Article Text

Abstract
The introduction of endoscopy of the upper digestive tract as a routine diagnostic procedure has increased the number of duodenal biopsy specimens. Consequently, the pathologist is often asked to evaluate them. In this review, a practical approach to the evaluation of a duodenal biopsy specimen is discussed. An overview of the handling of specimens is given and the normal histology and commonly encountered diseases are discussed. Finally, a description of commonly seen infections is provided, together with an algorithmic approach for diagnosis.
- CMSE, cow’s milk protein-sensitive enteropathy
- CMV, cytomegalovirus
- DGM, duodenal gastric metaplasia
- DPAS, diastase periodic acid Schiff
- EMA, endomysial antibodies
- EITCL, enteropathy-type intestinal T cell lymphoma
- GFD, gluten-free diet
- GSE, gluten-sensitive enteropathy
- H&E, haematoxylin–eosin
- IEL, intraepithelial lymphocyte
- IPSID, immunoproliferative small intestinal disease
- NSAID, non-steroidal anti-inflammatory drug
- PAS, periodic acid Schiff
- V:C ratio, villous to crypt ratio
- TCR, T cell receptor
- tTGA, transglutaminase antibody
Statistics from Altmetric.com
- CMSE, cow’s milk protein-sensitive enteropathy
- CMV, cytomegalovirus
- DGM, duodenal gastric metaplasia
- DPAS, diastase periodic acid Schiff
- EMA, endomysial antibodies
- EITCL, enteropathy-type intestinal T cell lymphoma
- GFD, gluten-free diet
- GSE, gluten-sensitive enteropathy
- H&E, haematoxylin–eosin
- IEL, intraepithelial lymphocyte
- IPSID, immunoproliferative small intestinal disease
- NSAID, non-steroidal anti-inflammatory drug
- PAS, periodic acid Schiff
- V:C ratio, villous to crypt ratio
- TCR, T cell receptor
- tTGA, transglutaminase antibody
The development of the intestinal tract begins as a tube that joins the stomach to the cloaca. The proximal portion of this tube becomes the segment that extends from the distal duodenum to the proximal ileum. The more caudal portion develops into the terminal ileum and proximal two thirds of the transverse colon. The epithelium develops from simple endodermal tubules early during embryogenesis. Between 9 and 10 weeks, the stratified epithelium converts to simple columnar epithelium. Formation of villi begins at 9 weeks. The epithelium completes its morphological differentiation in 4–5 days before birth. Primordial lymphoid structures appear in the intestine roughly halfway through gestation. Aggregates of T and B cells form early Peyer’s patches by 16 weeks’ gestation, with organised Peyer’s patches present by 19 weeks.1
PRACTICAL POINTS
Evaluation of a small-intestine biopsy specimen
In the histological evaluation of the duodenal biopsy specimen, a clinical pathological correlation is essential for diagnosis. Communication between the clinician and the pathologist is essential for evaluation of all duodenal biopsy specimens.
Initial evaluation should begin with a careful examination of the requisition to ascertain the relevant clinical features of the patient and to ascertain the biopsy site.
The following clinical data should be provided to the pathologist:
-
Age and sex of the patient
-
Signs and symptoms, site of the biopsy, endoscopic findings, radiological findings
-
Clinical diagnosis or impression
-
Medical and surgical history
-
History of taking drugs or alcohol
-
History of immunosuppression
-
Findings of previous biopsies.
Indications for a duodenal biopsy
The main indications for a duodenal biopsy are
-
Evaluation of patients with malabsorption
-
Investigation on patients with iron-deficiency anaemia
-
Diagnosis or monitoring of gluten-sensitive enteropathy (GSE)
-
Diagnosis of neoplasia
-
Investigation on patients with diarrhoea, particularly in patients in whom infection is suspected (AIDS)
-
Confirmation of ulceration induced by non-steroidal anti-inflammatory drugs (NSAIDs) or in cases of bleeding from an unknown site.
The issue of carrying out a duodenal biopsy regardless of the indications for endoscopic and macroscopic findings is somewhat controversial. On the one hand, a routine duodenal biopsy may yield an unsuspected pathology, which may have major clinical implications. In contrast, a duodenal biopsy on an apparently normal mucosa increases the risk of anaesthesia and procedural complications. Overall, the costs to benefits ratio may not be justified. Nevertheless, many studies have shown that unsuspected duodenal pathology may be found in routine duodenal biopsies.2,3 A study on a paediatric population showed that a routine duodenal biopsy yielded pathological findings in 17.4% of cases.2 Unexpected findings have been reported, such as Giardia (4.9% of cases), mild chronic inflammation in the lamina propria, with an increased number of plasma cells associated with Helicobacter pylori infection in a gastric biopsy specimen (6.5%), an increase in the intraepithelial lymphocyte (IEL) count, with negative antiendomysial antibodies (3.9%) and Crohn’s disease (n = 1).2 In addition, the probability of finding a duodenal pathology may also be related to the underlying symptoms. In this study, the most frequent indication (50% of the cases) for endoscopy was anaemia. The negative predictive value of the normal duodenal mucosa was 81.5%, indicating that a normal-appearing mucosa may have some pathological changes.2 Thus, the evaluation of a routine duodenal biopsy specimen is a valuable diagnostic aid in recognising unsuspected pathology in asymptomatic patients or those with atypical symptoms.2,3
A biopsy report should include the following information
-
Number and site of the biopsy specimens. Are the specimens normal or abnormal? What is the villous height and architecture: normal, broad or blunted?
-
Normal villous to crypt (V:C) ratio (range from 3:1 to 5:1; fig 1)
-
Presence of crypt hyperplasia
-
Surface enterocytes: normal, flattened or damaged
-
Brush borders: preserved or lost
-
IEL count
-
Gastric metaplasia in chronic duodenitis
-
Presence of microorganisms: Giardia, cryptosporidia, microsporidia, Isospora belli, cyclospora, Mycobacterium avium intracellulare, cytomegalovirus, Cryptococcus neoformans
-
Neoplasia: presence of benign or malignant tumour (adenoma or carcinoma, carcinoid, lymphoma).
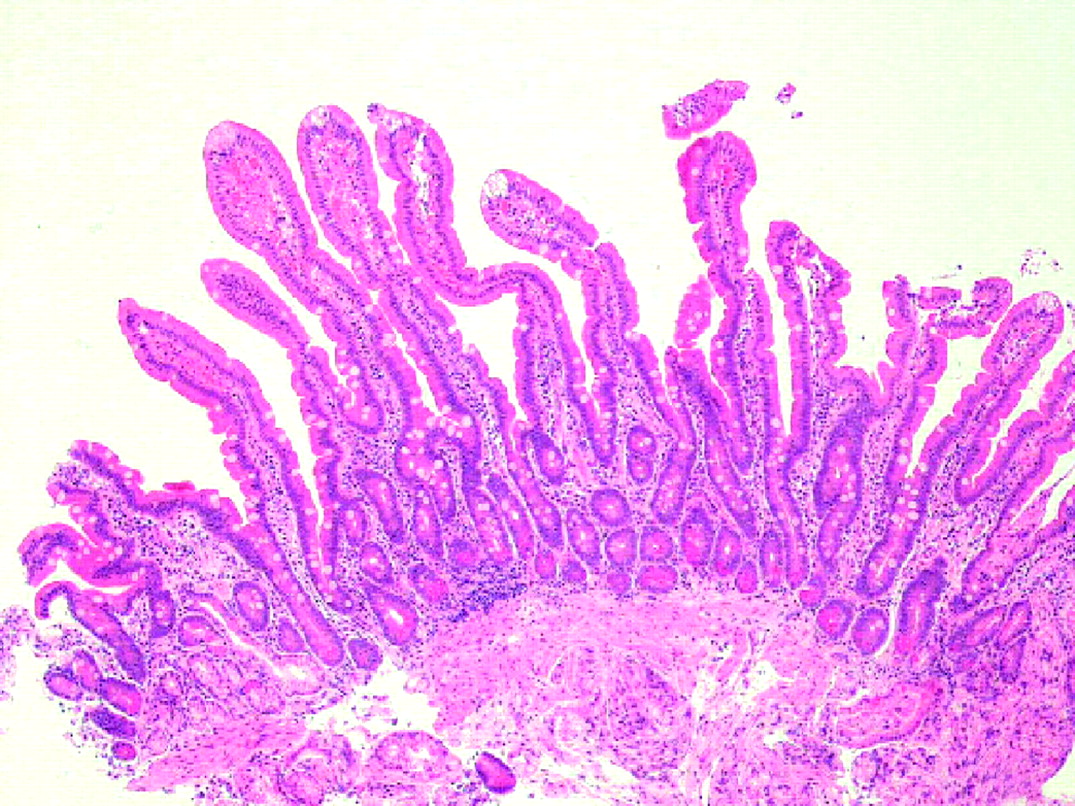
A well-oriented duodenal biopsy specimen; 4–5 elongated villi are seen from the base to the tip. The villous to crypt ratio is at least 3:1. Brunner’s glands are present in the submucosa (haematoxylin–eosin staining, ×50).
How many specimens should be taken for biopsy and where from?
The number of duodenal biopsy specimens simultaneously taken is variable as is the site. Some authors suggest that at least three specimens be taken in the distal duodenum.4
Since partial and patchy villous atrophy may be found in cow’s milk protein-sensitive enteropathy (GMSE), in postenteritis enteropathy and in GSE, multiple biopsies should be taken to minimise the risk of underdiagnosis or misdiagnosis.5
The duodenal damage that is suggested to be induced by gluten starts in the duodenal bulb and progressively extends to affect the descending duodenum and the proximal jejunum. Consequently, the site and the number of the specimens are important to make a correct diagnosis of GSE.6
In GSE, duodenal lesions may have a patchy distribution, especially in children,6 and villous atrophy may be contiguous with or coexist with mild atrophy or normal mucosa. The bulb mucosa may be the only duodenal area affected, both at diagnosis and after gluten challenge,6 and total or moderate villous atrophy may affect the duodenal bulb exclusively, with a normal distal duodenum.6
Thus, multiple endoscopic biopsy specimens should always be taken, both in the distal duodenum and in the bulb.6
On the other hand, Ravelli et al5 showed that villous atrophy was markedly more common in the more distal areas of the duodenum and in the duodenojejunal flexure, and that it was also established throughout the duodenum. Different histological types of lesions, however, may be present in different biopsy specimens taken from different sites of the duodenum in the same patient, usually without exceeding grade I of the classification given by Oberhuber et al,7 and a normal duodenal histology in any biopsy site is never found in patients with GSE.5 The discrepancy between these studies can be explained by the duration of the gluten-free diet (GFD), the stage of evolution of the disease and the experience of the pathologist, by the orientation of the biopsy specimen and the use of CD3 immunostaining, which facilitates the IEL count, which is generally higher in the distal duodenum than in the duodenal bulb.5
According to Ravelli et al,5 a single endoscopic biopsy specimen that is taken by a suction capsule from any site in the duodenum, which is adequately oriented and stained, may be sufficient to make a diagnosis of GSE in a genetically susceptible person (HLA-DQ2 or HLA-DQ8 positive) with a positive serology: tissue transglutaminase antibodies (tTGA) and endomysial antibodies (EMA).5 As villous atrophy, may be confined to the duodenal bulb and to reduce the histological variability, taking two biopsy specimens is recommended, one from the descending or distal duodenum and the other from the duodenal bulb, if atrophic areas are not identified.5 If atrophic areas are seen by endoscopy, two specimens should be taken in these areas.5
Also, in case of Giardia infection, the parasites are homogeneously distributed in the duodenum and two duodenal biopsy specimens may be sufficient to diagnose the infestation in most cases.8
In patients with certain or suspected Crohn’s disease, the duodenum should be well sampled to show the focality of the lesions.9
Therefore, in summary, the site and number of biopsy specimens taken varies with the clinical setting.
How to take a duodenal biopsy specimen
Duodenal biopsy specimens can be taken in two ways: by suction or by endoscopy.
Suction biopsy specimens are taken from the jejunum by Crosby suction capsules and as these are large in size, they are more easily oriented in the laboratory.
Currently, mucosal endoscopy has replaced suction biopsies. It is more convenient, easier to take and better tolerated by the patient. Also, endoscopic biopsy specimens can be targeted better as they are taken under observation.10–14
How to orient the biopsy specimen
The orientation of the duodenal biopsy specimen is essential for accurate histopathological assessment. The evaluation of the V:C ratio or the count and distribution of the lymphocytes in the duodenal epithelium in well-oriented biopsy specimens is critical. In addition, some organisms tend to colonise the enterocytes in the tip of the villi and a poorly oriented specimen can make their identification difficult, if not impossible. Orienting the duodenal biopsy specimen on filter paper5,15 will help the endoscopist have a well-oriented specimen.
The specimen is oriented with the luminal side uppermost. In case of multiple specimens, they can be oriented on a strip of Millipore filter, cut obliquely (like a clarinet mouthpiece) to conventionally mark the beginning of the biopsy sequence5 (fig 2).

Representation of orientation of a biopsy specimen. The specimen is positioned on the Millipore filter with the luminal side uppermost. In case of multiple specimens, they can be oriented on a strip of Millipore filter, cut obliquely to mark the beginning of the biopsy sequence.
Poor quality of the sample and tangential sectioning are often the source of misinterpretation of the specimen and, consequently, of misdiagnosis.4
Special stainings commonly carried out
Histochemical analysis is mainly used to stain microorganisms or cellular components.
-
Periodic acid Schiff (PAS) stain for macrophages in Whipple’s disease; fungi, gastric metaplasia in chronic duodenitis; and integrity of the brush border
-
Diastase periodic acid Schiff (D-PAS) or methanamine silver stains for C neoformans
-
Wade Fite, Ziehl–Nielsen or Auramine stain for mycobacteria
-
Warthin Starry stain for microsporidia
-
Iron haematoxylin counterstain in trichrome technique, Giemsa, toluidine blue for G lamblia
-
Immunoperoxidase for cytomegalovirus.
Immunohistochemistry is used for CD3, CD4 and CD8 in GSE and refractory sprue.
INTERPRETATION OF THE DUODENAL BIOPSY SPECIMEN
Evaluation of the architecture
Low-power magnification can give information on the general appearance and quality of the duodenal biopsy specimen and about its the architecture.
A well-oriented biopsy specimen (fig 1) should have at least 4–5 consecutive elongated, well-distended villi from the base to the tip. Villous architecture shows a wide spectrum of morphological differences across populations. Villous morphology includes variations such as finger-like, leaf-like, tongue-like or ridge-like villi. In the duodenum, it is common to see branched villi, villi containing fused tips16 or mixed populations.17 Villous morphology may also be related to geographical areas: in temperate areas villi are longer, with a finger-like appearance, whereas in tropical areas leaf-like and ridge-like variants are present in the proximal duodenum and the finger-like variants occur distally.18
Normal V:C ratio ranges roughly from 3:1 to 5:1 (fig 1).
Villous atrophy is defined as a flattening of surface secondary to the shortening and blunting of the intestinal villi. The degree of shortening can be variable: total villous atrophy occurs when the V:C ratio varies from 0:1 to 1:1 and partial villous atrophy when it varies from 1:1 to 4:1.19
Villous atrophy is a non-specific reaction of the intestinal mucosa to a variety of injuries. The pathogenesis is either associated with a hyper-regenerative increase in crypt cell mitoses leading to crypt elongation (eg, in patients with GSE) or it results from hyporegeneration—that is, reduced mitotic rate with shortened crypts (as seen in starvation or total parenteral nutrition).20
Crypt cell proliferation is induced by T cell activation; therefore, activated CD4 T cells in the normal lamina may be associated with the maintenance of the normal mucosal architecture.20
Duodenal mucosal specimens cause certain problems of interpretation: the architecture shows shorter and thicker villi than those found in the jejunum, especially in areas overlying Brunner’s glands21 or lymphoid follicles; villous atrophy in the duodenal bulb may therefore be difficult to diagnose.5
Villi may be blunted and shortened or appear atrophic when the lamina propria is infiltrated by macrophages, such as in Whipple’s disease or in M avium intracellulare infections, or by a dense infiltrate of plasma cells and centrocyte-like lymphocytes or small, pleomorphic lymphocytes. In these cases, the overlying epithelium is usually intact, crypts are spared and the IEL count is normal.
Crypt hyperplasia is considered to be a reparative or regenerative process.22 It is characterised by an increase in the length of crypts, a reduction in the normal C:V ratio and an increased number of mitoses due to extension of the proliferative compartment from the crypt bases along the length of the crypt.
In patients with GSE, the assessment of crypt hyperplasia is often difficult, especially when the villous architecture is preserved. The most sensitive marker of crypt hyperplasia seems to be the Ki-67 index.23
The surface epithelium is composed of columnar absorptive cells, the enterocytes, and mucin-secreting cells, the goblet cells. The enterocytes are characterised by basally located, evenly aligned nuclei. The luminal surface of enterocytes has a PAS-positive brush border. Goblet cells are scattered among the enterocytes. The goblet cells contain Alcian blue-positive sialomucin. Paneth cells in the crypts are characterised by brightly eosinophilic, supranuclear, cytoplasmic granules.
Endocrine cells are present in the crypts as single cells or in clusters. Unlike Paneth cells, these are found in the basal part of the cells (infranuclear position).
Spaces between the villi on the surface epithelium have to be carefully checked to exclude the presence of G lamblia.
Careful examination of the superficial epithelium over the tips of the villi is required because some studies have reported a top-heavy distribution pattern of CD3+ IELs, suggestive of GSE.18,24–26 In addition, numerous small-intestinal protozoans (microsporidia, cyclospora and isospora) have a predilection for the enterocytes at the tips of the villi and the surface epithelium can show architectural disarrangement and focal degeneration.27
Enterocytes may also show non-specific degenerative changes, such as vacuolisation of the cytoplasm (in GSE) or gastric metaplasia.
Lamina propria
The lamina propria usually consists of plasma cells and lymphocytes with the rare occurrence of eosinophils and macrophages. Plasma cells secrete IgA in the intestinal lumen and in the lamina propria itself. Lymphoid nodules (mucosa-associated lymphoid tissue) are scattered throughout the mucosa and aggregate into visible Peyer’s patches.
A thickening of the mucosa can result from oedema and an increase in lymphocytes, plasma cells, mast cells, basophils, eosinophils and neutrophils.28 The volume of the lamina propria is increased twofold in the flat destructive lesion of GSE compared with that in control mucosa.28
In duodenal biopsy specimens from patients with dermatitis herpetiformis, the progressive distension of the lamina propria occurs with infiltration of plasma cells, neutrophils and basophils, as changes in mucosal architecture progress to types 1, 2 and 3, to eventually become flat. Certainly, oedema and neutrophil infiltration of the lamina propria are early features that occur with crypt hypertrophy, which is the only evidence of any architectural change.28 The acute inflammation can be so intense that it mimics a peptic ulcer.22 The increase in neutrophils is dependent on the gluten dose.28
Eosinophils are sometimes prominent and infiltrate the epithelium22 in GSE and in food allergy.29,30
The lamina propria may be colonised by Cryptococcus or infiltrated by plump macrophages in mycobacterial infection, leishmaniasis or Whipple’s disease.
Typical and atypical inclusions of cytomegalovirus (CMV) may be found in endothelial cells, Brunner’s glands, stromal fibroblasts and endothelial cells, and possibly in smooth-muscle cells in the muscularis mucosa.
Intraepithelial lymphocytes
IEL count
The epithelium of the whole length of the villus should be evaluated. The count should be avoided in the vicinity of small lymphoid aggregates so as not to overestimate the IEL count.31 The IEL morphology can also influence the count. IELs tend to be squeezed between epithelial cells; they are sometimes surrounded by a pale halo and they may also show various shapes.22 This variation in the appearance can increase the risk of underestimating the IEL count. The thickness of the sections may influence the IEL count.22 The use of immunohistochemical analysis in architecturally normal villi is suggested, especially when GSE is suspected.22
The assessment of IELs has evolved since the 1970s. The normal upper limit of IELs was set at 40 per 100 epithelial cells (ECs) around 30 years ago.32 Recently, a revision of the IEL count in duodenal or jejunal biopsy specimens has been proposed. In the distal duodenum biopsy specimen, the count assessed the normal upper limit between 20 IELs31 and 25 IELs25,33) per 100 epithelial cells in sections stained with haematoxylin and eosin (H&E). According to this, the normal ratio of IELs to epithelial cells is 1:5. Immunohistochemical analysis helps to provide a more accurate count. Indeed, when immunohistochemistry is used for CD3, the upper limit is 25 IELs per 100 epithelial cells and the 95% confidence limit is 29 CD3+ IELs per 100 epithelial cells.31 Consequently, it has been suggested that values between 26 and 29 CD3+ IELs should be reported as borderline intraepithelial lymphocytosis and that ⩾30 CD3+ IELs should be diagnosed as intraepithelial lymphocytosis.31
These values can also suggest a two-step approach to the evaluation of the duodenal biopsy: H&E staining is adequate only when the villous architecture is normal with only a few scattered IELs, or when the duodenal mucosa shows villous atrophy and the IEL count is obviously increased.31
When the duodenal mucosa has a normal architecture or partial villous atrophy with suspected intraepithelial lymphocytosis, however, CD3 staining is useful, if not mandatory, to define the IEL count. This may be the case in infiltrative-type lesions in a case of suspected GSE where the duodenal biopsy specimen shows a normal architecture and the IEL count is difficult to assess.
Although uncommon, this may be a sign of latent GSE, but there may be other causes and the clinical relevance of this finding needs to be assessed by long-term follow-up or gluten challenge.34
Distribution of IELs
Although the IEL count has been used as an important diagnostic feature, the distribution of the IELs is gaining considerable value in the diagnosis of latent GSE with preserved villous architecture. The normal distribution of IELs has been described as decrescendo like, with the IEL count being higher at the bases of the villi and decreasing progressively towards the tips.24 On the other hand, the distribution is considered to be even if the IEL count is similar over the tip and at the base of the villus.24 A continuous and even distribution of the IELs is considered to be indicative of GSE,22,26 and a non-specific increase in IELs is more likely to decrease along the villous tip.22 The IEL distribution pattern along the villi, however, does not seem to be a reliable indicator of early GSE because of the overlapping of findings between patients with GSE and controls without GSE and also because of the interobserver variability.24 Although the IEL distribution pattern seems to be a sensitive feature of GSE, it has low specificity.
IELs at the tip of the villi
Interestingly, the feature that seems to be more specific and sensitive is the IEL count per 20 villous-tip epithelial cells,24 calculated from the mean value of 5 random villi.18,24–26 The value found in controls without GSE ranges from 0.5 to 6.3 IELs per 20 villous-tip epithelial cells.24 A value of 1.5–12.4 IELs per 20 villous-tip epithelial cells is a reliable indicator of early GSE, which includes probable GSE without villous atrophy, latent GSE or dermatitis herpetiform (mean values 6.6, 6.8 and 6.7 IELs per 20 villous-tip epithelial cells, respectively),24 whereas a count between 2.1 and 21.0 (mean value 11.6) IELs per 20 villous-tip epithelial cells is found in patients with untreated GSE.24 Another study, using the same method of IEL count, reported an IEL count slightly higher (1.4–7.8 (mean 4.6)) in controls without GSE, 2.0–18.6 (mean 7.9) in patients with treated GSE and 5.8–21.8 (mean 9.2) IELs per 20 villous-tip epithelial cells in patients with potential GSE.25 The IEL count between patients with potential GSE and controls without GSE differs markedly.25 A third study reported a mean villous-tip IEL count take of 11.6, 4.3 and 2.2 in patients with GSE, in those without GSE and in the controls, respectively.26 Although these findings are not specific, this study also showed that an appreciable pattern of even distribution of IELs along the villus was the most sensitive morphological feature of GSE.27 The IEL count taken in the villous tip compared with the traditional method is simpler and sufficiently reliable.18,25
In patients with GSE, CD3 T lymphocytes are more often found at the tip of the villi than at the base, and the concentration of these lymphocytes in architecturally normal villi may help to distinguish between latent GSE and non-specific increase.18,22
Immunophenotype of IEL
The normal population of IELs consists of T cells that can be divided into several subgroups on the basis of their T cell receptors (TCRs) and surface coreceptors. In normal duodenal biopsy specimens, most IELs are CD3 and CD8 T lymphocytes, mostly bearing TCRαβ, whereas CD4+ IELs are few in number.22 A second minor subgroup (15%) expresses a distinct TCR, the TCRγδ, expressing CD8 inconstantly.35
Finally, all subgroups of IELs express an integrin of the β7 family, CD103, to enable their adhesion to epithelial cells.35
A subset of IELs, CD3+, CD4−, CD8− and TCRγδ+, has been found in patients with GSE, characterising about half of the IELs.22 The immunohistochemical analysis for IEL TCRγδ+ is as sensitive and specific as the villous-tip IEL count and results in effectively distinguishing other intestinal disorders from GSE,24 but its diagnostic role in early and latent GSE is still controversial.24 Furthermore, it is limited by the non-availability of an assay in formalin-fixed, paraffin-wax-embedded tissue.36
Finally, an increased IEL count in an otherwise normal small-bowel biopsy specimen is not specific for GSE and may be associated with many other conditions such as immunological disorders and the use of NSAIDs, lymphocytic or collagenous colitis and bacterial overgrowth. Patients with intraepithelial lymphocytosis, however, should be investigated clinically for GSE.36
In patients with active GSE, immunohistochemical studies have shown an increase in the IEL count, with T lymphocytes expressing either TCRγδ or TCRαβ and CD103.35
Gastric metaplasia
Duodenal gastric metaplasia (DGM) is defined as foci of gastric-type mucus-secreting cells interspersed between duodenal enterocytes (fig 3). These foci of gastric epithelial cells contain PAS-positive neutral mucin and lack a brush border.37 Despite structural analogy, the epithelium in the DGM differs from true gastric epithelium with respect to lectin composition. DGM is considered to be an acquired condition related to gastric acid injury and H pylori may also be associated in its pathogenesis.37 DGM can be divided into three types according to the amount of mucus in the metaplastic cells: complete, intermediate and incomplete.38 Tall, mucin-abundant cells characterise the complete type. In contrast, the incomplete type is dark with cuboidal cells poor in mucin, with the characteristics of the intermediate type being between these two types. H pylori is often seen colonising the incomplete type of DGM.38

Focal gastric metaplasia. Enterocytes are replaced by foci of gastric-type mucus-secreting cells. Villi are shortened and blunted. The lamina propria shows an increase in the inflammatory cells (lymphocytes and plasma cells), associated with the hypertrophy and prolapse of Brunner’s glands. These features are typical of non-specific chronic duodenitis (haematoxylin–eosin staining, ×100).
DGM is associated with a progressive flattening of the mucosal surface. The villi become initially flattened, then widened and finally bulbous in shape. As a result, if H pylori is present, this progressive process can lead to inflammation and duodenitis.39
Gastric metaplasia in the duodenal bulb is an acquired non-specific response to mucosal injury resulting from gastric acid. H pylori may increase gastrin and gastric acid secretion.37 Gastric acid secretion and, consequently, acid loading of the duodenal bulb are also related to the type and grade of chronic gastritis. Atrophic gastritis has been shown shown to protect against gastric metaplasia and inflammation of the duodenal bulb.37
PATHOLOGY
Inflammatory and lymphoproliferative disorders
Table 1 shows the differential diagnosis of inflammatory and lymphoproliferative disorders.
Differential diagnosis of inflammatory and lymphoproliferative disorders
Chronic non-specific duodenitis induced by H pylori
Duodenal inflammation can be secondary to various causes, and different pathological mechanisms may cause the same morphological appearance. Thus, duodenal inflammation can be divided into two main groups according to the aetiology: duodenitis secondary to H pylori infection (associated with chronic active gastritis and ulcer disease), also called chronic active duodenitis or chronic non-specific duodenitis or Hpylori bulbitis and duodenitis due to other causes such as GSE, Crohn’s disease, drugs, Whipple’s disease, parasitic infections or ulcerative colitis.40
Non-specific duodenitis or peptic duodenitis is a condition associated with acid injury.
H pylori infection has a role in the pathogenesis of the DGM and inflammation of the duodenal bulb.37 The prevalence of H pylori infection increases progressively with age, reaching a plateau after the fourth decade of life.41
Endoscopy shows DGM or chronic duodenal bulb inflammation to be associated with H pylori-positive chronic gastritis, villous atrophy of the distal duodenal mucosa (ie, GSE), duodenal ulcer and duodenal bulb deformity and scarring.37 DGM and duodenitis are not age related and are independent of the use of NSAIDs.37
DGM and H pylori are both usually found in the proximal duodenum. H pylori colonises the duodenal mucosa only in areas of gastric metaplasia and such colonisation leads to a chronic active duodenitis.21,42,43 Madsen et al42 showed chronic active duodenitis to be associated with H pylori in 94.1% cases.
H pylori colonisation of the duodenal bulb may affect the pathogenesis of duodenal ulcer.43,44 A much higher prevalence and extent of DGM and H pylori in the duodenal bulb in patients with duodenal ulcer than in those with gastric ulcer or chronic gastritis supports this hypothesis.44H pylori is associated with duodenal ulcer: 90% of the patients with duodenal ulcer are infected by H pylori.45
Only a small percentage of cases of duodenitis are associated with the use of NSAIDs. Clearly, however, patients with duodenal ulcers of unknown aetiology may be more common than previously believed. H pylori-negative duodenal ulcers are associated with older age, pre-existing malignancy, recent surgery, underlying sepsis and NSAID usage. Only 13% of patients with H pylori-negative duodenal ulcers, however, had a history of NSAIDs, suggesting that other risk factors, such as stress secondary to surgery or to sepsis, may have a key role in the development of ulcer.45
Gastric metaplasia of intestinal crypts is well recorded in chronic ulceration of the small intestine from any cause such as Crohn’s disease or ingestion of potassium tablets.21
Histological features of chronic non-specific duodenitis
Mononuclear cells such as lymphocytes and plasma cells are normally present in the lamina propria of the duodenum. Thus, their presence is not considered to be diagnostic for chronic duodenal inflammation.37 The diagnosis of duodenitis is made when there is infiltration by inflammatory cells with changes in villous architecture and surface and crypt epithelium. Duodenitis can be graded according to the amount of neutrophilic and plasma cell infiltration, villous height, Brunner’s gland hyperplasia with prolapse into the lamina propria and gastric metaplasia46 (fig 3). Duodenitis can show a spectrum of mucosal changes. Mild duodenitis is characterised by a small increase in the number of chronic inflammatory cells in the lamina propria, associated with slight widening and flattening of villi, whereas severe duodenitis shows an intense, mixed acute and chronic inflammatory cell infiltrate of the lamina propria and infiltration of polymorphonuclear neutrophils into the surface epithelium, together with changes in the mucosal architecture: DGM and increasing flattening of the villi.21 Moderate duodenitis is defined by a severity that is between mild and severe.39
The activity of duodenitis is dependent on the neutrophilic infiltration.39,46 Heavy polymorphonuclear invasion is associated with epithelial degeneration, with cytoplasmic vacuolisation, intercellular oedema, and frequent microerosions and true erosions. H pylori is often, but not always, present in this degenerated epithelium.39
DGM and inflammation of the duodenal bulb may be associated with villous atrophy of the mucosa of the distal duodenum.37
DGM can also be found in 13%48 to 42% of children infected with H pylori.47 Duodenitis seems to be the only feature associated with DGM development and is not a consequence of H pylori infection.48 A high prevalence of DGM and duodenitis is found in children infected with H pylori, but duodenal ulceration does not seem to be related to the presence of DGM and duodenitis.48
Histological assessment for duodenal H pylori seems to be less reliable than culture.49
Differential diagnosis of chronic non-specific duodenitis
The differential diagnosis of duodenitis includes mainly GSE. In peptic duodenitis, prominent foci of polymorphonuclear leucocytes and villous atrophy may be difficult to distinguish from the changes seen in GSE.21 In addition, typical features of GSE may coexist with infiltration of the polymorphonuclear leucocytes in the lamina propria, in the crypts and extending focally into the surface epithelium, and with focal DGM.21
Features useful in distinguishing peptic duodenitis from GSE include the relative lack of architectural changes in non-specific duodenitis, the scanty polymorphonuclear leucocyte infiltrate and the absence or focal presence of gastric metaplasia in GSE.21
Severe inflammation, however, may be very difficult to distinguish from GSE and some assessment of IEL, together with the clinicopathological correlation, is the best way to distinguish between the two different causes of inflammation in the duodenum.21
Active duodenitis is less common in patients taking NSAIDs, but is strongly associated with gastric metaplasia, H pylori-positive gastritis and duodenal ulceration.46
Eosinophilic duodenitis
Eosinophilic gastroenteritis is manifested by eosinophilic infiltration of the gastrointestinal tract and peripheral eosinophilia. Three main diagnostic criteria are used: (1) the presence of gastrointestinal symptoms; (2) biopsy specimens showing eosinophilic infiltration of one or more areas of the gastrointestinal tract; and (3) no evidence of parasitic, intestinal or extraintestinal disease. The aetiology remains unclear, although an association with various allergic diseases such as asthma, food sensitivities and eczema has been reported. The age of the patients is variable and the disease is diagnosed in children as well as in adults. An increase in the eosinophil count may occur secondarily in inflammatory bowel disease, autoimmune diseases, as a reaction to drugs, infections, hypereosinophilia syndrome and after solid-organ transplantation.
Eosinophils are normally present in the lamina propria. The precise histological criteria required to diagnose eosinophilic gastroenteritis are ambiguous.
Eosinophilic gastroenteritis may have a patchy disease distribution or the mucosa is spared altogether, as in muscular and serosal types of eosinophilic gastroenteritis. Degranulated eosinophils and eosinophil cationic protein in the intestinal mucosa are seen along with histological damage in eosinophilic gastroenteritis.
The duodenum may be affected with other segments of the gastriontestinal tract.
Histological features of eosinophilic duodenitis
The architecture is variably perturbed and numerous eosinophils are seen in the lamina propria, forming clusters and infiltrating crypts and the surface epithelium. Many of them may also be degranulated. Intermixed neutrophils, plasma cells and lymphocytes are also seen. Eosinophilic microabscesses are rarely seen.
An increase in the eosinophil count may also be found in other conditions such as GSE and food allergy.50
Crohn’s disease
The exact frequency of the stomach and duodenum being affected in adult patients with Crohn’s disease is not known. In referral centres, however, endoscopic and histological observation may show evidence of disease in 34–83% of these patients.9
Histological features of Crohn’s disease
The typical finding in duodenal (40%) and gastric (31%) biopsy specimens of H pylori-negative patients with Crohn’s disease is focal acute inflammation flanked by almost normal-appearing mucosa. Focal acute inflammation has been defined as a cluster of at least two neutrophils in the lamina propria or epithelium, with 2–3 foci in a piece of tissue.9 Although this is not a sensitive feature in Crohn’s disease, it has high specificity (92%) and high predictive value (93–95%).9 High positive predictive values are also associated with acute inflammation found in the surface epithelium and deep stroma of the duodenum, which may represent precursors of aphthoid ulcers. The duodenum is often affected by acute inflammation, either alone (18.4% of the H pylori-negative patients) or with the stomach (18.4%), whereas acute inflammation limited to the stomach is seen in only 10% of cases.9
The incidence of granulomas is variable (0–83%), depending on the age of the patients and duration of the disease, being more common in younger patients and in those with a shorter duration of disease.9
Although uncommon, granulomas are found less often in the duodenum than in the stomach;9,51 they, however, have a positive predictive value of 100%, with low sensitivity (6%).9 They tend to be associated with a nearby acute inflammation and may be more common near aphthous ulcers or associated with the gastric metaplasia.9
Yao et al51 found gastric and duodenal microaggregates of 5–10 epithelioid cells in all the patients who had granulomas and in the non-inflamed gastroduodenal mucosa of patients with Crohn’s disease. The 67% of patients with Crohn’s disease who had an apparently normal gastroduodenal mucosa endoscopically showed such microaggregates histologically.51
According to Yao et al,51 immunostaining with only one monoclonal antibody (CD68) applied to a single section of several biopsy specimens is simple and highly specific for distinguishing between Crohn’s colitis and ulcerative colitis, and much more sensitive, compared with conventional light microscopy detecting granulomas only.
Wright and Riddell9 found chronic inflammation with plasma cells in 69% of the duodenal biopsy specimens of H pylori-negative patients with Crohn’s disease.9 Gastric metaplasia is not a common finding; when present, however, there should be a careful examination to exclude H pylori.9
Other findings such as villous atrophy, erosions and eosinophils, and superficial or deep plasmacytosis may be present, but these are not important. The IEL count is normal.9
Differential diagnosis of Crohn’s disease
Differential diagnosis can be GSE, H pylori infection of the stomach or duodenum, other infections, NSAIDs or Zollinger–Ellison syndrome.9 A biopsy specimen from the stomach also permits the ruling out of parietal cell hyperplasia that is seen with Zollinger–Ellison syndrome, which is a rare cause of H. pylori-negative acute duodenitis.9
Gluten-sensitive Enteropathy
GSE or coeliac disease is considered to be an autoimmune enteropathy in susceptible people, triggered by the ingestion of gluten-containing grains.52 It has a genetic background, being associated with HLA-DQ2 and HLA-DQ8. The pathogenesis entails a T cell-mediated immune response and autoreactive B lymphocytes that produce autoantibodies directed against tissue transglutaminase or endomysium.52
Because of the protean nature of the disease, the exact prevalence of GSE is still underestimated and the correct diagnosis is directly related to the criteria used.52 The prevalence is variable in different countries, ranging from 1 in 70 to 1 in 550 people, with an estimated worldwide prevalence of 1 in 266.52
The clinical presentation varies with the age of the patient, the duration and extent of the disease and the presence of extraintestinal disease.52 Three forms of GSE are described. The classic form, characterised by gastrointestinal symptoms such as diarrhoea, abdominal distension and malabsorption, is diagnosed in patients aged 6–8 months, after the introduction of weaning foods in the diet.52 Pathological changes are mainly found in the duodenal mucosa and in the upper jejunum, but in some cases the entire small intestine may be affected. The histological spectrum of the lesions ranges from a slight villous flattening to a decreased V:C ratio, crypt hyperplasia, variably increased plasma cell and lymphocyte infiltration in the lamina propria and a marked increase in the IEL count.
The atypical form of GSE is characterised by extraintestinal symptoms such as dermatitis herpetiformis, iron-deficiency anaemia, short stature, dental enamel hypoplasia, arthritis and arthralgia, chronic hepatitis and hypertransaminasaemia, osteoporosis, idiopathic cerebellar ataxia, delayed puberty, recurrent miscarriages and reduced fertility.
The asymptomatic or silent form is characterised by the presence of changes in the mucosa, probably limited to the upper tract of the small intestine. Careful clinical investigation can, however, disclose subtle symptoms.52 The potential or latent form shows isolated positivity of coeliac serology at first testing and the typical intestinal damage later in life.53 Patients with GSE who do not comply with a GFD have persistent mucosal damage and may develop complications such as gastrointestinal malignancies, principally lymphoma.
The diagnostic protocol is based on the following:
-
History and clinical presentation
-
Serological screening (tTGA, EMA and anti-gliadin antibodies)
-
Histological findings
-
Obvious clinical and serological response to a GFD
-
Age >2 years
-
Exclusion of other clinical conditions mimicking GSE.52
A single duodenal biopsy, followed by a favourable response to the GFD, is sufficient to confirm the diagnosis.52
A recent study on a paediatric population proposed a duodenal biopsy for conclusive diagnosis in children with a tTGA titre <100 U (results of <20 U or between 20 and 100 U) and negative IgA. Patients with a tTGA titre >100 U should be considered to be positive for GSE, without evaluating a duodenal biopsy specimen. However, a biopsy specimen should be taken if patients do not experience any improvement in symptoms with the GFD. Patients with a normal tTGA titre (<20 U) with highly suggestive symptoms or predisposition to GSE should also undergo biopsies.54
On the other hand, antibody titres may be normal in up to 5% of all patients with GSE, in 20–30% of those with early mucosal changes22 and in 20–50% of patients, mostly adults, who do not present with obvious symptoms of malabsorption. In these instances, duodenal and jejunal biopsies are an essential diagnostic tool.22 GSE has a wide spectrum of histological abnormalities, ranging from normal villous architecture to total villous atrophy.
The biopsy can also confirm the diagnosis or suggest it in patients with atypical presentation or when the serology does not support the diagnosis. Once the diagnosis is established, the biopsy is a useful tool to follow up adherence to a GFD in patients with unsatisfactory clinical response, and also to detect compliance.22
Pathogenesis of the small intestine damage can be divided into three phases: (1) an infiltrative phase characterised by an increase in the IEL count; (2) a hyperplastic phase characterised by crypt hyperplasia; and (3) a destructive phase, characterised by progressive villous atrophy, leading to a flattened mucosa.
The current histopathological diagnosis is made using the Marsh Classification28 and consists of a four-stage grading system with 40 IELs per 100 epithelial cells as the normal upper limit:
-
Type I: infiltrative lesion, characterised by intraepithelial lymphocytosis and a normal villous architecture of the duodenal mucosa
-
Type II: hyperplastic lesion, characterised by intraepithelial lymphocytosis and crypt hyperplasia, with a normal villous architecture
-
Type III: destructive lesion, characterised by intraepithelial lymphocytosis, crypt hyperplasia and villous atrophy
-
Type IV: hypoplastic lesion, characterised by a normal IEL count, normal crypt length and villous atrophy (fig 4).

Diagrammatic representation and comparison of the different classification proposed in gluten-sensitive enteropathy. V:C, villous to crypt ratio.
Oberhuber et al7 modified this classification by splitting the type III lesions in three substages: (A) mild villous atrophy, (B) marked villous atrophy and (C) completely flat mucosa (fig 4). This modification, however, has reproducibility problems. Recently, a new classification with three grades was proposed by Corazza and Villanacci.55 Marsh–Oberhuber’s type I infiltrative lesion is maintained; the normal upper limit of IELs is 25 IELs per 100 epithelial cells and CD3 immunostaining is carried out on biopsy samples lacking villous abnormalities (grade A). The type II hyperplastic lesion is rarely seen and regression from villous atrophy to isolated crypt hyperplasia has never been shown after treatment. Oberhuber stage IIIA and IIIB are grouped into a single stage and considered to be a single diagnostic category (grade B1). In fact, grading the villous atrophy into mild or marked can result in considerable interobserver and intraobserver variation. Stage IIIC, often seen and considered to be the diagnostic feature of GSE, is maintained in the revised classification as grade B2.
Marsh–Oberhuber’s type-IV hypoplastic lesion in virtually never seen and was made obsolete by the recent finding of an aberrant IEL clone that is characteristic of refractory sprue, ulcerative jejunoileitis and enteropathy-type intestinal T cell lymphoma. Thus, this classification divides lesions seen in GSE into non-atrophic (grade A) and atrophic (grade B); grade B is further split into grade B1 when the V:C ratio <3:1 and grade B2 when the mucosa is flat and no villi are present55 (fig 4).
The validity, reproducibility and accuracy of this classification, however, are yet to be proved.
In patients with GSE, the response to a GFD is characterised by an improvement in clinical symptoms and mucosal damage. The clinical improvement may occur in days, whereas the mucosal damage may take up to 2 years. The healing of the mucosa occurs more rapidly in the distal part of the small bowel and is characterised by an increase in villous size, reduction in crypt hyperplasia and reduction in the IEL count with raised γδ T cells. A reduction in the IEL count and an improvement in the V:C ratio are observed, although they may not normalise, indicate a favourable response to the GFD. An abnormal histopathological appearance may persist in many patients who are on a GFD.19
Refractory GSE (refractory sprue, unclassified sprue)
The term refractory sprue is often used generically and ambiguously to define a pathological condition affecting the small bowel, which histologically resembles GSE.
It is correctly defined as symptomatic severe small-intestinal villous atrophy mimicking GSE, not responding to at least 6 months of a strict GFD.56
The diagnosis of refractory sprue is rare and should be made in patients with GSE after unresponsiveness to a strict GFD and after exclusion of any other disorder mimicking GSE.35 Refractory sprue can be divided into primary and secondary. An initial resistance to the GFD characterises primary refractory sprue, whereas secondary refractory sprue is defined by an initial response to the GFD followed by a relapse.56 Thus, primary refractory sprue may erroneously include many different pathological conditions lacking any relationship to GSE.
A strict GFD for 12 months is considered to be a reasonable period of waiting for mucosal improvement before making a diagnosis of refractory sprue.
The prevalence of refractory sprue has been estimated to be around 7–8%.57
The male to female ratio is 1:3.2 and the mean age of patients is 51 years.56 Patients present with diarrhoea, abdominal pain, weight loss and microcytic anaemia.35,56 An initial diagnosis of GSE may be made because of the villous atrophy with an increased IEL count. Anti-gliadin or EMA are often found before the GFD, but disappear during the diet. The association with HLA-DQ2 phenotype suggests that refractory sprue is related to GSE.56 Associated conditions are collagenous sprue, ulcerative jejunitis, hyposplenism, mesenteric lymph node cavitation, lymphocytic colitis, collagenous colitis and dermatitis herpetiformis.56
Histological features of refractory sprue
Architectural changes in the duodenal biopsy specimen range from partial to total (grade IV) villous atrophy.35 The mucosa contains a diffuse and dense mononuclear infiltrate of mainly plasma cells in the lamina propria and a massive increase in the IEL count. The IELs and lymphocytes in the lamina propria are normal to medium in size, with a normal cytological appearance.35
In refractory sprue, most IELs have an abnormal phenotype, characterised by intracytoplasmic CD3ε and CD103, but a loss of expression of TCR, CD3, CD4 or CD8 on their cell surface in 52–98% of cases56 and they show a restricted rearrangement of the TCRγ gene.35 Clonal TCRγ gene rearrangement is expressed in as many as 75% of patients with refractory sprue. The lamina propria CD3+ T cell population is a mixture of CD4 and CD8 cells.58
On the other hand, in specimens from untreated patients with active GSE, the number of IELs that express CD103, CD7, CD3, TCRαβ and CD8 is markedly increased compared with those of controls, but most IELs express TCRαβ or TCRγδ and CD8 or CD4,35 and there is no TCRγ gene clonal rearrangement.56
A simple immunohistochemical method using anti-CD3 and anti-CD8 antibodies on paraffin wax sections has been suggested to distinguish between GSE and refractory sprue. Its utility in clinical practice, however, is yet to be proved.59
CD30 expression by IELs of patients with refractory sprue indicates a poor prognosis, and it has been associated with the presence of overt enteropathy-associated T cell lymphoma60 or enteropathy-type intestinal T cell lymphoma (EITCL), which is the preferred term for this condition.61,62
Immunohistochemical negativity for several antigens that are normally found on IELs, such as CD8 or the TCRβ chain, in combination with clonal T cell populations by polymerase chain reaction may help in identifying refractory sprue with malignant transformation.63
Although a morphologically identifiable tumour is absent, the presence of an abnormal T cell population is now diagnosed as crypt EITCL, an early intraepithelial form of EITCL.56,62,64
Enteropathy-type intestinal T cell lymphoma
Lymphomas of the small intestine are usually of T cell origin and tend to be a complication of long-standing GSE.65 In 50% of cases, the patient presents with an EITCL, whereas the underlying GSE is still dormant.65 The annual incidence rate is 0.5–1 per million people in Western countries. This is a rare form of malignancy, accounting for around 35% of all small-bowel lymphomas.66
Patients in their fifth or sixth decade present with abdominal pain, diarrhoea and weight loss secondary to malabsorption, signs of obstruction or even (spontaneous) perforation or haemorrhage.58,65 A palpable tumour may be found.
Macroscopic observation showed EITCL to be often multifocal, with ulcerative lesions, with a high perforation rate at presentation or during chemotherapy.65
The T cell lymphomas of the small bowel are roughly divided into those with enteropathy and those without.65
Histological features of EITCL
The architecture is distorted, with villous atrophy and ulcerations. An atypical population of neoplastic lymphocytes infiltrates the mucosa. Lymphoma cells may consist of pleomorphic medium to large cells that are CD3+, CD4− and CD8−, or of small and monomorphic cells that are CD3+, CD4−, CD8+ and CD56+. The neoplastic cells also contain T-cell Intracellular Antigen 1 cytotoxic granules.58,65
The adjacent intact mucosa shows the histological features of GSE, a variable grade of villous atrophy with marked increase in IEL count,58,65 where the percentage of CD4− and CD8− IELs ranges from 48% to 86% and from 7% to 18% in pleomorphic and monomorphic lymphomas, respectively. In monomorphic lymphomas, most CD3+ IELs express both CD8 and CD56.58
The tumour cells of EITCL virtually always express CD30. CD30+ IELs are present in the tissue adjacent to or merging with overt lymphoma and are scattered in villi a long way away from such tumours and even in jejunal biopsy specimens.60 This marker has been associated with a poor outcome.60
The immunophenotype is not absolutely specific, however; CD3 may be lacking, CD8 may be positive and CD30 may be negative.65
The same monoclonal T cell population is present in intact mucosa, benign-appearing ulcers and overt lymphomas. The multifocality of the monoclonal IELs suggests that crypt EITCL affects the entire length of the small intestine.
Little is known about T cell lymphomas of the small intestine without enteropathy.
Immunoproliferative small-intestinal disease
Immunoproliferative small-intestinal disease (IPSID) is a mucosa-associated lymphoid-tissue lymphoma, characterised by infiltration of the bowel wall with a plasma cell population that secretes a monotypic, truncated immunoglobulin αheavy chain lacking an associated light chain.67–69 The so-called non-secretory IPSID variant is characterised morphologically by the proliferation of small centrocyte-like lymphoid cells lacking the extreme plasmacytic differentiation.70
IPSID principally affects young adults with approximately equal incidence in both sexes, predominantly affects the duodenum and jejunum and tends to be associated with chronic diarrhoea and abdominal pain.70
Most cases reported are from the Middle East, North and South Africa and the Far East. Sporadic cases are reported in other regions, usually in immigrants from high-prevalence regions.70 Patients usually present with intermittent diarrhoea and abdominal pain and symptoms related to malabsorption. Obstruction and abdominal masses are typical of the advanced stage. The final diagnosis is usually established by endoscopic biopsies or laparotomy.
In early disease, the duodenal mucosa may appear normal. Thickening, erythema and nodularity of the mucosal folds may be seen in the duodenum and upper jejunum.70 The stomach is rarely affected.70
Histological features of IPSID
The spectrum of the histopathological lesions ranges from apparently benign lymphoid infiltration to malignant, diffuse, large B cell lymphoma.71
The duodenal and jejunal biopsy specimens show a dense infiltrate of dysmorphic plasma cells and centrocyte-like lymphocytes in the lamina propria, with villous blunting or villous atrophy.70,71 The overlying epithelium is usually intact and crypts are spared. Lymphoepithelial lesions caused by centrocyte-like lymphocytes are, however, present. Immunohistochemical studies show that the plasma cells are CD20−, whereas the centrocyte-like lymphocytes are CD20+. The cytoplasm of both types of cells shows intense staining for immunoglobulin αheavy chain, with no detectable expression of light chains or surface immunoglobulin.71 Low-grade IPSID may progress to higher-grade large-cell lymphoplasmacytic and immunoblastic lymphoma. This is characterised by an increment in the atypia of plasma cells arranged in aggregates, and later by sheets of dysmorphic plasma cells and immunoblasts invading into the submucosa and the muscularis propria.70
CD4 T cell lymphoproliferative disorders
This is a rare condition characterised by a diffuse infiltration of the small intestine by monoclonal CD4 T lymphocytes, αβ subtype.72,73 Symptoms include long-standing chronic diarrhoea, malabsorption, exudative enteropathy and weight loss, without any association with abdominal mass or peripheral lymphadenopathy.72,73 Although this condition can clinically mimic GSE, the absence of anti-gliadin antibodies, EMA and tTGA, and the unresponsiveness to a GFD, excludes the diagnosis.72,73 The outcome is variable and the disease has a slow progression, regardless of the response to chemotherapy. The mean age of the patients is 49.4 (range 28–60) years,73,74 and the disease occurs predominantly in men (5:1).72,73
Histological features of CD4 T cell lymphoproliferative disorders
The architecture is preserved or minimally distorted. Intestinal villi are slightly blunted, with preservation of the crypt architecture.72,73 The IEL count is usually within normal limits (17–30 IELs/100 epithelial cells) but variable in different areas and there is no evidence of lymphoepithelial lesions.72 Enterocytes, however, may show cytoplasmic vacuolisation and flattening.72 A lymphoid infiltrate homogeneously affects the duodenum and jejunum. It consists of a dense, diffuse abnormal population of small pleomorphic lymphocytes in the lamina propria, with variable permeation of the superficial part of the submucosa.72 The small lymphocytes, which show a pleomorphic-indented nucleus, are mixed with polymorphonuclear eosinophils and may be associated with non-caseating granulomas.72 The lymphocytic population shows a clonal rearrangement of the TCRβ, positivity to CD2, CD3, CD5, CD7 and CD4 and negativity to CD8, CD103 and CD57.72,73 Scattered CD20+ B lymphocytes are found only in the lamina propria.73
Autoimmune enteropathy
Autoimmune enteropathy is a condition characterised by villous atrophy, indistinguishable from that of GSE but unresponsive to a GFD. The classic criteria for the diagnosis are histological evidence of enteropathy, a lack of any triggering food protein, presence of anti-enterocyte antibodies, persistent diarrhoea after prolonged fasting and presence of organ-specific autoantibodies.74 Anti-gliadin antibodies may be present.76 HLA-DQ2 may be found, being generally associated with autoimmune diseases.76 Under this name, however, we can group different conditions that are characterised by the presence of autoantibodies against various cellular components in the small bowel.
These autoimmune conditions usually occur in children75 and rarely in adults.76,77 Clinically, patients present with chronic diarrhoea and malabsorption. This condition may also be associated with colitis.77 In adults, a possible association between the autoimmune enteropathy and a hepatitis C virus infection, believed to be a trigger for autoimmune diseases, has been reported.77 Patients have a family history of autoimmune diseases.77
A recessively inherited defect of the small intestine is characterised by intractable infantile diarrhoea, family history of sibling death from chronic diarrhoea, opportunist infections (of the respiratory tract) associated with a defective T cell activation and autoantibodies, anti-enterocytes and anti-goblet cells.78 Serum autoantibodies can be directed against enterocytes or goblet cells and different immunological changes (either a T cell abnormality or immunoglobulin deficiency) may favour the appearance of gut epithelial cell autoantibodies.79–83
Histological features of autoimmune enteropathy
The duodenal biopsy specimen is characterised by varying degrees of architectural changes, ranging from normal to mild, patchy, villous blunting to partial or total villous atrophy.77,83 Crypts may be normal or hyperplastic.83
The histological findings in the jejunal biopsy specimen show villous blunting with normal crypts and a dense mucosal inflammatory infiltrate. When autoantibodies against goblet cells are present, the small bowel and the colon are strikingly characterised by goblet cell depletion.78
Immunohistochemically, the mucosal inflammatory infiltrate has CD2, CD3, CD4 and CD8 lymphocytes. The IEL count may be normal or increased76,77 and is predominantly represented by CD8.78 The number of γδ+ lymphocytes in the lamina propria or epithelial compartment is normal,78 which helps in distinguishing autoimmune enteropathy from GSE.
The differential diagnosis is GSE with food intolerance or allergy enteropathy.
Food allergy
Food allergy may produce a wide variety of patchy or diffuse mucosal lesions in any part of the gastrointestinal tract. The mucosal pathology may manifest as oesophagitis, gastritis, mild villous atrophy or colitis.81
Lymphonodular hyperplasia of the duodenal bulb is found in people with untreated food allergy and in people on an elimination diet.84
The lesion tends to be most prominent on the duodenal bulb just after the pylorus and spreads to the distal duodenum in only a few patients.84
Villous atrophy, even partial villous atrophy, is not found in patients with food allergy, although crypt hyperplasia and an increase in the eosinophil count may be observed in the lamina propria in both untreated and treated patients. These features are non-specific, however, and are also found in patients with GSE.84
A considerable increase in the density of γδ+ IELs of the duodenal mucosa may be present in children even beyond infancy and characterises the active and untreated phase of food allergy.
Cow’s milk protein-sensitive enteropathy
CMSE may also affect school-aged children and may be responsible for unexplained and prolonged gastrointestinal problems in young adults.
Although the pathogenesis does not seem to be mediated by IgE, EMA, HLA-DQ2 or HLA-DQ8, and duodenal villous changes are not seen in these patients, the duodenal IEL count expressing T-cell Intracellular Antigen 1, perforin and granzyme A is increased, however, suggesting the association of abnormal cytotoxic lymphocytes.30
Lymphonodular hyperplasia without villous atrophy, mainly found in the bulb of the duodenum, characterises CMSE endoscopically. This lymphoid enteropathy does not seem to cause malabsorption and it is not specific to this condition.
Histological features of CMSE
Histological features are not specific, as they can also be seen in the early phase of GSE. The villous architecture is normal29 and there is an increase in CD3+, αβ+ and γδ+ IELs, which is less prominent than in GES. Although not exclusive to CMSE, another histological feature consists of lymphoid follicles with reactive germinal centres, which are also found in the terminal ileum and colon.29
Thus, the dilemma in differentiating CMSE from GSE may exist at the presentation of GSE, when the typical lesion is infiltrative and characterised only by an increase in the IEL count. The IEL count in GSE is much higher and most prominently increased in the duodenal bulb. Granzyme B expression by lymphocytes is increased only in GSE.
Biopsy specimens from patients with CMSE from the bulb of the duodenum usually show a normal villous architecture; if any villous atrophy is present, however, it is less prominent than that seen in GSE.
The location of lesions is more variable in patients with CMSE and extends to all parts of the gastrointestinal tract in some patients.
In CMSE, the cytotoxic IEL count is increased in the descending part of the duodenum but not in the bulb. In GSE, the most severe villous changes are located in the most proximal parts of the intestine.30
Infections
Table 2 lists the common infections seen in the duodenum.
Common infections seen in the duodenum
Viral gastroenteritis
Viral gastroenteritis may be responsible for a duodenal injury in children and adults, with morphological features resembling GSE. Patients may present with diarrhoea, steatorrhoea, weight loss and flu-like symptoms. Anti-gliadin antibodies may be slightly increased and the improvement of the symptoms is unrelated to gluten abstinence or ingestion.
Histological features of viral gastroenteritis
The duodenal biopsy specimen shows the typical features of GSE: moderate to marked villous atrophy with numerous crypt mitoses and an increase in IEL count and intramucosal lymphocytes. The IEL phenotype is CD3+CD4+ or CD3+CD8+, with a variable admixture of the two cell populations. The percentage of CD4−CD8− IELs is small. There is complete recovery with normal morphology.85
Giardiasis
Giardiasis is defined as a symptomatic or asymptomatic infection by the flagellated parasite G lamblia.8
G lamblia is the most common protozoan isolated from the gastrointestinal tract. The annual incidence is variable, being greater in the population with poor hygienic conditions or in immunocompromised patients.3 Giardiasis is distributed equally among men and women;8 however, a predominance in men was reported in one study.86
The clinical symptoms and histological changes seen in duodenal biopsy specimens show major differences.8
Although patients tend to present with non-specific symptoms such as diarrhoea and anaemia, patients without diarrhoea have also been described.3
The presence of trophozoites in faecal and duodenal biopsy specimens confirms Giardia infection.8G lamblia is binucleate, has a ventral disc, four pairs of flagella, measures 5×20–30 μm and resembles a pear cut lengthwise.8
Trophozoites have been found in duodenal (82.5%) and jejunal (2.1%) mucosa and also in gastric antral (8.7%) and ileal mucosa (12.1%) but rarely in the colon (0.4%).88 The severity of duodenal colonisation is variable.8
Histological features of giardiasis
In the duodenal biopsy specimen, Giardia is found among the duodenal villi, attached to the mucosa without invading it. Rarely, however, the colonisation may be severe, with mucosal invasion by trophozoites87 (fig 5). The mucosa has a normal appearance (96.3%), although mild villous flattening and mild inflammation of the lamina propria may be seen occasionally (3.7%).86 The mononuclear cell component in the lamina propria is usually normal,8 but intraepithelial neutrophils, infiltration of the lamina propria with plasma cells and eosinophils have rarely been described.88 The mean IEL count is not markedly increased, average 24.5 (range 10–66) per 100 epithelial cells, but may be increased in some cases.8

Giardia lamblia on the surface of the villi. The trophozoites are variable in shape. The surface epithelium is morphologically unremarkable (haematoxylin–eosin staining, ×400).
Furthermore, reactive lymphoid follicles may also be found.8 Some changes are related to the density of Giardia colonisation—for example, depletion of the goblet cells and the density of plasma cell infiltration in lamina propria.88
Giardia can be stained with Giemsa and toluidine blue stains.8
Whipple’s disease
Whipple’s disease is a rare multisystemic disorder caused by the bacterium Tropheryma whippelii.89–92 The disease occurs mainly in middle-aged men89 and the gastrointestinal tract is affected most often (80–90%). The most common symptoms include watery diarrhoea, steatorrhoea and colicky abdominal pain with weight loss, fever and night sweats.89 Joint symptoms are the most common extraintestinal manifestations, occurring in 90% of patients. The lungs, heart and eyes may be affected, as well as the central nervous system.89,92 Antibiotic treatment is mandatory and leads to rapid clinical improvement and remission in most patients.93
T whippelii is an intracellular bacterium observed mainly in monocytes or macrophages.92 In Whipple’s disease, the most severe changes are usually seen in the small intestine and mesenteric lymph nodes, where biopsy shows foamy macrophages.
Histological features of Whipple’s disease
The thickening of duodenal villi is seen, with the lamina propria packed with foamy macrophage with numerous, and strongly PAS-positive, diastase-resistant intracytoplasmic granules. PAS-positive macrophages may be seen in other conditions, including intestinal M avium intracellulare complex infection.90,92
In addition, dilated lymphatic channels and flattened villi may be present.92 The IEL count is increased and the CD4:CD8 ratio is decreased.94
A polyclonal antibody against the bacterium permits the detection and direct visualisation of T whippelii in paraffin-wax-embedded tissues.92 Immunohistochemistry stains the bacilli as coarse granular material in a distribution pattern similar to that seen with the PAS stain.92
After antibiotic treatment, the histological picture changes. The foamy macrophages migrate from the villi towards the deeper part of the lamina propria and rarely into the submucosa. The PAS-positive material detected in these macrophages is non-homogeneous, finely stippled and pale, rather than granular.92
The intensity of immunoreactivity also varies, showing similar or less intense staining than that before antibiotic treatment, but the granular pattern preserved.92 Because macrophages may persist for years after successful treatment, the finding of PAS-positive macrophages in biopsy specimens is not considered to be evidence of bacterial relapse.92
Other diagnostic procedures to confirm the diagnosis of Whipple’s disease include electron microscopy, which shows the distinctive trilaminar cell wall of T whipplei in phagolysosomes of histiocytes89,90 and polymerase chain reaction, which is sensitive but with a variable degree of specificity.92
The differential diagnosis includes chronic multisystemic infections and granulomatous disorders, including histoplasmosis and M avium intercellulare complex. The condition can also resemble sarcoidosis, protozoan and bacillary infections.92
An association between Whipple’s disease and G lamblia infection has also been reported and may be related to defects in the immune system.90,91
AIDS enteropathy
HIV enteropathy may be defined as atrophy with epithelial hypoproliferation and dysmaturation of enterocytes,20 which in turn impairs small-bowel absorption, causing diarrhoea and weight loss.95,96 However, no relationship between abnormalities of villous architecture and symptoms (diarrhoea), even after controlling for other variables such as enteric pathogens was found.97
The term idiopathic AIDS enteropathy defines a chronic diarrhoeal illness in patients with HIV infection, who lack an identifiable pathogen. HIV may be responsible for changes in the intestinal immune system, resulting in damage to the intestinal mucosa.20
In duodenal mucosa from patients with HIV infection, changes in the intestinal immune system are associated with both CD4 and CD8 T lymphocytes. Mucosal CD4 T cells are markedly depleted even in the early stages of the disease.21 Activated and resting CD4 T cells are similarly reduced. The loss of activated CD4 T cells may contribute to the partial villous atrophy.21
HIV infection is associated with decreased proliferation in the crypt.98,99,100,101 It is seen in late-stage disease and is a feature of impaired activation and a loss of lamina propria CD4 T cells. This may lead to a breakdown of the mucosal immune barrier, resulting in a variety of opportunist infections, and to malabsorption due to mucosal atrophy or enterocyte dysfunction.20
In contrast, the relative CD8 T cell count has been found to be consistently increased.20 The CD8 T cell-activated cytotoxic cells in the mucosa may recognise HIV antigens and may have a role in controlling HIV infection, but they may also damage the intestinal epithelium.20 Activation of CD8 effector cells may result in the production of proinflammatory and immunoregulatory cytokines such as tumour necrosis factor α and interferon γ.20 Increased levels of these cytokines may lead to villous atrophy with hyper-regeneration, probably mediated by the activation of mesenchymal cells and the production of matrix metalloproteinases.20 Villous architecture is normal, however, in 50% of the patients; villous flattening may be present but villous atrophy is not observed.98 Crypt depth is increased, but mitoses per crypt are normal.97
In addition, mononuclear cells in the lamina propria and enterochromaffin in the base of the crypts are infected with HIV.98,102 HIV may thus directly infect the bowel, raising the possibility that the virus causes some of the gastrointestinal disorders in patients with AIDS.98
Histological features of AIDS enteropathy
Histological features include normal villous architecture to partial villous atrophy, marked depletion in mucosal CD4 T lymphocytes, an increase in CD8 lymphocyte count and increased crypt depth with normal mitoses per crypt.
Gastrointestinal opportunist infections in HIV-positive patients
Microsporidiosis
Microsporidiosis is an opportunist infection seen in immunosuppressed organ transplant patients, those with AIDS and occasionally in immunocompetent patients as traveller’s diarrhoea.
Microsporidia are widespread obligate intracellular parasites; they were rarely seen in humans before the AIDS epidemic and are believed to cause about 50% of cases of chronic diarrhoea in patients with AIDS. Infection is seen only when the CD4 count is <100 CD4 T cells/ml.
The most common infections due to microsporidiosis are caused by Enterocytozoon bieneusi and Encephalitozoon intestinalis.
Patients with microsporidiosis present with chronic watery diarrhoea and malabsorption, as well as cholangitis and acalculous cholecystitis in immunosuppressed patients.
An E bieneusi infection is almost always restricted to the enterocytes of the small bowel and can be focal. E intestinalis infects the enterocytes of the small bowel and colon and also the macrophages and occasional endothelial cells in the lamina propria. The gastrointestinal infection is not exclusive, and both organisms can infect the epithelium of the biliary tree, gallbladder, nasal sinuses and the respiratory tract, but E intestinalis can also disseminate and cause granulomatous lesions in the kidney and the brain.
Histological features of microsporidiosis: In the small bowel, both types of microsporidia cause a partial villous atrophy, mild crypt hyperplasia with short blunt villi and a mild increase in lymphocytes, plasma cells and eosinophils in the lamina propria. Microsporidia are mainly seen in the enterocytes over the villi; their number decreases along the sides of the villi and they are never found in the crypts. The superficial enterocytes are disordered and degenerate with extrusion of infected cells. E bieneusi plasmodia resemble vacuoles in the supranuclear cytoplasm indenting the nucleus. These plasmodia contain clear slits or basophilic granules and are seen only in the enterocytes. The 1×1.5-μm-long, slightly basophilic spores may be seen in or on the surface of the enterocytes.27 The larger supranuclear parasitophorous vacuoles of E intestinalis contain sporonts, sporoblasts and spores, often indent the enterocyte nucleus and are also found in macrophages in the lamina propria. The spores of E intestinalis are larger, 1.2×2.2 μm in size, and more numerous than E bieneusi. In H&E-stained duodenal and terminal ileal biopsy specimens, the presence of microsporidia can be easily missed. Conversely, the Warthin Starry stain shows the developing stages and spores of both microsporidia species, whereas the Brown–Brenn Gram stain shows only the spores.27
Cyclosporidiosis
Cyclospora cayetanensis has a prevalence of 0.3–0.5% in healthy individuals. It has a worldwide distribution, particularly in the developing countries, in which it is endemic with a seasonal variation.
The incubation period is 2–11 days. Immunocompetent patients present with watery diarrhoea, abdominal cramps, vomiting, anorexia, weight loss, severe fatigue and, occasionally, a flu-like illness after having returned from developing countries.
In an HIV-positive patient, C cayetanensis produces prolonged diarrhoea, wasting and weight loss, but treatment with trimethoprim–sulfamethoxazole eradicates infection.
Histological features of cyclosporidiosis: The duodenal and ileal mucosa show villous blunting, mild crypt hyperplasia and variably increased chronic inflammatory cells in the lamina propria and a mild increase in the IEL count. The surface epithelium is irregular. In the apical cytoplasm overlying the tips of the villi, the enterocytes contain parasitophorous vacuoles (rounded and elongated fusiform, up to 6 mm in length), with C cayetanensis in various stages of its sexual and asexual life cycle.27
Isosporiasis
Isospora belli is an obligate, intracellular, coccidian, protozoan parasite and has a prevalence of 0.3–0.5% in healthy individuals. Isosporiasis has a worldwide distribution and is endemic in tropical developing countries, where it infects 15% of patients with AIDS, but it is rare in the USA (2%) and in Europe. Overseas travellers’ infections in developed countries are the main presentation. Clinically, immunocompetent patients present with acute self-limiting diarrhoea and enteritis, whereas patients with AIDS present with chronic watery diarrhoea. Transmission is by ingestion of oocyst-contaminated water or food and possibly by person-to-person contact.
Histological features of isosporiasis: The duodenal biopsy specimen shows non-specific changes, such as mild to moderate villous atrophy and crypt hyperplasia with increased inflammatory cells, especially eosinophils, in the lamina propria. The superficial epithelium is disordered with a loss of nuclear polarity. The microorganisms are rounded or elongated, banana shaped and show pale staining. They are found in the subnuclear cytoplasm of duodenal enterocytes of the villi, but not in the crypts. The organisms are usually found beneath the nucleus, transversally oriented to the superficial cytoplasm (the so-called “T” sign). Subnuclear vacuoles (20–30 μm), merozoites and more frequent sexual forms are present.27
Cryptosporidiosis
Cryptosporidium parvum is a protozoan. Immunocompetent patients present with acute, self-limiting diarrhoea, and immunocompromised patients, including patients with AIDS, present with chronic watery diarrhoea.
Cryptosporidiosis has a worldwide distribution and is endemic in developing countries, where it is found in more than 50% of patients with AIDS, but it is less frequent in the USA (15%). It is highly infectious, with waterborne, person to-person and zoonotic (including dairy cow) transmission, causes hospital and institutional epidemics and traveller’s diarrhoea.
Cryptosporidiosis may be found in the gastrointestinal tract in the stomach, duodenum, ileum, colon and rectal mucosa. In addition, it is seen in acalculous cholecystitis, ascending cholangitis and occasionally in the respiratory tract and oesophagus.
Histological features of cryptosporidiosis: Histological features in the duodenum are non-specific, with partial villous atrophy, crypt hypertrophy and increased chronic inflammatory cells, particularly eosinophils and plasma cells and occasional neutrophils in the lamina propria. The numbers of organisms, the intensity of neutrophilic infiltrate and epithelial degeneration are directly correlated. The organisms vary in size from 2 to 5 μm and may be seen along the brush border of the surface and crypt epithelium (fig 6). The maturing trophozoite is found beneath the enterocyte microvillous membrane in a parasitophorous vacuole.

Cryptosporidium on the epithelial surface. The epithelium shows degenerative changes and a mononuclear inflammatory infiltrate is seen in the surrounding lamina propria.
Variation in size and basophilia with pale apparent structures in each organism help to distinguish it from mucin droplets and apoptotic debris. Coinfection with CMV is common and CMV, mycobacteria and Giardia should be routinely excluded.27
Mycobacterium
Mycobacterial gastrointestinal infections in patients with AIDS are mostly caused by M avium intracellulare. People with mycobacterial gastrointestinal infections commonly present with diarrhoea, malabsorption and, often, fever. M avium intracellulare and M genavense infection can affect the whole gastrointestinal trait.
Histological features are characterised by an infiltration of pale macrophages packed with acid-fast and DPAS-positive curved bacilli. These macrophages often fill and distend the lamina propria of the duodenum, resulting in shortened, broad villi. In some cases, however, macrophages may be scant.
The acid fast stain differentiates mycobacterial infections from rare cases of Whipple’s disease and Rhodococcus equi. Well-formed granulomas with epithelioid histiocytes are uncommon. Coinfections with CMV, microsporidia and other organisms may be observed.27
Cytomegalovirus
CMV is considered to be an opportunist pathogen and it may be seen in the context of severe immunodepression, especially in HIV infection and AIDS. CMV is a common coinfection with atypical mycobacterial infection and giardiasis.103
Histological features of CMV infection: It is often seen in ulcers and other pathological conditions associated with granulation tissue, more commonly in nuclei of endothelial cells in small capillary-type blood vessels and in stromal cell nuclei rather than in epithelial cells. Venulitis, haemorrhage and oedema are present. Cytomegaly and intranuclear and intracytoplasmic inclusions in endothelial cells are accompanied by venulitis and a mixed inflammatory cell infiltration in the lamina propria. Leucocytes may also infiltrate the epithelium. Epithelial cells may show regenerative changes.
CMV has a central dense eosinophilic intranuclear inclusion and surrounding halo, giving an “owl’s eye” nuclear inclusion, and may also have basophilic, granular cytoplasmic inclusions (fig 7). Immunoperoxidase is useful to identify CMV-infected cells.27,100

Cells with cytomegaly show nuclear and cytoplasmic inclusions (haematoxylin–eosin staining, ×400).
Cryptococcosis
Gastrointestinal infection by C neoformans occurs usually in the setting of a disseminated infection and it is the most common systemic mycosis in patients with AIDS.
Histological features of cryptococcosis: Cryptococci can be seen in the lamina propria of the duodenum and other organs of the gastrointestinal tract, often with minimal or no inflammatory response. Villi may be shortened and blunted. C neoformans is easily recognised on routine H&E staining, but D-PAS or methanamine silver stains show narrow neck budding. D-PAS stains the body and the outer part of the capsule weakly. The mucicarmine stain gives a modest contribution to the diagnostic process.27
Visceral leishmaniasis
Visceral leishmaniasis is caused by the obligate intracellular parasite Leishmania donovani. Leishmaniasis is endemic to Spain, Portugal, Italy and southern France, where it is spread by a sand-fly vector. It is the third most common opportunist infection in patients with AIDS in Spain and Portugal. L donovani infects reticuloendothelial cells of the bone marrow, liver and spleen; and patients present with fever, hepatosplenomegaly and anaemia.
Histological features of leishmaniasis: The infection is characterised by an infiltration of macrophages in the lamina propria of the duodenum packed with copious 1–2-μm-long basophilic amastigotes in an identifiable parasitophorous vacuole. H&E stains the round to oval amastigote and shows a nucleus and bar-like kinetoplast visible under oil immersion lens, at ×100 magnification. An associated mild villous shortening and increase in plasma cells and other chronic inflammatory cells is seen, but no acute inflammation or tissue necrosis.27
Take-home messages
-
Interpretation and evaluation of a duodenal biopsy specimen requires clinicopathological correlation.
-
Good orientation of the biopsy specimen is essential for accurate histopathological assessment. A helpful method to have a well-oriented biopsy specimen is for the endoscopist to orient the specimen on a filter paper.
-
A well-oriented biopsy specimen should have at least 4–5 consecutive elongated, well-distended villi from the base to the tip. The evaluation of the villous:crypt ratio, the count and distribution of the intraepithelial lymphocytes (IELs) as well as the evaluation of the enterocytes in the tip of the villi is critical.
-
Different methods to evaluate the IELs have been reported and an increase in the IEL count is not specific for gluten-specific enteropathy.
-
Infections can be accompanied by subtle changes in the architecture and minimal inflammation.
Epithelial neoplasms
Neoplasms of the ampulla of Vater
The ampulla of Vater is an anatomical canal, which drains into the second portion of the duodenum and consists of the confluence between the distal parts of the common bile duct and the main pancreatic duct. These two structures are lined by a pancreatobiliary-type of epithelium. The duodenal surface of the papilla is covered by intestinal epithelium.104
Adenomas of the papilla of Vater including high-grade dysplasia seem to be associated with a high risk of exhibiting invasive carcinoma postoperatively and a high rate of recurrence. Recurrence is not associated with adenoma containing low-grade dysplasia after local resection. In contrast, recurrence of villous adenoma is present in 17% of cases and development of invasive carcinoma in 42% of cases with high-grade dysplasia. The overall risk of carcinoma after primary diagnosis of a high-grade dysplasic adenoma was 44% (14/32).15
Carcinomas of this region are differentiated into intestinal type, pancreatobiliary type and an unusual type, which includes signet-ring cell carcinoma and undifferentiated adenocarcinoma. Immunohistochemical expression of apomucin MUC2 helps in the distinction between intestinal and pancreatobiliary types.104 Of the intestinal-type carcinomas, 60% are CK20+/CK7−, 87% of the pancreaticobiliary-type are CK7+/CK20−; some carcinomas are, however, positive or negative for both markers. Carcinomas of the intestinal type or mixed pattern have a higher nodal stage than those of the pancreaticobiliary type.
Of the intestinal-type carcinomas, 92% expressed non-significant amounts CK20 and MUC2, whereas the pancreatobiliary type never stains with these two antibodies.
Neither histology nor any of these markers identifies a subgroup of tumours with a better or worse outcome, whereas prognosis of ampullary carcinomas depends on tumour stage, nodal stage and histological grade.104
The aberrant expression of KL-6 mucin is considerably related to unfavourable behaviours of the carcinoma of the ampulla of Vater.106
Villous adenomas of the duodenum are infrequent lesions of the gastrointestinal tract, but have a high risk of recurrence and malignancy.
CONCLUSIONS
The common disease processes encountered in evaluation of duodenal biopsy specimens have been provided. Figure 8 suggests an algorithmic approach as a guideline to diagnose the most common diseases in duodenal pathology.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
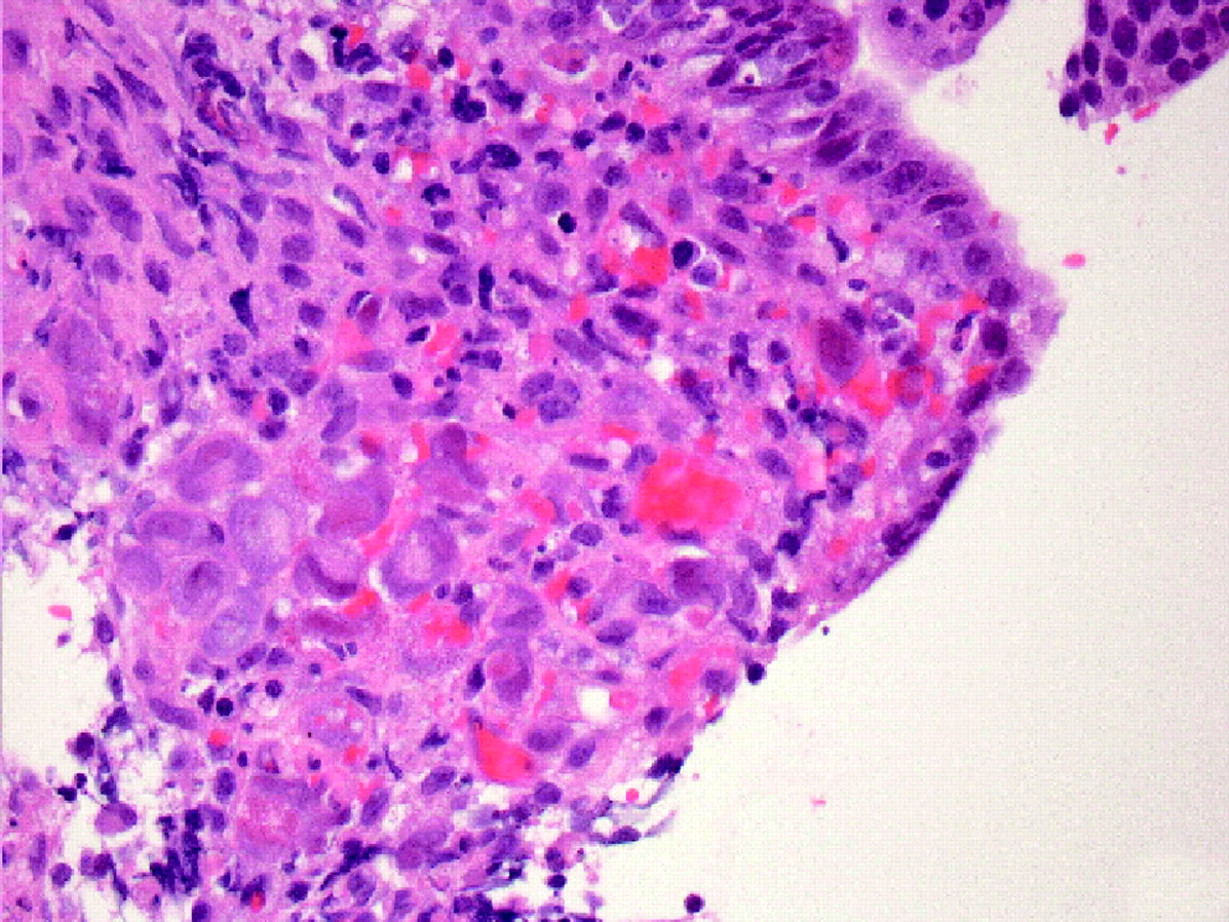{kind=link}
{kind=link}
An algorithmic approach to the diagnosis of duodenal biopsy specimens. AE, autoimmune enteropathy; CD, Crohn’s disease; CD4 TLPD, CD4 T cell lymphoproliferative disorders; FA, food allergy; GDM, gastric duodenal metaplasia; GSE, gluten-sensitive enteropathy; IELs, intraepithelial lymphocytes; IPSID, immunoproliferative small intestinal disease; MAI, Mycobacterium avium intracellulare; RS, refractory sprue; VA, villous atrophy; VG, viral gastroenteritis.
REFERENCES
Footnotes
-
Published Online First 10 May 2006
-
Competing interests: None declared.