Article Text

Statistics from Altmetric.com
- ulcerative colitis
- intestinal microbiota transplantation
- inflammatory bowel disease
- faecal microbiota transplantation
We read with interest the paper by Ng et al, 1 which discussed the need to optimise faecal microbiota transplantation (FMT) processes in order to increase its therapeutic potential, especially in inflammatory bowel disease (IBD). While there is randomised controlled trial evidence that FMT can be effective in the induction of remission in patients with ulcerative colitis (UC),2–5 the durability of therapeutic response following FMT cessation is unknown. Furthermore, there is limited long-term safety data following FMT, especially in patients with IBD. In the FOCUS study, FMT delivered via an initial colonoscopy infusion, followed by enema therapy for 8 weeks was effective in mild to moderate UC remission induction.2 Here, we report the long-term outcomes from the FOCUS study.
Enrolled study participants who received FMT (2013–2015) were contacted to assess time to disease relapse for patients in clinical remission following FMT induction (defined as worsening symptoms requiring escalation of medical therapy or surgery), disease progression and the development of adverse events or new medical conditions.
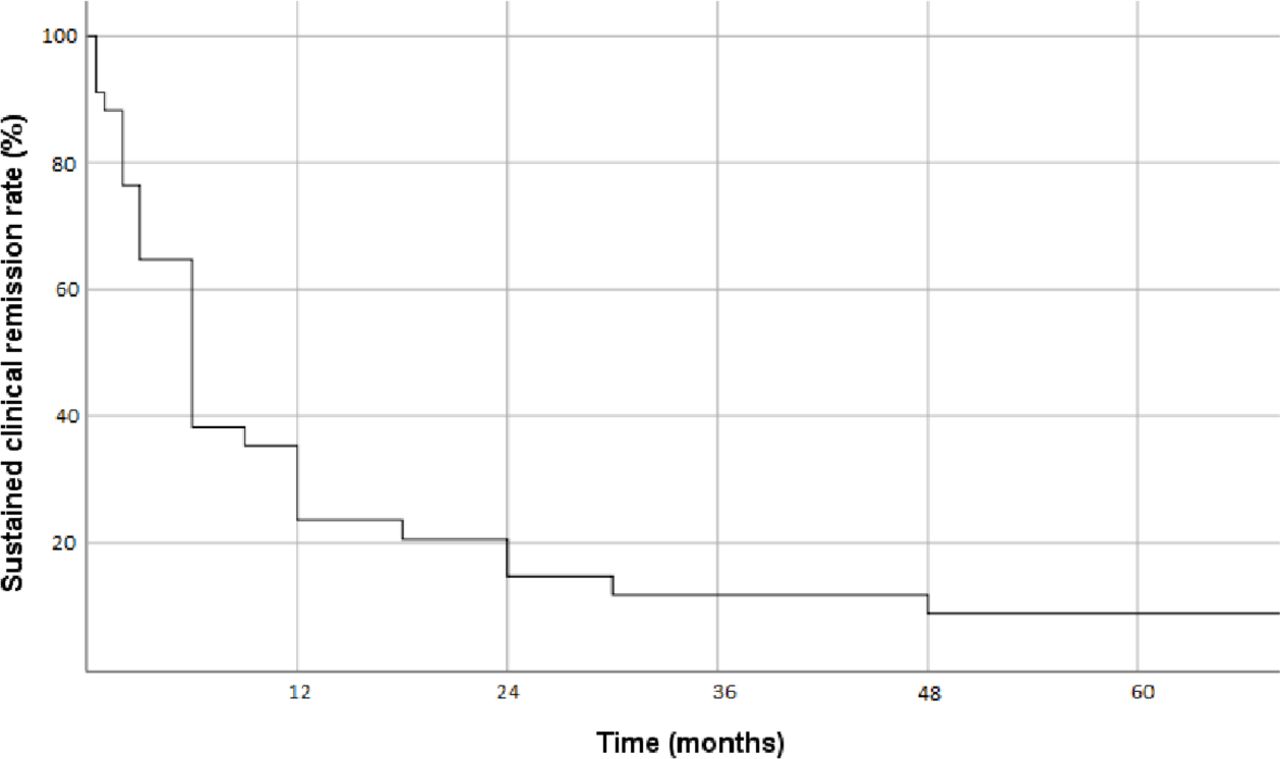
Long-term data were obtained from 87% (68/78) of participants who received FMT, with a median follow-up of 66 months (IQR 62–69 months). Of the 35 patients achieving steroid-free clinical remission after FMT, the median time to disease relapse was 6 months (figure 1). Remission for over 12 months was noted in 12 patients (34·2% of patients in remission at study conclusion; 15·4% of FMT recipients), of whom three patients (3·8% of FMT recipients) had sustained clinical remission over 5 years poststudy conclusion. All patients in remission for more than 12 months had either self-initiated further FMT (n=3) or implemented some form of dietary modification (n=9). Common elements of reported dietary modification included high dietary fibre and decreased intake of animal fats and processed foods (See online supplemental Appendix).
Supplemental material

{kind=link}
Time to UC disease relapse for patients in clinical remission following FMT induction defined as worsening symptoms requiring the escalation of medical therapy or surgery. FMT, faecal microbiota transplantation; UC, ulcerative colitis.
Twenty-nine patients (42·6%) were on biological medications (tumour necrosis factor (TNF) inhibitor, n=12; vedolizumab, n=14; tofacitinib, n=2; ustekinumab, n=1) at follow-up. Six patients (7·7%) underwent a proctocolectomy for disease worsening, with an additional patient undergoing surgery for colonic adenocarcinoma in longstanding UC. There were no related serious adverse events or adverse events of special interest related to infection. Adverse events deemed possibly related to FMT included fibromyalgia in a 44-year-old man, and a perianal fistula attributed to trauma from enema self-administration.
This is the first reported long-term outcomes following FMT in patients with UC. It indicates limited durability of treatment response in the absence of adjunctive therapies. All patients in clinical remission for greater than 1 year had either further FMT or adhered to some form of dietary modification, suggesting a need for ongoing microbial manipulation to maintain disease control after remission induction with FMT. The role of maintenance FMT in UC is unclear. A single trial of 61 patients did not demonstrate a difference in its primary endpoint of steroid-free clinical remission but did show improvement in more rigorous secondary endpoints of endoscopic and histological remission.6 We did not see any long-term safety signal or adverse outcomes from FMT in UC in our limited cohort.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @NOKaakoush
Contributors CH, RP, NOK, RL, TB, MK and SP designed the study. CH and AS were responsible for data collection and analysis. CH and SP wrote the initial draft of the correspondence. All authors critically reviewed the correspondence and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests CH has received speaker fees and educational support from Janssen, Pfizer, Takeda, Ferring and Abbvie; and received a research grant through the Royal Australasian College of Physicians. AS has no disclosures. RP has received speaker fees or research support from Janssen, Aspen, Pfizer, Abbvie and Takeda. NOK has no disclosures. RL reports advisory board fees from AbbVie, Aspen, Celgene, Ferring, Gilead, Hospira, Janssen, MSD, Novartis, Pfizer, and Takeda; research fees from Gastrointestinal Society of Australia (GESA), Endochoice, Janssen, National Health and Medical Research Council of Australia, Shire, and Takeda; and speaker fees from Emerge Health, Ferring, Janssen, Shire, and Takeda. TB has interests in Redhill Biopharma, and Finch Therapeutics, as well as in the Centre for Digestive Diseases, where faecal microbiota transplantation (FMT) is a treatment option for patients. He has filed patents relating to FMT. MK has received speaker fees, research funding, educational support or honorarium for advisory board participation from Ferring, AbbVie, Janssen, Takeda and received research support from AbbVie. SP is a consultant for Finch Therapeutics; has received speaker fees from Ferring, Janssen and Takeda; and has received a National Health and Medical Research Council of Australia Investigator Grant.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.