Article Text

Statistics from Altmetric.com
SUMMARY
Sepsis is a systemic inflammatory response to the presence of infection, mediated via the production of many cytokines, including tumour necrosis factor α (TNF-α), interleukin (IL)-6, and IL-1, which cause changes in the circulation and in the coagulation cascade. There is stagnation of blood flow and poor oxygenation, subclinical coagulopathy with elevated D-dimers, and increased production of superoxide from nitric oxide synthase. All of these changes favour endothelial apoptosis and necrosis as well as increased oxidant stress. Reduced levels of activated protein C, which is normally anti-inflammatory and antiapoptotic, can lead to further tissue injury. Cirrhotic patients are particularly susceptible to bacterial infections because of increased bacterial translocation, possibly related to liver dysfunction and reduced reticuloendothelial function. Sepsis ensues when there is overactivation of pathways involved in the development of the sepsis syndrome, associated with complications such as renal failure, encephalopathy, gastrointestinal bleed, and shock with decreased survival. Thus the treating physician needs to be vigilant in diagnosing and treating bacterial infections in cirrhosis early, in order to prevent the development and downward spiral of the sepsis syndrome. Recent advances in management strategies of infections in cirrhosis have helped to improve the prognosis of these patients. These include the use of prophylactic antibiotics in patients with gastrointestinal bleed to prevent infection and the use of albumin in patients with spontaneous bacterial peritonitis to reduce the incidence of renal impairment. The use of antibiotics has to be judicious, as their indiscriminate use can lead to antibiotic resistance with potentially disastrous consequences.
INTRODUCTION
Bacterial infections are a common complication of cirrhosis.1,2 Once infection develops, renal failure, shock, and encephalopathy may follow, which adversely affect survival. In fact, the inhospital mortality of cirrhotic patients with infection is approximately 15%, more than twice that of patients without infection. More importantly, infection is directly responsible for 30–50% of deaths in cirrhosis. Therefore, the International Ascites Club dedicated its 7th meeting to discussions on the most recent developments in the pathophysiology and management of sepsis in cirrhosis. The following is a summary of the meeting.
DEFINITION OF SEPSIS
Sepsis is the syndrome of the systemic inflammatory response to infection. However, insults such as trauma, pancreatitis, burns, etc, may provoke a syndrome that resembles sepsis. Hence the term systemic inflammatory response syndrome (SIRS) was proposed,3 as defined by the presence of at least two of the following criteria: (1) altered temperature, (2) elevated respiratory rate or hyperventilation, (3) tachycardia, and (4) altered white blood cell count (high, low, or immature forms) (table 1). Sepsis is then defined as SIRS in response to a proven or suspected microbial event.3 Both sepsis and SIRS comprise a continuum of injury. Sepsis is severe when associated with organ dysfunction. In sepsis with hypotension, systolic blood pressure decreases to >40 mm Hg from a baseline level or persists at <90 mm Hg despite adequate volume resuscitation. Septic shock refers to the requirement of vasopressors or inotropes, or the presence of lactic acidosis and perfusion abnormalities. Finally, multiple organ dysfunction syndrome is alteration of organ function such that normal homeostasis cannot be maintained without intervention. An infected patient may progress through these stages unless medical interventions can halt the disease process (table 1). The currently accepted clinical definition of SIRS and hence sepsis may not be entirely applicable to cirrhotic patients for various reasons, as listed in table 2.
Definitions of systemic inflammatory response syndrome (SIRS), sepsis, severe sepsis, and shock
Characteristics of the cirrhotic patient which may make definitions of systemic inflammatory response syndrome (SIRS) and sepsis difficult
INCIDENCE
Sepsis has an estimated annual incidence of 300/100 000 or 1/100 hospital admissions for any cause.4 The incidence of sepsis in cirrhosis is estimated to be at least 30–50% of hospital admissions.5 Once admitted, between 15% and 35% of cirrhotic patients develop nosocomial infections compared with an infection rate of 5–7% in the general hospital population.5 In addition to the factors which predispose the general population to the development of sepsis, the severity of the underlying liver disease also makes cirrhotic patients more susceptible to the development of sepsis.6 Infections in cirrhosis are mainly caused by bacteria, and are a common cause of death. The main sites of infection are ascites, lungs, urinary tract, and blood.1,2 The commonest organism is Escherichia coli, followed by Staphylococcus aureus, Enterococcus faecalis, Streptococcus pneumoniae, Pseudomonas aureginosa, and Staphylococcus epidermidis.2
PATHOPHYSIOLOGY OF SEPSIS
Infection activates various mechanisms to cause tissue injury and organ failure, including cytokine production such as TNF-α, IL-6, and IL-1, which initiate and propagate the inflammatory response, as well as changes in the circulation and coagulation cascade.
Endotoxin signalling
Bacterial derived toxins, lipopolysaccharides (LPS) from gram negative bacteria, and peptidoglycan/lipopeptides from gram positive bacteria, when bound to toll-like receptors (TLRs), which are specific pattern recognition receptors for pathogen derived substances on mammalian cells, can orchestrate other cosignalling molecules to release cytokines. This process involves other receptors and kinases, as well as the mitogen activated protein kinase (MAP kinase) and nuclear factor κB (NFκB) pathways (fig 1). Cytokines then cause cell influx and oxidant stress, affecting target molecules such as lipids, proteins, and DNA; ultimately tissue injury ensues.7

Pathogenesis of sepsis: endotoxin signalling pathway. IL, interleukin, LPS, lipopolysaccharides, LP, lipopeptides, MAP-k, mitogen activated protein kinase, NFκB, nuclear factor κB; PGN, peptidoglycan; TLR, toll-like receptors; TNF-α, tumour necrosis factor α. Flash points represent changes that occur in cirrhosis that make them more susceptible to the development of infection.
Physiological and biochemical changes
Cytokine release during sepsis results in profound physiological changes in the host, including fever, tachycardia, tachypnoea, hypotension, and microcirculatory alterations. Red cell deformability is altered and they become wedged in the pulmonary microcirculation, sludge, and decrease blood flow in an attempt to wall off bacteria and limit ongoing proliferation. Microvascular pooling results, with up to 30% decrease in the macrovascular volume lost to the microcirculation. Furthermore, vascular resistance changes markedly reduce splanchnic blood flow and send an inordinate amount of cardiac output to the skin and resting skeletal muscle. Eventually, blood flow stagnation and poor oxygenation result in endothelial apoptosis and necrosis, setting off the beginning of coagulopathy, via tissue factor induced activation of the extrinsic coagulation pathway (fig 2). Moreover, thrombin activates endothelial cells which induce leucocyte recruitment, a mechanism that plays a central role in sepsis induced tissue inflammation and injury.8
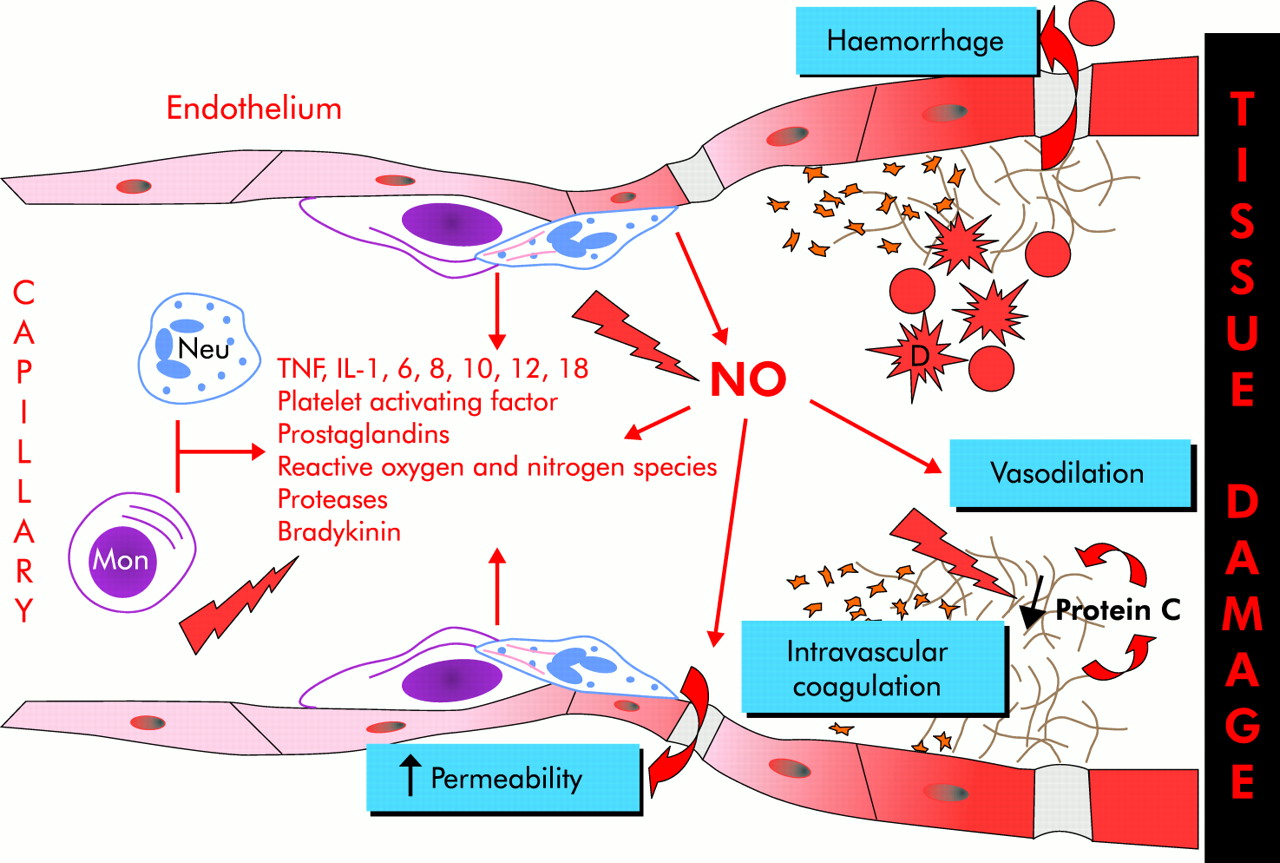
Pathogenesis of sepsis: changes in the circulation during sepsis. D, deformed red blood cells; IL, interleukin; mon, monocytes; neu, neutrophil; NO, nitric oxide; TNF-α, tumour necrosis factor α. Flash points represent changes that occur in cirrhosis that make them more susceptible to the development of infection.
Protein C
Activated protein C has been shown in vitro to induce “protective” (anti-inflammatory and antiapoptotic) genes in endothelial cells.9 Thus reduced protein C activation during sepsis may contribute to enhanced procoagulant and proinflammatory responses (fig 2).10 Indeed, non-survivors of septic illnesses have persistently reduced serum protein C below a critical level of approximately 60% of normal,11 and reconstitution of activated protein C can improve survival in patients with severe sepsis. In a landmark multicentre study12 involving over 1600 patients with infection, three SIRS criteria, evidence of acute organ dysfunction, and low protein C levels, patients who received an infusion of activated protein C for 96 hours had a significantly reduced 28 day mortality from 30.8% to 24.7%, and the relative risk of dying was reduced by 19.4% compared with placebo.
Nitric oxide
A key mediator contributing to hypotension in patients with septic shock is nitric oxide (NO). NO also exerts several beneficial effects by opposing platelet aggregation and terminating free radical chain reaction. NO excess in sepsis is produced by the inducible form of nitric oxide synthase (NOS), using arginine as a substrate and cofactors. When there is an abundance of substrate and cofactors, NOS produces NO efficiently. However, when such supplies are deficient, NOS can generate large amounts of superoxide with attendant oxidation of lipids, proteins, and DNA (fig 2). The hepatic urea cycle, which is the major non-dietary arginine source for NO synthesis, is depressed in mice with severe sepsis, which is probably also true in patients. Relative arginine deficiency contributes to NOS uncoupling, resulting in increased oxidant stress.13
SEPSIS INDUCED SYSTEMIC INFLAMMATORY RESPONSE SYNDROME IN CIRRHOSIS
Cirrhotics have increased levels of endotoxin.14–16 Similarly, plasma TNF-α and IL-6 levels were higher in cirrhotic patients with early bacterial infection than non-cirrhotic patients,17 with enhanced proinflammatory cytokine responses following LPS challenge in cirrhotic rats.18,19 Furthermore, ex vivo, LPS induced proinflammatory cytokine production by monocytes was more marked in cirrhotics than in controls.20 There is evidence that LPS induced cytokine production is mediated via upregulation of endothelin productions, as the use of a non-specific endothelin receptor, tezosentan, was associated with reduced cytokine production and less hepatic inflammation.19 More interestingly, activation of TLR-4 by LPS is related to upregulation of IL-8 and monocyte chemoattractant protein 1 expression in hepatic stellate cells, a process regulated by NFκB,21 associated with enhanced stellate cell survival, and potentially increased hepatic fibrosis. However, in a recent study by Riordan et al, the relationship between endotoxins, enterotoxins, their TLRs, and cytokine production was re-evaluated.16 While levels of endotoxins were elevated in patients with cirrhosis of all aetiologies, TLR-4 (receptors for products of Gram negative organisms) expression was not increased nor was there a correlation between endotoxin levels and TNF-α levels in these patients.16 On the contrary, peripheral blood mononuclear cell expression of TLR-2 (receptors for products of Gram positive organisms) was significantly upregulated and correlated significantly with serum TNF-α levels. These findings suggest that Gram positive microbial components, but not endotoxin, as previously assumed, mainly contribute to increased circulating levels of this cytokine in cirrhosis.
The liver synthesises precursors (zymogens) of coagulation factors, and cirrhosis is associated with decreased synthesis of the factors VII, X, V, and II. Cirrhotic patients with sepsis present greater coagulation abnormalities than their counterparts without sepsis, reflecting more severe underlying liver disease.22 The consumption of coagulation factors by sepsis induced activation of extrinsic coagulation pathway leads to a further worsening of coagulation abnormalities.
The protein C zymogen, which is also synthesised by the liver, is reduced in cirrhosis, and further decreases with severe sepsis.22 Thus failure to achieve adequate levels of activated protein C may be a mechanism contributing to the sepsis severity. To our knowledge, plasma concentrations of activated protein C have not yet been measured in cirrhotic patients. However, in patients with fulminant liver failure, protein C activity is reduced.23 This may be one of the mechanisms underlying the susceptibility of these patients to sepsis.
NO production is usually increased in cirrhosis, the highest levels being found in patients with the worse hepatic function. With bacterial infection, LPS induces NOS, especially in the liver, leading to increased production of TNF-α and nitrates.18 Plasma nitrate and nitrite concentrations, metabolites of NO, are correlated with those of endotoxins, which are also increased, suggesting a causal relationship between endotoxin levels and NO production in cirrhosis.24 The release of various cytokines and endotoxins in sepsis further enhances NO production, which mediates some of the damaging effects of infection by reacting with superoxides to form reactive oxygen species. These species bind irreversibly to multiple components of the mitochondrial respiratory chain, affecting cell respiration and precipitating cell necrosis.25 Indeed, in an animal model of cirrhosis, there was increased formation of S-nitrosothiols, the circulating form of NO during endotoxaemia.26 S-nitrosothiols are potent inhibitors of platelet aggregation, and this may be one of the explanations why infection is associated with an increased risk of variceal bleeds in cirrhosis.27
BACTERIAL TRANSLOCATION AND ITS ROLE IN THE PATHOGENESIS OF SEPSIS SYNDROME IN CIRRHOSIS
Intestinal bacterial translocation is defined as the migration of viable microorganisms from the intestinal lumen to mesenteric lymph nodes and other extraintestinal sites. In cirrhotic patients, bacterial translocation was significantly increased only in Child C patients in whom the rate was 30% compared with 8% in Child B and 3% in Child A patients.28 In fact, the only independent predictor of translocation was Child-Pugh class, and this is consistent with similar results from experimental cirrhosis29 and can be attributed to the more immunocompromised state of these patients. Although bacterial translocation is not the only source of sepsis in cirrhosis, it is an important route of entry of bacteria into the cirrhotic host. Enteric bacteria and their products such as endotoxins reach the blood stream from the mesenteric lymph nodes and whence dissemination into other organs occurs.
Bacterial translocation becomes clinically significant when it produces recognisable conditions such as spontaneous bacterial peritonitis (SBP), bacteraemia, or post surgical infection. It contributes to the morbidity and mortality of the sepsis syndrome by further deteriorating the circulatory disturbance in cirrhosis. Ascitic cirrhotic animals with bacterial translocation, when given the potent vasoconstrictor methoxamine, showed impaired contractility of their mesenteric arterial bed,30 compared with their counterparts without translocation. These haemodynamic abnormalities were closely related to increased production of TNF-α and endothelial NO. Treatment with an NO inhibitor almost abolished hyporeactivity to methoxamine, suggesting that the effects of bacterial translocation manifest via excessive NO production.
CLINICAL ASPECTS AND CONTROVERSIES ON THE MANAGEMENT OF SEPSIS IN CIRRHOSIS
Gastrointestinal bleeds
The high incidence of infection, particularly SBP, in patients with variceal bleeding has long being recognised.31 A subsequent prospective study confirmed the high frequency of infection in patients with variceal bleeds, and found that infection predicted variceal rebleeding.32 In a retrospective study, antibiotic therapy and proven bacterial infection were the only factors independently predicting failure to control bleeding.27 Conversely, in patients with controlled bleeding, the incidence of sepsis was significantly lower versus those with uncontrolled bleeding,32 a finding confirmed in further studies.33,34
Infection may favour variceal bleeding by increasing sinusoidal pressure and altering haemostasis. In fact, endotoxaemia stimulates endothelin production, which activates sinusoidal stellate cell contraction. Sinusoidal pressure increases, significantly enhancing the risk of variceal bleeding.34 Endotoxins also stimulate endothelial NO production, leading to abnormal platelet aggregation and primary haemostasis failure.33 Moreover, infected cirrhotic patients show increased amounts of heparin-like substances (heparinoids) which disappear once infection resolves.34 Bacterial infection could stimulate endothelial cells to release heparinoids. This, coupled with their reduced clearance by the liver and increased tissue plasminogen activator production, further impairs coagulation.
Pragmatically, it is recommended that patients with gastrointestinal bleeding be given antibiotic prophylaxis35 (level of evidence = I ACE). Recently, a randomised controlled trial showed that the use of prophylactic antibiotics as secondary prevention of variceal bleeding can reduce the incidence of early rebleeding, especially in the first seven days after the index bleed36 (fig 3) (level of evidence = II DE). None the less, reducing the risk of sepsis may be one of the beneficial effects of prophylactic treatment with beta blockers which reduce bacterial translocation in cirrhotic rats37 (level of evidence = II D).

Incidence, risk factors, and complications of bacterial infections within seven days from variceal bleeding (blue area), and the improvement following antibiotic prophylaxis (red area).
Spontaneous bacterial peritonitis
Early diagnosis and prompt treatment with effective antibiotics significantly improves the prognosis of this complication. The recommended treatment is a third generation cephalosporin given intravenously for five days. The most commonly used is cefotaxime, up to 4 g/day in 2–4 divided doses because of its efficacy and safety.38 Repeat diagnostic paracentesis to document response by a greater than 25% decrease in ascitic fluid neutrophil count at 48 hours after commencement of antibiotic is recommended. With this regimen, recovery from SBP is higher than 80–90% and 30 day survival is at least 80%.38 Patients should receive secondary prophylaxis with a quinolone such as oral norfloxacin 400 mg/day, and be assessed for liver transplantation38 (level of evidence = I ACE) (table 3).
Treatment of spontaneous bacterial peritonitis (SBP) in cirrhosis
Alternatively, ciprofloxacin, whether given for seven days intravenously or firstly for two days intravenously and then five days orally, results in a similar SBP resolution rate and hospital survival compared with cefotaxime, but with a significantly higher cost.39 Amoxicillin/clavulanic acid, first given intravenously then orally, also gave similar SBP resolution and hospital mortality rates compared with cefotaxime40 and with a much lower cost. For patients developing SBP while on norfloxacin prophylaxis, the response to amoxicillin/clavulanic acid was slightly better. Finally, oral therapy with ofloxacin has given similar results as intravenous cefotaxime in uncomplicated SBP, without renal failure, hepatic encephalopathy, gastrointestinal bleed, ileus, or shock.41
Treatment failure (10%) is associated with a poor prognosis and hospital mortality of 50–80%.42 Antibiotic should be changed according to in vitro susceptibility or empirically in culture negative cases.38 Secondary bacterial peritonitis should be sought for, and surgery may be necessary.38 Treatment failure may be related to the change in the profile of infecting bacteria in the past 10 years (see section “Antibiotic prophylaxis and antibiotic resistance” below).
Use of albumin in the treatment of SBP
The physiological effects of albumin infusions are threefold: (i) albumin can bind and then deliver toxins to removal sites, (ii) albumin can increase the protein concentration of extracellular compartments such as ascites, improving opsonic activity, and (iii) blood volume expansion. To date, there are no reports on the effects of albumin on toxin removal. Long term albumin infusions lead to protein redistribution into extravascular sites such as ascites. However, it is doubtful that this is significant in short term infusions. Thus albumin improves haemodynamics mainly by blood volume expansion.
SBP carries the risk of further deterioration of haemodynamic renal insufficiency from additional splanchnic vasodilatation, which is magnified by baseline renal insufficiency.43 The development of renal failure (creatinine value >2.1 mg%) is the most important indicator of reduced patient survival in SBP.44 In the only study assessing the effect of albumin infusion on renal function and survival in SBP, 126 patients were randomised to receive either cefotaxime or cefotaxime with albumin.45 Albumin was given at a dose of 1.5 g/kg body weight within six hours of SBP diagnosis, followed by 1 g/kg on day 3. This resulted in a large albumin infusion of 105 g on day 1 and 70 g on day 3 in a 70 kg patient. Albumin infusions prevented the rise in renin, decreased the incidence of renal failure, and improved mortality from 29% to 10% compared with cefotaxime alone (level of evidence = II ADE). Interestingly, baseline elevation in blood urea nitrogen (BUN) predicted a further increase in renin and renal deterioration after SBP. The renin rise was prevented by albumin in patients with baseline BUN elevation, who also received the greatest benefit in terms of renal dysfunction and mortality. It is unclear whether albumin infusions were necessary in patients with normal baseline BUN, bilirubin <4 mg/dl, or protime >60% of control, as their mortality rate was only 4% without albumin versus 0% with albumin. Furthermore, those patients who did not receive albumin did not receive any other fluid support. It is not clear at present whether fluid support with crystalloids or other colloids would have produced the same results. This underscores the need for further studies to assess the efficacy of albumin in the management of SBP. Until further trials are completed, albumin infusion seems a valuable adjunction in the treatment of SBP.
Antibiotic prophylaxis and antibiotic resistance
Prophylactic antibiotics are usually oral non- or poorly absorbable antibiotics which selectively eliminate aerobic Gram negative bacilli from the intestinal flora while preserving aerobic and anaerobic bacteria. The rationale for their use is the fact that aerobic Gram negative bacilli are mostly responsible for infections in cirrhosis. Moreover, quinolones per se may have immunoregulatory functions, stimulating the bactericidal capacity of polymorphonuclear cells or decreasing bacterial adhesion to mucosal surfaces.46 The current indications for antibiotic prophylaxis in cirrhosis are gastrointestinal haemorrhage35 (level of evidence = I ACE), irrespective of the presence of ascites, and a past history of SBP47 (level of evidence = I ACE) (table 4). Norfloxacin, ciprofloxacin, and trimethoprim/sulfamethoxazole have all been used with these indications with good results. A benefit from antibiotic prophylaxis in cirrhosis with ascites but no previous SBP has not been demonstrated and cannot be recommended. However, a low ascitic fluid protein count of <10 g/dl and poor hepatic function identify a subset of patients who are at high risk for developing SBP and therefore may benefit from prophylaxis47 (level of evidence = III D).
Studies on antibiotic prophylaxis for gastroenterology haemorrhage
Prolonged antibiotic prophylaxis has led to the emergence of quinolone resistant bacteria. In a recent survey, 26% of SBP episodes were caused by quinolone resistant Gram negative bacilli over a two year period,2 related to long term treatment with norfloxacin: 50% of culture positive SBP in patients on prophylaxis was due to such microorganisms versus 16% in patients not receiving prophylaxis. Long term norfloxacin was also associated with a high rate (44%) of culture positive SBP caused by trimethoprim/sulfamethoxazole resistant Gram negative bacteria, suggesting that this antibiotic is not an alternative to norfloxacin. Fortunately, quinolone resistant E coli are still sensitive to third generation cephalosporins. In addition, there is an increased likelihood of infections from Gram positive bacteria in patients who have received SBP prophylaxis (fig 4).48 In a recent study, the relative prevalence of infections from Gram positive bacteria in patients who received norfloxacin prophylaxis was substantially increased; in particular, bacteraemia was entirely due to Gram positive bacteria (fig 4).48 This underlines the need to restrict the use of prophylactic antibiotics to patients with the greatest risk of SBP.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevalence and type of severe hospital acquired bacterial infections in patients with cirrhosis who either did or did not receive norfloxacin prophylaxis. BE, bacteraemia; SBP, spontaneous bacterial peritonitis; Px+, prophylactic norfloxacin; Px−, no prophylactic norfloxacin. *Significantly different from Px−.
Alternative SBP prophylaxis such as prokinetic agents can reduce the incidence of bacterial overgrowth and translocation in cirrhotic rats.49 Lactobacilli constitute an integral part of the normal gastrointestinal microecology and can inhibit the growth of various potentially pathogenic bacteria, stimulate host immunity, increase host resistance against infection, activate liver and peritoneal macrophages, and enhance intestinal immune function.50 However, no significant difference either in bacterial overgrowth or bacterial translocation was documented between patients receiving lactobacilli prophylaxis and those who did not.51 Addition of antioxidants to the lactobacilli seems to hold promise in preventing bacterial translocation. Finally, non-selective beta blockers can also reduce the incidence of intestinal bacterial overgrowth and translocation in cirrhotic rats with ascites.37
Key messages
-
Infections are common in cirrhosis, especially in ascites, lungs, urinary tract, and blood. Clinicians should have a high index of suspicion for infection when cirrhotic patients are unwell or present with non-specific symptoms.
-
Circulatory changes, increased cytokine production, activation of coagulation pathway, reduced protein C production, and increased bacterial translocation favour the development of sepsis in cirrhosis.
-
Bacterial infections are common in cirrhotic patients with variceal bleeds. Conversely, the presence of infection may favour variceal bleeding by increasing sinusoidal pressure and altering haemostasis. Prophylactic antibiotics are therefore recommended in cirrhotic patients with variceal bleeding.
-
Prompt treatment of spontaneous bacterial peritonitis with a third generation cephalosporin can significantly reduce morbidity and improve survival.
-
The use of albumin with cephotaxime in the treatment of spontaneous bacterial peritonitis has been shown in one study to reduce the incidence of renal failure as a complication in patients who have pre-existing renal failure, and decrease mortality. It is not clear at present whether fluid support with crystalloids or other colloids would have produced the same results.
-
Secondary prophylaxis of spontaneous bacterial peritonitis has led to a significant reduction of recurrence due to Gram negative organisms but associated with a substantial rise in infections due to Gram positive organisms.
-
New treatments that have shown some effects for the management of sepsis in cirrhosis include the use of probiotics, non-selective beta blockers, and prokinetic agents.
There are several trials in post liver transplant patients suggesting the prophylactic use of selective intestinal decontamination as a means of reducing the incidence of sepsis postoperatively.52,53 Although the overall results seem to favour the use of selective intestinal decontamination, the latest study suggests that this also favours the development of infections caused by Gram positive organisms and fungi.53 Therefore, careful consideration needs to be given before widespread use of selective intestinal decontamination can be recommended. Likewise, the widespread use of antibiotic prophylaxis in the non-transplant setting cannot be encouraged as this may promote antibiotic resistance with disastrous consequences.
SUMMARY
There have been significant strides in the understanding of the pathophysiology of sepsis in cirrhosis. Prophylactic treatment with a quinolone antibiotic such as norfloxacin for up to seven days in patients with acute gastrointestinal bleed has been shown to decrease the incidence of infection and improve patient survival.35 Early diagnosis and treatment of SBP with a third generation cephalosporin for five days means that 80% of them will survive for at least 30 days.8 It is not clear at present whether the use of albumin is better than other colloids or crystalloids in preventing renal impairment complicating SBP. Preliminary evidence suggests that albumin may be useful in reducing the development of hepatorenal syndrome in those with pre-existing high BUN levels.45 Lifelong secondary antibiotic prophylaxis with a quinolone will further improve their prognosis. All of these measures against infections mean that cirrhotic patients now have a much better prognosis. However, one cannot become complacent, as pathogenic organisms are continuously developing antibiotic resistance, and every effort is warranted to identify newer forms of prophylaxis and treatment.
APPENDIX
Level of evidence is rated according to recommendations given by the Practice Guidelines Committee of the American Association for the Study of Liver Diseases. The letters A through E determine the strength of the recommendation and roman numerals, I through III, determine quality of evidence upon which recommendations are based, as follows: A, survival benefit; B, improved diagnosis; C, improvement in quality of life; D, relevant pathophysiological parameters improved; E, impacts cost of health care; I, evidence from multiple well designed randomised controlled trials, each involving a number of participants to be of sufficient statistical power; II, evidence from at least one large well designed clinical trial with or without randomisation from cohort or case control analytic studies or from well designed meta-analysis; III, evidence based on clinical experience, descriptive studies, or reports of expert committees; and IV, not rated.
Acknowledgments
The authors and the International Ascites Club would like to thank Grifols International, Barcelona Division, Spain, and Roche USA for sponsoring the 7th Meeting of the International Club, Sepsis in Cirrhosis.
REFERENCES
Footnotes
-
Conflict of interest: None declared.