers in the prevention of stress-induced disease relapse in IBD would be of great interest.
CRH is one of the key mediators of the stress response and its direct central nervous system administration in animals mimics the behavioural, autonomic and visceral responses to stress.5 ,31 Animal studies have also implicated peripheral CRH receptors in the GI tract in the stress-induced alterations of intestinal motility and permeability.31 Peripheral injection of CRH impaired colonic barrier function, and this could be blocked by pretreatment with the mast cell stabiliser doxantrozole45 or genetic deletion of mast cells.46 Moreover, application of CRH in vitro to rodent14 or human47 intestinal and colonic biopsies in Ussing chambers reproduced stress-induced permeability alterations, identifying CRH as a pivotal player in the stress-induced alterations of the intestinal barrier. The cellular source of peripheral CRH has been localised to mucosal eosinophils in human colonic biopsies and jejunum of chronically stressed rodents.6 ,48 CRH1 receptors have been identified on human intestinal mucosal mast cells.49 After activation, intestinal mucosal mast cells can subsequently release mediators like proteases and tumor necrosis factor alpha (TNFα), which can alter intestinal permeability.50 In the current study, we extended these observations by demonstrating increased intestinal permeability in a mast cell-dependent fashion after in vivo administration of CRH in humans. CRH1 receptor antagonists are under evaluation for the treatment of IBS.51 ,52 Targeting the peripheral CRH system may also represent a novel complementary treatment option in IBD.
Despite the rigorous methodology and the use of a naturalistic psychological stressor, some limitations have to be mentioned. Inherent to the in vivo study design, we were unable to elucidate the molecular mechanisms at the tight junction level underlying increased permeability. Similarly, we did not determine the presence and activation state of immune cells, in particular mast cells. These analyses necessitate endoscopic mucosal biopsies, the anticipation and the actual procedure of which are likely to induce psychological stress by themselves, potentially distorting the results. Our data do not provide final proof of the involvement of CRH in the in vivo human stress response, as this would involve administration of peripherally acting CRH receptor antagonists. Further, in the second study the public speech situation was only performed with DSCG pretreatment without a public speech control condition. However, due to the nature of the exam (the defence of the bachelor or master thesis) it was not feasible to repeat the public speech with a similar stress induction in the same volunteer twice. In addition, we did not standardise the meals on the days before and the morning of the test. However, since every volunteer underwent all test situations we do not expect the nutritional habits to have exerted a major influence on the permeability results. Finally, we cannot exclude that part of the observed effect of DSCG on stress-induced and CRH-induced permeability changes can be mast cell independent. Indeed, it has been reported that DSCG can stabilise both mast cells and eosinophils through the activation of the G-protein coupled receptor 35, which is present on both mast cells and eosinophils.53–55
In conclusion, we demonstrated that an acute psychological stressor increases small intestinal permeability in a subset of healthy humans with endocrinological signs of stress axis activation. Exogenous peripheral CRH recapitulated the effects of stress on barrier function. Finally, both the stress-induced and CRH-induced hyperpermeability were suppressed by previous mast cell stabilisation. Our data support further evaluation of CRH receptors, mast cells and mucosal barrier function as therapeutic targets in stress-sensitive GI disorders like IBS and IBD.
Acknowledgments
We thank all the students who participated in the studies. We are grateful to Anouk Desmet, Dr Els Melis, Professor John Creemers and Professor Minne Casteels for their help in the recruitment of volunteers.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Contributors Study concept and design: TV, SVW, RF, LVO, GB and JT. Acquisition of data: TV, SVW, EH, SSR, JTό, LH, HV, CV and SV. Data analysis: TV, LVO, RF and KV. Interpretation of data: TV, RF, LVO and JT. Drafting of the manuscript: TV and JT. Critical revision of the manuscript: SVW, HV, RF, LVO, GB, KV and JT. Obtained funding and study supervision: JT.
-
Funding Funding was provided by a Methusalem grant from Leuven University to JT and by the Research Foundation Flanders (Fonds Wetenschappelijk Onderzoek Vlaanderen, FWO) through doctoral (TV and HV) and postdoctoral (LVO and RF) fellowships. GB is funded by a grant of the Flemish government (Odysseus programme, Fonds Wetenschappelijk Onderzoek (FWO), grant G.0905.08). LVO is a research professor of the KU Leuven Research Fund.
-
Competing interests None.
-
Ethics approval Ethics committee of Leuven University Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.