Article Text

Abstract
The systemic circulation in patients with cirrhosis is hyperdynamic with an increased cardiac output and heart rate and a reduced systemic vascular resistance as the most pronounced alterations. The concomitant cardiac dysfunction has recently been termed “cirrhotic cardiomyopathy”, which is an entity different from that seen in alcoholic heart muscle disease. Clinically, these patients present with sodium fluid retention and strain often unmasks the presence of latent heart failure. No specific treatment can yet be recommended but caution should be used with respect to procedures that may stress the heart such as shunt implantation and liver transplantation.
- cirrhotic cardiomyopathy
- hyperdynamic circulatory dysfunction
- liver failure
- heart failure
- CO, cardiac output
- PAP, pulmonary artery pressure
- PCWP, pulmonary capillary wedge pressure
- RAP, right atrial pressure
- TIPS, transvenous intrahepatic portosystemic shunt
Statistics from Altmetric.com
- CO, cardiac output
- PAP, pulmonary artery pressure
- PCWP, pulmonary capillary wedge pressure
- RAP, right atrial pressure
- TIPS, transvenous intrahepatic portosystemic shunt
Past decades have seen the appearance of new techniques for the study of different aspects of cardiac function. Our knowledge of cardiovascular pathophysiology has improved considerably, including our understanding of cardiovascular complications of liver disease. Kowalski et al1 were the first to report that patients with cirrhosis had abnormal cardiovascular function and a prolonged QT interval. The systemic circulation in patients with decompensated cirrhosis is hyperdynamic and characterised by increased heart rate and cardiac output (CO) and decreased systemic vascular resistance with low normal or decreased arterial blood pressure.2–4 Among the factors that may increase the CO in patients with cirrhosis are increased sympathetic nervous activity, increased blood volume (increased preload), and the presence of arteriovenous communications.5–7 Many of the patients present with dyspnoea, fluid retention, and limited exercise capacity.4,8,9
The use of new investigative modalities has shown several lines of evidence of impaired cardiac contractility and performance in patients with cirrhosis and has led to the introduction of the new clinical entity, cirrhotic cardiomyopathy. This term implies a condition with defective myocardial contractility under physical and pharmacological strain, although the entity has not yet been finally classified and the mechanisms behind the cardiac abnormalities are only partly understood.10 The objective of this review is to summarise pathophysiological and clinical evidence of cardiac dysfunction in cirrhosis.
THE CIRRHOTIC HEART
Heart mass and volumes
In most studies of patients with cirrhosis, the heart mass has been found to be within the normal range.11,12 However, some have reported an increased left ventricular mass13,14 and in a recent experimental study of portal hypertensive rats, left eccentric hypertrophy was found to correlate directly with the degree of hyperdynamic circulation.15 The determination of heart volumes in patients with cirrhosis has given somewhat different results depending on the methods used.16–18 In echocardiographic studies, Kelbæk et al19 and Rector et al17 found the size of the left ventricle to be normal and that of the left atrium enlarged.20,21 Others, however, have reported increases in both the end diastolic and the end systolic volumes of the left ventricle.13,22–25 Wong et al16 used radionuclide angiography and they reported normal left ventricular systolic and diastolic volumes, including the stroke volume. Normal and increased right ventricular and atrial volumes have been found by echocardiography.17,20,21,26,27 In contrast, magnetic resonance imaging has shown reduced right ventricular and atrial dimensions and slightly increased left ventricular and atrial volumes.12 Reduced right heart volumes could reflect a general contraction of the central blood compartment in patients with cirrhosis, as previously suggested by other techniques.28 The change in the left ventricular dimensions in cirrhosis is related to haemodynamic dysfunction. Thus, Lewis et al29 found significant correlations between the left ventricular end diastolic diameters on one hand and CO, stroke volume, mean arterial blood pressure, and blood volume on the other. Moreover, significant direct correlations between plasma atrial natriuretic peptide and left atrial volume and left ventricular end diastolic diameter have been reported.20,21
In conclusion, the size of the left atrium and ventricle in patients with cirrhosis is normal to increased. No definite conclusion can be offered as to the size of the right heart.
Heart pressures
Most published studies show the right ventricular pressure, pulmonary artery pressure (PAP), and left atrial or pulmonary capillary wedge pressure (PCWP) to be at the upper normal limit but within the normal range during rest (table 1); the severity of the liver disease per se does not seem to affect cardiac pressures.30–32 However, fluid retention with formation of ascites and haemodynamic disturbances with increased blood volume may result in increased right atrial pressure (RAP),30 and paracentesis with removal of ascitic fluid has been shown to lower the RAP, PAP, and PCWP.33 Physical exercise, pharmacological stress, and therapeutic procedures may affect cardiac pressures. Thus, the left ventricular end diastolic pressure increases but the cardiac stroke index and left ventricular ejection fraction fall during exercise, which indicates an abnormal ventricular response to an increase in ventricular filling pressure.19,31,34 Reduced left ventricular afterload (reduced systemic vascular resistance, low arterial blood pressure, and increased arterial compliance) may mask left ventricular failure.14,19,35–37 By infusion of angiotensin, Limas et al38 increased the systemic vascular resistance by 30% and found that the PCWP, which reflects left ventricular end diastolic volume, increased twice with no change in CO. A failure to increase CO despite an increased ventricular filling pressure indicates that normalisation of the afterload impairs cardiac performance and unmasks left ventricular failure.38 Interestingly, this effect on the PCWP was not improved after addition of digoxin. Similar results, with increases in the RAP, PAP, right ventricular pressure, and PCWP, have been achieved by normalising the arterial blood pressure with infusion of terlipressin and octreotide.39–41 Infusion of a plasma protein solution increased CO, as well as RAP, PAP, and PCWP, whereas infusion of packed red blood cells did not change these variables.42 In a recent study by Forrest et al,43 oral administration of the adenosine antagonist theophylline significantly decreased PAP and PCWP, thus suggesting that adenosine could be implicated in the cardiovascular dysfunction present in cirrhosis. Surprisingly, lowering the afterload by infusion of the nitric oxide donor L-arginine in cirrhotic patients produced significantly increased RAP, PAP, and PCWP, despite a decreased arterial blood pressure.44 However, it is possible that this is a direct effect of nitric oxide on myocardial contractility.
Haemodynamic changes in different vascular territories in patients with cirrhosis at rest
Transvenous intrahepatic portosystemic shunt (TIPS) is frequently used in the treatment of bleeding oesophageal varices and refractory ascites.45 Insertion of a TIPS results in an immediate increase in the ventricular preload because a high splanchnic blood flow is delivered into the systemic circulation. Several studies have noted an aggravation of the hyperdynamic circulation with increased CO, RAP, PAP, and PCWP immediately after TIPS placement.46–48 However, cardiac pressures and CO tend to become normal two or three months after this therapeutic procedure and some authors report no or only transient changes in cardiac pressures after TIPS insertion.49,50 In the past, a peritoneovenous shunt for treatment of refractory ascites was frequently implanted. This procedure, which further increased CO, was in a considerable number of patients complicated by the development of pulmonary oedema indicating a latent cardiac inability unmasked by the increased preload.51 At present, it is not possible to predict which patients will develop cardiac complications such as high output congestive heart failure after implantation of TIPS and peritoneovenous shunts, and the procedures should be considered with caution in patients with limited cardiac reserve.46,48
Most patients with cirrhosis have almost normal cardiac pressures when resting supine. These pressures become abnormally raised by procedures stressing the heart, such as pharmacological vasoconstriction, exercise, and the increased portosystemic shunting resulting from insertion of a TIPS. This should be considered when applying these procedures in patients with limited cardiac reserve, but at present no specific guidelines for the identification of patients at risk can be given.
LEFT VENTRICULAR DYSFUNCTION
Systolic dysfunction
The circulation of the patient with cirrhosis is hyperdynamic, with increased CO and heart rate, expanded plasma volume, and low arterial blood pressure and systemic vascular resistance.52 The pathophysiological background of the increased CO is under discussion and a key feature is the size of the central and arterial blood volume.16,20,53,54 Reduced central and arterial blood volume would lead to deactivation of arterial baroreceptors, increased sympathetic nervous activity and, thereby, increased heart rate and CO.52 However, the circulation seems to be hyperdynamic only in the supine position, normalising after tilting.55,56 Results of studies with postural changes suggest that an increased preload contributes to the increased CO in the supine position. Interestingly, in patients with compensated cirrhosis and arterial hypertension there is no evidence of a hyperdynamic circulation.57 In addition, Laffi et al25 recently described reduced left ventricular end diastolic volume and reduced ejection fraction after standing, which indicate an impaired myocardial response to an erect posture. Studies of patients with cirrhosis found after head out water immersion an increase in CO and central and arterial blood volume, which also support an altered distribution of the plasma volume as a cause of the hyperdynamic circulation.58 Left ventricular ejection fraction has been reported to be normal at rest in some studies.13,19,34,59 After exercise, the left ventricular ejection fraction increases significantly less in patients with cirrhosis than in matched controls.19,34 Aerobic exercise capacity and maximal heart rate are lower in most patients with cirrhosis.19,34,59 The reduced cardiac performance is probably caused by a combination of blunted heart rate response to exercise, reduced myocardial contractility, and profound wasting of skeletal muscle with impaired extraction of and demand for peripheral oxygen.8,59,60
After liver transplantation, CO decreases and arterial blood pressure and the systemic vascular resistance increase.32,61,62 These changes may be attributed primarily to normalisation of the liver function whereas specific treatments with, for example, cyclosporin also may play a part. Liver transplantation is associated with a high incidence of cardiovascular complications, which is an important cause of mortality after transplantation.63 Identification of patients at risk of developing cardiac failure in the post-transplantation period has been attempted by dobutamine stress echocardiography.64 However, in this study of 190 patients, no preoperative echocardiographic parameters, including ischaemia on dobutamine echocardiography, predicted these perioperative events.64
Diastolic dysfunction
Patchy fibrosis and increased heart weight may affect the stiffness of the myocardial wall and result in impaired left ventricular filling and diastolic dysfunction.10 Expanded blood volume may increase the cardiac preload, thus contributing to the persistent increase in CO, with overloading and impaired cardiac contractility as the outcome.12,35,56 Studies in which dextran was infused in human and experimental cirrhosis showed a limited cardiac preload reserve with a decreased ability to modulate cardiac performance under various loading conditions.11,65 Recent studies of ventricular diastolic filling in cirrhosis support the presence of a subclinical myocardial disease with diastolic dysfunction with a decreased E:A ratio, which in patients with ascites improves after paracentesis.14,26,27,66
Patients with cirrhosis may have an increased, normal, or even reduced preload and a reduced afterload. Latent systolic and a diastolic dysfunction with reduced work capacity is present and becomes in some patients manifest if the heart is challenged. The type of cardiac insufficiency in cirrhosis may best be characterised as a high CO failure. It is likely that the reduced systolic cardiac dysfunction in cirrhosis contributes to the general low degree of physical activity reported in several studies.3,67 Thus, after liver transplantation, both physical activity and cardiac function seem to improve.67 Diastolic dysfunction may be a significant factor in the development of heart failure, may precede systolic dysfunction in patients with cirrhosis, and may play a part in the pathogenesis of sodium fluid retention in cirrhosis.14,66
Conductance abnormalities
The fluidity of the plasma membrane and the function of its ion channels have been shown to be impaired in cirrhosis.68 Thus, Moreau et al69,70 have shown an altered control of vascular tone by K+ and Ca++ channels in various cells in experimental and human cirrhosis. A result of these changes, if they are generally present, could be electrophysiological abnormalities in cardiac excitation. Thus, Ward et al71 have recently shown a decrease in K+ currents in ventricular myocytes from cirrhotic rats, which would tend to prolong the QT interval. A prolonged QT interval has previously been described in patients with liver disease, leading to ventricular arrhythmias and sudden cardiac death.1,72 Recently, Bernardi et al73 described a prolonged QT interval in patients with cirrhosis, which was significantly related to the severity of the liver disease, plasma noradrenaline (norepinephrine), and survival. Changes in the QT interval seem to revert with improved liver function, for instance, after liver transplantation.74 Results from a preliminary study from our group have indicated that the frequency adjusted QT is partly normalised in patients with cirrhosis after oral β blocker administration. Whether this may be a beneficial effect of β adrenergic blockade in addition to the effects on risk of bleeding from oesophageal varices remains to be validated. The prolonged QT interval in cirrhosis should most likely be considered an element in the cirrhotic cardiomyopathy and may be of potential use in identifying patients at risk. Future pathophysiological and clinical research is needed to assess the prognostic and therapeutic significance.
EXTRACARDIAC FACTORS
Autonomic dysfunction
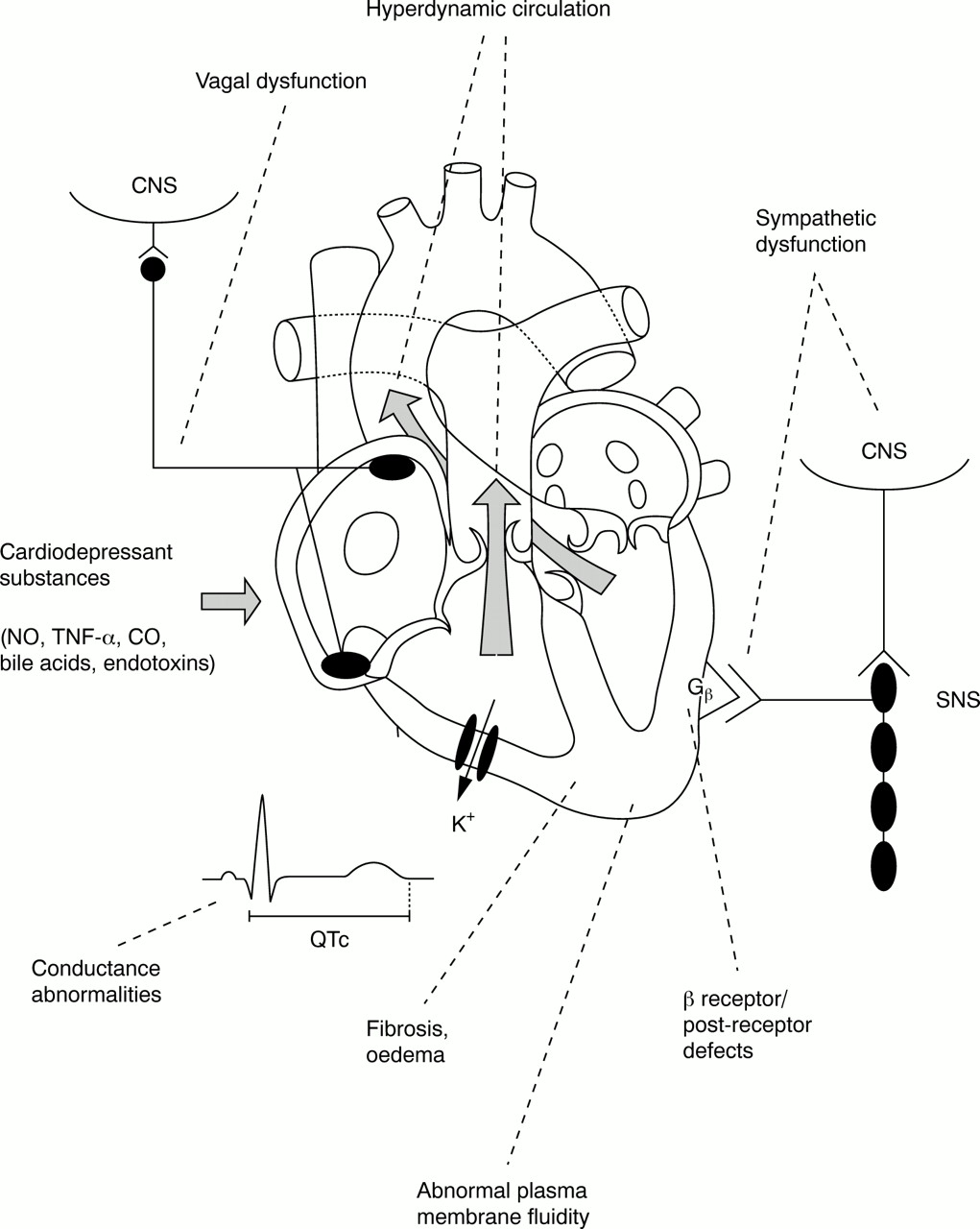
Haemodynamic alterations may per se affect the function of the heart and reduced performance of the heart in cirrhosis may, on the other hand, contribute to low arterial blood pressure and the activation of vasoactive systems analogous to congestive heart failure.75,76 Cardiovascular reflex tests of various studies have shown sympathetic and parasympathetic autonomic dysfunction in patients with cirrhosis depending on the severity of the disease.77–79 The location of the autonomic dysfunction is unknown but could be within the central nervous system because of damage to the peripheral nerves or because of changes in hormonal neurotransmission80,81 (fig 1).
{kind=link}
Potential pathophysiological components implicated in the development of cirrhotic cardiomyopathy. CNS, central nervous system; CO, carbon monoxide; NO, nitric oxide; QTc, frequency adjusted QT interval; SNS, sympathetic nervous system; TNF-α, tumour necrosis factor α.
Patients with cirrhosis exhibit enhanced activity of the sympathetic nervous system with increased burst frequency and increased circulating catecholamines in direct relation to the severity of the disease.5 The major triggers of the sympathetic overactivity seem to be baroreceptor mediated stimulation, owing to the low arterial blood pressure and hepatic dysfunction, and a volume receptor mediated stimulation, owing to reduced central and arterial blood volume.5,82 The sympathetic response to dynamic exercise seems to be normal in patients with cirrhosis, but the response to isometric exercise is clearly impaired.8,34,60,83 Similarly, blood pressure responses to orthostasis are impaired, probably because of a blunted baroreflex function.25,84–86 The haemodynamic effects of posture have been studied in detail by Bernardi et al,55,56,87 who have reported reversal of the hyperdynamic circulation after standing, but unaltered heart rate and arterial blood pressure, and increased circulating noradrenaline and increased renin activity. The blood pressure after active tilting is largely unchanged or even increased, and the prevalence of orthostatic hypotension in cirrhosis may not be significantly different from that in the normal population.79,88 In addition, abnormal cardiovascular responses to pharmacological stimulation with angiotensin II, noradrenaline, and vasopressin in terms of impaired responses in the blood flow and blood pressure have been reported.89–91
Enhanced sympathetic tone with increased cellular exposure to noradrenaline for longer periods is known to cause myocardial injury and impaired β adrenergic function.76 Increased cardiac troponin I in patients with cirrhosis indicates that cardiac injury occurs in some patients.92 The pressor response to noradrenaline and other potent pressor substances, such as angiotensin II and vasopressin, is blunted in patients with cirrhosis.89,93–96 The decreased responsiveness could be a result of defective β adrenergic function. Thus, Gerbes et al97 showed that leucocytes from patients with cirrhosis have fewer β adrenoceptors. Moreover, studies in cirrhotic animal models indicate downregulation with reduced β adrenergic receptor density in cardiomyocytes and receptor desensitisation.10 Recent studies have provided evidence that the cardiac dysfunction in experimental cirrhosis is in part brought about by the combination of receptor and postreceptor defects in the heart. Thus, Ma et al98 reported reduced function and expression of the cardiac G protein in experimental cirrhosis, and Zavecz et al99 found impaired cardiac excitation contraction coupling in rats with portal hypertension. Impaired β adrenergic signal transduction may then be an important element in the pathogenesis of cirrhotic cardiomyopathy.
Recent reports have emphasised the importance of a vagal impairment. Dillon et al100 reported that captopril corrected the autonomic dysfunction, which suggests that vagal dysfunction in cirrhosis is partly caused by neuromodulation by angiotensin II. Cardiac muscarinic receptors may counterbalance the positive inotropic and chronotropic effects of β adrenergic stimulation. Recently, Jaue et al101 reported a blunted muscarinic response in cirrhotic rat hearts. This response was not caused by downregulation of muscarinic receptors, which suggests a potential postreceptor defect. However, the changes in muscarinic function may be compensatory, and overactivity of the parasympathetic nervous system is not likely to be a major factor in the genesis of cirrhotic cardiomyopathy.
Cardiodepressant substances
Alcoholic heart muscle disease, or alcoholic cardiomyopathy, is a well known cause of reduced left ventricular performance in alcoholic patients with and without cirrhosis.102,103 The distinction between alcoholic and cirrhotic cardiomyopathy can be difficult59,60 but the pathogenesis of alcoholic and cirrhotic cardiomyopathy seems to be dissimilar. Thus, in alcoholic heart muscle disease, left ventricular performance is reduced, owing to impaired contractile protein synthesis and formation of immunogenic cardiac protein acetaldehyde adducts.104 The presence of antibodies to these adducts may be a marker for the diagnosis of this type of heart disease or possibly for its pathogenesis. The major features in cirrhotic cardiomyopathy are impaired β adrenergic receptor function, plasma membrane dysfunction, and increased CO.
Other potential mechanisms of impaired cardiac function in cirrhosis are production of other cardiodepressant substances, such as endotoxins, endothelins, cytokines, and bile acids.105,106 Nitric oxide may also play a part in cardiac contractility. In an animal model, Van Obbergh et al107 observed that decreased left ventricular pressure increased after blockade of nitric oxide synthesis, which indicates that cardiac depression may be associated with nitric oxide. In a recent study on the effects of l-arginine infusion in patients with cirrhosis, left ventricular pressures were not measured, but RAP, PAP, and PCWP were all significantly increased.44 Haem oxygenase is an enzyme responsible for haem degradation into carbon monoxide, iron, and biliverdin. Carbon monoxide is a potent vasodilator and this compound may also be involved in vascular hyporeactivity and defective myocardial contractility in cirrhosis.108 Liu et al109 reported increased cardiac cytokines—tumour necrosis factor α and interleukin 1b—in bile duct ligated rats. Patients with decompensated cirrhosis have increased concentrations of interleukin 6, interleukin 8, and tumour necrosis factor α, which indicate that proinflammatory signals are involved in the pathogenesis of compensated and especially decompensated cirrhosis.110 As in cirrhosis, patients with congestive heart failure and dilated cardiomyopathy have an activated sympathetic nervous system and increased circulating cytokines.111 Recently, treatment with β blockers has been shown to decrease the plasma concentration of interleukin 6 and tumour necrosis factor α in patients with dilated cardiomyopathy.112,113 β blockers may then—in addition to their neuroendocrine effects—have an important immunoregulatory role.111 However, no such studies have yet been performed in patients with cirrhosis and whether such effects can be achieved in cirrhotic patients must be answered by future research. New anticytokine treatments are being developed to inhibit neuroendocrine and cytokine activation in chronic heart failure, and these treatments may also be relevant in the potential treatment of cirrhotic cardiomyopathy.111,114 Cytokine stimulated activation of cardiac nitric oxide synthase in cirrhotic animal models adds further support to the involvement of the nitric oxide system in cirrhotic cardiomyopathy and should stimulate studies on nitric oxide inhibition.109
In patients with jaundice without cirrhosis, heart function may also be impaired. The reason is not clear but increased concentrations of bile salts have been shown to inhibit cardiac contractility.115 Ma et al116 recently showed that cardiac function was decreased in experimental cirrhosis with various degrees of jaundice. The mechanism in this model seems to be the blockade of adenyl cyclase.
There is now basic and clinical evidence that cirrhotic cardiomyopathy differs from alcoholic cardiomyopathy, now termed alcoholic heart muscle disease, and that cirrhotic cardiomyopathy occurs frequently in non-alcoholic cirrhotic patients. In addition, toxic substances that accumulate because of impaired hepatic function may further inhibit cardiac function in these patients. Potential new treatments such as anticytokines have potential relevance.
CONCLUSIONS
Heart diseases can affect the liver with development of, for instance, cardiac cirrhosis and liver diseases may affect the heart with development of cirrhotic cardiomyopathy. Cardiac and liver diseases may also have a common aetiology, as is seen in metabolic and infectious diseases.117 From a functional point of view, the heart in cirrhosis is at the same time hyperdynamic and dysfunctional. Experimental and clinical studies of patients with cirrhosis strongly suggest the presence of latent heart failure with impaired reactions to standardised provocations. This has given rise to the introduction of the clinical entity cirrhotic cardiomyopathy, which may cover different pathophysiological mechanisms. Cirrhotic cardiomyopathy is clinically and pathophysiologically different from alcoholic heart muscle disease. Cirrhotic cardiomyopathy comprises changes in impaired cardiac contractility during the preload and afterload, decreased β adrenergic receptor function, postreceptor dysfunction, defective excitation contraction coupling, and in some patients conductance abnormalities (fig 1). Clinically significant cardiac dysfunction and latent heart failure are the outcome. A pertinent issue for forthcoming studies is whether cirrhotic cardiomyopathy affects mortality. At present no specific treatment can be recommended and evident ventricular failure in patients with cirrhotic cardiomyopathy should be treated as non-cirrhotic causes with sodium restriction, diuretics, and afterload reduction. Cardiac glycosides may not be expected to be of significant value in cirrhotic cardiomyopathy as these failed to improve cardiac contractility after angiotensin infusion.38 Special caution should be taken during and after stressful procedures such as surgery, shunt implantation, and liver transplantation. Effects of β blockers on cardiac function, QT interval prolongation, and mortality are subjects for future research. Newer treatments with anticytokines may also prove to be of interest in patients with cirrhotic cardiomyopathy.
REFERENCES
Linked Articles
- Miscellanea
- Miscellanea