Article Text

Abstract
Objective Little is known about the long-term clinical outcome and durability of HBsAg seroclearance following nucleos(t)ide analogue (NUC) therapy in patients with chronic hepatitis B (CHB).
Design During a median follow-up period of 6 years (33 567 patient-years) of 5409 CHB patients who were initially treated with lamivudine or entecavir, a total of 110 achieved HBsAg seroclearance (0.33% annual seroclearance rate) and were included in this study.
Results Baseline alanine aminotransferase (ALT) level >5 times of upper limit of normal was associated with higher probability of HBsAg seroclearance (HR 1.80, p<0.01), while HBeAg positivity (HR 0.46, p<0.01), high HBV DNA level (log10 IU/mL; HR 0.61, p<0.01), and cirrhosis (HR 0.48, p<0.01) were inversely associated with the probability of HBsAg seroclearance by multivariable analysis. During follow-up for 287 patient-years after HBsAg seroclearance, only two patients with baseline cirrhosis developed hepatocellular carcinoma (HCC) or died (0.7% annual risk), which was of a significantly lower rate compared with propensity score-matched patients without HBsAg seroclearance (HR 0.09, p<0.01). HBsAg reversion and/or HBV DNA reversion occurred in 18 patients, most of which were transient with extremely low serum levels of HBsAg (0.05–1.00 IU/mL) and HBV DNA (17-1818 IU/mL). None required retreatment. The cumulative probability of anti-HBs seroconversion (detection of anti-HBs) at 4 years was 67.4% by Kaplan–Meier analysis. Selection for lamivudine-resistance HBV mutants during treatment was not associated with composite reversion (p=0.66).
Conclusions HBsAg seroclearance achieved after NUC treatment was associated with favourable clinical outcomes and was durable in most cases during long-term follow-up.
- Hepatitis B
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
-
Spontaneous or interferon-induced seroclearance of HBsAg is durable and is associated with improvements in liver histology, a decreased risk of hepatocellular carcinoma (HCC) and prolonged survival.
-
Little is known about the long-term clinical outcome and durability of nucleos(t)ide analogue (NUC)-induced HBsAg seroclearance.
-
Seroclearance of HBsAg during lamivudine therapy may not indicate viral clearance, but may only reflect a point mutation in the S gene that results in failure to detect HBsAg.
What are the new findings?
-
HBsAg seroclearance achieved after NUC treatment was associated with favourable clinical outcomes and was durable in most cases.
-
Selection for lamivudine-resistance HBV mutants during treatment was not associated with serological or virological reversion.
-
Liver failure or HCC could occur after HBsAg seroclearance in some patients with baseline cirrhosis.
How might it impact on clinical practice in the foreseeable future?
-
HBsAg seroclearance can be regarded as an optimal endpoint of treatment with NUC.
-
For patients with baseline cirrhosis, long-term clinical monitoring and surveillance for HCC may be still required after HBsAg seroclearance.
Introduction
Approximately 400 million people worldwide are chronically infected with HBV. These patients have a substantially increased risk of cirrhosis and hepatocellular carcinoma (HCC) which are responsible for approximately one million deaths worldwide each year.1 ,2
Hepatitis B surface antigen (HBsAg) seroclearance rarely occurs in patients with chronic hepatitis B (CHB). The annual incidence of spontaneous HBsAg seroclearance is estimated to be approximately 0.1–0.8% in CHB patients who acquire the infection early in life.3 HBsAg seroclearance is also rarely observed in patients who are treated with interferon or nucleos(t)ide-analogues (NUC).4–10 It has been reported that spontaneous or interferon-induced seroclearance of HBsAg is durable and is associated with improvements in liver histology, a decreased risk of HCC and prolonged survival.8 ,9 ,11 ,12 These data have been extrapolated to patients who are being treated with NUC, and HBsAg seroclearance has been regarded as an optimal endpoint of treatment with NUC in clinical practice guidelines.13 ,14 However, little is known about the long-term clinical outcomes and durability of NUC-induced HBsAg seroclearance. Moreover, it has been suggested that seroclearance of HBsAg during lamivudine therapy may not indicate viral clearance because it may reflect a point mutation in the S gene that results in failure to detect HBsAg.15
Therefore, in this large-scale cohort study, we analysed the data of 110 CHB patients who achieved HBsAg seroclearance after NUC therapy to evaluate the long-term clinical outcomes and durability after NUC-induced HBsAg seroclearance.
Patients and methods
Study subjects
The study population was recruited from 5409 consecutive patients with hepatitis B who commenced treatment with lamivudine (100 mg/day, n=3408) or entecavir (0.5 mg/day, n=2001) at Asan Medical Center, Seoul, Korea, between 1 November 1999 and 31 December 2011. The characteristics of the 5409 patients are as follows; previously untreated adults aged 20–80 years; detection of HBsAg and serum HBV DNA (>10[4] copies/mL) for more than 6 months, no evidence of co-infection with hepatitis C virus, hepatitis D virus, or HIV, no treatment with interferon, before starting treatment with lamivudine or entecavir; no organ transplantation or death within 6 months, no evidence of HCC within 1 year after starting the treatment; duration of the treatment for more than 6 months. Patients who developed HCC before HBsAg seroclearance were excluded.
The patients routinely underwent clinical examinations, liver function tests and HBV DNA analyses every 3–6 months. Additionally, serum HBsAg and anti-HBs analyses and ultrasonography were performed every 6–12 months during treatment and during follow-up.
Serum assays
Serum HBsAg was tested qualitatively (Architect assay, Abbott Laboratories, Chicago, Illinois, USA or immunoradiometric assay kit; DiaSorin, Vercelli, Italy) or quantitatively (Architect assay, Abbott Laboratories; lower limit of detection (LLOD), 0.05 IU/mL). Serological markers, including anti-HBs, HBeAg, and anti-HBe, were determined by using enzyme immunoassays (Abbott Laboratories). Serum HBV DNA levels were measured by using a hybrid capture assay (Digene hybrid capture II assay, Digene Diagnostics, Gaithersburg, Maryland, USA; LLOD, 20 000 IU/mL) before 2007, and then, by using a real-time PCR assay (Abbott Laboratories; LLOD, 15 IU/mL).
Genotypic analyses for HBV resistance mutations to lamivudine were performed in patients who developed HBV DNA breakthrough (≥1 log10 copies/mL increase in serum HBV DNA from nadir on two consecutive tests) during treatment by restriction fragment mass polymorphism analyses as described.16 The HBV genotype was not determined because almost all Korean patients with CHB have genotype C HBV.17 Serum aspartate aminotransferase (AST), alanine aminotransferase (ALT), albumin and total bilirubin concentrations, and international normalised ratio (INR) for prothrombin time were measured by using standard laboratory procedures. The upper limit of normal (ULN) of ALT was defined as 30 IU/L for men and 19 IU/L for women. Liver cirrhosis and HCC were diagnosed by imaging studies such as ultrasonography and/or CT scanning.
Definitions of events
The events of interest during follow-up after HBsAg seroclearance were defined as follows: HBsAg seroclearance, loss of HBsAg detectability at least once in the serum after treatment; anti-HBs seroconversion, detection of anti-HBs combined with HBsAg negativity; sustained response, HBsAg negativity combined with undetectable HBV DNA by PCR; serological reversion or HBsAg reversion, reappearance of serum HBsAg; virological reversion, detection of HBV DNA after HBsAg seroclearance; composite reversion, virological reversion and/or HBsAg reversion; biochemical relapse, ALT flare >5×ULN.
Statistical analysis
Patients were followed-up from the date of starting treatment with lamivudine or entecavir to the death, liver transplantation, or last follow-up date (31 March 2013). Baseline characteristics were analysed by χ2 test and the Student t test for categorical and continuous variables, respectively. Predictive factors for HBsAg seroclearance were analysed by Cox proportional hazard model. To reduce the effect of bias and potential confounding, we performed rigorous adjustment for significant differences in the baseline characteristics of patients by propensity score-matching. Propensity scores were derived by using multiple logistic regression analysis and were matched for the patients with and without HBsAg seroclearance (1:4) by using nearest-neighbour matching algorithm with a range of 0.1 SD of the estimated propensity scores. The cumulative rates of HBsAg reversion, anti-HBs seroconversion, and virological reversion were estimated and compared with the use of methods described previously.18 A log-rank test was used to compare the cumulative rates of virological reversion by the prior selection for lamivudine-resistance HBV mutants. Potential predictive factors for composite reversion were evaluated by an extended Cox proportional hazards model for time-dependent covariate (anti-HBs seroconversion).18 Statistical analyses were performed by using SPSS V.20 (SPSS, Chicago, Illinois, USA) and R V.2.13.2 (http://cran.r-project.org/). A p value less than 0.05 was considered statistically significant.
Results
Baseline characteristics
During a median follow-up period of 6 years (33 567 patient-years), a total of 110 among 5409 patients achieved HBsAg seroclearance, corresponding to a 0.33% annual seroclearance rate. The median years from the initiation of treatment to HBsAg seroclearance were 6.77 (IQR 4.56–10.02).
The baseline characteristics of the 110 patients who achieved HBsAg seroclearance after treatment with lamivudine or entecavir were compared with 5299 patients who did not achieve HBsAg seroclearance (table 1). At the initiation of NUC therapy, the HBsAg seroclearance group was significantly younger (p=0.02), had lower prevalence of HBeAg-positivity (p=0.01), lower level of serum HBV DNA (p<0.01), higher level of ALT (p=0.03) and albumin (p=0.02), and lower prevalence of cirrhosis (p<0.01), compared with no HBsAg seroclearance group. In the HBsAg seroclearance group, more patients had been treated with lamivudine compared with no HBsAg seroclearance group (97.3% vs 62.3%; p<0.01). In the HBsAg seroclearance group, 37 (33.6%) patients were selected for resistance HBV mutants during lamivudine treatment: 27 with rtM204V/I+rtL180M, 7 with rtM204V/I, and three with rtM204V+rtL180M+rtA181T+rtN236T. Of these, 13 patients switched treatment to adefovir monotherapy and four were treated with the combination of lamivudine and adefovir. One patient switched treatment to entecavir monotherapy. The other patients continued lamivudine monotherapy without further virological breakthrough afterwards. The overall median treatment duration and overall median follow-up period were 4.3 years (IQR 2.1–6.8 years) and 9.8 years (IQR 7.5–12.0 years), respectively, in HBsAg seroclearance group. The overall median follow-up period was significantly longer in HBsAg seroclearance group compared with no seroclearance group (p<0.01).
Characteristics of patients by HBsAg seroclearance in the entire and propensity score-matched cohorts
Of the 55 patients with baseline HBeAg-positivity in the HBsAg seroclearance group, all experienced HBeAg loss, and 38 (69.1%) achieved anti-HBe seroconversion during treatment before HBsAg seroclearance. The median duration of consolidation therapy after HBeAg loss was 35 months (IQR 12–59 months).
Predictive factors for HBsAg seroclearance
Baseline factors that showed significant difference between groups with and without HBsAg seroclearance were examined by multivariable analysis as potential predictors for HBsAg seroclearance (table 2). ALT level >5 times of ULN was significantly associated with higher probability of HBsAg seroclearance (HR 1.80, p<0.01). On the contrary, HBeAg positivity (HR 0.46, p<0.01), high HBV DNA level (log10 IU/mL; HR 0.61, p<0.01), and cirrhosis (HR 0.48, p<0.01) were inversely associated with the probability of HBsAg seroclearance. Age (HR 1.01, p=0.19), albumin level (HR 0.80, p=0.20), and antiviral agent (entecavir; HR 0.30, p=0.05) were not significantly associated with HBsAg seroclearance.
Predictive factors for HBsAg seroclearance
Clinical outcomes after HBsAg seroclearance
During a median follow-up period of 2.1 years (287 patient-years) after HBsAg seroclearance, one patient with cirrhosis at baseline received liver transplantation for liver failure after surgical operation for benign colon disease, but died. Another patient who had cirrhosis at baseline developed HCC at 6 months after HBsAg seroclearance. These patients had undetectability of HBsAg in two consecutive determinations before the occurrence of clinical events. No other patient died, received liver transplantation, or developed HCC.
Comparison of clinical outcomes in propensity score-matched cohorts
Two separate propensity score-matched cohorts with 1:4 matching were generated to compare the clinical outcomes between patients with and without HBsAg seroclearance.
First, the patients were matched at the time of treatment initiation for age; gender; duration of follow-up; cirrhosis; HBeAg status; treatment drug; HBV resistance; and levels of HBV DNA, ALT, albumin and bilirubin. After matching, there were no significant differences in most baseline characteristics between the patients with and without HBsAg seroclearance (table 1). Among the patients in the matched cohort, all with HBsAg seroclearance and 309 of 372 patients (83.1%) with no HBsAg seroclearance achieved undetectable HBV DNA during NUC treatment (p<0.01). The mean time to HBV DNA undetectability was 10.6 months and 24.0 months in HBsAg seroclearance group and no HBsAg seroclearance group, respectively (p<0.01). The overall treatment duration was shorter in patients with HBsAg seroclearance, because the treatment was discontinued after achieving HBsAg seroclearance. In the matched comparison, HBsAg seroclearance group showed significantly higher overall transplant-free survival (HR 0.10; 95% CI 0.01 to 0.72; p=0.02; figure 1A) and significantly lower incidence of HCC (HR 0.06; 95% CI 0.01 to 0.41; p<0.01; figure 1B).
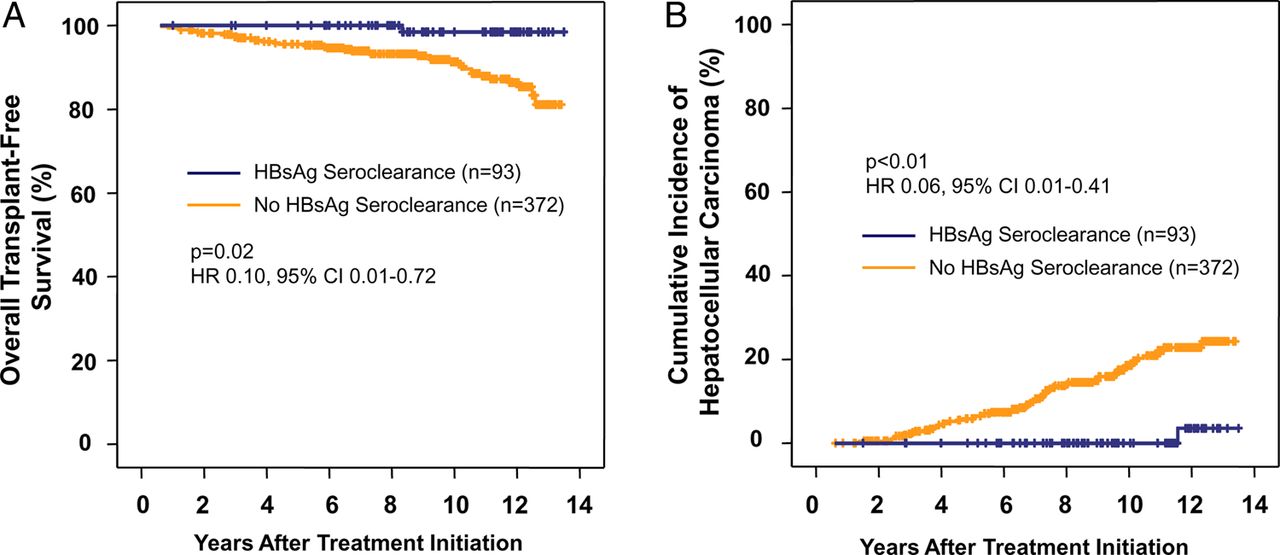
Kaplan–Meier curves for clinical outcomes after nucleoside analogue therapy in a propensity score-matched cohort. Propensity scores were derived from the variables at the treatment initiation and were matched for the patients with and without HBsAg seroclearance creating 93:372 (1:4) matched pairs. Panel A shows overall transplant-free patient survival; Panel B, cumulative incidence of hepatocellular carcinoma.
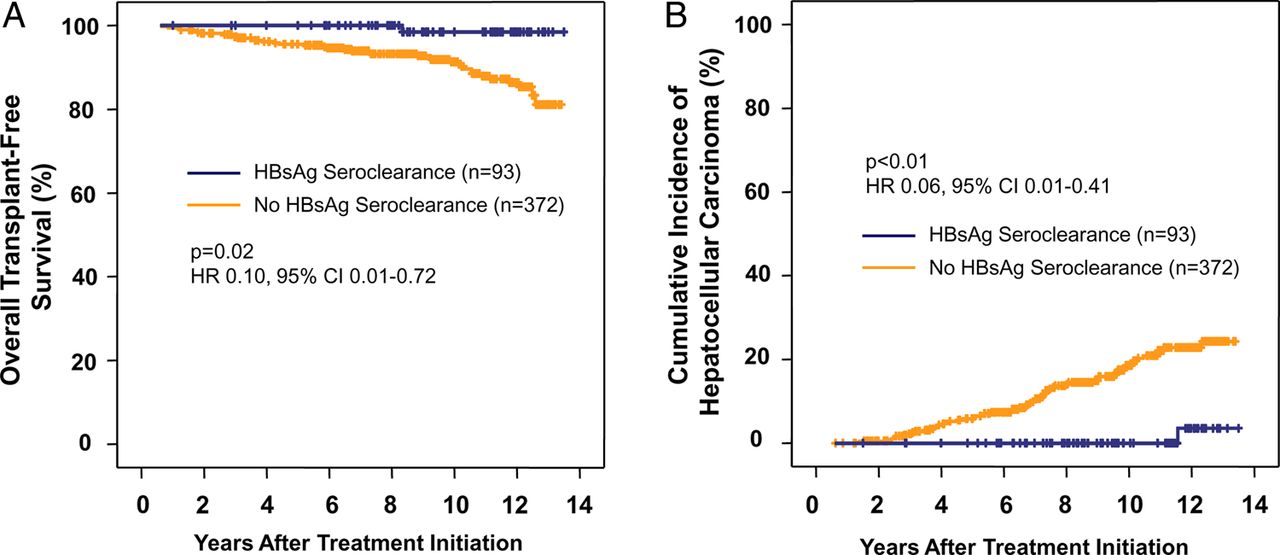
Second, to compare the clinical outcomes after HBsAg seroclearance, we included only those who were followed-up for more than 6.77 years, which was the median time to HBsAg seroclearance in the HBsAg seroclearance group, for the matching in the no HBsAg seroclearance group. After then, the two groups were matched for the variables at baseline (see online Supplementary table), and were analysed for clinical outcomes from the HBsAg seroclearance, or 6.77 years after treatment initiation. In this matched comparison, HBsAg seroclearance group showed similar overall transplant-free survival (HR 0.21; 95% CI 0.03 to 1.52; p=0.12; figure 2A), but significantly lower incidence of HCC (HR, 0.13; 95% CI 0.02 to 0.95; p=0.04; figure 2B).

Kaplan–Meier curves for clinical outcomes after HBsAg seroclearance in a separate propensity score-matched cohort. The patients without HBsAg seroclearance were analysed from 6.77 years after treatment initiation which was the median time from the treatment initiation to HBsAg seroclearance in the HBsAg seroclearance group. Panel A shows overall transplant-free patient survival. Panel B, cumulative incidence of hepatocellular carcinoma.
Durability of HBsAg seroclearance
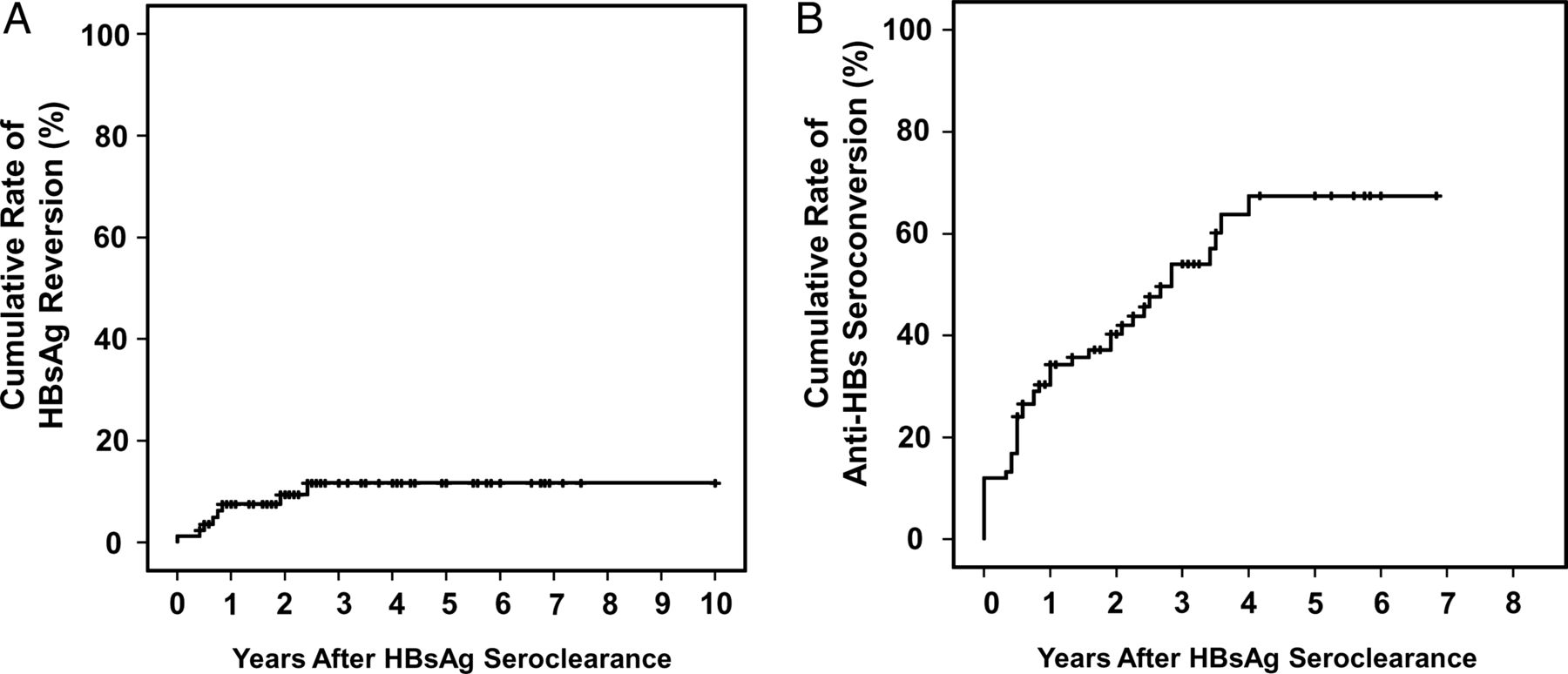
HBsAg reversion occurred in eight patients within 3 years after HBsAg seroclearance and treatment discontinuation (figure 3A). Quantitative or semiquantitative HBsAg level was measured in all the eight patients at HBsAg reversion, which was extremely low (0.05–1.0 IU/mL). Seven of these patients achieved spontaneous reclearance of HBsAg without retreatment during further follow-up. One remaining patient was HBsAg-positive at the end of the 2-year follow-up period after HBsAg seroclearance, with extremely low HBsAg level (1.0 IU/mL) and undetectable serum HBV DNA by PCR assay. The cumulative rate of HBsAg reversion by Kaplan–Meier analysis at 12 months and 36 months were 7.6% and 11.7%, respectively, with no further increase thereafter (figure 3A).

Kaplan–Meier curves for the cumulative rates of HBsAg reversion and anti-HBs seroconversion after HBsAg seroclearance. Panel A shows cumulative rates of HBsAg reversion. Panel B, anti-HBs seroconversion.
The cumulative rates of anti-HBs seroconversion at 1, 2, 3 and 4 years after HBsAg seroclearance were 34.3, 40.3, 54.0 and 67.4%, respectively, by Kaplan–Meier analysis (figure 3B). All the patients maintained the status of anti-HBs seroconversion until the end of follow-up, except one who experienced HBsAg reversion and HBV DNA reversion after development of HCC.
Durability of virological response
A total of 17 patients experienced virological reversion (serum HBV DNA > 60 IU/mL) with cumulative rates of 13.8, 18.7 and 29.6% at 1, 2 and 4 years after HBsAg seroclearance, respectively, by Kaplan–Meier analysis (figure 4A). The maximal level of HBV DNA in these patients was <2000 IU/mL. Virological reversion was transient in nine patients, and became spontaneously undetectable within 6 months of the first HBV DNA detection and, thereafter, remained persistently negative until the end of follow-up. Six patients had low levels of HBV DNA (37–99 IU/mL) at the end of follow-up. No one showed HBV DNA level higher than 2000 IU/mL during follow-up.

Kaplan–Meier analysis of the cumulative rates of virological reversion after HBsAg seroclearance. Panel A shows cumulative rates of virological reversion by HBV DNA levels at the time of reversion. Panel B, cumulative rates of HBV DNA reversion (>60 IU/mL) by the selection for lamivudine (LAM)-resistance mutants during treatment.
The patients with and without lamivudine-resistant HBV mutants during treatment did not differ significantly in terms of the cumulative rates of virological reversion (p=0.66; figure 4B).
A sustained response, which was defined as HBsAg negativity combined with undetectable HBV DNA, was observed in more than 90% of the patients at most of the time points during follow-up, namely 66 of 73 patients (90.4%), 51 of 55 patients (92.7%), and 31 of 33 (93.9%) patients at 1, 2 and 3 years, respectively.
Predictive factors for composite reversion
Potential predictive factors were analysed for composite reversion by the extended Cox proportional hazard model (table 3). Only anti-HBs seroconversion during follow-up period was significantly associated with a decreased rate of composite reversion by multivariable analysis (HR 0.21; p=0.03).
Predictive factors for composite reversion after HBsAg seroclearance
Serial changes in HBsAg levels before HBsAg seroclearance
Comparison of serial HBsAg levels during 2 years before HBsAg seroclearance in a propensity score-matched cohort of patients showed significantly lower levels and greater decline of HBsAg titres in patients with HBsAg seroclearance than those without HBsAg seroclearance (p<0.01; figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Serial changes in HBsAg levels during 2 years before HBsAg seroclearance in a propensity score-matched cohort of patients with and without HBsAg seroclearance. The data of patients without HBsAg seroclearance were derived from the last 2 years of follow-up.
Discussion
In this study, we showed that CHB patients who achieve HBsAg seroclearance after treatment with NUC were associated with minimal risk of death, liver transplantation, or HCC. Among 110 patients with HBsAg seroclearance, only two patients with baseline cirrhosis died or developed HCC. The HBsAg seroclearance was durable in most patients during long-term follow-up period. Few patients experienced serological and/or virological reversion; however, it was transient and characterised by extremely low serum levels of HBsAg and/or HBV DNA in all patients.
To the best of our knowledge, this is the largest study investigating the long-term clinical outcomes and durability of NUC-induced HBsAg seroclearance. Moreover, the majority of the patients included in this study were assumed to have genotype C HBV and long duration of infection by the vertical mode of transmission, both of which are associated with significantly lower chance of HBeAg seroconversion or HBsAg seroclearance.12 ,19–23
The results of this study are comparable with previous natural course studies which showed that spontaneous HBsAg seroclearance was associated with a reduced risk of disease progression, HCC and mortality, compared to patients who remain HBsAg-positive.12 ,24 ,25 However, our study also indicates that liver failure or HCC could still develop in some patients with baseline cirrhosis, as also documented in previous studies for patients with spontaneous HBsAg seroclearance.12 ,24 ,25
Several small case series have questioned the durability of HBsAg seroclearance after NUC therapy. In particular, a recent report suggested that HBsAg seroclearance during lamivudine therapy may not necessarily indicate viral clearance because it may reflect a point mutation in the S gene that results in the failure to detect HBsAg.15 In that report, six of 11 patients who experienced HBsAg seroclearance had the P120A mutation in the S gene, and all 11 patients had detectable serum HBV DNA, as determined by PCR. Since the HBV polymerase gene overlaps the envelope gene, the lamivudine-selected polymerase mutations M204I and L180M/M204I may produce changes within the overlapping S gene that encodes the HBsAg protein,15 ,26 ,27 which makes HBsAg protein to be less antigenic and unable to be detected by anti-HBs antibody.28–31 However, such drug-driven changes in HBsAg will not substantially affect the performance of recent ELISA-based diagnostic assays for HBsAg because these assays increasingly rely on multiple monoclonal and polyclonal components that bind to known HBsAg variants.32 In any case, potential S gene mutant selection can only be considered in patients who have persistent viremia despite having apparently become HBsAg-seronegative. Thus, HBsAg seroclearance should only be regarded as an optimal endpoint if it is associated with long-lasting and complete HBV DNA suppression, and also with favourable clinical outcomes.
In the present study, about 20% of patients experienced transient detection of extremely low serum levels of HBV DNA after treatment discontinuation after HBsAg seroclearance. However, the results are comparable with previous natural course studies which showed that 10–20% of patients with spontaneous HBsAg seroclearance had persistent low-level viremia between 1 year and 10 years after HBsAg seroclearance.12 ,33 ,34 Thus, the present study suggests that the HBsAg seroclearance observed after NUC therapy reflects a decrease in HBsAg production that is secondary to extremely low viral replication rather than the occurrence of escape mutations that hamper HBsAg detection by commercially available assays. Further supporting this, in the present study, the selection for lamivudine-resistance HBV mutants during treatment did not associate with increased virological reversion. These results are in accordance with previous experimental data that showed that lamivudine-associated compensatory substitutions alone do not appear to affect HBsAg epitope reactivity despite inducing amino acid substitutions in HBsAg.27 ,31 However, since other lamivudine-compensatory mutations and the entecavir-resistance mutations can act synergistically to induce significant alterations in the ‘a’ determinant,31 there is still possibility that the presence of multiple-resistance mutations might be associated with a higher risk of failing to detect HBsAg.
Although the mechanism of HBsAg seroclearance remains largely unknown, it has been suggested that the role of an as yet unknown immune-related mechanism is crucial.30 ,35 Our data showing that high baseline ALT levels and anti-HBs seroconversion during follow-up was a significant protector from composite reversion support the importance of immunological mechanisms in HBsAg seroclearance. The production of anti-HBs may reflect more profound immune pressure from the host, resulting in more efficient control of viral replication.34 ,36 It has been suggested that the hypo-responsiveness of HBV-specific T cells in CHB patients can be restored after long-term effective treatment with NUC,37 ,38 and high baseline ALT and interferon-inducible protein-10 levels were associated with stronger HBsAg decline in patients on NUC treatment.35 ,39 Interestingly, the later studies also found no difference between different NUCs on HBsAg decline,35 ,39 which fits with the data presented here. These data are in line, that the immune response rather than the effect on reverse transcription of HBV replication is associated with HBsAg seroclearance.
Previous studies suggested that early changes in HBsAg levels are associated with HBsAg seroclearance, and decline of HBsAg levels is less pronounced in HBeAg-negative patients compared with HBeAg-positive patients during NUC therapy.35 ,40 In randomised trials with entecavir or tenofovir, the HBsAg seroclearance occurred exclusively in HBeAg-positive patients.4 ,5 ,7 However, this issue is still controversial because a more recent long-term study showed no association between the rates of HBsAg reduction and baseline HBeAg status during 10 years of NUC treatment.41 Furthermore, similar to our study, other recent studies showed that HBeAg-negativity was associated with high chance of HBsAg seroclearance during NUC therapy.6 ,42 ,43 It is worthy to note that the curves for changes in HBsAg levels shown in most of the previous studies were fitted including all serum HBsAg measurements at each time point. However, patients may show markedly different kinetics of HBsAg decline during interferon or NUC therapy regardless of their basal HBeAg status.39 ,44–46 Thus, some of the patients show rapid decline of HBsAg levels during therapy which is dissociated with the mean changes of HBsAg levels, eventually achieving HBsAg seroclearance. Lower levels of HBV DNA were identified as an independent predictive factor for HBsAg seroclearance, and may be associated with higher chance of HBsAg seroclearance among HBeAg-negative patients in our study.
The patients in this study showed markedly low levels of HBsAg during 2 years before achieving HBsAg seroclearance of less than 10 IU/mL. It has been suggested that, in HBeAg-negative patients with HBV genotype B or C infection who have low HBV DNA level, HBsAg level of less than 200 IU/mL or 10 IU/mL may be a strong predictor of spontaneous HBsAg seroclearance.47–49 Another German study showed that patients who received no treatment demonstrated similar HBsAg kinetics during the natural course of HBV infection compared with those who are being treated with NUC.39 These results suggest the possibility that the patients in this study would have lost spontaneously HBsAg without NUC treatment. This suggests that NUC therapy may have only a limited impact on HBsAg suppression.50 However, long-term NUC therapy has proven efficacy in preventing hepatic necro-inflammation and fibrosis, and also may increase the cumulative rates of HBsAg seroclearance over time to above 10%.4–7 These results indicate that with the recent availability of highly potent NUC agents, HBsAg seroclearance is not as rare as it once was, and that it might be a realistic goal that can be achieved by the profound and sustained suppression of HBV replication if the treatment is combined with active host immune responses.
This study may have several limitations. The main limitation is its retrospective design. This reflects the fact that HBsAg seroclearance is rare. However, all patients who were treated with lamivudine or entecavir in our institution and met the eligibility criteria for this study were enrolled. Thus, the enrolled patients may adequately represent the population of interest. Second, the duration of treatment with entecavir was shorter than the duration of lamivudine treatment because entecavir was introduced in our institution later than lamivudine. This may explain why fewer patients achieved HBsAg seroclearance with entecavir than with lamivudine at least in part. However, the antiviral agent used was not identified as a significant predictor for HBsAg seroclearance by multivariable analysis. Third, not all patients were tested for HBsAg quantitatively before HBsAg seroclearance due to the unavailability of the test during the early period of the study span. The incidence of HBsAg seroclearance may be associated with the detection sensitivity of HBsAg assay. The LLOD of HBsAg assay used at early phase of this study, before 2005, was relatively higher (1.0 IU/mL) than the LLOD of that used at later phase (0.05 IU/mL), after 2005, in our study. It might also explain apparently lower HBsAg seroclearance rate in patients who were treated with entecavir compared with lamivudine. Fourth, because of the lack of stored serum samples, we could not analyse the presence of point mutations in S gene of HBV in patients with virological reversion after HBsAg seroclearance. However, the virological reversions in our study patients might have little clinical and virological significance because they were transient with extremely low levels of HBV DNA. Finally, the HBV genotype in our study patients was not tested. This reflects the fact that HBV genotyping is not performed in routine clinical practice because almost all Korean CHB patients have genotype C HBV.17
In conclusion, HBsAg seroclearance achieved after NUC treatment was associated with favourable clinical outcomes and was durable in most patients with CHB during long-term follow-up. However, sustained clinical monitoring and surveillance for HCC may be required because liver failure or HCC could occur after HBsAg seroclearance in some patients with baseline cirrhosis.
Acknowledgments
The authors thank Dr Seungbong Han for his excellent help in statistical analyses.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Contributors G-AK and Y-SL were responsible for the concept and design of the study, the acquisition, analysis and interpretation of the data, and the draughting of the manuscript. DL, JHS, KMK, HCL, Y-HC and YSL helped with the acquisition of the data and critically revised the manuscript for important intellectual content. DJS supervised the study and provided critical revision of the manuscript.
-
Competing interests None.
-
Ethics approval This study was approved by the Institutional Review Board of Asan Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.