Article Text

Statistics from Altmetric.com
Traditionally, small intestinal bacterial overgrowth (SIBO) has been characterised by symptoms of diarrhoea, bloating and sometimes signs of malabsorption. It has been defined as >105 colony-forming units (cfu)/ml of bacteria in aspirates obtained from the small intestine.1 This condition has typically been diagnosed in patients with readily identifiable alterations in small bowel function which predispose patients to SIBO (eg, resected ileocaecal valve, small intestinal hypomotility and possibly hypochlorhydria). Recently, however, this clinical paradigm has been challenged by new theories about the aetiology of irritable bowel syndrome (IBS) and has led to renewed scrutiny of the tests employed to diagnose this condition and controversy concerning the use of antibiotics to treat IBS for suspected SIBO.
The proposal that SIBO accounts for the symptoms of IBS2 3 is a novel and interesting hypothesis, given the rapidly growing evidence that luminal bacteria have previously unrecognised actions on multiple intestinal functions.4 While it has long been recognised that increased numbers of luminal bacteria in the small intestine disrupt digestion and absorption, it is now clear that they have other important actions, such as immune activation4 5 Immune-mediated cytokines could have multiple actions including altered epithelial secretion, exaggerated nociceptive signalling and abnormal motility.4 Together, these changes could lead to symptoms which meet the criteria for IBS. It has also been proposed that this mechanism could account for overlap syndromes, such as fibromyalgia.6
The publication of Pimentel and colleagues in 20007 played a pivotal role in establishing the concept that SIBO is a major pathogenic mechanism underlying IBS. Two major tenets emerged from this study: (1) based on the results of the lactulose hydrogen breath test (LHBT), the large majority of patients with IBS have SIBO, and (2) when SIBO is eradicated with antibiotics based on the findings of a postantibiotic LHBT, a large proportion of patients with IBS have symptom improvement. Although major concerns about the validity of these tenets have been raised in subsequent studies and reviews,8–15 there has been a rapidly growing acceptance of the use of the antibiotics, such as rifaximin, to treat IBS in the USA16 and elsewhere. This paper rigorously examines the validity of the LHBT for diagnosing SIBO in IBS and the supporting evidence that SIBO underlies IBS, and explores the findings from clinical trials examining the effects of antibiotics on IBS.
LHBT FOR DIAGNOSING SIBO IN IBS
Small intestinal bacterial flora in health and disease
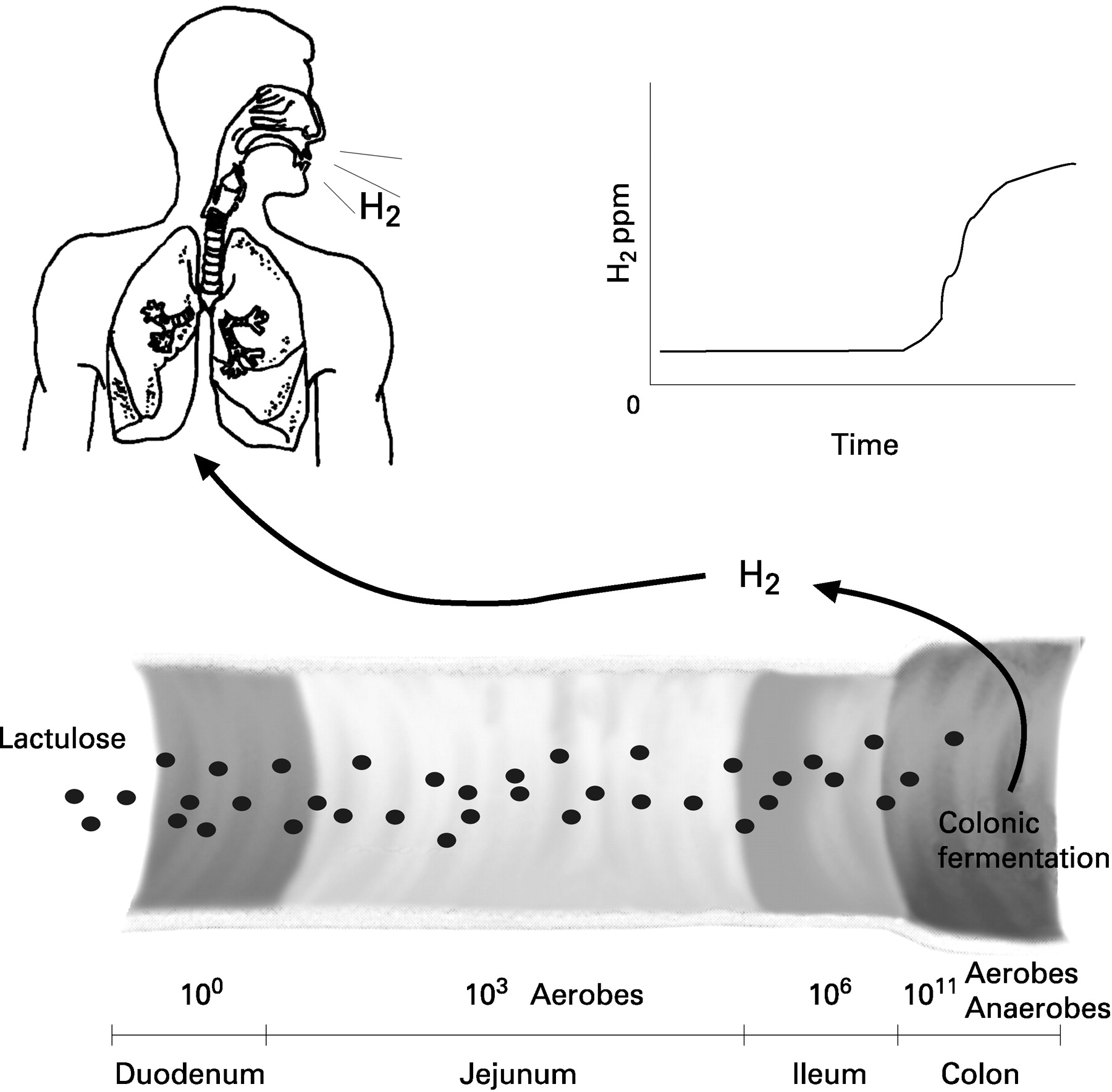
Under normal conditions, the small intestine is a relatively sterile environment and at the ileocaecal valve there is an abrupt rise in bacterial counts (fig 1).1 8 The proximal small intestine is populated with relatively small numbers of Gram-positive aerobes with the addition of anerobes in the ileum.1 Using standard culture techniques, counts in the ileum range from 105 to 108 and increase to 1010 to 1012 in the caecum, with a predominance of anerobes. Overgrowth of bacteria in the small intestine is traditionally defined by counts >105 cfu/ml, based on the correlation of symptoms and counts obtained from aspirates from the proximal small intestine. However, it has been suggested that this definition may not be sufficiently precise because these cultures can contain largely Gram positives from the upper respiratory flora and these have not been correlated with symptoms of SIBO.1 Hence, a more precise definition appears to be >105 cfu/ml of “colonic-type” bacteria (ie, Gram negatives, strict anaerobes and enterococci) which have been correlated with symptoms of SIBO and possess known pathogenic mechanisms which could result in the symptoms of SIBO. Ultimately, the most precise definitions may rely on emerging molecular techniques with greater accuracy in identifying bacterial species which are difficult to culture.5 17
Lactulose hydrogen breath test
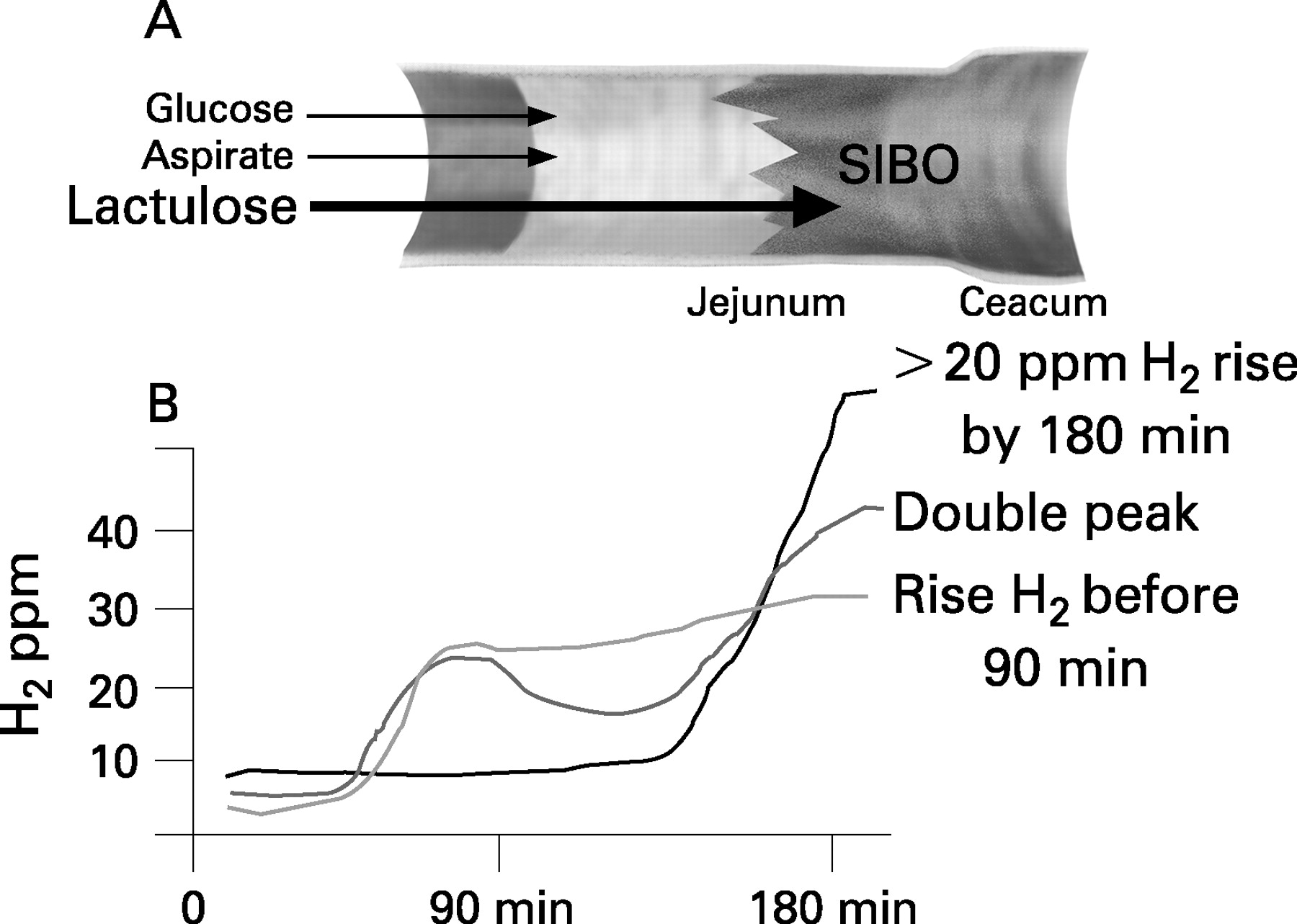
According to the proponents of the SIBO–IBS hypothesis, the overgrowth of bacteria is largely confined to the distal small intestine.3 As shown in fig 2, this could explain why the standard diagnostic test using jejunal aspirates fails to detect overgrowth in this patient group.3 Similarly, the glucose hydrogen breath test also would be inaccurate because this sugar is absorbed in the more proximal small intestine.3 In contrast, lactulose is a non-absorbable carbohydrate, allowing it to reach the site of potential overgrowth in the small intestine even if it is in the distal portion of the small intestine.

The LHBT exploits the fact that the only source of H2 gas production in the body is the fermentation of carbohydrate substrate1 and this can be monitored be measuring H2 ppm in expired breath because it readily diffuses from the lumen into the circulation (fig 1). In the normal setting, repeated measurements of breath H2 ppm remain low as the lactulose transits through the relatively sterile environment of the small intestine, until it reaches the high numbers of bacteria within the caecum. This leads to a rapid rise in H2 gas as a result of bacterial fermentation of the sugar. When these colonic bacteria migrate proximally into the small intestine, as proposed to occur in IBS, the timing of the rise in H2 should be altered. More recently, measurements of expired methane (CH4) gas following lactulose ingestion in studies of patients with IBS have been reported, because this gas has been implicated in constipation-predominant IBS (see later).
Three different criteria have been employed in clinical trials to define an abnormal LHBT in patients with IBS (fig 2). In Pimentel’s original study,7 they used the traditional double peak criteria. The initial peak is thought to result from fermentation of the initial bolus of lactulose in the region of SIBO and the second peak from the arrival of the residual lactulose in the caecum.1 In subsequent studies, Pimentel and others rejected these criteria, accepting either a rise in H2 before 90 min (>20 ppm in some studies) and/or an absolute rise from baseline of 20 ppm by 180 min (fig 2).
Recently, a Canadian,13 Swedish15 and US18 study have examined the validity of these criteria by examining LHBT in patients with IBS and healthy controls (fig 3). In Pimentel’s original study in 2000, they reported that 78% of patients with IBS have SIBO based on the double peak criteria. In contrast, none of the recent studies was able to detect levels >17%, and these proportions did not differ from those of healthy controls (fig 3). Subsequent studies by Pimental et al,19 applying the criteria of a rise of H2 by 90 min or an absolute rise in H2 >20 ppm by 180 min, again reported high numbers of patients with IBS having SIBO (∼80%). When these criteria were applied in the three subsequent studies (fig 3), a high proportion of patients with IBS with “positive tests” were also found; however, no differences were found between patients with IBS and healthy controls.

{kind=link}
{kind=link}
{kind=link}
Closer scrutiny of the origins of the criteria for diagnosing SIBO with the LHBT suggests that these have been a source of controversy since the test’s inception.1 10 The association between an early rise in H2 levels following lactulose ingestion and SIBO overgrowth was first observed by Levitt and colleagues,20 and over time the LHBT became recognised as a non-invasive means of diagnosing SIBO. However, subsequent studies designed to test the validity of the original “double H2 peak” criteria (see fig 2) compared results in culture-positive patients predisposed to SIBO and found a disappointing low sensitivity (17–68%) and specificity (44–70%).21 22 Proposed explanations for these poor results included fermentation by oral and gastric flora, and the effects of transit time.1
The influence of transit time is an important consideration, particularly for the more recent “single peak” criteria proposed by Pimental and colleagues—that is, H2 rise by 20 min or >20 ppm by 180 min (fig 2). In fact, the LHBT was first proposed as a means of diagnosing orocaecal transit time,23 using the sharp rise in H2 levels as an indication that the lactulose had reached the fermenting anaerobes in the caecum (fig 1). This association was confirmed in healthy controls by intubating the distal ileum and aspirating polyethylene glycol (PEG) which was co-ingested with the lactulose. In each case, the PEG was aspirated before the rise in H2, reflecting the lag time to reach the caecum. These studies showed that in healthy controls the transit time was dose dependent and there was a wide range in times, from 25 to 118 min, with a mean of 72 min. A number of reviews1 10 have drawn attention to the fact that several studies show that up to 50% of asymptomatic individuals have a rise in H2 by 90 min. These findings highlight the concern that single H2 peaks simply reflect transit to the caecum, as opposed to resulting from fermentation by colonic bacteria in the small intestine. These concerns were further supported by studies which combined lactulose with 99Tc, enabling the tracer to be temporally aligned with the H2 levels, to determine if increases occur before or after reaching the caecum.21 In patients predisposed to SIBO, the initial rise in H2 was preceded by the arrival of 99Tc in the caecum in 22% of cases, and a caecal source for double peaks was suggested in 50% of patients. Twenty-four hour calorimetric studies also indirectly suggest that H2 gas in patients with IBS originates from colonic bacteria. They have shown increased rates of H2 excretion in unselected cases of IBS and that a reduction of gas excretion occurs following elimination diets, including fibre reduction.24 They have also shown that two groups exist, one with high H2 excretion and another which did not differ from controls.25 This latter group did not respond to an exclusion diet and the LHBT did not differentiate between the two IBS groups (ie, high and low H2 excreters). The implication is that some patients with IBS have greater numbers of gas-forming bacteria in the colon, and fibre reduction decreases fermentation. Thus, based on the available evidence, it seems highly unlikely that single peak criteria for an abnormal LHBT can discriminate between IBS and healthy controls, because these values fall within the range of normal transit times to the caecal flora.
UNRESOLVED LINKS IN THE SIBO–IBS HYPOTHESIS
Why would patients with IBS be predisposed to develop SIBO?
A missing link in the SIBO–IBS hypothesis is the mechanism which predisposes patients with IBS to SIBO. Most conditions known to predispose patients to SIBO, such as small bowel dilatation, mechanical factors, terminal ileal resection and diverticuli, are not associated with IBS, but hypomotility cannot be excluded. One study examined small bowel motility in patients with IBS with positive LHBTs and found that the duration and frequency of the migrating motor complex (MMC) were significantly reduced in these patients.26 Moreover, 50% of patients with IBS lacked an MMC during the recording interval. While potentially important, there are major limitations to this study. This was a retrospective study where patients were referred because of an abnormal LHBT (defined by the double peak criteria), not because they had IBS. Most important, however, was the absence of a comparable control group. The controls were obtained from a different centre which used a different catheter (solid state) and recorded for differing lengths in the small intestine and for a longer time period. Other studies of patients with IBS have reported widely variable results27–32 and the LHBT status was not assessed. The discrepancy between these studies may reflect differences in techniques and the wide variability in motility patterns observed in healthy controls.32 In a more recent study which combined manometry with jejunal aspirates in patients with IBS, the very small number of patients (4%) with a positive aspirate (>105 cfu/ml) had a reduced number of MMCs compared with those with normal aspirates (96%). It is unknown how patients with IBS with an abnormal LHBT correlated with controls in this study, but the frequency of MMCs in the aspirate-negative group approximated that of the control group used in the Pimentel study.26 The relationship between small bowel motility and IBS is further complicated by the possibility that the IBS group could be contaminated by small numbers of patients suffering from mild chronic intestinal pseudo-obstruction, given that patients with IBS are largely identified by symptom criteria. Taken together, the technical differences and lack of adequate controls suggest that further studies are needed to clarify this issue.
Can SIBO account for symptoms in patients with IBS with both constipation and diarrhoea?
Another pathogenic uncertainty is the explanation as to how SIBO could result in diarrhoea in some patients with IBS and constipation in others. Pimentel and colleagues suggest that the production of CH4 gas in the constipation group provides the explanation.16 All CH4 gas is a metabolic product of intestinal bacteria, and methanogenic bacteria reside in the colon under normal conditions.33 CH4 production is estimated to occur in 36–50% of healthy subjects.34 35 In IBS studies, an association between constipation-predominant IBS and CH4 production (abnormal test defined as a rise in CH4 following lactulose ingestion within 90 min or >20 ppm during 180 min measurement19) has been well documented,36 but its causal relationship is not clear. On one hand, animal studies have shown that CH4 gas can reduce antroduodenal motility in vivo, yet exaggerate contractile responses in vitro.37 In addition, in a retrospective review of a small number of cases of IBS who underwent LHBT and antroduodenal motility testing, CH4-producing patients had an increased motility index compared with H2-producing patients.37 Based on these findings, it was suggested that CH4 production could result in increases in non-propagating contractions in the small intestine, leading to constipation. While these data are intriguing, there are a number of inherent biases in the human studies and plausible alternative explanations, including the effects of methane production on colonic motility.33 38 The finding that patients with diarrhoea due to other conditions such as Crohn’s disease or ulcerative colitis33 34 have a very low prevalence of CH4 excretion may suggest that diarrhoea simply precludes the proliferation of methogens in the colon.33 This notion is supported by the finding that colon cleansing34 and low fibre diets dramatically lower CH4 excretion. The proposed relationship is further complicated by a recent study which found that the prevalence of CH4 producers is not different between patients with IBS and healthy controls,18 raising further questions about the validity of breath testing in IBS. Taken together, these studies suggest that more rigorous studies of methane production in IBS and the effects of CH4 on small and large bowel motility are needed.
Box 1
The lactulose hydrogen breath test does not discriminate between patients with irritable bowel syndrome and healthy controls
Further studies are needed to determine if CH4 production causes hypomotility in patients with IBS or is simply a physiological marker of constipation
Does SIBO account for IBS overlap syndromes?
IBS is known to overlap with a number of other poorly understood chronic conditions, including fibromyalgia. Recently, it has been suggested that SIBO may also be a unifying hypothesis between these conditions6 given that very high numbers of patients in both groups had an abnormal LHBT and that patients had a symptomatic response to antibiotic treatment.6 10 However, the findings in these studies are undermined by the absence of a proper control group, confirming that the LHBT can accurately discriminate between these patients and healthy controls (see also discussion of LHBT above).
CLINICAL TRIALS USING ANTIBIOTICS TO TREAT IBS
Results of clinical trials
The symptom response of patients with IBS to antibiotics has been examined in three relatively small, prospective placebo-controlled studies (table 1).19 39 40 Several important differences in study design need to be taken into account when comparing these results. In particular, the entry criteria in the study by Sharara and colleagues (gas and flatulence; ∼60% met Rome II on retrospective analysis) differed significantly from the others (Rome I). In addition, the most recent study by Pimentel and colleagues39 analysed the data using a complex statistical mixed model which creates a blending of symptom responses over the entire period rather than a conventional single end point.12 Each of these three studies reports a significant, albeit modest, reduction in either global symptom or composite symptom scores (mean range = 15–24% over placebo) although the placebo responses were low (range = 11–21%), particularly for IBS studies. These findings are only applicable to the time periods studied (7 days–10 weeks).
A number of other studies7 41–45 are often referenced in support of these prospective studies. Although all report symptom reduction with antibiotics, the interpretation of their findings is seriously limited by their study design. These studies lack a placebo group, are retrospective and/or do not examine a clearly defined group of patients with IBS.
Several studies have examined specific symptoms which underlie the improvement in global symptom scores following antibiotic treatment.24 39 40 45 Two of these studies40 45 recruited patients with gas–bloat syndrome rather than IBS, but many of these patients met the criteria for IBS. All of these studies found that a reduction in bloating and/or related symptoms correlated with global symptom reduction (table 2). In the two larger studies,39 40 logistic regression of the individual symptoms showed a correlation with bloating, but not with other IBS symptoms. Two of these studies40 45 also showed a correlation with these specific symptoms and changes in H2 excretion following antibiotic treatment. In the one study24 where faecal anaerobes were cultured, both antibiotics and fibre reduction resulted in a significant reduction in bacterial counts. Although larger studies are required to confirm these observations, these data do suggest that the major benefit of antibiotics in IBS results from a decrease in gas-forming bacteria. It is unclear whether they reside in the colon as opposed to the small intestine.
Does symptom improvement correlate with normalisation of the LHBT?
The hypothesis that SIBO accounts for the symptoms of IBS is based on the LHBT, but the correlation between the normalisation of the LHBT following antibiotics and symptom improvement has become less clear (table 3). In the study by Pimentel et al,19 only 20% of the LHBTs normalised following antibiotics and, although symptom reduction correlated best with this group, there was a much larger number of patients who had a significant reduction in symptom scores compared with placebo who did not normalise their LHBT. Moreover, in the subsequent 2006 study by this same group, although LHBTs were performed, these data were not reported (results removed in the review process, M Pimentel, personal communication). The post hoc analysis of rifaximin responders by Sharara and colleagues (see table 3) showing a correlation between decreased bloating and a reduction in H2 at 180 min may be supportive, but could also simply reflect a reduction in gas-forming bacteria in the colon, given the 180 min time interval (see LHBT above).
Could antibiotics be detrimental in IBS?
Although the favourable short-term safety profile of newer non-absorbable antibiotics, such as rifaximin,46 may make the use of antibiotics in IBS more attractive, enthusiasm should be tempered by several considerations. There are no long-term studies with antibiotics in IBS and less is known about the safety of these antibiotics long term. IBS is a common disorder with a recognised high placebo response rate, and studies show that the effects of antibiotics on measurable outcomes are short lived. Hence there is significant potential for committing large numbers of patients to antibiotics.
There are also indirect studies which imply that antibiotics could play a role in the pathogenesis of IBS. A study in a general practice setting found that prior antibiotic use strongly correlated with patients having the symptoms of IBS.47 It has also been shown that the use of antibiotics is related to increased reporting of functional bowel symptoms.48 In an animal model,49 the use of non-absorbable antibiotics was shown to induce low level colonic inflammation and visceral hypersensitivity. Clearly, further studies are needed to confirm these associations in humans, but given that antibiotics suppress bacteria in the small and large bowel, these studies highlight the potential for antibiotic use to have detrimental effects, particularly with continuous or repeated courses.
Box 2
Antibiotics result in a modest reduction in global symptoms that is short lived
Bloating is the major symptom which is reduced by antibiotics
There is insufficient evidence to recommend antibiotics for the treatment of irritable bowel syndrome at present
CONCLUSIONS AND FUTURE DIRECTIONS
The hypothesis that SIBO accounts for the symptoms of IBS has helped to focus on the role of bacteria in the intestine and in particular their potential to modulate sensation and motility. Although this is an intriguing hypothesis which has stimulated significant work in this area, this remains an unproven hypothesis. The inability of the LHBT to discriminate between patients with IBS and healthy controls, together with the findings of available IBS studies examining antibiotic treatment, make it plausible that colonic, rather than small bowel, bacteria account for the findings of these studies. Proof of the SIBO–IBS hypothesis requires more definitive studies to resolve this issue, such as direct culture from the distal small bowel either with oral intubation or with double balloon enteroscopy. Continued use of the LHBT to diagnose SIBO in IBS requires validation studies, such as combined 99Tc scanning with the LHBT to determine whether changes in H2 levels suggesting bacterial fermentation correlate with 99Tc in the small intestine or caecum. Given the absence of reasonable proof for the SIBO–IBS hypothesis at present and the concerns about antibiotic use, it is difficult to recommend antibiotic treatment for IBS at this time.
Despite the current lack of evidence, it remains possible that quantitative and/or qualitative differences in bacteria exist within the small intestine in patients suffering from IBS. One study15 examining bacterial aspirates in patients with IBS failed to detect significant numbers with >105 cfu/ml of colonic bacteria (4%) but, when they defined a positive test as ⩾5×103, they found a significant increase in patients with (43% IBS vs 12% controls). Whether these findings are relevant to the expression of IBS, however, is unclear. These findings did not correlate with small bowel manometry or with positive LHBT and glucose hydrogen breath tests. An emerging area of investigation which may also help to resolve the implications of such observations is the use of quantitative DNA fingerprinting of faecal bacteria. This technique has the advantage of identifying large numbers of species, especially obligate anaerobes, which cannot be identified using traditional culture techniques.50 Using faecal samples, recent molecular studies suggest that quantitative alterations in the microbial biota exist in patients with IBS.51 52 This may provide another approach to evaluate bacteria in the small intestine to determine if abnormal numbers or qualitative species differences exist in patients with IBS.
Even if the SIBO–IBS hypothesis is ultimately rejected, findings from these studies will help to stimulate new treatments for IBS. For example, if the reduction in bloating due to antibiotics results from suppression of colonic bacteria, studies are needed to characterise the species involved and safe, long-term treatment modalities explored (eg, probiotics, see5 53 54). The evidence that CH4 may inhibit motility is also intriguing, even if the methanogenic bacteria originate in the colon, and further basic and clinical studies are needed to explore the mechanism and possible treatments.
Acknowledgments
SV is supported by funding from the Canadian Institute of Health Research (CIHR) and a Crohn’s and Colitis Foundation Canada (CCFC) Scientist Personnel Award.
REFERENCES
Footnotes
Competing interests: None.