Article Text

Abstract
Objectives Despite being proposed 4 years ago, there has been no independent validation study of the Rome IV criteria for IBS. We assessed their performance for the diagnosis of IBS in secondary care and compared them with the previous iteration, the Rome III criteria.
Design We collected complete symptom data from consecutive adult patients with suspected IBS referred to a single UK clinic. All subjects underwent relatively standardised workup, with assessors blinded to symptom status. The reference standard used to confirm IBS was the presence of lower abdominal pain or discomfort in association with altered stool form or frequency, in a patient with no evidence of organic gastrointestinal disease after investigation. Sensitivity, specificity and positive and negative likelihood ratios (LRs), with 95% CIs, were calculated for each of the diagnostic criteria.
Results The level of agreement between the Rome IV and Rome III criteria was good (kappa=0.65). Compared with the reference standard, sensitivity and specificity of the Rome IV criteria in 572 patients (431 (75.3%) women, mean age 36.5 years) were 82.4% and 82.9%, respectively. Positive and negative LRs for the Rome IV criteria were 4.82 (95% CI 3.30 to 7.28) and 0.21 (95% CI 0.17 to 0.26), respectively. The Rome IV criteria performed best in those with IBS with constipation or mixed bowel habits. In 471 patients (350 (74.3%) women, mean age 36.7 years), compared with the reference standard, the sensitivity and specificity of the Rome III criteria were 85.8% and 65.0%; positive and negative LRs were 2.45 (95% CI 1.90 to 3.27) and 0.22 (0.16 to 0.29), respectively. Incorporating mood and extraintestinal symptom reporting into diagnostic criteria did not improve their performance significantly.
Conclusions The Rome IV criteria performed significantly better than the Rome III criteria in diagnosing IBS in this single centre secondary care study, although the clinical relevance of this is uncertain.
- irritable bowel syndrome
- abdominal pain
- diarrhoea
Data availability statement
No additional data available.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
IBS is common, but physicians can find it challenging to diagnose.
Symptom-based diagnostic criteria were developed to facilitate a positive diagnosis of IBS, but previous studies demonstrate that they perform only modestly.
The Rome IV criteria are the current gold standard for diagnosing IBS, but their performance has not been assessed in an independent validation study.
What are the new findings?
The Rome IV criteria were more specific than the Rome III criteria in diagnosing IBS in secondary care, in this single centre study.
The positive likelihood ratio of the Rome IV criteria was 4.82 compared with 2.45 with Rome III, and the 95% CIs around these estimates did not overlap, although the clinical relevance of this is uncertain.
The Rome IV criteria were significantly more accurate, in terms of the positive likelihood ratio, in patients with IBS with constipation or mixed bowel habits, compared with those with IBS with diarrhoea.
How might it impact on clinical practice in the foreseeable future?
The Rome IV criteria should continue to be the gold-standard diagnostic approach to IBS, although further independent validation studies are required.
However, physicians consulting with patients with IBS with diarrhoea should remain alert to organic causes of symptoms before making a diagnosis of IBS.
Introduction
IBS is a functional bowel disorder, or disorder of gut–brain interaction,1 characterised by abdominal pain, in association with altered stool form or stool frequency.2 Although the condition is common, affecting between 4% and 10% of otherwise healthy people in the community at any one time,3 physicians can find it challenging to diagnose, because symptoms often overlap with those of organic gastrointestinal conditions such as coeliac disease,4 5 inflammatory bowel disease,6 microscopic colitis7–9 or bile acid diarrhoea.10
Partly because of this uncertainty, symptom-based diagnostic criteria were developed to help physicians make a positive diagnosis when consulting with patients with suspected IBS. The Manning criteria were proposed in the 1970s11 and, leading on from these, factor analysis studies demonstrated that the lower gastrointestinal symptoms thought to make up IBS clustered together.12 This led to the development of the Rome criteria in the 1990s,13 which have undergone three subsequent revisions, the most recent being the Rome IV criteria in 2016.2 Previous validation studies of symptom-based diagnostic criteria demonstrate that they perform only modestly in diagnosing IBS.14–17 Nevertheless, their use is important to minimise over investigation, which can be anxiety-provoking for patients with IBS.18 In addition, if they perform accurately, this may help reassure patients that the physician’s diagnosis of IBS is correct as well as reducing costs to the health service of managing the condition.
In moving from the Rome III criteria to the Rome IV criteria for IBS, important changes were made: the term ‘abdominal discomfort’ was removed from the definition, and the symptom frequency at which abdominal pain needed to be experienced to meet criteria for IBS was increased to a minimum of 1 day per week, from 3 days per month.2 There were two main reasons for these changes. First, ‘discomfort’ is not an understandable term in many languages.18 Second, a normative survey revealed that using a higher threshold for the frequency of abdominal pain required to meet criteria would lead to fewer healthy people in the general population being misclassified as having IBS, potentially improving the specificity of the Rome IV criteria compared with their predecessor.19 These changes appear to have led to the Rome IV criteria selecting a group of patients with IBS with more severe symptoms and higher levels of psychological comorbidity.20–22
In an initial validation study, performed by the Rome Foundation, sensitivity of the Rome IV criteria was assessed in more than 800 patients with a functional gastrointestinal disorder and estimated to be 63%.19 In a separate cohort of almost 6000 people from the general population, specificity was reported to be 97%.19 Taken together, these results yield a positive likelihood ratio (LR) for the Rome IV criteria in diagnosing IBS of 21, implying that patients meeting these criteria are 21 times more likely to have IBS than to not have IBS. However, their performance was not compared with the previous gold standard, the Rome III criteria, and to our knowledge, there have been no independent validation studies performed, to date. It is important for current diagnostic criteria for IBS to have been validated independently, and compared with the previous iteration, to assess whether the changes made have indeed improved their diagnostic performance. We therefore validated the Rome IV and III criteria for IBS simultaneously in secondary care.
Methods
Participants and setting
The study was conducted among individuals newly referred from primary care with suspected IBS between September 2016 and March 2020. Unselected, consecutive new patients aged ≥16 years referred to our specialist IBS clinic in Leeds Teaching Hospitals NHS Trust, Leeds, UK, were recruited. The hospital serves a local population of 800 000, and the clinic does not take tertiary referrals from other centres but instead provides a pathway to rapid diagnosis and treatment for patients suspected to have IBS referred by local primary care physicians. Four experienced gastroenterologists provide their services to this clinic. There were no exclusion criteria, other than an inability to understand written English. All patients were provided with a detailed questionnaire as part of their clinical assessment at their first appointment. As these data were collected to guide treatment in routine clinical practice, ethical approval was not required.
Data collection and synthesis
Demographic, symptom and mood data
All demographic, symptom and mood data were collected prospectively at the initial clinic visit, prior to referral for investigations. Age and gender were recorded, and symptom data captured using the Rome IV questionnaire for IBS in all patients2 and the Rome III questionnaire in a subset.23 The presence or absence of Rome III or Rome IV-defined IBS was assigned according to the scoring algorithms proposed for use with these questionnaires,2 24 detailed in online supplemental table 1. We assessed symptom severity using the IBS severity scoring system (IBS-SSS),25 a validated seven-item self-administered questionnaire measuring presence, severity and frequency of abdominal pain, presence and severity of abdominal distension, satisfaction with bowel habit and degree to which IBS symptoms are affecting, or interfering with, the person’s life. The maximum score is 500 points: <75 indicates remission of symptoms; 75–174 mild symptoms; 175–299 moderate symptoms and 300–500 severe symptoms. Anxiety and depression data were collected using the hospital anxiety and depression scale (HADS).26 The total HADS score ranges from a minimum of 0 to a maximum of 21 for either anxiety or depression. Severity for each was categorised into normal (total HADS depression or anxiety score 0–7), borderline abnormal (8-10) or abnormal (≥11). We collected extraintestinal symptom data using the patient health questionnaire-12 (PHQ-12),27 derived from the validated PHQ-15.28 The total PHQ-12 score ranges from a minimum of 0 to a maximum of 24. All questionnaire data were entered into a database at the initial clinic visit, prior to referral for investigations.
Supplemental material
Investigative workup
Patients underwent relatively standardised workup. All patients had full blood count and C reactive protein, either prior to referral by their general practitioner or at their first visit to the clinic. Coeliac serology was checked in all patients, regardless of predominant bowel habit. Faecal calprotectin was checked in patients aged <40 years who reported diarrhoea, with subsequent colonoscopy if ≥100 μg/g. In those aged ≥40 years with either diarrhoea or a recent change in bowel habit, a colonoscopy was requested. Colonoscopy was also requested, at the physician’s discretion, in other patients with atypical features, such as nocturnal symptoms. Irrespective of age, patients with diarrhoea underwent 23-seleno-25-homo-tauro-cholic acid (SeHCAT) scanning to exclude bile acid diarrhoea as a cause for their symptoms. Given the response to bile acid sequestrants is best in those with moderate to severe bile acid diarrhoea,29 only patients with a SeHCAT retention of <10% at 7 days were classed as having bile acid diarrhoea. Finally, in patients with constipation with symptoms suggestive of obstructive defaecation, anorectal physiology studies were requested. Any other investigations, for example, faecal elastase or small bowel investigations, including magnetic resonance enterography or wireless capsule endoscopy, were at the discretion of the consulting doctor. The responsible clinicians performing colonoscopic examinations, radiological or physiologic investigations or histological interpretation of biopsy specimens remained blinded to questionnaire data. We classified the following findings as being consistent with organic disease after investigation: coeliac disease, Crohn’s disease, ulcerative colitis, inflammatory bowel disease-unclassified, microscopic colitis, ischaemic colitis, radiation enteritis, colorectal carcinoma, bile acid diarrhoea or exocrine pancreatic insufficiency (defined as faecal elastase <200 μg/g). Diverticular disease, colorectal adenoma, haemorrhoids or anal fissures were not considered to represent organic disease. Using these data, we were able to classify patients according to the presence or absence of organic gastrointestinal disease after investigation.
Reference standard
For the Rome IV criteria, the reference standard used to define the presence of IBS was the presence of lower abdominal pain in association with altered stool form or frequency elicited during the clinical history at the first outpatient clinic appointment, in a patient who exhibited no evidence of organic gastrointestinal disease after the investigative algorithm described above. For the Rome III criteria, this was identical other than including the presence of abdominal pain and/or discomfort.
Statistical analysis
We measured agreement between the Rome IV and III criteria for the diagnosis of IBS, and the reference standard, using the modified Kappa statistic, where a value <0.2 indicates poor agreement and a value >0.8 indicates very good agreement beyond chance. These statistical analyses were performed using SPSS for Windows V.26.0 (SPSS, Chicago, Illinois, USA). The primary aim of the study was to describe the performance of the Rome IV criteria for IBS overall, and according to subtype, in evaluating the presence of IBS versus the reference standard. However, we also wanted to compare the performance of the Rome IV criteria for IBS with the previous iteration the Rome III and assess the impact of incorporating measures of abnormal mood and extraintestinal symptom reporting, which are both associated with IBS, into the diagnostic criteria. In the case of the latter, we combined the Rome IV or III criteria with the presence of either abnormal levels of anxiety or depression on the HADS or with the presence of high levels of extraintestinal symptom reporting according to the PHQ-12. The sensitivity, specificity and positive and negative predictive values, and their 95% CIs, were calculated for each of these. The positive LR and negative LR, and their 95% CIs, were also calculated. The positive LR is derived from the formula: positive LR=sensitivity/(1−specificity), while the negative LR is derived from the formula: negative LR=(1−sensitivity)/specificity. All these analyses were performed using StatsDirect V.3.2.10 (StatsDirect, Sale, Cheshire, England).
Results
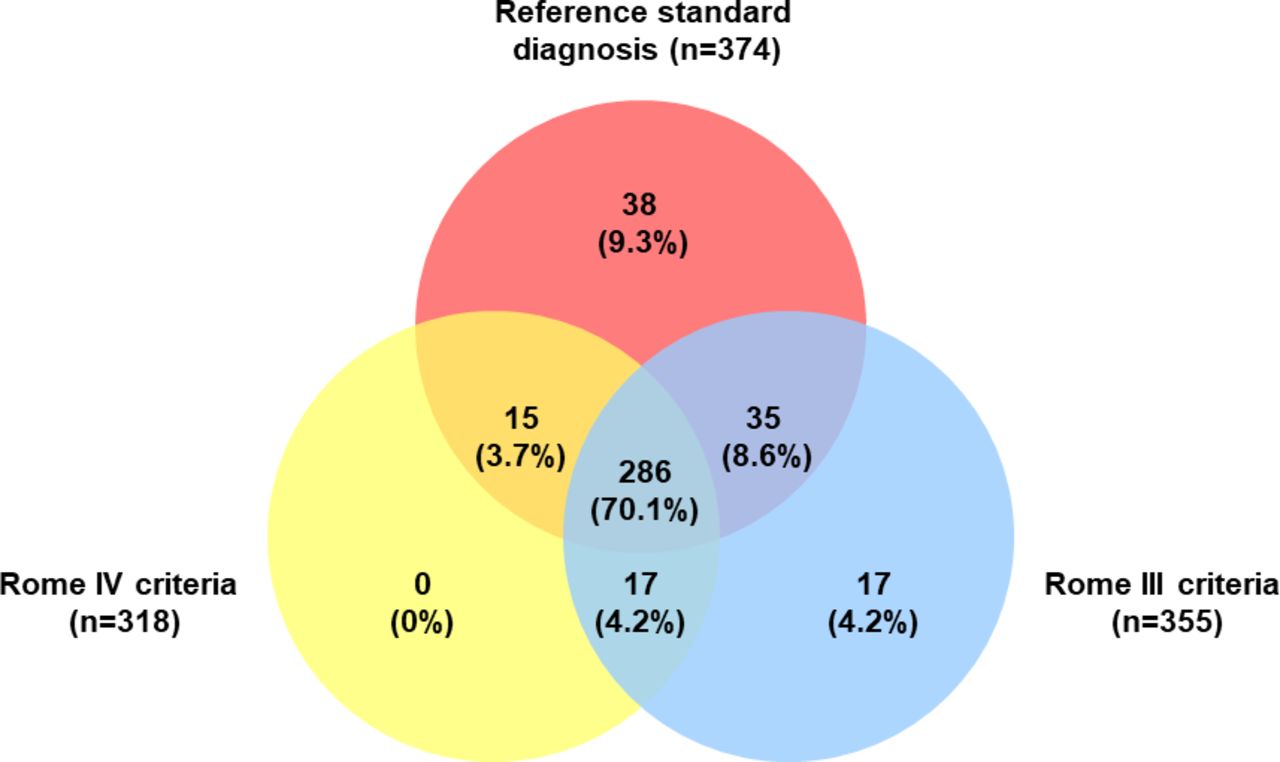
We recruited all 577 patients attending the clinic during the study period, of whom 436 (75.6%) were women (age range 16–88 years; mean age 36.6 years). Of these, 572 (99.1%) provided sufficient data to ascertain Rome IV IBS symptom status (431 (75.3%) women, mean age 36.5 years) and 471 (81.6%) Rome III IBS symptom status (350 (74.3%) women, mean age 36.7 years). Characteristics of individuals meeting the Rome IV and Rome III criteria are provided in table 1. The majority had severe symptoms, according to the IBS-SSS, and there were high levels of mood disorders and extraintestinal symptom reporting, in keeping with a referral population of patients with IBS. There were 471 individuals who provided sufficient symptom data to examine the degree of overlap between the Rome IV and III criteria for IBS, as well as the reference standard, of whom 408 (86.6%) had IBS according to at least one of these definitions. The degree of overlap between the three is provided in figure 1. The level of agreement, as measured using the kappa statistics, between the Rome IV and III criteria as well as the reference standard are provided in table 2. Agreement between the Rome IV and the Rome III criteria was good (kappa=0.65); agreement between the Rome IV criteria and the reference standard was greater than that for Rome III.
{kind=link}
Overlap between Rome IV and III criteria and the reference standard among 408 patients with irritable bowel syndrome.
Characteristics of patients meeting the Rome IV or Rome III criteria for irritable bowel syndrome
Kappa statistic for levels of agreement between the Rome IV and III criteria and the reference standard diagnosis of irritable bowel syndrome after investigation
The proportion of patients undergoing each of the diagnostic tests, and the diagnostic yield is reported in table 3. The prevalence of organic findings after investigation in those who met the Rome IV or Rome III criteria for IBS is detailed in table 4. One case of coeliac disease and one case of ulcerative proctitis were diagnosed in the clinic, but neither of these patients met either the Rome IV or Rome III criteria for IBS. The most common organic diagnosis detected among patients meeting Rome IV or Rome III criteria was bile acid diarrhoea, followed by exocrine pancreatic insufficiency. There was only one case of small bowel Crohn’s disease detected in a 29-year-old patient meeting the Rome IV criteria, and one case of microscopic colitis diagnosed in a 37-year-old patient meeting both the Rome IV and III criteria. Although six patients meeting criteria for IBS with constipation were diagnosed with defaecatory disorders following anorectal physiology studies, in all cases, these were felt to be coexistent with a diagnosis of IBS. The initial diagnosis of IBS was not revised in any of these patients.
Investigations requested in patients with suspected IBS
Prevalence of organic disease in patients meeting the Rome IV or Rome III criteria for irritable bowel syndrome
Validation of the Rome IV criteria for IBS
Among the 572 patients providing complete Rome IV symptom data, 395 (69.1%) met the Rome IV criteria for IBS. The mean age of these 395 individuals was 35.3 years and 300 (75.9%) were women. Among the 455 patients with a diagnosis of IBS according to the reference standard, 375 met the Rome IV criteria for IBS, giving a sensitivity of 82.4% (table 5). Reasons for these 80 patients with IBS according to the reference standard not meeting the Rome IV criteria are provided in online supplemental table 2. Among 117 subjects who were not judged to have IBS according to the reference standard, 97 did not meet the Rome IV criteria, giving a specificity of 82.9%. The positive LR of the Rome IV criteria for the diagnosis of IBS was therefore 4.82 (95% CI 3.30 to 7.28), while the negative LR was 0.21 (95% CI 0.17 to 0.26). When performance of the Rome IV criteria was assessed according to subtype, they performed significantly better in predicting a diagnosis of IBS in patients with IBS with constipation (positive LR=25.7; 95% CI 5.07 to 145) and IBS with mixed bowel habits (positive LR=10.6; 95% CI 3.39 to 38.2). Including abnormal levels of anxiety or depression led to a large decrease in sensitivity to 60.8%, and only a small increase in specificity to 84.6%, giving a positive LR of 3.95 (95% CI 2.62 to 6.14) (table 6). When high levels of extraintestinal symptom reporting were incorporated, sensitivity fell further to 24.1%, but specificity increased to 95.7%, giving a positive LR of 5.64 (95% CI 2.47 to 13.3).
Sensitivity, specificity, positive and negative predictive values, and positive and negative likelihood ratios for the Rome IV and Rome III criteria for irritable bowel syndrome, and by subtype for Rome IV
Sensitivity, specificity, positive and negative predictive values, and positive and negative likelihood ratios for modifications to the Rome IV and Rome III criteria for irritable bowel syndrome incorporating mood and extraintestinal symptom reporting
Validation of the Rome III criteria for IBS
When we attempted to validate the Rome III criteria, there were 471 individuals providing complete symptom data. Of these, 355 (75.4%) met the Rome III criteria for IBS (mean age 35.9 years, 260 (73.2%) women). Among the 374 patients with a diagnosis of IBS according to the reference standard, 321 met the Rome III criteria for IBS, giving a sensitivity of 85.8% (table 5). Reasons for these 53 patients with IBS according to the reference standard not meeting the Rome III criteria are provided in online supplemental table 2. Among 97 subjects who were not judged to have IBS according to the reference standard, 63 did not meet the Rome III criteria, giving a specificity of 65.0%. The positive LR of the Rome III criteria for the diagnosis of IBS was therefore 2.45 (95% CI 1.90 to 3.27), while the negative LR was 0.22 (95% CI 0.16 to 0.29). Similar to the Rome IV criteria, incorporating abnormal levels of anxiety or depression or high levels of extraintestinal symptom reporting did not lead to any significant improvement in the performance of the Rome III criteria in diagnosing IBS (table 6).
Discussion
This study has validated the Rome IV criteria independently in secondary care and compared their performance with their predecessor, Rome III. We used an accepted reference standard, of symptoms compatible with IBS, as elicited by the clinical history, and no organic cause for the symptoms after a relatively standardised workup. Although the degree of agreement between the Rome IV and III criteria was good, the Rome IV criteria were more specific than Rome III, which was the aim of the Rome IV process. The specificity we observed in this study, conducted in routine practice, was 82.9%, which is substantially higher than the 65.0% seen with Rome III. Although sensitivity was lower with Rome IV at 82.4%, compared with 85.8% with Rome III, the positive LR was higher at 4.82, compared with 2.45 with Rome III. This means if a patient with suspected IBS meets the Rome IV criteria, they are almost five times more likely to have IBS than to not have IBS. The 95% CIs around these estimates for the positive LRs did not overlap, meaning that the Rome IV criteria performed significantly better than Rome III in diagnosing IBS. The Rome IV criteria were significantly more accurate, in terms of the positive LR, in patients with IBS with constipation or mixed bowel habits, compared with those with IBS with diarrhoea, because most of the false positives who were found to have organic disease were in the latter subgroup. We also examined the effect of incorporating abnormal levels of anxiety and/or depression or high levels of extraintestinal symptom reporting into both the Rome IV and III criteria. In both instances, positive LRs increased when high levels of extraintestinal symptom reporting were included, with a positive LR of 5.64 with Rome IV, compared with 3.34 with Rome III, but 95% CIs around these estimates overlapped with those for the Rome IV or III criteria alone.
Strengths of this study include the large sample size, with over 500 individuals referred to our clinic recruited and providing complete symptom data. We used a relatively standardised workup, with all patients screened for coeliac disease, a faecal calprotectin to exclude inflammatory bowel disease in those aged <40 years with diarrhoea, and a colonoscopy in those with diarrhoea or a recent change in bowel habit aged ≥40 years. We also performed SeHCAT scanning in those with diarrhoea, to exclude bile acid diarrhoea as a cause of symptoms. It is, to our knowledge, the first independent study to validate the Rome IV criteria and to compare their performance with their predecessor. In addition, the study was designed to adhere closely to the STARD guidelines for the reporting of studies of diagnostic accuracy,30 with consecutive patients recruited, assessors blinded and an accepted reference standard used. Finally, the fact that most patients we recruited were referrals to secondary care with suspected IBS means that the results are likely to be generalisable to clinicians consulting with individuals with IBS in usual clinical practice.
Weaknesses of the study include the fact that we did not mandate an exhaustive diagnostic workup to exclude organic disease in all individuals as part of the study design. However, other previous studies that have applied a routine panel of blood tests, such as a full blood count, C reactive protein and thyroid function tests or small bowel investigations, in patients with suspected IBS have demonstrated a yield for organic disease of ≤1%.31–34 In fact, the prevalence of abnormal thyroid function in patients with suspected IBS is not higher than that seen in the general population.35 Some investigators have reported a high prevalence of exocrine pancreatic insufficiency in patients with suspected IBS,36 although other studies have not confirmed this.37 We did not perform extensive testing to detect this, as current UK guidelines for the management of diarrhoea only recommend screening with faecal elastase in patients with suspected fat malabsorption.38 Faecal elastase has a sensitivity of between 73% and 100% and specificity of 80%–100% for a diagnosis of moderate to severe pancreatic insufficiency,39 40 so it is reasonable to assume that the three patients with an abnormal elastase had genuine exocrine pancreatic insufficiency. Furthermore, exhaustive investigation is not how management guidelines recommend a diagnosis of IBS should be reached,41–43 so our study reflects usual clinical practice in this respect. Our choice of reference standard could be criticised, but for a condition such as IBS, which lacks a biomarker or histopathological entity to confirm a diagnosis, this is inevitably an artificial construct to some degree. Others have used typical symptoms and a negative colonoscopy, so it could be argued that our reference standard is more rigorous, given we incorporated other tests in certain situations. In addition, we varied this according to the criteria under study to reflect the changes made in moving from Rome IV to Rome III. Finally, we did not perform longitudinal follow-up to ensure that an organic diagnosis was not missed in individuals who met the reference standard for IBS, although previous studies have suggested that a diagnosis of IBS is unlikely to be revised during extended follow-up, despite repeated investigation.44 45
Previous meta-analyses of symptom-based criteria for IBS have demonstrated only modest performance of prior gold standards such as the Manning, Rome I and Rome II criteria.14 46 Two previous validation studies of the Rome III criteria demonstrated positive LRs of 3.35 and 3.87,16 17 higher than was observed in this study. Reasons for this are speculative, although in these two earlier studies, the reference standard included a normal colonoscopy, but did not mandate screening for coeliac disease, and SeHCAT scanning was not performed in individuals with diarrhoea. It may be, therefore, that in these studies, some patients who met Rome III criteria, and who were felt to have IBS according to the reference standard, had a missed diagnosis of coeliac disease or bile acid diarrhoea. In terms of the Rome Foundation validation study of the Rome IV criteria,19 the sensitivity we observed was higher than the 63% they reported, but specificity was lower than the 97% they observed. It is important to point out that the Rome Foundation validation study was done in two separate cohorts, rather than in a single population in routine clinical practice. Nevertheless, our results confirm that the increase in the abdominal pain symptom frequency required to meet criteria for IBS, in moving from Rome III to Rome IV, does indeed increase the specificity of the Rome IV criteria over their predecessor. This led to a better performance than Rome III, in terms of a positive LR of 4.82. In a secondary or tertiary referral population in a University Hospital practice with a prevalence of IBS of 50% or more, a positive LR of this magnitude would be clinically useful for the diagnosis of IBS, identifying IBS with a post-test probability of 83%, compared with 71% with Rome III.
The Rome IV criteria performed significantly better in patients with IBS with constipation or mixed bowel habits, compared with those with IBS with diarrhoea. Although some patients with IBS with constipation were found to have defaecatory disorders after investigation in our study, in all cases, these patients were also felt to have coexistent IBS. However, as we did not conduct exhaustive testing for these disorders in all patients with IBS with constipation, this may explain the superior positive LR in this group of patients. Nevertheless, the poorer performance in patients with IBS with diarrhoea highlights the importance of considering alternative diagnoses, such as microscopic colitis,7 bile acid diarrhoea47 or exocrine pancreatic insufficiency36 in this group of patients, prior to making a diagnosis of IBS. Previous studies have demonstrated that microscopic colitis is more common in women ≥45 years. Other clues to a possible diagnosis of microscopic colitis, rather than IBS, include a shorter duration of symptoms, coexistent autoimmune disease, nocturnal diarrhoea and weight loss or prescription of a precipitating drug such as a non-steroidal anti-inflammatory or a proton pump inhibitor.9 48 Clues suggesting bile acid diarrhoea in IBS with diarrhoea include higher body mass index, higher faecal fat and, on specialised testing, faster colonic transit and increased small intestinal permeability.47 49 However, it is unclear whether bile acids entering the colon is part of the pathophysiology of IBS with diarrhoea,49 response to bile acid sequestrants is variable, and they may be poorly tolerated.50
In our previous validation study of the Rome I, II and III criteria,16 the degree of agreement between the criteria was good to very good in all instances. This is probably not unexpected, as the various criteria are derived from each other, meaning that the same strengths and weaknesses are, for the most part, passed on from one set of criteria to another. In that study, regardless of attempts to tighten the definition of IBS by refining the symptoms used to diagnose the condition, there was little to choose between the various sets of criteria in terms of their diagnostic performance. The current study suggests that the Rome IV criteria may be an advance on Rome III, in terms of their accuracy in diagnosing the condition. However, as this study was conducted in a secondary care cohort of patients with more severe symptoms, as evidence by high IBS-SSS scores and HADS scores, and the Rome IV criteria themselves select patients with more severe symptoms and higher levels of mood disorders,20 this is, perhaps, to be expected. Performance of the Rome IV criteria in this single centre study cannot, therefore, be extrapolated to primary care or office-based gastroenterology clinics.
IBS is a complex and heterogeneous condition, and many patients report psychological comorbidity,51–53 something that current diagnostic criteria fail to consider or incorporate. It may be that including psychological features, such as mood, or extra-intestinal symptom reporting, into future iterations of the Rome criteria will further improve their performance. This approach to diagnosis acknowledges the fact that IBS is a gut–brain disorder1 and is in keeping with the Rome Foundations proposed multidimensional clinical profile.54 This is a framework that, in addition to clinical symptoms, includes assessment of psychological factors, and impact of the illness, to build a unique clinical profile for each patient. In a previous validation study of the Rome III criteria, incorporating either abnormal levels of anxiety and/or depression or high levels of extraintestinal symptom reporting led to an increase in the positive LR.17 However, when we examined this approach in this study, although the positive LRs increased when high levels of extraintestinal symptom reporting were incorporated into either the Rome IV or III criteria, sensitivity fell considerably. In both instances, less than one-in-four patients with IBS would be diagnosed correctly with the condition. Reasons for the disparity in these findings are uncertain, but the prior study included unselected patients with lower GI symptoms undergoing colonoscopy, whereas this study was conducted in a population of patients referred with suspected IBS. Levels of abnormal anxiety and depression and extraintestinal symptom reporting among these patients were already high, which may explain why including these measures led to little improvement in performance.
In summary, this validation study of the Rome IV and III criteria simultaneously in a secondary care population of patients with suspected IBS in routine clinical practice has demonstrated that the Rome IV criteria performed significantly better in terms of confirming a diagnosis of IBS, mainly due to a higher specificity, although the clinical relevance of this is uncertain. The positive LR observed in this study is encouraging, and clinically useful, as in a patient population with a pretest probability of IBS of 50% the Rome IV criteria would identify IBS with a post-test probability of >80%. In the absence of an accurate and accepted biomarker for IBS and the failure of complex statistical techniques to facilitate a diagnosis of IBS,55 the Rome IV criteria should continue to be the gold-standard diagnostic approach to IBS, although further independent validation studies are required. Nevertheless, physicians consulting with patients with IBS with suspected diarrhoea should be aware that they are less accurate in this subgroup and therefore remain alert to the possibility of organic disease.
Data availability statement
No additional data available.
Footnotes
Twitter @DrCJBlack
Contributors CB, OC, DJG, and ACF conceived and drafted the study. ACF and CB collected all data. ACF analysed and interpreted the data. ACF drafted the manuscript. All authors have approved the final draft of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.