Article Text

Abstract
Background The York faecal calprotectin care pathway (YFCCP) was developed to optimise effective primary care differentiation between irritable bowel syndrome (IBS) and inflammatory bowel disease (IBD). We undertook an audit of colonoscopy activity at York Teaching Hospitals after the introduction of the YFCCP, to assess its impact.
Methods Faecal calprotectin (FC) results were reconciled with colonoscopy activity in patients 18–60 years after the implementation of the YFCCP. This permitted individual patient tracking of their FC values, the timing of those requests by primary care, the date of subsequent referral and investigation and the end clinical diagnoses.
Results Primary care uptake of FC increased fourfold with the introduction of the YFCCP. Following implementation, FC-related referrals for colonoscopy fell from 24% to 13%. The number of patients needed to colonoscope to diagnose organic colonic disease (IBD, significant adenomatous polyps or colorectal cancer) fell from 6.8 to 3.8 when the YFCCP was applied. This represents a cost saving of £41 015 per thousand patients tested in primary care. We estimate that outpatient time to diagnosis fell from a median of 41 to 29 days.
Conclusion This audit of FC activity and colonoscopy outcomes provides substantial supportive evidence for the effectiveness of the YFCCP. Popular in primary care, it has led to a reduction in referrals. The diagnostic accuracy determined in this audit is in line with earlier evaluations. Accepting the weaknesses of audit we conclude that this evaluation likely underestimates the benefits of the YFCCP in terms of resource use saving and time to diagnosis.
- inflammatory bowel disease
- diagnostic and therapeutic endoscopy
- primary care
- stool markers
Statistics from Altmetric.com
Significance of this study
What is already known on this topic
The York faecal calprotectin care pathway (YFCCP) was introduced, in support of National Institute of Clinical and Care Excellence DG11, with the aim of optimising the clinical and cost-effectiveness of faecal calprotectin (FC) use in primary care.
What this study adds
This audit of FC activity and colonoscopy outcomes provides substantial supportive evidence of the effectiveness of the YFCCP.
How might it impact on clinical practice in the foreseeable future
The YFCCP, implemented more widely, could safely offer significant healthcare savings.
Introduction
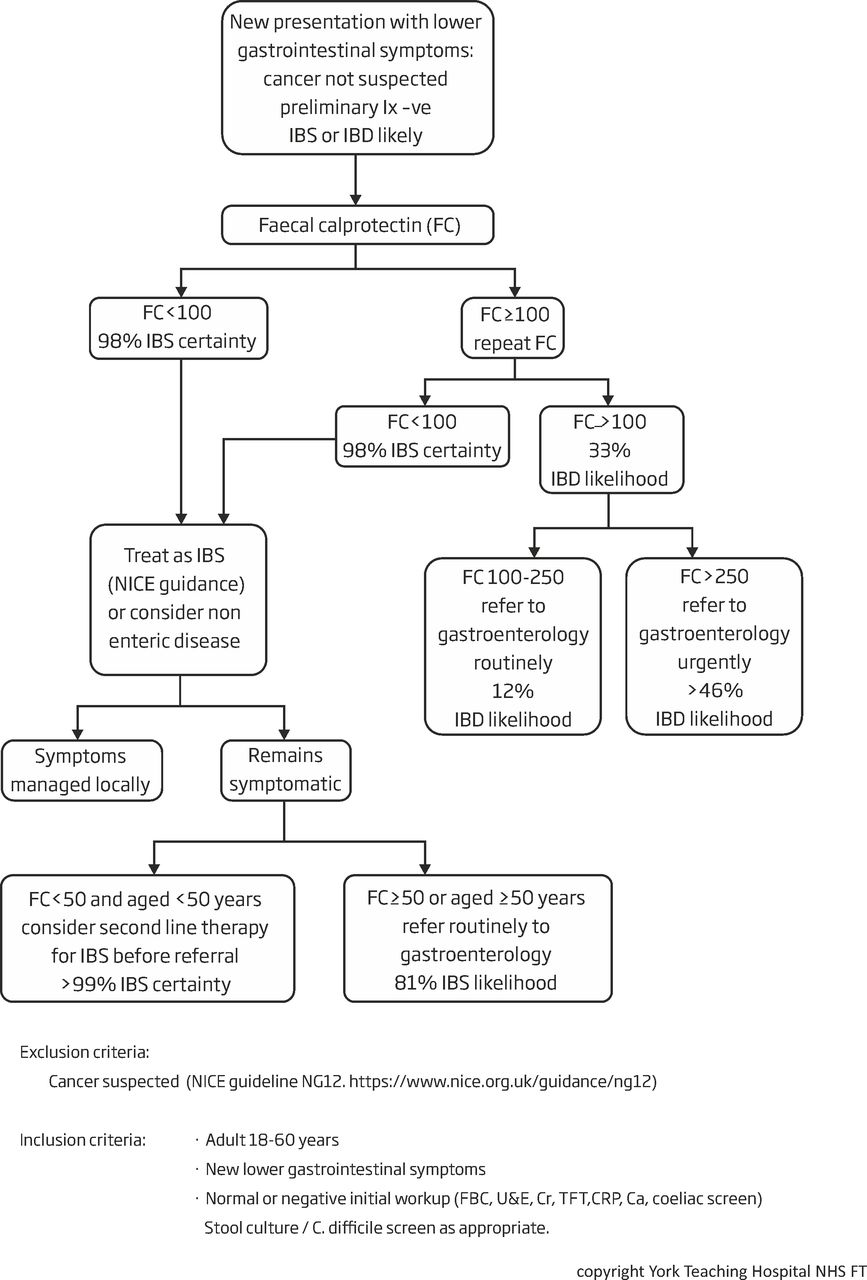
The York faecal calprotectin care pathway (YFCCP) was introduced across the region from 2016 onwards (figure 1).1 Formatted for the patient management systems, EMIS and SystmOne, it is now embedded into all primary care practices that feed into York Teaching Hospitals NHS Foundation Trust. It supports the guidance issued by the National Institute of Clinical and Care Excellence (NICE) for the use of faecal calprotectin (FC), in primary care, to distinguish those patients with the irritable bowel syndrome (IBS) from those with inflammatory bowel disease (IBD), where colorectal cancer (CRC) is not suspected.2 An evaluation of the YFCCP conducted by York Health Economics Consortium has been favourable. However that evaluation used published, historic data against which to benchmark diagnostic accuracy.3
{kind=link}
Flowchart of the YFCCP. IBD,inflammatory bowel disease; IBS, irritable bowel syndrome; NICE, National Institute of Clinical and Care Excellence; YFCCP, York faecal calprotectin care pathway.
Aims
To audit colonoscopy activity at York Teaching Hospitals NHS Foundation Trust to assess the impact of the YFCCP.
Methods
A record of all first colonoscopies (and flexible sigmoidoscopies) performed by York Teaching Hospital NHS Foundation Trust in patients 18–60 years during the period 2016–2018 was obtained. All patients with a clinical diagnosis of IBD, CRC or adenomatous polyps were included and those with quiescent IBD and non-significant polyps were excluded. Significant adenomatous polyps were defined as those polyps ≥10 mm, those with high-grade dysplasia and those patients with ≥5 polyps. These diagnoses combined are referred to as organic colonic disease (OCD). Diverticular disease data were excluded because disease severity could not be readily distinguished.
FC results were reconciled with colonoscopic activity to permit individual patient tracking of their FC values and the timing of the requests by primary care, the date of subsequent referral, the date of investigation (61% had a colonoscopy and 39% a flexible sigmoidoscopy) and the end clinical diagnoses. Requests as part of the ongoing care of patients with an established diagnosis of IBD were not included in the dataset and those patients who had a repeat FC as part of the YFCCP design were identified so as to avoid double counting. Faecal immunochemical testing for haemoglobin was not available during this time.
Of note, patient symptomatology and indications for referral could not be accessed and so certain assumptions about referral behaviour had to be based on the prevalence of disease at subsequent diagnosis. This is addressed in the Results section.
Data analysis after dataset collation was completely anonymised. Descriptive statistics were used to determine the performance of the YFCCP in terms of
Use of the YFCCP to inform referral for colonoscopy.
Whether or not there was a reduction in the number of patients without OCD being referred.
An estimate of any cost savings
Whether or not there was a more rapid identification of patients with IBD.4
Results
Use of the YFCCP by primary care increased significantly from 1037 patient tests in 2016 to 3126 in 2017 and 4279 in 2018. During this time, in line with projections, the rate of colonoscopy referrals fell from 24% to 13%. Compliance with the YFCCP was 91% for patients with an initial FC 100–250 µg/g faeces and 44% when >250 µg/g. The YFCCP sensitivity in the referred population was 90.6% (CI 86 to 94) and specificity 57.6% (54 to 61) giving a negative predictive value (NPV) of 94.9% (93 to 97) and a positive predictive value (PPV) of 41.1% (37 to 45). These findings are similar to those of the original pilot. Risks of OCD were 1% for those with continuing symptoms aged <50 years and with a FC <50 µg/g faeces and rose to 49% for those with a repeat FC >250 µg/g faeces.1
Between 2016 and 2018 the YFCCP was increasingly used by primary care to inform referral decision making (table 1). However, many patients continued to be referred without first entering the YFCCP and, because the indications for referral are not known, it is uncertain whether this was or was not appropriate. During the period of the evaluation, there were in existence three patient referral pathways into endoscopy. York Hospital endoscopy unit had separate medical and surgical pathways while the Scarborough service was pooled. The York surgical service accepted all patients referred for suspected CRC.5 Significant differences in FC requesting are seen dependent both on age and endoscopy pathway. This likely reflects differences in patient symptomatology and the clinical suspicion of disease at referral, particularly for CRC.
Percentage of patients based on age and investigative unit/pathway that had an FC request prior to referral for endoscopy (2016 and 2018)
Recognising that patient symptomatology could not be used to compare those patients who did and did not enter the YFCCP, the prevalence of endoscopic clinical diagnosis was instead determined to ensure a ‘like for like’ comparator patient population to act as the control limb. These data are summarised in table 2. We postulated that a similar disease prevalence would infer a similar clinical presentation. Across all ages and colonoscopy referral pathways, the most common OCD diagnosis was IBD. There was a low prevalence of polyps and CRC in all patients aged 18–49 years. Only in patients >50 years in the York surgical cohort did the prevalence of CRC exceed the 3% NICE NG12 target. We therefore pooled data in the York surgical cohort aged 18–49 years with all York medical and Scarborough data to generate a non-YFCCP control group as a comparator.
Prevalence of OCD: IBD, significant polyps and CRC by age and endoscopy unit referral
The age related and total numbers of OCD diagnoses were determined with reference to the total number of patients investigated to give a ‘diagnostic yield’. This was split according to whether the patient had or had not entered the YFCCP. This permitted the ‘number needed to test’ (NNT) for one diagnosis of OCD to be determined for both the YFCCP (3.8) and non-YFCCP (6.8) groups. These data are summarised in table 3.
‘Diagnostic yield’ dependent on age and the YFCCP giving a ‘number needed to test’ (NNT) for a positive diagnosis of OCD
During 2016–2018, 1038 patients were colonoscoped within the YFCCP while ~7304 patients were FC tested in primary care (accepting that some of the total 8442 FC requests represent repeat testing in the same patient). From this the OCD prevalence in primary care was estimated to be 3.8% and from this a cost saving was calculated. Within the YFCCP group, three procedures (two colonoscopies and one flexible sigmoidoscopy) were saved for every 3.8 patients investigated, compared with the non-YFCCP group, amounting to £1793.6 Since for every 1000 patients FC tested within primary care 144 were referred ((prevalence of OCD in primary care/prevalence of OCD in secondary care) × 1000), this is a saving of £67 945 (144/3.8×1793). The additional cost of FC testing for every 1000 patients entering the YFCCP is £26 930 (£23.30 per test).2 We estimate therefore endoscopic savings of £41 015 per thousand patients entered into the YFCCP in primary care.
For those patients within the YFCCP group, the median time from the first FC test result >100 µg/g faeces to clinical diagnosis was 29 days (IQR: 15–47). Referral times were not recorded in the non-YFCCP group, however, in a random selected sample, the median time from initial referral to clinical diagnosis was 41 days (19-72).
Discussion
The purpose of this audit has been to use readily available indicative datasets of colonoscopic activity to evaluate the impact of the roll out of the YFCCP on healthcare resource usage and early diagnosis. We had developed, piloted, implemented and evaluated the YFCCP in support of NICE DG11 guidance.
The advantage of service evaluation when introducing a clinical pathway such as the YFCCP, in support of NICE guidance, is that the process can be rapid. Since 2016 the YFCCP has been introduced across the Yorkshire and Humber region and beyond. However, it is often the case that service evaluation does not readily support detailed data collection. As a result, robust assessment of effectiveness of the pathway may prove challenging. This is particularly the case with the YFCCP which is used within primary care while the endoscopy and many clinical diagnoses are recorded within secondary care. Ideally, clinical outcome data would be identified in patients attending primary care with symptoms fulfilling the criteria for NICE DG11. However, we did not have access to primary care records and currently primary care and secondary care datasets are not reconciled. Therefore, we have looked for local indicative datasets to inform a pragmatic evaluation of the YFCCP.
The endoscopy dataset was the closest we could achieve to our target cohort of symptomatic patients, newly referred from primary care without a prior diagnosis. The choice of the control limb was based on the prevalence of disease, and particularly a low prevalence of CRC, since the YFCCP is not to be used in the context of suspected cancer. Patient symptomatology was not, however, recorded in the dataset and we accept that for many primary care physicians the question will not have been as straightforward as IBS versus IBD. The control limb will additionally have contained patients admitted acutely as emergencies and those previously diagnosed with IBD who had come from other parts of the country, the paediatric service or who had been diagnosed radiologically. Patients diagnosed with IBD locally before the introduction of the endoscopy reporting system in 2008 will also have degraded the data and it is possible that patients who had both a flexible sigmoidoscopy and colonoscopy were double counted. All of these factors would favour the control limb over the YFCCP in any comparative analysis since they increase the seeming prevalence of IBD in the non-YFCCP control cohort. On the basis of our previous evaluation, we also judge that ~10% of IBD patients will have isolated small bowel disease and so would have been missed by this endoscopy-based audit. These patients would be expected to improve the diagnostic accuracy of the YFCCP.
Accepting these limitations, for every age group the use of FC within the YFCCP reduced the total number of endoscopic procedures required to achieve a diagnosis of OCD. We estimate a saving of £41 000 per thousand patients tested by primary care. In an earlier analysis of historic comparators, some of which used FC and others the C reactive protein, we found the YFCCP resulted in an saving ranging from £152 043 and -£25 825 per thousand patients tested.1 Importantly, this saving frees up secondary care endoscopy resource that can be directed at patients with suspected CRC.
It is difficult to draw robust comparative conclusions about the effect of the YFCCP on the time to diagnosis. The time of the initial consult with the GP was not recorded and so instead the time of the first FC test is used. It was at this point that the decision to refer would have been made. The purpose of the YFCCP is to allow those at high risk of IBD to be referred urgently (usually as ‘straight to test’) and this we believe has been achieved with a median time to diagnosis of 29 days. The wide IQR in non-YFCCP cohort likely reflects the composite of routine and ‘two week wait’ referrals.
We conclude that this audit of FC activity and colonoscopy outcomes provides substantial supportive evidence for the effectiveness of the YFCCP and supports its wider implementation. Popular in primary care, it is being used appropriately and has led to a reduction in absolute numbers of referrals. The diagnostic accuracy determined in this audit is in line with earlier evaluations of the YFCCP. Accepting that the control population has a similar disease prevalence despite different clinical suspicion, the findings of this evaluation likely underestimate the benefits of the YFCCP in terms of resource use saving and time to diagnosis. In young patients, the YFCCP should be used more often.
Footnotes
Contributors JT is the guarantor of the article. JT was the chief investigator, directed the study and wrote the first draft. DT provided laboratory oversight and the faecal calprotectin datasets, advice to JT and assisted in the preparation of the manuscript.
Funding Data was generated from the routine work of York Teaching Hospital NHS Foundation Trust.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.