Article Text

Abstract
Objective Procedure-intense specialties, such as surgery or endoscopy, are a major contributor to the impact of the healthcare sector on the environment. We aimed to measure the amount of waste generated during endoscopic procedures and to understand the impact on waste of changing from reusable to single use endoscopes in the USA.
Design We conducted a 5-day audit (cross-sectional study) of all endoscopies performed at two US academic medical centres with low and a high endoscopy volume (2000 and 13 000 procedures annually, respectively). We calculated the average disposable waste (excluding waste from reprocessing) generated during one endoscopic procedure to estimate waste of all endoscopic procedures generated in the USA annually (18 million). We further estimated the impact of changing from reusable to single-use endoscopes taking reprocessing waste into account.
Results 278 endoscopies were performed for 243 patients. Each endoscopy generated 2.1 kg of disposable waste (46 L volume). 64% of waste was going to the landfill, 28% represented biohazard waste and 9% was recycled. The estimated total waste generated during all endoscopic procedures performed in the USA annually would weigh 38 000 metric tons (equivalent of 25 000 passenger cars) and cover 117 soccer fields to 1 m depth. If all endoscopic procedures were performed with single-use endoscopes and accounting for reprocessing, the net waste mass would increase by 40%. Excluding waste from ancillary supplies, net waste generated from reprocessing and endoscope disposal would quadruple with only using single-use endoscopes.
Conclusion This quantitative assessment of the environmental impact of endoscopic procedures highlights that a large amount of waste is generated from disposable instruments. Transitioning to single-use endoscopes may reduce reprocessing waste but would increase net waste.
- environmental health
- endoscopy
- endoscopic procedures
Data availability statement
Data are available on reasonable request. All data are under the auspices of Heiko Pohl (heiko.pohl@dartmouth.edu) and will be furnished upon reasonable request.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
The healthcare sector contributes 8% to the total amount of greenhouse gas emissions in the USA.
The environmental impact of endoscopic procedures is unknown.
What are the new findings?
An endoscopic procedure generates approximately 2 kg of disposable waste from periprocedural single use disposable materials and supplies (excluding reprocessing waste).
Replacing reusable with single-use endoscopes and accounting for reduced waste from reprocessing of endoscopes would increase total waste mass by 40%.
How might it impact on clinical practice in the foreseeable future?
We need to better quantify the environmental impact of performing endoscopies and identify ways to minimise this impact.
Any cost-benefit analyses of endoscopy should also consider potential environmental harms.
Introduction
The healthcare sector is responsible for 4.4% of total greenhouse gas (GHG) emissions worldwide and for 8% in the USA, thereby contributing to climate change and global warming.1–4 Although the very goal of healthcare is to treat disease and prevent death, the way we provide healthcare may harm long-term human health through this environmental impact.5–8
Procedure-intense specialties, such as surgery or endoscopy, require a large number of instruments and supplies and therefore have a considerable impact on the environment, primarily through the production, transport and energy consumption of these materials.9 10 Eighteen million endoscopies are performed in the USA each year, and the majority of the supplies used in these procedures are single use and disposable.9 The increased utilisation of disposable supplies in endoscopic procedures is related to efficiency, profitability, costs of reprocessing reusable supplies and the concern for patient to patient transmission of infection.11–14 Because of concerns about infection transmission, the FDA has recently approved single-use endoscopes.15–19
Although endoscopists have anecdotally suggested that large amounts of waste are generated during an endoscopy, procedural waste has not been formally quantified, and the environmental footprint of endoscopic procedures is unclear. With this study, we sought to quantify waste associated with endoscopic procedures at a low-volume and high-volume hospital.
Methods
We performed an audit of waste generated during endoscopic procedures at a low and high endoscopy volume academic medical centre over a 5 work-day period in January and February 2020 (VA White River Junction, Vermont, USA; Dartmouth Hitchcock Medical Center, New Hampshire, USA). At the end of each day, endoscopic waste in the preprocedure and postprocedure areas and in the endoscopy examination rooms was documented as mass and volume. At the high-volume hospital, we also obtained waste from endoscope reprocessing. We did not assess waste in the patient waiting area or staff break rooms.
Volume was measured as the number of 20-gallon (76 L) waste bins filled with waste. If bins were of different sizes, the dimensions of such containers were measured, and the volume converted to represent a 20-gallon (76 L) bin. In addition, we expressed the volume in m3. To provide context, we further calculated the waste volume as the number of soccer fields (7140 m²) and football fields (5351 m²) that could be covered with waste at a 1 m depth. We measured the mass of waste of trash bags in gram and converted it to kg and metric tons (1.1 US ton) for presentation. For context, we expressed mass as the equivalent mass of the number of single passenger cars (1532 kg). To facilitate presentation, results were rounded (m3 to the nearest 1000, and tons and number of cars to the nearest 100).
We calculated total waste and further categorised it as regular trash destined for the landfill, biohazard waste (representing here all medically regulated waste) and recyclable waste if collected. We did not account for instruments that were collected as sharp objects in separate containers. We further documented the number and type of procedures performed during the audit and in the previous calendar year at each hospital. The type and weight of disposable and non-biohazard material were documented at the low-volume hospital and was used to estimate the proportion of potentially recyclable material. We considered all paper, cardboard, metal and most types of plastic (resin identification code 1–5) as recyclable.20
The main outcome of interest was the average amount of waste of using disposable materials and supplies generated per endoscopic procedure at each hospital and combined. The relative increase in waste from reprocessing of endoscopes that was obtained from one hospital was used to estimate the average proportion of waste from reprocessing for any endoscopic procedure at either hospital.
We then applied the mean waste generated per endoscopy at both hospitals as the representative waste to calculate the waste generated from endoscopic procedures in the USA each year. We used the most recent data on endoscopies that were performed in the USA in 2013. In that year, 18 million endoscopic procedures were performed in the USA; of these, 11 million were colonoscopies, 6 million upper endoscopies and at least 170 000 endoscopic retrograde cholangiopancreatography (ERCPs).9
We further estimated the contribution of waste from single-use disposable endoscopes, assuming first that no single-use endoscopes were used, second that all colonoscopies and ERCPs were performed with single-use endoscopes (as currently approved by the FDA) and third that all endoscopies were performed with single-use endoscopes. For this analysis, we computed the net waste that included waste related to reprocessing and waste related to disposing endoscopes. Currently available single-use duodenoscopes have the same dimension as reusable endoscopes. Volume was estimated by packing three endoscopes into the smallest box possible (14×14×12 cm). For the analysis, we applied the mean mass of both available duodenoscopes including packaging material (1.26 kg). Considering minimal variation in mass between reusable endoscopes, we applied the same mass to all types of endoscopes. We finally considered that the main difference between reusable and single-use endoscopes is related to reprocessing and calculated the waste from reprocessing and from endoscope disposal that excluded all ancillary supplies during the lifetime of a reusable endoscope. We assumed that use of ancillary supplies would be similar in a reusable and a single use endoscope practice. We considered that a reusable endoscope can be reused at least 2000 times. This estimate was based on the average use of Olympus (190 series) endoscopes during a 4-year leasing period (n=1500) at the high-volume hospital and the company’s practice of reselling these after the lease as used endoscopes (assumed at least 500 additional uses).
We assessed waste volume at a third medium size hospital; however, mass was not assessed, and therefore total waste could not be reliably estimated. We include volume estimates of waste at that hospital in the supplementary analysis for comparison.
Results
Endoscopic procedure waste at two medical
During the 5-day audit, 278 endoscopies were performed for 243 patients combined between the low and high endoscopy volume hospitals (table 1). Total waste produced (including packaging material and personal protective equipment (PPE)) during these procedures filled 190 20-gallon (75 L) waste bins and weighed 619 kg. Approximately two thirds of the waste was destined for the landfill. Biohazard waste filled 17% of waste bins and represented 28% of the waste mass. At the high-volume hospital, 29% of waste volume (16% of waste mass) was recycled; the low volume hospital did not recycle any waste. Waste related to endoscope reprocessing was assessed only at the high-volume hospital, where it increased waste volume by 11% and mass by 14%.
Hospital endoscopic procedure volume and waste generated during 5-day audit
On average, each endoscopy produced 2.1 kg of waste mass, filling 0.6 waste bins (0.046 m3 or 46 L), and 2.4 kg when including waste from reprocessing (0.7 waste bins (0.051 m3 or 51 L)). Waste varied between the hospitals in volume (relative difference (RD) 1.37) more than in mass (RD 1.15). Despite recycling efforts at the high-volume hospital, landfill waste was similar between both hospitals (RD 1.03 for mass). The high-volume hospital produced less biohazard waste than the low volume centre (RD 0.85 for mass).
Data from the third and medium sized hospital (5000 endoscopic procedures per year) that were limited to landfill waste were very similar to the waste generated at the medium and high-volume facilities (online supplemental table 1).
Supplemental material
Material composition of waste
Supplies that were made of plastic represented the majority (54%) of disposable non-biohazard waste (figure 1). Forty per cent of supplies were composed of more than one material, of which 23% contained plastic (eg, blood pressure cuff) and 15% contained metal (eg, cautery connecting wires). A small proportion (5%) were made of either metal, fabric (eg, cotton) or paper/cardboard. PPE represented 8% of all disposable material. 48% of non-biohazard or 35% of all disposed wastewas potentially recyclable.
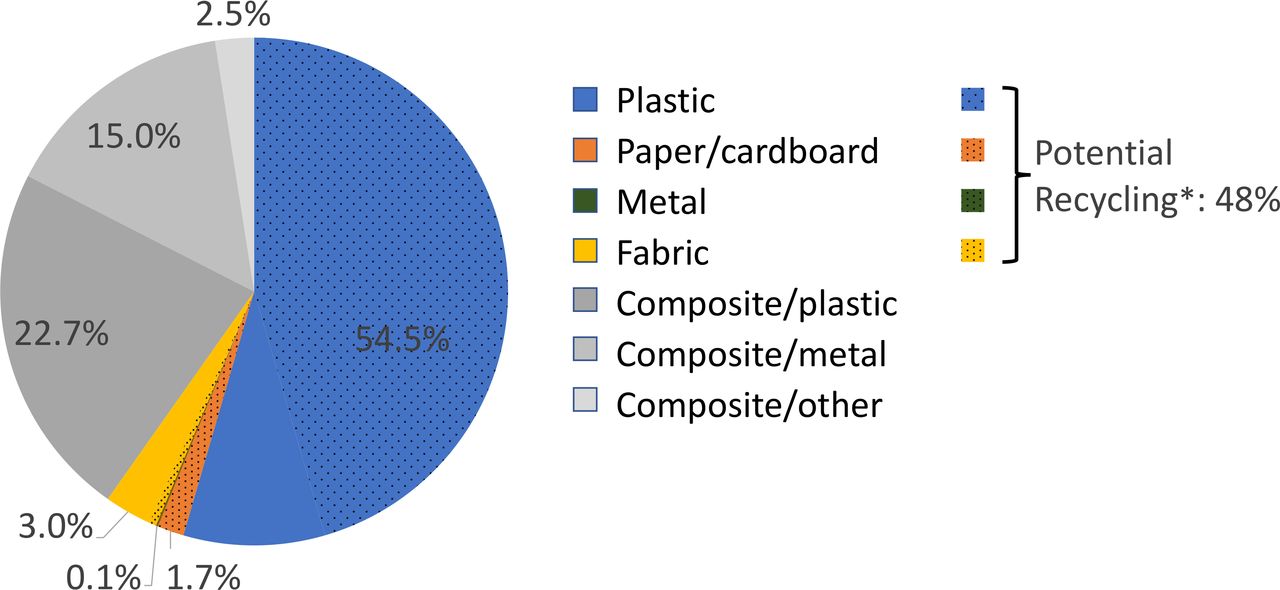
Material components of non-biohazard waste of disposable supplies used for endoscopic procedures and potential for recycling (data based on waste audit at the low volume hospital, see Methods section). *Potentially recyclable plastic included: PET, HDPE, PVC, LDPE, PP (Resin identification code 1–5). HDPE, high-density polyethylene, LDPE, low-density polyethylene; PET, polyethylene terephthalate; PVC, polyvinyl chloride; PP, polypropylene.
Endoscopic procedure waste in the USA
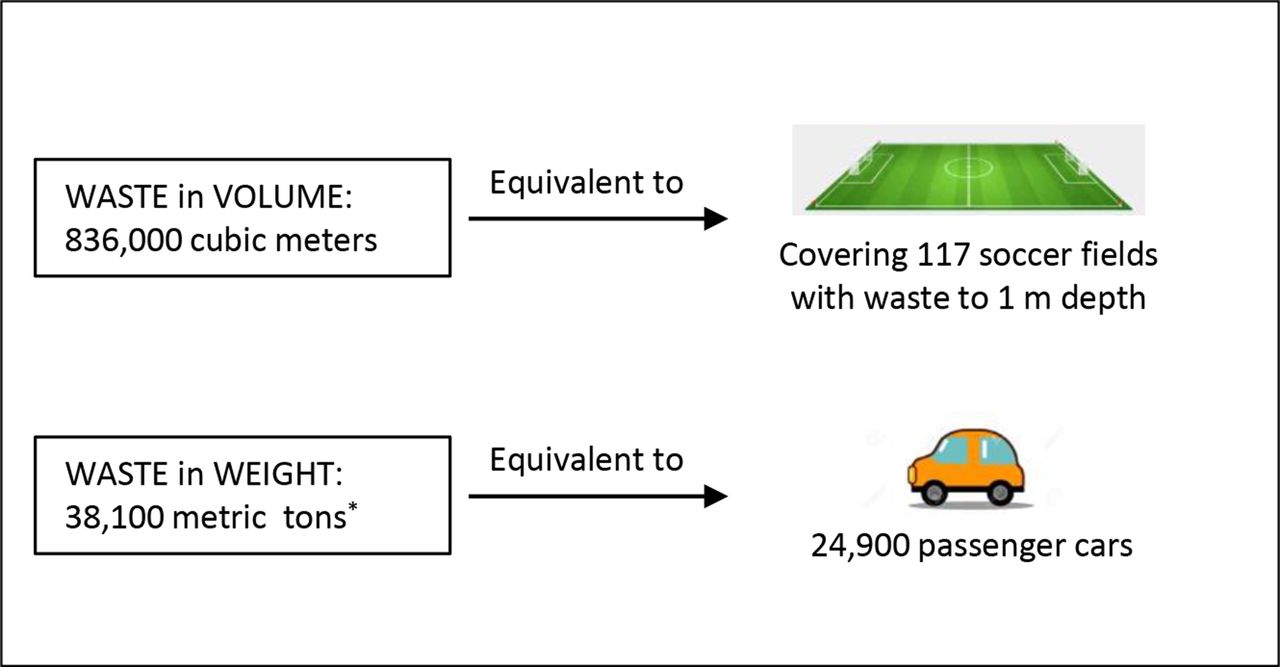
When applying the average waste estimates from the low-volume and high-volume centres to all endoscopic procedures performed in the USA annually, the total waste produced from disposable single-use supplies would fill more than 11 million waste bins (836 000 m3) and weigh 38 100 metric tons (42 000 US tons).9 This amount of waste would be the equivalent of covering approximately 117 soccer fields (156 football fields) with waste to a height of 1 m, or equivalent to the mass of 24 900 passenger cars (figure 2). When also considering reprocessing of endoscopes, the total waste volume would increase to 927 000 m3 covering 130 soccer (173 football fields), and the waste mass would increase to 43 500 metric tons (48 000 US tons) weighing as much as 28 400 passenger cars.

Estimates of annual disposable waste in the USA from endoscopic procedures (18 million, including 11 million colonoscopies, 6.8 million upper endoscopies and 170 000 ERCPs), not including waste from reprocessing of endoscopes. *42 000 US tons.
Waste estimates when using single-use endoscopes
If colonoscopies and ERCPs were performed with currently FDA-approved single-use instead of reusable endoscopes, waste mass related to reprocessing endoscopes would decrease by 62% but the net waste mass per endoscopic procedure would increase by 25% (figure 3, middle bar). If all endoscopies were performed by single-use endoscopes, the total net waste mass from all performed procedures would increase by 40%, even after accounting for the lack of waste from reprocessing (figure 3, right bar).

Annual waste produced during endoscopic procedures in the US overall and by proportion of procedures performed with reusable or single-use endoscopes. Percentages represent the absolute increase in waste from using disposable endoscopes.
The overall waste from only reprocessing of a reusable endoscope during its lifetime (minimum of 2000 procedures) would amount to 610 kg. In contrast, single-use endoscopes would generate 2520 kg of waste to accomplish the same number of procedures. This difference represents a 4.1-fold increase in waste, or a net plus of 1.0 kg per single-use endoscope, when only considering waste from reprocessing and endoscope disposal.
Discussion
This study quantified volume and mass of waste generated during endoscopic procedures at a low and high endoscopy volume hospital. We found that single-use disposable endoscopic supplies generate approximately 2 kg of waste per procedure. When applied to the annual endoscopy volume in the USA of 18 million procedures, total endoscopic waste would be equivalent to 25 000 passenger cars and cover approximately 120 soccer fields (160 football fields) to 1 m depth.9 The proportion of waste that was actually recycled was low (10%); however, close to 50% of non-biohazard supplies were potentially recyclable. When assuming that all endoscopic procedures were performed with single-use endoscopes, waste from reprocessing would decrease; however, overall disposable waste would increase by 40%. The waste generated from reprocessing and endoscope disposal alone would quadruple when changing to a single-use endoscope practice.
This is the first study to formally examine the environmental impact of endoscopic procedures. Prior studies in the surgical field have examined waste from disposable material. For instance, laparoscopic hysterectomies generate approximately 12 kg and cataract surgery 3 kg of waste per procedure.21 22 For comparison, the average American generates 2 kg of waste every day.23
Our study is not the first to examine endoscopy waste. A prior commentary reported that each endoscopy generates 1.5 kg of waste; however, this assessment did not include all components related to performing an endoscopy; for instance, preprocedure and postprocedure patient care was not considered in that study.24 In contrast, our 5-day audit attempted to comprehensively capture all preprocedure, intraprocedure and postprocedure aspects. Furthermore, the number and type of procedures performed during the audit were representative of procedures performed in the previous year. We were also surprised to see how similar the amount of generated waste was between the participating hospitals. For these reasons, we believe that the results may represent a good estimate of waste generated during endoscopic procedures in general.
However, we also noted differences. The high-volume hospital generated slightly more non-biohazard waste. This may be in part related to variation in practices. For instance, the high-volume hospital used disposable gowns while the low-volume hospital used reusable gowns. Furthermore, we performed this waste audit before the COVID-19 outbreak. We calculated that 8% of waste was related to PPE use. We can expect that PPE use has increased the overall amount of waste during the pandemic.12 25
The final destination of disposable supplies was not always evident. For instance, biohazard waste may be incinerated or sent to a landfill after being processed. We found a large discrepancy between potentially recyclable material (approximately 35% of all disposed waste) and waste that was actually recycled (10%). This observation highlights potential for improvement, in particular when considering that recycling of surgical waste may have a net positive impact on GHG emissions.26 27 Adequate recycling requires a recycling partner, who will assist and guide in sorting material, dismantle composite supplies and start the appropriate recycling process. It must be noted that there are limitations to recycling. Recycled material may not always be reused. It has been estimated that up to 91% of recyclable plastic is not recycled; 79% ends up in a landfill and 12% is incinerated.8
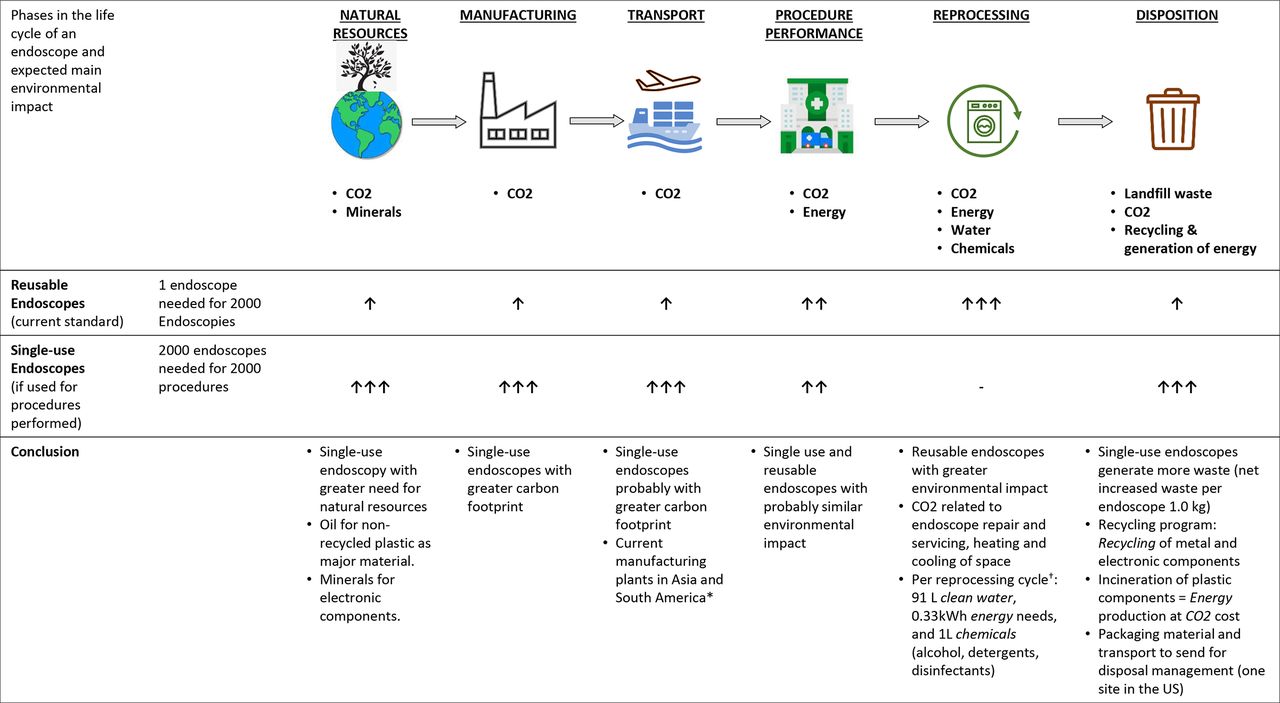
Our findings must be viewed within the entire context of potential environmental impact of each material—from its production to its final disposition (figure 4). Interestingly, waste contributes a very small proportion to GHG emissions and carbon footprint. For instance, waste treatment is responsible for only 3% of GHG emissions within the healthcare sector. In fact, hospitals’ usage of electricity, gas, heating and cooling has been demonstrated to be the single largest contributor to the healthcare sector-related GHG emissions, accounting for up to 40% of total emissions.2 28 We did not consider the environmental impact of these ancillary services, which suggests that the true environmental impact of endoscopy is far greater than the impact of procedural waste alone. A full life cycle assessment would account for the environmental impact of such ancillary services.29

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Life cycle of an endoscope from manufacturing to disposal. Up-arrows indicate a possible harmful impact on the environment. *Boston Scientific and Ambu. †Data obtained from Olympus endoscope washing machines. One cycle cleans two gastroscopes or colonoscopes and one duodenoscope.
Our findings are of particular relevance to the recent introduction of single-use endoscopes. Such practice would eliminate the risk of patient to patient transmission of infection.17 For any endoscopic procedure, this risk has been estimated to be 1 in 1.8 million; however, reported outbreaks related to performing ERCPs would suggest a far greater risk (at least 1:10 000).18 19 A recent study reported 490 infections and 32 deaths since 2008 related to duodenoscope contamination, which translates into an overall risk of death of approximately 1 in 150 000 ERCPs.19 This rate is far lower than the all-cause mortality after an ERCP of 1:500.30 31 While endoscopists strive to provide safe endoscopic procedures, these considerations highlight the challenge of finding the balance between the magnitude of the problem (overall rare risk of death from infection), the way we may change our practice (eg, use of single-use endoscopes) and the unintended consequences of such change (resources, environmental impact).
Using single-use endoscopes would impact the environment in two main ways. First, it will generate a large amount of waste beyond the reduction in reprocessing waste (figure 4). In the USA, single-use endoscope companies have partnered with a medical waste company (SHARPS). The company will dismantle endoscopes, recycle electronic and metal components and incinerate plastic (which is the major endoscope component) for energy production. While plastic incineration has been termed a renewable energy (online supplemental figure 1), it generates more GHGs (plastic is a product of fossil fuels) than coal plants and produces toxic byproducts and fine particles, which have been associated with respiratory diseases.2 32–34 Thus, medical waste incineration cannot be considered an environmentally sustainable practice. Unfortunately, details related to recycling and incineration practice related to single-use endoscopes to better understand the environmental impact were not available from the company. In addition to waste, the major impact on the environment can be expected from the manufacturing of single-use endoscopes (figure 4). For each reusable endoscope, approximately 2000 single-use endoscopes need to be produced to perform the same number of procedures. Unless single-use endoscopes are returned, refurbished or remanufactured as part of a circular economy, single-use endoscopes within the current linear economy will continue to be produced, which in turn will result in ever increasing amount of at best recyclable waste.25 35 Such practice is of particular concern when considering that resources are limited and that the anthropogenic mass—all human-made mass—has recently surpassed all living biomass.36
It is important to note that the current multiple-use endoscope practice also impacts the environment, primarily related to endoscope reprocessing. Reprocessing requires energy, a large amount of clean water and chemicals, and it generates potentially toxic waste.14 37 Reprocessing requires extra space (energy needs, heating and cooling requirements), washing machines (energy) and extra personnel. In addition, reusable endoscopes need servicing and repair, which requires transportation and new materials. While it appears that a reusable practice is more environmentally sustainable, the discussed components of the life cycle of an endoscope (figure 4) provide a roadmap to performing a more in-depth analysis and what aspects need to be examined to fully understand the effect of reusable and single-use endoscope practice on the environment.
This study has several important limitations. Our waste estimates may not represent all endoscopy units, although a limited assessment suggested that a similar volume of landfill waste was generated at a third medium endoscopy volume hospital (online supplemental table 1). Used supplies may differ; however, supply companies provide endoscopy supplies globally, and there is probably little variation. Therefore, we believe that our waste estimates may well represent endoscopy practice outside the USA. Disposition of waste, including incineration and recycling practice, may vary and further study may help in understanding differences and ways to minimising waste. While measuring mass and volume is a first step towards quantifying the environmental impact of endoscopy, these measures are rather imprecise. Other outcomes are used to express types of environmental impact and include carbon foot print as a representative for GHG (impact on climate), energy use (impact on fossil fuel depletion) or water consumption (impact on fresh water depletion).3 Such measures should be a part of future studies. Finally, cost has not been considered. While cost is an important aspect for local and national healthcare, climate change and its associated effects on health are global and can hardly be captured by cost.
Perhaps the most important value of our study is that it brings awareness to the fact that performing endoscopic procedures comes at some cost to the environment. All who contribute may re-examine their involvement and consider changing their practice. (1) Industry needs to engage and provide information on the carbon footprint equivalents of their products (in service of the goal of reducing carbon footprint), (2) professional societies need to set the framework for and promote an environmentally sustainable practice, (3) administrators may consider the environmental impact when selecting products, (4) endoscopy practice managers may help to establish a more sustainable practice (eg, minimise waste, institute recycling, energy conservation) and finally (5) physicians may scrutinise procedure indications to reduce unnecessary endoscopies. For instance, studies suggest considerable overutilisation of upper and lower endoscopies. Approximately 40% of upper endoscopies may be repeated unnecessarily, and a similar proportion of patients have a repeat colonoscopy too early.38–41 Furthermore, re-examining screening approaches with less invasive tests as the primary choice (eg, faecal immunochemical testing instead of colonoscopy for colorectal cancer screening) may be viewed as more environmentally sustainable. These considerations should be more formally included in any harms-benefit analyses.
In conclusion, our quantitative assessment shows that endoscopic procedures generate a large amount of waste from disposable instruments. Transitioning to single-use endoscopes would eliminate reprocessing waste but greatly increase net waste. Future studies should employ life cycle assessment to better quantify the environmental impact of performing an endoscopic procedure with reusable or single-use instruments. Such analyses will help understand and acknowledge environmental consequences of our practice and identify ways to minimise its impact.
Data availability statement
Data are available on reasonable request. All data are under the auspices of Heiko Pohl (heiko.pohl@dartmouth.edu) and will be furnished upon reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors HP and DvR: planned and designed the study. SN, JD, LB, JB, AA-F and HP: data collection. HP, SN and DvR: data analysis. SN and HP: drafted the manuscript. All authors contributed to editing and finalising the manuscript. HP: guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs or the US government.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.