Article Text

Statistics from Altmetric.com
Clinical presentation
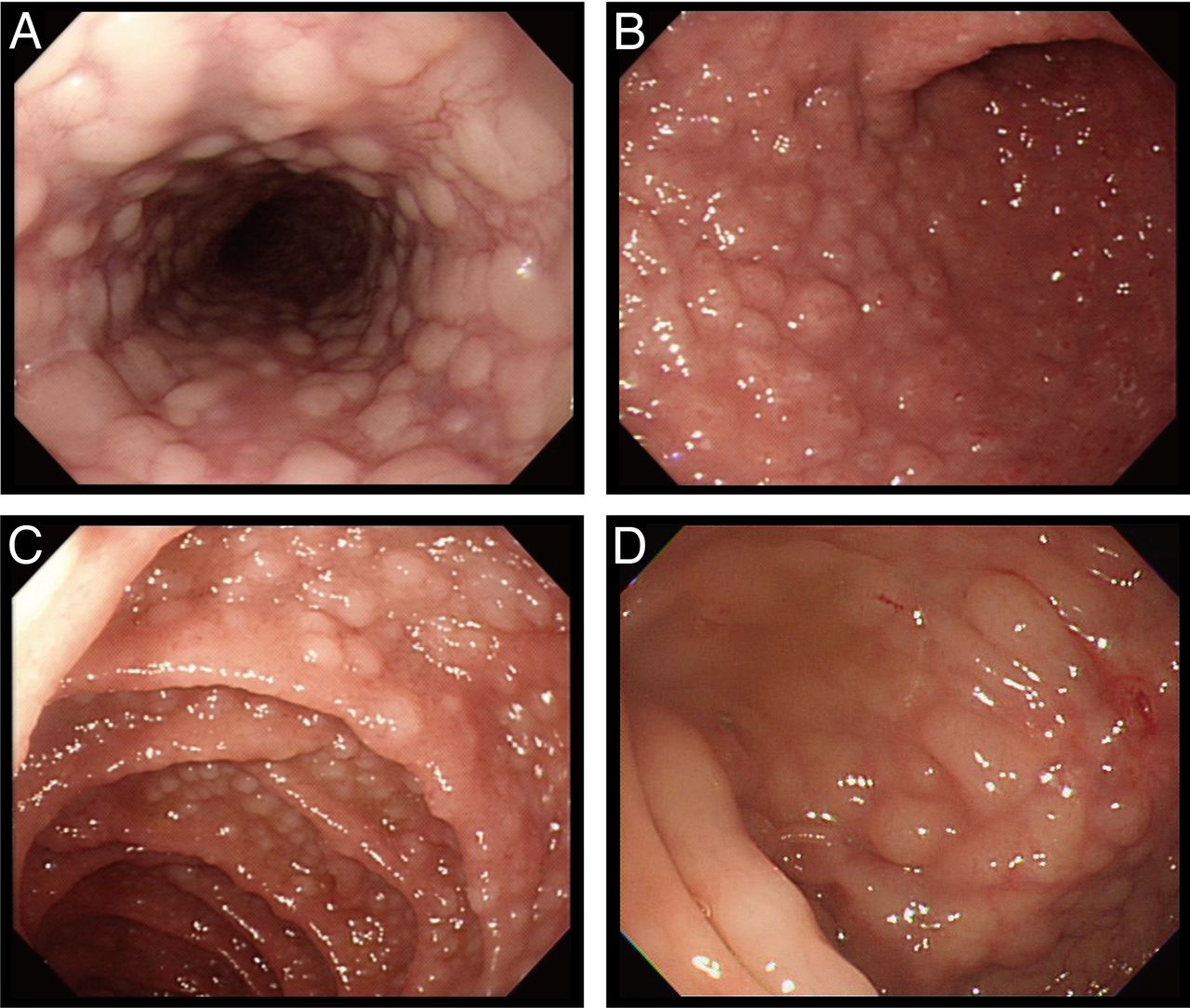
A 73-year-old man presented with abdominal fullness for 2 months. He had lost 5 kg in the previous 2 months. He did not have fever or abdominal pain. He had a history of chronic hepatitis B. Physical examination showed enlarged lymph nodes over bilateral neck, axillary and inguinal areas. Laboratory study revealed leucocytosis with white cell counts 14.1×109/L; haemoglobin level 12.8 g/dL; platelet count 227×109/L; hypoalbuminaemia with albumin level 2.8 g/dL, as well as normal blood sugar, aminotransferase, urea, creatine, serum uric acid and lactic acid dehydrogenase levels. Tumour markers carcinoembryonic antigen, carbohydrate antigen 19–9 and alpha-fetoprotein were all within normal limits. The upper GI panendoscopy showed multiple whitish sessile polypoid lesions over the whole circumference of oesophagus, extending form upper third to the gastro-oesophageal junction (figure 1A). Enlarged gastric rugae with polypoid lesions were seen from the fundus to the body of the stomach, and numerous erosive lesions were noted on the gastric antrum (figure 1B). Various sizes of polypoid lesions were also seen in the bulb and second portion of duodenum (figure 1C). Colonoscopy showed multiple polypoid lesions with shallow ulcerations scattered from the rectum to caecum (figure 1D).

Multiple sessile polypoid lesions were seen in the oesophagus (A), stomach (B), duodenum (C) and colon (D).
Question
What is the diagnosis?
Answer
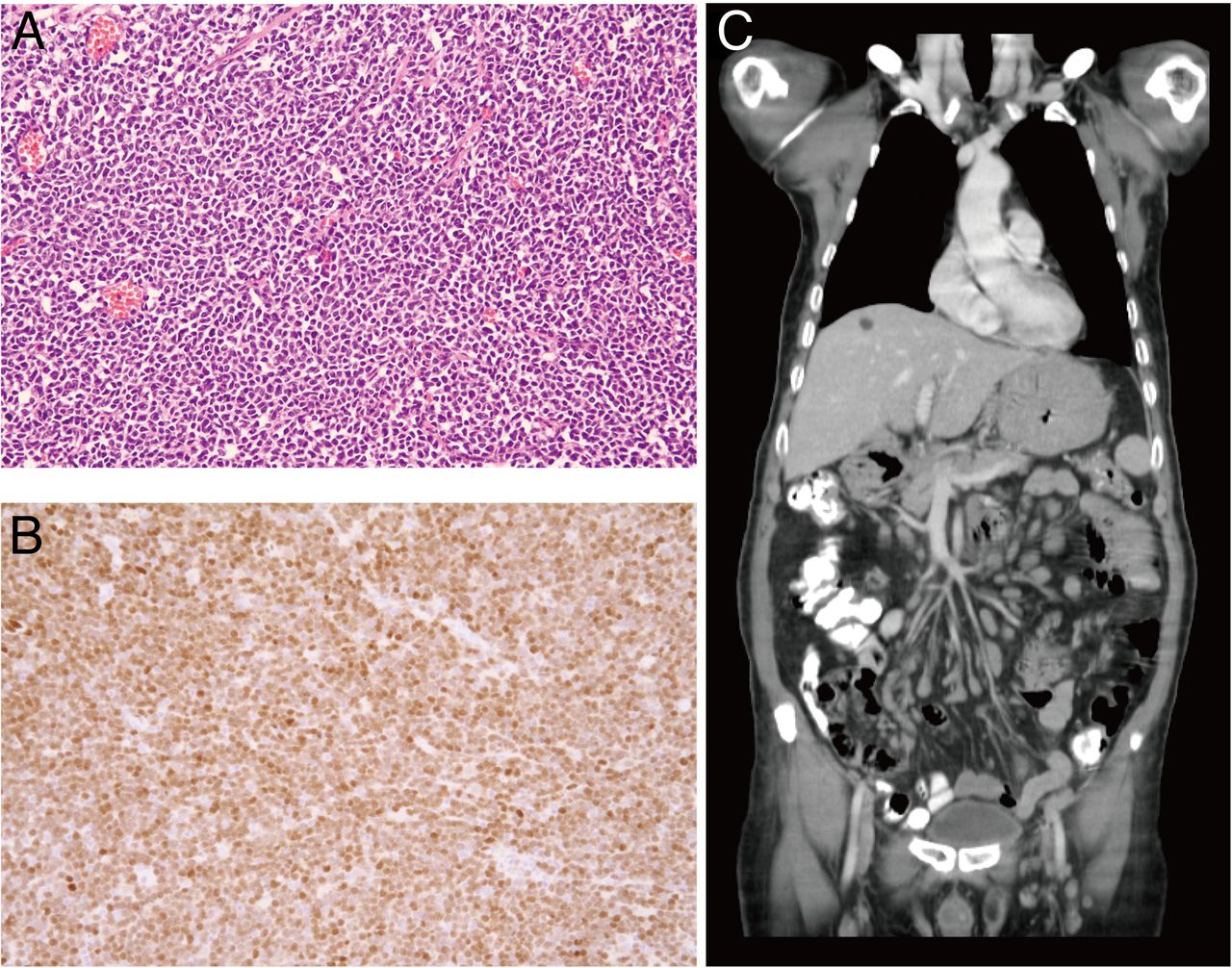
Histopathology of the oesophagus, stomach, duodenum and colon specimens revealed dense infiltration of monotonous atypical lymphoid cells (figure 2A). Immunohistochemical staining showed positive reaction for CD5, CD20 and cyclin D1 (figure 2B), but negative reaction for CD3 and CD10. The Ki-67 proliferative index was 70%. These histopathological findings suggest mantle cell lymphoma (MCL). CT scan revealed multiple enlarged lymph nodes in the neck, mediastinum, mesenteric, para-aortic space, and wall thickening at the stomach and colon (figure 2C). Bone marrow examination disclosed the finding of lymphoma cell involvement. Fluorescence in situ hybridisation testing showed chromosome translocation t (11;14) (q13;q32). The patient received the regimen of combination chemotherapy with bendamustine and rituximab. Follow-up CT scan and endoscopy revealed regression of the GI lesions (figure 3) and lymphadenopathy.
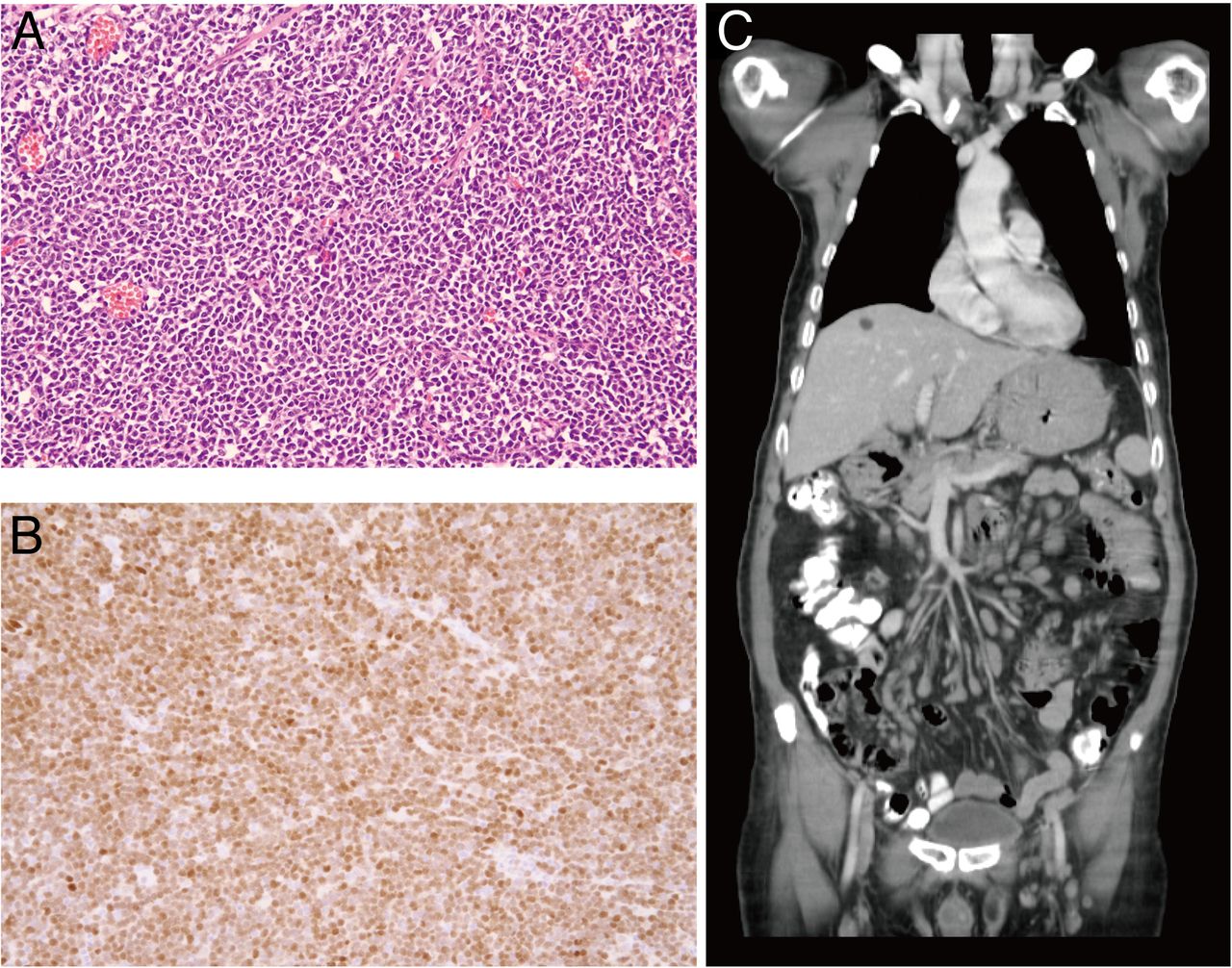
(A) Histopathology of the duodenum revealed a picture of a dense infiltration of monotonous atypical lymphoid cells (H&E stain 400×). (B) Immunohistochemical stains showed positive reaction for cyclin D1. (C) The coronal view of abdominal CT showed multiple enlarged lymph nodes at mesenteric area, thickening of gastric wall and a cyst in the right lobe of liver.

{kind=link}
{kind=link}
{kind=link}
After chemotherapy, follow-up endoscopy showed regression of the polypoid lesions in the oesophagus (A), stomach (B), duodenum (C) and colon (D).
The oesophagus, stomach, duodenum and colon are involved in 5.7%, 74.3%–77%, 34.3%–77% and 57%–77% of patients with MCL, respectively.1 ,2 But, no reported case of whole GI tract involvement exists in patients with MCL. Nowadays, no gold-standard therapy is recommended for the treatment of MCL. A combination of bendamustine plus rituximab regimens provides 75% overall response rate in patients with MCL.3
Footnotes
Contributors P-JH: collecting clinical specimens and drafting the manuscript C-LC: interpretation of data and drafting the manuscript. F-MS: inform consent, interpretation of data and drafting the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.