Article Text

Statistics from Altmetric.com
- HCC, hepatocellular carcinoma
- HCV, hepatitis C virus
- HBV, hepatitis B virus
- AFP, α-fetoprotein
- CT, computed tomography
- MRI, magnetic resonance imaging
- PEI, percutaneous ethanol injection
- HBsAg, hepatitis B surface antigen
1.0 FOREWORD
This document, on the diagnosis and treatment of patients with hepatocellular carcinoma (HCC), was commissioned by the British Society of Gastroenterology as part of a wider initiative to develop guidelines for clinicians in several areas of clinical practice.
Cancer care has been the subject of increased scrutiny, with the development of care guidelines forming a major part of the strategy to reduce cancer related mortality in the UK. There is a strong suggestion that HCC is a disease which will be seen more frequently over the next few years, mainly as a result of the hepatitis C virus (HCV) epidemic. Previously, HCC has been a relatively rare tumour in the UK and much of the data pertaining to its diagnosis and therapy are derived from studies outside of the UK. Because of the lack of screening programmes and the fact that a significant proportion of HCC presents as symptomatic disease in individuals not known to have liver disease, most non-surgical therapies have been used in patients with advanced disease. There are a significant number of variables known to influence prognosis, with stage of underlying liver disease and tumour size at presentation being the most important. Controlling for these variables is difficult and these factors have contributed to a dearth of randomised controlled trials of treatment for this tumour. There is however a substantial amount of evidence available which can form the basis of a framework for diagnosis and management.
Guidelines are not rigid protocols and they should not be construed as interfering with local clinical judgement. Hence they do not represent a directive of proscribed routes but a basis on which clinicians can consider the options available more clearly.
2.0 INTRODUCTION AND OBJECTIVES
These guidelines cover two areas of clinical practice relating to HCC: firstly, its diagnosis, including surveillance of high risk individuals; and secondly, treatment of the patient where the diagnosis has been made. HCC remains one of the commonest malignant diseases in the world but it has not previously been a leading cause of death in the Western world. There is now conclusive evidence from the USA and a strong suggestion from the UK that HCC is becoming a more common cancer, primarily due to the HCV epidemic. These guidelines relate to adult medical practice; high risk paediatric conditions predisposing to HCC and the management of paediatric patients with HCC will not be considered.
Guidelines are proposed on a number of issues:
which patients are at high risk for the development of HCC and should be offered surveillance;
what investigations are required to make a definite diagnosis; and
which treatment modality is most appropriate in a given clinical context.
3.0 FORMULATION OF GUIDELINES
A systematic review of the relevant literature and synthesis of available evidence with later phases of peer group appraisal and then expert review was performed. Draft proposals were amended at this stage. The strength and evidence used in these guidelines was that recommended by the north of England evidence based guidelines development project.
3.1 Categories of evidence
-
Ia: Evidence from meta-analysis of randomised controlled trials.
-
Ib: Evidence from at least one randomised trial.
-
IIa: Evidence obtained from at least one well designed controlled study without randomisation.
-
IIb: Evidence obtained from at least one other type of well designed quasi experimental study.
-
III: Evidence obtained from well designed non-experimental descriptive studies such as comparative studies, correlation studies, and case studies.
-
IV: Evidence obtained from expert committee reports or opinions, or clinical experiences of respected authorities.
3.2 Grading of recommendations
Recommendations are based on the level of evidence presented in support and are graded accordingly.
Grade A: Requires at least one randomised controlled trial of good quality addressing the topic of recommendation.
Grade B: Requires the availability of clinical studies without randomisation on the topic.
Grade C: Requires evidence from category IV in the absence of directly applicable clinical studies.
4.0 SUMMARY OF RECOMMENDATIONS
-
Surveillance using abdominal ultrasound and α-fetoprotein (AFP) estimation can detect HCC of a smaller size than those presenting without screening (evidence IIa).
-
The only potentially curative therapies depend on detection of small HCC (evidence IIa).
-
Despite the above, there are no data confirming that these advantages in detection of earlier lesions produces an improvement in long term survival or cost saving (evidence IIa).
-
Surveillance for hepatocellular carcinoma should be considered in the following high risk groups:
– Males and females with established cirrhosis due to hepatitis B virus (HBV), particularly those with ongoing viral replication (evidence grade III, recommendation grade B).
– Males and females with established cirrhosis due to HCV (evidence grade III, recommendation grade B).
– Males and females with established cirrhosis due to genetic haemochromatosis (evidence grade III, recommendation grade B).
– Males with alcohol related cirrhosis who are abstinent from alcohol or likely to comply with treatment (evidence grade III, recommendation grade B).
– Males with cirrhosis due to primary biliary cirrhosis (evidence grade III, recommendation grade B).
-
The risk of HCC development in cirrhosis due to autoimmune hepatitis, primary sclerosing cholangitis in both sexes, and alcoholic and primary biliary cirrhosis in women is generally low. Non-cirrhotic HCCs do occur in viral cirrhosis but the absolute risk is low (evidence IIb).
-
If surveillance is offered, it should be six monthly abdominal ultrasound assessments in combination with serum AFP estimation (evidence grade III, recommendation grade B). Abdominal ultrasonography should be undertaken with appropriate dedicated equipment and by an operator skilled in the assessment of patients with cirrhosis (evidence grade IIb, recommendation grade B).
-
If surveillance is offered, patients should be aware of the implications of early diagnosis and the lack of proven survival benefit.
4.1 Diagnosis of HCC
-
A focal lesion in the liver of a patient with cirrhosis is highly likely to be HCC (evidence grade IIa).
-
Initial assessment should be by spiral computed tomography (CT) of the liver (local spread) and thorax (metastases) (evidence grade IIa, recommendation grade B).
-
Magnetic resonance imaging (MRI) with contrast enhancement or angiography with lipiodol injection and follow up CT may increase the accuracy of detection of other liver lesions (evidence grade III, recommendation grade C).
-
Biopsy is rarely required for diagnosis, and seeding of tumour in the needle tract occurs in 1–3%. Biopsy of potentially operable lesions should be avoided where possible (evidence grade IIa, recommendation grade B).
4.2 Treatment of HCC
The only proven potentially curative therapy for HCC remains surgical, either hepatic resection or liver transplantation, and patients with single small HCC (≤5 cm) or up to three lesions ≤3 cm should be referred for assessment for these treatment modalities.
Liver transplantation should be considered in any patient with cirrhosis and a small (5 cm or less single nodule or up to three lesions of 3 cm or less) HCC (evidence grade IIa, recommendation grade B).
Patients with replicating HBV had a worse outlook due to HBV recurrence and were previously not considered candidates for transplantation. Effective antiviral therapy is now available and patients with small HCC, as defined above, should be assessed for transplantation (evidence grade IIa, recommendation grade B).
Hepatic resection should be considered as primary therapy in any patient with HCC and a non-cirrhotic liver (including fibrolamellar variant) (evidence grade IIa, recommendation grade B).
Resection can be carried out in highly selected patients with hepatic cirrhosis and well preserved hepatic function (Child-Pugh A) who are unsuitable for liver transplantation. Such surgery carries a high risk of postoperative decompensation and should be undertaken in units with expertise in hepatic resection and management of liver failure (evidence grade IIa, recommendation grade B).
4.3 Non-surgical management
Non-surgical therapy should only be used where surgical therapy is not possible.
Percutaneous ethanol injection (PEI) has been shown to produce necrosis of small HCC. It is best suited to peripheral lesions, less than 3 cm in diameter (evidence grade IIb, recommendation grade B). Radiofrequency ablation may be a good alternative ablative therapy but data are limited (evidence grade IIb).
Chemoembolisation can produce tumour necrosis and has been shown to affect survival in highly selected patients with good liver reserve. Chemoembolisation using lipiodol is effective therapy for pain or bleeding from HCC (evidence grade IIa, recommendation grade B).
Systemic chemotherapy with standard agents has a poor response rate and should only be offered in the context of trials of novel agents (evidence grade I, recommendation grade A).
Hormonal therapy with tamoxifen has shown no survival benefit in controlled trials (evidence grade I, recommendation grade A) and is not recommended.
5.0 BACKGROUND
5.1 Epidemiology of HCC
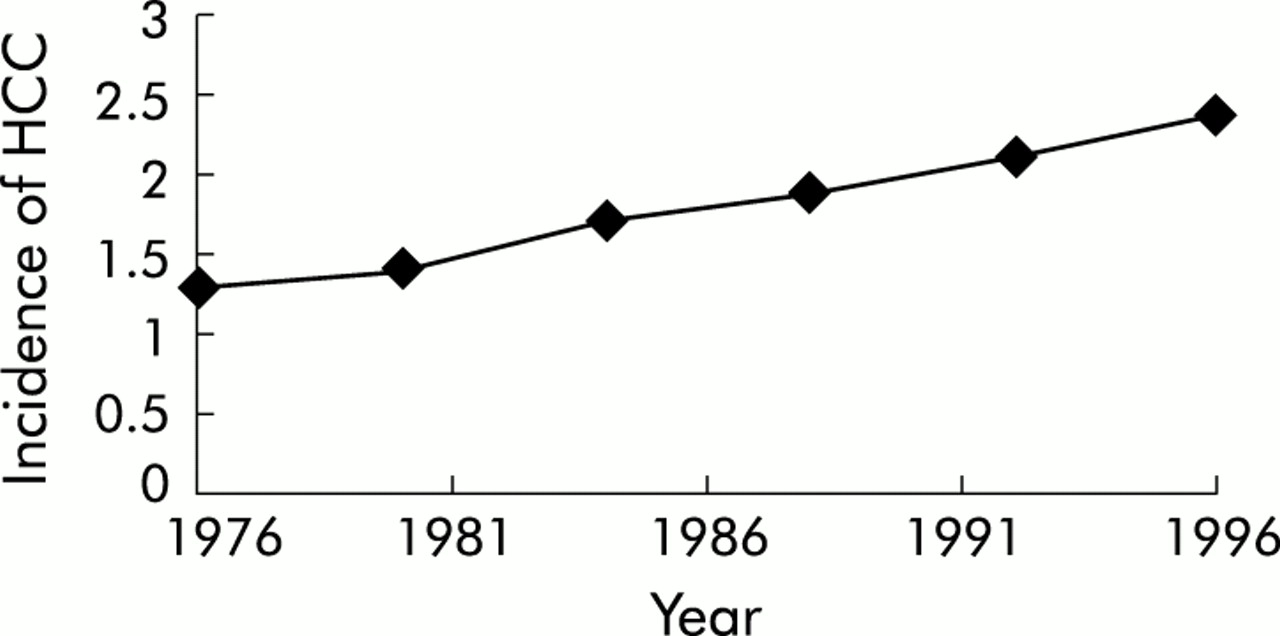
HCC causes approximately 1500 deaths per year in the UK. There is strong evidence from the USA that the incidence of HCC is rising1: nine cancer registries reporting via the National Cancer Institute showed a 41% rise in mortality from primary liver cell cancer between 1980 and 1995 with a 70% rise in overall incidence (fig 1). Similar although less robust evidence is emerging in the UK.2 HCC is unusual among human cancers in that the aetiological agent responsible is usually readily identifiable. The prevalence of HCC worldwide parallels that of viral hepatitis and the majority of cases are associated with HBV and HCV. The increase in HCC incidence in the developed world is likely to be a direct result of the HCV epidemic occurring some 20–30 years after the rise in this infection in target populations.3 Alcohol, genetic haemochromatosis, and rarely primary biliary cirrhosis are associated. In the UK, up to 40% of cases present with HCC as the first indication of underlying liver disease, in distinction to countries such as Japan where 80% of HCC are detected at an asymptomatic stage by screening of patients with known cirrhosis.4

Incidence (per 100 000 population) of hepatocellular carcinoma (HCC) in the USA from 1976 to 1996 (from El-Serag and Mason 19991).
5.1.1 Factors influencing the risk of HCC development
(1) Sex
The risk of HCC development is much greater in men for the majority of aetiologies.5 This is independent of the fact that males are more likely to develop chronic HBV carriage than women. HCV may be a relative exception to this with a male to female ratio of 1.2:1 compared with 1.9:1 for HBV. The reasons for this are unclear.6
(2) Age
The average age of HCC development in the UK is 66 years, which probably reflects the long term nature of most underlying liver diseases producing tumour development. This tumour is rare below the age of 45 years in areas with low levels of HBV infection. In high HBV prevalence areas, HCC has a bimodal age distribution with peaks at ages 45 and 65.7
(3) The presence of hepatic cirrhosis
Cirrhosis is present in the vast majority of patients with HCC in the UK and Europe: estimates vary between 90% and 95%.8,9 It is unclear if cirrhosis per se is biologically important in the tumorigenic pathway, or if tumour development and fibrogenesis take place concurrently but with fibrosis taking a shorter time period. Non-cirrhotic HCCs occur in young patients (fibrolamellar variant) and in the elderly (apparent de novo HCC). Fibrolamellar HCC has an equal sex incidence and an average age at diagnosis of 30 years.10 Non-cirrhotic HCC does occur in patients with viral liver disease, particularly HBV11 where direct viral integration into host DNA may play a role.12 Non-cirrhotic HCC is described in HCV13 and haemochromatosis14 but is rare.
(4) Aetiology of liver disease
There is a considerable variation in the risk of HCC development in follow up studies of patients with cirrhosis of different aetiologies. Viral infection, either HBV or HCV, carries a high risk, with cirrhotic patients with either infection having approximately a 3–5% per year risk of HCC development.15,16 In some studies the risk is even higher, up to 12% per year in HBV infected patients,17 but this may represent patient selection; those with more severe liver disease may be at greater risk. In HCV infection there is compelling evidence that HCC development occurs with higher frequency at a very advanced stage of underlying liver disease18: up to 30% of patients undergoing liver transplantation for end stage HCV cirrhosis have undetected HCC found in the explanted liver.19
In non-viral cirrhosis, again a great divergence of risk of HCC is seen with aetiology. Patients with cirrhosis due to genetic haemochromatosis who were iron loaded at presentation had a very high risk of HCC development (7–9% per year).20 The risk falls with venesection but not to baseline levels (1–3% per year).21 In contrast, patients with cirrhosis of autoimmune hepatitis have a very low risk of HCC development. Descriptions of HCC in the literature in this group are rare, despite a substantial number of cirrhotic individuals under long term follow up. Those which do exist suggest HCV coinfection may be an important factor.22 Alcoholic cirrhosis carries an increased risk of HCC development; this risk is difficult to quantify as mortality from continued alcohol consumption and cardiovascular disease is very high in this group. The available data suggest that abstinence from alcohol does not protect against HCC development, and that tumour development is seen in 1–4% of male cirrhotics per year, a similar level to that produced by HBV or HCV infection.23,24 The rate of HCC development in women with alcohol related cirrhosis is more difficult to establish but seems significantly lower with few reports in the literature.24 Primary biliary cirrhosis does carry a risk of HCC development but studies quantiating risk in this group are rare. However, the available data suggest that women, even with established cirrhosis, have a low risk but males have a similar risk to patients with alcohol related cirrhosis.25,26 Wilson’s disease is rare, but an increasing number of patients are surviving into adulthood with pre-existing hepatic cirrhosis. HCC is well described despite adequate copper chelating therapy, although the true incidence is difficult to establish.27
5.2 Natural history of HCC
HCCs develop as small nodules. The majority of their growth takes place in an asymptomatic phase which may be years in length. Estimated doubling times of HCC vary between one and 19 months,28,29 with a median of six months. There has been a suggestion that tumours with certain defined aetiologies may have more aggressive behaviour but there are no conclusive data to support this. There are data as to survival in untreated patients with HCC, showing that the major factors influencing overall survival are severity of underlying liver dysfunction and tumour size at initial detection. Between 50% and 90% of patients with Child-Pugh A cirrhosis will survive a year untreated compared with only 20% with Child-Pugh C.29–31 Small HCCs at presentation have relatively long tumour doubling times, and overall survival with tumours of less than 5 cm was 81–100% at one year and 17–21% at three years with no therapy.29,32 This suggests that if earlier diagnosis can be made, the opportunity for intervention may be greater.
5.3 Potential screening tests for HCC
AFP, a normal serum protein synthesised by fetal liver cells and yolk sac cells, is the most widely studied screening test used as a tumour marker for HCC. The normal range for AFP is 10–20 ng/ml and a level >400 ng/ml is usually regarded as diagnostic. Two thirds of HCCs less than 4 cm however have AFP levels less than 200 ng/ml and up to 20% of HCC do not produce AFP, even when very large.33 Modifications of AFP with differing carbohydrate structures may occur in HCC and can be detected by altered patterns of lectin binding. These altered profiles have led to the development of alternative diagnostic tests34 but none are widely available or have been shown to markedly enhance diagnostic ability over AFP. Desgamma-carboxy prothrombin has been used as an alternative tumour marker for HCC; 67% of HCC have elevated levels but only 8% of small (<2 cm) HCCs have abnormal levels35 and it has not gained wide acceptance. Using AFP testing also produces false positives; levels in the range 20–250 ng/ml are frequently seen in regenerating nodules in viral cirrhosis.36 A rising AFP over time, even if the level does not reach 400 ng/ml, is virtually diagnostic of HCC.
Ultrasound can detect large HCCs with high sensitivity and specificity. It is less able to reliably identify smaller lesions, which are required if better therapy is to be offered. Expertise of the operator and dedicated equipment seem important in enhancing results; where this is available ultrasound detects 85–95% of lesions 3–5 cm in diameter and can achieve 60–80% sensitivity in the detection of lesions of 1 cm.37,38 In the UK at present, detection of lesions below 2 cm by ultrasound is uncommon.
Combining AFP and ultrasound improves detection rates. Ultrasound screening was initially suggested at six monthly intervals on the basis of tumour doubling times. There is some evidence that more frequent examinations may enhance sensitivity but at the expense of more false positive tests.39,40 Patients with a negative ultrasound and an elevated but not diagnostic level of AFP appear to be at high risk and more frequent ultrasound examination in this group, probably three monthly, may have a higher yield.38
5.4 Screening studies in HCC
There are no randomised controlled studies of screening for HCC development in cirrhosis of any aetiology. It is highly unlikely that any such randomised study could be undertaken now as surveillance of patients with cirrhosis is widely accepted and it would be almost impossible to recruit patients to a no screening arm of such a study. In the absence of such data, practice has been based on non-randomised studies either screening at risk populations or from clinic based series.
There are a number of series demonstrating the ability of either AFP alone as a screening investigation or, more commonly, the combination of AFP and ultrasound. The largest study of screening is in the Alaskan population with a high HBV carriage rate. Screening was undertaken in the total population with hepatitis B surface antigen (HBsAg) positivity, irrespective of viral replication. The results of this study show that from 1982 to 1998, 18 299 AFP estimations were undertaken in 2230 HBsAg positive individuals. Twenty patients developed HCC, five were inoperable at presentation, 14 had resections, but six recurred.41 A similar study of patients with HBV, only 4% of whom had proven cirrhosis, detected 14 cancers in 1069 patients screened, with six curative surgical procedures undertaken.42 Prospective studies of patients with viral cirrhosis have been carried out using ultrasound and AFP measurements and showed that 64–87% of detected tumours were single and 43–75% were 3 cm or less in diameter.43–46 In these studies, 29–66% of the detected cancers were treated surgically with an attempt at cure. These studies are not directly comparable with the situation in the UK as few centres had liver transplantation available as a therapeutic option.
5.5 Diagnostic tests for HCC
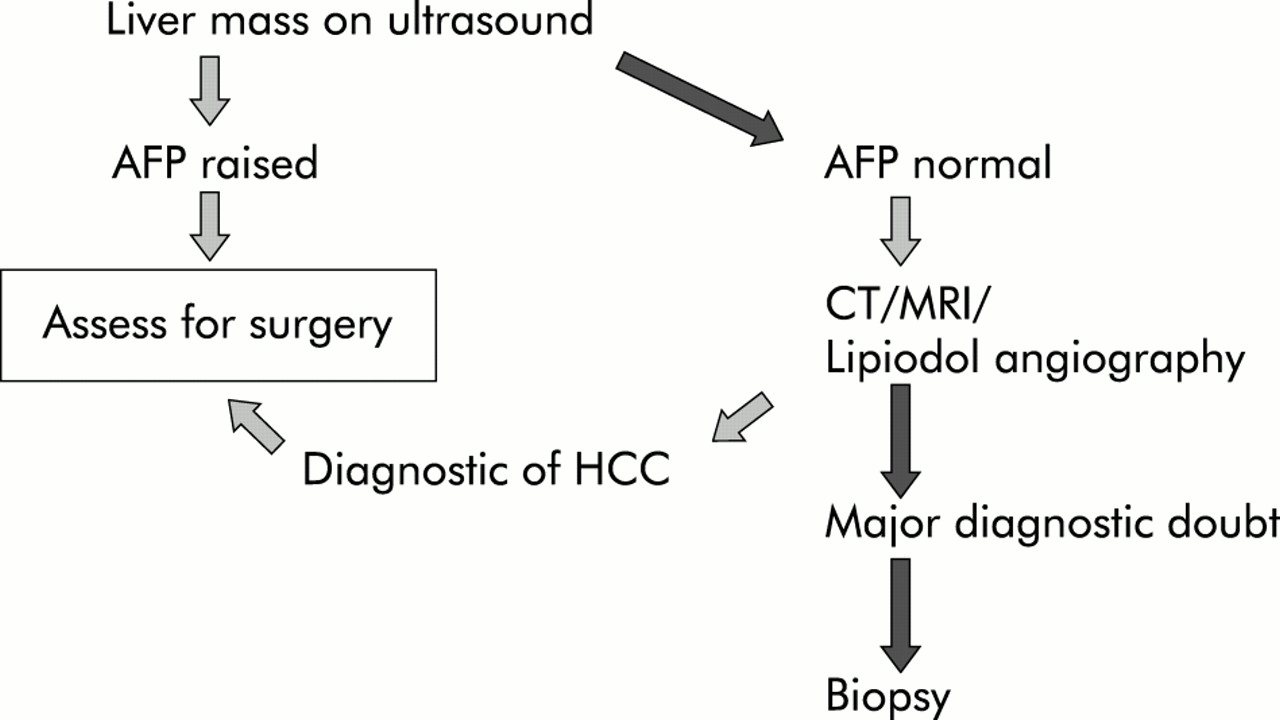
When a patient presents with a liver mass, irrespective of screening, there is a requirement to make a diagnosis and to stage the disease. The commonest clinical scenario is a patient with a mass discovered on ultrasound where AFP may or may not be raised. If the patient is known to have pre-existing cirrhosis and the mass is greater than 2 cm in diameter, there is a greater than 95% chance that the lesion is a HCC.47,48 If AFP is raised, this confirms the diagnosis and further investigation is only required to establish the most appropriate therapy (fig 2). If AFP is normal, further radiological imaging (CT, MRI, or lipiodol angiography with follow up CT) will usually allow a confident diagnosis to be made49–51 and proceed to assessment of treatment without the need for biopsy. In the few cases where real diagnostic doubt persists, biopsy may be indicated. In the uncommon situation of discovery of a small mass (<2 cm diameter) on ultrasound, the level of diagnostic certainty over a diagnosis of HCC is lower; probably 75% of such nodules turn out to be HCC.52 Again, other radiological techniques or a raised AFP may establish a definitive diagnosis. If not, either a repeat examination to show enlargement of the lesion, percutaneous fine needle aspiration, or biopsy may be indicated.53 The risk of seeding of HCC does not appear to be related to tumour size54 and if surgical therapy is possible biopsy should be avoided.

{kind=link}
{kind=link}
Investigating a mass in a cirrhotic liver. HCC, hepatocellular carcinoma; AFP, α-fetoprotein; CT, computed tomography; MRI, magnetic resonance imaging.
In a patient not known to be cirrhotic, usually where the first presentation is with a liver mass, the initial investigation should be AFP. If raised in the absence of a testicular primary, this confirms the diagnosis. If the lesion is potentially operable, then biopsy of the non-tumour liver may be required to determine the best treatment option. If AFP is normal, a search for other causes (non-liver primary) and further radiological assessment of the mass are required. If investigations suggest HCC, then again biopsy of non-tumour liver will determine the surgical approach. Radiological imaging can exclude benign liver lesions with a high degree of sensitivity and specificity.51,52,54 Only in situations where considerable doubt exists will biopsy of the lesion be required.
Radiological imaging with ultrasound, CT, and angiography usually understages HCC.54,55,56 This however has little significance in the selection of patients for liver transplantation as despite this understaging, studies have shown that prognosis relates to preoperative radiological assessment of the tumour rather than the actual stage at examination of the removed organ.55,56 With hepatic resection however, the situation is more difficult as a more extensive tumour will not be treatable by a more extensive resection.
The development of ultrasound contrast agents and the improving technology of MRI, using iron or gadolinium contrast agents, may enhance the ability to detect satellite or second distant lesions within the liver.57,58 The exact role of this investigation in treatment planning is uncertain and while these may produce major changes in the diagnostic radiology of HCC in the near future, at present their role should be regarded as experimental.
5.6 Liver transplantation or surgery for HCC in cirrhosis
There are no randomised controlled trials comparing the outcome of surgical resection and liver transplantation for HCC. Both techniques are primarily suited to small volume unifocal disease, and only a small proportion of patients with HCC in the UK will be suitable for either of these potentially curative treatments. The decision as to which therapy is appropriate will depend on availability of resources and individual tumour characteristics.
Early results of liver transplantation for HCC were poor59–61 with five year survival figures well below 50%, mainly due to tumour recurrence. It is now clear that this was the result of poor selection of patients for transplantation. It is well established that patients with single lesions of 5 cm diameter or up to three lesions of less than 3 cm in the absence of vascular invasion, as defined by imaging, have an almost zero recurrence rate for HCC and the prognosis after transplantation is the same as for a similar underlying liver disease without HCC.62,63,64 Resection of HCC is a viable option, with short term survival figures very similar to transplantation.60,61,65–69 After three years of follow up however, there is a clear advantage for transplantation in terms of tumour free survival.66,69 Resection is only suitable for patients with excellent liver function (Child Pugh A) because of the high risk of hepatic decompensation. Perioperative mortality in experienced centres remains between 6% and 20% depending on the extent of the resection and the severity of preoperative liver impairment.70–73 The majority of this early mortality is due to liver failure. The residual liver after resection continues to have a malignant potential. Recurrence rates of 50–60% after five years of follow up after resection are usual74,75 and the majority of this recurrence is intrahepatic, representing either satellite nodules or do novo second tumour development. Small satellite nodules are not usually detected by preoperative imaging and where resection is undertaken the use of intraoperative ultrasound may allow detection and better resection margins.76
Fibrolamellar HCC has a very different biology and arises in non-cirrhotic liver. Surgical resection for this tumour is therefore less likely to produce liver failure. The overall survival for fibrolamellar hepatoma at five years is 25–36%.77,78 Because it arises without pre-existing liver disease, fibrolamellar hepatoma usually presents with symptoms, and therefore even though resection may be undertaken there is often vascular or diaphragmatic involvement. Survival rates following resection vary from 65% to 12.5%.79,80 Liver transplantation has been performed for fibrolamellar hepatoma with five year survival rates of 28–49%.81,82 Tumour recurrence is however relatively common and resection remains the mainstay of therapy for this rare tumour, particularly in parts of the world where donor organ shortages exist.
Approximately 7% of hepatocellular cancers, excluding the fibrolamellar variant, arise without cirrhosis. As with fibrolamellar tumours these usually present with symptoms at an advanced stage. Survival overall tends to be longer than with tumours arising in cirrhosis, and five year survival after surgical resection is approximately 25%.83 Liver transplantation has been undertaken for tumours which are too extensive for resection but the results are poor. A review of 77 patients undergoing transplantaion for non-cirrhotic HCC showed a five year survival of 11%.84 Such poor survival figures suggest that resection should remain the primary therapy and transplantation will rarely be offered for this indication.
In patients with cirrhosis, both resection and transplantation probably have a role. In areas of the world where organ donation rates cannot supply existing demand, resection is likely to be widely used. Transplantation probably offers the best chance of cure for patients with small tumours and cirrhosis, and is therefore the treatment of choice, even in Child’s A cirrhosis. In the UK at present, most patients requiring transplantation are able to undergo this treatment without major delay and it should therefore be considered in all suitable cases. Any patient with a single small tumour (5 cm or less) should be assessed for surgery in a centre where resection or transplantation is available.
5.7 Ablative therapy
A number of non-surgical therapies are in clinical use for HCC; percutaneous ablative therapies are well described, most commonly using ethanol injection. Radiofrequency ablation is a relatively new technique where high frequency ultrasound probes are placed into a liver mass, usually under ultrasound control. Series show that tumour necrosis can be produced and that morbidity and mortality are low for both techniques. There are no randomised controlled trails of alcohol injection versus radiofrequency ablation or of either technique versus surgical resection, and assessment of the literature relies on comparisons of series of patients treated by the different techniques.
Although PEI has not been subjected to randomised controlled trials there is a considerable literature on its use in HCC. In large series, complete response rates of 75% in tumours less than 3 cm in diameter have been reported, with five year survival rates of 35–75%.85–88 These studies have generally been restricted to patients with good underlying liver function. The largest series with 746 patients showed 79% and 47% three and five year survival, respectively, in patients with Child’s A cirrhosis (239 patients) and 63% and 29% in Child’s B cirrhosis (149 patients).88 This study was restricted to tumours less than 5 cm in diameter. The results of series from Asia and Europe report similar survival rates. One problem in interpretation of the outcome in these series is that biopsy or fine needle aspiration diagnosis of HCC was not obtained in all series. This clearly could introduce a major error in series with a substantial number of lesions less than 2 cm in diameter where the diagnosis may be uncertain. Treatment of larger and multiple lesions is possible, often requiring repeated sessions and a general anaesthetic, but recurrence occurs in more than 50% at one year, and only 10% of 3–4 cm lesions were completely ablated.89 Treatment is technically very difficult in lesions affecting the posterior segments of the liver.90 Complications are uncommon, but seeding in the needle tract occurs in 3%91 and serious bile duct injury in 1%.86,92 The largest series to report complications92 included 1066 patients. The mean number of sessions needed to destroy a HCC nodule was 6.7. One death (0.09%) and 34 complications (3.2%) were reported, and eight episodes of bleeding and seven cases of tumour seeding occurred. Pain following injection requiring cessation of therapy occurred in 3.2%.
Comparison with other techniques is difficult but most published series where comparisons with historical series were made showed little difference in survival rates between resection, transplantation, and percutaneous alcohol injection in tumours less than 3 cm in diameter. A study of 260 <5 cm tumours in Child A cirrhosis showed a three year survival of 79% for surgery and 71% for PEI compared with 26% for no treatment.93 Similar results have been reported from other centres.94 Most centres still regard surgery as the best proven therapy, providing a chance of cure, but PEI represents the best therapy for patients with small inoperable HCCs.
Experimental studies have been undertaken using agents other than ethanol as a tumour damaging agent (cis-platinum, cold acetic acid) but to date none has shown convincing advantages.95,96
Radiofrequency ablation of HCC is a relatively newly described technique using a probe placed into the tumour mass, usually percutaneously.97–100 It uses high frequency ultrasound to generate heat at the probe tip which can destroy tissue. A single probe can destroy lesions of up to 3 cm and a multiple tipped probe has been used to target lesions of up to 6 cm in diameter. In a single series of 149 tumour nodules treated either percutaneously or at open operation, with an average tumour diameter of 3.5 cm, the local recurrence rate at 19 months was 3.6%, with all nodules showing initial complete ablation.101 Distant metastases or a second tumour developed in 46%. Larger tumours can be treated by radiofrequency ablation; the largest series is 126 HCCs greater than 3 cm in diameter. Complete necrosis was produced in 47%.102 There are few data on long term outcome in larger HCCs.
A comparison of 112 patients treated by percutaneous alcohol injection or radiofrequency ablation showed that 47 of 52 treated by radiofrequency ablation had complete tumour necrosis with a median of 1.2 treatment sessions versus 48 of 60 having complete ablation by alcohol injection with 4.8 sessions required.103 The authors suggested that radiofrequency ablation was more effective but also had a higher complication rate. Unpublished data suggest a possible higher rate of tumour seeding. Randomised trials of alcohol injection versus radiofrequency ablation are required.
5.8 Embolisation/chemoembolisation
Chemoembolisation has been widely used as primary therapy for inoperable HCC. The literature is difficult to interpret and compare, as the techniques used differ substantially and the patient groups treated are frequently those with very advanced disease where the risk of therapy as well as potential benefits may be greatest.
Initial interest in radiological techniques producing tumour devascularisation developed in the 1970s.104 There is good evidence that it is effective at reducing tumour size105,106 and treating pain or bleeding from HCC.107,108 In all of the six initial randomised controlled trials of chemoembolisation as primary treatment for HCC109–114 none show any increase in survival, although tumour shrinkage was seen. All of these trials included patients with predominantly large tumours and severe underlying liver disease, which may have masked any beneficial effect. There is evidence from non-controlled series that small HCCs are more likely to respond to chemoembolisation.106 This has recently been confirmed in a trial of repeated chemoembolisation using lipiodol and doxorubicin versus arterial embolisation without chemotherapy in patients with small tumours and good liver function.115 In the 38 patients treated with chemoembolisation, survival was 63% at two years versus 50% (n=34) in the embolisation group, and 27% (n=35) in the untreated arm. This study establishes the role of chemoembolisation in the treatment of HCC but it will only be applicable to a relatively small group of patients; 903 patients were screened for the trial to enrol 107.112 This has been confirmed in a further randomised trial.116 It is also clear that patients responding to repeated chemoembolisation are likely to be the same group with a significant chance of response to ablative therapy, and randomised trials of these modalities are now required.
Side effects of chemoembolisation are those of the chemotherapeutic agent used (usually doxorubicin) in addition to the complications of arterial embolisation, pain, fever, hepatic decompensation, and rarely infarction of organs other than the liver.117,118 Serious complications occur in 3–5% of treated patients. A small number of studies have combined ethanol injection with chemoembolisation.119–121 There is as yet no evidence available to support this.
Hormonal manipulation with tamoxifen has been the subject of randomised clinical trials. Initial data suggesting a positive effect on survival in patients with inoperable HCC122,123 has not been confirmed in larger randomised studies.124–126 Other agents with hormonal targets, stilbestrol, and flutamide have been used in HCC but there is no evidence of effectiveness. Some authors have suggested that hormonal manipulation may be effective where the oestrogen receptor status is known127–129; this is an area where clinical trials are required.
Chemotherapy given intravenously has a very limited role in the treatment of HCC. The best single agent is doxorubicin with response rates of 10–15%.130,131 More aggressive combination chemotherapy regimens show no improvement in response rates and may even produce a reduction in survival of treated patients.132,133 Any agents used in HCC should be given in the context of clinical trials.
Interferon therapy may have a role in the prevention of HCC in hepatitis C cirrhosis. There is a scientific rationale for this therapy as interferon alpha has a broad range of antitumour activity and is known to be effective therapy for some haematological malignancies. Initial data from both Japan and Europe showed a lower risk of HCC in cohorts of patients with hepatitis C cirrhosis who were given interferon therapy compared with those who were not treated.134–137 This effect was irrespective of the antiviral effects of interferon alpha, and was seen with treatment duration of only three months. These studies were not randomised controlled trials and have inherent selection bias. There is other evidence showing no effect of interferon on tumour development rates138,139 and such tumour preventative therapy in patients with cirrhosis can only be currently recommended as part of clinical trials. Two other approaches to prevent tumour development have been used, retinoids and adaptive immunotherapy. Both of these approaches have been used in the context of prevention of second tumour development after initial tumour resection or ablation. Adaptive immunotherapy, using primed peripheral lymphocytes, showed a significant increase in tumour free survival.140 Retinoids and compounds involved in the vitamin A metabolic pathway are known to be differentiation inducing agents with hypoproliferative effects. A single study using retinol showed a 20% reduction in second tumour development in patients who had been treated with percutaneous alcohol injection.141 Further studies are required in these areas.
Interferon has been used as treatment for HCC rather than for the underlying viral infection. A randomised study using high doses of interferon alpha showed an improved survival142 but a more recent randomised controlled trial of more conventional doses of interferon alpha showed no improvement in survival and a high rate of side effects.143
A single randomised trial of octreotide therapy has suggested a survival benefit in HCC.144 Fifty eight patients were randomised to no therapy or octreotide 250 μg twice daily. Median survival in the treated group was 13 months versus four in the control group. There was also a significant effect on AFP levels. A subsequent study of 70 patients treated with long acting octreotide showed no significant improvement in either survival, quality of life, or AFP levels.145 Further studies using octreotide or its longer acting analogues should be undertaken.
Acknowledgments
The contents of these guidelines were reviewed and revised by Dr J O’Grady, Dr M Lombard, Mr N Heaton, Professor OJ Garden, Dr D Patch, Professor M Bassendine, and Dr A Burroughs on behalf of the British Society of Gastroenterology Liver Section Committee.
This guideline is due for review in 2005.