Article Text

Statistics from Altmetric.com
- Cirrhosis
- ascites
- portal hypertension
- bacterial overgrowth
- bacterial translocation
- portal hypertension
- gastrointestinal haemorrhage
- intestinal bacteria
- bacterial translocation
- liver cirrhosis
Background
Cirrhosis is one of the most frequent and severe chronic diseases worldwide. In the initial stages it has few or no symptoms, but advanced stages of cirrhosis are characterised by reduced liver function, complications due to portal hypertension and neuroendocrine abnormalities with increased activity of the sympathetic nervous system (SNS) and renin-aldosterone axis. The prognosis is severe, with an increasing frequency of complications including variceal bleeding, ascites and spontaneous infections with subsequent development of hepatic encephalopathy and hepatorenal syndrome. More than one-third of patients diagnosed with cirrhosis develop oesophageal varices within 3 years after the diagnosis is made. Varices develop and later bleed when the portal pressure is increased and the hepatic vein pressure gradient (HVPG) is more than 10–12 mm Hg. Life-threatening spontaneous bacterial infections are another common complication of advanced cirrhosis. The infections are mainly triggered by gut bacterial translocation, which is the migration of microorganisms from the intestinal lumen to the mesenteric lymph nodes or other extraintestinal sites.1 Small intestinal bacterial overgrowth of Gram-negative rods, structural and functional alterations of the intestinal mucosa and deficiencies in defence mechanisms contribute to bacterial translocation.2 Increased serum levels of lipopolysaccharide binding protein and circulating bacterial DNA are markers of bacterial translocation and both predict a poor outcome in cirrhosis and ascites.3 4 Selective gut decontamination prevents spontaneous bacterial infections and improves survival in advanced cirrhosis.5
Non-selective β-blockers (BB) are the only drugs shown to improve survival in patients with cirrhosis and medium to large oesophageal varices.6 BB inhibit the binding of catecholamines (norepinephrine and epinephrine) to the β1 and β2 adrenoreceptors. β1 blockade reduces the cardiac output and β2 blockade leads to splanchnic vasoconstriction. The combined inhibition of β1 and β2 adrenoreceptors is necessary to achieve a sufficient reduction in portal pressure. The benefit of BB has been attributed to portal pressure reduction which decreases the risk of variceal bleeding as well as other complications of portal hypertension.7–10 There is increasing evidence to suggest that BB also have non-haemodynamic effects and that they may be ineffective in early cirrhosis and may be detrimental in certain patients with end-stage cirrhosis.11–13 In the present paper we propose that the benefit of BB is related both to haemodynamic and non-haemodynamic effects during a window in the cirrhotic disease. Outside the therapeutic window, BB may be ineffective or even have detrimental effects.11–13
Non-haemodynamic effects of BB
Clinical evidence
To assess a possible beneficial effect of BB in cirrhosis beyond the reduced risk of variceal bleeding, we performed a meta-analysis of eight randomised trials with 970 patients comparing BB and isosorbide mononitrate (IsMn) with banding ligation for patients with oesophageal varices and previous variceal bleeding.14 The mean dose of BB was 48–120 mg/day and the mean dose of IsMn was 30–60 mg/day. In total, 98 of 480 patients randomised to BB and IsMn and 121 of 490 patients randomised to banding ligation died. Thus, BB and IsMn reduced mortality compared with banding ligation (RR 0.78, 95% CI 0.64 to 0.96). There were no apparent differences between treatment groups in the risk of upper gastrointestinal bleeding (RR 1.15, 95% CI 0.81 to 1.63), variceal rebleeding (RR 1.23, 95% CI 0.74 to 2.06) or bleeding-related mortality (RR 0.75, 95% CI 0.37 to 1.50). These findings suggest that the reduced mortality did not reflect reduced bleeding rates. Additional effects that are not related to the risk of variceal bleeding may exist. The data in the meta-analysis did not allow for an assessment of the reasons for the survival benefit. However, a meta-analysis of randomised trials and observational studies found that BB may reduce the risk of spontaneous bacterial peritonitis,8 an effect that was independent of the portal pressure response to BB.
Experimental evidence
In the early stages of cirrhosis the activity of the SNS is close to normal levels. SNS activity increases with the severity of cirrhosis. In end-stage cirrhosis the SNS is highly active. Fibres from the SNS terminate in blood vessels, gut-associated lymphatic tissue and the intestinal mucosa. The level of norepinephrine increases with the activity of the SNS. In the intestinal lumen, norepinephrine is absorbed by gut bacteria resulting in an increased growth of Escherichia coli and other Gram-negative bacteria.15 16 The absorption also increases the bacterial virulence and ability to adhere to the gut mucosa.15 16 The increased norepinephrine levels are also known to decrease the intestinal transit time, impair the mucosal barrier function and inhibit chemotaxis and phagocytosis.17 In experimental cirrhosis, splanchnic sympathectomy and BB reduce the rate of spontaneous bacterial translocation and migration of E coli to the peritoneal cavity and the bloodstream.18 19
The therapeutic window of BB
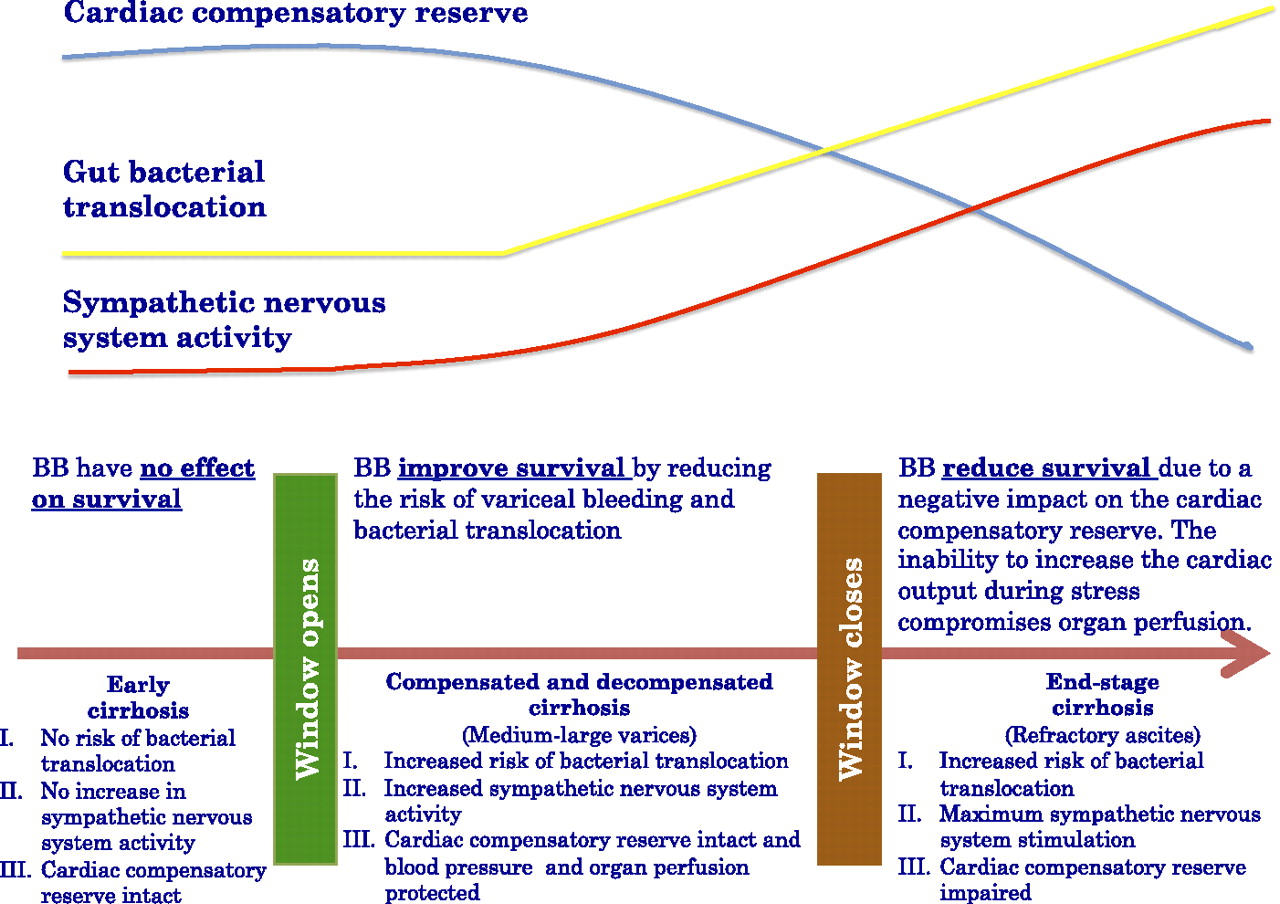
We hypothesise that BB improve survival in cirrhosis during a certain window in the disease (figure 1).
{kind=link}
Hypothesis of the therapeutic window for non-selective β-blockers (BB) in cirrhosis.
When does the window open?
BB have no clear effects in early cirrhosis without varices or ascites.13 At this stage of cirrhosis the portal pressure is increased but has not reached the threshold value of 10 mm Hg. The SNS is not substantially activated and the splanchnic blood flow is normal. Clinical trials have not found beneficial effects of BB on clinical end-points (ie, complications of portal hypertension or death) in this patient group.13 Indeed, BB fail to reduce portal pressure in patients with an HVPG <10 mm Hg.20
As the portal pressure increases the SNS becomes increasingly activated and gut bacterial translocation and splanchnic hyperaemia occur.21 Medium to large oesophageal varices and ascites develop. The current treatment recommendations specify that BB should not be used before medium to large oesophageal varices are developed. The experimental evidence suggests that the non-haemodynamic effects begin when gut bacterial translocation is seen at the stage of decompensated cirrhosis with ascites. Pathological gut bacterial translocation does not occur in experimental cirrhosis until ascites appears.19 22 In observational studies, bacterial translocation is seen in patients with advanced (Child C) cirrhosis but not in those with earlier stages of the disease (Child A–B).23 The exact time when the therapeutic window opens may be debated. The question may be answered in an ongoing multicentre randomised controlled trial (NCT01059396) which is being conducted to assess whether BB decrease the risk of decompensation in patients with compensated cirrhosis and portal hypertension with an HVPG >10 mm Hg.
When does the window close?
End-stage cirrhosis is associated with pronounced circulatory changes and high SNS activity. Both aspects may influence the upper limit of the therapeutic window.
In end-stage cirrhosis the circulatory changes are related to the cardiac output, which is increased to preserve blood pressure and organ perfusion due to the peripheral vasodilation. The result is a gradual decrease in the cardiac compensatory reserve. Maintenance of an increased cardiac output improves survival.24 25 Conversely, a fall in the cardiac output is associated with the development of hepatorenal syndrome and has a negative impact on survival.24 26 BB are cardio-inhibitory and reduce the cardiac output and the cardiac compensatory reserve.
Patients with refractory ascites have increased levels of proinflammatory cytokines in the splanchnic compartment. Chronic inflammation may induce a β to α adrenergic shift with a reduced expression of β-adrenergic receptors and loss of sympathetic nerve fibres.27 The effects of BB are thereby diminished.
The combined evidence suggests that the beneficial effects of BB are lost in end-stage cirrhosis (figure 1). In theory, BB may have detrimental effects in end-stage cirrhosis due to their negative effect on the cardiac compensatory reserve. An observational study found that BB may decrease survival in advanced cirrhosis with refractory ascites.11 The patients in the study were not randomised to receive BB. Confounding by indication may influence the overall results. Since the choice to treat the included patients with BB may reflect underlying prognostic factors (known and unknown), the evidence does not allow for clear treatment recommendations. However, we believe that high doses of BB need to be used with great care or perhaps avoided in patients with refractory ascites.
Suggestions for future research
Additional evidence is needed to determine the non-haemodynamic effects of BB and the therapeutic window for them. However, performing trials or studies to test these questions is very difficult. At present we have no reliable methods to test the effects of BB on the SNS activity in the splanchnic compartment. The plasma concentrations of norepinephrine are unreliable because they depend on the release rate and clearance from the plasma pool and because post-synaptic concentrations may be up to 1000 times higher than plasma levels. In theory, the non-haemodynamic effects of BB may be identified in large multicentre multinational randomised controlled trials comparing BB with placebo. One potential outcome measure could be spontaneous bacterial peritonitis, which is a clinical marker of gut bacterial translocation. The trial would have to include patients with ascites but exclude those with medium to large varices for ethical reasons. Considering that several patients have contraindications to BB or decline participation, the number of patients to be screened would be considerable. Alternatively, it would be possible to use surrogate markers of bacterial translocation such as increased serum lipopolysaccharide binding protein or circulating fragments of bacterial DNA as outcome measures.3 4
Conventional echocardiography is not useful for assessing the cardiac compensatory reserve. First, it is dependent on age and the preload and afterload condition. Second, systolic dysfunction or impaired reserve is subclinical at rest and will only be clinically significant with increasing circulatory demands as seen during acute complications. This takes a cardiac stress test to unmask. This has not been studied prospectively in advanced cirrhosis and cut-off values cannot be recommended. Cardiac output in advanced cirrhosis may be influenced intrinsically due to reduced contractility or impaired chronotropic responses, but it is also highly dependent on the preload and afterload condition. Potential options include a dobutamine test or an afterload test with a loading independent echocardiography measure or MRI to assess the rise or fall in left ventricular ejection fraction, respectively.28–31 Treadmill testing is difficult in patients with advanced cirrhosis as they are often in poor shape, have muscle wasting and may also have pulmonary dysfunction.
Current evidence supports the notion that BB act in cirrhosis through haemodynamic and non-haemodynamic mechanisms in a window period of cirrhosis. The non-haemodynamic effects of BB may improve survival in a proportion of patients with cirrhosis and ascites with repeated gut bacterial translocation and no (or small) oesophageal varices. These patients are not offered BB today. Additional clinical and experimental research is needed to analyse the effects of BB in different stages of the disease and to identify valid surrogate markers for clinical outcome measures.
References
Footnotes
Funding AA is supported by grant nos PS09/00485 and PI051871 (CIBERehd) from the Spanish Ministry of Science. CIBERhed is funded by the Instituto de Salud Carlos III.
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.