Article Text

Statistics from Altmetric.com
The relationship between the gut and the liver in primary sclerosing cholangitis (PSC) has puzzled researchers since the relationship was established almost 50 years ago.1 ,2 In Northern European populations, the prevalence of IBD in PSC ranges between 60% and 80%,3 and even in populations where the relationship is less apparent (eg, Asia) typical PSC patients (young males) show similar frequencies.4 It is by now reasonably well established that the type of IBD occurring in PSC differs from UC or Crohn's disease.5 From the clinical perspective, PSC-IBD is typically extensive yet quiescent, and shows a right-sided predominance often with subtle ileal inflammation and rectal sparing. From the genetic perspective, PSC-IBD appears more so an autoimmune condition than apparent for IBD.6 ,7
Only about 8.1% of the patients with IBD develop sclerosing cholangitis.8 The mechanisms are unknown and several explanatory models have been proposed over the years. The earliest hypotheses were built on a ‘leaky gut concept’, in which the mucosal injury in IBD would lead to ‘leakage’ of bacteria and bacterial products into the portal circulation.9 Later, a gut–liver T-cell trafficking axis emerged in which gut-derived T cells would contribute to biliary inflammation.10 A more recent hypothesis relates to the possibility of an antigen deriving from colonic content driving biliary inflammation,11 along the same logic dietary gluten drives small intestinal inflammation in coeliac disease.12 Common to all hypotheses is the gut is to blame for what happens to the bile ducts. So what is actually found there—in the gut?
There have been rapid advances in our knowledge on the composition and physiology of the gut microbiota in health and disease over the last 5 years.13 The field has opened up due to technological advances. DNA sequencing now allows for relatively cheap characterisation of the bacterial composition of any given sample. The same technology allows for complete characterisation of the genetic variability of the bacterial content (metagenome sequencing),14 as well as similar assessments of gut-resident viruses (the gut virome) and fungi (the gut mycobiome).15 ,16 The gut microbiota in metabolic and inflammatory diseases show significant deviations from the healthy state, typically with reduced diversity of the overall bacterial flora (loss of microbial diversity) and altered abundance of particular bacteria.
A series of small studies have now established that the gut microbiota in PSC differs from that of patients with IBD without PSC and healthy controls.17–23 The sample size of the studies ranges from 12 to 85 patients with PSC (table 1). Data from altogether 283 patients with PSC have so far been reported and some general considerations can be drawn from this growing pool of observations:
Gut microbial diversity appears reduced in PSC.
Genus and species level findings are mostly inconsistent between studies.
The gut microbial community composition in PSC exhibits biomarker utility.
Studies of the gut microbiota in primary sclerosing cholangitis (PSC)
Biodiversity loss is a critical concern of any ecosystem.24 ,25 The loss of microbial diversity observed (LOMD) in a variety of disease states, PSC now included, is hitherto the major outcome of studies of the gut microbiota in humans.26 The debate as to an inherent ‘chicken and the egg’ problem of this general observation cannot be firmly concluded. Most studies performed in human diseases to date have analysed mucosal or stool samples from diseased individuals, in which the LOMD can be a consequence as much as a cause of the disease. In Crohn's disease, LOMD appears independent of severity of inflammatory affection.27 In type 1 diabetes, LOMD precedes onset of disease and associates with autoantibody positivity in individuals at risk.28 ,29 As such, the LOMD may be pathogenic and itself originating from dietary alterations and specific environmental changes (antibiotics included). Along this thinking, the LOMD observed in PSC may play a causal role in disease development by mechanisms that remain to be established.
The sources of bias in studies of the gut microbiota are numerous and span diverse aspects including sampling challenges, dietary constituents and other exposures (eg, smoking), technology (eg, primer bias), analytical bias (eg, software and reference database) along with disease-related factors (eg, inflammation and drugs). By the study of healthy and population-derived individuals,14 ,30 the impact of these factors on the outcome of gut microbiome assessments is increasingly clear. Several points are noteworthy regarding our interpretation of data from the PSC studies. Most importantly, data on relevant confounders are incomplete (at best) and mostly missing. This particularly accounts for dietary data and markers of inflammation (calprotectin). Furthermore, study size of the PSC reports (n<100) is likely too small to account for the noise introduced by the many confounders. As evident in these larger analyses (n>1000),14 ,30 the impact from each variable is also small (<2–3% of the variance), making PSC assessments so far severely underpowered.
On this background, the inconsistency of findings at the genus and species level between studies of the gut microbiota in PSC so far is not surprising (table 1). Most of these are likely to represent type 1 statistical errors and should be interpreted with caution. The current studies remind me of the candidate-gene era of genetics, when gene findings were flourishing and rarely reproduced. Only upon large-scale international collaborations and considerable enhancement of study size, robust findings were obtained.7 This should also be the way forward for studies of the gut microbiota in PSC, and consensus within the PSC community on collection of confounders is urgently needed. The Veillonella/Streptococcus (symbiosis) finding is an interesting exception in this regard,26 but may, as evident in the Sabino et al analysis (table 1) and related studies of lung microbiota,31 associate with disease stage and fibrosis development more than PSC per se.
Patients with PSC are in desperate need of improved diagnostics and therapy. The discriminatory efficacy of gut microbial signatures to distinguish PSC with IBD from patients with IBD without biliary disease should be pursued for its ability to also determine early-stage PSC. As to therapeutic options the road will be longer. Antibiotics influence alkaline phosphatase levels in patients with PSC,32 which has led to trials on long-term administration in paediatric populations (eg, NCT02137668). I would want to pose a word of caution in this regard, since antibiotics potentially would add to microbial disturbances shown to associate with PSC (eg, LOMD) and since protective features of the gut microbiota may also be affected.14 ,33 ,34 Similar considerations would apply to other interventions currently undertaken (eg, faecal transplantation, NCT02424175). Signals of efficacy by surrogate markers (eg, alkaline phosphatase) in these early-phase trials should be interpreted as additional evidence the gut microbiota plays a role in PSC pathogenesis (proof-of-concept, not proof-of-therapy).
Careful dissection of the biological relationship between this new co-variable in PSC research and biliary immunology and physiological functions should be the next step, and may open up the ‘black box’ of PSC that so far has positioned us devoid of appropriate management of our patients. These efforts will need to move beyond the current level of refinement (species and genus level) by the application of metagenome sequencing to determine gene content associations as markers of functional biology. Findings will need to be complemented by metabolic (eg, bile acid measurements35) and immunological assessments (figure 1), and the role of the biliary microbiota in these patients should be studied in parallel.36–38 The ‘PSC bug’ is unlikely to exist. However, the perception of the gut microbiota as a complex physiological machinery that integrates with host metabolism and immune functions goes beyond such simplistic models. As such, the direction of the field taken by the ‘new model’ of PSC is a wise one, where the gut is still to blame as in the previous models, but where the mechanism of the involvement is kept open for the research to come.
{kind=link}
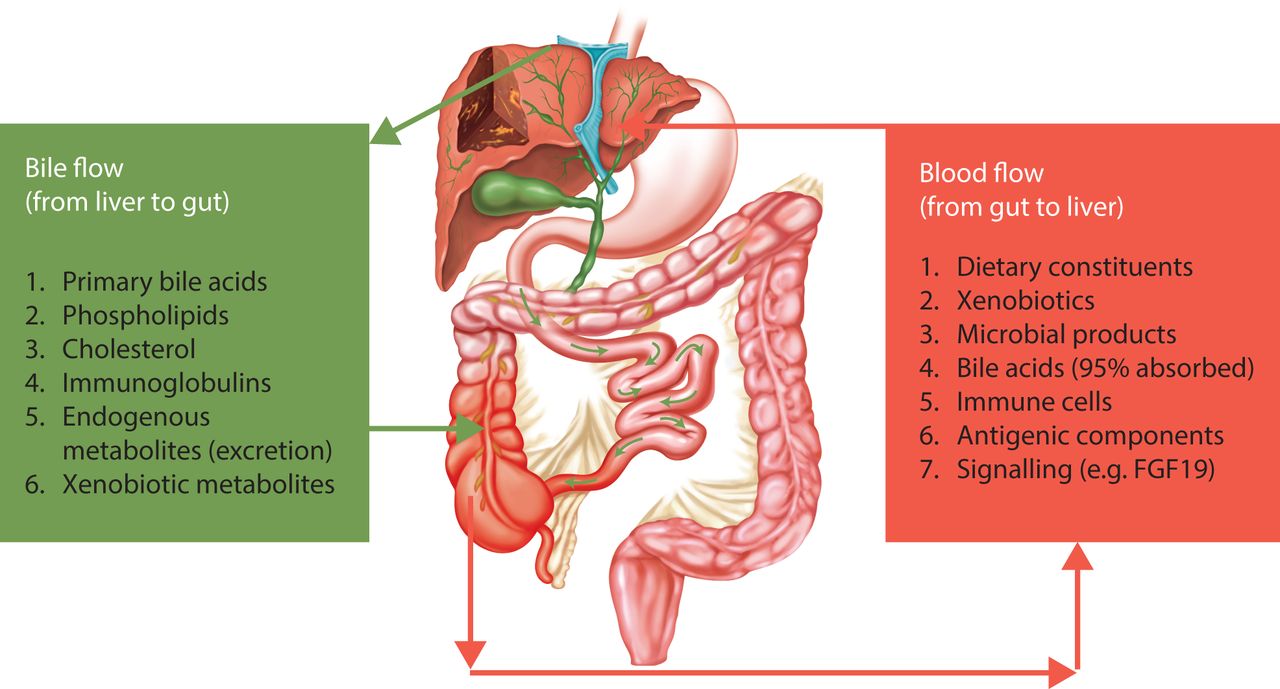
Simplified illustration of the bidirectional relationship between the gut and the liver in primary sclerosing cholangitis (PSC). In an anatomical perception, PSC is a disease with inflammatory affection throughout the distribution of the enterohepatic and cholehepatic circulation of bile acids (terminal ileum, proximal colon, large bile ducts). As shown by recent studies (table 1), the gut microbiota as an integral part of this machinery is disturbed, either by primary or secondary mechanisms. Studies aiming to understand how inflammation develops throughout these mucosal surfaces in PSC need to account for these observations and their implications for human metabolism and immune function.
References
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.