Article Text

Statistics from Altmetric.com
Screening for colorectal polyps and neoplasms has been accepted and instituted in the United States. As most colorectal neoplasms arise from pre-existing polyps, detection and removal of precursor adenomas result in a decrease in the incidence of and mortality from colorectal cancer.1-9 Two American expert panels have recently reviewed the scientific basis of various colorectal screening tests and recommended their adoption.10 ,11 Furthermore, the United States Congress has recently approved national Medicare coverage for colorectal screening. A broad range of screening choices are available for patients and physicians to choose from. Depending upon the patient’s risk factors, screening choices include faecal occult blood testing, flexible sigmoidoscopy, barium enema, and colonoscopy. Unfortunately, none of the currently available colorectal screening tests is optimal in terms of examination performance, safety, or patient acceptance. Physicians and scientists interested in colorectal cancer screening continue to look for novel methods to detect adenomas and early cancers.
In 1994 using volumetric computed tomography (CT) data produced by a spiral CT scanner, CT colonography (CTC) was first introduced.12 The three dimensional images displayed in a cine loop (simulating the endoluminal views seen at colonoscopy) excited many investigators in the field of gastrointestinal imaging. Today, several academic centres in the United States are actively investigating this new technique. The purpose of this article is to review the current state of knowledge in this field, to compare CTC with other accepted colorectal screening tests, and to identify future areas of study and development.
CTC today
TECHNIQUE
Today CTC refers to an examination performed on a spiral CT scanner with acquisition of volumetric data of the entire colon. Combining these data with advanced imaging software, the colon is examined at an off-line workstation using the combination of two dimensional and three dimensional images (fig 1).

Colonoscopic, endoluminal three dimensional view, and two dimensional image of a 2.5 cm sessile polyp. (From: Hara AK, Johnson CD, Reed JE. Colorectal lesions: Evaluation with CT colography. RadioGraphics 1997;17:1157–67.)

Two dimensional and endoluminal three dimensional image of a lobulated 1.8 cm polyp. (From: Johnson CD, Hara AK, Reed JE. Computed tomographic colonography (virtual colonoscopy): a new method for detecting colorectal neoplasms. Endoscopy 1997;29:454–61.)

Colonoscopic and endoluminal three dimensional image of a 4 mm colonic polyp.


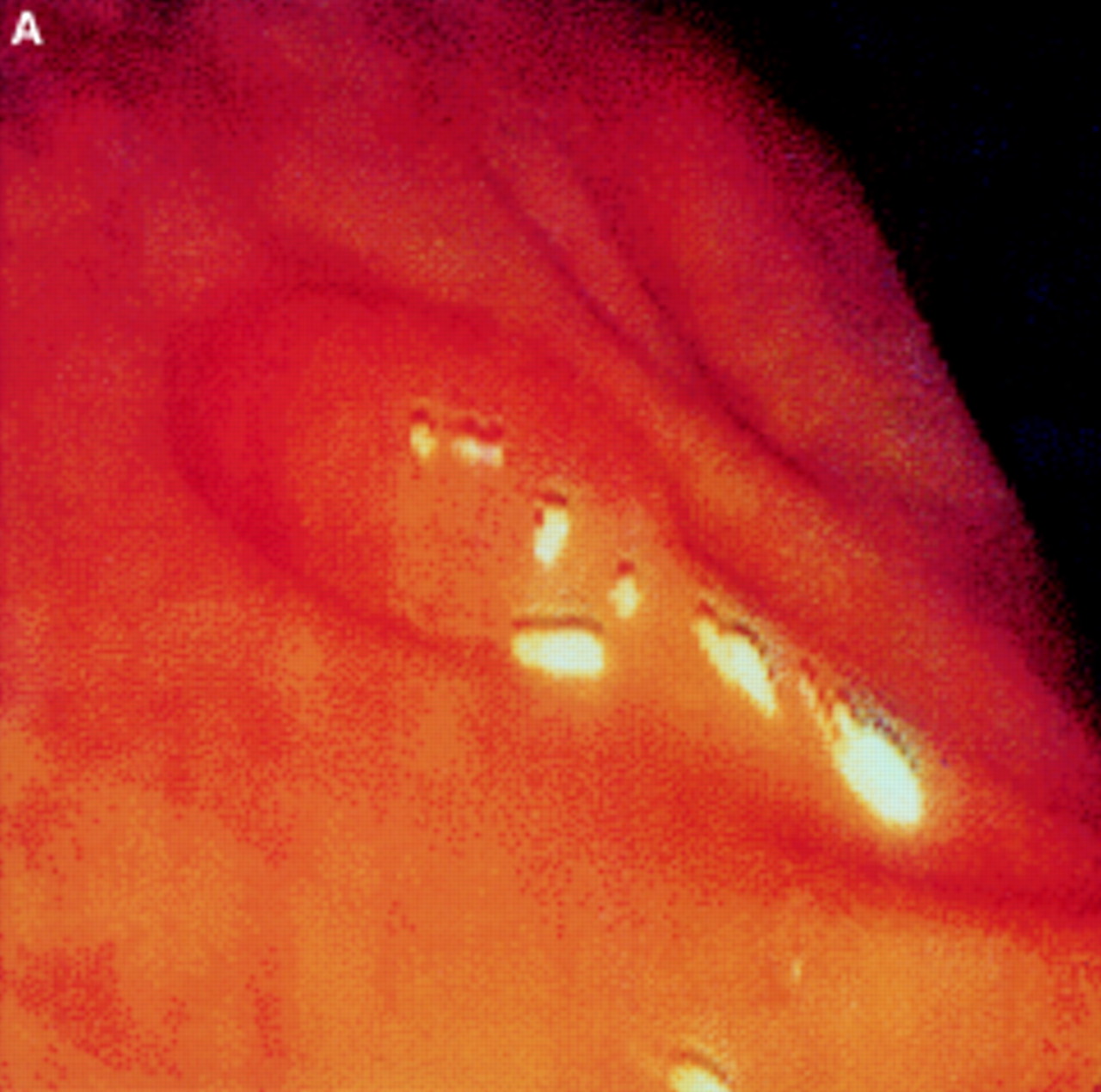
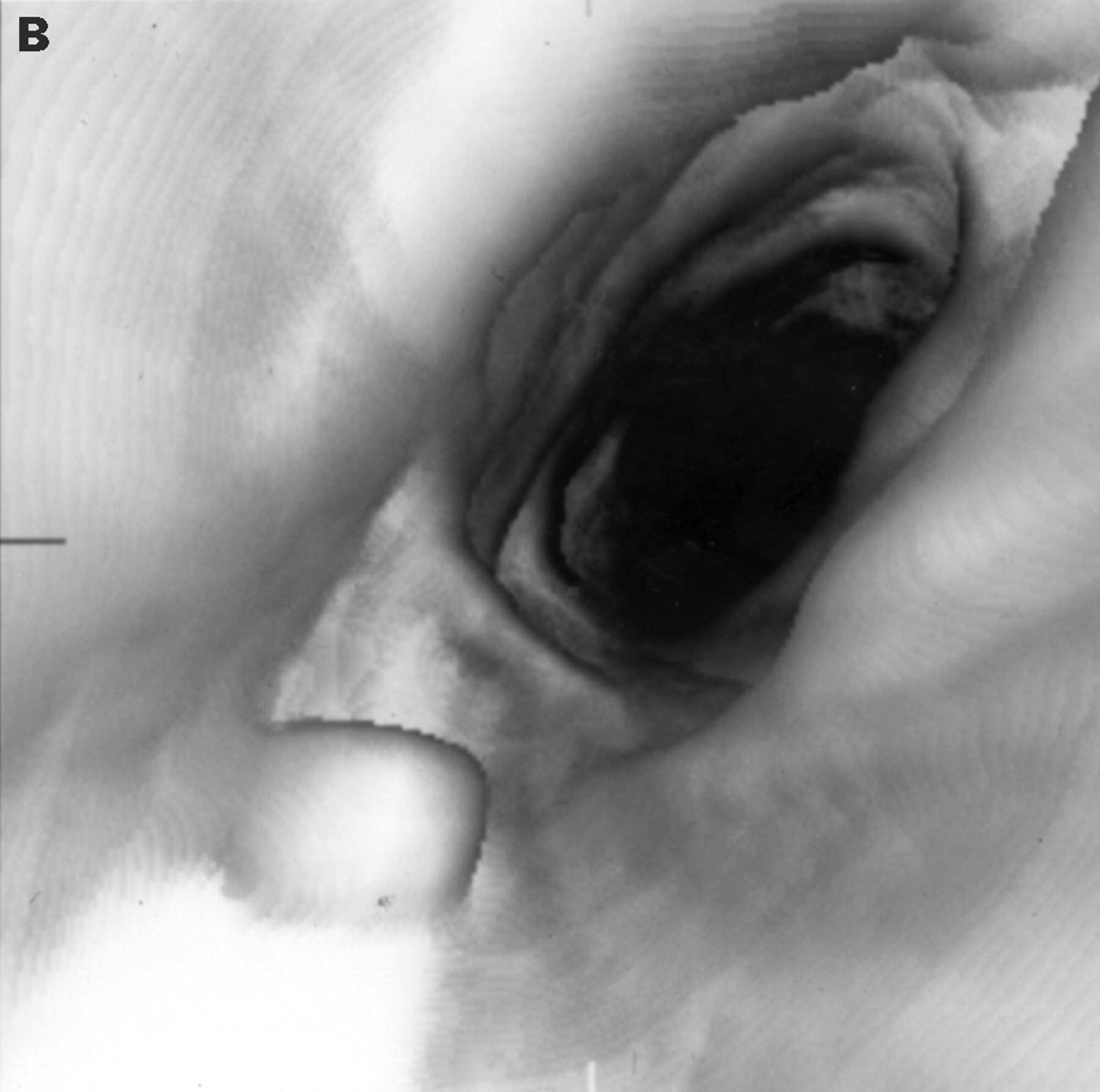
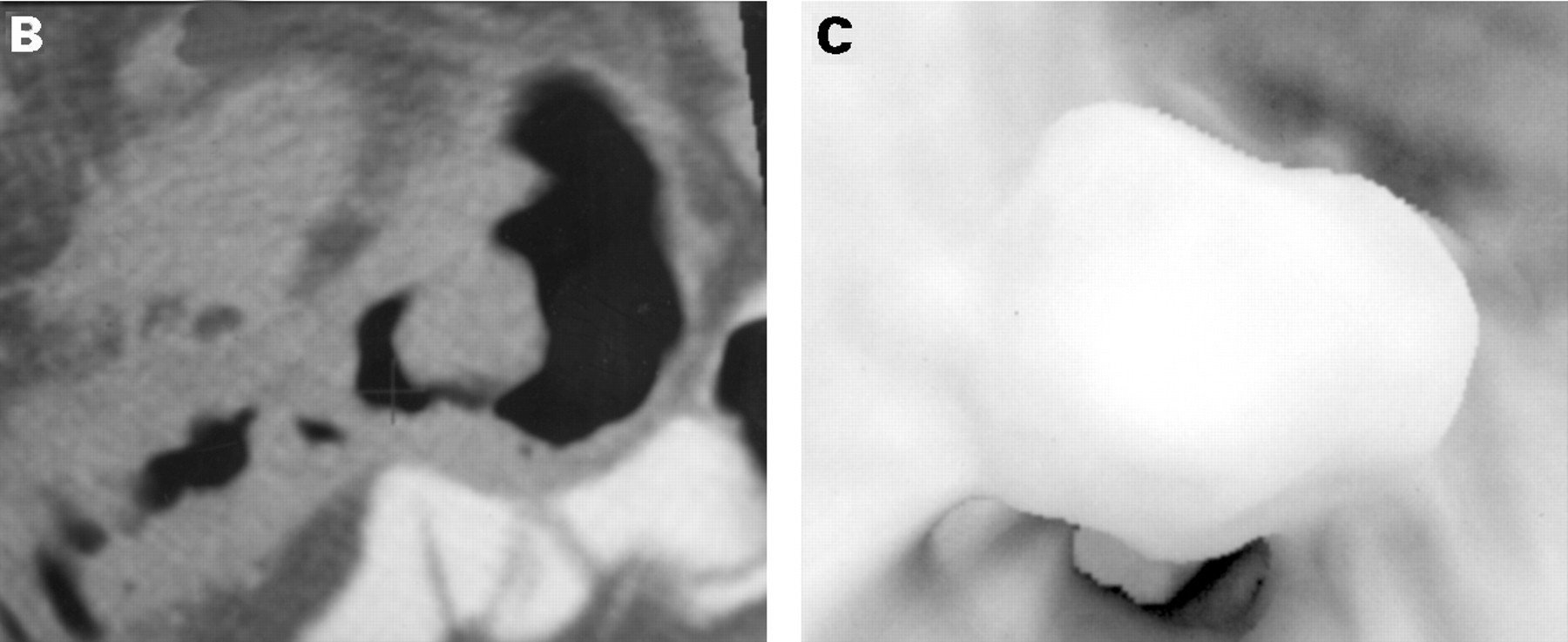
(A) Colonoscopic, (B) two dimensional view and (C) endoluminal three dimensional image of a polypoid carcinoma.
The data acquisition phase of the examination is very brief. After thorough bowel preparation the patient is placed in the lateral decubitus position and the small enema tip is placed into the rectum. Using either room air or carbon dioxide, the colon is fully distended without causing the patient undue discomfort. A single acquisition generally takes three to four 20 second breath holds (60–80 seconds of CT scanning total). Most centres have chosen to collect data in both the supine and prone positions. For data acquisition in the prone position, the patient is turned, additional gas is introduced into the colon if necessary, and another 60–80 second session of CT scanning is performed. This rapid examination without the use of sedation, intervention, or compression is very well tolerated and assessed by patients to be more comfortable when compared with other full colonic examinations such as barium enema or colonoscopy.13
Following data acquisition, the examination is reviewed by a radiologist at an off-line workstation using specialised imaging software to produce three and two dimensional images of the colon. In some cases it may be necessary to perform a midline trace of the colon in order to develop an electronic path for the “camera” to follow as endoluminal images are displayed throughout the length of the colon. A midline trace can usually be performed in about 10 minutes, but in some tortuous and redundant colons defining the midline trajectory can be more time consuming.14 Methods of developing automated midline tracing are under development. Some software systems do not depend on a midline trace, but examine the colon using traditional axial CT images primarily and reserve the use of the two dimensional reformatted views and three dimensional views to confirm the presence of a lesion, or to solve an imaging problem. Other methods of image display are also under development. Methods simulating the colon opened by a surgical pathologist (sometimes referred to as “virtual pathology”) display long segments of the colon opened along its longitudinal axis.15 The “best” method for displaying the colon has not been agreed. In all likelihood, each type of image display provides helpful information to the examiner. It is likely that all of these methods of image display will be found to be complementary, and that the “best” software will be able to display the colon in a variety of unique ways.
The radiation dose necessary for CTC is much lower than that used for a conventional CT examination because of the high contrast between the air filled colonic lumen and the soft tissue density wall. At our institution, a 75% dose reduction has been obtained without sacrificing examination performance.16 Examining the colon by CT in both the supine and the prone positions provides an overall radiation dose equivalent to the barium enema. This dose saving allows CTC to be considered as a routine colon screening examination. The lower radiation dose does result in images with a lower signal to noise ratio, reducing the diagnostic effectiveness in evaluation of solid abdominal organs (liver, kidneys and spleen).
CLINICAL ASSESSMENT
The first blinded prospective study assessed 70 patients (half with confirmed colorectal polyps, and half from a surveillance population).17 All patients underwent colonoscopy which served as the gold standard. For the detection of patients with lesions 1 cm or larger in diameter the sensitivity of CTC was 75% and the specificity 90% (figs 2-4). Performance decreased as the size of the lesion decreased. The sensitivity and specificity for lesions 5–9 mm in diameter were 62% and 69%, respectively.17 False negative examinations resulted from perceptive errors or technical problems. A major technical issue was fluid filled segments of bowel caused by the lavage bowel preparation and a single supine scan. Collapsed segments of bowel from colonic spasm were also considered important causes of technical errors. One 3 cm flat lesion (elevated = 2 mm from the surface of the colon) in the caecum could not be detected either prospectively or retrospectively. Flat lesions will continue to be a challenge with the current CT technique, unless surface textural differences can be increased.
It is encouraging that technical problems related to retained fluid and incompletely distended segments of the colon can often be corrected with the addition of prone imaging. A prone scan in combination with a supine scan will readily move colonic fluid into opposite parts of the colon. Although a large prospective study has yet to be published on the added value of prone imaging, we expect that the sensitivity for the detection of lesions 1 cm or larger to improve significantly to the 80–90% range.15 Other changes may also help to improve performance including online monitoring of CT examinations, the addition of added intracolonic gas between supine and prone acquisitions, intravenous or subcutaneous, or both, spasmolytic agents, and scanning of problematic areas in decubitus positions.
False positive examinations are generally the result of misinterpretation of retained stool or colonic folds as polyps. Retained stool, commonly seen in many examinations, was less problematic than originally anticipated. Retained stool often contained incorporated air that can be recognised at CT as a heterogeneous filling defect (fig 5). Colorectal neoplasms would be expected to be of solid soft tissue density, without intratumoural air. It may be possible in the future that oral stool markers administered 24–48 hours prior to the CT examination can be used to alter the density of stool and improve differentiation of stool from soft tissue neoplasms.

(A) A polypoid filling defect is present on the endoluminal three dimensional image. (B) The filling defect is of heterogeneous internal density, characteristic of retained air in stool. (From: Hara AK, Johnson CD, Reed JE. Colorectal lesions: evaluation with CT colography. RadioGraphics 1997;17:1157–67.)
The detection of large colorectal polyps and cancer has been studied by Roister and colleagues in 20 patients.18 All 20 lesions 2 cm in diameter were detected using CTC. Fourteen of the 15 lesions less than 2 cm in diameter were also successfully detected. Colonoscopy was only possible in 12 of these 20 patients because of large obstructing colonic lesions. Detection of abnormalities proximal to obstructing cancers and localisation of abnormalities within the colon prior to colonoscopy are important advantages of CTC.
Diagnostic interpretation time remains an important issue in moving CTC from the research laboratories to routine clinical practice. Early studies of this technique were plagued with long interpretation times, often requiring in excess of 60 minutes. Image displays other than three dimensional endoluminal views have been studied, and are helpful in reducing interpretation time significantly (average 11 minutes) without sacrificing diagnostic performance.19
Comparison with other techniques
CTC represents another colorectal screening option for physicians and patients. As a full structural colorectal imaging test it competes with barium enema and colonoscopy. Its diagnostic potential seems to be much greater than faecal occult blood testing (FOBT). More than half of all colorectal cancers and the large majority of polyps will be missed on a single screening pass with FOBT, and most positive test results are false positive.20-22 Because premalignant adenomas are not adequately detected, FOBT screening does not affect the incidence of colorectal cancer.1 ,23 ,24 The small but significant reduction in colorectal cancer mortality associated with FOBT seems to be largely because of the detection of early stage cancers. As such, FOBT screening effectiveness drops precipitously if screening intervals are lengthened beyond one to two years.1 ,23 ,24 As CTC would detect both cancers and polyps, screening could be done much less frequently.
Proctosigmoidoscopy is inherently flawed by its ability to examine only the left colorectum. As a full structural colorectal screening test it is anticipated that CTC would yield substantially more neoplasms.
CTC competes most directly with screening barium enema and formal trials comparing these two techniques have not yet been completed. There are some inherent advantages to CTC over barium enema. These advantages include no requirement for coating the colon with barium, little affect from retained fluid if prone imaging is performed, lack of complex overlapping radiographic lines (an important source of radiographic perceptive errors at barium enema), ability to produce an infinite number of different projections of a colonic segment, and no need for a second cathartic preparation prior to colonoscopy if a polyp is discovered. In addition, because the examination is very rapid, it is more comfortable and better tolerated by patients.
In comparison with colonoscopy, CTC cannot be used to remove tissue. Potential advantages of CTC include visualisation of colonic anatomy from both an endoluminal perspective as well as in multiple cross-sections, elimination of “blind spots” behind colonic folds as the entire colon is almost always evaluated, assessment of the internal density of lesions, and characterisation of many lesions (polyps, stool, lipomas) without the risks associated with sedation and biopsy (fig 6). Although a formal study on compliance with CTC has not been performed, in a survey after CTC, barium enema and colonoscopy patients stated that they were more willing to return for CTC at the recommended screening interval than for the other two tests.13

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Large polypoid intraluminal filling defect on an endoluminal three dimensional image. (B) The internal density of the mass is fatty on the two dimensional image, pathognomonic of a benign lipoma. (From: Hara AK, Johnson CD, Reed JE. Colorectal lesions: evaluation with CT colography. RadioGraphics 1997;17:1157–67.)
The future
CTC is an important and exciting technique for imaging the colorectum. Theoretically, this technique has advantages over all existing colorectal screening tests. Early results are promising, but rigorous scientific evaluation of this technique in comparison with other colorectal tests needs to be done. We can expect continued technological developments both in CT scanners that enable more rapid and effective data acquisition and in imaging software. It is likely that the entire colon data set will be acquired at CT within a single breath hold. In addition, automated methods of displaying the colon and computed assessment of colon wall thickness may assist radiological interpretation. It is conceivable that examinations will be interpreted correctly within only a few minutes and some of these may be read entirely by a computer. The cost of these examinations has not been determined as yet but will be dependent upon both the use of resources and the time required for interpretation of data. Costs will probably decrease as efficiencies improve with technical advances. Within the next few years charges for CTC are likely to be highly competitive with those of other structural colorectal screening tests.
Preparation for colorectal screening is a major obstacle for patient compliance. Development of a preparationless CTC scan is possible, but only preliminary work has been done to date. Theoretically, patients would drink a contrast agent one to two days before the examination. This agent would alter stool density sufficiently so that it could be recognised and removed electronically. Purging would not be required. Many different stool markers are currently under development and clinical trials are likely to begin within the next few years.
Colorectal screening has come of age. Traditional screening methods have now been approved in the United States for widespread general colorectal screening. New techniques such as CTC offer the promise of improved performance and better compliance. Hopefully, such new developments will identify patients with polyps and cancer and, in conjunction with colonoscopy, will reduce significantly the incidence of and mortality from this common disease.
Abbreviations
- CT
- computed tomography
- CTC
- computed tomography colonography
- FOBT
- faecal occult blood testing.
References
Footnotes
Leading articles express the views of the author and not those of the editor and editorial board.