Article Text

Abstract
Aim We queried whether extrahepatic cholangiocarcinoma featured clinically relevant genomic alterations that could lead to targeted therapy.
Methods Comprehensive genomic profiling by hybridisation capture of up to 315 genes was performed on 99 clinically advanced extrahepatic cholangiocarcinoma.
Results There were 60 male and 39 female patients with a median age of 60.5 years. A total of 400 alterations were identified (mean 4.0; range 0–13) in 84 genes. Eighty-two (83%) of extrahepatic cholangiocarcinoma patients featured at least one clinically relevant genomic alterations including KRAS (43%); ERBB2 (9%), PTEN (7%); ATM and NF1 (6%) and CCND1, FBXW7, GNAS, MDM2 and NRAS (all at 5%). BRAF, BRCA2, CDK4, CDK6, FGFR1, FGFR3, PTCH1, RAF1 and STK11 were each altered in a single patient. No IDH1/2 mutations or FGFR2 gene fusions were identified.
Conclusions Comprehensive genomic profiling of extrahepatic cholangiocarcinoma differs significantly from intrahepatic cholangiocarcinoma and pancreatic adenocarcinoma, and reveals diverse opportunities for the use of targeted therapies.
- BILIARY
- ONCOLOGY
- HISTOPATHOLOGY
Statistics from Altmetric.com
Introduction
Cholangiocarcinoma is a carcinoma of the bile duct epithelium, which comprises 3% of all gastrointestinal malignancy and features an incidence of 1–2 per 100 000 people in the USA.1 ,2 The established risk factors include chronic inflammatory conditions such as primary sclerosing cholangitis, liver fluke, viral hepatitis, biliary cysts and stones, and an exposure to thorotrast.3 Approximately 70–90% of cholangiocarcinomas arise in the extrahepatic biliary tree at any point from the confluence of the left and right hepatic ducts (Klatskin tumour) to the distal common bile duct.4 Extrahepatic cholangiocarcinoma (EHCCA) is more prevalent in Asia than in the USA.4–6
Currently, radical resection is the only potential curative treatment for cholangiocarcinoma including EHCCA.3 Unfortunately, patients with cholangiocarcinoma frequently present with unresectable tumour due to lack of clinical symptoms until the advanced stages of the disease have developed.3 ,7 Only 46.7% of EHCCA were deemed resectable at diagnosis according to one study, 8 ,9 and even after the resection, the 5-year survival rate is only 20–30%.8–10 Options for unresectable EHCCA are extremely limited at the current time. The current chemotherapy regimen for cholangiocarcinoma is generally extracted from protocols used in gastrointestinal cancers and features non-targeted gemcitabine and cisplatin-based regimens regardless of the location.11 The prognosis is poor with median overall survival rates of <12 months.4 ,12–14 The recent discoveries of targetable genomic alterations (GAs) in cholangiocarcinomas have created new interest for changing the approach to systemic treatment.15–32 Molecular profiles of cholangiocarcinoma have been studied by a number of different methodologies including western blotting, immunohistochemistry (IHC), mass spectrometry and next-generation sequencing (NGS).15–32 However, the significant majority of the cholangiocarcinoma cases that have undergone genomic analysis were intrahepatic tumours (IHCCA), with only a small number of EHCCA cases included. To date, there have been limited attempts to establish the similarities and differences of genomic profiles of EHCCA compared with IHCCA and gallbladder carcinoma.17 ,18 One recent genomic profiling study of cholangiocarcinoma using multigene NGS showed that Kirsten rat sarcoma viral oncogene homologue (KRAS) and tumour protein p53 (TP53) mutations were frequent in EHCCA and gallbladder carcinoma. In contrast, isocitrate dehydrogenase 1 and 2 (IDH1/2) mutation was exclusively identified in IHCCA.17 The findings in this study were subsequently confirmed by another genomic profiling study by the group at The University of Texas MD Anderson Cancer Center,18 in which 23.6% of IHCCA demonstrated IDH1/2 mutations in contrast to no IDH1/2 mutations in 20 cases of EHCCA. These studies suggested distinct pathways for cholangiocarcinomas of different sites and a potential for tumour loci-specific therapeutic modality.
Given the dismal prognosis of EHCCA, development of effective systemic treatment options to improve cancer-related mortality is greatly needed. In the following study, we characterised 99 cases of EHCCA using hybrid capture-based comprehensive genomic profiling (CGP). This is by far the largest CGP study of EHCCA and was designed to survey the genomic landscape in search of GAs that could be targetable with currently available drugs and agents available in mechanism-driven clinical trials for relapsed or metastatic EHCCA.
Materials and methods
Local site permissions to use clinical samples were obtained for this study. On routine microscopy, all samples had a minimum percentage of tumour nuclear area compared with benign nuclear area of ≥20% (see online supplementary table S1). CGP was performed on 99 cases of relapsed or metastatic EHCCA in a Clinical Laboratory Improvement Amendments-certified, College of American Pathologists-accredited laboratory (Foundation Medicine, Cambridge, Massachusetts, USA). In brief, ≥50 ng DNAs were extracted from tumour samples of formalin-fixed, paraffin-embedded tissue blocks. Hybridisation capture of 3320 exons from up to 315 cancer-related genes and 47 introns of 19 genes commonly rearranged in cancer were applied to the extracted DNA. Subsequently, the samples were subject to sequencing to high, uniform coverage, with a mean sequencing depth of 719× as previously described.33 GAs (base substitutions, small indels, rearrangements and copy number alterations) were determined and then reported for these samples. Clinically relevant GA was defined as alteration that is targetable by currently available anticancer drugs on the market or in registered clinical trials.
Results
The samples were obtained from 60 male and 39 female patients with a median age of 60.5 years (range 24–90 years). The ethnic background of the patients included in this study was not uniformly available. All patients were residents of the USA at the time their disease presented, and no patients were known clinically or diagnosed pathologically with any type of parasitic infection of the biliary tract. Five (5%) EHCCA were grade 1, 64 (65%) grade 2 and 30 (30%) grade 3. There were 2 (2%) stage II, 27 (27%) stage III and 70 (71%) stage IV tumours at the time of CGP. The tumour samples obtained for sequencing originated from the primary bile duct tumour in 44 (44%) of cases and from metastatic sites in 55 (56%) of the cases including the liver in 31 cases, peritoneal cavity and surfaces in 9 cases, lymph nodes in 8 cases, soft tissue in 4 cases, bone in 2 cases and lung in 1 case (table 1).
Clinicopathological features of extrahepatic cholangiocarcinoma
A total of 400 GAs were identified, with a mean 4.0 alterations per sample (range 0–13) in 84 genes (figure 1). Of the 400 alterations, 37% were base substitutions/deletions, 31% were truncating mutations, 17% were gene amplifications, 12% were homozygous deletions and 3% were gene rearrangements. Ninety-eight (99%) of the EHCCA samples harboured at least one GA, and 82 (83%) samples harboured at least one clinically relevant GA (CRGA). The distribution of the total GAs is seen in figure 1. There were 165 total CRGA with a median of 1.67 CRGA per EHCCA sample.

Long tail plot of the distribution of genomic alterations in 99 cases of extrahepatic cholangiocarcinoma.
The most frequently altered CRGA involved KRAS (43%); ERBB2 (9%); PTEN (7%); ATM and NF1 (6%) and CCND1, FBXW7, GNAS, MDM2 and NRAS (all at 5%). BRAF, BRCA2, CDK4, CDK6, FGFR1, FGFR3, PTCH1, RAF1 and STK11 were each altered in a single patient (table 2; see online supplementary table S1). The most common non-clinically relevant alterations involved TP53 (45%), CDKN2A (28%) and CDKN2B (15%), followed by SMAD4 (15%) and ARID1A (13%). The frequency of ERBB2 alterations was 9% (figures 2 and 3). No IDH1/2 mutations or FGFR2 gene fusions were identified (table 2).
Most frequently altered genes in 99 cases of extrahepatic cholangiocarcinoma
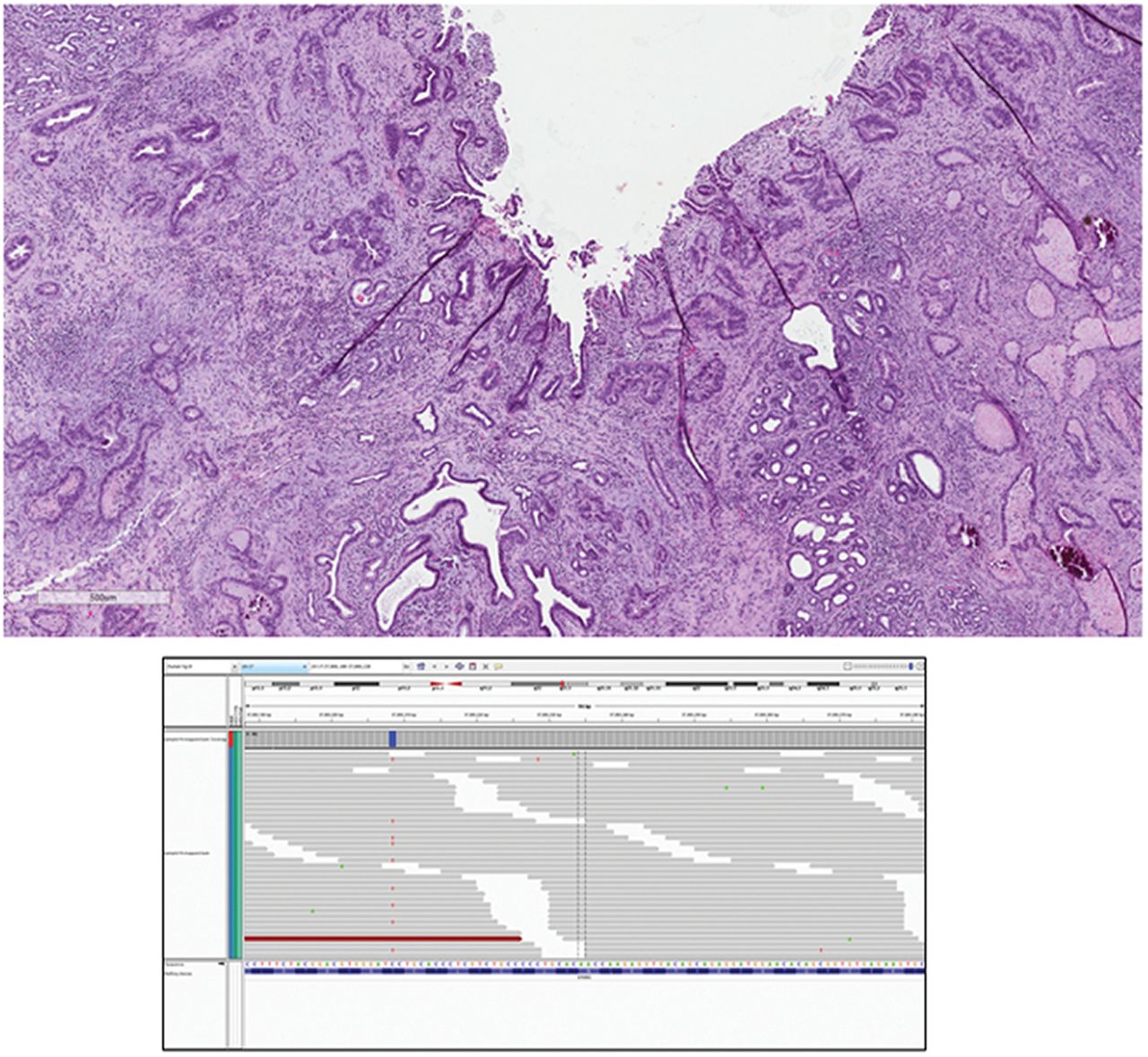
ERBB2 S310F mutation in a case of extrahepatic cholangiocarcinoma. Upper panel demonstrates the moderately differentiated (grade 2) adenocarcinoma of the bile duct in a 74-year-old man (H&E ×100). Lower panel shows the missense base substitution in the extracellular domain of the ERBB2 gene creating the S310F alteration, as well as base substitution in ATM and SMAD4. Extracellular domain ERBB2 mutations are known to enhance ERBB2-ERBB3 dimerisation and respond to anti-HER2 targeted therapies.
{kind=link}
{kind=link}
{kind=link}
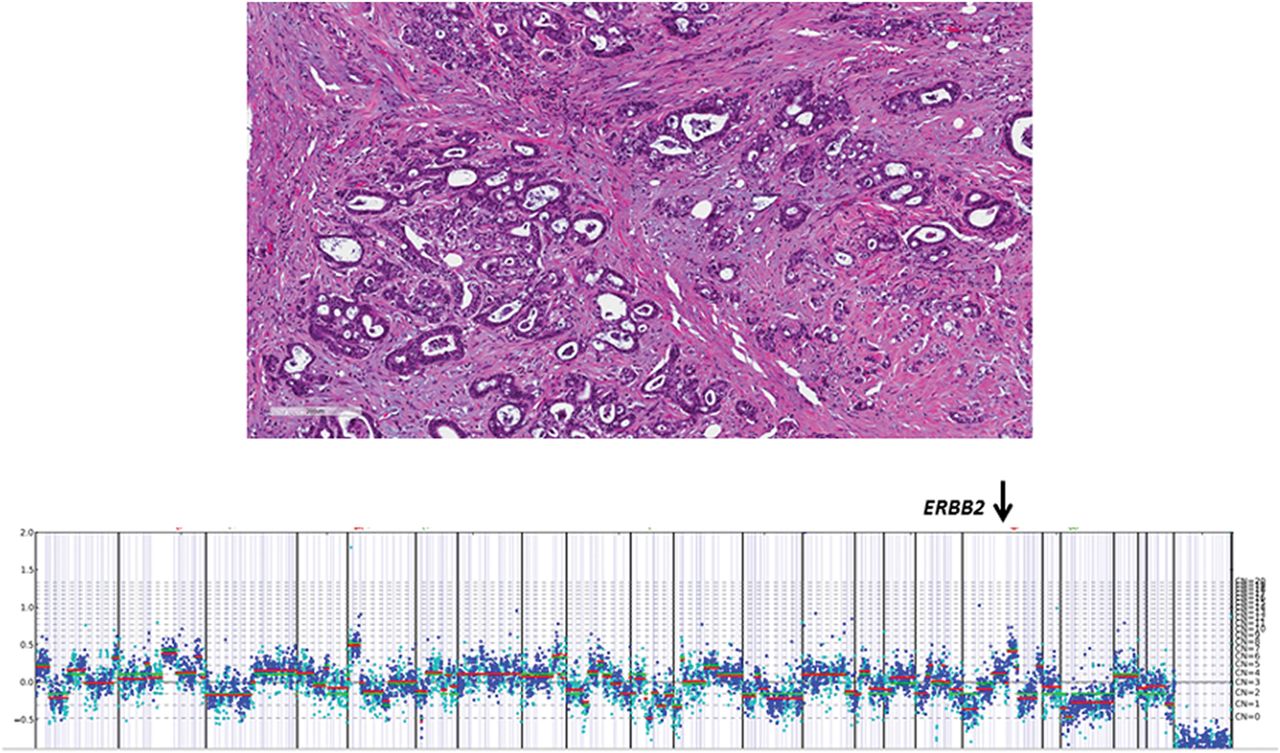
Upper panel demonstrates primary grade 2 extrahepatic cholangiocarcinoma invading the pancreas in a 63-year-old man. The tumour was stage IV at presentation (H&E ×100). In the lower panel, the comprehensive genomic profiling revealed amplification on ERBB2 at seven copies and homozygous loss of PTEN. RICTOR amplification and TP53 base substitution were also identified.
No matched primary tumour and metastatic tumour biopsies were available in the same patient to compare the GA patterns. When the GA pattern in the patient group where the primary tumour was sequenced was compared with that seen in the patients whose metastatic lesions were sequenced, no significant differences in the GA were observed in this study.
Discussion
Noteworthy in this study was the relatively high frequency of alterations in the ERBB2 (HER2) that was present in 9% of EHCCA. Interestingly, unlike breast and upper gastrointestinal carcinomas, of the nine total ERBB2 alterations, six (67%) of these alterations were base substitution and insertion mutations and not amplifications. These six cases would not have been detected as having ERBB2-driven tumours if they had only been tested by slides-based methods for gene copy number by fluorescence in situ hybridisation (FISH) or protein overexpression by IHC. ERBB2 overexpression detected by IHC has been reported in 5.1–29.1% of EHCCA.14 ,29–31 In one study, 4 (5%) of 78 cases showed overexpression of ERBB2 by IHC of which 3 (75%) were confirmed to have ERBB2 gene amplification by FISH.29 In another study, ERBB2 overexpression was found in 16 (29%) of 55 patients with EHCCA by IHC, of which only 10 (63%) were confirmed to have ERBB2 amplification by chromogenic in situ hybridisation.30 ERBB2 amplification has been found to be an independent poor prognostic factor in EHCCA with nodal metastasis.30 Although the data for IHCCA are somewhat conflicting, recent genomic profiling studies using NGS platforms have reported extremely low ERBB2 alteration rates with no (0%) ERBB2 alterations found in two studies: one with 98 IHCCA17 and one with 28 IHCCA.32 Another study reported only one (2%) ERBB2 alteration detected in a series of 55 IHCCA.18 Thus, ERBB2 alterations in IHCCA appear to be significantly less frequent in IHCCA than found in EHCCA.
ERBB2 has been a target of therapy for breast cancer for >15 years, and this indication has been expanded to gastroesophageal carcinomas more recently.34 Both anti-HER2 antibody therapeutics (trastuzumab, pertuzumab and trastuzumab-DM1) and small-molecule tyrosine kinase inhibitors (lapatinib, afatinib) have been approved.35–37 Of these, lapatinib has been subject to two phase II clinical trials for advanced cholangiocarcinoma. The overall response was poor and one trial was terminated, although the enrolment was not based on ERBB2 alteration status.38 ,39
Second, 28% of EHCCA harboured alterations related to the phosphatidyl inositol 3 kinase (PI3K)/protein kinase B (AKT)/mammalian target of rapamycin (mTOR) signalling pathway. Phosphatase and tensin homologue (PTEN), NF1 and PIK3CA were altered in 11%, 7% and 7% of EHCCA, respectively. Also, FBXW7 and STK11 were altered in two patients. For the PTEN alterations, two featured a homozygous deletion, three were truncation mutations and one was a substitution/indel. All the NF1 alterations were truncation mutations. Four PIK3CA alterations were substitution/indel. The loss of the lipid phosphatase function of PTEN results in uncontrolled activation of PI3K/AKT/mTOR pathway.28 Decreased PTEN protein expression has been associated with reduced survival in EHCCA.40 Interestingly, for IHCCA, overexpression of PTEN protein has been reported as predictive of a better prognosis.41 NF1 encodes neurofibromin, which functions as a tumour suppressor via inactivation of RAS oncogene that serves to downregulate mitogen-activated protein kinase and the PI3K/AKT/mTOR pathway. Somatic NF1 alterations have been reported in various sporadic tumours including glioblastoma, melanoma, cancers of ovary, breast and lung, hematolymphoid malignancy and sarcoma.42 Data on NF1 in cholangiocarcinoma are limited; 1 of 28 IHCCA was found to harbour somatic NF1 mutation using an NGS-based platform.32
PIK3CA gene encodes the p110 alpha catalytic subunit of PI3K; thus, its mutation activates the PI3K/AKT/mTOR pathway, leading to cell proliferation and survival.24 Somatic mutation of PIK3CA has been found in variable cancers including breast, colon, endometrial, bladder and hepatocellular, as well as cholangiocarcinoma and gallbladder carcinomas.24 The PIK3CA mutation has been observed in 4–32.4% of cholangiocarcinoma.32 ,43 To date, GAs directly or indirectly involved in PI3K/ATK/mTOR pathway have been reported in 33–40% of EHCCA by NGS-based platforms, usually more frequently compared with IHCCA.17 ,18 ,32 In the current study, 28% of EHCCA showed these alterations, thus falling within the previously reported range. Several mTOR inhibitors, such as temsirolimus and everolimus, are available in the market and are US Food and Drug Administration-approved for several tumour types. A phase I clinical trial of everolimus in combination with gemcitabine and cisplatin for solid tumours, including cholangiocarcinoma, showed some promise.44 Another phase I clinical trial of MK-2066, oral pan-AKT inhibitor, also showed favourable outcome in a subset of patients with solid tumours.45 In addition, various PI3K inhibitors such as GDC-0980 and BAY80-6946 are under investigation for clinical trials.44 ,46
KRAS mutation was observed in 42% of EHCCA, which also falls within the reported range of the KRAS mutation in EHCCA.17 ,18 ,26 KRAS mutation in EHCCA has been consistently more prevalent than IHCCA and gallbladder cancers.17 ,18 ,26 ,32 However, the alteration is significantly less frequent in EHCCA compared with pancreatic adenocarcinoma.47
Due to striking morphological resemblances between some of the biliary and pancreatic diseases and tumours, the concept that biliary disease represents biliary counterpart of pancreatic disease has gained popularity.48–50 Similarly, the presumed precursor lesion of cholangiocarcinoma, biliary intraepithelial neoplasia, was shown to share common carcinogenesis with pancreatic intraepithelial neoplasia.51 In fact, the initial systemic chemotherapy regimen for advanced cholangiocarcinoma, gemcitabine, has been devised based on regimen for advanced pancreatic cancer.52 Despite the morphological similarities, the differences in molecular profiles including the contrasting frequencies of KRAS and ERBB2 mutations (71% and 0.4% in pancreatic adenocarcinoma, respectively) lend support that EHCCA and pancreatic adenocarcinoma are distinct diseases with distinctive therapeutic implications. Moreover, in contrast to previously studied IHCCA, no IDH1/2 mutations or FGFR2 gene fusions were identified in this study, and ERBB2 was more frequently altered in EHCCA, further supporting that IHCCA and EHCCA differ in carcinogenesis and therapeutic targets.32 Common alteration of KRAS in EHCCA and pancreatic cancer in contrast to IHCCA may be explained by the shared embryological developmental stages between extrahepatic biliary tree and ventral pancreas, unlike intrahepatic biliary tree, which originates from progenitor cells of the liver.53
From a clinical standpoint, targeting the downstream pathways of KRAS, such as Raf/mitogen-activated protein kinase (MEK)/extracellular signal-related kinase and PI3K/AKT pathways, is under investigation. For example, phase II trial of an inhibitor of MEK1/2, selumetinib, for patients with metastatic cholangiocarcinoma showed modest response in some patients.54 Another phase II study of a multikinase inhibitor of vascular endothelial growth factor receptor-2/-3, platelet-derived growth factor receptor-beta, B-Raf and C-Raf, sorafenib,55 ,56 for advanced cholangiocarcinoma and gallbladder carcinoma showed some therapeutic benefit. Development of direct inhibitor of KRAS may be of potential therapeutic utility in the future.
In summary, a variety of CRGAs has been identified in 89% of relapsed and metastatic EHCCA by CGP. The long tail of potential therapy targets generated from the CGP analysis mandates comprehensive diagnostic approaches to maximise targeted treatment options for patients with clinically advanced disease to potentially improve disease outcomes for this aggressive form of malignancy.
Take home messages
Extrahepatic cholangiocarcinoma portends a dismal prognosis due to advanced stage at presentation and limited treatment options.
Molecular profiling in search for targetable genomic alterations has been performed predominantly on intrahepatic cholangiocarcinomas; data on extrahepatic cholangiocarcinoma are scarce. This is by far the largest comprehensive genomic profiling series of extrahepatic cholangiocarcinoma.
Eighty-two (83%) of 99 cases of extrahepatic cholangiocarcinoma featured at least one clinically relevant genomic alteration. The genomic profiling of extrahepatic cholangiocarcinoma was distinct from intrahepatic cholangiocarcinoma.
Comprehensive genomic profiling of extrahepatic cholangiocarcinoma reveals diverse opportunities for the use of targeted therapies.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table
Footnotes
Handling editor Runjan Chetty
Contributors HL: literature review and manuscript preparation. DMJ, MJ and JSR: idea and retrieval of cases, manuscript review. KW, AJ, SMA, JAE, RY, DL, VAM and PJS: Generation of data and data analysis, and photography.
Competing interests KW, AJ, SMA, JAE, RY, DL, VAM, PJS and JSR have employment with and own equity in Foundation Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.