Article Text

Statistics from Altmetric.com
Surgical Section in Association with the Association of Coloproctology (ACPGBI) and IBD Section joint symposium
001 CLINICAL AND MOLECULAR CHARACTERISTICS OF ISOLATED COLONIC CROHN’S DISEASE
L. Hancock1,2, T. Ahmad1, B. F. Warren3, N. J. Mortensen2, D. P. Jewell1.Departments of 1Gastroenterology, 2Colorectal Surgery, 3Histopathology, University of Oxford, Radcliffe Infirmary, Oxford OX2 6QX, UK
Background: Clinical, serological, and molecular data support the existence of discrete subsets of Crohn’s disease (CD) defined by location of disease. Little is known about the epidemiology and natural history of isolated CD of the colon (Montreal Classification L2) because most studies have not accurately distinguished L2 from L3 disease (ileo-caecal).
Aims: (1) To describe the clinical features and natural history of isolated colonic CD in a rigorously characterised patient cohort. (2) To confirm the association with HLA-DRB1*0103, reported in smaller cohorts, and to investigate its role in predicting disease course and need for surgery.
Methods: Patients with L2 disease were identified from a database of 1318 CD patients. Only patients with a normal small bowel enema (70%), ileoscopy alone (30%), or both (20%) were included. No patients had capsule endoscopy. HLA genotyping was performed using PCR-SSP.
Results: 136 (10.3%) patients were classified with L2 disease after a median follow up of 10.8 years (range 1.4–39.8). The mean age at diagnosis was 30.7 years. L2 disease was more common in women (74.3% v 61.0%; p = 0.001; RR = 1.7) and in never smokers (52.2% v 41.3%; p = 0.007; RR = 1.5). 29.4% and 14.0% reported a family history (1st or 2nd degree) of CD and UC respectively. Stricturing colonic disease was noted in 10% of patients. 12% of the entire cohort received ⩾1 Infliximab infusion and 19% underwent colonic resection for severe disease (cumulative risk at 2 years, 10.6%; 5 years, 17.1%; 10 years, 32.8%). We confirmed the association with DRB1*0103 (14.7% cases v 2.7% controls; p = 5.5×10−9; RR = 3.2) and report the novel association of this allele with time to first surgical event (Log Rank p = 0.002) and time to first “severity event” (resection/diversion ileostomy/Infliximab) (p = 0.001).
Conclusions: This study reports the clinical manifestations of isolated colonic CD. We confirm the association with HLA-DRB1*0103 and further demonstrate that this allele may predict disease course.
002 ANALYSIS OF CCL20 VARIANTS IN IBD PROVIDES FURTHER EVIDENCE FOR GENETIC HETEROGENEITY IN DISEASE SUSCEPTIBILITY
C. W. Lees, E. R. Nimmo, R. K. Russell, J. van Limbergen, A. Smith, H. E. Drummond, J. Satsangi.GI Unit, Molecular Medicine Centre, University of Edinburgh, UK
Introduction: Recent data have suggested that variants of the CCL20 gene are associated with susceptibility to ulcerative colitis (UC).1 In a South Korean population, the 1706G→A polymorphism in the CCL20 promoter was strongly associated with susceptibility to UC (p<0.0001).1 These data have yet to be replicated in other populations. The CCL20 gene is located on chromosome 2q36.3 in a short haplotype block containing no other genes (see http://www.hapmap.org). The protein is a key immunological signal, fundamental to the pathogenesis of inflammatory bowel disease (IBD). We have assessed the contribution of the 1706G→A polymorphism in determining susceptibility and disease phenotype in UC and Crohn’s disease (CD).
Methods: 523 UC, 442 CD, and 351 healthy controls (HC) were studied. The Scottish IBD population was 100% white with a mean age of diagnosis of 28.1 years. Genotyping for the 1706G→A variant was carried out using the Taqman system for allelic discrimination.
Results: In all Scottish IBD cases there was a non-significant increase in the allelic frequency and carriage rate of the variant A allele compared with HC (see table). Genotype analysis reveals borderline increased heterozygosity in Scottish IBD compared with HC (p = 0.049, RR 1.37).
Abstract 2
Conclusions: The weak effect in the Scottish population contrasts strongly with the strong effect in the South Korean population. Heterogeneity between Eastern and Northern European populations is the most plausible explanation, paralleling the experience of NOD2/CARD15 in CD.2 Direct sequencing has been performed and the contribution of further SNPs is currently under study in both the Scottish population and in complementary Scandinavian and Japanese studies.
1
2
003 INTENSIVE GRANULOCYTE AND MONOCYTE APHERESIS VERSUS INTRAVENOUS PREDNISOLONE IN PATIENTS WITH SEVERE ULCERATIVE COLITIS: A MULTICENTRE RANDOMISED CONTROLLED STUDY
H. Hanai1, T. Iida1, F. Watanabe2, M. Yamada3, K. Takeuchi1, M. Kikuyama4, Y. Maruyama2, Y. Iwaoka3, K. Hirayama5, A. R. Saniabadi6.1Department of Medicine, Hamamatsu University; 2Fujueda General Hospital; 3Hamamatsu Medical Centre; 4Hamamatsu Rosai Hospital; 5Hamamatsu Insurance Hospital; 6Japan Immunoresearch Laboratories, Japan
Background: Recently several uncontrolled studies have reported on the efficacy of adsorptive depletion of peripheral blood granulocytes and monocytes/macrophages (GMA) in patients with moderate or severe ulcerative colitis (UC). This study compared the efficacy and safety of intensive GMA with intensive intravenous (iv) prednisolone (PSL) in patients with severe UC.
Methods: Sixty six patients with clinical activity index CAI 10–18 were randomly assigned to intensive GMA with the Adacolumn, at two sessions/week in the first 3 weeks and then one session/week for up to 10 sessions (n = 33) or iv PSL, 40–60 mg/day for 5–10 days. Up to 65% of granulocytes and monocytes/macrophages and a small fraction of lymphocytes (FcγR and complement receptors bearing leucocytes) adhere to the column leucocytapheresis carriers. No patient received immunomodulators. Efficacy was assessed at weeks 2, 6, 12.
Results: Four patients in the PSL group withdrew within the first 5 days, while all 33 patients in the GMA group completed their treatment course. At weeks 2, 6, and 12, the remission (CAI = or <4) rates (%) in the GMA group were 9.1, 54.5, 75.8, respectively. The corresponding values in the PSL group were 21.2, 45.5, and 39.4. In the GMA group, flushing and light-headedness were observed in four patients versus typical steroid side effects in 43% of the PSL group.
Conclusions: In this study, GMA appeared to be safe and induce sustainable remission in the majority of the treated patients compared with PSL. The results support the view that granulocytes and monocytes/macrophages, which in patients with UC are elevated with activation behaviour and increased survival time contribute to the exacerbation and perpetuation of UC.
Liver free papers
004 FACTORS ASSOCIATED WITH EARLY MORTALITY IN DECOMPENSATED ALCOHOLIC LIVER DISEASE: THE EFFECT OF CORTICOSTEROIDS
E. McFarlane, J. Kerss, J. Jones, J. Skinner1, D. Gleeson.Liver Unit, Sheffield Teaching Hospitals; 1West Sheffield Primary Care Trust, Sheffield, UK
Background: Determinants of mortality in severe alcoholic liver disease (ALD) are incompletely characterised and the benefits of corticosteroids remain uncertain.
Aim: Assessment of factors associated with short term survival in patients with first presentation of decompensated ALD (defined as Child grade B or C).
Methods: Review of 227 patients (150 men, median age 50 (range 28–77) years), presenting consecutively between 1/4/98 and 31/3/05. Townsend and Jarman indices of social deprivation derived from postcodes in the 155 Sheffield residents.
Results: Median of initial hospital stay was 14 (range 0–93) days, during which 37 patients (16%) died. Overall survival 28 and 84 days after admission was 89% and 78% respectively. In 92 patients with Maddrey-Discriminant Function >32 on day 1 (admission) or day 7, 28 day survival was higher in patients receiving corticosteroids (n = 27) than in those (n = 65) who did not. (89 (SD 6)% v 69 (SD 6)%). After 84 days these differences were not significant (70 (SD 9)% v 57 (SD 7)%). Using Cox regression analysis, MELD, Glasgow scores and Maddrey scores on day 1 were all found to be highly predictive of 28 and 84 day survival (p = 0.00–0.01). Corticosteroid treatment was not a significant covariate with these scores. However, together with MELD and with Maddrey scores at day 7, corticosteroid treatment was an independent predictor (p<0.05) of survival at 28 days, although not at 84 days. A similar interaction with Glasgow score at day 7 was almost significant (p = 0.055). Age, gender, presence of infection or gastrointestinal bleeding, serum sodium, serum AST, and Townsend and Jarman social deprivation scores were not significant predictors of 28 or 84 day mortality.
Conclusions: The most important predictors of early mortality in decompensated ALD are the MELD, Glasgow, and Maddrey scores. Data are consistent with a modest beneficial effect of corticosteroid treatment on survival at 28 days.
005 HEPATIC INFLAMMATION INCREASES PORTAL PRESSURE THROUGH INHIBITION OF ENOS ACTIVITY: POTENTIAL MECHANISMS
R. P. Mookerjee, N. A. Davies, S. J. Hodges, R. N. Dalton1, R. Williams, R. Jalan.Institute of Hepatology, University College London, London WC1E 6HX, UK; 1Guys Hospital Medical School, Kings College, London SE1 9RT, UK
Background: Previously we have described an acute and sustained reduction of portal pressure in alcoholic hepatitis (AH) patients following anti-TNFα antibody therapy. Animal data suggest inflammation can modulate eNOS activity by reducing the hepatic metabolism of an endogenous inhibitor, ADMA.
Aims: (1) To demonstrate reduced eNOS activity in AH compared to cirrhosis alone. (2) To assess hepatic tissue ADMA, and NOSTRIN (NOS traffic-inducing protein) and Caveolin-1(other mediators believed to modulate eNOS activity).
Methods: HVPG and hepatic blood flow (HBF) (ICG extraction) was measured in 24 decompensated cirrhotics undergoing TJ biopsy, 15 of whom had additional AH defined histologically. Additional measures in a subset of patients: tissue eNOS activity (variation of 3H-arginine to 3H-citrulline assay); tissue ADMA quantification (isotope dilution electrospray mass spectrometry); NOSTRIN and Caveolin-1 mRNA quantification (real time PCR).
Results: AH patients had significantly higher HVPG compared to only cirrhosis (24 (SD 2.5) v 15.7 (SD 1.3) mmHg; p = 0.007) and lower HBF (p = 0.03). Hepatic tissue eNOS activity was significantly lower in AH patients (p<0.05) and ADMA levels significantly higher (p<0.05) compared to cirrhotics. Mean CT values for mRNA expression in hepatic tissue for AH v cirrhosis were: NOSTRIN: 2.3 (SD 0.3) v 3.4 (SD 0.2); p = 0.01; Caveolin-1: 4.6 (SD 0.3) v 6.3 (SD 0.4); p = 0.007 (the lower the value, the higher the expression—that is, fewer PCR cycles required for detection).
Conclusion: Superadded inflammation on cirrhosis in AH patients is associated with higher portal pressures, reduced hepatic blood flow, and significantly reduced eNOS activity. Furthermore, AH patients have high hepatic tissue ADMA, and increased expression of NOSTRIN (an inhibitory protein believed to translocate eNOS to intracellular sites away from interaction with its substrate, arginine) and increased Caveolin-1 (an eNOS inhibitor described in animal cirrhotic models). Our findings suggest that hepatic inflammation in AH exacerbates portal hypertension through multiple and complex regulators of hepatic eNOS, which could serve as targets for future therapy. To address causal relationships of these eNOS regulators with inflammation requires studies in appropriate models.
006 AN ASSESSMENT OF CARDIOVASCULAR MORBIDITY AND MORTALITY FOLLOWING ORTHOTOPIC LIVER TRANSPLANTATION
N. C. McAvoy, J. W. Ferguson, P. C. Hayes.Scottish Liver Transplant Unit, Royal infirmary of Edinburgh, UK
Background: Cardiovascular (CV) disease is a major cause of morbidity and mortality in the first year post OLT and, in the limited studies performed to date, it accounts for between 30 and 70% of major clinical events.
Aims: The American College of Cardiology (ACC) has issued guidelines aimed at identifying patients at risk of cardiac disease. The aim of this study was to (1) document the prevalence of CV risk factors pretransplantation in OLT recipients and (2) the incidence of CV events following OLT. We also evaluated the use of ACC clinical predictors as a guide to identifying patients in a high risk group.
Method: Single centre retrospective observational study. We studied 100 consecutive patients who underwent OLT from July 2000–December 2002. Only patients with chronic liver disease who were undergoing elective OLT were included. Cardiac risk factors were identified at transplant assessment and patients were followed for 6/12 post OLT. The incidence of CV events or cardiovascular death was recorded. Predictors of CV risk as defined by ACC guidelines; two or more of the following (obesity, hypertension, smoking, elevated total cholesterol, family history of premature CV disease, age >50 years) or one of the following (previous MI or CVA, abnormal echocardiogram, evidence of an arrhythmia, LBBB, ST, or T wave changes on ECG). A cardiac event was defined as CV death, non-fatal myocardial infarction, hospitalisation for myocardial ischaemia or cardiac failure, stroke or transient ischaemic attack, or coronary revascularisation.
Results: Ninety three patients (56 males and 37 females) were studied in total. Seven patients were excluded (three transplanted for acute liver failure and four retransplants). Indications for transplant were ALD 22 patients (23.7%), PBC 20 patients (21.5%), HCC 12 patients (12.9%), PSC 11 patients (11.8%), cryptogenic cirrhosis 11 patients (11.8%), Hepatitis C seven patients (7.5%), CAH three patients (3.2%), and other causes such as haemachromatosis, Wilson’s disease, and Caroli’s syndrome accounted for the remaining seven patients (7.5 %). The mean age at transplant was 54.8 years. 21.5% of patients were smokers, 20.4% had a diagnosis of DM and 10.8 % of patients had documented hypertension. Mean BMI was 26.6 with 28% of patients classified as obese with a BMI>30. During the 6/12 follow up period seven patients died (7.5%), with two deaths attributable to CV events. Non-fatal CV events occurred in 10 patients (10.8%) (three had MI, one CCF, four documented arrhythmias, one new onset angina, and one CVA). Preoperatively 38.7% of patients were deemed to be at high risk of CV events with only 50% of total CV events occurring in this group.
Conclusion: 12.9% of our patients had a CV event within six months of OLT. The American College of Cardiology clinical predictors of CV risk did not identity the group of patients who are at increased risk of CV events post OLT, with half the patients being in the low risk group.
007 HOW GOOD ARE WE AT MINIMISING CARDIOVASCULAR RISK FOLLOWING ORTHOTOPIC LIVER TRANSPLANT?
D. G. Oliver, K. Agarwal, D. Manas, M. Hudson.Freeman Hospital, Newcastle-upon-Tyne, UK
Introduction: Cardiovascular complications are a major cause of late morbidity and mortality following liver transplantation. Treatable risk factors are possibly overlooked during long term follow up. In Newcastle, 40 orthotopic liver transplants (OLT) are undertaken every year but no formal strategy exists to minimise post-transplant cardiovascular disease.
Aim: To assess the prevalence of pre- and post-transplant risk factors for cardiovascular disease in a cohort of patients who underwent OLT between 1997 and 1999 and who were randomised to either tacrolimus or cyclosporin as part of the TMC study.
Methods: Retrospective review of patients’ hospital records.
Results: Forty three patients (18 female, 10 smokers, median age at OLT = 57 years) were included over a median follow up time of 72 months. Indication for transplant was alcoholic liver disease (17), autoimmune liver diseases (13), cryptogenic cirrhosis (4), viral hepatitis (2), fulminant liver failure (2), tumours (2), others (3). Two patients had ischaemic heart disease before transplant, eight (19%) suffered a cardiovascular event post-transplant. Seven patients died, none from cardiovascular complications. 84% patients gained weight with 28% being obese (body mass index >30 kg/m2) by three years. Only 56% patients had a pretransplant cholesterol checked and of these 21% were above 5 mmol/l. 63% developed hypercholesterolaemia after transplantation but only 20% were treated for this. Eleven patients developed new onset or a progression of diabetes. Nine (75%) of all diabetics had blood pressure recordings persistently outside national target ranges despite seven being on antihypertensive treatment and four (33%) developed cardiovascular complications. Neither weight gain nor diabetes were associated with choice of immunosuppressant. Twenty seven (63%) patients developed hypertension requiring drug therapy post OLT.
Conclusion: Liver transplant patients have a one in five chance of suffering a significant cardiovascular complication in the first six years. Several of the risk factors are undertreated or underrecognised. A formal long term programme of assessment, risk stratification, and appropriate therapy should be mandatory for all liver transplant patients in the UK.
008 MANAGEMENT OF BLEEDING ECTOPIC VARICES: THE EDINBURGH EXPERIENCE
N. Kochar1, D. Tripathi1, N. C. McAvoy1, H. Ireland2, D. N. Redhead2, P. C. Hayes1.1Department of Hepatology and 2Department of Radiology, Royal Infirmary of Edinburgh, UK
Introduction: Bleeding from ectopic varices is uncommon but can be difficult to manage. We report our experience of uncontrolled bleeding from ectopic varices managed by insertion of TIPSS.
Methods: Patients in whom TIPSS was inserted for ectopic varices were selected from a TIPSS dedicated database.
Results: Over 14 years, 732 TIPSS have been inserted. TIPSS was inserted for bleeding ectopic varices in 24 (11 male) patients. Mean age (SD) at TIPSS insertion was 56.6 (10.6) years. Mean (SD) Child Pugh score was 7.6 (1.84); A/B/C (%): 9/59/32. Aetiology of liver disease: (alcoholic 15, cryptogenic 3, viral 2, others 4). Site of bleeding was rectal 11, stomal 7, duodenal 3, caput medusae 1, falciform ligament varix 1, and intraperitoneal varix 1. TIPSS was successful in 23/24 (96%). Complete data available on 20 patients. Portal pressure gradient (PPG) fell from 19 (6.34) to 7.47 (3.84) mmHg. Covered stents were used in four patients. Embolisation of varices was performed in four at the initial procedure. TIPSS insertion was initially effective in controlling bleeding in 18 (90%) patients. In four (covered stents 2, uncovered stents 2) of these patients bleeding recurred at 13 to 202 days after TIPSS insertion. This necessitated parallel shunt insertion for occluded shunts in two, shunt extension for shunt insufficiency in one, thrombin injection into the stomal varix in two patients and embolisation of varices in one. These measures effectively controlled rebleeding in three patients and the fourth patient continues to have intermittent bleeding despite patent TIPSS. TIPSS was unsuccessful in controlling bleeding in two patients and one of these died due to liver failure eight days post TIPSS. Fourteen patients died (7 liver related, 1 due to GI bleed) since the TIPSS insertion and six patients had liver transplant at a median duration of 248 (5 to 1869) days.
Conclusions: TIPSS is effective in the management of bleeding ectopic varices. Variceal rebleeding is frequently related to shunt insufficiency. Additional therapies such as thrombin and embolisation may be effective in difficult cases and may have a role in index therapy as an adjunct to TIPSS.
009 LONG TERM FOLLOW UP OF ENDOSCOPIC HISTOACRYL INJECTION FOR THE MANAGEMENT OF GASTRIC VARICEAL BLEEDING
N. Rajoriya, J. Gray, D. Gaya, G. Reid, E. H. Forrest, A. J. Morris, J. F. MacKenzie, R. C. Carter1, C. J. McKay1, R. Stuart1, A. J. Stanley.Department of Gastroenterology and 1Surgery; Glasgow Royal Infirmary, UK
Background and Aim: The optimum therapy for gastric variceal bleeding is unclear. Several treatments are available including endoscopic injection of histoacryl glue (HA). However, most data describes only short term follow up. We studied the long term efficacy of HA as treatment for bleeding gastric varices in our hospital.
Method: Endoscopy records were used to identify patients requiring HA for gastric variceal bleeding between 2001–05. A standard protocol of 1:1.4 histoacryl and lipiodol mixture was used. Case notes were reviewed to obtain data on efficacy, complications, and outcome.
Results: Thrty three patients (85% male; average age 53.7 (SD 12.4) years) received HA for gastric variceal bleeding. Aetiology of liver disease was: alcohol 70%, alcohol and HCV 10%, NRH 6%, HBV/HCV 6%, other 9%. Childs grade was A, B, and C in 45%, 41% and 14% respectively. 30% patients had prior IV vasopressor therapy and 58% were actively bleeding during the procedure. Immediate haemostasis achieved in 100%. Two patients developed a pyrexia within 24 hours of HA which settled with antibiotic therapy. No other complications were encountered. The mean follow up for all patients was 24 months (33 months for survivors). The mean number of endoscopy sessions for treatment was two (average of two injections HA per session). 48% patients had subsequent endoscopic ultrasound assessment of their varices. 15% required TIPS during follow up and none had surgery. 6% rebled as an inpatient (3% within 48 hours). Six and 12 month gastric variceal rebleeding rates were 18% and 21% respectively, with no rebleeds after one year. Inpatient, 6 month, 12 month, and 2 year mortality was 3%, 27%, 33%, and 36% respectively.
Conclusion: Endoscopic injection of histoacryl glue appears to be a safe and effective treatment for gastric variceal bleeding, although randomised trials are required to compare it with other therapies.
010 WITHDRAWN
011 INVESTIGATING THE ROLE OF VASCULAR ENDOTHELIAL GROWTH FACTOR SIGNALING IN CEREBRAL OEDEMA DUE TO EXPERIMENTAL ACUTE LIVER FAILURE
R. J. Aspinall1,2, S. Weis2, L. Barnes2, D. A. Cheresh2, P. J. Pockros1.1Division of Gastroenterology/Hepatology, Scripps Clinic, La Jolla, CA 92037; 2Moores UCSD Cancer Center, University of California San Diego, La Jolla, CA 92093, USA
Introduction: Cerebral oedema remains a major cause of mortality in patients with acute liver failure (ALF). Vascular endothelial growth factor (VEGF) mediated increases in endothelial permeability have been shown to cause cerebral oedema around neoplasms, strokes, and in acute lead poisoning. The effects of VEGF on permeability are mediated by the VEGF receptor Flk and the Src family kinases, Src and Yes (Weis et al, J Clin Invest 2004). We examined whether these pathways might also contribute to cerebral oedema in a murine model of experimental acute liver failure.
Methods: ALF was induced by ip injection of azoxymethane 100 μg/g. Mice were either Balb/c, Tie2-GFP, VEGF-GFP transgenic, or Yes or Fyn knockout strains. Animals were actively maintained in isothermic conditions and ip dextrose used against hypoglycaemia and dehydration. Plasma VEGF levels were measured by ELISA. Size selective BBB permeability was assessed using tracer dyes of varying molecular weight. Brains were harvested for immunohistochemistry, confocal microscopy, and quantitative PCR of VEGF, Flk and Flt mRNA. Histological specimens and protein lysates for immunoblotting were also prepared from livers and brains at set time points.
Results: All mice developed severe hepatic necrosis on histology. Encephalopathy progressed through to coma and death. Plasma VEGF levels were undetectable in normal mice but rose significantly after liver injury, reaching a mean of 172 pg/ml (SD 45) by Grade III/IV (p<0.001). VEGF-GFP transgenic mice with advanced ALF demonstrated enhanced fluorescence of astrocytes in the cerebral cortex.
Discussion: Both cerebral and circulating levels of VEGF are significantly raised following azoxymethane induced liver failure in mice. We are currently examining the effects of genetic and pharmacological inhibitors of VEGF signaling pathways on the pathogenesis of cerebral oedema due to acute liver failure in this model.
012 CAN ERYTHROPOIETIN TREATMENT DURING ANTIVIRAL DRUG TREATMENT FOR HEPATITIS C BE COST EFFECTIVE?
W. J. Cash, K. Patterson, M. E. Callender, N. I. McDougall.Liver Unit, Royal Victoria Hospital, Belfast, UK
Introduction: Sustained viral response (SVR) of hepatitis C to antiviral drug treatment with ribavirin and PEG interferon is dose dependent. Dose reduction is required in up to 45% of patients. Erythropoietin (Epo) treatment reduces ribavirin induced anaemia and therefore should reduce the need for dose reduction and thus increase the SVR rates.
Aims: Our aims were twofold: (1) to prevent dose reduction of ribavirin by intervening with Epo therapy when a ribavirin dose reduction would otherwise be indicated and (2) to determine the cost of such intervention and the potential cost effectiveness.
Methods: Twenty three patients with chronic hepatitis C (9 with genotype 1, 14 genotypes 2/3) commenced treatment with ribavirin and PEG-interferon (in keeping with manufacturer’s guidelines) between June 2004 to February 2005. If the haemoglobin fell below 10 g/dl or dropped by 3 g/dl below the pretreatment value with symptoms, subcutaneous Epo was commenced. The dose was increased as necessary until the haemoglobin was sustained at or above 10 g/dl. Standard NHS drug costs were used in the calculations.
Results: (1) Dosing: 13/23 patients required Epo therapy (7/9 genotype 1 and 6/14 genotypes 2 and 3), all but one within eight weeks of beginning antiviral therapy. Genotype 1 patients required higher doses of Epo, with 6/7 needing dose increases, and three needing doses in excess of 7500 iU twice weekly. For genotype 2 and 3 patients, a dose of 2000 iU twice weekly was sufficient in 4/6. Ribavirin dose was reduced due to anaemia in two (9%) patients. (2) Costs: The cost of full dose PEG-interferon and ribavirin is £11,500 for genotype 1 and £5000 for genotypes 2 and 3. The mean additional cost of Epo was £4700 for genotype 1 and £864 for genotypes 2 and 3.
Conclusions: Epo treatment sustained 91% of patients at optimal ribavirin dose. This intervention increased the drug costs by 40.9% for genotype 1 and 17.3% for genotypes 2 and 3. To achieve cost effectiveness, Epo would thus need to increase the SVR by 40.9% for genotype 1 and by 17.3% for genotypes 2 and 3. Using previous trial data this would mean increasing the SVR from 42% to 59.2% for genotype 1 and from 80% to 93.8% for genotypes 2 and 3.
013 PRIMARY SCLEROSING CHOLANGITIS: EDINBURGH LIVER TRANSPLANT EXPERIENCE 1992–2005
S. Din, A. MacGilchrist, A. Bathgate.Scottish Liver Transplant Unit, Edinburgh, UK
Introduction: Primary sclerosing cholangitis (PSC) is a chronic progressive cholestatic liver disease of unknown aetiology. It is characterised by inflammation, structuring, and fibrosis of the biliary tree. 70–80% of patients have concomitant inflammatory bowel disease, usually ulcerative colitis (UC). The medium survival is 12 years from diagnosis. Liver transplantation is performed in patients with end stage liver disease and has a reported five year survival of 85%.
Methods: Fifty five patients (37M) that underwent liver transplantation for PSC were identified. Demographic data, disease characteristics treatment interventions, and survival post-transplant were collected. Kaplan-Meier analysis, the log rank test, and multiple logistic regression was used to identify independent factors associated with disease recurrence.
Results: Sixty one liver transplants were conducted for 55 patients in the study period. The median follow up time was 4.89 years during which seven patients died. Patient and graft survival at 1, 5, and 10 years was 94%, 86%, 79% and 89%, 82%, 74% respectively. 12 patients had PSC recurrence with a median time to recurrence of 45 months. Cumulative PSC recurrence rates at 1, 5, and 10 years were 2%, 34%, and 45% respectively. Multivariate analysis identified pretransplant therapy of cyclical antibiotics (p = 0.04) and pre-OLT UC (p = 0.03) as independent predictors of recurrence. 77% of patients had concomitant inflammatory bowel disease (33UC/7CD) at time of liver transplantation. Nine patients had total colectomies prior to transplant and 10 (18%) had colectomies post transplant (three neoplastic disease). Of those that had pretransplant colectomies none developed recurrence of PSC (p = 0.14, log rank test).
Conclusion: Liver transplantation is an effective treatment for PSC with a five year survival rate of 86%. PSC recurrence developed in 21.8% of patients with a 45% cumulative risk of developing PSC at 10 years. Pretransplant therapy with cyclical antibiotics and UC are independent predictors of PSC recurrence. Pre-OLT total colectomy may protect against recurrent PSC after successful liver transplantation.
Endoscopy free papers
014 ENTONOX IS SUPERIOR TO INTRAVENOUS SEDATION: PROOF FROM RANDOMISED CONTROLLED TRIAL
S. Maslekar, M. Hughes, E. Skinn, A. Gardiner, B. Culbert, G. S. Duthie.Academic Surgical Unit, University of Hull, Cottingham, UK
Introduction: Intravenous sedation for colonoscopy is associated with respiratory complications, delayed recovery, and prolonged drowsiness. We aimed to determine whether inhaled Entonox (50% nitrous oxide: 50% oxygen) provides adequate analgesia compared to midazolam/fentanyl, and its impact on psychomotor recovery and patient satisfaction.
Methods: All patients undergoing elective colonoscopy except those with history of surgical resection were included in the study. Randomisation was stratified by endoscopist grade with adequate allocation concealment. Patients completed anxiety score (HAD questionnaire), baseline letter cancellation test and pain score on visual analogue scale. Post-procedure patients completed letter cancellation tests and marked pain assessment on visual analogue scale. Secondary endpoints were completion rates, nurse and patient satisfaction, and complication rates.
Results: 100 patients were randomised to receive Entonox (n = 50) or intravenous midazolam and fentanyl (n = 50). None of entonox patients needed conversion to intravenous medications. Entonox patients reported significantly lesser pain (mean score 26 v 40, p<0.003), with similar pre-procedure anxiety scores in both groups (HAD scale, p = 0.1). Though pre-colonoscopy letter cancellation tests were similar, Entonox group patients scored significantly better than the intravenous group (p = 0.001). The discharge time was significantly lesser (p = 0.004) for the entonox patients (mean 26 minutes) than intravenous group (mean 40 minutes). Patient satisfaction was higher in entonox group (median 98) than intravenous group (median 80; p = 0.001).
Conclusion: Entonox is more effective than midazolam with fentanyl in colonoscopy and has greater patient satisfaction, early psychomotor recovery, and facilitates early discharge. This has significant implications with introduction of screening programmes and non-medical colonoscopists.
015 A PROSPECTIVE, RANDOMISED, COMPARISON OF ADRENALINE INJECTION IN COMBINATION WITH DETACHABLE SNARE VERSUS ADRENALINE INJECTION ALONE IN THE PREVENTION OF POST-POLYPECTOMY BLEEDING IN LARGE COLONIC POLYPS
G. A. Paspatis1, K. Paraskeva2, A. Theodoropoulou1, N. Mathou2, E. Vardas1, P. Oustamanolakis1, G. Chlouverakis3, I. Karagiannis2.Departments of 1Gastroenterology, Benizelion General Hospital, Heraklion-Crete, 2Konstantopoulio-Agia Olga General Hospital, Athens; 3School of Education, University of Crete, Heraklion, Greece
Background and Aims: Our study sought to compare the efficacy of adrenaline injection in combination with detachable snare versus adrenaline injection alone in the prevention of post-polypectomy bleeding in large colonic polyps. To the best of our knowledge, this is the only prospective, randomised study in this issue.
Methods: At the time of colonoscopy patients with at least one colonic polyp ⩾2 cm, were randomised to receive treatment with either injection of 1:10.000 solution of adrenaline and the position of a detachable snare followed by conventional snare polypectomy (group A) or injection of adrenaline followed by conventional snare polypectomy (group B). 152 consecutive patients were randomly assigned to one of the above groups. 77 patients (35 males, 42 females, mean age 61 years) were assigned to group A and 75 (38 males, 37 females, mean age 64 years) to group B. Early (<12 hours) and late (>12 hours–30 days) bleeding complications were assessed.
Results: Overall bleeding complications occurred in 9/152 (5.9%) of the patients. There was one case of late bleeding in group A (1.2%), and 8 in group B (10.6%) (p = 0.03). Late bleeding was more frequent than early bleeding in group B (7 v 1). Multivariate stepwise logistic regression analysis revealed that among sex, age, polyp size, and the use of detachable snare, the latter was independently and significantly associated with the presence of a post-polypectomy bleeding episode (χ2 = 6.7, p<0.01). The use of detachable snare is more likely to result in a lower possibility of a bleeding episode.
Conclusions: Our data suggest that the use of adrenaline injection in combination with detachable may significantly decrease the number of post-polypectomy bleeding episodes in patients with large colonic polyps.
016 A COMPARISON OF MIDAZOLAM PLUS FENTANYL OR PETHIDINE AS SEDATION FOR COLONOSCOPY
B. H. Hayee, D. S. Rowbotham, V. Saxena, A. McNair.Queen Elizabeth Hospital, Woolwich, London SE18 4QH, UK
Introduction: Pethidine (meperidine) and fentanyl are commonly used in sedation for colonoscopy. Fentanyl is an analogue of pethidine, but is more potent, has fewer adverse effects and requires reversal less often. It is hypothesised that these properties would allow the use of smaller doses of midazolam, increasing safety and reducing recovery time, without a significant impact on sedation, analgesia, and patient satisfaction.
Methods: Patients were randomised to receive either midazolam with pethidine (MP) or midazolam with fentanyl (MF) in a predetermined incremental dose regime. Patients indicated their anticipated level of pain before the endoscopy and their recollection of pain afterwards using a visual analogue scale (VAS). They completed a questionnaire after the endoscopy and 24 hours later. The colonoscopist and a designated endoscopy nurse, both of whom were blinded to the sedation given, also completed a VAS for their estimation of patient discomfort.
Results: 168 patients were analysed (97 female). Patients received a mean dose of 2.62 mg midazolam with fentanyl 123.52 μg (MF; n = 83) or 4.88 mg midazolam with 53.53 mg pethidine (MP; n = 85). There were no significant differences between the two groups in terms of procedure time or completion rates. Mean recovery time was shorter with MF (12.59 v 31.65 minutes, p<0.00005). Whilst patients’ pre-endoscopy VAS scores did not differ between the two groups, post-endoscopy VAS scores were higher with MF (28.08 v 15.02, p<0.0005). Recall of consent was near total (MP 99%, MF 100%) but the MF group had greater recall of events both peri- (87% v 71%, p<0.01) and post-endoscopy (92% v 72%, p<0.001). In addition, patient recall of any pain during the procedure was higher with MF (65% v 45%, p<0.01). The number of patients requiring step-up doses was significantly higher for MF (25 v 6, p<0.001).
Conclusion: Using a combination of fentanyl and low dose midazolam significantly reduces the recovery time following colonoscopy when compared to pethidine and midazolam, but this effect is achieved at the expense of increased patient discomfort.
017 THE BSG DRAFT SAFETY AND QUALITY INDICATORS FOR COLONOSCOPY: ARE THEY ACHIEVABLE?
I. A. Murray, H. R. Dalton.Royal Cornwall Hospital, Truro, Cornwall TR1 7LJ, UK
Introduction: The British Society of Gastroenterology has produced draft standards for safety and quality measures for endoscopy. We explored whether those for colonoscopy are achievable.
Method: Our endoscopy nurses performed a prospective audit of 415 consecutive colonoscopies performed from July–September 2005 inclusive. Data collected included planned extent of examination, actual extent of examination (intention to treat: ITT), endoscopist performing (trainee and supervisor where appropriate), polyp detection rate and polyp removal and retrieval rate, and complication rate. Although not part of the BSG indicators, we also recorded time to reach caecum and withdraw the colonoscope and whether the magnetic imaging system (Scopeguide) was used.
Results: Fourteen independent colonoscopists (performing 10–105 colonoscopies individually) and five trainees colonoscoped over the study period.
A trainee commencing the procedure had no effect on completion rate (89.4% without, 90% with trainee). Time to reach caecum varied from a mean 8.6–21.2 minutes (for surgical consultants) and 13.2–20.2 minutes (for medical consultants) and was related only to the presence of a trainee on endoscopy lists. Trainees lengthened intubation time from a mean 14 to 23.6 minutes and there was a slight reduction in the number of polyps detected (31.3% procedures to 28.6%). Extubation time varied from 2.3–11.9 minutes (surgical) and 4.6–11 minutes (medical) and was significantly correlated to polyp detection rate (r = 0.64). There was a slightly lower completion rate using the Scopeguide than procedures without (89.1 v 90.8%). No perforations, significant bleeding or need for sedation reversal was recorded.
Discussion: The BSG safety and quality measures are achievable. There was difficulty defining an adenoma without histology. Our nurses recorded polyp detection rate. This resulted in a higher detection rate than the BSG standard but may have resulted in a lower polyp retrieval rate (experienced endoscopists may have left definite metaplastic polyps). Individuals maintaining their own records would be able to record histology and hence determine whether they were achieving BSG standards. Rapid withdrawal of the scope appeared to result in lower polyp detection rate and this information has been fed back to individual endoscopists within the unit.
Abstract 17
018 NON-MEDICAL COLONOSCOPISTS ARE SAFE AND EFFECTIVE: RESULTS FROM RANDOMISED CONTROLLED TRIAL
S. Maslekar, M. Hughes, E. Skinn, A. Gardiner, B. Culbert, G. S. Duthie.Academic Surgical Unit, University of Hull, Cottingham, UK
Introduction: There is an increasing demand for colonoscopy, especially with introduction of screening programmes. Though it is performed by doctors and nurses, there is an acute shortage of trained colonoscopists. Non-medical personnel were therefore trained to perform colonoscopy. The aim of this study was to prospectively compare the outcome and efficacy of non-medical colonoscopists (NMC), with both medical (MEC) and nurse colonoscopists (NC).
Methods: This study was drawn from a randomised controlled trial of sedation for colonoscopy. Randomisation was stratified by endoscopist grade: MEC or NMC or NC. Patients undergoing elective colonoscopy completed anxiety questionnaires, and baseline letter cancellation test and pain score on visual analogue scale (VAS). Post-procedure all patients marked assessment of pain and satisfaction on VAS and completed letter cancellation test. Secondary outcome variables included completion rates, nurse satisfaction and rate of complications.
Results: Out of 110 patients, 40 were randomised to MEC and NC group each and 30 patients to the NMC group. Demographic characteristics of all groups were similar. Completion rate was 95%, 97.5%, and 91% in MEC, NC, and NMC groups respectively (p = 0.3). There was no statistically significant difference between the groups in terms of median pain scores (p = 0.1), patient satisfaction (p = 0.8), nurse satisfaction (p = 0.6), and time to discharge (p = 0.08). No complications occurred.
Conclusion: This first prospective randomised controlled trial on non-medical colonoscopy has shown that NMC is safe, feasible, and therapeutic as well as diagnostic procedures can be performed with comparable completion rates and patient satisfaction. We conclude that this is a viable and effective option that complements and reduces clinician’s workload.
019 THE USE OF HUMAN THROMBIN FOR THE TREATMENT OF GASTRIC AND ECTOPIC VARICES
N. C. McAvoy, P. C. Hayes.Scottish Liver Transplant Unit, Royal Infirmary of Edinburgh, UK
Background: Gastric and ectopic varices occur in approximately 20% of all patients with portal hypertension. Although less likely to bleed than oesophageal varices, they are still associated with high morbidity and mortality. Numerous therapeutic modalities exist for the treatment of non-oesophageal ectopic varices but there is no consensus on best treatment.
Aim: The aim of this study was to evaluate the use of human thrombin in the treatment of gastric and ectopic varices.
Method: Single centre retrospective observational study. We identified 37 patients who had human thrombin from the Scottish National Blood Transfusion Service from January 1999–October 2005 to treat gastric and ectopic varices. The volume of thrombin used and the incidence of complications were recorded, as was the incidence of rebleeding.
Results: Thirty seven patients were included (28 males: 9 females). Mean age of 53.2 years (range 18–83). Underlying diagnosis ALD, 15; splenic vein thrombosis, 6; PBC, 2; cryptogenic cirrhosis, 6; CAH, 2; PVT, 2; PSC, 2; and α1 antitrypsin and hepatitis C, 1. Thrty three patients (89%) had thrombin for gastric varices, two (5.4%) for duodenal varices, one for rectal varices, and one for gastric and rectal varices. The average total volume of thrombin used per patient was 15.2 ml (range 5–47.5 ml, combined rectal and gastric varices) over 1–7 endoscopy sessions.
1. Gastric varices (33 patients), an average of 15.2 ml of thrombin was used per patient. Rebleeding occurred in four of the 33 patients (12.1%), managed in two by TIPSS (one unsuccessfully who died), and in the other two by a distal splenorenal shunt. In only two patients were the varices visually eradicated.
2. Rectal varices, an average of 18.3 ml was used per patient over three endoscopy sessions. No rebleeding occurred in this group.
3. Duodenal varices, an average of 12.5 ml was used per patient over 2–3 endoscopy sessions. Rebleeding occurred in one patient who was treated by TIPSS. No complications of thrombin use occurred in this study.
Conclusion: Human thrombin can be used to effectively control haemorrhage from gastric and ectopic varices. Despite lack of visual eradication of the varices, thrombin therapy had a low rebleeding rate, is easy to use, and appears safe. Continued thrombin injection to achieve visual eradication appears unnecessary. Randomised control trials are necessary to further assess its use.
020 SUCCESSFUL CANNULATION AT ERCP: ARE WE AS GOOD AT IT AS WE THINK WE ARE? RESULTS OF A LARGE SCALE SURVEY OF ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY
E. J. Williams.the Steering Committee. BSG Audit of ERCP, 3 St Andrews Place, London, UK
Introduction: It has been suggested that trained ERCP endoscopists should achieve a minimum selective cannulation rate of 80–90%.
Aims: To examine cannulation rates, using data from the British Society of Gastroenterology (BSG) audit of ERCP.
Methods: In 2004 information was collected prospectively on 5264 unselected ERCPs, performed in five English regions, by 182 endoscopists, working in 66 hospitals.
Results: Deep cannulation of the duct(s) of interest was achieved in 2687/3214 (83.6%) of patients undergoing their first ever ERCP and 4554/5264 (86.5%) of all procedures recorded. A total of 465/5264 procedures (8.8%) involved use of a pre-cut papillotomy. Individual endoscopists performed a mean of 29 ERCPs (range 1–145) during the study period. A cannulation rate of 80% or higher was achieved by 140/182 (77%) of endoscopists with a cannulation rate of 90% or higher observed in 77/182 (42%). Patient and procedural factors associated with failure at first ERCP are summarised in the table. In this survey cannulation at first ERCP was not associated with endoscopists’ lifetime experience, annual caseload, or performance in a university hospital.
Abstract 20
Conclusion: Cannulation rates achieved by individual endoscopists vary significantly, though defining operator and institutional factors that are predictive of competence remains difficult. Previous gastric surgery makes successful cannulation less likely, but these cases account <1% of the ERCPs undertaken.
021 PRELIMINARY RESULTS OF A RANDOMISED TRIAL OF CANNULATION TECHNIQUE IN ERCP: EFFECTS ON TECHNICAL SUCCESS AND POST ERCP PANCREATITIS
P. M. Lynch, A. A. Bailey, E. Y. T. Lee, P. R. Walsh, M. A. Murray, V. Kwan, S. J. Williams, M. J. Bourke.Endoscopy Unit, Westmead Hospital, Sydney, Australia
Aim: Inadvertent contrast injection of the pancreatic duct is believed to be an important contributor to post-ERCP pancreatitis (PEP). Our aim was to examine if primary deep biliary cannulation with a guidewire is associated with a reduced rate of PEP as compared to contrast assisted cannulation.
Methods: From August 2003 to September 2005 all patients with an intact papilla referred for ERCP were eligible for inclusion. Exclusion criteria included pancreatic or ampullary cancer. Eligible patients were randomised to undergo sphincterotome cannulation of the CBD with either contrast injection or guide wire. The trainee attempted initially for 300 s. If unsuccessful, the consultant attempted for 300 s with the same technique. Cannulation failure with the first technique was followed by an attempt with the alternate technique in the same fashion. Cannulation time was recorded. 24 hour and 30 day complication rates were assessed by phone interview and by a 24 hour serum amylase and lipase level.
Results: 297 eligible cases from 1152 ERCPs were prospectively enrolled. Ten patients were excluded. Overall technical success was achieved in 280/287 cases (98.0%). 221/287 (77.0%) patients had a successful cannulation without crossover: 118/143 (82.5%) wire and 103/144 (71.5%) contrast (p = 0.027). Of the 61 patients who failed initial cannulation, 7/19 (36.8%) from the wire group and 23/42 (58.4%) from the contrast group were successfully cannulated with the alternate technique after crossover. Pancreatitis occurred in 17/287 (5.9%): 10 wire, 7 contrast (p = 0.047). Mean number of papilla attempts was 6.52 in the patients who developed PEP compared with 4.34 in those patients that did not develop PEP (p = 0.027).
Conclusions: Cannulation success rate is significantly higher with guidewire technique compared with contrast injection but the frequency of post-ERCP pancreatitis does not differ according to cannulation technique. Repeated attempts to cannulate the papilla significantly increases the risk of developing post-ERCP pancreatitis.
022 RISK FACTORS FOR POST-ERCP COMPLICATION: RESULTS OF A LARGE SCALE PROSPECTIVE MULTICENTRE STUDY
E. J. Williams.the Steering Committee. BSG audit of ERCP, British Society of Gastroenterology, 3 St Andrews Place, London, UK
Aims: To identify risk factors for ERCP complication.
Method: Prospective multicentre study based in five English regions. Data were collected at the time of ERCP, and 30 days post procedure. Events were defined using consensus criteria.
Results: Sixty six centres participated for a mean period of 195 days. Data were collected on 5264 ERCPs. Overall 268 (5.1%) of ERCPs resulted in ⩾1 complication: pancreatitis in 79 (1.5%); cholangitis in 59 (1.1%); haemorrhage in 46 (0.9%); perforation in 22 (0.4%); and miscellaneous in 74 (1.4%). Univariate analysis identified the following significant (p<0.1) associations: (1) for overall complication: precut; cannulation attempt >1 and suspected sphincter of Oddi dysfunction (SOD); (2) for pancreatitis: pancreatic sphincterotomy; cannulation attempt >1; pancreatic duct injection >1; female sex; previous post ERCP pancreatitis; suspected SOD; younger age, and lower bilirubin levels; (3) for haemorrhage following sphincterotomy: use of pure cutting current for entire procedure; visible bleeding at time of procedure; lower platelet count and concurrent haemodialysis; (4) for perforation: suspected malignancy and use of precut. Variables significant in univariate analysis were selected for entry into a multiple regression. Significant factors from multiple regression were subjected to multilevel analysis to account for the hierarchical nature of the dataset (see table).
Abstract 22
Conclusion: Although overall complication rates compare favourably with other large studies, certain patient factors (SOD, female sex, younger age) and procedure factors (difficult cannulation, precut) increase risk.
023 SELF REPORTED EXPERIENCES OF 2059 PATIENTS UNDERGOING ERCP: RESULTS OF A MULTICENTRE SURVEY IN FIVE ENGLISH REGIONS
E. J. Williams.the Steering Committee. BSG audit of ERCP, British Society of Gastroenterology, 3 St Andrews Place, London, UK
Introduction and Methods: Professional bodies emphasise the importance of appropriate counselling of patients undergoing ERCP. However little has been published on patients’ experiences of this. In 2004 the BSG conducted a prospective multicentre survey of ERCP practice, which involved analysis of 5264 unselected ERCPs performed on 4561 patients. As part of this, patients were supplied with a (voluntary) questionnaire to complete one week post procedure.
Results: In total 2059/4561 patients (45%) completed a questionnaire following their first recorded procedure, at a mean of 11 days post ERCP (date of response unknown in 9.4%). Mean age of respondents was 64.6 years, and 128/2059 (6%) of respondents had undergone an urgent ERCP. ASA grade was <3 in 1829/2059 (89%; ASA unknown in n = 60). A total of 1602/2059 (78%) recalled being given written information though only 986/1602 (62%) of these indicated that they received this >24 hours prior to ERCP. Although 1745/2059 (85%) were informed of complications, only 740/1745 (42%) recalled receiving this information in writing. No verbal explanation of the procedure was reported by 20/2059 (1%) of patients. The majority (1935/2059; 94%) of patients knew why their doctor had recommended an ERCP and 1815/2059 (88%) had been given a chance to ask questions before the procedure. Aftercare varied with 1076/2059 (52%) patients reporting that they were warned of specific symptoms to be aware of post ERCP and 876/2059 (43%) being given an information sheet post procedure. At the time of reply 1724/2059 (84%) of patients had had the result of their ERCP explained. The majority of patients (1968/2059; 96%) were “fairly” or “very” satisfied with the explanation they had been given, with 1908/2059 (93%) reporting the ERCP to be similar or very similar to what they had been led to expect.
Conclusion: Though based on a self-selecting sample, responses suggest that most ERCP patients are satisfactorily counselled prior to ERCP. However clinicians should look to improving provision of information post procedure.
Service development free papers
024 IS THE TWO WEEK CANCER WAIT SAVING LIVES? A PROSPECTIVE FOLLOW UP OF PATIENTS DIAGNOSED WITH OESOPHAGOGASTRIC AND PANCREATIC CANCER IN 2003
G. Moran, H. Iyer, A. Bailey, J. R. Butterworth (introduced by J. Bateman).Gastroenterology Department, The Shrewsbury and Telford Hospital NHS Trust, Mytton Oak Road, Shrewsbury, Shropshire SY3 8XQ, UK
Background: The NHS Cancer Plan, published by the government in September 2000 promised that patients with suspected cancer would be seen by a specialist within 14 days. It was claimed that cancer survival would be improved by immediate access to diagnostic services. Despite scepticism about this claim, few long term data are available comparing survival outcomes of patients referred through the two week rule (TWR) or the traditional route of referral.
Aims: We examined the difference in survival between patients with oesophagogastric (OG) or pancreatic (Panc) cancer diagnosed in 2003 who were referred either via the TWR or via the traditional route.
Methods: Data were collected prospectively from all patients diagnosed with OG or Panc cancer from 1 January 1 to 31 December 2003.
Results: In 2003, we received 356 referrals via the TWR, of which 18 (5%) were diagnosed with an OG or Panc cancer, out of an overall total of 124 patients diagnosed. TWR patients were significantly younger at diagnosis (mean age 65 (SD 10.6) v 71 (SD 11.3), p = 0.04). Only 8/67 (12.5%) of oesophageal cancers (44 adenocarcinomas: 23 squamous carcinoma); 7/31 (22.5%) of gastric cancers, and 3/26 (11.5%) of pancreatic cancers were referred via the TWR (p<0.0001 for all diagnoses). Rates of surgery with curative intent were similar for oesophageal (37.5% TWR v 27%), gastric (0% TWR v 41.6% (p = 0.07)), and pancreatic cancer (33.3% TWR v 8.7%). Kaplan Meier survival analysis at a mean follow up of 311 days (range 0–856 days) indicates no difference in survival between the patient groups for each of oesophageal (adenocarcinoma/ squamous carcinoma), gastric, or pancreatic cancer (p = NS for all).
Conclusion: Only 5% of TWR referrals for suspected upper GI cancer turn out to have an OG or Panc cancer. Contrary to government expectations, survival of these patients is not improved despite faster diagnosis. Scarce NHS resources are not being optimally utilised in the fight to detect upper GI cancer earlier and improve overall survival.
025 DECLINING PREVALENCE OF CANCER IN TWO WEEK WAIT REFERRALS FOR SUSPECTED UPPER GASTROINTESTINAL MALIGNANCY
D. H. Dewar, M. Chouhan, V. B. R. Sagili, T. S. N. Wong, T. Lynch, K. M. Leong, D. Reffitt, J. O’Donohue.Department of Gastroenterology, University Hospital Lewisham, London, UK
Background: The two week wait (TWW) referral initiative for suspected upper gastrointestinal (GI) cancer was introduced in July 2000. This standard now forms the gateway to a larger framework to diagnose and initiate treatment of cancer cases within a 62 day period. We aimed to examine the current referral pattern for suspected upper GI cancers to our institution in 2004.
Methods: We identified all TWW referrals for the year 2004 and examined their medical records. This list was correlated with a database of all cases of diagnosed upper GI cancers in our institution. The results were compared with a previous study at our institution which took place in 2000–02, following the initial implementation of the two week wait. We included all diagnosed cases of upper GI malignancy.
Results: In the year 2004, 321 patients (mean age 62.7 years, 57% female) were referred using the TWW route, out of which 12 cases (3.73%) were diagnosed with upper GI cancer. This constituted 16% (12/75) of all diagnosed cases of upper GI cancer in that year. In particular 288 endoscopies (11.4% of upper GI endoscopy activity) were performed of which nine (3.1%) showed cancer, 50 (17.4%) showed gastroduodenal pathology related to H pylori and 94 (32.6%) were normal. Figures from 2001/02 show 200.5 patients referred by the TWW route per year, with cancer being diagnosed in 5.7% of referrals. This constituted a similar proportion of the total upper GI cancers in this period (15.4%). The incidence of diagnosis of upper GI cancers remains similar with 65 cancers annually in 2001/02 and 75 cases in 2004.
Conclusion: The proportion of actual cancer cases among TWW referrals appears to have fallen to 3.73%, while the referral activity has risen. The TWW route remains the preferred pathway for rapid cancer diagnosis but poses a significant workload for a small overall return, amounting to only 16% of all diagnosed cases upper GI cancer.
026 NURSE LED VERSUS GP LED MANAGEMENT OF DYSPEPSIA FOLLOWING DIRECT ACCESS GASTROSCOPY
D. Chan1, S. Harris2, P. Roderick2, D. Brown3, P. Patel4.1Southampton City PCT & PhD student Portsmouth University; 2Southampton University; 3Portsmouth University; 4Southampton General Hospital, UK
Background: Nurse Practitioners (NP) are now well established in undertaking roles traditionally carried out by doctors. However, whether NPs are as effective as doctors in managing patients is limited.
Aim: To compare the effect of systematic “nurse led” follow up to that of “GP led” follow up, after direct access gastroscopy (DAG), for dyspepsia.
Methods: We prospectively recruited dyspeptic patients undergoing DAG. Inclusion criteria were those with normal findings or grade I–II oesophagitis. They were randomised into follow up at two weeks with either the trained NP or GP. Data on demography, Short Form (SF) 12, Glasgow Dyspepsia Severity Scores (GLADYS), ulcer healing drugs (UHD) used, and follow up attendance were collected at 0 and 6 month after DAG.
Results: Of 196 patients 175 were eligible (GP = 86, NP = 89) and 15 (GP = 7, NP = 8) were lost at month 6. The table below compared changes within and between the two groups at 0 and month 6.
Abstract 26
Conclusion: This study shows that “nurse led” follow up is highly effective in improving patients’ general health and reducing dyspepsia, when compared with traditional GPs’ follow up; and there is scope for significant cost savings with reduced UHDs use.
027 PROSPECTIVE AUDIT OF COLONOSCOPY QUALITY IN KENT & MEDWAY
A. W. Harris, K. Arais, T. Rouse.Kent Cancer Network, Preston Hall, Kent, UK
Background: National standards exist for quality of diagnostic colonoscopy. IOG on colorectal cancer and BSG/JAG recommend ⩾90% caecal intubation where indicated and that >100 cases are performed per annum. It is recognised however that there is a wide variation in the quality of colonoscopy: an earlier study found caecal intubation in only 57% of cases (Bowles et al. Gut 2004;53:277). This audit is intended to provide clinical data as a benchmark to improve our service.
Methods: The audit was approved by the Kent Endoscopy Board & Colorectal Cancer DOG. A letter was sent to all colonoscopists explaining the process. Data were collected prospectively in all seven endoscopy units in Kent & Medway between February and September 2005. After first four months results were sent to each colonoscopist; where total colonoscopy was achieved in ⩽79% of cases retraining or stopping colonoscopy was recommended. After first six months coded results were presented to Kent Executive and Endoscopy Boards.
Results: Sixty colonoscopists participated in the audit: 34 (57%) achieved total colonoscopy in ⩾90% of cases; 12 (20%) achieved total colonoscopy in 80–89% of cases, and seven (12%) in ⩽79% of cases. Seven (11%) stopped performing colonoscopy during the course of this study. Only 23 of 63 (36%) colonoscopists are expected to perform >100 colonoscopies each year.
Discussion: This eight month prospective colonoscopy quality audit found that 57% of colonoscopists in Kent & Medway met the national standard for total colonoscopy. However only 36% are performing enough to meet the benchmark of >100 procedures each year. As a consequence of this audit, seven endoscopists stopped performing colonoscopy and seven who achieve total colonoscopy in ⩽79% of cases are considering either stopping colonoscopy or retraining. These data are of particular interest in view of the forthcoming NCCSP where more rigorous colonoscopy quality criteria will be applied.
Acknowledgment: we thank the Trust Chief Executives for permission to share these results and the Modernisation Agency for funding.
028 DOES SCREENING DECREASE EMERGENCY ADMISSIONS FOR COLORECTAL CANCER? A FIVE YEAR EXPERIENCE
A. Menon, S. Pedamallu, L. S. Wong.University Hospital Coventry and Warwickshire, UK
Aim: The colorectal cancer screening programme is currently in its fifth year of trial at Coventry. Wallsgrave hospital is the major centre catering to this unique population of screened patients. Our primary aim was to see if there was a progressive decrease in emergency colorectal cancer admissions over this period. Our secondary aim was to see if it had any effect on Dukes staging, workload of emergency operations, and mortality of emergency cancer admissions.
Methods: A retrospective analysis of data of colorectal cancer admissions over a period of five years from 1999 to 2004 was done. The first year represented the prescreening year 1999 (PSY) which was taken as base line. Data for the next five years SY1-SY5 were recorded for the mode of admission, emergency surgery, mortality, Dukes staging with emphasis on the last three years.
Results: In PSY 29.4% of colorectal cancers were admitted as emergency. In SY3: 57, SY4: 37, SY5: 32 patients were admitted as an emergency showing a gradual decline. There was an appreciable decline in emergency colorectal cancer operations: PSY: 57, SY1:53, SY2:50, SY3:52, SY4:34, SY5:30. This had significant impact with a steep lowering of 30 day mortality (PSY 29, SY1-5: 15, 13, 5, 2, and 4 deaths). Majority cancers were poor prognosis Dukes staging: SY3-B38%, C60%, SY4-B40%, C43%, SY5-B30%, C53%.
Conclusion: These unique data have shown that three years following the screening programme there has been a significant decline in the emergency colorectal cancer workload with an improvement in 30 day mortality. Unfortunately there has been a trend towards a worse Dukes staging. We feel the huge positive impact in such a short duration is because of increased awareness of the symptoms of colorectal cancer and change in attitude both in patients and referral patterns of general practitioners.
029 AUDIT OF COLONOSCOPY SURVEILLANCE WAITING LIST IN A DISTRICT GENERAL HOSPITAL: THE BENEFIT OF BSG GUIDELINES
G. J. Johnson, V. Edge, J. Palmer, D. A. Burke.Cumberland Infirmary, Newtown Road, Carlisle, Cumbria CA2 7HY, UK
Introduction: The British Society of Gastroenterology (BSG) published guidelines into the screening for colorectal cancer in high risk groups in 2002.1 Increasing pressures on our endoscopy services with escalating waiting times and the desire to provide a timely service prompted a review of our practice.
Aims: (1) To validate the requirement for colonoscopy against current guidelines for patients referred to the Cumberland Infirmary. (2) To improve access times for colonoscopic examinations in those patients meeting referral criteria.
Methods: The case notes and pathology reports of patients awaiting a follow up colonoscopic examination as of July 2004 were reviewed to ascertain the indications. The case for further examination was then reconsidered in light of guidance given in the current BSG Guidelines.1 If further colonoscopy was not indicated, the GP and patient were informed by letter and offered the opportunity to discuss this change.
Results: 250 sets of case notes were reviewed, 79 (31.6%) were deemed appropriate to continue with surveillance as planned in accordance with BSG guidelines. Seventy one (28.4%) did not meet criteria for repeat colonoscopy; 37 (14.8%) had their follow up period extended (their previous review interval having been inappropriately short). Four patients had died, 16 (6.4%) sets of case notes were missing, and guidance from the Regional Genetics Centre was awaited in 24 (9.6%) cases with a family history of colorectal cancer.
Conclusions: The process of evaluating the need (clinical and administrative validation) and timing of colonoscopy in patients in a surveillance programme against modern criteria is definitely worthwhile. Of our population nearly a third were deemed not to need further surveillance and a third had the surveillance period extended thus reducing demand and allowing a more timely assessment for those who will most benefit from surveillance. The cost of regular validation would be offset by the savings in demand.
1
Neoplasia free papers
030 SUPPRESSION OF COLONIC EPITHELIAL APOPTOSIS AND CRYPT HYPERPLASIA OCCURS IN BAK-NULL MICE
C. A. Duckworth, D. M. Pritchard.Division of Gastroenterology, University of Liverpool, UK
Background: Apoptosis is a tightly regulated process that plays an important role in gastrointestinal homeostasis. Anti-apoptotic members of the bcl-2 family such as bcl-2 and bcl-w have previously been shown to be important regulators of small intestinal and colonic apoptosis in vivo. Although we have previously shown that small intestinal and colonic apoptosis is slightly suppressed in bax-null mice, the importance of pro-apoptotic family members is less well understood. We hypothesise that other pro-apoptotic members of the bcl-2 family play important roles in regulating intestinal apoptosis and have therefore assessed mice in which the pro-apoptotic gene bak has been deleted.
Methods: H and E sections were prepared from formalin fixed small intestine and colon from 10–12 week old female bak-/- mice and their wild-type (C57BL/6) counterparts. Apoptosis was induced by a single 10 mg/kg intraperitoneal injection of the carcinogen azoxymethane (AOM). Cell number, apoptosis, and mitosis were assessed on a cell positional basis.
Results: The colonic crypts of bak-/- mice were significantly longer (1.6-fold) than C57BL/6 and increased colonic epithelial mitosis (twofold) was observed in bak-/- mice. Significantly fewer apoptotic cells (fivefold) were observed in the colonic table region of bak-/- mice relative to C57BL/6. However, no significant differences were observed in small intestinal crypt or villus cell number or small intestinal apoptosis or mitosis between bak-/- and C57BL/6 mice. Colonic crypt apoptosis was significantly reduced in bak-/- mice 8 hours following AOM. Whereas mitosis was suppressed in C57BL/6 colon following AOM, persistent mitosis was observed in bak-/- colon following this treatment. No differences were observed in small intestinal apoptosis or mitosis following AOM.
Conclusions: (1) Bak-/- mice demonstrate an altered colonic phenotype with reduced apoptosis in the table region, increased epithelial mitosis and crypt hyperplasia. (2) AOM induced apoptosis is suppressed in the colonic crypts of bak-/- mice. (3) Bak expression has little effect upon small intestinal homeostasis.
031 INHIBITION OF VEGFR REDUCES POLYP BURDEN IN THE APCMIN/+ MOUSE MODEL OF INTESTINAL CANCER
D. Alferez1, R. A. Goodlad1, A. J. Watkins1, R. Poulsom1, A. Ryan2, S. R. Wedge2, I. T. Pyrah2, N. Mandir1, R. W. Wilkinson2.1Cancer Research UK, Histopathology Unit, 44 Lincoln’s Inn Fields, London WC2A 3PX, UK; 2Departments of Cancer and Infection Research and Safety Assessment, AstraZeneca Pharmaceuticals, Alderley Park, Macclesfield, Cheshire SK10 4TG, UK
Introduction: AZD2171, a novel, orally active inhibitor of vascular endothelial growth factor receptor-2 (VEGFR-2) tyrosine kinase activity was used to study the effect of blocking angiogenesis in multiple intestinal neoplasia (ApcMin/+) mice. ApcMin/+ mice develop numerous polyps due to a mutation in the adenomatous polyposis coli (APC) gene, as occurs in familial adenomatous polyposis (FAP) in humans.
Methods: Two studies were performed in which 5 mg/kg/day of AZD2171 or vehicle was administered daily by oral gavage to 6 week old or to 10 week old ApcMin/+ mice for 28 days after which the number and size of polyps in the small and large intestines were scored.
Results: In the first study, AZD2171 reduced polyp number in the small bowel and colon by 46% and 62%, respectively p<0.05. Polyp diameter was also reduced by 39% in the small bowel (p<0.001) but was unchanged in the colon. Mean tumour burden (the product of number and volume) in the small intestine was thus reduced 85% (p<0.001). In the second study small bowel polyp number was not altered by AZD2171 but diameter was reduced by 24%, in turn decreasing polyp burden by 46% (p<0.059). AZD2171 had little effect on the nuclear localisation of β-catenin but reduced the number of cells expressing VEGFR-2 from 7.4 (SD 0.6) to 4.0 (SD 0.9) per villus (p<0.022).
Conclusion: AZD2171 significantly reduced the number and size of polyps, mainly in the earlier stages of polyp formation. VEGFR-2 signalling plays a key role in the development of intestinal adenomas.
032 TRANSGENIC MOUSE MODEL FOR P-CADHERIN EXPRESSION
L. A. Harrison1, E. Nye3, G. Stamp3, N. A. Wright2, R. Goodlad2, J. A. Jankowski1.1Digestive Diseases Centre, University Department of Cancer Studies and Molecular Medicine, Leicester Medical School at University Hospitals Trust, Leicester, UK; 2Histopathology Unit, Cancer Research UK, London, UK; 3Experimental Pathology Laboratory, Cancer Research UK, London, UK
Background: Epithelial (E), neuronal (N), and placental (P) cadherin isoforms belong to a highly conserved superfamily of calcium dependent cellular adhesion molecules. They are involved in the development and homeostasis of normal tissue function. p-cadherin upregulation in particular has been associated with the early stages of cancer in the gastrointestinal (GI) tract. p-cadherin has also been shown to have a proliferative effect on the GI tract.
Methods: Transgenic mouse models have provided great insights into the pathological role of specific cadherins in the intestine. Our hypothesis was to test if cadherins could have a proliferative effect in the GI tract. To study the mechanism of action of p-cadherin, an in vivo model was designed consisting of transgenic animals and a fatty acid binding promoter was used to force the expression of p-cadherin within a site of the GI tract where it is not normally expressed.
Results: Test crosses were set up between F1 and transgene positive animals to generate a homozygous mouse model stable for p-cadherin expression. A total of six animals (two animals from each genotype of wild type, heterozygous, and homozygous) were examined blindly. The pathology report determined that all organs samples were normal, with no sign of Crohn’s disease and no significant difference between the wild type, heterozygous, or homozygous animals.
Conclusion: It would appear that while p-cadherin upregulation may be necessary for a metaplastic or dysplasic phenotype in man, it may alone not be sufficient. Subtle changes of p-cadherin on mucosal biology will be discussed.
033 GASTRIN AND CCK2 PROCESSING IN NEUROENDOCRINE TUMOURS AND CELL LINES: THERAPEUTIC TARGETS
K. Khan, M. Stubbs, T. Shah, K. Savage, A. P. Dhillon, M. E. Caplin.Neuroendocrine Tumour Unit, Royal Free & University College Medical School, London, UK
Background: Neuroendocrine tumours predominantly express type 2 somatostatin receptors and this has been used for imaging and therapeutic purposes. The presence of the CCK2 (gastrin) receptor has been demonstrated in some neuroendocrine tumours (NET). Gastrin is a known growth factor for tumours including neuroendocrine tumours in particular type I and type II gastric carcinoids.
Aim: To assess CCK2/gastrin receptor expression in patients with NETs and to determine precursor progastrin (ProG) and Gly-gastrin (Gly-G) expression within these tumours. To correlate this expression with immunoblotting for CCK2 using neuroendocrine cell lines and to observe localisation of fluorochrome labelled gastrin in these cell lines.
Methods: The following patients with neuroendocrine tumours were assessed by immunohistochemistry: 24 carcinoid and 12 pancreatic neuroendocrine tumours. For histology, formalin fixed resection specimens were used. The expression of CCK2 was determined by immunohistochemistry using a specific polyclonal antibody to the CCK2 receptor. Antibodies to ProG, Gly-G, and G were also used to assess expression of gastrin forms on tumour specimens. Sections were scored by two independent observers (0 to 3: 0 = no staining, and 3 = strong staining). Rat and human carcinoid cell line lysates were used to identify specific CCK2 bands by western blotting.
Results: Of the carcinoid tumours significant expression (score>2) was observed in 22/24 (91%) for CCK2; 19/24 (88%) expressed ProG; 16/24 (66%) GLY-G; and 5/24 (22%) G. For pancreatic neuroendocrine tumours 12/12 (100%) expressed CCK2; 10/12 (83%) ProG; 6/12 (50%) Gly-G; and 4/12 (33%) expressed G. Immunoreactivity to CCK2 was detected in all neuroendocrine cell lines and fluorescent microscopy demonstrated nuclear and cytoplasmic localisation.
Conclusions: CCK2 is expressed by most neuroendocrine tumours and cell lines and the expression may be associated with the autocrine/paracrine proliferative effect. Targeting gastrin peptides at the CCK2 receptor may be worth exploring for potential therapy.
Paediatric section symposium
034 TUMOUR NECROSIS FACTOR α PROMOTER POLYMORPHISMS INFLUENCE DISEASE PHENOTYPE AND SEVERITY IN CHILDHOOD INFLAMMATORY BOWEL DISEASE
J. Van Limbergen1,2, R. K. Russell1,2, E. R. Nimmo1, H. E. Drummond1, N. Anderson3, D. C. Wilson2,4, P. M. Gillett2, P. McGrogan5, K. Hassan5, L. T. Weaver6, W. M. Bisset7, G. Mahdi7, J. Satsangi1.1Gastrointestinal Unit, Western General Hospital, University of Edinburgh; 2Department of Paediatric Gastroenterology and Nutrition, Royal Hospital for Sick Children, Edinburgh; 3Public Health Sciences, Edinburgh University; 4Department of Child Life and Health, University of Edinburgh; 5Department of Paediatric Gastroenterology, Yorkhill Hospital, Glasgow; 6Department of Child Health, University of Glasgow; 7Department of Paediatric Gastroenterology, Royal Aberdeen Children’s Hospital, Aberdeen, UK
Background and Aims: The incidence of childhood inflammatory bowel disease (IBD) in Scotland is rising and is among the highest worldwide. Tumour necrosis factor α (TNFα) is thought to play a pivotal role in the pathogenesis of IBD. The TNF gene lies within the HLA class III region of chromosome 6, a region identified as containing an IBD susceptibility gene in genome wide scans. Our aims were to assess the contribution of the promoter polymorphisms -1031T/C,-863C/A, -857 C/T, and -806 C/T with regard to disease susceptibility and phenotype in childhood IBD.
Methods: 277 patients (male/female 148/129, median age (SD) 11 (3.26) years at diagnosis) (174 Crohn’s disease (CD), 77 ulcerative colitis (UC), and 26 indeterminate colitis (IC)) and their parents were enrolled. Transmission disequilibrium testing (TDT) and case control analysis with 256 controls. Detailed genotype–phenotype analysis were performed. Haploview 3.2 was used for analysis.
Results: By case control analysis, associations were found between TNF -863A and susceptibility to UC/IC (p<0.05) and between the CACC haplotype and IC (p = 0.01, OR 2.46, CI 1.22 to 4.97). TDT analysis was negative. Analysis showed a protective effect of the CCCC haplotype with small bowel disease and ileal disease in CD patients (p = 0.0003, OR 0.24, CI 0.10 to 0.59 and p = 0.003, OR 0.31, CI 0.13 to 0.77), irrespective of NOD2 carriage. A positive association was found between colonic disease and the CACC haplotype (p<0.05) in CD. Negative associations were found between the TCCC haplotype and mild disease (BMI>50th centile and inflammatory disease (p<0.05)), whereas stricturing disease, raised CRP, albumin<35, and granuloma formation were negatively associated with the CACC haplotype (p<0.05). Multifactorial analysis confirmed the negative association of TNF-1031CC with small bowel disease (p = 0.009, OR 0.02, CI 0.00 to 0.38).
Conclusion: These variant alleles of the TNF promoter polymorphisms have a significant effect on disease location, severity, and behaviour in the Scottish early onset CD population. The negative association of TNF-1031CC with small bowel disease may underlie the haplotypic associations with milder disease phenotypes.
035 ASCA POSITIVITY INDEPENDENTLY PREDICTS ORAL CROHN’S DISEASE IN A LARGE EARLY ONSET INFLAMMATORY BOWEL DISEASE POPULATION
R. K. Russell1, B. Ip1, M. C. Aldhous1, H. E. Drummond1, I. D. R. Arnott1, M. McDougall2, D. C. Wilson3,4, P. M. Gillett3, P. McGrogan5, K. Hassan5, L. T. Weaver6, W. M. Bisset7, G. Mahdi7, J. Satsangi1.1Gastrointestinal Unit, Western General Hospital, Edinburgh; 2Public Health Sciences, Edinburgh University; 3Department of Paediatric Gastroenterology and Nutrition, Royal Hospital for Sick Children, Edinburgh; 4Department of Child Life and Health, University of Edinburgh; 5Department of Paediatric Gastroenterology, Yorkhill Hospital, Glasgow; 6Department of Child Health, University of Glasgow; 7Department of Paediatric Gastroenterology, Royal Aberdeen Children’s Hospital, Aberdeen, UK
Introduction: Anti-saccharomyces cerevisiae antibodies (ASCA) have been proposed to be useful in the diagnosis of Crohn’s disease (CD). ASCA status and its relationship with disease phenotype was determined in a cohort of Scottish early onset inflammatory bowel disease (IBD) patients.
Patients and Methods: ASCA status (IgA, IgG) was determined in 301 IBD patients (197 CD, 76 UC, 28 IC) using an ELISA kit. ASCA data from 78 healthy adult controls was also available. ASCA status was matched with phenotypic features of IBD at diagnosis.
Results: CD patients had a higher prevalence of ASCA antibodies compared to UC patients and healthy controls (41.6% v 15.8%, p = 0.0001, odds ratio (OR) 3.80 (1.93–7.50) and 41.6% v 7.7% p<0.0001, OR 8.56 (3.55–20.62) respectively). ASCA status predicted CD with sensitivity of 41.6% and specificity of 88.6%.
In CD patients univariate analysis demonstrated a positive ASCA was associated with oral (68.0% v 38.6%, p = 0.008, OR 3.39 (1.38–8.34)) and perianal (50.6% v 35.2%, p = 0.04, OR 1.89 (1.04–3.44)) disease location, raised CRP (48.9% v 24.5%, p = 0.006, OR 2.95 (1.36–6.37)), hypoalbuminaemia (51.8% v 29.0%, p = 0.01, OR 2.28 (1.19–4.37)), the need for surgery (55.1 v 36.6%, p = 0.03, OR 2.11 (1.10–4.06)), and the presence of granulomata (47.7% v 28.8%, p = 0.02, OR 2.25 (1.13–4.48)). On a multivariate binary logistic regression analysis, oral CD location was an independent predictor for a positive ASCA status (adjusted p = 0.001, OR 22.22 (3.41–142.86)).
Conclusions: ASCA prevalence is 41.6% in Scottish early onset CD patients. Phenotypic analysis demonstrated association with a number of factors most notably the presence of oral CD.
036 CHILDREN REQUIRING HOME PARENTERAL NUTRITION: HOW MUCH TIME IS REALLY SPENT AT HOME?
E. T. Ooi1,2, C. Paxton1, P. M. Gillett1, F. D. Munro2, D. C. Wilson1, (introducedby H. Gillett)3.1Department of Paediatric Gastroenterology and Nutrition, Royal Hospital for Sick Children, Edinburgh; 2Department of Paediatric Surgery, RHSC, Edinburgh, UK; 3Child Life and Health, University of Edinburgh, Edinburgh, UK
Introduction: Home parental nutrition (HPN) is central to the care of children with intestinal failure. However, HPN related complications, especially central venous catheter (CVC) related infections, still lead to substantial morbidity. We aimed to quantify the time spent in hospital rather than at home for children on HPN, and to identify the risk factors for HPN related complications and prognostic factors for prolonged stay out of hospital.
Methods: Eleven children (six boys) discharged on HPN (median age at first discharge on HPN of 15.1 months; seven with short bowel syndrome) were studied retrospectively for 7131 patient days in a regional paediatric centre during the period of 09/97 to 02/05. This centre provided all paediatric HPN to a total population of 1.25 million. Relevant data were extracted from case notes and entered onto Microsoft Excel and SPSS and statistical analysis was performed using SPSS.
Results: These children spent a mean of 31% of their time in hospital, 80% of which was due to HPN related complications (that is, not respite care, review/assessment, non-CVC related sepsis, or elective admissions). CVC related infections comprised 76% of HPN related complications, 11% were metabolic issues, and 10% mechanical issues. Children with later onset of infections and longer CVC lifespans spent less time in hospital and had better outcomes. Children who had longer total HPN durations had a lower incidence of infections. The annual incidence of HPN related complications decreased over the study time.
Conclusions: A significant proportion of the life of children on HPN is spent in hospital, not at home. Although our sample size was small, it appears that a high incidence and early occurrence of CVC related infections predict a longer time spent in hospital and a poorer prognosis. Identifying high risk patients and CVC related infection prevention may improve their prognosis and improve both their and their carers’ quality of life.
037 DIAGNOSTIC DELAY OR FAILURE IN PAEDIATRIC COELIAC DISEASE: A REGIONAL EXPERIENCE
P. M. Gillett1, C. L. Bradshaw, R. K. Russell1, J. Satsangi2, D. C. Wilson1,3.1Department of Paediatric Gastroenterology and Nutrition, Royal Hospital for Sick Children, Edinburgh; 2Gastrointestinal Unit, Western General Hospital, Edinburgh; 3Child Life and Health, University of Edinburgh, UK
Aims: To identify reasons for delay or failure to diagnose paediatric coeliac disease (CD) in children less than 16 years presenting to hospitals in Southeast Scotland during the 15 years from 1990–2005.
Methods: During a retrospective case note review, establishing the incidence of CD in SE Scotland, patients were identified where there had been significant diagnostic delay or likely diagnostic failure. Significant diagnostic delay was defined as greater than 24 months from symptom presentation to definitive diagnosis. Failure was defined as positive serology without performance of a biopsy. CD was defined according to the revised ESPGHAN criteria.
Results: 141 patients matched the criteria. Symptom onset data were identifiable in 135. From these, 18 had a delay of over 24 months. Reasons for diagnostic delay: failed biopsy not repeated within 2 years (4), IgA deficiency (3), initial reassurance despite family concern (2), positive serology without initial biopsy (3), dietary manipulation by family (1), administration problems leading to delay in biopsy (1), inconclusive histopathology (1), language problems with no suitable translation (1), lost to follow up following positive serology (1), and failure to adequately investigate iron deficiency anaemia and growth delay (1). In addition, there were six failed diagnoses (positive serology, no biopsy).
Conclusions: From our review we recommend: (a) all children must have IgA measured along with serology; (b) all children with positive serology should be biopsied; (c) all biopsies should be endoscopic to ensure adequate samples are obtained and (d) four biopsies should be taken to ensure adequate sampling; (e) biopsies should be repeated without delay if initial biopsies inadequate; (f) good communication should be ensured in all patient contact; (g) CD must be considered in investigation of growth delay and iron deficiency anaemia in children.
Small bowel and nutrition free papers
038 PLASMA CITRULLINE CONCENTRATION: A SIMPLE, SENSITIVE, AND NON-INVASIVE METHOD TO MONITOR SMALL BOWEL ABSORPTIVE FUNCTION IN PATIENTS WITH CROHN’S DISEASE
C. Papadia1, R. A. Sherwood2, T. Kalanzakis1, U. Volta3, E. Fiorini3, A. Forbes1.1Department of Gastroenterology University College Hospital, London, UK; 2Department of Biochemistry King’s College Hospital, London, UK; 3Department of Internal Medicine University of Bologna, Italy
Background and Aims: Plasma citrulline concentration (PCC) has been suggested as a marker of remnant enterocyte mass in patients with short bowel. A significant correlation between dramatically reduced PCC and histology has been shown in patients with intestinal damage, but the potentially confounding impact of intestinal inflammation has not been assessed. The aim of this study was to evaluate citrulline as a marker of intestinal functional integrity in patients with Crohn’s disease (CD) and to determine whether citrulline plasma concentrations are influenced by inflammation.
Methods: Fifty five patients were divided into eight groups according to diagnosis, small bowel length and degree of bowel inflammation: (1) CD with massive small bowel resection with ⩽50 cm remaining bowel (n = 6); (2) CD with small bowel resection with 50–150 cm remaining bowel (n = 9); (3) CD with no bowel resection but active inflammation (n = 7); (4) CD with no resection and no active inflammation (n = 6); (5) mesenteric infarction (MI) with massive small bowel resection with ⩽50 cm remaining (n = 6); (6) mesenteric infarction with small bowel resection leaving 50–150 cm; (7) active coeliac disease (n = 6); (8) healthy volunteers (n = 6). Post absorptive fasting plasma citrulline (in μmol/l) was measured using reverse phase high performance liquid chromatography (HPLC). All patients had standard laboratory markers performed and were scored according to the Crohn’s Disease Activity Index (CDAI). Five hour urine collections were carried out on each patient following sugar mix ingestion (5 g lactulose, 1 g L-rhamnose, 0.5 g D-xylose, and 0.2 g 3-O-methyl-D-glucose in 100 ml of demineralised water) after overnight fasting.
Results: Plasma citrulline concentration strongly correlated with small bowel length (p<0.0001) and carbohydrate absorption (p<0.0001). No correlation was found between plasma citrulline concentration and small bowel permeability, and there was no correlation with CRP, ESR, WBC, platelets, or albumin. Plasma citrulline was significantly higher (p<0.0004) in CD/MI patients with a remnant small bowel length of 50–150 cm (mean value 21.02 μmol/l) compared to CD/MI patients with a small bowel length ⩽50 cm (mean value 9.20 μmol/l). No significant difference (p = 0.734) was found between groups of patients with CRP<10 compared to those >10, nor between active and inactive CD patients in whom the intestinal length remained intact.
Conclusion: Citrulline plasma concentration is a simple, sensitive and reliable surrogate for small bowel absorptive capacity and is not influenced by intestinal inflammation.
039 COELIAC DISEASE: IS BIOPSY STILL REQUIRED FOR DIAGNOSIS AT ALL LEVELS OF IGA TISSUE TRANSGLUTAMINASE ANTIBODY?
P. G. Hill, G. K. T. Holmes.Departments of Chemical Pathology and Medicine, Derbyshire Royal Infirmary, Derby DE1 2QY, UK
Aim: To review raised TGA results in adults in order to assess at what level the positive predictive value (PPV) for coeliac disease is 1.00.
Methods: adult subjects (age >15 years) with TGA results >3 times the upper limit of normal (ULN), (Celikey kit, Sweden Diagnostics, Milton Keynes, UK) in the period April 2002 to December 2003 and with a small bowel biopsy (Bx) were included. For new diagnoses of coeliac disease, the result immediately prior to Bx was included; for subjects with a prior histological diagnosis of coeliac disease, the first TGA result in the review period was included. For patients with a normal Bx, the highest result was included. Two patients with normal Bx reports were excluded because of the long interval (17 and 24 months) between Bx and subsequently abnormal serology in the review period.
Results: After exclusions, there were results on 149 individual patients. All samples with values greater than 10 times the upper limit of normal were from subjects with coeliac disease (see table).
Abstract 39
Conclusions: These results show that for TGA results >10 times the ULN, the PPV for CD is 1.00 which suggests that small bowel biopsy should not continue to be mandatory for diagnosis when TGA is above this cut-off. At lower levels, as shown in the table, the PPV falls and biopsy is still required to confirm the diagnosis. Numerical values for kits differ but most kits correlate well1, 2 suggesting that a cut off of 10 times the upper limit of normal will give similar PPVs for most kits.
1
2
040 INTESTINAL DENDRITIC CELLS IN COELIAC DISEASE
A. Di Sabatino1 3, K. M. Pickard1, J. N. Gordon1, M. R. Beattie2, G. Monteleone4, T. T. MacDonald1 3.1Division of Infection, Inflammation and Repair, University of Southampton, UK; 2Pediatric Medical Unit, Southampton General Hospital, UK; 3Centre for Infectious Disease, ICMS, Barts and the London School of Medicine and Dentistry, UK; 4Dipartimento di Medicina Interna, University Tor Vergata, Rome, Italy
Background and Aims: To identify the changes in dendritic cells (DC) that may underlie the dysregulated T-cell response to gluten in coeliac disease, we examined coeliac lamina propria DC in terms of phenotype, activation/maturation and cytokine production, and investigated the in vitro effects exerted on DC by the immunodominant (p57–68) and the non-immunodominant (p31–43) gliadin epitopes, the latter of which is supposed to activate the innate immune system.
Methods: DC were identified in LPMC isolated from untreated coeliac disease patients and controls by multicolor flow cytometry as an HLA-DR+ lineage- population. Plasmacytoid (CD123) and myeloid (CD11c) receptors, together with activation (CD80/CD86) and maturation (CD83) markers were assessed by flow cytometry. IFN-γ, IL-5, IL-12p40, IL-18, IL-23p19, and TGF-β transcripts were analysed by RT-PCR in sorted DC. After 24 hour culture with p31–43 or p57–68 or TNF-α, CD83, and HLA-DR expression on DC and COX-2 levels in duodenal biopsies were respectively assessed by flow cytometry and immunoblotting.
Results: A significantly higher number of plasmacytoid DC were found in active coeliac disease than in controls. Coeliac DC expressed higher levels of maturation/activation molecules, and expressed greater IL-18 and IL-23 transcripts. CD83 and HLA-DR expression on coeliac DC were increased after incubation with TNF-α, but not p31–43 or p57–68. Organ culture experiments failed to show an increase in mucosal COX-2 after treatment with either p31–43 or p57–68.
Conclusions: In active coeliac disease, lamina propria DC are activated and express higher number of transcripts of pathologically relevant cytokines. The non-immunodominant epitope appears to have no effects on DC maturation, HLA-DR expression, and COX-2 levels in our hands.
041 CONSIDERATION OF THE BLOOD SUPPLY OF THE ILEO-CAECAL SEGMENT IN VALVE PRESERVING RIGHT HEMICOLECTOMY
E. D. P. S. Fernando, K. I. Deen.Departments of Anatomy and Surgery, Faculty of Medicine, Ragama, University of Kelaniya
Introduction: The ileo-caecal valve (ICV) is known to control the flow of chime and to prevent bacterial colonisation of the small intestine. Preservation of this segment during right hemicolectomy will prevent loss of its function. This study aimed at evaluating the arterial supply of the ileo-caecal valve to help preserve the valve during right hemicolectomy.
Methods: Fifty four fresh human cadavers (37 male, 17 female; median age 54 years, range 18–90 years) were studied after relatives gave written, informed consent. At postmortem, 20 cm of terminal ileum with the ileo-caecal segment and up to 20 cm of ascending colon were removed en block with its mesentery and blood supply. The ileo-colic artery was cannulated and injected with 10 ml of water soluble red dye under pressure. The arterial supply was dissected to demonstrate a pattern.
Results: In all, the ICV was supplied by the ileo-colic artery, a branch of the superior mesenteric, which divided into an anterior and a posterior caecal artery. A marginal branch of the right colic was noted to contribute to ICV blood supply in only two (4%). Furthermore, study of the anastomosis at the ICV showed that the anterior caecal artery was present in all (100%), posterior caecal in 48 (89%), and recurrent ileal artery present in 53 (98%). A rich anastomosis between vessels at the ICV; small “windows”, short tributaries, was seen in 38 (70%) while a poor anastomotic network at the ICV; large “windows”, long tributaries, between these vessels was seen in 12 (22%). Other variants included absent posterior caecal artery in three (6%) and absent recurrent ileal artery in one (2%).
Conclusion: The ileo-caecal valve has a predictable blood supply in the majority of patients. Preservation of the anterior caecal artery would ensure a vascularised ileo-caecal valve in right hemicolectomy.
042 PUSH ENTEROSCOPY IN THE ERA OF CAPSULE ENDOSCOPY
R. Sidhu, B. S. Horoldt, A. D. Hopper, M. E. McAlindon, K. Kapur, D. P. Hurlstone, M. C. Wheeldon, D. S. Sanders.Royal Hallamshire Hospital, Sheffield, UK
Background: With the advent of capsule endoscopy (CE) the role of push enteroscopy (PE) needs to be reassessed.
Aim: To evaluate the diagnostic yield of PE in relation to referral indication. We also compared the diagnostic yield in patients who had CE followed by PE against those who only had a PE performed.
Methods: All patients who underwent push enteroscopy from January 2002 to August 2005 were included in this retrospective audit.
Results: 143 patients underwent PE over the 44 months. Of these there were 63 cases where both PE and CE were performed. Forty per cent (57/143) were external referrals (87 females, average age 55 years). Indications for PE were iron deficiency anaemia (n = 48), overt bleeding (n = 25), suspected coeliac disease (n = 32), refractory coeliac disease (n = 17), assessment for Crohn’s disease (n = 10), and miscellaneous (n = 11). The procedure was completed in 136 patients with an average length of 70 cm of small bowel examined (range 30–130 cm). PE was unsuccessful in seven patients due to anatomical strictures or patient distress. The overall diagnostic yield was 29%. A standard endoscope could have reached 10% of the lesions. The diagnostic yield based on subgroup was 29% in iron deficiency anaemia, 64% in overt bleeders, 16% in suspected coeliac disease, 5.9% in refractory coeliac disease, 10% in Crohn’s disease, and 36% in the miscellaneous category. Overt bleeding when compared to all subgroups had a greater diagnostic yield (χ2 p<0.001). Overt bleeding was also compared to individual subgroups: iron deficiency anaemia (p<0.025), suspected coeliac disease (p<0.001), refractory coeliac disease (p<0.001), Crohn’s disease (p<0.01), and miscellaneous (p = 0.2). Comparison of the diagnostic yield in patients who had CE followed by PE against CE naïve patients was 44% versus 46% respectively (p<1). There were no cases where PE recognised a lesion that had not already been detected at CE.
Conclusion: Push enteroscopy has the greatest diagnostic yield in overt bleeders when compared to other referral indications. A negative CE would appear to exclude the need for a PE. PE should be used for therapeutic intervention following CE.
043 NITROGEN BALANCE AND UREA KINETICS IN ILEOSTOMY PATIENTS
D. H. L. Ng, S. A. Wootton, A. A. Jackson, M. A. Stroud.Institute of Human Nutrition, University of Southampton, Southampton, UK
Background: Colonic urea-nitrogen (N) salvage has been shown to play a significant role in maintaining overall N balance, especially when N availability is reduced. Colectomy patients may not be able to operate urea-N salvage and may therefore be more prone to negative N balance when protein intake is poor (for example, during illness), especially if stomal N losses are excessive. We therefore assessed N balance and urea kinetics in colectomy patients with and without small bowel resection (SBR and NSBR respectively) on habitual (HD) and low protein diets (LPD).
Methods: Six ileostomy patients with NSBR, six with SBR, and six reference subjects (Ref) were recruited. Habitual intakes using weighed food diary were measured along with urinary and stool N losses over a five day period. Urea kinetics, using 15N15N-urea, were conducted on day 5. These studies were repeated when protein intakes were reduced by 40% but total calories were similar to HD.
Results: On HD, ileostomy patients, particularly SBR, had higher N intakes and stool N losses but lower urinary N losses compared to Ref. Urea-N salvage was also higher on HD in SBR (31.9%) than in NSBR (26.7%) and Ref (28.4%). On LPD, stool N losses remained unchanged and as urea-N salvage did not increase substantially (SBR 42.2%; NSBR 30.2%; Ref 34.2%), all three groups went into negative N balance.
Conclusions: Ileostomy patients, especially those with SBR, largely compensate for high stomal N losses by eating more, but they are also capable of urea-N salvage. However, when N availability is reduced, ileostomy patients have little reserve capacity to upregulate urea-N salvage and are therefore vulnerable to marked negative N balance.
Abstract 43
044 THE SIGNIFICANCE OF LOW URINARY SODIUM EXCRETION IN ILEOSTOMY PATIENTS
D. H. L. Ng, S. A. Wootton, A. A. Jackson, M. A. Stroud.Institute of Human Nutrition, University of Southampton, Southampton, UK
Background: Chronic sodium (Na) and water depletion is well recognised in colectomy patients with ileostomies. The withdrawal of Na from intravenous nutrition has been shown to inhibit retention of nitrogen (N) and calcium (Ca) in underweight adults leading to the failure of lean tissue and bone mineral repletion.1 This study examined the relationships between urinary Na excretion and body mass index (BMI), lean body mass (LBM), urinary excretions of N, Ca, and Mg, and bone mineral density (BMD) in ileostomy patients.
Methods: Urinary excretions of Na, N, Ca, and Mg were measured along with BMI and LBM (using bioelectrical impedance analysis) in 59 ileostomy patients. Urinary Na below 100 mmol/day was considered to be low compared to chemical pathology reference values. BMD of lumbar spine (LS) and right femoral neck (FN) were also determined using DEXA in these subjects. Results are presented in median (range).
Results: Median urinary Na excretion was 73 mmol/day (5–456). Thirty seven (62.7%) had low urinary Na and 22 (37.3%) had normal urinary Na.
Conclusions: Ileostomy patients who have Na depletion are not only at risk of renal impairment from chronic dehydration but may also have compromised nitrogen and mineral status. These patients, who are often asymptomatic, are therefore at risk of subclinical malnutrition and osteoporosis.
Abstract 44
1
045 THE HYPOPHAGIA AND WEIGHT LOSS INDUCED BY TRICHINELLA SPIRALIS ENTERITIS ARE TNFα INDEPENDENT
J. Worthington, R. K. Grencis1, J. T. McLaughlin.GI Sciences and 1Faculty of Life Sciences, Manchester University, UK
Background: The molecular mechanisms linking enteric inflammation to reduced food intake are poorly understood, despite their clinical significance. We have recently demonstrated that CD4+ T-lymphocytes and IL4/13 contribute to the hypophagic response using the Trichinella spiralis nematode model of small intestinal infection (McDermott et al, Gut; in press). Food intake is at a minimum ∼9 days post infection, then normalises as the gut expels the parasites. This model is now underpinning a mechanistic study of the mediators responsible for reduced food intake during gut inflammation.
Aim: As TNFα is pivotal in many gastrointestinal inflammatory responses, we explored its functional role in the hypophagic response in this model.
Methods: Wild type C57BL/6 (WT) or TNFα receptor knockout (p55/75) adult male mice were infected by gavage with 300 T spiralis larvae. Daily food intake and body weight were monitored. The role of TNFα on worm expulsion was assessed by counting residual intestinal parasites at 20 days post infection.
Results: WT mice displayed a significant fall in food intake: at day 9 post infection, infected mice consumed 1.77 (SD 0.24) v naïve 2.94 (SD 0.04) g/mouse (p<0.05). Body weight during infection fell to 90.3 (SD 0.8)% of baseline, while rising to 108.5 (SD 1.7)% in naïve WT mice (p<0.001). However TNFα activity was absolutely not required for these effects: infected p55/75 KO mice consumed 1.75 (SD 0.15) v naïve 3.46 (SD 0.15) g/mouse (p<0.05). Body weight again fell to 87.6 (SD 1.1)% of baseline, compared to 104.0 (SD 1.5)% in naïve p55/75 KO mice (p<0.001). Functional TNFα was however functionally important in the infection, as demonstrated by the host response to clear parasites. At day 20, WT mice retained 1.5 (SD 1.0) larvae, while p55/75 KOs retained 18.1 (SD 4.5) larvae (p<0.05).
Conclusions: Although TNFα contributes strongly to the host response to expel T spiralis, this key cytokine is not functionally necessary for the profound hypophagic response and weight loss observed during small intestinal inflammation in this model.
046 THE ROLE OF SCREENING AND ANTIBIOTIC PROPHYLAXIS IN THE PREVENTION OF PERCUTANEOUS GASTROSTOMY SITE INFECTION CAUSED BY METHICILLIN RESISTANT STAPHYLOCOCCUS AUREUS
S. Thomas, S. Cantrill, D. J. Waghorn, A. S. McIntyre1.Departments of Microbiology/Infection Control and 1Gastroenterology, Wycombe Hospital, High Wycombe, Buckinghamshire HP11 2TT, UK
Background: Peristomal wound infection is a common complication of percutaneous endoscopic gastrostomy (PEG) especially in hospitals where methicillin resistant Staphylococcus aureus (MRSA) is endemic. Recent evidence suggests antibiotic prophylaxis at the time of PEG insertion may reduce infection rates. We have examined rates of PEG associated MRSA infection before and after the introduction of an MRSA screening, decontamination, and antibiotic prophylaxis protocol.
Methods: Retrospective case detection ascertained new MRSA associated PEG site infections (isolated to one month post procedure) over 33 months (January 2002 to September 2004). Prospectively from October 2004 patients requiring PEGs and found MRSA positive underwent nose (Mupirocin ointment tds) and skin (Aquasept shampoo 2% triclosan) decontamination for five days prior to PEG insertion and received prophylactic teicoplanin 400 mg IV 30 minutes before the procedure. MRSA negative patients were given co-amoxiclav prophylaxis 1.2–1.8 gm IV. Peristomal wound sites were monitored for one month post PEG insertion for inflammation, purulent discharge and infected looking sites were swabbed.
Results: Peristomal MRSA infection was identified in five of 41 (12%) PEG insertions in 2002, seven of 35 (20%) in 2003, and seven in 24 (29%) in nine months of 2004: overall infection rate of 19%. Of 25 patients undergoing new PEG insertions from October 2004 (4 known and 5 identified by the screening as MRSA positive) only one (not previously MRSA positive) developed MRSA PEG site infection but only 14 days post procedure (4%)(Chi2 p<0.05 for 2004 comparison, p>0.05 for 2002, 2003 and pooled).
Conclusion: Screening for MRSA before a PEG procedure, followed by treatment of positive patients, and appropriate antibiotic prophylaxis, can reduce PEG associated MRSA wound infections. In MRSA endemic clinical areas the risk of developing wound site infection may remain for some time post procedure unless high standard wound care is maintained.
047 WHY EVERY TRUST PRACTICING PARENTERAL NUTRITION SHOULD HAVE A NUTRITION TEAM
G. W. Moran, B. J. M. Jones.Dudley Group of Hospitals NHS Trust, Pensett Road, Dudley, West Midlands DY1 2HQ, UK
Introduction: Only 55% of UK Acute Trusts have a nutrition team for adults, varying from 68% in university and teaching hospitals to 38% in non-teaching hospitals. No long term reports of central venous catheter (CVC) sepsis rates have been reported from a district general hospital in the UK. We have already demonstrated that CVC sepsis rates in our home parenteral nutrition patients are comparable to those in large tertiary centres.
Aim: To assess CVC sepsis since the start of an adult inpatient parenteral nutrition (PN) service in a District General Hospital in 1986.
Methods: Cumulative prospectively collected annual data of CVC sepsis rates from 1985 to 2003 at a single district general hospital in all patients receiving parenteral nutrition via a central venous catheter.
Results: 859 patients received PN with a total of 15 223 patient days (mean 17.2 days). Sixty four CVC lines were infected. CVC sepsis varied from 0–16 per year with a mean of 3.36. Before 1986 the mean sepsis rate was 30.5% patients/year but after the introduction of the nutrition team and PN protocols in 1986 and later with a nutrition nurse specialist in 1997 this fell to 6.6% (range of 0–15.1%) with no septic CVC lines in 1990, 1991, and 2000. All septic events were investigated and most were attributed to breaches of PN CVC protocols.
Conclusions: CVC sepsis rates fell dramatically with the introduction of a nutrition team. The team played a pivotal role in controlling line sepsis by training ward nurses in a strict aseptic technique but it has proved difficult to hold CVC sepsis down to less than 10% every year. These results reflect the reality of controlling CVC sepsis in a DGH. They compare well with those obtained from tertiary centre nutrition teams and support the recommendations of NICE, The Royal College of Physicians, and King’s Fund that every acute trust should have a nutrition team.
Inflammatory bowel disease free papers
048 ARE ALL MESALAZINES EQUAL? A META-ANALYSIS OF PH7-DEPENDENT VERSUS CONTROLLED RELEASE MESALAZINE IN THE MAINTENANCE OF MEDICALLY INDUCED REMISSION OF INACTIVE CROHN’S DISEASE
A. H. Steinhart1, A. Forbes2, A. Bhatt3, S. P. L. Travis4.1Mount Sinai Hospital, Toronto, Canada; 2University College Hospital, London; 3Procter and Gamble Pharmaceuticals, UK, 4John Radcliffe Hospital, Oxford, UK
Background: Research indicates that the maintenance of quiescent Crohn’s disease with oral mesalazines is most frequently observed following surgical rather than medically induced remission. Studies assessing the effectiveness of mesalazine in treating patients with medically induced remission have yielded inconsistent results. It is possible that these inconsistencies arise from differences in the formulation of mesalazine administered.
Methods: A meta-analysis was undertaken to evaluate the efficacy of pH7 dependent and controlled release mesalazine in maintaining medically induced remission of Crohn’s disease. A MEDLINE literature search identified six relevant (two pH7 dependent, four controlled release) randomised controlled trials (RCTs), involving a total of 683 patients (191 pH7 v 492 controlled release). The crude rate of symptomatic relapse (CDAI >150 or an increase in baseline from 60 to 100 points) for both treatment and control groups was extracted for each RCT using the intention-to-treat method The Mantel-Haenszel approach was used to derive a pooled estimate of odds ratio (OR) and the number needed to treat (NNT) calculated.
Results: Treatment with pH7 dependent mesalazine significantly reduced the risk of symptomatic relapse (pooled OR 0.430; 95% CI 0.229 to 0.809) but not with controlled release mesalazine (pooled OR 0.888; 95% CI 0.603 to 1.307) when compared with placebo. There were also differences in treatment effectiveness by NNT, 5 and 36 for pH7 dependent and controlled-release mesalazine trials, respectively.
Conclusion: The results of this meta-analysis, although involving only a small number of studies, suggest that differences in mesalazine delivery may partially account for inconsistencies in the literature. Moreover, pH7 dependent mesalazine may offer an effective treatment for maintaining medically induced remission of Crohn’s disease.
049 TRANSFORMING GROWTH FACTOR-β SIGNALING AND MATRIX METALLOPROTEINASE PATTERN IN INTESTINAL STRICTURES IN CROHN’S DISEASE
A. Di Sabatino1 2 3, M. Buckley1, K. M. Pickard1, R. Morera3, P. Cazzola3, G. R. Corazza3, T. T. MacDonald1 2, S. L. F. Pender1.1Division of Infection, Inflammation and Repair, University of Southampton, UK; 2Centre for Infectious Disease, ICMS, Barts and the London School of Medicine and Dentistry, UK; 3First Department of Medicine, IRCCS Policlinico S Matteo, University of Pavia, Italy
Background and Aims: In addition to its crucial role in dampening tissue damaging immune responses in the gut, TGF-β has a potent profibrogenic action that it exerts by inducing fibroblast proliferation, by downregulating matrix metalloproteinase (MMP) expression, and by enhancing TIMP expression. To elucidate the mechanisms which may underlie intestinal fibrogenesis and stricture formation in Crohn’s disease (CD), we explored intracellular proteins, whose phosphorylation is involved in activating (pSmad2/3) or inhibiting (Smad7) the TGF-β signal transduction, and MMP pattern in CD.
Methods: Endoscopic biopsy specimens were collected from strictured and non-strictured mucosa of 12 fibrostenosing CD patients. Biopsies from inflamed mucosa of nine non-fibrostenosing CD patients and from 11 controls were also studied. pSmad2/3, Smad7, MMP-3, MMP-12, and TIMP-1 were determined by western blotting. TGF-β transcripts were analysed by RT-PCR.
Results: A lower Smad7 expression was found in strictured than in non-strictured mucosa in CD. As expected, Smad7 was strongly upregulated in CD inflamed mucosa. pSmad2/3 was higher in strictured than in non-strictured mucosa. Strictures expressed greater number of TGF-β transcripts than non-stricures. MMP-3 and MMP-12 were decreased in strictured in comparison to non-strictured mucosa. High expression of MMP-3 and MMP-12 was found at level of CD inflamed lesions. TIMP-1 was higher in strictured that in non-strictured areas.
Conclusions: Our findings of decreased Smad7 and increased pSmad2/3 in strictures support the profibrogenic role of TGF-β in CD. Reduced MMP-3 and MMP-12 together with increased TIMP-1 in strictured mucosa suggest that TGF-β may induce intestinal fibrogenesis by changing the balance between MMP and TIMP expression in CD.
050 ACUTE PSYCHOLOGICAL STRESS INCREASES RECTAL MUCOSAL AND LPS STIMULATED BLOOD RELEASE OF TNF-α IN PATIENTS WITH INACTIVE ULCERATIVE COLITIS
J. E. Mawdsley, D. S. Rampton.Centre for Gastroenterology, ICMS, Barts & London, Queen Mary School of Medicine & Dentistry, London, UK
Introduction: Psychological stress is reported to increase relapse in ulcerative colitis (UC) but the mechanism is unclear. We hypothesised that stress might increase colorectal mucosal and lipopolysaccharide stimulated whole blood (LPS-WB) production of TNF-α.
Aim: To assess the effects of acute stress on the concentration of TNF-α in rectal perimucosal fluid (RPMF), and on the production of TNF-α by LPS-WB in inactive UC.
Methods: For 50 minutes patients with inactive UC (Baron score<2) underwent (1) Stress (n = 25), dichotomous listening test (IQ test during contrasting music in each ear) or (2) Control (n = 10), relaxing music. Autonomic response was assessed by pulse and BP changes. RPMF was collected before and after each protocol from a 7×30 mm strip of filter paper placed sigmoidoscopically against rectal mucosa for 1 min. The filter paper was incubated in 1 ml BSA (0.3%), sodium azide (0.01%), and Tween 20 (0.002%) in PBS for 24 hours; TNF-α in the buffer was measured by ELISA. Before and after each protocol, TNF-α production by 1 ml whole blood incubated with 25 μg/ml LPS at 37°C in 95%O2/5%CO2 for 24 hours was measured by ELISA (LPS-WB).
Results: The control protocol did not change any variable. Stress increased pulse by 5bpm, systolic BP by 11mmHg, and rectal (RPMF) and LPS-WB TNF-α production by 102% and 54% respectively.
Conclusion: Acute psychological stress increases release of TNF-α by rectal mucosa and by LPS-WB. Both mechanisms could contribute to the pathogenic effects of psychological stress in UC.
Abstract 50
051 EXPRESSION OF HUMAN DEFENSIN-5 IN INFLAMMATORY BOWEL DISEASE TISSUE
D. A. Elphick, Y. R. Mahida.Institute of Infection, Immunity and Inflammation and Division of Gastroenterology, University of Nottingham, UK
Introduction: Human defensin-5 (HD-5) is a major antimicrobial peptide which is present in the lumen in its mature form but stored in normal small intestinal Paneth cells in its precursor form. Alterations in the expression of HD-5 in Paneth cells of Crohn’s small intestine or metaplastic Paneth cells of colon affected by inflammatory bowel disease (IBD) may lead to impaired mucosal innate immunity.
Methods: Surgical resection specimens of terminal ileum (6 normal, 7 Crohn’s disease) and colon (4 normal, 7 IBD) were studied. Tissue sections were used for immunohistochemistry. Paneth cell containing epithelial crypts were detached from mucosal strips with EDTA. HD-5 was purified from acid extracts of epithelial crypts using cation-exchange chromatography and C18 RP-HPLC, using anti-HD-5 antibody to identify fractions containing the alpha-defensin. Purified HD-5 was characterised by mass spectrometry and N-terminal amino acid sequencing. HD-5 isolated from normal and IBD tissue was also studied by acid-urea western blot analysis.
Results: Immunohistochemical studies showed that HD-5 was expressed predominantly in Paneth cells in normal terminal ileum and in IBD tissue, but absent in normal colon. On acid-urea western blot analysis of purified HD-5 from normal small bowel (6), Crohn’s small bowel (7) and IBD colon (7), identical immunoreactive bands were seen. Purified HD-5 from each tissue type had a similar elution profile on the C18 RP-HPLC column (39% acetonitrile). Identical N-terminal sequence (ESLQERADEAT, of precursor form) was found for HD-5 extracted from Crohn’s small intestine (2), IBD colon (2), and normal terminal ileum. Mass of HD-5 purified from normal small intestinal crypts was the same as that predicted for the precursor form (8103.83 Da).
Conclusions: In our studies to date, in Paneth cells of Crohn’s small intestine and in metaplastic Paneth cells of IBD colon, HD-5 is stored in the precursor form, identical to HD-5 stored in normal small intestine.
052 MUCOSAL E coli isolates from inflammatory bowel disease mediate IL-8 release from colon epithelial cells by shed outer membrane vesicles containing flagellin
S. Subramanian, J. M. Rhodes, C. A. Hart, B. Tam, L. G. Yu, H. M. Martin, B. J. Campbell.Division of Gastroenterology, School of Clinical Science, University of Liverpool, Liverpool L69 3BX, UK
Background and Aims: Inflammatory bowel disease (IBD) and colon cancer mucosae contain increased numbers of E coli. These cause IL-8 release from colon epithelial cells that is mediated via ERK1/2 and p38 MAPK pathways (Gut 2005;S11:A21). We have now investigated the bacterial moieties responsible for this IL-8 release.
Methods and Results: Mucosal E coli isolates, six each from UC, CD, colon cancer, and control (IBS/polyposis) patient groups were pooled (according to disease group) and assessed for their ability to release IL-8 from HT29 colon epithelial cells. Filtered (0.2 μm) supernatants caused an IL-8 response, (overall mean 659 (SD 239) pg/ml) that was approximately half that produced by whole bacteria (1393 (SD 478) pg/ml). Ultracentrifugation of supernatant from UC E coli showed that 99 (SD 5)% of the IL-8 stimulating activity sedimented with the outer membrane vesicle fraction. Centrifugal membrane filtration of the supernatant showed that 70 (SD 30)% of the IL-8 release was in response to components >30 kDa. Pretreatment of the supernatant with either elastase or an anti-flagellin antibody inhibited IL-8 release by 68 (SD 30)% (p<0.001) and 50 (SD 19)%, (p = 0.008) respectively compared to untreated supernatant. Similar results were seen using elastase treated supernatants prepared from CD, colon cancer, and control E coli. The IL-8 response to whole bacteria was TLR5 (flagellin receptor) dependent in 8/21 E coli from CD and colon cancer as judged by a median IL-8 response of 525 pg/ml (range 201–892) from TLR5-transfected HEK293 epithelial cells in comparison to 24 pg/ml (range 10–190) from gene control LacZ transfected cells. Inhibition of LPS by polymixin B, 10 mg/ml, only resulted in a 7 (SD 4)% reduction in IL-8 response to two CD E coli isolates.
Conclusion: Mucosal E coli cause IL-8 release from colon epithelial cells, largely by interaction between flagellin/TLR5. Much of this stimulatory activity is present in shed microvesicles. This process, which is only partially related to bacterial adhesion, may be at least as relevant to UC as to Crohn’s disease.
053 REMISSION AND CLINICAL RESPONSE TO OPEN LABEL ADALIMUMAB OVER ONE YEAR IN PATIENTS WITH CROHN’S DISEASE
S. B. Hanauer1, M. Lukas2, D. G. Macintosh3, P. F. Pollack4, J. Kent5, (introduced by S. Ghosh). 6.1Chicago, IL, US; 2Prague, Czech Republic; 3Halifax, NS, Canada; 4Abbott, Parsippany, NJ, US; 5Abbott, Abbott Park, IL, US; 6Imperial College, London, UK
Aim: To assess long term efficacy and safety of open label (OL) adalimumab (ADA) therapy in patients with active Crohn’s disease (CD).
Methods: Patients from CLASSIC I, a controlled four week ADA trial, were eligible to receive ADA 40 mg sc at weeks 0 and 2 in CLASSIC II. Those in remission (CDAI<150) at both weeks 0 and 4 entered a blinded, controlled cohort (results reported elsewhere). Patients with CDAI ⩾150 received OL ADA 40 mg every other week (eow) for up to one year. Escalation to 40 mg/week was permitted for flare or non-response. CDAI and adverse events (AE) were assessed each visit. Remission, CDAI reductions of 70 or 100 (Δ70 or Δ100) points (clinical response), and serious AE (SAE) were tabulated.
Results: Of 221 patients entering OL therapy, 131 completed 56 weeks: 54% with 40 mg eow and 46% with weekly dosing. By week 56, 43% of patients achieved remission, 69% a CDAI Δ70, and 61% a CDAI Δ100 response (table). AE were generally mild to moderate. In all, 54 SAE occurred in 37 patients.
Abstract 53
Conclusion: Remission was induced in 43% of patients treated, and 69% achieved clinical response within one year. Improvements were long lasting. Adalimumab was well tolerated.
054 GENE-WIDE HAPLOTYPIC ANALYSIS DEMONSTRATES NOVEL ASSOCIATION BETWEEN ATP BINDING CASSETE 3/MULTIDRUG RESISTANCE PROTEIN 3 (ABCC3/MRP3) GENE AND INFLAMMATORY BOWEL DISEASE
G. T. Ho, N. Soranzo, E. Nimmo, A. Tenesa, D. B. Goldstein, J. Satsangi.Molecular Medicine Centre, University of Edinburgh and Goldstein Laboratories, University College London, UK
Background: Increasing evidence implicates the disruption of xenobiotic defence mechanisms in the pathogenesis of inflammatory bowel disease (IBD).1, 2 We have recently demonstrated association between variations of the ABCB1/MDR1 gene and UC; microarray data now implicate a series of other genetic determinants involved in the maintenance of intestinal barrier function.
Aim: We have analysed the contribution of a panel of genes (derived from recent microarray data by Langmann et al) consisting of the Pregnane-X receptor (PXR), ABCC2, ABCC3; and MEKK1 genes using a gene-wide haplotype tagging approach.
Methods/Results: We have assessed the linkage disequilibrium pattern in these candidate genes by resequencing 24 CEPH white trios leading to the identification of 71 SNPs. A set of 22 haplotype tagging SNPs representing the common variations of these genes, both known and unknown were then selected using the multiple marker criterion of haplotype r2>0.8 for all genotyped SNPs. These SNPs were then genotyped in the Scottish cohort consisting of 388 UC, 328 CD, and 338 HC. Within the ABCC3 gene, two haplotype tagging variants demonstrated significant associations with CD (rs739921 C→G, p = 0.005, OR 1.41, 95% CI 1.11 to 1.79) and UC (rs2277624 C/T SNP, p = 0.003, OR 1.52, 95% CI 1.15 to 2.00) respectively. In contrast, no associations were demonstrated at the allelic or haplotypic level (using log-likelihood ratio tests, p = 0.9–0.1) for the other genes studied.
Conclusion: The present data provide the first evidence of the involvement of the ABCC3 gene in determining susceptibility to IBD. ABCC3 gene encodes for multidrug resistance protein 3 (MRP3) which is expressed in the gut and liver. Further fine mapping of associated interval of the implicated SNPs and replication in other datasets are in progress, together with functional and expression data.
1
2
055 ASSOCIATION OF A NONSENSE MUTATION IN THE TUCAN (CARD8) GENE WITH INFLAMMATORY BOWEL DISEASE
M. M. Mirza1, S. A. Fisher1, C. Onnie1, J. Sanderson2, A. Forbes3, J. Mansfield4, C. M. Lewis1, C. G. Mathew1.1King’s College London School of Medicine, UK; 2Guy’s and St Thomas’ Hospitals, London, UK; 3St Mark’s Hospital, Harrow, UK; 4University of Newcastle, UK
Background: The TUCAN gene (CARD8, CARDINAL) maps to a region of linkage to inflammatory bowel disease (IBD) on chromosome 19 and is a negative regulator of the transcription factor NF-κB, which has a central role in the inflammatory response. Our aim was to investigate conflicting evidence of a role for TUCAN in IBD susceptibility by sequencing the coding region of the gene in IBD patients and testing single nucleotide polymorphisms for association in a large case control sample.
Methods: The 10 exons, splice sites, promoter, 5′ and 3′ untranslated regions of TUCAN gene were sequenced in 24 IBD (12 CD, 12 UC) patients. Pairwise linkage disequilibrium coefficients (LD) between SNPs (Δ and D′) were calculated using HAPLOVIEW. Selected SNPs were genotyped in over 1000 IBD cases and 400 controls.
Results: Sequencing detected six SNPs: T-29C, T30A producing a premature stop codon at amino acid 10 (C10X), a frameshift in exon 4 (126insAA> V43fsX67) and synonymous SNPs, G933A in exon 8, G1110A in exon 10 and the rare C1227T in exon 10 (frequency 1%). The five common SNPs fell into four LD groups. The frequency of the C10X SNP was significantly increased in CD, in UC and in the combined phenotype of IBD: controls (n = 652) 29.1%, CD (n = 831) 33.2% (p = 0.017, OR 1.21), UC (n = 528) 33.2% (p = 0.033, OR 1.22), IBD (1359) 33.2% (p = 0.009, OR 1.21). However, the frameshift 126insAA was not significantly different in cases of CD (5.1%) or UC (4.9%) compared to controls (6.2%), and no other SNPs were associated with IBD. There was no significant difference in the frequency of C10X in CD cases that did or did not carry one or two mutations in CARD15.
Conclusions: These data suggest that a nonsense mutation, C10X, in the TUCAN/CARD8 gene, which would produce a highly truncated protein, may be associated with a moderately increased risk of IBD. This result requires independent replication in other patient cohorts.
056 EVIDENCE OF MONOCLONAL ORIGINS IN DYSPLASIA IN ULCERATIVE COLITIS
S. J. Leedham, L. C. Maia, O. Sieber, S. L. Preston, S. A. C. McDonald, I. P. M. Tomlinson, N. A. Wright.Cancer Research UK, 44 Lincoln’s Inn Fields, London WC2A 3PX, UK
Aim: Ulcerative colitis (UC) is a chronic inflammatory condition that increases the risk of developing colorectal cancer (CRC). UC associated colorectal cancers (UCACRC) often develop from areas of dysplasia, which can be widespread or multifocal. Loss of heterozygosity (LOH) of important tumour suppressor genes such as denomatous polyposis coli (APC), deleted in colon cancer (DCC) and SMAD4, can occur in UC associated dysplastic tissue. LOH analysis can be used as a simple and reliable marker of clonality. The aim of this study was to use LOH at the above three loci for the assessment of clonality within dysplastic and inflamed tissue in UC to test the hypothesis that dysplastic lesions arise from a single mutated clone.
Methods: Paraffin embedded tissue from colectomy specimens was obtained from St Marks Hospital pathology library. Tissue was categorised histologically into normal, acutely, or chronically inflamed or dysplastic, based on H&E slides. Laser capture microdissection was used to isolate individual crypts. If no normal crypts were available from the tissue, regions of lamina propria or muscularis mucosae were taken to allow LOH analysis comparison. DNA was extracted and amplified for microsatellite markers close to the loci of APC (5q21.1), DCC (18q21), and SMAD4 (18q21.1). PCR product was analysed with ABI 3100 sequencer and genotyper software and abnormal tissue allelic areas were compared with normal tissue allelic areas as a ratio.
Results: LOH for microsatellite markers was found in chronic inflammation in one patient at a low frequency (one marker, 50% of crypts). LOH of the same microsatellite marker was seen in low grade dysplasia at a low frequency (44%) but at a very high frequency across multiple high grade dysplastic patches in different patients (up to 100%). LOH of multiple markers was seen in some patients.
Conclusions: Lower LOH frequency in inflamed and low grade dysplasia compared to high grade dysplasia suggests which marker is lost first, and the earliest lost marker can be used a clonal marker. “Across the patch” loss of the same allele in high grade dysplasia suggests monoclonal derivation. Increased crypt fission is likely to be responsible for mutation spread.
057 OROFACIAL GRANULOMATOSIS: A TERTIARY REFERRAL CENTRE EXPERIENCE
C. Nunes1, M. Escudier2, P. J. Shirlaw2, S. J. Challacombe2, J. D. Sanderson1.1Department Gastroenterology, Guy’s & St Thomas’ Hospital; 2Oral Medicine and Pathology, Guy’s, King’s & St Thomas’ Dental Institute, UK
Background: Orofacial granulomatosis (OFG) is a rare chronic inflammatory disease of unknown aetiology sharing histological features with gut Crohn’s disease (CD). We have been running a combined Oral Medicine/Gastroenterology clinic since 1995 dedicated to patients with OFG. Previous studies addressing the clinical features and natural history of OFG are limited.
Aims: To gain insight into the overall presentation and clinical features in patients with OFG referred to a dedicated OFG tertiary referral centre.
Methods: In a retrospective study, case notes of patients with OFG attending a combined Oral Medicine/Gastroenterology clinic were reviewed. Data were extracted for age of onset, sex, clinical features, blood parameters, concurrent CD, and patch testing. A concurrent diagnosis of CD was established by standard criteria.
Results: Results were available on 73 patients of which 36 (49%) were female. Median age of disease onset was 24 years. Thirty six per cent were referred by maxillo-facial surgeons and only 15% by gastroenterologists. Fifteen (21%) had concurrent CD. Lip swelling (69%) and buccal involvement (75%) were the most common sites involved followed by gingivae and floor of the mouth. Mucosal tags (47% v 28%) and cobblestoning (40% v 19%) were more common in patients with concurrent CD as were haematinic deficiencies (53% v 29%) and raised inflammatory markers (60% v 17%). Those with OFG alone (29% v 9%) were more likely to be patch test positive.
Conclusion: OFG affects predominantly young adults with lip and buccal involvement the most common clinical presentation. Mucosal tags and cobblestoning are more likely in those with concurrent CD. Tests for cutaneous sensitivity are more often positive in OFG than CD in keeping with the view that OFG has an allergic component.
Pancreatic symposium
058 EARLY ADMISSION TO ITU/HDU OF PATIENTS WITH ACUTE PANCREATITIS IN ENGLAND, 2003–04
G. David, A. Al-Sarira, K. Cummins, D. J. Corless, M. Deakin, J. P. Slavin.Department of General Surgery, Leighton Hospital, Crewe CW1 4QJ, UK
Objectives: British Society of Gastroenterology (BSG) guidelines for management of acute pancreatitis (AP) suggest that severity stratification should be undertaken in all patients within 48 hours of diagnosis and those with predicted severe pancreatitis should be managed on a high dependency or intensive therapy unit with full monitoring and support. We analysed early admissions to ITU/HDU (within three days of presentation) in England for patients admitted with AP during the year April 2003–March 2004.
Methods: Hospital Episode Statistics data for the year 2003–04 were obtained from The Department of Health and imported into a database (Access) for analysis.
Results: There were 16 245 emergency hospital admissions with a diagnosis of AP during the year 2003–04. 1173 (7.22%) were managed on ITU/HDU during their hospital stay. Only 958 (5.90%) patients were admitted to ITU/HDU care within 72 hours of presentation.
Conclusion: Twenty five per cent of patients with AP will be predicted severe. If BSG guidelines are being followed, we would have expected to see a much higher proportion of patients admitted to ITU/HDU within the first 72 hours. This clearly has huge implications for ITU/HDU provision. We would recommend that further work is undertaken to develop the guidelines, looking at levels of monitoring required and where this is best initiated, minimal levels of supportive care, and routine use of scoring systems that would allow the prioritisation of patients with organ dysfunction to a higher level of care.
059 SOCIOECONOMIC STATUS CORRELATES WITH OUTCOME IN PANCREATIC CANCER
J. J. S. Brown, B. Ashton, R. M. Charnley, D. Forman1, B. C. Jaques.Hepato-Pancreato-Biliary Unit, Freeman Hospital, Newcastle upon Tyne and 1Northern and Yorkshire Cancer Registry, Leeds, UK
Aim: To investigate the impact of deprivation on outcome in patients with pancreatic cancer, data were collected from the NYCRIS (Northern and Yorkshire Cancer Registry) database for new patients registered from January 1998 to December 2002.
Methods: The IMD2000 score (a validated socioeconomic deprivation tool) was attributed to each patient. Five quintile groups of similar size were generated with graded deprivation profiles, higher scores representing greater deprivation. The difference between the rank of socioeconomic deprivation and average survival in days was also calculated for the cohort of patients who underwent surgery and those who had no surgical intervention.
Results: From a total of 3976 patients the five quintiles had between 739 and 804 patients, the difference of the mean deprivation score between all groups being significant, p<0.0001, using Student’s t test (see table). The mean survival in days, for all treatment modalities between Q1 and Q5, was significantly different, p = 0.0003.
The mean deprivation scores for those undergoing surgery (n = 229) and those not undergoing surgery (n = 3640) were 28.31 and 31.64 respectively, p = 0.002. The mean survival of the surgical cohort in the most deprived quintile (n = 33) was 329 days (95% CI 198 to 460) and the least deprived (n = 53), 424 days (95% CI 320 to 527), p = 0.26.
Conclusion: Although the cohorts represent a varied casemix, socioeconomic deprivation appears to have a major effect on survival in patients with pancreatic cancer and also correlates with treatment by surgical intervention. Further work is required to determine the underlying cause of this effect.
IBD/Pathology sections joint symposium
060 DETECTION OF MURAMYL DIPEPTIDE SENSING PATHWAY DEFECTS IN PATIENTS WITH CROHN’S DISEASE
D. A. van Heel1, K. A. Hunt1, S. Ghosh1, K. King2, S. Gabe3, C. G. Mathew2, A. Forbes3, R. J. Playford1.1Imperial College London; 2King’s College London School of Medicine; 3St Mark’s Hospital, UK
Background and Aims: Crohn’s disease is strongly associated with double mutations in NOD2/CARD15. Three common mutations (Arg702Trp, Gly908Arg, Leu1007fs) impair innate immune responses to bacterial muramyl dipeptide. Rare NOD2 variants occur, but it is difficult to both identify them and assess their functional effect. We assessed the true frequency of defective muramyl dipeptide sensing in Crohn’s disease and developed a rapid diagnostic assay.
Methods: An ex vivo assay was established and validated based on muramyl dipeptide stimulation of peripheral blood mononuclear cell cytokine production. Muramyl dipeptide induced enhancement of IL-8 secretion, and synergistic increase in lipopolysaccharide induced IL-1β secretion were studied. Assay results were compared with NOD2 genotype status (three common mutations and rare variants) in 91 individuals including a prospective cohort of 49 Crohn’s disease patients.
Results: The assay was highly sensitive and specific for detection of profound defects in muramyl dipeptide sensing caused by double NOD2 mutations (IL-8 p = 0.0002; IL-1β p = 0.0002). Disease state, active inflammation or concurrent use of immunosuppressive medication did not influence results. Healthy NOD2 heterozygotes had modest impairment of muramyl dipeptide induced IL-8 secretion (p = 0.003). Only one of seven Crohn’s disease patients with both a common mutation and a second amino acid-changing rare variant had a profound muramyl dipeptide sensing defect.
Conclusions: Profound defects in muramyl dipeptide sensing were found in 10% of Crohn’s disease patients. Inherited mutations in NOD2 (and not any other genes) accounted for all defects. The ex vivo assay has multiple potential applications as a clinical diagnostic tool to distinguish patients with muramyl dipeptide sensing defects, and for research investigation.
061 IGG PLASMA CELLS IN INFLAMMATORY BOWEL DISEASE EXPRESS LARGE QUANTITIES OF STROMELYSIN (MMP-3)
J. N. Gordon1, K. M. Pickard1, P. M. Goggin2, T. T. MacDonald1.1Division of Infection, Inflammation and Repair, University of Southampton School of Medicine, UK; 2Department of Gastroenterology, Queen Alexandra Hospital, Portsmouth, UK
Introduction: In both ulcerative colitis and Crohn’s disease there is a marked increase in IgG plasma cells in the lamina propria which may be of primary pathogenic significance. In addition, gut plasma cells can secrete functionally active immune mediators capable of driving inflammation in the gut. Using a novel method for isolating gut plasma cells we have previously shown that long lived IgG plasma cells persist in inflammatory bowel disease (IBD) and may contribute to tissue injury. In this study we have investigated the production of MMP-3 by gut plasma cells from normal subjects and patients with IBD.
Methods: Biopsy and resection tissue specimens were obtained from patients with active IBD and from normal controls. Lamina propria mononuclear cells were isolated and immunomagnetic selection used to positively select plasma cell populations. MMP-3 expression was investigated using western blotting, and Taqman PCR. The types of plasma cell making MMP3 were studied by confocal microscopy.
Results: Plasma cells from patients with CD and UC expressed significantly higher levels of MMP-3 protein and transcripts (100 000 fold increase) than controls (p<0.001). Levels of TIMP-1 were not significantly different from controls. In patients with IBD, 92% of IgG+ve plasma cells expressed MMP-3 compared with 20% of IgA+ve cells. In contrast very few plasma cells from controls expressed any MMP-3.
Conclusion: We have demonstrated that plasma cells from subjects with IBD express large amounts of MMP-3. Furthermore the primary source of MMP-3 is IgG+ve plasma cells. These results identify a new pathway by which IgG plasma cells can damage the gut.
Endoscopy free papers
062 POSITION CHANGE IMPROVES LUMINAL DISTENSION DURING COLONOSCOPE WITHDRAWAL: A RANDOMISED, CROSSOVER, BLINDED TRIAL
J. E. East, N. Suzuki, N. Arebi, D. Swain, N. Palmer, P. Bassett, B. P. Saunders.Wolfson Unit for Endoscopy, St Mark’s Hospital, London, UK
Background: Adenoma miss rates may be as high as 27% for lesions <5 mm and 12% if ⩾10 mm. Part of this miss rate may be due to lesions hidden in colon that is inadequately distended to allow complete visualisation of the mucosal surface. Changing the patient’s position during colonoscopy may alter colonic configuration and gas distribution to improve luminal distension, compared to performing the entire withdrawal sequence in the left lateral position.
Method: During the withdrawal phase, 14 patients were randomised to one of two sequences first: either examination entirely in the left lateral (LL) position or with position changes (PC). Position change involved examination of caecum (C), ascending colon (AC), and hepatic flexure (HF) in left lateral; transverse colon (TC) supine; and splenic flexure (SF) and descending colon (DC) in right lateral. At the sigmoid descending junction, the colonoscope was reintroduced to the caecum and the patient was re-examined with the other sequence. Luminal distension was scored on a scale 1–5: 1, total collapse; 5, widely patent to limit of vision, by the endoscopist (e) and by a blinded video reviewer (v). All patients received hyoscine butylbromide 20 mg IV.
Results: Scores for each colonic area are expressed as means (table). Scores were significantly different for TC, SF, and DC, paired t test.
Abstract 59
Conclusion: Position change during the withdrawal phase of colonoscopy improves luminal distension in the transverse colon, splenic flexure, and descending colon compared to examination in the left lateral position, and has the potential to reduce adenoma miss rates.
063 INTRASTRICTURE INJECTION OF STEROID FOR CROHN’S ANASTOMOTIC STRICTURES POST ENDOSCOPIC BALLOON DILATATION: RESULTS OF A RANDOMISED, DOUBLE BLIND, PLACEBO CONTROLLED TRIAL
J. E. East, N. Patterson, J. C. Brooker, M. D. Rutter, C. Thapar, D. Swain, P. Bassett, D. S. Rampton1, B. P. Saunders.Wolfson Unit, St Mark’s Hospital; 1Royal London Hospital, London, UK
Background: Colonoscopic balloon dilatation of ileo-colonic anastomotic strictures has been a successful treatment since the 1970s; however repeated dilatations are often needed and some patients still require surgery. Retrospective case series (Endoscopy 2003;35:333–7) have suggested that injection of steroid at colonoscopy after stricture dilatation may reduce the incidence of stricture recurrence.
Aims and Methods: Randomised, double blind, placebo controlled, trial to assess the effect of post balloon dilatation quadrantic intrastricture injection of steroid (Triamcinolone 40 mg, total) or placebo (saline). All strictures were <5 cm in length. Primary end point: time to redilatation or surgery. Patients were followed for 52 weeks.
Results: Groups were well matched, n = 13 (table, median values). Five of seven patients in the steroid group required redilatation and two of these five subsequently required surgery. One of six patients in the placebo group required redilatation, none required surgery. There was a trend to earlier dilatation failure in the steroid group p = 0.06, log rank test; hazard ratio (steroid to placebo) 6.1 (95% CI 0.7 to 53.0), Cox regression.
Abstract 62
Conclusion: In this small trial, intrastricture steroid injection post balloon dilatation of Crohn’s disease related ileocolonic anastomotic strictures does not extend time to redilatation and may shorten it. Steroid injection after stricture dilatation should be reconsidered.
064 INTRAEPITHELIAL NEOPLASIA AND COLON CANCER DETECTION IS SIGNIFICANTLY IMPROVED AND CHARACTERISED USING HIGH MAGNIFICATION CHROMOSCOPIC COLONOSCOPY: DO BSG GUIDELINES NOW REQUIRE MODIFICATION?
D. P. Hurlstone1, D. S. Sanders1, M. E. McAlindon1, A. J. Lobo1, M. Thomson1, S. Brown1, S. S. Cross2.1Gastroenterology, Royal Hallamshire Hospital, Sheffield; 2Academic Department of Pathology, Royal Hallamshire Hospital, Sheffield, UK
Background: Data suggest that pan-chromoscopy using methylene blue may improve the detection of intraepithelial neoplastic (IN) lesions in UC surveillance. Interval cancers are known to occur.
Aims: We hypothesised that targeted chromoscopy alone with high magnification imaging may increase the total number of intraepithelial neoplastic lesions detected as compared to conventional colonoscopy and biopsy protocols.
Methods: 350 patients with longstanding UC (⩾8 years) underwent surveillance colonoscopy using high magnification imaging. Quadrantic biopsies at 10 cm intervals were taken on extubation in addition to targeted biopsies of abnormal mucosal areas. Defined lesions were further evaluated using modified Kudo crypt pattern analysis and Paris guidelines. Data were compared to disease and extent matched controls who had undergone conventional colonoscopic surveillance between January 2001–April 2005.
Results: Significantly more IN lesions were detected in the magnification chromoscopy group as compared to controls (69 v 24; p<0.0001). IN was observed in 67 lesions of which 53 (79%) were detected using magnification chromoscopy alone. Chromoscopy increased the number of flat lesions detected with IN as compared to controls (p<0.001). Twenty IN lesion were detected from 12 950 biopsies using conventional colonoscopy (0.15%) with 49/622 (8%) in the HMCC targeted group. From 12 482 biopsies taken in the control group, 18 (0.14%) yielded IN. However, from the targeted biopsy group without HMCC imaging, the yield was modestly improved at 1.6% (6/369). Total procedure time was significantly longer in the magnification chromoscopic group as compared to controls (p<0.02).
Conclusions: Magnification chromoscopy significantly improves the detection of IN in this group. These techniques have important clinical implications and may change current practice guidelines.
065 AUTOFLUORESCENCE IMAGING AND NARROW BAND IMAGING WITH MAGNIFICATION IN COLONOSCOPY: AN EARLY EXPERIENCE
J. E. East, N. Suzuki, N. Palmer, C. Thapar, D. Swain, B. P. Saunders.Wolfson Unit for Endoscopy, St Mark’s Hospital, London, UK
Background: Narrow band imaging (NBI) uses optical filters to improve contrast for superficial mucosal vessels to highlight vascular neoplastic lesions as well as the mucosal (pit) pattern. Autofluorescence imaging (AFI) relies on neoplastic lesions blocking endogenous tissue autofluorescence to provide colour contrast (magenta on green) against the background mucosa.
Method: We report our experience with a third-generation prototype AFI/NBI system with high definition and ×100 magnification in the colon in the first 92 cases (XCF-H240FZL/I video colonoscope, XCLV-260HP xenon light source and XCV-260HP video system centre, Olympus Medical System Corp, Tokyo, Japan). We compared the adenoma detection rate in those without a polyposis syndrome or colitis with that of the preceding 92 cases performed with standard colonoscopy (Olympus CF240/260 series)
Results: Mean adenoma detection rate was 0.85 v 0.35/patient, with 47% v 26% having at least one adenoma (range 0–6 v 0–4) for NBI/AFI system v standard colonoscopy, p<0.005 for patients with at least one adenoma, χ2 test. Both NBI and AFI were effective in highlighting adenomas down to 2 mm in size, but image resolution was poorer with AFI which failed to detect some adenomas. NBI and magnification gives a similar appearance to contrast chromoendoscopy but in negative—that is, the pits and grooves look pale and ridges dark; we have been able to detect adenomas <1 mm and determine their Kudo pit pattern. Chromoendoscopy seems to provide a slightly clearer pit pattern and contrast for very small lesions.
Conclusion: The increased adenoma detection rate with this tri-modal system should be interpreted with caution, but is promising. NBI provides many of the advantages of chromoendoscopy without requirements of extra time and equipment, and problems with incomplete mucosal coverage. AFI is not yet consistent enough to replace standard endoscopy but may be a valuable adjunct to NBI in endoscopic assessment of polyps for neoplasia in equivocal cases.
066 COLONIC POLYP TO CANCER: AN ANIMATED STORY
G. J. M. Webster1, R. Doshi2, A. R. Ward3.1Department of Gastroenterology, University College Hospital, UCLH NHS Foundation Trust; 2AS&K Skylight and 3Remedica, 1 New Oxford Street, London, UK
Background: Embarrassment and ignorance about colonic disease is widespread, yet this needs to be overcome if the national colorectal cancer screening programme is to be a success. Many potential patients do not understand the concept of the “polyp-to-cancer sequence”, and this may affect the uptake of screening. Medical textbooks/web information only demonstrate static “snapshots” of the progression from benign polyp to invasive tumour, yet the process is, of course, a dynamic one. Employing state-of-the-art 3D animation and information graphics we have created a dynamic “life-like’ visual representation of the process of polyp and tumour development, based on current concepts of tumour pathophysiology.
Description of animation: The animation lasts approx 50 seconds and begins in the colon, as if during routine colonoscopy. On advancing proximally, a small sessile polyp is identified. Over several years (spread over 14 seconds of animation), this polyp is seen to grow, become pedunculated and lose blood (this process, and the possibility of faecal occult blood detection, is described in the voice over). Over further years it enlarges and undergoes malignant change (the voice over stresses that only a small proportion of polyps become malignant). Information graphics are used to help convey some of the genetic changes that must occur for the polyp ultimately to become cancerous. The animation then follows the spread of the tumour as it moves through the bowel wall, demonstrating the Duke’s stages of tumour invasion, and including haematogenous tumour spread to the liver. We end by showing a snare polypectomy which completely removes the polyp during its premalignant stage.
Conclusion: We hope that this novel way of describing the dynamic nature of disease pathophysiology may be of use to both patients and doctors, and be applicable to other areas of gastroenterology teaching and practice.
Oesophageal free papers
067 SHORTENING OF THE ABDOMINAL COMPONENT OF THE LOWER OESOPHAGEAL SPHINCTER FOLLOWING A MEAL
J. J. Manning, A. Wirz, K. E. L. McColl.University Department of Medicine, Western Infirmary, Glasgow, UK
Introduction: There is a high prevalence of intestinal metaplasia and inflammation of the gastric cardia in H pylori negative healthy subjects. This may represent relaxation of the distal (abdominal) portion of the lower oesophageal sphincter (LOS) and consequently, gastric juice damaging the most distal oesophageal squamous mucosa. The LOS is under most strain following a large meal.
Aim: To study the effect of a large meal on the LOS of healthy volunteers.
Method: Fifteen healthy volunteers, all H pylori negative by breath test, fasted on three separate occasions. Baseline slow motorised pull-through (SMPT) manometry was then performed, during quiet respiration, with a standard manometry system. The SMPT was repeated 5 minutes following a battered fish and chip meal. Pooled data were analysed (n = 45), each subject acting as their own control. Distances quoted are means and measured from the nares.
Results: Following the meal the total length of the LOS reduced from 4.9 cm to 3.5 cm (p<0.0001). The upper border position did not change. The respiratory inversion point (RIP) elevated from 44.8 cm to 44.2 cm (p<0.0001). The lower border of the LOS elevated from 47.6 cm to 46.0 cm (p<0.0001). The thoracic portion of the LOS reduced from 2.1 cm to 1.7 cm (p<0.0001). The abdominal portion of the LOS reduced from 2.9 cm to 1.8 cm (p<0.0001). The maximum end expiratory pressure reduced from 24.5 mmHg to 21.2 mmHg (p<0.04).
Conclusion: This study demonstrates shortening of the LOS after a meal due to shortening of the abdominal sphincter. There is also slight shortening of the thoracic sphincter. There is movement of the RIP proximally, probably due to a mild elevation of the diaphragm caused by gastric distension.
Discussion: Shortening of the abdominal segment of the LOS following a large meal is likely to predispose to gastric acid reaching and damaging the squamocolumnar junction. This may explain the high prevalence of carditis and intestinal metaplasia at the squamocolumnar junction.
068 THE CLINICAL IMPACT OF PROLONGED (48 AND 96 HOUR) OESOPHAGEAL PH MONITORING BY THE BRAVO SYSTEM
A. Thakur, M. Fox, R. Anggiansah, A. Anggiansah, T. Wong.Departments of Gastroenterology & Oesophageal Laboratory, St Thomas’ Hospital, London, UK
Introduction and Aims: The catheter-free Bravo system is designed to record intra-oesophageal pH over 48 hours; however the capsule remains in place for an average 5–6 days. This provides an opportunity to examine day-to-day variability in pH recordings over an extended period, and the impact of prolonged recording on the diagnostic yield of gastro-oesophageal reflux disease (GORD).
Methods: Fifty six consecutive patients (48 (35–61) years) with reflux symptoms referred for pH monitoring were studied. 43 patients were monitored for two days and 13 patients over four days (returning after 48 hours to download pH data). The day-to-day variability of pH measurements was assessed. Patients were classified with normal or abnormal (>4.2%/24 hours pH<4) acid exposure during each test period. The potential increase in diagnostic yield of GORD by prolonging pH recording from 24–48 and 96 hours was assessed. Kappa (κ) values were calculated.
Results: Two-day recordings were available for 47/56 patients (incomplete (n = 8), early detachment (n = 1)). Four-day pH studies were available for 12/13 patients (day 3 detachment (n = 1)). There was no difference in mean acid exposure day 1–4 (8.2%, 7.8%, 7.9%, 7.3% respectively, p = 0.61); however within patient day-to-day variability was high, ±30% relative to the mean. Pathological acid exposure was present in 29/46 day 1 and 27/46 day 2 (12 patients changed diagnostic classification). Cumulative diagnostic yield increased from 29/46 (48%) day 1 to 34/46 (74%) day 2. Diagnostic reproducibility of 24 hour pH recording was fair (κ = 0.45). Within patient variability between 48 hour test periods was lower than that for 24 hour test periods ±16% v ±30% relative to the mean (p<0.01). Only 1/12 patients changed diagnostic classification from the first to the second 48 hour test period. Diagnostic reproducibility of 48 hour pH recording was very good (κ = 0.76).
Conclusions: Increasing the duration of pH studies from 24 to 48 hours significantly improved the reliability of clinical measurement and raised the diagnostic yield of GORD by 25%. 96 hour pH studies provided little further improvement. 48 hour pH monitoring provides important advantages in the investigation of reflux symptoms in clinical practice.
069 OESOPHAGITIS IS ASSOCIATED WITH ENLARGED UNBUFFERED POSTPRANDIAL ACID POCKET
A. T. Clarke, A. A. Wirz, J. Manning, S. Ballantyne, D. Alcorn, K. E. L. McColl.Western Infirmary, Glasgow G11 6NT, UK
Background: Previous work has demonstrated the presence of an unbuffered pocket of highly acidic juice at the gastric cardia after a meal in healthy volunteers.
Aims: To compare the postprandial acid pocket in healthy volunteers and patients with severe reflux and to define its position relative to the squamocolumnar junction and manometric landmarks.
Methods: Twelve healthy volunteers and 16 patients with grade III/IV reflux oesophagitis or Barrett’s oesophagus were studied. At endoscopy radiopaque clips were placed at the proximal gatric folds and at the diaphragmatic pinch and barium meal documented the anatomy. While fasted, a pull-through study was performed using a combined dual pH and solid state manometry catheter, withdrawing at consecutive 1 cm intervals every minute. The position of the pH/manometry apparatus relative to the anatomical landmarks was obtained by identifying the radiopaque clips fluoroscopically. The patients were then fed a standardised fatty meal and 15 minutes after the meal, the pull-through study and x rays repeated.
Results: A hiatus hernia was identified endoscopically in 13 of the reflux oesophagitis patients and its median length was not significantly altered by the meal (fasting = 1.5 cm, range 0.8 cm to 4.0 cm v postprandial = 2.2 cm, range 0.5 cm to 4.6 cm). There was a significantly longer unbuffered acidic region (pH<2) distal to the proximal margin of the gastric folds in the oesophagitis patients versus healthy volunteers (median length 2 cm, range 0 cm to 15 cm v 0 cm, range 0 cm to 4 cm; p = 0.0004). Its location in the oesophagitis patients corresponded with the hiatus hernia sac, the midpoint of which remained highly acidic (median pH 1.49, range 0.78 to 7.54) after the meal.
Conclusion: Oesophagitis is associated with an enlarged unbuffered postprandial acid pocket. This may be due to the hiatus hernia providing a reservoir of highly acidic gastric juice isolated from food in the main stomach which may reflux into the oesophagus.
070 ARE OESOPHAGEAL PERISTALTIC OR LOWER OESOPHAGEAL SPHINCTER FUNCTIONS GENETICALLY DETERMINED IN GORD? A DISCORDANT CO-TWIN CASE CONTROL STUDY
I. Mohammed, A. Anggiansah1, R. Anggiansah1, L. F. Cherkas2, T. D. Spector2, N. J. Trudgill.Department of Gastroenterology, Sandwell General Hospital, 1Oesophageal Laboratory, and 2Twin Research & Genetic Epidemiology Unit, St Thomas’ Hospital, London, UK
Background: Differences in basal lower oesophageal sphincter (LOS) pressure, LOS length and peristaltic function have been described in patients with GORD. However, it is not clear whether these differences contribute to the development of GORD or are caused by GORD. We have examined peristaltic and LOS function in twin pairs who are discordant for GORD symptoms—that is, where only one of the pair has GORD symptoms.
Method: Four monozygotic (MZ) and 12 dizygotic (DZ) discordant twin pairs were studied. Manometry assessed basal end-expiratory LOS pressure, total and intra-abdominal LOS length by station pull through and peristaltic function by ten 5 ml water swallows. Ineffective oesophageal motility was defined as at least 30% of contractions less than 30 mmHg or non-transmitted.
Results: MZ twins mean age 63 (range 53–75 years), DZ twins mean age 57 (44–74 years). Univariate analysis revealed no significant differences between twins with GORD symptoms and twins without GORD symptoms for LOS pressure (mean 8.2 mmHg (SD 5.7) v 9.9 (7.1); p = 0.4), proximal oesophageal peristaltic amplitude (45 (17.8) v 56 (23.6) mmHg p = 0.17), mid oesophageal amplitude (72 (35) v 75 (34) p = 0.80), distal oesophageal amplitude (80 (41) v 79 (38) p = 0.88), total LOS length (3.75 cm (SD 0.75) v 3.65 (0.62) p = 0.56), intra abdominal LOS length (1.74 (0.61) v 1.80 (0.58) p = 0.70), and ineffective oesophageal motility (19% v 13% p = 0.48).
Conclusion: There was no difference in LOS pressure, LOS length, or peristaltic function between twins with GORD symptoms and their asymptomatic co-twins. This suggests that abnormalities of LOS and peristaltic function are genetically determined and not a consequence of GORD.
071 TIME TRENDS IN THE PREVALENCE AND INCIDENCE OF DYSPLASIA IN BARRETT’S OESOPHAGUS OVER TWO DECADES
S. A. Sonwalkar1, O. Rotimi2, S. M. Everett1.1Centre for Digestive diseases, The Infirmary at Leeds, Leeds, UK; 2The Department of Histopathology, The Infirmary at Leeds, Leeds, UK
Introduction: Barrett’s oesophagus (BO) and oesophageal adenocarcinoma (OA) is increasing over time in the last 2–3 decades. The prevalence of BO in GORD is between 2–11% and in OGDs are 7.9–8.9/1000.
Population prevalence is 22.6/100 000 (377/100 000 autopsies). Incidence of BO increased from 0.37 in 1961–69 to 10.5 in 1995–97. Community incidence increased from19.8 in 1997 to 40.5 in 2002 per 1000 OGDs. OA is known to follow the metaplasia-dysplasia-neoplasia sequence but little is known about trends in the incidence and prevalence of dysplasia in BE.
Aims and Method: In this longitudinal, dynamic cohort study (study period 1 October 1984 to 31 December 2004), the aim was to establish the changing trends in the incidence and prevalence of dysplasia in patients with BO attending the General Infirmary at Leeds for endoscopy over the last two decades. Barrett’s oesophagus was defined as specialised intestinal metaplasia (SIM) on histology and dysplasia diagnosis was based on Riddell’s and Vienna criteria.
Histology, endoscopy, and case notes were reviewed. Dysplasia on index endoscopy or within six months was defined as prevalent and any subsequent dysplasia as incident. For prevalent dysplasia the denominator was the number of endoscopies performed and for incidence calculations the denominator was the number of cases of BO and number of OGDs in a year. Prevalent cases were excluded from subsequent incidence measurements and tertiary referrals were excluded.
Results: 5812 episodes of SIM were diagnosed in 2500 patients with BO. 1217 (48.%) entered surveillance with a total follow up of 4434 years. 376 episodes of dysplasia were detected in 213 (8.52%) patients, who had 4084 OGDs and 1010 biopsies performed. Dysplasia was prevalent in 122 (62%) and incident in 75 (38%). 14 (7%) patients had indefinite, 60 (30%) low grade, 80 (41%) high grade dysplasia, and 43 (22%) had adenocarcinoma. There was no significant difference in mean age, sex ratio, mean weight, smoking, PPI/H2 therapy, or symptoms of GORD among the prevalent and the incident groups. However the prevalent patients had a longer mean length of BO. Prevalent dysplasia increased from 10/10 000 OGDs in 1984–89 to 21/10 000 OGDs in 2000–04 (95% CI 0.125 to 1.055, p = 0.016). The cumulative incidence (CI) was 0.04 in 1984–89 and 0.032 in 2000–04 (95% CI −180 to +154, p = 0.927). Incident dysplasia per 10 000 OGDs went up from 21 to 57 (95% CI 0.133 to 0.818, p = 0.008). The incidence density (ID) increased from 14 to 135 per 1000 surveillance years. There was an increasing trend towards the total number of dysplasias diagnosed each year. However, there were less dysplasia episodes (both, total, and prevalent) as a proportion of SIM diagnosis. Prevalent dysplasia doubled while the cumulative incidence went down slightly.
Conclusion: Patients with BO are twice likely to present with dysplasia on first endoscopy. Further progression of dysplasia on surveillance is slightly reduced. There is more resource utilisation because of the increasing number of dysplasia episodes.
072 NATURAL HISTORY OF DYSPLASIA IN BARRETT’S OESOPHAGUS
W. Faisal, G. Anagnostopoulos, P. Kaye, R. Logan, K. Ragunath.Wolfson Digestive Diseases Centre, University Hospital, Nottingham, UK
Introduction: The aim of any Barrett’s surveillance programme is to detect early oesophageal adenocarcinoma (AC) arising in dysplastic Barrett’s oesophagus (BO). The natural history of high grade dysplasia (HGD) is still debated and the general opinion about the benign course of low grade dysplasia (LGD) has been challenged by some recent studies.
Patients and Methods: A retrospective analysis of patient records who developed dysplasia at some point during their BO surveillance between the periods of 1985 to 2005, identified from a pathology database. All histopathology slides were reviewed according to Vienna classification, by an independent consultant GI histopathologist.
Results: We identified 67 cases of dysplasia in BO (48 male). Median length of follow up was 61 months (range 1–244). After review, 13 patients were downgraded from LGD to no dysplasia (ND) and were subsequently excluded from further analysis. The dysplasia progression data are shown in the table.
Abstract 63
In patients with HGD/AC, 13 had oesophagectomy, three had endoscopic mucosal resection (EMR), and two had radiotherapy. Overall, three out of six patients with persisting HGD had AC on operative histology (50%). All cause mortality was 31.5% (24% BO cancer related deaths).
Conclusion: In our cohort of patients with LGD, 24% progressed to AC over a period of five years, emphasising the fact that this is indeed a high risk group.
073 CANCER RISK IN BARRETT’S OESOPHAGUS: A META-ANALYSIS
T. Thomas, K. A. Abrams, J. de Caestecker, R. J. Robinson.Digestive Diseases Centre, Leicester, UK; Epidemiology and Public Health, University of Leicester, UK
Background: The risk of cancer in Barrett’s oesophagus (BO) is uncertain with studies showing a variable annual incidence (from 1/52 to 1/450). Recent reports have suggested regional variations in cancer incidence in the west.1 However no formal meta-analysis has been performed.
Aims and Methods: We aimed to determine by meta-analysis the incidence of oesophageal cancer in patients undergoing surveillance for BO and to examine geographical variation. A MEDLINE, EMBASE, and PubMed search of all English articles from 1966 to 2004, using the key words “Barrett’s oesophagus”, “Oesophageal cancer”, “surveillance”, “short segment Barrett’s” (SSBO) was done. References in retrieved papers and relevant review articles were scrutinised to identify papers missed on the initial search. Studies with patients who had histological confirmation of BO on surveillance, documented follow up data, and cancer as the outcome measure were included. Heterogeneity statistic (Q value) between studies was significant (p<0.05); hence a random effects model of meta-analysis was used. Conventional BO was defined as length of >3 cm.
Results: Forty two articles were included in the analysis for conventional BO and an additional seven articles were included for SSBO. The overall incidence rate for cancer was 8/1000 person-years duration of follow up (pyd) (95% CI 6 to 10). There was some geographical variation, with the incidence rate in UK being 9/1000 pyd (95% CI 4 to 17), USA 10/1000 pyd (95% CI 7 to 15), Europe 10/1000 pyd (95% CI 7 to 15), and others (Canada, Australia, New Zealand) 5/1000 pyd (95% CI 1 to 25). The overall cancer incidence in SSBO was 5/1000 pyd (95% CI 2 to 12). There was a non-significant increase in cancer risk in conventional BO compared to SSBO (OR 1.6, 95% CI 0.56 to 4.91, p = 0.30).
Conclusion: We found less geographical variation in BO cancer risk than previously suggested between US and UK and a non-significant increase in the risk of cancer in conventional BO versus SSBO.
1
074 ARGON PLASMA COAGULATION FOR BARRETT’S OESOPHAGUS: LONG TERM FOLLOW UP
T. Thomas, V. Talwar, K. K. Basu, J. de Caestecker.Digestive Diseases Centre, University Hospitals of Leicester, UK
Background: The long term efficacy of argon plasma coagulation (APC) for treating Barrett’s oesophagus (BO) is uncertain with concern about “buried glands” on histology.
Aims and Methods: To determine long term efficacy of APC treatment of BO. Follow up data of 50 patients entering an APC trial in 19991 followed up to August 2005 were obtained from endoscopy and pathology; all patients’ GPs were contacted.
Results: Forty were males, mean age 68 years (range 35–85). The median FU was 38 months (range: 3–75). Median BO length prior to APC was 5 cm (range 3–12) and median length on the last follow up endoscopy was 2 cm (range 1–12). There was a significant reduction in length of Barrett’s mucosa (mean reduction 3.2 cm, 95% CI 1.7 to 3.8, p<0.001). Although patients were instructed to remain on full dose twice daily PPI, significant reduction in PPI dose (half dose PPI: n = 13, standard dose PPI: n = 37, p<0.001) was observed. A mean of 9.2 biopsies per endoscopy was taken on the last follow up endoscopy. Of the 50 patients, 19 (38%) had a sustained endoscopic response (>90% squamous re-epithelisation) to APC but only nine (18% of 50) had complete histological clearance of BO at the end of follow up. The remaining patients (10/19) had either focal or multifocal buried glands on histology. No patient developed dysplasia or cancer. There was a weak but significant negative correlation between initial BO length (r = −0.3, p = 0.02) and eventual histological clearance of BO. Dose of PPI and eventual histological clearance was significantly correlated (r2 = 0.5, p = 0.006).
Conclusions: Sustained macroscopic clearance of BO following APC occurs in 38%. However 82% patients had histologically proven recurrence including 20% with buried glands. Initial length of Barrett’s mucosa and final dose of maintenance PPI correlate with successful outcome.
1
075 REACTIVE OXYGEN SPECIES INDUCED DNA DAMAGE IN OESOPHAGEAL ADENOCARCINOMA
N. J. Clemons, R. C. Fitzgerald.Oesophageal Group, Cancer Cell Unit, Hutchison-MRC Centre, Hills Road, Cambridge CB2 2XZ, UK
Introduction: Oesophageal adenocarcinoma develops in a step-like fashion from Barrett’s oesophagus (BO) through low and high grade dysplasia. Luminal components such as acid and bile salts are thought to contribute to the neoplastic progression. For example, pulsatile acid and bile exposure can alter proliferation and differentiation status in ex vivo and in vitro models and low pH can induce DNA damage in vitro. Recently, increased oesophageal concentrations of nitric oxide (NO) have been demonstrated in patients with BO. NO and its derivates have been shown to induce DNA damage in colorectal carcinogenesis.
Aims: In this study we have investigated the ability of NO and low pH to induce DNA damage in vitro by studying the phosphorylation of histone H2AX (γH2AX), a specific and early marker of double strand breaks (DSBs).
Methods: Adenocarcinoma cell lines BIC, SEG, and FLO and Barrett’s HGD cell lines ChTERT and GihTERT were treated with 25–200 μM NO donor NOC-9 (Axxora) or with pH3.5 media for 10–30 minutes. γH2AX was assessed by flow cytometry and confocal microscopy. Intracellular ROS production following acid treatment was assessed by flow cytometry using a fluorescent indicator. Long term survival was assessed by clonogenic assay.
Results: NO induced γH2AX in a dose dependent manner (p<0.05 for all doses). The ability of NO to induce γH2AX appears to occur only in cells that are in S-phase. Exposure of cells to low pH media also induced γH2AX (p<0.05), which was independent of cell cycle. Acid induced damage correlated with the intracellular production of reactive oxygen species (ROS), (p<0.05 at pH3.5 for 15 or 20 minutes). Mitochondria were not depolarised following exposure to low pH, ruling out mitochondrial damage as a source of ROS. Long term clonogenic survival studies demonstrated that cells were able to continue to grow following this initial insult.
Conclusions: NO and acid have the potential to generate DSBs in the oesophagus. If not repaired correctly these lesions could lead to gross genetic and chromosomal abnormalities that may aid in the progression of BO to adenocarcinoma.
076 PHOTODYNAMIC THERAPY OF EARLY OESOPHAGEAL CARCINOMA
C. Craig, M. Macpherson, H. Hodgson, J. Gray, M. Zammit, G. Fullarton.Department of GI Surgery, Gartnavel General Hospital, Glasgow, UK
Background: Surgical resection remains the gold standard treatment of early oesophageal cancer although with an increasingly elderly population many patients are unfit for this radical therapy and less invasive curative options are required.
Aim: To relate our experience of photodynamic therapy (PDT) in treating early oesophageal cancer.
Methods: Thirty oesophageal cancer patients (median age 74 years (range 64–90)) ; 80% adenocarcinoma, 20% squamous) over a six year period were found to have early stage disease based on endoscopic/CT and latterly endoscopic ultrasound(EUS)/CT staging criteria. Patients were deemed medically unfit for major resectional surgery and were selected for PDT. Each patient received iv sodium porfimer (Photofrin) at a dose of 2 mg/kg as the photosensitising agent 48 hours prior to endoscopy. Red light laser activation of the drug was initiated at endoscopy using a 630 nm fibre delivering a light dose of 300 j/cm. All patients had follow up endoscopy at 6–12 week intervals indefinitely. Routine biopsies of the treated area were obtained. Median follow up was 30 months (range 2–56).
Results: Overall 20/30 patients had an initial complete endoscopic and histological response to therapy at eight weeks post procedure. Of these 20 patients, 12 developed local recurrence and had further PDT with a median survival of 922 days (254–2049) and 2/12 cancer related deaths. Eight of 20 patients who had initial complete response remain disease free at follow up of 32.5 months (9–55). Only the latter 14 patients referred for PDT with suspected early cancer had EUS staging. Nine patients had early cancer T1 (n = 8),Tis(n = 1) and all currently remain disease free at a follow up of 1103 days (249–2019) although 5/9 required one further course of PDT. Five of 14 patients had T2 or 3 disease confirmed by EUS and all these patients have had recurrent disease post PDT. The major complication of PDT in this study was oesophageal stricturing which occurred in 50% of cases. These strictures have required a median of five dilatations (1–31).
Conclusion: PDT is an alternative potentially curative treatment in EUS confirmed early oesophageal carcinoma.
Neurogastroenterology and motility free papers
077 A DOSE RESPONSE TRIAL OF PHARYNGEAL STIMULATION FOR THE TREATMENT OF DYSPHAGIA POST STROKE
S. Singh1, M. Power2, P. Tyrrell2, D. G. Thompson1, S. Hamdy1.1Department of GI Science and 2Stroke Medicine, Hope Hospital, Salford, UK
Background: Up to half of patients suffering a stroke will be dysphagic; a complication that carries a sevenfold increased risk of pneumonia and is an independent predictor of mortality. Recently, electrical stimulation of the pharynx has been shown to enhance compensatory (swallowing) changes in the unaffected hemisphere of stroke patients which is associated with a 30% reduction in short term aspiration.
Aims: To assess the longer term dose response effects of electrical pharyngeal stimulation in dysphagic stroke.
Methods: Patients admitted with a clinical diagnosis of acute anterior circulation stroke were screened with a standardised videofluoroscopic swallowing assessment. Dysphagic patients were randomised by minimisation to one of four treatment groups or to a control group with age and stroke severity the controlled factors. The four treatment groups received 10 minutes of stimulation daily or three times a day and for three or five days. The control group received no intervention. Change in aspiration severity at the follow up videofluoroscopy at two weeks was then determined.
Results: Of 61 patients who underwent the baseline videofluoroscopy, 22 were found to be dysphagic and completed the study. Fifteen were male with a mean age of 73 (SD 11) years. Six were allocated to the control group with four in each active arm. Group data showed reduced aspiration following daily stimulation (−17% p<0.02) (fig 1) and three days of stimulation (−12% p<0.04) (fig 2) compared to controls (+13%).

Abstract 77, figure 1 Change in videofluoroscopy aspiration following different frequencies of pharyngeal stimulation.

Abstract 77, figure 2 Change in videofluoroscopy aspiration following different periods of pharyngeal stimulation.
Conclusion: These initial data suggest there is a long term clinical benefit from electrical pharyngeal stimulation. Further clinical trials are underway.
078 HYPERSENSITIVITY AGAINST INTRAGASTRIC CAPSAICIN IN PATIENTS WITH NON-ULCER DYSPEPSIA
J. Hammer, J. Matiasek, S. Ban.AKH Wien, Universitätsklinik Innere Medizin 4, Vienna, Austria
Background: We have recently demonstrated that chemical stimuli in the small intestine induce sensations comparable to mechanical distension and that chemical hypersensitivity against capsaicin might exist in the small intestine of dyspeptic subjects.
Aim: To develop a non-invasive test for the diagnosis of gastric capsaicin sensitivity and to evaluate whether chemical hypersensitivity is involved in the pathophysiology of non-ulcer dyspepsia (NUD).
Methods: Twenty healthy controls and 64 outpatients ingested a capsule containing 75 mg capsaicin after an overnight fast. Before and 30 minutes after ingesting the capsule, the severity of nine upper abdominal symptoms, were quantified by a graded questionnaire; an aggregate perception score was calculated by adding all symptom scores. The final perception score was calculated as the difference between pre- and post-test aggregate perception score. Data are given as mean (SD), a p value<0.05 was considered significant.
Results: Perception scores and p values are given in the table. Healthy controls developed week symptoms (mainly pressure, acid regurgitation, warmth), scores up to nine comprised 75% of the healthy volunteers and was considered as normal range. N = 14 (43.8%) of NUD patients were within the normal range, while n = 18 (56.3%) were above that limit. Other patient groups (inflammatory bowel disease with dyspeptic symptoms but no gastric involvement, peptic ulcer, other diseases) had an aggregate perception score comparable to controls, but significantly less than NUD patients.
Abstract 72
Conclusion: Patients with NUD are hypersensitive against gastric capsaicin. The intragastric capsaicin test is a non-invasive method to detect a subgroup of NUD patients with chemical hypersensitivity. The capsaicin receptor VR-1 is involved in the pathophysiology of more than 55% of NUD patients.
079 DIFFERENTIAL SELECTIVE AUTONOMIC RESPONSES IN VISCERAL AND SOMATIC PAIN
P. A. Paine, S. F. Worthen, A. R. Hobson, D. G. Thompson, L. J. Gregory, M. L. Phillips1, S. Williams1, Q. Aziz.Department of GI Sciences, Manchester University; 1Brain Imaging Unit, Institute of Psychiatry, King’s College London, UK
Background: Differences between visceral and somatic pain perception have been explored with brain imaging, however little attention has been given to differences in autonomic nervous system (ANS) responses such as skin conductance response (SCR) and heart rate variability band variance (BV). These are selective non-invasive central sudomotor sympathetic and cardiac parasympathetic measures respectively.
Aim: To determine differences in selective ANS responses for visceral and somatic pain matched for intensity and temporal characteristics.
Methods: In 19 healthy adults (eight male) SCR, BV and heart rate (HR) were measured at baseline and in response to oesophageal balloon distension and thermal cutaneous stimuli at pain intensity. 10 stimuli for each modality were delivered in two runs in counterbalanced order. Phasic SCR latency and rise time (powerlab), and 1 minute HR and BV blocks (MXedit) were processed offline and analysed with paired student t tests.
Results: HR was increased from baseline (mean 69.7(SE 2.35) beats per minute) during somatic (71.36 (2.2), p = 0.045) and visceral pain (72.73 (2.3), p = 0.006). There was greater increase in HR by visceral than somatic pain (p = 0.017). BV withdrawal from baseline (6.64 (0.32) ms2) was greater for somatic (6.35 (0.29)) than visceral pain (6.6 (0.27), p = 0.007). SCR latency was shorter for visceral (4.45 (0.4) seconds) than somatic pain (6.77 (0.59), p = 0.0002) as was SCR rise time (visceral 8.41 (0.67); somatic 11.08 (0.77) seconds, p = 0.005).
Conclusion: In comparison to somatic pain, the larger HR response to visceral pain was mediated by greater sympathetic activation despite lesser central cardiac parasympathetic withdrawal. These differential ANS responses for visceral pain may reflect its greater unpleasantness compared with somatic pain of the same intensity. Selective ANS measures hold promise both for understanding mechanisms and as markers of differences in pain response.
080 GUT RESPONSE TO STRESS CAN BE PHARMACOLOGICALLY MODULATED: AMITRIPTYLINE MODIFIES VISCERAL HYPERSENSITIVITY IN IRRITABLE BOWEL SYNDROME
C. D. R. Murray, E. Tripoli, M. C. L. Pitcher, M. A. Kamm, A. V. Emmanuel.St. Mark’s Hospital, Watford Road, Harrow HA1 3UJ, UK
Introduction: Acute physical stress causes a measurable acute alteration of gut autonomic function and visceral hypersensitivity in patients with irritable bowel syndrome (IBS) (Murray et al. Gastroenterology 2004). Low doses of amitriptyline are effective in over 50% of IBS patients, through mechanisms that are unclear. We present the first report of the effects of amitriptyline on the gut neural response to acute stress.
Methods: Nineteen patients with constipation-predominant IBS (16 female, mean age 32, range 19–58) were given amitriptyline 25–50 mg at night. Patients underwent stress assessment at baseline and after three months of treatment. Stress assessment comprised a physical (cold pressor) and psychological (dichotomous listening) stress given in random order at least one day (median 1, range 1–4 days) apart. Physiological parameters measured included: perception of stress (visual analogue scale); systemic autonomic tone (heart rate and blood pressure); gut specific autonomic innervation (laser Doppler flowmetry of rectal mucosal blood flow (RMBF)); and visceral sensitivity (rectal electrosensitivity). 13 patients underwent barostat assessment of rectal sensitivity.
Results: Fourteen of 19 (74%) patients were symptomatically improved after three months of amitriptyline (median dose 25 mg). Acute stress resulted in increased perception of stress and systemic autonomic tone, and reduced RMBF, which was similar in responders and non-responders (p>0.05 for all). In contrast, all non-responders and only three out of 14 of responders, continued to exhibit stress-induced reduced pain threshold at three months (change from baseline −31% v +2%, p<0.03 respectively). Responders increased thresholds for pain from 21 (pre-) to 31 mmHg (post-treatment) above distending pressure (p<0.03). No such change was seen in non-responders (from 23 to 24 mmHg, respectively).
Discussion: Amitriptyline is effective in constipation predominant IBS patients. This effect is primarily on stress induced visceral hypersensitivity, independent of autonomic tone. The gut response to acute stress is a viable target to study drug efficacy in IBS.
081 PREGABALIN, A SECOND GENERATION α2δ LIGAND REDUCES HYPERSENSITIVITY TO RECTAL DISTENSION IN PATIENTS WITH IRRITABLE BOWEL SYNDROME
L. A. Houghton, C. Fell, R. Lea, P. J. Whorwell, I. Jones1, D. P. Sudworth1, J. D. Gale1.Academic Department of Medicine, University Hospital of South Manchester; 1Pfizer Global R&D, Sandwich, UK
Background: Visceral hypersensitivity is an important pathophysiologic factor in irritable bowel syndrome (IBS). Preclinical data indicate that pregabalin reduces trinitrobenzene sulfonic acid (TNBS) induced hypersensitivity but not basal sensitivity to colonic distension.1
Aim: To assess the effect of pregabalin on the perception of rectal distension in hypersensitive IBS patients.
Methods: Twenty six rectally hypersensitive Rome II IBS patients (aged 18–46 years, 7 male) were included in a randomised, double blind, placebo controlled, parallel group study in which they received either three weeks oral pregabalin (titrated: 50 mg tid days 1–3, 100 mg tid days 4–7, 150 mg tid days 8–11; fixed: 200 mg tid days 12–21±4) or placebo control. Rectal sensitivity was assessed using a barostat technique, in which sensory thresholds were determined using the ascending methods of limits followed by tracking, both prior to treatment (baseline) and on day 21±4 of treatment. Rectal hypersensitivity at baseline was defined as a pain threshold of ⩽28 mmHg.
Results: Pregabalin significantly increased the sensory thresholds from baseline for first sensation (median difference from placebo (95% CI): 2.0 mmHg (0 to 4.0) mmHg; p = 0.045), stool (6.0 mmHg (2.0 to 10.0) mmHg; p = 0.008), and pain (5.4 mmHg (0.12 to 11.25) mmHg; p = 0.048) compared with placebo. Baseline sensory thresholds were comparable between treatment groups. An emax model provided the best fit to the compliance data. Pregabalin significantly increased rectal compliance (slope of the volume pressure curve was 1.96 steeper than placebo (95% CI 1.50 to 2.41) p<0.0001).
Conclusions: Pregabalin increases the pain threshold to distension in IBS patients with rectal hypersensitivity. This may result from an increase in rectal compliance. These data suggest that α2δ ligands might prove useful in the treatment of the visceral pain disorders, such as IBS.
1
Colorectal free papers
082 CAN ARTIFICIAL NEURAL NETWORKS PREDICT WHICH PATIENTS NEED A COLONOSCOPY?
S. Maslekar, A. Gardiner, G. S. Duthie.Academic Surgical Unit, University of Hull, Cottingham, UK
Introduction: Artificial neural networks (ANN) are computer programs used to identify complex relations within data sets undetectable with conventional linear statistical analysis. One such complex problem is the prediction of need for lower gastrointestinal endoscopy in individual patients consulting for gastrointestinal symptoms. Routine predictions have low accuracy and result in large numbers of normal colonscopies with obvious implications, both logistic and economic. We aimed to develop a neural network algorithm which can predict the need for lower gastrointestinal endoscopy in patients attending the routine outpatient clinics.
Methods: Prospective clinical data of 200 patients undergoing elective colonoscopy were collected. The specifically developed questionnaire included 40 variables based on clinical features. Complete data sets of 50% of the series were used to train the ANN: remaining 50% used for internal validation. The primary output was a positive finding on the colonoscopy, including polyps, cancer, diverticular disease, or colitis.
Results: The outcome and pathology reports of all patients were obtained and assessed. Clear correlation between actual data value and artificial neural network value were found (r = 0.931; p = 0.0001). The predictive accuracy of the neural network was 95% in the training group and was 89% (95% CI 84 to 96) in the validation set. This accuracy was significantly higher than the clinical accuracy (69%).
Conclusions: Artificial neural networks are more accurate (89% correlation) than standard statistics (67%) when applied to the prediction in individual patients of the need for lower gastrointestinal endoscopy. The results obtained highlight their obvious usefulness, which could now be used in a prospective evaluation for application of the technique.
083 ASSESSMENT OF INFLAMMATION WITHIN SPORADIC COLORECTAL POLYPS
M. H. McLean, G. I. Murray1, N. Fyfe1, G. L. Hold, N. A. G. Mowat, E. M. El-Omar.GI Research Group, Department of Medicine and Therapeutics, Aberdeen University; 1Department of Pathology, Aberdeen University, UK
Background: Chronic inflammation is a risk factor for many cancers yet its relevance to sporadic colorectal cancer is often dismissed. Most cancers arise from adenomatous polyps, which are constantly exposed to physical, chemical, microbial, and hypoxic stress. We hypothesise that chronic inflammatory activity within benign precancerous polyp tissue is central to cellular transformation towards colorectal malignancy.
Aims: To assess the inflammatory cell infiltrate in adenomatous polyps of varying sizes and their adjacent normal mucosa.
Methods: Paraffin embedded tissue from 58 colonic polyps (29 small ⩽1 cm and 29 large >1 cm) and 35 corresponding normal mucosal biopsies from 35 patients were studied. Inflammatory cell infiltrate was assessed using immunohistochemistry. Antibodies against CD3, CD4, CD8, CD25, CD20, CD38, CD56, CD68, and neutrophil elastase were used to assess the presence of T cells (helper, cytotoxic, and activated subsets), B cells, plasma cells, NK cells, macrophages, and neutrophils, respectively.
Results: In small polyps neutrophil infiltrate was increased compared to normal mucosa (p<0.001). Macrophage infiltrate was significantly increased in large polyps compared to paired normal mucosa (p<0.01). There was also a significantly increased neutrophil and activated T cell infiltrate in large polyps compared to paired normal mucosa (p<0.01 and p<0.001, respectively). Large polyps had an increased activated T cell (p<0.001) and macrophage (p<0.001) infiltrate compared to small polyps. B cells, TH cells, TC cells, mast cells, and NK cells were present in similar numbers in both normal and polyp tissue.
Conclusion: Inflammatory cell infiltrates are a key feature of adenomatous polyps and manifest as acute inflammation in small polyps and acute on chronic in larger polyps. These findings may be relevant to the pathogenesis of sporadic colorectal cancer and the aetiology of this inflammatory activity warrants further investigation.
084 EXPRESSION OF CYCLOOXYGENASE-2 IN HUMAN SPORADIC COLORECTAL ADENOMAS
M. H. McLean, G. I. Murray1, N. Fyfe1, G. L. Hold, N. A. G. Mowat, E. M. El-Omar.GI Research Group, Department of Medicine and Therapeutics, Aberdeen University; 1Department of Pathology, Aberdeen University, UK
Background: Aspirin and other NSAIDs are effective chemopreventive agents in colorectal neoplasia but the mechanisms by which they work remain unclear although inhibition of cyclooxygenase-2 (COX-2) is thought to be a key molecular target. COX-2 is overexpressed in the majority of human colorectal cancers (CRC) and in a variable proportion of colonic adenomas. However, there are conflicting data regarding the extent and localisation of COX-2 expression within adenomatous polyps.
Aim: To assess COX-2 expression in colonic polyps of varying sizes and immediately adjacent normal mucosa.
Methods: Immunohistochemistry for COX-2 was performed on 35 normal mucosal biopsies and 49 colonic polyps from 35 patients. Expression and localisation of COX-2 was studied using an antihuman COX-2 isoform specific antibody. Immunoreactivity was detected by signal amplification following heat induced antigen retrieval. A CRC tissue microarray was used as a positive control.
Results: The colorectal cancer cores exhibited positive staining in the cytoplasm of neoplastic epithelial cells. All (100%) of the normal mucosal sections were negative for COX-2 staining. In contrast, 69% of the polyps stained positive for COX-2 (p<0.001). Of these, 77% displayed immunoreactivity within the stroma alone and 23% showed positivity in the neoplastic epithelium, with or without stromal positivity. Immunoreactivity was focal with stromal positivity mainly localised to the periphery of the polyp lesions. 80% of large polyps (>1 cm) and 55% of small polyps (⩽1 cm) were positive for COX-2 (large v small p<0.001).
Conclusion: COX-2 expression was demonstrated in the majority of colonic adenomas. Localisation of this was mainly in stromal cells. The stromal microenvironment of colonic adenomas and its interface with neoplastic epithelium may be important in cellular transformation towards malignancy, and warrants further investigation.
085 MITOCHONDRIAL DNA (MTDNA) MUTATIONS IN HUMAN COLONIC CRYPTS: A NOVEL BIOMARKER OF COLORECTAL CANCER
R. P. Arasaradnam, L. C. Greaves1, D. Commane, J. C. Mathers, R. W. Taylor1, D. M. Turnbull1.Human Nutrition Research Centre; 1Mitochondrial Research Group, University of Newcastle, UK
Background: There is considerable interest in the quest for a reliable “biomarker” of colorectal cancer (CRC). Mitochondrial DNA (mtDNA) mutations have been suggested to play a role in ageing and given that CRC occurs more commonly as we age there may be an association. Furthermore, mtDNA mutations have been shown to accumulate within colonic crypt stem cells to levels that result in respiratory chain deficiency. The presence of mtDNA mutations within colonic crypt stem cells suggests that these mutations are present before the development of colorectal cancer, thus it is not unreasonable to suggest that mtDNA mutations may prove to be a putative biomarker of risk of CRC.
Aim: To characterise mtDNA mutational load in colonic crypts of patients with macroscopically normal colorectal mucosa.
Methods: Fresh frozen colorectal tissue from 21 patients (8 males) with macroscopically normal colorectal mucosa were analysed histologically and histochemically. Standard H&E histology was performed as well as dual cytochrome c oxidase/succinate dehydrogenase (COX/SDH) histochemistry to determine respiratory deficiency within crypts. The percentage of COX deficient crypts were calculated from transverse sections counted; only crypts that had more than 50% COX deficient cells were defined as COX deficient.
Results: See table. These are results from the initial pilot study. COX deficiency was identified in colonic crypts of patients with macroscopically normal colon; thus confirming the presence of mtDNA mutations. The mitochondrial mutational load was significantly higher in those over 50 years of age (Wilcoxon signed ranks; p = 0.016), compared to those under 50 years. These findings lend further support to the hypothesis that mtDNA mutational rate increases with age. Given that CRC occurs more commonly as we age there could be an association.
Abstract 78
Conclusions: We have shown that COX deficient colonic crypts have been identified in the macroscopically normal colon. Hence, mtDNA mutations may prove to be a useful putative biomarker of CRC risk especially in those over 50 years. Further studies on the influence of dietary intake on mtDNA mutational load are ongoing.
Abstract 85
086 EVALUATION OF AUTOFLUORESCENCE COLONOSCOPY FOR THE DETECTION AND DIAGNOSIS OF COLONIC POLYPS
A. L. McCallum, J. T. Jenkins, D. Gillen1, R. G. Molloy.Department of Surgical Gastroenterology; 1Department of Gastroenterology, Gartnavel General Hospital, Glasgow, UK
Background: Autofluorescence (AF) has been developed to enhance conventional white light (WL) endoscopy in the diagnosis of neoplastic lesions of the GI tract. It is based on the stimulation of endogenous fluorophores and produces a pseudo-colour image of tissue. Metaplastic polyps are common and do not need to be treated, whereas adenomatous polyps carry a neoplastic potential. It would therefore be helpful to be able to distinguish between adenomatous polyps and metaplastic polyps when performing colonoscopy.
Aim: To evaluate AF for the endoscopic detection and differentiation of colorectal polyps.
Methods: Patients were invited to attend for colonic assessment with both AF and WL colonoscopy. The intensity of autofluorescence (AI) is quantified automatically and readings, pictures, and biopsies were recorded of any visible pathology or areas of high AF. The biopsy results were analysed and an AI reading for each biopsy site obtained by subtracting the actual AI reading from the background reading for the rectum of each patient.
Results: A total of 47 patients were assessed with AF and WL colonoscopy. A total of 33 polyps were detected (19 adenomatous and 14 metaplastic polyps). It was found that adenomatous polyps had higher AI readings (median 0.53, IQR 0.15–1.05), than metaplastic polyps (median 0.09, IQR 0.06–0.10) (Mann-Whitney U test: p = 0.00003).
Conclusion: These early data suggest that autofluorescence colonoscopy has the potential to differentiate between metaplastic and adenomatous polyps and may have a role as a new diagnostic technique for the improved detection of colonic dysplasia and early malignancy.
Plenary session
087 ALPHA-FETOPROTEIN SPECIFIC CD4+ T cell responses are unmasked during transarterial embolisation in hepatocellular carcinoma
L. Ayaru1, S. P. Pereira1, T. Meyer2, B. R. Davidson3, A. K. Burroughs3, R. Williams1, S. Behboudi1.1UCL Institute of Hepatology, 2Academic Depatrment of Oncology and 3University Department of Surgery and Liver Transplantation, RF&UCL Medical School, University College London, UK
Background: Tumours regulate immune responses and may mask anti-tumour immunity. We hypothesised that necrosis produced by transarterial embolisation (TAE) of HCC may induce and/or expand pre-existing T cell responses to tumour rejection antigens such as AFP. We have recently reported the presence of AFP364-373 reactive CD4+ T cells in HCC patients (Clin Can Res 2005). Here we aimed to identify populations of CD4+ T cells unmasked by TAE and characterise further epitopes which could be targeted in an AFP based vaccine against HCC.
Methods: In the peripheral blood of 31 untreated HCC patients and 24 controls (chronic liver disease, liver metastases, normal), AFP specific CD4+ T cell responses to a panel of 59 AFP derived peptides were analysed using intracellular cytokine assays for IFN-γ, IL-2, and IL-5. Blocking HLA antibodies were used to determine the presenting MHC class II molecules. Six patients were recruited from a randomised trial of TAE versus chemoembolisation (TACE) and the presence of AFP reactive CD4+ T cell responses analysed longitudinally for six months.
Results: Two novel AFP derived CD4+ T cell epitopes, AFP32 and AFP94, were identified that were recognised by circulating lymphocytes in association with HLA-DR. Of the 31 untreated patients with HCC, eight had CD4+ T responses to AFP364-373, one to AFP32, and none to AFP94. There were no detectable responses in the controls. In all treated patients, AFP-reactive CD4+ T cells were expanded in vivo during therapy and then declined in frequency. Preliminary data point to an association between clinical responses (as assessed by CT criteria) and high frequencies of AFP specific CD4+ T cells.
Conclusion: Necrosis produced by TACE/TAE unmasks AFP specific CD4+ T cell responses and provides a potential window for successful immunotherapy. We have identified novel AFP derived CD4+ T cell epitopes which could be targeted in an AFP based vaccine against HCC.
088 REAL-TIME IMAGING AND FUNCTIONAL ANALYSIS OF HUMAN COLONIC CRYPT RENEWAL EX VIVO
A. Parris, A. Reynolds, A. Spahos, A. Munsterberg, R. Tighe, M. Lewis, J. Cook, A. Prior, C. Speakman, H. J. Stebbings, K. Ellamin, M. Williams.School of Biological Sciences, University of East Anglia, UK; Department of Gastroenterology, Norwich and Norwich University Hospital, UK
Background: Following on from classical animal studies and work on adenocarcinoma cell lines, recent gene targeted and transgenic mice studies have provided profound insights into the molecular determinants of epithelial renewal in the intestine. Despite, and because of, this progress, there is an increasing call for a complementary in vitro model of the intact human colonic epithelium.
Aims: To apply bio-imaging and functional genomic approaches to the study of intestinal tissue renewal in cultured human colonic crypts.
Methods: Colonic crypts were isolated from tissue biopsies obtained at sigmoidoscopy from healthy subjects (ethical approval). Isolated crypts were attached to collagen coated coverslips and cultured for 24 hours–7 days in serum-free DMEM (5%CO2/37°C). Expression constructs and siRNA oligonucleotide duplexes were introduced to cells by low voltage square wave electroporation. Gross morphology was monitored in real-time by digital video time lapse microscopy (24–48 hours). For immunofluorescence studies cultured crypts were fixed in 4% paraformaldehyde and specific protein expression probed for by a primary antibody and visualised using a FITC conjugated secondary antibody in conjunction with confocal microscopy. A range of markers for cell polarity (for example, NKCC1), cell proliferation (for example, BrdU incorporation and Ki67), and viability (for example, propidium iodide) were employed. Cell migration was assessed by monitoring Hoechst 33342 or α−tubulin-GFP labelled cells. Intracellular calcium signalling was monitored in Fura2 loaded crypts.
Results: Colonic crypts maintained their gross morphological flask-like appearance bounded by a distinctive lumen for at least sevendays in culture. Expression of basolateral membrane transporters (for example, NKCC1) and membrane receptors (for example, M3AChR) continued throughout the culture period as did the topological gradient of expression along the crypt axis. Accordingly, the colonic crypt calcium wave signature induced by acetylcholine maintained its site of initiation at the base and unidirectional propagation along the crypt axis. The proliferative zone was maintained at the crypt base (Ki67 positive). Autocrine mitogenic signals were confirmed by the presence of nuclear β-catenin in cells located at the crypt base; all other cells exhibited membranous β-catenin labelling. BrdU labelled cells migrated to the upper crypt (Ki67 negative) over the course of 48 hours. Tracking of Hoechst 33342 and GFP labelled cells revealed a migration rate of approximately 10–15 μm/hour. Cells were shed at crypt mouth and were positive for propidium iodide, whereas cells located elsewhere in the crypt excluded propidium iodide. Cell viability was compromised in lower crypt compartments by siRNA knockdown of β-catenin.
Conclusions: Isolated human colonic crypts are amenable to real-time imaging and functional genomic studies. We have demonstrated that many of the cellular processes associated with rapid renewal of the colonic epithelium are recapitulated ex vivo.
089 IMPROVING THE EXPERIENCE OF PATIENTS HAVING AN ENDOSCOPY WITH THE ENDOSCOPY GLOBAL RATING SCALE
R. M. Valori, D. Johnston1, V. Tailor1.Gloucestershire Royal Hospital, Great Western Road, GL1 3NN; 1National Endoscopy Team
The endoscopy Global Rating Scale (GRS) is a web based instrument designed to help endoscopy units deliver a patient focused service and assess how well they are doing. The GRS includes 12 items that reflect the experience of a patient having an endoscopy. The items are ranked into four levels: D to A. Level D is very basic and A is excellent. All endoscopy units in England were invited to complete the GRS on two census dates: April and October 2005. Of registered units 80% completed scores in April and 66% in October (to date). The results are presented as the percentage of A and B scores for each of the items.
The very high completion rates of the GRS indicate that the service finds the GRS acceptable and useful. All items showed an increase in the percentage of A and B scores between the two census dates. These changes reflect real improvements in the processes that underpin the experience of a patient having an endoscopy and/or the ability of the service to demonstrate that it provides high quality care. These data show that the GRS is an effective service improvement tool.
090 ASPIRIN FOR THE PREVENTION OF RECURRENT COLORECTAL ADENOMAS: RESULTS OF THE UKCAP TRIAL
R. F. A. Logan, K. R. Muir, M. J. Grainge, V. Shepherd on behalf of the ukCAP Trial GroupDivision of Epidemiology & Public Health, University of Nottingham, University Hospital, Nottingham NG7 2UH, UK
Background: Many observational studies have found regular aspirin use is associated with a reduced risk of colorectal (CR) cancer and two randomised trials have shown that aspirin reduces risk of recurrent CR adenomas, although results were not wholly consistent. We report the preliminary aspirin results of a large factorial trial of aspirin (enteric 300 mg/day) and folate supplements in patients under surveillance for recurrent CR adenomas.
Methods: A double blind, placebo controlled randomised trial was carried out in 10 centres (nine in the UK and one in Denmark). Patients who had one or more adenomas (⩾0.5 cm) removed in the six months before enrolment were randomised to receive either aspirin (enteric 300 mg/day) or placebo. All participants were followed up at intervals of four months to assess compliance, with a second colonoscopy arranged for three years after the date of trial entry. The primary outcome measure was a histologically confirmed CR adenoma or cancer either at the end examination or during the course of the trial.
Results: 945 patients were recruited into the study, of which 853 (434 receiving aspirin and 419 placebo) underwent a second colonoscopy and were included in an intention to treat analysis. Full compliance with trial medication was reported by 700 patients. In total, 101 (23.3%) patients receiving aspirin had a recurrent adenoma compared with 120 (28.6%) patients who received placebo (relative risk = 0.81; 95% CI 0.65 to 1.02). 103 advanced CR adenomas were observed (on the basis of villous/tubulovillous features, size ⩾1 cm or evidence of severe dysplasia or cancer); 39 (9.0%) of these were in the aspirin group and 64 (15.3%) in the placebo group (RR = 0.59; 95% CI 0.40 to 0.86), 11 CR cancers were included among these (3 aspirin and 8 placebo).
Conclusion: Aspirin use (300 mg/day) resulted in a 19% reduction in risk of any colorectal adenoma recurrence and a marked, statistically significant, 41% reduction in risk of advanced adenoma development.
Gastrointestinal physiology associates group
091 INGESTED LIPID MODULATES HYPOTHALAMIC AND BRAINSTEM NEURONAL ACTIVITY IN MAN
D. J. Lassman1, S. McKie1, L. J. Gregory1, G. J. Dockray2, S. Williams3, D. G. Thompson1.1University of Manchester, UK; 2Department of Physiology, University of Liverpool, UK; 3Institute of Psychiatry, London, UK
Background: In animals, ingested lipid releases cholecystokinin (CCK) which is known to regulate food intake via activation of vagal CCK-1 receptors. This leads to modification of eating behaviour via activation of brainstem and hypothalamic neural circuits. In man, however, techniques for assessing lipid/CCK modulation of neuronal activity in these brain regions have not hitherto been possible and the mechanisms are therefore unknown.
Methods: Five fasted healthy volunteers underwent blood oxygenation level dependent (BOLD) functional magnetic resonance brain imaging using a 1.5T scanner before and after intraduodenal infusion of a CCK releasing lipid. Visual analogue scores of satiety sensations were also recorded.
Results: A rapid and early increase in hypothalamic 1.2% (0.7) and brainstem 0.9% (0.1) neuronal activation was seen after lipid compared to baseline (mean % increase in BOLD signal at 11 minutes +/−SE p<0.002). The infusion of lipid was associated with a 32% (11%) decrease in hunger and 163% (30%) increase in fullness scores compared to baseline (mean change in score +/− SE, p<0.05).
Conclusion: This is the first demonstration of brainstem and hypothalamic activation by ingested lipid in normal humans and the feasibility of this type of approach using fMRI is hereby established. Further studies using a CCK-1 receptor antagonist will demonstrate the extent to which these effects are specific to CCK-vagus signalling.
092 ACETYLCHOLINE STIMULATION OF THE NKCC1 TRANSPORTER IS CALCIUM DEPENDENT AND IS RAPIDLY DESENSITISED BY ENDOCYTOSIS: IMPLICATIONS FOR INTESTINAL FLUID SECRETION
A. Reynolds, A. Parris, R. Tighe, M. Lewis, D. Westgarth, D. Bell, C. Jamieson, K. Murray, J. Southgate, K. Sargen, M. Williams.School of Biological Sciences, University of East Anglia, UK; Department of Gastroenterology, Norwich and Norwich University Hospital, UK
Background: Intestinal fluid secretion is driven by transcellular active transport of chloride. NKCC1 mediates basolateral uptake of chloride and is emerging as a master controller of intestinal fluid secretion. Although it has long been established that acetylcholine (ACh) stimulates transient intestinal fluid secretion, the regulation of NKCC1 activation and its role in governing the nature of this response has not been investigated in the intact human colonic epithelium.
Aim: To characterise NKCC1 expression along the human colonic crypt axis and study its activation by propagating cholinergic calcium signals.
Methods: Colonic crypts were isolated from tissue biopsies obtained at sigmoidoscopy from healthy subjects (ethical approval). Isolated crypts were attached to collagen-coated coverslips and cultured for 24 hours–7 days in serum-free DMEM (5%CO2/37°C). Total NKCC1 expression was probed for using a panel of polyclonal antibodies. Labelling was visualised using a FITC conjugated secondary antibody in conjunction with confocal microscopy and semiquantitative image analysis. Phospho-NKCC1 was detected using a specific polyclonal antibody raised against a diphosphopeptide containing Thr212 and Thr217. For calcium imaging experiments colonic crypts were loaded with the calcium-sensitive dye Fura2-AM.
Results: NKCC1 exhibited an expression gradient along the crypt axis; labelling was basolateral and predominated at the crypt base. The secretagogue acetylcholine (ACh) initiated calcium signals at the human colonic crypt base, which propagated in a unidirectional fashion along the entire crypt axis. Calcium responses were greatest at the crypt base and progressively diminished towards the crypt mouth (n>30; p<0.01). Calcium signal intensity and degree of propagation along the crypt axis was concentration dependent (EC50 = 1–10 μM; n>20, p<0.01). Ach stimulated phospho-NKCC1 labelling exhibited a similar concentration dependency and kinetics to the calcium response. TMB-8 (100 μM), an inhibitor of intracellular calcium mobilisation, abolished Ach stimulated calcium signals and NKCC1 phosphorylation. Phospho-NKCC1 levels peaked at 3 minutes post-stimulation and diminished in the continued presence of ACh (10 μM). After prolonged exposure (15 minutes) NKCC1 membrane labelling diminished and NKCC1 levels accumulated in cytosolic vesicles juxta lateral membranes towards the apical pole.
Conclusions: A striking spatial correlation exists between ACh induced colonic crypt calcium signals, and calcium dependent NKCC1 activation. These observations suggest that propagating cholinergic calcium signals coordinate fluid secretion along the human colonic crypt axis and that NKCC1 endocytosis may be an important mechanism in downregulating the secretory response.
This work was supported by the BBSRC.
Gastroduodenal free papers
093 PREDICTING CLINICAL OUTCOME IN UPPER GASTROINTESTINAL BLEEDING COMPLICATING LOW DOSE ASPIRIN AND ANTI-THROMBOTIC THERAPY
A. S. Taha1, W. J. Angerson2, R. P. Knill-Jones3, O. Blatchford4.1Gastroenterology Unit, Crosshouse Hospital, Kilmarnock and Departments of 2Surgery and 3Public Health & Health Policy, University of Glasgow, and 4Public Health Medicine, Argyle & Clyde Health Board, UK
Background and Aims: Current risk stratification systems have not specifically corrected for the intake of low dose aspirin and other anti-thrombotic drugs. As the incidence of upper gastrointestinal bleeding (UGIB) related to these agents has been increasing, we aimed at testing the Blatchford scoring system in predicting the clinical outcome in bleeders using these drugs.
Methods: The Blatchford scores cover risk factors and associated components measured on admission (Lancet 2000;356:1318–21). These include blood urea, haemoglobin, systolic blood pressure, pulse, melaena, syncope, hepatic disease, and cardiac failure. We assessed the ability of this system to predict the clinical outcome of UGIB in 529 patients attending a single centre, including 129 on low dose aspirin, 46 on other anti-thrombotic drugs, and 68 on NSAIDs.
Results: The median scores were as follows: no risk factors, 5; NSAIDs, 8; aspirin, 7; other anti-thrombotics, 6; excess alcohol, 4; multiple risk factors, 7; (p = 0.003, Kruskal-Wallis). Scores in all groups except excess alcohol users were elevated relative to those with no risk factors (p⩽0.05). Scores correlated positively with the duration of admission in the entire study group (r2 = 0.267; p<0.001) and in those taking aspirin and other anti-thrombotics (r2 = 0.189; p = 0.017). The median scores in patients requiring blood transfusion were 10 in the entire study group and 10 in users of aspirin or anti-thrombotic drugs, compared with 3 and 4 respectively in those not transfused (p<0.001).
Conclusions: The Blatchford scores, derived on admission from clinical details of patients with UGIB, are significantly elevated in users of NSAIDs, low dose aspirin, and other anti-thrombotic drugs. They also correlate positively with the duration of admission, and can predict the need for transfusion in such patients.
094 HELICOBACTER PYLORI INFECTION CONFERS AN INCREASE IN 10 YEAR MORTALITY FROM ALL CAUSES: DATA FROM A COMMUNITY SCREENING PROGRAMME
A. C. Ford1, A. G. Bailey1, D. Forman2, A. T. R. Axon1, P. Moayyedi3.1Centre for Digestive Diseases, Leeds General Infirmary, Leeds; 2Centre for Epidemiology and Biostatistics, Leeds University Medical School; 3Gastroenterology Division, Health Sciences Centre, Hamilton, Canada
Introduction: Population screening and treatment of Helicobacter pylori has been advocated to reduce mortality from gastric cancer. Screening programmes have been conducted in the West, but follow up was at two years, therefore long term mortality data are not yet available.
Methods: This was a 10 year follow up study of individuals currently aged 50–59 years, previously recruited into a screening and treatment programme for H pylori. Those testing positive were randomised to receive either eradication therapy, or placebo. All those involved were traced with a list cleaning service provided by the Office for National Statistics, and death certificates were obtained for deceased individuals.
Results: Of 8407 original participants, 140 (1.7%) were dead at 10 years. 92 (66%) were male. 64 (46%) deaths were due to cancer, and 31 (22%) to ischaemic heart disease (IHD). Mortality from all causes and IHD were significantly increased in H pylori positives compared to negatives (odds ratios (OR) 1.65; 95% CI 1.15 to 2.36 and 2.46; 95% CI 1.13 to 5.32 respectively) but there was no difference in cancer mortality (OR 1.37; 95% CI 0.78 to 2.36). Following logistic regression controlling for age at study entry, gender, tobacco and alcohol consumption, and social class, all-cause mortality remained significantly higher in H pylori positives (OR 1.46; 95% CI 1.02 to 2.09). There was a trend towards higher all-cause mortality and mortality from IHD in those receiving eradication therapy at 10 years compared to placebo (relative risks 1.46; 95% CI 0.85 to 2.49 and 2.0; 95% CI 0.69 to 5.84 respectively), though neither were statistically significant.
Conclusions: Infection with H pylori is associated with an increased mortality from all causes, even when possible confounding factors are controlled for. However, screening and treatment of positive individuals may confer an increased risk of death from IHD, which should be borne in mind when recommending the adoption of such a strategy.
095 INNATE IMMUNE RESPONSE GENE POLYMORPHISMS AND THEIR ROLE IN H PYLORI INDUCED PRECANCEROUS CHANGES
G. L. Hold1, M. G. Smith1, S. H. Berry1, K. E. McColl2, E. M. El-Omar1.1Department of Medicine and Therapeutics, Aberdeen University; 2Department of Medicine and Therapeutics, Glasgow University, UK
Background: The innate immune system plays a crucial role in the initial handling of H pylori infection. Toll-like receptors (TLRs) are important members of this system and at least five TLRs (TLR2, 4, 5, 9, and 11) are involved in recognising bacterially derived pathogen associated molecular patterns. Most of these genes have functionally relevant polymorphisms but apart from TLR4, there have been few data on the role of these polymorphisms in H pylori pathogenesis.
Aim: We examined whether SNPs in TLR2 (TLR2 Arg753Gln), TLR5 (TLR5392Stop), TLR9 (TLR9-1237 C/T), and CD14 (CD14-159 C/T) influenced the risk of developing gastric atrophy and hypochlorhydria (ATR/HC), the most important precursors of gastric cancer.
Subjects and Methods: We used PCR-RFLP and 5′ nuclease assays to genotype the four SNPs in 170 healthy gastric cancer relatives (GCR) and 100 population controls.
Results: There was a significant association between carriage of TLR9: 1237G/A and CD14-159C/T SNPs and presence of hypochlorhydria and gastric atrophy. Compared to infected subjects who did not develop ATR/HC, the odds ratio for H pylori induced ATR and HC in subjects with the TLR9: 1237G/A was 3.9 (95% CI 1.7 to 8.6) and CD14-159 C/T was 3.8 (95% CI 1.4 to 9.8). Although the functional consequences of the TLR9 promoter polymorphism are unknown, in silico analysis indicates disruption of an NF-κB binding site. In contrast, the functional CD14 polymorphism affects binding of the GC box and also Sp proteins.
Conclusions: Our results indicate that carriage of the TLR9 –1237G/A and CD14-159 C/T polymorphisms predispose H pylori infected subjects to a severe phenotype characterised by hypochlorhydria and gastric atrophy. These findings call for further evaluation of innate immune gene polymorphisms in the context of H pylori induced gastric cancer.
096 GASTRIN INCREASES MCL-1 EXPRESSION IN AGSGR gastric epithelial cells to cause supression of apoptosis
S. Przemeck1, A. Varro2, D. M. Pritchard1.Division of 1Gastroenterology and 2Physiological Laboratory, University of Liverpool, UK
Introduction: The gastric antral hormone gastrin acts as a cofactor during gastric carcinogenesis and has been shown to regulate important cellular processes in the stomach including proliferation, migration, and differentiation. In addition, several previous studies have shown that gastrin inhibits apoptosis. The mechanisms responsible for the anti-apoptotic action of gastrin are currently not fully understood.
Methods: AGSGR cells, a human gastric carcinoma cell line stably transfected with the CCK-2 receptor were used. The expression of genes involved in the regulation of apoptosis was investigated by pathway specific cDNA microarray following treatment with 10 nM gastrin for six hours. Abundance and subcellular location of mcl-1 protein was subsequently assessed by Western blotting and immunofluorescence. Various inhibitors were used to investigate relevant downstream signalling pathways. The functional consequences of mcl-1 upon apoptosis were investigated using mcl-1 siRNA.
Results: Treatment of AGSGR cells with 10 nM gastrin for six hours resulted in increased expression of mcl-1 transcripts by cDNA microarray and increased protein abundance was confirmed by western blot analysis. Immunofluorescence showed increased cytoplasmic accumulation of mcl-1 following gastrin treatment. Increased mcl-1 abundance was inhibited by a transcription inhibitor actinomycinD and by a protein synthesis inhibitor cycloheximide. Downstream signalling occurred via the CCK-2 receptor, protein kinase C, and MAP kinase pathways, but not via PI3 kinase. Transfection with mcl-1 siRNA for 24 hours caused >90% suppression of mcl-1 protein abundance and resulted in a 2–3-fold increase in apoptotic cells six hours following addition of 10 nM gastrin.
Conclusions: Gastrin signals via the CCK-2 receptor, PKC, and MAP kinase to induce expression of the anti-apoptotic protein mcl-1. Mcl-1 prevents induction of apoptosis following addition of gastrin. This demonstrates a novel pathway by which gastrin suppresses gastric epithelial apoptosis.
097 THE MAGNITUDE OF VISCERO-VISCERAL AND VISCEROSOMATIC SENSITISATION INDUCED BY INTRADUODENAL CAPSAICIN INFUSION IS DOSE DEPENDENT
B. J. Unsworth, Q. Aziz, P. Holzer1, A. R. Hobson.Section of GI Sciences, University of Manchester, UK; 1Department of Pharmacology, Medical University of Graz, Austria
Background: Capsaicin activates TRPV-1 receptors on spinal and vagal afferents and its infusion into the jejunum evokes burning and cramping sensations, the intensity of which is dose dependent. In this study we wished to determine if capsaicin infusion into the proximal duodenum would result in increased excitability of spinal dorsal horn neurones and the development of sensitisation of convergent visceral and somatic structures.
Methods: We recruited 16 subjects (12 female). A catheter was positioned in the proximal duodenum with a second in the distal oesophagus. Pain thresholds (PT) to electrical stimulation (ES) were assessed in the oesophagus, area of somatic referral (AOR) on the abdominal wall and control region (Foot). Capsaicin was then infused into the duodenum (2 ml/min for 30 minutes). The concentrations of capsaicin used were 100 and 200 μg/ml with a saline control. Subjects were studied on four occasions (1×100 μg/ml, 2×200 μg/ml, 1×saline) in a randomised order and both operator and subject were blinded. PT in all regions were recorded at 15 and 45 minutes post infusion. Visual analogue scales (VAS) for pain, unpleasantness, nausea, and anxiety were recorded at five minute intervals during the infusion and a short McGill pain questionnaire was used.
Results: Significant and reproducible reductions in oesophageal PT were seen on both occasions at 200 μg/ml (−9.2 mA and −11 mA, p = 0.004) but this was not significant at 100 μg/ml (−6.3 mA, p = 0.06) or with saline (−0.7 mA, p = 0.77). Significant reductions in AOR PT were seen on both occasions at 200 μg/ml (−4.9 mA and −4 mA, p = 0.004) and 100 μg/ml (−2.7 mA, p = 0.001) but not with saline (0.7 mA±12, p = 0.77). No differences were seen in foot PT. VAS scores for pain were higher that for the other psychophysical measures and highest at the 200 μg/ml concentration. The most common verbal descriptors used to describe the capsaicin infusion were cramping, hot burning, and aching.
Conclusion: Capsaicin infusion into the proximal duodenum induces sensitisation in visceral and somatic regions known to have convergent afferent input at the spinal cord level. The magnitude of sensitisation increases with increasing concentrations of capsaicin as does the subjective awareness of the infusion. These data provide further evidence that central sensitisation plays an important role in the development of visceral hypersensitivity.
Inflammatory bowel disease section symposium
098 FULLY HUMAN ANTI-TNF ADALIMUMAB MAINTAINS REMISSION FOR ONE YEAR IN PATIENTS WITH ACTIVE CROHN’S DISEASE: A RANDOMISED, CONTROLLED COHORT
W. J. Sandborn1, M. Lukas2, P. Rutgeerts3, P. F. Pollack4, J. Kent5, (introduced by S. Ghosh)6.1Rochester, MN, US; 2Prague, Czech Republic; 3Leuven, Belgium; 4Abbott, Parsippany, NJ, US; 5Abbott, Abbott Park, IL, US; 6Imperial College, London, UK
Aim: To assess the efficacy and safety of adalimumab (ADA) in maintaining remission in patients with CD.
Methods: All patients completing CLASSIC I, a four week, randomised controlled trial of ADA in patients with moderately to severely active CD, were eligible to receive ADA 40 mg sc at weeks 0 and 2 of CLASSIC II. Patients in remission (CDAI<150) at weeks 0 and 4 of CLASSIC II were randomised to receive ADA 40 mg every other week (eow) or 40 mg/week, or placebo (PBO) for up to one year. Patients with CDAI ⩾150 entered an open label adalimumab cohort (results reported separately). CDAI and adverse events (AE) were assessed at each visit.
Results: Of 55 eligible patients randomised, 44 completed one year (33 randomised and 11 OL). ADA treated patients stayed in remission over time (table). Overall, AEs were mild to moderate in severity. Serious AEs occurred in two patients with PBO and one patient with ADA 40 mg eow therapy.
Abstract 89
Conclusions: In this exploratory cohort, remission was maintained in patients treated for up to one year with adalimumab. Adalimumab was well tolerated. A definitive study powered to assess long term adalimumab efficacy is ongoing.
099 MESALAZINE (5-ASA), BUT NOT HYDROCORTISONE, INHIBITS E coli induced IL-8 release from colonic epithelial cells at therapeutic concentrations
S. Subramanian, B. J. Campbell, H. M. Martin, C. A. Hart, L. G. Yu, J. M. Rhodes.Division of Gastroenterology, School of Clinical Sciences, University of Liverpool, Liverpool L69 3BX, UK
Background and Aims: Inflammatory bowel disease colonic mucosal E coli isolates release interleukin-8 (IL-8) from colonic epithelial cells (Gastroenterology 2004;127:80–93). We have now investigated the effect of 5-ASA and hydrocortisone on this IL-8 response.
Materials and Methods: Preliminary experiments showed that 0.2 μm filtered supernatant, pooled from six E coli mucosal isolates from 3 UC patients, induced a substantial IL-8 response from HT29 colon epithelial cells (pooled supernatant, 1262 (SD 110) pg/ml; pooled whole bacteria, IL-8 1901 (SD 67) pg/ml). HT29 cell monolayers were therefore pre-treated for one hour with 2.5–20 mM 5-ASA or 10–100 μM hydrocortisone followed by addition of the pooled supernatant. After four hour treatment, IL-8 release was measured by ELISA. In parallel experiments, IL-8 release was assessed in the presence and absence of BAY11-7082, an NFκB inhibitor.
Results: 5-ASA dose dependently inhibited the IL-8 response to a pooled E coli supernatant, with reductions of 22 (SD 15)% at 2.5 mM, 45 (SD 17)% (5 mM), 51 (SD 11)% (10 mM), and 97 (SD 1)% at 20 mM (all p<0.01; ANOVA). Hydrocortisone only caused significant inhibition of the IL-8 response (49 (SD 13)%, p = 0.01) at a supra-therapeutic concentration (100 μM). This is in keeping with the fact that inhibition of NFκB only had a modest effect on IL-8 release (mean reduction 39 (SD 35)%, n = 21). In a separate experiment, 5-ASA (5 mM) and hydrocortisone (100 μM) in combination inhibited IL-8 response by 82 (SD 7)%, compared with 38 (SD 8)% for 5-ASA alone and 51 (SD 6)% for hydrocortisone alone (p<0.001).
Conclusions: 5-ASA, at therapeutic concentrations, markedly inhibits the release of IL-8 by colon epithelial cells in response to mucosal E coli whereas hydrocortisone only has a significant inhibitory effect at concentrations almost 20-fold greater than are likely to be seen therapeutically. This confirms the epithelial cell as the target for mesalazine (JEM 2005 201:1205–15) but implies that other cell types probably represent therapeutic targets for corticosteroids in IBD.
Cell/molecular biology free papers
100 DEOXYCHOLIC ACID DAMAGES DNA THROUGH ITS PRODUCTION OF REACTIVE OXYGEN SPECIES: ANTIOXIDANTS PREVENT THIS DAMAGE
G. Jenkins, F. D’Souza, A. Alhamdani, P. Griffiths, J. Baxter.School of Medicine, Swansea University, Swansea SA2 8PP, UK
DNA damage induction is a key initiating mechanism in cancer development in most tissue types. Recent reports have shown that Barrett’s tissues carry higher levels of DNA damage than squamous tissue, suggesting that Barrett’s tissues are exposed to DNA damaging agents. Bile acids are implicated in oesophageal adenocarcinoma induction, although there is some contention as to whether they can cause DNA damage and it not known how they do so. Hence, we assessed whether a range of bile acids were capable of inducing DNA damage in cultured oesophageal cells. Using the cytokinesis blocked micronucleus assay, we showed that DCA was the only bile acid tested that damaged chromosomes. We further showed that this damage was induced at both neutral and acidic pH (pH6). DCA was also shown to induce point mutations in the human p53 gene, using the restriction site mutation assay. Hence DCA is a genotoxin, but how does it damage DNA?
As bile acids do not bind to DNA directly, we suspected that DCA’s ability to induce DNA damage involved the generation of reactive oxygen species. Indeed, using an ROS sensitive fluorescent dye (H2DCFDA), we were able to show the induction of reactive oxygen species (ROS) by DCA in oesophageal cells (OE33 and KYSE). In order to demonstrate that these ROS were responsible for DCA’s genotoxicity, we co-exposed cells to DCA and two antioxidants (vitamin C and curcumin). Both antioxidants prevented DCA from damaging DNA. These data correlate well with previous data from our lab, showing that DCA’s activation of NFKB is ROS dependent and can be blocked by the same antioxidants. Therefore, we can confirm that bile acids (DCA) can damage DNA (and activate NFKB) by inducing ROS. Hence antioxidant supplementation may be an effective chemopreventative strategy in Barrett’s patients. These observations are supported by epidemiological data showing that there is an inverse correlation between fruit and vegetable intake and cancer progression in Barrett’s patients.
101 MONOCLONAL CONVERSION OF HUMAN GASTRIC GLANDS PROVIDES INSIGHTS INTO STEM CELL AND CLONAL ARCHITECTURE
S. A. C. McDonald, L. G. Greaves1, S. J. Leedham, C. Yin-Lee, M. Deheragoda, D. Oukrif, M. R. Novelli, R. W. Taylor1, D. M. Turnbull1, J. A. Z. Jankowski, N. A. Wright.Histopathology Unit, Cancer Research UK, London, UK; 1Department of Neurobiology, University of Newcastle-upon-Tyne, UK
Studies on the intestine of animals and man have confirmed, beyond reasonable doubt, that the structural units, the crypts, are clonally derived. The unit found in the stomach, the gastric gland, especially in the human, remains an enigma. Some animal reports show clonal derivation, whereas others show that a minority of glands remain polyclonal, suggesting the possibility of multiple, possibly independent stem cells. In the human, results are also mixed.
We have used mutations in the mitochondrial cytochrome c oxidase subunit 1 gene (COXsu1), as a clonal marker (J Clin Invest 2003:112), detecting COXsu1 in conjunction with a nuclear encoded oxidative enzyme, succinate dehydrogenase (SDH), by double enzyme histochemistry. We have observed body-type gastric glands which are partially filled with mutated cells, and others glands where all the cells in the gland are mutated (COXsu1-, SDH+). These suggest that a stem cell bearing this mutation expands to fill the entire gastric gland. Early observations suggest that all cell lineages in these mutated body-type glands are involved in this process. Moreover, the mutated gland then appears to spread in the mucosa by gland fission.
Several conclusions are made possible by these observations:
1. Gastric glands undergo a process of monoclonal conversion, where the gland becomes gradually replaced by mutated cells
2. Human gastric glands are maintained by a number of stem cells
3. Each body-type gland is derived ultimately from a single stem cell which gives rise to all the contained lineages, and are therefore multi-potential
4. These mutated glands then appear to expand by gland fission, even in the adult stomach
102 USE OF GROWTH HORMONE RELEASING PEPTIDE-6 FOR THE PREVENTION OF HEPATIC AND MULTI ORGAN FAILURE
D. Cibrián1, H. Ajamieh1, J. Berlanga1, O. S. León1, J. S. Alba1, M. J. T. Kim2, T. Marchbank2, J. J. Boyle2, F. Freyre1, D. Garcia del Barco1, P. Lopez-Saura1, G. Guillen1, S. Ghosh2, R. A. Goodlad3, R. J. Playford2.1Center for Genetic Engineering and Biotechnology, PO Box 6162 and Center for Biological Studies, Food and Drug Institute, University of Havana; 2Imperial College, Hammersmith Hospital, London; 3CRUK, Lincolns Inn Fields, London
Background/Aims: Novel therapies for the treatment of multiple organ failure are required.
Methods: We examined the effect of synthetic growth hormone releasing peptide-6 (GHRP-6) on cell migration and proliferation using rat intestinal epithelial (IEC-6) and human colonic cancer (HT29) cells as in vitro models of injury. In addition, we examined its efficacy when given alone and in combination with the potent protective factor epidermal growth factor (EGF) in an in vivo model of multi-organ failure (using two hepatic vessel ischemia-reperfusion protocols; 45 min ischaemia-45 min reperfusion and 90 min ischaemia-120 min reperfusion).
Results: In vitro studies showed GHRP-6 directly influenced gut epithelial function as its addition caused a threefold increase in the rate of cell migration of IEC-6 and HT29 cells (p<0.01) but did not increase proliferation ([3H]-thymidine incorporation). In vivo studies showed that, compared to baseline values, ischaemia/reperfusion caused marked hepatic and intestinal damage (histological scoring), neutrophilic infiltration (MPO assay, fivefold increase), and lipid peroxidation (MDA assay, fourfold increase). Pretreatment with GHRP-6 (120 μg/kg sc) alone truncated these effects by 50–85% (all p<0.05) and additional benefit was seen when GHRP-6 was used in combination with EGF (1 mg/kg sc). Lung and renal injuries were also reduced by these pretreatments.
Conclusion: Administration of GHRP-6, given alone or in combination with EGF to enhance effects, may provide a novel, simple approach for the prevention and treatment of multi-organ failure and other injuries of the gastrointestinal tract. Further studies appear justified.
103 HYPERAMMONEMIA ALTERS THE LPS INDUCED ACTIVATION OF TNF-α IN PERIPHERAL BLOOD MONONUCLEAR CELLS
R. G. Mathew, D. L. Shawcross, N. A. Davies, S. J. Hodges, R. Jalan.Liver Failure Group, Institute of Hepatology, University College London, UK
Background: Patients with liver dysfunction are prone to infection which is frequently a precipitant of decompensation associated with hepatic encephalopathy, renal failure, and shock. Bacterial infections in patients with cirrhosis are poorly tolerated and responsible for 30–50% of deaths. We have shown that hyperammonemia impairs neutrophil phagocytosis and induces spontaneous oxidative burst but the effect on peripheral blood mononuclear cells (PBMCs) has not been studied. TNF-α plays a key role in the development of sepsis and an imbalance of TNF-α with its soluble receptors (sTNFR) is associated with a poor outcome.
Aims: To determine if ammonia affects PBMC cytokine activation in response to endotoxin.
Methods: PBMCs were isolated from healthy volunteers on a Ficoll-Paque gradient. Cells were incubated with 0–125 μM ammonium chloride (NH4Cl) immediately, or after 24 hours, when a 1 ng/ml lipopolysaccharide (LPS) challenge was administered. TNF-α, sTNFRI, and sTNFRII were measured from cell supernatants at 48 hours with ELISA. Live cell counts were obtained using the trypan blue exclusion assay.
Results: Significant TNF-α release occurred only in the presence of LPS stimulation. NH4Cl caused a concentration related decrease in TNF-α (20–48% reduction with 125 μM NH4Cl (p<0.05)). sTNFR was produced in the absence of LPS stimulation, however 125 μM NH4Cl potentiated the LPS induced rise of sTNFRI by 21.4% (p<0.00005) and of sTNFRII by 9.9% (p<0.005). A linear relationship was demonstrated between sTNFRI and sTNFRII in their regulation by LPS and NH4Cl. Neither LPS nor NH4Cl produced significant changes in live cell numbers.
Conclusion: Hyperammonaemia influences endotoxin induced release of TNF-α and soluble receptors. This may have implications for resisting infections in liver disease.
104 COLONIC STEM CELLS ARE UNABLE TO SELECTIVELY SEGREGATE GENOME AT THE TIME OF MITOSIS: REPLICATION ERRORS SURVIVE
S. L. Preston, N. Mandir, T. Hunt, R. A. Goodlad, S. J. Leedham, N. A. Wright, M. R. Alison.Cancer Research UK, 44 Lincoln’s Inn Fields, Holborn WC2A 3PX, UK
Background: There is evidence that one way in which small intestinal stem cells are able to protect themselves from errors of DNA replication is by segregating their genome at the time of cell division; always retaining the old (or “template”) strand and passing on only the newly synthesised DNA strand to their progeny (Potten et al. J Cell Sci 2002). Here, we try to establish whether or not the same process takes place in the colon at a time when new stem cells and new “template” strands are being produce following a single dose of ionising radiation.
Methods: Thirty Min and 20 C57Bl/6J mice underwent whole body irradiation at a dose of 8 Gy, followed by six hourly i.p. injections of tritiated thymidine (3HTdR) over 48 hours. The mice were then left for eight days and a cohort sacrificed. The remaining mice were injected with bromodeoxyuridine (BrdUrd) i.p. every six hours for 48 hours and sacrificed at time points from 40 minutes to 25 days following the final injection. The colons of all mice were removed post mortem and embedded in paraffin wax in a Swiss roll fashion. μm sections were cut and stained with the anti-BrdUrd antibody, before autoradiography was performed. Crypts were counted and labelled cells mapped on a positional basis.
Results: After eight days 1.9% of cells were labelled with 3HTtdR, with none seen after 20 days. Labelled cells were distributed equally throughout the length of the crypt and there fewer labelled cells in the Min mice. BrdUrd labelling was almost complete throughout the crypt at one day, but declined sharply 3–5 days after the last injection, with no labelled cells seen at 25 days. Cells containing both proliferative markers were very rare indeed and occurred only in the first 24 hours.
Conclusions: Since the stem cell cycle time is reduced by irradiation, the presence of 3HtdR labelling at eight days is indicative of retention of part of the genome. The disappearance of the label over the following 12 days and the dilution of BrdUrd at the same rate, suggests that this process is stochastic and there is no mechanism in the colon selectively retaining the “template” strand at the time of mitosis. This may contribute to the higher incidence of tumours found in the colon compared to the small intestine.
105 TARGETED KILLING OF COLORECTAL CELL LINES AND MURINE ADENOMAS USING A MONOCLONAL ANTIBODY AGAINST MEMBRANE BOUND CARCINOEMBRYONIC ANTIGEN
P. J. Conaghan1,2, J. L. Wilding1, M. G. Tytherleigh1,2, E. Tchilian1, N. J. Mc C Mortensen2, W. F. Bodmer1.1Cancer & Immunogenetics Laboratory, Weatherall Institute of Molecular Medicine; 2Department of Colorectal Surgery, John Radcliffe Hospital, Headington, Oxford OX3 9DS, UK
Introduction: The anti-CEA antibody PR1A3 binds only membrane-bound CEA. The distribution of carcinoma-embryonic antigen (CEA) in colorectal cancer (CRC) differs from that in normal colorectal tissue, being found throughout the cell membrane of the cells, thus enabling access to intravenous antibody. Our aim was to assess whether PR1A3 is suitable to be considered as a therapeutic agent in the treatment of CRC.
Methods: Humanised PR1A3 was assessed in in vitro cytotoxic assays with CEA positive and negative colorectal cell lines using peripheral blood mononuclear cells as a source of natural killer (NK) cells. In addition PR1A3 was injected intraperitoneally twice weekly for six weeks into a transgenic murine model of CRC which expresses human CEA on adenomatous polyps predominantly in the small bowel (MIN CEA mice).
Results: PR1A3 demonstrated antibody dependent and CEA dependent killing of tumour cell lines by human effector cells. The effect increased with increasing concentration of antibody and was lost by using antibody to block the Fc-γIIIA receptor which is found predominantly on NK cells. Tumour cell lysis increased by a mean of 25% (range 15–38%) compared to spontaneous killing in the absence of antibody. 46 transgenic MIN CEA mice treated with PR1A3 had a 24% reduction in average adenoma size (p = 0.0014) compared to 33 untreated controls.
Discussion: PR1A3 mediates NK killing of CEA-positive tumour cells in vitro and in vivo. This killing is dependent on effector cells binding the Fc-portion of the antibody and so is likely to act via antibody dependent cellular cytotoxicity and not by blocking cellular function. These findings suggest promising therapeutic potential in CRC.
Pathology free papers
106 EVOLUTION OF HELICOBACTER PYLORI VIRULENCE FACTORS IN INDIVIDUALS AND FAMILIES FROM AN ISOLATED AFRICAN POPULATION
J. L. Hale1, R. H. Argent1, K. Robinson1, S. van der Merwe2, J. C. Atherton1.1Wolfson Digestive Diseases Centre, and Institute of Infection, Immunity and Inflammation, University Hospital, Nottingham; 2Department of Internal Medicine and Gastroenterology, University of Pretoria, South Africa
Background:Helicobacter pylori are constantly evolving and are passed between individuals. We have previously studied virulence factor evolution in strains from Scottish families and more recently Nottingham individuals. We have now studied H pylori evolution in a rural Black, South African community (Ogies Tribe from Mpumulanga).
Methods: The study collection consists of 90 individuals. Initially 10 single colony isolates were taken from a single gastric biopsy specimen from each of nine individuals. Evolution in the H pylori virulence genes vacA, cagA, and iceA was determined by PCR typing and nucleotide sequencing and OipA protein status was determined by western blot analysis. Similarities between strains were determined by RAPD-PCR.
Results: RAPD-PCR revealed that each stomach had a single unique strain. However, their strains had evolved to change vacA (4/9) and oipA. We found multiple vacA alleles within the same stomach at a higher frequency then in a UK population (4/9 African strains compared to 2/49 Nottingham strains showed evolution within vacA, p<0.001 Fisher’s exact test). Variation in oipA functionality was investigated following a six hour co-culture with gastric epithelial (AGS) cells. OipA is believed to cause IL-8 secretion. However, in this case no difference was found between the levels of IL-8 secretion induced by oipA “on” and oipA “off” strains.
Conclusions: We have shown evolution of H pylori by recombination. Evolution occurs commonly within individual stomachs, particularly in Africa where infection is very common. This may be due to increased contact between strains. We speculate that this may allow H pylori to adapt rapidly to its environment. This may result in H pylori evolving to become more or less virulent and, if the latter, it may help explain the low incidence of H pylori associated disease in Africa (the African enigma).
107 HUMAN REGULATORY T CELL RESPONSES ARE ASSOCIATED WITH PROTECTION FROM HELICOBACTER PYLORI INDUCED PEPTIC ULCER DISEASE
R. Kenefeck, K. Robinson, J. C. Atherton.Wolfson Digestive Diseases Centre, Queen’s Medical Centre, University of Nottingham, Nottingham, UK
Introduction:Helicobacter pylori (Hp), the major cause of peptic ulcer disease, provokes a vigorous immune response. Despite this, however, most infections are persistent. We hypothesise that Hp subverts regulatory T cells (Tregs) to suppress protective immunity and gastric inflammation and promote co-existence. The aim of this study was to characterise the human Treg response to Hp.
Methods: Gastric antral biopsies were collected from 63 consenting patients attending the Queen’s Medical Centre, Nottingham for an upper GI tract endoscopy. Flow cytometry was used to quantify Tregs by staining for the markers CD4 and CD25 and also interleukin-10 (IL-10). Expression of the natural Treg-specific gene FOXP3 was quantified by real-time PCR.
Results: Elevated frequencies of CD4+CD25hi regulatory T cells were detected in the gastric mucosa of Hp infected compared with uninfected donors (p = 0.04). A 12-fold higher frequency of CD4+CD25hiIL-10+ cells was found amongst gastric cells from infected compared to uninfected donors (p = 0.002). Up to 95% of the gastric CD4+CD25hi cells from infected donors were IL-10+ (median 61.3%; IQR 32.2–83.3%), and the proportion of IL10+ Tregs was 18-fold greater than that obtained with cells from uninfected donors (median 3.5%; IQR 0.0–24.3%; p = 0.002), suggesting that suppression of the normal T-cell response may be IL-10-mediated.
Real-time PCR revealed a sevenfold increase in FOXP3 expression in gastric tissues from infected compared to uninfected donors (p = 0.003), indicating the presence of natural Tregs during infection. To address the hypothesis that Treg responses influence the inflammatory response to infection, the frequency of CD4+CD25hiIL-10+ cells in the gastric mucosa of Hp positive patients diagnosed with or without peptic ulcer disease was compared. Significantly elevated frequencies of Tregs were found in the tissues of nine patients without peptic ulcer disease (median 2263; IQR 1766–3636) compared to 12 patients with disease (median 946; IQR 524–2365; p = 0.05).
Conclusion: We show that IL-10 secreting natural Tregs are present in the gastric mucosa of Hp infected patients and are inversely associated with disease severity. We propose that Tregs not only impede the ability of the immune system to clear infection, but also modulate inflammation and protect against peptic ulcer disease.
108 THE STOMACH PERI-GLANDULAR FIBROBLAST SHEATH EXPANDS IN INFLAMED TISSUE BEFORE DEVELOPMENT OF INTESTINAL METAPLASIA
S. J. Leedham, M. G. Deheragoda, M. Brittan, N. C. Direkze, S. L. Preston, S. A. C. McDonald, N. A. Wright.Cancer Research UK, 44 Lincoln’s Inn Fields, London WC2A 3PX, UK
Background: The stomach periglandular fibroblast sheath forms a protective fenestrated sheath around the stem cell niche at the isthmus/neck of the gastric gland and are important coordinating cells that possess significant influence on their environment by virtue of their receptor profile and the signals they produce. A recent publication by Mutoh et al (2005) used alpha smooth muscle actin (α-SMA) staining, and failed to show any peri-glandular fibroblasts surrounding en face glands of normal mouse and human stomach. In intestinal metaplastic tissue however the peri-glandular sheath was obvious and the authors concluded that the fibroblast sheath was only generated in metaplastic tissue possibly through Cdx 2 expression.
Aim: To demonstrate the presence of the peri-glandular fibroblast sheath in normal as well as metaplastic tissue and to determine at what point in the gastritis-metaplasia pathway the fibroblast sheath expands.
Methods: Mouse and human gastric tissue was classified histologically into normal, inflamed, atrophic, and metaplastic tissue. Alpha-SMA and vimentin staining was used to stain myofibroblasts and these were counted on a per en face crypt basis. H pylori status was determined using immunohistochemical methods.
Results: α-SMA and vimentin positive cells were clearly and consistently seen surrounding normal mouse and human gastric glands in both the en face and cross sectional plane. A significant expansion in the peri-glandular fibroblast sheath appeared to occur in inflamed tissue, and was present throughout the next stages of the gastritis-metaplasia sequence.
Conclusions: The peri-glandular fibroblast sheath is present in normal stomach tissue and performs a vital homeostatic role in regulating epithelial cell behaviour. The expansion of the myofibroblast sheath is more likely to result from recruitment of circulating bone marrow derived precursor cells than from generation by metaplastic mucosa via a Cdx 2 pathway.
1
109 ROUTINE ELASTIC STAINING ASSISTS DETECTION OF VASCULAR INVASION IN COLORECTAL CANCER
M. Abdulkader, K. Abdulla, E. Rakha, P. V. Kaye.Queens Medical Centre, Nottingham, UK
Aim: Vascular invasion (VI) is an independent prognostic factor in colorectal cancer (CRC). Some studies have recommended elastic stains to facilitate the recognition of VI, however, the usefulness of routine staining in CRC is not clear and this is not widely performed. The aim of this study was to determine the value of routine elastic staining of CRC specimens.
Methods: 498 cases of CRC were included in this study (65, 215, and 218 Dukes’ A, B, and C). In 208 cases, VI was assessed using elastic stains that were introduced as a routine staining in CRC. As a control, 290 cases in which VI was assessed solely on H&E staining were included.
Results: Vascular invasion (VI) was detected in 198 cases (40% of the whole series); 11 (16.9%), 62 (28.8%), and 125 (57.8%) in Dukes A, B, and C respectively There was a statistically significant increased detection of VI in the elastic stained group; 46.2% in the test group compared to 35.5% in the control group (p<0.05). Particular increase was noted in Dukes’ stage A and B and in rectal tumours (p<0.05).
Conclusion: Elastic stains are useful and practical in evaluation of VI status in CRC, and we recommend implementing these stains in routine pathological practice.
Trainee/Trainers computer workshop
110 BEWARE OF THE DIAGNOSTIC IMITATION IN DYSPHAGIA!
N. V. Radhakrishnan, P. Ellul, P. Winarso, J. Barlow1, K. Akhtar, B. J. Sebastian, R. George.Rochdale Infirmary, The Pennine Acute Hospitals NHS Trust, Whitehall Street, Rochdale OL12 0NB, UK; 1Hope Hospital, University of Manchester, Salford M6 8HD, UK
Case report: A 39 year old school teacher was referred by her GP for open access gastroscopy with six weeks’ history of mid-retrosternal dysphagia to solids. There was no history of chest pain, vomiting or weight loss, arthralgia, or Raynaud’s phenomenon. Gastroscopy showed a benign looking 3 cm stricture near OG junction through which only a paediatric scope could be passed. Biopsies showed chronic active carditis. Patient was commenced on empirical PPI therapy and at repeat gastroscopy the stricture was dilated up to 20 mm with Microvasive balloon with no improvement in symptom. Repeat biopsies showed no dysplasia/malignancy. Barium swallow study and oesophageal manometry were carried out. Oesophageal manometry showed changes consistent with diagnosis of achalasia. Further history revealed lumpectomy and axillary node clearance for ductal carcinoma in 1996 for which she received chemotherapy and was commenced on Tamoxifen. In 1997 she developed contralateral carcinoma which led to left mastectomy. She was regularly followed up in the breast clinic with no evidence of recurrent disease and remained in good health until she developed dysphagia which led to her referral for gastroscopy. Routine blood tests revealed abnormal liver function tests. Ultrasound scan of the liver showed multiple hypoechoic lesions consistent with metastases. A CT scan showed circumferential thickening of the lower oesophagus, metastases in the liver, lungs, vertebral body. Antineuronal nuclear antibody type 1 was negative. In the light of ultrasound and CT findings and the previous history of breast carcinoma a diagnosis of pseudoachalasia was made and she was referred to the oncologist for chemotherapy. A percutaneous gastrostomy tube was placed to provide her nutrition. Learning points: (1) Both achalasia and pseudoachalasia can produce identical manometric appearances. (2) In dysphagic patients with manometric features of achalasia consider pseudoachalasia if the patient had a history of carcinoma, short duration of symptoms, and difficulty/inability in passing the endoscope through the OG junction.
111 AN UNUSUAL ENDOSCOPIC DUODENAL APPEARANCE
R. P. Willert1, S. M. Weerasinghe2, D. A. F. Lynch1.1Gastroenterology and 2Histopathology Departments Blackburn Royal Infirmary, Bolton Road, Blackburn BB2 3LR, UK
Case report: A 59 year old female non-smoker initially presented in 2000 with progressive weight loss of 8 kg (BMI 22) and painless, watery diarrhoea. There was no history of foreign travel. Stool cultures were negative for cysts, ova, and parasites. Her full blood count, U&Es, LFTs, glucose, inflammatory markers, haematinics, and thyroid function were all normal and her anti-endomysial antibodies were negative. A CXR suggested evidence of basal bronchiectasis. She underwent a gastroscopy with duodenal biopsies, received a specific therapy, and was lost to follow up.
Five years later she represented with further progressive weight loss of 15 kg (BMI 17) but with no change in bowel habit, pain, or systemic symptoms. Examination was unremarkable apart from vitiligo and coarse basal crackles in keeping with her bronchiectasis.
Repeat bloods and stool cultures were again all normal and her anti-endomysial antibodies remained negative. An ultrasound scan demonstrated mild splenomegaly but her pancreas, biliary tree, and liver were normal. A repeat gastroscopy was performed which demonstrated an unusual appearance in the duodenum and further duodenal biopsies were taken.
This case discusses the differential cause for the abnormal duodenal findings and the appropriate investigations and treatment required in this uncommon condition.
112 AN UNUSUAL CAUSE OF FACIAL SWELLING IN A JAUNDICED PATIENT
J. Gasem, S. Khalid, M. Babores.Macclesfield General District Hospital, Macclesfield, UK
Case report: A 63 year old gentleman was admitted to hospital complaining of feeling unwell for six months, with jaundice, weight loss of 1½ stones in two years, poor appetite, leg ulcers for one month, and loose stools for 11 years. He had no significant medical history prior to admission and had no risk factors for liver disease. On examination he had jaundice, finger clubbing, and an ulcerating skin rash on his legs. Abdominal examination was unremarkable. His blood results confirmed microcytic anaemia with cholestasis and a bilirubin of 139 μmol/l (2–22). His CRP was raised at CRP 93 mg/l (0–8), and his albumin was reduced at Albumin of 16 g/l (30–50). His chest x ray was normal. CT scan of the liver failed to reveal biliary obstruction. Colonoscopy and biopsy confirmed ulcerative colitis with a moderately well differentiated rectal adenocarcinoma. He was treated with high dose steroids and azathioprine. After a brief discharge from hospital, the patient was readmitted with breathlessness, a productive cough, and facial swelling. He was found to be hypoxic with a PO2 of 7.2 on 80% O2. CXR showed surgical emphysema and evidence of bronchopneumonia with faint ground-glass shadowing. A bronchoscopy was performed and showed non-specific findings of inflammation. Despite appropriate antibiotics and supportive therapy, the patient died a few days later.
Discussion: In this case, ulcerative colitis was complicated by a skin rash, primary sclerosing cholangitis, and rectal adenocarcinoma. Opportunistic infection complicating steroid therapy alone or in combination with immunosuppressive therapy for inflammatory bowl disease is rare. However, this complication should be considered in the differential diagnosis in such patients. Prophylactic therapy against opportunistic infection has been advocated by some authors in patients receiving prolonged steroid therapy as a treatment for inflammatory bowel disease. This case shows the complexity of inflammatory bowel disease complications and the potential side effects of its treatment.
113 A RASH CAN CAUSE GI BLEEDING?
J. Parr, D. A. Burke, C. E. Macdonald.Cumberland Infirmary, Carlisle CA2 7HY, UK
Case report: A 19 year old man presented after two days of dyspepsia and witnessed haematemesis. He had a history of ulcerative colitis (UC), well controlled on oral Asacol. He had been taking a tetracycline for acne. He was otherwise well. O/E he had tachycardia, postural drop in BP, and mild epigastric tenderness. No rash, fever, or other significant findings were noted. Admission biochemistry + CXR were normal. Hb was normal but the WCC = 21.4×109/l and CRP = 143 mg/l. Urinalysis was negative. An OGD was carried out. Thickened cobblestone like mucosa, superficial ulceration, and oozing of blood was noted to extend from the OG junction along the lesser curve. Biopsies (Bx) were taken and he was started on IV PPI. CLO test was negative. Oxytetracycline was stopped. The Bx showed haemorrhagic acute gastritis with ulceration. Also present was vasculitis with fibrinoid change and leukocytoclasis at the small vessels. No granulomata were seen. Special stains for bacteria and fungi were negative. Autoantibodies and viral hepatitis screen was requested. This showed normal complement levels, ANA, immunoglobulins, and hepatitis serology. There was cANCA 1/160 present, with a positive antiproteinase 3 antibody. Rpt OGD at day 10 showed dramatic change with only minor generalised patchy erythema noted. Chronic active inflammation was noted in the gastric Bx mainly around the vessels and was still suspicious for vasculitis. H pylori not seen. Given the persistently raised cANCA, tetracycline use, and vasculitis on Bx, he was diagnosed with microscopic polyangiitis (MPA) of the stomach.
Discussion: MPA is identical to polyarteritis nodosa (PAN) except for the presence of vasculitis in vessels smaller than arteries. Presentation is similar in both, though GI tract involvement is more common in PAN. The lesions in MPA are thought to represent a hypersensitivity reaction and can involve skin, GI tract, and other organs. Autoimmune phenomena (incl MPA) are well recognised with tetracycline use. MPA affecting the skin has been associated with ulcerative colitis. Most cases of MPA require no treatment. UC patients have pANCA positivity in 60–80%. cANCA is uncommon in UC but positive in 25% of MPA.
Conclusion: Vasculitis can affect any organ of the body, and although rare, GI involvement should be considered.
114 A FATAL PULMONARY EMBOLISM SECONDARY TO A RARE SMALL BOWEL INFECTION
A. H. Shenoy, N. A. Shepherd, J. L. Brown.Gloucestershire Royal Hospital, Gloucester GL1 3NN, UK
Case report: A 76 year old man presented with diarrhoea, borborhygmi, and weight loss of a month’s duration. There was no rectal bleeding or abdominal pain. His symptoms started on return from a holiday in Portugal. His stool culture and microscopy were negative and he did not respond to oral tinidazole for suspected giardiasis. He had been on long term low dose prednisolone and methotrexate orally for rheumatoid arthritis, which had been quiescent for a long time. He had suffered a single episode of deep vein thrombosis many years ago. There was no other comorbidity or any symptoms of gastrointestinal disease in the past.
At presentation he was anaemic with haemoglobin of 9.1 g/dl due to iron and folate deficiency. C reactive protein (CRP) was 38 mg/l (normal <10 mg/l) and albumin was 26 g/dl (35–44). A repeat stool test and other blood tests including vitamin B12 levels, thyroid function tests, glucose, anti-endomysial antibody were normal. Flexible sigmoidoscopy and colonic histology were normal. Gastroscopy showed a granular and finely nodular appearance of duodenum. Duodenal histology showed subtotal villous atrophy, dilated lymphatics, and abundant PAS positive inclusion filled macrophages infiltrating the submucosa, which are diagnostic of the chronic small bowel infectious disease this patient was suffering from.
Soon after the diagnosis, before any treatment could be initiated, the patient suddenly took ill with pleuritic chest pain and severe shortness of breath. The electrocardiogram and echocardiogram showed severe right heart strain suggesting massive pulmonary embolism (PE) from which he died. The risk factors for the PE were likely to be the previous DVT and possibly the underlying small bowel disease.
115 A BLEEDING CATCH-22
G. Pritchard1, E. Roche2, P. Foster2.1Royal Liverpool University Hospital, UK; 2Macclesfield District General Hospital, UK
Case report: We report a 56 year old patient who sustained recurrent bleeding from oesophagogastric varices over a four year period while on lifelong warfarin for a previous mesenteric vein thrombosis and femoral deep vein thrombosis. CT scanning demonstrated extensive thrombosis involving the portal, splenic, and superior mesenteric veins. We trace his course through episodes of bleeding in which the combination of his underlying condition, need for oral anticoagulation, and the therapeutic procedures used to treat varices resulted in significant and challenging complications.
Discussion: We discuss the management of extra-hepatic portal vein thrombosis in light of the current literature, with a particular focus on aetiology, anticoagulation in the setting of varices, techniques to prevent rebleeding, and the implications of the presented complications.
116 AN UNUSUAL CAUSE OF UPPER GI BLEED
J. Mannath, I. S. Shaw1.New Cross Hospital, Wolverhampton WV10 0QP; 1Gloucestershire Royal Hospital, Gloucester, UK
Case report: A 45 year old gentleman presented with a history of haemetemesis, melaena, and recurrent abdominal pain. He gave a history of consuming 84 units of alcohol a week and had a past history of abdominal pain and anaemia. Investigation for the anaemia and pain had been undertaken previously and both an upper and lower GI endoscopy had been normal.
Clinical examination at the time of his latest admission was unremarkable apart from tenderness in epigastrium. He required regular oral morphine to control his pain.
On admission his amylase was 341 μ/ml with an albumin of 28 g/l and normal U&Es and LFTs. His haemoglobin dropped from 11.9 g/dl to 7.3 g/dl during admission. A repeat OGD showed mild duodenitis, and colonoscopy showed diverticular disease. Ultrasound examination of his abdomen showed a dilated common bile duct at 8 mm and an echo poor mass in the pancreatic head. The gall bladder was normal. His CA 19–9 was 80. A contrast enhanced CT scan of the abdomen was performed which showed a bulky pancreatic head and a well circumscribed intensely enhancing lesion in it. This was suggestive of a splenic artery pseudoaneurysm secondary to chronic pancreatits.
He underwent mesenteric angiogram a few days later which failed to show the aneurysm. A repeat CT scan confirmed that the aneurysm is thrombosed. To date he did not have a further episode of GI bleed. In this case the aneurysm thrombosed spontaneously and this may have had a therapeutic effect preventing further admissions with haemorrhage.
Haemobilia is an uncommon cause of GI bleeding which is often overlooked. Pseudoaneurysms of branches of coeliac axis are rare causes of haemobilia. Aneurysms arising from hepatic artery, gastro duodenal artery, splenic artery, cystic artery, and left gastric artery have been reported.
117 RAISED SERUM HCG: AN ACUTE SURGICAL PROBLEM
B. J. Sebastian, N. L. P. Barnes, D. Mittappali, M. Hussain, S. Aly, N. V. Radhakrishnan, P. Winarso, R. George, P. S. P. Senapati.Department of Gastrointestinal surgery, Medical Gastroenterology and Radiology, Rochdale Infirmary, Pennine Acute Hospitals NHS Trust, Whitehall Street, Rochdale, OL11 0NB, UK
Case report: A 47 year old lady was admitted as an emergency with abdominal pain and vomiting. Investigations revealed a raised serum hCG and evidence of renal failure. Pregnancy was excluded by ultrasound scanning. Subsequently a mass lesion in the apex of left lung was demonstrated on the chest x ray, and a contrast follow through revealed a jejunal intussusception, both of which were confirmed by CT scanning. The patient underwent a laparotomy, where a polypoidal mass was found in the jejunum causing the intussusception. The involved segment of bowel was resected. Histology revealed an anaplastic sarcomatoid carcinoma with positive cytokeratin, EMA, and TTF-1 stains, which was suggestive of metastasis from carcinoma of the lung. A PET scan failed to show any additional site of activity other than the lung lesion. A left upper lobectomy was performed, showing concordant histology with the previously excised jejunal mass. The patient is currently under follow up and is clinically asymptomatic at six months. The serum hCG level has now returned to normal.
118 A FLUKE DIAGNOSIS?
A. J. Lawson1, A. Zaitoun2, G. P. Aithal1.1Wolfson Digestive Disease Centre, University Hospital, Nottingham, UK; 2Department of Histopathology, University Hospital, Nottingham, UK
Case report: A 33 year old man was admitted with a four week history of diarrhoea and abdominal pain. He described 3–4 loose motions per 24 hours, associated with occasional blood per rectum. He was originally from Zimbabwe but had been living in the UK for 18 months. On examination he had a temperature of 38.1°C and he was mildly tender in the right iliac fossa. His haemoglobin was 10.6 g/dl (13–18), platelets 442×109 (140–400), and ESR 133 mm/hr. There had been no positive culture from two stool samples sent by his general practitioner. Flexible sigmoidoscopy was performed to the transverse colon with the finding of several small ulcers in both the sigmoid and distal transverse colon with normal intervening mucosa. The histological appearances of specimens from the colon threw up a surprising finding.
119 AN UNUSUAL CAUSE OF CONSTIPATION
K. P. Basavaraju, M. S. Musa, A. Pickersgill, K. G. Morgan, N. K. Ahluwalia.Stepping Hill Hospital, Stockport, UK
Case report: A 31 year old female was referred to the clinic with a long history of constipation that had become progressively worse over the last two years. She opened her bowels on average once every 2–3 weeks alternating with watery diarrhoea for 2–3 days. She complained of lower abdominal cramping pain worse after eating and severe rectal pain on defecation. She occasionally noticed bright red blood per rectum with associated mucus. Her constipation failed to improve with the use of various laxatives and suppositories. She was single with no children. Her general physical examination was normal. Her blood results including FBC, U&E, LFT, glucose, CRP, and TFT were all normal.
Her colonic transit study was compatible with slow transit constipation. Ano-rectal manometry showed a significant anomaly with a rise in anal canal pressure of up to 204 mmHg upon deflation of the rectal balloon, which was not initiated by the patient, suggestive of extremely obstructed defecation. A flexible sigmoidoscopy showed a large mucosal bulge at recto-sigmoid area suggestive of either submucosal or extrinsic lesion. The transvaginal ultrasound and MRI scan of the pelvis were unremarkable. The laparoscopy showed superficial thickened lesions below both ovaries, thickened areas at the top of both uterosacral ligaments, and a partly occluded pouch of Douglas. There was a large nodule at about 15 cm from the anus involving 8 cm of anterior sigmoid wall, corresponding to the image seen at flexible sigmoidoscopy. The histological assessment of the lesions seen during laparoscopy confirmed the diagnosis of colonic and pelvic endometriosis.
Not surprisingly, her symptoms failed to respond to hormonal therapy. Hence, she underwent laparoscopic excision of her endometriosis and resection of the anterior wall of the sigmoid colon. Following the surgery, patient has been completely asymptomatic and opens her bowels regularly. Endometriosis should be considered in the differential diagnoses of young females with chronic constipation.
120 AN INTERESTING CASE OF JAUNDICE WITH MULTISYSTEM INVOLVEMENT
K. K. Peddi1, D. O’Riordan2.1Hope Hospital, Salford Royal NHS Trust, Stott Lane, Salford M6 8HD; 2Colchester General Hospital, Turner Road, Colchester, Essex CO4 5JL, UK
Case report: We present an interesting and rare case of jaundice with multisystem involvement. A 43 year old fit and healthy man presented with one week history of jaundice. There was a suggestion of excess alcohol intake but no other risk factors for developing chronic liver disease. He was unwell with jaundice and mild confusion. Clinical examination did not show any evidence of chronic liver disease. His blood tests revealed hyperbilirubinemia, thrombocytopenia, acute renal failure, and elevated creatine kinase. He then went on to develop respiratory failure with an interesting chest x ray and required invasive ventilation. His blood film showed interesting features. His renal failure improved with haemofiltration and required very aggressive ITU support. The initial picture raised the possibility of acute liver failure secondary to excess alcohol consumption but subsequent investigations confirmed it to be a rare form of infectious hepatitis. Eventually he made excellent recovery despite presence of multisystem failure and poor prognostic factors.
121 A BELLY FULL OF BEAUJOLAIS: AN UNUSUAL CASE OF ASCITES
A. D. Farmer, D. Redford, J. R. Butterworth.Departments of Gastroenterology and Gynaecology, Princess Royal Hospital, Telford & Shrewsbury NHS Trust, Apley Castle, Telford, Shropshire TF1 6TF, UK
Case report: We describe the case of a 44 year old lady who presented to the gastroenterological service with progressive painless ascites in the absence of other symptoms. Initial evaluation failed to reveal an underlying cause of her ascites. Subsequent diagnostic paracentesis showed the presence of an exudative haemorrhagic ascites.
Further tests were inconclusive apart from a moderately elevated CA-125. Computed tomographical scanning suggested a prominence of both ovaries. We proceeded to diagnostic laparotomy which demonstrated the presence of multiple dark chocolate coloured deposits throughout the abdominal cavity, but most prominently on the small bowel. Histological examination of these lesions confirmed the presence of ectopic endometrial tissue.
Endometriosis is a rare cause of haemorrhagic ascites, with only 41 cases having been described in the world literature since 1951.
122 SKIN BLISTERS AND LIVER
Y. Reddy, D. Das.Stepping Hill Hospital, Stockport, UK
Case report: A 63 year old female was referred to a dermatologist with blistering, non-pruritic lesions on the dorsum of both hands, and excoriations on her face which did not improve with one week of oral corticosteroids. Apart from lansoprazole she was not on any medications. She was a non-smoker but drank 20 units of alcohol a week on average. Her body mass index was 33 and there were no signs of chronic liver disease.
Liver function tests showed Bilirakis 15 μmol/l, AST 155 IU/l, ALT 199 IU/l, GGT 599 IU/l, Alk Phos 114 IU/l. She tested negative to presence of viral B&C markers and auto-antibodies. Ultrasound scan revealed a heterogenous architecture of the liver. Her fasting serum ferritin was elevated at 971 μmol/l and transferring iron saturation was 50%.
Genetic screening for haemochromatosis showed a heterozygous status for H63D mutation. Liver biopsy appearances were in keeping with steato-hepatitis and grade 1 siderosis. No porphyrin crystals were identified in the unstained section of liver.
High levels of prophyrins were detected both in plasma and urine. A diagnosis of porphyria cutanea tarda (PCT) was made on the basis of a positive fluorescence emission at 620 nm for the plasma and excretion of uroporphyrin/creatinine at a level of 626.9 (<4.4 μmol/mol) in the urine. Red blood cell protoporphyrin was not elevated.
She was commenced on regular venesections. After nine sessions of venesection the skin lesions began to disappear, her LFTs returned to normal, serum ferritin came down to 7, and the uroporphyrin/creatinine levels fell to 53.4 μmol/mol .
PCT should always be considered in any patient with blistering skin lesions in the background of high alcohol intake and abnormal LFTs and venesection is effective in preventing relapses and reducing tisuue damage.
123 CAPSULE ENDOSCOPY: FRIEND OR FOE?
E. Wood, S. McCartney, S. Bloom.Department of Gastroenterology, Middlesex Hospital, UCLH NHS Trust, Mortimer Street, London W1T 3AA, UK
Introduction: We describe the case of an 81 year old man with known ischaemic and valvular heart disease (aortic stenosis (AS) with a gradient of 52 mmHg) and non-insulin dependent diabetes mellitus who had been previously investigated for an episodic transfusion requiring anaemia. He was also known to have a chronically infected hip prosthesis. OGD and colonoscopy at that time were unremarkable and subsequent bone marrow sampling to exclude myelodysplasia revealed low iron stores. He presented to the orthopaedic team with a normocytic anaemia (haemoglobin 6.6 g/dl) and low serum iron levels.
Investigations: A repeat OGD revealed minimal oesophagitis and colonoscopy was normal. A Meckel’s scan was unremarkable. Over the next 10 weeks the patient was transfusion dependent requiring a total of 28 units of blood. A limited enteroscopy was performed using a paediatric colonoscope. Multiple angiodysplastic lesions were seen in the duodenum and proximal jejunum which were coagulated with the heater probe. Unfortunately he continued to require blood transfusions and so went on to have a capsule endoscopy with the aim of assessing the extent of the angiodysplasia. Only two non-bleeding angiodysplastic lesions within the duodenum were identified. In light of this he had a mesenteric angiogram which revealed multiple small bowel arteriovenous malformations without a clear bleeding point. None was felt to be large enough to warrant embolisation or focal enough to be felt suitable for segmental resection. Both the enteroscopy and angiogram findings would suggest that the capsule endoscopy in this case failed to detect the extent of the underlying pathology. The patient has since had two further enteroscopies with Nd:YAG laser treatment and has required only two admissions for transfusion in the last two months.
Discussion: This centres on the cause and investigation of obscure GI bleeding, the mechanism of bleeding in Heyde’s syndrome (angiodysplastic bleeding in association with AS), endoscopic treatment of angiodysplasia, and the potential benefits and pitfalls of capsule endoscopy.
124 AN UNUSUAL PRESENTATION OF CHRONIC DIARRHOEA
A. Dias, G. Eryian, I. Cropley, O. Epstein.Royal Free Hospital, Pond Street, London NW3 2QG, UK
Case report: A 76 year old lady underwent surgery for intraductal breast carcinoma which was followed by three courses of radiotherapy. Two months after starting her radiotherapy she developed severe watery diarrhoea opening her bowels 8–10 times per day. There was no family history of bowel disease and she had not been abroad recently. After two weeks of persistent diarrhoea she was admitted to hospital. On examination she was noted to have perioral aphthous ulceration, a temperature of 38.5°C, and bilateral leg oedema. Her CRP was raised. Blood and urine cultures were negative. Stool samples were sent for Clostridium difficile toxin, ova, cysts and parasites, and electron microscopy and were all negative. Early morning urine for TB was negative. CT abdomen showed some thickening of ascending colon. A limited unprepared colonoscopy was performed and the scope was passed to the distal ascending colon. Colonic biopsy histology revealed non-specific chronic inflammation. Her pyrexia and diarrhoea continued which necessitated further investigation to exclude an unusual infective cause.
In this case we discuss how we investigated this patient and how appropriate treatment controlled her colitis.
Plenary posters
125 ROLE OF PROTEIN KINASE C IN ALDOSTERONE INDUCED NON-GENOMIC INHIBITION OF BASOLATERAL POTASSIUM CHANNELS IN HUMAN COLONIC CRYPTS
J. E. Linley1, K. A. Bowley2, G. G. Robins2, M. Hunter1, G. I. Sandle2.1Institute of Membrane & Systems Biology, University of Leeds, Leeds LS2 9JT; 2Institute of Molecular Medicine, St James’s University Hospital, Leeds LS9 7TF
Background: Aldosterone has a rapid, non-genomic, inhibitory effect on Ca2+-sensitive basolateral intermediate conductance K+ (IKCa) channels in human colonic crypt cells, which reduces the colon’s Cl- secretory capacity. However, the intracellular second messenger pathways involved in this effect are unclear.
Aim: To evaluate the role of protein kinase C (PKC) in aldosterone’s non-genomic inhibitory effect on basolateral IKCa channels in human colonic crypt cells, using the patch-clamp technique.
Methods: With informed consent, biopsies were obtained from healthy sigmoid colon during colonoscopy, and intact colonic crypts isolated by Ca2+ chelation. In cell attached patches (n = 6), IKCa channel activity decreased to 38 (SD 8)% (p<0.001) of the basal value 10 minutes after adding 1 nM aldosterone. This effect was inhibited by pre-treatment with 1 μM chelerythrine chloride, a PKC inhibitor (n = 6). In further experiments using cell attached patches, (n = 6), IKCa channel activity decreased to 60 (SD 9)% (p<0.02) of the basal value 10 minutes after adding 500 nM 4β-phorbol 12-myristate 13-acetate PMA), an activator of PKC. Using excised inside-out patches (n = 8), adding PMA to the bath solution rapidly produced a similar degree of IKCa channel inhibition, indicating a direct regulatory link between IKCa channel protein and membrane bound PKC.
Conclusions: Taken together, these results indicate that the activation of PKC has an important role in aldosterone’s non-genomic inhibitory effect on basolateral IKCa channels in human colonic crypt cells. PKC mediated phosphorylation of basolateral IKCa channels in human intestine may provide a novel approach to the treatment of secretory diarrhoea.
126 EGFR INHIBITION IMPROVES HELICOBACTER PYLORI INDUCED PATHOLOGY AND EPITHELIAL CELLULAR KINETICS IN VIVO
A. H. T. Jeremy, K. Danjo, M. F. Dixon1, P. A. Robinson, J. E. Crabtree.Molecular Medicine Unit, St James’s University Hospital, Leeds, UK; 1Department of Pathology, The General Infirmary, Leeds, UK
Introduction:H pylori has been shown to transactivate the EGF receptor (EGFR) in gastric epithelial cells. H pylori activation of the EGFR signalling pathway may be relevant to the epithelial hyperproliferation and increased risk of gastric carcinogenesis associated with infection. The aim of this study was to examine whether inhibition of the EGFR with the specific inhibitor EKB-569 would alter H pylori induced pathology in the Mongolian gerbil model.
Methods: Male Mongolian gerbils were infected with H. pylori (SS1 strain). Six weeks post-infection, infected and uninfected controls were fed on either, control, or EKB-569 (∼10 mg/g gerbil/day) supplemented diet. Gerbils were killed at 38 weeks post-infection. Gastric pathology was assessed and epithelial proliferation and apoptosis quantified respectively by anti-BrdU and activated caspase-3 histochemistry.
Results: No difference in antral pathology was observed in treated and untreated infected gerbils. EKB-569 treatment in infected gerbils resulted in a significant reduction in corpus atrophy (p<0.03) and mucous metaplasia (p<0.05), but chronic corpus inflammation was similar to untreated gerbils. There was significant (p<0.05) reduction in submucosal herniations in EKB-569 treated gerbils. Increased epithelial proliferation (p<0.001) was observed in the antrum and corpus of both infected groups. Apoptosis was only significantly increased (p<0.001) in the EKB treated group compared to uninfected control groups. There was a marked increase in apoptotic subepithelial mononuclear cells in the EKB-569 treated infected gerbils. In infected gerbils, the proliferation/apoptosis ratio in the untreated group was significantly greater (p<0.02) in both the antrum and corpus than in the EKB-569 treated group, where the ratio was comparable to uninfected controls.
Conclusion: EGFR inhibition reduces H pylori induced corpus pathology in vivo and promotes apoptosis in both epithelial and subepithelial mononuclear cells.
127 THE COLORECTAL NURSE PRACTITIONER TRAINING IN COLONOSCOPY AND POLYPECTOMY
M. T. Castle, K. Ragunath, T. Balfour, J. H. Scholefield.Division of Surgery and Wolfson Digestive Diseases Centre, University Hospital Nottingham, UK
Background and Aim: An audit of the colorectal nurse practitioner’s (CNP), (MTC), performance in lower GI endoscopy, between January 2003 and January 2004, revealed that CNP had performed 374 lower GI procedures and 104 polyps were found. The CNP with the assistance of the supervising consultant excised 52 (50%) of the polyps that were <2 cm. Polyps >2 cm was dealt by the consultant. It was proposed that given a specific programme of training there was a significant opportunity for the CNP to excise successfully and safely polyps <2 cm.
Method: Review of practice before and after one to one focussed training in colonic polypectomy.
Results: After a six month period of intensive supervised learning, 240 lower gastrointestinal procedures were performed independently by the CNP from July 2004–May 2005, (101 colonoscopy and 139 flexible sigmoidoscopy). One hundred and fifty six (65%) patients were female and the median age was 55. Eighty nine (88%) of colonoscopies were carried out to the caecum. Cancers were detected in 13 (5%) of patients. In addition 65 polyps were found in 54 (23%) patients. Out of the 65 polyps, seven (11%) measured >2 cm and were referred to the consultant, as were two other patients with polyps each on warfarin. Fifty six (86%) polyps measured <2 cm and were safely snared or hot biopsied by the CNP. There were no immediate or late (30 days) complications.
Conclusion: After a period of one-to-one learning and supervisory practice it is safe for the CNP to perform polypectomy on polyps measuring up to 2 cm. With limited NHS resources and the introduction of bowel cancer screening, the role of CNP may be extended to colonoscopy and polypectomy.
128 THE THREAT TO SPECIALIST TRAINING FROM THE EUROPEAN WORKING TIME DIRECTIVE: RESULTS FROM THE BSG TRAINING COMMITTEE SURVEY OF SPRS
B. H. Hayee, I. C. Forgacs.King’s College Hospital, London SE5 9RS (on behalf of the BSG training committee)
Introduction: The implementation of the European Working Time Directive (EWTD) on 1 August 2004 has created major changes in the working patterns of specialist registrars (SpRs). On-call rotas for acute general medicine and mandatory rest periods now prevent attendance at a proportion of fixed specialty training sessions. The curriculum for Higher Training in Gastroenterology had previously specified that SpRs should attend 40 consultant-led ward rounds, 80 endoscopy lists, and 80 training clinics over a 12 month period. To determine whether these targets could still be met within the constraints of the EWTD, the BSG Training Committee sent a questionnaire to SpRs in Gastroenterology.
Methods: Each SpR in a training programme in Gastroenterology was asked to complete a questionnaire in April 2005 (chosen as the month when training was least likely to be affected by major meetings, public holidays or annual leave). SpRs stated the number of total number training opportunities in their timetable and the number their working patterns allowed them to attend.
Results: 110 responses (∼40%) were received. Seventy (67%) were in the first three years of training. Less than 10% took any leave during the study month. As a result of the EWTD (excluding leave), SpRs were unable to attend 26% of scheduled clinics, 25% of supervised endoscopy lists, 34% of consultant-led ward rounds, 40% of cancer MDT meetings, 18% of histopathology meetings, and 45% of journal clubs. In addition, 24% of regional training days were not attended. A maximum of 48 supervised endoscopy lists, 66 clinics and 60 consultant-led rounds could be attended over the course of a year.
Conclusions: Implementing the EWTD has reduced training for SpRs by 25 to 40%. As a result the current requirements for higher specialist training in Gastroenterology are not being met. The service commitment for acute medicine is highly damaging to specialty training.
129 THE EFFECT OF FOOD COMPOSITION AND PREPARATION ON REFLUX SEVERITY IN PATIENTS WITH REFLUX DISEASE
M. Fox, C. Barr, S. Nolan, A. Anggiansah, M. Lomer, T. Wong.Department of Gastroenterology and Oesophageal Lab, St. Thomas’, London
Introduction: Patients with gastro-oesophageal reflux disease (GORD) are often told to avoid fatty food in the hope that this will decrease acid reflux; however evidence from healthy volunteers suggests that reflux severity may not associated with fat content per se but calorie density. Moreover effects of meal preparation on reflux have never been studied. Bravo (Medtronic) is a catheter-free oesophageal pH monitoring system that is well tolerated by patients. The device remains attached and provides accurate measurements for several days.
Aim: To examine the effects on GORD of high fat (58%) v low fat (25%) meals (calories constant), high calorie (1000 kcal) v low calorie (500 kcal) meals (fat constant), and high fat mixed solid/liquid v liquid meals (composition constant). Meals volume was controlled (800 ml).
Method: Twenty one patients referred for investigation of reflux symptoms were studied. Bravo was placed under sedation at endoscopy. All meals were supplied, providing 24 hours in each “dietary condition”. Patients returned after 48 hours and 96 hours to download data. Friedman test was used to identify associations of food composition and preparation with acid reflux.
Results: Data were available from 15 patients (9 female, median age 48 (26–70) years, BMI 26 (21–35) kg/m2). Demographic variables and meal sequence had no effect on reflux parameters. Acid reflux was reduced in low compared to high calorie meals (fat constant) 5.3 v 8.4% time pH<4 (p<0.01). No difference was observed between low and high fat meals (calories constant); 8.6 v 8.2% time pH<4 (p = NS). Food preparation did not affect reflux parameters (p = NS).
Conclusion: Prolonged pH recordings by BRAVO allowed the first detailed comparison of dietary conditions on reflux severity in GORD. A clinically relevant (∼40%) decrease in reflux severity was found on a low calorie, low fat diet compared with an isovolumetric high calorie, low fat diet. In contrast, no difference in reflux parameters was seen after a high fat meal compared with an isocaloric and isovolumetric low fat meal. GORD patients should be advised that lowering the calorie density (richness) of meals can significantly reduce acid reflux.
130 THE MALLORY WEISS TEAR
J. M. Thomson, D. L. Armour, J. Masson, A. Fraser, N. A. G. Mowat.Gastrointestinal Unit, Aberdeen Royal Infirmary, Aberdeen, UK
Introduction: Bleeding from Mallory Weiss Tear (MWT) is generally considered to be trivial, self-limiting, and rarely requiring acute intervention. There are, however, only limited community based published data to support this benign perception. The 10 year prospectively collected data from the Aberdeen Gastrointestinal Bleeding Unit (AGIBU) have given us the opportunity to evaluate this further.
Aim: To evaluate the natural history of Mallory Weiss Tears in the stable at risk population (458 536) of Grampian over a 10 year period.
Method: Prospectively collected data on all admissions with gastrointestinal bleeding to the AGIBU were stored on a Microsoft Access database. Analyses were then performed on the data collected from all admissions with bleeding from Mallory Weiss Tears.
Results: From October 1991 to October 2001, 9.3% (n = 658) of admissions to the AGIBU, with suspected upper GI bleeding, bled from a MWT. A positive correlation (p<0.0001) was seen with young male patients, acute and chronic alcohol intake, smoking, and a history of vomiting when compared to the other AGIBU admissions. Of those with haematemasis, 36% did not have a prior history of retching or vomiting. The bleeding episode was defined as significant (haemodynamic compromise, Hb<10 g/dl) in 36.7%. The proportion with significant bleeding increased with age (p<0.01) and was more common in females (p<0.01). The majority had a short hospital admission with no complications. However 5% (n = 28) rebleed within 30 days and 1.71% (n = 9) died within 30 days. All of the deaths were associated with significant comorbid disease.
Conclusions: Contrary to popular belief bleeding from MWT is not only common but is often significant. It often occurs without retching or prior vomiting and can be associated with rebleeding. There is a small but significant mortality.
131 ATTENTIONAL MODULATION OF VISCERAL AND SOMATIC PAIN
P. Dunckley1,2, Q. Aziz3, R. G. Wise1,2, J. Brooks1,2, I. Tracey1,2, L. Chang4.1Departments of Human Anatomy and Genetics & FMRIB, University of Oxford, Oxford, OX1 3QX, UK; 3Department of GI Science, Clinical Sciences Building, University of Manchester, Hope Hospital, Salford M6 8HD, UK; 4Center for Neurovisceral Sciences and Women’s Health, Division of Digestive Diseases, David Geffen School of Medicine at UCLA, LA, USA
Background: Hypervigilance, an increased state of guardedness, watchfulness, or attention, has been proposed as a possible underlying aetiology in irritable bowel syndrome. As hypervigilance must be a centrally mediated process, functional magnetic resonance imaging of the brain can be used to test this hypothesis. However, a better understanding of the normal attentional mechanisms during visceral pain in health is initially required. The aim of this experiment was to identify the neural correlates underlying the attentional modulation of visceral and matched somatic pain.
Methods: Twelve healthy, pain-free, right handed subjects were recruited for the study. Simultaneous electrical pulses and auditory tones lasting 6 seconds were delivered to the subjects during a whole-brain functional scan acquisition. The electrical catheter was placed into the rectum for the visceral scan and onto the lower abdomen for the somatic scan. Subjects were instructed to attend to and count either the auditory tones or electrical pulses. Electrical pulses and auditory tones were delivered at either 2, 3.5, or 4.3 Hz thereby varying the cognitive demand of the tasks. Pain intensity, unpleasantness, and tone/pulse count were recorded after each stimulus.
Results: During the 3.5 Hz and 4.3 Hz conditions alone, distraction by the auditory tones resulted in a significant reduction in pain report (p<0.05) in both sensory modalities. There was a marked spatial overlap in group statistical activation maps during somatic and visceral pain. The typical “pain matrix” was activated. Using pain intensity values as regressors in a group level regression analysis, the primary somatosensory cortex (SI) increased in activity with increasing pain report, independent of attentional direction. Likewise the primary auditory cortex (AI) increased in activation with decreased pain report. Right dorsolateral prefrontal cortex (DLPFC) activity correlated positively with pain intensity during somatic pain.
Conclusions: Pain perception during attentional modulation is reflected in the primary sensory cortex activity and may be influenced in a top-down manner by the right DLPFC during somatic pain.
132 DEVELOPING A NOVEL STIMULATION PARADIGM FOR ENHANCING HUMAN BRAIN-SWALLOWING PATHWAYS
S. Singh1, S. Mistry1, J. Rothwell2, D. G. Thompson1, S. Hamdy1.1Department of GI Science, Hope Hospital, Salford, UK; 2Sobell Department, Institute of Neurology, London, UK
Background: Neuronal excitability can be amplified by the synchronous activity of two afferent stimuli. This process, known as paired associative stimulation (PAS), has been successfully applied in enhancing hand motor cortex excitability. The effect of PAS on the swallowing motor cortex, which is bilaterally represented, remains unknown.
Aims: We investigated the optimal timing for the two stimuli of PAS for altering bi-hemispheric swallowing motor cortex excitability.
Methods: Healthy volunteers underwent transcranial magnetic stimulation with resultant pharyngeal electromyograph (EMG) traces recorded through an intraluminal catheter. Mean EMG amplitude representing cortical excitability was assessed before and after PAS (paired pharyngeal electrical and transcranial magnetic stimuli every 20 s for 30 minutes). Twelve subjects attended on four occasions to test the effect of various interstimulus intervals (ISI) between the two PAS pulses (50, 75, 100, and 125 ms). In six further subjects, the effect on the contralateral hemisphere was assessed.
Results: PAS with a 100 ms ISI produced an immediate increase in cortical excitability that reached 130% compared to baseline and was sustained at 2 hours (fig 1). All other ISIs produced less than 40% change in cortical excitability (p<0.02). The contralateral hemisphere showed a smaller but non-significant increase in cortical excitability (fig 2, p = 0.2).

Abstract 132, Figure 1 Change in cortical excitability following PAS at various ISIs.
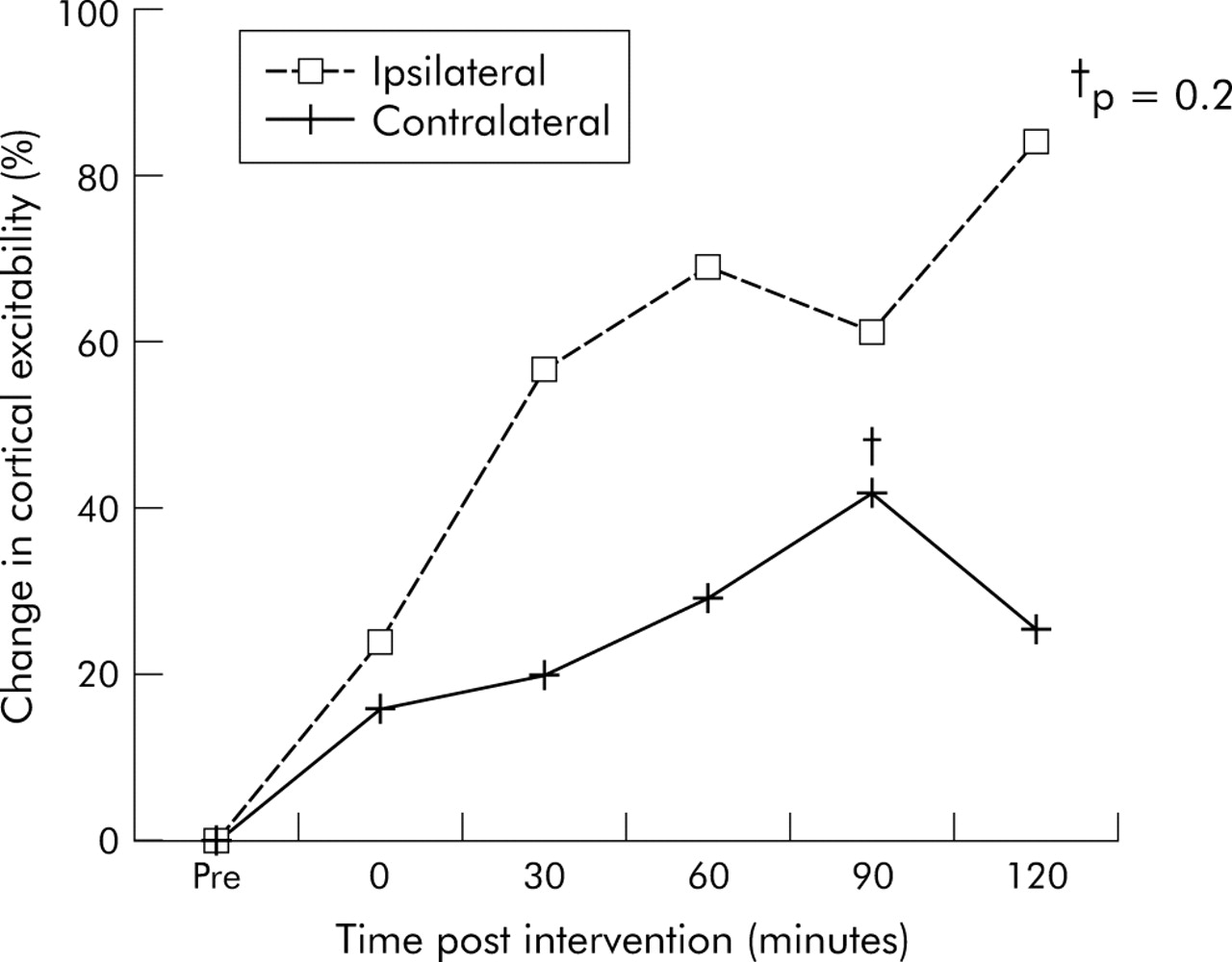
Abstract 132, Figure 2 Change in cortical excitability following PAS at an ISI of 100 ms.
Conclusion: PAS applied to swallowing motor cortex can induce sustained increases in cortical excitability of the stimulated hemisphere. These changes may have implications for the rehabilitation of dysphagic stroke patients.
133 WHO CONSULTS WITH DYSPEPSIA? A 10 YEAR CROSS SECTIONAL SURVEY
A. C. Ford1, A. G. Bailey1, D. Forman2, A. T. R. Axon1, P. Moayyedi3.1Centre for Digestive Diseases, Leeds General Infirmary, Leeds; 2Centre for Epidemiology and Biostatistics, Leeds University Medical School; 3Gastroenterology Division, Health Sciences Centre, Hamilton, Canada
Introduction: Dyspepsia is a chronic relapsing, remitting disorder, the natural history of which has been studied extensively. However, there are few studies examining factors that influence likelihood of consulting a general practitioner (GP) with symptoms in those who are symptomatic, particularly over a long time period.
Methods: The authors performed a 10 year follow up cross sectional survey of individuals recruited into a community screening and treatment programme for Helicobacter pylori. All surviving, traceable participants were contacted, by validated postal dyspepsia questionnaire. Baseline demographic data, quality of life at study entry, and dyspepsia and irritable bowel syndrome (IBS) symptom data were already on file. Written informed consent was sought to examine primary care records, and data on NSAID and aspirin use, and number of dyspepsia related consultations over the 10 year period were extracted from these.
Results: Of 8407 individuals originally involved, 3266 (39%) gave consent to examination of primary care records. The mean age of included individuals was 55 years, and 1799 (55%) were female. 1738 (53%) had dyspepsia at any point during 10 year follow up, when dichotomised according to questionnaire data. Of these, 729 (42%) consulted their GP. The mean number of consultations in these individuals was 3.5 (range 1 to 23). Univariate analysis revealed that H pylori infection, female gender, tobacco use, Asian ethnicity, lower social class, lower quality of life at study entry, IBS, and NSAID or aspirin use significantly increased likelihood of consultation, while the opposite applied to regular alcohol use. Following logistic regression H pylori infection, lower social class, lower quality of life at study entry, and aspirin use remained independent risk factors for consultation.
Conclusions: The reasons for consulting a GP with dyspepsia are multifactorial, but H pylori infection, aspirin use, low social class, and poor quality of life are independent predictors of consultation.
134 DECOMPENSATED ALCOHOLIC LIVER DISEASE: DETERMINANTS OF SUBSEQUENT DRINKING BEHAVIOUR
E. McFarlane, C. Gellion, J. Jones, J. Skinner1, D. Gleeson.Liver Unit, Sheffield Teaching Hospitals; 1West Sheffield Primary Care Trust, Sheffield UK
Background: In patients with decompensated alcoholic liver disease (ALD), continued heavy drinking is associated with mortality. Its determinants are not well understood.
Aim: Evaluation of drinking behaviour after diagnosis of decompensated ALD.
Methods: Review of records of 190 consecutive patients discharged from hospital following admission with first episode of decompensated ALD; phone calls as required to patient, family, and GP. Drinking behaviour since discharge up to 1/4/05 or to death evaluated in all patients and classified as grade 1–4 (see below). Time to first drinking relapse was also recorded. In the 130 Sheffield residents, Townsend and Jarman indices of social deprivation were derived from postcodes.
Results: The proportion of patients remaining abstinent after 3, 12, and 24 months was 42+4%, 31+4%, and 24+3% respectively. Predictors of relapse by Cox regression analysis were younger age and living alone. 49 patients were fully abstinent (drinking grade 1), 54 drank (18 occasionally, 36 regularly) below the safety limits (grade 2), 44 patients reduced their previous intake to a level above the safety limits (15 binge drinkers, 29 regular drinkers) (grade 3), and 49 patients failed to reduce previously heavy intake (grade 4). Patients with drinking grade 4 (a) had higher alcohol intake prior to admission (median 142 v 105 U/wk) and higher Townsend (4.1 v 0.9) and Jarman (21 vs 5) scores (all p<0.01 by Mann-Whitney) and (b) were more likely to live alone and to have failed to stop drinking prior to admission (p<0.01 by χ2), compared to patients with grades 1–3, between which these parameters did not differ. Patients with drinking grades 3–4 were younger than those with grades 1–2 (median age 45 v 50 years). Gender and MELD score on admission were not associated with drinking behaviour.
Conclusions: After hospital discharge, continued heavy drinking in patients with decompensated ALD is associated with young age, previous heavy drinking, failure to stop prior to admission, social deprivation, and living alone. These associations may help target interventions to modify drinking behaviour.
135 A STUDY TO ASSESS EXPERTISE AND TRAINING IN TRANSCUTANEOUS LIVER BIOPSY AMONG TRAINEE GASTROENTEROLOGISTS
P. F. Marden, B. Colleypriest (introduced by D Robertson).Royal United Hospital, Combe Park, Bath BA1 3NG, UK
Background: The JCHMT Gastroenterology Curriculum Feb 2005 states trainees should be skilled in liver biospy. Increasingly transcutaneous liver biopsy is conducted under ultrasound guidance by radiologists suggesting trainee gastroenterologists are no longer routinely experienced in the procedure despite the stated curriculum aims.
Aim: This study aims to determine the level of training and competence in transcutaneous liver biopsies amongst SpRs in gastroenterology in a training region (Wessex deanery)
Methods: All gastroenterology SpRs in the Wessex deanery received a questionnaire aimed at assessing their training in liver biopsy and knowledge of the current British Society of Gastroenterology guidelines on the use of liver biopsy in clinical practice.
Results: Thirty one SpRs were eligible for the study and 77% responded. None currently worked in a trust where transcutaneous liver biopsy was routinely conducted by a gastroenterologist. Only 54% had practical experience of liver biopsy under supervision and 29% without supervision. Just 25% had a written record of this training. None had conducted a liver biopsy in the last twelve months. Only 4% knew the pre-procedure platelet count quoted as safe in the BSG guidelines, although 94% knew the safe level of INR. With regards to pain post procedure and significant haemorrhage only 4% and 16% respectively knew guideline figures. Only 25% could quote accurate mortality figures post liver biopsy. No respondent had received training in transabdominal ultrasound although 45% felt gastroenterologists should be trained in conducting liver biopsies.
Conclusion: This study shows trainees in gastroenterology have a low level of practical and theoretical knowledge with regards to transcutaneous liver biopsy. Only a more comprehensive survey can determine if this is a national phenomen. If stated JCHMT curriculum aims are to be addressed training in transabdominal ultrasound scanning may need to be compulsory for trainees.
136 PREVALENCE AND CHARACTERISTICS OF OVERLAP SYNDROMES IN AUTOIMMUNE LIVER DISEASE, A 20 YEAR COHORT FROM A DEFINED COMMUNITY IN SOUTH WALES
M. A. Czajkowski, J. G. C. Kingham.Department of Gastroenterology, Singleton Hospital, Swansea, UK
Background: The characteristics and relative frequency of overlap syndromes between autoimmune hepatitis (AIH) and both primary biliary cirrhosis (PBC) primary sclerosing cholangitis (PSC) are well described. Published data come from tertiary centres rather than a community setting and so may be affected by referral bias.
Methods: 252 consecutive cases of autoimmune liver disease have been followed prospectively from 1984–2005 in a community hospital serving a stable population of 250 000 (98.6% white) in South Wales, UK. 27 overlap syndromes have been seen among the 121 cases of PBC, 78 of AIH, and 53 of PSC. Overlap syndromes were defined by clinical, biochemical, histological, serological, and cholangiographic features. Antimitochondrial antibody (AMA) negative PBC cases were excluded. 27 cases (22 female) aged 11–74 years (median 58) at presentation, have been followed for 1–29 years (median 11); 314 patient-years.
Results: There were 21 PBC/AIH, 4 AIH/PSC, 1 PBC/PSC, and 1 sequential overlap between PSC, PBC, and AIH. The dominant clinical picture was PBC in 7, PBC with bouts of AIH in 4, PBC evolving to AIH in 1; AIH in 6, AIH evolving to PBC in 2; PSC in 2, PSC with bouts of AIH in 3 and asymptomatic cirrhosis in 2. The biochemical pattern was cholestasis in 16, hepatitis in 12, both in 6 and mild mixed enzyme elevations in 5. Antinuclear +/− anti-smooth muscle antibodies (mean titre 1:640) were seen in 21, AMA (mean titre 1:640) in 14, both in 10. Histologically 6 had PBC, 5 AIH, while 10 showed features of both. 11 were cirrhotic at initial biopsy. There have been 6 liver related and 2 unrelated deaths and one liver transplant while 18 are in remission. 16 were treated with corticosteroids and Azathioprine and 10 with Ursodiol. Steroid induced osteoporosis was particularly common in PBC/AIH overlaps. Outcome reflected the dominant clinical picture and did not differ from the whole cohort with autoimmune liver disease.
Conclusion: In this community setting over a 21 year period, overlaps were seen in 22 of 199 patients with AIH or PBC (11%), five of 131 patients with AIH or PSC (4%), and two of 174 patients with PBC or PSC (1%). The PBC/PSC overlap is a newly recognised syndrome.
137 REMIFENTANIL VERSUS MIDAZOLAM AND PETHIDINE SEDATION DURING COLONOSCOPY: A PROSPECTIVE, RANDOMISED STUDY
M. Manolaraki2, G. A. Paspatis1, E. Vardas1, A. Theodoropoulou1, P. Oustamanolakis1, A. Gritzali2, A. Anastasiadou2.1Department of Gastroenterology; 2Anesthesiology, Benizelion General Hospital, Heraklion-Crete, Greece
Background and Aims: Our study sought to compare the safety and efficacy of remifentanil (group A) versus the standard regimen of midazolam and pethidine (group B) for sedation during colonoscopy. To the best of our knowledge, this is the only prospective, randomised comparative study for the two regimens.
Methods: 116 consecutive patients undergoing colonoscopy were randomly assigned to groups A or B. In group A, patients were started with a loading dose of 1 μg/kg/min remifentanil followed by a continuous infusion at an initial rate of 0.05 μg/kg/min, adjusted accordingly. Patients in group B (n = 56) received intravenously 4.3 (SD 1) mg midazolam and 81.7 (SD 21) mg pethidine. The quality of the analgesia was assessed with a four point scale; recovery level was evaluated with the Aldrete score, while patients’ suitability to home readiness was evaluated by a Modified Post Anesthesia Discharge Scoring system (MPADS). Patients’ comfort level was assessed 24 hours after the procedure.
Results: Recovery time and time to home readiness was significantly shorter for the group A than for group B (Aldrete 10: 0 v 70.7 (SD 13.6) minutes and MPADS of 10: 28.7 (SD 4.3) v 157.8 (SD 34.2) minutes) (p<0.01). Multivariate stepwise logistic regression analysis revealed that among sex, age, duration of the test, ASA grade, and the type of sedation, the latter was the only factor associated with a quicker patient recovery time (χ2 = 160.6, p<0.01). Patient satisfaction was significantly higher in group B patients than group A (p<0.05). Alterations in mean arterial blood pressure, respiratory rate and SpO2 were significantly higher in group B compared to those of group A (p<0.05).
Conclusions: Our data suggest that remifentanil sedation during colonoscopy provides sufficient pain relief, better hemodynamic stability, less respiratory depression, and significantly faster recovery comparing to midazolam/pethidine. However, the use of midazolam/pethidine was associated with a higher patient satisfaction.
138 IS A PHOTOGRAPH OF THE CAECUM OR TERMINAL ILEUM RELIABLE ENOUGH FOR DOCUMENTING COMPLETION OF COLONOSCOPY? A PROSPECTIVE STUDY
R. Guruswamy, J. Skinner, B. Brett.James Paget Hospital NHS Trust, Great Yarmouth, Norfolk NR31 6LA, UK
Introduction and Aim: Documenting colonoscopy completion may become an important aspect of quality assurance if a suitable tool becomes available. The aim of this study was to independently assess the reliability of caecal or terminal ileal photographs as a proof of colonoscopy completion.
Materials and Methods: Colonoscopists were requested to take a convincing photograph of the caecum or terminal ileum to document completion of their examination during a prospective colonoscopy audit. Caecal photographs captured the following landmarks in various combinations (appendicial opening, ileocaecal valve and tri-radiate fold). Terminal ileal photographs were either taken after water flush (to enhance the villi) or without. 177 photographs were collected over eight months and a further 23 bluff photographs were added randomly. Eight clinicians (surgeons and gastroenterologists) were requested to categorise the photos as “caecum, terminal ileum or not sure”. Those identified as caecum and terminal ileum were further graded as 1, 2, or 3 depending on the level of certainty.
Results: A total of 200 photographs were used. The true locations were caecal in 91 (45.5%) cases, terminal ileal in 86 (43%) cases, and 23 (11.5%) were bluff photographs. Thirty eight per cent of the caecal photographs, 71% of the terminal ileal photographs (combined), and 85.8% of the terminal ileal photographs with water flush technique were identified with a certainty of grade 2 or 3. When all the grades were considered, 93.9% of the terminal ileal photographs with water flush technique were identified. Interestingly 15% of the bluff photographs were interpreted as caecum and a further 15% as terminal ileum.
Conclusion: A photograph of the terminal ileum after flushing with water appears to be a reliable and safe technique for documenting colonoscopy completion. This is less invasive when compared to terminal ileal biopsy. Caecal photographs do not appear to be a reliable way to document completion due to high interobserver variability.
139 WITHDRAWN
140 COMPARISON OF TIME TO SYMPTOM RESOLUTION WITH ORAL MESALAZINE 4.8 G/DAY (800 MG TABLET) VERSUS 2.4 G/DAY (400 MG TABLET): ANALYSIS OF DATA FROM TWO RANDOMISED, double blind, clinical trials in patients with moderately active ulcerative colitis
J. F. Marion1, M. Safdi2, D. A. Schwartz3, G. Regalli4, R. Eusebio4, L. Law (introduced by S Ghosh)4.1Mount Sinai School of Medicine, NY; 2Greater Cincinnati Gastroenterology Associates, Cincinnati, OH; 3Vanderbilt University, Nashville, TN; 4Procter & Gamble Pharmaceuticals, Cincinnati, OH, USA
Aim: To evaluate the time to resolution of the cardinal symptoms associated with ulcerative colitis (UC) (stool frequency, rectal bleeding, and both stool frequency and rectal bleeding) in patients with moderately active UC (Physician’s Global Assessment of 2) taking mesalazine dosed at 4.8 g/day with a new 800 mg tablet (P&G Pharmaceuticals), and 2.4 g/day dosed with the currently marketed 400 mg tablet (Asacol, US)
Methods: Data from two randomised, double blind, six week, parallel group studies (ASCEND I & II) conducted in patients experiencing a flare of active UC were pooled and analysed. Time to resolution of UC symptoms was based on first day of resolution according to daily diaries kept by the patients through an integrated voice response system. In this prespecified analysis, resolution of stool frequency (SF) was defined as a patient’s return to his/her normal number of stools per day, and resolution of rectal bleeding (RB) was defined as the absence of visible blood in stools.
Results: A total of 687 patients with mild to moderate disease were randomised into the study, of which 423 analysable patients had moderately active UC. Results of the median time to resolution analysis are shown in the table.
Abstract 98
Conclusion: Mesalazine at a dose of 4.8 g/day (800 mg tablet) significantly decreases the median time to resolution of rectal bleeding and the composite of both stool frequency and rectal bleeding compared to mesalazine at a dose of 2.4 g/day (400 mg tablet) in patients with moderately active UC.
This research was funded by Procter & Gamble Pharmaceuticals.
141 CANCER RISK OF LOW GRADE DYSPLASIA IN CHRONIC ULCERATIVE COLITIS: A META-ANALYSIS
T. Thomas1, K. R. Abrams2, R. J. Robinson1, J. F. Mayberry1.1Gastroenterology, Leicester General Hospital; 2Epidemiology and Public Health, University of Leicester, Leicester, UK
Introduction: The risk of colorectal cancer when low grade dysplasia (LGD) is diagnosed in chronic ulcerative colitis is variable in various studies. The management of the lesions therefore remain contentious.
Aims and Methods: The aim of this meta-analysis was to determine the cancer incidence of LGD when detected on surveillance and the risk of developing cancer or any advanced lesion once LGD is diagnosed. A MEDLINE, EMBASE, and PubMed search was conducted using the key words “surveillance”, “colorectal cancer”, “low-grade dysplasia”, and “ulcerative colitis”. A search of reference lists of all relevant review articles and the retrieved original articles were made to identify articles missed on the initial search. Surveillance studies that involved patients with histological proof of low grade dysplasia, documented follow up data, and the outcome measure was cancer or high grade dysplasia were included. The heterogeneity between the studies was calculated using the Q homogeneity statistic and if significant (p<0.05) a random effects model of meta-analysis was used.
Results: Twenty one surveillance studies met the inclusion criteria. This included 2808 patients with chronic ulcerative colitis on surveillance of which 534 had either flat LGD or LGD with dysplasia associated lesion or mass. An average of four colonoscopies were done/patient (range: 1.5–8.4) over an average duration of 12 years (range: 4–22). An average of 19 biopsies taken per colonoscopy (range: 8–56) detected 69 advanced lesions (cancer or high grade dysplasia) preoperatively. The average duration of colitis before LGD was diagnosed was 17 years (range: 11.5–33.8). The cancer incidence was 13/1000 pyd and the incidence of any advanced lesion was 30/1000 pyd. When LGD is detected on surveillance there is an 8× higher chance of developing cancer (OR 8.1, 95% CI 4 to 17.5) and 11× higher chance of developing any advanced lesion (OR: 11, 95% CI 5.1 to 23). There is a significant rise in cancer incidence over time (p = 0.002)
Conclusion: The risk of developing any advanced lesion in patients with LGD in chronic UC is high. The cancer incidence rates when LGD is detected on surveillance has significantly increased over time. These figures are valuable in an informed decision process when managing these patients.
142 PROBIOTIC BACTERIA INHIBIT EPITHELIAL CELL IL-8 PRODUCTION: ROLE OF TOLL-LIKE RECEPTOR ENGAGEMENT
B. N. Hudspith, G. Rouzaud*, G. R. Gibson*, N. B. Rayment, L. Petrovska, K. Bruce, J. D. Sanderson, J. Brostoff.Nutritional Sciences Research Division, King’s College London, London, UK; *University of Reading, Food Microbial Sciences Unit, Reading, UK
Background and Aims: There is increasing interest in the use of probiotics as modulators of intestinal inflammation and gut flora homeostasis. Although the mechanism involved is unknown, it is likely to involve an interaction with gastrointestinal epithelial cells. The aim of this study was to study probiotic suppression of E coli induced IL-8 production in epithelial cell lines and investigate the potential role of toll-like receptors (TLRs) in this interaction.
Methods: HT29 and Caco-2 cells were grown until confluent. Probiotic strains and specific TLR agonists and antagonists were then added one hour before stimulation with E coli. Supernatants were collected at 20 hours and IL-8 assayed by ELISA. E coli adherence was assessed by culture of washed lysed cells on MacConkey’s agar.
Results: The addition of E coli induced significant IL-8 production in both cell lines. Pretreatment with B longum or lactus and L casei, acidophilus, pentosus, or plantarum probiotics completely blocked E coli induced IL-8 production. Culture of recoverable E coli was in keeping with loss of adherence. The TLR-2 agonist lipoteichoic acid (LTA) reduced IL-8 production in HT29 and Caco-2 cells by 60%. Although LPS on its own only produced a low response, the TLR-4 antagonist Polymixin B suppressed E coli-induced IL-8 production (35% in HT29, 20% in Caco-2 cells). TLR-3, 5, and 7 agonists and antagonists had no effect. Finally, IL-8 production after addition of E coli K12 msbB, which fails to bind TLR-4, was 40% and 20% less in HT29 and Caco-2 cells respectively compared to E coli K12 supporting a role for TLR-4.
Conclusions: Probiotics demonstrate potent inhibition of E coli induced IL-8 production and loss of adherence in vitro highlighting their therapeutic potential in gut inflammation. These findings suggests a role for TLR-2 and TLR-4 receptors in these suppressive probiotic effects.
143 EVIDENCE FOR DIFFERENT REGULATION OF ILEAL BILE ACID TRANSPORTER TRANSCRIPTS IN PATIENTS WITH CHRONIC DIARRHOEA
S. Balesaria, K. M. Chavele, U. Khair, J. R. F. Walters.Department of Gastroenterology, Imperial College & Hammersmith Hospital, London, UK
Background: Chronic diarrhoea can result from disease or resection of the terminal ileum leading to bile acid malabsorption. The cause of primary idiopathic bile acid malabsorption is unknown, despite being a frequent cause of unexplained chronic diarrhoea. The aim of this study was to determine whether changes in transcriptional regulation of bile transporters in the ileum could be identified.
Methods: Ileal biopsies were obtained at colonoscopy from patients with chronic diarrhoea (n = 17) and from controls without diarrhoea (n = 21). No evidence of any ileal disease or of other causes of diarrhoea was present. RNA and cDNA were prepared and gene expression measured by quantitative real-time RT-PCR. Expression was normalised to that of the housekeeping gene GAPDH.
Results: No significant differences in the mean or median values were found for transcripts of the apical membrane sodium-linked bile acid transporter ASBT, the cytoplasmic ileal bile acid binding protein IBABP, or the putative basolateral organic solute transporters alpha and beta. There was no significant correlation between ASBT and IBABP in controls although they were related in those with diarrhoea. Expression of transcription factors previously shown to affect ASBT or IBABP expression was then measured. Mean or median values for FXR, LRH-1, SHP, c-Fos, or CDX2 were not significant different between groups. However the relationships of expression of these factors with ASBT and IBABP differed. Multiple stepwise regression showed that ASBT was significantly associated with LRH-1 and SHP in controls, and with SHP and CDX2, but not LRH-1, in diarrhoea. IBABP was associated with LRH-1, SHP, and CDX2 in controls, but only with CDX2 in diarrhoea.
Conclusion: Bile acid transporters were expressed at similar levels in patients with chronic diarrhoea and controls, but ASBT and IBABP may be regulated differently in patients with chronic diarrhoea.
Liver posters
144 H63D MUTATION AND LIVER DISEASE
Y. Reddy, R. Hunt, D. Das.Stepping Hill Hospital, Stockport, UK
Background: Haemochromatosis was first described by Von Recklinghausen in 1889 but the phenotypic heterogenecity became apparent only since the discovery of candidate genes in the early 90s. 90% of patients with haemochromatosis have C282Y mutation and its clinical effects are well known. The effects of H63D mutation remain unclear despite its world wide prevalence. Data available from the available studies show that H63D disease remains clinically silent in the majority and is not associated with significant hepatic iron overload or scarring.
Methods and Results: We looked at our database of 57 cases of haemochromatosis diagnosed between 1998 and 2005. Six homozygous H63D patients (1 female, 5 males) presenting with serum ferritin of 16, 350, 2000, 801, 203, 263 respectively. Four patients underwent liver biopsy for clinical indications not related to iron overload. The severity of iron overload in none of these biopsies was greater than grade 1. Three cases displayed a minor degree of portal fibrosis. One case progressed from mild fatty change to micro nodular cirrhosis in three years time and developed severe portal hypertension. His alcohol consumption was moderate (<20 g/day) and viral markers were negative. His ferritin remained normal throughout and no other cause for the progression of his liver disease was found.
Conclusion: We suspect that in the background of his genetic predisposition this risk of moderate alcohol consumption could have triggered the onset of cirrhosis. The safety of moderate alcohol drinking should be reviewed in H63D homozygous individuals.
145 REGENERATION IS INCREASED IN JNK2 KNOCKOUT LIVER
C. M. Bates, N. C. Henderson, K. J. Simpson.(introduced by P. C. Hayes). Centre for Liver and Digestive Disorders, Royal Infirmary of Edinburgh, UK
Background: The ability for liver to regenerate following toxic injury or resection is almost unique and involves the complex interaction of multiple factors to produce a rapid regenerative response. C-jun N terminal kinase (JNK) is a mitogen activated protein kinase (MAPK), involved in intracellular signalling. Upon activation by stress signals, proinflammatory stimuli, and mitogens, its main action is the phosphorylation of the transcription factor c-jun. JNK intracellular signalling pathway has a crucial role in liver regeneration. Three isoforms JNK1, JNK2, and JNK3 exist, JNK3 being mainly confined to brain, heart and testis. JNK1 is the main isoform involved in phosphorylation of c-jun and is a positive regulator of cellular proliferation. JNK2 in contrast is the main isoform that facilitates ubiquitination of c-jun and subsequent proteosome degradation, therefore is possibly a negative regulator of proliferation.
Methods: Using genetically modified JNK2 knockout mice we investigated if JNK2 knockout liver has increased hepatocyte proliferation compared to wild-type littermate controls following toxic liver injury. Both wild-type controls and JNK2 KO mice (8 weeks old) were injected with carbon tetrachloride (CCl4 - 1 in 3 in 3 olive oil, 1 μl/g body weight). Liver injury, assessed by H&E stained histology and ALT, was similar in JNK2 KO and wild type controls. Hepatocyte proliferation was determined by the incorporation of 5-Bromo-2′-deoxy-uridine (BrdU) into nuclei synthesising DNA, BrdU positive nuclei per 1000 nuclei were counted and calculated for each time point, and also western blot for cell cycle related cyclin-cyclin D1.
Results: At 30 hours post CCl4 injection hepatocyte proliferation was significantly increased in the JNK2 KO mice as determined by BrdU incorporation (JNK2 KO 2.47 (SD 0.86) nuclei per high power field, control 0.4 (SD 0.17); n = 4). Expression of cyclin D1 was significantly elevated at 30 hours in JNK2 KO mice compared with littermate controls. This research has demonstrated earlier and increased hepatocyte proliferation in a murine model of toxic injury in JNK2 knockout liver.
146 PRACTICAL MODIFICATIONS OF THE 13C-METHACETIN BREATH TEST STILL FULFIL CLINICAL DEMANDS FOR THE QUANTITATIVE ASSESSMENT OF LIVER FUNCTION
B. Braden1,2, A. Schneider1, C. F. Dietrich1, W. F. Caspary1, W. Kueker3, C. Sarrazin1.1Medical Department I, Johann Wolfgang Goethe University of Frankfurt/Main, Germany; 2John Radcliffe Hospital, Oxford, United Kingdom; 3Radcliffe Infirmary, Oxford, UK
Background and Aims: The 13C-methacetin breath test measures the activity of the cytochrome P450 dependent enzyme system and has been developed to assess the functional hepatic mass. We evaluated simple modifications of the 13C-methacetin breath test in order to further increase its practicability and therewith clinical acceptance.
Methods: 104 patients with different chronic liver diseases (including 35 patients with histologically proven cirrhosis) and 65 healthy controls underwent the 13C-methacetin breath test. Breath test results of two-point measurements at baseline and 5, 10, 20, 25, and 30 minutes after ingestion of the test solution, respectively, were compared to conventional breath test results (cumulative recovery after 30 minutes) and liver histology.
Results: The receiver operator curve analysis revealed the two-point measurement at 15 minutes (Delta over baseline value at 15 minutes DOB) best compared to the cumulative recovery at 30 minutes and the presence of cirrhosis in histology. Using a cut-off <14.6‰ the DOB 15 minutes reached 92.6% sensitivity and 94.1% specificity with respect to the presence of cirrhosis in liver histology. However, even the two-point measurements at 5 and 10 minutes provided good discrimination between cirrhotic and non-cirrhotic subjects.
Conclusion: The 13C-methacetin breath test reliably indicates decreased liver function in liver cirrhosis, even in its modification as two-point measurement using breath samples at baseline and after 15 minutes. This simplification of the 13C-methacetin increases practicability and cost efficiency and therewith will facilitate its clinical acceptance and distribution.
147 COVERED STENT GRAFTS FOR TIPS INSERTION PROVIDE IMPROVED CLINICAL OUTCOME: A DECADE OF EXPERIENCE
S. Masson1, H. Mardini1, J. Rose2, C. O. Record1.1The Liver Unit; 2Department of Radiology, The Newcastle Hospitals NHS Trust, Newcastle, UK
Introduction: The principal disadvantages of TIPS are the development of shunt dysfunction and hepatic encephalopathy. The introduction of covered stent-grafts is thought to improve shunt patency with a theoretical consequent increase in hepatic encephalopathy. We report on 10 years’ experience in a single centre.
Methods: Data collected prospectively at the time of TIPS insertion and surveillance portography were correlated with retrospective case note analysis. Complete data were available for 192 patients.
Results: Most patients were male (62.4%) with alcoholic liver disease (66.7%) and bleeding varices (86.6%). The procedure was unsuccessful in eight. There were 35 deaths within one month and a further five patients underwent liver transplantation during the same admission. A further seven were lost to follow up. No further analysis was undertaken on these 55. TIPS was created using a covered stent-graft in 58 patients and a bare stent in the remainder. Successful portal pressure reduction was achieved in all patients. In patients who had surveillance portography, primary patency at 1 year was 86.7% v 53.4% for the covered and bare stents respectively. Shunt insufficiency requiring intervention occurred in 5 v 35 patients requiring a total of 8 v 60 interventions during mean follow up of 19.8 (SD 1.7) v 43.2 (SD 4.1) months (covered v bare). Hepatic encephalopathy developed in 52 (38.8%) patients. HE was present within three months of TIPS insertion in 26 patients but completely resolved thereafter in 10. HE may have contributed to the death of 10 patients. In three of these the TIPS was radiologically occluded but none of these improved prior to death. HE occurred with equal frequency after both covered (37.9%) and bare stents (39.4%).
Conclusion: Newer covered stents appear to improve patency compared to bare stents with implications for surveillance and intervention. Clinically important hepatic encephalopathy develops in a minority of patients and there is no increase in frequency with covered stents.
148 ACUTE LIVER FAILURE IN SCOTLAND: 13 YEAR OBSERVATIONAL STUDY
C. M. Bates, J. S. Davidson, K. J. Simpson.(introduced by P. C. Hayes). Scottish Liver Transplant Unit, Royal Infirmary of Edinburgh, UK
Acute or fulminant hepatic failure (FHF) is a rare, life threatening condition with no specific treatment except liver transplant. Paracetamol is the commonest cause of FHF in the UK. Legislative changes to paracetamol packaging were introduced 1998 in order to reduce the number of overdoses and the prevalence of FHF. The incidence, causes or outcomes of FHF in Scotland are unknown. A prospectively collected database was analysed to obtain information on patients admitted to the Scottish Liver Transplant Unit (SLTU) with FHF.
Between November 1992 and 1 November 1 2005 there have been 783 admissions to SLTU with FHF, 351 males (45%) and 432 (55%) females. 563 (71.9%) patients had taken a paracetamol overdose (POD). Other causes included non A–E hepatitis, 59 (7.5%); idiosyncratic drug reactions, 36 (4.6%); Budd Chiari syndrome,15 (2.0%); and ischaemic hepatitis,14 (1.8%). 157 PODS (27.9%) met poor prognostic criteria, 84 (53.5%) were considered transplant candidates and 41, (49%) died prior to transplant. In patients with non-POD FHF more patients met poor prognostic criteria (85 patients, 38.6%), more were candidates (76 patients, 89%) and 57 patients (75%) survived to transplant. Paracetamol was taken as a staggered overdose in 140 (24.9%) cases—associated with increased morbidity and greater per cent of patients being too sick for transplant (22 patients (56%) were candidates, 64% became too sick). Mortality was increased with staggered mortality, 34.3% v non-staggered mortality, 21.8%.
The legislative changes have not significantly decreased admissions to SLTU (275 admissions Nov 92–Sept 98 compared with 285 admissions Oct 98–Nov 05). Increased numbers of patients met KCH criteria for poor prognosis (25% Nov 92–Sept 98 v 30.5% Oct 98–Nov 05). There is a significant increase in patients with staggered overdose following legislation changes (43 Nov 92–Sept 98 v 97 patients Oct 98–Nov 05).
Paracetamol overdose remains the commonest reason for admission to SLTU. Legislative changes have not significantly reduced the number of admissions or deaths. Staggered overdoses have increased since the legislative change and are associated with poorer prognosis.
149 WHAT IS THE DELAY TO DIAGNOSIS IN PATIENTS REFERRED WITH ABNORMAL LIVER BIOCHEMISTRY?
M. Maida, S. Unigwe, R. Rajak, R. Hocking, L. Yassin, R. Crimmins, J. T. Green, G. Swift.Gastroenterology, Llandough Hospital, Cardiff, UK
Introduction: Clear guidelines exist for the management of many of the patients seen in the primary care setting. Many of the tests to screen patients for the various causes of abnormalities in liver biochemistry are available to primary care practitioners and if employed as per a suitable guideline may reduce only time to diagnosis.
Aims and Methods: The aim of this study was to determine the extent to which patients who were referred because of abnormalities in liver biochemistry were investigated prior to referral to hospital, and the time to final diagnosis after referral. Patients with abnormalities in liver biochemistry who were referred over a one year period between October 2002 and October 2003 were identified. Their presenting complaint, investigations requested by their general practitioner, eventual diagnosis and time to diagnosis and management were analysed from the medical records.
Results: The notes of 38 patients were reviewed; 25 were new referrals during the study period. Abnormalities in liver biochemistry were an incidental finding in 16. Four patients had associated abdominal pain, three had jaundice, three had pruritis, three had weight loss, one with fatigue and one with an abdominal mass. 11 patients had had an ultrasound scan prior to referral; viral serology had been checked in five, with three patients having had a ferritin estimation, and three had autoimmune antibodies. None of the patients had had the full complement of tests at the time of referral. The final diagnosis was non-alcoholic fatty liver disease (NAFLD) in seven patients and alcohol related liver disease in five patients; four patients had autoimmune liver disease, three had gallstones, one patient was found to have a hepatoma and another had liver metastases. Medication was responsible for liver test abnormalities in one patient and no cause was found in three patients, who had isolated elevations in their test results. The average time to definitive diagnosis and a management plan after referral was seven months (2 weeks–13 months).
Conclusion: In many instances, a diagnosis could have been made had the results of preliminary tests been available at the index visit. To reduce the delay to diagnosis, we have developed a simple algorithm of tests for the investigation of patients found to have abnormal liver biochemistry in primary care, to help streamline management.
150 NON-INVASIVE MARKERS OF FIBROSIS IN NAFLD: A SYSTEMATIC REVIEW
I. N. Guha2,3, J. Parkes1,3, P. J. Roderick1,3, W. M. Rosenberg2.1Applied Clinical Epidemiology Group; 2Division of Inflammation, Infection and Repair; 3Southampton Liver Unit, University of Southampton, Trenoma Road, Southampton, UK
Background: Long term studies suggest that the presence of fibrosis within non-alcoholic fatty liver disease (NAFLD) has the most significant prognostic implication. Currently liver biopsy is the gold standard diagnostic test for liver fibrosis but due to its limitations there is a need to develop effective non-invasive tests.
Methods: We conducted a systematic review of the performance of non-invasive tests in NAFLD. Data were extracted from electronic databases 1996–September 2005: Cochrane Library 2004, MEDLINE, and EMBASE. Key measures of diagnostic accuracy and variables statistically associated with fibrosis were extracted. Inclusion criteria: NAFLD proven on biopsy, n>30 and analysis of fibrosis stages.
Results: Electronic search yielded 1781 abstracts; 27 primary studies in separate populations were included in the final analysis. Only four studies produced a true diagnostic score with details of an AUC and sensitivities and specificities at critical cut-off points. The majority of studies presented associations of variables with fibrosis found by univariate (UVA) or multivariate analysis (MVA). 17 studies compared severe to mild fibrosis, four studies compared mild fibrosis to moderate fibrosis, and six studies compared no fibrosis to any fibrosis. The most frequent variables associated with severe fibrosis were: increased age, presence of diabetes, raised AST/ALT ratio, raised homeostatic model assessment (HOMA-IR), increased BMI, raised serum hyaluronic acid, raised serum ferritin, and elevated platelet count. The data are extremely heterogeneous and presentation of odds ratios, by UVA or MVA, was variable and did not allow meta-analysis for strength of association.
Conclusion: Simple clinical and biochemical parameters appear to be associated with fibrosis in NAFLD. Studies incorporating these variables into diagnostic tests have started to emerge. It is likely that accuracy will continue to improve with refinement of these diagnostic algorithms by the addition of novel biomarkers.
151 SERUM UNDERCARBOXYLATED PROTHROMBIN (PIVKA II) HAS AN INVERSE RELATIONSHIP WITH HEPATIC STEATOSIS
B. Baburajan, A. Li, U. Mahadeva, W. Tong, S. Ranjagaran, M. Shearer, G. Savidge, T. Wong.Departments of Gastroenterology, Haemophilia, Histopathology, and Virology, Guys and St Thomas’ NHS Trust, London, UK
Background and Aims: Hepatic steatosis is a condition with an increasing prevalence and can progress to hepatic inflammation and probably cirrhosis. The functional activity of vitamin K dependent clotting factors synthesised in the liver is dependent on the integrity of the microsomal γ-glutamyl carboxylation system. This converts the inactive protein precursors to their active forms. In the absence of adequate hepatic function, the precursors may be secreted into the systemic circulation and can be detected (Proteins Induced by Vitamin K Absence or Antagonism, PIVKA II). Previous studies have shown that PIVKA II estimation to predict subclinical coagulopathy in liver failure, and may predict prognosis on treatment in hepatocellular carcinoma. The aim of the present study is to determine the relationship between PIVKA II levels and hepatic steatosis.
Methods: We studied PIVKA ΙΙ levels in 85 patients investigated for abnormal liver function tests who have had liver biopsies. The biopsies were assessed and reported by a pathologist blinded to the PIVKA II measurements, and steatosis was graded as absent, mild, moderate or severe. Fibrosis was graded 0–4. PIVKA levels were measured by enzyme linked immunosorbent assay (ELISA). Patients with biliary stasis or obstructive jaundice were excluded.
Results: Of the 85 patients, 25 had chronic hepatitis C, seven chronic hepatitis B, one SLE, two auto immune hepatitis, 12 alcoholic liver disease, five methotrexate induced liver fibrosis, and one sarcoidosis. Patients with no steatosis on liver biopsy had a significantly higher PIVKA level) when compared with patients with severe steatosis (1.27 v 0.43, p = 0.01). PIVKA ΙΙ levels did not correlate with hepatic fibrosis.
Conclusion: These preliminary results may indicate an augmented mechanism of vitamin K metabolism in the presence of hepatic steatosis. Whilst PIVKA did not correlate with fibrosis it maybe a useful non-invasive marker of hepatic steatosis and warrants further investigation.
152 ELEVATED ALANINE TRANSAMINASE LEVEL IN NEWLY DIAGNOSED TYPE 2 DIABETES IS ASSOCIATED WITH OBESITY AND HIGH TRIGLYCERIDE LEVEL AND NOT GLYCAEMIC CONTROL
E. J. Williams, P. W. Thomas2, M. G. Masding (introduced by J. A. Snook)1.1Departments of Gastroenterology and Diabetes; 2Dorset Research and Development Support Unit, Poole Hospital NHS Trust, Longfleet Road, Poole, Dorset BH15 2JB, UK
Introduction: Type 2 diabetes is recognised as a risk factor for non-alcoholic fatty liver disease (NAFLD). We examined the incidence of elevated (>35 U/l) alanine transaminase (ALT), as a surrogate marker for NAFLD, in patients with newly diagnosed type 2 diabetes.
Methods: Retrospective analysis of ALT level and various routine metabolic parameters from 606 consecutive patients presenting to our district wide education sessions for newly diagnosed type 2 diabetics.
Results: ALT was elevated in 155 patients (25.6%, 95% CI 22.1 to 29.2). Individuals with elevated ALT tended to be older (mean difference 7.4 years (5.2 to 9.5) p<0.001), heavier (mean difference in BMI 2.0 kg/m2 (1.0 to 3.2), p<0.001), and more likely to be male (M:F elevated ALT 104:51, normal ALT (⩽35 U/l) 219:232, p<0.001), with higher triglycerides (median difference 0.2 mmol/l p = 0.001) and lower HDL cholesterol (mean difference 0.08 mmol/l (0.02 to 0.15), p = 0.001). There were no statistically significant differences between those with normal v elevated ALT in HbA1c (elevated ALT 7.18 (SD 1.45)%, normal ALT 6.97 (SD 1.26)), or total cholesterol (elevated ALT 4.97 (SD 1.09) mmol/l, normal ALT 5.00 (SD 1.18) mmol/l).
Conclusion: There is a high incidence of elevated ALT levels in our well defined population of newly diagnosed type 2 diabetics, but no significant correlation between ALT and glycaemic control. Rather, an elevated ALT is associated with increasing age, obesity, elevated triglyceride and lower HDL cholesterol levels. These observations are in keeping with the currently understood pathogenesis of NAFLD as a hepatic manifestation of the metabolic syndrome and may help identify individuals at increased risk of developing chronic liver disease who should be investigated further.
153 IS THE METABOLIC SYNDROME A USEFUL CRITERION IN THE DECISION TO BIOPSY IN NON-ALCOHOLIC FATTY LIVER DISEASE?
S. Barker, M. Farrant.Royal United Hospital, Combe Park, Bath BA1 3NG, UK
Introduction: NAFLD represents a spectrum of disorders with NASH only representing a stage within it. Liver biopsy at present is the only way of distinguishing those with NASH from fatty liver alone. It cannot be predicted reliably on clinical or laboratory grounds. Patients with NASH are at risk of progression of their disease and therefore need to be identified. A recent study showed that those with three or more criteria for the metabolic syndrome were at significantly increased risk of NASH rather than fatty liver alone.1
Aim: To measure the prevalence of the metabolic syndrome in patients with NAFLD and to verify that these patients are more likely to have histological features of NASH rather than fatty liver alone.
Methods: Patients referred to gastroenterology OP with abnormal LFTs and fatty liver on USS were reviewed. A full liver screen was undertaken. Alcohol and drug histories were taken to exclude other causes of liver disease. Those with three of five criteria for the metabolic syndrome and no other cause for liver disease identified were offered a liver biopsy.
Results: Forty six patients with fatty liver on USS and abnormal LFTs were identified from May 04 to June 05. Thirty seven were male and nine were female. Twenty two had three of more features of the metabolic syndrome and 21 of these under went liver biopsy. The results are shown in the table.
Abstract 140 Median time (in days) to resolution of RB, SF, and both RB and SF
Conclusion: 71% of patients biopsied in this study who had the metabolic syndrome had features NASH, with or without fibrosis. There is a need for criteria to distinguish those at greater risk of NASH and therefore at risk of progression of their liver disease. The metabolic syndrome may be a useful criterion and larger studies are needed to verify this.
Abstract 153
1
154 LAMIVUDINE IN ACUTE HEPATITIS B INFECTION: A CASE SERIES
R. Hussain, N. C. Fisher.The Dudley Group of Hospitals NHS Trust: Russells Hall Hospital, Dudley, West Midlands DY1 2HQ, UK
Background: Lamivudine is a nucleoside analogue that improves outcome in chronic hepatitis B infection. It is not licensed for other indications but may have a role in acute hepatitis B infection. We present here our experience of this treatment.
Methods: Case note review of patients treated between 2001 and 2004. We recorded clinical and serological findings at presentation and after treatment. Treatment protocol for patients with clinically severe hepatitis was lamivudine 100 mg daily for six months.
Results: Six patients were treated (median age 35 years, range 16–75; 5M 1F; five white, one south Asian). No patient had a prior history of liver disease. At presentation median ALT level was 1150 iu/l (range 468–5847) and median bilirubin level was 225 μmol/l (range 21–355). All patients were HBsAg and anti-HBc IgM positive; one was HBeAg positive. Hepatitis B DNA levels in four patients were <400, 2700, 72 000, and 80 000 iu/ml. Liver biopsy was done in two older patients and revealed active hepatitis without cirrhosis. After four weeks of lamivudine, ALT fell to a median of 116 iu/l (range 34–506) and median bilirubin was 21 umol/l (range 12–85). At 12 weeks liver function had normalised in all patients; median ALT was 25 iu/l (range 16–37) and median bilirubin was 11 umol/l (range 7–17). One patient was then lost to follow up; all remaining patients were HBsAg negative by completion of therapy at six months. No adverse effects of the treatment were reported and no patient had recurrent disease thereafter (median follow up 10 months, range 3–22).
Conclusions: This uncontrolled series suggests a favourable role for lamivudine in acute hepatitis B infection; further case series or controlled studies may help to confirm this.
155 RESISTANCE AND SENSITIVITY TO INSULIN AFFECT THE RESPONSE TO INTERFERON IN PATIENTS WITH CHRONIC HEPATITIS C
D. N. Samonakis1,2, M. Koulentaki2, C. Xidakis1, P. Manousou1, J. Moschandreas3, A. Voumvouraki2, M. Tzardi4, P. Antoniou1, E. A. Kouroumalis1,2.1Liver Research Laboratory, Faculty of Medicine, University of Crete, Heraklion, Greece; 2Department of Gastroenterology-Hepatology, University Hospital of Heraklion, Crete, Greece; 3Department of Social Medicine, Faculty of Medicine, University of Crete, Greece; 4Department of Histopathology, University Hospital of Heraklion, Crete, Greece
Aims: Insulin resistance (IR) is related to hepatic inflammation in patients with CHC infection. The possible association with fibrosis development and the response to treatment is under intense research; we therefore studied IR in patients with chronic hepatitis C (CHC) in relation to these parameters.
Patients and Methods: Seventy patients with biopsy proven CHC were included: 23 before any treatment, 18 with sustained virological response (SVR) after interferon and ribavirin, 19 non-responders, and 10 relapsers. We evaluated IR (HOMA-IR), sensitivity to insulin (Quicki) and β cell function (HOMA-B) of the patients and related to BMI, steatosis and Ishak’s stage; we also measured serum factors linked to fibrosis: laminin, leptin, hyaluronic acid, collagen IV and TGF-β.
Results: HOMA-IR was significantly lower (p<0.05) and Quicki higher (p>0.05) in those who responded to treatment compared to non-responders or relapsers. HOMA-B was found significantly lower in relation to steatosis and advanced fibrosis (p<0.05). Hyaluronic acid (395.9 (SD 63.5) v 182.1 (SD 24.3), p<0.0003) and collagen IV (65.8 (SD 11.4) v 38.5 (SD 2.2), p<0.0006) were statistically higher in advanced compared to early fibrosis, while laminin, leptin, and TGF-β did not have statistical correlation with fibrosis nor with response to treatment.
Conclusions: Resistance and sensitivity to insulin was related to the response to interferon treatment in patients with CHC, while β cell function correlated with steatosis and advanced fibrosis. Serum hyaluronic acid and collagen IV were the best discriminators between early and advanced fibrosis.
156 ACTIVATION OF EFFECTOR CD8+ T CELLS FROM THE LIVER TISSUE MICROENVIRONMENT IN PATIENTS WITH CHRONIC VIRAL HEPATITIS
P. T. F. Kennedy, A. Gehring, D. Patch, C. Selden, M. Rees1, G. Dusheiko, A. Bertoletti.The UCL Institute of Hepatology, London; 1North Hampshire Hospital, Basingstoke
Background: CD8+ T cells mediate liver damage and protection in hepatitis B and C virus infection. Activation of CD8+ T cells requires a primary signal through the T cell receptor with specific MHC class I–peptide complex. A secondary signal provided by co-stimulatory molecules, has been characterised in naïve-memory CD8+ cells present in lymph nodes and in the circulation. In contrast, co-stimulation of effector CD8+ cells in the liver microenvironment is ill defined.
Aim: To evaluate the role of the co-stimulatory molecules CD28 and NKG2D on T cell receptor mediated activation of intrahepatic CD8+ T cells in viral hepatitis.
Methods: Peripheral blood lymphocytes and intrahepatic lymphocytes from 30 patients with viral hepatitis were studied. Five patients undergoing resection of liver metastases were included as controls. Phenotypic NKG2D/CD28 expression on CD8+T cells was investigated. Functional study of CD28/NKG2D co-stimulatory ability was analysed in lymphocytes (intrahepatic and circulating) and in HBV-specific CD8+ NKG2Dhigh CD28low T cell clones.
Results: Intrahepatic CD8+ T cells phenotypically display increased NKG2D and low CD28 in patients with viral hepatitis. In contrast, circulating CD8+ T cells show a high level of CD28 positivity with low NKG2D expression. Consistent with this, CD28 has a profound co-stimulatory effect in the activation of circulating CD8+ cells, while the co-stimulatory effect of CD28/NKG2D is minimal on intrahepatic T cells. IL-15 however could induce NKG2D co-stimulation on purified intrahepatic CD8+ T cell. Furthermore, NKG2D had the ability to modulate antigen specific recognition of HBV specific CD8+ NKG2D+CD28-T cell clones.
Conclusions: Both phenotype and co-stimulatory requirement of intrahepatic and circulating CD8+ T cells differ. The NKG2D co-stimulatory function of intrahepatic CD8+T cell activation is IL-15 dependent. Cytokine profile of the liver microenvironment in chronic viral hepatitis can influence CD8+ T cell activation and disease profile.
157 NURSE CONSULTANT LED HEPATITIS C MANAGEMENT IN A LARGE DISTRICT GENERAL HOSPITAL
M. K. Nayar, P. Madigan, J. McLindon, R. Chandy.Department of Gastroenterology, Whiston Hosptial, Merseyside, UK
Aim: There is a growing role of hepatology specialist nurses in the management of patients with chronic hepatitis C. These benefits include patient education and support, patient adherence to treatment regimes and greater efficiency in the delivery of care.1, 2 We present our experience in the management of chronic hepatitis C in a large district general hospital (DGH).
Methods: We included all patients treated in our department for the treatment of Hepatitis C from 1992 to 2004. The patients were identified by the database maintained by the nurse consultant (PM).
Results: Thirty one patients were treated during this period. Mean age was 39.96 years (range 24–55) with a 2:1 male: female ratio (M, 21; F, 10). Mode of transmission were previous IVDU (23), blood transfusion (3) and no cause was identified in the rest. The distribution as per genotype was: 1A (12), 1B (1), 3A (15), 2A (1), and 4A (1). One patient had coexistent hepatitis B infection and four had alcoholic liver disease. Prior to treatment the mean alanine transaminase levels was 122. 48 IU/l (range = 15–474). Most patients (29) had liver biopsies performed by PM. Treatment was give in accordance with the BSG guidelines. All patients were followed up in the unit by PM and if necessary he also provided telephone advice. Thirty patients received a combination of ribavarin and pegylated interferon. 24 patients completed the treatment with sustained virological response at six months. The reasons for non-completion of treatment were: non-responders, 5 (3, 1a; 1, 3a; and 1, 4a); non-compliance, 1; and severe depression, 1.
Conclusion: Majority of our patients were compliant to treatment (97%). All patients were satisfied with the information and care provided by the nurse consultant during treatment. This study emphasis the importance of specialist nurses in the management of chronic hepatitis C infection.
1
2
158 SERIAL MEASUREMENTS OF HYALURONIC ACID: A USEFUL MARKER OF CIRRHOSIS IN HEPATITIS C
N. C. McAvoy1, R. Dennis2, P. C. Hayes1.1Liver Unit, and Thrombosis; 2and Haemophilia Centre, Royal infirmary of Edinburgh, UK
Background and Aim: Hyaluronic acid (HA) is a linear polysaccharide that has been shown to correlate with fibrosis in patients with chronic hepatitis C. The use of serial measurements in monitoring fibrosis over time has not been established. The aim of this study was to evaluate the usefulness of serial HA measurements in predicting cirrhosis in hepatitis C haemophilia patients.
Method: Single centre retrospective observational study. We identified 97 haemophilia (A or B) or von Willebrand patients with active or past hepatitis C infection. From this group we selected 19 patients with at least three serial HA measurements of which at least one value was >100 (group 1) and 10 patients who had serial HA levels persistently <100 (group 2). Only HA levels measured after 1998 were included as the assay was changed at that time. Patients were classified as cirrhotic based on a combination of clinicopathological parameters including ALT/platelet ratio index (APRI) ⩾2.0, AST/ALT ratio ⩾1.0, U/S evidence of portal hypertension or histology. Hepatitis C PCR status was also recorded.
Results: In group 1 (18 males: 1 female), mean age was 50 (range 28–77 years) and Hep C PCR was positive in 11. 13 patients had previously undergone treatment for hep C. The mean HA over a median four year follow up period was 112. In those in whom HA values were persistently >100 (at least two consecutive values) (n = 10; group 1a), eight (80%) were classified as cirrhotic. In those in whom HA was >100 once or intermittently (not consecutive values) (n = 9; group 1b) none were classified as cirrhotic. Of the two patients in group 1a classified as non-cirrhotic one had severe arthropathy and the other was one of two with HIV.
Conclusion: In haemophilia patients with serum HA levels persistently >100, cirrhosis is generally present. In those in whom HA is <100 or intermittently >100, cirrhosis is generally absent. Serial measurements of HA are more value than single HA estimations.
159 HEPATITIS C CARE: ARE WE ACHIEVING WHAT WE THINK? REPORT FROM A SINGLE CENTRE VIRAL HEPATITIS CLINIC 1995–2004
M. Neilson, T. Joyce, A. J. Stanley, E. Forrest, J. Mackie, A. J. Morris.Glasgow Royal Infirmary, Glasgow, UK
Aims: To report the clinical and treatment outcomes of hepatitis C patient care in a single centre hepatitis C service.
Methods: We prospectively recorded demographic information, hepatitis status, liver biopsy results, and treatment outcomes on a viral hepatitis database.
Results: 1235 patients with viral hepatitis were referred; hepatitis C, n = 1185 (96%); hepatitis B, n = 50 (4%). HCV genotypes were known in 453 cases; 209 (46%) genotype 1; 244 (54%) genotype 2 and 3. Liver biopsies were performed in 228 patients, 25 (11%) cirrhotic. Of patients attending, nine (1.03%) developed hepatocellular carcinoma and 44 (5.04%) died of which 14 (32%) were related to liver disease. 691 patients (56%) have been discharged from the service due to non-attendance. The table shows sustained response (SR) rate to three treatment regimes.
Conclusions: (1) Treatment response rates in clinical practice were lower than published data. In particularly only 16% of HCV genotype 1 patients achieved sustained response. (2) An overall 5.04% mortality rate, with 1.6% liver related deaths was observed in those attending. (3) The high non-attendance rate indicates the need to establish alternative methods of delivery of care.
Abstract 159
160 EUROPEAN LIVER FIBROSIS MARKERS ACCURATELY DISTINGUISH FIBROSIS SEVERITY IN CHRONIC HEPATITIS C
J. Parkes1, R. Cross2, S. Harris1, S. Ryder3, W. Irving3, A. Zaitoun3, TheTrent Hepatitis C Research Group3, W. M. C. Rosenberg1,2.1The Liver Group, University of Southampton; 2iQur Limited, MP811 Southampton General Hospital, Southampton; 3Queens Medical Centre, University of Nottingham, Nottingham, UK
Introduction: Liver biopsy is the reference method for assessing liver fibrosis. However this is painful, hazardous, costly, and inaccurate as it is subject to significant sampling error and problems with processing and interpretation. The quest for accurate non-invasive markers of liver fibrosis has led to the development of a panel of highly sensitive serum ELISA assays that measure matrix components and enzymes involved in their turnover. We have previously shown that these European liver fibrosis (ELF) markers are accurate in assessing liver fibrosis in a range of chronic liver disorders. Here we present the validation of the performance of the ELF makers in an independent cohort of patients with chronic hepatitis C (CHC).
Methods: Subjects were 173 patients with CHC in the Trent Cohort, naïve to antiviral treatment, for whom serum samples were available and linked to a liver biopsy obtained within six months. All biopsies were scored by a single pathologist using the Ishak staging system. TIMP-1, PIINP, and HA were measured in the samples, all of which were anonymous to the investigators. Discriminant scores (DS) were derived using the published ELF algorithm. The area under the curve (AUC) for receiver operator characteristic curves was measured along with sensitivity (Sens) and specificity (Spec) for distinguishing between different degrees of severity of fibrosis.
Results: See table.
Abstract 160
Conclusion: The ELF markers can be used in the assessment of liver fibrosis in CHC either as an adjunct to, or in place of liver biopsy where appropriate.
161 AN EPIDEMIOLOGICAL STUDY OF HEPATITIS C GENOTYPE RELATED TO URBAN/RURAL LIVING
R. J. Oakey, M. J. Dibb, A. D. Higham, C. M. Brown, J. J. Keating.Morecambe Bay NHS Trust, Ashton Road, Lancaster LA1 4RP, UK
Background: Little is known about the geographic breakdown of hepatitis C genotypes between urban and rural areas. We analysed the genotype of all hepatitis C positive patients attending the liver clinic at Lancaster Royal Infirmary and Furness General Hospital between 1997 and 2004. Results of the genotyping were then geographically mapped according to postcode.
Methods/Results: 105 patients were studied. There was a noticeable increase in the numbers of patients diagnosed during 2000 and 2001 (24 and 18 patients respectively). 44.8% of patients (n = 47) were genotype 3a, 43.8% (n = 46) were genotype 1 with the reminder being genotype 2 or other subtypes. Only a small number of patients (n = 10) lived in rural postcodes. The majority of patients (n = 95) were clustered around urban areas.
There was no noticeable difference between the distribution of genotypes between urban and rural areas. The increase in numbers of patients diagnosed with hepatitis C during 2000 and 2001 may have been related to a co-existing research trial during that period and may indicate an underlying undiagnosed larger population with hepatitis C within Morecambe bay. The relatively higher incidence of genotype 3a in our patients has implications for local funding for Hepatitis C treatment. NICE guidelines currently recommend 48 weeks treatment with Ribavirin and Peg-interferon for genotype 1 disease but only 24 weeks treatment for genotype 2 and 3. According to the BNF the cost difference is £6199 (for a 70 kg man). Urban clustering may follow the fact that hepatitis C infection is largely contracted through IV drug use. Cheaper accommodation costs in the Northwest particularly in Lancaster, Morecambe, and Barrow may attract current or reformed drug users who are hepatitis C positive. Rural lifestyle is associated with a much lower prevalence.
Conclusion: Larger regional studies into the geographic breakdown of hepatitis C genotypes are needed to elucidate small trends within urban and rural areas.
162 LATE SPONTANEOUS CLEARANCE OF HEPATITIS C
P. H. Thurairajah, D. Hegazy, E. Kaminski, A. Demaine1, R. Cunningham2, M. E. Cramp3.1Peninsula Medical School; 2Department of Microbiology; 3Department of Hepatology, Derriford Hospital, UK
Background: Hepatitis C typically runs a chronic and protracted course with only 15% of individuals who clear the virus spontaneously in the acute phase. We present a patient who spontaneously cleared HCV after an established chronic infection and have examined his immune responses to HCV proteins using an Elispot assay.
Case report: A 44 year old former IVDU known to have been HCV Ab positive since 1998 and probably infected in the 1980s. In October 2002 he was admitted to hospital with an unexplained acute hepatitis. He was HCV RNA positive. His liver biochemistry showed parenchymal dysfunction with coagulopathy (INR 1.6, albumin 38, AST 1906, ALT 3906, Bili 177). Despite extensive investigations no clear cause was found for his acute hepatitis. His autoimmune profile, toxicology screen, Hepatitis A, B, E, and EBV serology were negative; however, before his illness he had received a flu vaccination. In November 2003 he represented with a further acute hepatitis. Once again investigations were unremarkable and he remained HCV RNA positive. One month earlier he had received a flu vaccination for winter. Liver biopsy from 2004 showed early bridging fibrosis but no inflammatory activity. Repeated testing for HCV RNA since 2004 has been negative.
Methods/Results: An Elispot assay was used to characterise HCV specific T cell responses to a range of HCV proteins. This showed responses to Core, NS3 and NS4.
Conclusion: Late spontaneous clearance of HCV is very rare. There is some evidence that influenza virus T cell responses can cross react with the HCV protein NS3. The temporal relationship between flu vaccination and our patients illness raises the interesting possibility that vaccine stimulated heterologous immunity resulted in a vigorous T cell response which helped to clear the virus.
Abstract 162
163 RESULTS OF COMBINATION TREATMENT WITH PEGYLATED INTERFERON AND RIBAVIRIN IN CIRRHOTIC PATIENTS WITH HEPATITIS C INFECTION
B. Höroldt, G. Haydon, K. O’Donnell, T. Dudley, P. Nightingale, D. Mutimer.Liver Unit and Wellcome Trust Clinical Research Facility, Queen Elizabeth Hospital, Birmingham, UK
Background: The treatment of hepatitis C patients with advanced cirrhotic liver disease remains challenging. These patients were excluded from the registration trials of pegylated interferon and ribavirin, so data on the outcome of treatment for this patient group are limited.
Patients and Methods: Between September 2000 and August 2004, 61 (42 male, age range: 29–69 years, 26 Asian) patients with either biopsy proven cirrhosis, or blood tests suggestive of cirrhosis, started treatment with pegylated interferon and ribavirin. None had evidence of significant hepatic decompensation at start of treatment.
Results: Forty three of 61 (70%) patients were serum HCV RNA negative at the end of treatment and 24 (39%) achieved a SVR. SVR was achieved for 35% (6 of 17) of patients with genotype 1, and for 39% (16 of 41) with genotype 3. Comparison of SVR rates for Asian versus white patients infected by genotype 3 demonstrated a higher cure rate for white patients (SVR observed for 10/18 = 56%) than for Asians (SVR for 6/24 = 25%). No female Asian patient achieved a SVR (9 treated). Failure to achieve SVR was associated with baseline features including a lower platelet count, neutrophil count, and albumin compared to those who achieved SVR. 22 patients (39%) did not finish the treatment course 10 patients decompensated clinically, five required hospitalisation. Two patients died. Patients who experienced hepatic decompensation tended to be older at baseline (>45 years) and to have baseline characteristics associated with more advanced liver disease.
Conclusion: The treatment of patients with advanced liver disease from hepatitis C is challenging, though a significant number can achieve a sustained virological response. Significant toxicity is experienced and there is treatment-related mortality. This balance of efficacy and toxicity needs to be considered before commencement of treatment. Older patients and those with more advanced cirrhosis should be told about the significant risk of hepatic decompensation.
164 WHY IS GAMMAGLUTAMYLTRANSPEPTIDASE ACTIVITY INCREASED IN PATIENTS WITH CHRONIC HEPATITIS C?
A. Lanzini, F. Benini, L. Bercich1, M. G. Pigozzi, L. Romanini2, P. Donati, A. Pozzi, F. Lanzarotto, C. Ricci.Gastroenterology Unit; 1Histopathology Unit; 2Radiology Unit, University and Spedali Civili, Brescia, Italy
Background: Serum gammaglutamyltranspeptidase activity (GGT) is often increased in chronic hepatitis C, a factor predicting poor response to antiviral treatment. The mechanism involved in this effect is unclear, although hepatic steatosis has been identified as a possibile cause in unselected patients. The aim of our study was to assess factors affecting GGT activity in patient with chronic hepatitis C by carefully selecting patients with no present or past hystory of alcohol intake.
Methods: We selected 63 consecutive patients with biopsy proven chronic hepatitis C and no history of alcohol consumption. We measured anthropometric parameters, insuline resistance (HOMA IR) and the conventional virological and serological liver tests. Liver histology was classified according to Knodell and hepatic steatosis according to Brunt. All patients were treated with PEG-interferon α 2-b (1.5 μg/kg/weekly) plus ribavirin (800–1200 mg/day according to body weight).
Results: Thirty eight patients had pretreatment GGT>1 the upper limit of normal, and 25 had values within the normal range. There was no difference in pretreatment viral load and genotype distribution among the two groups. Peptide-C (mean (SD): 2.98 (SD 1.66) ng/ml v 2.04±0.90 ng/ml, p = 0.0175), insuline resistance (2.83 (SD 1.9) v 1.79 (SD 1.12), p = 0.023), and hepatic steatosis score (0.78 (SD 0.5) v 0.22 (SD 0.43), p = 0.001) were significantly higher in patients with high than in those with normal GGT. Insuline resistance (r = 0.467, p<001), hepatic staging (r = 0.313, p<0.05) and steatosis (r = 0.399, p<0.007) were significantly correlated (Pearson correlation) with serum GGT. Hepatic steatosis was the only parameter independently correlated with serum GGT (r = 0.510, p<0.007) at multiple regression.
Conclusion: This study confirms that serum GGT is increased in a substantial proportion of patients with chronic hepatitis C that are not alcohol consumers. This effect is indipendent of virological characteristics and is attributable and is surrogate marker of hepatic non-alcoholic steatosis.
165 MANAGEMENT OF VARICEAL BLEEDING: A SINGLE CENTRE EXPERIENCE
J. Holmes, D. Tripathi, P. C. Hayes.Department of Hepatology, Royal Infirmary, Edinburgh, UK
Background/Aims: Variceal bleeding is an important. We aim to audit our current practice and assess the efficacy of our management strategies.
Methods: A retrospective study on the management of variceal hemorrhage in a single tertiary referral centre from April 2002–July 2004. 92 patients were identified using clinical coding. Data were collected and analysed in a dedicated database.
Results: The mean follow up was 11.4 (SD 12.2) months. The mean age was 52.8 (SD 14.9) years. The male to female ratio was 3:1. Alcoholic aetiology in 80%; Child’s grade (A/B/C, 10%/35%/55%). 90% of patients bled from esophageal varices alone whilst 10% bled from gastric and esophageal varices. 84% of patients had an endoscopy within 24 hours. 18% of patients were ventilated. Average time spent in intensive care was 1.6 (0–18) days, and total hospital stay was 13 (1–70) days. 38% of patients received vasoconstrictor therapy, while 86% of patients received antibiotics. The most used initial endoscopic therapy for acute bleeding was variceal band ligation (79%) followed by sclerotherapy (8%) and others (13%). 59% of patients went on to have TIPSS (70% in Child’s grade C), where there was failure of acute hemostasis or variceal rebleeding. The average volume of transfusion (blood) received by each patient was 4.5 (SD 4.9) units. Cumulative survival rates at 6 weeks, 1 year, and 2 years were 71%, 57%, and 53% respectively. Six week, 1 year, and 2 year rates of variceal rebleeding were 53%, 57%, and 61% respectively. Independent variables predicting poor survival were a Child’s score of >10 (p<0.001) and a creatinine >110 (p<0.001). Failure to administer antibiotics (p = 0.02) and a Child’s score >10 (p<0.05) were independent variables predicting variceal re-bleeding.
Conclusions: Our experience highlights the poor outcome of patients with variceal bleeding, especially within the first six weeks, which reflects the fact that most had significantly impaired liver function. The use of pre-endoscopic therapy, particularly antibiotics, needs to be optimised. A significant number of patients required a TIPSS. Adherence to recommended guidelines is essential and needs to be improved.
166 SPORADIC HEPATITIS E IS MORE COMMON THAN PREVIOUSLY THOUGHT: A SINGLE CENTRE EXPERIENCE
P. H. Thurairajah1, I. Samreen2, W. Stableforth1, R. Cunningham3, C. G. Teo2, H. Dalton4, J. Mitchell1.1Departments of Hepatology and; 3Microbiology, Derriford University Hospital, Plymouth; 2Virus Reference Department, Centre for Infections, Health Protection Agency, London; 4Gastrointestinal Unit, Royal Cornwall Hospital, Truro, UK
Background: Hepatitis E (HEV) is an oro-faecal borne viral infection which is endemic in parts of Asia. The incidence of autochthonous hepatitis E is poorly documented in the United Kingdom but one study estimated the sero-prevalence of anti-HEV IgG in London between 3.9% to 8.8%. A possible source of autochthonous infections is believed to be the UK pig herd in which there is an estimated sero-prevalence of 85%. We present nine cases of non travel associated HEV which occurred over the last 18 months. The incidence of HEV in our mixed urban and rural population is far higher than expected.
Results: Nine cases of unexplained hepatocellular jaundice tested positive for HEV IgM/IgG antibodies over an 18 month period, six of whom were PCR +ve. Three cases were PCR −ve but IgM and IgG titres were consistent with acute HEV. There were six males and the mean age was 66 (range 35–83) years. All cases exhibited symptoms of an acute hepatitis and made a complete recovery. All lived within a 10 mile radius from the shore but none lived in proximity to or worked on a farm. None had travelled to an endemic area. Four had regular contact with domesticated animals. All PCR positive cases were genotype 3 and phylogenetic analysis revealed high homology to HEV genomes infecting both sporadic HEV cases in the UK and to those seen in the UK pig herd.
Conclusion: The incidence of acute HEV amongst our catchment population is far higher than expected. The high sequence homology between these cases and those seen in the pig herd raise the possibility of zoonotic transmission. Hepatitis E virus is a public health issue in the United Kingdom.
167 A SYSTEMATIC REVIEW OF ACUTE HEPATITIS E VIRUS INFECTION IN A SEMI-RURAL POPULATION IN THE UK
E. N. Fogden, A. Shah, J. Gröning, M. J. Hall, S. Edmondson, R. A. J. Ransford.Department of Gastroenterology, County Hospital, Hereford Hospitals NHS Trust, Union Walk, Hereford HR1 2ER, UK
Background: Hepatitis E virus (HEV) infection in the UK has previously been considered an infection predominantly associated with travel to the HEV endemic and epidemic countries of Asia, Africa, and Mexico.
Methods/Results: HEV serology at County Hospital, Hereford (a semi-rural population of 220 000) was reviewed over a 12 month period (2004–05). Seven patients had evidence of HEV infection with four patients demonstrating acute HEV on serological testing and three showing evidence of past infection. Two acute HEV cases were elderly patients (ages 73, 85): one developed hepatic decompensation from cryptogenic cirrhosis and died from hepatorenal syndrome; the other developed fulminant liver failure complicated by a fatal myocardial infarction. The two other cases of acute HEV (ages 49, 61) presented with acute, severe viral hepatitis requiring admission to hospital with jaundice lasting 3–4 weeks and both patients subsequently made a full recovery. Only one of the four cases of acute HEV gave a history of recent foreign travel (Spain and Australia). In our review none of the cases of HEV were found to be associated with travel to recognised HEV endemic countries.
A previous report of 186 cases of acute HEV diagnosed in England and Wales between 1996 and 2003 revealed 17 cases with no history of recent foreign travel1 but identified risk factors of coastal and estuary settings and increased age.
Conclusion: HEV now appears to be endemic across the UK and acute HEV infection should be considered in all patients with acute viral hepatitis irrespective of a history of travel to HEV endemic countries. Acute HEV infection carries a significant mortality in elderly patients and is a risk factor for decompensation in chronic liver disease.
1
168 HEPATOTOXICITY ASSOCIATED WITH ATORVASTATIN USE
A. T. Clarke, P. R. Mills.Gastroenterology Unit, Gartnavel General Hospital, Glasgow, UK
Background: Atorvastatin, an HMG-CoA reductase inhibitor, is widely used in the treatment of dyslipidaemia. A transient rise in serum transaminases occurs in up to 3% of patients but this is usually self-limiting and inconsequential. Recent literature has indicated some potential for serious but rare idiosyncratic reactions related to this drug.
Methods/Results: We report seven cases of significant liver dysfunction related to atorvastatin use from one centre during the period 2002–05, with one death. No cases of hepatotoxicity with other statins were noted at this centre. A total of seven other patients are reported in the literature.
The 14 patients were usually over 60 years, had a female: male ratio of 2:1 and showed a mixed cholestatic/hepatocellular reaction. Six patients had marked hyperbilirubinaemia (>100 μmol/l). The daily dose of atorvastatin varied with five patients taking 10 mg, four 20 mg, one 30 mg, two 80 mg, and two unrecorded. Seven patients had liver biopsies with four demonstrating a cholestatic pattern and three a hepatitic pattern. The mean interval to onset of reaction was nine weeks and the liver often took several months to recover. Three deaths occurred.
In Scotland there were 0.91M prescriptions for atorvastatin and 1.62M for simvastatin in the year ending March 2005.
Adverse drug reaction reports from the UK Committee on Safety of Medicines reveal four deaths due to hepatobiliary disease with atorvastatin treatment over eight years. Simvastatin had no fatalities reported over 15 years and pravastatin one death in 14 years.
It is possible that atorvastatin is more likely than other statins to occasionally cause serious idiosyncratic hepatotoxicity. Mechanisms might include longer duration of action, drug interactions with CYP 3A4 or more pronounced lowering of LDL influencing membrane integrity.
Conclusion: While significant hepatotoxicity with atorvastatin remains uncommon, any persistent abnormality in liver function should be treated with caution.
169 HIGH PREVALENCE OF HISTOLOGICAL ABNORMALITIES IS COMMON IN INCIDENTALLY REMOVED GALLBLADDERS
K. Riyad, D. Subar, T. Mitchell, A. Hussaini, H. Vadeyar, D. Sherlock.North Manchester General Hospital, Manchester, UK
Introduction: Gallbladder disease accounts for a significant proportion of acute and elective surgery. Previous prevalence studies of gallbladder disease have been autopsy or radiological based and little detailed histological research has been reported. Cholecystectomy is carried out during liver resection as necessitated by the surgical technique. Our aim was to define the prevalence of abnormalities detected in these incidentally removed gallbladders.
Methods: 228 liver resections were carried out between January 2000 and December 2003. We excluded gallbladders removed in cirrhotics for hepatocellular carcinoma, cholangiocarcinomas or those with colorectal metastasis within 5 cm of the gallbladder bed. Statistical comparisons were made between prevalence of abnormalities between age, sex, and preoperative chemotherapy.
Results: 155 gallbladders (96 males/59 females; mean age 60.9, SE 59 to 69) were included. 66/155 (43%) had abnormal histology including chronic cholecystitis and cholesterolosis and 13% of the total had incidental gallstones. No statistically significant differences were seen between age groups, sex or with preoperative chemotherapy.
Conclusions: High prevalence of abnormalities exists in gallbladders removed incidentally at time of liver resections. Whilst the prevalence of gallstones is comparable to published autopsy series, the degree of histological abnormalities is unexplained and may represent changes in the natural history. Chemotherapy does not seem to alter the prevalence of chronic inflammation. Prevalence of abnormal histological features seems to be significantly higher than previously appreciated and may reflect the existence of undiagnosed abnormalities in the general population.
170 ASSOCIATION BETWEEN COELIAC DISEASE AND PRIMARY BILIARY CIRRHOSIS
K. Baird, D. Das, Y. Reddy.Department of Gastroenterology, Stepping Hill Hospital, Stockport, UK
Introduction: Coeliac disease and primary biliary cirrhosis are thought to be associated with each other, since they share similar autoimmune features. Many studies have sought to prove a definite link between these two diseases, but the results are often conflicting. This small systematic review seeks to summarise the findings of several studies to aid in the investigation of a link between coeliac disease and primary biliary cirrhosis.
Methods: A comprehensive search was undertaken in MEDLINE (1966 to June week 1 2005), EMBASE (1980 to 2005 week 24), CINAHL (1985 to June week 1 2005), and SIGLE databases. Studies meeting inclusion criteria were critically appraised using a self-designed appraisal form based on several epidemiological and prognostic checklists. The results of these studies were collated allowing for an overall estimated prevalence to be calculated, which was analysed using the χ2 test.
Results: Eight articles reported the prevalence of coeliac disease among patients with primary biliary cirrhosis, which revealed that coeliac disease was more common in the primary biliary cirrhosis group when compared to controls (0.28% v 0%, p = 0.01). Two articles reported the prevalence of primary biliary cirrhosis amongst patients diagnosed with coeliac disease, both of which revealed that primary biliary cirrhosis was more common in the coeliac group compared to controls (0.24% v 0.05%, p<0.0001).
Conclusions: There is a statistically significant association between coeliac disease and primary biliary cirrhosis according to this systematic review.
171 WITHDRAWN
172 DID CELTS REACH ROME ON THE EAST SIDE OF APPENNINI MOUNTAINS? AN OPEN POPULATION SCREENING STUDY FOR HFE GENE MAJOR MUTATIONS IN CENTRAL ITALY
E. Rosa Rizzotto1, A. Floreani1, D. Basso2, F. Navaglia2, I. Petridis3, O. Di Andrea4, R. Testa5, C. Marra5, M. Chiaramonte3.1Gastroenterology Department, Padova University, Italy; 2Laboratori Department, Padova University, Italy; 3Hepatogastroenterology Unit, L’Aquila University, Italy; 4Arsita GP, Italy; 5IRCS Ancona, Italy
Background: Two HFE genotypes are strongly associated with hereditary hemochromatosis (HH): homozygosis or the C282Y mutation and compound heterozigosis C282Y and H63D mutation seem to have a Celtic origin. It is still debated whether Celt migrations reached Italy on the east or on the west side of Appennini Mountains. According to the literature, the allele frequency of C282Y mutation decreases from Northern to Southern Italy, however in Central Italy there are no studies on HFE mutations.
Aims: To investigate the allele frequency of HFE mutations and the association between mutations and cases of HH or other liver diseases in an open population of Central Italy.
Patients and Methods: This study is part of a survey for liver and methabolic diseases in an open population of East Appenini. Arsita is a mountain village with a high rate of inbreeding and scarce exchanges with neighbouring areas. Its population likely derives from old latin groups. Five hundred and two subjects (299 F and 203 M), aged >18 years (1004 chromosomes), were tested for C282Y, H63D, and S65C mutations of the HFE gene by Taqman probes. All subjects had tested transferrin, ferritinemia, serum iron, liver function tests, HCV and HBV assay, Homa test. Information on alcohol intake and diet were collected with a questionnaire. Liver ultrasound was performed in 334 (66.5%) subjects. Data were analysed by logistic regression analysis.
Results: Allele frequencies for C282Y, H63D and S65C were 1.9%, 14.8%, and 0.01% respectively. Genotype distribution was within Hardy-Weinberg equilibrium for all the three mutations. C282Y +/− was found in 19 subjects (3.8%), H63D +/− in 127 (25.3%), H63D +/+ in 11 (2.2%), S65C +/− in 1 (2.0‰). No homozigosity for C282Y or compound mutation (C282Y/H63D) was found in the study population, however 27 subjects (5.4%) had TfSat >45 (including 10 subjects with high SF). Overall, 49 subjects (9.8%) were found HCV-RNA positive. Univariate analysis showed a significant correlation between SF and the following parameters: steatosis at ultrasound (any grade), alcohol intake (>40 g/day), insulin sensitivity (HOMA), age >45 years, BMI >25, and male gender. Logistic regression analysis indicated that male gender (p = 0.000) and hepatic steatosis (p = 0.017) were independent variables related to high SF.
Conclusions: This study confirms that C282Y HFE mutation is less frequent in Central Italy than in Northern Italy. This results are in favour of the hypothesis that Celtic groups never reached these mountain areas of East Appennini. HH in this area might be associated with other mutations on genes involved in iron metabolism.
173 DOES VENESECTION AND SUBSEQUENT IRON DEPLETION REVERSE ARTERIAL STIFFENING SEEN IN HEREDITARY HAEMOCHROMATOSIS?
W. J. Cash1, N. McDougall1, D. McCance2, I. S. Young3, M. E. Callender1.1Liver Unit; 2and Endocrinology and Diabetes Centre; 3Royal Victoria Hospital, Belfast and Queen’s University Belfast, Northern Ireland
Introduction: Increased cardiovascular risk has been associated with heterozygosity for the HFE gene and with states of iron overload, including hereditary haemochromatosis (HH). The mechanism could be either genetic or a direct effect of excess iron causing vascular dysfunction and increased arterial stiffening.
Aims: To assess the effect of venesection on arterial stiffness in HH.
Methods: We have used the non-invasive technique of pulse wave analysis (PWA) to study arterial stiffness in patients with HH. PWA uses applanation tonometry to record the radial artery pressure waveform non-invasively. Each waveform is composed of a forward and reflected wave. The compliance of the vascular tree can be expressed quantitatively as the augmentation index (AIx), following application of a validated transfer function, which is expressed as a percentage change in height of the pulse waveform as a result of the reflected wave.
Patients: The AIx of 10 patients (nine male) with haemochromatosis (diagnosed by homozygosity for the cys282tyr mutation or appropriate hepatic histology) was recorded following a 10 hour fast. Each patient then entered a standard venesection protocol and had subsequent AIx recordings taken at 6 weeks, 3 months, and 6 months under the same conditions.
Results: The mean AIx of the 10 patients dropped from 20.30% (SD 11.8) at initial attendance to 13.04% (SD 9.26) at six months representing a reduction in arterial stiffness over this time. There was a strong correlation between the reduction in serum ferritin and AIx, r2 = 0.85. There was no significant difference in other variables including blood pressure, body mass index, or smoking status during the study period.
Conclusions: These results confirm, using a non-invasive, in vivo technique that arterial stiffness diminishes during venesection for haemochromatosis. This suggests that it is the excess iron rather than other genetic factors which produces the vascular damage in haemochromatosis.
174 A PROSPECTIVE AUDIT INTO THE INCIDENCE, DIAGNOSIS, AND TREATMENT OF SPONTANEOUS BACTERIAL PERITONITIS IN CIRRHOTIC INPATIENTS WITH ASCITES IN A UK HOSPITAL
E. Pettitt1, M. Raza2, M. Brown1, J. Harding1, C. Challenor1, R. H. Heyderman2, R. L. Jones1.1Departments of Gastroenterology and 2Microbiology, Bristol Royal Infirmary, UK
Background: Spontaneous bacterial peritonitis (SBP) in cirrhotic patients with low protein ascites is often fatal. Early diagnosis, treatment, and secondary prophylaxis are indicated. Prophylaxis may cause microbial resistance. We prospectively audited local guidelines on diagnosis, treatment, and prophylaxis of SBP, monitoring local incidence, microbiology, and antibiotic resistance.
Methods: Clinical Audit Department registration was obtained. Admissions of cirrhotic patients with ascites were included and data including patient demographics and indications for and results of diagnostic paracentesis were collected. An ascitic PMN count of >250 mm3 was considered diagnostic of SBP, and “on admission” if performed within 24 hours of admission.
Results: Fifty admissions (42 patients, M = 28, F = 14, mean age 50.86 years) were included. SBP was diagnosed during nine admissions (18%) with 55.5% (n = 5) of cases diagnosed on admission. In 44.4% (n = 4) the causative organism was not identified. 100% (n = 5) of cases of culture positive SBP were isolated by injecting ascites into blood culture bottles. 44.4% (n = 4) were due to Gram negative infection. 11.1% (n = 1) were due to Gram positive infection. Two cases of quinolone resistance were identified.
Conclusion: There are no data on frequency and microbiology of SBP in the UK. SBP frequency in this unit is consistent with published rates from Europe and the USA. Of culture positive cases gram negative bacteria were most commonly identified. Inoculating ascites into blood culture bottles improves the yield and this guideline will be emphasised in our unit as a result of this audit.
175 MORBIDITY AND MORTALITY ASSOCIATED WITH ALCOHOLIC LIVER DISEASE FOLLOWING ADMISSION TO ST GEORGE’S HOSPITAL HDU/ICU
M. Cowan1, A. Tilliard2, M. Cook2, S. Clarke1, D. Forton1, T. M. Rahman1,2.1Departments of Gastroenterology; 2Intensive Care Medicine, St George’s Hospital, Blackshaw Road, London SW17 0QT, UK
Introduction: Alcoholic liver disease (ALD) is associated with significant mortality in the ICU setting. Decompensated liver disease with three organ dysfunction (OD) has a reported mortality of >85%. Much of these data are from transplant centres based on patients referred from other hospitals. It is likely they have had organ(s) failure/dysfunction for sometime before referral.
Aims: We hypothesise that early admission to HDU/ICU and introduction of aggressive therapy would improve expected mortality.
Methods: We prospectively monitored patients with ALD admitted to the HDU/ICU for 11 months; clinical, biochemical, and physiological parameters were recorded, including Child-Pugh (CP), APACHE, and SOFA scores.
Results: See table.
Abstract 175
Conclusion: Increasing organ dysfunction associated with ALD leads to increasing morbidity and mortality. Mortality for the severe group is maximally 50%. This is markedly better survival than data from similar studies. We postulate that this difference is due early referral, admission, and aggressive treatment usually within 24 hours of organ dysfunction.
176 DECOMPENSATED ALCOHOLIC LIVER DISEASE: FACTORS ASSOCIATED WITH MEDIUM TERM MORTALITY FOLLOWING HOSPITAL DISCHARGE
E. McFarlane, C. Gellion, J. Jones, J. Skinner1, D. Gleeson.Liver Unit, Sheffield Teaching Hospitals; 1West Sheffield Primary Care Trust, Sheffield UK
Background: In patients with decompensated alcoholic liver disease (ALD), continued heavy drinking is associated with mortality. Whether continued drinking at a lower level affects mortality is unclear. Other determinants of medium term outcome are not well characterised.
Aim: Evaluation of factors associated with mortality over 1–4 years after diagnosis of decompensated ALD.
Methods: Review of records of 190 consecutive patients discharged from hospital following admission with first episode of decompensated ALD; phone calls as needed to patient, family, and GP. Drinking behaviour from discharge to 1/4/05 or to death was classified as: fully abstinent (grade 1), drinking below the safety limits (grade 2), reduced drinking but above the safety limits (grade 3), and failure to reduce previously heavy intake (grade 4).
Results: By Cox regression analysis, higher drinking grade, higher Townsend and Jarman social deprivation scores (available in the 130 Sheffield residents), and female sex were independently associated with mortality. With analysis confined to patients with grades 1–3 and grades 1–2, the association of mortality with drinking grade disappeared but that with social deprivation remained. Age and admission MELD score were not independently associated with mortality.
Conclusions: Following discharge from hospital, mortality in decompensated ALD is associated with failure to reduce alcohol intake, female sex, and social deprivation. Continued drinking below safety limits may not prejudice survival.
Abstract 176
177 DECOMPENSATED ALCOHOLIC LIVER DISEASE: ACCURACY OF GLASGOW, MELD, MADDREY, AND CHILD PROGNOSTIC SCORES
J. Kerss, E. McFarlane, J. Jones, D. Gleeson.Liver Unit Sheffield Teaching Hospitals, Sheffield, UK
Background: The Glasgow prognostic score (Forrest. Gut 2005;54:1174) may be more accurate that the MELD, Child, and Maddrey scores in predicting early mortality in patients with presumed alcoholic hepatitis (defined as ALD with serum bilirubin ⩾80 μmol/l).
Aim: Evaluation of these scores in prediction of early mortality in a broader range of patients with first presentation of decompensated ALD (defined as Child grade B or C).
Methods: Review of 198 patients presenting consecutively between 01/04/98 and 31/03/05, who did not receive corticosteroids. Predictive value of prognostic scores (calculated on admission (day 1) and on day 7) with respect to 28 and 84 day mortality was assessed by comparing areas under ROC curves (AUROC) and accuracy (ACC; = % of cases correctly assigned using published cut-off values).
Results: 28 and 84 day mortality was 12+2% and 21+3% respectively. The table shows results for prediction of 28 day mortality.
Abstract 177
For prediction of 84 day mortality, accuracies of the Glasgow, MELD, and Maddrey scores (82, 81, and 76% for day 1 values, 85,84 and 80% for day 7 values) were similar to one another but were greater (p<0.01) than that of the Child scores (57% for day 1 and 61% for day 7). Accuracy of the Glasgow score was not diminished by including patients with bilirubin <80 μmol/l.
Conclusions: Accuracy of the Glasgow and MELD scores is similar and is greater than accuracy of Maddrey and Child scores for prediction of early mortality in decompensated ALD. Accuracy of the Glasgow score is preserved in patients with serum bilirubin <80 μmol/l.
178 MORTALITY AND MORBIDITY TRENDS DUE TO ALCOHOLIC LIVER DISEASE IN A DISTRICT GENERAL HOSPITAL POPULATION IN NORTH EASTERN UK
S. Maitra, B. K. Chaudhury, M. Kurmani, K. D. Bhattacharjee, C. Berthou, S. K. Singh, V. Sathyanaryana, J. Vasani.Gastroenterology, University Hospital Hartlepool, Hartlepool, United Kingdom
Introduction: With the advent of International Classification of Disease tenth revision (ICD-10) ONS (Office of National Statistics) data until 2003 show that alcohol related death (ARD) is still on the rise and is second highest in northeastern part of the UK.1 Moreover alcoholic liver disease (ALD) and its related complications constitute a significant proportion of hospital admissions and prolonged hospital stay.
Aims and Methods: We aimed to ascertain the current mortality and morbidity trends from ALD in University Hospital Hartlepool (UHH), a small town in northeast UK with a population of approximately 90 000. ALD patients admitted during the period of January 2002 to December 2004 were identified using ICD-10 code K 70.
Results: Out of 99 patients (68 male; 31 female) majority, both sex inclusive, belonged to age group 40–60 years peaking at 50–60 years. There were 29 deaths (male 19; female 10) in the two year study period, equivalent to a death rate of 16.1 per 100 000 populations. Mortality rate was higher among younger age group, that is, 40–60 years (male 12; female 7), which conforms to the national ARD. Number of admissions (male 1.5; female 1.7) and mean hospital stay per year (male 17–27 days; female 21–31 days) were quite similar across all age groups in both male and female patients.
Conclusion: Mortality rate due to ALD in UHH is almost equal to total ARD rate in the area, as estimated in 2003 by ONS, which confirms that ALD is the major cause of all ARDs. Also mortality rate from ALD in UHH is twice in males than in females and younger age groups show a much higher mortality and morbidity trends as would be expected from current national trends.
1
179 DOES THE GLASGOW ALCOHOLIC HEPATITIS SCORE (GAHS) ACCURATELY PREDICT SURVIVAL IN SEVERE ALCOHOLIC HEPATITIS?
A. S. Austin, P. Kaye, G. P. Aithal, S. D. Ryder.Liver Units, Derby City General Hospital, Uttoxeter Road, Derby, DE22 3NE and Queens Medical Centre, Nottingham NG7 2UH, UK
Introduction: Approximately 30%–40% of patients with a discriminant function >32 die within six months but many physicians are reluctant to use corticosteroids because of the potential risk of steroid side effects in this patient population. GAHS has been developed to more accurately predict poor outcome.
Method: We identified 38 patients with a DF>32 who underwent transjugular liver biopsy. The GAHS was calculated from five parameters at admission (age, leucocyte count, bilirubin, prothrombin ratio, urea. Forrest, Gut 2003) and compared to survival at 28 and 84 days and to accepted histological features of alcoholic hepatitis scored semiquantitatively from 0 to 4.
Results: Only six patients received corticosteroids, 1/6 died within 84 days. Of six histological variables (steatosis, portal inflammation, lobular infiltration with neutrophils and monocytes, ballooning and Mallorys hyaline), only higher scores for Mallorys hyaline were correlated with the GAHS ⩾8 (Kendall U tab, p = 0.051).
Conclusion: A GAHS ⩽7 accurately predicts 28 day survival without treatment in alcoholic hepatitis (DF>32). The extent of Mallory’s hyaline deposition is the only histological feature that correlates with clinical predictors of survival.
Abstract 179
180 HETEROGENEITY OF LIVER HISTOLOGY IN SEVERE ALCOHOLIC HEPATITIS DIAGNOSED ON CLINICAL CRITERIA
A. S. Austin, P. Kaye, G. P. Aithal, S. D. Ryder.Liver Units, Derby City General Hospital, Uttoxeter Road, Derby, DE22 3NE and Queens Medical Centre, Nottingham NG7 2UH, UK
Introduction: Recent studies suggest up that up to 20% of patients thought to have severe alcoholic hepatitis (AH) on clinical grounds will not meet histological criteria for this diagnosis (Ramond, 1992 #13; Spahr, 2002 #51). Furthermore, it is possible that patients with a discriminant function greater than 32 may have a severe histological lesion yet do not manifest the clinical criteria and might be denied treatment if a biopsy is not undertaken. We sought to compare the histological findings in jaundiced patients with a discriminant function greater than 32 with and without clinical stigmata.
Method: Transjugular liver biopsies from jaundiced patients with alcoholic liver disease (ALD with DF>32, n = 36, group 1) and 21 controls with stable ALD (bilirubin <100, group 2) were scored semiquantitatively from 0 to 4 for four histological features of AH by a single experienced liver pathologist. Clinical features suggestive of AH were tender hepatomegaly, leucocytosis >12 000/mm3, fever, hepatic bruit, and encephalopathy.
Results: Biopsies had median length 12–14 mm (3–28) and width 0.6–0.7 (0.4–0.9) and were similar between groups. All biopsies were cirrhotic (Ishak 6), had pericellular fibrosis consistent with an alcoholic aetiology and scored similarly for steatosis and cholestasis. The alcoholic hepatitis activity index (lobular neutrophils and monocytes, ballooning and Mallory’s) (AHAI–maximum score 16) was greater in the absence of clinical features (median 10 (2–13)) compared to the presence (8 (4–13)) (p = 0.483) and compared to controls (4 (1–9) (both p<0.001).
Conclusion: In jaundiced patients with severe alcoholic hepatitis the histological picture varies widely but there is no difference in liver injury/inflammation observed in groups with and without accepted clinical criteria. Clinical criteria should not be used to determine those suitable for therapeutic intervention.
181 “ALCOHOLIC HEPATITIS” AFTER GASTROINTESTINAL BLEEDING HAS A GOOD PROGNOSIS
H. Lafferty, V. Johnson, R. Keith, A. J. Morris, A. J. Stanley, E. H. Forrest.Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow, UK
Introduction and Aims: The management of alcoholic hepatitis (AH) remains controversial. Trials of treatment have variably included or excluded those patients who present with gastrointestinal (GI) bleeding. We aimed to look at patients with AH who were admitted with GI bleeding to determine whether the natural history of such patients is differs from those without GI bleeding.
Methods: We retrospectively examined the records of patients presenting with GI bleeding who developed a clinical picture in keeping with AH: a history of excess alcohol in last four weeks, serum bilirubin ⩾80 μmol/l, AST <500 iu. The modified Discriminant Function (mDF) and Glasgow Alcoholic Hepatitis Score (GAHS) were calculated on admission and two days after stabilisation from the GI bleed. Outcome at 28 days was determined and a comparison was made with a historical control group with a clinical diagnosis of AH without GI bleeding (n = 163). Neither group received corticosteroids or pentoxifylline.
Results: Forty patients were identified of whom 28 (70%) were male and three of whom had coexistent chronic hepatitis C. Variceal haemorrhage occurred in 32 (80%) patients and three patients required a TIPSS. Two days after stabilisation 35 (87.5%) patients had a mDF ⩾32 and 15 (37.5%) had GAHS ⩾9. Overall survival at 28 days was 90%. Kaplan-Meier analysis demonstrated a significant 28 day survival advantage for patients presenting with GI bleeding compared with non-bleeding historical controls for patients with a mDF ⩾32 (87% v 65%; p = 0.0077) and a GAHS ⩾9 (80% v 41%; p = 0.0143).
Conclusions: The 28 day outcome of patients with apparent AH 48 hours after stabilisation from a GI bleed appears to be significantly better compared with those who do not present with GI bleeding. Standard clinical criteria for the diagnosis of AH may not be applicable to this group of patients and such patients might be best excluded from clinical trials of AH treatments.
182 CONTRAST ENHANCED ULTRASOUND SCAN IN THE MANAGEMENT OF FOCAL LIVER LESIONS
K. Pujar, R. Marudanayagam, D. Cochlin, N. Kumar (introduced by B. Hawthorne).University Hospital of Wales, Cardiff, UK
Background: Focal liver lesions (FLL) present a diagnostic and management dilemma for almost all specialities of medicine including surgery, general medicine, general practice, and gynaecology. This study evaluates the sensitivity, specificity, positive and negative predictive values, and accuracy of contrast enhanced ultrasound (CEUS) in the assessment of focal liver lesions (FLL).
Methods: 109 patients attending the Cardiff Liver unit at the University Hospital of Wales, Cardiff, between 01/10/03 and 01/05/05, who were found to have focal liver lesions underwent Contrast enhanced ultrasound with Sonovue as the contrast. The results of the scan were analysed retrospectively in comparison with the gold standard investigation like CT scan, MRI, or PET scans and histopathology if the patients were operated on.
Results: The accuracy of CEUS in diagnosing FLL as hepatocellular carcinoma is 100%, metastases is 97%, cholangiocarcinoma is 99%, haemangioma is 100%, focal nodular hyperplasia is 99%, and as benign condition is 97%.
Conclusions: Our results suggest that CEUS should be considered as a standard investigation in every patient with incidental FLL.
183 IS INSERTION OF UNCOVERED TRANSJUGULAR INTRAHEPATIC PORTO SYSTEMIC STEM SHUNTS REALLY A RISK FACTOR FOR DEVELOPMENT OF HEPATOCELLULAR CARCINOMA?
N. Kochar1, D. Tripathi1, T. E. Delahooke1, D. N. Redhead2, H. Ireland2, P. C. Hayes1.1Departments of Hepatology; 2Radiology, Royal Infirmary of Edinburgh, UK
Introduction: Hepatocellular carcinoma (HCC) is a major complication of cirrhosis which necessitates surveillance by regular ultrasound examinations and alfafetoprotein measurements. A recent retrospective study reported an increased incidence of HCC in cirrhotic patients with uncovered transjugular intrahepatic porto systemic stem shunts (TIPSS).1
Aim: To determine whether the patients treated with non-covered TIPSS for complications of cirrhosis have higher incidence of HCC.
Methods: Retrospective study; patients identified from a dedicated database. Inclusion criteria: Patients with uncovered TIPSS with ⩾6 months of follow up. Exclusion criteria: HCC diagnosis within 6 months of TIPSS, <6 months follow up, deaths/transplants with in 6 months of TIPSS.
Results: Of 732 TIPSS insertions over a 14 year period, 518 were uncovered stents, of which 203 were excluded due to various exclusion criteria. Of the remaining 315, HCC was diagnosed in eight patients (median age 64 years). Aetiology of cirrhosis: alcohol, 7 and hepatitis C, 1; Child’s A/B/C –1/2/5. Indication for TIPSS: variceal bleed, 6 and ascites, 2. Median time from TIPSS to HCC diagnosis was 36.5 (18–89) months. Five patients have died and one has had a transplant at a median of 8 (1–32) months. Cumulative rates of HCC diagnosis at 1, 3, and 5 years were 0.3%, 1.8%, and 2.5% respectively compared with 3%, 24%, and 34% as reported in the recent study.1
Conclusions: We could not find an increased incidence of HCC in patients with uncovered TIPSS, when we compared it with the HCC incidence in patients with cirrhosis of any aetiology (1–3% per year).2 Higher frequency of HCC surveillance is probably not indicated.
1
2
184 NEOADJUVANT THERAPY WITH OXALIPLATIN BASED REGIMENS FOR DOWNSTAGING OF COLORECTAL LIVER METASTASIS DOES NOT REDUCE VIABILITY OF HEPATOCYTES
K. Riyad1, C. Pattenden2, D. Subar1, J. Trafford2, C. Brailsford2, S. Kingston2, G. Crees2, R. Patel2, S. Peak2, M. Saunders3, H. Vadeyar1, D. Sherlock1.1North Manchester General Hospital, Manchester; 2United Kingdom Human Tissue Bank (De-Montfort University), Leicester; 3Christie Hospital, Manchester, UK
Introduction: Significant steatohepatitis has been observed both macroscopically and microscopically in patients receiving oxaliplatin based neo adjuvant chemotherapy for downstaging of colorectal liver metastasis with concerns about impairment of liver regeneration. We compared the viability of hepatocytes (and cells/gram of digested liver) in patients who had received oxaliplatin and those who were chemotherapy naïve.
Methods: All patients with colorectal liver metastasis who underwent liver resection between January 2003 and June 2005 and had a specimen of normal liver analysed and cultured by UKHTB were included in the study. Two sample t test was used to compare the mean percentage of viable cells (and cells per gram of digested liver tissue) between the group that received oxaliplatin based neo adjuvant chemotherapy and the group that was chemotherapy naïve.
Results: Eighty seven liver samples (11 oxaliplatin group/76 chemotherapy naïve) were included in this study. The two groups were similar in age and sex distribution. The mean percentage of viable cells in the chemotherapy naïve group and the oxaliplatin group was 78.28 and 82.28 respectively though this was not statistically significant with a p value of 0.275 (95% confidence interval: −11.2 to 3.2). No difference was noticed in the postoperative biochemical profile between the two groups or length of stay in hospital.
Conclusions: Oxaliplatin based neoadjuvant therapy does not reduce the viability of hepatocytes or alter the post operative course of liver resection.
185 PREVALENCE AND MANAGEMENT OF ANAEMIA AFTER LIVER TRANSPLANTATION
C. Preston, V. Mills, M. Arundel, A. McVerry, C. Millson.Department of Hepatology, St James’s University Hospital, Leeds, UK
Background: Anaemia is well recognised after solid organ transplantation. Specific data on its prevalence in adults after liver transplantation are not available and little is known about how to manage anaemia during long term follow up post-liver transplant.
Aims: To investigate the prevalence of anaemia in our post-transplant population during long term follow up. To establish a pragmatic algorithm for the management of this anaemia and to assess whether our current practice approximates to this algorithm.
Methods: We identified all post-transplant patients under follow up in this institution who were more than six months post-transplant. We included them in our analysis if they were found to be anaemic. We defined anaemia as Hb<12 in males, Hb<11 in females, persisting for six months or more. Patients’ notes were examined to determine the following: (1) Has the anaemia been noted? (2) Have relevant aspects of the history been sought? (3) Have basic blood tests been performed? (4) If iron deficient, have endoscopic investigations been considered? (5) Has a referral to a haematologist been made?
Results: Sixty five patients fulfilled criteria. This represents 14% of the total post transplant population of 456. The average age was 52 years (range 27–78 years). Mean Hb = 9.8. The anaemia was noted in 36/65 (55%). All 65 patients were on potentially myelosuppressive medications. Haematinics were measured in 22/36. 24/36 underwent endoscopic investigations. 7/36 patients were referred for a haematological opinion. The aetiology of the anaemia was multifactorial and included; myelosuppressive medications, iron deficiency, and hypersplenism.
Conclusion: Anaemia after liver transplant represents a significant problem in our in our institution with a prevalence of 14%. Our review identifies shortfalls in our current approach to these, patients probably due to the lack of existing information about how this problem should be managed. We intend to implement the management algorithm used in our study in the outpatient setting.
186 POSTOPERATIVE COURSE AFTER LIVER RESECTION IS NOT INFLUENCED BY THE USE OF PORTAL INFLOW COMPRESSION (PRINGLE’S MANOEUVRE)
V. Patil, M. Ali, K. Riyad, D. Subar, H. Vadeyar, D. Sherlock.North Manchester General Hospital, Manchester, UK
Introduction: Portal inflow compression (PIC) is used to reduce blood loss at the time of parenchymal transection though hepatic ischaemia with reperfusion injury has been a theoretical possibility. Emerging evidence seems to indicate intermittent PIC may precondition the liver to tolerate ischaemia with some hepatoprotection. Our aim was to compare the post operative recovery and outcome of patients who had PIC at the time of major liver resection (>2 segments) with those who did not.
Methods: The biochemical and haematological data of patients were recovered from our prospectively maintained database for the period from January 2004 to June 2005. All patients who had undergone a major liver resection were included in our study. The change in haemoglobin concentration, the perioperative blood transfusion, liver function test, and coagulation profile were all compared between the two groups along with length of hospital stay.
Results: A total of 102 (81 with no PIC v 21 with PIC) were included in the study. The two groups were similar in age and sex distribution and type of liver resection. The postoperative course did not show any statistically significant difference in peak elevation of liver function tests, change in haemoglobin concentration, postoperative morbidity, and length of hospital stay. The blood product transfusion rates were similar in both groups with no statistically significant difference.
Conclusions: PIC does not seem to influence the postoperative recovery of patients undergoing liver resection and can be safely used without fear of postoperative hepatic dysfunction. However there seems to be no difference in the perioperative blood usage in both groups. PIC is a safe technique to be used in liver resection.
187 ANTHROPOMETRIC MARKERS AND OUTCOME FROM LIVER TRANSPLANT
D. G. Oliver, J. Barbour, B. Davidson, D. Manas, N. P. Thompson.Freeman Hospital, Newcastle-upon-Tyne, UK
Introduction: Malnutrition is common among patients undergoing liver transplantation and is often difficult to quantify because of confounding factors such as ascites and oedema. Anthropometric tests such as hand grip strength (GS), mid-arm circumference (MAC), triceps skin fold thickness (TSF) and mid-arm muscle circumference (MAMC) provide additional information. It is unclear whether poor nutrition is simply a marker for severity of liver disease or an independent and treatable risk factor for poor outcome.
Aims: To assess whether preoperative anthropometry in patients undergoing elective liver transplantation is associated with duration of time ventilated, stay on the intensive therapy unit (ITU) and hospital stay overall.
Methods: Retrospective study of patients transplanted for end-stage chronic liver disease.
Results: Nutritional records were obtained for 173 (72%) of 241 consecutive transplants between 1997 and 2005. Anthropometry had been performed during pre-transplant assessment in 72 (42%) patients. Indications for transplant were as follows: autoimmune liver disease 25 (35%), alcoholic liver disease 24 (33%), cryptogenic cirrhosis 6 (8%), viral hepatitis 2 (3%), other 15 (21%). Seven patients had co-existent hepatocellular carcinoma. 90 day and 12 month mortality were both 6%. Significant inverse relationships were found for MAC, TSF and MAMC with days spent on ITU (r2 = −0.26, p = 0.048; r2 = −0.28, p = 0.036; r2 = −0.26, p = 0.048 respectively) and for TSF with total days in hospital (r2 = −0.36, p = 0.007). The effect of nutritional status was more pronounced for those transplanted for alcoholic or cryptogenic aetiologies than for others. Patients who died within 90 days had higher initial MAC and MAMC than survivors (p = 0.04; 0.01 respectively). There was no relationship of nutritional markers with overall mortality. Model for End-Stage Liver Disease (MELD) score did not significantly correlate with nutritional status or with the outcome variables.
Conclusion: Nutritional status may influence outcome from liver transplantation independently of the severity of underlying liver disease but the overall effect is likely to be small.
188 PROGNOSIS IN ADULT PATIENTS WITH CHRONIC LIVER DISEASE REQUIRING ICU ADMISSION AND THOSE ADMITTED FOR TRANSPLANT ASSESSMENT
M. Austin, W. Bernal, G. Auzinger, E. Sizer, J. Wendon.Institute of Liver Studies, Kings College Hospital, London SE5 9RS, UK
Background: Multivariate analysis of 363 intensive care unit (ICU) admissions for advanced chronic liver disease (CLD) highlighted key organ failures (OF) as indicators of prognosis. In a cohort of patients admitted to the Liver Unit we examined presence of OF, scoring systems and outcome in patients admitted for liver transplant assessment (TP).
Methods: Consecutive patients with CLD admitted to ICU (09/99–03/05) and liver transplant assessment (01/05–10/05) were studied. Demographic features, severity of CLD and presence of key OF were reviewed in TP (n (%) or median (interquartile range)). Dataset validation is ongoing.
Results: Analysis of ICU patients revealed that cumulative cardiovascular, renal and neurological failure resulted in 100% mortality (p<0.0001). Other determinants: Age>50, Child Pugh (CP) class C and 1 key OF >70% mortality (p>0.0001). In 101 TP: 23% CP A, 44% CP B, and 31% CP C, MELD median 9 (6–33). 21% had no OF, 34% 1, 30% 2, and 16% 3 OF. The CP (p<0.01), MELD (p<0.001) and key OF (CNS p<0.008, CVS p<0.006, renal p<0.05) predicted outcome. Of TP 63% had renal dysfunction CrCl 67 ml/min (0–194). 45% had CVS dysfunction, 35% structural (LVH/cardiomyopathy) and 9% conduction abnormalities. 32% TP had CNS dysfunction. During the study period 9% died (70% all key OF) and 9% underwent liver transplantation.
Conclusions: Patients with CLD requiring admission to ICU with all key OF have 100% mortality. Those not requiring ICU admission have a high prevalence of organ dysfunction. Of the patients who died, 70% had three key OF. With ongoing data collection, these prognostic scores will to highlight the clinical importance of extrahepatic OF in the assessment of patients with CLD both on the ward and in intensive care.
Pancreas posters
189 EVALUATION ON A MEXICAN COHORT OF A UK COMPUTER MODEL DEVELOPED TO PREDICT SEVERITY OF ACUTE PANCREATITIS
C. B. Pearce1, J. A. Gonzalez-Gonzalez2, D. A. Garcia-Cantu2, S. R. Gunn3, C. D. Johnson1.1Southampton General Hospital Departments of Medicine and Surgery; 2Servicio de Gastroenterologia, Facultad de Medicina y Hospital Universitario UANL, Monterrey, Mexico; 3School of Electronics and Computer Science, University of Southampton, UK
Background: It has been reported (BSG March 2004) that a computer model using eight admission variables (age, C-reactive protein (CRP), respiratory rate, pO2 on air, arterial pH, serum creatinine, white cell count, and GCS) created using UK data can provide accurate severity prediction in acute pancreatitis (AP). An evaluation of this model on a dataset from a different geographical and social setting (Monterrey, Mexico) is presented. Severity and organ failure were defined by Atlanta criteria.
Method: Admission data were collected from 202 Monterrey patients with a diagnosis of AP between October 2002 and November 2004. The data were retrospectively evaluated using the UK computer model, and the area under the receiver operating characteristic curve (AUC) was used to evaluate its accuracy in predicting severity in AP.
Results: Forty two patients (20.8%) developed severe AP, and three died (1.5%). 11 patients (5.4%) developed renal failure, and 23 respiratory failure (11.4%). 146 patients had a biliary aetiology (72.3%), 25 alcohol (12.4%), 17 other aetiology (5.4%), and 14 idiopathic (6.9%). The UK model predicted severity in the Monterrey patients with an AUC of 0.81 (identical to the figure obtained previously in UK patients). This gives an optimum sensitivity and specificity of 0.80 and 0.77 and compares favourably with the CREED system developed in Mexico (AUC 0.70) and admission CRP (AUC 0.76; p = 0.001) in the same patients.
Comments: This system can give a prediction within a few hours of admission, and is more accurate than admission CRP or APACHE-II. The validation of the model on a separate cohort of patients confirms the merit of the computer assisted approach. A prospective multicentre study using the Southampton computer system is required.
190 MANAGEMENT AND OUTCOME OF ACUTE PANCREATITIS VARIES BETWEEN CENTRES
K. Ashfaq, P. Fee, D. Moothoo, B. Teague, L. Wood, K. Sanders, A. Goel, R. Sekhar, I. Crighton, J. Keating.Department of Medicine, Morecambe Bay Hospitals NHS Trust, Cumbria, UK
Introduction: National guidelines suggest pancreatitis should be managed as an acute emergency with severity scoring and stratification of patients with a high score to either HDU/ITU. In this study we compared the management and outcome of acute pancreatitis in two DGHs (RLI at Lancaster and FGH at Barrow in Furness). This retrospective study was undertaken between January 2003 and December 2004 and a total of 60 patients at RLI and 44 at FGH were reviewed.
Results: The groups were similar for age and sex. The aetiology of pancreatitis at RLI was gallstones 47% v 55% at FGH, alcohol 18% v 5%, idiopathic 23% v 18%; others including trauma and viral were 14% v 16%. Only 7% of patients at FGH v 55% at RLI had severity scoring done at 48 hours. A retrospective calculation revealed 36% at FGH had severe scores at any given time of which only 37% were admitted to HDU/ITU v 8% with severe scores at RLI of which 60% were admitted to HDU/ITU. Of the 28 patients with gall stone pancreatitis at RLI, three had scores consistent with severe pancreatitis. A total of 12 patients underwent ERCP of which two were from the severe pancreatitis group. At FGH 8/24 patients had severe gall stone pancreatitis. A total of two patients underwent ERCP, but none from the severe pancreatitis group. In the severe pancreatitis group 67% underwent ERCP at RLI v 0% at FGH. The overall mortality at FGH was 18% and in the severe pancreatitis group was 37% which was higher than the nationally accepted levels of 10% and 30% respectively. In contrast, the overall mortality at RLI was 2% and 20% in the severe group.
Conclusion: We conclude that severity scores are useful in stratifying patients for HDU/ITU treatment where appropriate. Patients who underwent ERCP for gall stone pancreatitis had a better outcome as reflected by the low mortality and higher number of ERCPs performed at RLI.
191 AUTOIMMUNE PANCREATITIS: RESPONSE TO THERAPY IN A UK SERIES
N. I. Church, S. P. Pereira, A. R. W. Hatfield, G. J. M. Webster.Department of Gastroenterology, University College Hospital, UCLH NHS Foundation Trust, London, UK
Background: Autoimmune pancreatitis (AIP) is a rare condition which usually presents with a pancreatic mass, biliary and pancreatic duct stricturing, jaundice, and a raised serum IgG4. A response to steroids is a diagnostic criterion, although historical data from our unit suggest that spontaneous improvement may occur. This is the first UK series of AIP patients in which objective responses to active treatment are reported.
Methods: All nine patients treated for AIP at our centre in 2004–05 were included. Intrahepatic/hilar stricturing was present in eight at diagnosis, and plastic stents for jaundice/dominant CBD/hilar strictures were sited at ERCP in five (although four patients remained jaundiced despite apparently optimal stenting). Oral prednisolone 30 mg OD was commenced in all patients, with gradual dose reduction over 4 weeks. In cases of disease relapse following steroid reduction, azathioprine was commenced. Response was assessed in terms of pre- and post-steroid symptoms, liver biochemistry and radiological appearances.
Results: Within 4 weeks of starting steroids, all patients reported significant symptomatic improvement. After 8 weeks, median bilirubin levels had fallen from 38 μmol/l (range 8–232) to 9 μmol/l (5–27), (p = 0.004 by Wilcoxon matched pairs test); median ALT from 88 IU/l (22–276) to 57 IU/l (26–76), (p = 0.008), and ALP from 496 IU/l (149–978) to 193 IU/l (64–424), (p = 0.004). Repeat ERCP (seven patients) and MRCP (two patients) after 3–6 months showed improvement in pancreatic and extrahepatic/intrahepatic biliary stricturing in all cases, with almost complete resolution in four. Biliary stents were removed in all cases, with no recurrence of jaundice (median follow up 4, range 3–12 months). CT/MRI showed resolution of mass lesions in three, and significant improvement in the rest. Eight patients remain on low dose steroids (range 3–12 months). Two patients relapsed on steroid dose reduction, with improvement on adding azathioprine. One patient discontinued steroids after nine months and has remained well.
Conclusion: Patients with AIP appear to show a good objective response to steroids. Disease relapse may occur following steroid reduction, but introduction of azathioprine may be of benefit. Further work is required to define the clinical course of this unusual condition, its aetiopathogenesis, and the optimal treatment regimen.
192 BILIARY STENTING VERSUS PALLIATIVE BYPASS SURGERY IN LOCALLY ADVANCED PANCREATIC ADENOCARCINOMA
E. N. Scott, C. Hoh, H. Doucas, W. P. Steward, D. M. Lloyd, G. S. Robertson, A. R. Dennison, D. P. Berry.University Hospitals of Leicester, UK
Background: The role of palliative bypass surgery versus biliary stenting in patients with locally advanced pancreatic cancer is controversial with no randomised study to date.
Methods: After exclusion of patients with resectable disease, 56 consecutive patients with proven pancreatic adenocarcinoma presenting to two units were studied. One unit advocated stent insertion for all patients unless there was evidence of gastric outlet obstruction. The other unit favoured palliative bypass surgery if there was no laparoscopic evidence of metastatic disease.
Results: Twenty three patients underwent palliative surgery and 33 patients underwent stent insertion. CA19.9 was the only significant demographic difference between the two groups (mean 5537.55 kU/l in stent group versus 2282.56 kU/l, p = 0.04). There was no difference in total admission duration. There was a lower emergency readmission rate for the surgical group (17% v 30%) and more surgical patients underwent chemotherapy (61% v 18%, p = 0.004). 30 day mortality for the surgical group was 4% v 18% in the stent group. There was a significant improvement in long term survival for the surgical patients with median survival of 382 days v 135 days in the stent group (log rank test p = 0.03).
Conclusion: These data suggest palliative bypass surgery improves long term survival with an acceptable procedure related mortality and support surgical exploration of patients with pancreatic cancer in the absence of metastatic disease.

Abstract 192, figure 1.
193 CT AND ENDOSCOPIC ULTRASOUND IN THE DIAGNOSIS AND STAGING OF PANCREATIC AND PERIAMPULLARY MALIGNANCY
S. D. Mansfield, J. Scott1, K. Oppong, D. L. Richardson1, G. Sen, B. C. Jaques, C. B. O’Suilleabhain, D. M. Manas, R. M. Charnley.Departments of Hepato-Pancreato-Biliary Surgery and 1Radiology, Freeman Hospital, Newcastle-upon-Tyne, UK
Introduction: Multislice CT, which offers improved scanning speed and resolution compared to conventional CT, was compared with endoscopic ultrasound (EUS) in patients with pancreatic and periampullary malignancy.
Methods: Prospective data collection on all suspected pancreatic and periampullary cancers between June 2002 and June 2004. Dynamic triple phase multislice CT and EUS were performed where clinically indicated. For quality reasons only in-house CTs were accepted for the analysis. Presence of malignancy, portal vein invasion and resectability were compared using McNemar’s test of paired proportions (table).
Abstract 193
Results: Of 345 patients, 134 underwent in-house multislice CT, 188 EUS and 84 both. Of these, 35 underwent laparotomy. The use of EUS guided fine needle aspiration was not assessed.
No significant difference was demonstrated between the modalities either in the whole cohort or when small tumours (⩽20 mm) were analysed separately. When the clinical impact was assessed EUS had most impact in the following groups of patients: benign on CT – 5/21, 23.8%; portal vein invasion on CT – 18/37, 49%; uninterpretable CT findings – 9/9, 100%.
Conclusion: Multislice CT is the primary imaging modality in assessing these tumours. EUS is not indicated in those patients in whom CT confidently demonstrates a resectable tumour. In those patients in whom CT suggests benign disease or borderline vascular invasion, however, EUS has an important role in determining resectability.
Endoscopy posters
194 DOES A TWO DAY ON-SITE REGIONAL TRAINING PROGRAMME IMPROVE COLONOSCOPY SERVICE IN A DISTRICT GENERAL HOSPITAL: A PROSPECTIVE STUDY
R. Guruswamy, D. Kejariwal, J. Dron, M. Williams, B. Brett.James Paget Hospital NHS Trust, Great Yarmouth, Norfolk NR31 6LA, UK
Background and Aims: Three national and seven regional training centres have been funded to support endoscopy training in England in view of the low national completion rate and the imminent Bowel Cancer Screening Programme. The aim of this study was to assess the effect of this training programme on our endoscopy unit.
Materials and Methods: A prospective audit of our colonoscopy service was undertaken between August 2003 and March 2005. After an initial data collection period of nine months, a two day on-site training course facilitated by the regional training centre was offered to all our colonoscopists using Magnetic Endoscopy Imager (MEI) in April 2004. The MEI was available for a further three weeks and the colonoscopists completed a questionnaire at the end. A grace period of three months then elapsed. Following this further audit data collection was continued for eight months until March 2005. Independent endoscopists who contributed to both study periods were included. Variables such as completion rate, sedation doses, and complications were compared between the periods.
Results: 93% of the colonoscopists felt that this would help improve their technique while 95% felt that the course had a significant impact on their sedation usage practise. Seven colonoscopists contributed to the study undertaking 408 and 569 procedures before and after the training. The mean adjusted completion rates were 82.3% (73.5–94.2%) before and 82.4% (62–95%) after the training. The mean pethedine doses fell from 43.3 mg to 34.38 mg and the mean sedative doses fell from 4.31 mg to 3.2 mg. Complication rates did not change (rectal bleeding in three patients and abdominal pain in four). There were no perforations or deaths.
Conclusion: Colonoscopists rated the course very high. There was a significant reduction in the doses of analgesics and sedatives used while maintaining the same caecal intubation rate. The sample size may be too small to detect changes in complication rates. Further training is required for some to improve our unit’s intubation rates.
195 PERCEIVED VALUE OF TEACHING COMPONENTS USED ON COLONOSCOPY TRAINING COURSES
A. I. Thuraisingam, J. T. Anderson.Cheltenham General Hospital, Cheltenham, Gloucester, UK
Background: Endoscopy training courses are a recommended component of learning endoscopy. Trainees often have their training recorded on video/DVD. It is unclear how trainees rate the different components of the training courses and in particular whether they value watching recordings of their own performance.
Methods: A questionnaire was sent to 62 trainees who had attended a colonoscopy course at least three months earlier. All trainees were from centres that gave trainees video recordings of their own performance. Trainees were asked to rate 11 possible course components on a 6 point Likert scale and comment on the use of video recording of their training.
Results: There was a 63% response rate and the course components were ranked as shown in the table. Less than half of trainees reviewed video of their own training while on the course. Although most trainees felt video recordings should be kept, 29% never watched their videos and of those who did the mean number of times recordings were watched was only twice.
Abstract 195
Discussion: There are potential benefits to using video feedback for endoscopy training but at present video appears under utilised. Its long term usefulness is also limited by data protection and patient confidentiality issues. The course components currently most valued by trainees are hands-on experience and the magnetic endoscopic imager.
196 ONE-TO-ONE HANDS-ON COLONOSCOPY TRAINING COURSE IMPROVES COLONOSCOPY PERFORMANCE
N. Suzuki, S. Thomas-Gibson, M. Vance, C. Fraser, D. Swain, G. Schofield, B. P. Saunders.St Mark’s Hospital, London, UK
Background: Poor performance and inadequate training in colonoscopy in the UK has been reported.1 Ten centres across the UK run intensive hands-on training courses but their efficacy has not been established.
Aim: To assess whether a four day course delivering one-to-one training can improve colonoscopy performance.
Methods: Forty one specialist registrars (24 physicians, 14 surgeons) and three nurses have individually attended the course since the unit became a national training centre (15 months). The course objectives were to increase core knowledge and improve the basic hand skills required for colonoscopy. Trainees attended three microteaching, two computer simulator, and four hands-on training sessions. They performed two multiple choice question (MCQ) papers (previously validated and shown to be of equal difficulty).2 Performance parameters measured at the beginning and the end of the course included the MCQ score, time taken to complete the simulator test cases and Direct Observation of Procedural Skills (DOPS) using 100 point visual analogue scales for all aspects of colonoscopy technique. Trainees completed an anonymous feedback form to evaluate the course content.
Results: The MCQ score significantly increased: mean score 56.6% v 65.7% (p<0.0001). Mean total time taken to complete simulator test case improved significantly from 700 seconds v 500 seconds (p = 0.02). Trainees performed a median number of 16 cases during the course. DOPS demonstrated an improvement in clinical skills. Pre and post course mean scores were: general approach 7.5 v 8.1 (p = 0.007), basic handling technique 5.9 v 6.7 (p = 0.002), understanding and control of looping 5.4 v 6.7(p<0.0001), caecal/ileal intubation 6.1 v 7.6 (p<0.0001) and extubation technique 6.5 v 7.7(p<0.0001) respectively. All trainees had a high level of satisfaction and found the hands-on training most beneficial.
Conclusion: This intensive course improves core knowledge and clinical skills in colonoscopy. One-to-one tuition maximises hands-on training which may accelerate the learning curve.
1
2
197 ENDOSCOPIC TRAINING AND ADVERSE OUTCOMES (30 DAY POST PROCEDURE MORTALITY): AN AUDIT OF 5715 PROCEDURES IN A LARGE TEACHING HOSPITAL
B. Doshi, K. Muckerjee, S. Sagi, M. Tedford, G. Sharma, A. Byrne, L. Brown, K. Jones, K. Bodger, R. Sturgess, S. Sarkar.Aintree Centre for Gastroenterology, University Hospitals Aintree, Liverpool, UK
Introduction: Although it is widely believed that endoscopy outcome is operator dependent, only recently have endoscopy training, quality, and adverse outcomes been pushed to the forefront of the political agenda. The two main reasons are; firstly, the NCEPOD report “scoping our practice”, and secondly, the imminent national bowel cancer screening programme. JAG and the Endoscopy Modernisation Agency have the task to improve endoscopy standards and training
Aim: To determine whether trainees and training in endoscopy has adverse patient outcomes as measured by the 30 day post procedure mortality (PPM).
Methods: 5715 consecutive endoscopic procedures were audited from 01/03/05 to 31/07/05 after being identified by endoscribe database. The hospital IT medway system and coding was used to identify patients that died (PPM).
Results: Forty seven different users (endoscopists) performed 5715 procedures; including 22 trainees (TR) (performed 18% (22% if included supervised)), 12 Consultants (CON) (perform 20% (26% if supervised included)), seven Non-Training Grades (NGT) (perform 27%), and six Nurse Specialists (perform 35%). PPM was 1.2% (n = 69; mean age 74.2 and ASA Score 3 (mode 4); all inpatients). This included 32 patients who had therapeutic procedures (48.5%). There was no difference in PPM when comparing procedures (alive and dead patients) that involved TR only with CON led (CON only plus supervised) procedures (3.4 v 2.2%; p = 0.5). When assessing the impact of training on PPM, there was a clear difference between procedures that involved TR (TR only and supervised) with other medical practitioners (CONS & NTG) (3.6 v 1.5%; p = 0.006). The overall percentage of the therapeutic procedures performed over the period within the NTG, TR only, TR involved, CON only, and CON led groups were 3.2, 23, 42, 73, and 70% and adjusted PPM were 0.9, 3.4, 3.6, 2.3, and 2.6% respectively. All fatalities in the TR only were performed by senior SpRs (year ⩾3).
Conclusions: Although there was no worse adverse outcome with trainees performing procedures without supervision (TR only), patients who had procedures that involved trainees (TR only + Supervised) did do worse. Furthermore these results are not adjusted for case mix or complexity. This highlights the ethical dilemma of training verses patient safety.
198 A REGIONAL OUT OF HOURS ENDOSCOPY SERVICE IS AN EFFECTIVE WAY OF PROVIDING COVER FOR GI BLEEDING ACROSS A NUMBER OF DIFFERENT HOSPITALS
M. Fullard1, M. Benson2, M. Mendall3, G. Lim4, S. Clark1.1Department of Gastroenterology, St George’s Hospital, London; 2Department of Gastroenterology, St Helier Hospital, Carshalton, Surrey; 3Department of Gastroenterology, Mayday Hospital, Croydon, Surrey; 4Department of Gastroenterology, Epsom General Hospital, Epsom, Surrey, UK
Background and Aim: In 2004, a region-wide out of hours endoscopy service for gastro-intestinal bleeding was introduced to cover five hospitals in South London (St George’s Tooting, the Royal Marsden Sutton, Epsom General Hospital, St Helier Hospital, and Mayday Hospital). We believe this to be a unique service. Year 4–5 SpRs cover all five hospitals, with consultant cover at each hospital as well as agreed referral criteria. A prospective audit was undertaken to assess the workload generated by the service and the outcome of endoscopies performed.
Methods: Over a two month period, the SpRs were asked to complete two forms each time they were on call, one detailing the calls received, the other clinical details of endoscopies performed.
Results: Data for 32 days (24 weekdays and 6 weekend days) were available. Forty four calls were received during this period, 26 during the week, 18 at weekends. 66% of calls were from St George’s Hospital. Seventeen calls resulted in out of hours endoscopy, 19 led to telephone advice being given about GI bleed patients, and eight calls were about non-GI bleed matters (for example, PEG fallen out, general gastroenterology advice). Of the 17 endoscopies (all upper GI) performed, three occurred after midnight. The mean age of the patients was 68, and the mean Rockall score prior to endoscopy was 4.4. All patients had iv access on arrival for endoscopy, but 47% were haemodynamically compromised on arrival. Five cases revealed oesophageal varices, five peptic ulcer disease. Only one endoscopy was entirely normal. Endoscopic therapy was undertaken in 71%. One patient died from the GI bleed, eight went to ITU and subsequently recovered.
Conclusions: The regional GI bleed service in South London is a new initiative which has been successful and has enabled a number of hospitals to provide an effective and safe out of hours endoscopy service
199 ENDOSCOPISTS’ ATTITUDES ON THE PUBLICATION OF “QUALITY” DATA FOR ENDOSCOPIC PROCEDURES
S. A. Hearnshaw, H. M. Maddock, D. Nylander, M. I. Prince.Sunderland Royal Hospital, Kayll Road, Sunderland SR4 7TP, UK
Background: The public now have access to experience, mortality & morbidity data for certain surgical procedures (BMJ 2005;330:506–10). Such “quality” data for endoscopy are not generally available, although Cotton has suggested this (Am J Gastro 2002;97:922). We studied endoscopists’ attitudes to and the practicality of these data being published.
Methods: We sent a questionnaire to all consultant GI surgeons, physicians, and gastroenterology registrars in the Northern region who currently endoscope (n = 132). We recorded doctor demographics, current data collection methods, and the acceptability and utility (5 point Likert scale; higher = less useful/acceptable) of nine items describing endoscopic “quality” (for example, mortality, complication, and completion rates).
Results: 103 (78%) doctors responded of whom 79 were consultants (77%), 61 physicians (59%), and 90 male (87%). 77 (75%) collect any “quality” data. The most frequently collected item was colonoscopy completion rate (57, 74%). Data were collected for audit by 26 (34%), clinical governance by 30 (39%), and appraisal by 62 (81%). For 42 (54%) these data were only available to themselves, 34 (44%) to other doctors, and just one (1%) to the public. Respondents consistently considered data publication as more acceptable than useful (p<0.01). The most acceptable/useful data item was annual number of endoscopies performed (mean acceptability = 1.9, utility 2.3), and the least was crude upper GI bleeding mortality (2.9, 3.2). Surgeons rated information less acceptable (2.9 v 1.9, p<0.01) and less useful (3.0 v 2.4, p<0.01) than physicians. Acceptability and utility scores were not related to gender, length of experience or current activity levels. Registrars rated utility better than consultants (2.0 v 2.7, p<0.01). Only two respondents thought all items totally unacceptable and useless.
Conclusions: The majority of endoscopists currently collect “quality” data for their practice although this is not widely available. If these data were to be made available to patients, consideration must be given to the value of such data and their acceptability. The majority of endoscopists do not find this completely unacceptable.
200 IMPACT OF ENDOSCOPIST PERFORMED TRANSABDOMINAL ULTRASOUND ON INVESTIGATION OF DYSPEPSIA IN DIRECT ACCESS ENDOSCOPY LISTS
S. Levi, B. J. Johnston, F. Hossain, R. Sekhar.Lady Sobell Gastrointestinal Unit, Wexham Park Hospital, Slough SL2 4HL, UK
Introduction: Endoscopy (OGD) and transabdominal ultrasound (TAUS) are complementary investigations in the investigation of upper GI symptoms. In the UK, OGD and TAUS are traditionally undertaken by different personnel in different departments thus fragmenting the investigation of dyspepsia, increasing the workloads in the departments, resulting in multiple hospital visits and delaying the diagnosis and management.
Methods: Our consultant gastroenterologist (SL) undertook formal training in TAUS in line with Royal College of Radiology guidelines for medical non-radiologists. A scanner was purchased for the endoscopy unit from charitable funds. Patients attending for direct access OGD underwent concurrent TAUS on this endosopist’s lists. Outcomes were compared with the pattern for six endoscopists not trained in TAUS for a period of 18 months starting in April 2004.
Results: 1204 sequential patients attended for investigation of dyspepsia during the study period. Undertaking concurrent TAUS had no impact on the throughput of the endoscopy lists (mean time in procedure room for OGD alone was 10.4 minutes, TAUS + OGD 10.6 minutes). With concurrent TAUS + OGD, investigations for dypsepsia were completed in 100% of cases during a single hospital visit. On the OGD alone lists, investigations were concluded in only 87% during the initial visit. Concurrent TAUS thus substantially reduced follow up visits, outpatient clinic workload, and waiting times. Several patients had diagnoses made on TAUS that precluded the need for OGD.
Conclusion: Abdominal ultrasound scanning by endoscopists is feasible and leads to major efficiency gains in the investigation of dyspepsia, accelerating diagnosis, minimising hospital visits, and improving waiting times, all without detriment to the throughput of endoscopy lists. We recommend that all UK endoscopists consider training in ultrasound, in view of the efficiency gains and earlier diagnosis that this would bring. Two other endoscopists are now training in ultrasound in our unit, and the rest may follow suit!
201 COMPARISON OF THE EFFICACY, ACCEPTABILITY, AND SAFETY OF A NEW TWO LITRE PEG+E GUT CLEANSING SOLUTION VERSUS TWO ESTABLISHED COLON CLEANSING REGIMENS
C. Ell1, A. Bitoun2, M. Halphen3, H-J. Gruss3.1Dr Horst Schmidt Kliniken GmbH, Wiesbaden, Germany; 2Hopital Lariboisiere, Paris, France; 3Norgine International Ltd, Harefield, UK
Aim: To compare the efficacy, safety and acceptability of a new 2 l PEG+E oral gut cleansing solution (MOVIPREP) to a standard 4 l PEG+E or sodium phosphate solution (NaP) as bowel preparation prior to colonoscopy.
Methods: Two similar randomised, single blinded, active controlled, multicentre studies were performed and datasets combined. Gut lavage solutions were taken either as single dose the day before the colonoscopy or as split dose with half dose the evening before followed by the other half on the morning of the colonoscopy. Primary efficacy criterion was the gut cleansing quality, as judged by a blinded expert panel on the basis of videotapes. Secondary endpoints were the degree of gut cleansing in predefined gut segments, overall quality of gut cleansing, evaluation of taste, patient’s satisfaction and acceptability, and a full safety assessment.
Results: A total of 699 patients (349 with Moviprep, 179 with 4 l PEG+E and 171 with NaP) in 27 centres received study medication. 588 patients (290 with MOVIPREP, 155 with 4 l PEG+E and 143 with NaP) were analysed for the primary efficacy endpoint using the available video tapes. The overall success rate was 81.4% in the MOVIPREP group versus 94.8% in the 4 l PEG+E group and 64.3% in the NaP group. Similarly, the mean scores of gut cleansing per colon segment were 2.3 (SD 0.8) to 2.8 (SD 0.8) in the MOVIPREP group versus 2.3 (SD 0.5) to 2.5 (SD 0.6) in the 4 l PEG+E group and 1.9 (SD 0.9) (colon ascending) to 2.8 (SD 0.8) in the NaP group. Patients consistently preferred MOVIPREP over 4 l PEG+E (patient satisfaction, overall acceptability, and taste) and NaP (taste, satisfaction with food recommendation, and professional/social impact). Both PEG+E containing solutions were well tolerated and had similar mild adverse event profiles. No relevant shifts in the laboratory tests were observed. In contrast, NaP was more frequently associated with the occurrence of adverse events and clinical significant laboratory shifts. Two cases of serious hypopotassemia were observed after the intake of NaP.
Conclusions: MOVIPREP is at least as effective as established gut cleansing regimens. Patients consistently preferred MOVIPREP as gut lavage solution to the established comparators. In summary, this new 2 l PEG+E bowel cleansing solution provides a better patient acceptability without any loss of efficacy or enhanced safety concerns for colon cleansing prior to colonoscopies.
202 WHAT HAPPENS TO PATIENTS WITH IRON DEFICIENCY ANAEMIA IN WHOM NO CAUSE IS FOUND?
L. Haine, R. Pinder, M. Rogers, (introduced by G. S. Duthie).Pinderfields Hospital, Aberford Road, Wakefield WF1 4DG, UK
Background: All adults with iron deficiency anaemia (IDA) need upper and lower GI tract investigation to exclude malignancy (BSG guidelines). In our series 15% of patients had cancer and 11% benign pathology to explain their IDA.
Aim: To follow up patients with unexplained IDA to see if they were re-investigated for persistent IDA and if our approach had missed malignancies or if other causes of IDA.
Methods: We investigate all adults with IDA by endoscopy with duodenal biopsy and colonoscopy. All patients investigated by this means from 01/05/1999 to 01/05/2002 were identified. In those where no cause was identified the hospital records system (PAS) was used to identify their GP. GPs were sent a questionnaire about these patients.
If there was no reply a further questionnaire was sent and if not returned this was followed by a telephone call. PAS was used to identify patients who died and patients who had been diagnosed with GI malignancy since investigation.
Results: Forty five patients had unexplained IDA. 33 replies were received from GPs. PAS showed 0 of 12 about whom we got no replies had died. Three of 33 patients had died; 1 hypothermia, 1 MI, and 1 stroke. No patient was diagnosed with GI malignancy since investigation. Seven of 33 patients had recurrent IDA with four diagnoses; 1 thalassaemia trait, 1 prosthetic valve haemolysis, 1 GORD, and 1 GI angiodysplasia. The other 24 of 33 patients did not have recurrent IDA but one developed a colovesical fistula due to diverticular disease and one an acute GI bleed and endoscopy revealed oesophageal varices.
Conclusion: Investigation of patients with IDA by endoscopy with duodenal biopsy and colonoscopy is adequate. This approach does not seem to miss malignancies though one angiodysplasia and was probably “missed” and one patient later was found to have varices though in the absence of IDA.
203 ANTIBIOTIC PROPHYLAXIS FOR INFECTIVE ENDOCARDITIS: IMPACT OF NEW BRITISH CARDIAC SOCIETY GUIDELINES
G. Mehta, J. E. East, N. Galletly, J. Goodhand, N. Thoua, G. V. Smith, D. S. Bansi, A. V. Thillainayagam.Gastroenterology Section, Hammersmith Hospitals NHS Trust, Faculty of Medicine, Imperial College London, UK
Background: The British Cardiac Society (BCS) recently updated their guidelines for antibiotic prophylaxis of infective endocarditis, proposing a more aggressive approach. These contrast with those of the British Society of Gastroenterology (BSG), American Gastroenterological Association (AGA), American Heart Association (AHA), and European Society of Cardiology (ESC). Although there remains consensus regarding prophylaxis for patients at high risk of endocarditis undergoing diagnostic endoscopy, the BCS also propose prophylaxis for patients at moderate risk with acquired valvular lesions.
Methods: Prospective study to assess the prevalence of patients with moderate or high risk cardiac lesions attending for diagnostic endoscopy. Patients underwent cardiovascular examination before the procedure. Clinical records and endoscopy referral forms were reviewed to confirm the presence or absence of known structural cardiac lesions.
Results: Sixty two patients (mean age 67 years) were examined. Of these, 40 (64.5%) underwent gastroscopy and 22 (35.5%) underwent colonoscopy. Eleven patients (17.7%) were found to have haemodynamically significant valvular lesions on clinical examination. Of these 11, the lesion had been previously documented in four patients (36.4%). No patients would have received antibiotics under BSG guidelines. If BCS guidelines were implemented in our Trust (7000 procedures/year), it would result in 1239 extra doses of antibiotics/year.
Conclusions: More than one in six patients attending for diagnostic endoscopy has a clinically detectable valvular lesion. These patients would receive broad spectrum antibiotics under BCS guidelines, without clear evidence of benefit. Iatrogenic complications from anaphylaxis, C difficile diarrhoea, previously unknown penicillin allergy, and antibiotic resistance may be incurred. Implications extend to cost, workload and training of nurse endoscopists for cardiac examination. Clearly, the BCS guidelines need to be reassessed urgently, possibly in collaboration with the AHA, ECS, AGA, and BSG.
204 PREDICTORS OF RE-INTERVENTION IN ENDOSCOPIC PALLIATION OF MALIGNANT GASTRODUODENAL OR COLORECTAL OBSTRUCTION WITH SELF-EXPANDABLE METALLIC STENTS
P. M. Lynch, E. Y. T. Lee, A. Alrubaie, A. A. Bailey, V. Kwan, S. M. Loh, S. J. Williams, M. J. Bourke.Endoscopy Unit, Westmead Hospital, Sydney, Australia
Aims: Enteral stenting is a minimally invasive option for the palliation of malignant obstruction. We sought to evaluate potential factors that may predispose to re-intervention in enteric and colonic stent failures in long term survivors.
Methods: Patients undergoing palliation of malignant gastroduodenal or colorectal obstruction with self-expandable metallic stents (SEMS) were identified from our endoscopic database over a six year period. In patients surviving 30 days or more an analysis was made of potential factors which may predispose to re-intervention including stent angulation and post-stenting survival. Stent angulation was graded: 1 (no angulation), 2 (1–15°), 3 (16–45°), 4 (46–90°), 5 (>90°).
Results: Eighty eight patients (49 male, mean age 71 years) were identified (47 gastroduodenal and 41 colorectal obstruction). Immediate technical success was achieved in 79/84 (94%) cases (four lost to follow up). With stenting symptoms resolved and oral intake resumed in 74/79 (94%) patients. Overall median survival following stenting was 71 days (range 2–785) and 101 days for the 52 patients surviving 30 days or longer. 16 of these patients required re-intervention due to stent obstruction (n = 13) or migration (n = 3) at a median time of 85 days (range 34–481). The mean stent angulation score for these patients was 3.94; the mean score in the group not requiring re-intervention was 2.89 (p = 0.004). Patients with post-stenting survival >60 days were likely to need reintervention (p = 0.01). The site of obstruction, type of primary malignancy, concurrent chemoradiotherapy did not influence stent functional longevity.
Conclusion: SEMS provide excellent palliation of malignant gastroduodenal or colonic obstruction. Re-intervention is necessary in almost 1/3 of long term survivors. Initial stent angulation and duration of survival post-stenting may be predictive of the need for re-intervention in patients surviving 30 days or longer. In strictures that are severely angulated, primary intervention with longer or more flexible SEMS may avoid the need for re-intervention.
205 DOES SENDING A VIDEO TO PATIENTS LEAD TO BETTER INFORMED CONSENT?
A. Tawil, M. J. Dew.Prince Philip Hospital, Llanelli, Wales, UK
Introduction: Informed consent is the cornerstone of good medical practice. We have previously assessed the level of understanding of consent in patients undergoing endoscopy1 and found it to be deficient in around one third. This study investigates whether understanding can be improved by sending a video of the procedure to patients prior to an upper GI endoscopy.
Method: Eighty five patients were sent a video prepared in-house, with professional support, detailing the procedure, showing images of the endoscope and detailing risks and alternative procedures as recommended in DOH guide to informed consent.2 Patients were then consented in the unit on the day of the procedure. Following obtaining consent and prior to the procedure their level of understanding was assessed using previously audited criterion to decide if consent was good, fair, poor, or displayed no understanding.
Results: Of the 85 patients sent videos only 74 had watched it. The 11 who did not watch sited reasons of “too frightened” (no), “couldn’t be bothered” (no), no video at home (no). Of the 74 who watched the video, 95% had good overall understanding, 90% understood the benefits, but only 70% understood the risks compared to 63%, 65%, and 68% respectively in the previous study. Whereas in the patients who watched the video these results are impressive, if those who did not watch it are included, there is no significant overall difference. Some patients (64, 86%) commented the video was helpful, others found it frightening (9, 12%), 1 felt the same.
Conclusions: The use of videos can help the understanding of some patients undergoing an endoscopic procedure but given that 13% do not watch such material the overall group level of understanding is not improved. We suggest for those patients who express an interest, such material should be available in the endoscopy unit, but routine sending of this type of material cannot be justified. Some patients were frightened by it (12%).
1. Guidelines for Informed Consent for Endoscopic Procedures. BSG Guidelines in Gastroenterology January, 1999
2. Guidelines on Consent for Examination or Treatment. Department of Health Publications 2001
206 UPPER AND LOWER GI TRACT FINDINGS IN PATIENTS WITH MACROCYTIC AND NORMOCYTIC ANAEMIA
N. Powell, A. McNair.Gastroenterology Department, Queen Elizabeth Hospital, Woolwich, London, UK
Background: Occult GI tract blood loss is the most common cause of iron deficiency anaemia (IDA). Evaluation of both the upper and lower GI tract is warranted to identify culprit lesions. IDA is readily defined by haemoglobin levels below laboratory reference ranges in combination with microcytic/hypochromic red cell indices or reduced serum ferritin concentrations. Unfortunately, endoscopy units receive many referrals for invasive investigation of patients with anaemia in the absence of supporting evidence of iron deficiency.
Methods: We conducted a retrospective study designed to evaluate whether significant GI tract pathology exists in patients with a macrocytic or normocytic anaemia in the context of elevated, normal, or undetermined serum ferritin concentrations. For comparison we studied a control group with documented IDA. We identified 130 patients referred to our unit for endoscopy who had a macrocytic or normocytic anaemia without evidence of IDA. All 130 patients were investigated with OGD and 65 patients (50.0%) were additionally investigated with colonoscopy or barium enemas. The comparator group comprised 201 patients with documented IDA, all of whom were investigated with both OGD and lower GI tract investigations.
Results: There were no lower GI tract malignancies identified in the 65 (0%) patients with a macrocytic or normocytic anaemia who underwent either colonoscopy or barium enema, as compared 23 colon cancers diagnosed in patients with documented IDA (11.4%), (p<0.01). Similarly, there were no upper GI tract cancers found in the macrocytic/normocytic group as compared to nine (4.5%) upper GI tract cancers found in their iron deficient counterparts (p<0.025). Other potential cause of occult blood loss were identified in the upper GI tract 21.9% of patients with documented IDA as compared to only 7.7% of patients without evidence of IDA (p<0.001). In summary, evaluation of the GI tract in patients with macrocytic or normocytic anaemia without evidence of iron deficiency has a very low diagnostic yield and is not warranted.
207 ENDOSCOPIC INVESTIGATION MUST BE CONSIDERED IN PATIENTS WITH SEVERE UNEXPLAINED ANAEMIA IRRESPECTIVE OF MCV
L. Connelly, B. Burns, P. M. Moncur, S. Saksena (introduced by A. F. M. Macklon).University Hospital of North Durham, DH1 5TW, UK
Introduction: The British Society of Gastroenterology (BSG) guidelines for management of iron deficiency anaemia recommend all patients considered for endoscopic investigation of anaemia should have a documented low haemoglobin, mean corpuscular volume (MCV), and ferritin.1 It also recommends that 90% of patients with anaemia have examination of both upper and lower GI tracts. The aim of this audit was to confirm the relevance of these targets within our elderly population in Durham.
Methods: Data were collected retrospectively from casenotes/computerised records for 99 consecutive UGIE performed at University Hospital North Durham in April–Sept 2004 to investigate anaemia.
Results: Ninety nine patients (29 males, median age 71 years, range 30–95 years) were included. There were 54 patients (55%) >70 years of age who had UGIE for anaemia, 26% did not have lower GI investigation due to significant co morbidity. Cancers were detected in seven patients (gastric cancer 2, colon cancer 5) of which four patients (57%) had normal MCV.
Conclusions: Cancer was detected in 7% patients which is significantly lower than most large studies,2 however only 72% of patients referred were suitable for lower GI investigations in contrast to the target of 90% by the BSG. Four of seven patients with cancer had a normal MCV despite severe anaemia and would have been excluded from GI investigations as per BSG guidelines.1 These data suggest that future BSG guidance must consider patient age and comorbidity specific targets and requires prospective validation. Importantly these data support the endoscopic investigation for severe anaemia irrespective of the MCV.
Abstract 207
1
2
208 MULTIFACTORAL ANAEMIA IN THE ELDERLY: WELL WORTH A LOOK
G. Mehta, B. Ancock, N. Galletly, J. Goodhand, G. V. Smith, D. S. Bansi, A. V. Thillainayagam.Gastroenterology Section, Charing Cross Hospital Campus, Faculty of Medicine, Imperial College London, UK
Background: In the elderly, anaemia of chronic disease (ACD) is more common than iron deficiency anaemia (IDA). However, comorbidity is common in this population, and therefore elucidating the dominant cause in any individual patient may be challenging.
Aim: To discover potential aetiological factors in patients referred for endoscopic investigation of anaemia. Endoscopic findings were then categorised according to biochemical classification of anaemia. Blood samples from within three months of endoscopy were analysed for serum ferritin, serum iron, and iron binding capacity (TIBC). The classifications were: (1) IDA defined as either low ferritin, or low iron and high TIBC; (2) ACD defined as low iron and low TIBC in the absence of low ferritin; and (3) mixed anaemia (MA). Endoscopically diagnosed bleeding lesions were cancer, ulceration, angiodysplasia, telangiectasia, and colitis.
Results: Ninety three patients over the age of 75 years (mean age 82 years) underwent endoscopic investigation for anaemia between July 2004 and October 2005. All underwent colonoscopy, and 75 underwent gastroscopy.
Conclusions: Biochemical IDA was present in a small minority (7.5%) of elderly patients referred for investigation of anaemia. Many patients (39.8%) were found to have ACD, and these were least likely to have endoscopic pathology. The majority had MA, surprisingly the best predictor of endoscopic pathology. Therefore, the absence of classical iron deficiency in the elderly must not preclude endoscopic investigation. However, the paucity of endoscopic pathology in patients with ACD suggests that in frail patients investigation may be deferred, at least until more convincing indications for endoscopy emerge.
Abstract 208
209 THE CHANGING FACE OF OGD AND COLONOSCOPY IN A TERTIARY REFERRAL CENTRE: 11 YEAR AUDIT OF ENDOSCOPIC PRACTICE
S. Campbell, M. Lombard, A. I. Morris.Royal Liverpool University Hospital, Liverpool, UK
Background: Colonoscopy is performed poorly in the UK, with caecal intubation rates (CIR) <60% in a recent national audit. Upper GI endoscopy (OGD) can have significant cardiorespiratory morbidity in part attributed to poor sedation practise. We were interested to examine whether changes in awareness of problems, sedation guidelines, and endoscopy training during the last 10 years had altered our practice.
Aim: To examine OGD and colonoscopy practise in a large University Hospital over 11 years and compare with current advisory guidelines.
Patients and Methods: A database of 75 956 procedures was used 1994–2005 (OGD: 65 728; colonoscopy: 10228). Recorded parameters for both were analysed: sedation/opiate use, therapeutic trends, caecal intubation rates (CIRs), reporting practise and use of LA spray for OGD. Statistical analyses included log rank analysis (LRA) and MWT using Minitab 13 software.
Results: 90% OGD (59017) and 73% c/scopy (7506) reports had complete data for analysis. OGD analysis—a significant decrease (p<0.001) in midazolam dose (1994 mean 5.9 mg, range 1–20 mg; 2005 mean 3.1 mg, range 1–8 mg); LA spray use has not changed (mean 50%, range 45–56%) but use of pethidine has increased (p<0.001) in parallel with therapeutic OGD (r2 = 0.69 p<0.001). Colonoscopy had a similar reduction in midazolam use (1994 mean 7.4 mg, range 2–20 mg; 2005 mean 3.6 mg, range 1–8 mg) and pethidine use has risen from 17% in 1994 to 87% in 2005 (p<0.0001). This parallels improvement in CIR: 70% 1994 to 85% 2005 (r2 = 0.8 p<0.0001). Therapeutic colonoscopy has also risen from 9% 1994 to 26% in 2005 (r2 = 0.9 p<0.0001) in part representing better patient selection. Reporting practise for both OGD and c/scopy has improved significantly from 1994–2005: 30% of 1994 reports did not accurately state drug doses cf with only 3% in 2005 (r2 = 0.8 p<0.0001).
Conclusion: Sedation dose has reduced in line with current guidelines and parallels improved training of SpRs. CIRs have risen over the last 11 years and reporting practise has improved. Further improvements in audited outcomes require more accurate recording of details of selection and clinical outcomes.
210 CHANGING PRACTICES IN BENZODIAZEPINE SEDATION FOR ENDOSCOPY
N. P. Galletly, J. Goodhand, G. Mehta, G. V. Smith, D. S. Bansi, A. V. Thillainayagam.Gastroenterology Section, Hammersmith Hospitals Trust, Faculty of Medicine, Imperial College London, UK
Background: Most endoscopic procedures are performed under conscious sedation with a short acting benzodiazepine such as midazolam. The 2004 NCEPOD report “Scoping our Practice” found that in 14% of peri-endoscopy deaths the dose of benzodiazepine given for sedation was inappropriately excessive. Awareness of safe practice in sedation is increasing in part due to guidelines from the BSG and other authorities. The 2003 BSG Safety and Sedation During Endoscopic Procedures Guidelines recommend that the “dosage of benzodiazepines … should be kept to a minimum to achieve sedation.” The aim of this study was to determine whether our use of midazolam sedation for endoscopy has changed over the last six years.
Methods: A snapshot retrospective review of sedation records for all gastroscopies (OGDs), colonoscopies and ERCPs performed in one of the Trust’s endoscopy units during the years 2000 and 2005.
Results: A total of 1135 OGDs, 989 colonoscopies, and 82 ERCPs were performed with iv sedation in 2000; 840 OGDs, 987 colonoscopies, and 120 ERCPs were performed with iv sedation (to date) in 2005.
Conclusion: Benzodiazepine doses used for all endoscopies and the use of sedation for upper GI endoscopy have reduced significantly between 2000 and 2005. This encouraging trend highlights the increasing awareness of safe sedation practices among endoscopists.
Abstract 210
211 CONTINUING THE AUDIT CYCLE: RE-AUDIT INTO COLONOSCOPY SEDATION PRACTICE AND SEDATION COMPLICATIONS 1992–2004: 14 521 CASES REVIEWED
T. Sivayokan, R. Leicester, A. Poullis.St George’s Hospital, London, UK
Background: A national audit into colonoscopy practice revealed high average doses of midazolam (5 mg) and pethidine (50 mg) were being used resulting in oversedation in 3.4% of cases (CJA Bowles, R Leicester et al. Gut 2004). When previously audited in 2000 we found high doses of sedatives were often administered and following this earlier audit in-house re-education and training took place. In 2002 skills courses were regularly carried out in the unit. We re-audited our practice to asses the impact of these on our sedation practice.
Method: We analysed 14 521 colonoscopies in our department from 1992 and 2004 to determine changes in sedation practice and sedation related complication rates in particular comparing practice before and after our previous audit. Oversedation was defined as the need to administer naloxone or flumazenil or being noted as a specific complication on the endoscopy report.
Results: 6849 colonoscopy results were available in the 1992–99 period and 7672 between 2000–04. Fortral was used at a mean dose of 29.5 mg (SD 3.2), between 1992–2002 and diazemuls at a mean dose of 6.1 mg (SD 2.4). Between 1992–2004 midazolam was used at a mean dose of 3.9 mg (SD 1.4). Between 1993–2004 pethidine was used at a mean dose of 40.9 (SD 13.5). Between the 1990s and 2000s there has been a significant reduction in the dosages of midazolam (4.6 mg v 3.1 mg p<0.001) and pethidine (47.3 mg v 31.6 mg p<0.0001), no changes were seen with fortral or diazemuls. 61 cases of oversedation were recorded (0.4%) with 46 cases in the 90s (0.7%) and 15 cases in the 2000s (0.2%) (p<0.003).
Conclusion: Regular auditing and re-education can help to improve endoscopic standards and reduce the dosages of sedatives administered and subsequent oversedation.
212 DOES BODY MASS INDEX INFLUENCE PAIN FOLLOWING COLONOSCOPY?
P. S. A. de Silva, J. M. Sayer.Department of Gastroenterology, Doncaster Royal Infirmary, Thorne Road, Doncaster DN2 5LT, UK
Introduction: The incidence of obesity is growing in the United Kingdom. This has resulted in more overweight and obese subjects undergoing colonoscopy. There is an increasing interest in assessing complication outcomes and suitable remedial action in this category.
Aims: To assess the incidence of pain in obese patients who underwent colonoscopy in a district general hospital over a four month period.
Methods: Data were collected from HCNscribe database and a questionnaire from all patients who consented to participate. Patients were asked to complete and return a questionnaire stating any symptoms that they experienced upto two weeks after their procedure. Case notes were also reviewed. Inaccurately/incompletely filled questionnaires were excluded from data analysis. BMI values were calculated from weight and height measurements on the day of the procedure and classified according to British Heart Foundation criteria. Corresponding details of sedation type, dosage, and procedures undertaken during colonoscopy were obtained from HCNscribe.
Results: During the study 508 patients underwent colonoscopy. 462 had a valid BMI recording. A total of 162 with valid BMIs had accurately completed forms: 58 obese, 60 overweight, 41 normal, 3 underweight. 121 had complications (abdominal pain, bleeding, vomiting, faint, respiratory or urinary tract infections, non-specific) Pain was noted in 97 (78.2%)—34 obese, 35 overweight, 27 normal, and 1 underweight. There was no significance in the incidence of pain among the different groups. 124 patients had sedation. There was no significant difference amongst BMI groups, occurrence of pain, administration of sedation (type, dosage, single or combined administration) and incidence of procedures undertaken during colonoscopy. Sedatives used were pethidine, midazolam, buscopan, nubain.
Conclusion: This study reveals that BMI does not affect the incidence of pain after colonoscopy irrespective of sedation administered and procedures undertaken.
213 UNSEDATED COLONOSCOPY: FOR THE MANY OR FOR THE FEW?
A. Sarkar, K. S. Smith, S. S. Johal, M. T. Donnelly.Department of Gastroenterology, Northern General Hospital, Sheffield Teaching Hospitals NHS Foundation Trust, Herries Road, Sheffield S5 7AU, UK
Introduction: A colorectal screening programme, with colonoscopy at its centre, is imminent in the United Kingdom. Perhaps the most dangerous aspect of colonoscopy is intravenous (iv) sedation related complication.
Aim: The aim of this study was to discover whether unsedated colonoscopy could be well tolerated by a large group of UK patients.
Methods: We retrospectively analysed sedated and unsedated colonoscopies carried out on our unit over a period of January 2002 to September 2005. All patients had their tolerance of the procedure independently assessed by an experienced endoscopy nurse on a four point scale (“good”, “acceptable”, poorly tolerated”, “not tolerated”). We correlated these assessments with demographic and other data.
Results: Between January 2002 and September 2005 we performed 1442 unsedated colonoscopies, 1901 with Entonox only, and 4617 with intravenous midazolam. The age range of the patients was 16–95 years. As can be seen from the table, patients who were unsedated or received nitrous oxide alone tolerated colonoscopy significantly better than those who received intravenous sedation.
Abstract 213
The nitrous oxide or no sedation group and the no sedation group both tolerated colonoscopy better than the iv sedation group (p<0.001, χ2 test)
Conclusion: Significant numbers of patients can tolerate colonoscopy without sedation or by using nitrous oxide alone. Patients who choose to have colonoscopy without sedation or with nitrous oxide tolerate colonoscopy better than those who choose to have iv sedation. These data encourage the practice of unsedated colonoscopy
214 ENDOSCOPY IN HIGH RISK CARDIOVASCULAR PATIENTS
G. Parkes, P. Fairclough, J. O. Lindsay.Department of Gastroenterology, Royal London Hospital, London, UK
Backround: Early percutaneous transarterial coronary angioplasty (PTCA) improves outcomes in patients with acute coronary syndromes (ACS). Many cardiologists require endoscopic investigation of patients with anaemia or evidence of a GI blood loss prior to PTCA, resulting in an increase in the number of procedures in patients with a recent history of ACS. The diagnostic yield in this patient group has not been reported; furthermore, performing endoscopy within three months of ACS may be associated with increased morbidity and mortality.
Objectives: To review the incidence of complications and diagnostic yield in patients undergoing endoscopy with recent ACS compared to matched controls, over one year period in a London teaching hospital with a large interventional cardiology department.
Methods: A retrospective review was performed using the Adam endoscopic reporting system. Patients referred for endoscopic procedures with a history of ACS within the previous 60 days were identified. The control group consisted of inpatients referred for endoscopic procedures, matched for age, sex, and indication.
Results: Over a one year period 57 patients with ACS within the previous 60 days underwent a combination of gastroscopy (40) and colonoscopy (17). The median (range) time between ACS and endoscopy was 14 (1–58) days. Three cardiovascular complications were reported in the ACS group—one acute atrial fibrillation and two episodes of profound hypotension (5.2%); compared to none in the control group. There were no fatalities in either group. The yield of important diagnoses in the ACS group was 37% of cases compared to 51% in the control group. The diagnostic yield in ACS patients referred for anaemia as opposed to a GI bleed was 24% v 38% in controls. Cancer was detected in one ACS patient v three patients in the control group.
Conclusions: This small study suggests that endoscopic procedures in patients with a recent history of ACS are associated with increased morbidity compared to non-cardiac inpatient endoscopy. The diagnostic yield in ACS patients is low, suggesting the need for more specific referral criteria.
215 CARDIOVASCULAR ASSESSMENT IN PATIENTS FOLLOWING BOWEL PREPARATION WITHOUT INTRAVENOUS FLUID REPLACEMENT: INCREASED AGE DOES NOT MEAN DECREASED FUNCTION
S. E. Noblett, A. F. Horgan.Department of Colorectal Surgery, Freeman Hospital, Newcastle Upon Tyne, UK
Introduction: It is recognised that bowel preparation prior to colonoscopy/colorectal surgical procedures has a dehydrating effect such that many advocate intravenous fluid replacement, particularly in elderly patients. We compared the cardiovascular effects of bowel preparation in patients under and over 65 years of age.
Method: Thirty nine patients having bowel preparation prior to elective colorectal surgery were prospectively assessed. All received bowel preparation using sodium picosulphate without intravenous fluid replacement. Data collected included age, POSSUM physiology score, and preoperative cardiovascular parameters which were measured in all patients using an oesophageal doppler; these included stroke volume (SV), cardiac index (CI), descending aortic flow time (FTc), heart rate (HR), and mean arterial pressure (MAP). The patients under 65 years of age were compared with those over 65 years. Data were compared using Student t test or Mann-Whitney U test as appropriate.
Results: Patients less than 65 years (group 1) had a median age of 55 years (range 24–63), the over 65 group (group 2) had a median age of 77 years (66–93). As could be expected the medical comorbidity assessed by the POSSUM physiology dataset was increased in group 2 (16.8 v 13.7, p<0.001). No differences were found in routinely measured indices, HR (73 bpm v 65 bpm, p = 0.079) or MAP (74 mmHg v 79 mmHg, p = 0.122) between the two groups. Similarly, no significant differences were found in the cardiac function parameters SV (77.2 ml v 79.9 ml, p = 0.908), CI (2.92 l/min/bsa v 2.86 l/min/bsa, p = 0.915), or FTc (368 ms v 360 ms, p = 0.547).
Conclusion: The use of bowel preparation without supplementary intravenous fluid replacement did not significantly reduce cardiac function in our elderly patient group compared with younger patients. With an increasingly elderly patient population combined with pressures on resources and a drive towards day-case procedures, our finding that despite being a susceptible group for bowel purgative induced dehydration, no significant difference in cardiac function is reassuring.
216 CONSCIOUS SEDATION AND COLONOSCOPY. ARE WE NEGLECTING PATIENT’S COMFORT FOR SAFETY?
J. M. Hancock1, D. Nylander2, K. Tirou1, S. Zubair1, R. Kasturi1, M. Connelly1, B. Gilbank1, J. Painter2, G. D. Bell3.1South Tees NHS Trust; 2Sunderland Royal Hospital; 3Department of Computing Sciences, UEA
Introduction: Several of us who either regularly teach colonoscopy on courses held at different Regional and National Centres (JH, DN, JP, GDB) or alternatively supervised trainees who had attended such courses (MC) wondered if the admirable trend to using much smaller doses of sedation and analgesia might, at times, have gone too far and thus patient comfort might be suffering. MC, a largely self-taught colonoscopist, had a sedation practice which was known to be markedly different from that of the other trainers and he agreed to take part in a comparative prospective audit to monitor patients’ experience and overall satisfaction with their colonoscopy.
Method: 132 patients undergoing a colonoscopic examination (at which trainees were present) agreed to complete a patient satisfaction questionnaire. The form included an assessment of pre-procedure worries, estimated degree of discomfort, severity of pain experienced during the procedure, and the usual post procedural questions regarding overall satisfaction. The nurse and endoscopist involved in each procedure also filled in an appropriate form which included a record of sedation and analgesics used and observed patient discomfort/pain.
Results and Discussion: MC and trainees under his supervision carried out 68 colonoscopies while JH, DN, and JP plus trainees together performed 64 examinations. Despite the fact that MC’s performance scored significantly lower in terms of caecal intubation (p = 0.0013), speed of withdrawal (p<0.0001) and nurse rated pain score (p = 0.0014), MC’s patients themselves rated their overall satisfaction to be higher (p = 0.017) as a consequence of their recall of discomfort being somewhat less (p = 0.09). These paradoxical findings are almost certainly explained by MC’s use of significantly (p<0.001) larger doses of both midazolam and opioid plus his more frequently resorting to “top ups” than the other consultants. The importance of patient comfort is stressed in the GRS (see http://www.grs.nhs.uk) and clearly the balance between safety and comfort needs to be kept in mind when sedating patients.
217 IS SEDATION PRACTICE LINKED WITH ADVERSE ENDOSCOPIC OUTCOME? AN AUDIT IN RESPONSE TO THE NCEPOD REPORT
J. McPhillips, K. Bowering, U. Vithanarchchi, P. Mahindra, A. Byne, R. Sturgess, K. Bodger, S. Sarkar.Aintree Centre for Gastroenterology, University Hospital Aintree, Liverpool, UK
Introduction: The NCEPOD report “Scoping our practice” (2004) emphasised sedation practice as a possible contributor to endoscopy related mortality (ERM). Recommendations included regular audit and national guidelines for sedation. Current BSG and Academy of Medical Royal Colleges guidelines recommend the use of no more than 5 mg midazolam (MD), and for reduced doses in the elderly or in combination with opioids (COM).
Aim: To audit endoscopy sedation practice to establish rates of procedure-related complications (PRC) (including ERM and immediate complication rate) for all diagnostic and therapeutic upper and lower endoscopy (excludes ERCP).
Methods: 7234 consecutive procedures performed in 5999 patients were audited. Patients were identified from Endoscribe database and deaths correlated using the hospital medway IT system. Death certificates were reviewed in all fatalities.
Results: Sedation was used in 53% of procedures. Mean MD dose (SD) was 4.87 mg (2.5). 18.75% (6/32) endoscopists used doses >5 mg. Overall 30 day mortality was 0.73% (n = 53) but true ERM was 0.25%. The lower ERM was seen in non-sedated versus sedated patients (0.09% v 0.4%;p = 0.02) perhaps reflected a younger age group (p<0.001) undergoing mainly non-therapeutic procedures (97% v 65%). PRC was again lower in the non-sedated group (0.18% v 1.1%; p<0.001). Mean doses of MD were lower in ERM patients than survivors (2.6 mg v 4.9 mg ;p<0.001) with none receiving >5 mg or COM. Also, MD doses were comparable for those with or without any complication (p = 0.2). There were no differences in PRC when comparing patients receiving ⩽5 mg versus >5 mg MD (1 v 1.4%;p = 0.4) or MD only verses COM (1.1 v 0.95;p = 0.7). Endoscopists consistently using >5 mg MD did not have greater ERM or PRC compared to other operators (p = 0.7 and 0.2).
Conclusions: We found no strong evidence to link higher sedation doses or the use of combined sedation with endoscopic related mortality (ERM) or procedural related complications (PCR). Endoscopists who exceeded recommended doses had comparable outcomes. This suggests that the heavy emphasis placed on sedation practice by NCEPOD on mortality was unfounded and highlights the need to audit both favourable and adverse outcomes.
218 A SCORING SYSTEM GENERATED FROM PATIENT CONSULTATION QUESTIONNAIRE TO STRATIFY RISK OF UPPER GASTROINTESTINAL CANCER
A. Al-Sarira, M. Ballal, S. Selvachandran, J. Mckay, I. London, D. Cade, D. Corless.Leighton Research Unit, Leighton Hospital, Crewe, Cheshire, UK
Background: Published guidelines for symptomatic upper gastrointestinal (GI) referrals resulted in an overwhelming referral rate. And its effectiveness has been questioned, as is evident from many audits and studies throughout UK. Previous work using patient consultation questionnaire (PCQ) linked to an electronic patient record (EPR) and computer generated scoring system has been shown to be an effective and objective way of predicting colorectal malignancy and streamlining referrals.
Objective: The aim of this study is to derive and evaluate diagnostic determinants of gastro-oesophageal cancer based on patients’ symptomatic profile derived from an upper GI PCQ.
Method: A detailed upper GI PCQ was sent to all patients coming for first time endoscopy. All symptoms and diagnostic outcomes were collected and stored in the EPR to create a databank.
Results: 402 patients were included. 4% of these had cancer, 31.3% of which had curative surgery. Univariate and multivariate analysis resulted in four factors being positive predictors for cancer. These were age, retrosternal dysphagia, duration of abdominal pain less than six months, and worsening abdominal pain. On the other hand there were two negative predictors, those being female sex and abdominal pain, which is more than six months and not progressive. When the generated scoring system applied on the study population it excluded 40% of the workload and detected cancer in 10% with AUC (area under curve) of 0.87 in the ROC (receiver-operating characteristic) analysis.
Conclusion: Scoring system for upper GI symptoms as predictor of cancer is possible and it will result in reducing the workload in endoscopy by prioritisation of referrals.
219 AN AUDIT OF MORTALITY FOLLOWING PEG INSERTION AND THE IMPACT OF A NURSE LED PRE-ASSESSMENT SERVICE
R. Riley, M. M. Ahmed.Department of Gastroenterology, Good Hope Hospital, Birmingham B75 7RR, UK
Introduction: Percutaneous endoscopic gastrostomy (PEG) is a common procedure that provides enteral access for the administration of tube feeding in patients who are unable to obtain adequate nutrition by mouth. The recent NCEPOD report (Oct 2004) has raised concerns over improper PEG usage and recommends in-depth assessment of the patient to determine potential benefit prior to PEG insertion.
Aim: We performed a two year audit (01/01/03–31/12/04) to examine mortality after PEG insertion and determine the impact of a nurse led pre-assessment service which was set up one year into the audit (on 01/01/04).
Method/Patients: Over the two years, 102 patients (51 female, 41 male) were fitted with a Fresenius Freka (9 or 15 French) pull through gastrostomy tube. A prospective database of all patients was kept.
Results: See table.
Abstract 219
Conclusion: The introduction of a pre-assessment service has resulted in better patient selection (by excluding inappropriate referrals) and this in turn has resulted in a decrease in post-procedure mortality.
220 UPPER GASTROINTESTINAL POLYPS: WHY BIOPSY?
S. Cherian, M. M. Ahmed.Good Hope Hospital NHS Trust, Sutton Coldfield B75 7RR, UK
Aim: Polyps are a common finding at oesophageo-gastro-duodenoscopy (OGD). Up to 90% of gastric polyps are reported to be hyperplastic. We conducted a retrospective audit on all patients in whom a polyp was detected at OGD to establish the yield from biopsies of these polyps.
Methods: All OGDs performed over a nine year period (1996 to 2005) were reviewed and cases where a polyp was detected were identified and analysed further.
Results: 367 patients (225 male) underwent 425 OGDs. The median age was 69 years. Polyp location was: gastric (412), duodenal (1) and both (12). In 254 of 425 cases, polyps were multiple. Polyps were >10 mm in size in 38 procedures, 6–10 mm in 63 and 0–5 mm in 184. Polypectomy was performed in 11 procedures (2 endoscopic mucosal resections). Argon plasma coagulation was used to ablate polyps in two cases. Adrenaline injections were used to control post polypectomy bleeding in two patients. Biopsies were performed in 225 procedures: 89 were fundic gland polyps/cystic glandular polyps, 10 were Corpus glandular and 57 were either inflammatory, hyperplastic or regenerative. Normal mucosa was detected in 42. Significant histology was detected in 29 procedures. These are listed in the table.
Abstract 220
Conclusion: Significant diagnostic yield from upper gastrointestinal polyp sampling is not as low as sometimes assumed. In addition when polyps are found, the biopsy result can alter patient management. Hence we recommend that histological confirmation be obtained in all new polyps.
221 VALUE OF 3D EUS IN STAGING AND DETAILED ACCURATE LOCALISATION OF EARLY OESOPHAGEAL CANCER PRIOR TO TREATMENT
S. Inglis, S. Paterson-Brown1, D. Patel2, J. N. Plevris3.Departments of Medical Physics, 1Surgery, 2Radiology, and 3Centre for Liver & Digestive Disorders, The Royal Infirmary of Edinburgh, UK
Background: Endoscopic ultrasound (EUS) is routinely used in the staging of oesophageal cancer. The majority of these tumours at diagnosis are advanced, but when the disease is diagnosed early there are several treatment options available depending on patient fitness, age and their preference of treatment.
Aims: To investigate the use of 3D EUS as a means to provide detailed and accurate information in the staging and localisation of T1 cancers of the oesophagus.
Methods: Between 2002 and 2005, we retrospectively studied, 14 patients (5 F/9 M, mean age 72/65 years respectively), diagnosed with T1 cancer of the oesophagus. As part of their staging a CT of thorax/abdomen and EUS with subsequent 3D reconstruction (3D-EUS) were performed. A reconstruction of the oesophagus was generated from images acquired during a free pullback of the echo-endoscope at a constant speed and at a rate of 12.5 fps. Using an oesophagus mimicking phantom, we have previously estimated the max error of the 3D EUS technique in estimating length and depth of tumour as <2.5%.
Results: In all cases there was agreement between standard EUS and 3D EUS in the staging of the disease (T1). The tumour was not visible by CT scan in any of the cases. Seven patients had upper/mid oesophageal Ca, six patients at lower third, and one junctional tumour. No definite lymphadenopathy seen by EUS or CT. In addition to standard EUS, 3D EUS provided more information and accurately determined tumour dimensions, layer involvement and in particular length relative to reference anatomical structures such as the aortic arch, subcarinal area, or the OGJ. Four of seven patients with upper/mid tumour received radiotherapy.
Conclusion: 3D EUS provided additional detailed information regarding tumour dimensions and layer involvement in early (T1) disease. Such information can be of use in treatment planning, in particular in cases treated by radiotherapy in order to accurately localise tumour in the absence of tumour imaging by CT and focus the administration of radiotherapy.
222 THE VALUE OF REPEATING UPPER GI ENDOSCOPY AFTER NORMAL INITIAL FINDINGS
C. P. C. Boger, S. Bridger.Dorset County Hospital, Dorchester, Dorset UK
Introduction: Repeat endoscopy on patients who have already had a normal upper gastrointestinal investigation often seems unrewarding. Despite this observation no study has investigated whether repeating endoscopy in these patients yields any additional pathology in particular new cancers.
Method: We conducted a review of our endoscopy database over a seven year period between July 1997 and July 2004. We included all patients who had undergone two or more upper GI endoscopies with a normal first endoscopy. We then looked at all subsequent endoscopies for that patient to ascertain the number of new cancers discovered.
Results: 15 758 patients underwent an endoscopy during this time period with 2991 patients (19%) having two or more procedures. 1379 patients (8.8%) underwent repeat endoscopy despite a normal initial procedure. In this group only 20 new cancers (1.5%) were found; seven within one year of the first endoscopy, two between 1–2 years, five between 2–3 years, and five over three years. Of those found in the first year, all seven (35%) were probable missed cancers that had undergone repeat procedures prompted by continuing or new worrying symptoms, or other additional investigation. Of those cancers picked up after one year, only one was a probable miss with the rest again prompted by worrying symptoms.
Discussion: A large number of endoscopies are performed on patients who have already had a normal initial endoscopy using up valuable resources. With such a low yield of cancer the necessity of repeating the procedure should be strongly considered, and only undertaken on those with continuing worrying symptoms.
223 WIRELESS CAPSULE OESOPHAGOSCOPY (PILLCAM ESO) COMPARED TO UPPER GI ENDOSCOPY IN THE DETECTION OF OESOPHAGEAL VARICES
S. Donnelly, N. Campbell, E. H. Forrest, A. J. Stanley, A. J. Morris.Gastroenterology Unit, Glasgow Royal Infirmary, UK
Introduction: Detection of oesophagal varices is essential for primary and secondary prophylaxis of variceal haemorrhage but requires U.G.I. endoscopy examination (OGD).
Aim: To assess if wireless capsule oesophagoscopy (WCO) can detect oesophageal varices and compare WCO findings with OGD results.
Patients and Methods: Eight patients (5M, 3F) with suspected (n = 4) or previously documented oesophageal varices (n = 4) were included. All had chronic liver disease; alcohol, n = 5; Hep C, NAFLD, and PSC, n = 1. All patients had wireless capsule oesophagoscopy 30 minutes before UGI endoscopy. WCO recordings were analysed independently by two investigators blinded to UGI endoscopy results. WCO grading of varices was Fo = no varices, F1 = <33%, F2 = >33%, and <66%, F3 = >66% of radius of oesophagus respectively. Presence or absence of portal hypertensive gastropathy was assessed. Other findings in the UGI tract were noted. Oesophageal transit time by WCO (first oesophageal image to first gastric image) was measured.
Results: See table for comparison of WCO and OGD results.
Abstract 223
Conclusion: (1) WCO can detect oesophageal varices in patients with chronic liver disease. (2) WCO has a high sensitivity and PPV compared to OGD in detection of oesophageal varices.
224 CLINICOPATHOLOGICAL VARIABLES PREDICT MORBIDITY AND EARLY MORTALITY FOLLOWING COMBINED BILIARY STENTING: A MULTIVARIATE RISK FACTOR ANALYSIS
C. P. Neal, D. Bools, S. C. Thomasset, C. D. Sutton, C. J. Pattenden, G. Garcea, Y. Rees, A. R. Dennison, D. P. Berry, R. Robinson.Departments of Surgery, Gastroenterology and Radiology, Leicester General Hospital, Leicester, UK
Introduction: Combined percutaneous and endoscopic biliary stenting permits drainage of biliary obstruction not treatable by ERCP alone, but is associated with significant morbidity and mortality. We present the largest reported series of combined procedures and examine factors that may predict procedure associated morbidity and mortality.
Methods: A retrospective study of patients undergoing a combined procedure for biliary decompression between January 2001 and December 2004. Sixteen pre-procedure clinicopathological and laboratory variables were correlated with outcome and significance determined using the χ2 test (for morbidity) and the log rank test and Cox regression analysis (for mortality).
Results: Combined biliary stenting was attempted in 80 patients over the study period and was technically successful in 72 cases. Underlying pathology in those stented included carcinoma of the pancreas (n = 31), cholangiocarcinoma (n = 19), metastatic disease (n = 13), benign pathology (n = 7), and ampullary carcinoma (n = 2). Inpatient morbidity was 30% and 30 day mortality 21%. Low serum albumin, low haemoglobin, elevated white cell count, and clinical evidence of sepsis were significantly associated with morbidity (p<0.05). High ASA grade (p = 0.001), elevated serum creatinine (p = 0.01), low serum albumin (p = 0.01), elevated white cell count (p = 0.003), and clinical evidence of sepsis (p = 0.0002) were associated with increased 30 day mortality on univariate analysis. Of these factors, high ASA grade (p = 0.009) and elevated white cell count (p = 0.04) were independently associated with increased 30 day mortality.
Conclusion: Combined biliary stenting is associated with a high technical success rate and acceptable mortality and morbidity in our centre. Clinicopathological and laboratory variables predict poor outcome following combined biliary drainage and optimisation of patient status may reduce procedure associated risk.
225 SERIAL INCREMENTAL STENTING OF SYMPTOMATIC COMMON BILE DUCT STRICTURES SECONDARY TO PANCREATITIS
P. M. Lynch, A. A. Bailey, E. Y. T. Lee, T. L. C. Lee, S. J. Williams, M. J. Bourke.Endoscopy Unit, Westmead Hospital, Sydney, Australia
Aims: Common bile duct (CBD) strictures occur in 1/3 of patients with chronic pancreatitis. Operative management carries significant morbidity and potential mortality. Single placed CBD stents are associated with early symptomatic stricture recurrence. Our aim was to determine the clinical and biochemical benefit of multiple simultaneous stents for symptomatic distal CBD strictures due to pancreatic fibrosis.
Methods: Patients with symptomatic distal CBD strictures secondary to pancreatitis were managed by a standardised protocol of serial incremental stenting at ERCP; the therapeutic goal being placement of two 10F biliary stents. Three monthly stent exchanges were performed over one year. Stents were then removed and the patients followed with three monthly LFTs. Three 10F stents were placed for refractory strictures.
Results: From July 2000 to May 2005 ten patients with symptomatic CBD stricture related to pancreatic fibrosis were included (chronic pancreatitis: n = 8; acute pancreatitis: n = 2). All patients were male (mean age 57 years; range 39–77 years). Clinical features at presentation were indicative of biliary obstruction. Eight patients had two (10F) stents placed simultaneously, while two patients with refractory strictures required three (10F) stents. At mean follow up (15 months; range 2–46) after initial stent placement there was a significant reduction in mean ALP level from 282 to 106 U/l (p = 0.012). Of eight patients presenting with abdominal pain, pain persisted in only one patient post treatment. Mean initial distal CBD stricture diameter was 2.0 mm. In all cases a 15 mm balloon could be drawn through the stricture at stent removal. Six patients have completed the treatment protocol with a mean stent free follow up of 12 months; of which one had recurrent CBD stricturing at one year after stent removal, requiring reintervention with triple stenting.
Conclusions: Our results suggest that serial incremental stenting for symptomatic distal biliary stricture related to pancreatic fibrosis results in symptom resolution, biochemical improvement and radiographic improvement in CBD diameter with minimal complications.
226 ERCP BRUSH CYTOLOGY OR EUS-FNA FOR TISSUE DIAGNOSIS OF OBSTRUCTIVE JAUNDICE SECONDARY TO BILIARY STRICTURES
D. Raine, S. Ramakrishnan, V. Wadehra1, M. Egan1, R. M. Charnley, K. Oppong.HPB Unit Freeman Hospital and 1Department of Cellular Pathology (Cytology) Royal Victoria Infirmary Newcastle upon Tyne, UK
Background: ERCP guided biliary brushings (ERCP-BB) has a reported sensitivity for malignancy between 30–88% with generally higher sensitivity for bile duct malignancies compared to pancreatic. Endoscopic ultrasound guided fine needle aspiration (EUS-FNA) has a reported sensitivity between 64–96%. However there have been few direct comparisons of the two sampling techniques.
Methods: Retrospective study of patients with obstructive jaundice secondary to a mass or stricture (on CT) who required biliary drainage, EUS staging, and a tissue diagnosis prior to surgery or palliative chemotherapy. 17 consecutive patients (9F, 8M) were identified in whom EUS-FNA and ERCP-BB were performed during the same session (6 patients) or within a few days (11). The results of the first sampling technique were not known at the time of the second procedure. EUS-FNA and biliary brushings were performed using standard techniques. Malignant cytology by either technique, surgical histology, or one year follow up were used to determine final diagnosis
Results: Fifteen individuals had tissue diagnosis (14 malignant) or follow up (1 benign). Five of these had surgery. 10 of the biliary brushings were indicative of malignancy (5 definite, 5 suggestive). There were four false negatives (atypia) and one benign. Sensitivity 71%, specificity 100%, NPV 20%. For EUS-FNA there were also 10 indicative of malignancy (7 definite, 3 suggestive) There were four false negatives (2 benign, 2 low cellularity/unsatisfactory aspirates) and one benign. Sensitivity 71%, Specificity 100%, NPV 20%. Excluding the unsatisfactory aspirates sensitivity was 83%. Combining the two tests sensitivity 93% specificity 100%, NPV 50%
Conclusion: In this series the sensitivity of EUS-FNA and ERCP-BB are the same, whilst the combination is associated with an improved sensitivity and NPV. Therefore individuals undergoing ERCP and EUS-FNA either concurrently or in quick succession should have both BB and FNA performed.
227 ENDOSCOPIC CYSTGASTROSTOMY FOR PANCREATIC PSEUDOCYSTS: AN OUTCOME ASSESMENT
S. Nair, S. Ramakrishnan, R. M. Charnley, K. Oppong.Hepatobiliary Unit, Freeman Hospital, Newcastle Upon Tyne, UK
Background: Endoscopic cystgastrostomy is increasingly used as therapy for pancreatic pseudocysts (PP). Endoscopic ultrasound (EUS) guidance has been advocated to facilitate the procedure and reduce complications.
Aim: To evaluate the efficacy and safety of Endoscopic drainage of pancreatic pseudocysts and evolution of EUS use.
Methods: A retrospective study of all patients considered for Endoscopic drainage of pancreatic pseudocysts in a regional pancreatobiliary referral centre between 1 June 2002 and 30 July 2005.
Results: Thirty two patients underwent an endoscopic procedure with intent to drain a pancreatic pseudocyst during the study period. Data were available for 26 of the 32 patients (15 men, 11 female; median age 54 years). Three patients did not undergo pseudocyst drainage following a EUS examination. These three patients subsequently showed complete resolution on repeat imaging without any further intervention. 23 patients underwent cystgastrostomy; four patients with a duodenoscope without EUS assessment, seven with a radial EUS assessment followed by drainage using a duodenoscope, and 12 with EUS assessment and subsequent drainage using a therapeutic linear echoendoscope. During a median follow up period of 14.5 months, Endoscopic drainage was successful in 20 of the 23 patients (87%). Of these 20 patients, eight had complete resolution after the first procedure (40%) while 12 required multiple Endoscopic procedures (60%). Of the remaining three, one required additional percutaneos radiological pseudocyst drainage and two required surgical cystgastrostomy for complete resolution. The site of drainage was gastric body in 16, antrum in two, cardia in one, and duodenum in one. Following the initial endoscopic procedure complications occurred in seven of the 20 patients (35%) within 30 days. Puncture site bleeding in three (requiring transfusion in two), pancreatitis in one, secondary cyst infection in two, and pneumonia necessitating HDU care in one. All complications were managed conservatively and there were no deaths.
Conclusions: Endoscopic cystgastrostomy is an effective treatment for PP in carefully selected individuals. However this is associated with a 35% complication rate. Prior EUS examination altered management in 11%.
228 ENDOSCOPIC PALLIATION OF CONCOMITANT MALIGNANT BILIARY STRICTURE AND GASTRODUODENAL OUTFLOW OBSTRUCTION
A. Anderloni, F. Montino, M. Del Piano.Azienda Ospedaliera “Maggiore della Carità”, Novara, Italy
Background: Malignant biliary stricture (MBS) is a well known condition often complicating duodenal, biliopancreatic or hepatic malignancies. Nowadays endoscopic stenting is the treatment of choice of MBS palliation. More than 15% of the cases are complicated by gastroduodenal outflow obstruction (GOO). Recently Yim et al, Wang et al, and Del Piano et al proposed self expanding metallic stents (SEMS) as the best palliation in GOO if compared with surgical treatment. In the majority of the cases MBS precedes GOO but sometimes the two conditions can present concomitantly. In such situation a surgical bypass could be a good option but due to the short life expectancy of these patients an endoscopic approach can be proposed.
Aim: To evaluate the efficacy and the feasibility of endoscopic palliation of concomitant MBS and GOO.
Materials and Methods: Between January 1997 and February 2005, 10 consecutive patients (4 male, aged 66–82) presenting concomitant MBS and GOO were enrolled. All these patients underwent CT scan, MRCP, and perendoscopic duodenal and jejunal x ray during stenting procedure. The patients were sedated with diazepam and meperidine. The following two steps procedure was performed: (1) Enteral Wallstent 9×2 cm was positioned without dilation; (2) 24 hours later, the enteral stent was fully dilated with a 2 cm diameter balloon. Then, using the balloon lightly deflated as guide, the duodenoscope was introduced and, if feasible, a biliary stent was positioned. The 24 hour waiting time between step 1 and step 2 would be necessary to permit a sufficient stent expansion and anchorage to duodenal wall.
Results: The duodenal stent was succesfully positioned in all patients. Three anatomic conformation types were found: (A) biliary outlet proximal to the stricture (1 pt), (B) at the stricture (4 patients), or (C) distal to the stricture (5 patients). Biliary endoscopic stenting was successful in all patients with conformation type A and C and only one out of four patients with conformation type B. The remaining type B patients were managed by PTC. No procedure related mortality or morbidity were observed.
Conclusions: This procedure is a feasible and safe treatment for concomitant MBS and GOO. 70% success rate was achieved and these patients were discharged after 48–72 hours.
229 COMPARISON OF DIAGNOSTIC YIELD BETWEEN BILIARY BRUSHINGS AND BILIARY BIOPSY: RESULTS OF A PILOT STUDY
F. Ali1, D. Richards1, G. Anagnostopoulos2, A. Zaitoun2, P. Griffiths1, N. Tofazzal1, K. Ragunath2, G. Aithal2.1Morriston Hospital, Swansea; 2Queen’s Medical Centre, Nottingham, UK
Purpose: To evaluate the diagnostic accuracy of Mighty Bite biliary forcep biopsy compared with biliary brush cytology in the analysis of suspected malignant biliary strictures at ERCP.
Methods: A two centre collaborative prospective study was carried out involving 49 patients (21 male, 28 female; mean age 70 years) undergoing ERCP for suspected malignant strictures. Both forcep biopsies and brush cytology taken in each patient. First tissue sampling technique randomised. Sample size and difficulty with sampling recorded. The histology and cytology samples were analysed separately. The final diagnosis was confirmed at surgery, further pathology, or subsequent clinical course.
Results: Available in 44 cases (23 Swansea, 21 QMC). Five excluded (1 no results, 4 sampling not possible). There were 42 malignant strictures inc. 17 pancreatic and 23 cholangio carcinomas. Overall sensitivity of Mighty Bite was 44% (57% Swansea, 30% QMC) 95% CI 28 to 60% v 55% (45% Swansea, 65% QMC) 95% CI 39 to 70% for brush cytology. Specificity and positive predictive value was 100% in both groups. Diagnostic accuracy was 46.5% v 56.8%. Overall sensitivity improved to 69% (95% CI: 53 to 82%) for combined sampling. Sensitivities were greater for cholangiocarcinoma compared to pancreatic cancer (brushings 61% v 47%, Mighty Bite 44% v 37%). Sensitivity of mighty bite improved from 35% to 53% if Mighty Bite preceded cytology. There were no immediate or late complications in either technique.
Conclusion: Mighty Bite cannot be recommended as a single sampling modality. However, it is generally safe and can improve diagnostic yield if combined with brush cytology in the investigation of suspected malignant biliary strictures.
230 LONG TERM OUTCOME OF PATIENTS WITH SPHINCTER OF ODDI DYSFUNCTION AFTER ENDOSCOPIC SPHINCTEROTOMY: A PROSPECTIVE STUDY
S. P. Pereira1, A. Gillams2, S. N. Sgouros1, G. J. M. Webster1, A. R. W. Hatfield1.Departments of Gastroenterology1 and Radiology2, University College Hospital, UCL Hospitals NHS Foundation Trust, London, UK
Background and Aims: Sphincter of Oddi manometry (SOM) is the gold standard for the diagnosis of sphincter of Oddi dysfunction (SOD) and predicts response to sphincterotomy. However, most studies have had relatively short follow up and there are few data from the UK. We aimed to assess the long term outcome of consecutive patients with suspected SOD II (pancreaticobiliary-type pain + duct dilatation or abnormal liver biochemistry/recurrent pancreatitis) or III (pain alone) who were referred for SOM ± sphincterotomy.
Methods: SOM was performed using a standard water perfused manometry catheter, and SOD diagnosed when the mean basal sphincter pressure was >40 mm Hg (sustained for >30 seconds and observed in both leads). Where indicated, an endoscopic sphincterotomy of the affected segment (biliary, pancreatic, or both) was performed. Patients were assessed clinically before SOM and at outpatient review or by telephone after discharge. Patients were asked to rate their symptoms on an 11-point Likert scale (0 = no pain at all, 10 = worst pain imaginable).
Results: Of 47 patients (M/F 9/38; mean age 46 years, range 27–69 years) referred for SOM, 27 (57%) had manometrically proven SOD: 16 type II and 11 type III. During a mean follow up of 31.6 months (range 17–44 months), patients with SOD type II experienced a significant reduction in symptoms (mean Likert score 9.0 v 1.6; p = 0.0002), as did those with normal SOM who did not undergo sphincterotomy (8.0 v 4.0; p = 0.03). However, in patients with SOD type III there was no improvement in mean pain scores after sphincterotomy (8.0 v 6.1; p = 0.24). Patients with SOD II were more likely to benefit from endotherapy than those with SOD III (p = 0.0009).
Conclusions: Patients with manometrically proven SOD type II derive a sustained benefit from endoscopic sphincterotomy of the affected segment, in contrast to those with SOD type III.
Gastroduodenal posters
231 IMPLEMENTATION OF CONVENTIONAL AND REAL-TIME PCR FOR ROUTINE DIAGNOSIS OF HELICOBACTER PYLORI INFECTION AND ANTIBIOTIC RESISTANCE
S. A. Chisholm, R. J. Owen, (introducedby KEL McColl).Health Protection Agency Centre for Infections, London NW9 5HT, UK
Background: Culture from gastric biopsy is the standard approach to determine H pylori antibiotic susceptibility. However test sensitivity may be compromised by the fastidiousness of H pylori, by effects of therapy, and by loss of viability and/or overgrowth of contaminating microorganisms. We demonstrated previously the excellent sensitivity and specificity of a multiplex PCR assay when applied to gastric biopsies for detection of H pylori and/or “H heilmannii”-like organisms (HHLOs), and of two real-time probe hybridisation assays for clarithromycin and tetracycline susceptibility testing.
Aim: To evaluate, in parallel with culture based methods, the implementation of a specialist molecular service for detection and susceptibility testing of helicobacters from gastric biopsies.
Results: From 2003 to date, gastric biopsies from 154 patients, of whom at least 50% were known treatment failures, were tested. None was HHLOs PCR positive. Of the 63 H pylori culture positive biopsies (41%), 62 were PCR positive (98% sensitive). Interestingly for the culture negative biopsies, PCR identified a further 25 H pylori positive patients (16% of all patients). Of these, overgrowth of microbial contamination was recorded for 10 samples, while three samples underwent severe transport delays. In spite of the failure to obtain culture from these 25 samples, susceptibilities to clarithromycin (17 resistant, seven sensitive) and tetracycline (23 sensitive, one resistant) could be determined in 24 biopsies by real-time PCR.
Conclusion: PCR assays are an invaluable adjunct to culture methods for diagnosis and drug resistance determination of H pylori infection.
Discussion: Routine PCR based testing was particularly useful in instances where the specimen was contaminated or underwent severe transport delays. Of the 88 H pylori positive results, 25 (28%) were determined by PCR alone. Furthermore for 16% of all patients, molecular identification of antibiotic resistance provided information that otherwise could only be obtained by repeat endoscopy.
232 HELICOBACTER PYLORI INDUCED UPREGULATION OF HB-EGF, BUT NOT COX-2 TRANSCRIPTS IN GASTRIC EPITHELIAL CELLS IS VIA THE EPIDERMAL GROWTH FACTOR RECEPTOR
P. Tomtitchong, P. A. Robinson, J. E. Crabtree.Molecular Medicine Unit, St James’s University Hospital, Leeds, UK
Introduction:H pylori transactivates the epidermal growth factor (EGFR) and upregulates HB-EGF in gastric epithelial cells. The aim of this study was to investigate if H pylori induced upregulation of COX-2 and HB-EGF transcripts in gastric epithelial cells was through the EGFR.
Methods:H pylori (NCTC11637, cag PAI+ and G50, cag PAI-) were co-cultured with MKN-28 gastric epithelial cells for 45 minutes to 24 hours. EGF (100 ng/ml) was used as a positive control. Both COX-2 and HB-EGF transcripts were determined by Northern blot. EKB-569 (0.01-1 μM), a specific inhibitor of EGFR, was used in co-culture experiments.
Results: Both H pylori strains upregulated COX-2 and HB-EGF transcripts with maximum expression at 12 hours post-infection. EGF-induced COX-2 and HB-EGF transcripts were maximal at 3 hours post-stimulation. EKB-569 did not significantly reduce H pylori induced COX-2 expression at 12 hours (n = 4), but significantly inhibited EGF induced COX-2 expression (n = 5, p<0.01) at a concentration of 0.5 μM. EKB-569 dose dependently at 3 hrs reduced H pylori induced HB-EGF expression (n = 4, p<0.05; 0.5 μM). Significant inhibition of EGF induced HB-EGF expression (n = 6, p<0.05) was observed at an EKB-569 concentration of 0.01 μM. EKB-569 dose dependently reduced basal COX-2 (n = 5, p<0.05; 0.5 μM) and basal HB-EGF transcripts (n = 7, p<0.05; 0.1 μM) in unstimulated cells 3 hours post-treatment.
Conclusions:H pylori induced upregulation of COX-2 and HB-EGF transcripts in gastric epithelial cells. H pylori induced HB-EGF transcripts, but not COX-2 transcripts, could be inhibited by a specific inhibitor of the EGFR.
233 GASTRIN AND MEMBERS OF THE BCL-2 FAMILY REGULATE GASTRIC EPITHELIAL APOPTOSIS IN VIVO
S. Przemeck1, C. A. Duckworth1, A. Varro2, D. Pritchard M. Pritchard1.1Division of Gastroenterology and 2Physiological Laboratory, University of Liverpool, UK
Introduction: Gastric epithelial cells undergo apoptosis following Helicobacter infection and this is thought to be important during gastric carcinogenesis. Factors which alter the susceptibility of gastric epithelium to undergoing apoptosis may therefore have consequences for the development of gastric carcinoma. We have investigated the induction of gastric epithelial apoptosis in two transgenic mouse models (hypergastrinaemic (INS-GAS) mice and gastrin knockout (GAS-KO) mice) which develop spontaneous gastric carcinoma. In addition, as the bcl-2 family of proteins are important regulators of small intestinal and colonic apoptosis in vivo, we have investigated whether the expression of a pro-apoptotic (bak) or anti-apoptotic (bcl-2) family member alters sensitivity to induction of gastric epithelial apoptosis.
Methods: Apoptosis was assessed on a cell positional basis in H and E stained sections of formalin fixed gastric antrum and corpus of 10–12 week old male INS-GAS, GAS-KO, bak-/-, and bcl-2-/- mice and their wild-type counterparts 6 hours and 48 hours following 12 Gy γ-radiation.
Results: Apoptotic cells were observed in the proliferative zones of gastric antrum and corpus in all mice following γ-radiation. Mice with abnormal concentrations of serum gastrin showed little difference in antral apoptosis compared to wild-type, but radiation induced apoptosis was significantly increased in INS-GAS corpus at 48 h (2-fold) and in GAS-KO corpus at 6 hours (4-fold) and 48 hours (1.5-fold). Radiation induced apoptosis was significantly suppressed in bak-/- antrum at 6 hours (1.5-fold) and bak-/- corpus at 48 hours (twofold) and was significantly increased in bcl-2-/- antrum (fourfold) and corpus (10-fold) at 6 hours compared to wild-types.
Conclusions: (1) Increased serum concentrations of gastrin and the absence of gastrin (leading to achlorhydria and bacterial overgrowth) both render the gastric corpus more susceptible to radiation-induced apoptosis. (2) Radiation induced gastric epithelial apoptosis is suppressed in bak-/- mice and increased in bcl-2-/- mice, suggesting that this family of proteins may be important during gastric carcinogenesis.
234 GASTRIC HISTOLOGY, SEROLOGICAL MARKERS AND AGE AS PREDICTORS OF GASTRIC ACID SECRETION IN H PYLORI INFECTED SUBJECTS
M. H. Derakhshan, E. El-Omar, K. Oien, D. Gillen, V. Fyfe, J. E. Crabtree, K. E. L. McColl.Department of Medicine and Therapeutics, University of Glasgow, UK
Background and Aim: Acid secretion is intimately associated with most upper gastrointestinal diseases. H pylori infection is a major environmental factor modifying acid secretion. We have studied the association between the pattern of H pylori gastritis and gastric secretory function in a large number of subjects without specific upper GI disease.
Method and Materials: Maximal acid output was measured in a total of 255 dyspeptic patients with normal endoscopy. Activity and severity of gastritis, atrophy, and H pylori infection were assessed in body and antral biopsies. The correlations of histologic parameters as well as age, gender, height, weight, smoking, serum gastrin, pepsinogen I, II, and their ratio with acid output were determined. We used multiple linear regression to show possible best predictors of acid output.
Results:Negative relationships: Body atrophy and body combined (active and chronic) inflammatory scores showed potent inverse correlation with acid output (correlation coefficients (CC): 0.59, p<0.01 and CC: 0.50, p<0.01 respectively). Body/antral chronic gastritis ratio and body/antral combined inflammation ratio (both with CC: 0.49, p<0.01) and age (CC: 0.44, p<0.01) were also inversely correlated with acid output. Positive relationships: Serum pepsinogen I, body H pylori density/combined inflammation ratio and pepsinogen I/II ratio with CC of 0.38 (p<0.01), 0.38 (p<0.01), and 0.30 (p<0.01) respectively, correlated with acid output. The H pylori density/combined inflammation of both antrum and body positively correlated with acid output (CC: 0.29 and CC: 0.38 respectively). Male gender and patient height also positively correlated with acid output. Modelling showed that body combined inflammatory score, body atrophy, age and serum pepsinogen I are independent predictors of acid output (r2 = 0.62).
Conclusion: Combination of body inflammation, body atrophy, age, and serum PGI can be used for prediction of acid secretory state in H pylori infected population.
235 PRE-ENDOSCOPY DISCHARGE FOR UPPER GASTROINTESTINAL HAEMORRHAGE: IS IT SAFE?
U. Warshow, N. Hare, A. Sanyal, I. A. Murray, H. R. Dalton.Royal Cornwall Hospital, Truro, Cornwall TR1 7LJ, UK
Introduction: Upper gastrointestinal haemorrhage (UGIH) is a very common indication for acute medical admission. The commonest cause is peptic ulcer bleeding, 80% of which will stop spontaneously. Many patients will have minor bleeding from gastritis or oesophagitis. Scoring systems for UGIH have been devised to determine the severity of bleeding with regard to need for endoscopic therapy, transfusion or surgery, and death. We studied whether any could be used to determine safety of discharge pre-endoscopy.
Method: For all patients admitted with UGIH over one year, we prospectively recorded their pre-endoscopy Rockall score and Glasgow Blatchford score (GBS: Blatchford et al, 2000). From our previous retrospective audit using ROC analysis, we were particularly interested in those under the age of 70 with a GBS ⩽2 or a pre-endoscopy Rockall score ⩽1. After discharge, we reviewed their casenotes and recorded endoscopic therapy, rebleed, transfusion requirements, need for surgery, length of stay (LOS) and death.
Results: 232 patients were admitted over one year, solely due to UGIH. Of these 66 were under the age of 70 with a GBS of ⩽2, 5 of whom required endoscopic intervention (7.5%). 105 patients presented with a pre-endoscopy Rockall score of ⩽1, 18 of whom (17%) required endoscopic intervention. One patient with low GBS and 19 of the low pre-endoscopy Rockall group required transfusion (1.5% v 18%). None of the low GBS group but two of the low pre-endoscopy Rockall group required surgery. There were no deaths in either group. The LOS for the low GBS group was similar to the low pre-endoscopy Rockall group (2.66 days v 2.92 days respectively).
Discussion: The GBS identified 28% of patients admitted with UGIH as being potentially safe for early discharge (with planned early outpatient endoscopy). The pre-endoscopy Rockall score identified 45% as being potentially suitable, but with considerable loss of sensitivity with respect to need for endoscopic intervention, transfusion and surgery. Even with low GBS, there was a need for endoscopic intervention in 7.5% of patients, calling into doubt whether early pre-endoscopy discharge can ever be safe.
236 HOW SIGNIFICANT IS A HISTORY OF COFFEE-GROUND VOMITING?
D. Gavin, O. Saraj, D. Ng.General Hospital, St Helier, Jersey, UK
Objectives: Many clinicians believe that a history of vomiting coffee-grounds is a poor predictor for the presence of a significant haemorrhagic lesion in the upper gastrointestinal tract. We aimed to test this hypothesis.
Methods: This was a retrospective study of patients presenting to an island district general hospital with upper gastrointestinal bleeding over a three year period. The case notes for each patient were reviewed and the history of presenting complaint scrutinised for a history of “coffee-ground vomiting”, “fresh haematemesis”, or “melaena”. The endoscopic findings for these patients were then reviewed.
Results: A total of 100 patients were identified. Of these, 33 had a history of “coffee-ground vomiting”, 38 “haematemesis”, and 29 “melaena”.
Conclusion: We can conclude from this series that a history of coffee-ground vomiting alone is a poor predictor for the presence of a significant haemorrhagic lesion at endoscopy. It would be reasonable to manage these patients without inpatient endoscopy. A history of fresh haematemesis and particularly of melaena is a strong predictor and these patients should undergo endoscopy as part of their acute management.
Abstract 236
237 GASTROINTESTINAL SYMPTOMS IN PATIENTS UNDERGOING HAEMODIALYSIS TREATMENT
A. E. Cano, A. Barnabas, A. K. Neil, S. R. Nelson1, I. C. R. Hartley2, J. D. Maxwell, J. Y. Kang.Departments of Gastroenterology and 1Renal Medicine, St Georges Hospital, 2Pepys Road Surgery, London, UK
Background: Gastrointestinal (GI) symptoms are said to be common in patients with end-stage renal disease undergoing maintenance haemodialysis treatment (HD), but few data are available.
Aims: To assess the prevalence of GI symptoms in patients with end-stage renal failure undergoing HD, and to compare them to sex and age matched (±10 years) general medical outpatients without renal failure, as well as community subjects.
Methods: Patients and hospital controls completed a locally validated Rome II questionnaire. Community controls received and returned questionnaires by post.
Results: Of 104 patients on HD treatment 100 (96%) completed the study. The prevalence of various gastrointestinal symptoms was compared with that of 100 general medical outpatients and 100 community controls. Some of the comparisons are shown in the table.
Abstract 237
Conclusions: Almost half of HD patients use laxatives regularly and one fifth report constipation as defined by Rome II criteria. These prevalence rates are higher than those for medical outpatients and community controls. Heartburn and IBS are also more common among patients on HD.
238 COMPARISON OF ZINC VERSUS TWO BISMUTH BASED THERAPIES AFTER FAILURE TO ERADICATE HELICOBACTER PYLORI WITH STANDARD TRIPLE TREATMENT
B. Baburajan1, S. Bridger2, L. Doig1, R. P. H. Thompson3.1Guy’s and St Thomas’s Hospitals NHS Trust; 2Worcestershire Acute Hospitals NHS Trust; 3The Rayne Institute, King’s College, London, UK
Background: Treatment failure of Helicobacter pylori remains a problem. There are limited data on the efficacy of second line regimens. Increasing antibiotic resistance is probably a factor in primary and secondary treatment failure. Metal based approaches may reduce antibiotic resistance and have a synergistic antibiotic effect.
Aim: To compare bismuth and zinc based quadruple regimes in peptic ulcer patients with H pylori refractory to triple treatment.
Methods: Eighty consecutive patients with peptic ulcer disease with positive 13-C urea breath tests at least four weeks after standard triple treatment, received one of three regimes: (1) ranitidine bismuth citrate 400 mg bd (B), omeprazole 200 mg bd (O), amoxicillin 1 g bd (A) and clarithromycin 500 mg bd (C) (BOAC); (2) BOA and metronidazole 400 mg bd (M) (BOAM) or (3) Solvazinc 125 mg tds (Z) and OAM (ZOAM). Eradication was defined as a negative breath test at least one month after completing therapy.
Results: Per protocol eradication was achieved in 20/22 (90.9%) with BOAC, 29/34 (85.3%) BOAM, and 10/18 (55.6%) with ZOAM. Intention-to-treat eradication was 20/25 (80%), 29/36 (80.6%), and 10/19 (52.6%), respectively. The bismuth based regimes were both significantly better than the zinc regimen, with a combined odds ratio of 5.5 (95% confidence limits 1.6–19, p = 0.0034). Metronidazole was not significantly different from Clarithromycin.
Conclusion: Ranitidine bismuth citrate, omeprazole, amoxicillin, and either clarithromycin or metronidazole is an effective quadruple combination for salvage treatment of H pylori without knowledge of antibiotic resistances. Zinc was not as effective as bismuth.
239 EVALUATION OF THE EFFICACY OF HELICOBACTER PYLORI ERADICATION IN A DISTRICT GENERAL HOSPITAL
M. R. Aljabiri, G. Arora, S. Nugent, D. O’Riordan, R. E. Cowan.Colchester General Hospital, Colchester, Essex, UK
Introduction:Helicobacter pylori is a very important pathogenic factor in peptic ulcer disease and its eradication can lead to cure. Thus the National Institute of Health recommended in 1994 giving H pylori eradication treatment to all patients with active peptic ulcer disease or a history of the same and proven infection. Likewise, the European Helicobacter Study Group in 1996 made similar recommendations while adding bleeding peptic ulcers and low grade MALT lymphoma to the list of those requiring eradication therapy. The combination of proton pump inhibitor and two antibiotics (triple therapy) is widely used for eradication but most GI endoscopy units do not routinely check the efficacy of this treatment.
Aim: To evaluate the efficacy of H pylori eradiation in a British district general hospital, using the C13-urea breath test (UBT).
Methods: Retrospective analysis was performed of 399 UBT results from patients treated for H pylori infection identified at gastroscopy during the period February 2001 to December 2004 in a district general hospital in provincial UK, serving both rural and urban populations. There were 235 (59%) males and 164 (41%) females with a male: female ratio of 1.4:1. Indications for the diagnostic gastroscopy included dyspepsia 119 patients (29.7%), epigastric pain 41 patients (10.2%), gastrooesophageal reflux symptoms in 37 patients (9.2%), and nausea 25 patients (6.2%).
Results: 374 (93.7%) of the 399 patients who received eradication therapy were UBT negative 8–12 weeks post treatment. The 25 patients (6.3%) with positive UBT results received a further course of triple therapy and of these 15 patients produced a negative UBT when this was repeated at 12 weeks post treatment. The remaining 10 patients received a further course of therapy and six remained UBT positive. Four of these patients had a third course of treatment, comprising quadruple therapy and of these two patients became breath test negative. The two patients who remained positive did not attend for further testing.
Conclusions: This high eradication rate (93.7%) after one course of triple therapy is reassuring and concurs with published results (BMJ 1998;316:1648–54). This was achieved with the combination of Lansoprazole, Amoxicillin, and Clarithromycin, except when sensitivities or adverse drug reactions suggested that alternative agents should be used, usually Metronidazole or Ciprofloxacin. Patients who were UBT positive post eradication (6.3%) were assumed to be either poorly compliant with treatment or their organism was resistant to one or more of the antibiotics.
Conclusions: In this small group of patients H pylori eradication continued to be difficult with 24% remaining positive after a second course of eradication treatment and 50% after a third. This raises two questions: (1) are those patients with persistent H pylori infection more liable to complication and (2) should they be the subject of further testing to determine whether their particular organism is either cagA or cagB positive—analysis that might help to decide whether successful eradication must continue to be pursued?
240 PREVALENCE OF DYSPEPSIA SYMPTOMS IN THE ELDERLY: HOW THEY VARY WITH SEX AND INCREASING AGE, AND THE EFFECT ON RESOURCE USE
S. J. Philpott1, K. Sundaram2, M. Mendall1.1Mayday Hospital, Croydon, CR7 7YE; 2St Georges Hospital, London SW17, UK
Background: The burden of dyspepsia and reflux disease has not been studied in extreme old age in a community sample. It is likely that at extreme old age, with autonomic failure, symptoms may become less severe despite the fact that pathology is likely to become more severe. We therefore aimed to determine the prevalence of reflux and dyspepsia symptoms in an elderly community sample and sought to determine whether symptoms do indeed become less prevalent as age progresses or whether they differ for men and women. We also examined dyspepsia related resource use and how it varied with extreme age.
Method: Cross sectional, retrospective study. Patients aged 60+ were randomly selected from local GP lists Croydon and sent a questionnaire containing Leeds Dyspepsia questions. GP list were scrutinised for resource use in the participating patients over the past five years.
Participants: 2100 pts were randomly selected from 28 GP lists, of which 1116 patients responded (60%). Patients were divided into three age groups: (1) 60–69 years (n = 564), (2) 70–79 years (n = 390), and (3) 80+ years (n = 162).
Results: Dyspepsia was prevalent in 33%, 28%, and 27% of the age groups respectively, and reflux in 35%, 32%, and 30% (p = NS). When broken down, abdominal pain decreased with age (18% v 12% v 9%, p = 0.002), though only significantly in women. Among men, reflux symptoms decreased with age significantly (36% v 30% v 17%), whereas in women this increased though not significantly (34% v 34% v 40%). Resource use did not vary significantly across the age groups for either sex.
Conclusion: There is some evidence of a level of reduction in reflux and dyspeptic symptoms with extreme old age, but the pattern differs between men and women. Resource use did not vary with age suggesting that elderly patients remain a burden on the health service.
241 H PYLORI, SEX, AND THE RELATION OF EXTREME OLD AGE TO DYSPEPSIA
S. J. Philpott1, K. Sundaram2, M. Mendall1.1Mayday Hospital, Croydon, CR7 7YE; 2St Georges Hospital, London SW17 0RE, UK
Background:H pylori (HP) is a risk factor for dyspepsia (non-ulcer and ulcer associated). However this association has only been studied in younger populations. There is also controversy as to whether HP through destroying the acid making capability of the stomach may actually protect against reflux disease. The best population to observe this effect on would be the elderly in whom HP infection would have run the longest course. We aimed to investigate the association of HP with reflux and dyspeptic symptoms in an elderly population.
Method: Cross sectional, retrospective study. Patients aged 60+ were randomly selected from local GP lists in Croydon and sent a questionnaire containing the Leeds Dyspepsia questions, and a kit for saliva collection to determine HP status. Medical records were examined for all events over a five year period. HP status was determined using ELISA and Western blotting methods as previously described.
Participants: 2100 patients were randomly selected from 28 GP lists, of which 1116 patients responded (60%). Patients were divided into three age groups: (1) 60–69 years (n = 564), (2) 70–79 years (n = 390), and (3) 80+years (n = 162).
Results: 137/499 men and 167/617 women were HP positive. Dyspepsia was prevalent in 23% men and 35% women and did not change with age, and reflux in 31% men and 34% women. Reflux symptoms decreased with age for men only. HP infection increased with age for men (21% in group 1 v 34% in groups 2 & 3) but not for women (27%, 28%, and 25%). In men, 31% with HP had dyspepsia v 20% without (p = 0.01). This risk was not seen in the 80+ group (21% with HP v 17% without). There was no association with reflux. In women those with HP were less likely to have any reflux symptoms than those without (29% v 37%), although this was not significant (p = 0.06), and did not differ by age group.
Conclusion: In men, HP was associated with having dyspepsia, but this was not seen in extreme old age suggesting the effect of HP reduces with age. We found that HP may be protective against reflux but this was more marked in women.
242 EFFECT OF SIBLING NUMBER AND BIRTH ORDER ON HELICOBACTER PYLORI PREVALENCE: A CROSS SECTIONAL SURVEY
A. C. Ford1, A. G. Bailey1, D. Forman2, A. T. R. Axon1, P. Moayyedi3..1Centre for Digestive Diseases, Leeds General Infirmary, Leeds; 2Centre for Epidemiology and Biostatistics, Leeds University Medical School; 3Gastroenterology Division, Health Sciences Centre, Hamilton, Canada
Introduction: Social conditions influencing the acquisition of Helicobacter pylori in childhood are well recognised, but the effect of number of siblings, and birth order on prevalence of H pylori has not been extensively reported.
Methods: The authors performed a 10 year follow up cross sectional survey of individuals previously enrolled in a community screening and treatment programme for H pylori. Prevalence of H pylori was assessed with 13carbon-urea breath testing. All individuals who were alive, and could be traced were contacted by postal questionnaire, to obtain information on both total number of siblings, and their order of birth. Data concerning other social conditions in childhood were stored on file from the original study.
Results: 3928 (47%) of the 8407 original participants provided data. Prevalence of H pylori infection increased steadily according to total number of siblings, from 20% in those with no siblings, to 63% with eight or more. Odds of infection were significantly increased with three siblings (odds ratio (OR) for infection = 1.79; 95% CI 1.34 to 2.38), and a clear gradient of effect continued up to eight or more siblings (OR = 6.66; 95% CI 3.94 to 11.44). Odds of infection became significantly higher with two older siblings (OR = 1.32; 95% CI 1.04 to 1.68), and again increased steadily up to six (OR = 3.78; 95% CI 1.51 to 9.74). Even among firstborn individuals, prevalence of infection significantly increased with three or more siblings (OR = 1.59; 95% CI 1.02 to 2.44). When number of siblings, and other social conditions in childhood were controlled for in a logistic regression model, the association between birth order and odds of H pylori infection was no longer statistically significant.
Conclusions: Number of siblings and birth order appear to influence prevalence of H pylori infection, though the observed effect of birth order may be due to confounding by other factors in childhood.
243 A 10 YEAR NATURAL HISTORY OF GASTROOESOPHAGEAL REFLUX DISEASE
A. C. Ford1, A. G. Bailey1, D. Forman2, A. T. R. Axon1, P. Moayyedi3.1Centre for Digestive Diseases, Leeds General Infirmary, Leeds; 2Centre for Epidemiology and Biostatistics, Leeds University Medical School; 3Gastroenterology Division, Health Sciences Centre, Hamilton, Canada
Introduction: Gastrooesophageal reflux disease (GORD) is common in the general population, with a reported incidence as high as 20%. However, there is little information regarding the long term natural history of the disorder.
Methods: The authors performed a 10 year follow up cross sectional survey of individuals recruited into a community screening and treatment programme for Helicobacter pylori. All surviving, traceable participants were contacted, by validated postal dyspepsia questionnaire, which contained items relating to GORD symptoms. Baseline demographic data and GORD symptom data were stored on file from the original study.
Results: Of 8407 individuals, 4003 (48%) responded to the questionnaire. The mean age of responders was 55 years, and 2247 (56%) were female. Males, those with dyspepsia at baseline, smokers, and those of lower social class were significantly less likely to respond (p<0.0001). There were 550 (14%) subjects with GORD symptoms at a frequency of more than once a week at baseline. Of these 240 (44%) still had at least one dyspeptic symptom at a frequency of once a week or more at 10 year follow up, and heartburn remained the predominant symptom in 167 (30%) of these, while 301 (55%) had symptoms less than once a week or were entirely asymptomatic. Of the 3421 individuals who were asymptomatic at baseline, 629 (18%) had heartburn at a frequency of once a month or more, 196 (5.7%) once a week or more, and 39 (1.1%) once a day or more. Heartburn was the predominant dyspeptic symptom in 540 (16%) of these individuals at 10 years.
Conclusions: During 10 years of follow up approximately a third of individuals with GORD remained symptomatic, while in those without symptoms at baseline over five percent had developed new onset GORD symptoms at a frequency of once a week or more.
244 A CROSS SECTIONAL SURVEY OF THE RELATIONSHIP BETWEEN GASTROOESOPHAGEAL REFLUX DISEASE AND CHRONIC COUGH
A. C. Ford1, A. H. Morice2, A. G. Bailey1, D. Forman3, A. T. R. Axon1, P. Moayyedi4.1Centre for Digestive Diseases, Leeds General Infirmary, Leeds; 2Division of Academic Medicine, University of Hull, Castle Hill Hospital, Cottingham; 3Centre for Epidemiology and Biostatistics, Leeds University Medical School; 4Gastroenterology Division, Health Sciences Centre, Hamilton, Canada
Introduction: Gastrooesophageal reflux disease (GORD) has been recognised as an important cause of chronic cough, but the frequency with which the two are reported to be related varies widely.
Methods: The authors performed a cross sectional survey to establish prevalence of self-reported chronic cough and its relationship to GORD. The study was performed as part of a 10 year follow up of individuals recruited into a population Helicobacter pyloriscreening programme. All surviving, traceable participants were contacted, by validated postal dyspepsia questionnaire, and were also asked how often in the last two months they had experienced bouts of coughing, rated on a five-point Likert scale. Baseline demographic data were already on file.
Results: Of 8407 individuals originally involved, 3880 (46%) responded, 425 (11%) of whom had GORD at 10 years. The odds ratio (OR) for GORD increased with frequency of cough (cough less than once a month OR 1.79; 95% CI 1.36 to 2.36, once a month to once a week OR 2.35; 95% CI 1.66 to 3.30, once a week to once a day OR 3.71; 95% CI 2.62 to 5.20, once a day or more OR 4.15; 95% CI 2.86 to 5.96). This association remained stable during logistic regression controlling for age, gender, smoking status, social class, and alcohol use. The ORs for presence of cough were also higher in those who complained of passing mucus PR, though lower than for GORD.
Conclusions: Subjects with cough are more likely to suffer from symptoms of GORD than those without; supporting the contention that reflux is an important cause of chronic cough in the community. However, the fact that some of the observed association may be due to individuals who complain of multiple symptoms cannot be excluded.
Endoscopy posters
245 PROSPECTIVE 19 MONTH AUDIT OF THE CLINICAL USE OF CAPSULE ENDOSCOPY: THE ROYAL LONDON HOSPITAL EXPERIENCE
S. Mukherjee1, T. Taylor2, N. U. Beejay1,2.1Newham Healthcare NHS Trust, Glen Road, London; 2Barts and the London NHS Trust, Whitechapel Road, London, UK
Background: Capsule Endoscopy (CE) was co-developed by Professor Paul Swain at Royal London Hospital in 2001. Despite widespread use in N America and Europe, CE uptake and service provision has been slower in the UK.
Methods: Prospective data on demographics, indications, findings, and complications were collected in a database since February 2004. The database was examined from February 2004 until September 2005. Summary statistics were calculated.
Results: 101 patients (49M), mean age was 49 (range 13–86). Indications included suspected Crohn’s disease (CD) (30/101), iron deficiency anaemia (IDA) (28/101), overt GI bleed (21/101), obscure GI bleed (4/101), anaemia of unknown aetiology (10/101), suspected Peutz Jeghers (PJ) (2/101), chronic abdominal pain (3/101), and 1/101 each of refractory coeliac disease, suspected small intestinal lymphoma, and suspected Behcets disease. Mean gastric and small bowel emptying time were 36.4 and 240 minutes respectively. CE explained the cause of IDA in 14/28 patients, the cause of suspected CD in 11/30, the cause of GI bleed in 15/21 (all 15 angiodysplasias). Each of 4/101 with obscure GI bleed had findings to explain their symptoms. One of the 2/101 with suspected PJ syndrome had a positive result. A single complication of capsule retention occurred in a single patient but resolved with conservative management. Image quality was good in 93/101 cases performed.
Conclusion: CE was diagnostic in 45% of patients, having a higher yield in patients with overt/obscure GI bleed than in suspected CD and IDA. CE is an extremely valuable tool for further evaluation of a difficult diagnostic group of patients.
246 CLINICAL IMPACT OF NORMAL AND ABNORMAL CAPSULE ENDOSCOPY FINDINGS IN 150 CONSECUTIVE PATIENTS
N. Arebi, B. P. Saunders, G. Schofield, D. Swain, R. Man, M. Vance, C. Fraser.St Mark’s Hospital, Harrow, UK
Background: Capsule endoscopy (CE) is useful for investigating small bowel disease. Its value in altering the clinical management of patients with a normal result has not been studied.
Methods: We conducted a retrospective analysis of all the cases of CE undertaken in St Mark’s Hospital over 20 months. Diagnostic yield and the impact of the findings on further clinical management were determined from the CE database and patient interviews.
Results: During the period under study 150 consecutive cases were performed. The indications were obscure gastrointestinal bleed (GIB) (100), Peutz-Jeghers Polyposis (PJP) (30), abdominal pain (10), Crohn’s disease (CD) (6), and others (4). CE was reported as normal in 52 (35%), abnormal in 73 (49%), equivocal in 16 (10%), and incomplete in nine (6%) cases. The overall diagnostic yield was 48.7%. The yield according to the indication was 39% for overt GIB, 46% for occult GIB, 83% for PJP, 11% for pain, 50% for CD, 25% for suspected CD, and 50% for other indications. In group with normal results 31/52 cases were contacted; 5/31 (16%) had a cause for symptoms identified while 26/31 (84%) had no cause identified by further investigations. A normal result changed clinical management in 15 of these 26 patients (58%). From the abnormal group 47/73 cases were contacted: 25 had PJP and 22 had other abnormalities. In the PJP group, the CE result led to a change in management in seven patients (28%) but had no influence on clinical management in 18 (72%). In the non-polyp group, the abnormality was treated with symptom resolution in 19 patients (86%) but had no effect on outcome in three (14%) cases where further intervention did not detect the lesion noted on CE. Although PJP had the highest diagnostic yield, it had the lowest impact on clinical management
Conclusion: This study suggests that the value of CE should be assessed by the clinical outcome of patients with both normal and abnormal results in addition to the diagnostic yield. Future studies on the benefit of CE in clinical management should include the impact of a normal result on future management decisions.
247 THE ROLE OF CAPSULE ENDOSCOPY IN SMALL BOWEL SURVEILLANCE OF ADULTS WITH PEUTZ-JEGHERS SYNDROME
C. Fraser1, G. J. E. Brown2, G. Schofield1, S. Taylor1, C. I. Bartram1, R. Phillips1, B. P. Saunders1.1Wolfson Unit for Endoscopy, St Mark’s Hospital UK; 2Colorectal Medicine and Genetics, RMH, Australia
Introduction: Capsule Endoscopy (CE) is a novel radiation-free tool for imaging the entire small bowel (SB), and has enormous potential in Peutz-Jeghers syndrome (PJS). We compared the performance of CE with barium follow through (BFT), the current standard, for the detection of significant SB polyps (SSBPs) in PJS adults.
Methods: Adults with PJS undergoing routine surveillance underwent both CE and BFT, which were reported blindly. SB polyps 1 cm or more were considered significant. The total number of SSBPs detected by each test and the number of participants in whom significant polyps were detected by each test were compared. Participants stated their preference for future surveillance.
Results: There were 19 participants (10 women; mean age 37); 10 had the BFT first. All capsules were excreted naturally. The caecum was visualised in 12 patients and the ileocaecal valve in a further two. The median total number of SSBPs detected in each participant by CE was four (range 0–18) and by BFT was one (range 0–5; p = 0.008). 12 participants had SSBPs by both CE and BFT; a further five had SSBPs by CE only (p = 0.06), and 2 had no SSBPs by either test. Of interest, all participants had evidence of gastric polyps by CE. Only limited verification of the SB findings has been possible to date. 16 patients preferred to have CE next time and one preferred BFT (p<0.001); one had no preference and one did not respond.
Conclusion: CE appears to detect more SB polyps of 1 cm or greater in more adults with PJS than BFT. Patients clearly prefer CE to BFT. Where available, CE should replace BFT for the surveillance of SB polyps in PJS adults.
248 WIRELESS OESOPHAGEAL VIDEO CAPSULE ENDOSCOPY: PRELIMINARY EXPERIENCE IN SEVEN PATIENTS
J. Pendlebury, S. Douglas JN Plevris.Centre for Liver and Digestive Disorders, Royal Infirmary of Edinburgh, UK
Background: Wireless oesophageal video capsule endoscopy (WOVCE) is a non-invasive, disposable imaging methodology for visualisation of the upper GI tract. These attributes make WOVCE a desirable investigative tool in select patients, notably those who may constitute a public health risk through transmissible infections and those who cannot tolerate conventional endoscopy.
Methods: In Edinburgh we have investigated an initial seven patients who fall into these categories. WOVCE was performed after a standard six hour fast, correct placement of the recording electrodes, and ingestion of 100 ml of water to clear saliva from the oesophagus. The capsule was ingested in a recumbent position, with sequential elevations of 30, 60, and 90 degrees over a period of 5 minutes. In the three most recent patients, left and right lateral positional manoeuvres were added to the protocol. At the end of this period each patient remained seated upright until capsule battery depletion ended the recording.
Results: In all seven patients oesophageal images were excellent, the OG junction was well defined and areas of pathology—for example, oesophagitis/varices were clearly visible. Images of the gastric mucosa were of variable quality with generally poor images of fundus (due to shadowing) improving as capsule neared antral/pyloric region. There were two instances where excessive food residue impaired all gastric views. Proximal duodenum was visualised in two patients. WOVCE was repeated in one of these patients with an extended fasting period (24 hours) and administration of metoclopramide (5 mg) 20 minutes prior to capsule ingestion. These protocol modifications resulted in improved gastric images showing no significant pathology and visualisation of a normal proximal duodenum.
Conclusions: From this early experience we consider that WOCVE is a valuable oesophageal imaging modality, for use in those patients where conventional endoscopic techniques are not possible, or as a non-invasive screening method. Modifications to protocols can enhance images recorded and result in a more detailed investigation of the upper GI tract, particularly the duodenum.
249 DOUBLE BALLOON ENTEROSCOPY UNDER CONSCIOUS SEDATION: PATIENT SAFETY, COMFORT, AND TOLERABILITY COMPARED TO OTHER ENDOSCOPIC PROCEDURES
J. A. Shah, P. A. Flower, R. Przemioslo, S. Hughes.North Bristol NHS Trust, UK
Introduction: Double balloon enteroscopy (DBE) allows examination of whole small bowel with therapeutic capability. It may be prolonged procedure associated with discomfort, raising the question as to whether it should be performed under conscious sedation or general anaesthetic.
Aim: To assess patient safety, comfort and tolerability of DBE under conscious sedation and compare it to other endoscopic tests.
Method: Nineteen patients with suspected small bowel disease were examined (17 oral and two anal). Data were recorded on sedation and reversal agents used and conscious level during procedure, depth of insertion, time taken, and therapy performed. A patient questionnaire was used to assess comfort during DBE and compare it to comfort during OGD, colonoscopy, and push enteroscopy (PE) and side effects experienced.
Results: DBE was performed in 19 (15 outpatients, 4 inpatients) patients. In 17 patients DBE was well tolerated after 50 mg Pethidine and average of 11 mg midazolam (range 5–20) and terminated prematurely in two patients. Flumazenil was used in one patient. Depth of insertion averaged 540 cm (range 80–880) taking an average of 48 minutes (20–95). There were no complications and therapy was carried out in 10/19 patients. Questionnaires were completed by 14/19 patients, of which 11 felt they were drowsy but arousable during DBE and three had no recollection. During DBE, one had severe discomfort, four each reported mild or moderate discomfort and one reported no discomfort. 10 patients felt OGD was as or more uncomfortable than DBE. 12 patients felt colonoscopy was as or more uncomfortable than DBE. Five patients had same discomfort as during PE and DBE. Mild side effects after DBE like bloating and diarrhoea were seen in six patients and were short lived. 13 patients said they would consent to further DBE under conscious sedation if required.
Conclusion: DBE is a safe and relatively comfortable procedure under conscious sedation. Mild side effects occurred in less than half the patients. Most patients found DBE to be as comfortable as other endoscopic tests and all except one patient would consent to further DBE under conscious sedation if necessary.
250 INITIAL EXPERIENCE OF DOUBLE BALLOON ENTEROSCOPY IN A NATIONAL TRAINING CENTRE FOR ENDOSCOPY
R. N. Patterson, J. Hoare, D. Swain, B. P. Saunders, C. Fraser.Wolfson Unit for Endoscopy, St Marks Hospital, London, UK
Background: Double balloon enteroscopy (DBE) is a novel technique allowing complete examination of the small intestine (SI), coupled with the ability to biopsy and perform therapeutic intervention. We report our initial experience of this new technique, describing a case series of the first 19 patients undertaken at St Mark’s Hospital.
Methods: We performed a chart review of all patients undergoing DBE during the period February to October 2005 in our Unit.
Results: Twelve male and seven female patients underwent DBE (mean age 55 years, range 20–90 years); 14 were performed per-oral and 5 per-rectum; 12 under sedation and seven under general anaesthesia. Of those performed orally, the duodenum, jejunum, and ileum were attained in 2, 5, and 7 patients respectively with a mean SI intubation distance of 235 (SD 81) cm. Rectal insertion achieved a mean SI intubation distance of 118 (SD 40) cm. The mean duration of DBE was 60 (SD 25) minutes. Indications included: 6/19 recurrent anaemia/obscure GI bleeding (32%), 9/19 overt GI bleeding (47%), 3/19 assessment/treatment of Crohn’s disease (16%), and 1/19 “other”. Of those 15 patients who previously had capsule endoscopy (CE) performed, DBE confirmed CE findings in 8/15 (53%), while in 6/15 (40%) patients, DBE was normal where CE had suggested pathology, and in one a small bowel neoplasm was misdiagnosed as a Dieulofoy lesion on CE. Directed biopsies were performed in 6/19 (32%) and therapy in 8/19 (42%; 7 APC, 1 ileal stricture dilatation). Of the seven patients who underwent APC, 3/7 (43%) have had ongoing bleeding and 4/7 (57%) have had either no or reduced blood transfusion requirements. No complications were observed either during or in the short term post-procedure period.
Conclusion: DBE is an exciting advance within GI endoscopy. It appears to be well tolerated and safe. For the first time, it provides the means to endoscopically investigate and treat disorders of the SI that have previously been inaccessible to conventional endoscopy. It has complimentary attributes to CE. Indications for its use continue to be defined.
251 CHROMOENDOSCOPY IN THE DIAGNOSIS OF EARLY OESOPHAGEAL NEOPLASIA
M. Gwiggner, S. R. Green, D. Poller, S. A. Somers, S. K. C. Toh, P. Bhandari.Portsmouth Hospitals NHS Trust, Portsmouth, UK
Introduction: Chromoendoscopy has shown great potential in diagnosis of early cancers. The procedure is more time consuming compared to conventional endoscopy reducing the number of endoscopies per session with obvious cost implications. This study aims to clarify the role of chromoendoscopy in improving the diagnosis and management of early oesophageal neoplasia.
Methods: A mixture of N-acetyl cystine and simethicone was administered per os prior to the endoscopy. Indigo carmine (0.4%) dye spray was used to detect subtle mucosal abnormalities. Acetic acid (2.0%) and/or methylene blue (0.5%) was used to characterise lesions in suspected Barrett’s oesophagus and Lugol’s Iodine (2.0%) in suspected squamous dysplasia. Pre- and post-chromoendoscopy histology data was collected and its influence on clinical management decisions noted. McNemar’s test was applied (SPSS) to the paired categorical data with respect to the change in histological staging.
Results: Seventy three consecutive patients undergoing oesophageal chromoendoscopy were analysed and divided into two groups. Group A consisted of 47 patients undergoing routine Barrett’s surveillance and group B of 26 patients who presented as a diagnostic challenge based on previous endoscopy and histology. Three of the 47 patients in group A were found to have indeterminate dysplasia. In group B, chromoendoscopy led to an alteration in histological grading in 14 of 26 patients, resulting in a p value of <0.001. Of the 16 patients with either high grade dysplasia or cancer, chromoendoscopy delineated focal lesions in seven patients so well that potentially curative endoscopic mucosal resection (EMR) could be performed. In the nine remaining patients the lesion was either multifocal or not well delineated so either PDT or surgery was required. Chromoendoscopy assisted in rationalising future surveillance intervals in the 10 patients with lower grades of dysplasia.
Conclusion: This series shows the potential of chromoendoscopy as a staging tool in the management of patients with suspected oesophageal dysplasia or early cancer. Its role in routine Barrett’s surveillance remains uncertain and calls for larger studies.
252 OPTICAL MICROANGIOGRAPHY: HIGH DEFINITION ZOOM COLONOSCOPY WITH NARROW BAND IMAGING TECHNIQUE FOR VISUALISING MUCOSAL CAPILLARIES AND RED BLOOD CELLS IN THE LARGE INTESTINE
K. Yao1, G. K. Anagnostopoulos1, A. U. Jawhari1, P. Kaye2, C. J. Hawkey1, K. Ragunath1.1Wolfson Digestive Disease Centre and 2Department of Pathology, University Hospital Nottingham, UK
Introduction: The recent advances in zoom endoscopy techniques had enabled endoscopists to observe the organ specific subepithelial capillary network (SECN) pattern in gastrointestinal mucosa. However, we had not been able to visualise a honeycomb-like SECN pattern which has been proved to be the normal microvascularture in the large intestine by anatomical study. Recently, a new optical method called NBI technique, designed to help specifically the visualisation of superficial microvascularture, has been developed. The aim of this study was to investigate whether High definition zoom colonoscopy with NBI is useful for visualising capillaries and RBC in the large intestine.
Methods: Total colonocscopies were performed in six patients with abdominal symptoms using a high definition zoom colonoscope (CF-H260Z, Olympus) and a prototype high definition electronic endoscopy system that incorporates NBI function (Hyperpro, Olympus). Each part of the large intestine (caecum, ascending, transverse, descending, sigmoid colon and rectum) was observed at maximal magnification (X150), with NBI and without NBI, alternatively. The SECN pattern and RBC movement in the capillaries was recorded for each part of the large intestine. The colonoscopies and biopsies were normal.
Results: In all patients, high definition zoom colonoscopy with NBI could constantly visualise a honeycomb-like SECN pattern together with RBC movement in each part of the large intestine except for the rectum. In contrast, without NBI, neither such SECN pattern nor RBC movement could be detected.
Conclusion: This method could be a new optical method that facilitates non-invasive investigation for both microvascular architecture and microcirculation without any contrast materials.
253 OLYMPUS LUCERA HIB VASCULAR ECTASIA MAPPING IN COMBINATION WITH THE NAGATA TYPE V(C) CRYPT PATTERN FOR INVASIVE DEPTH ESTIMATION IN PARIS TYPE II COLORECTAL CANCERS: A comparative prospective analysis to 20 mhz mini probe ultrasound
D. P. Hurlstone1, D. S. Sanders1, S. Brown1, M. Thomson1, S. S. Cross2.1Gastroenterology, Royal Hallamshire Hospital, Sheffield; 2Academic Department of Pathology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: We have previously shown that 20 MHz high frequency EUS is superior to the modified type V Nagata crypt criteria when differentiating T1/2 disease in Paris type II neoplastic lesions. 20 MHz EUS has a high PPV for sm3 differentiation. Hib differential vascular mapping permits visualisation of superficial neoplastic vascular structure in combination with magnification endoscopy where neoplastic superficial “vascular ectasia” (VE) may be an additional marker for sm3 disease.
Aims: To assess the efficacy of the Nagata type (c) crypt pattern in combination with Hib vascular mapping for the invasive depth of Paris type II neoplasia as compared to 20 MHz EUS.
Methods: Paris type II neoplasic lesions were imaged using HMCC followed by 20/12.5 MHz EUS. Crystal violet staining permitted Nagata crypt criteria to be defined. Sm3+ invasion was defined at ultrasound by the presence or absence of a disrupted third sonographic layer. Neoplastic superficial VE using Hib was defined as vascular disruption+/−tortuousity. Predicted T0/1:N0 lesions were resected using EMR with the remaining referred for surgery. The EUS and HMCC staging was then compared to the resected histopathological specimens.
Results: n = 68 (12 sm1/13 sm2/27 sm3+). EUS was significantly more accurate for invasive depth staging as compared to Nagata stage alone (p<0.0001). Combining Nagata (c) with VE positive criteria although not superior to EUS (p>0.05) significantly improved T2 staging accuracy (p = 0.02). The sensitivity for lymph node metastasis detection using ultrasound and combined VE/Nagata (c) was 80% and 68% respectively (p<0.001).
Conclusions: Combination Nagata (c) and + ve VE criteria permit an accepatable in vivo staging modality without the requirement for repeat 20 MHz imaging. Sm3+ invasion was associated with nodal metastasis.
254 DETECTION OF HELICOBACTER PYLORI GASTRITIS AND GASTRIC ATROPHY BY REAL TIME HIGH RESOLUTION MAGNIFICATION ENDOSCOPY
G. K. Anagnostopoulos, K. Yao, C. J. Hawkey, K. Ragunath.Wolfson Digestive Diseases Centre, University Hospital, Nottingham, UK
Background: High resolution magnification endoscopy (HRME) offers the ability to examine the gastric mucosa in detail that is not visible by conventional endoscopy. The aim of our study was to correlate the magnified endoscopy findings with histopathology of normal stomach, Helicobacter pylori (HP) associated gastritis, and gastric atrophy.
Methods: One hundred consecutive patients (57 male, mean age 59 years) scheduled to undergo gastroscopy were enrolled. Conventional and magnifying endoscopies were performed with the Olympus GIF Q240Z endoscope (x115). Biopsies were taken from the sites observed, and according to Sydney protocol.
Results: The magnified findings in gastric body were classified into five types: (A) honeycomb-type subepithelial capillary network (SECN)/normal collecting venules (CVs), (B) loss of normal SECN/irregular CVs, (C) normal SECN/loss of CVs, (D) loss of normal SECN-CVs/enlarged-white pits/erythema, and (E) antral-type SECN in gastric body. Normal mucosa corresponded to type A, gastric atrophy to type B, and HP gastritis to types C–E. 33 patients had magnified endoscopic evidence of HP infection (18C, 11D, 4E) and 22 had histology positive for HP. 23 patients had findings suggestive of gastric atrophy and 22 had histologically proven gastric atrophy. The sensitivity/specificity/predictive values of: type A for the prediction of normal gastric mucosa, type B for the prediction of gastric atrophy, and types C, D for the prediction of HP gastritis are shown in the table. All four cases with type E mucosa corresponded to HP gastritis.
Abstract 254
Conclusion: HRME has the potential for real time diagnosis of H pylori associated gastritis and gastric atrophy during endoscopy.
255 NOVEL ZOOM ENDOSCOPY TECHNIQUE BASED ON GASTRIC MICROVASCULAR ARCHITECTURE IS USEFUL TO DIFFERENTIATE BETWEEN FLAT EARLY GASTRIC CANCERS AND GASTRITIS
K. Yao1, A. Iwashita2, S. Sou1, T. Nagahama1, H. Tanabe1, T. Yao1, T. Matsui (introduced by K Ragunath)1.Department of 1Gastroenterology and 2Pathology, Fukuoka University Chikushi Hospital, Fukuoka, Japan
Introduction: During gastroscopy we frequently encounter flat reddened lesions in the stomach. In order to diagnose a flat, small, early gastric cancer, it is common practice to obtain multiple biopsies from such lesions. We investigated the diagnostic accuracy of magnified endoscopic findings for differentiating between reddened mucosa due to gastritis and flat reddened gastric cancer, prospectively and blindly.
Methods: Six hundred and three consecutive patients were examined by zoom endoscopy (GIF-Q240Z, Olympus, ×80) and the prevalence of each of the following magnified endoscopic findings, which had been already reported as characteristic for differentiated carcinoma, was recorded. (1) Presence of a demarcation line between the reddened lesion and the surrounding mucosa, (2) disappearance of the regular subepithelial capillary network (SECN) pattern, and (3) presence of an irregular microvascular pattern (IMVP) within the flat reddened lesion.
Results: One hundred and fifty seven flat reddened lesions from 157 patients were detected. Pathologically, 144 flat reddened lesions showed only gastritis, while 13 lesions were newly diagnosed as differentiated carcinoma. The prevalence of the findings is shown in table.
Abstract 255
Conclusion: The novel zoom endoscopic findings based on microvascular architecture are useful for making a differential diagnosis between flat early gastric carcinoma and gastritis.
256 NARROW BAND IMAGING WITH MAGNIFICATION TO DISTINGUISH NEOPLASTIC AND NON-NEOPLASTIC POLYPS IN THE COLON
J. E. East, N. Suzuki, D. Swain, N. Palmer, B. P. Saunders.Wolfson Unit for Endoscopy, St Mark’s Hospital, London, UK
Background: NBI has been described as “electronic dye-spray”. Using optical filters it enhances the contrast for superficial blood vessels which enhances the mucosal pattern (pit pattern); with magnification this allows an estimate of the likely histology of a polyp in vivo.
Method: Using a third generation prototype narrow band imaging (NBI) system which can magnify ×100 (XCF-H240FZL/I video colonoscope, XCLV-260HP xenon light source and XCV-260HP video system centre, Olympus Medical System Corp, Tokyo, Japan) we took 21 NBI magnification endoscopic photographs of neoplastic and non-neoplastic polyps. Two experts (NS and BPS) were asked to assess the pit pattern according to the Kudo classification and judge the polyps to be neoplastic or non-neoplastic. One assessor also graded the intensity (darkness) of the pit pattern. These were compared with histological findings
Results: Polyps size ranged from 1–10 mm. Adenomatous (Ad), hyperplastic (Hp), and inflammatory (Inf) polyps were assessed (see table, assessor 1/assessor 2). Pit pattern mean sensitivity and specificity for neoplasia was 62% and 50%; however specificity improved to 75% if inflammatory polyps were excluded. Positive and negative predictive values were 66% and 44%. Some inflammatory polyps were considered non-neoplastic despite type III/IV pit pattern. Pattern intensity alone gave a sensitivity of 77% and specificity 75%, PPV 83%, NPV 75%.
Abstract 256
Conclusion: Early experience using NBI with magnification and Kudo pit pattern suggests that it is inferior to chromoendoscopy. Inflammatory polyps were especially difficulty to classify correctly. This may reflect lack of experience and the need to modify the Kudo classification to take specific additional NBI features such as strong pattern intensity and vessel irregularity to optimise discrimination.
257 IMMEDIATE COLONOSCOPY COMPLICATIONS 1992–2004: AN AUDIT OF 14 521 CASES
T. Sivayokan, R. Leicester, A. Poullis.St George’s Hospital, London, UK
Background: A national audit into colonoscopy complications revealed a perforation rate of one in 769, a post procedure minor bleed rate of one in 263, and major haemorrhage rate of one in 1537 (Bowles, Leicester, et al. Gut 2004). We audited our units results to compare them to the national results.
Method: We analysed 14 521 colonoscopies in our department from 1992 and 2004 to determine immediate colonoscopy complication rates. Hospital records were reviewed to obtain more details of the complications and determine their severity.
Results: There were five perforations (one in 2904): two cases occurred post polypectomy, two cases occurred in patients with diverticular disease, and one occurred in a patient with radiation colitis. All five required surgery. 26 cases of post procedural bleeding occurred. 14 were immediately controlled without the need for hospital admission. In 12 cases bleeding was immediately controlled but the patient was admitted for observation. One patient required a blood transfusion but none required surgery (minor bleed rate 1 in 1037, moderate bleed rate one in 1210, significant bleed one in 14 521). There was no mortality in this series.
Conclusion: The perforation rate in this series is one in 2904. The risk of a moderate post polypectomy bleed is one in 1210, that of a significant haemorrhage is 1 in 14,521. The risk of a complication is increased for therapeutic procedures and in those with an underlying abnormality. Regular reviews of complication rates after endoscopy are an important part of clinical governance.
258 FLEXIBLE SIGMOIDOSCOPY: IS TIME RUNNING OUT?
K. Manoj, S. G. R. G. Barton.Department of Gastroenterology, Kent and Canterbury Hospital, Canterbury, Kent, UK
Introduction: Population based screening for colorectal cancer, revalidation of colonoscopists and virtual colonoscopy are all going to impact on UK endoscopy services. Flexible sigmoidoscopy (flexisig) is seen as a valid investigation for cancer screening and is stated to take one unit of endoscopy time. Full colonoscopy is allocated two units of endoscopy time. A full list should comprise five or six colonoscopies or 10 flexisigs.
Aims: To see if the units of endoscopy time allocated to the two procedures reflect time actually taken.
Methods: Six colonoscopists in our unit were timed during colonoscopy by endoscopy nurses. Three time-points were recorded: (1) time to the point the endoscopist felt he would have achieved satisfactory flexisig, (2) time to caecal/terminal ileal intubation, and (3) time to extubation. Times for procedures where the caecum was not reached were discarded. Data for 121 completed colonoscopies over a two month period were obtained.
Results: The overall mean colonoscopy time was 17.7 minutes. Flexisig was achieved a mean of 6.0 minutes after intubation and the caecum reached after a mean of 13.5 minutes. The terminal ileum was accessed in 22 cases. The fastest colonoscopist averaged 12 minutes for total colonoscopy. 17 of the 22 terminal ileal intubations were achieved by the two fastest colonoscopists (out of 48 colonoscopies).
Discussion: Allocating two units of endoscopy time to colonoscopy and one unit to flexible sigmoidoscopy appears justified in terms of the relative times taken. One unit of endoscopy time does not equate to 20 minutes. A list of six colonoscopies would take 1 hour 46.2 minutes of endoscopy time. The extra time needed to convert a flexible sigmoidoscopy to a full colonoscopy is only 7.5 minutes and this small difference does not support intentionally limiting the scope of a large bowel investigation to trade-off for increased patient throughput.
259 TERMINAL ILEAL BIOPSY IS UNNECESSARY TO CONFIRM COMPLETE COLONOSCOPY
S. McMillan, P. Sharma, R. Ahmad, E. Grabham, J. S. McCourtney.Colorectal Research Unit, Royal Alexandra Hospital, Paisley, UK
Background: Objective proof of completion at colonoscopy is best obtained by terminal ileal (TI) intubation and biopsy. However, with increasing demands on histopathologists and the predicted increase in the number of colonoscopies in 2007 as a result of a national bowel cancer screening programme in Scotland, we wished to assess whether this manoeuvre was of value in confirming completion when performed by an experienced colonoscopist.
Methods: TI biopsies collected prospectively to confirm completion at colonoscopy in patients with intact colons were audited. All colonoscopies were performed either by or under the direct supervision of one colonoscopist. Cases referred for TI intubation in light of imaging studies suggesting ileal pathology were excluded. Data were retrieved to establish if TI biopsy correlated with histology and to assess the incidence of histologically confirmed ileal pathology.
Results: 642 TI biopsies were audited. In two cases submitted specimens were too small for processing. Three cases were reported as biopsies of colonic mucosa with no evidence of ileal tissue. Four patients had coincidental abnormal histology (0.06%), comprising one carcinoid tumour, one adenocarcinoma, and two Crohn’s disease. Three of these four cases were clinically diagnosed at the time of ileal intubation. Normal terminal ileal mucosa was confirmed in 633 cases (98.6%).
Conclusion: TI biopsy is unnecessary for colonoscopists who can regularly intubate the ileocaecal valve and should therefore be reserved for those cases where ileal pathology is encountered or clinically suspected, avoiding both considerable expense (£245 per biopsy) and histopathology time. Simple alternatives such as photography after dye spraying should be used to record ileal intubation.
260 ARE PARIS TYPE I AND II HYPERPLASTIC POLYPS ASSOCIATED WITH SYNCHRONOUS COLORECTAL CARCINOMA? A PROSPECTIVE 1000 PATIENT CHARACTERISATION USING HIGH MAGNIFICATION CHROMOSCOPIC COLONOSCOPY
D. P. Hurlstone1, D. S. Sanders1, S. Brown1, M. Thomson1, S. S. Cross2.1Gastroenterology, Royal Hallamshire Hospital, Sheffield; 2Academic department of Pathology, Royal Hallamshire Hospital, Sheffield, UK
Background: We have previously reported an increased prevalence of right hemi-colonic Paris type II hyperplastic (HP) polyps in HNPCC using high magnification chromoscopy (HMCC). Recent data now suggest that patients with right hemi-colonic Paris type I/II lesions in addition to high density diminutive left hemi-colonic lesions may be at increased risk of colorectal neoplasia.
Aims: To establish the prevalence, morphology, anatomical location, and relationship of HP to synchronous colorectal cancer.
Methods: 1000 patients underwent HMCC using the Olympus CF240Z and 0.5% indigo carmine pan-chromoscopy. Lesion morphology was classified according to Paris guidelines and crypt analysis as per modified Kudo criteria. Biopsy and resection practice was performed as per recommended practice (Hurlstone DP et al. Gut 2004;53:284–90.
Results: n = 1000; median age 66 (range 24–92 years).
Conclusions: Intermediate/large Paris type II HPs cluster within the right hemi-colon and represent valid biomarkers of synchronous neoplasia. CRC screening colonoscopy protocols may require revision.
Abstract 260
261 FACTORS PREDICTING A SUCCESSFUL COLONOSCOPY
C. H. Lim, D. Ng, M. M. Ahmed.Department of Gastroenterology, Good Hope Hospital, Sutton Coldfield B75 7RR, UK
Objective: UK colorectal screening is around the corner but a recent national colonoscopy audit suggest most endoscopy centres do not achieve the unadjusted completion rate of 85% or more to qualify as a screening centre. We have recently completed a five year colonoscopy audit in a district hospital setting and our unadjusted completion rate was 74.6% which was similar to the recent national colonoscopy audit.1 We looked at factors that may predict the colonoscopy completion rate.
Methods: Retrospective audit from June 1999 to May 2004. We performed multiple logistic regression analysis to calculate the odds ratio and to determine the predictive factors for successful colonoscopy. We excluded colonoscopist performing less than 100 procedures for the multiple logistic regression analysis.
Results: 3873 colonoscopic examinations were done but 674 were excluded, hence 3199 procedures were available for analysis. The unadjusted completion rate remained at 74%. The gender ratio was one to one. The mean age was 61.2 years old (2SD = 31.4 to 90.9 years old).
Conclusions: There is a significant improvement trend for successful colonoscopy over the five year audit period. We would recommend performing at least 200 colonoscopy examinations per year to maintain your skill. The use of midazolam, male patient and trained GI physician are independent predictors for successful colonoscopy.
Abstract 261
1
262 RETROFLEXION IN FLEXIBLE POUCHOSCOPY CAN INCREASE ADENOMA DETECTION IN PATIENTS WITH FAMILIAL ADENOMATOUS POLYPOSIS AFTER RESTORATIVE PROCTOCOLOECTOMY
R. F. S. Man1, C. Fraser1, B. P. Saunders1.1Wolfson Unit for Endoscopy, St Mark’s Hospital, Harrow, UK
Introduction: Restorative proctocolectomy eliminates the risk of colorectal cancer in patients with familial adenomatous polyposis. However, approximately 35% (Parc2001) of these patients have reported to develop adenomas after the formation of ileal pouch anal anastomosis (pouch). The most common areas of developing adenomas are in the ileo-anal vault especially at the anal-pouch anastomotic site and the columnar cuff. This is possibly due to the present of some residue rectal tissue despite mucosectomy. In fact, cancers in these areas have been reported in patients who had regular endoscopic surveillance suggested the possibility of missed adenomas during their examination (Ooi et al 2003, Vrouenraets et al 2004). Studies have demonstrated retroflexion can increase adenomas detection in the rectal vault (Hanson at el 2001) when performing colonoscopy. However, retroflexion in pouch is often not performed despite the risk of causing perforation is unknown.
Aims: This study is aimed to demonstrate retroflexion can increase adenoma detects on in the ileo-anal vault in FAP patients with ileal pouch-anal anastomosis.
Methods: A prospective study of 105 FAP patients with ileal pouch anal anastomo sis (IPAA) whom had undergoing surveillance unsedated flexible pouchoscopy (Olympus CF200) by a single nurse endoscopist (RM) between March 2003 to July 2005.
Results: One hundred and twenty two patients were seen during this period. Seven patients were excluded due to tight/stricturing anal anastomosis. Forty eight patients (about 42.5%) were found to have polyps seen on retroflexion (mean interval of IPAA formation was 8.8 years). All polyps were removed either by endoscopic resection or transanal excision surgically. Only one patient required a permanent ileostomy for extensive polyposis in the whole pouch. With the adenomas found, 12 (28/%) of these were ileal pouch mucosa type. The remaining 27 adenomas (72%) were found to be arising from the residual rectal tissue. No endoscopic complications such as pain or perforation were reported. More inportantly, no missed cancers were reported during a follow up period of two and half years in this patient group.
Conclusion: This study has demonstrated an increased in adenoma detection when retroflexion is performed in flexible pouchoscopy than the previous literatures. This technique is simple and safe to perform in surveillance endoscopy. Early detection of these adenomas in these patients can lead to early removal of these premalignant lesions; hence can prevent cancer and avoid the need for permanent ileostomy.
263 THE ANATOMY OF THE COLON ON VIRTUAL COLONOSCOPY AND ITS VALUE IN PREDICTING THE DIFFICULTY OF PERFORMING OPTICAL COLONOSCOPY
N. Q. Khan, P. M. Casey, J. Bell, M. Bose, L. Jackson, O. Epstein.Centre for Gastroenterology, Royal Free Hospital, London, UK
Background: Colonoscopy can be demanding and may be accompanied by significant patient discomfort. This study aims to use virtual colonoscopy (VC) measurements to predict difficulty in advance of optical colonoscopy.
Methods: Eighty seven patients were entered into a prospective trial investigating the sensitivity and specificity of virtual colonoscopy. CT images were processed using V3D software which allowed accurate measurements of colon segments and angulation of landmark flexures. All patients subsequently underwent same day optical colonoscopy. The time taken for complete optical colonoscopy was recorded as was the number of incomplete procedures and correlated with colonic lengths and angles derived from the virtual colonoscopy.
Results: Eighty two out of 87 endoscopic procedures were completed.
Conclusions: Improvement in the sensitivity and specificity of VC suggests that this technique followed by targeted colonoscopy will play a major role in colorectal imaging. This study indicates that incomplete colonoscopy is more likely when distance from the anus to the JDS or splenic flexure is long or when the total sigmoid length is increased. This information may be useful in the scheduling of colonoscopy lists and operators.
Abstract 263
264 ASSESSING PAIN DURING COLONOSCOPY: WHO GUIDES SEDATION?
B. H. Hayee, M. Wong, D. S. Rowbotham, V. Saxena, A. McNair.Queen Elizabeth Hospital, Woolwich, London SE18 4QH, UK
Introduction: Accurate assessment of pain during colonoscopy allows the dose of intravenous sedation and analgesia to be titrated to minimise discomfort. Patients who remember a painful colonoscopy may decline repeat examinations and this may be a significant issue for the institution of a national screening programme for colorectal cancer.
Aims and Methods: We sought to determine whether the assessments of pain by endoscopists and nurses during colonoscopy correlated with patients’ reports and whether this influenced sedation or procedure time. Information was collected using visual analogue scales (VASs) and patient questionnaires.
Results: The mean patient post-endoscopy VAS score for 167 patients (93 female) was 21.4 (SE 23.8). Mean VAS scores from endoscopists and nurses and from patients pre-endoscopy (patients anticipation of pain) tended to be higher than the patient’s post-endoscopy score. Correlation coefficients between patients’ post-endoscopy VAS scores and pre-endoscopy scores, endoscopist VAS and nurse VAS were 0.15, 0.39 and 0.41 respectively. 28 patients received a “step up” sedative dose. Mean endoscopist and nurse VAS scores for these patients were higher than patients not requiring additional sedation/analgesia (54.03 v 27.58, p<0.0005 and 50.74 v 17.58, p<0.0005), as were pre- and post-endoscopy scores (37.42 v 31, p = 0.07 and 38.48 v 17.42, p<0.0005). This group also had longer intubation times (19.79 v 13.35 minutes, p<0.0005) and overall procedure times (45.77 v 27.58 minutes, p<0.0005). There was a tendency for patients with endoscopist VAS above 54.03 (n = 21: F = 8) to receive additional analgesia or sedative compared to patients with nurse VAS above 50.74 (n = 25: F = 15) but this did not reach significance (15/21 v 13/25, p = 0.21).
Conclusions: Endoscopist and nurse assessments of discomfort do not appear to correlate well with patient recollection and neither group appears superior in this regard. Patients receiving additional sedation still reported more pain than those that did not. In addition, endoscopist assessment of pain appears more likely to influence sedation practice. Assessment of pain during colonoscopy remains a challenging, yet central issue to patient satisfaction.
265 TERMINAL ILEUM VILLI PHOTOGRAPHY TO DOCUMENT EXTENT OF COLONOSCOPY
N. Powell, B. Hayee, D. Yeoh, D. Rowbotham, V. Saxena, A. McNair.Gastroenterology Dept, Queen Elizabeth Hospital, Woolwich, London, UK
Background: Documentation of complete colonoscopy confirms thorough colonic examination. Photography of caecal landmarks may be used to verify the extent of colonoscopy but they are inconsistently recognised with significant inter-observer disagreement. Terminal ileum (TI) biopsies are regarded by some as the most reliable means of verifying total colonoscopy, but concerns including possible transmission of prion particles and additional expense may limit its utility. The purpose of this study was to prospectively evaluate the reliability of TI photography demonstrating the presence of villi as documentation of total colonoscopy. We also evaluated the diagnostic yield of TI biopsies in patients with normal macroscopic TI appearances.
Methods: We conducted a prospective study of 211 unselected patients referred for colonoscopy. The endoscopic appearance of the TI was recorded and photographs acquired following instillation of water via the endoscope water channel to flood the visual field and illustrate villi. These images were independently evaluated by three gastroenterologists and categorised as “definitely”, “probably”, and “definitely not” depicting villi.
Results: Histological assessment of TI biopsies confirmed small bowel mucosa in 202 patients. There was inadequate sample for assessment in nine cases. Photograph evaluation by reviewers described villi as “definitely” present in 93.1%, 93.6%, and 92.1% of cases and “probably” present in 6.9%, 5.4%, and 7.9% of cases. One reviewer considered villi “definitely not” present in two cases. There was good agreement between the reviewers (Cohen’s kappa values for concordance = 0.78). Microscopic TI changes in patients with a normal TI appearance were only present in 2.1% (all four with features of Crohn’s disease). In all four cases macroscopic and microscopic features of Crohn’s disease were apparent in the colon. In summary, photography of TI villi is an effective means of documenting total colonoscopy. Furthermore, if the TI mucosa appears normal the diagnostic yield from routine TI biopsy is very low. All patients with microscopic disease alone had an abnormal colonoscopy.
266 ARE VARIABLE STIFFNESS COLONOSCOPES REALLY SUPERIOR? RESULTS OF A POST HOC ANALYSIS
B. H. Hayee, D. S. Rowbotham, V. Saxena, A. McNair.Queen Elizabeth Hospital, Woolwich, London SE18 4QH, UK
Introduction: The use of variable stiffness colonoscopes (VSCs) is reported to improve intubation time, completion rates and reduce the perception of pain during the procedure. In its unstiffened state, the VSC (Olympus PCF-240AL) is significantly less stiff than a conventional colonoscope (CC; Olympus PCF-240S) and at maximal stiffness, it is just as stiff, but only at its distal end.1, 2 The evidence that the VSC is superior to conventional colonoscopes is limited.
Aims and Methods: We sought to determine whether our experience with the use of VSC reproduced the results of other studies. As part of a larger trial of sedation regimens for colonoscopy, we gathered data for post hoc analysis of caecal intubation rates, completion times and patient discomfort using a visual analogue scale (VAS) for colonoscopy with a CC and a VSC. All operators involved in the study had confirmed caecal intubation rates in excess of 90%.
Results: 169 examinations were performed (97 females); 82 with the VSC. There was no significant difference between operators, or between males and females for all parameters studied. Additional sedative was given on 12/82 occasions with the VSC and 20/87 with the CC (p = 0.20). No significant difference was found for the VSC over the CC in terms of completion rates (94% v 92%, p = 0.24), intubation times (13.96 v 14.80 minutes, p = 0.55), total procedure time (30.08 v 30.93 minutes, p 0.72), VAS assessment by endoscopist (23.77 v 25.40, p = 0.64), by nurse (23.63 v 23.18, p = 0.91) or by patients after the procedure (20.69 v 22.42, p = 0.64).
Conclusions: These results demonstrate no statistical or clinical superiority for VSCs over CCs for colonoscopy in adult patients.
1
2
267 COLONOSCOPY PERFORMANCE AFTER 190 CONSECUTIVE PROCEDURES: DOES TYPE OF INSTRUMENT MATTER?
R. P. Arasaradnam1, D. P. Hurlstone2.1Wansbeck Hospital, Ashington & School of Clinical Medical Sciences, University of Newcastle upon Tyne; 2Department of Gastroenterology, RHH & NGH, Sheffield Teaching Hospitals, UK
Background: The BSG has set out guidelines as to the expected level of competence an endoscopist should strive to achieve. This is vital given the variation in practice throughout the UK as published in the first National Audit in 2002. However, one issue which did not come to light was the variation in types of instruments used and how this may impact on colonoscopic performance.
Aim: To determine if colonoscopy performance including caecal completion rate, analgesic dose and sedation practice is affected by variation in instrument.
Methods: 190 consecutive procedures performed by a single endoscopist were analysed prospectively. The first 105 procedures were performed using a Olympus CF 240 variable stiffness scope. Subsequent 85 procedures were performed using a Fujinon EC-450WL scope. Demographic data, dose and type of sedation (Midazolam (Mdz)) used as well as caecal and terminal ileal intubation rates (CIR and TIR) were recorded.
Results: See table. Indications for colonoscopy were similar in both groups as were hysterectomy rates (5%). Number of patients with previous colonic resections were almost double (10%) in those examined with the Fujinon instrument. Mean list size was five (range 4–6) patients and the number of therapeutic procedures was eight (8%) in the first 105 procedures and 20 (24%) in the subsequent 85. The adjusted completion rates as well as sedation practise were both highly significant (χ2; p = 0.001) respectively whilst the adjusted anlgesic dose used was borderline significant (χ2; p = 0.05). One immediate complication in the first 105 procedures occured in a 78 year old lady who developed acute Left ventricular failure secondary to severe aortic stenosis. She recovered uneventfully.
Abstract 267
Conclusions: It is evident that type of instrument does influence colonoscopic performance and sedation practice. Perhaps this factor should be taken into account when assessing individual endoscopists or when comparing data between different units.
268 ARE PATIENTS GOOD JUDGES OF THEIR RESPONSE TO THE BOWEL PREPARATION FOR COLONOSCOPY?
M. Rashid, S. D. Mann.Department of Gastroenterology, Barnet Hospital, London, UK
Introduction: The Department of Health are introducing colorectal cancer screening into the UK in April 2006.1 This programme will lead to an increase in colonoscopy requests for patients with positive faecal occult bloods. Cancer screening with colonoscopy requires optimal views for successful visualisation of the colon. Endoscopists often document poor views and inadequate bowel preparation despite claims by the patients that the clear-out was successful.
Aim: To determine how reliable is the patients’ assessment of their own response to bowel preparation (two sachets of picolax).
Method: Consecutive patients attending for routine out-patient colonoscopy were given a questionnaire asking them what type of stool they were passing after the bowel prep and whether they felt the clearout had worked. After completion of the procedure, the endoscopist had to evaluate the adequacy of the bowel prep using a 5-point scale.
Results: Complete data were available from 69 out of 110 patients (63%) over a six month period. Of those 69 patients, 67 (97%) “felt that the preparation worked”. The description of effluent prior to the procedure was described as “clear watery liquid” in 26 (38%), clear closured liquid in 40 (58%), and “mushy consistency stool” in three cases (4%). The endoscopist rating of the preparation was “excellent with views obtained in >90% of the mucosa” in 28 (40%), “reasonable with liquid residue that was easily washed” in 18 (26%), “modest with some solid stool that could be washed in 13 (19%), and “poor with residue coating >50% of the mucosa” in 11 cases (16%). In no cases was the procedure abandoned due to “prep failure”.
Conclusion: Although the bowel prep used in our trust gives reliable views in 85% of cases, patients tend to overestimate their response to the prep. Poor prep leads to longer procedure times and risks of complications and missed polyps. We still need to look for a better indicator of those patients who may benefit from additional bowel cleansing such as an enema when they attend for their procedure.
1
269 COLONOSCOPY SURVEILLANCE PRACTICE IN A DISTRICT GENERAL HOSPITAL
A. Indar, H. Willmott, A. F. Goddard, D. MacAfee, J. Lund.Departments of Surgery and Gastroenterology, Derby Hospitals NHS Trust, Derby, UK
Background: Demand for colonoscopy has increased over the years, and consequently waiting lists have expanded. BSG has published guidelines for colonoscopic surveillance following polypectomy and cancer resection. We performed a retrospective analysis of our colonoscopic surveillance practice in such patients.
Method: Details of patients who underwent surveillance colonoscopy for “previous polyps” or “previous cancer” between Jan 2002 and Jun 2005 were retrieved from our Endoscopy database. Index colonoscopy was the first post-resection or when a polyp was initially excised completely.
Results: 193 patients underwent 312 surveillance colonoscopies. Overall, 288 (92%) examinations occurred sooner than, 15 (5%) occurred longer than and nine (3%) were appropriate to the guidelines. The table shows their median surveillance intervals with the respective risk stratification.
Abstract 269 Risk stratification and surveillance
There were 95 unnecessary examinations at a direct overspend of £62,518. A further 86 examinations occurred sooner than half the recommended interval (unnecessarily early). Indirect costs are estimated to be exponentially higher.
Conclusion: 92% of surveillance colonoscopies were performed earlier than recommended at significant cost, with 30% of these being unnecessary. These examinations have the potential for unnecessary risk, inappropriate management, and highlights areas where our colonoscopic practice can be improved.
270 UTILITY OF COLONOSCOPY FOR EVALUATION OF PATIENTS WITH IRON DEFICIENCY ANAEMIA
V. Subramanian, K. Dhake, R. C. G. Pollok.Department of Gastroenterology, Cellular and Molecular Medicine, St George’s University of London, UK
Introduction: Occult bleeding from the gastrointestinal tract is an important cause for patients with iron deficiency anaemia without obvious sources of blood loss. Current guidelines suggest that such patients should have endoscopic evaluation of the both the upper and lower gastrointestinal tracts. One of the major reasons for recommending colonoscopic evaluation is to pick up colorectal carcinoma in this population. We aimed to assess the utility of colonoscopic evaluation of patients with iron deficiency anaemia.
Methods: Retrospective audit of all patients who underwent colonoscopy for the sole indication of anaemia at St George’s Hospital in 2003 and 2004. Patients were identified from a computerised endoscopy database and data collected from electronic patient records. IDA was defined as having haemoglobin less than the reference range associated with a low mean corpuscular volume and/or a low ferritin. Significant pathology considered were GI malignancy, inflammatory bowel disease, colonic polyp larger than 1 cm, vascular malformations, bleeding diverticular disease, and bleeding hemorrhoids. ROC curves were constructed for variables of interest and p values were calculated using standard t tests of proportions for independent samples.
Results: 145 patients with confirmed IDA, 120 with anaemia but no evidence of iron deficiency were included. There were no differences overall detection of significant lower GI pathology, between patients with IDA (15.2%) and patients with anaemia (12.5%) without evidence of iron deficiency. However colorectal cancer rates were significantly higher among patients with IDA. Levels of haemoglobin, ferritin, and iron were not useful in predicting the overall detection of a significant lower GI pathology in either group.
Conclusions: Patients with IDA are more likely to have colorectal cancer than patients with anaemia without evidence of iron deficiency. Haemoglobin, ferritin, and iron levels do not appear to predict the detection of clinically significant lesions on colonoscopy other than colorectal cancer. Prospective studies are required to confirm these observations.
271 WHY WAIT FOR A COLONOSCOPY? AN EASY CURE
K. Chivers, B. Seunarine, A. Shoaib, P. Basnyat, N. Taffinder (introduced by AW Harris).Colorectal Unit, Willam Harvey Hospital, East Kent Hospitals NHS Trust, Ashford, Kent TN24 0LZ, UK
Background: Guidelines for surveillance and screening colonoscopy were released in October 2002 from the British Society of Gastroenterology and the Association of Coloproctology of Great Britain and Ireland. They were based on sound evidence of the chance of finding malignant polyps in patients who had had a cancer or a polyp in the past, or for those with a family history of bowel cancer. These guidelines were expected to lead to a change in clinical practice.
Methods: Before starting the audit, the process was discussed at, and approved by, the Kent Endoscopy Board and Colorectal Cancer DOG. 4837 patients were waiting for a colonoscopy in our network and a team of researchers reviewed their notes in the light of the BSG guidelines. Over two thirds of the list were waiting for screening or surveillance colonoscopy. Those waiting for diagnostic colonoscopy were excluded from the study. The wait times for an urgent diagnostic colonoscopy were measured before and after the audit.
Results: 2369 (78% of those waiting) did not need to have a colonoscopy according to the guidelines. Those patients were identified and each of the seven hospitals within the network received a booklet identifying their patients who could be removed from the waiting list. This could save the network £1.2 million (assuming £500 per colonoscopy). Patients who were removed from the waiting list were contacted with a standardised letter. This review halved the size of our total waiting list and subsequently the average wait time for an urgent diagnostic colonoscopy fell from 70 days to 33 days.
Discussion: Guidelines can have dramatic impact on avoiding unnecessary investigations and reducing waiting lists. In addition our waiting times for a diagnostic colonoscopy fell, with increased compliance with the cancer waiting time targets. Most clinicians were comfortable with the guidelines although some exceptions to the recommended surveillance were accommodated for.
272 HOW MANY ENDOSCOPISTS FULFIL QUALITY ASSURANCE CRITERIA FOR THE BOWEL SCREENING PROGRAMME?
M. C. Allison.Gastroenterology Unit, Royal Gwent Hospital, Newport, South Wales NP20 2UB, UK
Background: Colonoscopists who will participate in the forthcoming screening programme are expected to perform or directly supervise >150 procedures per year, to have an adenoma detection rate of >15%, an adjusted caecal intubation rate of >90% and a lifetime perforation rate for diagnostic colonoscopy of <1:1000. Although the programme will start in England in April 2006 it is not known how many colonoscopists fulfil these requirements. A survey of colonoscopists in Wales was therefore done.
Methods: Questionnaires were sent to all 100 career grade endoscopists believed to be doing regular colonoscopy lists in Wales. Completed forms were returned by post to ensure anonymity.
Results: The response rate was 70%. Seven no longer undertook colonoscopy. Of 63 responding colonoscopists, only nine (14%) could quote their adenoma detection rate (median 18%, range 10–33%), and 33 (52%) could quote their adjusted caecal intubation rate (median 92%, range 70–96%). Median colonoscopy caseload fell within the range of 101–150 procedures per year. Lifetime perforation rates were given by 59 respondents, of whom 43 quoted a figure of <1:1000. Overall only 12 colonoscopists (19%) met the required criteria for screening colonoscopists (sufficient caseload with acceptable caecal intubation and perforation rates). Of these, 10 indicated keenness to support a screening programme. To support an FOB based programme in Wales each of these 10 endoscopists would need to undertake an additional 500 colonoscopies per year. Most of those who failed to meet the required criteria did so through having insufficient caseloads.
Conclusions: The findings cast doubt on whether there are enough colonoscopists ready to support a bowel screening programme in Wales. This deficiency could be rectified by (1) concentrating service provision among fewer endoscopists; (2) better record keeping by existing colonoscopists; (3) better training in colonoscopy; and (4) training colonoscopy nurse specialists. Similar surveys should be done to determine whether such deficiencies exist in other parts of the UK.
273 A TWO TIERED ULCERATIVE COLITIS SURVEILLANCE STRATEGY BASED ON RISK STRATIFICATION OF ULCERATIVE COLITIS PATIENTS
N. Suzuki1, N. Arebi1, M. D. Rutter2, B. P. Saunders1.1St Mark’s Hospital, London; 2University Hospital of North Tees, Stockton on Tees, UK
Background: Ulcerative colitis (UC) surveillance is offered to patients with pancolitis of at least eight year duration. Additional risk factors for UC dysplasia have been reported in previous studies (table). Further subdivision of UC surveillance patients into high and low risk subgroups would enable a better cancer pick up rate and appropriate allocation of resources. A two tiered surveillance strategy based on patient risk is needed.
Abstract 273
Aim: To evaluate the appropriateness of this surveillance strategy, we have conducted an audit of colonoscopies performed on UC surveillance patients.
Methods: All the colonoscopies undertaken for UC surveillance (475) between January 2004 and March 2005 were audited.
Results: Seventeen neoplastic lesions were detected. Four of these lesions were considered to be a sporadic adenoma as they were located in unaffected areas. The remaining 13 lesions were found in areas of colitis with a median size of 20 mm (ranging 3–200 mm). Histologically, these lesions showed invasive cancer (2), high grade dysplasia (5), and low grade dysplasia (6). Macroscopically, 7/13 dysplastic lesions had a flat profile: flat elevation (2), completely flat (1) depressed lesion (2), laterally spreading tumour (2). Dye spray accentuated these lesions. The 13 lesions were detected from 11 patients of whom 10 patients belonged to the high risk group.
Conclusion: The risk stratification on UC patients may identify those patients most likely to benefit from colonoscopy surveillance.
274 COLONOSCOPIC SURVEILLANCE: A NATIONAL SURVEY
A. Indar, L. Pearce, A. F. Goddard, J. Lund.Departments of Surgery and Gastroenterology, Derby Hospitals NHS Trust, Derby, UK
Background: The BSG guidelines determine minimal but safe surveillance of patients after cancer resection or polypectomy. Locally, non-compliance with these recommendations resulted in a significant number of unnecessary examinations. We present results of a national survey into colonoscopic surveillance practice.
Method: 626 colonoscopists nationally comprising mainly consultant members of the ACPGBI and BSG, and their respective Trainees were sent an online questionnaire. This consisted of clinical case scenarios on polypectomy, with questions on patient surveillance and criteria used for this decision. We asked that their answers reflected their actual practice.
Results: 328 colonoscopists responded, of which >75% were consultants performing >10 colonoscopies per month. 60% of colonoscopists surveyed patients after cancer resection either 3 or 5 yearly, and less than 50% would cease follow up at age 75. Following polypectomy, the % of colonoscopists conforming to the guidelines were: 49% in a high risk patient (multiple small polyps), 34% in a high risk patient (advanced adenoma), 38% in an intermediate risk patient (single large polyp), and 57% in a low risk patient (single small polyp). The criteria that determined surveillance intervals varied widely among colonoscopists; using >20 combinations of the following criteria: age, size of polyps, number of polyps, degree of dysplasia, and morphology of polyps. The criterion ranked as most important in determining surveillance after polypectomy were: degree of dysplasia – 39.0%, size of polyps – 37.0%, number of polyps – 17.3%, morphology – 4.1%, age – 2.6%. Fewer than 1/3 of units measure the macroscopic size of polyps, while 85% of units always measure the polyp size microscopically.
Conclusion: Colonoscopic practice throughout the UK is extremely varied. In most cases, surveillance occurs more frequently than recommended by the guidelines. Colonoscopists consider histology very strongly in determining follow up of patients.
275 MODEL OF IMPLEMENTING BSG GUIDELINES FOR POLYP SURVEILLANCE: ROLE OF A GI NURSE PRACTITIONER
J. Burdon, S. Gilbert, P. Patel.Southampton University Hospitals NHS Trust, UK
Background: The policy and implementation of polyp surveillance is very variable across Trusts and consultants. This has contributed to long waiting lists for colonoscopy.
Aim: To evaluate the impact of a trained nurse practitioner in implementing BSG polyp guidelines on frequency of colonoscopy.
Method: A single nurse practitioner was assigned to screen patients on the polyp surveillance waiting list. This was carried out using the British Society of Gastroenterology (BSG) guidelines (2002). Consultants reviewed the notes of patients where rescope frequency was altered. They were required to provide a reason for any decision that did not meet the guidelines. All consultants reviewed notes of patients whose surveillance programme was stopped.
Results: Of 235 patients awaiting surveillance colonoscopy, 138 were for polyp surveillance. The table shows the outcomes after this process. There was a change in management in 66% of cases, with the majority of cases having either a reduction in frequency of colonoscopy (37%) or where surveillance was stopped (16%).
Abstract 275
Conclusion: Screening of waiting lists for polyp surveillance by a nurse practitioner is feasible. This strategy is useful in appropriately reducing the number and frequency of unnecessary colonoscopy.
276 WAITING LIST VALIDATION FOR SCREENING AND SURVEILLANCE COLONOSCOPY. AN AUDIT USING BSG GUIDELINES AS THE STANDARD
R. J. Warner, S. V. Murugesan, J. Iqbal, R. Thornton, P. L. Shields.Royal Preston Hospital, Preston, Lancashire PR2 9HT, UK
Introduction: Colonoscopy is a limited resource associated with potentially serious complications. Waiting times are likely to be stretched further with the introduction of screening for bowel cancer. We conducted an audit to assess and identify the appropriateness of those patients who are undergoing a repeat colonoscopy.
Aims: To compare local practice for repeating a colonoscopy against current BSG guidelines1 and thereby identifying patients who did not require the procedure, those whose procedure needed expediting or delaying. In addition to offering best practice, it would potentially reduce the waiting time for a colonoscopy.
Methods: 536 patients were on the waiting list for a colonoscopy. Only 483 case notes were located. Previous endoscopy and histology reports were reviewed and indications for a repeat procedure were matched to the guidelines. An audit proforma was used.
Results: 237 (49.1%) were for polyps, 118 (24.4%) for cancer follow up, 112 (23.2%) for family history, and 16 (3.3%) for inflammatory bowel disease (IBD). No other indications were identified. Of the 483 patients listed only 181 (37.43%) were due to have their repeat colonoscopy at the appropriate interval. 136 (28.15%) were too early, 39 (8.07%) too late and 83 (17.18%) did not require a further procedure. In the remaining 44 patients (9.10%) there was no clear follow up documented or they had failed to keep appointments. One had surveillance with barium enema.
Conclusion: Follow up colonoscopy for polyps was haphazard and that for colorectal cancer often over cautious. The screening of high risk families was usually too frequent by many years. For IBD we found far fewer patients on the waiting list for surveillance than we expected for the size of population served. The financial cost for a colonoscopy is approximately £457 leading to an immediate cost saving of £37,931 by removing the “not indicated” patients from the list.
1
277 ARE WE READY FOR NHS BOWEL CANCER SCREENING?
D. H. L. Ng, W. C. Tsang, M. M. Ahmed.Good Hope Hospital, Sutton Coldfield, Birmingham, B75 7RR, UK
Background: The implementation of NHS bowel cancer screening is imminent but a recent national colonoscopy audit reported an overall crude completion rate (OCCR) of 76.9% (Bowles et al. Gut 2004), with most endoscopists failing to achieve the target of 85% OCCR needed to qualify as a screener. To assess our performance against these standards, we examined the quality of colonoscopy at our hospital.
Methods: Computerised data mining techniques were used to examine all colonoscopy records over a five year period (June 1999–June 2004) obtained from our unit’s database. We considered colonoscopy to be complete if the caecum, (neo)terminal ileum, or ileocolic anastomosis was intubated.
Results: 3878 colonoscopies were performed in 3307 patients (mean age 61.2 years, range 14.9–94.9) by 40 endoscopists. OCCR was 74.3% but if caecal intubation was confirmed by identification of the ileocaecal valve, then definite crude completion rate (DCCR) was 62.8%. When cases of marked faecal contamination, physical obstruction, severe colitis, planned limited examination, and equipment failure were excluded, definite adjusted completion rate (DACR) was 68.0%. OCCR, DCCR, and DACR improved progressively from year 1 to year 5:
OCCR for medical consultants was 78.8% (n = 1436), surgical consultants 69.7% (n = 1488), medical SpRs 87.9% (n = 232), surgical SpRs 66.3% (n = 560), and “others” 85.8% (n = 162). The most common reasons for failed completion were patient discomfort, looping and diverticulosis. Common diagnoses were: normal (43.6%), polyps (20.4%), cancer (12.1%) and colitis (9.1%). There was one procedure related death (perforation) and nine cases of minor complications.
Conclusions: Our completion rates compared favourably with the national audit (DCCR 56.9%). Although we did not achieve the threshold of 85% set by the screening programme, our year 5 OCCR is only 5% short and the yearly trend is encouraging. Completion rate is operator and specialty dependent and efforts, through targeted training, should be made to improve performance.
Abstract 277
Inflammatory bowel disease posters
278 IS SMALL BOWEL MEAL EXAMINATION USEFUL IN THE INVESTIGATION OF CHRONIC DIARRHOEA IF COLONIC IMAGING IS NORMAL?
V. Sharma, I. M. Patanwala, F. Mohammed, R. Tuono, S. Lee, J. M. Hebden.Manchester Royal Infirmary, Manchester, UK
The optimal investigative scheme for chronic diarrhoea is suggested in the recent British Society of Gastroenterology guidelines.1 If initial coeliac serology and colonic imaging is negative, small bowel examination is suggested. The yield in this clinical setting is however unclear.
Aim: To evaluate the utility of small bowel meal examination (SBM) in patients with chronic diarrhoea, and the influence of associated positive or negative inflammatory markers.
Methods: A retrospective case note review of all SBMs requested by a single gastroenterologist with the primary indication being chronic diarrhoea. Information on diagnostic tests, as well as inflammatory markers (ESR, C-reactive protein, and platelet count) were collected.
Results: 230 SBMs were requested from Mar 02–Apr 05. Case notes were retrieved in 220/230 (96%). In 127 diarrhoea was the main indication, and data were extracted from these case notes. Eighty eight patients had undergone total colonic evaluation (colonoscopy or barium enema). Crohn’s disease was detected in 19 (15%) patients (isolated small bowel Crohn’s in 10 (8%), small and large bowel Crohn’s in four (3%), and isolated large bowel Crohn’s in five (4%)). All 10 patients with isolated small bowel Crohn’s had undergone normal colonic evaluation. At least one inflammatory marker was raised in 6/10 (CRP elevated in all six cases). In the other four cases, all inflammatory markers were normal. A raised inflammatory marker gave an odds ratio of 7.5 (95% CI, 1.9 to30.4) for the presence of isolated small bowel Crohn’s disease.
Conclusion: SBM identified isolated small bowel Crohn’s disease in 10 out of 88 (11%) patients with chronic diarrhoea and normal colonic evaluation. 40% of these cases would have been missed if SBM had been reserved only for those patients with raised inflammatory markers.
1
279 CAPSULE ENDOSCOPY FOR THE DIAGNOSIS OF CROHN’S DISEASE IN ROUTINE CLINICAL PRACTICE
R. Sidhu, D. S. Sanders, D. P. Hurlstone, M. E. McAlindon.Royal Hallamshire Hospital, Sheffield, UK
Background: The mean time to diagnosis of small bowel Crohn’s disease from onset of symptoms is 1–7 years. Despite a high clinical suspicion, in a subgroup of patients, the diagnosis remains elusive with negative investigations. There is now increasing evidence for the use of capsule endoscopy (CE) in the diagnosis of Crohn’s disease.
Aim: To evaluate the diagnostic yield of CE in suspected Crohn’s disease or recurrence of disease in established Crohn’s patients, undetected by conventional modalities. We also assessed the impact of CE findings on the management of these patients.
Methods: All patients who underwent CE from January 2002 to August 2005 for suspected Crohn’s disease were included in this analysis.
Results: Forty six patients underwent CE for a clinical suspicion of Crohn’s disease, on a combination of patient history, raised inflammatory markers and inconclusive tests. In 59% (n = 27) of patients, a diagnosis of Crohn’s disease was made after detecting erosions, ulceration and mucosal oedema on CE. In 26% (7/27), CE was able to identify recurrence of disease in the small bowel in patients with an established diagnosis of Crohn’s disease. Prior to CE, 70% (n = 19) of patients had evidence of raised inflammatory markers and 85% (n = 23) of patients had undergone small bowel radiology: 70% normal (16), equivocal (6), abnormal (1). Additionally, five patients had a computed tomographic scan: thickening of bowel wall (3), normal (2). Previous histology of the small bowel was normal in five patients and equivocal in six patients despite the presence of terminal ileal ulceration on colonoscopy. 74% of patients with findings of Crohn’s disease on CE, underwent a change of management. This was in the form of medical treatment for Crohn’s disease (n = 17) or surgery (n = 3). In three patients, no treatment was initiated due to lack of symptoms at outpatient review, post CE.
Conclusion: CE has a high diagnostic yield in patients suspected of a new diagnosis of Crohn’s disease or recurrence in established disease. Findings of CE led to the change of management in the majority of patients suspected of Crohn’s disease.
280 VALUE OF ENDOSCOPIC ULTRASOUND TO IDENTIFY THICKENING OF THE EXTRAHEPATIC BILIARY TREE WALL IN PRIMARY SCLEROSING CHOLANGITIS
S. Mesenas, C. Vu, B. Baburajan, L. Doig, J. Meenan.Department of Gastroenterology, Guy’s and St Thomas’ Hospital, London, UK
Background: Diagnosing primary sclerosing cholangitis (PSC) is problematic and requires meeting a burden of proof through clinical, biochemical, radiological, and histological features. Endoscopic ultrasound yields detailed images of the extra-hepatic biliary tree but its value in contributing to the diagnosis of this condition is unknown.
Method: A prospective, controlled, single centre study with retrospective, blinded data analysis. Four groups of patients were assessed with radial endosonography: (a) PSC (n = 9); inflammatory bowel disease with abnormal liver blood tests (n = 21); choledocholithiasis (n = 15), and (d) normal controls (n = 50). Measurements were made of common bile duct diameter and wall thickness.
Results: Common bile duct diameter for the PSC, IBD, choledocholithiasis, and normal control groups were 8.9 (2.8 mm), 5.4 (1.7 mm), 7.2 (2.2 mm), and 5.0 (1.9 mm) respectively (PSC and choledocholithiasis as compared to the IBD group, p<0.05 for a single test of hypothesis; however, correction for the multiple testing of data removed this significance and normal control group p<0.005). Ductal wall thickness was 2.5 (0.8 mm) (PSC), 0.7 (0.4 mm) (IBD), 0.8 (0.4 mm) (choledocholithiasis), and 0.8 (0.4 mm) (normal control) groups respectively (PSC group compared to the other three groups, p<0.005).
Conclusion: Thickening (>1.5 mm) of the common bile duct wall is seen in patients with PSC but not in those with apparently uncomplicated IBD or choledocholithiasis. The results of this study suggest that standard endosonography contributes to the imaging and potentially the diagnosis of PSC.
281 RELATION OF OBESITY TO LATE ONSET CROHN’S DISEASE
B. J. John, S. Philpott, A. M. Abulafi, M. A. Mendall.Mayday University Hospital, Thornton Heath, Croydon CR7 7YE, UK
Introduction: Crohn’s disease (CD) is associated with innate immune (IM) activation. Smoking, its strongest main environmental risk factor is also associated with innate immune activation. Another potent condition associated with IM activation is obesity. In an earlier study we demonstrated that obesity was associated with subclinical bowel inflammation as determined by faecal levels of calprotectin.1 The main genetic risk factors for CD are associated with early age of onset. It is likely that environmental risk factors are collectively more important with older age of onset. We sought to determine whether premorbid obesity is associated with late onset CD.
Methods: We used a validated questionnaire for recall of premorbid weights. 214 subjects (CD = 100, UC = 114; 53% men) were recruited. The mean age of diagnosis was 38.9 (10–82) years. There was a bimodal distribution at age of presentation and we chose a cut off point of 50 years to define the older age group. 23/100 CD and 38/114 UC subjects were diagnosed aged 50+. 11/38 (29%) of UC and 13/23 (56.5%) of CD had a maximum premorbid BMI>30 (p = 0.03). There was a significant effect modification of obesity by age at diagnosis >50 (OR 8.67 (1.78–42.330, p = 0.0076)) after adjustment for age, sex, smoking, and age at diagnosis.
Conclusion: A possible association of obesity with late onset CD warrants further investigation. Further work is being undertaken to assess the difference in clinical characteristics of late and early onset CD. It is also possible that obesity associated IBD could be a different entity to other forms of CD.
1
282 DO THIOPURINE METHYL TRANSFERASE LEVELS GUIDE PRESCRIBING AND MONITORING OF THIOPURINES IN OUR CURRENT PRACTICE?
E. Wood, L. Medcalf, S. McCartney.Department of Gastroenterology, Middlesex Hospital, UCLH NHS Trust, Mortimer Street, London W1T 3AA, UK
Introduction: Thiopurines (azathioprine (AZA) and mercaptopurine (MP)) can cause potentially fatal myelotoxicity. Audit of our practice indicates that, despite postal reminders from our inflammatory bowel disease (IBD) nurse specialist, only 82% of patients taking maintenance thiopurine therapy attend for 3-monthly blood testing. Appreciating the uncertainties that remain regarding the role of thiopurine methyl transferase (TPMT) testing our aim was to review whether checking TPMT levels prior to initiating therapy can help guide the safe prescribing and monitoring of thiopurines in our practice.
Methods: All IBD patients taking thiopurines were identified over a six month period (October 04–March 05) and their notes reviewed retrospectively.
Results: Ninety patients were identified, 72/90 (80%) were on maintenance therapy whilst 18/90 (20%) were initiated on therapy during the study period. TPMT levels had been checked in all of the initiation group compared with 33/72 (45.8%) of the maintenance group. TPMT levels were low in 11/90 (12.2%) patients; four in the initiation group and seven in the maintenance group. The 4 patients in the initiation group with a low TPMT level were all started on low dose AZA (1 mg/kg) compared with 4/7 (57.1%) patients in the maintenance group. In the initiation group one patient with a low TPMT level developed hepatitis while in two patients with normal TPMT levels leucopenia (1) and hepatitis (1) occurred. In the maintenance group one patient with a low TPMT level, who had been started on AZA 2 mg/kg, developed leucopenia, whilst a further three patients with normal TPMT levels developed hepatitis.
Conclusion: TPMT levels did not appear to predict side effects in this small group of patients however it is noteworthy that none of the patients with low TPMT levels initiated on AZA 1 mg/kg developed myelotoxicity and that all episodes of leucopenia/hepatitis were identified by standard blood monitoring. TPMT testing does not obviate the need for regular blood monitoring but may identify patients at risk and thus help to guide the safe prescribing and monitoring of AZA/MP.
283 INCIDENCE OF GALLSTONES AND RELATED RISK FACTORS IN CROHN’S DISEASE AND ULCERATIVE COLITIS. A PROSPECTIVE COHORT STUDY
F. Parente1, L. Pastore2, S. Bargiggia1, S. Greco2, M. Molteni2, S. Gallus3, G. Bianchi Porro2.Gastrointestinal Units, 1A Manzoni Hospital, Lecco; 2L Sacco University Hospital, Milan; 3Epidemiology Lab, Mario Negri Institute, Milan, Italy
Background and Aim: Crohn’s disease (CD) has been associated with higher prevalence of gallstone disease (GD) in several retrospective studies,but the main contributing factors to the increased risk have not been well established yet as many may be similar to those in general population (age, sex, BMI). Aim of this prospective study was to evaluate the risk of developing GD in a defined cohort of CD and UC patients and to assess the possible predictors.
Material and Methods: We prospectively evaluated a cohort of 600 patients with inflammatory bowel disease (415 CD, 185 UC), who were free of previous GD at baseline liver ultrasound (US) as compared to 600 age, sex and BMI matched GD-free controls during a median follow up of seven years (range 5–12 years). Both patients and controls were followed up with periodic visits including liver US every 12 months. The incidence of GD was described by Kaplan-Meier plots. Multivariate analysis was used to discriminate among the impact of different variables (including age, sex, BMI, site and duration of disease, number of recurrences, type of medical therapy, number and extent of bowel resections, number and total length of hospitalisations) on the risk of developing GD.
Results: The 12 year incidence of GD was 3.1% in CD patients v 2.1% in matched controls and 1.2% in UC patients v 1.6% in matched controls. The risk of developing GD was 2.09 (95% CI 1.22 to 3.64) in CD patients and 1.33 (95% CI 0.56 to 3.16) in UC patients as compared to matched controls. On logistic regression analysis, ileo-colonic site of CD (OR 2.14, 95% CI 1.02 to 4.52), disease duration longer than 15 years (OR 4.26, 95% CI 1.64 to 11.1), >3 clinical recurrences (OR 8.07, 95% CI 1.03 to 63.3), ileal resection >30 cm (OR 7.03, 95% CI 2.56 to 19.3), >3 hospitalisations (OR 20.7, 95% CI 4.73 to 90.5), and total number of days in hospital >40 (OR 24.8, 95% CI 7.14 to 86.3) were independently associated with GD in CD.
Conclusions: Our data show that CD pts have a double risk of developing GD compared with age, sex, and BMI matched healthy controls, whereas the risk of GD in UC is similar to the general population. Site of disease, surgery, extent of ileal resections but also number of clinical recurrences, frequency, and duration of hospitalisations are the most important independent risk factors for GD.
284 THE IMPACT OF TWO WEEK REFERRAL INITIATIVE ON THE REFERRAL PATTERN OF PATIENTS WITH SUSPECTED INFLAMMATORY BOWEL DISEASE
S. Aroori, N. Jain, A. Valliattu, S. Jeyaretna, E. Whitehead, K. Hosie.Colorectal Surgery Unit, Derriford Hospital, Plymouth, UK
Background: Two week referral guidelines were introduced in the year 2000 to improve colorectal cancer services across the United Kingdom. We believe that since the introduction of these guidelines there is a change in the referral pattern of patients with inflammatory bowel disease (IBD).
Aims: To study the impact of two week referral initiative on the referral pattern of patients with suspected IBD.
Material and Methods: The referral, treatment, and histological details of all newly diagnosed IBD patients between 1999 and 2004 were retrospectively reviewed and analysed.
Results: 227 new patients, 48 in 1999, 36 in 2000, 37 in 2001, 38 in 2002, 27 in 2003, and 41 in 2004 were newly diagnosed to have IBD. Details of diagnosis includes; ulcerative colitis (UC) = 118 (52%), Crohn’s colitis (CC) = 84 (37%), and indeterminate colitis (IDC) = 25 (11%). There was a significant change in the referral pattern following introduction of guidelines. In 1999, 36% of newly diagnosed IBD patients were seen by surgeons compared to 66% in 2002 (p = 0.005), 59% in 2003 (p = 0.04), and 66% in 2004 (p = 0.004). We also examined the primary prescription of drugs for the rectal disease. Seventy eight patients (34.4%) had rectal disease. Among 78, 53 patients had isolated rectal UC, nine had rectal disease due to IDC, eight had left colonic CC, and eight had left sided UC. Fifty eight patients received rectal preparations along with or without systemic treatment and 17 received systemic treatment alone. Three patients did not require any treatment due to mild disease. Fifty six per cent of patients seen by surgeons were treated with rectal steroid preparations compared to only 17% of patients seen by gastroenterologists (56% v 17%, p = 0.01).
Conclusions: There has been significant change in the referral pattern of patients with IBD following introduction of two week referral guidelines. More patients were referred to surgeons following the introduction of two week referral guidelines. Surgeons tend to prescribe steroids more often than gastroenterologists do for the rectal disease.
285 LONG TERM PROGNOSIS IN CROHN’S DISEASE: AN EPIDEMIOLOGICAL STUDY OF PATIENTS DIAGNOSED MORE THAN 20 YEARS AGO IN CARDIFF
C. Canavan1, K. R. Abrams2, B. Hawthorne3, J. F. Mayberry1.1Digestive Diseases Centre, University Hospitals of Leicester; 2Centre for Biostatistics and Genetic Epidemiology, University of Leicester; 3University Hospital of Wales, Cardiff, UK
Background: Early studies into mortality associated with Crohn’s disease suggested standardised mortality rates (SMR) significantly higher than the general population, especially in those recently diagnosed. One study recognised a second mortality peak in those diagnosed over 13 years. Recent studies report SMR near normal, but these studies have insufficient follow up to capture a second peak. This study investigates mortality experience of patients diagnosed over 20 years ago, representing the longest follow up to date.
Methods: The Cardiff database of patients with Crohn’s disease was established in the 1970s containing data on all patients diagnosed in Cardiff since 1934. 394 patients diagnosed before 1 January 1985 were traced and their mortality status on 31 December 2004 established.
Results: Overall SMR is 1.29 (95% CI 1.12 to 1.45) and has not statistically significantly changed since the 1970s. Mortality decreases with increasing age, from 16.95 (95% CI 14.99 to 18.91) for patients aged 10–19 years, to 0.92 (95% CI 0.65 to 1.19) in those over 75 years. Kaplan-Meier analysis of age at death shows patients diagnosed aged 10–26 years have mean age at death of 58.3 years, for those aged 27–52; 66.3 years, aged 53–58; 74.5 years and those over 59 years; 79.3 years.
Discussion: This study represents the longest follow up of a cohort of patients with Crohn’s disease to date. It shows significantly raised SMR, not statistically changed since the 1970s and similar to other chronic conditions. Patients diagnosed younger have worse prognosis than those diagnosed later and a reduced life expectancy compared to the general population.
286 THE IBD DATABASE: USE AND ACHIEVEMENTS
C. M. Edwards1, C. Royston2, H. Durbin1, A. Coulson1, K. D. Bardhan (on behalf of the User Group)2.1Torbay Hospital, Devon; 2Rotherham DGH, S Yorks, UK
Background: The Rotherham Inflammatory Bowel Disease Database (IBD-DB) has been developed in response to the need for easy access to data on patients with IBD. Two centres from the larger user group have piloted the IBD-DB over the last year for clinical, audit, and monitoring purposes.
Principal difficulties: IT; financial and human resource to support IBD-DB set up and data entry.
Principal gains: Electronic patient record; generation of clinic letters; prescribing record and pharmacy audit; immuno-suppression monitoring; medical and surgical activity; colonoscopic surveillance programme; validated phenotypic description of IBD population.
Results: Preliminary demographic data from the two centres show good agreement (see table).
Abstract 286
Conclusion: The use of the IBD-DB supports good clinical practice, informs the national evidence base for IBD. Its potential for clinical audit, governance, and clinical research is self-evident. Ten centre data will be available shortly.
287 HYPNOTHERAPY DECREASES RECTAL MUCOSAL RELEASE OF SUBSTANCE P, HISTAMINE, AND IL-13 IN PATIENTS WITH ACTIVE ULCERATIVE COLITIS
J. E. Mawdsley, D. G. Jenkins, D. S. Rampton.Centre for Gastroenterology, ICMS, Barts & London, Queen Mary School of Medicine & Dentistry, London, UK
Introduction: Hypnotherapy is effective for functional GI disorders and has been claimed to improve ulcerative colitis (UC). How hypnotherapy may act is unknown but could involve reductions in mucosal neurotransmitter, mast cell mediator and cytokine production.
Aim: To assess the effects of one session of hypnotherapy on the concentrations of substance P (SP), histamine, TNF-α, and IL-13 in rectal peri-mucosal fluid (RPMF) in patients with active UC.
Methods: For 50 minutes patients with active UC (Baron score>1) underwent either (1) gut focused hypnotherapy or (2) control session—relaxing music. Autonomic response was assessed by pulse and BP every 15 minutes. A sample of RPMF was collected before and after each protocol by placing a 7×30 mm strip of filter paper via a rigid sigmoidoscope against the rectal mucosa for 1 minute until wet. The filter paper was incubated in 1 ml BSA (0.3%), sodium azide (0.01%) and Tween 20 (0.002%) in PBS for 24 hours and SP, histamine, TNF-α, and IL-13 concentrations in the buffer measured by ELISA.
Results: The control protocol did not change any variable. Hypnosis reduced pulse rate by 7 bpm, systolic BP by 2 mmHg, and RPMF concentrations of SP by 81%, histamine by 35% and IL-13 by 54%.
Conclusion: Hypnotherapy reduces rectal mucosal release of SP, histamine, and IL-13, but not of TNF-α, in active UC. These changes could provide a basis for a beneficial effect of hypnotherapy in UC.
Abstract 287
288 REGULATION AND AUTOCRINE ACTION OF AMPHIREGULIN AND EPIREGULIN IN HUMAN COLONIC SUBEPITHELIAL MYOFIBROBLASTS
O. Inatomi, A. Andoh, Y. Yagi, S. Bamba, T. Tsujikawa, Y. Fujiyama.Department of Internal Medicine, Shiga University of Medical Science, Otsu, Japan
Backgrounds: Human amphiregulin (AR) and epiregulin (EP) belong to the epidermal growth factor (EGF) family and exert their effects as mitogenic stimulators. Recent studies have suggested that AR and EP support reconstitution of the gastrointestinal tissue. However, the local secretion of AR and EP in the intestine remains unclear. Subepithelial myofibroblasts (SEMFs) play a central role in processes involved in inflammation and wound healing in the intestine. In this study, we investigated AR and EP secretion in human colonic SEMFs.
Methods: Primary cultures of SEMFs were prepared according to the method reported by Mahida et al. The studies were performed on passages 2–6 of SEMFs isolated from three resected specimens. AR and EP mRNA expressions were evaluated by Northern blotting, and the protein secretion was determined by Western blotting. Cell proliferation of SEMFs was tested for by using a MTT assay.
Results: AR and EP mRNAs were not detected in unstimulated SEMFs by Northern blotting. Among the various kind of cytokines and growth factors, interleukin (IL)-1β, tumour necrosis factor (TNF)-α, and EGF strongly induced AR and EP mRNA expression. In addition, AR and EP induced their own mRNA expressions by themselves. The effects were detected in dose and time dependent manner. These responses were significantly reduced by AG1478, the specific inhibitor of EGF recepter tyrosine kinases. AR and EP secretion were also observed at the protein levels. A MTT assay demonstrated that AR and EP stimulate the proliferation of SEMFs at concentrations of 1.0 ng/ml–100 ng/ml
Conclusions: (1) IL-1β, TNF-α, and EGF were strong inducers of AR and EP in human colonic SEMFs. (2) AR and EP acted as autocrine growth factors for SEMFs and stimulated their proliferation. These results show that AR and EP may play an important role in the mechanism of wound healing in the inflamed intestinal mucosa such as inflammatory bowel disease.
289 PHENOTYPIC SUBGROUP ANALYSES REVEAL AN INTERACTION BETWEEN THE NOD1 INSDEL POLYMORPHISM (INSDEL) AND SMOKING STATUS IN CROHN’S DISEASE
D. P. B. McGovern, P. Hyssi, T. Ahmad, W. O. C. Cookson, D. P. Jewell.The Wellcome Trust Centre for Human Genetics and Gastroenterology Unit, The University of Oxford, UK
Introduction: The development of IBD is under the influence of genetic (for example NOD2) and environmental (for example smoking) factors. We have reported an association between an insertion/deletion polymorphism (INSDEL) in NOD1(CARD4) and IBD.
Aim: To assess the role of the INSDEL in defining IBD subgroups and to explore NOD1 gene-gene or gene-environment interactions.
Methods: The INSDEL was genotyped in 335 CD, 306 ulcerative colitis (UC) and 335 controls (HC) (cases reported in the original paper) and data was available regarding the presence of extra-intestinal manifestations (EIMs) from the 556 IBD trios also reported in the original paper. Associations were analysed using standard statistical methods.
Results: Univariate analyses demonstrated association between INSDEL and ileal (p = 0.007), perianal (p = 0.03), stenotic (p = 0.005), and fistulating (p = 0.004) CD, although these associations were not independent in multivariate analyses. Independent associations with the development of CD under 16 years (p = 0.015) and >25 years (p = 0.002) when compared respectively with those developing disease over the age of 16 and 25 were seen. The INSDEL is found at higher frequency in CD non-smokers than in CD smokers (p = 0.0004). Logistic regression analyses suggest association with smoking status (p = 0.034) and not with age of onset (p = 0.38). No significant association with any UC phenotype was seen. INSDEL was associated with the presence of large joint arthritis (RR 1.76), erythema nodosum (RR 1.81), uveitis (RR 2.15) and PSC (RR 2.14) in univariate analyses. Multivariate analyses only revealed association with the presence of any E.I.M. (p = 0.039). There was no gene-gene interaction between NOD1 and NOD2/IBD5.
Conclusion: The risk for developing CD conferred by the NOD1 INSDEL appears to be greatest in non-smokers. This may reflect, in part, the greater influence of genetic, rather than environmental, risk factors in patients who develop CD at a young age.
290 NORMAL RESPONSES TO SPECIFIC NOD1 ACTIVATING PEPTIDOGLYCAN AGONISTS IN THE PRESENCE OF THE NOD2 FRAMESHIFT AND OTHER MUTATIONS IN CROHN’S DISEASE
D. A. van Heel1, K. A. Hunt1, S. Ghosh1, M. Hervé2, R. J. Playford1.1Imperial College London, London, UK; 2Université Paris-Sud, Paris, France
Background and Aims: Both NOD2/CARD15 alleles are mutated in ∼10% of Crohn’s disease patients, causing loss of functional responses to low dose muropeptide agonists. We hypothesised that NOD2 mutations may also impair NOD1/CARD4 responses, supported by data suggesting NOD2 1007fs/1007fs patients had reduced responses to a putative NOD1 agonist, M-TriDAP (Netea et al. J Biol Chem 2005).
Methods: We measured peripheral blood mononuclear cell (n = 8 NOD2 wild type, n = 4 1007fs/1007fs, n = 6 702Trp/1007fs, n = 5 702Trp/702Trp, n = 3 908Arg/1007fs) responses to NOD1 agonists alone (IL-8), and agonist enhancement of lipopolysaccharide responses (IL-1β).
Results: Significant responses were seen with M-TriDAP at 10 nM (as with NOD2 agonists), but only at ⩾100 nM with FK565 and TriDAP. M-TriDAP induced IL-8 and enhancement of lipopolysaccharide IL-1β responses were significantly reduced between NOD2 double mutation carriers versus healthy controls. However there was no difference with FK565 or TriDAP stimulation, or between 1007fs/1007fs cells and other genotypes.
Conclusions: M-TriDAP contains the minimal structures for both NOD1 (γ-D-Glu-mesoDAP) and NOD2 (MurNAc-L-Ala-D-Glu) whereas FK565 and TriDAP contain only NOD1 activating structures. M-TriDAP has dual NOD1/NOD2 agonist activity in primary cells, perhaps due to different intracellular peptidoglycan processing compared to the HEK293 cell system typically used for agonist specificity studies. Responses to specific NOD1 agonists are unaffected by NOD2 genotype. NOD1/NOD2 crosstalk does not occur.
291 CO-LOCALISATION OF TOLL-LIKE RECEPTORS WITH SIGNALLING MOLECULES IRAκ-1 AND NFκB IN COLONIC BIOPSIES OF PATIENTS WITH INFLAMMATORY BOWEL DISEASE
A. De Costa1, N. Rayment1, M. Mylonaki1, L. Petrovska1, B. N. Hudspith1, J. Brostoff1, C. Nunes1, G. Parkes1, J. D. Sanderson1, D. S. Rampton2.1Nutritional Sciences Research Division, King’s College London; 2Academic Dept of Adult & Paediatric Gastroenterology, Barts & the London, Queen Mary’s School of Medicine & Dentistry, London, UK
Background: We have previously reported anomalies in mucosa associated bacterial flora in inflammatory bowel disease (IBD) patients as well as the presence of E coli associated with macrophages in the lamina propria of these patients. By looking at signalling molecules IRAK-1 and NFκB we have now investigated the activation status of both epithelial cells and lamina proprial macrophages and compared this with their co-expression of toll-like receptors (TLRs) 2, 4, and 5.
Methods: Snap frozen rectal biopsies were taken at routine colonoscopy from patients with ulcerative colitis (UC, n = 8), Crohn’s (CD, n = 8) and controls with normal colorectal mucosa (n = 8). TLR 2, 4, and 5, signalling molecules IRAK-1, NFκB expression and macrophages (CD68) was determined using immunofluorescence. Co-localisation was confirmed using confocal microscopy.
Results: In controls, moderate epithelial expression of TLRs 2 and 4 but not 5 was seen. This correlated with a complete absence of IRAK-1 or NFκB. IBD biopsies showed an increase in epithelial expression of TLRs 2 and 4 but not 5 with a corresponding increase in IRAK-1 and NFκB levels. Lamina propria, macrophages showed greater expression of TLRs 2 and 4 in IBD patients compared to controls. Modest amounts of TLR-5 were also seen in this group. Co-localisation of TLRs with IRAK-1 and NFκB in lamina proprial macrophages showed a significant increase in activation compared to that seen in epithelial cells.
Conclusion: The increased expression of TLRs in IBD patients may contribute to the heightened immunological response to bacteria especially those associated with lamina proprial macrophages.
292 HISTOLOGICAL PHENOTYPE OF CARD15 GENOTYPE
C. Todhunter, L. Wilkinson, J. Henry, C. G. Mathew, A. Burt, J. C. Mansfield.University of Newcastle upon Tyne, Queen Elizabeth Hospital, Gateshead, Guy’s, King’s and St Thomas’ School of Medicine, London and Royal Victoria Infirmary, Newcastle upon Tyne, UK
Introduction: The histological features of Crohn’s disease (CD) are varied. The characteristic features of CD are considered to be skip lesions and focal ulceration with transmural inflammation, lymphoid aggregates and granulomas. Pyloric metaplasia is a well recognised feature of CD. The aim of this study was to investigate the relationship between the histological features and CARD15 genotype. CARD15 is expressed in Paneth cells of the small bowel. We therefore investigated whether Paneth cell numbers and distribution were related to CARD15 genotype.
Method: Forty nine patients with CD and 10 controls who had had terminal ilectomy/right hemicolectomy were included in this study. Archival tissue that had been processed routinely was used for histological analysis. Venous blood was obtained for genotyping of the patients with CD. This study was approved the local research ethics committees.
Results: Ten CD patients carried two CARD15 mutations, 17 one mutation, and 22 were wild type. CD patients who carried two CARD15 mutations had a significantly greater mean number (6.4) of Paneth cells than controls (2.1) and patients who had none (4.2) or one mutation (5.0) p<0.001. Paneth cells were found significantly higher up the sides of crypts in patients who carried two CARD15 mutations than controls and other genotypes, p<0.001. The presence of pyloric metaplasia was significantly associated with carriage of at least one CARD15 mutation, p<0.001. There was no association with CARD15 and inflammatory score, lymphoid aggregates, and granulomas.
Conclusion: We have found a distinct histological phenotype correlated to CARD15 genotype. The finding of an association between pyloric metaplasia and CARD15 in CD is new and warrants further investigation. The increase in Paneth cell numbers in patients with 2 CARD15 mutations independent of degree of inflammation suggests that CARD15/NOD2 pathway may be involved in Paneth cell regulation.
293 ASSOCIATION OF THE MDR1 GENE WITH INFLAMMATORY BOWEL DISEASE: A CASE CONTROL AND META-ANALYSIS STUDY
C. Onnie1, S. A. Fisher1, R. Pattni1, J. Sanderson2, A. Forbes3, C. M. Lewis1, C. G. Mathew1.1King’s College London School of Medicine, London, UK; 2Guy’s and St Thomas’ Hospitals, UK; 3St Mark’s Hospital, Harrow, UK
Background: Allelic variants of the multidrug resistance gene (MDR1/ABCB1) which encodes the membrane bound efflux transporter P-glycoprotein 170 (PGP-170) have been associated with inflammatory bowel disease (IBD), but with conflicting results. Our aim was to examine the association of MDR1 variants in a large British case control sample, and to carry out a meta-analysis of published studies.
Methods: The MDR1 variants C3435T and G2677T/A were genotyped in 828 Crohn’s disease (CD) and 580 ulcerative colitis (UC) cases and 285 healthy controls, and their effect on disease heterogeneity was examined. A meta-analysis was carried out of our results and those from eight published association studies of the C3435T variant in IBD, which included a total of 1743 cases of UC, 2311 of CD, and 2931 controls.
Results: The 2677T allele was significantly increased in British UC cases compared to controls (45.2% v 39.6% p = 0.034). In particular, the TT genotype was significantly associated with severe UC (OR 1.90, 95% CI 1.01 to 3.55) and in UC patients receiving steroids (OR = 1.77 95% CI 1.08 to 2.88). No significant association was seen with C3435T and UC, CD or any clinical subgroup. A meta-analysis of nine association studies of C3435T showed a significant association of the 3435T allele with UC (OR 1.12, 95% CI 1.02 to 1.23 p = 0.013), but not with CD.
Conclusions: The meta-analysis we have carried out confirms the association of the C3435T sequence variants in MDR1 with susceptibility to UC but not to CD. The small size of the effect in UC is consistent with difficulties in replicating the association in individual studies. Our finding of the association of the 2677T allele with specific clinical subgroups of UC suggests that MDR1 may influence disease behaviour in IBD. Analysis of MDR1 gene expression in patients with defined MDR1 genotypes may clarify the role of this gene in disease susceptibility and behaviour in IBD.
294 PREVALENCE OF CYTOMEGALOVIRUS IN COLECTOMY SPECIMENS FROM ULCERATIVE COLITIS PATIENTS
R. B. Jones, C. Bratten, O. Rotimi, P. J. Hamlin.Department of Gastroenterology, Leeds General Infirmary, LS1 3EX, UK
Aim: Controversy remains over the importance of cytomegalovirus (CMV) in ulcerative colitis refractory to medical therapy. It has been suggested that the infection rate is as high as 27% in steroid refractory disease (Maconi et al. 2005). Our aim was to determine the prevalence of cytomegalovirus (CMV) in colectomy specimens taken from UC patients.
Methods: Forty nine colectomy specimens taken from patients with ulcerative colitis were identified between the years 1990 and 2000. The indication for surgery and history of immunosuppressive drug therapy were noted along with disease duration. The indication in 41 patients was chronic refractory or relapsing disease not fully responding to medical therapy, in six there was severe disease not responding to medical therapy, there was one case of fulminant colitis with megacolon and one cancer. Haematoxylin and eosin (H&E) and immunohistochemical staining for CMV inclusions was carried out on each specimen and interpreted by two pathologists.
Results: Twenty of 49 patients were taking azothioprine at the time of surgery, of which 15 were taking concomitant steroids. 24 were receiving steroid therapy alone prior to colectomy. Contrary to recent studies CMV was not identified in any of our specimens, either by H&E or the more sensitive immunohistochemistry.
Conclusions: Our data suggest no role for CMV in ulcerative colitis refractory to medical therapy. This is clearly reassuring when the treatment for severe UC frequently involves increased immunosuppression before surgery. In cases of resistant colitis biopsy and immunohistochemistry are not routinely required to look for CMV.
295 ACTIVE BACTERIA ASSOCIATED WITH COLORECTAL BIOPSIES
G. L. Green, J. D. Sanderson, L. Petrovska, B. N. Hudspith, D. S. Rampton1, J. Brostoff, K. D. Bruce.King’s College London; 1The Royal London Hospital, London, UK
Background: In order to differentiate between the bacteria merely associated with gut mucosa and those that are active, we have studied the marker bacterial rRNA. This molecule, only present in active bacterial cells, allows us to determine the levels of activity of species associated with diseased and non-diseased regions within patients.
Methods: Paired colorectal biopsies were taken for 10 patients with active inflammatory bowel disease (IBD). One inflamed biopsy and one uninflamed biopsy was taken. Nucleic acids were recovered directly from each biopsy. After dividing into DNA or RNA, rRNA was converted to cDNA by reverse transcription. Both DNA (bacteria present) and cDNA (bacteria active) templates were separately amplified using primers specific for phylogenetically informative ribosomal sequences within the Domain Bacteria. Both sets of PCR products were separated by using Denaturing Gradient Gel Electrophoresis (DGGE) to form profiles from which mean similarity coefficient (MSC)s were generated.
Results: cDNA DGGE profiles were generated for every sample indicating an active bacterial community. Although the MSCs obtained for all paired comparisons were generally high, differences in species present were observed. The similarity between the DNA and cDNA samples for the uninflamed biopsies had a MSC of 92% (SD 9%, n = 5), with the similarity between the DNA and cDNA samples for the uninflamed biopsies having a MSC of 93% (SD 3%, n = 5). Comparisons between the uninflamed biopsy and the paired uninflamed biopsy gave MSC values of 93% (SD 8%, n = 5) for DNA and 98%, (SD 3%, n = 5) for cDNA.
Discussion: Overall, these data suggest that the bacterial communities from a “non-diseased” and a diseased colorectal region of an IBD patient are broadly similar. These results also indicate however that many bacterial species associated with the gut mucosa are active and that differences can be identified in the species that are present and active in these samples.
296 DETECTION OF HELICOBACTER SPECIES IN ARCHIVAL HUMAN ULCERATIVE COLITIS TISSUE BY FLUORESCENT IN SITU HYBRIDISATION
I. A. M. Cooper1, J. M. Thomson1, G. L. Hold1, M. G. Smith1, N. Fyfe1, N. A. G. Mowat1, Z. Shen2, J. G. Fox2, E. M. El-Omar1.1GI Research Group, Department of Medicine and Therapeutics; 2Division of Comparative Medicine, Massachusetts Institute of Technology, Boston, MA, USA
Background: The role of Helicobacter species in human inflammatory bowel disease (IBD) is controversial. This in part is due to differences in techniques used and to lack of definition of disease phenotypes.
Aim: To investigate archival paraffin embedded tissue from patients with confirmed ulcerative colitis (UC) for the presence of Helicobacter species.
Subjects and Methods: 100 UC patients (65 relapsing, 35 de novo) and 39 controls with a normal colonoscopy, had archival biopsies investigated. The biopsies were taken from throughout the colon. Fluorescent in situ hybridisation (FISH) assays were designed to differentiate H pylori from non-pylori Helicobacter species. The sections were analysed in triplicate.
Results: The Helicobacter genus was present in 33 of the 100 patients with UC. Of these, 31 were non-pylori and two were pylori species. However in the control group 23 (60%) were positive for the Helicobacter genus but only nine (23%) were non-pylori Helicobacter and 14 (35%) were H pylori. The only statistically significant difference between the UC cases and controls was the lower prevalence of H pylori in the colitis group (p<0.01). There was no difference in prevalence of non-pylori Helicobacters between de novo presenting and relapsing colitis patients. The distribution of Helicobacter species was predominately in the left side of the colon in both the colitis and control patients. The Helicobacter species were detected on the mucosa and in colonic crypts, in both inflamed and non-inflamed biopsies.
Conclusions: Non-pylori Helicobacter species are commonly detected in UC patients and subjects with normal colons. The role of these species in the pathogenesis of UC, if any, remains to be established.
297 FURTHER CHARACTERISATION OF MUCOSA ASSOCIATED ESCHERICHIA COLI ISOLATES FROM CROHN’S DISEASE AND COLON CANCER PATIENTS
H. M. Martin1, B. J. Campbell2, S. Subramanian2, C. A. Hart3, J. M. Rhodes1.1Provexis Plc, Biosciences Building, Crown Street, Liverpool, UK; 2Department of Medicine, University of Liverpool, UK; 3Department of Medical Microbiology, University of Liverpool, UK
Introduction: We previously reported that E coli isolated from biopsies taken from Crohn’s disease and colon cancer patients displayed enhanced adherence to erythrocytes and intestinal cell lines whilst lacking the conventional markers of bacterial pathogenicity (Gastroenterology 2004;127:80–93). Here we describe further phylogenetic and phenotypic characterisation of these strains.
Methods: For phylogenetic analysis, 21 strains of CD and colon cancer associated E coli (14 adherent and 7 non-adherent strains) were screened for the presence of the chuA, and yjaA genes, and the TSPE4.C2 DNA fragment (Appl Environ Microbiol 2000;66:4555–8). Haemagglutination (HA) and HEp-2 cell adhesion assays were performed using all adherent E coli strains.
Results: All adherent isolates and 2/7 non-adherent isolates were classed into E coli phylogenetic groups D1 or D2, characteristic of virulent extra-intestinal E coli. This grouping was performed on the basis of the presence of the chuA gene required for heam transport in enterohaemorrhagic O157:H7 E coli. Five out of seven non-adherent isolates were classed into E coli phylogenetic groups A1 or B1, characteristic of commensal E coli. 11/14 adherent isolates displayed adherence to HEp-2 cells in a pattern characteristic of diffusely adherent E coli (DAEC). All adherent strains displayed chloramphenicol resistant HA indicative of specificity to cell surface receptors other than DAF (CD55), possibly CEACAMs. Strong haemagglutinating activity was found in some bacterial supernatants suggesting secretion of a bacterial adhesion factor, possibly on shed microvesicles.
Conclusions: Adherent mucosa associated E coli strains isolated from CD and colon cancer display attributes characteristic of virulent extra-intestinal E coli, and probably represent typical or atypical DAEC.
298 EFFECT OF INFLAMMATION ON GUT FLORA DIVERSITY IN INFLAMMATORY BOWEL DISEASE PATIENTS: 16S RDNA SEQUENCE ANALYSIS
L. Petrovska1, J. Sanderson1, D. Pickard2, B. Hudspith1, N. Rayment1, K. Bruce1, J. Brostoff1, D. Rampton1, J. Parkhill2, G. Dougan2.1Nutritional Sciences Research Division, King’s College London, UK; 2Wellcome Trust Sanger Institute, Hinxton, Cambridge, UK
Introduction: Gut mucosa associated flora play a key role in the pathogenesis of inflammatory bowel disease (IBD). 16S rDNA is universally distributed among prokaryotes and is reliable source for deducing phylogenetic relationships.
Aim: The aim of this study was to examine how the mucosal adherent microbial communities differ between inflamed and non-inflamed sites in the GI tract of IBD patients and also between different mucosal sites by using large scale 16S rDNA sequencing
Methods and Results: Mucosal biopsies of the inflamed and non-inflamed sites were obtained from IBD patients and controls undergoing colonoscopy. The 16S rDNA genes from each separate biopsy sample were amplified using a low number of PCR cycles, clone library established and approximately 1000 clones from each library sequenced. Phylotype census was constructed for each sample and total and novel phylotype presence calculated. Nonchimeric 16S rDNA sequences were further analysed and phylogenetic groups determined. The bacterial phylum distribution generated from four different mucosal sites in two patients, based on 4000 clone sequences (fig) revealed increased Bacteroidetes and decreased Proteobacteria in inflamed sites.
Conclusions: 16S rDNA molecular characterisation of the mucosal associated flora demonstrates specific changes at sites of inflammation. Further characterisation may provide insights into pathogenetic significance of these changes.

Abstract 298 Samples from inflamed and non-inflamed sites from patients with Crohn’s disease and ulcerative colitis.
299 INFLIXIMAB THERAPY FOR CROHN’S DISEASE CAN BE SAFELY INFUSED OVER ONE HOUR WITHOUT INFUSION REACTIONS
L. Younge, M. O’Connor, N. Arebi, D. Lloyd.St Mark’s Hospital, Harrow, UK
Background and Aim: Infliximab (chimeric monoclonal anti-TNFα antibody therapy) is licensed for the treatment of rheumatoid arthritis (RA) and Crohn’s disease (CD). Maintenance therapy is indicated for both refractory and fistulating CD. In both conditions maintenance treatment is prescribed at 8 weekly intervals. A two hour infusion regime followed by a two hour observation period is recommended, meaning patients spend ½ day in hospital every 8 weeks receiving their infusion. Reduced infusion time for the treatment of RA has been studied with good success. The aim of this study was to determine whether reduced infusion time would be tolerated in patients with CD, and to assess the safety within the day care setting.
Methods: Patients who had previously received at least four infusions of infliximab at the standard rate of two hours with no adverse effects and no other excluding factors were selected over a 10 week period. Informed consent was obtained. All patients received pre-medication with intravenous hydrocortisone, followed by a one hour infliximab infusion with a one hour post infusion observation period. Infusion reactions, side effects or delayed hypersensitivity reactions were noted.
Results: Thirteen patients received the one hour infliximab regime compared to 20 who received the usual two hour regime during the study period. Within the one hour infusion group, 9/13 (69%) were receiving concomitant immunosuppressant therapy compared to 18/20 (90%) within the two hour infusion group. No infusion reactions or adverse events were observed in either patient group. No patients reported symptoms of delayed hypersensitivity reactions.
Conclusion: CD patients who had previously received four or more infliximab infusions over two hours with no adverse events tolerated reduced infusion rates of one hour well with no immediate or delayed adverse reactions. Faster infusion rates save time for both patients and health care professionals and facilitate better use of healthcare resources within the day care setting.
300 COMBINATION THERAPY OF INFLIXIMAB AND AZATHIOPRINE REDUCES DISEASE PROGRESSION IN CROHN’S DISEASE
S. Din, C. J. Cochrane, C. L. Noble, J. Satsangi, I. D. R. Arnott.Gastrointestinal Unit, University of Edinburgh, Edinburgh, UK
Introduction: The Vienna classification of Crohn’s disease (CD) categorised disease behaviour into a hierarchy of inflammatory, structuring, and penetrating types. 92% of patients have been shown to progress over a 20 year period. Infliximab induces mucosal healing and clinical remission; it is unknown whether this drug reduces the progression of disease type. We aimed to examine the impact of episodic infliximab treatment on the progression of disease behaviour in CD.
Methods: Seventy three CD (38F) patients who received episodic infliximab were assessed, together with an age and sex matched control group comprising 73 patients who had received azathioprine for at least four months. Both groups had two years’ follow up during which disease progression events were identified. Demographic details, disease characteristics and treatment history were collected. Kaplan-Meier survival curve analysis, the log rank test, and multiple logistic regression were used to test for differences and identify independent variables associated with disease progression.
Results: Twice as many patients experienced progression of disease type in the control (azathioprine) group (10/50) compared with the infliximab group (5/42), p = 0.165, log rank test. Patients on both azathioprine and infliximab (n = 17) had less disease progression compared to those on azathioprine alone (0/17 v 10/50, χ2, p = 0.045). Surgical rates did not differ. Disease progression was also associated with significantly more disease flares (p = 0.017) and higher surgical rates (p = 0.000). Multivariate analysis identified smoking at treatment induction and concomitant usage of corticosteroids as independent predictors of disease progression.
Conclusion: Combination therapy with episodic infliximab and azathioprine retards the progression of disease in CD and therefore may alter the “natural” history of this disease. Smoking at treatment induction and concomitant corticosteroid therapy are independent predictors of disease progression. In this short term study, the need for surgery was not affected by infliximab usage.
301 USE OF PHOTOIMMUNE THERAPY IN THE TREATMENT OF REFRACTORY CROHN’S DISEASE
S. C. Kong1, K. W. Douglas2, A. Todd2, A. J. Stanley1, J. F. MacKenzie1.1Department of Gastroenterology, 2Clinical Apheresis Unit, Glasgow Royal Infirmary, Glasgow, UK
Introduction: Crohn’s disease (CD) is an incurable chronic debilitating illness. Despite conventional treatments that include steroids, aminosalicylates, 2nd line immunosuppressants, infliximab, and surgery, management remains difficult with many side-effects. Photoimmune therapy (photopheresis) is a treatment modality that is emerging as a new treatment for CD.
Aim: To study the response of patients with refractory CD, who had failed conventional treatments and undergone multiple surgeries, to photopheresis treatment.
Methods: Five patients with refractory CD were treated with photopheresis on a Therakos cell separator. Ultraviolet A light was used for photoinactivation of T cells and macrophages which have been photosensitised by 8-methoxypsoralen. Each treatment session consisted of two photopheresis sessions in two consecutive days. In four patients treatment sessions were planned for every fortnightly for six months then monthly for another six months. One patient was treated fortnightly for six weeks, then monthly for six months followed by 3-monthly for a year.
Results: All five patients treated were male and their mean age was 37.2 years old. One patient withdrew from the treatment due the long distance he had to travel. The patient on the longer but less intense treatment regime had a partial response. The remaining three patients had good response to the treatment. The response included needing less medication (one patient stopped steroid after being steroid dependent for years), decrease in bowel movement frequency, less abdominal pain, less PR discharge, or improvement in the quality of life. None of the patients had significant side effects.
Conclusion: Early experience shows that photopheresis could be effective in the treatment of refractory CD. The treatment is well tolerated. This is the largest cohort of patients with refractory CD treated with photophersis to date in United Kingdom. A larger formal study will now be undertaken to study the effectiveness of this treatment
302 A PHARMACOECONOMIC EVALUATION OF HIGH DOSE ORAL MESALAZINE FOR MODERATELY ACTIVE ULCERATIVE COLITIS: A DECISION ANALYTIC MODEL
J. Borrill1, A. Bhatt2, K. Bodger3.1Abacus International, Bicester, Oxfordshire, UK; 2Procter and Gamble Pharmaceuticals, UK; 3University Hospital Aintree, Liverpool, UK
Objective: To evaluate the economic impact of high dose oral mesalazine as a first line treatment for patients with moderately active ulcerative colitis (UC).
Design: A decision tree model was constructed to estimate the patterns of treatment, resource consumption and cost impact of treating moderately active UC with 4.8 g/day of Asacol 800 mg MR tablets compared to a conventional dose of 2.4 g/day. Differences in treatment effects were obtained from a pooled analysis of two, phase III clinical trials. Resource use data was derived from a UK study that assessed the direct costs of IBD in secondary care. These data were supplemented with information from the literature and expert opinion. The analysis was conducted from the perspective of the NHS using a time horizon of six months. Participants: A hypothetical cohort of 1000 patients with moderately active UC
Results: Treatment success at six weeks was achieved in 72% of patients treated with Asacol 4.8 g/day compared to 59% in the Asacol 2.4 g/day group (p = 0.0034). The model projected that fewer patients receiving Asacol 4.8 g/day would require surgery (5% v 7%) or intensive intravenous or immunosuppressive therapy (7% v 10%) compared to those given 2.4 g/day. Over six months, the mean expected cost per patient was £1300 for the Asacol 4.8 g/day treatment pathway compared to £1640 for the 2.4 g/day pathway—a cost saving of £340 per patient. Sensitivity analysis demonstrated that the cost savings observed were robust to changes in both clinical and economic parameters.
Conclusion: From a UK hospital perspective, Asacol 4.8 g/day is a cost effective option for the management of moderately active UC. This result provides an economic argument for clinicians to adopt this treatment strategy in the given patient population.
303 INFLIXIMAB IS EFFECTIVE AS RESCUE THERAPY FOR ACUTE SEVERE ULCERATIVE COLITIS: THE INITIAL EDINBURGH EXPERIENCE
C. W. Lees, A. G. Shand, I. D. Penman, I. D. Arnott, J. Satsangi.Gastrointestinal Unit, Western General Hospital, Edinburgh, UK
Introduction: As many as 40% of patients with acute severe ulcerative colitis (UC) will fail to respond to medical therapy. Treatment of these patients has been limited to surgery or second-line medical therapy (cyclosporine). Doubts remain about the efficacy of cyclosporine and concerns over its toxicity.1 Infliximab therapy is well established for Crohn’s disease, but its role in UC remains contentious.2 Most recently, Jarnerot et al demonstrated in a randomised controlled trial that infliximab as “rescue” therapy for severe UC was effective with emergency colectomy rates of 29% versus 67% for placebo (p = 0.017, NNT<3).3 For the first time, this trial provided evidence to support the clinical use of infliximab as rescue therapy for UC.
Methods: Data were retrospectively collected from all patients treated with infliximab for acute severe UC requiring hospitalisation for intensive medical therapy.
Results: Nine patients (6 male, 3 female, mean age 41) treated with infliximab for acute severe UC were identified. They were characterised by either lack of response to initial intravenous steroid therapy (6/9) or by deterioration following conversion from iv to oral steroids (3/9). Infliximab (5 mg/kg) was given an average of 7.8 days (range 4–16) after admission. 6/9 (67%) acutely treated patients demonstrated a good clinical response to infliximab within 48 hours, were commenced on azathioprine/6-MP therapy whilst in hospital and discharged on reducing courses of oral steroids. The median duration from infliximab to discharge was 6.5 days. All avoided colectomy to the most recent point of follow up (median 108 days, range 59–178). One patient developed uncomplicated herpes zoster and another asymptomatic transaminitis following infliximab therapy. The other three patients (33%) underwent emergency colectomy (median 5 days post-treatment). Baseline clinical data (stool frequency, CRP, albumin, calprotectin) did not predict response. Additional follow up and steroid withdrawal data will be presented.
Conclusions: These data provide further evidence that infliximab may successfully rescue acute severe UC. The treatment can function as a bridge to long term immune-suppression and immediate colectomy can be avoided.
1
2
3
304 INFLIXIMAB IN CROHN’S DISEASE: A PRAGMATIC APPROACH?
D. Kevans, D. Keegan, H. Mulcahy, D. P. O’Donoghue.Centre for Colorectal Disease, St Vincent’s University Hospital, Dublin 4, Ireland
Background and Aims: Infliximab is recognised as an effective therapy in unresponsive luminal and fistulating Crohn’s disease. Controlled trials point to the superiority of regular (scheduled) therapy as compared to episodic (“on demand”) Infliximab. However, only one third of patients in these studies were receiving concomitant immunosuppressive agents. The primary aim of this study was to assess the need for scheduled infliximab therapy in a setting where episodic therapy is the only initial treatment on offer and where immunomodulatory agents are widely used. A secondary aim was to assess what factors, if any, are associated with a favourable long term response.
Methods: Retrospective chart review was performed along with an analysis of a prospectively maintained database of inflammatory bowel disease patients. Ninety three patients with Crohn’s disease receiving infliximab were identified. Data collected included disease site and duration, surgical and smoking history, initial response rates, duration of response maintenance, and concomitant medications. All infusions were at a dose of 5 mgs/kg/body weight. Patients with luminal Crohn’s were given a single infusion which was only repeated if a response was elicited. Fistulous disease was treated with three infusions at 0, 2, and 6 weeks.
Results: Fifty six of 72 patients (78%) with luminal disease and 11 of 18 (52%) with fistulous disease achieved an initial response. Ten of 67 responders have required conversion to a scheduled infliximab regime. Eighteen patients remain free of symptoms more than 12 months following induction of remission, only one of whom is on low dose steroids. The group without small bowel disease (n = 48) had better response rates than those with small bowel disease (n = 40) 82% versus 68% and were more likely to maintain response over time (p = 0.01). Patients >35 years of age at time of treatment also had significantly better response and remission rates (p = 0.02). Smoking status did not affect initial response rates or likelihood of relapse. Nine of 36 patients in the episodic group have required resection surgery as has one of the 10 in the maintenance group. One elderly patient died of pulmonary disease six weeks after a successful single infusion of Infliximab. Postmortem showed adult respiratory distess syndrome. Three patients on episodic therapy developed allergic reactions.
Conclusions: Many patients with Crohn’s disease can be treated successfully with an episodic infliximab regime. Older patients and those with large bowel and perianal disease had significantly better response and remission rates.
305 PREOPERATIVE STEROID USE IN PATIENTS WITH INFLAMMATORY BOWEL DISEASE AND RISK OF POSTOPERATIVE COMPLICATIONS: META-ANALYSIS OF OBSERVATIONAL STUDIES
V. Subramanian, S. Saxena1, J. Y. Kang, R. C. G. Pollok.Department of Gastroenterology, Cellular and Molecular Medicine, St George’s University of London and 1Division of Epidemiology, Public Health and Primary Care, Medicine Imperial College, London, UK
Introduction: Patients with inflammatory bowel disease (IBD) are frequently treated with steroids. Almost a third of them will require surgery within a year of treatment with steroids. Studies examining postoperative complication risk associated with use of steroids in patients with IBD have yielded conflicting results. The purpose of this meta-analysis was to estimate the risk of postoperative infectious complications following abdominal surgery in patients with IBD on steroids at the time of surgery.
Methods: We searched electronic databases Pubmed, EMBASE, CINAHL, Ovid, Zetoc, and Ingenta, and hand searched citations from the reference lists in all the articles identified. Studies were included if patients had been on steroids in the month preceding surgery, compared with a control group. Studies that evaluated infectious postoperative complications in the two groups with duration of postoperative follow up of a maximum of 30 days or the hospitalisation period were included in the analysis. Data for calculation of odds ratios (OR) had to be provided or could be calculated from the tables or figures for the study to be included. We used the random effects model to calculate pooled odds ratio and 95% confidence intervals.
Results: All six studies that met the inclusion criteria were observational studies. Pooled analysis showed an increased risk of infectious postoperative complications among patients on steroids (OR 1.60, 95% CI 1.17 to 2.20).
Conclusions: This is the first meta-analysis on risk of postoperative infectious complication in patients with IBD taking steroids. Our data indicate that there is an increased risk of infectious complications following the preoperative use of steroids. This is consistent with data on preoperative steroid use and risk of postoperative complications in other general medical patients.
306 ADVERSE EFFECTS AND RELAPSE RATE IN PATIENTS WITH INFLAMMATORY BOWEL DISEASE TAKING AZATHIOPRINE VERSUS 5-ASA AND AZATHIOPRINE
J. A. Shah, C. M. Edwards, C. S. Probert.Bristol Royal Infirmary, Torbay Hospital, UK
Introduction: An interaction between AZA and 5-ASA may exist, but the mechanism is unclear. There are limited data looking on the clinical impact of this interaction.
Aims: To assess the effect of 5-ASA treatment in conjunction with AZA on adverse events (AEs) and relapse rate in IBD.
Method: A retrospective study of 223 patients taking AZA for IBD was performed. 95 patients received AZA alone (group I) and 104 received combination of 5-ASA and AZA (group II). In 24 patients it was not known whether AZA was given alone or with 5-ASA (group III). Data were collected on AE while taking AZA, its dose and the TPMT level. In 114 patients, rate of relapse of IBD was compared in groups I and II. Relapse was defined as symptoms requiring increased medical therapy or surgery while on >3 months of AZA. Patients in whom AZA was withdrawn in <3 months due to AEs were recorded in both groups.
Results: Total frequency of AE was 39% (88/223). AE were more common in group II (48%, 50/104), than in group I (30%, 29/95) (p = 0.05). AEs occurred in 37% (9/24) of group III. In group I patients with AE, TPMT was normal in 18/20 in whom it was measured. In group II, TPMT was normal in 23/24 with AE. Low dose AZA (<2 mg/kg) was taken in 19/31(61%) of group 1 and 32/50 (64%) of group II. Normal TPMT level and taking low dose of AZA did not reduce AE. Relapse rate was higher in group II (29/73, 43%) than in group I (12/41, 29%) (p = 0.02). Patients in whom AZA was discontinued in <3 months due to AEs were more common in group II (33%), cf. Group I (12%). Patients taking AZA and 5-ASA were more likely to suffer relapse or discontinue AZA (due to AEs), than patients who took AZA alone (p = 0.001)
Conclusion: Adverse effects appeared more common in those taking combination treatment. These AE were noted despite patients being on low dose of AZA and with normal TPMT levels. The incidence of relapse was significantly higher in patients taking AZA + 5-ASA. In light of chemopreventive effects of 5-ASA, we would not recommend the combination is not prescribed, rather that lower dose of 5-ASA may be preferable and better tolerated in patient taking AZA.
307 ACCELERATED INFLIXIMAB INFUSIONS ARE SAFE AND WELL TOLERATED IN THE TREATMENT OF CROHN’S DISEASE
A. Fairclough4,3, P. Emery4,3, R. V. Heatley2, S. M. Everett1,3, D. M. Chalmers1,3, A. T. Axon1,3, P. J. Hamlin1,3.Department of Gastroenterology1 and Rheumatology4 St James’s Hospital2, and Leeds General Infirmary3, UK
Aims: To assess whether shortened infliximab infusion times are safe and well tolerated in the treatment of Crohn’s disease.
Background: The manufacturer’s instructions recommend that infliximab is administered as a two hour infusion with obs for two hours post infusion. A previous retrospective audit at the LGI of 352 infliximab infusions in 62 patients (average 5.7 infusions/patient) revealed a total of five infusion reactions. Reduced infusion times after 4th dose is standard for RA patients in the Leeds IMID centre (Buch et al. 2004).
Methods: The Leeds IMID centre has been established to provide biological therapies to patients with IBD, RA, psoriatic arthritis, ankylosing spondylitis, and psoriasis. A prospective audit of accelerated infliximab infusion in patients with Crohn’s disease was performed. The infusions were given over the standard two hours then reduced to one hour or 30 minutes as follows:
Results: Between May 2003–Oct 2005 56 patients were treated according to the above regimen (17 male, 39 female; age range 17–84). 38 patients were taking azathioprine or 6MP, 11 methotrexate, one mycophenolate, and six received 200 mg hydrocortisone pre-infusion. Of a total of 116 infusions 58 were completed over one hour and 10 over 30 minutes. There were four infusion reactions (3.4% of total infusions: three patients with two hour infusions, one in one hour infusion, none in 30 minute infusions). No patient required cessation of IFX therapy.
Conclusion: Accelerating IFX infusions according to protocol is safe and well tolerated in the treatment of Crohn’s disease. This allows more patients to be treated per session and improves patient convenience.
Abstract 307
308 SAFETY OF MODIFIED RELEASE ORAL MESALAZINE 4.8 G/DAY (800 MG TABLET) COMPARED TO 2.4 G/DAY (400 MG TABLET) FOR TREATMENT OF ACTIVE ULCERATIVE COLITIS: ANALYSIS OF COMBINED DATA from two randomised, double blind, controlled trials
S. B. Hanauer1, E. V. Loftus2, D. G. Binion3, G. L. Gordon4, N. Smith-Hall5, L. Law (introduced by S. Ghosh)5.1Section of Gastroenterology and Nutrition, University of Chicago, Chicago; 2Department of Gastroenterology, Mayo Clinic, Rochester; 3Gastroenterology and Hepatology, Medical College of Wisconsin, Milwaukee; 4Gastroenterology and Hepatology, Center for Digestive and Liver Diseases, Inc, Mexico; 5Research and Development, Procter and Gamble Pharmaceuticals, Cincinnati, USA
Introduction: To evaluate the safety of an investigational 800 mg mesalazine dosed at 4.8 g/day, compared to that of a currently marketed US 400 mg mesalazine tablet dosed at 2.4 g/day for the treatment of mildly to moderately active ulcerative colitis.
Aims and Methods: Two randomised, double blind, six week, parallel group studies (ASCEND I & II) were conducted to compare the safety and efficacy of a new 800 mg tablet formulation of modified-release mesalazine (P&G Pharmaceuticals), dosed at 4.8 g/day, to that of a marketed 400 mg tablet (Asacol, USA), dosed at 2.4 g/day, in patients with newly or previously diagnosed mildly to moderately active ulcerative colitis. Safety assessments included adverse events (AEs), physical examinations, vital signs, and clinical laboratory evaluations.
Results: In both treatment groups, the most commonly reported AEs (headache; flu syndrome; respiratory infections; and digestive symptoms) were similar to the US marketed 400 mg tablet. The majority of AEs were assessed by investigators as mild or moderate in severity. The AE experience was similar across subgroups examined, including age, sex, race, and baseline disease state. Serious AEs were reported in 9 patients (two in the 4.8 g/day group and seven in the 2.4 g/day group), and primarily involved the digestive system (worsening ulcerative colitis signs and symptoms, nausea, vomiting, epigastric pain, cholecystitis, and pancreatitis). Non-gastrointestinal serious AEs assessed as related to mesalazine therapy were nephritis (one patient in the 2.4 g/d group) and pericarditis (one patients in the 4.8 g group).
Conclusion: The safety profile of mesalazine 4.8 g/day, administered as an 800 mg tablet, is comparable to the post-marketing and clinical experience of the 400 mg marketed tablet at 2.4 g/d.
309 MESALAZINE STARTING DOSE AND TIME TO FLARE AMONG ULCERATIVE COLITIS AND CROHN’S DISEASE PATIENTS
W. A. Blumentals, R. L. Sheer, M. Steinbuch, B. R. Yacyshyn (introduced by S. Ghosh).Procter & Gamble Pharmaceuticals, Mason, OH, USA
Introduction and Aim: It has been hypothesised that newly diagnosed inflammatory bowel disease (IBD) patients who start on a higher dose of mesalazine therapy may prolong the time to occurrence of a flare compared to patients who begin with a lower dose. The aim of this study was to quantify the time to flare among IBD patients receiving at or above the median average daily starting dose versus below the median average daily starting dose.
Methods: A retrospective cohort study was conducted using data from Saskatchewan Health (Canada). Patients with a 400 mg strength/tablet mesalazine prescription between 1 January 1990 and 31 December 2002 (index date) were followed until the time of a flare. A flare was defined as an interval of ⩾6 months until a subsequent 5-aminosalicylate (5-ASA) prescription at the same dose or a 5-ASA prescription at a higher dose; or a glucocorticosteroid or immunomodulator prescription ⩾4 months after the index date. We identified ulcerative colitis (UC) and Crohn’s disease (CD) patients with a diagnosis ±60 days from the index date. Mesalazine patients with a UC or CD diagnosis >60 days to ⩽12 months before the index date and patients with a record of 5-ASA or immunomodulator therapy in the 12 month period prior to the index date were excluded from the study. The median average daily starting dose over the first 100 days following the index date was computed to differentiate between higher starting dose and lower starting dose.
Results: 896 UC and CD patients with a 400 mg strength/tablet mesalazine prescription were identified (566 patients were UC and 330 were CD). The median time to flare after the index date was 346 days among patients with UC (n = 310) and an average daily starting dose of ⩾1.6 g/day, compared to a median time to flare of 269 days for UC patients (n = 256) with an average daily dose of <1.6 g/day (p = 0.01). CD patients (n = 165) with an average daily starting dose of ⩾1.35 g/day had a median time to flare of 286 days versus 260 days for CD patients (n = 165) averaging <1.35 g/day (p = 0.02).
Conclusions: The results suggest that patients with UC or CD starting mesalazine therapy and receiving a higher average daily starting dose prolong their time to flare occurrence compared to patients with a lower average daily starting dose.
310 HIGH DOSE MESALAZINE 4.8 G/DAY (800 MG TABLET) COMPARED TO MESALAZINE 2.4 G/DAY (400 MG TABLET) DEMONSTRATES INCREASED EFFICACY IRRESPECTIVE OF DISEASE LOCATION
W. Sandborn1, S. Hanauer2, R. Eusebio (introduced by S. Ghosh)3.1Mayo Clinic, Rochester, MN, US; 2Division of Gastro & Hep, University of Chicago, IL, USA; 3Procter and Gamble Pharmaceuticals Inc, Cincinnati, OH, USA
Background: Extent of disease is an important aspect of ulcerative colitis. The purpose of this analysis was to investigate the consistency of the treatment effect across various disease extents. Disease extents were recorded as proctitis, proctosigmoiditis, left sided colitis, and pancolitis.
Method: Two prospective, double blind, randomised controlled trials (ASCEND I and II) were pooled and analysed. Patients with mildly to moderately active ulcerative colitis (UC) were randomised to receive either mesalazine 4.8 g/day with an 800 mg tablet or mesalazine 2.4 g/day with a 400 mg tablet for six weeks. The primary endpoint was the % of patients with moderately active UC who achieved treatment success, defined as complete or partial response based on clinical, endoscopic, and physician assessments. The Cochran Mantel-Haenszel test was calculated after stratifying for trial and baseline disease extent and the Breslow-Day test for homogeneity was used to investigate if the treatment effect was different across the varying disease extents.
Results: Of the 448 patients with active moderate UC at baseline, 152 (34%) had left sided colitis, 129 (29%) had proctosigmoiditis, 100 (22%) had pancolitis, and 67 (15%) had proctitis. There were no statistically significant differences for any baseline characteristics of extent of disease between the two treatment groups. Overall treatment success at week 6 observed a statistically significant efficacy benefit for 4.8 g/d regardless of disease extent (p = 0.003). There was insufficient evidence to suggest that the treatment effect was different across each of the disease extent areas (p = 0.965). Patients with left sided disease, (including proctitis, proctosigmoiditis and left sided colitis) demonstrated a significant treatment success in the 4.8 g/d (72%) group versus the 2.4 g/d (59%) p = 0.0132.
Conclusion: The treatment differences observed between the 2.4 g/d and the 4.8 g/d groups were consistent across all extents of disease indicating that 4.8 g/d dosing provides an increased efficacy benefit regardless of disease extent. Moderately active UC patients, with left sided disease, demonstrate an increased treatment benefit taking mesalazine 4.8 g/day compared to 2.4 g/day.
311 THE EFFECTIVENESS OF CONTINUING THE INDUCTION DOSE OF ASACOL INTO THE MAINTENANCE PHASE: RESULTS FROM THE COMMUNITY SETTING
W. Sandborn1, B. Sands2, S. Hanauer3, R. Bloomfeld (introduced by S. Ghosh)4.1Mayo Clinic, Rochester, MN, US; 2Massachusetts General Hospital, Boston, MA, US; 3Division of Gastro & Hep, University of Chicago, IL, USA; 4Wake Forest University School of Medicine, Winston-Salem, NC, USA
Aim: There is anecdotal evidence that maintaining the induction dose may be better than dose reduction to prevent relapse. This study used a naturalistic, retrospective design to compare the outcomes of community based ulcerative colitis (UC) patients maintained on the dose used to induce remission with those whose maintenance dose was reduced.
Methods: The medical records from 411 UC patients from 39 geographically dispersed, community gastroenterology practices, within the United States, who had a disease flare between 1999 and 2003 successfully treated with US Asacol (Procter and Gamble Pharmaceuticals, Inc) without requiring steroids were reviewed. The review included the single flare of interest and the subsequent maintenance period of 12 months. Outcome measures examined were maintenance of remission post-induction, and % rated “normal” on the physician global assessment of symptom severity (PGA) at final data capture. The primary explanatory variable was the relation between maintenance (M) and induction (I) dose, coded as M = I versus M<I. Other covariates examined were:
-
Final induction dose: grouped on g/day, ⩽2.4, 3.2–4.0, ⩾4.8
-
Extent of disease: proctitis+proctosigmoiditis v left-sided v extensive
-
Severity of disease: mild v moderate+severe
-
Prior treatment history (PH): 1st flare v subsequent flare without immediately prior maintenance medication v subsequent flare while on maintenance medication.
Results: Of the 411 patients, 178 (43%) patients had mild starting PGA and 233 (57%) had moderate/severe starting PGA. No variables were significantly (p<0.05) predictive of maintenance of remission. In logistic regression analysis, starting PGA and M = I vs M<I were significantly associated with final PGA. M = I patients were twice as likely to achieve “normal” final PGA compared to M<I patients (p<0.01, OR = 2.21, 95% CI 1.36 to 3.58).
Conclusions: Maintaining the same dose of Asacol used to induce remission significantly increased the likelihood of UC patients receiving a physician’s global assessment of “normal” at one year post-induction.
312 UNDER APPROPRIATE CONDITIONS LYMPHOCYTE APOPTOSIS IS CAUSED NOT ONLY BY INFLIXIMAB AND ADALIMUMAB BUT ALSO BY ETANERCEPT IN VITRO
R. Chaudhary, M. Butler, R. Playford, S. Ghosh.Gastroenterology Section, Division of Medicine, Imperial College, London, UK
Background: Apoptosis is considered an important mechanism of action of anti-TNF therapy in Crohn’s disease. Infliximab, but not etanercept, has been reported to cause apoptosis in stimulated peripheral blood and lamina propria T lymphocytes in healthy controls and Crohn’s disease patients (as detected by annexin-V). We report on the importance of the timing of anti-TNF drug addition on the induction of stimulated peripheral CD4 T lymphocyte apoptosis.
Methods: Peripheral CD4 T lymphocytes were isolated from healthy subjects (n = 4) and stimulated with antiCD3 and antiCD28 antibody. Medium with or without drug was added either simultaneously or delayed for 72 hours. Control antibody was used as a negative control and cisplatin as a positive control. Apoptosis was detected after seven days stimulation using annexin V and topro-3 by flow cytometry. Three anti-TNF agents—infliximab, adalimumab, and etanercept—were used at 10 μg/ml.
Results: Following anti-TNF drug addition to lymphocytes stimulated for 72 hours the apoptosis rates compared to background apoptosis (that is apoptosis of stimulated cells with medium alone added) were 91%, 89%, and 88% for infliximab, adalimumab, and etanercept respectively. With simultaneous stimulation and anti-TNF drug addition lymphocyte apoptosis compared to background was 240%, 212%, and 172% with infliximab, adalimumab, and etanercept respectively. This increase in apoptosis following synchronous drug addition and stimulation was significant for all three anti-TNF agents (paired t test p<0.05).
Conclusion: We detected an increase in lymphocyte apoptosis above background when anti-TNF drug was added concurrently at the time of stimulation but not when the addition of the agent was delayed for 72 hours post stimulation. In our in vitro model anti-TNF induced apoptosis is dependant on the degree of lymphocyte stimulation. Under these conditions not only infliximab and adalimumab but also etanercept causes lymphocyte apoptosis.
313 5Q31 HAPLOTYPE AND RELAPSE AFTER SMALL BOWEL RESECTION
C. Todhunter, J. Barbour, K. Mohuiddin, M. Price, C. Onnie, C. G. Mathew, J. C. Mansfield.University of Newcastle upon Tyne, Guy’s, King’s and St Thomas’ School of Medicine, London and Royal Victoria Infirmary, Newcastle upon Tyne, Uk
Introduction: Crohn’s disease is a relapsing remitting disease. The majority of patients with terminal ileal Crohn’s disease will require surgery and often this will need to be repeated. There are few reliable predictors of outcome after surgery. The c allele of the 5q31 haplotype has been found to be associated with Crohn’s disease. We therefore investigated whether carriage of this allele was associated with more rapid relapse after terminal ileal resection in a cohort of well characterised patients with Crohn’s disease.
Method: Patients who had had ileal resection for Crohn’s disease were genotyped for the c and g allele of the 5q31 haplotype. Results are expressed as wild type gg genotype, heterozygote gc and homozygote cc. Age at first operation and postoperative smoking status were obtained from patient records and direct interview. Duration of follow up if no surgical recurrence and time to second operation was analysed with respect to 5q31 genotype using Kaplan-Meier survival curves.
Results: 172 (111 female, 82 smokers) patients were genotyped for the 5q31 haplotype; 45 were wild-type, 87 heterozygote, and 40 homozygote. There was no difference in survival to second operation between 5q31 genotypes. The detrimental effect of smoking on survival to second operation was maintained between 5q31 genotypes, p = 0.017. There was no difference in age at first operation or number of resections and 5q31 genotype.
Conclusion: We confirm the association between smoking and shorter time to second small bowel resection. Carriage of the disease associated 5q31 allele is not associated with more rapid or more frequent relapse after small bowel surgery in this cohort of Crohn’s disease patients.
314 SERUM PROTEIN SIGNATURES DETERMINED BY MASS SPECTROMETRY (SELDI-TOF) ACCURATELY IDENTIFIES PATIENTS WITH INFLAMMATORY BOWEL DISEASE
V. Subramanian1, D. Subramanian2, S. Krishna1, D. Agranoff3, R. C. Pollok1.1Cellular and Molecular Medicine, St George’s University London; 2Department of Computer Science, Rice University, Houston; 3Division of Investigative Science, Medicine, Imperial College, UK
Introduction: Inflammatory bowel disease (IBD) is an idiopathic chronic disease of the gastrointestinal tract with many debilitating sequelae some of which be life threatening. Diagnosis of IBD often depends on invasive tests. Non invasive serological testing such as ASCA and p-ANCA are insufficiently specific or sensitive for routine diagnostic use. We aimed to develop a novel diagnostic approaches based on differences in protein signatures in sera obtained from individuals with IBD and controls using surface enhanced laser desorption and ionisation time of flight (SELDI-ToF) mass spectrometry (MS).
Methods: We studied protein signatures from 59 patients with IBD and 64 controls (normal and patients with other inflammatory pathology). Protein signatures were obtained using a CM10 chip (weak cation exchange chip), and analysed with SELDI-ToF MS. Preliminary analysis was performed using ‘p’ value determination of integrated peaks. Statistical and neural network analysis was performed using support vector machine techniques using radial basis function kernels. Significant peaks used for discrimination were selected using both Fisher’s and recursive feature elimination (RFE) techniques.
Results: Comparing IBD and controls using support vector machine SVM) analysis with a radial basis function kernel (width 5), limited to two peaks selected by RFE, we obtained an accuracy of 97%, sensitivity of 95%, and specificity of 98%. The same analysis for two peaks chosen by Fisher techniques, resulted in an accuracy of 98%, sensitivity of 98% and specificity of 98%. The peaks selected by both techniques were also significantly discriminative when used in individual peak analysis.
Conclusions: Using protein signatures of patients with IBD and controls we have developed a model of classification which has high accuracy and is more informative than currently available serological tests. Cross validation and characterisation of discriminant peaks is currently underway.
315 ROLE OF INFLIXIMAB IN DOWNREGULATING MATRIX METALLOPROTEINASE-3 IN CROHN’S DISEASE
A. Di Sabatino1,2,3, U. Saarialho-Kere4, L. Picariello5, M. Buckley1, J. N. Gordon1, R. Morera3, P. Cazzola3, F. Tonelli5, G. R. Corazza3, T. T. MacDonald1,2, S. L. F. Pender1.*Division of Infection, Inflammation and Repair, University of Southampton, UK; 2Centre for Infectious Disease, ICMS, Barts and the London School of Medicine and Dentistry, UK; 3First Department of Medicine, IRCCS Policlinico S. Matteo, University of Pavia, Italy; 4Department of Clinical Physiopathology, University of Florence, Italy; 5Department of Dermatology, Helsinki University Central Hospital, Finland
Background and Aims: Excessive matrix metalloproteinase (MMP) induced degradation of mucosal matrix is the final step in the cascade of events leading to tissue injury in inflammatory bowel disease. TNF-α blockade prevents matrix degradation concomitant with inhibition of MMP-3 production in an ex vivo model of gut T cell mediated matrix degradation. On this basis, we investigated the effect of infliximab on the mucosal expression of MMP-3 in Crohn’s disease (CD) patients.
Methods: Six steroid refractory CD patients received 3 consecutive infusions of infliximab administered at week 0, 2, and 6 at a dose of 5 mg/kg. Colonoscopy and ileoscopy were performed immediately before the start of the therapy and 10 weeks later, with collection of multiple biopsies. MMP-3 mucosal transcript expression was studied by in situ hybridisation. Fibroblasts isolated from 6 active CD patients and five controls were stimulated in vitro with infliximab, etanercept or TNF-α. After 24 hours culture, MMP-3 expression was determined by western blotting.
Results: All six CD patients responded to treatment, four with a complete response, and two with a partial response. MMP-3 mucosal expression was reduced after 10 week treatment, with a higher decrease in patients who had a complete response. While TNF-α increased MMP-3 production, infliximab inhibited spontaneous MMP-3 production. Etanercept was more effective than infliximab in downregulating MMP-3 production.
Conclusions: These findings suggest that one of the way in which anti-TNF-α strategies heal mucosa in CD patients is by directly inhibiting MMP-3 production by fibroblasts.
316 ASSOCIATION OF CLINICAL RESPONSE WITH ELEVATED PLASMA INTERLEUKIN-1 RECEPTOR ANTAGONIST DURING SELECTIVE GRANULOCYTAPHERESIS IN PATIENTS WITH REFRACTORY ULCERATIVE COLITIS
K. Sakimura1, S. Miura2, S. Ota3, Y. Takeda4, A. Saniabadi (introduced by B. Danesh)4.1Internal Medicine, Saitama Red Cross Hospital; 2Second Department of Internal Medicine, National Defense Medical College; 3Gastroenterology, Saitama Medical School; 4JIMRO, Japan
Background: In inflammatory bowel disease (IBD), granulocytes and monocytes/macrophages (GM) are elevated with activation behaviour, prolonged survival, and are found in vast numbers within the intestinal mucosa. They are potential sources of cytokines, other tissue damaging substances and therefore, are suspected to contribute to IBD. The Adacolumn can deplete activated GM, up to 65% of GM and a small fraction of lymphocytes adhere to the column leucocytapheresis carriers. This is followed by an increase in the naïve (CD10 negative) fraction of neutrophils in the peripheral blood. This study was to investigate the effect of Adacolumn on plasma concentration of interleukin-1 receptor antagonist (IL-1ra), a potent anti-inflammatory cytokine.
Methods: Twenty six patients with chronic or repeated relapses of UC were included. Patients received one Adacolumn session/week for five consecutive weeks. Clinical response was defined as Δclinical activity index (ΔCAI = CAI at entry – CAI at post ⩾4), while remission was defined as CAI⩽4. During the procedure, blood was collected for measuring IL-1 family members (IL-1α, IL-1β, and IL-1ra).
Results: Twenty one of 26 patients responded (19 achieved remission). Plasma from responder patients, but not non-responders showed a significant (p<0.01) increase in IL-1ra in the Adacolumn outflow (blood return to patients). Further, incubation of blood with the Adacolumn carriers in in vitro settings showed that the release of IL-1ra from GM was adhesion dependent. Neither at the column outflow nor during the incubation of blood with the carriers, TNF-α or IL-1β increased.
Conclusions: The high level of clinical response in patients who had failed drug therapy reflects that GM might have a major role in the perpetuation of UC. Release of IL-1ra might be another mechanism by which Adacolumn can alter cytokine profiles in the circulation.
Colorectal posters
317 DOES UNCOMPLICATED COLONIC DIVERTICULAR DISEASE CAUSE SYMPTOMS?
A. Poullis1, A. Barnabus1, H. Matthews1, L. T. Tan2, G. Lim2, J. Y. Kang1.1Departments of Gastroenterology, St George’s Hospital, London; 2and Epsom General Hospital, Surrey. UK
Background and Aims: Colonic diverticular disease (DD) is often found among older individuals with colonic symptoms but it is unclear whether DD causes symptoms in the absence of acute diverticulitis.
Methods: Subjects aged over 50 referred for elective colonoscopy or barium enema completed a locally validated questionnaire based on the Rome II criteria, prior to the investigation.
Results: Of 567 subjects undergoing colonoscopy or barium enema, 118 had DD without other structural disease while 224 had normal colons. Indications for investigation were similar in the two groups and there was no sex difference. Mean age was 70.3 years in those with DD and 62.1 in those with normal colons (p<0.001). There was no significant difference between the two groups in the frequency of the following symptoms: abdominal pain, <3 bowel actions per week, >3 bowel actions per day, hard or loose stools, straining, urgency, passage of mucus per rectum, abdominal fullness, the need for manual evacuation, rectal pain. However, more patients with DD found it difficult to pass a stool compared those with normal examinations (64% v 30%, p = 0.002). In contrast, faecal incontinence (16% v 22%, p = 0.05) and sensation of incomplete evacuation (39% v 66%, p = 0.03) were less common in those with DD.
Conclusion: Among patients who underwent colonic investigations but were not found to have structural disease, the frequency of abdominal pain, diarrhoea and constipation, and most other colonic symptoms, except for difficulty in passing a stool, was no different among those with DD compare with those with normal colons. In the absence of acute diverticulitis, DD is probably not a major cause of abdominal symptoms.
318 DARK BLOOD ON THE RECTAL MUCOSA: IS IT SINISTER?
K. Flood, D. ElFadl, M. Rogers (introduced by G. S. Duthie).Pinderfields Hospital, Aberford Road, Wakefield WF1 4DG, UK
Background: Assessment of patients by rigid sigmoidoscopy occasionally reveals dark (transported) blood on the rectal mucosa but not its origin. We felt this was sinister. There is however, no evidence to support or refute this view.
Aim: To assess the significance of finding dark red blood on the rectal mucosa.
Method: All patients in whom dark blood was seen on the rectal mucosa in the outpatient clinic of one surgeon underwent colonoscopy.
Results: Thirty six patients, (16 M, 20F), mean age 61 years (range 31–87) had dark blood seen on the rectal mucosa with no obvious source at rigid sigmoidoscopy. In 12 patients (33%) colonoscopy was normal. Five patients (15%) had colonic cancer and 15 (45%) adenomas. Four patients had colitis; (IBD 2, non-IBD 2). The adenomas were large, 5–25 mm (median 15, IQR 8–15); 12 of 15 adenomas were 10 mm or larger; (high risk adenomas by the BSG criteria for surveillance). In all cases (20 of 20) the cancer or largest polyp was distal to the splenic flexure, (judged on colonoscopy). In 17 of 20 cases the polyp or cancer lay in the sigmoid colon. Five patients had neoplasia at more than one site. The only patient who had iron deficiency anaemia and dark blood on the mucosa had a sigmoid carcinoma.
Discussion: Dark blood on the mucosa is a significant finding. The underlying pathology is usually a high risk adenoma but 15% of patients have colonic cancer. The cancer or largest adenoma is usually found distal to the splenic flexure but 20% of cases will have synchronous proximal neoplasia.
Conclusion: Patients in whom rigid sigmoidoscopy reveals dark blood on the rectal mucosa require prompt, complete colonoscopy with polypectomy as required.
319 BOWEL HABIT CHANGES IN PATIENTS WITH DIVERTICULAR DISEASE AND THE EFFECT OF SOCIAL ISOLATION AND PSYCHIATRIC MORBIDITY
D. J. Humes, J. Simpson, K. Neal, J. H. Scholefield, R. C. Spiller.Wolfson Digestive Disease Centre, Floor C, South Block, University Hospital Nottingham NG7 2UH, UK
Introduction: Diverticulosis affects two thirds of the population over the age of 65. It is estimated that between 10–20% develop symptoms although the mechanism underlying these symptoms is unknown. We previously reported an increased incidence of recurrent abdominal pain in patients with diverticulosis following an episode of acute diverticulitis. We now report the effect of psychosocial factors on symptoms in this group.
Methods: A questionnaire regarding episodes of abdominal pain, normal bowel habit (IBS symptoms, Rome 1 criteria) and markers of social and psychiatric morbidity was sent to 379 patients with radiologically proven diverticula.
Results: Median (range). 68.9% completed questionnaires, 55% female, age 69 years (36–91). Only 59 (22.6%) patients were asymptomatic. We identified two groups of patients with regard to reported bowel habit changes. Group 1: 142/261 (54%) patients reported altered bowel habit, reporting loose watery stools 51/142 (36%), hard lumpy stools 38/142 (27%) or both 53/142 (37%). Group 2: 119/261 (46%) patients reported no abnormalities of bowel habit. Patients in group 1 were more likely to experience recurrent short-lived abdominal pain (<24 hours duration) than patients in group 2 (χ2 11.08, 73 v 21, p<0.001). Patients in group 1 were more likely to be socially isolated (widowed, single or divorced) than patients in group 2 (χ2 7.4, 66 v 23, p<0.01). Patients in group 1 were also more likely to use a psychiatric medication than patients in group 2 (Fisher’s exact test, 16 v 2, p<0.02).
Conclusion: Patients with diverticular disease report a high level of symptoms. Social isolation and psychiatric conditions may increase symptom reporting.
320 DO RADIO OPAQUE TRANSIT STUDIES PREDICT QUALITY OF LIFE IN PATIENTS WITH CHRONIC CONSTIPATION?
S. Cowlam1, D. Wooff2, I. Minty1, S. Green1, J. Varma1, Y. Yiannakou1.1University Hospital of North Durham, Durham, UK; 2Statistics & Mathematics Unit University of North Durham, UK
Introduction: Transit marker studies are commonly used to assess severity in chronic constipation but have not been validated for this purpose.
Aim: To determine whether results of transit studies correlate with QOL measurements obtained using validated QOL instruments in patients with chronic constipation.
Methods: 110 out of 163 consecutive patients referred to a dedicated constipation clinic at Durham completed evaluations of QOL and colonic transit. Patients met Rome II criteria for idiopathic constipation. Median age 40.5 years. 96% of patients were female. Median symptom duration; 10.5 years. The Gastrointestinal Quality of Life Index (GIQLI) and Patient Assessment of Constipation–Quality of Life (PAC-QOL) were completed by the patients. A high GIQOLI suggests better QOL. A high PAC-QOL suggests poorer QOL. Transit studies performed using a recognised protocol with Sitzmark markers (Konsyl), one capsule on three consecutive days, with an x ray on the 4th day. Segmental marker counts obtained and results expressed as TSM-out (number of markers passed at day four, ie 72–total remaining) and TSM-centre (the average marker position). The assessments were performed at the first consultation and represented the baseline state before intervention or therapy in clinic. Analysis using Pearson correlation coefficient.
Results: There was no correlation between transit study results and QOL assessments. Correlation coefficients: TSM-centre v GIQLI, −0.057; TSM-centre v PAC-QOL, −0.036; TSM-out v GIQLI, 0.034; TSM-out v PAC-QOL 0.092. There was good correlation between GIQLI and PAC-QOL, −0.562 (p<0.001). Correlations between other pairs were effectively not different to zero.
Conclusion: Transit study results in chronic constipation did not predict quality of life. We have previously shown that they do not correlate with symptoms either. It is therefore unlikely that they could be used to assess the severity of constipation. They may still have a use in management to confirm the diagnosis of constipation.
321 A RANDOMISED TRIAL OF ORAL BISACODYL COMPARED WITH SMALL OR LARGE VOLUME ENEMA BOWEL PREPARATION FOR ENDOSCOPY OF THE RECTOSIGMOID AND DESCENDING COLON
M. A. B. Fernando1, K. I. Deen2, R. Fernando2, M. H. J. Ariyaratne2.1University Surgical Unit, North Colombo Teaching Hospital; 2Department of Surgery, University of Kelaniya, Sri Lanka
Introduction: Although, during flexible sigmoidoscopy, it would suffice to evaluate only the anorectum and sigmoid colon, visualisation of the descending colon is an advantage and is possible in the majority. Therefore, it is essential to achieve cleansing of the entire left colon before this procedure.
Patients and Methods: After informed consent, 132 patients (60 male, 72 female; median age −41 years, range 17 to 65) were randomised to have either sodium docussate (5 ml) small volume enema (SVE, n = 45), phosphate (133 ml) large volume enema (LVE, n = 44), or bisacodyl tablets (BIS, n = 43) before flexible sigmoidoscopy for rectal bleeding, constipation, left iliac fossa pain, recurrent anal sepsis, and rectal prolapse. Bowel preparation was assessed as excellent, good, poor, or very poor based on a pictorial guide of endoscopic appearances. We also assessed the extent of colon that was evaluable and patients’ preference for bowel preparation. All patients were given a standardised diet one week before examination.
Results: For evaluation up to the sigmoid colon, LVE was superior to SVE or BIS (excellent or good preparation; LVE −38 (86%) v SVE −28 (62%), p = 0.009 and LVE v BIS−38 (86%) v 29 (67%), p = 0.03). Furthermore, descending colon evaluation was also facilitated best after LVE bowel preparation compared with SVE or BIS (excellent or good preparation ;LVE v SVE; 37(84%) v 18 (40%), p⩽0.001 and LVE v BIS; 37(84%) v 24 (56%) respectively, p = 0.003). Ninety six (73%) of 132 patients preferred oral preparation compared with 36 (27%) who preferred enemas (p<0.05).
Conclusion: A large volume enema is the preferred option of bowel preparation before flexible sigmoidoscopy. It enables evaluation of the entire left colon in a greater proportion of patients compared with small volume enemas or oral bisacodyl.
322 ANORECTAL PHYSIOLOGY IN MALES WITH FAECAL INCONTINENCE
M. Titi, A. L. McCallum, J. T. Jenkins, A. Uri, R. G. Molloy.Department of Surgical Gastroenterology, Gartnavel General Hospital, Glasgow, UK
Introduction: Faecal incontinence (FI) is a significant clinical problem. Historically, it has been considered a condition that mainly affects women with childbirth related trauma. However, some studies suggest that men have been found to be equally affected, particularly with advancing age. We aimed to prospectively assess male faecal incontinence in relation to potential aetiology, anorectal physiology, and diagnostic approach to the condition.
Methods: Fifty nine consecutive male patients referred to a coloproctology outpatient clinic with symptoms of faecal incontinence were prospectively recruited to the study. Symptom severity was assessed using the Wexnor Score. All patients followed a standard pathway of investigation, starting with anal manometry and rectal sensation studies followed by endo-anal ultrasound (EAUS). Patient comorbidities and previous anorectal surgical history were recorded.
Results: Median age at diagnosis was 60 years (IQR 46–71), median Wexner Score was 18 (IQR 4–20). Manometry showed normal sphincters function in 48/59 (81.4%). 12 patients had anal surgery and five had rectal surgery. No significant differences were noticed in sphincter’s function for patients who had surgery compared to those with no previous surgery (maximum resting pressure (MRP), 61 (IQR 45–81) v 67 (IQR 46–89)), (maximum squeeze pressure (MSP), 184 (IQR 142–270) v 184 (IQR 139–234)). This was also the case when patient co morbidities were compared in relation to sphincter function. However, age >60 years was significantly associated with reduced MRP (52 (IQR 42–76) v 77 (IQR 57–94); p = 0.007), but no other manometry results. EAUS revealed totally normal sphincters in 38/59 (64.4%). 16 patients had some degree of thinning of either one or both sphincters but without defects. Only 5/59 (8.5%) had sphincter defects and these were more common post surgery (2 external sphincter defects (1 post surgery), 3 internal sphincter defects (all post surgery)). All rectal surgery patients had abnormal rectal sensation (4 had low maximum tolerated rectal volume, 1 had loss of sensation).
Conclusion: Male incontinence is an existing problem that deserves more attention. It is infrequently attributed to sphincter dysfunction or defects even post surgery and other causes should be investigated.
323 COLORECTAL STENTING: A CANCER UNIT’S EXPERIENCE
R. Hussain, A. N. Hamlyn, N. C. Fisher, B. J. M. Jones.The Dudley Group of Hospitals NHS Trust: Russells Hall Hospital, Dudley, West Midlands DY1 2HQ, UK
Background: Colorectal stenting is increasingly used for interim and definitive management of obstructing colorectal tumours as highlighted in the 2004 NICE guidelines. We assessed the outcome following colorectal stenting at our Trust.
Methods: Retrospective case note review from September 2005 to 1997. The following details and outcomes were assessed: patient characteristics, symptomatic relief, discharge from hospital, emergency or elective surgical intervention and survival.
Results: Twenty–four patients underwent stenting (17M, 7F, median age 76 years (51–91). Boston Scientific enteric wall stents were used, and all were inserted by gastroenterologists under endoscopic and fluoroscopic guidance. Carcinomas were ano-rectal (1), rectal (5), rectosigmoid (9), sigmoid (7), descending colon (1), and transverse colon (1). Metastases were present in 16 patients (66%). All patients had subacute obstruction or acute obstruction. Two patients had stents as interim management prior to successful resection. In remaining patients, stent insertion was intended as definitive therapy (with or without chemotherapy). Two had early stent failure (<1 week) and required emergency surgery. All others had technically successful outcomes with no procedure related complications. Of these twenty patients 73% were discharged home. Eighteen patients are now deceased (median survival 50 days, range 6–349).
Conclusion: Most patients had a technically satisfactory outcome in this series. Our experience supports a role for colorectal stenting as an important therapeutic option in improving outcome and reducing morbidity in the management of advanced or metastatic colorectal cancer.
324 NEOADJUVANT THERAPY FOR ADVANCED RECTAL CANCER: RESULTS OF SHORT TERM FOLLOW UP
M. T. P. R. Perera1, S. R. E. Wijesuriya3, J. Hewavisenthi2, K. I. Deen3.1Senior Resident in Surgery, Professorial Surgical Unit–North Colombo Teaching Hospital, Ragama; 2Department of Pathology; 3Department of Surgery, Faculty of Medicine–University of Kelaniya, Ragama, Sri Lanka
Introduction: The outcome of advanced rectal cancer has improved with the introduction of neoadjuvant chemoradiotherapy. Our objective was to evaluate the short term outcome of patients who were treated with neoadjuvant therapy and total mesorectal excision (TME).
Method: Thirty five consecutive patients (male 22, female 13; median age 55 years (25–77)) diagnosed with locally advanced rectal carcinoma, were treated with protocol based long course chemoradiotherapy (radiation 4500cGy and 5-Fluorouracil) before they were subjected nerve sparing rectal excision with total mesorectal excision (TME). All patients were prospectively followed up between April 2000 and September 2005. Data sought were; duration of operation, operative blood loss, tumour stage prior to chemoradiation, histopathological evaluation of resection margin (R0–no resection margins involved, R1–at least one involved margin), tumour regression grade (TRG 1–4, 1 = complete response, 4 = poor or no response) and tumour recurrence. Statistical analysis was performed with χ2 test and Kaplan Meier method using SPSS.
Results: Thirty four patients were subjected to low anterior resection while one patient had abdominoperineal resection. Fifteen patients (43%) each had either stage II or III cancers, 5 (14%) had stage IV cancer. Lymph nodes were positive in 19 (54%). The mean operative time was 230 minutes (range 150–300), and mean blood loss was 900cc (range 300–2500). R0 margins were seen in 26 (74%); R1 in 9 (26%). Complete tumour response (TRG 1) was seen in 10 (28%). At median follow up of 14 months (range 1–67), local recurrence was seen in 6 (17%) patients. Mean duration to recurrent disease was 8 months (range 4–60). Positive resection margin (R1) and incomplete tumour regression (TRG 2–4) were adversely associated with local recurrence (p = 0.004 and p = 0.016 respectively). Estimated overall survival at 2 and 5 years were 51% and 46%, while disease free survival was 52% and 48% respectively.
Conclusion: Involvement of the resection margin by tumour and incomplete tumour regression may accurately predict recurrent disease in advanced rectal cancer. Factors that result in poor response to chemoradiotherapy should be evaluated further in controlled studies to improve the outcome.
325 RAMAN SPECTROSCOPIC MAPPING TO EVALUATE THE BIOCHEMICAL CHANGES ASSOCIATED WITH THE DEVELOPMENT OF COLORECTAL NEOPLASIA
J. C. Taylor1,3, C. A. Kendall3, N. A. Shepherd2, N. Stone3, T. A. Cook1.1Department of Colorectal Surgery; 2Department of Pathology; 3Biophotonics Research Group, Gloucestershire Royal Hospital, Great Western Road, Gloucester GL1 3NN, UK
Introduction: Raman spectroscopy is an objective, highly sensitive and specific technique used to assess biological tissues. Point spectroscopic measurements can be used to identify changes in a tissue which may enable differentiation between normal, metaplastic, adenomatous, and malignant mucosal colonic lesions. Raman spectral mapping has potential to demonstrate biochemical changes that are associated with the development of neoplasia across an entire lesion rather than at a single point. The purpose of this study was to determine if Raman spectral mapping can define biochemical changes cross a variety of colonic lesions.
Methods: Ten colonic biopsies were obtained at colonoscopy. Each biopsy demonstrated histological heterogeneity on H&E staining. Specimens were snap-frozen and 20 μm sections were mounted on calcium fluoride slides for mapping studies. Raman spectra were recorded at 50 μm intervals across each specimen, and the data used to create pseudocolour maps representing biochemical changes within the tissues.
Results: Pseudocolour maps generated using principal component analysis demonstrated spectral differences in different regions of each specimen. These spectral differences correlated well with the different areas of histological classification within the specimen that had been identified in the heterogenous H&E specimens.
Conclusions: Raman spectroscopy allows identification of the biochemical changes across colonic mucosa associated with the development of colorectal neoplasia, and may characterise changes at a molecular level that precede the development of histologically detectable malignancy. In the longer term this may be a useful method of distinguishing malignant and premalignant conditions at colonoscopy to allow targeted endoscopic excision.
326 MOLECULAR SCREENING FOR HNPCC IN AN IRISH POPULATION
K. Sheahan1, E. J. Fox2, D. Keegan1, D. T. Leahy2, R. Geraghty1, H. Mulcahy1, A. Green3, J. M. Hyland1, D. P. O’Donoghue1.1Centre for Colorectal Disease, St Vincent’s University Hospital, Dublin, Ireland; 2Conway Institute, University College Dublin, Dublin, Ireland; 3National Centre for Medical Genetics, Dublin, Ireland
Background and Aims: Tumours resulting from inherited defects in DNA mismatch repair (HNPCC) exhibit molecular features distinct from sporadic tumours. These features may be used to identify clinically unrecognised syndromic kindreds and to expedite confirmatory molecular diagnosis. We describe a defining pattern of molecular features in families meeting the Amsterdam Criteria for HNPCC and apply this pattern to prospectively identify unrecognised kindreds.
Methods: We employed detailed family history, immunohistochemistry for hMLH1, hMSH2, hPMS2, and hMSH6, microsatellite instability (MSI) testing, and methylation-specific PCR of the hMLH1 promoter to molecularly characterise tumours from individuals belonging to 14 families meeting the Amsterdam Criteria. We subsequently screened a prospective cohort of 100 consecutive tumours for these features. Individuals with molecular features suggestive of HNPCC (with or without fulfilling the Amsterdam Criteria) underwent germ-line testing.
Results: Tumours from 10 of the 14 families meeting the Amsterdam Criteria displayed features consistent with an underlying mismatch repair defect. To date, the causative mutation has been identified for six of these families. Using molecular characterisation as a screening strategy, we prospectively identified nine cases with atypical molecular features. Five of these tumours displayed immunohistochemical loss of hMLH1 together with hMLH1 promoter hypermethylation, suggestive of sporadic colorectal cancer. Four individuals with tumours showing a molecular pattern indicative of a potentially unrecognised familial cancer were identified.
Conclusion: Characterisation of molecular features indicative of hereditary cancer has the potential to accelerate molecular diagnosis and to detect clinically unrecognised cases of HNPCC.
327 ALTERATIONS IN THE LEVELS OF OXIDATIVE DAMAGE IN SPORADIC COLORECTAL CANCER
J. Sheridan, H. Mulcahy, E. Fox, D. Leahy, S. Sullivan, K. Sheahan, J. Hyland, D. O’Donoghue, J. O’Sullivan.Centre for Colorectal Disease, St Vincents University Hospital, Elm Park, Dublin 4, Ireland
Background: Oxidative DNA damage can be caused by reactive oxygen species (ROS), and 8-oxo-dG is a key biomarker of oxidative DNA damage. The base-excision repair pathway (BER) is the major pathway for repair of oxidative damage, the mismatch repair (MMR) system being an important backup repair pathway.
Methods: Using tissue microarrays and immunohistochemistry, we examined levels and localisation of 8-oxo dG in matched tumour and normal tissues from 60 sporadic colorectal cancers. Loss of mismatch repair proteins, MLH1 and MSH2 was assessed to determine interactions between BER and MMR pathways.
Results: There was no association between 8-xo-dG and loss of mismatch repair proteins in tumours. Total 8-oxo dG positivity was significantly elevated in normal mucosa (mean 71.6 (SD 23.3)) compared to tumour (36.4 (37.4)), (p<0.001). Individual levels, both in epithelial and stromal cells were greater in normal than tumour (p<0.001 in each case). Total intensity levels were also significant in each case (p<0.001). The percentage positivity and intensity levels of staining in epithelial and stromal tumour cells was significantly greater in non-metastatic versus metastatic cancers (p<0.05 in all cases).
Conclusion: Increased ROS and inflammation may contribute to the increased levels of 8-oxo dG with subsequent promotion of genomic instability, consequent risk of cancer development, and further neoplastic progression.
328 RADIATION AND CHEMOTHERAPY BYSTANDER EFFECTS IN COLORECTAL CANCER
S. Gorman, M. Tosetto, O. Howe, F. Lyng, H. Mulcahy, D. O’Donoghue, J. Hyland, D. Fennelly, J. Armstrong, K. Sheahan, J. O’Sullivan.Centre for Colorectal Disease, St Vincent’s University Hospital, Elm Park, Dublin 4, Ireland; Radiation & Environmental Science Centre, Dublin Institute of Technology; and St Lukes Hosptial, Dublin
Background: Bystander effects occur when an irradiated cell communicates with non-irradiated cells possibly via secreted factors, the non-irradiated cells then displaying characteristics of irradiated cells. Little is known regarding bystander radiation and chemotherapy effects alone and in combination in colorectal cancer.
Design: Using five colorectal cell lines and 5 Gy radiation dosage alone and with 5FU, Oxaliplatin or FOLFOX treatment, the aim of this study was to determine if medium from irradiated cells (at different time points) could cause growth inhibition, apoptosis and cell cycle disturbances in non-irradiated cells. These were monitored at 24, 48, 72, and 96 hours after medium transfer. Growth inhibition was assessed using a crystal violet assay and apoptosis and cell cycle disturbances using propidium iodine and flow cytometric analysis.
Results: Using medium conditioned by cells irradiated with 5Gy alone or chemotherapy alone, a bystander effect caused significant reduction in cell proliferation, rates of apoptosis, and cell cycle disturbances. These bystander effects were more pronounced in late stage colorectal cells lines using medium from cells treated with both radiation and chemotherapy simultaneously.
Conclusion: Bystander effects may induce secretory signals produced by both irradiated and chemotherapy treated cells. In vivo, this stress response could accelerate genomic instability.
CELL/MOLECULAR BIOLOGY POSTERS
329 MEDIA CONTAINING ENERGETICS SUBSTRATES AFFECT MITOCHONDRIA BIOGENESIS AND INCREASE METABOLISM IN THE C3A HEPATOCYTE CELL LINE
C. Filippi, P. C. Hayes, J. N. Plevris.University of Edinburgh, Edinburgh EH16 4SB, UK
Background: We have previously shown that culturing C3A cells in a medium with high concentrations of lactate (L), pyruvate (P), octanoate (O) and NH4Cl (N) improved gluconeogenesis, ureogenesis albumin synthesis, and galactose elimination capacity.
Aim: To investigate the mechanism of the LPON preconditioning by studying (1) the effect of individual and combined L, P, O, and N on C3A cell metabolism and (2) the effect of preconditioning on mitochondrial ultrastructure and function.
Methods: C3A cells were cultured until confluent in minimum essential medium Eagle (MEME) supplemented with 10% foetal calf serum (FCS). L, P, O, and N were added to MEME at different concentrations/combinations (mM): LP 10/1; N4; LPN10/1/4; LPON10/1/2/4; LPON10/1/4/4. Cells were preconditioned for 10 days before being incubated for two hours with substrates to assess their metabolic capacity (gluconeogenesis, ureogenesis, galactose elimination) and oxidative phosphorylation function (redox and phosphate potential). Cell ultrastructure was studied by electron microscopy. Mitochondrial membranes changes were further analysed by western blotting of VDAC and COX (respectively external and internal mitochondrial membrane proteins).
Results: LP improved glucide metabolism, while N affected both glucide and ureogenesis. The combination of LP and N did not further improve the metabolism while addition of O further increased glucide metabolism. LPON-preconditioned cells cytosolic NADH/NAD was significantly lower. Ultrastructural studies showed that, compared to control C3A cells, LPON preconditioned cells had reduced number but larger mitochondria, with much denser inner mitochondrial membrane. This result was further confirmed by the western blot.
Conclusion: The LPON induced significant ultrastructural and functional changes of the mitochondria of C3A cells. This was associated with improvement of cell differentiation markers such as gluconeogenesis, galactose elimination, and ureogenesis capacity.
330 POLLUTION DERIVED NANOPARTICLES PROFOUNDLY AFFECTS HEPATOCYTE BIOENERGETICS
C. Filippi, P. C. Hayes, K. Donaldson, J. N. Plevris.University of Edinburgh, Edinburgh EH16 4SB, UK
Background: Air pollution, mostly fuel combustion derived nanoparticles, is responsible for exacerbations of chronic airways disease and even death from cardiorespiratory causes. Blood borne nanoparticles reaching the liver may induce acute phase proteins (risk factors for death from acute coronary syndrome), as seen in populations exposed to air pollution.
Aim: To investigate (1) if NP end up in the liver when delivered in the circulation and (2) the effects of nanoparticles on liver cell metabolism and bioenergetics.
Methods: (1) Wistar male rats were injected with 200 μg nanoparticulate ultrafine carbon black (UfCB) in the tail vein and left for one hour before being sacrificed. The liver was prepared for H&E staining. (2) C3A cells were exposed to increasing concentrations (10–50 μg/ml) of UfCB, CuO, ZnO, or TiO2 for 24 hours. Dihydroxyacetone was used for studies of intermediary metabolism.
Results: (1) UfCB was found in Kuppfer cells in the liver samples. (2) CuO and ZnO induced profound concentration-dependant changes in cell metabolism: at 25 μg/ml, total DHA flux was respectively decreased by 40% and 80% (p<0.05), and by 40% at 10 μg/ml for both nanoparticles (p<0.05). These changes reflected a dramatic reduction in the glycolysis for both nanoparticle types. Gluconeogenesis was increased by 80% in the cells exposed to 25 μg/ml ZnO. These metabolism changes were associated with a decrease in the cytosolic redox potential. The phosphate potential did not change at 10 and 25 μg/ml of ZnO or CuO. At 50 μg/ml, ZnO and CuO were cytotoxic and cells detached from the culture wells, preventing any assessment of metabolism. UfCB and TiO2 nanoparticles did not have any effect on liver cells at the concentrations studied. These results indicate that CuO and ZnO nanoparticles had a profound oxidative effect of these particles on liver cells, which merits further evaluation.
Conclusion: Fuel combustion derived nanoparticles such as CuO and ZnO had dramatic effects on liver cell metabolism, probably due to oxidative stress. Thus in the context of high air pollution, if large quantities of nanoparticles reach the liver this could lead to acute phase protein synthesis and increase the risks of death from acute coronary syndrome in susceptible individuals.
331 DEVELOPMENT OF A COLLAGEN-CERAMIC COMPOSITE FOR FISTULA REPAIR
H. Keshaw1,2, P. D. Sibbons3, A. Forbes2, R. M. Day1,2.1Burdett Institute of GI Nursing, St Mark’s Hospital & King’s College London, UK; 2Department of Gastroenterology & Clinical Nutrition, University College London, UK; 3Department of Surgical Research, Northwick Park Institute for Medical Research, Harrow, UK
Background: Tissue adhesives, such as fibrin sealant, continue to be used for treatment of complex anal fistulae despite widely varying success rates. This is partly due to a lack of suitable alternatives and the desire for a relatively simple procedure with low morbidity that avoids more radical surgical intervention. Permacol, a cross-linked porcine dermal collagen implant, has been used for treating small bowel fistulae and tissue bulking and is currently being investigated for perianal fistula repair. Growth factors regulate tissue healing and are likely to enhance fistula repair. Vascular endothelial growth factor (VEGF) is a fundamental regulator of angiogenesis. Stimulation of angiogenesis with exogenous VEGF dramatically accelerates healing of experimental ulcers. VEGF secretion from colonic fibroblasts is significantly increased by 45S5 bioactive glass (BG).
Aim: To modify Permacol with BG particles to enhance its growth factor induced bioactivity for use in fistula repair.
Methods: 45S5 BG particles (0%–1% w/v) were added to a cryogenically milled form of Permacol (Permacol Injection) to produce a composite paste. Colonic myofibroblasts (CCD-18Co) were incorporated into the composite and cultured. Conditioned culture medium was collected after 24, 48, and 72 hours and the amount of VEGF secreted was measured by ELISA. The amount of collagen bound VEGF was similarly measured at 72 hours after dissolving the composite with collagenase type 1A. Viability of the incorporated cells was determined at 72 hours using an MTT assay.
Results: At 48 hours, the amount of VEGF secreted from the composites containing 0.1% w/v 45S5 BG was significantly increased (2209 pg (SEM 26); p<0.01) compared with 0% w/v 45S5 BG (1822 pg (50)). The amount of VEGF secreted at 72 hours was significantly increased from composites containing 0.01% (1720 pg (17); p<0.001) and 0.1% (1804 pg (53); p<0.01) w/v 45S5 BG compared with 0% w/v 45S5 BG (1602 pg (17)). At 72 hours, the amount of VEGF retained in Permacol containing 0.1% w/v 45S5 BG was significantly increased (107 pg (18); p<0.01) compared with 0% w/v 45S5 BG (52 (2)). At 72 hours, there was no significant difference in cell number between composites containing 0%, 0.01% and 0.1% w/v 45S5 BG indicating increases in VEGF secretion were independent of an increase in cell number. VEGF secretion was reduced with composites containing 1% w/v 45S5 BG corresponding with a significant reduction in cell number at 72 hours (72% (10); p<0.01).
Conclusion: The results from the current study indicate that Permacol 45S5 BG composites might provide a safe filler material for repair of perianal fistulae. The increased secretion of VEGF from cells in contact with or infiltrating the material may accelerate the healing of fistulae treated with this composite.
332 TRANSCRIPTIONAL ACTIVATION OF HUMAN SMALL INTESTINAL GENE EXPRESSION STUDIED IN ENDOSCOPIC BIOPSIES IN SHORT TERM CULTURE
S. Balesaria, S. Sangha, J. R. F. Walters.Department of Gastroenterology, Imperial College & Hammersmith Hospital, London, UK
Background: Investigation of human small intestinal function has been impaired by the lack of a suitable differentiated cell line and by differences compared with animal models. We aimed to develop a human small intestinal explant system which could be used to determine transcriptional regulation of gene expression.
Methods: Volunteers undergoing diagnostic upper endoscopy were recruited after giving informed consent for studies, approved by the local research ethics committee. Subjects with various specific disorders were not included. After diagnostic biopsies had been obtained, eight mucosal biopsies were taken and placed in pre-oxygenated tissue culture medium. Biopsies in groups of 2–4 were cultured on microporous membrane inserts and treated with either hormone or vehicle control. After culture, biopsies were placed in RNAlater; subsequently RNA and cDNA was prepared using standard methodology. Real-time quantitative RT-PCR was used to assay gene expression.
Results: Initial experiments were performed after 6 hour exposure to the active hormonal form of vitamin D, 1,25(OH)2D3 (10−9M), or control. The expression of transcripts for the brush-border membrane calcium channel, TRPV6, were standardised to those for the housekeeping gene, GAPDH. TRPV6/GAPDH ratios were 1.50 (0.21) (mean (SEM)) in controls, and 5.38 (1.00) in the treated group (p<0.001, Wilcoxon signed rank test). 29 out of 30 subjects showed an increase; the median change in expression ratios was 3.1. Similar changes occurred in men and women and were not related to age.
Conclusion: A robust human small intestinal explant system has been developed. This was able to show a marked increase by 6h in expression of transcripts for the TRPV6 transporter with physiological doses of 1,25(OH)2D3. It has the potential to study other agents that may regulate gene expression including other hormones and drugs.
333 COLONIC IRON LOADING REDUCES E-CADHERIN EXPRESSION AND ENHANCES PROLIFERATION
M. J. Brookes1, S. Hughes1, J. Boult1, N. Sharma1, F. Turner2, T. Ismail1, T. Iqbal1, C. Tselepis1.1Division of Medical Sciences, University of Birmingham, UK; 2School of Biosciences, University of Birmingham, Birmingham, UK
Background and Aims: There is increasing evidence to suggest that the colon has the capacity to directly absorb iron. Previous studies have implicated total body iron and high dietary iron intake as major risk factors for colorectal cancer. Murine studies have shown that high dietary iron can increase colorectal tumour incidence, and tumour multiplicity when administered along with a carcinogen. E-cadherin is an adherens junction protein known to be repressed in epithelial cancer.
Methods: Two colorectal carcinoma cell lines SW480 (poorly differentiated) and Caco-2 (well differentiated) were routinely cultured. Cells were subsequently stimulated with either growth medium alone (control) or iron loaded medium. Real-time PCR, western blotting, and immunoflouresence were used to determine mRNA and protein expression and localisation of E-cadherin. The effects on E-cadherin expression was further examined by using a promoter assay. The effect of cellular loading on proliferation was examined using an ATP dependent assay.
Results: Iron loading of Caco-2 and SW 480 cells resulted in a significant repression in both E-cadherin mRNA (37% and 48%, p<0.05) and protein (30% and 54%, p<0.05) respectively. Consistent with these results we demonstrated a significant fold repression in E-cadherin promoter activity in both iron loaded Caco-2 and SW-480 cells (p<0.05). Immunoflourescence for E-cadherin in both cell lines revealed preserved immunoreactivity at cell borders in the control group, however the intensity of staining was markedly reduced in the iron loaded groups. The effect of iron loading was to significantly increase proliferation in both cell lines.
Conclusions: Iron loading in well and poorly differentiated colorectal carcinoma leads to increased proliferation and decreased E-cadherin expression. This is likely to increase motility, invasiveness, and ultimately metastasis in colorectal carcinoma.
334 CANNABINOIDS PROMOTE SURVIVAL OF NORMAL HUMAN COLONIC EPITHELIAL CELLS
K. L. Wright1, D. A. F. Robertson2, P. Moyer3, S. G. Ward1.1Department of Pharmacy and Pharmacology, University of Bath; 2Department of Gastroenterology, Royal United Hospital, Bath; 3Incell Corporation LLC, San Antonio, TX, USA
Background and Aim: Important roles for the endocannabinoid system in the gastrointestinal (GI) tract under physiological and pathophysiological conditions have been demonstrated. We have shown that cannabinoids promote colonic epithelial wound closure through the CB1 receptor at nanomolar concentrations, which had no significant effect on proliferation. Previous work showed that low micromolar concentrations were antiproliferative in DLD-1 and Caco-2 tumour cell lines. Interestingly, cannabinoids exert opposite effects on the survival of transformed and non-transformed neuronal cells, inducing apoptosis in tumour cells, but not in primary cells. In this study, we investigated whether cannabinoids influenced the proliferation of non-transformed colonic epithelial cells (NCM460), which are non-tumorigenic cells derived from normal human colonic epithelial tissue.
Methods: NCM460 cells express both CB1 and CB2 receptors under normal culture conditions. Proliferation experiments were performed in the presence or absence of synthetic and endogenous cannabinoids (10 nM–10 μM) or vehicle over a five day period.
Results: ACPA (CB1 agonist), JWH (CB2 agonist), and metAEA (methanandamide, endogenous CB1/CB2 agonist) had no influence on the proliferation of these cells, even under low serum conditions. However, the CB1 receptor antagonist, AM251 (1–10 μM) alone had a profound antiproliferative effect on these cells. This implies that the activity of cannabinoid receptors is linked to the viability and survival of normal colonic epithelial cells. Further investigations revealed that cannabinoids impact on heme-oxygenase (HO)-1 expression, a protein thought to be important during restitution of inflammation.
Conclusion: These results support our suggestion that cannabinoids may have therapeutic potential during the healing phase of gastrointestinal inflammation.
335 PILOT STUDY OF A NOVEL TISSUE ENGINEERED INTESTINAL CONSTRUCT
D. A. J. Lloyd1, T. I. Ansari2, P. Gundabolu3, S. Shurey2, V. Maquet4, P. D. Sibbons2, A. R. Boccaccini3, S. M. Gabe1,3.1St Mark’s Hospital, Harrow; 2Northwick Park Institute for Medical Research, Harrow; 3Imperial College, London; 4University of Liege, Belgium
Background and Aim: Tissue engineering of the small intestine is a novel discipline uniting material scientists, cell biologists and clinical scientists. It offers the possibility of an alternative to long-term intravenous nutrition and transplantation in patients with short bowel syndrome. Initial work, although encouraging, is limited by the large volumes of neonatal tissue required to produce a small cyst of neomucosa. Our group have developed a novel approach based on a subcutaneously implanted highly porous tubular biodegradable poly-lactide-co-glycolide (PLGA) foam scaffold. The aim of this study was to investigate whether this scaffold would support growth of intestinal neomucosa.
Methods: PLGA scaffolds were implanted subcutaneously into eight male Lewis rats. After five weeks, a suspension of “organoid units”, derived via partial digestion of neonatal rat small intestine, was implanted into the lumen of the scaffolds. Tissue was assessed histologically after harvesting. Immunohistochemistry was performed using antibodies against vascular endothelial growth factor (VEGF), vascular endothelial growth factor receptor 2 (VEGF-R2), fibroblast growth factor basic (bFGF) and fibroblast growth factor receptor 2 (FGF-R2). Stereological techniques were used to quantify the density of positively stained cells.
Results: At four weeks post organoid unit implantation, clearly recognisable mucosa and submucosa showing histological features similar to small intestine were present on the luminal surface of the scaffold. The scaffold showed evidence of vascularisation and early capillary formation. Densities of VEGF and VEGF-R2 positive cells increased with time post organoid unit implantation while those of bFGF and FGF-R2 remained constant. The yield of the tissue engineering process was approximately four times that documented in the literature.
Conclusion: This pilot study demonstrates that it is possible to tissue engineer small intestinal neomucosa using subcutaneously implanted PLGA scaffolds. The yield of the process compares favourably to the published literature. Further work is required to optimise the technique.
336 THE STOMACH AND BCL-2
H. W. Steer.Southampton General Hospital, Southampton, UK
Bcl-2 is a protein produced by the B cell lymphoma/leukaemia–2 gene and is known to block apoptosis. Previous studies have found no change in the Bcl-2 expression in inflammatory gastrointestinal diseases.1
An immunohistochemical study has been performed using glycol methacrylate (GMA) processing of gastric biopsies to investigate the expression of Bcl-2 in Helicobacter pylori infection. The study has involved endoscopic biopsies from 77 patients (33 normal stomachs and 44 stomachs infected with Helicobacter pylori).
In the normal stomach Bcl-2 expression is limited to the mucosal blood vessels with the particulate expression consistent with a localisation in platelets.2 Bcl-2 is known to be expressed by megakaryocytes.
The present study has shown that Helicobacter pylori infection is associated with a marked upregulation of Bcl-2 in the mucosal connective tissue.
Bcl-2 is associated with lymphoma development in transgenic mice and in humans it is associated with follicular lymphomas as well as some diffuse large cell lymphoma. The upregulation of Bcl-2 in Helicobacter pylori infection would be ideally sited to influence B cell survival resulting in the potential for lymphoma development. It would explain why treatment of the Helicobacter pylori infection with the resultant downregulation of Bcl-2 is beneficial and may result in the regression of gastric “lymphoma” which has been noted under such circumstances.2
1
2
337 LACK OF ASSOCIATION BETWEEN POLYMORPHISMS OF GSTP1, SOD2 AND GPX2 AND RISK OF OESOPHAGEAL ADENOCARCINOMA: RESULTS FROM A POPULATION BASED STUDY IN IRELAND (THE FINBAR STUDY)
S. J. Murphy, L. A. Anderson, A. E. Hughes, R. G. P. Watson, B. T. Johnston, H. Comber, C. C. Patterson, J. McGuigan, J. V. Reynolds, L. J. Murray.Departments of Epidemiology and Public Health and Medical Genetics, Queen’s University, Belfast
Introduction: Oxidative stress appears to be important in the pathogenesis of Barrett’s oesophagus (BO) and oesophageal adenocarcinoma (OAC). Genetic polymorphisms of enzymes involved in antioxidant pathways may play a part in determining individual susceptibility to OAC. The aim of our study was to determine if single nucleotide polymorphisms (SNPs) of antioxidant enzyme genes were associated with risk of OAC in a population based setting.
Methods: The FINBAR study is a population based case control study of OAC in Ireland (population 5.5 million). Cases of OAC (n = 230) were prospectively enrolled as were subjects with BO (⩾3 cm BE at endoscopy with specialised intestinal metaplasia on biopsy, n = 190), and normal population controls (n = 230). DNA was extracted from frozen white cell buffy coats. Several SNPs spanning the genes for glutathione S-transferase P1 (GSTP1), superoxide dismutase 2 (SOD2), and glutathione peroxidase 2 (GPX2) were selected to identify the major haplotypes. SNP genotyping was carried out using multiplex PCR and SNaPshot. The χ2 test was used to compare genotype and allele frequencies between case and control subjects.
Results: Seven informative SNPs were genotyped (2 for GSTP1, 3 for SOD2, 2 for GPX2). All SNPs were in Hardy-Weinberg equilibrium. None was significantly associated with OAC or BO even before Bonferroni correction. Odds ratios (OR) for OAC for individual SNPs ranged from 0.88 (95% CI 0.59 to 1.33) to 1.31 (95% CI 0.84 to 2.06). SNPs in all 3 genes were in strong LD (D′>0.887) but haplotype analysis did not show any significant association with OAC or BO.
Conclusions: SNPs involving the GSTP1, SOD2 and GPX2 genes were not associated with OAC. Further studies aimed at identifying susceptibility genes should focus on different antioxidant genes.
338 A ROLE FOR IRON TRANSPORTERS IN OESOPHAGEAL ADENOCARCINOMA
J. Boult, S. Hughes, M. J. Brookes, K. Roberts, P. Taniere, T. Iqbal, C. Tselepis.Division of Medical Sciences, University of Birmingham, Birmingham, UK
Background: Iron is essential for cellular metabolism, growth, and cell cycling. Iron has previously been implicated in the malignant progression of Barrett’s metaplasia (BM) to oesophageal adenocarcinoma (ADC). To date there has been no characterisation of the proteins involved in iron transport in the progression of ADC. Thus the aims of this study were to characterise several of the proteins involved in cellular iron import (Divalent metal transporter 1 (DMT1), duodenal cytochrome B (DcytB) and transferrin receptor 1 (TFR1]), cellular iron export (hephaestin (HEPH)) and cellular iron storage (ferritin) in normal oesophagus (NO), gastric mucosa (GM), BM, and ADC.
Methods: Perl’s Prussian staining was used to examine cellular iron content. mRNA expression of the iron transporters were determined by quantitative real-time PCR in 18 ADC specimens. Semiquantitative immunohistochemistry was performed to assess cellular localisation and protein expression.
Results: Perl’s staining demonstrated increased intracellular iron in ADC whilst there was no evidence of staining in NO, GM or BM. Cellular iron import proteins DMT1, DcytB and TFR1 were all significantly overexpresed in ADC (p<0.01). These changes were also seen at the mRNA level where DMT1 (p = 0.004), DcytB and TFR1 (both p<0.001) were overexpressed. Conversely the iron export protein HEPH was transcriptionally repressed in ADC (p<0.05). Ferritin was overexpressed at both the mRNA (p = 0.02) and protein level (p<0.001) in ADC. The transcriptional upregulation of TFR1 and ferritin was also observed in matched samples of Barrett’s metaplasia (p<0.05).
Conclusions: Oesophageal adenocarcinoma was associated with increased expression of iron import proteins (DMT1, DcytB, and TFR1) and decreased expression of the cellular iron export protein HEPH. We conclude that this causes iron loading of columnar cells which may represent a mechanism of tumourigenesis.
339 MECHANISMS OF THE GROWTH FACTOR AND ANTI-APOPTOTIC ACTIONS OF LEPTIN IN OESOPHAGEAL ADENOCARCINOMA CELLS
O. O. Ogunwobi, E. Cameron, K. Elamin, G. Mutungi, M. Wilkinson, I. L. P. Beales.Gastroenterology & Histopathology Units, Norfolk and Norwich University Hospital & School of Medicine, University of East Anglia, Norwich, UK
Background: Obesity increases the risk of oesophageal adenocarcinoma (OAC). Leptin is secreted by adipocytes and levels are elevated in obesity. Leptin receptors are expressed in Barrett’s oesophagus. We have hypothesised that leptin may directly influence the oesophageal epithelium and examined the effects of leptin on the OE33 OAC cell line in culture.
Results: Expression of the long leptin receptor isoform (Ob-Rb) and most common short form (Ob-Ra) were confirmed by RT-PCR and immunoblotting. Cell surface expression was confirmed by immunocytochemistry. Leptin increased proliferation and inhibited apoptosis. These effects were abolished by the COX-2 inhibitor NS-398. Leptin increased COX-2 mRNA levels and PGE2 secretion. Leptin stimulated phosphorylation of ERK, p38 MAP kinase, JAK2, and Akt: inhibitor studies confirmed that all these pathways were upstream of COX-2. Pharmacological inhibition of JNK and the epidermal growth factor receptor (EGFR) also inhibited the proliferative and anti-apoptotic actions of leptin but stimulation with leptin did not lead to immediate phosphorylation of JNK or the EGFR. By RT-PCR the EP-4 receptor was the only prostaglandin receptor type expressed by OE33 cells. PGE2 itself increased proliferation and inhibited apoptosis. The growth factor and anti-apoptotic effects of leptin and PGE2 were abolished by the EP-4 receptor antagonist AH23848. PGE2 stimulated JNK phosphorylation in an EGFR dependent manner and the activation of EGFR required protein kinase C, src and matrix metalloproteinase activity.
Conclusions: Leptin stimulates proliferation and inhibits apoptosis in OAC cells via a complex sequence of events involving Akt and MAP kinase activation, COX-2 mediated PGE2 production, PGE-2-induced transactivation of the EGFR, and JNK activation. Leptin may directly contribute to the development of oesophageal adenocarcinoma.
340 ANALYSIS OF INHERITED MYH MUTATIONS IN BRITISH ASIAN PATIENTS WITH COLORECTAL CANCER
S. Dolwani1,7, G. T. Williams2, K. P. West3, J. Newman4, D. Stock5, A. P. Griffiths6, J. Best2, J. P. Cheadle1, J. R. Sampson1.1,7Department of Med Genetics and Gastroenterology, Cardiff University & Cardiff & Vale NHS Trust; 2Departments of Pathology at University Hospital of Wales, Cardiff; 3University Hospitals Leicester; 4Birmingham Heartlands Hospital; 5Royal Glamorgan Hospital; 6Swansea Hospitals NHS Trust
Background and Aim: Biallelic mutations of the DNA base excision repair gene MYH are known to be associated with multiple colorectal adenomas and colorectal cancer (CRC). This recessively inherited disorder MYH associated polyposis (MAP) is distinct from dominantly inherited familial adenomatous polyposis (FAP). We had previously noted that all four families of British Asian origin out of 115 families on the Wales polyposis register had MAP. We conducted a retrospective study after MREC approval to characterise the contribution of MYH mutations to CRC in this group particularly E466X and Y90X which have not been found in any other ethnic group.
Methods: Cases were ascertained through five departments of pathology in the UK. Archived paraffin blocks of tissue of cases with CRC were identified and British Asian cases (n = 120) selected by name, then suitably anonymised and re-examined to ensure analysis of only normal background mucosa prior to analysis. The control group (n = 100) consisted of paraffin blocks from Asian individuals from the same centres with a diagnosis of inflammation without neoplasia. DNA was extracted and PCR and restriction enzyme digestion used for analysis of the unique Asian mutations E466X (using ApoI), and Y90X (using RsaI) along with the common Caucasian mutations G382D (using BglIII) and Y165C (using ARMS PCR). Positive results were confirmed by bidirectional sequencing as well as sequencing of all exons of MYH.
Results: One case (1/120) and one control (1/100) sample were found to be heterozygous for the E466X variant in MYH. No case or controls had bi-allelic mutations or any of the other three mutations tested. Sequencing of all exons of MYH did not reveal any second mutations in these two individuals.
Conclusion: The allele frequency of E466X in this study is comparable to that of Y165C and G382D in the general British population. There is thus a strong case for initial testing for this mutation in Asian individuals with MAP or CRC with apparent recessive transmission.
341 A ROLE FOR IRON TRANSPORTERS IN COLORECTAL ADENOCARCINOMA
M. J. Brookes, J. Boult, S. Hughes, N. Sharma, T. Ismail, E. Hamilton, T. Iqbal, C. Tselepis.Division of Medical Sciences, University of Birmingham, Birmingham, UK
Background and Aims: Iron is essential for a number of key cellular processes, including cell cycling. There is increasing evidence to suggest that high dietary iron intake is an important risk factor for colorectal carcinoma (CRC). There are no studies to date which have comprehensively characterised the expression of iron transporters in the progression of CRC. The aim of this study was to characterise the expression of key iron transport proteins within the colon; Divalent metal transporter 1 (DMT1), duodenal cytochrome B (DcytB), transferrin receptor 1 (TFR1), ferritin, hephaestin (HEPH), and ferroportin (FPN).
Methods: Enhanced Perl’s Prussian staining was used to examine cellular iron content. Real-time PCR and western blotting were used to examine mRNA and protein levels in 15 human CRC resections. Semiquantitative immunohistochemistry was used to determine protein levels and cellular localisation in normal human colon and colorectal carcinoma.
Results: Perl’s staining showed an increased iron content within CRC, compared to normal colon. Expression studies revealed overexpression of the iron import machinery Dcytb, DMT-1, and TFR1 in CRC compared to normal colon. Regarding the export proteins, although FPN was overexpressed at the mRNA and protein levels, HEPH was decreased in the majority of CRC examined. Immunohistochemistry however revealed a cytoplasmic relocalisation of FPN, with a loss of membranous expression. A loss of HEPH and FPN expression was associated with more advanced disease.
Conclusions: The progression from normal colon to CRC is associated with increased expression of iron import proteins, associated with either a repression or relocalisation of iron exporters HEPH and FPN respectively. This results in increased intracellular iron which is likely to be necessary for tumour proliferation.
342 CHARACTERISATION OF ISOLATED HUMAN COLONIC CRYPT EPITHELIAL CELLS AND THEIR INTERACTIONS WITH INTESTINAL MYOFIBROBLASTS
S. Samuel1,2, R. A. Robins1,3, J. Webb1,2, Y. R. Mahida1,2.1Institute of Infection, Immunity & Inflammation; 2and Divisions of Gastroenterology; 3Immunology, University of Nottingham, UK
Introduction: Intestinal stem cells are located at the base of small and large intestinal crypts and give rise to distinct subopulations of epithelial cells. Factors that regulate intestinal stem cell survival, proliferation, and differentiation remain to be characterised. Subepithelial myofibroblasts are likely to be important in regulating stem cell function via secreted factors, including extracellular matrix. We have investigated interactions between the two cell types following isolation.
Methods: Crypt epithelial cells were isolated and disaggregated from normal colonic mucosal samples following treatment with ethylenediaminetetraacetic acid and pancreatin. Their viability was assessed using trypan blue and they were also studied by FACS and immunohistochemistry, before and after co-culture with monolayers of intestinal myofibroblasts. Expression of stem cell specific musashi-1 transcripts was studied by RT-PCR. Data are expressed as mean (SD).
Results: The disaggregated crypt epithelial cells were immunoreactive for cytokeratin (specific for epithelial cells) and their viability was 71.2 (15.6)% (n = 25). They expressed β1 integrin, as demonstrated by significantly increased mean fluorescence intensity (MFI) using β1 integrin specific antibody compared to isotype control antibody (190.3 (109.9) v 11.6 (9.0), p<0.02). Expression of musashi-1 transcripts was confirmed by RT-PCR (n = 3). Following application to monolayers of myofibroblasts for 10 minutes (and subsequent washing), many (10.4 (8.3) per high power field) cytokeratin positive adherent epithelial cells were seen. After culture with myofibroblasts for three days, cytokeratin positive cells with processes were seen.
Conclusions: Viable, stem cell containing, disaggregated human colonic crypt epithelial preparations can be consistently obtained for subsequent studies to investigate their interactions with isolated intestinal myofibroblasts. The latter may facilitate survival of the crypt epithelial cells, including stem cells.
Service development posters
343 DO PATIENTS APPRECIATE A COPY OF THEIR ENDOSCOPY REPORT? AN AUDIT
N. C. Fisher.Dudley Group of Hospitals, Dudley, UK
Background: Patient involvement in clinical documentation is increasingly regarded as best practice. This is especially relevant to endoscopy reporting, where subjects may be sedated and thus unable to retain verbal information after their procedure. The endoscopy global rating scale (GRS) includes provision of a patient-focussed endoscopy report as a criterion of quality. An example of this practice is reviewed here.
Methods: The author routinely provides all endoscopy patients (other than those with a first diagnosis of malignancy) with a copy of their printed report, which is worded in a “patient friendly” manner, upon discharge. To audit this practice, 100 consecutive patients were sent a questionnaire asking their views on this practice.
Results: Sixty eight gastroscopy, 20 colonoscopy, and 12 ERCP patients were sent a questionnaire within four weeks of their endoscopy; 78/100 replied. Of these, 88% had kept a copy of their report. 82% reported being able to understand the report and 82% felt that it had helped “recap” on the findings later on. 71% found the report helpful and 86% found it reassuring. 6% felt it caused anxiety. Out of 42 freetext comments, 76% were favourable and 14% unfavourable.
Conclusions: Provision of a patient focussed endoscopy report is easy to do, complies with best practice guidance, and is widely appreciated by patients.
344 INVESTIGATING DYSPEPSIA: BRINGING NATIONAL GUIDELINES TO A LOCAL LEVEL
S. M. Rehman, M. S. Nazir, S. Konda, J. P. Teo, J. Kwan (introduced by T. D. Heymann).Tanaka Business School, Imperial College, South Kensington, London SW7 2AZ, UK
Objective: Dyspepsia has traditionally been investigated using serology; however NICE (2004) guidelines recommend urea breath testing (UBT) or faecal antigen testing (FAT). This study aims to find the optimal method of investigating dyspepsia under the new guidelines within a primary care trust (PCT).
Methods: Of the UBT/FAT options, only UBT in secondary care is presently available to patients within Kingston PCT. Process mapping and cost minimisation analyses of four possible methods of investigating dyspepsia (UBT/FAT in primary/secondary care) were performed. A questionnaire based survey of 88 patients was conducted to determine patient preferences regarding UBT and FAT, and primary and secondary care. Interview based questionnaires of five GPs were conducted to identify implementation issues regarding shifting the investigation of dyspepsia to primary care.
Results: Analysis revealed, in descending order of cost: UBT in secondary care, FAT in secondary care, UBT in primary care, and FAT in primary care (FAT in primary care is £36.56 cheaper per patient than UBT in secondary care). 60% of patients preferred UBT, 33% preferred FAT; 66% preferred to be investigated in primary care, 10% preferred secondary care. GP interviews indicated that clinician knowledge about guidelines is limited. GPs highlighted time and space constraints, and difficulties in redistributing resources to implement investigation of dyspepsia in primary care.
Discussion: A recommendation of a shift in the investigation of dyspepsia from secondary care to primary care was made. Implementation of FAT would further reduce costs, although patient resistance to FAT needs to be overcome. Despite potential cost savings and improved patient experience, implementation may flounder due to lack of clinician awareness, ability to benefit from change, or patient preference.
Conclusion: Successful local implementation needs relevant stakeholder involvement and resource reallocation whilst considering patient opinion. These pose substantial barriers to change.
345 AUDIT: IS THE AGE LIMIT OF 55 YEARS (NICE 2004) FOR ENDOSCOPING DYSPEPTIC PATIENTS WITHOUT ALARM SYMPTOMS SAFE?
A. Koulaouzidis, G. I. Leontiadis, S. Eliades, F. Azam, A. Saeed, S. Kadis (introduced by B. Linaker).Combined Gastroenterology Unit, Queen Elizabeth Hospital, Gateshead, UK
Background: In August 2004 NICE published its guidelines for managing dyspepsia in primary care, which stated that patients below the age of 55 years without alarm symptoms do not need endoscopic investigation. They can be safely managed with proton pump inhibitors or eradication therapy. This represents a rise in the age limit from that of 45 years (Maastricht II-2000 consensus).
Aim: To check the validity of the age limit change through estimation of incidence and presenting symptoms of oesophageal and gastric cancer in patients below the age of 55 years in the catchment of a District General Hospital (Queen Elizabeth Hospital) of North East.
Methods: In this retrospective study we identified through the database of Queen Elizabeth Hospital (catchment area 250 000), all patients below the age of 55 years with diagnosis of oesophageal or gastric cancer, diagnosed by histology, between April 2000 and March 2003. We included all patients living in the Hospital’s catchment area, even if treated in other Hospitals.
Results: Oesophageal or gastric cancer was diagnosed in 17 patients below the age of 55 years; incidence 1.7/100 000/year. The incidence for ages below 45 was 0.3/100 000/year. The youngest patient was 41 years old. For a patient of 47 years old with adenocarcinoma of the gastro-oesophageal junction we did not manage to delineate his presenting symptomatology. In the remaining 16 patients the cancers presented with alarm symptoms which led to urgent diagnostic endoscopy.
Conclusion: It is very rare to diagnose cancer of the upper gastro-oesophageal tract in younger age groups without preceding alarm symptoms. The age limit of 55 years for endoscopy in patients without alarm symptoms seems safe when applied to our population.
346 AN AUDIT OF THE INFLUENCE OF A NURSE LED DYSPEPSIA SERVICE
R. C. Prudham1, C. McGovern1, J. Taylor2, M. Campbell2, M. J. Goodman1, N. Haslam1.1Fairfield General Hospital, Bury, Lancashire; 2Bury PCT
Background: NICE guidelines on dyspepsia management in the community were published in 2003. In response a nurse led dyspepsia service was established by Bury PCT in December 2003. A Nurse Endoscopist was appointed to manage the diagnostic gastroscopy service, triage patients, liaise with GPs and to have educational sessions with the GPs with a view to reducing referrals and improving access times.
Aim: To investigate the influence of the service on Consultant referrals, access times, and prescribing costs.
Method: Local guidelines on dyspepsia management were developed by representatives from primary and secondary care from the NICE guidelines. The Nurse Endoscopist disseminated these via mail, education sessions, and visits.
Results: Prior to the Dyspepsia service in 2003 there were 990 referrals to three Consultant Gastroenterologists. Following the start of the dyspepsia service Consultant referrals had dropped to 662, with 218 to the nurse led dyspepsia service. Data for the first six months of 2005 are 331 referrals to Consultants and 90 to the Nurse Endoscopist. Maximum wait time for the nurse led service is three weeks from referral to endoscopy.
Data for prescribing costs for 2003/04 were £960,757 and £910,669 for 2004/05 a cost saving of £50,000. (not all attributable to the Nurse Endoscopist as proton pump inhibitor costs have reduced)
Conclusion: The nurse led dyspepsia service reduced referrals to Consultants by 330 per year and overall referrals by 110 (11%) without increasing prescribing costs. Patients receive a fast diagnostic service, average time from referral to endoscopy for the nurse led service, is three weeks with a corresponding improvement in Consultant access times. Under payment by results the service almost pays for itself.
347 THE AGREEMENT BETWEEN GP REPORTED DYSPEPSIA AND PATIENT FILLED DYSPEPSIA QUESTIONNAIRE IS POOR FOR “TWO WEEK” ENDOSCOPY REFERRAL
C. H. Lim, R. Child, M. P. Skander, M. M. Ahmed.Department of Gastroenterology, Good Hope Hospital, Sutton Coldfield B75 7RR, UK
Objective: NICE referral guidelines for suspected cancer in adults and children recommend urgent specialist referral for endoscopic examination (to be carried out within two weeks) for patients with predefined alarming symptoms or signs for suspected upper gastrointestinal (GI) cancer.1 There is concern that these predefined criteria may be subjected to misuse as an alternative route for urgent endoscopy for patients who do not actually fulfil the criteria. Hence, the aim of this study is to determine the agreement between the general practitioners (GP) filled referral form with patient self filled questionnaire.
Methods: Leeds validated dyspepsia questionnaire (SFLDQ v7 (3))2 with additional alarming symptoms were sent to all patients referred under the “two week wait” criteria and the data were collected prospectively from July to October 2005. Agreement was assessed by Kappa statistics. Kappa value of less than 0.2 is considered poor agreement and more than 0.6 as good agreement.
Results: Two hundred and eight patients were referred for urgent endoscopy. Nine patients were redirected to urgent outpatient assessment and six patients failed to attend their appointment. Hence 193 patients were available for analysis. Fifty four per cent were female (n = 105) and the median age was 71 years (IQR = 62 to 79 years). Sixteen (8%) cancers were found (12 oesophagus, 4 stomach). Normal endoscopy was reported in 99 (51%) patients, reflux oesophagitis in 33 (17%) patients, and peptic ulcer disease in 10 (5%) patients. The commonest three alarming symptoms were persistent dyspepsia above 55 years old (62%), dysphagia (40%), and weight loss (34%). One hundred patients (52%) returned their questionnaire and this subgroup had similar commonest three alarming symptoms as the overall group (67%, 31%, and 36% respectively). The percentage of patients reported these symptoms were 74%, 40%, and 45% respectively. The kappa values were 0.2 for dyspepsia, 0.4 for dysphagia, and 0.65 weight loss.
Conclusions: The agreement for the symptom of dyspepsia is poor. These suggest GP may be using incorrect definition for the diagnosis of dyspepsia. Regular feedback and education to GP may reduce the number of urgent referrals for this commonest alarming symptom.
1
2
348 PEPTIC ULCERS ARE BEING UNDERTREATED DUE TO THE LACK OF AVAILABILITY OF SPECIALIST NURSING AND EQUIPMENT OUT OF HOURS: AN AUDIT OF 116 CONSECUTIVE REFERRALS FOR GI BLEEDING
J. M. Hoare, D. MacDonald, A. Siddiqui, T. R. Orchard, J. P. Teare, H. J. Thomas, R. Negus.Department of Gastroenterology, St Mary’s Hospital, Paddington, London W2 1NY, UK
We audited all referrals for acute upper GI bleeding in a central London hospital over six months. We recorded patient demographics and haemostatic therapy used on 116 patients undergoing 143 procedures and calculated mortality and re-bleed statistics. Many of these patients were high risk ITU, cardiothoracic, and renal patients reflecting the population of a tertiary referral hospital.
Mortality was 15%. 45% of all procedures were performed using a mobile endoscopy stack, remote from the endoscopy department, either in A&E, ICU, HDU or theatres. Either the patient was too sick to move or the procedure was done “out of hours”. These patients were significantly higher risk than those performed “in hours” and in the endoscopy department (mean Rockall score 3.75 v 6.09, p<0.001, Mann-Whitney U test).
Only 6/17 peptic ulcers with stigmata of recent haemorrhage received “dual therapy”. 17% of peptic ulcers re-bled and this was associated with 50% mortality. Acute variceal haemorrhage was associated with 15% mortality (2/13) and all variceal bleeders admitted to ICU survived to discharge (3/13). High dose PPI infusion was used appropriately for high risk lesions and patients. Endoscopists found it difficult to utilise haemoclips without trained assistants whereas adrenaline injection and band ligation were frequently and successfully performed.
Unassisted emergency upper GI endoscopy with a mobile endoscopy unit, without trained nurses or thermal therapy is unsatisfactory. The audit has lead to the purchase of a bipolar therapy unit for the mobile stack. Re-bleeding rates will be re-audited once this treatment modality is established. The creation of a dedicated inpatient/emergency endoscopy facility, with nursing support is being discussed.
349 SELECTION OF PATIENTS WITH UPPER GI BLEEDING FOR EARLY DISCHARGE USING THE BLATCHFORD SCORE
E. C. Thompson, C. W. Wells, C. Patvardhan, M. D. Rutter, D. Ashley.University Hospital of North Tees, Stockton on Tees TS19 8PE, UK
Background and Aim: Acute upper GI haemorrhage (UGIH) is a common medical emergency. Mortality is between 5–12%, however a large number of patients are at “low risk” and could be safely discharged early if they could be identified. The Rockall score is a validated post-endoscopic score that predicts risk of rebleeding and death. The Blatchford score is a pre-endoscopic score that predicts the need for intervention. We applied both these scores to a retrospective cohort of patients who presented to our trust with UGIH to identify which scoring system would have best identified patients for early discharge.
Results: 123 consecutive patients admitted with UGIH were identified. Duration of stay, need for intervention, and mortality was collected. Blatchford score, pre- and post-endoscopy Rockall scores were calculated. The mean age was 58.6 years (16.6–96.3 years). The mean length of stay in hospital was 5.4 days (0–153 days). A total of 83 patients underwent OGD. 42 patients required an intervention i.e. transfusion (n = 26), endoscopic treatment (n = 12), surgery (n = 1), death (n = 7), re-bleed (n = 8). Negative predictive value (NPV) for need for intervention was calculated and compared against the scores. A Blatchford score of 0 (17% of patients) and ⩽2 (34%) had NPV of 100% and 95% respectively. Pre-endoscopy Rockall score of 0 (27%) and Post endoscopy Rockall score of ⩽2 (42%) had a negative predictive value of 90% and 75% respectively.
Conclusion: In our population of patients the Blatchford score was superior to the Rockall score in identifying patients who did not need clinical intervention and were thus suitable for early discharge. Had the Blatchford score been applied to this cohort almost 20% of patients could have been safely identified for early discharge without inpatient endoscopy. The score would also have reduced the number of emergency endoscopies by 15%. In light of this audit we now apply the Blatchford score to all UGIH patients and discharge without inpatient endoscopy in those with scores of 0. This change in policy is currently being prospectively audited.
350 IMPACT OF REFERRAL ASSESSORS ON GASTROSCOPY REFERRALS FOLLOWING GUIDELINE INTRODUCTION
D. Owen1, P. Duane2, L. l. Roberts3, K. Wareham3, G. Elwyn1.1Department of Primary Care, University of Wales Swansea; 2Morriston Hospital, Swansea; 3Clinical Research Unit, Swansea, UK
Introduction: There is evidence that effective dissemination practices are required to ensure that guidelines are followed. Increasing demands on endoscopy services and increasing evidence have led to the development of guidelines for the management of dyspepsia. The All-Wales Dyspepsia Management Guidelines (based on the NICE and SIGN guidelines) were circulated throughout Wales in October 2004.
Aim: The aim of the study was to see whether dissemination and education of referrers via feedback improved quality of gastroscopy referrals received by gastroscopy units.
Method: All gastroscopy referrals to three endoscopy units in S Wales were obtained for a period of six months before and six months following the introduction of the All Wales Guidelines. Primary Care Referral Assessors evaluated each referral compared to the current Guidelines. No change was made to the actual referral process. For the six months after publication of the guidelines, the referrer of a guideline incongruent endoscopy request was sent a letter and a copy of the guidelines.
Results: Percentages of Guideline congruent OGD dyspepsia referrals for the six months before and after intervention are shown in the table.
Abstract 350
Conclusion: The results indicate that formative feedback of referrals is effective in increasing the quality of gastroscopy referrals from primary care but has limited impact on secondary care referral practices. As well as improving quality and numbers of referrals meeting guidelines, referral assessing resulted in lower numbers of referrals overall. This novel scheme may be extended to other procedures in order to increase quality and appropriateness of referral practices for primary care.
351 PARTIAL BOOKING FOR OUTPATIENT GASTROSCOPY: ARE SOME PATIENTS DISADVANTAGED?
S. Mehmet, D. S. Rampton.Department of Gastroenterology, Barts & the London NHS Trust, London E1 1BB, UK
Introduction: Partial booking for appointments is being widely introduced in the NHS to improve convenience of appointments for patients and to shorten waiting lists by reducing non-attendance rates. We hypothesised that the system might disadvantage certain groups of patients, for example non-English speakers or the elderly who might have difficulty in understanding and/or responding to the written instructions they receive from appointments staff.
Aim: To compare non-response rates to written invitations to make out-patient gastroscopy (OGD) appointments in different subgroups in an inner city population.
Method: Data on response to letters of invitation and on attendance for OGD were collected. 100 responders and 100 non-responders were subdivided by age, gender, and ethnic group during a one month period in 2004. Results were analysed by χ2 test.
Results: Introduction of partial booking was associated with a reduction in waiting time for OGD from six months in 2003 to two months in late 2004; non-attendance rates for booked OGDs fell from 25% to 10%. There were no differences in response rates to letters of invitation in relation to age or ethnicity. Overall, of non-responders, 63% were males (p<0.05): this difference related primarily to Caucasians, in whom 77% of non-responders were male (p = 0.01).
Conclusions: Partial booking has been associated with marked reductions in waiting times and in non-attendance for OGD. Contrary to our expectations, patients failing to make contact to fix appointments for OGD were mainly English speaking white men. It is reassuring that this system of booking appointments for OGD does not seem to disadvantage either elderly patients or those whose first language is not English.
352 HOW TO REDUCE INAPPROPRIATE ENDOSCOPIC GASTROSTOMY (PEG) REQUESTS
T. Shirazi, A. Saleem, A. K. Awasthi, T. K. Daneshmend.Department of Gastroenterology, Royal Devon & Exeter Hospital, Exeter EX2 5DW, UK
Introduction: The NCEPOD Report 2004 Scoping our Practice found that 19% of 719 PEG procedures were “futile” and in 63% there was a definite risk of death as assessed by the consultant treating them. We had noticed a steady increase in requests, many inappropriate, for PEG insertions in our hospital.
Aim: To reduce inappropriate PEG requests in our hospital.
Methods: We examined our PEG requests over a 10 year period (1996–2005) using our endoscopy database. We devised an inpatient endoscopy request form to obtain more detailed information if the patient was referred for a PEG. It was emphasised that PEG was an operative procedure and death within 30 days would need to be reported formally. The A5 form was piloted then launched in August 2004. We examined the number of PEG insertions in the 12 months before and after introduction of the new request arrangements.
Results: Between 1996 and 2005, we performed 637 PEG insertions. We inserted 25 PEGs each year in 1996 and 1997, rising to about 90 per year from 2002 onwards. In the 12 months before the introduction of the new request form we had inserted 98 PEGs. In the 12 months after the new arrangements we inserted 51 PEGs, a reduction of 46%. The reduction was maintained beyond the first year.
Conclusion: We were able to successfully reduce inappropriate requests for PEGs by the introduction of a simple and clear request form. The impact of this change in the request procedure has been maintained.
353 THE SCOPE OF INPATIENT ENDOSCOPY PRE-ASSESSMENT
H. Ludlow, P. Mizen, R. Crimmins, J. Swift, J. Green, S. Dolwani.Department of Gastroenterology, Llandough Hospital, Cardiff and Vale NHS Trust, UK
Background: Assessment of demand and capacity forms part of Improving Endoscopy Services NHS (2005) guidelines. Since pre-assessment of outpatients has been shown to improve utilisation of lists, we wanted to see if a similar intervention for in-patients would be of value.
Objectives: To assess the feasibility, via a pilot study, of specialist nurse led intervention in prioritisation of referrals, thereby reducing inappropriate procedures and delays due to unprepared patients.
Methodology: Every inpatient request for all endoscopic procedures was assessed by a nurse specialist, discussing any concerns with the gastroenterology consultants or SpR. A check list was placed in the patients’ notes and ward staff were advised on correct preparation. Liaison took place between the referring doctor, waiting list manager, gastroenterology team, endoscopy staff, and the nurse specialist, thus maximising use of slots. A written report of any problems encountered was made by the endoscopist.
Results: In the three months since pre-assessment began in July 05, only four problems have been recorded. Out of 227 inpatient requests, 45 patients (20% of referrals) were pre-assessed as inappropriate or unnecessary and directed to more suitable treatment options.
Discussion: Inpatient pre-assessment for endoscopy is feasible and this study demonstrates the potential for its clinical and economic benefits.
354 EVALUATION OF THE OUTCOME AND EFFECTIVENESS OF DIGITAL DICTATION AND INTERNATIONAL OUTSOURCING OF MEDICAL TRANSCRIPTION IN GASTROENTEROLOGY
N. U. Beejay1, S. Austin2.1Newham University Hospital NHS Trust, Glen Road, London E13 8SL, UK; 2ScribeTech UK Ltd, 15 Colman House, Empire Square, London SE20 7EX, UK
Background: Communication with referring physicians and other medical colleagues has traditionally been accomplished using analogue dictation with subsequent transcription by medical secretaries. The quality and speed of transcription can be variable and at best take up to one week to reach intended recipients. Digital dictation and international outsourcing of transcription has been suggested as being an efficient and cost effective alternative method.
Objective: To evaluate the clarity, speed, accuracy, safety, and effectiveness of digital dictation and outsourced transcription.
Methods: A pilot project was commenced using an established service provider (ScribeTech UK Ltd, London). Dictation was performed using a digital voice recorder (Olympus DS-330). The anonymous files were downloaded to the hospital server and routed via a secure file transfer protocol (FTP) to a transcription centre in Bangalore, India. Although the standard turnaround time was 24 hours, the system could accommodate a four hour turnaround time if requested. The transcription was routed back to the hospital for storage, merged with patient demographics on the hospital electronic patient record (EPR) (Cerner Corporation, USA). Transcriptions were checked, errors were noted and corrected, and the transcription approved. Transcriptions could be sent by letter or by email to multiple recipients.
Results: 574 transcriptions were sent through the system (June 2005–October 2005. Clarity of dictation was excellent in all cases and 100% transcriptions were processed within prescribed times with no files lost. Interface with the EPR was successful. The overall error rate in the transcribed files was 1.9% and the errors were minor.
Conclusion: Digital dictation and international outsourcing of transcription is an effective and viable method. The procedure leads to production of more accurate transcriptions, significantly faster turnaround, and allows dictations to be sent to multiple recipients.
355 HOW ACCURATE IS A CLINICAL “HUNCH” AFTER THE FIRST CONSULTATION IN GASTROENTEROLOGY?
S. Amin, N. van Someren, K. Besherdas, S. D. Mann.Department of Gastroenterology, Chase Farm Hospital, Middlesex, UK
Background: The NHS is under increasing pressure to cut costs and process patients as quickly as possible. Investigations focused on the initial working diagnosis are likely to be cost effective if the clinical “hunch” is accurate.
Aim: To review the accuracy of the first working diagnosis.
Method: Consecutive new patients referred to Gastroenterology outpatient clinics (NVS, KB, SM) were given a working diagnosis (12 categories) following the consultation. Diagnoses were re-analysed after appropriate investigations and non-parametric analysis was used to evaluate any associations.
Results: Data were available for 154 patients (female = 78 (51%)). 95% of the initial diagnoses were the same as the final diagnosis following a diagnostic work-up (χ2 = 16.93 (n-1) < p0.05 = 19.6).
Conclusion: Our initial “hunch” in outpatients is accurate in more than 95% of cases. This is very reassuring and suggests that tests can usually be targeted at confirming the diagnosis avoiding unnecessary follow up appointments which may generate further investigations. We acknowledge that there will always be a few patients who are challenging and do not fit into an obvious diagnostic category.
Abstract 355
356 ONE YEAR PROSPECTIVE AUDIT OF GASTROENTEROLOGY REFERRAL DEMAND TO A LONDON DISTRICT GENERAL HOSPITAL
N. U. Beejay1, R. Younis2, M. Guinane1, V. Kulhalli1.1Department of Gastroenterology, Newham Healthcare NHS Trust, Glen Road, London, E13 8SL; 2Newham PCT, Appleby Health Centre, Appleby Road, London E13 6LQ, UK
Background: Effective gastroenterology (GI) service provision depends on an accurate evaluation of demand, capacity, and activity. The understanding of the relationships between these factors is complex. GI demand at our hospital can be divided into inpatient, outpatient, and direct access endoscopy. Matching these factors is vital in assessing the effectiveness of GI service provision.
Methods: Prospective data on outpatient GI referral activity were systematically collected from January to December 2004. Numbers of referrals to Gastroenterology from each GP practice were divided into the following categories: Upper GI (UGI), Lower GI (LGI), Liver (L), Rectal Bleeding (RB), Direct Access Endoscopy (DAE) for upper endoscopy, and Others (O). The number of DAE was compared with total number of outpatient upper endoscopies. Summary statistics were calculated.
Results: 2362 referrals were made over the year: UGI (714), LGI (510), L (229), RB (49), DAE (740), Other (120). DAE comprised 47% of all upper endoscopies (740/1579). Monthly analysis demonstrated that demand variation was driven by DAE rather than consultant-led outpatient demand for upper endoscopy. Only 306 C13 urea breath test were performed suggesting that GP adherence to NICE dyspepsia guidance was poor. GP practice referral variation was marked: DAE (0–65), total referrals ((1–118) despite correcting for the size of the adult list of each practice.
Conclusion: There is marked variation (corrected for the list demographics) in the GP practice referral patterns to GI outpatients and through DAE. Investigation into the reasons for the demand variation may help in reducing demand, and matching with activity and capacity.
357 RATIONALISING THE MANAGEMENT OF BARRETT’S OESOPHAGUS: A DISTRICT GENERAL HOSPITAL AUDIT
F. Khan, C. B. Summerton, N. Haboubi.Trafford Healthcare NHS Trust, Moorside Road, Davyhulme, Manchester M41 5SL, UK
Introduction: The BSG have recently published Guidelines for the Management of Barrett’s oesophagus. It has been our practice to undertake annual endoscopic surveillance on patients with this condition. We conducted an audit on all such patients, with a view to modifying their management in accordance with the BSG Guidelines
Method: We conducted a retrospective case note audit for all patients in our surveillance programme for Barrett’s oesophagus. Patient details, together with the findings from previous endoscopies and histology results were carefully reviewed and recorded on an audit template. Two independent consultants in histopathology reviewed the biopsies of all patients with a previous report of dysplasia. Two separate clinicians independently appraised the appropriate management plan.
Results: A total of 55 patients were subjected to audit review. There was a male predominance (72%). Median age was 66. This group had together experienced a total of 140 endoscopic examinations. However, in only 54% of these procedures had quadrantic biopsies been taken according to BSG Guidelines. In patients deemed to have had adequate biopsies, there were reports of dysplasia in six patients (8%). On formal review, dysplasia was excluded in one patient. In the group of patients with inadequate biopsies, dysplasia was noted in only one report out of 60 (2%). In terms of clinical management, 23 patients (42%) were changed from yearly to two-yearly surveillance. Five patients were placed on six-monthly surveillance, due to the confirmation of low grade dysplasia. Seven patients (13%) had never had an acceptable surveillance examination, due to inadequate biopsy protocol. Eight patients (15%) were withdrawn from surveillance due to age and medical fitness.
Conclusion: In our hospital, the audit revealed a variety of practice, reflecting the lack of previous UK Guidelines. Implementing the BSG Guidelines in our hospital will reduce the number of OGDs being performed. Even following the recommended biopsy protocol, there will still be a decrease in overall samples being sent to histopathology. Audit is a useful tool to modify patient management in this area.
358 THE IMPACT OF THE EUROPEAN WORKING TIME DIRECTIVE ON THE CLASSIC GASTROENTEROLOGY FIRM: END OF AN ERA
G. T. Foley, F. Bhatti, S. Khan, N. Chiang, S. Moreea (introduced by C. G. Beckett).Department of Gastroenterology, Bradford Hospitals Trust, Duckworth Lane, Bradford BD9 6RJ, UK
Background: To comply with the European Working Time Directive most units have a full shift pattern consisting of weeks of nights, weeks on the acute Medical Admissions Unit (MAU) interspersed by weeks on the “Gastroenterology Firm” wards. As the workforce hasn’t increased to match the reduction in working hours there are fears relating to training, specially of the SpR grade, and of the care provided to patients by the traditional gastroenterology firm.
Aim: To audit the effect of a full shift pattern on the classical Gastroenterology Firm consisting of a Consultant, a Specialist Registrar (SpR), a Senior House Officer (SHO), and Pre Registration House Officer (PRHO) and to determine its implications in relation to service commitment, teaching and training.
Method: Between 4 February 2005 and 2 August 2005 the following were recorded for all the junior members of the team: night shifts, shifts on the Acute Admissions Unit, annual leave, study leave, recuperation time post nights as well as leave for any reason (for example, paternity leave).
Results: Over a period of six months, there were 129 week days. The Firm was present in its entirety (SpR/SHO/PRHO) in 23.3% of the time (30 days). There were no juniors on 11 days (8.5%). The percentage of the week day time on the wards was as follows: SpR/SHO 15.5%, SpR/PRHO 10.9%, SpR alone 7.8%, SHO/PRHO 11.6%, SHO alone 13.2%, and PRHO alone 9.3%. The SpR spent 15 nights on the MAU, 3 days of recuperation, 33 days of annual/paternity/sick leave, 4 days of study leave. The SpR had an equivalent of 14 weeks with the consultant for clinics and endoscopy sessions (54% of the time) and the SHO 11 weeks (42%).
Conclusion: The full shift pattern has a detrimental effect on the classic Gastroenterology Firm. Wards are understaffed and the SpR, when alone with the PRHO, has to sacrifice endoscopy training sessions. Training is compromised for a number of reasons: the same teaching has to be repeated as different members of the team are present on ward rounds at different times. The SHO and SpR do not get enough exposure on the wards, in clinics, and in endoscopy. We need to reassess these issues with the introduction of the Foundation Programmes and find a solution before training becomes suboptimal.
359 TRAINING AND USE OF ULTRASOUND BY GASTROENTEROLOGISTS TO IMPROVE SAFETY AND CONSENT IN PERCUTANEOUS LIVER BIOPSY
D. H. Dewar, J. S. Fraser, J. O’Donohue, A. Leslie, D. Reffitt.University Hospital Lewisham, London, UK
Background: Histological analysis of liver tissue remains the gold standard for diagnosis and staging of liver disease. The indications for liver biopsy are often complex and the procedure itself carries a significant risk of serious complications. Traditionally percutaneous biopsy is performed either blindly with the use of landmarks, or by radiologists with the help of ultrasound guidance. There is conflicting evidence regarding the comparative safety of these techniques. Radiologists may find it difficult to address the indications and benefits of obtaining a liver specimen during informed consent. Furthermore, in our institution we had noted a high rate of complication in a series of blind liver biopsies (16%) and elected to alter our protocol.
Methods: We describe a novel protocol for percutaneous liver biopsy. It was decided that all liver biopsies should continue to be performed by the gastroenterologists but using ultrasound to locate a safe site prior to biopsy. Respective gastroenterologists received supervision and training in basic liver ultrasound, until such time as they were deemed competent to independently locate a safe site. The actual biopsy and aftercare remain unchanged as a daycase procedure. We retrospectively examined the logistics and safety of this protocol.
Results: Over a three year period, 117 liver biopsies were performed using this protocol. Only patients with diffuse liver disease were included and no targeted biopsies were performed. The mean age of patients was 48 (23–70) years. The main indications for biopsy were assessment of non-alcoholic fatty liver disease (32.5%), abnormal liver function tests (18.4%) and hepatitis C assessment (14%). One complication occurred during the study period (0.87%). This patient was admitted to hospital with haemobilia four days after liver biopsy.
Conclusion: We believe that the use of ultrasound before liver biopsy by gastroenterologists is practical and safe, particularly in avoiding the inadvertent puncture of other viscera. This technique also ensures that the clinician can explain the clinical indication during consent.
360 FACTORS ASSOCIATED WITH SUCCESSFUL DAY-CASE ERCP: A 12 MONTH AUDIT AT A TERTIARY REFERRAL CENTRE
A. Hurst, K. Bodger, A. Byrne, R. Sturgess, S. Sarkar.Aintree Centre for Gastroenterology, University Hospital Aintree, Liverpool, UK
Introduction: The potential morbidity and mortality from ERCP is well recognised. Many ERCPs are performed in hospitalised patients (for example, to relieve obstructive jaundice) but day-case ERCP (DC-ERCP) is possible for less acute indications and is potentially more cost effective than elective hospital admission. Identifying in advance whether an individual patient is suitable for DC-ERCP or is at risk of an unplanned readmission following the procedure is difficult.
Aim: To determine whether there are demographic, clinical or procedure related factors that identify risk of unplanned hospitalisation following DC-ERCP.
Methods: Between 01/08/03 and 30/07/04, 92 DC-ERCPs were performed (23.2% of total ERCPs in that period), of which 91 were retrospectively audited using a standard proforma. Patients requiring unscheduled ward transfer after ERCP or hospital readmission within 30 days were identified using hospital IT system.
Results: Mean age (SD) was: 66.1 (17.1); 59.3% female. 29.7% (27/91) patients needed hospitalisation. There were no differences in age (63.3 (21) and 67.2 (15); p = 0.84), gender (p = 0.9), comorbidity (p = 0.9), or the presence of a trainee (34% v 43%; p = 0.84) between hospitalised patients (HOS) and non-hospitalised patients (non-HOS). There were trends towards more hepato-biliary-pancreatic (HPB) malignancies (27% v 10.8%; p = 0.16), less stone disease (38 v 52%; p = 0.16) and biliary leaks (7.8 v 0%; p = 0.07) in the HOS compared to the non-HOS. There was a difference in stent insertion (ST) (38.5 v 17%; p = 0.02), but not spincherotomy/pre-cut (54 v 43%; p = 0.4)) or mechanical lithotripsy(p = 0.9). Further analysis of ST suggested de novo ST rather than repeat ST was a risk factor (p = 0.07) for HOS. Post procedure symptoms were a good predictor of HOS (54 v 3%;p<0.001). Overall, the pancreatitis rate was 4.3% and commonest reason for admission was pain and nausea/vomiting. There were no fatalities.
Conclusions: Unexpectedly, age, comorbidity, or presence of a trainee were not predictors of hospitalisation after planned DC-ERCP. Diagnoses such as HPB malignancies and biliary leaks were more prevalent in the hospitalised patients. The best predictors of hospitalisation were the need for a stent (particularly de novo) or post-procedure symptoms. Whereas the former can occasionally be anticipated, the latter cannot. This audit further highlights that for ERCP, it remains difficult to identify patients that would be suitable for a successful day-case procedure.
361 DIAGNOSIS AND MANAGEMENT OF SUSPECTED COMMON BILE DUCT STONES IN PATIENTS FIT FOR CHOLECYSTECTOMY: A SURVEY OF FIVE UK REGIONS
E. J. Williams.The Steering Committee, BSG audit of ERCP, British Society of Gastroenterology, 3 St Andrews Place, London, UK
Introduction: The role of ERCP is changing with the advent of competing technologies such as endoscopic ultrasound (EUS), magnetic resonance imaging (MR), and laparoscopic common bile duct exploration (LCBDE). We aimed to establish how clinicians in English hospitals currently manage patients with suspected common bile duct stones (CBDS).
Methods: In 2004, 66 ERCP units from five English regions participated in the BSG audit of ERCP. In a separate questionnaire lead endoscopists were asked how their unit would manage the following: “A fit 60 year old patient with a history of abdominal pain is scheduled for laparoscopic cholecystectomy. Bilirubin = 25 μM, though the patient has never been jaundiced or septic. Alkaline phosphatase is ×2 the upper limit of normal. Ultrasound shows a calculous gallbladder and non-dilated common bile duct with no obvious ductal filling defects.”
Results: Responses were received from 44/66 (67%) of units. The most likely next investigation for such a patient was MR in 17/44 (39%), preoperative ERCP in 9/44 (21%), EUS in 5/44 (11%), intraoperative cholangiogram (IOC) in 4/44 (9%), and CT in 1/44 (2%), with 8/44 (18%) of units indicating a number of strategies were equally likely. Only 6/44 (14%) of units never used MR or EUS to investigate such patients though 15/44 (34%) reported inadequate access to these tests. Where stones were confirmed the most likely form of management was preoperative ERCP in 39/44 (89%) of units, with the remaining 5/44 (11%) of units using a combination of approaches. In total 29/44 (66%) of units indicated there was no possibility of LCBDE being used to treat CBD stones in such a patient.
Conclusion: Despite the attendant risks a significant number of UK hospitals continue to rely on ERCP to investigate patients with a low to intermediate probability of CBD stones. Access to MR and EUS needs to be widened and units should also consider the alternative strategy of IOC with selective postoperative ERCP. Despite published evidence of efficacy, LCBDE was unavailable in most of the hospitals surveyed.
362 USE OF SOLUBLE TRANSFERRIN RECEPTORS IS A VALUABLE, RESOURCE-SPARING TOOL IN IRON DEFICIENCY DIAGNOSIS
A. Koulaouzidis1, G. Leontiadis1, J. Singh1, G. P. Summerfield2, A. Saeed (introduced by B. Linaker)1.1Gastroenterology, 2Haematology- Queen Elizabeth Hospital, Gateshead, UK
Introduction: Anaemic patients, with normal MCV and ferritin, are often overinvestigated with endoscopic procedures. However, the ratio of sTfR/loge ferritin is a useful tool in discriminating iron deficiency anaemia (IDA) from other types of anaemia.
Aims and Methods: (1) To implement a protocol, using sTfR/loge ferritin ratio, in order to improve diagnosis of iron deficiency (ID) in those referred with anemia. (2) To assess the impact of this protocol on the workload of the Endoscopy Unit of a busy DGH and on the overall service delivery. Between June and December 2004, 30 patients referred with normocytic anaemia to our DGH were included in the study. All patients had ferritin and sTfR estimated on the first outpatient clinic visit. The BSG (British Society of Gastroenterology) guidelines for IDA were followed.
Results: Of thirty patients studied (mean age 70.3 years), eight had ferritin <30 μg/l, thus had further investigations for IDA. Ten patients had ferritin >100 μg/l, making ID unlikely according to BSG guidelines, and were not candidates for endoscopic investigations. Of the remaining 11 patients with ferritin values between 30 μg/l and 100 μg/l, seven had ratio >2 and were investigated, while one had ratio <1 and was not investigated according to the protocol. Three had ratios between 1 and 2, possibly necessitating investigations if they responded to iron. We found 610 patients on our DGH’s endoscopy register having procedures performed under the indication of “anaemia”. If our results above were applied, 154 patients belong to groups where ID could be excluded using the protocol based on sTfR (a single test costs £8; overall cost: £1232). Bidirectional endoscopies would have cost £123,000.
Conclusion: The use of sTfR is strongly recommended as a first line test in patients with of normocytic anaemia and normal ferritin. It can improve patient care by increasing the diagnostic yield of endoscopic tests and spare the inappropriate use of these valuable resources.
363 CLOSTRIDIUM DIFFICILE TOXIN POSITIVE DIARRHOEA IS A PREDICTOR OF MORBIDITY AND MORTALITY RATHER THAN A CAUSAL FACTOR
T. Wingfield, K. Law, K. Bowering, W. Azim, A. Byrne, K. Bodger, S. Sarkar.Aintree Centre Gastroenterology, University Hospitals Aintree, Liverpool, UK
Introduction: The incidence of clostridium difficile toxin (CDT) associated diarrhoea is rising throughout the NHS and is now the commonest hospital acquired infection. It is of considerable financial burden to the NHS due to the significant associated morbidity and mortality. University Hospitals Aintree (UHA) is a large teaching hospital, where the incidence of CDT at varies between 30–90 case per month with a general upward trend.
Aim: To determine the risk factors for the morbidity and mortality of CDT.
Methods: 105 episodes in 87 patients case notes in a three consecutive months period (01/10/04 to 01/01/05) were audited after being identified from the microbiology database of CDT positive stool samples. In all fatalities, the death certificates were used to verify the cause of death.
Results: 62% patients were female. The mean age (SD) was 77 (15). 75% of patients were elderly (>65) and 77% had multiple comorbidity. The average length of stay (LOS) was 22 days with 26.4% having LOS>60 days. The mortality was high at 43% (n = 37). Analysis between the patients that lived (LIV) and those that died (DIE) revealed no differences in the male to female ratio, blood parameters of CRP, haemoglobin, white cell and platelet count, antibiotics exposure, immunosuppressant, receipt of suboptimal treatment, or recent hospital admissions (p>0.05 all). The DIE had an increase frequency of previous diagnosis of CDT (13.6 v 6%) and multiple comorbidities (86.5 v 66.5%; p = 0.3). However, the DIE were older (81.5 v 74.2; p = 0.005) and had a lower serum albumin (25 v 29; p = 0.02). Cardiorespiratory disease (60%) and malignancy (19%) accounted for the majority primary causes of death. CDT was mention the primary cause of death only once (2.7%) and as a contributor in 6 (16.2%). The average age of these patients were 83 (range 74–95).
Conclusions: CDT is of significant cost to the NHS given the long LOS involved. However, this is probably due to the high prevalence of elderly patients with multiple comorbidities. The surprisingly high mortality in patients with CDT, is likely to be a reflection of the patients general illness (very elderly patients with multiple comorbidities and hypoalbuminaemia) rather than a direct causal effect of CDT itself. This may help explain the increase incidence of this infection given that the NHS is dealing with an increasing aging population.
364 IS CONSCIOUS SEDATION PRACTICED SAFELY IN PATIENTS UNDERGOING COLONOSCOPY?
G. Sisson, A. W. Harris.Kent Sussex Hospital, Tunbridge Wells, Kent, UK
Background: Diagnostic and therapeutic colonoscopy is a common procedure and requires patients to have conscious sedation. The procedure itself is relatively safe with an overall mortality of less than 1% (http://www.ncepod.org.uk). However, the sedation practice of endoscopists differs significantly and oversedation may be putting patients at excess risk particularly in the elderly (⩾70 years).
Aims: To compare the sedation practices of endoscopists performing colonoscopy at a district general hospital.
Methods: All patients undergoing colonoscopy during July and August 2005 were identified retrospectively using the computerised endoscopy reporting database and cross referenced with the endoscopy appointment diary. We considered safe conscious sedation practice as intravenous doses of 5 mg midazolam and 50 mg pethidine in patients aged under 70 and 2.5 mg midazolam and 25 mg pethidine in patients aged ⩾70 years.
Results: 12 endoscopists performed a total of 273 colonoscopies during the study period. The mean number of colonoscopies per endoscopist was 23 (range 2–64). The patients mean age was 64 (range 18–91); there was no significant difference in the patient’s mean age between endoscopists (average range 58–70). 40% (n = 110) of colonoscopies were performed in patients aged ⩾70 years (mean age 79, range 75–78). The modal sedation dose was 5 mg midazolam (range 2.5–15 mg) and pethidine 50 mg range (25–100 mg). Using our criteria 43% of all patients (n = 118), 18% (n = 30) in the under 70s and 80% (n = 88) of the ⩾70 years received more sedation than recommended; two patients required flumazenil and/or naloxone to reverse sedation.
Conclusion: Our findings raise concern regarding our use of sedation in the elderly and following the NCEPOD report on endoscopy changes in practice are required. A further audit will be performed six months after these results are discussed with our colleagues.
Acknowledgements: We thank the endoscopy unit administration staff for their help with date collection.
365 THE TWO WEEK RULE FOR COLORECTAL CANCER: EXPERIENCE OF A NURSE LED FLEXIBLE SIGMOIDOSCOPY CLINIC IN PRIMARY CARE
K. Maruthachalam1, E. Stoker2, G. Nicholson2, A. F. Horgan1.1Department of Colorectal Surgery, Freeman Hospital; 2Department of Endoscopy, Freeman Hospital, Newcastle upon Tyne NHS Trust, NE7 7DN, UK
Background: A nurse led flexible sigmoidoscopy clinic was established in a primary care setting to meet the increased demand generated by the lower GI two week rule.
Aim: To establish a protocol driven clinic in the community that would reduce the time to investigation and facilitate the pathway for patients referred for flexible sigmoidoscopy.
Methods: Prospective study of all patients referred under the lower GI two week rule to the community flexible sigmoidoscopy clinic from March 2004 to June 2005. Follow up was protocol based. Patients diagnosed with colorectal cancer were placed on a fast track pathway for further imaging.
Results: 1000 patients underwent flexible sigmoidoscopy in primary care from March 2004 to June 2005. 96 (9.6%) patients were investigated following referral under the two-week rule for colorectal cancer. The median age was 58 years (22–77). The median time to Flexible sigmoidoscopy was 12 days (4–48). Two patients were referred after an initial outpatient visit and 94 patients were investigated directly in primary care. 27 (28%) patients had a normal study. 24 (25%) patients were diagnosed with significant colonic pathology including nine (9%) patients with colorectal cancer. 53 (55%) patients underwent further imaging of their colon either in the form of a colonoscopy or barium enema. 28 patients were referred for outpatient follow up and 11 for other investigations. No complications have been encountered.
Conclusions: A nurse led flexible sigmoidoscopy clinic in primary care can provide a safe diagnostic service for patients referred under the two week rule. The use of protocols enables experienced nurses to refer patients for further investigations and safely discharge patients back to the community.
366 SURVEILLANCE COLONOSCOPY: DO THE BRITISH SOCIETY OF GASTROENTEROLOGY GUIDELINES CHANGE CLINICAL PRACTICE?
P. Sakellariou, G. Thompson, M. T. Donnelly, S. Johal.Northern General Hospital, Herries Road, Sheffield S5 7AU, UK
Aim: To asses the implementation of the British Society Guidelines (BSG) recommendations for “colorectal cancer screening in high risk groups” for patients awaiting surveillance colonoscopy at the Endoscopy Unit of a Teaching Hospital over a period of 12 months.
Method: Case note review was performed for patients due to undergo surveillance colonoscopy over 12 months and the BSG guidelines for “colorectal cancer screening in high risk groups” (October 2002) were used to validate patients on the waiting list.
Results: The case notes of 193 patients on the surveillance colonoscopy waiting list from July 2004 to July 2005 were reviewed. The median age (range) was 58 (29–83) and 97 (50.2%) patients were male. We were able to cancel or delay the colonscopy in 85 (44%) patients, with 48 (25%) patients being removed from the waiting list and 37 (19%) patients having their colonoscopy delayed. In this latter group of 37 patients who either had colonic polyps or a positive family history of colonic carcinoma, surveilance had been arranged earlier than advised by the BSG guidelines. It was also of note that 10 (5.1%) patients had their colonoscopy brought forward and six (3%) patients’ families were referred for genetic advice. The reasons identified for removing patients from the waiting list included: inappropriate polyp follow up, deterioration of general health, and calculation of lifetime colorectal cancer risk lower than 1:10.
Discussion: With the pressure on endoscopy waiting times and the potential impact of colorectal cancer screening, validation of waiting lists using the BSG guidelines may prevent large numbers of patients from having an inappropriate or mistimed colonoscopy.
367 RATIONALISING COLONOSCOPY REFERRALS: AN AUDIT OF COLONIC POLYP SURVEILLANCE IN A DISTRICT HOSPITAL
F. Munir, C. B. Summerton.Trafford Healthcare NHS Trust, Moorside Road, Davyhulme, Manchester M41 5SL, UK
Introduction: In 2000, the BSG produced guidelines detailing an appropriate follow up strategy for patients found to have adenomatous polyps within the colon. We became aware that a number of patients in our unit had been booked for examinations, which did not accord with these recommendations. In the light of this observation, we conducted an audit of patients waiting for surveillance colonoscopy, in order to review their treatment plan and modify this if appropriate.
Method: We conducted a retrospective case note audit for all patients due to undergo surveillance colonoscopy in the six month period from January 2005 to July 2005. Patient details, together with the findings from previous endoscopies and histology results were carefully reviewed and recorded on an audit template. Two separate observers, drawing from the published BSG Guidelines, independently appraised the appropriate management plan.
Results: A total of 111 case notes were reviewed. Out of this group, 39 patients were being followed up because of previous adenomatous polyps. On applying BSG guidelines, 25 patients (64% of the total) needed a change in their management plan. Nine patients (23%) needed no further follow up. In 11 patients (28%), the endoscopy interval was increased from three to five years. In contrast, four patients were noted to have indications for more frequent surveillance and one patient had been inappropriately booked for a sigmoidoscopy rather than colonoscopy.
Conclusion: In this six month audit, we changed the surveillance plan in a large proportion of our patients. This produced a considerable saving of endoscopy resources and contributed positively to patient safety, through reducing inappropriate examinations. This accords with similar findings reported from other endoscopy units. We would recommend that such audits be conducted on a regular and repeated basis, to avoid inappropriate referrals and to reduce endoscopy waiting times. This would address past clinical decisions. There is also a challenge to educate all endoscopists in the use of current guidelines.
368 NURSE LED INFLAMMATORY BOWEL DISEASE TELEPHONE HELP DESK: IMPACT ON CLINICAL MANAGEMENT AND PATIENT SATISFACTION
A. Saleem, A. K. Awasthi, F. Fry, T. Shirazi, T. K. Daneshmend.Royal Devon and Exeter Hospital, Exeter, UK
Introduction: The role of nurse specialists in management of inflammatory bowel disease is evolving. There is little evidence that it has an impact on hospital admissions, out patient appointments or patient satisfaction.
Aims: To evaluate the impact of nurse led inflammatory bowel disease (IBD) help desk on (1) the number of hospital admissions, (2) outpatient appointments, and (3) patient satisfaction from the service.
Method: The study was based in our hospital where the IBD help desk was established in August 2001. The patients who used the service between April 2004 and March 2005 (12 months) were identified from a call log book. The reason for the call and advice given were recorded. If a treatment was initiated on telephone advice it was considered to have saved an out patient appointment. A comparison of hospital admissions due to inflammatory bowel disease flare-ups was made between the study period and a similar 12 month period (April 2000 to March 2001) prior to the help desk being established. A questionnaire was sent to all patients who used the service during the study period.
Results: 234 patients made 836 calls. General practitioners made 10 calls. There was no reduction in the number of admissions (122 in study period v 106 in control period). However 87 potential outpatient appointments were saved. 111 patients responded to the questionnaire. Among them 78.30% believed that help desk avoided the need to see a doctor and 59.43% agreed that continuity of care was better than out patient appointments alone. Overall quality of service was judged excellent or good by 90.56% of respondents.
Conclusion: A nurse led IBD help desk provides high level of patient satisfaction. It can potentially save outpatient appointments but has no impact on hospital admissions.
369 ASSESSMENT OF GENERAL PRACTITIONER ATTITUDES TOWARDS MONITORING THIOPURINE THERAPY IN INFLAMMATORY BOWEL DISEASE PATIENTS
E. Wood, L. Medcalf, S. McCartney.Department of Gastroenterology, Middlesex Hospital, UCLH NHS Trust, Mortimer Street, London W1T 3AA, UK
Introduction: Audit of our practice has shown that general practitioners (GPs) monitor 6.7% of inflammatory bowel disease (IBD) patients taking thiopurine (azathioprine (AZA) or mercaptopurine (MP)) therapy yet a larger proportion of patients wish to have monitoring at their GP surgery. By assessing GP attitudes we hope to offer a solution which supports GP monitoring of AZA and MP.
Method: All IBD patients taking thiopurine therapy were identified over a six month period (October 04–March 05) and their GP’s attitudes assessed by a postal nine point “yes/no” questionnaire which included a free text ‘comments’ section.
Results: Ninety patients were identified. At the outset 78/90 and 12/90 patients were taking AZA and MP respectively. Questionnaire responses were obtained from 81/90 (90%) GPs and were thus felt to be representative of local opinion. Of responding GPs, 42% (34/81) agreed that they would be happy to monitor patients on AZA/MP increasing to 49.4% (40/81) if supplied with the department’s monitoring protocol. However, analysis of the “comments” section indicated that 29.6% (24/81) of respondents would monitor without any caveats whilst 19.8% (16/81) would only monitor if either; a protocol, named contacts and telephone numbers were provided per patient (7.4% (6/81)), further funding was provided (7.4% (6/81)), the patient was on AZA (2.5% (2/81)) or on maintenance therapy (2.5% (2/81)).
Conclusion: Our assessment of GP attitudes indicates that whilst only 6.7% are currently monitoring patients taking AZA/MP almost 30% of responding GPs would be happy to monitor patients without any caveats. By providing GPs with the department’s monitoring protocol and, in the event of an emergency, named contacts and telephone numbers for each patient taking maintenance therapy this can be increased to almost 40% (32/81). We plan to implement these changes and re-audit to assess if GP monitoring of AZA/MP has increased.
370 DO PATIENTS ATTENDING A COLORECTAL CLINIC PREFER TO SEE A DOCTOR OF THEIR OWN SEX?
T. D. Pinkney, A. Menon, S. Beraldo, B. Perakath, M. R. B. Keighley.Academic Unit of Surgery, University Hospital Birmingham, UK
Introduction: Patients with colorectal symptoms find it embarrassing to discuss their symptoms and be examined. Our aim was to determine if such patients in our multicultural society preferred to be seen by a doctor of their own sex and whether there is a need for more female colorectal surgeons.
Method: A pre-consultation questionnaire was distributed to patients attending colorectal clinics over 14 months. The data were analysed for patient demographics, presenting symptoms and their gender preference for the doctor they were to see.
Results: 626 patients (59% female) completed the questionnaire. 27% of males and 31% of females expressed a mild preference in the sex of the doctor they were to see, these numbers falling to 14% and 15% respectively for those with very strong feelings on the matter. Multiple statistical analyses were performed to identify any individual patient groups who were more likely to express a preference—the predominant ones found were Muslims patients of both sexes (males p⩽0.001; females p⩽0.01). Overall on questioning, 22% of patients did not want to see any trainee in clinic and 23% did no want to see a medical student.
Discussion: A significant proportion of patients attending a colorectal clinic had an opinion regarding the sex of the doctor they were to see, and Muslims were particularly concerned about this issue. This information has strong implications when planning provision of coloproctological services, particularly the potential need for more female surgeons in areas of high Muslim population density.
371 AUDIT OF INFLAMMATORY BOWEL DISEASE CLINICS: RESULTS FROM TWO PATIENT SATISFACTION SURVEYS
K. L. Robinson, A. J. Elsender, M. C. Gunn, J. C. Mansfield.Royal Victoria Infirmary, Queen Victoria Road, Newcastle upon Tyne NE1 4LP, UK
Background: British Society of Gastroenterology guidelines for the management of inflammatory bowel disease (IBD) emphasise the importance of considering “patient driven criteria” when auditing quality of care.1
Aims: To examine patients’ views about IBD outpatient clinics, to identify problems associated with clinic attendance or clinic facilities, and to assess patients’ usage of direct access to hospital care.
Methods: Interview based audit (Audit A) of 40 patients attending IBD outpatient clinics in 2005 and questionnaire based audit (Audit B) of 40 patients who attended the same clinics in 2004.
Results: Participation rates were high, exceeding 95% in both audits. Interviewees (Audit A) gave a mean score of 8.9 out of 10 (range 6–10) for overall clinic satisfaction, and also valued highly the availability of direct access to hospital-based care (mean score 9.3 out of 10, range 5–10). Lengthy waiting time at clinic was the most commonly reported problem (47.5%), but most of those reporting this problem (94.7%) indicated that shorter waiting times at the expense of direct access would not be acceptable. High numbers of the interviewees (80%) also indicated that the provision of more information on IBD at clinics would be useful. All questionnaire respondents (Audit B) rated overall satisfaction with outpatient clinics as good or excellent. These patients generally viewed waiting times of 40 minutes or more as unacceptable. Direct access to hospital based care by questionnaire respondents was used mainly in connection with disease flare-ups (71.4%) and/or to arrange a new appointment (42.9%).
Conclusions: Direct access to care was valued very highly and it was used most commonly in relation to disease flare-ups. Overall, patients viewed the IBD clinics positively.
1
372 NURSE LED METHOTREXATE SERVICE FOR PATIENTS WITH CROHN’S DISEASE: A 12 MONTH PROSPECTIVE AUDIT
C. Pearson, M. Meehan, K. J. Moriarty, K. Padmakumar, G. R. Lipscomb.Royal Bolton Hospital, Bolton, Lancashire BL4 0JR, UK
Background: We have introduced a dedicated nurse led clinic for methotrexate (MTX) administration. The audit examines the outcomes of patients with Crohn’s disease (CD) who attended a dedicated specialist nurse clinic for treatment, education and clinical review.
Methods: A drop-in clinic was established for patients requiring parenteral MTX. A Consultant Gastroenterologist reviewed each patient three-monthly. Protocols for the administration of MTX were developed in conjunction with a multidisciplinary team. Patient held records ensured effective communication between primary and secondary care. Protocols for patient education were adapted from the RCN rheumatology guidelines and agreed by the hospital trust board for use in patients with CD. A 12 month audit was undertaken, monitoring patients CD activity index (CDAI), outcomes of therapy and interventions undertaken in clinic. Consultant satisfaction was assessed using a questionnaire. A patient questionnaire was used to assess patients’ perceptions of the service.
Results: Eleven patients received MTX. All received IM MTX, 25 mg weekly for 12 weeks, administered and prescribed by a specialist nurse using supplementary prescribing. Of these, six converted to oral MTX and remained well. Four patients required long term parenteral MTX, and doses where adjusted to 15 mg. These patients were taught to self administer. One patient discontinued due to intolerance. At 12 weeks, CDAI had fallen from a mean of 308 to 212, and mean prednisolone dose from 36 mg to 12.5 mg. Consultants reported increased confidence in safe administration and monitoring of MTX. A patient questionnaire reported that a drop in clinic was an acceptable means of review, as they received emotional support from peers. Patients identified that a nurse specialist clinic reduced patient attendance, reduced waiting times, improved continuity, and increased satisfaction with care.
Conclusion: The development of a nurse led MTX clinic for patients with CD has facilitated a significant improvement in the overall quality of patient care.
373 TRAINEES IN GASTROENTEROLOGY VIEWS ON TEACHING IN CLINICAL GASTROENTEROLOGY AND ENDOSCOPY
S. Inglis, J. R. Barton.Northumbria Healthcare NHS Trust & University of Newcastle, North Tyneside Hospital, North Shields NE29 8NH, UK
Introduction: During the 2004 meeting of the British Society of Gastroenterology there were discussions in the Trainee in Gastroenterology meeting, regarding the quality of teaching, training and supervision. With the group, we surveyed all SpRs to obtain a wider perspective from the trainee body.
Aims: The questionnaire gathered data on the extent and quality of teaching, training, and supervision in outpatient clinics, on ward rounds and in endoscopy by procedure, as well as trainees’ teaching experience, training, and intentions to teach.
Methods: The questionnaire was pre-tested and piloted. The final document was sent out via the Trainees in Gastroenterology office using a private mailing company. All trainees who were in substantive training posts in England and Wales were included, approximately 500 SpRs. Only around 250 questionnaires were received by the trainees because of insufficient postage being franked on to the envelopes. 173 forms were returned. In view of the difficulties above, we felt that this was a representative sample.
Results: Of the trainees, 68/169 were never, rarely, or not often taught on ward rounds. 92/168 trainees “never, rarely, or not often” discussed new outpatients with the consultant, and only 13/170 trainees discussed review patients frequently or all the time. Although the quality of teaching was rated as “Quite good–Excellent” by 91/170, it was rated “so-so–very poor” by 79/170. Endoscopic supervision and training was inconsistent, with 76/170 being taught “frequently–all of the time”, 39 taught “about half the time”, and 53 “not often–never” for procedures in which they were still training. Trainees not fully trained in a procedure were being supervised by distant trainers.
Conclusions: Teaching and training in gastroenterology is very variable both in quality and quantity. Of particular concern, supervision for endoscopy is often inadequate or absent. There are many opportunities to improve our teaching and training in gastroenterology.
374 OPTIMISING TRAINING OPPORTUNITIES FOR A GASTROENTEROLOGY SPR IN A BRITISH DISTRICT GENERAL HOSPITAL
C. W. Wells, D. Ashley, M. D. Rutter, J. V. Metcalf, A. D. Dwarakanath.University Hospital of North Tees, Stockton on Tees TS19 8PE, UK
Background: The EWTD has reduced training time due to restructuring of on call rotas with compensatory time off. Recognising this we devised a prospective flexible timetable for the single SpR in our hospital to optimise training opportunities within a four consultant gastroenterology team.
Methods: An excel spreadsheet was created, dividing the working week into 10 sessions, covering the full 12 months. SpR absences due to days off post on call (total:8), days worked on MAU, SpR training sessions, study and annual leave, and consultant absences were identified and recorded on the spreadsheet in advance. In the available sessions left after taking these factors into account, two clinics, two endoscopy lists, and two ward rounds (one SpR led and one consultant led), were booked per week in a flexible manner. At the end of the year the number of days worked in gastroenterology was calculated and the numbers of clinics, endoscopy lists and ward rounds that actually occurred were recorded. The number of clinics, lists, and ward rounds that would have occurred had the SpR followed the previous year’s fixed timetable was also calculated.
Results: In 12 months 131 days (26.2 weeks) were worked by the SpR in gastroenterology. The SpR attended 57 clinics, 48 endoscopy lists, 36 consultant, and 33 SpR led ward rounds. Had the SpR followed a fixed timetable he would have attended 35 clinics, 42 endoscopy lists, 51 consultant led, and 25 SpR led ward rounds. There is a statistical difference between each figure (χ2 test p<0.05).
Discussion: In 12 months only 26 (5 day) weeks were spent doing gastroenterology as a result of the various absences. The EWTD has hence made training time a premium. Training centres, trainers, and trainees need to maximise training opportunities to allow SpRs to gain adequate experience. By adopting a flexible timetable we were able to significantly increase SpR training opportunities in endoscopy by 14%, clinic by 63% and SpR led ward rounds by 24%. The number of consultant led ward rounds was reduced but still over the one per week recommended by the JCHMT. A route to optimised SpR training?
Small bowel posters
375 ALTERATIONS IN HUMAN DEFENSIN-5 (HD-5) EXPRESSION FOLLOWING GASTRIC BYPASS SURGERY
D. A. Elphick1, M. Sundbom2, Y. R. Mahida1, R. N. Cunliffe1, T. Midtvedt3, L. Engstrand4, S. Gustavsson2, L-GAxelsson3.1Institute of Infection, Immunity & Inflammation, Univ Nottingham, UK; 2Deptartment of Surgery, University Hospital, Uppsala, Sweden; 3Cell and Molecular Biology, Karolinska Institute, Stockholm, Sweden; 4Swedish Institute for Infectious Disease Control, Solna, Sweden
Introduction: Roux-en-Y gastric bypass surgery provides a novel human model to investigate mucosal innate immunity, in which there is loss of gastric acid-mediated protection against orally-acquired microorganisms. We have studied changes in mucosal HD-5, which is an antimicrobial peptide normally produced by Paneth cells.
Methods: Mucosal samples were obtained from 18 female patients (24–54 years), from the same segment of jejunum during and after (at endoscopy) gastric bypass surgery. Samples were used for bacterial culture and immunohistochemistry using anti-HD-5 antibody. The number of immunoreactive cells per crypt and villus were determined and expressed as mean (SD)
Results: No bacteria were cultured from any of the perioperative jejunal samples but colonies of bacteria normally present in the pharynx were identified during culture of all postoperative jejunal biopsies (1–>100 colonies). Paneth cell numbers per crypt were unchanged after gastric bypass (4.16 (0.71) v 4.24 (0.78)). However, following surgery, there was an increase in: HD-positive intermediate cells per crypt (0.25 (0.41) v 1.12 (0.66), p<0.01), HD-5 staining enterocytes per crypt (0.31 (0.09) v 1.38 (1.10), p<0.01), HD-5 staining material in the crypt lumen (crypt lumens: 5.0 (10.9)% v 68.1 (27.9)%, p<0.01) and HD-5 immunoreactivity coating the luminal surface of villus enterocytes (villi sampled: 15.0 (31.0)% v 67.5 (42.0)%, p<0.01).
Conclusions: (1) Bacteria normally resident in the pharynx were present in the proximal jejunal mucosa following Roux-en-Y gastric bypass surgery. (2) After gastric bypass, there was increased secretion of HD-5 and an increase in HD-5 expressing intermediate cells and enterocytes in the crypt. (3) The increase in HD-5 expression in the jejunal mucosa following gastric bypass surgery is likely to be secondary to exposure to orally acquired microorganisms.
376 A PROSPECTIVE STUDY OF THE PREVALENCE OF EXOCRINE PANCREATIC INSUFFICIENCY IN PATIENTS WITH DIARRHOEA PREDOMINANT IRRITABLE BOWEL SYNDROME USING FAECAL ELASTASE-1
J. S. Leeds, A. D. Hopper, A. Simmonette, N. Azadbakht, S. Morley, D. P. Hurlstone, D. S. Sanders.Royal Hallamshire Hospital, Sheffield, UK
Introduction: Patients who meet the Rome II criteria for irritable bowel syndrome (IBS) may be found to have other underlying pathologies. Mild to moderate chronic pancreatitis may be under diagnosed. Previous evidence suggests that 20% of patients with IBS may have an abnormal triolein breath test suggesting pancreatic insufficiency. We wished to determine if exocrine pancreatic insufficiency may be present in patients who present with diarrhoea predominant IBS (D-IBS).
Patients and Methods: 294 consecutive patients referred to our unit meeting the Rome II criteria for D-IBS were assessed for evidence of exocrine pancreatic insufficiency using the faecal elastase-1 test (Fel-1). Baseline bowel frequency, stool consistency and weight were recorded. All D-IBS patients were investigated as per the British Society of Gastroenterology IBS guidelines (2000). Those patients with a pathologically low Fel-1 level (<100 μg/g stool) were offered pancreatic supplements and bowel habit and frequency assessed at six months. In this group the pancreas was also imaged using ultrasound or CT.
Results: 294 patients were included (median age 47 years, 84 males). 16 patients had a Fel-1 <100 μg/g stool (5.4%). Eight patients to date have been given pancreatic supplements. In this group the median number of stools per day reduced from 6 to 1.5 (p = 0.011). These patients also reported a marked improvement in urgency. There were no changes in weight. Other diagnoses in the remaining patients were D-IBS 80.3% (236/294), coeliac disease 6.1% (18/294), diverticular disease 2.4% (7/294), lactose intolerance 2% (6/294), thyroid dysfunction 1% (3/294), wheat intolerance 0.7% (2/294), IgA deficiency 0.7% (2/294), Crohn’s disease 0.3% (1/294), alcohol excess 0.3% (1/294), carcinoid 0.3% (1/294), and short bowel 0.3% (1/294).
Conclusion: The prevalence of a low Fel-1 in patients with diarrhoea predominant IBS was 5.4%. Patients report significant improvement in bowel habit and function on receiving pancreatic supplements. Routine testing use of Fel-1 in patients with D-IBS appears to be beneficial.
377 A NEUROPHYSIOLOGICAL STUDY IN COELIAC DISEASE
R. Hariraj, A. R. Tearle, J. Ray, R. Mathialagan (introduced by R. C. McGouran).Queen Elizabeth hospital, Kings Lynn, UK
Aim: To evaluate the incidence of subclinical neurological dysfunction in coeliac disease (CD).
Methods: Neurophysiological tests were done on a selection of CD patients who did not manifest any neurological abnormality. Electroencephalography (EEG), upper limb somatosensory evoked potential (SEP), visual evoked potential (VEP) and sural/radial amplitude ratio (SRAR) were performed. Patients also completed an “Epworth Sleepiness Scale” questionnaire to evaluate excessive daytime sleepiness (EDS). All had CD confirmed by serology and biopsy. EEG recording was for a minimum of 15 minutes employing hyperventilation and photic stimulation techniques. Two technicians reported EEGs “blind”. There were 14 patients, 12 were on gluten free diet, and two were not. Females were 12 and males 2. The mean age was 56.
Results: 74% had an EEG abnormality, 16% had a VEP abnormality, 6% had an SEP abnormality, 60% had SRAR abnormality, and 36% had abnormal Epworth scores. The EEG abnormalities in each case were sharp waves, largely localised. These are non-specific but may indicate subclinical neuronal dysfunction and a reduced seizure threshold. 50% of EEG abnormalities were focal to the left fronto-temporal region; remaining 50% were distributed between right frontal, right temporal, left occipital, and left posterior temporal regions. Among VEP abnormality, half showed unilateral slowing of the response (both on the right) and the other half showed bilateral slowing. SEP abnormalities included slowing at the cortical level, but the sample size is small to determine the relevance. SRAR testing indicated a 60% incidence of abnormal sural/radial amplitude ratio, reflecting the increased incidence of peripheral neuropathy in CD. Over a third, had Epworth scores to indicate EDS.But most were in the upper quartile for age, which probably accounts for this.
Conclusion: Clearly there are pointers to neurophysiological abnormalities in CD, which are not clinically manifest. Similar studies, both before and after a gluten free diet, are necessary to assess their sensitivity to gluten.
378 HIGH YIELD OF COLONOSCOPY IN INVESTIGATING COELIAC PATIENTS WITH DIARRHOEA
D. H. Dewar, M. W. Johnson, H. J. Ellis, P. J. Ciclitira.Department of Gastroenterology (GKT), Rayne Institute, St Thomas’ Hospital, London, UK
Background: Thirty per cent of patients diagnosed with coeliac disease (CD) continue to suffer symptoms despite a gluten-free diet. Diarrhoea is a common symptom. As colonoscopy is an invasive test it is important to exclude continued gluten ingestion. We report on the investigation by colonoscopy of individuals with CD who reported significant diarrhoea during follow up.
Patients: We reviewed patients with a diagnosis of CD seen in our centre over a 24 month period and identified those with a history of persisting diarrhoea, as defined by duration of greater than three months and bowel frequency in excess of three motions per day. We included all patients who had been investigated by colonoscopy and reviewed the reviewed the results of tests and diagnosis in each case.
Results: Eighty eight patients with coeliac disease reported significant diarrhoea and were investigated with a colonoscopy. Of these, 82 patients also underwent a repeat duodenal biopsy as part of their evaluation. Completed colonoscopy was performed in 84/88. Biopsy samples were obtained for analysis in 87/88 procedures. Seven patients had endoscopically detectable abnormalities (7.9%) with five cases of proctitis, one case of ulcerative colitis (UC), and one case of pouchitis in a patient who had previously had a colectomy for UC. Ten further cases of lymphocytic colitis (11.4%) were diagnosed on histological analysis of colonic biopsies. During other investigations, a cause for diarrhoea was identified in 89% of patients with the most significant diagnosis being continued gluten ingestion (50%). In performing 88 colonoscopies, pathology was identified in 17 patients (19.3%).
Conclusions: The quoted diagnostic yield for colonoscopy in any patient with diarrhoea is 6–10%. In our series, the diagnostic yield was 19.3% in coeliac patients with diarrhoea. The incidence of inflammatory bowel disease and microscopic colitis in coeliac disease appears to confirm the value of colonoscopy in investigating patients with coeliac disease who have continued diarrhoea while on a gluten-free diet.
379 IS THERE A RELATIONSHIP BETWEEN COELIAC DISEASE AND INFLAMMATORY BOWEL DISEASE? A BIDIRECTIONAL PREVALENCE STUDY WITH CONTROLS
B. S. Höroldt, J. S. Leeds, R. Sidhu, A. D. Hopper, K. Robinson, B. Toulson, A. J. Lobo, M. E. McAlindon, D. P. Hurlstone, D. S. Sanders.Royal Hallamshire Hospital, Sheffield, UK
Introduction: There are conflicting studies examining the relationship between coeliac disease and inflammatory bowel disease (IBD).
Aims: To determine the prevalence of coeliac disease in IBD and vice versa compared to healthy controls.
Patients and Methods: Patients were enrolled from the specialist IBD and coeliac clinic. Patients with IBD had blood taken for antigliadins, endomysial (EMA), tissue transglutaminase antibodies, and total IgA level. Patients with positive antibodies were offered duodenal biopsy. Patients with coeliac disease who had lower gastrointestinal symptoms had a colonoscopy and pan-colonic biopsies performed.
Results: 1170 patients were included; 305 with coeliac disease (222 females), 274 with IBD (165 females) and 591 healthy controls (361 females) with median ages 52, 43, and 45 respectively (p = <0.0001). Eight patients in the coeliac group were found to have coexistent IBD comprising four with UC, two lymphocytic colitis, one microscopic colitis, and one with Crohn’s disease. All eight had first been diagnosed with coeliac disease and IBD developed during follow up. The IBD group comprised 117 UC, 143 Crohn’s, 10 indeterminate colitis, and four microscopic colitis patients. 28 patients with IBD had positive antibodies of which 18 had UC, 12 Crohn’s, and one microscopic colitis (UC v Crohn’s p = 0.07). Of the 28 with positive antibodies only one patient had a positive EMA. Distal duodenal biopsy was performed on positive antibody patients and revealed coeliac disease in one patient (EMA positive). There was also one case of duodenal Crohn’s disease (IgG antigliadin positive only). Five controls had biopsy proven coeliac disease and two controls had IBD (1 Crohn’s and 1 UC). The prevalence of undiagnosed coeliac disease in IBD was 0.36% compared to 0.85% in controls (p = 0.43). The prevalence of IBD in coeliac disease was 2.3% compared to 0.34% in controls (odds ratio 7.9, 95% CI 1.67 to 37.59 p = 0.002).
Conclusions: Patients with coeliac disease had an ×8 increased risk of developing IBD during follow up compared to healthy controls. IBD patients had no increased risk of developing coeliac disease.
380 FREQUENCY OF DIAGNOSIS OF COELIAC DISEASE AND AGE AND SEX OF PATIENTS DIAGNOSED IN A SINGLE CENTRE 1975–2004
G. K. T. Holmes.Derbyshire Royal Infirmary, Derby DE1 2QY, UK
Aims: To determine the frequency of diagnosis of adult coeliac disease (CD) and the age and sex of patients diagnosed between 1975 and 2004 in a single centre.
Methods: The diagnosis of CD was based on characteristic small gut appearances of severe or total villous atrophy. Extensive efforts were made to identify all patients in the area served by the Derby hospitals. Sources of information included the hospital diagnostic index, histopathology records, dermatitis herpetiformis clinic, immunology laboratory, dietetic department, and membership lists of the Coeliac Society. Since 1978 patients have been followed prospectively in a weekly coeliac clinic run by the author. Information was stored on an Access database.
Results: Patients were diagnosed each year since 1975. Between 1975 and 2004, 994 patients were diagnosed. The numbers in successive quinquennia are shown (table). 12 times more patients were diagnosed per year in the last than the first quinquennium.
Abstract 380
Of the 994 patients, 678 (68%) were women (F:M ratio 2.15:1) With older age of diagnosis the ratio fell successively to 1.53:1 for those diagnosed over the age of 60 years. 286 (29%), 123 (12%), 36 (4%), and nine (1%) were diagnosed over the age of 60, 70, 80, and 85 years, respectively. One patient was diagnosed aged 92 years.
Conclusions: Approximately 12 times more patients with CD are now being diagnosed in Derby than in the later 1970s and about one third are now diagnosed over the age of 60 years and many well into old age. There is a preponderance of women particularly for those diagnosed under the age of 35 years.
381 THE NUMBER OF CANCERS ARISING TWO OR MORE YEARS AFTER THE DIAGNOSIS OF COELIAC DISEASE IS SMALL
G. K. T. Holmes.Derbyshire Royal Infirmary, Derby DE1 2QY, UK
Aims: To explore the numbers of cancers occurring in a large coeliac population accrued between 1958 and 2005 in a single centre. Selection bias was minimised because this cohort is representative of those patients seen in routine clinical practice.
Methods: The diagnosis of coeliac disease (CD) was based on small bowel biopsy appearances of severe or total villous atrophy. Extensive efforts were made to identify all patients in the area served by the Derby hospitals. Information on cancers arising in the group was obtained during clinical review, analysis of case notes available for all patients and comprehensive searching of the histological data base of the Derby hospitals. Cancers were classified as incident if these occurred two years or more after the diagnosis of CD. Cancers arising before the diagnosis of CD or within two years of the diagnosis of CD were regarded as prevalent. A dedicated weekly clinic for CD run by the author acted as a focus for care and research. Patients were followed prospectively from 1978. Those referred from other secondary care centres were excluded from consideration.
Results: Of 1146 patients with CD 115 (10%) developed malignancies. Of these, 57 were incident tumours while the remainder occurred either before (33) or within two years of the diagnosis of CD (37). A wide variety of cancers was encountered, mostly in small numbers. Of the cancers of interest in relation to CD only three oesophageal tumours were found all of which were incident. Three small intestinal adenocarcinomas were encountered, two prevalent, and one incident. 17 non-Hodgkin’s lymphomas occurred but only six were incident and just five were enteropathy-associated T cell lymphomas (EATL) all of which were prevalent.
Conclusions: In this large population based cohort study of malignancy in CD the number of cancers arising was very small, particularly two or more years after the diagnosis of CD even for oesophageal and small intestinal tumours which have been associated with CD. For lymphomas, particularly EATL, numbers were also small. These data can be used to reassure patients and their carers that two years after the diagnosis of CD only very small numbers of cancers arise.
382 LONG TERM MORTALITY IN PEOPLE WITH COELIAC DISEASE DIAGNOSED IN CHILDHOOD COMPARED WITH ADULTHOOD: A POPULATION BASED COHORT STUDY
M. Solaymani-Dodaran, J. West, R. F. A. Logan.University of Nottingham, Division of Epidemiology and Public Health, Medical School, Queen’s Medical Centre, Nottingham NG7 2UH, UK
Introduction: Recent studies have shown that people with coeliac disease have a 30–40% increased mortality rate when compared with the general population. We explored whether the excess mortality in coeliac disease remains many years after diagnosis and if there are differences between those diagnosed in childhood versus adulthood.
Methods: 285 children and 340 adults diagnosed between 1943 and 1983 with coeliac disease in the Lothian region of Scotland were followed until death, loss to follow up or the end of 2004 whichever came first. We calculated cause specific standardised mortality ratios (SMR) by comparing their mortality experience with that of the Lothian population between 1970 and 2004.
Results: We included 21 deaths in children and 174 deaths in adults in our analysis with a median follow up of 34 years and 23 years respectively. All cause mortality more than five years after diagnosis was increased threefold in children (SMR 3.32 95% CI 2.05 to 5.07) compared with only a 38% increase in adults (SMR 1.38 95% CI 1.16 to 1.63). This excess mortality in children was primarily due to an increased risk of accidents, suicides and violence (7 deaths, SMR 3.22 95% CI 1.29 to 6.63), cancer (5 deaths, SMR 3.72 95% CI 1.21 to 8.67)—particularly lymphoma (2 deaths, SMR 21.01 95% CI 2.54 to 76.00) and cerebrovascular disease (2 deaths, SMR 10.03 95% CI 1.21 to 36.00). The modest excess in adults was mainly due to lymphoma (8 deaths, SMR 10.62 95% CI 4.59 to 21.00). These differences persisted after 25 years or more of follow up.
Conclusions: Children diagnosed with coeliac disease have a long term threefold increased risk of mortality when compared with the general population. This is in stark contrast to the experience of adult coeliac disease where the increase risk is modest. Reasons why may reflect severity of disease in children and/or, for external causes of death, behavioural change related to having a chronic disease diagnosis.
383 LONG TERM HISTOLOGICAL FOLLOW UP OF PEOPLE WITH COELIAC DISEASE
G. G. Robins, T. Fitzgerald, P. D. Howdle.Academic Unit of Medicine, St James’s University Hospital, Leeds, UK
Background: Increasing numbers of people are being diagnosed with coeliac disease (CD) for which the only treatment is a gluten-free diet (GFD). There are few studies looking at the long term histological follow up of people with CD.
Methods: All CD patients, with an index small bowel biopsy and one or more sets of follow up biopsies and attending a CD clinic in either of two large UK teaching hospitals have their details entered into a Coeliac Patient Database (CPD). Clinical information is entered prospectively where possible and relevant retrospective data extracted from notes, including histological score (HS) (classified as normal, increased intraepithelial lymphocytes (IELs) only, partial villous blunting (PVB), subtotal villous atrophy (SVA) or total villous atrophy (TVA)) and overall compliance with GFD (good, partial, poor). The primary aim of this study is to look at the length of time to histological remission (HR) in CD patients. Correlation between HS, gender, age, and compliance was examined by Kendall’s rank, Mann-Whitney U or χ2 tests, as appropriate
Results: Of the 169 patients (125 female, 44 male) mean age at diagnosis was 42.8 (range 0.73–80.32) years with a mean follow up of 6.03 (range 0.13–26.21) years. Median number of sets of biopsies taken was three (range 2–12). Nine (all female) patients in the CPD had an initial biopsy reported as normal (that is, they had latent CD), 12 with IELs, 31 with PVB, 56 with PVA and 61 with TVA. Of the 160 patients with an initial histological abnormality, 58 (43 female, 15 male) patients had a documented complete HR. Only 28 (48%) remissions occurred within two years, 41 (71%) within five years and the remaining 17 took greater than five years to achieve HR. Overall 129 (81%) of these 160 patients showed either HR or some improvement in their HS at least once, but 26 (16%) showed no change and 5 (3%) a deterioration. There was no association between either gender or age and HR, although there was a significant trend towards faster HR as patients got older (p<0.01). There was a strong correlation (p<0.001) between good compliance with a GFD and better HS, but not between age and HS, gender and HS or age and compliance.
Conclusion: Time taken to histological remission even for CD patients with good compliance for GFD may take longer than many clinicians realise, especially in younger patients.
384 90% OF COELIAC DISEASE MAY BE BEING MISSED
V. K. T. Nootigattu, B. K. Sandhu.Paediatric Gastroenterology Unit, Bristol Royal Hospital for Children, Upper Maudlin Street, Bristol BS2 8BJ, UK
Background: Data from Avon Longitudinal Study of Parents and Children (ALSPAC) suggest that the prevalence of coeliac disease (CD) is 1%.1 In this study 5470 children randomly selected from a total of 14 000 were screened using Tissue Transglutaminase (TTG) and IgA endomysial antibodies (EMA). 54 children proved positive for CD.1 ALSPAC is an anonymous study and hence these children have not been referred for biopsy or told the results. Within Avon all children with suspected or serologically positive CD are referred to just one centre, Bristol Children’s Hospital, for small bowel biopsies for formal diagnosis of CD.
Aim: The aim was to identify children from ALSPAC (date of birth 01/04/1991 – 31/12/1992 and Avon postcodes) who had been formally diagnosed as CD.
Methods: Since 1990, data have been prospectively collected on all children having endoscopic small bowel biopsy for CD. These data and centralised computer and dietetic records within Avon have been analysed to identify children with CD.
Results: Twelve children from Avon diagnosed with CD since 1.4.91, have birthdays concordant with ALSPAC. This gives a prevalence rate of 1/1100. All had symptoms. Four had a family history. At time of diagnosis all were aged over 2 years, three were 2–5 years, six were 5–10 years, and three were aged 10–14 years.
Discussion: Based on screening data, 140 children from Avon would be expected to have CD. However only 12 of these children have been diagnosed with CD. This suggests that 90% of children with possible CD may be being missed. The screening data also recorded that children with positive screening tests were lagging behind in growth by nine months. There are other well documented long term health hazards of untreated CD. Our data suggest all children should be screened for CD.
1
385 RECOGNISING COELIAC DISEASE ON TERMINAL ILEAL BIOPSIES: SHOULD INTRAEPITHELIAL LYMPHOCYTES BE ROUTINELY QUANTIFIED?
A. D. Hopper, D. P. Hurlstone, J. S. Leeds, M. E. McAlindon, A. K. Dube, T. J. Stephenson, D. S. Sanders.
Background: Coeliac disease (CD) may cause histological changes throughout the small bowel but is conventionally accepted as being predominantly a proximal lesion. Reports have shown changes of ileal villous atrophy, crypt hyperplasia, or raised intraepithelial lymphocyte (IEL) counts on terminal ileal (TI) biopsy.
Aim: We wanted to assess whether TI histological abnormalities occurred more commonly in patients with CD by comparison to other disease groups.
Methods: TI biopsies were examined from 20 patients with a new diagnosis of CD. The controls comprised of four groups: CD established on a gluten free diet (GFD) but with persisting symptoms (n = 25), inflammatory bowel disease (IBD) (n = 47), chronic diarrhoea (n = 44), and polyp surveillance (n = 47). All the biopsies were examined for the presence of villous atrophy, crypt hyperplasia and IEL count per 100 enterocytes (IEL/100EC).
Results: One patient of 20 (5%) with new CD had changes of villous atrophy in the TI. The mean IEL count for the newly diagnosed patients with CD was 23.7 IEL/100EC. Comparisons between the new diagnosis CD group and other groups were significant: CD on a GFD 17.5 IEL/100EC (p<0.012), IBD 12.3 IEL/100EC (p<0.0001), chronic diarrhoea 12.6 IEL/100EC (p<0.0001), and polyp surveillance 13.7 IEL/100EC (p<0.0002). Validating TI villous IEL counts as a test for CD using an IEL/100EC of >25 gives a sensitivity of 45% and a specificity of 97.8% respectively.
Conclusion: IEL should be routinely requested and quantified in TI biopsies. The presence of IEL on a TI biopsy should alert the colonoscopist to the possibility of CD.
386 SURVEY OF THE USE OF SMALL BOWEL FOLLOW THROUGH
J. Groning, M. J. Hall, R. J. Ransford, D. Majumdar, E. Fogden, H. Rhodes, C. Goodwin, F. Akif.Hereford County Hospital, Union Walk, Hereford HR3 6QL, UK
Background: Small bowel follow through (SBFT) has been shown to under diagnose certain conditions.1 We felt that a large number of the tests requested in our hospital showed normal results and decided to examine our current practice of investigating the small bowel with SBFT.
Methods: We retrospectively identified consecutive small bowel follow through reports from the radiology department. Indications, results and final diagnosis (by other tests or operation) were noted.
Results: We identified 72 patients and retrieved 68 notes. Six of 68 patients had an abnormality diagnosed on SBFT. Indications (figures given in brackets: normal/abnormal test): known inflammatory bowel disease (IBD) (8/2); suspected IBD (16/1); IBS (3/0); abdominal pain (5/0); vomiting (2/0); diarrhoea (4/0); small Bowel Obstruction (SBO) (4/1); anxiety (1/0); lethargy (1/0); iron deficiency anaemia (IDA) (3/0); coeliac disease (8/0); malabsorption (1/1); suspected tumour (3/1); unknown (1/0). Abnormal SBFT (6 patients, 9%): two patients with previous radiation exposure for CA endometrium (indications: SBO and suspected tumour respectively), two patients with Crohn’s disease (SBO and known IBD), one patient with a Spighelian hernia (suspected IBD), one patient with small bowel diverticulae (malabsorption). Normal SBFT (62 patients, 91%). Missed diagnosis: Three patients with Crohn’s disease. One patient with coeliac disease on small bowel biopsy (abdominal pain). Negative test: normal in all three patients with known IBS. No patient with coeliac disease had any evidence of small bowel lymphoma. Diarrhoea, abdominal pain, and vomiting were not associated with positive SBFT result.
Conclusion: We will consider our investigation modalities for the small bowel. SBFT is a valid investigation for SSBO. In all other patients another modality, such as capsule endoscopy, is more appropriate.
1
387 ARE GASTROINTESTINAL SYMPTOMS A PREDICTOR OF NSAID INDUCED SMALL BOWEL INJURY? A PILOT STUDY
R. Sidhu, D. S. Sanders, A. Adebajo, M. E. McAlindon, K. Mitchell, D. Graham, K. Kapur.Barnsley Hospital NHS Foundation Trust, UK
Background: The use of non-steroidal anti-inflammatory drugs (NSAIDs) has been associated with small bowel (SB) injury. The spectrum of NSAID induced enteropathy varies from minor punctate haemorrhages to erosions, ulcers, and diaphragm like strictures. The frequency of these lesions in relation to symptoms is yet to be defined.
Aim: To assess the prevalence of SB injury, in patients taking long term NSAIDs and the role of gastrointestinal (GI) symptoms in predicting the presence of NSAID induced enteropathy.
Methods: Patients with arthritis and on NSAIDs (>3 months duration), were enrolled in this pilot study. Patients with obstructive symptoms or previous GI surgery were excluded. The presence of GI symptoms and ingestion of all drugs were noted. All patients underwent capsule endoscopy (CE) (Given Imaging, Yoqneum, Israel) after ingestion of two sachets of Kleen Prep and an overnight fast. The images were read by a gastroenterologist who was blinded to the presence of symptoms and type of NSAID. Lesions seen were classified as red spots, erosions, or ulcers.
Results: Twenty two patients were included in this pilot analysis (12 males), average age 58 years (range 38–75 years). Nine patients were symptomatic, with heartburn (6) or abdominal pain (3). In addition, four patients were on aspirin 75 mg and three patients were on proton pump inhibitors (PPI). Complete examination of the SB was achieved in all patients without complications. One patient underwent Roth net placement of CE due to chronic opiate intake. Evidence of SB injury was seen in 50% of patients: multiple erosions (n = 9), ulcers (n = 2), red spots (n = 4). There was no significant difference in the type of NSAID and frequency of lesions seen. GI symptoms were present in 36% of patients with NSAID enteropathy detected by CE (p<0.1). 75% of patients who were on aspirin in addition to other NSAIDs, and 67% of patients on a PPI had evidence of erosions in the SB.
Conclusion: NSAID induced enteropathy is common in chronic NSAID users. Small bowel injury detected by capsule endoscopy is poorly correlated with patient symptoms.
388 CAN SEROLOGICAL TESTING FOR COELIAC DISEASE PRIOR TO ENDOSCOPY REDUCE THE NEED FOR ROUTINE DUODENAL BIOPSY? A PROSPECTIVE ANALYSIS OF 1500 CASES
A. D. Hopper, D. P. Hurlstone, J. S. Leeds, M. Hadjivassiliou, D. S. Sanders.Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Background: Coeliac disease (CD) may be missed if the endoscopist relies solely on macroscopic changes. In addition, CD may present with atypical symptoms. For this reason many centres perform a duodenal biopsy (D2Bx) routinely.
Aim: Our aim was to assess whether patients with CD could be identified using serology prior to gastroscopy.
Methods: 1500 consecutive patients for gastroscopy were prospectively recruited from 01/02/04 to 01/10/05. All patients had their tissue transglutaminase (TTG), endomysial antibody (EMA) and immunoglobulins checked. All gastroscopies were performed by a single endoscopist. Patients were deemed seronegative if they had a negative EMA and TTG in the absence of IgA deficiency.
Results: Of the 1500 cases 26 had known CD (repeat D2BX). Of the remaining 1474, 512 had indications that would warrant a D2BX (classified as high risk: for example anaemia or malabsorption). 962 patients had symptoms, which could be related to CD but may be considered as atypical (low risk: for example reflux). The prevalence of CD in patients attending for gastroscopy was 3.4% (50/1474). The prevalence of antibody negative CD was 0.3% (4/1474). The prevalence of CD in the high risk group was 8.6% (44/512). The prevalence of CD in the low risk group was 0.6% (6/962).
Conclusion: Serological testing before gastroscopy would have recognised 92% of patients with CD (46/50). The four cases that were seronegative would still have been diagnosed if a D2BX was performed in high risk groups. We would recommend serological testing for CD in low risk group patients prior to gastroscopy, in our series we would have avoided D2BX in 832 patients without missing a case of CD.
Abstract 388
Nutrition posters
389 TIMING OF PERIOPERATIVE PARENTERAL NUTRITION SUPPORT AND CLINICAL OUTCOME
T. R. Smith, S. Wootton, M. Stroud.Institute of Human Nutrition, Southampton University Hospitals, Southampton, UK
Introduction: In our Institution we provide parenteral nutrition (PN) for patients with intestinal failure such that they can not be fed adequately by other means who are either severely malnourished (BMI <18.5 or >10% weight loss) or who have eaten very little for >5 days and/or are unlikely to eat for the next 5 days. We sought to investigate the merits of the latter indication in patients who were not severely malnourished with postoperative ileus.
Methods: Patients were grouped according to the number of days they had been without nutrition (0–5, 6–10, and >10 days). Clinical outcomes following the introduction of PN were recorded. Patients with severe malnutrition were excluded (BMI <18.5 or >10% weight loss).
Results: Sixty five patients were studied (55% female, median age 69 years). See table of results.
Abstract 389
Conclusions: These results demonstrate no detrimental effect of delaying PN support beyond five days on clinical outcome in patients without severe malnutrition. A randomised controlled trial examining optimal timing of PN support should be conducted and our data refute arguments against this type of trial made on ethical grounds.
390 IMPACT OF NUTRITIONAL STATUS ON CLINICAL OUTCOME FOLLOWING MAJOR ABDOMINAL SURGERY
T. R. Smith, S. Wootton, M. Stroud.Institute of Human Nutrition, Southampton University Hospitals, Southampton, UK
Introduction: Malnutrition is common, under-recognised and has a detrimental impact on clinical outcome. We sought to investigate the incidence and consequences of malnutrition in a population of perioperative patients requiring parenteral nutrition (PN) support.
Methods: Nutritional status was assessed by body mass index (BMI), percentage weight loss, and Malnutrition Universal Screening Tool (MUST) score. Clinical outcomes including duration of PN, recovery of gut function, septic complications, organ failure, length of stay, and inhospital mortality were recorded.
Results: 137 patients were studied (53% female, median age 69 years). 28 patients (20%) had a BMI ⩽20 kg/m2 and 32 patients (23%) had >10% weight loss during the preceding 3–6 months. All patients had a MUST score ⩾2; 22 (16%) had a MUST score of 5–6. The median duration of PN was eight days (interquartile range 6–14) and the median time to tolerance of solid food or enteral tube feeding was seven days (IQR 5–12). These outcomes and the incidence of septic complications were not influenced by nutritional status. The incidence of organ failure was significantly higher in those with a BMI ⩽20 kg/m2 (29% v 12%; p = 0.03) and those with a MUST score of 5–6 (32% v 12%; p = 0.02). Those with >10% weight loss tended to have a higher incidence of organ failure (25% v 12%; p = 0.08). The median length of stay was 33 days (IQR 22–56) and was not influenced by nutritional status. The overall mortality rate was 12%, which was significantly higher in those with a BMI ⩽20 kg/m2 (29% v 8%; p = 0.004) and a MUST score of 5–6 (32% v 9%; p = 0.003). Those with >10% weight loss tended to have a higher mortality rate (22% v 10%; p = 0.07).
Conclusions: These results demonstrate that malnutrition is a common problem in hospitalised patients and is clearly associated with poor clinical outcomes. This probably reflects nutritionally related risks and/or more advanced disease in the malnourished group but whatever the cause, MUST criteria are useful in identifying high risk patients and should be incorporated into clinical practice.
391 LONG TERM SUBCUTANEOUS FLUID INFUSION IN THE MANAGEMENT OF INTESTINAL FAILURE
D. A. J. Lloyd1, R. N. Cunliffe2, A. Postgate1, A. Forbes1, T. E. Bowling2, S. M. Gabe1.1St Mark’s Hospital, Watford Road, Harrow HA1 3UJ; 2Clinical Nutrition Unit, Queen’s Medical Centre, Derby Road, Nottingham NG7 2UH, UK
Background: Subcutaneous fluid infusion is a technique usually associated with the treatment of dehydration in the elderly and terminally ill. It is both safe and effective in this context. The technique has been described in the management of intestinal failure in only a single series of 10 patients.
Methods and Results: Records from two tertiary referral centres were reviewed. In Centre A, 42 patients were treated with subcutaneous infusion of 0.9% saline +/− magnesium over a 10 year period. 16 of these (38%) required conversion to intravenous fluid administration (+/− electrolytes or macronutrients) within three months of starting and were judged to have failed treatment. Reasons for failure included intolerance (68%) due to discomfort, poor absorption or haematoma, dehydration (13%), and death from unrelated causes (6%). The remaining 26 patients (62%) were compared with 12 patients successfully treated in Centre B. Of the 26 patients successful treated in Centre A, 12 (46%) continued treatment for >12 months and four (15%) continued for >60 months. Median treatment duration was 10.5 months (range 1–107 months). Treatment was discontinued due to dehydration (43%), corrective surgery (31%), no further requirement (13%), or death from unrelated causes (13%). 20% of patients resumed exclusive enteral support, 15% required IV fluids +/− electrolytes and 15% required IVN. Subcutaneous fluid infusion was ongoing in 38% of patients. Median treatment length in Centre B was five months (range 2–46 months). 64% of patients underwent surgical repair after a median of 3 months (range 2–8 months) and 84% were able to return to exclusive enteral support.
Conclusion: Subcutaneous fluid infusion is a useful treatment modality in the management of patients with moderate intestinal failure both as a long term measure to maintain fluid balance and as a bridge to definitive surgical treatment. It can be considered as a viable alternative to long term intravenous fluid replacement and magnesium supplementation in patients with high intestinal losses and overall negative fluid balance.
392 ONE YEAR EXPERIENCE OF NASOJEJUNAL FEEDING USING THE TIGER TUBE
A. Barnabas1, C. Collins2, P. Nield1, M. Grounds2, T. M. Rahman1,2.1Departments of Gastroenterology; 2Intensive Care Medicine, St George’s Hospital, Blackshaw Road, London SW17 0QT, UK
Introduction: Nutritional support is vital to improving the clinical outcomes in patients in the intensive care unit. Enteral nutrition should be administered early and aggressively, thereby reducing the need for parenteral nutrition (TPN). Nasogastric (NG) feeding may not be tolerated due to gastroparesis, small and large bowel ileus associated with drugs and/or surgery.
Aims: We hypothesised that if NG feeding was not tolerated by 24 hours then a self propelling Tiger Tube (TT) would be placed and NJ feeding commenced reducing TPN requirements.
Methods: We prospectively monitored patients with NG feeding intolerance pre- and post TT placement. (NG tube was also left in situ for aspirate assessment). Abdominal x ray was performed six hours after TT placement to confirm location and feeding regimen commenced.
Results: See table.
Abstract 392
Conclusion: The TT was easily placed aided by prokinetics (90%). All tubes were placed by the nurse/doctor at the bedside and did not require endoscopic placement. Massive savings have resulted from reduced TPN use, reduced associated morbidity associated with TPNand its complications and finally reduction in endoscopic episodes. No complications were associated with the use of Tiger Tubes.
393 PEGGING MORTALITY DOWN A STRUCTURED APPROACH TO PERCUTANEOUS ENDOSCOPIC GASTROSTOMY PLACEMENT
H. Firth (introduced by J. Corrigan).Endoscopy Department, Leeds General Infirmary, UK
Objective: To examine whether the pathway for percutaneous endoscopic gastrostomy (PEG) placement established following a project funded by Clinical Effectiveness has had an impact on 30 day post placement mortality.
The structure:
-
Procedure specific request card with clinical indication
-
Formal assessment of suitability of patient for procedure by Gastroenterology SpR
-
MRSA prophylaxis for all patients pre procedure.
Methodology: A comparison was made between the 30 day mortality rates recorded in the 1999–2001 audit and the results obtained from a two year retrospective audit ending August 2005.
Results: Thirty day post placement mortality had dropped from 13.6% in 2001 (66 PEGs placed) to 6.1% in 2005 (65 PEGs placed). A year on year decrease in the mortality rate can be demonstrated, as the mortality rate for 2004 was 8%
Conclusion: A structured approach to PEG placement has resulted in a significant decrease in post placement mortality.
394 THE KELLETT DRAINAGE ACCESS NEEDLE: AN AID TO IMPROVING COMPLETION RATES IN PEGS AND PEJS
N. C. Fisher.Dudley Group of Hospitals, Dudley, UK
Background: The Kellett Drainage Access needle (Cook Europe) is a 20 cm needle with a 5 Fr outer sheath. It is used by radiologists for access to deep cavities. Its length and slimness can make it helpful in percutaneous endoscopic gastrostomy (PEG) and jejunostomy (PEJ) placement, if difficulty is encountered in accessing or puncturing the gut lumen, although fluoroscopic guidance may also be required. A review is presented here.
Methods: An 18 month casenote review of all PEGs and PEJs done by the author. Fresenius 15Fr PEG kits were used in all cases. For PEGs, the Kellett needle was used in place of the Fresenius needle if there was difficulty accessing or puncturing the stomach, after which the procedure was completed in the usual manner. For PEJs, the Kellett needle was adopted routinely. Fluoroscopy was used in either case if necessary.
Results: PEGs: out of 52 cases, five were done with the Kellett needle, 3/5 under fluoroscopic guidance. PEJs: nine cases were done, all under fluoroscopic guidance. All PEGs and PEJs done with the Kellett needle were completed successfully with no procedural complications. Thus in this review, all patients requiring an artificial feeding prosthesis had successful placement of a PEG or PEJ.
Conclusions: The Kellett needle is a useful accessory which can improve completion rates in endoscopic placement of artificial feeding prostheses.
395 PERCUTANUOUS ENDOSCOPIC GASTROSTOMY: INDICATIONS, MORTALITY, AND RISK FACTORS. A DISTRICT GENERAL HOSPITAL EXPERIENCE
A. Al-Rifai, Z. Ali, C. E. F. Grimley.Burnley General Hospital, Casterton Avenue, Burnley, UK
Background: Percutanuous endoscopic gastrostomy (PEG) has been the preferred method for long term feeding in patients who cannot eat but otherwise have a functionally intact gut. Although it has been widely used for more than 25 years, and is considered safe and technically simple, yet PEG has been associated with a significantly high early mortality.
Aim: We aim to present the results of our experience looking at the outcome, indications, and the characteristics that predicted adverse outcome in a cohort of patients treated in our unit.
Methods: Records of 101 patients who underwent PEG were reviewed retrospectively. Demographic data, indications, pre-existing medical conditions, and death at 30 days and three months were obtained. Other factors that were suggested to predict outcome by previous studies were also recorded. When a comparison between groups was made the χ2 test was used.
Results: The indications for PEG in our series were acute Stroke (70%) other neurological disorders (15%), dementia (7%), and others (8%). The average age of patients was 75 years, and the average time from admission to the date of procedure was 24 days. The mortality rates at 30 days and three months were 24% and 40.6% respectively. Other results are presented in table.
Abstract 395
Conclusion: The early mortality in patients who undergo a PEG procedure remains significant. Referrals continue to increase, and there is no clear guidance when it comes to patient selection. Despite the evidence against, we are still performing PEG in patients with dementia. We have demonstrated an increase in 30 days mortality in older patients, in those with elevated WCC, and who had recent pneumonia. These factors should be considered when making decision about timing of PEG.
396 OUTCOMES OF INAPPROPRIATE PERCUTANEOUS ENDOSCOPIC GASTROSTOMY TUBE REFERRALS IN A DISTRICT GENERAL HOSPITAL
R. Dor, D. Grant, K. Besherdas, N. van Someren, S. D. Mann.Department of Gastroenterology, Chase Farm Hospital, Middlesex, UK
Background: The demand for percutaneous endoscopic gastrostomy (PEG) feeding has increased over the last few years. However, some referrals are deemed inappropriate, after assessment by the Nutrition Support Team (NST). The decision to withhold PEG feeding relies on assessment of prognosis, risks and benefits to the patients, and quality of life judgements.
Aims: To determine morbidity/mortality of those patients not accepted for PEG placement.
Methods: The records of patients, who were deemed inappropriate for a PEG tube, were reviewed noting the underlying diagnosis, comorbidity, and reason(s) for refusal. The clinical nurse specialist reviewed all these patients and the cases were discussed with and/or reviewed by a consultant gastroenterologist.
Results: Between January and December 2004, 32 out of a total 104 referrals (32%) for a PEG tube were felt to be inappropriate (female, 23; median age 81 years (range 22–95 years)). The referral to decision time was seven days (mean; range 3–36 days). The commonest underlying diagnoses were cerebrovascular accident (CVA) (53%) and dementia (19%). 15 patients died (47%) within two weeks of referral; eight died from a lower respiratory tract infection, seven from a CVA. Outcome data were not available on five patients who were deemed medically unfit. Eight patients had died before review by the NST. Eight patients (25%) successfully converted to oral feeding by the time of assessment and one was discharged.
Conclusion: One third of referrals for PEG placement do not undergo the procedure either due to active refusal by the NST, or due to the natural history of the underlying condition causing death or recovery within a few days of referral. Where the NST declined a PEG, those patients died quickly and the PEG would not have altered the outcome.
397 LONG TERM PEG-J FEEDING: A SINGLE CENTRE EXPERIENCE
E. A. B. Cameron, S. Cottee, J. M. Woodward.Nutrition team, Addenbrooke’s Hospital, Cambridge, UK
Introduction: The use of percutaneous gastrostomy (PEG) feeding has increased significantly in recent years. A proportion of patients require feeding distal to the pylorus (for example, in recurrent aspiration or diabetic gastroparesis). We have evaluated all consecutive patients in whom jejunal extension tubes (PEG-J) were inserted over a nine year period between May 1996 and April 2005 (Fresenius Freka intestinal 9Fr through Fresenius Freka 15Fr gastrostomy).
Methods: Data were collected regarding patient demographics, indication, length of PEG-J feeding, re-intervention, and patient outcome for all patients in whom PEG-J tubes were inserted at our institution.
Results: PEG-J tubes were inserted in 26 patients (12 male, mean age 43 years, SD 17) for recurrent aspiration (14), gastroparesis (5), recurrent vomiting (5), duodenal obstruction (1), and entero-cutaneous fistula (1). Patients were fed for a total of 31.9 years (mean 1.2, SD 1.2). Tubes had to be replaced on 40 occasions (mean 1.54 per patient, SD 1.84). The indications for replacement were external displacement (24), displacement into stomach (13) and blockage (3). The majority of tube failures occurred in a small number of patients (65% in six patients, 10 patients requiring no repositioning or replacement). PEG-J tubes lasted for a mean of 183 days (SD 52). Eight patients continued with PEG-J feeding at the end of the study. Five patients died while being fed via PEG-J (46, 74, 466, 533, and 774 days after insertion). The reasons for ceasing PEG-J feeding were death (5), recovery (4), patient preference (3), repeated displacement (3), surgical jejunostomy (2), and persistent aspiration (1). From November 2002, external connectors were superglued after one patient repeatedly disrupted his tube with no statistically significant effect on PEG-J longevity.
Discussion: This is the largest UK series to date of long term feeding via PEG-J tube. It is useful for patients requiring long term post-pyloric nutrition. Although there is a significant risk of tube failure requiring repositioning or replacement, the majority of carefully selected patients require one or fewer re-interventions.
398 REDUCING PEG MORTALITY RATES BY NURSE LED PRE ASSESSMENT AND PLACEMENT
A. Jones, R. J. Dickinson, P. J. Roberts.Department of Gastroenterology, Hinchingbrooke Hospital, Huntingdon PE 29 6NT, UK
Background: Prior to nurse led assessment, the 30-day mortality for percutaneous endoscopic gastrostomy (PEG)at this hospital was unacceptably high at 30%. All patients referred for a PEG had one placed if deemed appropriate by two clinicians without a set pre-assessment protocol.
Aims and Objectives: To reduce the 30 day PEG mortality by instituting a nurse led pre-assessment proforma for patients referred for (PEG) insertion, aligned with nurse PEG tube assisted placement.
Methods: A total of 66 patients were assessed over a two year period. No patients were excluded from the study. All patients were assessed by a dedicated nurse inorder to ensure continuity. The pre-assessment proforma was devised specifically for this study and includes discussion with a variety of healthcare professionals to ensure a multidisciplinary decision is made.
Results: Forty one PEG placements were recommended out of the 66 assessed. The 30 day mortality rate significantly reduced over the two years of the study using the pre-assessment proforma and when a dedicated endoscopist and nurse assistant placed the PEGs to less than 5%.
Conclusions: This process has demonstrated that assessing all patients considered for a PEG with good clinical guidelines, evidence based practice, and multidisciplinary decision can reduce both mortality and morbidity rate and improve the quality of treatment for this complicated group of patients. Aligned to this in our unit the practice of a dedicated nurse aiding PEG placement appears to be extremely safe.
399 DEMENTIA AND HOME ENTERAL TUBE FEEDING IN THE UK: THE REALITY OF CURRENT PRACTICE
B. J. M. Jones.Russells Hall Hospital, Dudley. Presented on behalf of the British Artificial Nutrition Survey committee (BAPEN), UK
Introduction: In the UK, chronic neurological diseases are the commonest indication for home enteral tube feeding (HETF) and gastrostomy insertion for which the ethics of consent are often controversial. Recent evidence suggests that dementia is a poor indication for enteral nutrition, with no improvements in quality of life, aspiration pneumonia or survival.
Aim: To determine the prevalence and characteristics of dementia and HETF in the UK.
Methods: Analysis of data from the British Artificial Nutrition Survey (BANS) for 2004 (British Association for Parenteral and Enteral Nutrition).
Results: In 2004, of 5656 new BANS HETF registrations, 221 (4%) in 107 centres had dementia. Point prevalence of dementia was 592/18 260 (3.2%) in 167 centres and period prevalence was 735/21 677 (3.4%) in 181 centres. The predominant age of new patients was 71–90 years (74%). The indication for HETF in dementia was “swallowing difficulty” in 59% and “to improve nutritional status” in 36%. HETF was by gastrostomy (89%), nasogastric tube (11%), and jejunostomy (0.5%). HETF was provided in a nursing home in 81% with only 15% at home. 61% were bed bound and 98% totally dependent. Commercial homecare companies supplied equipment and feeds in 81% cases. Mortality one year after commencing HETF was at least 48% although follow up underreporting may have led to over recording of survival.
Conclusions: A substantial number of demented patients receive HETF in the UK. They are characterised by total dependency and nursing home placement in majority of cases. It is possible that HETF is being offered to earlier cases of dementia with some residual cognitive function and that HETF can not be avoided in these patients but the majority appear to have very poor quality of life with high mortality. We have no data on whether nutritional status or clinical outcomes were improved by HETF. There is still insufficient evidence of benefit in favour of HETF for dementia.
400 15 YEAR AUDIT OF HOME PARENTERAL NUTRITION PROVISION
C. J. Green, H. Hamilton, V. C. Mountford, M. W. G. Kettlewell, S. P. L. Travis.John Radcliffe Hospital, Oxford OX3 9DU, UK
Introduction: Oxford has provided an home parenteral nutrition (HPN) service since 1984, through a multidisciplinary team (consultant, registrar, dietician, pharmacist, nutrition, vascular access nurse specialists) with designated protocols for vascular access, training, and catheter care.
Methods: A retrospective analysis of notes and prospectively collected data was performed on all patients on HPN between January 1990 and December 2004 inclusive. Demographics, mortality, and complications of HPN were collected and analysed. Data were divided into quintiles (five-year groups) to assess differences in the parameters over time.
Results: There were 121 patient years of experience, 55% female, median age 40 (range 3–73). Median duration of HPN was 218 days (18–3881). Indications were Crohn’s disease (35%), vascular (11%), dysmotility (10%), other (44%), but between 1st and 3rd quintiles Crohn’s became a less common indication (44% v 28%, NS). Overall mortality was 13.6% and HPN related mortality 1.1%. Complication rates (episodes per patient year) were: line sepsis 0.35, line occlusion 0.25, central venous obstruction 0.03, endocarditis 0.02, cholestasis (2/3 of bilirubin, ALP γGT with >1.5-fold elevation) 0.17. Line sepsis and occlusion were more common in the 1st than 3rd quintile (0.6 v 0.26% ns, and 0.53 v 0.18% respectively, p = 0.07). No cases of endocarditis occurred in the third quintile. 31% patients had double lumen catheters, one for HPN and the other for vascular access if peripheral access was limited.
Discussion: The 15 year reduction in the proportion with Crohn’s on HPN is consistent with other experience and probably reflects a reduction in surgery performed on poorly nourished patients. Many received HPN in preparation for definitive surgery. Mortality and line complications are comparable to the best series, and cholestasis less common. The trend to fewer line complications in the 3rd quintile cannot be accounted for by any change in practice. Double lumen catheters for HPN have an acceptable complication rate if strict management protocols are followed.
401 CONSUMPTION OF GLUTEN FREE FOODS AND MACRONUTRIENT INTAKES IN PATIENTS WITH COELIAC DISEASE
A. Holdoway, W. E. Fickling, A. K. Bhalla1, D. A. F. Robertson.Royal United Hospital; 1Royal National Hospital for Rheumatic Diseases, Bath, UK
Background and Aim: Management of coeliac disease (CD) relies on strict adherence to a gluten free (GF) diet. In the UK, GF foods are available on prescription for patients with CD to provide basic staples to help achieve an adequate energy and carbohydrate (CHO) intake and aid compliance to a GF diet. Little is known however about the consumption of GF foods in the UK, their contribution to the GF diet and whether the macronutrient intake among patients with CD is optimal. The aim of this study was to accurately assess intakes of energy, fat, CHO, and GF foods in patients with CD and compare intakes with the National Diet and Nutrition Survey (NDNS) 2002 and dietary guidelines, DOH, 1991.
Methods: Adults with established CD (diagnosed >2 years), confirmed by biopsy, who demonstrated histological improvement on a GF diet were recruited from out patient clinics and Coeliac UK. Diet was assessed through a 10 day weighed food intake. Diet records were analysed using a nutrient database to which the composition of manufactured GF foods were manually added. Dietary intakes were compared with the NDNS, 2002 and dietary reference values for macronutrients, DOH, 1991.
Results: Forty nine patients were recruited, 42 completed the study, 10 males, 32 females, mean age 55 years (25–71 years). Mean body mass index was 24.5 kg/m2. Diet records showed strict compliance to a GF diet in 41/42. Gastrointestinal symptoms were absent in the study period. Mean daily intakes for males = 2442 kcals/day,% energy from CHO = 47%, fat = 35%, females = 1819 kcals/day, CHO = 49.4%, fat = 32%. 41/42 consumed GF foods on a daily basis. Mean daily intake of GF foods as consumed was males 156 g, females 113 g. GF bread was the most frequently used GF food, median daily intake among consumers was males 144 g, females 73 g (NDNS; males 162 g, females 102 g/day).
Conclusion: This study showed that a GF diet did not adversely affect energy, CHO or fat intakes and dietary guidelines for macronutrients can be met while adhering to a strict GF diet. Specially manufactured GF foods were used by the majority and bread remained a basic staple.
Oesophagus posters
402 RISK FACTORS FOR THE DEVELOPMENT OF BARRETT’S OESOPHAGUS: A CASE CONTROL STUDY
S. Velmurugan, I. Mohammed, R. Lo, B. T. Cooper, N. J. Trudgill.Department of Gastroenterology, Sandwell and West Birmingham Hospitals NHS Trust, UK
Background: The main risk factor for Barrett’s oesophagus (BO) is chronic gastro-oesophageal reflux disease (GORD). It is not clear why some patients with GORD develop BO and some only develop oesophagitis. We hypothesised that BO may be associated with a familial predisposition to metaplasia and cancer.
Methods: 221 patients with BO (>3 cm in length) and 276 patients with oesophagitis (controls) were asked to complete two questionnaires. One measured symptoms of GORD, potential aetiological factors and demographic data. The second took a detailed family history, including the number of first degree relatives and their history of cancer.
Results: 149 (67%) BO and 174 (63%) controls responded. 130 (59%) BO and 141 (51%) controls completed the questionnaire fully. 116 BO were age, sex, and ethnicity matched with controls, 68 males. BO median age 67 (range 38–85), controls 65 (range 40–88). Univariate analysis revealed that BO was associated with a history of frequent acid regurgitation (p = 0.03) and a family history of BO (p = 0.03). There was an inverse association of BO with ever smoking (p = 0.04). No educational attainment (p = 0.06), cancers per first degree relative (p = 0.09), body mass index, alcohol intake, duration of GORD symptoms (all p>0.1) did not reach statistical significance. Forward stepwise logistic multivariate regression analysis revealed that BO was associated with frequent acid regurgitation odds ratio 1.9 (95 CI 1.1 to 3.5) (p = 0.03), no educational attainment 2.2 (1.3 to 4.0) (p = 0.007) and cancers per first degree relative 9.9 (1.7 to 57.7) (p = 0.01).
Conclusion: Frequent acid regurgitation, no educational attainment and a history of cancer within first degree relatives are independently associated with BO. The association of BO with a family history of BO and cancer in first degree relatives raises the possibility of an inherited predisposition to metaplasia in BO.
403 BARRETT’S OESOPHAGUS IN PATIENTS PRESENTING WITH SYMPTOMS UNRELATED TO GASTROESOPHAGEAL REFLUX DISEASE
S. Gupta, M. Fullard, R. J. Leicester, J. D. Maxwell, J. Y. Kang.Department of Gastroenterology and Colorectal Surgery, St George’s Hospital, London, UK
Introduction: Barrett’s oesophagus (BO) is a manifestation of severe gastroesophageal reflux disease (GORD) and predisposes to oesophageal adenocarcinoma (OAC). Many patients who present with OAC are found to have BO associated with the tumour and it is thought that BO remains undiagnosed in many patients throughout their lives. If so, BO may be an incidental finding in many patients.
Aim: To determine the proportion of patients newly diagnosed with BO in whom endoscopy was done for symptoms unrelated to GORD.
Methods: All endoscopies performed in the hospital are entered prospectively into a database (Micromed), which was examined retrospectively, looking for endoscopic diagnosis of BO and the symptoms that prompted the endoscopy.
Results: From 01/01/1998 to 31/12/2004, 14 170 endoscopies were performed on 12 966 patients at our hospital. There were 221 patients with a new diagnosis of BO. 11 patients with oesophageal cancer were excluded. These patients were divided into two groups: group 1 with symptoms of GORD (heartburn, reflux, abdominal pain, or dysphagia) and group 2 in whom endoscopy was performed for other indications. There were 132 patients (60%) in group 1 and 89 patients (40%) in group 2. Non-GORD indications for endoscopy included anaemia (42), haematemesis/melaena without oesophageal pathology (18), peptic ulcer followup (5), weight loss (10), variceal screening (4), and others (18).
Conclusions: Almost half of patients with BO present with symptoms unrelated to GORD. This supports the hypothesis that in many patients, BO remains unrecognised throughout their lives.
Abstract 403
404 DIAGNOSIS AND MANAGEMENT OF BARRETT’S OESOPHAGUS: RESULTS OF THE UK NATIONAL BARRETT’S OESOPHAGUS REGISTRY (UKBOR) ENDOSCOPIST QUESTIONNAIRE
J. R. Ramus, C. P. J. Caygill, P. A. C. Gatenby, A. Watson.UKBOR, University Department of Surgery, Royal Free Hospital, London, UK
Background: Criteria and techniques employed for the diagnosis of columnar lined oesophagus (CLO) have changed over the last decade. Guidelines for both diagnosis and management of CLO exist, but are limited by lack of evidence of the natural history of the disease. Biopsy techniques have been recommended for a precise histological diagnosis and surveillance intervals suggested to optimise detection of pre-neoplastic changes.
Methods: A questionnaire was designed on behalf of the UK National Barrett’s Oesophagus Registry (UKBOR) to examine consistencies in the diagnosis and management of CLO and its complications. Questionnaires were sent to the lead endoscopists of 41 centres spread throughout England, Scotland, and Wales. All centres currently register patients with UKBOR.
Results: Thirty (73%) centres replied. 12 (40%) centres said they had a specific policy for the management of CLO. 25 (83%) said that a diagnosis of CLO would be made if any length of Barrett’s mucosa observed with four (13%) requiring a length >3 cm in order to make a diagnosis. 27 (90%) centres surveyed CLO with five (17%) centres surveying all patients diagnosed with CLO routinely and 16 (53%) surveying more than half. The majority of centres (78%–93%) surveyed uncomplicated CLO at intervals between 1 and 3 years, with 54% surveying dysplastic disease at 1–6 monthly intervals. 22 (73%) centres said that they took four quadrant biopsies at 2 cm intervals at both diagnostic and surveillance endoscopy.
Conclusion: There is considerable variation throughout the U.K. in surveillance practice. Although some 90% of centres perform surveillance, in only 17% are all patients with CLO surveyed, the remaining 73% practising a selective surveillance policy. However, among those who do perform surveillance there was a high level of consistency relating to surveillance intervals and biopsy technique.
405 AUTOFLUORESCENCE ASSESSMENT IN THE SURVEILLANCE OF BARRETT’S OESOPHAGUS: PILOT STUDY
A. L. McCallum1, M. MacPherson1, P. Chong1, J. T. Jenkins1, D. Gillen2, K. Oien3, F. Duthie3, G. M. Fullarton1.1Department of Surgical Gastroenterology; 2Department of Gastroenterology, Gartnavel General Hospital, 3Department of Pathology, Western Infirmary, Glasgow, UK
Background: Barrett’s oesophagus is associated with an increased risk of oesophageal adenocarcinoma. Scotland has a high incidence of Barrett’s oesophagus and its male population has the highest rate of oesophageal adenocarcinoma in the world. Currently patients with Barrett’s undergo endoscopic surveillance in an attempt to detect dysplasia and/or early cancer. The current protocol is time consuming and it’s effectiveness has been put into question. Autofluorescence (AF) is a new technique which detects endogenous fluorescence in normal and diseased epithelium. It may be of value in detecting dysplasia in Barrett’s patients.
Aim: To establish if AF endoscopy is useful in detecting dysplasia in Barrett’s patients.
Methods: Patients with histologically proven Barrett’s were invited for endoscopic assessment using both AF and conventional white light (WL). High AF readings within the Barrett’s segment were recorded and biopsied followed by standard biopsies following the Seattle protocol. The histology was blindly reported by two pathologists scoring them according to the Vienna classification.
Results: A total of 57 patients were assessed with AF and WL endoscopy. Intestinal metaplasia was detected in 35 of 51 (68%) patients using random WL biopsies and in 27 of 46 (59%) patients biopsied with AF. One patient had high grade dysplasia which was detected with AF biopsy and not WL. The median number of biopsies per patient was four for WL and one for AF.
Conclusion: AF endoscopy has a similar detection rate of intestinal metaplasia and of dysplasia as WL endoscopy with the advantage of being a faster technique with fewer biopsies needed.
406 HIGH RESOLUTION MAGNIFICATION ENDOSCOPY WITH NARROW BAND IMAGING IN PATIENTS WITH BARRETT’S OESOPHAGUS
G. K. Anagnostopoulos, K. Yao, C. J. Hawkey, K. Ragunath.Wolfson Digestive Diseases Centre, University Hospital, Nottingham, UK
Background: The penetration depth of light depends on its wavelength; blue light penetrating only superficial tissue areas. Therefore, use of blue light with the help of a filter will enable imaging of the superficial structures. Narrow band imaging (NBI) is a novel imaging technique that uses such filters to enhance the mucosal contrast, revealing the superficial structural and microvascular patterns. The aim of our study was to describe the high resultion magnification endoscopy/narrow band imaging (HRME/NBI) endoscopy findings in Barrett’s oesophagus.
Methods: Consecutive patients with known Barrett’s oesophagus undergoing surveillance endoscopy were enrolled in the study. Conventional white light endsocopy was followed by magnification endoscopy with NBI using a high resolution magnification endoscope (Olympus GIF-Q240Z, 115×) and NBI light source. Structural and microvascular patterns within the Barrett’s segment were identified, biopsied and read by pathologists blinded to endoscopic findings.
Results: Fifteen patients with Barrett’s oesophagus were evaluated (mean age 57 years, 13 males). Mean length of Barrett’s segment was 3.6 cm (range 1–7 cm). With NBI, striking contrast was observed between squamous and columnar mucosa. Three distinct mucosal patterns (1, tubular/villous/linear; 2, circular; and 3, distorted) and two microvascular patterns (1, regular-fine lace-like network and 2, irregular-dilated, tortuous) were seen. A total of 93 biopsies were taken. All areas with tubular/villous/linear pattern showed specialised intestinal metaplasia (SIM) in histology. Both sensitivity and specificity of tubular/villous/linear pattern to detect SIM were 100%. One area had distorted pattern with irregular microvessels-biopsies showed high grade dysplasia. Six areas had circular pattern-biopsies showed columnar mucosa with no SIM in all cases.
Conclusion: Using HRME with NBI we described the non-dysplastic and dysplastic features in Barrett’s epithelium. Further randomised control studies are required to prove the efficacy of this technique in the surveillance of patients with Barrett’s oesophagus.
407 THE EFFECT OF ACID SUPPRESSION ON APOPTOSIS AND CELL PROLIFERATION IN BARRETT’S OESOPHAGUS
M. Fullard1, C. Gordon1, C. Finlayson2, S. Matthews2, P. Neild1, A. Poullis1, J. D. Maxwell1, J. Y. Kang1.1Departments of Gastroenterology; 2and Histopathology, St George’s Hospital, London, UK
Background: As Barrett’s oesophagus (BO) progresses through dysplasia to carcinoma, apoptosis is reduced and cellular proliferation increased. It is not known whether strict acid control can reduce the malignant potential of BO.
Aim: To determine the effect of acid suppression on apoptosis and proliferation in patients with BO.
Methods: Patients with BO rendered asymptomatic on acid suppressants underwent 24 hour lower oesophageal pH studies. Those with abnormal acid profiles had their acid suppression escalated before a repeat pH study. Oesophageal biopsies from 10 patients (5 with normal acid exposure, 5 abnormal acid exposure) were taken within two weeks of the pH study. Cellular proliferation in the crypts was assessed using the Ki-67 antibody, and apoptosis assessed using the m30 monoclonal antibody. Proliferation was expressed as the number of positively stained cells as a percentage of total crypt cells, with the crypt divided into lower, middle and upper thirds (proliferative index, PI). Apoptosis was graded between 0 (no apoptotic cells) and 3 (areas of confluent apoptotic cells).
Results: The two groups did not differ in terms of age and sex, but the Demeester score was significantly higher in patients with abnormal acid exposure (13.7 v 1.9, p = 0.01).
Proliferation was greater in the lower two thirds of the crypt compared to the upper third, but did not differ significantly between the two groups of patients. In patients with good acid control, the PI was: lower third 45.7, middle third 35.2, upper third 14.5. In the group with abnormal acid profiles, the PI was: lower third 45.7, middle third 34.3, upper third 10.9. The mean apoptosis grade was 0.8 for the group with normal acid profile, and 1.4 for the group with abnormal acid profile (p = 0.85)
Conclusion: In patients with Barrett’s oesophagus, effective control of acid reflux did not affect proliferation as assessed by the Ki-67 antibody and apoptosis as assessed by the m30 monoclonal antibody.
408 THE BILE ACID, LITHOCHOLIC ACID, ACTIVATES RETINOID SIGNALING IN BARRETT’S OESOPHAGEAL CELL LINES
C. Chang, R. C. Fitzgerald.MRC Cancer Cell Unit, Department of Oncology, University of Cambridge, Hills Road, Cambridge, UK
Background: The bile acid constituents of gastroduodenal reflux have been implicated in the pathogenesis of Barrett’s associated adenocarcinoma. The published data suggest that bile acids induce the expression of inflammatory cytokines or activate mitogenic pathways and thus contribute to carcinogenesis. The bile acid lithocholic acid (LCA) has recently been demonstrated to compete efficiently with 9-cis-RA for the RXR retinoid binding site. Retinoic acid is part of a family of ligand dependent transcriptional factors which are essential for cell differentiation, cell growth, and apoptosis. Hence we hypothesised that LCA may play a role in Barrett’s carcinogenesis via activation of the retinoid signalling.
Methods: A 3T3 cell line stably expressing a RARE-SEAP reporter was generated to assay retinoic acid (RA) activity. These cells were treated with one or both of All trans retinoic acid (ATRA) or LCA compared to serum-free medium as the control. The expression levels of retinoid target genes were determined in dysplastic Barrett’s cell lines (Gihtert and Gohtert) by real-time PCR.
Results: RA signalling induced by LCA and ATRA in combination were synergistic (p = 0.024; p = 0.018) (see figure). This synergistic effect was confirmed in two immortalised Barrett’s cell lines by examining the expression of the ATRA response gene p21. ATRA and LCA in combination resulted in a threefold increase in p21 mRNA expression compared to addition of either LCA or ATRA alone (p<0.01).
Discussion: These data suggest that LCA may induce RA activity in Barrett’s oesophagus. This could have physiological significance in view of the known role of RA in cell growth and differentiation.

Abstract 408
409 EPITHELIAL CELLS OVEREXPRESS THE LEPTIN RECEPTOR DURING MALIGNANT PROGRESSION IN BARRETT’S OESOPHAGUS
S. Ahmed1, A. L. Khan2, L. Pazmany3, K. Bodger1,3.1Aintree Centre for Gastroenterology; 2Department of Cellular Pathology, University Hospital Aintree, Liverpool; 3School of Clinical Sciences, University of Liverpool, UK
Introduction: Obesity is a recognised risk factor for oesophageal adenocarcinoma. The reason for a link between excessive weight and cancer is unclear. We hypothesised that leptin receptor (OB-R) might be overexpressed in metaplastic or neoplastic oesophageal epithelium during carcinogenesis. This would provide a mechanism whereby obesity related hyperleptinaemia might exert a direct growth promoting effect on oesophageal mucosa, potentially favouring malignant progression. Leptin has been shown to stimulate proliferation of various epithelial cell lines expressing Ob-R.
Methods: mRNA abundance of OB-Rb (main functional Ob-R isoform) was determined by quantitative PCR performed on cDNA generated by reverse transcription of RNA extracted from endoscopic biopsies. Values were normalised relative to h-HPRT housekeeping gene. Product was confirmed by agarose gel. Normal gastric fundus expresses Ob-Rb and was used as positive control. Immunohistochemistry for Ob-R was performed on formalin fixed biopsies and western blots on lysates of oesophageal cancer cell line (OE33).
Results: Ob-Rb is expressed at very low level in the normal squamous oesophagus but exhibits progressive expression during malignant progression at levels significantly in excess of the healthy stomach (see table: mean values (SD), p<0.001 ANOVA). Epithelial cell staining was confirmed by immunohistochemistry with marked upregulation of Ob-R in surface epithelial cells noted at the stages of dysplasia and cancer. OE33 cells express Ob-R.
Abstract 409
Conclusion: Overexpression of Ob-Rb occurs during malignant progression. This is consistent with our leptin hypothesis. The effects of leptin on Barrett’s epithelial cells require further study. Therapeutic manipulation of leptin receptor signalling might provide a novel mechanism for the prevention or treatment of oesophageal adenocarcinoma.
410 CYCLIN A IMMUNOCYTOLOGY AS A RISK STRATIFICATION TOOL IN BARRETT’S OESOPHAGUS SURVEILLANCE
P. Lao-Sirieix1, L. Lovat2, R. C. Fitzgerald1.1MRC-Cancer Cell Unit, MRC/Hutchison Research Centre, Cambridge; 2National Medical Laser Centre, Charles Bell House, London, UK
Background: The incidence of oesophageal adenocarcinoma (AC) is increasing rapidly. Endoscopic surveillance of patients with Barrett’s oesophagus (BO) using biopsies for histopathological assessment is prone to sampling bias, is not cost effective and interpretation of dysplasia is subjective. Alternative methods for surveillance are direly needed. We have previously demonstrated that surface expression of a proliferative marker, Mcm2, is a marker of progression. However, it lacked specificity for detection of patients at risk.
Aims: To determine whether cyclin A, which detects a proportion of proliferating cells, would be more specific.
Methods: Archival specimens (30 squamous esophagus (SE), 12 gastric antrum (GA), and 9 duodenum (D2), 62 BE+/−dysplasia, 16 AC) were stained for cyclin A. In addition, nine patients with 3–13 years follow up who developed AC were compared with 18 controls matched for age and length of follow up who did not progress. Endoscopic cytological brushings were taken from a prospective cohort (24 SE, 93 BE+/−dysplasia, and 36 AC) and scored blind as cyclin A positive or negative.
Results: There was no surface expression of cyclin A in control samples (NE, GA, D2) and its expression at the surface of BE samples correlated with the degree of dysplasia (p = 0.016). In the case control cohort, patient with biopsies expressing cyclin A at the surface were more likely to progress to AC than those who did not (odds ratio 10.0, 95% confidence interval 1.5–64.2). The sensitivity and specificity of cyclin A expression in brushings for the detection of high grade dysplasia (HGD) and cancer patients were 97.9% and 61.2% respectively. The associated negative predictive value was 98.2%.
Conclusions: Expression of cyclin A at the luminal surface is a marker of progression to AC. Detection of cyclin A positivity in endoscopic brushings could be used as a first step to stratify BO patients with a highest risk of progression. A large clinical study is still required to confirm those findings.
411 EVIDENCE FROM BARRETT’S CARCINOGENESIS THAT CYP26A1 IS IMPLICATED IN CANCER
C. Chang, R. C. Fitzgerald.MRC Cancer Cell Unit, Department of Oncology, University of Cambridge, Hills Road, Cambridge, UK
Background: Retinoic acid (RA) is an important signalling molecule for Anterior-Posterior (AP) patterning in embryogenesis. Tight control of intracellular RA levels results in an anterior shift in endoderm gene expression and induction of the caudal gene CdxA. CYP26A1 is the major RA catabolising enzyme responsible for maintaining exquisite control over cellular RA concentrations.
Hypothesis: We hypothesised that alterations in RA signalling may have a role in differentiation status in Barrett’s carcinogenesis.
Aims: In this study we have investigated the role of RA and CYP26A1 on Barrett’s metaplasia and associated dysplasia and adenocarcinoma.
Methods and Results: By using retinoic acid response element (RARE) reporter cells we demonstrated that non-dysplastic Barrett’s cell lines (BAR, QhTERT) and non-dysplastic Barrett’s tissues had the highest levels of RA bioactivity, which decreased progressively with the degree of dysplasia in cell lines (Chtert, Gihtert), and patient tissues (p<0.05). The degree of RA bioactivity was inversely correlated with CYP26A1 gene levels. Functionally, overexpression of CYP26A1 in Gihtert cells increased proliferation as determined by their cytometric DNA profile, CholordU and IododU incorporation and an MTT assay. An in vitro matrigel assay demonstrated that cells overexpressing CYP26A1 were more invasive (p<0.01). The increased invasion is likely to be due to alterations in matrix metalloproteinase expression (upregulation of MMP-3, down-regulation of TIMP-1 and TIMP-3 p<0.05) which were demonstrated by quantitative RT-PCR. Using an organotypic culture system we also demonstrated that CYP26A1 gene overexpressing cells are “dedifferentiated” as shown by co-localisation with a stem cell marker Oct-4. Pathway arrays showed induction of c-myc and EGFR expression in these CYP26A1 overexpressing cells.
Discussion: Overexpression of CYP26A1 causes intracellular RA depletion and drives the cell into a highly proliferative, undifferentiated, and invasive state with induction of other known oncogenes. These data suggest a previously unknown role for this gene in cancer.
412 HELICOBACTER PYLORI AND CAG A STATUS IN OESOPHAGEAL ADENOCARCINOMA, BARRETT’S OESOPHAGUS, AND REFLUX OESOPHAGITIS
L. A. Anderson, B. T. Johnston, R. G. P. Watson, S. J. Murphy, K. Bamford, A. Ghazy, H. Ferguson, H. Comber, J. McGuigan, J. V. Reynolds, L. J. Murray.Centre for Clinical and Population Sciences, Queen’s University, Belfast, Northern Ireland; Royal Group of Hospitals, Belfast, Northern Ireland; Imperial College London; National Cancer Registry, Cork, Ireland and St James’s Hospital, Dublin, Ireland
Introduction:Helicobacter pylori (H pylori) appears to reduce the risk of oesophageal adenocarcinoma (OAC), possibly by causing gastric hypochlorhydria. We set out to compare the prevalence of H pylori infection (including Cag A strains) in normal controls and reflux oesophagitis (RO), Barrett’s oesophagus (BO), and OAC patients from throughout Ireland.
Methods: In this population based case control study, data were collected about potential lifestyle and environmental risk factors and a 30 ml of blood obtained. Using stored serum, IgG antibodies to H pylori and CagA were measured in 253 population controls, 208 OAC, 215 BO and 229 RO patients by Western Blot (Helico Blot 2.1, Genelabs Diagnostics, Singapore).
Results:H pylori seropositivity was less common in OAC (OR 0.51 (95% CI 0.34 to 0.78)), BO (OR 0.40 (95% CI 0.26 to 0.61)) and RO patients (0.30 (95% CI 0.19 to 0.47)) compared to controls. OAC, BO and RO patients were also less likely than controls to be CagA positive, OR (95% CI): 0.58 (0.39–0.88), 0.55 (0.36–0.83), and 0.59 (0.38–0.91), respectively.
Conclusions:H pylori seropositivity, and to a lesser extent, Cag A positivity were less prevalent in patients with RO, BO, and OAC than in normal controls. H pylori infection may reduce OAC risk by a mechanism other than induction of gastric hypochlorhydria.
413 EXPRESSION OF TISSUE INHIBITORS OF METALLOPROTEINASES AND TARGET PROTEASES DURING BARRETT’S CARCINOGENESIS
S. Ahmed1, A. L. Khan2, L. Pazmany3, A. Varro4, K. Bodger1,3.1Aintree Centre for Gastroenterology; 2Department of Cellular Pathology, University Hospital Aintree, Liverpool; 3School of Clinical Sciences; 4Physiology Department, University of Liverpool, UK
Introduction: A multi-step pathway for oesophageal adenocarcinoma (AdCa) proceeds from squamous epithelium (SqEp) via Barrett’s metaplasia (BM) to dysplasia and cancer in the setting of reflux disease. These processes involve remodelling of tissue architecture and fundamental changes to extracellular matrix (ECM). Regulation of the ECM is under the influence of the matrix metalloproteinases (MMPs) and their natural tissue inhibitors (TIMPs), a system of molecules that have roles in ECM homeostasis, inflammation, angiogenesis, and metastasis.
Methods: The aim of the present study was to define expression profile of TIMPs (-1 to -4) and selected MMPs (-3 and -8) at different points in the cancer pathway. Oesophageal biopsies were obtained for mRNA extraction, histopathology and immunostaining. Real-time PCR was performed on cDNA generated by reverse transcription of RNA extracts. Expression of transcripts was normalised for h-HPRT housekeeping gene.
Results: Compared to SqEp, BM was associated with a significant increase in mRNA abundance for TIMPs -1, -2, -3, and -4 and MMP-8 (but not MMP-3), whereas AdCa was characterised by increases in TIMP-4 (but not other TIMPs) and MMP-8 but a decrease in MMP-3. Compared to BM, there was reduced TIMP-3 and MMP-3 but increased MMP-8 in AdCa. Immunostaining confirmed cell type specific changes in expression, with TIMP-4 in particular showing a progressive increase in epithelial and basal layer immunostaining from non-dysplastic BM through dysplastic BM to AdCa.
Conclusion: Neoplastic progression in the oesophagus is associated with altered expression of specific TIMPs and MMPs. Levels of TIMPs -1 to -3 mRNA are maximal at the stage of BM but decline at the stage of AdCa. In BM, enhanced expression of protease inhibitors would reduce ECM degradation and favour fibrosis (for example, peptic stricture), whereas in AdCa the finding of elevated MMP-8 but falling TIMPs would suggest enhanced proteolyis favouring malignant infiltration and metastasis. TIMP-4 may have potential as a biomarker of progression.
414 IMPACT OF THE “TWO WEEK RULE” AND ROUTE OF DIAGNOSIS ON OUTCOME OF OESOPHAGEAL CANCER
N. Stern1, N. Kapoor1, R. Sturgess1, K. Bodger1,2.1Aintree Centre for Gastroenterology, University Hospital Aintree; 2School of Clinical Sciences, University of Liverpool, Liverpool, UK
Background: The UK National Cancer Plan aimed to improve patient outcomes by raising awareness of “alarm symptoms” and establishing a two week waiting time standard for fast track specialist assessment. In this study we aimed to establish the impact of our Rapid Access Upper GI Cancer Service (RAUGICS)1 on patient outcomes and to assess whether patients continuing to access care via traditional routes are at a disadvantage.
Methods: (A) Using hospital IT systems, a cancer service database1 and casenotes, we audited outcome of all oesophageal cancer (O-Ca) diagnosed during two 2 year periods, one before (PRE-) and one after (POST-) the implementation of the RAUGICS system. Data for tumour type, stage, operability, and 2 year survival were obtained. (B) In the post “two week rule” (TWR) period, route of diagnosis of cancer was designated as: RAUGICS (preferred route, n = 3008 referrals), traditional open access endoscopy (OAE), outpatient clinic (OPD), emergency admission (A&E). We audited Barrett’s surveillance (BarS; n = 420 patients).
Results: (A) Pre versus post RAUGICS periods: Cases: 72 v 95; Mean age: 68 v 68; Surgery (curative intent): 38% v 26%; 2 year survival: 19.4% v 24.2% (AdenoCA: 22.5% v 25.4%; squamous cell CA: 16.1% v 25%). All non-significant. (B) Route of diagnosis: 2 year survival: RAUGICS 18%; other routes (OAE, OPD, A&E): 30%; and BarS 50%. BarS detected CA at a rate of 0.49% per annum (6.5% of all AdenoCA cases in the population).
Conclusions: Major service reorganisation took place to ensure fast-track assessment of patients with alarm symptoms. Overall survival for O-Ca has not improved significantly. Cases of cancer continue to be diagnosed by traditional routes but these selected cases have a better outcome than those in the RAUGICS system overall, suggesting earlier stage disease diagnosed “by chance” in patients without obvious alarm features. The current fast-track system selects mainly patients with late-stage disease and a poor outcome. Cancers detected via BarS have superior survival but represent only a minority of tumours diagnosed. Prompt palliation is a worthwhile outcome of the TWR but a screening programme is needed if survival is to improve for O-Ca.
1
415 A LARGE SERIES, RESECTION CONTROLLED STUDY TO ASSESS THE VALUE OF RADIAL EUS IN RE-STAGING OESOPHAGEAL CANCER AND PREDICTING SURVIVAL FOLLOWING NEOADJUVANT CHEMOTHERAPY
S. Mesenas, C. Vu, M. McStay, L. Doig, B. Baburajan, M. Forshaw, A. Botha, R. Mason, J. Meenan.Departments of Gastroenterology and Surgery, Guy’s and St Thomas’ Hospital, London, UK
Background: The utility of EUS post neoadjuvant chemotherapy for esophageal carcinoma is not established. Superior loco-regional detail may yield useful staging and prognostic information but information on its true clinical value as compared with CT is limited.
Method: We prospectively studied 109 patients with esophageal cancer; 99 undergoing surgery. All had EUS and helical CT imaging before and after neoadjuvant chemotherapy and results were compared with pathological staging of resected specimens. Tumour response was assessed by reduction in maximal tumour depth at EUS and correlated with patient survival.
Results: There was no difference in T and N stage accuracies between EUS and CT following neoadjuvant chemotherapy. Multivariate analysis showed a reduction in maximal tumour depth by >50% at EUS to be associated with longer survival (relative risk = 0.48, p<0.05). EUS responders had a median survival of 38 months compared to 30 months for non-responders (p<0.05). The identification of lymphadenopathy at radial EUS was not predictive of survival.
Conclusion: This large series study demonstrates the staging accuracy of CT and non-biopsy EUS in the setting of neoadjuvant chemotherapy for esophageal cancer to be equivalent and poor. Endosonography may contribute useful clinical information in respect of potential survival.
416 LOCAL RISK FACTORS FOR SQUAMOUS CELL OESOPHAGEAL CARCINOMA IN A SOUTH ASIAN COMMUNITY
A. A. Sheikh1, H. U. Qureshi2, A. J. Raja3 (introduced by R. Sutton1).1Royal Liverpool and Broadgreen University Hospitals, Liverpool, U.K; 2University Hospitals of Leicester, Leicester, UK; 3The Aga Khan University Hospital, Stadium Road, Karachi, Pakistan
Background: Squamous cell carcinoma of the oesophagus is the 8th most common cancer in women and the 5th most common cancer in men in South Asia. Tobacco is not only smoked but is also chewed in various forms (naswar and paan) extensively in South Asia as well as by South Asian communities living abroad. Naswar is a crude form of chewing tobacco where as paan is a quid of piper betel leaf containing areca nut, lime, condiment, sweeteners, and sometimes tobacco. Studies have linked the use of these products with oral and pharyngeal carcinomas however, no work examining their role in oesophageal carcinoma has been done.
Methods: The aims of this study were to identify the risks associated with oesophageal carcinoma in a South Asian population with a particular focus on paan consumption. Biopsy proven primary cases of squamous cell carcinoma of the oesophagus from three major tertiary referral centres were recruited for the study. Controls were pair matched for age, gender and hospitals, excluding subjects with a past or present history of any type of malignancy. Variables that were statistically significant in univariable analysis were further examined through multivariable conditional logistic regression.
Results: There were 91 cases and 364 controls with a male to female ratio of 1:1. The average age was 54 years (age range: 22–90). People with oesophageal carcinoma were at 11 times higher odds of being users of paan with tobacco (95% CI 5 to 24). Other significant associations were paan without tobacco (OR 3.6), naswar (OR 3.4), and smoking (OR 2.5), after adjustment for other covariates. No significant associations were identified between subethnic groups and oesophageal carcinoma.
Conclusion: This study identifies independent associations of paan (with or without tobacco), naswar and smoking with squamous cell oesophageal carcinoma. These findings are of public health significance in South Asian communities.
417 SIMVASTATIN INDUCES APOPTOSIS AND INHIBITS PROLIFERATION IN OESOPHAGEAL ADENOCARCINOMA CELLS BY INHIBITING ACTIVATION OF EXTRACELLULAR SIGNAL RELATED KINASE (ERK) AND AKT
O. O. Ogunwobi, I. L. P. Beales.Gastroenterology Unit, Norfolk and Norwich University Hospital & School of Medicine, University of East Anglia, Norwich, UK
Background: The incidence of oesophageal adenocarcinoma (OAC) is rapidly increasing in the western world. Statins are widely used in obese people and studies suggest that they may have oncoprotective actions. Obesity is an important risk factor for Barrett’s oesophagus and OAC. We hypothesised that statins may have beneficial effects in OAC.
Methods: The effects of simvastatin, lovastatin, and pravastatin on the OE33 OAC cell line were assessed. Proliferation was measured using thiazoyl blue and bromodeoxyuridine incorporation assays and apoptosis by ELISA for intracellular nucleosomes. Add back experiments were used to determine the involvement of intermediates in the cholesterol biosynthetic pathway. Direct detection of activated kinases and immunoblotting were used to determine the effects on intracellular pathways.
Results: All three statins inhibited proliferation in a similar dose dependent manner. This effect was partially dependent on farnesylation and the availability of mevalonate. Simvastatin increased apoptosis by 40%. Statins significantly enhanced the antiproliferative effect of the COX-2 inhibitor NS-398, but did not enhance the effects of cisplatin and 5-fluorouracil. These effects were associated with significant inhibition of serum-induced phosphorylation of extracellular signal-related kinase (ERK) and Akt but did not affect p38 MAP kinase or JNK phosphorylation. Statins did not affect levels of membrane associated Ras and Rho, or Ras activity.
Conclusions: Statins inhibit proliferation and induce apoptosis in OAC cells, and further enhance the antiproliferative effects of COX-2 inhibition. Statins inhibit the ERK and Akt pathways, which are involved in proliferation and cell survival, but this is not due to inhibition of membrane associated GTPases. Statins may have beneficial effects in Barrett’s oesophagus and further study is warranted.
418 DIETARY FISH OIL LOWERS MUCOSAL PGE2 LEVELS DURING OESOPHAGEAL ADENOCARCINOGENESIS
A. P. Boddy1, S. Mehta1, I. T. Johnson2, M. Rhodes1, E. K. Lund2.1Department of Surgery, Norfolk and Norwich University Hospital, UK; 2Institute of Food Research, Norwich, UK
Background: There is evidence that n-3 (omega-3) fatty acids can inhibit carcinogenesis, perhaps through suppression of prostaglandin biosynthesis. Using a previously developed animal model of oesophageal adenocarcinoma we have compared the effects of dietary fish oil versus corn oil on prostaglandin E2 (PGE2) levels during the early stages of carcinogenesis.
Methods: Oesophagojejunostomy was performed on 24 male Sprague-Dawley rats which were then given a diet providing 15% energy from fat. Twelve were fed a diet based on corn oil (high in n-6 fatty acids) and 12 on a diet based on fish oil (high in n-3 fatty acids). Twenty one animals survived 10 weeks post-surgery, at which point they were sacrificed and gastroesophageal tissues were harvested. Mucosa from the distal oesophagus was assayed for PGE2 levels and lipid peroxidation. Gastric tissue was analysed for fatty acid profile and serum CRP levels were also measured.
Results: Animals fed on fish oil had significantly higher levels of tissue n-3 fatty acids than those fed corn oil (5.46% v 0.31%, p<0.001). There was less oesophageal PGE2 in animals fed fish oil compared to corn oil (22.3 v 60.0 ng/mg protein, p = 0.005). Furthermore, CRP levels were also lower in the fish oil group (5.37 v 6.44 μg/ml, p = 0.007). However, there was no significant difference in the degree of lipid peroxidation as measured by thiobarbituric acid reactive substance (72.8 v 110.8 nmol/g protein, p = 0.117).
Conclusions: In this model dietary fish oil significantly altered the fatty acid profile in mucosal tissue and reduced biosynthesis of oesophageal PGE2. Further investigation is needed to determine whether n-3 supplementation in humans can cause similar changes in patients at risk of developing oesophageal adenocarcinoma.
419 NSAIDS INDUCE LTB4: A POSSIBLE MECHANISM BY WHICH NSAIDS PREVENT OESOPHAGEAL CANCER
A. Shonde, K. Ragunath, A. J. Bennett, C. J. Hawkey.Wolfson Digestive Diseases Centre University of Nottingham, Division of Gastroenterology, University Hospital Nottingham, Nottingham NG7 2UH, UK
Background: There are 4000 deaths per annum from oesophageal cancer and it has a five year survival rates in the UK of under 10%. Oesophageal cancer commonly arises from Barrett’s oesophagus. NSAIDs appear to reduce incidence of this cancer. This may be by substrate diversion from the cyclooxygenase pathway to the lipoxygease pathway producing LTB4, a PPARα ligand. We have investigated the hypotheses that:
1. Cyclooxygenase inhibition enhances production of leukotriene (LT)B4.
2. Enhanced LTB4 causes regression by ligand activation of peroxisome proliferators activated receptor (PPAR)α.
Aims: (1) To establish LTB4 synthesis in organ culture from normal oesophageal tissue, Barrett’s oesophagus, and oesophageal adenocarcinoma. (2) To assess if NSAIDs increase LTB4 synthesis in these three tissue types.
Method: Samples from oesophageal squamous epithelium, Barrett’s oesophagus, or oesophageal adenocarcinoma were placed in organ culture (RPMI 1640, 10% FCS, 95% 02/5% CO2, 37°C) with or without indomethacin 10−6M and 10−5M. After 24 hours LTB4 was measured in culture medium by ELISA.
Results: LTB4 levels are higher in oesophageal adenocarcinoma than in Barrett’s oesophagus and oesophageal squamous epithelium. The mean LTB4 level was 15.2 (4.1) (mean (SEM)) pg/mg in oesophageal squamous epithelium, 20 pg/mg (4.8) in Barrett’s oesophagus and 28.4 (7.1) pg/mg in oesophageal cancer (n = 6, not significant). Indomethacin caused a concentration dependant increase in LTB4 synthesis. The addition of indomethacin 10−6M and 10−5M resulted in mean LTB4 levels of 170 pg/mg (87.4) and 321 pg/mg (8.1) in squamous epithelium and 294 (89.8 and 543 (121.3) in Barrett’s oesophagus and 450 pg/mg (6.2), and 720 pg/mg (7.4) in oesophageal cancer.
Conclusions: Oesophageal mucosa is capable of synthesizing LTB4. Indomethacin causes a substantial significant increase in synthesis in all the above oesophageal epithelium, sufficient to affect PPARα activity substantially.
420 CHEMICALS FORMED FROM THE GASTRIC ACIDIFICATION OF SALIVARY NITRITE INFLUENCE OESOPHAGEAL AND GASTRIC FUNCTION
J. J. Manning, A. Wirz, K. E. L. McColl.University Department of Medicine, Western Infirmary, Glasgow, UK
Introduction: Saliva contains high concentrations of nitrite derived from the enterosalivary recirculation of nitrate and its reduction by buccal bacteria. Acidic gastric juice converts the nitrite to varying proportions of nitrous acid and nitric oxide determined by vitamin C availability. Nitric oxide (NO) and nitrous acid relax the stomach, lower oesophageal sphincter (LOS), and oesophageal body. Neuronally generated NO contributes to the pathophysiology of GORD, playing a major role in upper gastrointestinal motility.
Aim: To determine whether luminal administration of NO or nitrous acid alters oesophageal or gastric function.
Method: Fifteen Helicobacter pylori negative healthy volunteers were studied on three separate days. A manometry catheter was placed across the lower oesophageal sphincter (LOS) after a meal, to record oesophageal, LOS and gastric pressure and transient lower oesophageal sphincter relaxations (TLOSRs). Two pH probes were placed in the oesophagus to record reflux events. On each day one of three solutions was infused for one hour into the region of the LOS. (1) Control solution of hydrochloric acid pH1.0 (HCl), (2) HCl plus nitrite ie: nitrous acid, and (3) HCl plus nitrite, plus ascorbic acid to generate NO. Solutions were randomised and double blinded.
Results: The NO solution gave a significantly increased oesophageal acid exposure, 62.2%, compared to both control, 37.5% (p<0.03) and nitrous acid, 36.6% (p<0.002). The frequency of TLOSRs was also significantly increased by the NO solution (5.2/hour) compared to both control (3.5, p<0.01) and nitrous acid (3.1, p<0.0001). There was also evidence of impaired oesophageal clearance of acid refluxate following the NO infusion. Intragastric pressure was 3.4 mmHg lower in the nitrous acid group during the meal (p<0.03) compared to the control.
Conclusion: Luminal chemicals formed from the acidification of salivary nitrite influence both oesophageal and gastric motility and may play a role in the aetiology of gastric and oesophageal disorders.
421 ENDOSCOPIC PROGRESSION OF GASTRO-OESOPHAGEAL REFLUX DISEASE OVER SEVEN YEARS
M. Fullard, S. Gupta, R. J. Leicester, P. J. Neild, A. Poullis, J. D. Maxwell, J. Y. Kang.Departments of Gastroenterology and Surgery, St George’s Hospital, London, UK
Background and Aim: Some authors feel that non-erosive reflux disease (NERD), erosive oesophagitis and Barrett’s oesophagus (BO) represent different stages of gastro-oesophageal reflux disease (GORD), which can progress over time. Others have suggested they are distinct entities which tend to remain unchanged. We aim to determine whether the endoscopic severity of GORD progresses over time.
Methods: A prospectively collected database (Micromed) of all upper GI endoscopies (OGD) performed in the hospital was retrospectively examined, looking for disease progression.
Results: From 01/01/98 to 31/12/04, 14 170 OGDs were performed on 12 966 patients (48% male, mean age 58 years). 882 patients had more than one OGD. Of 739 patients initially without oesophagitis (277 of whom had reflux symptoms), 134 (18%) developed oesophagitis at the second endoscopy (mild 71 (54%), moderate 45 (34%), severe 15 (11%)), after a mean time interval of 134 days. BO developed in two patients. The mean age of the 134 patients was 60 years. Thirteen patients (9%) were using a proton pump inhibitor (PPI) at the first OGD, 38 at the second (28%). Of 143 patients with oesophagitis at the first endoscopy (mild 85 (59%) moderate, 37 (26%) severe 21 (15%)), oesophagitis resolved in 118 (83%) and remained unchanged in 20 (14%) but progressed in five (3%) (2 developed moderate oesophagitis, 1 severe oesophagitis, 2 developed BO and 1 developed a cancer). The five patients who progressed had a mean age of 56 years and a time interval between OGDs of 753 days. Only one of the patients was taking a PPI at either first or second OGD. The 138 patients in whom oesophagitis did not progress had a mean age of 62 years, a mean of 630 days between OGDs. 19 (14%) were using a PPI at the first OGD, 38 (28%) at the second.
Conclusion: Although the grade of oesophagitis remains stable in the majority of patients, it does progress in a small number, with oesophagitis progressing to more severe oesophagitis, BO or cancer in 3% of patients.
422 THE ORACLE (OESOPHAGEAL REFLUX AND CHANGE IN LIFESTYLE EVALUATION) STUDY
G. Sivaji1, S. Corbett2, S. Podbur1, M. Welfare2, R. K. Thomson1.1Wansbeck General Hospital, UK, 2North Tyneside General Hospital, UK
Background: Gastro-oesophageal reflux disease (GORD) is highly prevalent in the Western population. It has a significant effect on the sufferer’s physical health and health related quality of life (HrQOL). An ideal intervention should aim to improve both the symptoms and HrQOL. Lifestyle recommendations as treatment for GORD so far lacks strong scientific support.
Aim: To study in depth the effects of a patient targeted dietary advice and lifestyle intervention on the symptoms and HrQOL of the patient.
Methods: Patients with ongoing symptoms of GORD and Savary-Miller grade 1 or less oesophagitis on gastroscopy were screened and suitable subjects randomised. Subjects in arm 1 were met by the researcher for 30 minutes, leaflets provided and advised on standard lifestyle recommendations. Subjects in arm 2 met the researcher and then a dietician. A patient specific dietary intervention with special focus on weight loss was provided. The GORD questionnaire was used as the measuring tool. The main outcome measures were GORD symptom scores (GSF, GSB), eating related scores (ESF and ESB), and sleep related score (PSL). An increase of 9 or more at six months is considered significant.
Results: 2450 patients were screened over a period of 18 months. 180 patients were suitable and randomised. 110/180 (61%) were female. The GSF score increased by 19.5 and 24, the GSB score increased by 14 and 22, the ESF score increased by 9 and 18, the ESB score increased by 6.9 and 15.8, and the PSL score increased by 13.7 and 24 in the arms 1 and 2 respectively.
Discussion: There was a significant increase in all the scores except the ESB in arm 1.The increase in scores in arm 2 was seen in all outcome measures, was significant and more pronounced. However the increase in scores compared to arm 1 did not attain statistical significance.
Conclusion: A structured dietary and generic lifestyle advise given by a professional improves GORD symptoms and HrQOL in the sufferers. The intervention provided was pragmatic and could be replicated in the primary care setting. A further study with longer follow up to assess the sustainability of the improvement in score is needed.
423 MODERATE–SEVERE REFLUX OESOPHAGITIS HEALING RATES AT EIGHT WEEKS WITH FULL DOSES OF ESOMEPRAZOLE, PANTOPRAZOLE, LANSOPRAZOLE, AND OMEPRAZOLE
J. Labenz1, A. Leodolter1, E. Beresford2 (introduced by A. J. Morris).1Medical Department, Jung-Stilling-Krankenhaus, Siegen, Germany; 2AstraZeneca, Luton, UK
Introduction: Several large studies have compared reflux oesophagitis (RO) healing rates of esomeprazole versus pantoprazole, lansoprazole, and omeprazole.1–3 Data versus rabeprazole are not available. Patients with moderate to severe RO (LA Grades C and D) demonstrate higher failure rates at week 4 and 8 than those with RO Grades A–B. To investigate PPI efficacy in this difficult-to-treat group, this analysis pooled data from previous studies to determine healing rates in patients with LA Grades C & D only.
Aims and Methods: Patients with confirmed RO (LA Grades A–D) were enrolled into three randomised, controlled, multicentre studies of similar design. Patients received either esomeprazole 40 mg od (E40), pantoprazole 40 mg od (P40), lansoprazole 30 mg od (L30), or omeprazople 20 mg od (O20) for up to eight weeks. Crude healing rates for Grades C & D were pooled and differences assessed using a χ2 test.
Results: The percentage of patients with moderate to severe RO who were healed after four or eight weeks treatment was significantly greater with E40 compared with either P40, L30 or O20 (see table).
Abstract 423
Conclusion: Esomeprazole 40 mg provided significantly better healing of RO Grades C & D than pantoprazole 40 mg, lansoprazole 30 mg, and omeprazole 20 mg at both 4 and 8 weeks. Esomeprazole is therefore the PPI of choice in healing patients with moderate/severe RO.
1
2
3
424 MODERATE–SEVERE REFLUX OESOPHAGITIS REMISSION RATES AT SIX MONTHS WITH LOW DOSES OF ESOMEPRAZOLE, PANTOPRAZOLE, AND LANSOPRAZOLE
J. Labenz1, A. Leodolter1, E. Beresford2 (introduced by A. J. Morris).1Medical Department, Jung-Stilling-Krankenhaus, Siegen, Germany; 2AstraZeneca UK, Luton, UK
Introduction: The efficacy of low dose esomeprazole (20 mg) has been compared with low doses of pantoprazole (20 mg) and lansoprazole (15 mg) in two large studies.12 Patients with moderate to severe RO (LA Grades C & D) demonstrate higher failure rates at six months than those with RO Grades A and B. To investigate PPI efficacy in this difficult-to-treat group, this analysis pooled data from previous studies to determine remission rates in patients with LA Grades C and D only.
Aims and Methods: Patients with confirmed RO (LA Grades A–D) were enrolled into two randomised, controlled, multicentre studies of similar design. Patients received either esomeprazole 20 mg od, pantoprazole 20 mg od, or lansoprazole 15 mg od for up to six months. Life table estimates of the percentage of patients in remission at 6 months were calculated for Grades C and D only.
Results: The percentage of patients with moderate to severe RO who remained in remission after six months treatment was significantly greater with esomeprazole 20 mg compared with either pantoprazole 20 mg or lansoprazole 15 mg (see table).
Abstract 424
Conclusion: Esomeprazole 20 mg provided significantly better control of RO Grades C & D than either pantoprazole 20 mg or lansoprazole 15 mg at six months. Esomeprazole provides predictable efficacy in maintaining remission in patients with moderate to severe RO.
1
2
425 DOES LAPAROSCOPIC ANTIREFLUX SURGERY IMPROVE QUALITY OF LIFE IN PATIENTS WHOSE GASTRO-OESOPHAGEAL REFLUX DISEASE IS WELL CONTROLLED WITH MEDICAL THERAPY?
R. S. Gillies, J. M. Stratford, L. Jones, J. Sohanpal, M. I. Booth, T. C. B. Dehn.Departments of Upper GI Surgery and GI Physiology, Royal Berkshire Hospital, Reading, UK
Background: Both medical therapy and laparoscopic anti-reflux surgery (LARS) have been shown to improve quality of life in gastro-oesophageal reflux disease (GORD). While patients with poor symptom control or side effects on medical therapy might be expected to have improved quality of life after surgery, no study has examined whether patients well controlled on medical therapy who choose to undergo surgery (patient preference) might also experience improved quality of life.
Aim: To determine if LARS can improve quality of life in GORD patients even if their symptoms are well controlled on medical therapy.
Method: Between October 1998 and September 2003 all patients undergoing LARS were asked to complete three quality of life questionnaires preoperatively, while on medical therapy, and six months following LARS. Two questionnaires were generic, Short Form 36 (SF-36) and Psychological General Well-Being index (PGWB); one was disease specific, Gastrointestinal Symptom Rating Scale (GSRS). The indication of patient preference for LARS was clearly identified in all patients prior to surgery.
Results: Completed questionnaires were received from 44 patients who underwent LARS for patient preference: 36 male, 8 female; mean age 42 (15–66) years. Preoperative quality of life scores while on medical therapy were significantly improved six months following LARS: SF-36 median physical composite scores 52 and 54 (p<0.05) and mental composite scores 51.5 and 56 (p<0.05); PGWB median total scores 77 and 90 (p<0.0001); GSRS median total scores 2.13 and 1.70 (p<0.001) and reflux scores 2.25 and 1.00 (p<0.0001).
Conclusion: LARS can significantly improve quality of life in GORD patients whose symptoms are well controlled on medical therapy. Such patients, therefore, should be considered for LARS.
426 A RANDOMISED TRIAL OF LAPAROSCOPIC TOTAL FUNDOPLICATION VERSUS POSTERIOR PARTIAL FUNDOPLICATION FOR GASTRO-OESOPHAGEAL REFLUX DISEASE BASED ON PREOPERATIVE OESOPHAGEAL MANOMETRY
T. C. B. Dehn, J. M. Stratford, J. Sohanpal, M. I. Booth.Departments of Surgery, Royal Berkshire Hospital, Reading, UK
Aims: To assess (1) whether tailoring the operative procedure to preoperative oesophageal motility had any bearing on the results of fundoplication, whether performed by 360° or 270° laparoscopic fundoplication, and (2) whether there was any difference in outcome between total and partial fundoplication.
Methods: Prospective randomised trial. Preoperative motility assessed by solid state manometry. Patients were divided into normal or ineffective (more than 30% peristaltic waves with less than 30 mmHg amplitude) motility. Each group was randomised by sealed envelope into 360° or 270° laparoscopic fundoplication. All operations were performed with division of the short gastric vessels and fundoplication over a 56 Malonie bougie. A cruroplasty was performed in all patients. Follow up was by nurse physiologist. Symptoms were assessed by Visick grading and use of structured questionnaire pre and postoperatively (6 weeks, 6 months, and 1 year). Oesophageal manometry and pH were repeated at 6 months.
Results: Sixty seven patients underwent total and 63 partial fundoplication. No significant differences were reported in heartburn, regurgitation, dysphagia, post-prandial fullness, gas bloat inability to burp, increased flatus, diarrhoea, or abdominal pain at any of the postoperative intervals. Chest pain was more common at one year in the 360° group (p = 0.03). There were eight failures on postoperative pH test: three in the 360° and five in the 270° groups. Patients in the ineffective motility group did not suffer any more dysphagia postoperatively than those in the normal motility group, whether they underwent a total or partial fundoplication.
Conclusions: (1) any differences in the symptomatic outcome of laparoscopic total or partial fundoplication appear minimal. (2) Tailoring the fundoplication to preoperative oesophageal motility has no scientific or clinical basis.
427 OESOPHAGEAL SOLID BOLUS TRANSIT: STUDIES USING CONCURRENT VIDEOFLUOROSCOPY AND HIGH RESOLUTION MANOMETRY
M. Fox1, M. Fried2, W. Schwizer2.1St Thomas Hospital, London; 2University Hospital Zürich, Switzerland
Introduction: The efficacy of oesophageal solid bolus transit is less efficient than that of liquids in health and disease.1 The biomechanics of oesophageal function are complex and current investigations do not collect data that fully addresses the relationship between motor function and bolus transport. A recent study has shown that high-resolution manometry (HRM) demonstrates the segmental anatomy of the oesophagus and predicts the success of liquid bolus transport more accurately than conventional manometry.2
Aims and Methods: Concurrent HRM and videofluoroscopy were performed to study solid bolus transport. 18 healthy volunteers were studied while swallowing 10 ml liquid barium and 10 mm diameter barium marshmallow bolus in a supine posture. HRM and videofluoroscopy data was analysed separately and in a blinded fashion. The characteristics and coordination of oesophageal peristalsis on HRM were assessed and related to the success of solid bolus transport.
Results: Oesophageal clearance of liquid and solid bolus was 88% v 65% of swallows respectively (p<0.01). For successful swallows, peristaltic velocity was slower (p<0.05) with solid than liquid bolus, contraction pressures were higher (p<0.05) and the pressure gradient across the GOJ was greater (p<0.01). Intra-individual reproducibility was high for HRM and videofluoroscopy findings. Most failures (86%) of bolus transport occurred in 7/18 subjects. Solid bolus escape was most common at the pressure trough between the proximal and mid segments of oesophageal peristalsis. This “transition zone” was wider in failed than successful swallows (1.7 v 2.9 cm, p<0.01).
Conclusion: In healthy subjects bolus properties alter the pressure and velocity of peristalsis. When bolus escape occurs it is usually between the proximal and mid-oesophageal segments. Coordination between segmental contractions appears to be more important to the success or failure of solid bolus transport than contraction pressure.
1
2
428 EOSINOPHILIC OESOPHAGITIS, AN EMERGING CAUSE OF DYSPHAGIA
Y. Reddy, K. P. Basavaraju, N. K. Ahluwalia.Stepping Hill Hospital, Stockport, UK
Background: Eosinophilic oesophagitis (EO) in adults is a recently described but under recognised condition. EO is characterised by intermittent and often painful dysphagia which may become persistent as the disease progresses. It is predominantly seen in men and a small proportion of these patients have atopic predisposition. Endoscopic appearances vary from small calibre, multi-ringed to a normal looking oesophagus. The average time to diagnosis from the first presentation of the symptom is usually in terms of years. This is mainly due to lack of awareness of the condition and the reluctance to biopsy an otherwise normal looking oesophagus. Diagnosis is made by detection of >20 eosinophils per high power field in the oesophageal biopsies. Treatment with corticosteroids (topical or oral) or leukotriene antagonist (Montelukast) has been successful in resolving symptoms in majority of patients.
Methods: We have identified 11 cases of eosinophilic oesophagitis who presented to our unit with recurrent attacks of dysphagia of long duration between 2002 and 2005. The mean age of the patient was 45.09 years and 10/11 patients were males. Three patients had atopic predisposition with hay fever, asthma and eczema respectively. Endoscopic appearances varied from ringed oesophagus in two patients, small hiatus hernia in three, schatzki ring in one, and normal looking oesophagus in five patients. Random biopsies over a length of oesophagus were taken in all and the diagnosis was confirmed by histological demonstration of eosinophils >20 per high power field. Eight patients have been treated with oral corticosteroids and three patients with montelukast. Six patients have reported subjective improvement in the symptoms and others at present are under review.
Conclusions: The recognition of EO as an underlying cause of recurrent dysphagia is steadily increasing. High clinical and endoscopic vigilance along with histological assessment is the key to the diagnosis of this chronic condition. We would recommend oesophageal biopsies to look for EO in all patients presenting with recurrent dysphagia in the absence of any other obvious cause.
429 A REVIEW OF PATIENTS WITH ACHALASIA CARDIA AND MEGAOESOPHAGUS: A SINGLE CENTRE EXPERIENCE
R. Singh, G. Shanmugananthan, K. K. Kuat (introduced by K. Ragunath).Gastrointestinal and Endoscopy Unit, Hospital Kuala Lumpur, Malaysia
Introduction: Megaoesophagus is defined as an oesophagus measuring 8 cm or larger on the barium swallow examination in patients with achalasia cardia. Its existence defines a late stage of achalasia cardia and therapy will include an oesophagectomy or pneumatic dilatation in the management. The former carries a high morbidity and mortality especially in centres with low patient load.
Method: We reviewed retrospectively all patients with achalasia cardia from January 2000 to December 2004 and identified 10 patients with megaoesophagus who subsequently underwent pneumatic dilatation.
Results: The average presenting age is 52 (SD 15) (range 20–73) years with four males and six females, out of which five were Malays, three were Chinese, and two Indians. The duration of illness before diagnosis was 7 (SD 5) (range 1–16) years. All patients had dysphagia, regurgitation, and weight loss. All 10 patients demonstrated aperistalsis but interestingly eight patients failed lower oesophageal sphincter (LES) intubation during standard esophageal manometry due to coiling of the catheter. Failure to elicit failure of relaxation of the LES translates as a high technical failure of manometry (80%) in the diagnosis of achalasia cardia. A confident diagnosis of achalasia cardia was made on barium swallow all 10 cases (100%). All 10 patients underwent pneumatic dilatation. Eight patients required only single dilatation. However two patients required two dilatations. The durability of the 12 pneumatic dilatations was 27 (SD 13) (range 9–44) months with good symptomatic relieve and an objective post procedural weight gain of 10 (SD 6) (range 1–19) kg over a period of 3–12 months. There was no complications noted post procedure.
Conclusions: In advanced cases of achalasia cardia, barium swallow is superior to manometry for obtaining the diagnosis. Pneumatic dilatation is a safe procedure with good durability and symptomatic improvement in patients with megaoesophagus.
NEUROGASTROENTEROLOGY/MOTILITY POSTERS
430 INDUCING A VIRTUAL LESION IN THE HUMAN SWALLOWING MOTOR CORTEX
S. Mistry1, J. Rothwell2, D. G. Thompson1, S. Hamdy1.1University of Manchester, Department of GI Sciences, Hope Hospital; 2Institute of Neurology, Queens Square, London, UK
Background: Cortical control of swallowing is bilateral but displays inter-hemispheric asymmetry, with dominant (D) and non-dominant (ND) projections. However, the precise relationship between these D and ND pathways remains unclear. 1 Hz repetitive transcranial magnetic stimulation (rTMS) can transiently suppress brain excitability non-invasively (a virtual lesion) with effects on peripheral function. Until now, a virtual lesion has not been applied to bilateral systems such as swallowing.
Aims: We assessed the effects of a 1 Hz rTMS induced virtual lesion on the excitability of D and ND swallowing motor cortex (SMC) and compared this to hand MC.
Methods: Seven healthy adult volunteers (four male, age range 25–46) had EMG excitability measurements from the pharynx and the hand in response to TMS before and up to 60 minutes post 1 Hz rTMS. Real and sham rTMS paradigms (600 pulses over D SMC) were applied at 120% of pharyngeal resting motor threshold and randomised to separate days. Data were analysed using a non-parametric ANOVA.
Results: Real 1 Hz rTMS dramatically suppressed D SMC by 36 (SD 6)% (*p<0.006) immediately and for up to 45 minutes afterwards (fig). Hand MC was similarly suppressed by 41 (SD 13)% (†p<0.01) up to 30 minutes whereas ND SMC showed a transient increase in activity. In contrast, sham rTMS had no effect.
Conclusions: An rTMS induced virtual lesion can induce differential interhemispheric suppression and excitation of SMC. These compensatory changes may be relevant to mechanisms of recovery after dysphagic stroke, a likely consequence of the bilateral innervation pattern for swallowing.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract 430 Changes in excitability in swallowing and hand motor cortex following real 1 Hz rTMS.
431 A COMPARISON OF SELECTIVELY ATTENDED VISCERAL AND SOMATIC PAIN
P. Dunckley1,2, Q. Aziz3, R. G. Wise1,2, J. Brooks1,2, I. Tracey1,2, L. Chang4.1Departments of Human Anatomy and Genetics & FMRIB, University of Oxford, Oxford, OX1 3QX, UK; 3Department of GI Science, Clinical Sciences Building, University of Manchester, Hope Hospital, Salford M6 8HD, UK; 4Center for Neurovisceral Sciences and Women’s Health, Division of Digestive Diseases, David Geffen School of Medicine at UCLA, LA, USA
Background: Visceral and somatic pain differ in several key aspects—visceral pain is described as ill defined and diffuse and results in divergent coping strategies to somatic pain (quiescence as opposed to escape). These differences in perception must be reflected in differing cortical patterns of activation. We have used a paradigm of attentional modulation to study the differences in matched selectively attended visceral and somatic pain.
Methods: Twelve healthy, pain-free, right handed subjects were recruited for the study. Simultaneous electrical pulses and auditory tones lasting six seconds were delivered to the subjects during a whole-brain functional scan acquisition. The electrical catheter was placed into the rectum for the visceral scan and onto the lower abdomen for the somatic scan. Subjects were instructed to attend to and count either the auditory tones or electrical pulses. Electrical pulses and auditory tones were delivered at either 2, 3.5, or 4.3 Hz thereby varying the cognitive demand of the tasks. Pain intensity, unpleasantness and tone/pulse count were recorded after each stimulus.
Results: Pain intensity and unpleasantness were well matched for the two sensory modalities. Selective attention to both modalities resulted in activation in sensory-discriminative (secondary somatosensory cortex), affective (anterior insula, rostral-cingulate cortex), and cognitive (mid-cingulate cortex) regions. Subtraction analysis (selectively attended visceral pain minus somatic pain and vice versa) identified greater activation during visceral pain in the right thalamus, right hypothalamus, mid-cingulate cortex, bilateral cerebellum, and the right anterior insula (during the 4.3 Hz condition alone). There were no areas of greater activation during somatic pain.
Conclusions: Selectively attended visceral pain results in greater activation of affective (right anterior insula), autonomic (right hypothalamus), and attentive (mid-cingulate) regions compared with matched selectively attended somatic pain.
432 THE EFFECT OF PRE-STUDY ANXIETY STATE IN MEDIATING THE MAGNITUDE OF SENSITISATION IN A HUMAN MODEL OF VISCERAL PAIN HYPERSENSITIVITY
A. Sharma, Q. Aziz, C. Delaney, A. R. Hobson.Section of GI Sciences, University of Manchester, Hope Hospital, UK
Background: Patients with stress or anxiety at the time of gastrointestinal injury/inflammation (for example, gastroenteritis) have a higher risk of developing subsequent irritable bowel syndrome (IBS), but the mechanisms are uncertain. We have previously shown that oesophageal pain thresholds (PT) are inversely correlated with anxiety scores.1 In addition, we have shown that distal oesophageal acidification induces sensitisation of spinal dorsal horn neurones leading to the development of pain hypersensitivity (PH) in the non-acid exposed proximal oesophagus (PO) and chest wall (CW).2 The effect of anxiety in modulating the magnitude of sensitisation to oesophageal acid has not been studied.
Aim: To determine whether the magnitude of PH after oesophageal acidification correlates with pre-study anxiety state.
Methods: In 14 healthy volunteers the Spielberger State Anxiety Inventory (SAI), a validated measure of state anxiety, was completed. PT to electrical stimulation (in milliamperes, mA) were determined in the PO, CW, and foot pre and post a 30 minute distal oesophageal infusion of 0.15M HCl.
Results: Mean SAI score was 30.8 (SD 8.7, range 20–51). Acid infusion resulted in a reduction in PT in the PO (35.3 mA (SD 5.8 mA) v 25.8 mA (SD 7.7 mA), p<0.0001) and CW (31.3 mA (SD 13.5 mA) v 27.5 mA (SD 8.7 mA), p = 0.04) but not the foot (22.6 mA (SD 11.1 mA) v 22.3 mA (SD 9.7 mA), p = 0.8). There was a negative group correlation between baseline SAI score and maximum decrease in PT post acid (magnitude of sensitisation) in the PO (r = −0.572, 95% CI −0.845 to −0.059; p = 0.03) but not the CW (r = 0.333, 95% CI −0.240 to 0.734). Subgroup analysis showed this correlation was stronger if the SAI was over 30 than below (r = −0.953, 95% CI −0.997 to −0.448; p = 0.01 vr = −0.001, 95% CI −0.665 to 0.663; p = 0.99].
Conclusions: Increased baseline anxiety state is associated with a greater reduction of oesophageal PT after acid infusion. There may be a role for anxiety in modulating the sensory responses to injurious stimuli in the gut. Future studies with larger numbers and more objective physiological measures of stress and anxiety may more help to understand the mechanism by which anxiety influences post injury gut sensitisation.
1
2
433 EFECTS OF REPEATED EXPERIMENTAL OESOPHAGEAL ACIDIFICATION ON PAIN THRESHOLD REPRODUCIBILITY IN HEALTHY SUBJECTS
R. P. Willert, C. Delaney, A. R. Hobson, Q. Aziz.GI Sciences Department, Hope Hospital, University of Manchester, UK
Introduction: Distal oesophageal acid has been shown to sensitise oesophageal mucosa both at the site of acid infusion (peripheral sensitisation) and also proximally away from the site of acid exposure (central sensitisation). Decreasing the interval between infusions potentiates this response but the long term effects of distal oesophageal acid infusions on oesophageal mucosal sensitivity to acid is unknown.
Aims: To determine the duration and magnitude of response of oesophageal sensitisation to both a single and repeated acid infusions in healthy volunteers.
Methods: (1) Duration: In eight subjects oesophageal pain thresholds (PT) to electrical stimulation were recorded at baseline and hourly following a 30 minute distal oesophageal acid infusion. If by the end of the study day the PT had not returned to baseline the subject returned the next day for further PT measurements. (2) Magnitude: 10 subjects underwent a repeat acid infusion two weeks after the first infusion and baseline and post acid oesophageal PT were compared between visits. Data from 36 subjects who have previously undertaken >1 acid infusion were also analysed to investigate whether the number of acid infusions accounts for an individual’s magnitude of sensitisation.
Results: (1) In six subjects the oesophageal PT had returned to baseline within nine hours of the acid infusion. In two subjects their PT remained reduced at the end of the experimental day, but had reverted to baseline when reassessed the next morning. (2) No difference in magnitude of effect on PT was seen with the first acid infusion compared with the second (p = 0.61 ANOVA) in all 10 subjects. Of the 36 subjects’ data, 31 sensitised to acid on their latest visit while five subjects did not. Logistic regression analysis showed as the number of acid infusions increased by 1 then the probability of sensitising to a subsequent acid infusion reduced by 4%, accounting for the magnitude of sensitisation. However, this result is not significant (odds ratio 0.96, 95% CI 0.68 to 1.37).
Conclusions: Acid induced oesophageal sensitisation is temporary and normalises within 24 hours in healthy subjects. Repeated distal oesophageal acid infusions do not alter the magnitude of sensitisation provided a two week period occurs between visits. Further studies with more frequently repeated acid infusions are warranted to assess changes in the magnitude and duration of oesophageal sensitisation, which reflects the role of frequent acid reflux that occurs in patients with GORD.
434 INVESTIGATING THE FUNCTIONAL PROPERTIES OF THE SOMATOSENSORY CORTEX DURING EXPERIMENTAL VISCERAL PAIN USING MAGNETOENCEPHALOGRAPHY
S. F. Worthen, P. L. Furlong1, Q. Aziz, A. R. Hobson.Section of GI Sciences, University of Manchester, Hope Hospital, UK; 1Wellcome Trust Laboratory for MEG Studies, Aston University, Birmingham, UK
Background: The somatosensory cortex has been inconsistently activated in pain studies and the functional properties of subregions within this cortical area are poorly understood. To address this we used magnetoencephalography (MEG), a brain imaging technique capable of recording changes in cortical neural activity in real-time, to investigate the functional properties of the somatosensory cortex during different phases of the visceral pain experience.
Methods: In eight participants (4 male), 151-channel whole cortex MEG was used to detect cortical neural activity during 25 trials lasting 20 seconds each. Each trial comprised four separate periods of 5 seconds in duration. During each of the periods, different visual cues were presented, indicating that period 1 = rest, period 2 = anticipation, period 3 = pain and period 4 = post pain. During period 3, participants received painful oesophageal balloon distensions (four at 1 Hz). Regions of cortical activity were identified using Synthetic Aperture Magnetometry (SAM) and by the placement of virtual electrodes in regions of interest within the somatosensory cortex, time-frequency wavelet plots were generated.
Results: SAM analysis revealed significant activation with the primary (S1) and secondary (S2) somatosensory cortices. The time-frequency wavelet spectrograms showed that activation in S1 increased during the anticipation phase and continued during the presentation of the stimulus. In S2, activation was tightly time and phase-locked to the stimulus within the pain period. Activations in both regions predominantly occurred within the 10–15 Hz and 20–30 Hz frequency bandwidths.
Discussion: These data are consistent with the role of S1 and S2 in the sensory discriminatory aspects of pain processing. Activation of S1 during anticipation and then pain may be linked to its proposed role in attentional as well as sensory processing. The stimulus-related phasic activity seen in S2 demonstrates that this region predominantly encodes information pertaining to the nature and intensity of the stimulus.
435 POSTPRANDIAL GALLBLADDER EMPTYING AND SMALL INTESTINAL TRANSIT IN COELIAC PATIENTS: A DISTINCT EFFECT OF GLUTEN FREE DIET?
A. Lanzini, F. Benini, A. Mora, R. Morandini, S. Bertolazzi, F. Lanzarotto, C. Ricci.Gastroenterology Unit: University and Spedali Civili, Brescia, Italy
Background: Gallbladder (GB) motility and small intestinal transit time (SITT) have been reported to be altered in coeliac disease (CD) and to normalise during gluten free diet (GFD), but these parameters have always been studied separately and in response to “artificial” liquid meals. Our aim was to assess GB motility and SITT simultaneously and in response to a physiologic solid meal in CD patients studied before and during GFD.
Methods: We measured GB motility using ultrasonography and SITT using a validated H2 breath test in 17 CD patients studied twice, before (n = 17) and during (n = 10) GFD, and in 24 healthy volunteers. Patients and controls were studied after following ingestion of a physiologic solid meal (kcal 539; 1 fried egg, butter, tea, sugar, bread, and baked beans).
Results: GB fasting volume and postprandial residual volume were significantly higher in CD than in controls (mean (SEM): 32 (4) ml v 14 (1) ml, p = 0.0002 and 9 (2) ml v 2 (0.3) ml, p = 0.001, respectively). T ½ GB emptying and emptying rate were similar in CD and controls. SITT was longer in untreated CD (238 (21) min) than in controls (169 (16) min, p = 0.015). After 12 months GFD, GB fasting volume was unchanged (22 (3) ml during v 27 (5) ml before GFD) and GB residual volume was significantly smaller during (3±1 ml) than before GFD (16 (5) ml, p = 0.047). T ½ GB emptying was reduced (8 (0.5) min v 31 (6) min, p = 0.004) and GB emptying rate was increased during GFD by comparison with before diet (−0.08 (0.01) ml/min v −0.02 (0.003) ml/min, p = 0.0034, respectively). SITT remained unchanged during (232±20 min) and before GFD (228 (22) min). Endomysial-ab were negative and duodenal histopathology improved in CD during GFD, but Marsh II lesion persisted in all.
Conclusion: Postprandial GB emptying and SITT measured under physiologcal conditions in response to a solid meal are altered in CD patients. GB emptying, but not SITT, revert to normal during GFD, an effect mirroring incomplete histopathologic recovery.
GI physiology posters
436 ENDOSCOPIC PLACEMENT UNDER SEDATION DOES NOT AFFECT PH MONITORING BY THE BRAVO SYSTEM
A. Thakur, M. Fox, T. Wong, R. Anggiansah, A. Anggiansah.Department of Gastroenterology & Oesophageal Laboratory, St Thomas’ Hospital, London, UK
Introduction and Aims: The Bravo system is designed to provide catheter-free, intraoesophageal pH measurements over 48 hours. Early observations suggested that oesophageal acid exposure is less during the first than the second 24 hour period.1, 2 This study examined whether endoscopic placement under sedation had effects on pH measurement directly or indirectly through a reduction of activity or oral intake.
Methods: Fifty six consecutive patients (median age 48 (35–61) years) referred for pH monitoring were studied. The Bravo capsule was placed using a standard gastroscope under moderate sedation (midazolam 3–5 mg, fentanyl 0–50 μg) on an afternoon list and measurements began one hour after the procedure. “Refluxogenic” test meals (1000 kcal) were provided to 12/56 patients throughout the study. Acid exposures during the 3, 6, and 24 hours after endoscopy on the first day were compared to the same time periods on the second test day.
Results: Complete 48 hour pH data were available for 47 (85%) patients (incomplete recording/patient error (n = 8), early detachment (n = 1)). Pathological acid exposure (>4.2%/24 hour) was recorded on at least one day in 34/47 (74%) patients. Acid exposure was similar after endoscopic placement on day 1 than the same period on day 2 (at 3 hours 8.7 (SD 1.4)% v 7.3 (1.6)%, p = 0.28, at 6 hours 8.8% (1.8)% v 8.0% (1.5)%, p = 0.71). Moreover pH measurement during the first 3 hours after endoscopy was not significantly different to that during any other time period (p = 0.58 by ANOVA). Acid exposure was also comparable in the postprandial periods (11.5 (1.6)% v 11.2 (1.5)%) and during the first and second nights/supine periods (7.5 (1.4)% v 6.9 (1.5)%). The results were the same in the subset of patients that received set meals. Provision of set meals had no significant effects on pH measurements.
Conclusions: Endoscopic placement of the Bravo capsule under moderate sedation had no impact on pH recordings. Providing patients with set meals did not alter the reproducibility of pH measurements. The interpretation of pH recordings obtained by the Bravo system need not take the effects of endoscopy on acid reflux into account.
1
2
437 DEFINING THE THRESHOLD FOR HEXOSE INDUCED GASTRIC EMPTYING DELAY BY NON-INVASIVE BREATH TESTS
A. Gopinath1, D. Lassman, D. G. Thompson.GI Sciences, Hope Hospital, Stott Lane, Salford, Manchester M14 8HD; 1Undergraduate medical student, University of Manchester, UK
Background: Ingested nutrients including hexoses are known to delay gastric emptying (GE) and induce satiety. It is unknown however, what the threshold for this effect is or whether this effect is dose related, or whether it is specific for a particular hexose.
Aims: To define the threshold response and specificity of oral hexose on GE. To determine the relationship between GE and satiety effects.
Methods: Experiment 1: Six healthy subjects were studied on different occasions after an overnight fast. On each visit subjects drank a 500 ml glucose solution of varying concentrations (0.125M–2.0M.) and a water control, labelled with 13C acetate (total number of studies >30).GE was expressed as a cumulative ratio of exhaled breath 13CO2 to 12CO2 over 45 minutes. Experiment 2: Two subjects repeated the study with galactose solutions of identical concentrations. Experiment 3: In order to assess hexose effects on satiety a meal tolerance test was performed. This involved serial consumption of 200 ml of water at 1 minute intervals until maximum fullness was achieved after ingestion of multiple glucose meals ranging from 0.125M to 2M.
Results: The threshold at which glucose significantly delayed GE was found to be 0.5M (SD 17.82, p value = 0.0129). At this concentration the GE was delayed by 27.53% compared to water. Increasing glucose concentration above this threshold further delayed GE in a dose dependant manner to a maximum of 2M. At the same molar concentrations galactose was found to slow GE to the same extent as glucose. The meal tolerance test showed prior ingestion of glucose solution of 0.25M or above reduced the amount of water to that could be subsequently drunk. Close correlation existed between water tolerated and gastric emptying (r = 0.7, p<0.05).
Conclusions: These data show that the delay in GE caused by hexose sugars require a threshold of 0.5M, following which a dose dependant effect in GE is found. The meal tolerance test supports the concept that glucose regulates satiety primarily by delaying gastric emptying.
438 IDENTIFYING PHENOTYPIC VARIATIONS IN CCK INDUCED GASTRIC EMPTYING DELAY IN MAN
D. J. Lassman1, M. Potluri1, M. D’Amato2, G. J. Dockray3, D. G. Thompson1.1Gastrointestinal Sciences, Hope Hospital, Salford, UK; 2Rotta Laboratories, Monza, Italy; 3Department of Physiology, University of Liverpool, UK
Background: Ingested nutrients release cholecystokinin (CCK) which acts via CCK1 receptors on the vagus nerve to delay gastric emptying and limit meal intake. However, the invasive methods required to measure gastric emptying in previous studies have hitherto prevented their use in population studies.
Aims: To develop a non-invasive technique in order to define the range of responsiveness of gastric emptying delay to a CCK releasing meal in healthy adults and to determine the effect of CCK1 receptor antagonism on the responsiveness to the meal.
Methods: Thirty three healthy volunteers consumed multiple test meals comprising either, 500 ml water alone, half strength or full strength CCK releasing meal, labelled with 13C acetic acid. Gastric emptying was expressed as the cumulative ratio of exhaled 13CO2 to 12CO2 over 45 minutes. The effects of the CCK1 receptor antagonist, dexloxiglumide were also studied.
Results: Compared to water, half strength and full strength meal delayed gastric emptying by 26% (3.5) and 50% (2.8), respectively (mean % decrease in gastric emptying (SEM), p<0.005). Within the study group there was up to 95% difference in CCK responsiveness between individuals. Dexloxiglumide inhibited the effect of the CCK releasing meal by 50%.
Conclusion: A wide range of interindividual responsiveness in CCK induced gastric emptying delay exists in the presence of good intrasubject repeatability. Since gastric emptying delay is a major determinant of meal volume ingested, individuals who are less sensitive to CCK releasing meals are likely to be able to tolerate greater meal volumes. This is therefore a likely factor in calorie consumption and a risk factor in obesity development.
439 MRI STUDIES OF BLOOD FLOW THROUGH THE SUPERIOR MESENTERIC ARTERY
R. Gillott, A. D. Jeays1, P. V. Lawford1, S. Jacob2, K. D. Bardhan, D. R. Hose1, P. A. Spencer.District General Hospital, Rotherham; 1Medical Physics, University of Sheffield; 2Biomedical Sciences, University of Sheffield, UK
Introduction and Aims: Chronic ischaemia of the small intestine is uncommon. It is hypothesised that this may be related to the nature of flow in the superior mesenteric artery (SMA) and the dynamic response to calorific load. To investigate this, SMA blood flow was studied during fasting and following ingestion of a controlled calorific load.
Method: Flow in the SMA was assessed in 18 healthy volunteers (11 male, 7 female, average age 36) by 1.5 Tesla magnetic resonance (MR) imaging. ECG gated, flow sensitive (phase contrast), sequences were acquired with high temporal resolution (21 frames per heartbeat) over the cardiac cycle. Images were obtained after overnight fasting and 30 minutes after ingestion of a 600 kcal Scandishake milkshake. A period of 30 minutes post-prandial was chosen as it coincides with peak flow (as determined from previous Doppler flow studies1). Velocity fields in the SMA were monitored throughout the cardiac cycle and mean flow calculated throughout diastole.
Results: At 30 minutes post-prandial, mean diastolic flow was 3.7 times that of the fasted value (n = 18, SD 2.2, range 0.8–9.8). During systole, flow disturbances, indicative of high velocity flows, were seen in 15 subjects post-prandially. This phenomenon was also seen in two of these 15 subjects after fasting.
Discussion and Conclusions: (1) Diastolic flow in the SMA increases markedly in response to calorific load. (2) The velocity of blood in the SMA during systole is sufficient to cause instabilities in the flow: the resulting loss of MR signal prevents the quantitative interpretation of velocity data at these high flows. (3) For most subjects, flow during systole is undisturbed following fasting. (4) The change in flow regime over these timescales may have important effects on wall shear stress, endothelial cell morphology, and risk of atherosclerosis.
1
Pathology posters
440 BAX PROTEIN EXPRESSION IN GASTRIC CANCER: CLINICOPATHOLOGICAL AND IMMUNOHISTOCHEMICAL STUDY
G. K. Anagnostopoulos1, D. Stefanou2, E. Arkoumani2, L. Chalkley1, A. Shonde1, E. Tsianos2, N. J. Agnantis2.1Wolfson Digestive Diseases Centre, University Hospital, Nottingham, UK; 2University of Ioannina, Medical School, Ioannina, Greece
Background: Reduced pre-apoptotic Bax protein expression has been identified in various human malignant tissues but little is known about its expression and its relationship with the biological behavior of human gastric cancer. The aim of our study was to examine the expression of bax protein in gastric cancer and precancerous lesions and correlate it with clinicopathological features and prognosis.
Methods: The expression of bax protein was studied by immunohistochemistry, using monoclonal antibodies, in a total of 48 paraffin embedded blocks of patients (30 males, mean age 67 years) who underwent gastrectomy due to gastric cancer. Bax expression patterns was graded as follows: negative; very weak, less than 5% of cells stained; weak, 5–20% of cells stained; moderate, 20–50% of cells stained; intense, >50% of cells stained. The results were correlated with survival and clinicopathological data.
Results: Nineteen (39%) cases were positive for Bax protein staining which was mainly located in the cytoplasm of tumor cells. In 11/19 cases the staining was very weak. The rate of Bax protein expression was not correlated with age, sex, tumour size, or depth of invasion. A negative immunostaining reaction was significantly correlated with lymph node metastasis (p <0.05), intestinal type of gastric cancer (p<0.05), and with poorly differentiated neoplasms (p<0.05). In adjacent precancerous lesions, Bax was expressed in 81% of specimens with atrophic gastritis, 54% of specimens with intestinal metaplasia and 33% of dysplastic cases (p<0.001 compared with atrophy). Mean follow up of patients was 54 months. Median survival was 31 months in cases with positive bax expression and 22 months in patients with low bax protein expression. Negative expression of bax was associated with decreased survival.
Conclusion: Negative Bax protein expression in gastric cancer correlates with aggressive tumour characteristics. Positive bax protein expression is associated with favourable prognosis.
441 THE ROLE OF MATRIX METALLOPROTEASE-7 IN REDEFINING THE GASTRIC MICRO-ENVIRONMENT IN RESPONSE TO GASTRIN AND H pylori
A. Varro, D. M. Pritchard1, C. McCaig, C. Duval, F. Campbell1, S. Ahmed1, K. Bodger1, D. D. Kerrigan1.Physiological Laboratory, School of Biomedical Sciences; and 1Division of Gastroenterology, School of Clinical Sciences, University of Liverpool, Liverpool, UK
Background: Epithelial organisation depends on interactions between epithelial and subepithelial cells including myofibroblasts. Control of these interactions is likely to be important in responses to injury, infection, inflammation, and the progression to cancer. In the gastric epithelium, MMP-7 is increased in infection with Helicobacter pylori; there is also stromal cell expansion. Similar changes occur in patients with high plasma gastrin concentrations due to either pernicious anaemia (PA) or multiple endocrine neoplasia (MEN)-1 syndrome.
Methods: We investigated the role of MMP-7 as a signalling molecule between epithelial cells and a key stromal cell type, the myofibroblast. Media from primary human cultured gastric epithelial cells either infected with H pylori or treated with gastrin released active MMP-7.
Results: In media from primary human gastric myofibroblasts, 2-dimensional gel electrophoresis and mass spectrometry identified insulin-like growth factor binding protein (IGFBP)-5 as an abundant substrate of MMP-7. Western blots confirmed cleavage of IGFBP-5 and release of IGF-II in the media of MMP-7 treated myofibroblasts. Knockdown of IGF-1R by siRNA, and treatment with an IGF-1R tyrosine kinase inhibitor (AG1024) abolished myofibroblast responses to MMP-7. Interestingly, IGF-II but not MMP-7 stimulated proliferation of gastric epithelial cells and media from MMP-7 treated myofibroblasts stimulated epithelial cell proliferation that was reduced by neutralising IGF-II antibody.
Conclusion: MMP-7 acts as an epithelial derived signal to increase the bioavailability of IGF-II released from myofibroblasts. Since IGF-II can act on both stromal and epithelial cells the findings suggest that increased MMP-7 expression contributes to redefining the niche occupied by dividing cells and leading to hyperproliferation in both hypergastrineamia and H pylori infection.
442 IS BILE CYTOLOGY HELPFUL IN THE DIAGNOSTIC WORK UP OF PATIENTS WITH BILIARY STRICTURES? A DISTRICT GENERAL PERSPECTIVE
J. S. Leeds, G. Hill, G. Kurien, A. Verghese, J. M. Sayer, G. James, R. P. Bolton.Doncaster Royal Infirmary, Doncaster, UK
Introduction: Identifying pancreaticobiliary malignancy in patients who present with a biliary stricture can be difficult. In the absence of EUS reliance upon imaging modalities and pathological specimens is required. Biliary cytology and/or brushings at ERCP have a low sensitivity but a high specificity. Some studies suggest that utility is higher in cholangiocarcinoma than pancreatic cancer. Identifying malignant cells at cytology reduces the need to perform more invasive tissue sampling techniques before commencing of oncological therapy.
Aims: To determine the usefulness of biliary cytology and/or brushings in patients with biliary strictures in a district general setting.
Patients and Methods: Over the period January 2002 to December 2003 there were 119 patients diagnosed with pancreaticobiliary tumours (73 pancreatic) and discussed at the upper GI multidisciplinary team meeting. Retrospective notes audit identified patients in whom biliary cytology and/or brushings were taken and this was correlated with findings from surgical resection or biopsy. Bile cytology samples were examined by two dedicated pathologists.
Results: Twenty three of these patients had 27 pathological samples taken; 19 at ERCP and eight via PTC. 13 patients had both brushings and bile aspiration samples, seven had brushings only, and seven had aspiration samples only.
Sensitivity for a malignant report was 17.4% increasing to 43.5% if malignant/suspicious reports and specificity was 100%. Negative predictive value was 23.5%. Brushings and aspiration was superior to either alone and aspiration alone was superior to brushings alone (sensitivity 60%, 42%, and 16% respectively).
Conclusion: Positive cytology clearly aids management of these patients whereas a negative sample adds little reassurance. Combining aspiration with brushings gives the highest sensitivity and specificity.
Abstract 442
443 DETECTION OF GASTROINTESTINAL MALIGNANCY BY FLUORESCENCE LIFETIME IMAGING OF UV LASER INDUCED TISSUE AUTOFLUORESCENCE
N. P. Galletly1,2, J. M. McGinty4, P. Cohen3, I. Munro4, D. S. Elson4, J. Requejo-Isidro4, C. Dunsby4, M. A. A. Neil4, A. V. Thillainayagam1, P. M. W. French4, G. W. Stamp2.1Gastroenterology Section, Faculty of Medicine, Hammersmith Campus; 2Department of Histopathology, Hammersmith Campus; 3Department of Histopathology, Charing Cross Campus; and 4Photonics Group, Department of Physics, Imperial College London, UK
Background: There is increasing interest in fluorescence imaging to help the early detection of malignancy in the GI tract. Fluorescence lifetime imaging (FLIM) is a novel wide-field imaging technique based on the decay kinetics of fluorescence at each point in the image field. Imaging fluorescence lifetimes can potentially improve the specificity of fluorescence based widefield imaging techniques and enhance their ability of to discriminate between malignant and normal tissue. We present unique preliminary data from ex vivo imaging of GI malignancies obtained using a prototype FLIM system.
Methods: Unfixed macroscopic tissue samples were obtained from surgical specimens from oesophagus, stomach and colon immediately following resection for malignancy. Tissue autofluorescence was induced by exciting the samples en face with a pulsed UV (355 nm) Nd:YVO4 laser and a set of wide-field fluorescence lifetime images recorded for areas macroscopically diagnosed as containing normal and cancerous mucosa. Tissue samples were subsequently fixed in formalin and the FLIM images compared with the histopathology findings.
Results: There was a marked change in the lifetime characteristics of malignant oesophageal, gastric, and colonic tissue compared to normal epithelium. For the majority of malignant lesions, the lifetime of the autofluorescence was shorter than that of the contiguous corresponding normal mucosa.
Discussion: FLIM generates inherent contrast between malignant and non-malignant GI tract tissue. Wide-field images can be updated at near video rate. These promising early data suggest FLIM has the potential to become an endoscopically deployable tool in vivo to help identify areas of early cancer.
444 PREVALENCE OF HELICOBACTER PYLORI IN COLORECTAL NEOPLASMS
M. L. Jones, P. Heliwell, C. Pritchard, J. Tharakan, J. Mathew.Departments of Histopathology and Research and Development,Royal Cornwall Hospital,Truro TR1 3LJ and Department of Medicine, Princess Alexandra Hospital, Harlow, Essex, UK
Background:Helicobacter pylori (HP) has been implicated in the development of gastric inflammation, peptic ulcers, MALT lymphomas, and adenocarcinomas. Similar aetiological associations with colorectal lesions have not been substantiated. This study evaluated the presence of HP within normal colonic mucosa and different forms of colorectal neoplasia.
Methods: Paraffin processed colonoc tissue blocks of normal colonic mucosa (n = 60) and adenocarcinoma (n = 60) diagnoses were removed from archival histological samples. These were stained by immunohistochemical methods using anti-HP antibodies and were examined by light microscopy to identify HP.
Results: Significant numbers of HP were identified in tubular adenomas (OR 11.13; 95% CI 1.62 to 76.70), tubulovillous adenomas (OR 10.45; 95% CI 1.52 to 71.52) and adenocarcinomas (OR 8.13; 95% CI 1.40 to 46.99) compared to control tissue but not within villous adenomas (OR 2.95; 95% CI 0.29 to 9.96).
Conclusion: We conclude that there is an association in the incidence of HP with some, but not all colorectal neoplasms. We cannot however infer a causal association between the bacteria and the neoplasms. We cannot exclude their presence as a consequence of the environment created by the neoplasms. Further molecular studies would need to be carried out to determine whether there is a causal relationship between HP and the development of colorectal neoplasms.
445 ASSESSING INTEROBSERVER AGREEMENT IN THE REPORTING OF EXTRAMURAL VASCULAR INVASION IN COLON CARCINOMA
S. Littleford1, N. Scott1, A. Baird2, C. Verbeke1, O. Rotimi2.1St James’s University Hospital; and 2Leeds General Infirmary, Leeds, UK
Introduction: Extramural vascular invasion (EMVI) is a prognostic indicator of metastasis and survival in colon carcinoma, independent of Dukes’s stage and the degree of tumour differentiation. However, the reporting of EMVI has a variable prevalence of 10–90%. This has been attributed in part to variations in the use of an elastin stain to demarcate extramural blood vessels. This study aimed to determine for the first time the degree of interobserver agreement in the reporting of EMVI in colon carcinoma without the use of an elastic stain.
Methods: Twenty cases of pT3 and pT4 Dukes’s B colon cancers were identified from a pathology database and 49 H&E slides representing extramural tumour invasion were selected. Slides were anonymised and distributed to four specialist gastrointestinal pathologists who independently assessed the presence or absence of EMVI. Kappa values were performed to assess the degree of interobserver agreement.
Results: Kappa values ranged from 0.23 (poor agreement) to 0.45 (moderate agreement).
Conclusions: The reporting of EMVI in Dukes’s B colon carcinomas on H&E stained slides has only poormoderate agreement when assessed by specialist gastrointestinal pathologists. The introduction of standardised histological criteria or the use of an elastin stain in the diagnosis of EMVI may assist in improving interobserver agreement, and thus more accurate assessment of individual patient prognosis in colon carcinoma.
Neoplasia posters
446 THE POTENTIAL OF SIX DIETARY PHYTOCHEMICALS TO MODULATE NF-κB ACTIVITY IN OESOPHAGEAL CANCER CELLS IN VITRO
A. Alhamdani, J. Cronin, G. Jenkins, S. Doak, P. Griffiths, J. Parry, J. N. Baxter.Clinical School, University of Wales Swansea, Singleton Park, Swansea SA2 8PP, UK
Background: A wide range of evidence in the literature showed sequential increased activity of the anti-apoptotic transcription factor NF-κB during progression to oesophageal adenocarcinoma and enhanced expression of its target genes (IL-8 and IκB). Since bile acids had been implicated in the development of this cancer, previous work from our lab revealed that a specific bile acid (deoxycholic acid) could induce activation of NF-κB and augment the expression of its driven transcription targets particularly IL-8 and IκB.
Methods: A growing body of studies elucidated the effect of numerous phytochemicals in chemoprevention process in cancer. Hence, the objective in this study was to assess the effect of six dietary ingredients on the bile induced NF-κB activity in oesophageal cancer OE33. IL-8 and IκB mRNA expression were particularly utilised as surrogate of induction of NF-κB activity, since the link between them has been previously demonstrated.
Results: Of the six agents validated, curcumin (from turmeric), vitamin C, resveratrol (from red wine), and EGCG (green tea extract) seemed to be effective at blocking NF-κB activity, as determined by the specific expression of IL-8 and IκB utilising Real-time PCR. In some cases, this completely abrogated bile induced NF-κB activity. Furthermore, and to investigate these phytochemicals mode of action in oesophageal cancel cells, their impact on the level of reactive oxygen species as inducers of NF-κB plus the exerted effect on GFP tagged p65 construct in conjunction with a confocal microscope to monitor cellular localisation are curried out at present.
Conclusion: As NF-κB activity appears to be linked to neoplastic progression in Barrett’s patients, some of the dietary phytochemicals may have a role in oesophageal cancer chemoprevention.
447 DURING ACID REFLUX, LUMINALLY GENERATED NITRIC OXIDE FROM DIETARY NITRATE LEADS TO N-NITROSATIVE STRESS WHICH IS MAXIMAL IN THE OESOPHAGUS
J. Winter, S. Paterson, G. Scobie, A. Wirz, T. Preston1, K. E. L. McColl.University Department of Medicine and Therapeutics, Western Infirmary, Glasgow; and 1Scottish Universities Environmental Research Centre, East Kilbride, UK
Background: The mutagen responsible for the rising incidence of adenocarcinoma of the gastric cardia and distal oesophagus is unknown. In healthy volunteers, we have previously demonstrated that high concentrations of nitric oxide are generated from dietary nitrate, leading to in situ formation of N-nitroso compounds. In these subjects without reflux, this luminal nitrosative chemistry is maximal in the proximal region of the stomach.
Aim: To examine the influence of gastro-oesophageal reflux on the anatomical location of this in situ nitrosative stress.
Methods: Seventeen H pylori negative patients with Barrett’s oesophagus were studied. A segmented silastic tube containing the secondary amine morpholine was attached to a 4 channel pH catheter and passed naso or orogastrically. The tube wall has the same physical properties as the epithelial lipid membrane. Subjects then drank 2 μmol of 15N enriched potassium nitrate. On one visit they were studied in the absence of acid reflux, and on the other reflux was stimulated posturally and pharmacologically. The tube was removed after 2.5 hours and each segment analysed for markers of nitrosative stress.
Results: In the absence of acid reflux, nitrite and N-nitrosomorpholine were detected in the gastric sections, with concentrations maximal proximally. During reflux, 80% of nitrosative stress occurred in the oesophageal sections. A linear relationship existed between the duration of acid reflux and the proportion of stress occurring in the oesophagus (p<0.001). The N-nitrosomorpholine measured was enriched with 15N, indicating it was derived from the administered nitrate via nitric oxide production.
Conclusion: Acid reflux results in proximal migration of the area of nitrosative stress induced by dietary nitrate via nitric oxide production. The presence of nitrosative stress in a region already damaged by inflammation and metaplasia may contribute towards carcinogenesis at this site.
448 LONG TERM SURVIVAL OF OESOPHAGEAL AND GASTRIC CANCER PATIENTS TREATED SURGICALLY AT A DISTRICT GENERAL HOSPITAL
C. Lock, B. Rous, L. Aldred, H. Al-Rufaie, R. J. Dickinson.Hinchingbrooke Hospital, Huntingdon PE29 6NT, UK
Background: Survival following gastric/oesophageal cancer surgery is poor. In recent years, advances have been made in surgical techniques and chemoradiotherapy, as well as changes in the coordination of cancer services with the aim to improving mortality.
Aim: To identify patients who have survived in excess of seven years following gastric/oesophageal cancer surgery and factors that may have contributed to prolonged survival.
Methods: The pathology database was analysed for patients who were treated for gastric/oesophageal cancers between 1992 and 1998, and were matched against hospital patient administration system for survival. The surgical pathology was reviewed and staged according to TNM classification.
Results: 129 patients who were diagnosed with gastric/oesophageal cancer were identified between 1992 and 1998. Of these nine had survived to the present day (7%). Only five of the surviving nine patients had diagnostic CT scans prior to surgery. Many of the patients had advanced stage disease, three had nodal metastases, and one had pathologically involved surgical resection margins.
Conclusion: Surprisingly, many of the survivors is this series had poorly differentiated tumours of advanced stage. Exceptional longevity following gastric/oesophageal cancer surgery is not limited to those with well differentiated early stage disease.
449 PHOTOSTENT 1: A PHASE II TRIAL OF PORFIMER SODIUM PHOTODYNAMIC THERAPY IN LOCALLY ADVANCED BILIARY TRACT CARCINOMA
S. P. Pereira1, G. Aithal2, J. Devlin3, H. M. Meadows4.1University College Hospital, London; 2Queen’s Medical Centre, Nottingham; 3King’s College Hospital, London; 4Cancer Research UK and UCL Cancer Trials Centre, London, UK
Background: Phase II/III data from Germany suggest that photodynamic therapy (PDT) with porfimer sodium is effective in maintaining biliary drainage and may improve the survival and quality of life of patients with irresectable cholangiocarcinoma. The aim of this study was to evaluate the safety and efficacy of PDT in patients with locally advanced (T3/T4) biliary tract carcinoma (BTC).
Methods: Eligible patients had irresectable, histologically confirmed disease, a Karnofsky performance status (KPS) of ⩾30% and life expectancy >12 weeks. Patients received 2 mg/kg iv of porfimer sodium (Photofrin), followed by endobiliary laser activation and stent replacement 48 hours later. Patients were assessed clinically and by CT/MRI before treatment and on day 28, and followed up thereafter at three-monthly intervals.
Results: Thirty six patients were entered over an 18 month period: 14M/22F, median age 65 (30–79) years, median KPS 80 (50–100). Five patients experienced grade 3 toxicity: three biliary sepsis (days 7–28), one photosensitivity (day 28), and one pain (day 7); there was no grade 4 toxicity. 29 patients had assessable radiological response at day 28: seven partial responses, 14 stable disease, and eight progressive disease. Among the 34 patients with complete follow up data, there were 24 deaths (one died within 28 days of receiving treatment) during a median follow up of 23.9 months. The median survival from the date of treatment was 14.9 months (95% CI 9.2 to 17.4 months).
Conclusions: Porfimer sodium PDT can be delivered safely to patients with BTC and is suitable for testing in phase III studies.
450 ALPHA FETOPROTEIN IS A MARKER OF AGGRESSIVE AND PROGRESSIVE NEUROENDOCRINE TUMOURS
M. Bhogal, T. Shah, T. Amin, P. Bhogal, N. Sivathasan, D. Hochhauser, C. Witney-Smith, M. E. Caplin.Neuroendocrine Tumour Unit, Royal Free Hospital, London, UK
Background: Alpha fetoprotein (AFP) is a well established marker for germ cell tumours and hepatocellular carcinoma (HCC). Neuroendocrine tumours (NET) are usually slow growing although a small proportion can run an aggressive course. NETs are, in part, characterised by an ability to secrete hormones and biogenic amines, some of which—for example, Chromogranin A—have been shown to correspond to disease state.
Aims: To evaluate the role of AFP as a potential tumour marker in NETs.
Methods: A retrospective analysis of AFP, histological grade and radiological progression was conducted in 419 NET patients. Raised AFP was defined as a level >50% above the upper limit of normal. Patients in which another recognised cause of raised AFP was identified were excluded. Radiological status was determined using the Response Evaluation Criteria In Solid Tumours (RECIST) and divided into regressive, stable and progressive disease. Tumour grade was based on standard histological classification and cell proliferation markers (Ki67/MIB-1), being divided into low, intermediate, and high grade. These variables were correlated temporally.
Results: AFP was raised in 23 of 419 (5.5%) patients. One patient with HCC was excluded. AFP was associated with tumour progression in 78% of patients as compared with 24% in the AFP negative population (p<0.0001). High grade tumours represented 87% of the raised AFP group v 31% in the normal AFP group (p<0.0001).
Conclusion: AFP is a marker of aggressive disease in a subset of NET patients. It is associated with both histologically aggressive and clinically progressive disease. These patients are three times more likely to show radiological tumour progression and high grade histology compared to those with normal AFP levels. A prospective analysis of AFP alongside changes in disease state will allow us to determine the role of AFP as a clinical parameter for monitoring tumour behaviour in NET patients.
451 BIOMARKERS OF THE IMMUNE RESPONSE IN PRIMARY COLORECTAL CANCER
E. Hamilton1,2, L. Machado2, G. Reynolds1, P. Taniere1, S. Lee1,2, N. Steven1,2, T. Ismail (introduced by R Cockel)1.1University Hospital Birmingham NHS Foundation Trust; and 2Institute for Cancer Studies, University of Birmingham, UK
Aim: The object of this project is to characterise lymphocytes in colorectal cancer (CRC), to identify subpopulations that reflect immune activation or suppression. Our aim is to validate the methods used so that they may be used in future early vaccine trials to assess the effect of such trials on the immune microenvironment of this disease.
Methods: We recruited 34 patients undergoing surgery for CRC. Lymphocytes were harvested from blood (PBL) and tumour (TIL). Flow cytometry and immunohistochemistry were used to detect subpopulations within TIL, by identifying 18 markers for T cell homing and two of immune suppression (CD25 and Foxp3). To assess function, cells were stimulated and the supernatant was tested in cytokine ELISA.
Results: Using flow cytometry, the average number of CD4+CD25+ TIL was 9.98% (range 2–31) compared to 5.6% (0–27.5) for PBL (p = 0.1972). Immunohistochemical staining for Foxp3 was positive in samples obtained from 14 patients. Expression of homing markers differed between PBL and TIL, with the proportion expressing CXCR6 higher (p<0.0001)). Using flow cytometry to calibrate TIL input numbers enabled more accurate measurement of functional status. TIL released both interferon-γ and IL-10, associated with positive and negative antitumour responses respectively, but at levels lower than PBL.
Conclusions: We have confirmed the presence of immunosuppressive cells in CRC, however, there is not an increase in expression when compared to PBL. The percentage expression of the chemokine receptor CXCR6 is higher in TIL when compared to PBL. Subpopulations within TIL expressing particular cell surface markers may contribute differently to the immune microenvironment, and work is currently on going to isolate these cells and determine their functional properties. The methods we have developed to assess the immune response at the tumour site can be used to analyse the effect of future vaccine trials.
452 CONFOCAL MICROSCOPY: A NOVEL METHOD TO ASSESS ABERRANT CRYPT FOCI IN APCMIN+/− AND APCMIN+/− (PPARα−/−) MICE
A. Shonde, K. Ragunath, G. Anagnostopoulos, D. R. Bell, A. J. Bennett, C. J. Hawkey.Wolfson Digestive Diseases Centre, University Hospital, Nottingham, UK
Background: Peroxisome proliferator-activated receptorα (PPARα) is expressed at low levels in colon tumours. APCmin+/− mice fed with methylclofenapate (a PPARα ligand) have 50% less tumour burden in the small intestine and colon than control.1 Recent studies showed that aberrant crypt foci (ACF) are the earliest morphological lesion detectable in colorectal epithelium that may lead to cancer. However the relationship between PPARα and ACF formation is not known. Dissection microscopy is the most common method used for quantifying ACF. However it is time consuming and requires a great deal of skill to obtain a good preparation.
Aims: (1) To assess whether confocal microscopy is a viable method for identifying ACF in scientific practice. (2) Examine the role of PPARα in colon carcinogenesis using APCmin+/− and APCmin+/−(PPARα−/−) mice.
Method: Once weaned APCmin+/− mice and APCmin+/−(PPARα−/−) mice were fed standard chow throughout the study. Mice were weighed weekly, until mice showed signs of anaemia or lost >20% of weight at which time they were sacrificed. ACF were assessed using Cell∼vizio Confocal Microscopy probe (Mauna Kea Technologies, Paris) made of 30 000 optical fibers following colonic staining with acryflavine.
Result: High definition images with 2.5 μm lateral resolution of normal crypts and ACF were clearly identified using confocal microscopy. APCmin+/−(PPARα−/−) mice have more ACF than APCmin+/−mice in the colon, but this failed to reach significance (n = 9). The mean number of ACF was 5.0/ 10 fields (CI 2.10−7.90) in APCmin+/−(PPARα−/−) mice and 2.75/ 10 fields (CI 1.22–4.27) in APCmin+/− mice.
Conclusions: Confocal microscopy using the Cell∼vizio probe is a simple and quick method of accessing ACF, with the potential of refining experiments so that mice can be studied serially. PPARα role in colon carcinogenesis may be to inhibit the formation of ACF rather than their progression. Greater understanding of PPARα dependant genes may enable the pathogenesis of colon cancer to be further understood.
1
453 IS THE FULL BLOOD COUNT RELEVANT IN THE DIAGNOSIS OF COLORECTAL CANCER?
S. Masson1, D. Chin2, M. A. Tabaqchali1, G. Waddup1, J. A. Barbour1, A. D. Dwarakanath1.1University Hospital of North Tees, Stockton on Tees TS19 8PE; and 2University of Sunderland, Sunderland SR2 7EE, UK
Introduction: The national cancer 31 and 62 day waiting time targets are driving the diagnosis of colorectal cancer by a straight to test policy. We have looked at the full blood count (FBC) of proven cancer cases to see whether it is relevant to referral and diagnosis.
Method: The FBC at diagnosis of proven colorectal cancer was correlated to the patient gender and site of tumour, retrospectively over 18 months.
Results: 143 patients were included with a mean age of 67 years (male) and 71 years (female). The tumours were located on the left side in 96, including 68 rectal or rectosigmoid, and on the right side in 47. Mean haemoglobin (Hb) was 12.7 g/dl in males (n = 85) (lab ref 13.0–18.0 g/dl) and 12.0 g/dl in females (n = 58) (lab ref 12.0–16.0 g/dl) and was below the lower limit of normal in 48% (male) and 50% (female). Mean Hb was 93.0% of normal for rectal cancers v 82.5% of normal for non-rectal cancers (p<0.001), and was below the lower limit of normal in 32.4% v 64.0% (rectal v non-rectal; p<0.001). Mean Hb was 79.6% of normal in right sided v 91.3% of normal in left sided cancers (p<0.01) and was below the lower limit of normal in 70.2% v 38.5% (right v left sided; p<0.001). In multiple regression analysis, after first adjusting for sex, the mean difference in Hb associated with non-rectal compared with rectal cancers was −1.6 g/dl (SEM 0.3 g/dl).
Conclusion: Non-rectal cancer patients, particularly those with right sided lesions, are significantly more likely to have a greater degree of anaemia at presentation. However, this observation must not determine the referral, investigation or management of patients suspected to have colorectal cancer. Irrespective of haemoglobin, such patients should be referred via the two week rule pathway.
454 COLON CANCER RATE IN PATIENTS WITH A WELL RECOGNISED CAUSE OF IRON DEFICIENCY ANAEMIA IN THE UPPER GI TRACT
N. Powell, A. McNair.Gastroenterology Department, Queen Elizabeth Hospital, Woolwich, London, UK
Background: Upper and lower GI-tract investigations are mandatory in most in patients with iron deficiency anaemia (IDA). BSG guidelines indicate that only the presence of coeliac disease or malignancy encountered at OGD precludes lower GI tract evaluation. This is based on inconsistent results from studies suggesting that colon cancer may be uncovered even in a cause for IDA is found at OGD. It could be argued that such cases merely reflect the background prevalence of colon cancer.
Methods: We conducted a retrospective analysis of 408 patients with IDA (defined by red cell indices and/or reduced serum ferritin concentrations). All patients had undergone OGD and were then divided into two groups. The first comprised 73 patients with an upper GI tract lesion that could feasibly account for IDA (gastric/duodenal ulceration, severe oesophagitis, severe haemorrhagic gastritis/duodenitis, and vascular lesions). The second comprised 335 patients whose upper GI tract was normal, or contained minor lesions, considered unlikely to cause IDA (mild gastritis, duodenitis or oesophagitis, Barrett’s epithelium, and hiatus hernia). In the two groups we defined the prevalence of colon cancer in subsequent lower GI tract evaluation. Colonoscopy or double contrast barium enema studies were completed in 278/408 (68.1%) patients.
Results: Colon adenocarcinoma was present in 31 patients. Cancer was located in the right hemi-colon in 80.6% of cases. In 49 patients with a well recognised cause of IDA in the upper GI tract who underwent lower GI tract evaluation, colon cancer was only present in one case (2%). This isolated case had a chronic gastric ulcer and a proximal transverse adenocarcinoma. Conversely, in patients with upper GI tract lesions sufficient to account for IDA, colon cancer was present in 30 cases (13.1%), (p<0.05). In summary the prevalence of colon cancer is very low in patients with an upper GI tract lesion sufficient to account for IDA.
455 DO 31/62 DAY CANCER TARGETS WORK FOR PATIENTS WITH LIVER METASTASES?
B. Flont, B. Burns, R. Kent, I. Minty, I. Chasi, S. Saksena.Department of Gastroenterology & Radiology. (Introduced by Macklon AFM) University Hospital of North Durham, UK
Introduction: NHS Cancer Plan (2000) requires trusts to achieve “62 days” (urgent GP referral to first treatment) and “31 days” (decision to treat to first treatment) targets and stipulates specialist teams of clinicians and cancer nurse specialists should care for all patients with cancer.1 Patients with liver metastases and unknown primary often fall outside specific cancer multidisciplinary team meetings (MDT) and are at greater risk of missing targets.2 This study was aimed to determine if patients with liver metastases met these targets.
Methods: Patients with diagnosis of “liver metastasis” on outpatient abdominal ultrasound in August 2004–August 2005 were identified and notes and computerised records were reviewed retrospectively.
Results: Thirty nine patients (17 males, median age 73 years, range 51–91 years) had liver metastases on ultrasound, five with alternative diagnosis on further imaging excluded haemangioma (3), multiple liver abscesses (1), and focal nodular hyperplasia (1). Primary cancer was known at diagnosis in six patients, was diagnosed within 31 days in nine patients, and beyond 31 days in 11. No further tests were done in six patients, no primary was diagnosed despite investigations in two. 25 patients received treatment including symptom control, one refused treatment, and no treatment was offered to eight. Other treatment included radiotherapy (2), curative chemotherapy (2), chemo ablation (1), palliative chemotherapy (6), palliative procedures (6). Only 19/ 34 (56%) patients met the 31 day target and 16/34 (47%) met the 62 day target. 64% patients were discussed in cancer MDT; 59% were seen by cancer nurse specialist.
Conclusions: Patients with liver metastases have complex pathways with worse clinical outcome. Approximately half the patients failed the 62 day and 31 day target; a third did not have access to MDT nor support of a cancer nurse specialist. This highlights the need for streamlining cancer pathways for patients with liver metastases so they may benefit from advances in cancer therapy.
1
2
Radiology posters
456 INTEGRATED FDG PET/CT IN THORACIC OESOPHAGEAL AND GASTRO-OESOPHAGEAL JUNCTION CARCINOMA: A PICTORIAL REVIEW
I. D. Lyburn1, R. J. Chambers1, K. Goodchild2, M. Harrison2, E. Townsend3, R. G. Berrisford4, W. L. Wong (introduced by T. Brooklyn)1.1Paul Strickland Scanner Centre, Mount Vernon Hospital, Middlesex; 2Marie Curie Research Wing, Mount Vernon Hospital, Middlesex; 3Department of Surgery, Harefield Hospital, Middlesex; 4Department of Surgery, Royal Devon & Exeter Hospital, Devon, UK
Thoracic oesophageal and gastro-oesophageal junction (GOJ) cancers, in common with many other malignant tumours, usually have a high rate of glucose metabolism which enables their detection with 18F-labelled fluoro-2-deoxy-D-glucose (FDG). Integrated positron emission tomography/computed tomography (PET/CT) combines functional imaging with accurate anatomical localisation and is emerging as a powerful technique for the assessment of patients with these cancers.
Endoscopy and biopsy of suspicious areas remains the cornerstone for establishing the diagnosis of oesophageal carcinoma. Small volume primary disease is not reliably detected on FDG PET particularly at the gastro-oesophageal junction where normal physiological uptake may occur. Integrated FDG PET/CT may have a role in the detection of severe dysplasia associated with Barrett’s oesophagus.
In staging disease, endoscopic ultrasound remains the method of choice for assessing the primary site and adjacent para-oesophageal nodes. Integrated FDG PET/CT provides, however, the most comprehensive non-invasive tool for detecting distant metastases and can lead to more appropriate selection of patients for surgical resection. In patients with advanced disease undergoing neo-adjuvant chemotherapy, integrated FDG PET/CT is potentially useful for monitoring treatment response.
Between March 2004 and September 2005 the authors have conducted 76 integrated FDG PET/CTs for staging these tumours and correlated findings with surgery and the clinical course. Drawing from this data, the exhibit will outline the contribution of integrated FDG PET/CT in the management of thoracic oesophageal and GOJ cancer with several illustrative cases.
457 3D VIRTUAL REALITY COLONOSCOPY AND TARGETED OPTICAL COLONOSCOPY: THE LIGHT AT THE END OF THE TUNNEL?
M. Bose, J. Bell, L. Jackson, P. Casey, J. Saunders, O. Epstein.Institute for Minimally Invasive Gastroenterology. Royal Free Hospital NHS Trust, Hampstead, London, UK
Introduction: V3D-colon (Viatronix) is a validated CT application which generates a primary 3D virtual reality image of the colon.
Aim: To compare findings on V3D (VRC) with gold standard optical colonoscopy (OC) in symptomatic patients.
Method: 100 patients attending GI outpatients requiring colonoscopy agreed to participate in a study comparing VRC with OC. Colon cleansing was undertaken using a standard preparation with dilute barium and gastrograffin added to the preparation protocol. Air contrast VRC was performed with 4 sensor CT scanner and processed using the V3D-colon software engine. Contrast tagged stool and fluid were removed electronically. The 3D VRC image was used as the primary diagnostic image with 2D colography available for problem solving. Polyps >5 mm in diameter were considered significant.
Results: Pancolonoscopy was completed in 99 VRC examinations and 92 OCs. VRC demonstrated >99% of the mucosal surface with colonoscopists reporting a mean estimate of 88% surface visualisation. Both techniques revealed two rectal and one hepatic flexure cancer. Eleven polyps >5 mm were discovered in nine patients. One of these polyps was found on OC in the single patient who failed VRC and a 15 mm polyp missed on OC was found after unblinding (sensitivity for both VRC and OC was 91.6%). Two of three cancers and all the benign polyps >5 mm were present in the left-sided colon and rectum. Diverticulosis was reported in 39 VRC and 30 OC examinations. Significant extracolonic findings were reported in 29 patients. One OC patient experienced bradycardia.
Conclusion: 3D VRC is a major development in minimally invasive colonic imaging with sensitivity comparable to OC. In symptomatic patients, a case can be made for VRC followed if neccessary by immediate targeted colonoscopy.
458 HIGH FREQUENCY MINI PROBE EUS IS A VALID PREDICTOR OF DISEASE ACTIVITY IN ULCERATIVE COLITIS ADOPTING MODIFIED TSUGA SCORES: FIRST VALIDATION DATA WITH RELAPSE PREDICTION
D. P. Hurlstone1, D. S. Sanders1, M. E. McAlindon1, A. J. Lobo1, M. Thomson1, S. Brown1, S. S. Cross2.1Gastroenterology, Royal Hallamshire Hospital, Sheffield; 2Academic department of Pathology, Royal Hallamshire Hospital, Sheffield, UK
Background: In ulcerative colitis (UC) colorectal wall parameters using 20 MHz EUS can be classified into four discrete subgroups (Ts 1-IVb). Our group have previously shown 20 MHz EUS to be a usefull adjunctive activity index parameter. In UC prognosis is dependent on the severity of mucosal inflammatory change where accurate assessment of disease activity is required to optimise medical therapy. Relapse prediction using conventional endoscopic, histopathological and clinical criteria has proven unreliable.
Aims: (1) To evaluate the validity of Ts. EUS criteria in UC as compared with standardised measures of clinical, endoscopic and histopathological severity. (2) To asses the relapse rates in patients fulfilling baseline Ts class III/IV criteria.
Methods: Segmental colorectal 20 MHz imaging using water +/− Tseng balloon acoustic coupling was performed in 200 patients. Endoluminal EUS criteria were then compared to the endoscopic Baron score, Seo activity score, and Matts histopathological grade. Baseline indices were then repeated at “acute” presentation; otherwise 6, 12, and 18 months post index assessement.
Results: Rectum: Κ coefficient between Tsuga criteria I/II and Matts grade 1/2 was 0.78 (95% CI 0.67 to 0.89), 0.57 (95% CI 0.46 to 0.68), and 0.48 (95% CI 0.34 to 0.62) for Tsuga class IIIa/b, IVa/b, and Matts grade 3a/b and 4 respectively. Colonic imaging showed a Kappa coefficient between Tsuga class I/II and Matts grade1/2 of 0.76 (95% CI: 0.72 to 0.8). Tsuga class IIIa-b/IVa-IVb as compared to Matts grade 3a–3b/4 yielded Kappa coefficients of 0.49 (95% CI 0.43 to 0.55) and 0.62 (95% CI 0.56 to 0.69) respectively. 82% of patients with Tsuga IVb (irrespective of SAI/Matts score) relapsed at 12/12 post index imaging.
Conclusions: High frequency ultrasound is a valid adjunctive “tool” for the transmural assessment of the colorectal wall in ulcerative colitis. This technique may aid in the initial diagnosis, and ongoing chronic management of disease.
459 THE RADIOLOGY OF ABDOMINAL TUBERCULOSIS
M. R. Brown1, D. Derry2, R. L. Jones1, M. R. Hetzel2, M. Callaway3.1Departments of Gastroenterology; 2Respiratory Medicine; and 3Radiology, Bristol Royal Infirmary, Bristol, UK
Abdominal TB can involve any part of the GI tract, including the peritoneum, hollow and solid organs and the lymphatics. Although the high level of pulmonary TB seen during the last two centuries has declined, the number of cases of abdominal TB in the UK has risen due to a number of factors. The major reasons are HIV infection, and the subsequent development of AIDS, and the emergence of multidrug resistant TB. In addition, an increase in the immigrant population, thought to have an 80-fold higher incidence of non-pulmonary TB compared to the indigenous population, has produced a renaissance in abdominal TB.
Major diagnostic hurdles include the non-specific nature of the presenting symptoms and the unwillingness of the clinician to make the diagnosis of abdominal TB. It remains a disease primarily of the young, with a peak incidence in the third and fourth decades of life. Patients can suffer pain, fever, weight loss, anorexia, jaundice, or a change in bowel habit, and often investigated for a possible malignancy. In the majority of cases, radiological investigations are vital in correctly diagnosing mycobacterial infection in the gastrointestinal tract.
We present four cases of abdominal TB in young Somalian males referred to the department of gastroenterology with abdominal pain and constitutional symptoms suspicious of intra-abdominal malignancy. The cases include the following diagnoses: abdominal tuberculous adenopathy, gastric outflow obstruction secondary to pyloric stenosis, Potts disease of the spine, and two cases of tuberculous involvement of the pancreas. Radiological images, including plain radiographs, ultrasonographic images, computed tomography, and magnetic resonance imaging are included to illustrate the role of radiological investigations in the diagnosis of abdominal tuberculosis.
Linked Articles
- Abstracts
- Colon cancer
- Colon cancer
- Alcoholic liver disease