Article Text

Statistics from Altmetric.com
Summary
Gastric dysplasia is believed to be the penultimate stage of gastric carcinogenesis. Its clinical importance has been underscored since its close association with gastric cancer was established. However, diagnostic criteria and grading schemes have evolved differently in different parts of the world. This has resulted in disagreement regarding differentiating features of both preinvasive and early gastric cancer between Western and Japanese histopathologists thereby preventing their direct comparison. Therapeutic guidelines are also controversial. On this background we review the current concepts and contemporary issues related to gastric dysplasia and early invasive carcinoma, their definition, classification, grading, natural history, potential therapy, and outline some of the recent efforts to harmonise the differences in terminology between Japanese and Western pathologists in order to produce a single classification system that would potentially be applicable throughout the gastrointestinal tract.
In the field of gastrointestinal pathology the term dysplasia is used by histopathologists to describe premalignant lesions.1-3 In the stomach, like any other segment of the gut, it is defined as an unequivocal neoplastic non-invasive epithelial alteration.1 ,4 The observation of gastric dysplasia as a precursor lesion of gastric cancer was made over a century ago, but it is only with the accrued use of upper endoscopy that its clinical significance has been stressed.5 Thus, the relevance of standardising the diagnostic criteria for gastric dysplasia and early invasive carcinoma, and of refining our understanding of its natural history have become increasingly important. However, to date, several unresolved issues pertain to gastric dysplasia: (a) lack of a uniformly recognised classification; (b) significant interobserver variability in microscopic diagnosis; (c) absence of well defined dysplastic features associated with the diffuse type of gastric carcinoma; (d) a limited understanding of the clinical significance of a diagnosis of dysplasia; and (e) variations in the therapeutic approach.
We therefore review the concept of gastric epithelial dysplasia, its definition, classification and natural history. We also describe the recent attempts to define an internationally accepted classification.
The concept of gastric dysplasia and its clinicopathological background
CONCEPT OF GASTRIC DYSPLASIA
Retrospective analysis of gastrectomy specimens for cancer was instrumental in recognising the frequent association between dysplastic epithelium and gastric adenocarcinoma and in suggesting its role as a precursor lesion. What was called moderate to severe dysplasia was associated with 40–100% of early gastric cancers and was found adjacent to 5–80% of advanced adenocarcinomas, suggesting a direct role in cancer formation.4 ,6 ,7 With the introduction of fiberoptic upper endoscopy in the late 1960s and early 1970s, Nakamura and Nagayo in Japan were among the first to identify possible precursors of gastric cancer on biopsy material and develop several classification schemes for dysplasia (or atypia as it is frequently called in Japan).8 ,9 In the West, Grundmann in 1975 quoted for the first time the word dysplasia to describe exclusively precancerous gastric lesions.10 Shortly thereafter a WHO committee sanctioned this usage and detailed general diagnostic principles based on cellular atypia, abnormal differentiation and disorganised architecture.11 ,12 Some pathologists, however, initially interpreted as dysplastic what subsequently became identified as regenerative changes.13 ,14 Eventually dysplasia was defined as a benign unequivocal neoplastic epithelial lesion, histologically distinguished from invasive carcinoma and also from reparative changes.1 Although first coined for inflammatory bowel disease this has now become the preferred use for “dysplasia” throughout the gastrointestinal tract.
Epidemiological and histopathological studies pioneered by Correa have shown that intestinal type gastric cancer frequently develops through a sequence of histological events: namely diffuse chronic gastritis, often mucosal atrophy, intestinal metaplasia (complete and/or incomplete), dysplasia, and finally invasive carcinoma.15Following this scheme gastric dysplasia usually develops in the setting of intestinal metaplasia (frequently of incomplete type) although it may also occur in apparently normal gastric mucosa.16Several prospective and retrospective serological studies have now linked Helicobacter pylori infection to gastric cancer.17-20 Helicobacter pylori infection is clearly associated with the induction of chronic inflammation of the gastric mucosa and the progressive development of metaplastic changes.21 However, the exact biological role of Helicobacter pylori in the genesis of neoplastic changes is not clearly established. Although the role of nutritional habits and carcinogens in the carcinogenic process was initially favoured there is also mounting evidence of indirect DNA damage and increased mucosal proliferation secondary to the bacterial infection.22-25
CLINICOPATHOLOGICAL FEATURES OF GASTRIC DYSPLASIA AND ENDOSCOPIC APPEARANCE
Figures quoted for prevalence of gastric dysplasia vary widely. The diversity of the data results in part because of differences in the populations studied, and also in the differing use of the term dysplasia. The origin of the population (various ethnicities) or whether a population at large or a specific group at increased risk (i.e., patients with underlying chronic gastropathy) is surveyed, are important variables. Prevalences of dysplasia reported in the general Western population range from 0.5 to 3.75% but figures of between 9 and 20% are reported in high risk areas for gastric carcinoma like Colombia and China.7 ,11 ,26-28 The prevalence of dysplasia in patients with chronic atrophic gastritis, ulcers or after gastrectomy varies from 4 to 30% and up to 40% in patients with pernicious anemia.29-31 Although some variation results from actual difference in risk, it is probable that differences in histological classification account for some of the variation. For example, in one series, 92% of cases of dysplasia in a population displaying a prevalence of 20% were classified as mild, arguably sometimes representing a regenerative process and not a neoplastic process.32 In particular, reactive and reparative changes in complete and incomplete intestinal metaplasia are neither well described nor well recognised.
Most diagnoses of dysplasia are reported in men.27 ,32 ,33The female to male ratio has been reported to be between 1:3 and 1:3.9.26 ,27 ,34 The male predominance is not unexpected as the same pattern occurs for gastric carcinoma. This also seems to be the case in areas of low prevalence. One study in Colombia, however, failed to show the same sex disparity, finding same prevalence in both sexes.35 The average age of the patients ranges from the fifth to the seventh decade of life (range 28–86 years).26-28 ,33 Usually the patients with high grade dysplasia are older than those diagnosed with low grade dysplasia, whereas there is no age difference between patients with high grade dysplasia and those with adenocarcinoma.28 ,34 ,36 It one series37 age (>60 years of age), male sex and severe atrophic gastritis of the surrounding mucosa were independent risks factors for the progression of dysplasia.
All degrees of dysplasia are more prevalent in the gastric antrum and angularis.32 ,34 Dysplasia can be associated with a variety of endoscopic abnormalities. Overall the same gross lesions are equally associated with different grades of dysplasia. These include ulceration and atrophic gastritis, which have been noted in 30–60% and 8–93% of cases respectively, variations that probably include confusion of reparative changes with dysplasia, or the study of highly selected patients.27 ,33 ,34 ,38 ,39 Other endoscopic lesions associated with epithelial dysplasia are polyps (8–30%), erosions (0–9%), plaques (0–8%), and scars (0–3%).27 ,33 ,34 ,38 ,39 Dysplasia has been associated with an endoscopically unremarkable mucosa in 7–60% of cases depending on the series.27 ,33 ,34 ,38 ,39 Again, histological diagnostic criteria and possibly endoscopic technique may have resulted in these discrepancies.
Diagnostic criteria of gastric dysplasia and grading
Gastric dysplasia is characterised microscopically by a set of histological alterations. The diagnosis relies on cytological (cytoplasmic mucin depletion, cellular crowding and pleomorphism, nuclear hyperchromatism, pleomorphism and stratification, increased nuclear:cytoplasmic ratio, and increased mitotic activity) and architectural abnormalities (glandular disarray or budding with irregular branching and dilatation, and intraluminal folding). Several types of gastric dysplasia have been reported in the literature but what authors refer to most frequently isadenomatous dysplasia, thought to be the precursor of intestinal (or tubular) gastric adenocarcinoma, the most common type of gastric cancer in populations at risk.40 ,41
ADENOMATOUS DYSPLASIA
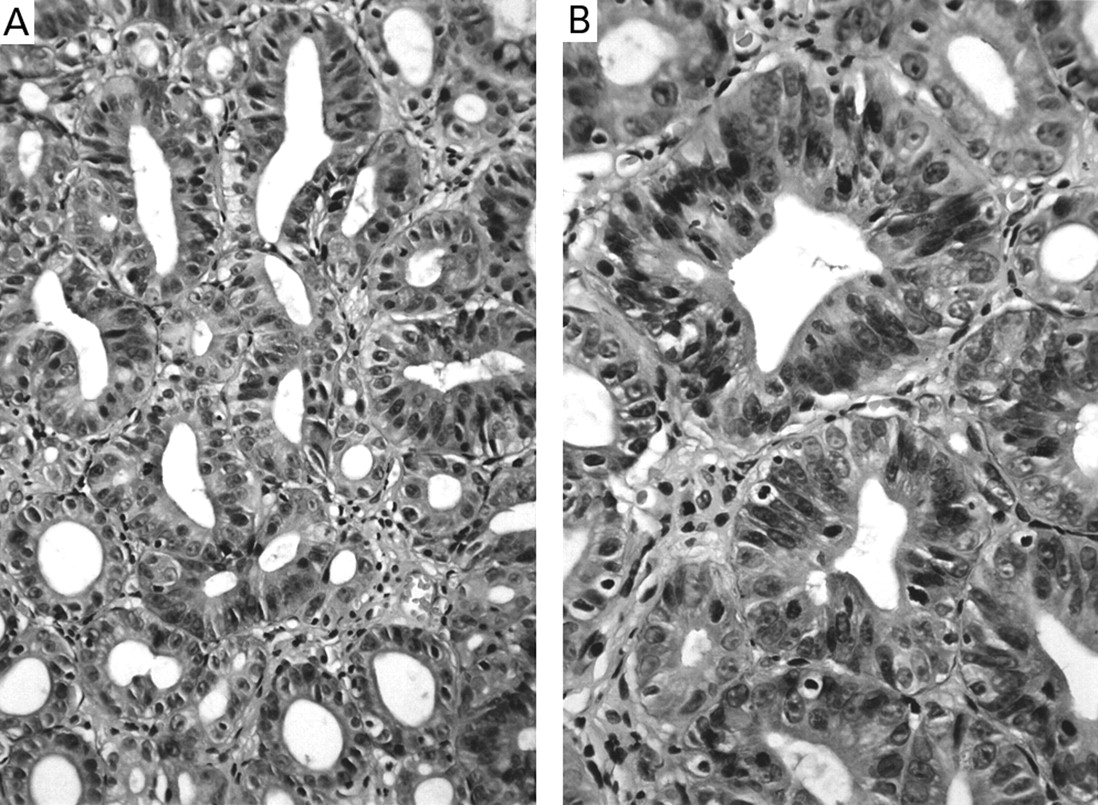
This term has been quoted to emphasise the similarity between the histological features of adenomatous lesions of the colon and dysplastic lesions arising in chronic inflammatory bowel disease and Barrett’s epithelium (fig 1).1 ,2 Some confusion exists in relation to the usage of the terms adenoma and dysplasia. Gastric dysplasia can arise as a flat or depressed process or present as a raised circumscribed lesion protruding above the mucosal surface, sometimes referred to as an adenoma.14 ,42 Most gastric adenomas are sessile and display either a flat (tubular), a tubulovillous or villous architecture.16 ,42-44 The term cryptal dysplasia has been used to describe the dysplastic changes involving predominantly the deeper portion of the mucosa.7

Low grade dysplasia, adenomatous type. (A) Large tubules resembling colonic adenomas. (B) At higher magnification, the cells have elongated, closely packed nuclei with dense chromatin. They are confined to the basal half of the cells and retain their polarity.
TYPE II DYSPLASIA
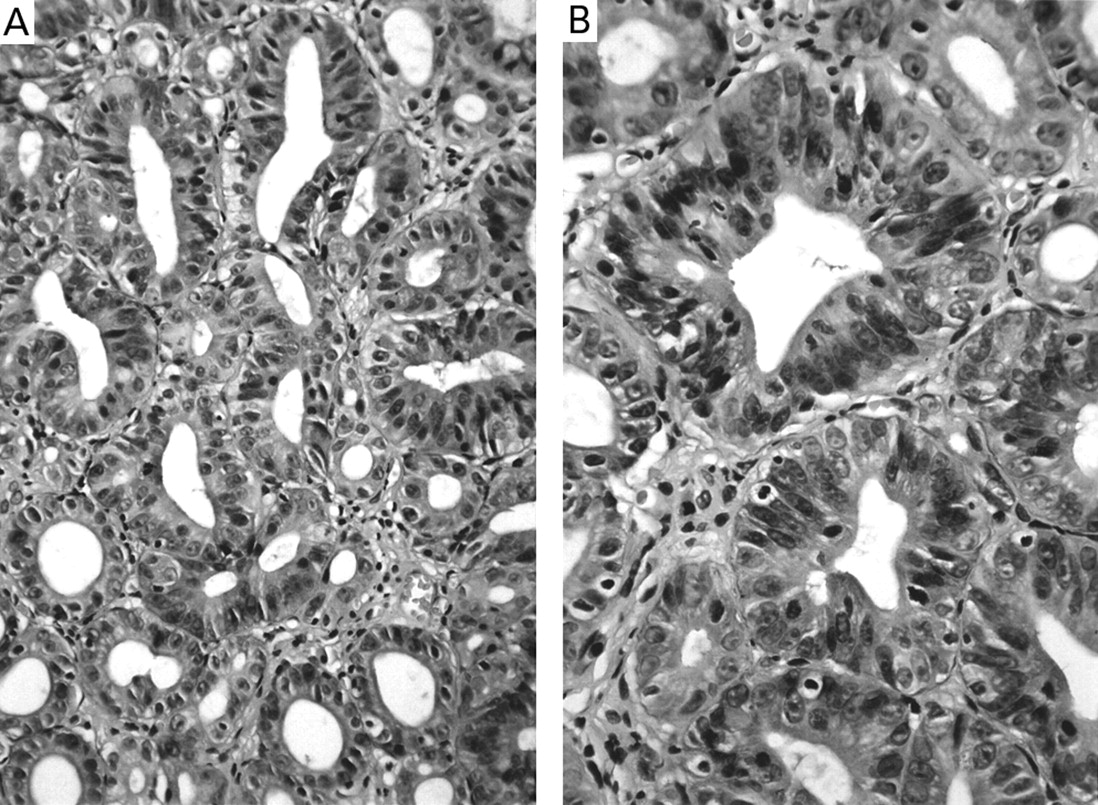
Type II dysplasia, reported by some as hyperplastic dysplasia, also frequently arises on a background of chronic atrophic gastritis with immature intestinal metaplasia.4 ,45 ,46 The histological features are less well established than in adenomatous dysplasia. Architecturally, it may display foveolar hyperplasia with irregular glandular branching and epithelial folding.5 ,46The lining epithelium is formed of tall columnar cells with pale cytoplasm with loss of polarity, hyperchromatic ovoid nuclei and few goblet cells. The mild form of this type of dysplasia is easily confused with regenerative changes. In the severe form prominent vesicular nuclei with an increased nuclear:cytoplasmic ratio and prominent nucleoli are seen. Nuclear stratification and numerous mitoses can also be seen (fig 2).
{kind=link}
{kind=link}
High grade type II (hyperplastic) dysplasia. (A) Closely packed glands with mild luminal festooning. (B) At higher magnification, the cells display oval/round open nuclei with prominent nucleoli and frequent mitoses can be seen. The nuclei reach the apical region of the cells and their polarity is partially lost.
TUBULE NECK DYSPLASIA
The identification of the precursor lesion of the diffuse type of gastric cancer has been a difficult task. This carcinoma, characterised by single cell infiltration of the lamina propria, is mainly associated with non-metaplastic mucosa.16 ,47 Early observers noticed that tumour cells seem to bud off the glandular neck regions of tortuous gastric tubules.10 ,47 Closer observation of the tubules revealed crowding of the neck region by enlarged clear cells. The nuclei of these cells also appear to be enlarged, vacuolated with prominent nuclei and loss of nuclear polarity, and look very similar to their invasive counterpart. These changes are believed to represent precancerous lesions and have been reported as tubule neck dysplasia or globoid dysplasia. One animal experiment was successful at reproducing these changes.48Another study also attempted to characterise different histological grades based on the degree of cytological atypia and the extent of glandular involvement.47 However, tubule neck dysplasia is very subtle and not readily recognisable, even on morphometric analysis.49 Thus although pathologists have no hesitation in recommending excision of conventionally dysplastic lesions, even those that recognise tubule neck dysplasia would not recommend resection if it appeared in a biopsy sample. Polyps of this type of dysplasia either do not seem to exist or are unrecognised.
Grading of (adenomatous) dysplasia and interobserver variability
GRADING OF DYSPLASIA
According to the severity of histological abnormality gastric dysplasia has been graded using either a two tier system of low and high grade dysplasia or three tier system of mild, moderate or severe dysplasia.7 ,12 ,33 ,42 ,45 ,46 ,50 Grading is easier and more reproducible in a two tier than in a three tier system. These inevitably become three or five tiered systems (e.g. mild to moderate dysplasia), although, surprisingly, the use of an intervening term for high and low grade dysplasia seems to have been largely avoided. In 1984 Ming and an international panel recommended that moderate and severe dysplasia be grouped in a single category as they cannot be sharply distinguished and actually coexist.51 However, the same can also be said of mild and moderate dysplasia, at least when both are defined as above and exclude reactive lesions. The use of low grade instead of both mild and moderate permits a reasonable comparison between both.
In low grade dysplasia, the cells have closely packed basal nuclei with dense chromatin (fig 1). The nuclei are also elongated in shape and if pseudostratified retain their polarity and are confined to the basal half or two thirds of the cell. Classic “moderate” dysplasia has nuclei that extend into the upper two thirds of the cell so that the broadening of low grade dysplasia to include this common morphological subgroup is appealing.
In high grade dysplasia, the nuclei regularly extend into the luminal aspect of the cell in the adenomatous variant but in type II dysplasia are frequently oval, round or irregularly shaped, with more open and clumped chromatin confined to the lower half or two thirds of the cells (fig 2). Prominent nucleoli are often seen, as are frequent mitoses. More often than not the nuclei reach the apical region of the cells and their polarity is partially or totally lost. Because the cells are small and relatively cuboidal and the nuclei relatively large, it is easy for them to occupy most of the cell so that the distinction between low and high grade dysplasia can be hazy. Low grade dysplasia may be difficult to differentiate accurately from atypical reactive/regenerative epithelial changes.4 ,14 ,52 ,53 In the latter, the cells usually appear immature and may be cuboidal with basophilic cytoplasm, large but often widely opened and relatively widely spaced vesicular nuclei and reduced or absent mucus secretion. They may or may not be uniform in shape and size with basally or centrally located nuclei. They are also arranged in a row and if present the pseudostratification is considerably less than in adenomatous, but not necessarily type II dysplasia. Mitoses are often present but not on the surface and abnormal mitoses are absent. Increased cellular differentiation and maturation is usually seen toward the luminal surface.
High grade dysplasia also includes the lesion referred to as carcinoma in situ, which is a non-invasive lesion so called because virtually identical changes can be found in invasive carcinoma. Less publicised is the fact that any dysplastic lesion can give rise directly to invasive carcinoma of identical morphology, but this is a much less frequent occurrence from low grade dysplasia. There is also no agreement on whether the changes known as carcinoma in situ should be architectural, cytological, either or both. Furthermore, in the Japanese system, many lesions called high grade dysplasia are also called carcinoma, especially those of type II dysplasia. This can result in overdiagnosis of cancer by Western standards by Japanese pathologists, or underdiagnosis by Japanese standards by Western pathologists. The implication of these differences is that data generated from these two systems are usually not directly comparable.
The difficulty in differentiating reactive from dysplastic changes may account for reports of reversibility of low grade dysplasia.4 ,32 In cases where there is a real interpretative problem, the term “indefinite for dysplasia” is sometimes used. However, operationally this is a diagnosis of exclusion obtained by getting a negative response to the two questions, “is this epithelium unequivocally negative for dysplasia?” (this including all reparative epithelium) and “is this epithelium unequivocally dysplastic?”. Epithelium that is not unequivocally negative or unequivocally dysplastic is, by definition, indefinite for dysplasia.
At the other end of the spectrum it can sometimes be very difficult to separate high grade dysplasia from intramucosal carcinoma. Numerous small glands budding out of the lamina propria can be difficult to distinguished from invasion. Previously held concepts such as breaching the basement membrane sound good in theory but are difficult or impossible to apply on haematoxylin and eosin sections, in which it is not visible. Irregularity of pit outlines with irregular infiltration into the lamina propria is what is used operationally.
INTEROBSERVER VARIABILITY
Interobserver variability in diagnosing dysplasia in the gastrointestinal tract is inevitable whenever a continuous spectrum is subjectively divided, as has been previously reported, particularly in Barrett’s oesophagus and ulcerative colitis.1 ,2 ,54 ,55Whenever a group of pathologists examine the same biopsy sample, the result is inevitably a distribution curve around a mean. The issue becomes the width of the curve. Usually this is about half a grade, although when the extremes of the spectrum (no dysplasia, high grade dysplasia) are used the variation can only go in one direction and therefore is inevitably less. The corollary is that it is also possible to select biopsy samples that are literally on the borderline between two categories, e.g. low and high grade dysplasia, so that one would expect that there will always be 50% of observers calling it low grade and 50% calling it high grade. Nevertheless, with severe reactive changes the alternative diagnosis may be high grade (type II) dysplasia. Similar problems have been found in the stomach.38 ,50 ,53 ,56 The problem may also be partly related to the relative lack of experience of some histopathologists in diagnosing gastric dysplasia. Differentiating reactive changes such as foveolar hyperplasia and metaplastic changes from low grade/moderate dysplasia is a challenge for many.38 ,50 In one series 51% of cases diagnosed as hyperplastic or metaplastic lesions by specialists were initially diagnosed as moderate dysplasia by general histopathologists.38 Less variation is usually noted for higher grade lesions. In the same series 65% of the original diagnoses of severe dysplasia were confirmed whereas 10% were downgraded to moderate dysplasia and 6% diagnosed as carcinoma.38Variations also exist among pathologists with an interest in gastrointestinal pathology.53 ,56 Inherent difficulties in agreeing upon the definitions of mild to moderate and high grade dysplasia are translated by moderate sensitivities of 82 and 83% in diagnosing these lesions whereas higher specificities (92.8 and 92.3% respectively) indicate agreement on the minimal diagnostic criteria.53 In the same series, when all dysplasias are included in a single category, a mean κ of 0.7, indicative of moderate agreement, was calculated.53 As major therapeutic decisions may be taken after a diagnosis of dysplasia, it has been suggested that such a diagnosis be confirmed by seeking a second opinion from a gastrointestinal pathologist.1 ,57
To the gastroenterologists this may appear as incompetence on the part of the histopathologists. However, it is worth pointing out that histopathologists are medical consultants rendering their diagnostic opinion based both on morphological grounds and also on their understanding of the biology of the lesions. Similarly, it is neither expected nor observed that a patient will always receive the same medical treatment for the same disease in different institutions.
Clinical significance of endoscopy and guidelines for surveillance
The observation of dysplasia at the periphery of gastric cancer and the high risk of detecting an adenocarcinoma shortly after an initial diagnosis of high grade dysplasia clearly underscore its clinical importance. Two questions are important in regard to the clinical relevance of gastric dysplasia: (1) what is the risk of a patient developing gastric cancer when dysplasia has been detected; and (2) what is the time frame for developing an adenocarcinoma once a diagnosis of gastric dysplasia has been made? Several articles have tackled these issues, with varying results, partly a function of the reasons stated previously, including the classification used.
DIFFERENT RISKS FOR DIFFERENT GRADES
Using the three tier classification scheme,mild dysplasia was shown to regress in up to 89%, to persist in 11–19% and to progress to higher grades in 0–19% of cases.27 ,34 ,36 ,38 ,58 Only between 0 and 5% of patients with an initial diagnosis of mild dysplasia were eventually diagnosed with gastric adenocarcinoma. The likelihood that many of these lesions were reactive is apparent, but the possibility that a focal lesion was either not re-biopsied or had been removed completely by biopsy remains for all lesions that appear to “regress”.27 ,34 ,36 ,38 ,58 Between 27 and 87% of patients diagnosed with moderate dysplasiashow regression of the lesion, with the same possible interpretation as mild dysplasia; between 12 and 32% showed persistence at the same grade and between 4 and 40% were diagnosed with severe dysplasia during follow up. Importantly, 4–38% of patients were eventually found to have an adenocarcinoma. Up to 30% of patients with severe dysplasia showed regression whereas between 0 and 12.5% showed persistence. Between 60 and 81% of these patients were eventually diagnosed with a gastric cancer.
When the two tier system was used low grade dysplasia was shown to regress in between 38 and 49%, to persist in 19–28% and to progress to high grade dysplasia in between 0 and 15% of cases. High grade dysplasiaregressed in about 5%, persisted in 14% and progressed in 81–85% of cases. These results are significant because they underscore the predictive value of gastric dysplasia. The notable variations in the results, however, may be even more so when a three tier system is used, undermining the clinical practicality of a diagnosis of dysplasia.28 ,33
CHRONOLOGY OF MALIGNANT EVOLUTION
The chronology of the progression from one dysplastic grade to a higher grade or adenocarcinoma is critical in order to recommend appropriate treatment. In several series the time frame between a diagnosis of severe/high grade dysplasia and the identification of gastric cancer was between less than one month to 39 months with a mean between four and 23 months.33 ,34 ,38 ,39 ,58 Clearly the possibility that some of these lesions were already carcinomatous but the invasive element was not included in the original biopsy sample cannot be excluded. Following a diagnosis of moderate/low grade dysplasia, cancer was found during a mean follow up of 10–30 months with extremes of one and 39 months.33 ,34 ,38 ,39 ,58 Finally, although most cases of mild dysplasia are believed to regress, rare cases with a diagnosis of carcinoma after a median follow up of 34.5 months and 41.5 months have been reported,34 ,39 suggesting that either some of these lesions were unequivocally neoplastic or that they were not included in the original biopsy specimen. Analysis of several Western series revealed that 57% of cancers discovered during follow up were early gastric cancer, a figure out of line with prevalence in the population at large, but which underscores the importance of following patients closely in order to detect these lesions early.27 ,28 ,33 ,34 ,36 ,38
Practically, several conclusions can be drawn: (a) gastric dysplasia, as defined earlier, should be regarded as an important marker of cancer risk; (b) the higher the grade of dysplasia the greater the risk of developing invasive gastric cancer; (c) surveillance leads to detection of “early”, potentially curable adenocarcinoma; and (d) a period of few months for high grade dysplasia and longer for moderate and mild dysplasia is usually available to plan an adequate therapeutic strategy.
Although gastric dysplasia is usually described as a dynamic process, with a reported possibility of progressing/regressing, limited evidence of transformation exists. The actual progression of repeatedly biopsied, flat dysplasias has never been shown. Evidently, one limitation is the difficulty in sampling identical mucosal areas during endoscopic follow up. Series focusing on adenomas observed malignant foci in 5.9% of flat (tubular) adenomas and up to 33% of large villous and tubulovillous adenomas.43 However these figures might be inflated as malignancy in that article was established both when invasion was seen and also when severe architectural and cytological atypia were noted in the absence of invasion. Others reported malignant transformation in 11% of 85 cases examined and sequentially biopsied during an average follow up of 49 months.44 Alternatively, the frequent demonstration of the multifocal neoplastic process would indicate the presence of diffuse mucosal instability which is prone to malignant transformation.59 Thus, the various dysplastic grades could be viewed as representing independent distinct end points of epithelial transformation in a genetically unstable gastric mucosa likely to develop an adenocarcinoma eventually.
THERAPEUTIC GUIDELINES
Factors to be considered when designing therapeutic guidelines include understanding of the biological process and current technical capability. With regard to the biology, recent molecular studies have supported the histological assessment that gastric dysplasia is a neoplastic lesion.16 ,60 In addition, follow up studies, as discussed earlier, have clearly established risks and time frames for the development of gastric cancer.27 ,33 ,34 ,38 ,39 ,58 However, in spite of abundant literature it was shown that most gastroenterologists do not equate epithelial dysplasia to a neoplastic process.61Yet, when confronted with a diagnosis of high grade dysplasia most of these same clinicians recommend surgical treatment. Neoplasia means tumour to most, and the concept of adenomas and areas of flat dysplasia being non-invasive neoplasia still requires considerable education. Given this information and with the knowledge of notable interobserver variability in the pathological diagnosis, different recommendations have been drafted.
Many of the Western publications to date call for close endoscopic follow up of patients with moderate/low grade gastric epithelial dysplasia.34 ,38 ,39 ,58 The frequency of the follow up is variable but given the risk of malignant transformation endoscopy has been recommended every three to 12 months at least during the first year.27 ,28 ,36 ,38 An open question is how long the follow up should be maintained when no progression has been detected. Some suggest suspending surveillance when two endoscopies with multiple biopsy samples are negative at the six month interval.28
Provided that a diagnosis of high grade dysplasia has been confirmed, many authors suggest surgical resection because of the intimate association with invasive gastric adenocarcinoma.27 ,33 ,34 ,36 ,38 However, others argue that endoscopic follow up might be sufficient.39Increasingly, endoscopic mucosal resection has a place in the management of these lesions, although it is a skill to which relatively few hospitals in the West have access compared particularly with Japan where it is the standard practice for most centres. Although with some merit, once a synchronous carcinoma has been excluded, this conservative therapy is not immune to criticism. Dysplastic lesions are not free of the risk of malignant transformation and non-surgical resection can be curative.57 Another issue to enter into the equation is the patient’s compliance with protracted and costly follow up.57
With advances in endoscopic localisation (chromoscopy) and staging techniques (endoscopic ultrasound), endoscopic mucosal resection can offer non-surgical cure for intramucosal adenocarcinoma.62-65 However, these modern interventional endoscopic procedures are not widely available outside of the specialist centres and their place in treatment needs to be defined and made more widely available. Furthermore, the issue of protracted follow up in these patients at high risk of developing metachronous adenocarcinoma has still to be settled.
Discrepancies between Japanese and Western pathologists
It is quite apparent that there are major differences in concept, terminology and definitions between the Western and Japanese systems and this has been confirmed in several recent publications.53 ,56 ,66-68 Japanese histopathologists usually refer to a widely accepted classification sponsored by the Japanese Research Society for Gastric Cancer.69 In the West the lack of a consensus classification for the diagnosis of gastric dysplasia has added to the confusion.
It has been claimed that Japanese pathologists would frequently interpret as adenocarcinoma lesions that would be diagnosed as dysplasia by Western pathologists. In a large series of endoscopic gastric biopsy samples, 16% of the cases unanimously diagnosed as adenocarcinoma in Japan were reported as dysplasia by Western histopathologists.53 In the same series about 90% of Western high grade dysplasias were reported as carcinoma by most Japanese histopathologists. Schlemper’s cardinal study clearly showed that Japanese pathologists base their diagnosis of carcinoma on cytological changes (anisokaryosis), loss of polarity, prominent nucleoli, and architectural changes (complex branching and budding and back to back glands).56 Japanese pathologists frequently use the term “mucosal carcinoma” irrespective of the presence/absence of infiltration of the lamina propria. In such cases most Western pathologists would make a diagnosis of dysplasia (either low or high grade) as the sine qua non for a diagnosis of carcinoma is the recognition of invasion into the lamina propria or beyond. Another reason for the discrepancy is the recognition in Japan of a lesser degree of dysplasia characterised by demarcation from, and compression of, the normal surrounding tissue.8 Finally, some of the Japanese histopathologists endorse the concept of intraepithelial carcinoma, a concept that is not accepted by most of the Western histopathologists.
These discrepancies are troublesome as apparently different morphological criteria are used among all histopathologists and words such as dysplasia and carcinoma which were thought to have the same meaning for all clearly do not. The implications may be important. As already underscored by some, the difference in the prevalence of early gastric cancer between the East and West might be partly caused by variations in histopathological interpretation.53 ,56These differences in interpretation may also be responsible for the differences between Japan and the West in the incidence of lymph node metastasis and survival of patients with early gastric cancer. Finally, how these differences in diagnosis influence therapeutic decisions has still to be settled.56 ,70
In an attempt to solve these problems, there have been several interobserver studies, varying from one on one to large groups of pathologists.53 ,56 ,68 Each has made a little more progress in defining the problems and therefore setting in place the groundwork for resolving them by trying to determine points of equivalence between both systems, defining better unusual variants of both reactive and neoplastic lesions, and also constructively finding a system that could potentially be shared by all.53 ,56 ,68An international effort led by gastrointestinal pathologists from Asia, Europe and North America took place during the 1998 World Congress of Gastroenterology held in Vienna (see box). The aim of the meeting was to develop a consensus classification for neoplasia. It was further decided that any resulting system should have relevance for the entire gastrointestinal tract and the potential for tackling clinical and research issues. For light microscopy to remain the standard for molecular research into neoplasia it should allow identification of subtle morphological variations which may be associated with more specific molecular markers. For example, the recognition of flat and depressed adenomas and carcinomas of the large bowel and their lack of K-ras compared with more typical adenomas and carcinomas.71 The classification suggested (see box) was designed keeping in mind the classifications currently in use on the different continents and also to reflect the expected histological behaviour of the lesions and the clinical implications. An interesting feature is the grouping of high grade dysplasia/non-invasive carcinoma in situ (intraepithelial carcinoma) and suspicious for invasive carcinoma in a single major category. This stratification should improve interobserver reproducibility. It should also not diminish the informative value of the diagnoses in reference to the suspected biological behaviour of the lesions. Conversely, the reintroduction of the morphological lesion defined as non-invasive carcinoma (carcinoma in situ) when clinically appropriate may raise eyebrows as its inclusion in high grade dysplasia over the past decade has greatly simplified reporting and the chance of inadvertent erroneous decisions resulting from failure to understand the implications of a diagnosis of carcinoma in situ. Fortunately surgeons are now better educated, but this category remains a subgroup of high grade dysplasia so the use of the generic category high grade dysplasia (or its synonym non-invasive neoplasia, high grade) rather than the subcategory carcinoma in situ, is still appropriate.
Vienna classification of gastric neoplasms
The proposed classification is a five tier system.
CATEGORY 1: NEGATIVE FOR NEOPLASIA/DYSPLASIA
This category encompasses either completely normal gastric mucosa or various gastritides (Helicobacter pylorigastritis) or gastropathies (bile reflux gastritis/non-steroidal anti-inflammatory drug (NSAID) related gastropathy) as well as intestinal metaplasia.
CATEGORY 2: INDEFINITE FOR NEOPLASIA/DYSPLASIA
This diagnosis should be rendered when there is uncertainty about the nature of the lesion, whether it represents a regenerative/reactive process or a neoplastic lesion.
The cause of the diagnostic difficulty might be secondary to inflammation (sometimes related to H pylorigastritis) or reactive chemical changes (bile reflux gastritis, NSAID gastropathy) or because of the inadequacy of the specimen (small size, crushing artefact).
CATEGORY 3: NON-INVASIVE NEOPLASIA, LOW GRADE (LOW GRADE ADENOMA/DYSPLASIA)
This represents an unequivocal neoplastic process with low risk of malignant degeneration. It roughly corresponds to the generally previously accepted low grade dysplasia.
CATEGORY 4: NON-INVASIVE NEOPLASIA, HIGH GRADE (HIGH GRADE ADENOMA/DYSPLASIA)
These are a group of lesions with features more severe than those seen in low grade dysplasia but without unequivocal invasion. This category has been subdivided into three groups:
- 4.1
- high grade adenoma/dysplasia;
- 4.2
- non-invasive carcinoma (carcinoma in situ);
- 4.3
- suspicious for invasive carcinoma.
The grouping of those three different types of lesions is important in order to achieve a high interobserver agreement among pathologists, whether under Japanese or Western influence in terms of diagnosis of gastric dysplasia. The word “non-invasive” stands for the absence of evident invasion. It places together a lesion that Japanese pathologists would classify as carcinoma based on the presence of notable cytological alterations (carcinoma in situ) but that most Western pathologists would interpret as high grade dysplasia because of the absence of invasion.
CATEGORY 5: INVASIVE NEOPLASIA
This category encompasses:
- 5.1
- intramucosal carcinoma and
- 5.2
- submucosal carcinoma or beyond.
Intramucosal carcinoma corresponds to adenocarcinoma with invasion limited to the lamina propria or the muscularis mucosa.
It was also hoped that this classification could be applied throughout the gastrointestinal tract. Several working groups have been set up to determine the feasibility of this system in different segments of the gastrointestinal tract including squamous oesophagus, Barrett’s oesophagus, stomach, small bowel, large bowel, and anus. The different issues to be settled include (a) the usefulness of the terminology, ensuring that the divisions between and within each category are defined well enough that there is good interobserver reproducibility, thereby allowing the system to be used internationally, (b) that there is consistency of terminology in different organs within the gastrointestinal tract, and (c) its acceptability by the pathology and gastroenterology communities at large if all of these problems are resolved. With the universal goodwill apparent to those in Vienna the possibility of achieving these goals is clearly in sight, but there is still much work to be done.
Conclusion
The clinical importance of gastric dysplasia has been emphasised because of its close association with the risk of developing gastric cancer. However, in spite of the large increase in epidemiological and clinical data, facilitated by the accrued usage of upper endoscopy, challenges regarding classification and grading remain. In addition, disagreement between Western and Japanese histopathologists regarding diagnostic criteria for both preinvasive and early gastric cancer has led to the development of different grading systems. As a result direct comparison and analysis of clinical series are limited. Therapeutic guidelines also seem to be controversial. In order to facilitate communication worldwide several groups have recently attempted to harmonise the differences in terminology between Japanese and Western pathologists. We hope that their efforts are successful.
Classification of gastrointestinal epithelial neoplasia
CATEGORY 1
Negative for neoplasia/dysplasia
CATEGORY 2
Indefinite for neoplasia/dysplasia
CATEGORY 3
Non-invasive neoplasia low grade (low grade adenoma/dysplasia)
CATEGORY 4
Non-invasive neoplasia high grade
- 4.1
- High grade adenoma/dysplasia
- 4.2
- Non-invasive carcinoma (carcinoma in situ)a
- 4.3
- Suspicious for invasive carcinoma
CATEGORY 5
Invasive neoplasia
- 5.1
- Intramucosal carcinomab
- 5.2
- Submucosal carcinoma or beyond
a“Non-invasive” stands for absence of evident invasion.
b“Intramucosal” stands for invasion into the lamina propria or muscularis mucosae.
Acknowledgments
Participants at the Vienna Meeting: F Borchard, H S Cooper, S M Dawsey, M F Dixon, C M Fenoglio-Preiser, J-F Fléjou, K Geboes, T Hattori, T Hirota, M Itabashi, M Iwafuchi, A Iwashita, Y Kato, Y I Kim, T Kirchner, M Klimpfinger, M Koike, G Y Lauwers, K J Lewin, G Oberhuber, A B Price, R H Riddell, C A Rubio, M Rugge, R J Schlemper, M Shimizu, T Shimoda, P Sipponen, E Solcia, M Stolte, H Watanabe, H Yamabe.
Abbreviation used in this review
- NSAID
- non-steroidal anti-inflammatory drug