Article Text

Statistics from Altmetric.com
Familial adenomatous polyposis (FAP) is one of two well described forms of hereditary colorectal cancer. The primary cause of death from this syndrome is colorectal cancer which inevitably develops usually by the fifth decade of life. Screening by genetic testing and endoscopy in concert with prophylactic surgery has significantly improved the overall survival of FAP patients. However, less well appreciated by medical providers is the second leading cause of death in FAP, duodenal adenocarcinoma. This review will discuss the clinicopathological features, management, and prevention of duodenal neoplasia in patients with familial adenomatous polyposis.
FAMILIAL ADENOMATOUS POLYPOSIS
FAP is an autosomal dominant disorder caused by a germline mutation in the adenomatous polyposis coli (APC) gene. FAP is characterised by the development of multiple (⩾100) adenomas in the colorectum. Colorectal polyposis develops by age 15 years in 50% and age 35 years in 95% of patients. The lifetime risk of colorectal carcinoma is virtually 100% if patients are not treated by colectomy.1
Patients with FAP can also develop a wide variety of extraintestinal findings. These include cutaneous lesions (lipomas, fibromas, and sebaceous and epidermoid cysts), desmoid tumours, osteomas, occult radio-opaque jaw lesions, dental abnormalities, congenital hypertrophy of the retinal pigment epithelium, and nasopharyngeal angiofibroma. In addition, FAP patients are at increased risk for several malignancies, such as hepatoblastoma, pancreatic, thyroid, biliary-tree, and brain tumours.1
Other gastrointestinal manifestations commonly found in FAP patients are duodenal adenomas, and gastric fundic gland and adenomatous polyps. Of concern, duodenal cancer is the second leading cause of death after colorectal cancer in these individuals.
EPIDEMIOLOGY OF DUODENAL POLYPS AND CANCER
After the colorectum, the duodenum is the second most commonly affected site of polyp development in FAP (fig 1).2,3 Duodenal adenomas can be found in 30–70% of FAP patients2–4 and the lifetime risk of these lesions approaches 100%.4,5

Polyps in the second part of the duodenum in a patient with familial adenomatous polyposis.
Duodenal/periampullary adenocarcinoma is the leading cause of death in FAP after colorectal cancer.6 These patients have a 100–330-fold higher risk of duodenal cancer compared with the general population.7,8 Of note, duodenal cancer is rare in the population, with an incidence of 0.01–0.04%.9 Estimates of the cumulative risk of developing duodenal cancer in FAP range from 4% at age 70 years to 10% at age 60 years.10,11 Recently, a large prospective five nation study set the cumulative incidence rate of duodenal cancer at 4.5% by age 57 years. The median age of duodenal cancer development was 52 years (range 26–58).4
UPPER GASTROINTESTINAL POLYP DISTRIBUTION AND TYPE
Polyps can be found throughout the duodenum, but the second and third portion and the periampullary region are the most commonly affected sites. This pattern probably reflects exposure of duodenal mucosa to bile acids,12 suggesting a role for these compounds in duodenal carcinogenesis.13 Most polyps in the duodenum are adenomas whereas polyps in the stomach are usually benign non-adenomatous fundic gland lesions. However, approximately 10% of gastric polyps are adenomas.3,12 Interestingly, Japanese and Korean FAP patients have a 3–4 times higher risk of gastric cancer compared with the general population14,15 whereas no increased risk has been found in Western countries.8 Besides polypoid neoplasia, flat adenomas can be found in the duodenum of approximately 30% of FAP patients and careful follow up of these lesions is recommended.16
GENOTYPE-PHENOTYPE CORRELATION IN DUODENAL POLYPOSIS
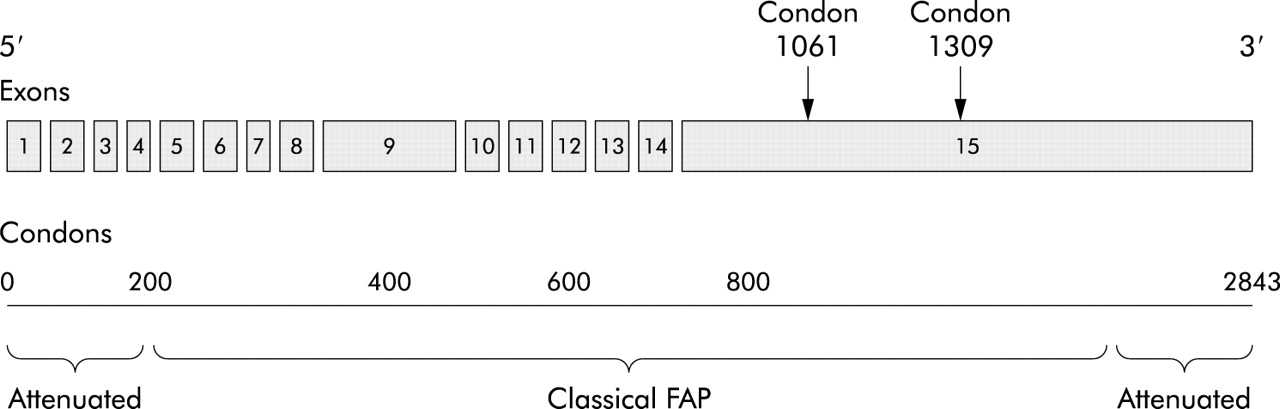
The cause of FAP is germline mutation of the APC gene. The APC gene is a tumour suppressor gene with 15 exons that encodes a 2843 amino acid protein with a molecular weight of 309 kDa. One third of all germline mutations occur in codons 1061 and 1309 (fig 2).1
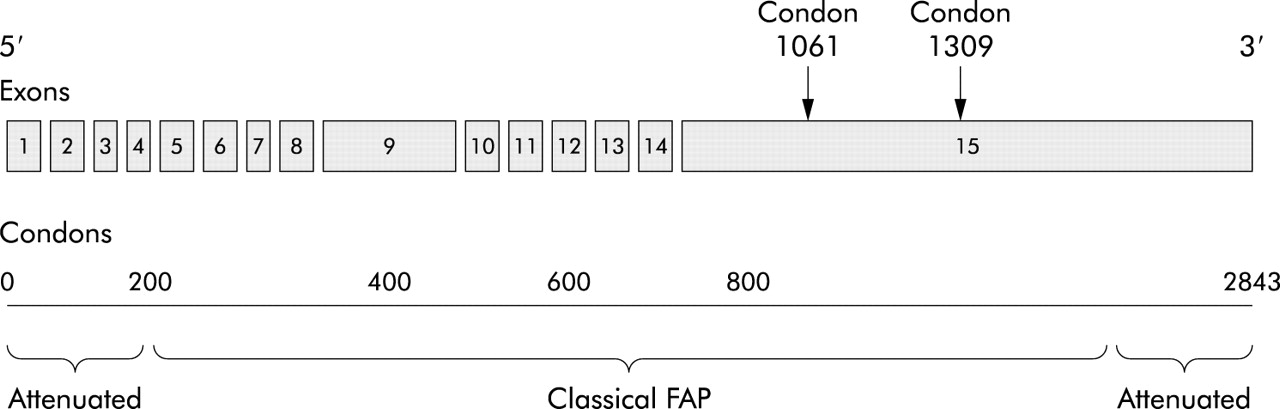
Schematic representation of the adenomatous polyposis coli (APC) gene, consisting of 15 exons and 2843 codons. One third of all germline mutations occur in codons 1061 and 1309. Mutations at the extremes of the APC gene present as attenuated familial adenomatous polyposis.
Several genotype-phenotype correlations for colonic polyposis in FAP have been established. Mutations between codon 1250 and codon 1464 are associated with profuse polyposis (>5000 colorectal polyps) and those in codon 1309 with early onset of adenoma development (10 years earlier) and colorectal cancer (age <35 years).17,18 Mutations at the 5′ and 3′ extremes of the APC gene cause attenuated FAP, characterised by oligopolyposis (less than 100 colorectal polyps) at presentation and later onset of colorectal cancer development (age >50 years).1
The relationship between severity of duodenal polyposis and mutations in the APC gene is less well understood. Taken together, published reports are inconsistent (table 1). One study failed to detect a correlation between the site of mutation and the severity of duodenal polyposis.17 In another, severe duodenal polyposis was found in patients with 5′ mutations.19 Still others correlate severe duodenal disease with mutations in the central part of the gene.20 However, most reports indicate that mutations in exon 15 of the APC gene, particularly distal to codon 1400, give rise to a severe duodenal phenotype.11,18,21–27
Genotype-phenotype correlations for upper gastrointestinal polyposis in familial adenomatous polyposis (FAP)
UPPER GASTROINTESTINAL ADENOMA-CARCINOMA SEQUENCE
The adenoma-carcinoma sequence describes colorectal carcinogenesis as a stepwise progression of normal intestinal mucosa to aberrant crypt foci, adenoma, and finally invasive carcinoma (fig 3). Activation of the Wnt signalling pathway, by biallelic inactivating APC mutation or an activating β-catenin mutation, can be regarded as the initiating step. Subsequent mutations in tumour suppressor genes (for example, p53 and SMAD4) and oncogenes (for example, K-Ras) lead to neoplastic progression of the adenoma-carcinoma sequence.28 Also, expression of important cell regulatory proteins is changed. One of these is cyclooxygenase 2 (COX-2), which is increasingly expressed in consecutive stages of the adenoma-carcinoma sequence.29,30

The adenoma-carcinoma sequence. Activation of the Wnt signalling pathway, by an inactivating adenomatous polyposis coli (APC) mutation or an activating β-catenin mutation, is regarded as the first step in the adenoma-carcinoma sequence. Then, additional mutations in oncogenes (for example, K-Ras) and tumour suppressor genes (for example, p53 and SMAD4) drive further progression of the adenoma-carcinoma sequence. COX-2, cyclooxygenase 2.
The adenoma-carcinoma sequence, first identified for colorectal tumorigenesis, has been observed in the setting of duodenal carcinogenesis in patients with both FAP and sporadic disease. Spigelman and colleagues31 found a strong association between duodenal adenomas and duodenal cancer, showing that villous histology, moderate or severe dysplasia, and the presence of stage IV duodenal polyps were associated with malignant change. Also, case reports of duodenal carcinoma development in or near adenomas have been described.32,33 Moreover, Kashiwagi et al noted p53 overexpression in 25% of tubular, 72% of tubulovillous/villous adenomas, and 100% of duodenal carcinomas,34 and K-Ras codon 12 mutations have been detected in duodenal adenomas and carcinomas.35 In addition, SMAD4 mutations play a role in polyp development in the upper intestine in mice.36 Lastly, Resnick and colleagues37 demonstrated that transforming growth factor α (TGF-α) expression was greater in duodenal carcinomas than in adenomas, and that epidermal growth factor receptor (EGF-R) expression correlated with the degree of dysplasia in duodenal adenomas. These studies reveal that additional molecular alterations drive the transition of adenoma into carcinoma.
COX-2 is known to be an important mediator of colorectal neoplasia progression but expression of COX-2 has not been extensively studied in duodenal or upper gastrointestinal adenomas. Shirvani and colleagues38 found constitutive COX-2 expression in normal duodenum and oesophagus and significantly higher levels in oesophageal dysplastic tissues. Furthermore, these investigators showed that COX-2 expression in Barrett’s oesophagus increased in response to pulses of acid or bile salts. COX-2 expression is also elevated in gastric cancers.39
CLASSIFICATION OF DUODENAL POLYPOSIS
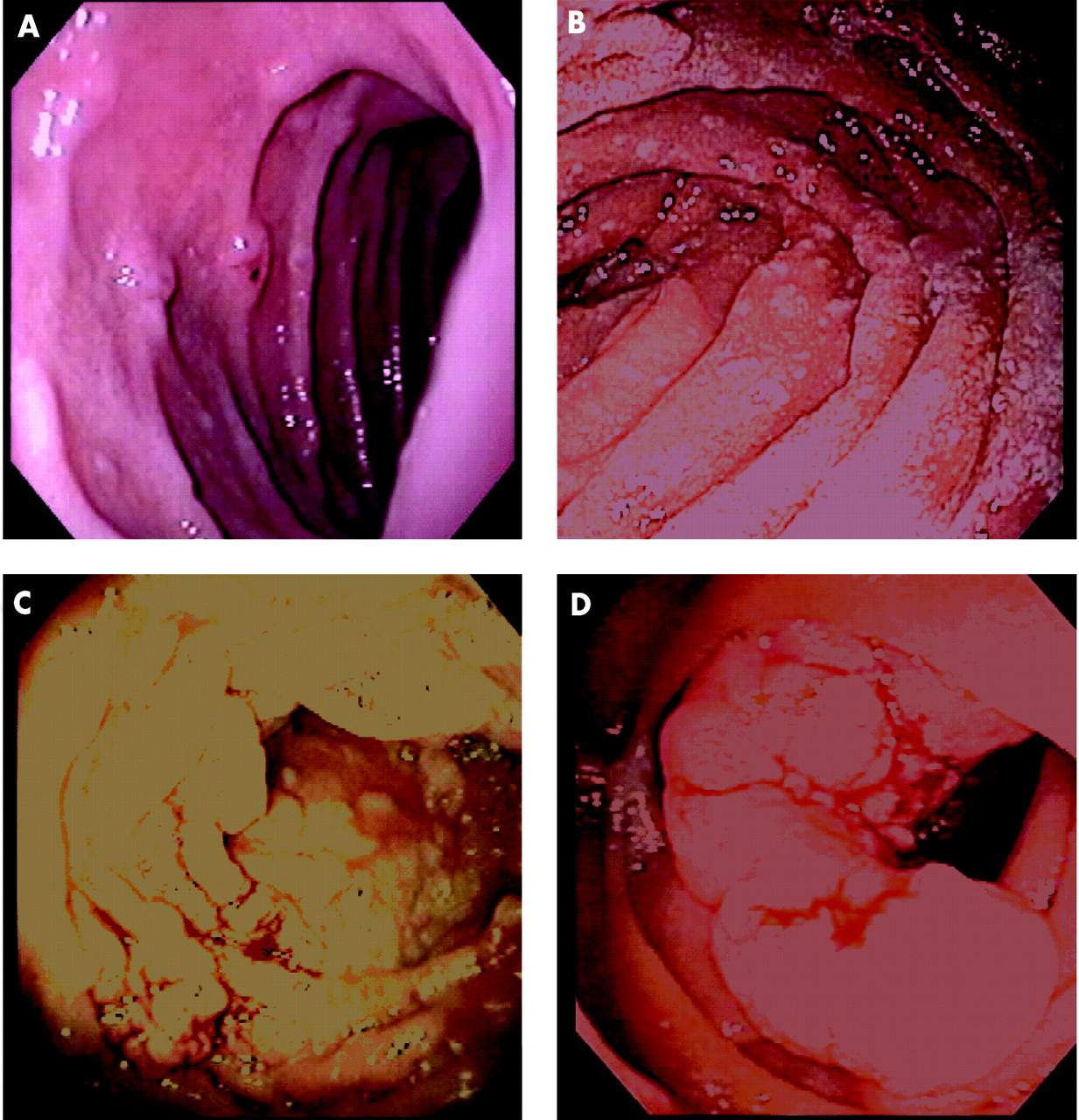
The most useful system for rating the severity of duodenal polyposis was developed by Spigelman and colleagues. This classification describes five (0–IV) stages. Points are accumulated for number, size, histology, and severity of dysplasia of polyps (table 2). Stage I indicates mild disease whereas stages III–IV imply severe duodenal polyposis (fig 4).12 Approximately 70–80% of FAP patients have stage II or stage III duodenal disease, and 20–30% have stage I or stage IV disease.12,40 The estimated cumulative incidence of stage IV duodenal disease however is 50% at age 70 years.4,41
Spigelman classification for duodenal polyposis in familial adenomatous polyposis

Spigelman stages of duodenal polyposis. (A) Stage I. (B) Stage II. (C) Stage III. (D) Stage IV.
Several investigators have shown that duodenal polyposis slowly progresses. One study followed 114 FAP patients for 51 months and found progression of polyps in size (26%), number (32%), and histology (11%).42 When individuals are followed for longer, duodenal polyps advance in Spigelman stage. Heiskanen and colleagues5 reported worsening polyposis in 73% of 71 FAP patients followed for 11 years. The median interval for progression by one stage was 4–11 years. Another group reported a stage change in 42% of patients with an average time of evolution by one stage of 3.9 years. Also, the risk of developing stage III or IV disease exponentially increases after age 40 years.43
The Spigelman classification also correlates with risk of duodenal malignancy. Stages II, III, and IV disease are associated with a 2.3%, 2.4%, and 36% risk of duodenal cancer, respectively.40
MANAGEMENT
Surveillance
As noted, duodenal polyposis is ingravescent over time. Consequently, surveillance of the upper gastrointestinal tract for the development of neoplasia by end and side viewing scopes is recommended by most authorities. One long term upper tract surveillance study of 114 FAP patients failed to prevent the development of duodenal adenocarcinoma in six patients.40 These findings emphasise the need to adjust the frequency of surveillance and to entertain surgical treatment with increasing severity of disease. Recommendations concerning the age of initiation of upper tract surveillance are not uniform. Some propose that screening for upper gastrointestinal disease should start at the time of FAP diagnosis.44 The NCCN (National Comprehensive Cancer Network), after review of all case reports of duodenal cancer in FAP patients, recommended a baseline upper gastrointestinal endoscopic examination at 25–30 years of age.45 Guidelines for continued endoscopic surveillance after baseline examination have been developed according to Spigelman stage by several authorities.40,45 In general, recommendations include stage 0 every 4 years; stage I every 2–3 years; stage II every 2–3 years; stage III every 6–12 months with consideration for surgery; and stage IV strongly consider surgery (table 3).
Recommendations for management of duodenal polyposis in familial adenomatous polyposis, adjusted to the Spigelman stage of duodenal polyposis
Endoscopic treatment
Endoscopic treatment options for duodenal lesions include snare excision, thermal ablation, argon plasma coagulation, and photodynamic therapy (PDT). Most reports of endoscopic therapy use snare excision. However, duodenal adenomas are often flat non-polypoid structures and, therefore, difficult to remove using conventional snare excision. For these cases, prior submucosal saline/adrenaline infusion may facilitate removal and reduce the risk of haemorrhage and perforation.40 In addition, thermal ablation,5,46 argon plasma coagulation,47 or PDT48–51 may be suitable.
PDT is a non-thermal technique relying on the combined effect of a low power activating light and a photosensitising drug that is selectively retained within neoplastic tissue with minimal retention in surrounding normal tissue. Few reports of PDT for adenomas in the gastrointestinal tract exist. Loh and colleagues50 successfully applied PDT for resection of colorectal adenomas: 7/9 treated adenomas were eradicated. Others have used PDT for resection of neoplastic lesions in the upper gastrointestinal tract but results are disappointing (table 4).48,49,51
Endoscopic treatment for duodenal neoplastic lesions
Endoscopic treatment of duodenal neoplasia for Spigelman stage II and III polyposis has been pursued by some investigators. However, the benefit of this approach in eradicating duodenal polyposis is difficult to justify but may be useful in individual cases. Literature reports of endoscopic treatment for FAP patients with duodenal/ampullary polyps are summarised in table 4. These publications reveal that endoscopic treatment is usually insufficient to guarantee a polyp-free duodenum and fraught with complications. Recurrence rates of adenomatous tissue in duodenum of FAP patients treated endoscopically range from 50% to 100%.44,46,52,53 Lower recurrence was reported by Norton and colleagues54,55 but their study population also included patients with sporadic duodenal lesions. In summary, endoscopic treatment appears useful in individual cases but follow up remains necessary and surgical intervention is often indicated in patients with more severe polyposis.
Surgery
Surgical options utilised to treat duodenal polyposis include local surgical treatment (duodenotomy with polypectomy and/or ampullectomy), pancreas and pylorus sparing duodenectomy, and pancreaticoduodenectomy. There are no randomised studies published to help guide surgical selection.
Publications of local surgical treatment with duodenotomy for duodenal polyposis in FAP patients are summarised in table 5. This surgery has proven insufficient to guarantee a polyp-free duodenum, with most studies reporting high recurrence rates in FAP patients with severe duodenal adenomatosis.5,52,44,46,56–59 Farnell and colleagues60 found a lower recurrence of duodenal polyps of 32% and 43% at five and 10 years of follow up, respectively. But this investigation also included sporadic duodenal polyposis cases and concludes that recurrence was higher in patients with a polyposis syndrome. Nevertheless, duodenotomy may be indicated in patients with one or two dominant worrisome duodenal lesions in otherwise uninvolved or minimally involved intestine. In the future, the postoperative use of chemopreventive medication may be a useful strategy.
Local surgical treatment (duodenotomy with polypectomy and/or ampullectomy) for duodenal neoplastic lesions
More radical surgery, in the form of classical pancreaticoduodenectomy, or pylorus or pancreas preserving duodenectomy, has been indicated for patients with severe polyposis (stage IV), failed endoscopic or local surgical treatment, and carcinoma development. Others recommend consideration of surgery in patients with stage III polyposis.44,46,52,57–63 Low recurrence rates of polyposis have been reported with these procedures (table 6). The specific choice of procedure appears related to local expertise and the site of polyp involvement. Use of endoscopic retrograde cholangiopancreatograpy to evaluate biliary duct involvement in patients with ampullary lesions or those with laboratory test perturbations has been suggested to direct appropriate surgery. In the final analysis, the morbidity and mortality of these surgeries must be weighed against the risk of developing duodenal adenocarcinoma.
Pancreaticoduodenectomy and pylorus or pancreas preserving duodenectomy for duodenal neoplastic lesions
Pharmacological treatment
Non-steroidal anti-inflammatory drugs (NSAIDs) regress colorectal adenomas in FAP patients. The value of these agents for duodenal polyposis regression is unclear. Studies of duodenal adenoma regression have primarily utilised sulindac (NSAID) and selective COX-2 inhibitors (table 7).
Familial adenomatous polyposis patients treated with sulindac, celecoxib, or refecoxib for duodenal adenomas
Nugent and colleagues64 compared the effect of sulindac (n = 12) and placebo (n = 12) on the number of duodenal polyps. Polyp number decreased in five patients, increased in one, and was unchanged in five after six months of treatment with sulindac 400 mg/day. The difference between sulindac and placebo treated patients was not significant, possibly due to lack of statistical power. However, a second evaluation of endoscopic videotapes from this cohort revealed a statistically significant effect on small (⩽2 mm) duodenal polyps whereas larger (⩾3 mm) duodenal polyps were unaffected.65 Another randomised crossover trial that compared sulindac 300 mg/day with calcium and calciferol revealed no effect on duodenal polyps in 15 patients who completed six months of treatment with sulindac.66
Richard and colleagues67 treated eight FAP patients with residual small periampullary polyps with sulindac 300 mg/day for at least 10 months. Sulindac was discontinued in three patients due to side effects. Follow up endoscopy was performed every six months or at discontinuation of treatment. None of the patients showed regression of polyps; three patients developed large polyps and one an infiltrating carcinoma while on this drug.
A large randomised trial by Phillips and colleagues,68 with statistical power to detect small differences, investigated the effect of the specific COX-2 inhibitor celecoxib on duodenal polyp number and total polyp area. A 14% decrease in polyp number was found after six months of celecoxib 800 mg/day (n = 32) compared with placebo (n = 17) which was not statistically significant. Paired assessment of endoscopic videotapes, however, revealed a significant difference (p = 0.033), although no effect on polyp area was noted.
Winde and colleagues69 preformed a prospective, controlled, non-randomised phase II dose finding study for sulindac. These investigators compared effects of sulindac suppositories (n = 28) with placebo (n = 10) on rectal and upper gastrointestinal adenomas in patients that underwent colectomy. They found complete or partial reversion of rectal polyps but no effects on duodenal and papillary adenomas.
Preliminary data from a trial comparing another specific COX-2 inhibitor, rofecoxib 25 mg/day, with ursodeoxycholic acid (controls) for duodenal polyps showed a response in two of six patients on rofecoxib and in none of the controls (n = 6). Of note, both responsive patients had stage III disease whereas none of the patients with stage IV disease improved.70
A case report described that sulindac 300 mg/day prevented the recurrence of severe duodenal polyposis in a patient with FAP.71 Another described two patients in whom treatment with sulindac 300–400 mg/day normalised an adenomatous ampulla and eliminated moderate dysplasia.72 In contrast, Waddell and colleagues73 observed no effect of sulindac 300–400 mg/day on gastric and small intestinal polyps in two patients with FAP. In addition to chemoprevention with NSAIDs, H2 blockers have been studied. No significant difference was found in duodenal polyp number or adduct formation between the ranitidine and placebo groups.74
In conclusion, the results of NSAID and other compounds on regression or prevention of duodenal adenomas in FAP appear disappointing, although regression of small adenomas may occur.65
MOLECULAR MECHANISMS OF CHEMOPREVENTION WITH NSAIDS
Studies of chemoprevention/regression of duodenal polyps in FAP have primarily utilised NSAIDs. The action of these agents has been divided into COX dependent, mediated through inhibition of the COX enzymes, and COX independent, caused by direct actions of NSAIDs on different molecular mechanisms.
COX dependent mechanisms
NSAIDs are best known for inhibitory effects on COX-1 and COX-2, key enzymes in the conversion of arachidonic acid to prostaglandins (PGs) (fig 5). COX-1 expression occurs in most tissues whereas COX-2 is expressed in response to growth factors, lipopolysaccharide, cytokines, mitogens, and tumour promoters.75 PGs are involved in cellular functions such as angiogenesis and cell proliferation. Therefore, inhibition of PG synthesis could explain part of the antineoplastic effects of NSAIDs. Also, COX-2 inhibition has antiangiogenic effects, as confirmed by several different studies.76–78 COX-2 inhibition may also induce apoptosis, mainly via inhibition of PGE2,79 and inhibit invasive properties of cancer cells. COX-2 was induced by coculture and promoted invasion in vitro that was inhibited by NSAIDs or RNAi against COX-2.80

Cyclooxygenase (COX) dependent chemopreventive mechanisms of non-steroidal anti-inflammatory drugs (NSAIDs). PG, prostaglandins; AA, arachidonic acid.
COX independent mechanisms
Several lines of evidence support the importance of COX independent means of action of NSAIDs. Firstly, high doses of NSAIDs induce apoptosis in COX-1 or COX-2 deficient cell lines81 and, secondly, PGs do not rescue these cells from apoptosis.82
Various COX-2 independent targets for NSAIDs have been proposed (fig 6). β-Catenin appears to be an important target as both indomethacin and exisulind reduce β-catenin expression in colorectal cancer cells.83,84 Also, NSAIDs induce apoptosis via both the membrane bound and mitochondrial pathway. High doses of aspirin antagonise the transcription factor nuclear factor κB,85 which regulates expression of antiapoptotic genes encoding proteins such as TRAF, c-IAP, c-FLIP, Bcl-XL, and A1. Several studies indicate a role for proteins of the Bcl-2 family in the apoptotic response to NSAIDs, and the membrane death receptor apoptotic pathway may also be involved.86 Furthermore, TGF-β signalling is implicated in NSAID chemoprevention.87 NSAIDs affect cell adhesion 88 and lipoxygenase metabolism,89 which reduce colorectal cancer cell invasion and could explain part of the apoptotic response to NSAIDs in colorectal cancer cells. Finally, it appears that members of the peroxisome proliferator activated receptor (PPAR) family, PPARδ and PPARγ, are directly targeted by NSAIDs and PGs.90–93

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cyclooxygenase (COX) independent chemopreventive mechanisms of non-steroidal anti-inflammatory drugs (NSAIDs). *Genes with a T cell factor 4 responsive element in their promoter, but no reports of downregulation in response to NSAIDs. **Contradictory reports. PPAR, peroxisome proliferator activated receptor; TGF-β, transforming growth factor β; NFκB, nuclear factor κB; VEGF, vascular endothelial growth factor; TRAIL, tumour necrosis factor related apoptosis inducing ligand.
CONCLUSIONS AND FUTURE DIRECTIONS
With improvement in the management of colorectal disease and increased life expectancy, duodenal polyposis and malignancy have emerged as major health problems in patients with FAP. Although most patients eventually develop duodenal polyps, these lesions occur at later age and have lower potential for malignant change compared with colonic polyps. Moreover, duodenal adenomas seem less responsive to chemoprevention with NSAIDs than colonic counterparts.
Currently, the main treatment options for duodenal polyposis are frequent surveillance and targeted endoscopic treatment, adjusted by severity of duodenal lesions. However, these modalities alone cannot guarantee a polyp-free duodenum.40 In patients with severe disease, duodenotomy or duodenectomy may be necessary. Drug therapy of duodenal adenomas would be appropriate treatment but most published reports find no significant effect of NSAIDs or COX-2 inhibitors on duodenal adenoma regression.
Summary
-
▸ FAP is characterised by innumerable adenomatous polyps throughout the colorectum and inevitable development of colorectal carcinoma usually by the fifth decade of life, if colectomy is not performed.
-
▸ Duodenal adenomas are found in 30–70% of FAP patients.
-
▸ The lifetime risk of duodenal adenoma development is virtually 100%.
-
▸ FAP patients have a 100–330-fold higher risk of developing duodenal cancer compared with the general population and an absolute lifetime risk of about 5%.
-
▸ No clear genotype-phenotype correlation exists, although mutations in the 3′ end of the APC gene (exon 15) appear to cause more severe duodenal manifestations.
-
▸ First screening for upper gastrointestinal adenoma is recommended at age 25–30 years.
-
▸ After baseline endoscopy, screening for duodenal polyposis is recommended as per Spigelman stage (see table 3).
-
▸ Recurrence of duodenal lesions after local endoscopic or surgical excision is common.
-
▸ Pancreaticoduodenectomy is the appropriate treatment for Spigelman stage IV duodenal polyposis and can be considered for stage III.
-
▸ Results of chemoprevention/regression studies for duodenal adenomas are equivocal or disappointing.
Increasing insights into the molecular changes during the adenoma-carcinoma sequence in the duodenum may point to future treatment strategies. Duodenal mucosa is exposed to different environmental factors than that in the colon. Low pH and bile acids may affect control of growth and malignant potential of duodenal tumours.12,13,38 Little is known about the role of potential molecular targets for chemoprevention, including COX-2, PPARδ, PPARγ, TGF-β receptor type II, EGF-R, and inducible nitric oxide synthase. More powerful chemopreventive/regressive regimens could result from combinations of NSAIDs or COX-2 inhibitors with other drugs, such as selective inhibitors of receptor tyrosine kinases or EGF-R. Further study is needed to understand the molecular changes in duodenal adenoma development and identify molecular targets for chemoprevention and regression of duodenal polyposis.
Acknowledgments
Supported in part by the Queen Wilhelmina Fund/Dutch Cancer Society, the John G Rangos, Sr Charitable Foundation, the Clayton Fund, and NIH grants 53801, 63721, 51085, and P50 CA 93–16.
REFERENCES
Footnotes
-
Conflict of interest: None declared.