Article Text

Statistics from Altmetric.com
Hepatorenal syndrome (HRS) is a serious complication of end-stage liver disease, occurring mainly in patients with advanced cirrhosis and ascites, who have marked circulatory dysfunction,1 as well as in patients with acute liver failure.2 In spite of its functional nature, HRS is associated with a poor prognosis,3,4 and the only effective treatment is liver transplantation.
During the 56th Meeting of the American Association for the Study of Liver Diseases, the International Ascites Club held a Focused Study Group (FSG) on HRS for the purpose of reporting the results of an international workshop and to reach a consensus on a new definition, criteria for diagnosis and recommendations on HRS treatment. A similar workshop was held in Chicago in 1994 in which standardised nomenclature and diagnostic criteria for refractory ascites and HRS were established.5 The introduction of innovative treatments and improvements in our understanding of the pathogenesis of HRS during the previous decade led to an increasing need to undertake a new consensus meeting. This paper reports the scientific rationale behind the new definitions and recommendations.
The international workshop included four issues debated by four panels of experts (see Acknowledgements). The issues were: (1) evidence-based HRS pathogenesis; (2) treatment of HRS using vasoconstrictors; (3) other HRS treatments using transjugular intrahepatic portosystemic stent-shunt (TIPS) and extracorporeal albumin dialysis (ECAD); and (4) new definitions and diagnostic criteria for HRS and recommendations for its treatment.
BACKGROUND
The definition and diagnostic criteria for HRS established in 19945 were based on the following three concepts:
-
renal failure in HRS is functional and caused by marked intrarenal arteriolar vasoconstriction;
-
HRS occurs in patients with systemic circulatory dysfunction caused by extra-renal vasodilatation;
-
plasma volume expansion does not improve renal failure.
Four new concepts have emerged since then, these are:
(a) Extra-renal arterial vasodilatation occurs mainly in the splanchnic vascular bed, whereas other vascular beds, such as those which supply the brain and the liver, may be vasoconstricted. This may contribute to the development of hepatic encephalopathy and hepatic failure, respectively.
(b) Cardiac output in patients with HRS may be low, normal or high, but it is insufficient for the patient’s needs because of reduced peripheral resistances.
(c) The most common trigger for the development of type-1 HRS is bacterial infection, mainly spontaneous bacterial peritonitis (SBP).
(d) Renal function can be improved by medical treatment in patients with HRS and is associated with improved survival.
Background for the new concepts
The first of these concepts was formulated following investigation conducted using Doppler ultrasonography or plethysmography both before and after 1994. These studies were performed in patients with varying degrees of severity of cirrhosis, and revealed arterial vasodilatation in the splanchnic circulation as well as arterial vasoconstriction in other areas such as the brain, kidneys and liver,6,7,8,9,10,11,12,13 whereas the cutaneous and muscular blood flow has been reported as low, normal or increased.13–16 The dilatation of the splanchnic vessels is mainly caused by local release of potent vasodilators such as nitric oxide (NO),17 which also render the splanchnic circulation resistant to various vasopressors including angiotensin II, norepinephrine, vasopressin and endothelin.18–24 The resistance of the splanchnic circulation to these vasopressor agents renders the control of arterial pressure in cirrhosis dependent on the extra-splanchnic effects exerted by the endogenous vasoconstrictor systems. As arterial vasodilatation increases with progression of cirrhosis, the role of vasoconstrictors in maintaining haemodynamic stability becomes critical, and explains why cirrhotic patients with HRS are predisposed to develop renal, hepatic and cerebral vasoconstriction.
Main pathophysiological and clinical aspects of HRS
-
HRS is a functional renal failure caused by intrarenal vasoconstriction which occurs in patiens with end-stage liver disease and circulatory dysfunction.
-
Circulatory dysfunction is characterised by vasodilatation in the splanchnic circulation with a relatively low and insufficient cardiac output, leading to effective hypovolaemia.
-
HRS may occur spontaneously with worsening liver function, or secondary to a precipitating event such as bacterial infection (eg, SBP).
-
HRS can be improved by the administration of vasoconstrictors and albumin, or by TIPS.
The second new concept—that is, that insufficient cardiac output contributes to renal hypoperfusion in patients with HRS—was first suggested by Tristani and Cohn,25 but it is only recently that this has been confirmed.26,27 The first study showed that the cardiac output of cirrhotic patients with SBP who developed progressive renal failure was relatively low, despite resolution of infection, when compared with a similar group of patients with SBP who did not develop renal failure.26 The second study compared non-azotaemic cirrhotic patients who developed HRS with similar patients who did not, and showed that low cardiac output and high plasma renin activity (PRA) were independent predictors of HRS.27 Moreover, in patients developing HRS, the progression of circulatory dysfunction leading to arterial hypotension and renal failure occurred in the setting of a continued decrease in cardiac output and increase in PRA. These findings support the hypothesis that hyperdynamic circulation is essential to maintain central blood volume and renal perfusion in cirrhosis. Therefore, when cardiac output decreases, effective hypovolaemia occurs, leading to renal hypoperfusion and HRS. The mechanism leading to impaired or insuffient cardiac output in patients developing HRS is unknown. In recent years, a specific cardiac abnormality, characterised by attenuated systolic and diastolic responses to stimuli, changes in repolarisation and hypertrophy of the cardiac chambers, has become increasingly recognised—the so-called “cirrhotic cardiomyopathy”.28 A fall in cardiac preload due to a decrease in venous return is another hypothesis that might justify the effectiveness of albumin infusion.27
HRS can be triggered by precipitating events. The most important of these are infection, bleeding and large-volume paracentesis without albumin administration.29–32 The role of SBP has recently been emphasised. Table 1 compares the results of two studies29,30 assessing the prevalence of renal failure in cirrhotic patients with SBP and in those with infections unrelated to SBP, and shows that: (a) in spite of an effective antibiotic therapy, a significant proportion of cirrhotic patients with bacterial infection develop progressive renal failure. This almost exclusively occurs in patients with SBP; (b) in patients not responsive to antibiotic therapy, progressive renal failure occurs and is independent of the type of infection. Furthermore, changes in circulatory function, endogenous vasoactive systems and renal function in patients developing renal failure triggered by SBP are identical to those observed in patients with HRS unrelated to infection, suggesting that the pathogenesis of progressive renal failure in cirrhotic patients with infection is the same as that of HRS.
Incidence and course of renal failure in cirrhotic patients with severe bacterial infections without shock according to response to antibiotic treatment and to type of infection
The most important concept of HRS, however, arises from studies exploring new therapeutic strategies.33 Since type-1 HRS is often associated with a rapid deterioration of liver function with increased levels of bilirubin and prothrombin time, it has traditionally been viewed as a manifestation of terminal hepatic failure. The demonstration that type-1 HRS can be improved by vasoconstrictors34 or by TIPS,35,36 and that reversal of type-1 HRS may be associated with improved survival, represents a major change in our understanding of the syndrome.
In conclusion, the main pathogenic mechanism in type-1 HRS is a potentially reversible deterioration of systemic circulatory function, mostly due to splanchnic vasodilatation and renal vasoconstriction and often triggered by a precipitating event (fig 1). In addition to renal failure, the syndrome may be associated with other organ dysfunctions, such as decreased cardiac output, hepatic failure and encephalopathy.

Schematic view of the pathogenetic mechanisms of hepatorenal syndrome in cirrhosis. Dotted arrows indicate that precipitating factors are frequent but not necessary. RAAS, renin–angiotensin–aldosterone system; SBP, spontaneous bacterial peritonitis; SNS, sympathetic nervous system.
TREATMENT OF HRS
New treatments of HRS are designed to expand the central blood volume by simultaneously increasing the total plasma volume and reducing intense peripheral vasodilatation. This strategy is not entirely new, as in 1967 Tristani and Cohn25 showed that dextran infusion improved cardiac output and renal perfusion in oliguric cirrhotic patients, and 18 years later Shapiro et al37 showed that the urine water and sodium excretion in cirrhotic patients with ascites was improved by the administration of norepinephrine combined with head-out water immersion, a manoeuvre aimed at expanding central blood volume. However, clinically relevant results have only been obtained more recently with the use of albumin and various vasoconstrictors.
The mechanism by which vasoconstrictors and albumin improve the glomerular filtration rate (GFR) in patients with HRS is incompletely understood. Nevertheless, administration of terlipressin to patients with HRS increases blood pressure and leads to a significant decrease in PRA and increase in GFR,38 indirectly indicating correction of circulatory dysfunction. It is conceivable that vasopressin analogues cause vasoconstriction of the splanchnic bed, thereby allowing redistribution of the blood volume to some of the extra-splanchnic organs including the central compartment and the kidneys. Filling of the central compartment will lead to the inhibition of the sympathetic nervous and renin–angiotensin systems, thereby shifting the autoregulatory curve to the left and making renal blood flow and GFR more responsive to changes in blood pressure.39,40 Albumin is traditionally considered to improve circulatory function in cirrhosis by expanding central blood volume and increasing cardiac output.41 Moreover, recent studies have shown that the administration of albumin to cirrhotic patients with SBP causes arterial vasoconstriction and blood pressure increase,42 probably attributable to the ability of albumin to bind vasodilators. It is therefore conceivable that an improvement of renal function in patients with HRS treated with vasoconstrictors and albumin is due to the additive effects that the two compounds have on cardiac function and peripheral arterial circulation.
Prophylaxis of HRS
One randomised controlled trial (RCT) showed that albumin prevented type-1 HRS in patients with SBP.41 Patients receiving albumin (1.5 g/kg body weight on the first day plus 1 g/kg body weight on the third day) showed a 66% reduction in the incidence of HRS (10% vs 33%) and a significant reduction of in-hospital and 3-month mortality rates (10% vs 29%, p<0.01, and 22% vs 41%, p<0.03, respectively,). The albumin effect was related to an improvement in systemic haemodynamics, as indicated by PRA suppression. Indeed, albumin infusion in cirrhotic patients with SBP improves both cardiac function and systemic vascular resistance.43 As type-1 HRS almost exclusively occurred in patients with serum bilirubin >68 μmol/l (4 mg/dl) and serum creatinine >88.4 μmol/l (1 mg/dl), the prophylactic use of albumin could probably be restricted to these patients, but trials need to be conducted so that the optimum dosage to be used can be defined more precisely.
New treatments of HRS
Vasoconstrictors and albumin
The use of an analogue of vasopressin to improve renal blood flow in cirrhotic patients was first proposed by Kew et al 35 years ago.44 More recently, Lenz et al45 showed that GFR may be moderately improved by ornipressin infusion in patients with HRS, but the drug was given for only 4 h, therefore precluding assessment of its long-term effects. Two more studies demonstrated that a long-term (1–2 weeks) infusion of ornipressin, combined with albumin or dopamine, normalised serum creatinine concentrations in many patients with type-1 HRS.34,46 Interestingly, recurrence of renal failure rarely occurred after treatment withdrawal, and in the few cases where it did recur a second course of therapy was successful. However, the drawback with ornipressin was the frequent occurrence of ischaemic complications.34,46
Therefore, widespread use of vasoconstrictors in patients with HRS has only become clinically feasible with the advent of safer compounds such as terlipressin,47–49 a vasopressin analogue with longer activity, and the α2-agonist midodrine combined with octreotide.50,51 Table 2 summarises the data available on the use of terlipressin in type-1 HRS. They include four RCTs,38,48,52,53 and many pilot or retrospective studies.
Characteristics and results of studies reporting the effect of terlipressin in patients with cirrhosis and type-1 HRS
These studies show that: (a) although GFR rarely reaches normal levels, a short period of treatment with terlipressin improves renal function in up to 65% of patients with type-1 HRS; (b) the effectiveness of terlipressin is probably enhanced by albumin;49 (c) HRS recurs after treatment withdrawal in approximately 20% of patients, but re-treatment is often effective; (d) in most cases, dilutional hyponatraemia associated with HRS improves with terlipressin treatment;48,49 (e) severe side effects of the treatment are uncommon (5–10%). With regards to survival, patients who experienced a complete reversal of type-1 HRS by terlipressin seem to have improved short-term survival, although the RCT of Sanyal53 reported similar survival at 60 days of follow-up between patients treated with terlipressin plus albumin and those treated only with albumin. Therefore, the long-term survival of patients with type-1 HRS treated with terlipressin merits further investigation. Nevertheless, using terlipressin to improve renal function is an important support resource for patients included on a liver transplant waiting list who develop type-1 HRS.54
The initial dose of terlipressin in many studies ranged from 0.5 to 1 mg every 4–6 h. This regimen was maintained until reversal of HRS, which usually occurred within the second week of treatment.47,52 In other studies, the initial dose in cases without an early response was increased up to 2 mg every 4–6 h.49 The daily dose of albumin was generally 20–40 g, preceded in some studies by a load of 1 g/kg body weight. Some refer to central venous pressure to establish and titrate albumin doses and to prevent fluid overload.
Experience of using midodrine in patients with type-1 HRS is more limited. To date, there have been two pilot studies.50,51 In both, midodrine was combined with octreotide to enhance the effect of splanchnic vasoconstriction, but doses and routes of administration were quite different. Angeli et al50 used 7.5–12.5 mg of oral or intravenous midodrine three times a day plus 100–200 μg of subcutaneous octreotide three times a day, whereas Wong et al51 used 2.5 mg of oral midodrine three times a day plus an intravenous infusion of octreotide (25 μg/h after a bolus of 25 μg). The dose of midodrine was adjusted to increase mean arterial pressure to 90 mm Hg. Albumin was also administered to patients in these studies. The results are similar to those observed with terlipressin, although the response was slower. Since octreotide alone had no impact on GFR in patients with HRS,55 it is likely that midodrine plays the main role in improving GFR.
A pilot study has also explored the effect of norepinephrine infusion (0.5–3 mg/h) combined with albumin and furosemide in type-1 HRS.56 The doses were titrated to increase mean arterial pressure by 10 mm Hg. Reversal of HRS was achieved in 10 out of 12 cases and was associated with improvement in urinary sodium excretion and decrease in PRA. Norepinephrine is cheaper and more widely available than terlipressin, but it is thought to have a greater propensity to induce cardiac arrhythmias. Therefore, the role of norepinephrine in patients with type-1 HRS still needs to be established on the basis of future comparisons with terlipressin or midodrine/octreotide.
Only a few patients with type-2 HRS have been specifically treated using terlipressin and albumin.33 In most cases, normalisation of serum creatinine was observed, but, in contrast to type-1 HRS, renal failure invariably recurred after treatment withdrawal.
Transjugular intrahepatic portosystemic stent-shunt
Only a few studies have assessed the role of TIPS in HRS—91 patients in total. Most were prospective but uncontrolled studies.35,36,51,57,58 Three were performed in patients with type-1 HRS,35,36,51 one in patients with type-1 or type-2 HRS,57 and the last specifically investigated type-2 HRS.58 The following can be observed:
-
significant suppression of the endogenous vasoactive systems, particularly the renin–angiotensin system,35 and a decrease of creatinine levels were recorded after TIPS in most patients with type-1 HRS. The rate of the creatinine decrease was slower than is usually obtained using terlipressin plus albumin;
-
recurrence of HRS was rare, provided that there was no shunt malfunction;
-
hepatic encephalopathy was a frequent complication of TIPS but was adequately managed by medical treatment;
-
TIPS almost always induced a reduction of ascites volume;
-
resolution of type-1 HRS by TIPS can improve survival;
-
sequential treatment with vasoconstrictors and albumin followed by TIPS could be used as an alternative approach to increasing the probability of long-term success;51
-
although TIPS may improve renal function and refractory ascites in patients with type-2 HRS, its effect on survival is still undefined.
However, since almost all studies excluded patients with a history of severe encephalopathy, serum bilirubin levels >85 μmol/l (5 mg/dl), or Child–Pugh score >12, the applicability of TIPS may be rather limited in patients with HRS who frequently show jaundice, encephalopathy and high Child–Pugh scores.59
There has been little investigation into the mechanism through which TIPS exerts beneficial effects in patients with HRS. Nevertheless, as TIPS functions as a side-to-side portocaval shunt, it is expected to relieve portal hypertension, which plays a pivotal role in the pathogenesis of splanchnic arterial vasodilatation.60 Moreover, TIPS insertion is associated with an increase in cardiac output and an expansion in central blood volume.61,62 The simultaneous effects on the splanchnic and systemic circulation may represent the mechanism by which TIPS improves renal perfusion, GFR, urine sodium and water excretion, and hyponatraemia.63
Extracorporeal albumin dialysis (ECAD)
This procedure uses a cell-free albumin-containing dialysate that is re-circulated and perfused through charcoal and anion exchange columns (molecular adsorbent recycling system (MARS)). The system is also connected to a haemodialysis or haemoperfusion apparatus. ECAD enables the removal of albumin-bound substances, including bilirubin, bile acids, aromatic amino acids, medium chain fatty acids and cytokines.64 There are few data available for ECAD in cirrhotic patients with HRS, and these data are controversial.65,66 ECAD decreases serum creatinine levels, but it is not definitively known whether or not this effect is due to a true improvement of renal function or simply to the filtration process. A few studies reported that systemic haemodynamics improved during ECAD, indicated by an increase in arterial pressure and systemic vascular resistances, and a decrease in cardiac output, PRA and norepinephrine levels. However, studies regarding the effect of ECAD on survival in patients with type-1 HRS included too few patients to draw any definite conclusions.66,67 Moreover, ECAD is a very expensive procedure and should still therefore be considered experimental.
Liver transplantation in patients with HRS
Liver transplantation was the only effective therapy for patients with HRS before the introduction of vasoconstrictors and TIPS, and is still the treatment of choice for these patients.68–71 Further impairment in GFR may be observed immediately after liver transplantation, and many patients require long-term dialysis (35% of transplanted patients with HRS vs 5% of transplanted patients without HRS).68,71 As calcineurin inhibitors (ciclosporin and tacrolimus) may contribute to GFR impairment, it is suggested to delay their administration until a partial recovery of renal function is recorded, usually 48–72 h after transplantation. After this early impairment, GFR starts to improve until an average value of 30–40 ml/min is reached 1–2 months postoperatively. This moderate renal failure persists during the follow-up and is probably due to an enhanced nephrotoxic effect of calcineurin inhibitors in patients with pre-transplant renal impairment. In fact, the haemodynamic and neurohormonal abnormalities associated with HRS disappear within the first month after transplantation, and the patients regain their ability to excrete sodium and free water.72
Patients with HRS who undergo liver transplantation tend to have more complications, spend more days in intensive care units and have higher in-hospital mortality rates than liver transplant patients without HRS.73,74 However, their 3-year probability of survival is acceptable (60% vs 70–80% in liver transplant patients without HRS).70
The main limitation of liver transplantation is that due to the shortage of donor organs, and their extremely short survival, most patients with type-1 HRS die before transplantation. The introduction of the model of end-stage liver disease (MELD) for organ prioritisation has partially solved this problem, since patients with HRS are generally given high priority on the waiting list. On the other hand, treatment of type-1 HRS with vasoconstrictors and albumin (see above) can improve patient survival, and therefore improve their probability of being transplanted. In one non-randomised pilot study, reversal of type-1 HRS using terlipressin and albumin was associated with reduction in early morbidity and mortality after liver transplantation.54
CONCLUSIONS OF THE CONSENSUS WORKSHOP
Improved knowledge of the mechanisms underlying HRS and the development of new treatment strategies are the reasons for the new consensus on definition, diagnostic criteria and HRS treatment modalities organised by the International Ascites Club.
Effective treatments of type-1 HRS
-
Albumin infusion may prevent HRS in patients with SBP.
-
Vasoconstrictors and albumin are recommended as the first line of treatment for type-1 HRS. Terlipressin is the most widely used vasoconstrictor. Midodrine+octreotide and norepinephrine are two possible alternatives requiring further clinical evaluation.
-
With the use of terlipressin (2–12 mg/day) and albumin (20–40 g/day after 1 g/kg on the first day), about 60% of renal failure cases recover. The improvement of survival using only vasoconstrictors and albumin seems rather limited.
-
TIPS is an alternative treatment in suitable patients, especially in those who do not show a complete response to vasoconstrictors, but it can also be used in patients who show a complete serum creatinine response to eliminate ascites and to maintain normal renal function.
-
Liver transplantation is the only treatment that assures long-term survival.
-
Pharmacological treatment and TIPS can bridge the time to liver transplantation and improve post-transplant survival.
New definition of HRS
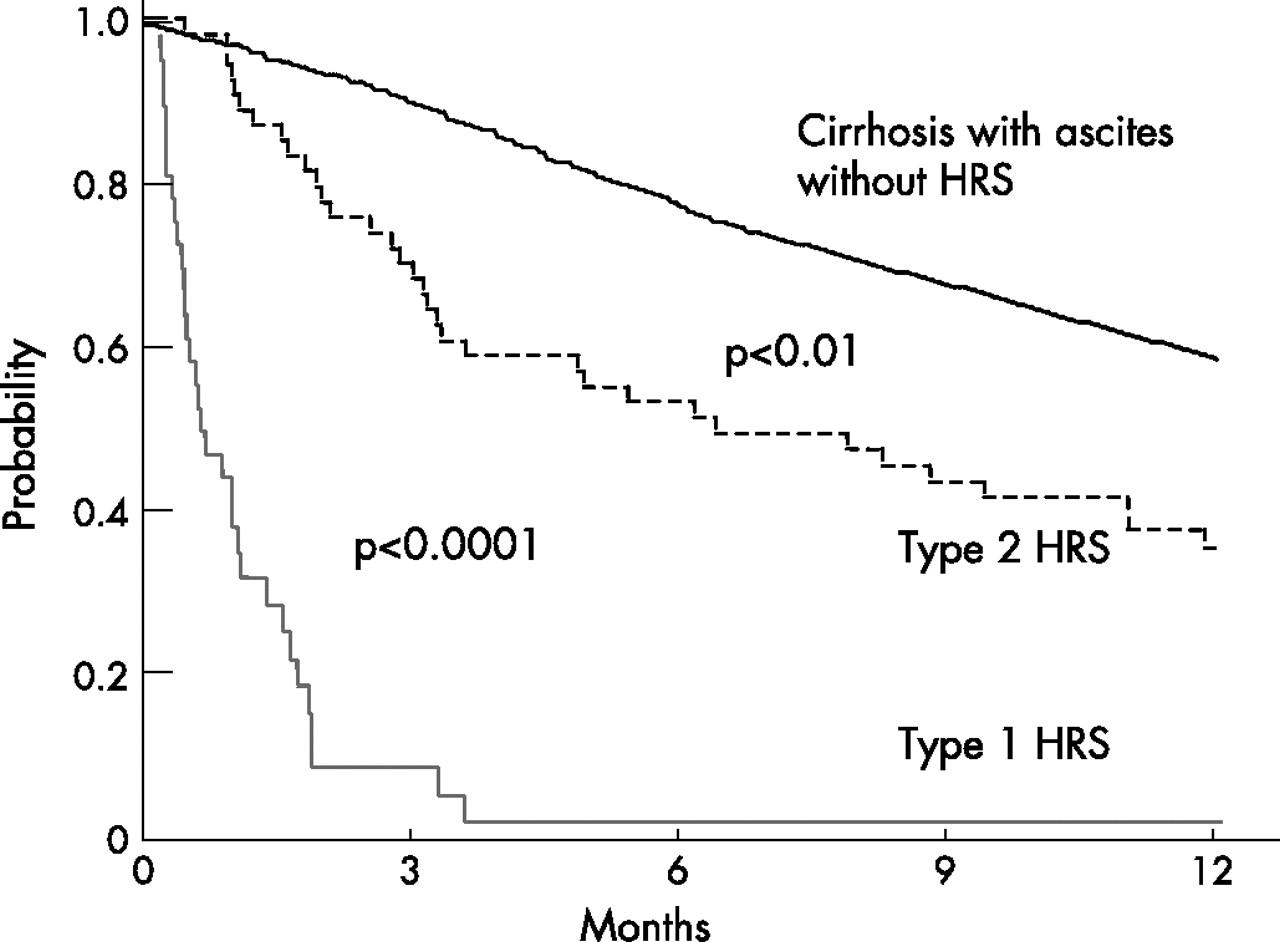
HRS is a potentially reversible syndrome that occurs in patients with cirrhosis, ascites and liver failure, as well as in patients with acute liver failure or alcoholic hepatitis. It is characterised by impaired renal function, marked alterations in cardiovascular function and overactivity of the sympathetic nervous and renin–angiotensin systems. Severe renal vasoconstriction leads to a decrease of GFR. There are two types of HRS. Type-2 HRS is characterised by moderate renal failure (serum creatinine from 133 to 226 μmol/l or from 1.5 to 2.5 mg/dl), with a steady or slowly progressive course. It appears spontaneously, but can also follow a precipitating event. Type-2 HRS is typically associated with refractory ascites. Survival of patients with type-2 HRS is shorter than that of non-azotaemic cirrhotic patients with ascites but better than that of patients with type-1 HRS (fig 2).75
{kind=link}
{kind=link}
Actuarial probability to survive in cirrhotic patients with different renal impairments: non-azotaemic patients (continuous line); patients with hepatic renal syndrome (HRS) type-2 (dotted line) and patients with HRS type-1 (red line). Adapted from Alessandria et al75.
Type-1 HRS is characterised by rapid progressive renal failure defined by doubling of the initial serum creatinine concentrations to a level greater than 226 μmol/l (2.5 mg/dl) in less than 2 weeks. It may appear spontaneously, but often develops after a precipitating event, particularly SBP. Type-1 HRS usually occurs within the setting of an acute deterioration of circulatory function characterised by arterial hypotension and activation of endogenous vasoconstrictor systems, and may be associated with impaired cardiac and liver functions as well as encephalopathy. The natural prognosis of type-1 HRS is very poor (fig 2).
The main differences from the definition reported in 19965 are:
-
the potential reversibility of HRS without liver transplantation;
-
the dominant role of the splanchnic bed in arterial vasodilatation;
-
the frequent role of SBP as an event precipitating type-1 HRS;
-
the concept that in addition to renal failure the function of other organs, particularly the heart, is frequently impaired.
Revised diagnostic criteria of HRS
As there are no specific hallmarks of HRS, the diagnosis is based on the exclusion of other types of renal failure. The criteria necessary to diagnose HRS are reported in the box below.
The main differences between these criteria and those previously established5 are:
-
creatinine clearance has been excluded because it is more complicated than simple serum creatinine for routine purposes, and it does not increase the accuracy of renal function estimation in cirrhotic patients;76
-
renal failure in the setting of ongoing bacterial infection, but in the absence of septic shock, is now considered HRS. This means treatment of HRS can be started without waiting for complete recovery from the infection;
-
plasma volume expansion should be performed with albumin rather than saline. Members of the panel agreed that albumin causes a greater and more sustained expansion than saline;
-
minor diagnostic criteria have been removed as they are not essential.
Treatments of HRS
Most data currently available on HRS treatments come from retrospective analyses, pilot studies, non-randomised comparative studies and only a few RCTs. Furthermore, most studies have included too few patients. Therefore, concepts and practical recommendations given in this part of the article are based on both published data and the personal experience of the panelists, and may be improved upon by further experience gained in the future
Prevention of HRS
The incidence of HRS in patients with SBP may be reduced by albumin administration, prevention which was associated with improved survival. The suggested dose of albumin is 1.5 g/kg body weight on the first day and 1 g/kg body weight on the third day, up to a maximum of 150 and 100 g, respectively. Albumin administration is clearly indicated for patients with SBP and serum bilirubin levels >68.4 μmol/l (4 mg/dl) or serum creatinine levels >88.4 μmol/l (1 mg/dl). Future studies are necessary to define better optimal doses of albumin and the subgroup of patients for whom treatment is highly indicated.
New diagnostic hepatorenal syndrome criteria in cirrhosis
-
Cirrhosis with ascites.
-
Serum creatinine >133 μmol/l (1.5 mg/dl).
-
No improvement of serum creatinine (decrease to a level of ⩽133 μmol/l) after at least 2 days with diuretic withdrawal and volume expansion with albumin. The recommended dose of albumin is 1 g/kg of body weight per day up to a maximum of 100 g/day.
-
Absence of shock.
-
No current or recent treatment with nephrotoxic drugs.
-
Absence of parenchymal kidney disease as indicated by proteinuria >500 mg/day, microhaematuria (>50 red blood cells per high power field) and/or abnormal renal ultrasonography.
Effective treatments of HRS
Liver transplantation
This is the treatment of choice for both type-1 and type-2 HRS. Morbidity after liver transplantation is higher in patients with HRS than in those without HRS,74 although the long-term probability of survival is only slightly lower. Reversal of type-1 HRS by pharmacological treatment before liver transplantation may improve survival after transplantation. The reduction in serum creatinine levels after treatment and the related decrease in the MELD score should not change the decision to perform liver transplantation since the prognosis after recovering from type-1 HRS is still very poor.
Pharmacological treatment with vasoconstrictors
Studies on the pharmacological treatment of HRS have mainly been performed in patients with type-1 HRS. Terlipressin is the most widely studied compound. It should be started at 0.5–1 mg every 4–6 h. If there is no early response (>25% decrease in creatinine levels after 2 days), the dose can be doubled every 2 days up to a maximum of 12 mg/day. Treatment can be stopped if serum creatinine does not decrease by at least 50% after 7 days of the highest dose, or if there is no reduction after the first 3 days. In patients with early response, treatment should be extended until reversal of HRS (see text box) or for a maximum of 14 days. Terlipressin may induce ischaemic side effects and arrhythmias requiring drug discontinuation.33
Other vasoconstrictors tested in HRS are midodrine, in combination with octreotide, or norepinephrine. The schedules for midodrine and octreotide and those of norepinephrine are reported above.
In addition to creatinine levels being useful in adjusting the doses of these vasoconstrictors, blood pressure, renal water and sodium excretion, and serum sodium levels may also be helpful.
The administration of albumin may improve the effect of vasoconstrictors. In the absence of dose/effect studies, the dose of albumin recommended is 1 g/kg of body weight on the first day, up to a maximum of 100 g, followed by 20–40 g/day. Albumin may be discontinued if serum albumin concentration is >45 g/l and should be withdrawn in the case of pulmonary oedema. Since this complication is uncommon, catheterisation to monitor central venous pressure is not mandatory, but careful physical and radiological monitoring of the cardiopulmonary function is recommended.
Types of response to treatment using vasoconstrictors
-
Complete response (reversal of HRS): decrease of serum creatinine to below 133 μmol/l (1.5 mg/dl).
-
Relapse of HRS: recurrence of renal failure (creatinine >133 μmol/l (1.5 mg/dl)) after discontinuation of therapy.
-
Partial response: decrease in serum creatinine to ⩾50% of its pre-treatment value, without reaching a level below 133 μmol/l (1.5 mg/dl).
-
No response: no decrease of serum creatinine or decrease to <50% of its pre-treatment value, with a final level above 133 μmol/l (1.5 mg/dl.
As reported in the text box, three types of response to treatment with vasoconstrictors and albumin can be observed. Complete response occurs in approximately 60% of patients treated with terlipressin and can improve survival. Renal failure may recur after discontinuation of therapy (relapse), but retreatment is usually effective. In contrast, partial response is frequently followed by a severe and irreversible relapse of renal failure.
TIPS
The small amount of data on the use of TIPS in HRS shows that it improves renal function and eliminates ascites. In patients with type-1 HRS, TIPS may also improve survival, but this is debatable in patients with type-2 HRS. The major disadvantage of TIPS is its low applicability. Indeed, it should not be used in patients with serum bilirubin levels >85.5 μmol/l (5 mg/dl), severe encephalopathy or history of recurrent encephalopathy, severe bacterial infection, serious cardiac or pulmonary dysfunction or a Child–Pugh score >11.
Final recommendations for the treatment of patients with HRS
Type-1 HRS
The first line of therapy is the use of vasoconstrictors combined with albumin. Patients with partial or no response to vasoconstrictors may be treated with TIPS. If there are contra-indications to TIPS, ECAD could be used in the setting of prospective trials.
The sequential use of vasoconstrictors plus albumin and TIPS in suitable patients is an interesting idea deserving further investigation.
Type-2 HRS
There are no definite data to support the use of vasoconstrictors in these patients. TIPS can be used to improve refractory ascites, which is often associated with type-2 HRS. Data on the effect of TIPS on survival are still insufficient.
Acknowledgments
Experts who participated to the four panels for the preparation of the consensus were the following:
(a) Evidence-based pathogenesis of HRS: chairman: P Gines (Spain), panelists: G di Bona (USA), S Lee (Canada), J H Henriksen (Denmark), L Ruiz del Arbol (Spain), F Wong (Canada).
(b) Treatment with vasoconstrictors: chairman: A Gerbes (Germany), panelists: P Angeli (Italy), G Garcia-Tsao (USA), V Gülberg (Germany), M Guevara (Spain), R Moreau (France), R Ortega (Colombia).
(c) Treatment with other resources: chairman: F Wong (Canada), panelists: P Kamath (USA), K Moore (UK), K Mullen (USA), F Salerno (Italy), A Sanyal (USA).
(d) Definitions, diagnostic criteria and recommendations: chairman V Arroyo (Spain), panelists: M Bernardi (Italy), L Blendis (Israel), G Garcia-Tsao (USA), R Terg (Argentina).
REFERENCES
Footnotes
-
Funding: The work of P Ginès in this project was supported by a grant from the “Fondo de Investigacion sanitaria (Fis 05/246)”. The work of F Salerno in this project was supported by a grant of Ministero della Università Italiana (FIRST 2005).
-
Competing interests: None.