Article Text

Statistics from Altmetric.com
We note with interest two recent publications in Gut regarding alterations to the gut microbiome in individuals on proton pump inhibitor (PPI) therapy.1 ,2 With PPI use, both studies observed an increase in oral bacteria in the stool. These changes overlap with those described in patients with cirrhosis of the liver.3 However, very little is known about the impact of this dysbiosis over the length of the GI tract, and how it may link to gut function.
While the data from both Jackson et al1 and Imhann et al2 are demonstrative of a shift towards oral-associated bacteria, it is important to note that many of these bacteria have also been identified in the stomach and small intestine. Recently, we have shown that although the microbiota found in the healthy duodenum are taxonomically similar to the oral microbiota, their presence and association with the intestinal mucosa is not merely a result of luminal contamination.4 Thus, small intestinal dysbiosis and its potential impact on the gut must also be considered.
Compared with studies targeting stool, the mucosal microbiota and in particular, that of the small intestine, presents many challenges. As a consequence, our understanding of the microbiota in this region is comparatively poor. We believe this area should be investigated and thus have recently shown the potential for dysbiosis in the small intestinal mucosa in functional dyspepsia (FD). Recent observations have revealed low level duodenal and systemic inflammation in patients with FD (notably duodenal eosinophilia),5 ,6 and increased duodenal permeability,7 making changes to the microbiota a factor of interest. Using previously described methods,4 the duodenal mucosal microbiota was assessed in patients with FD (Rome III; n=9) and controls (screening for iron-deficiency anaemia, mucosal/coeliac disease excluded; n=9) matched for age, sex and body mass index.
Notably, the predominant genus in the duodenal mucosa was Streptococcus in both control subjects and patients with FD (figure 1). An inverse relationship between the relative abundance of Streptococcus and the anaerobic genera Prevotella, Veillonella and Actinomyces was observed, which were significantly decreased in patients with FD (Mann-Whitney U test, p<0.05, false discovery rate q<0.2). When these differences were collectively compared using principal coordinates analysis, a divergence between cohorts was observed. Using redundancy analysis, the differences in the community profiles between patients with FD and controls were both clearly distinct and statistically significant (see online supplementary figure S1, p=0.02).
Supplementary figure

Relative abundance of bacterial genera in the duodenal mucosa, assessed using 16S rRNA gene sequencing. Differences between patients with functional dyspepsia (FD) and controls were established using the Mann-Whitney U test, with false discovery rate (FDR) correction for multiple comparisons (#—family).
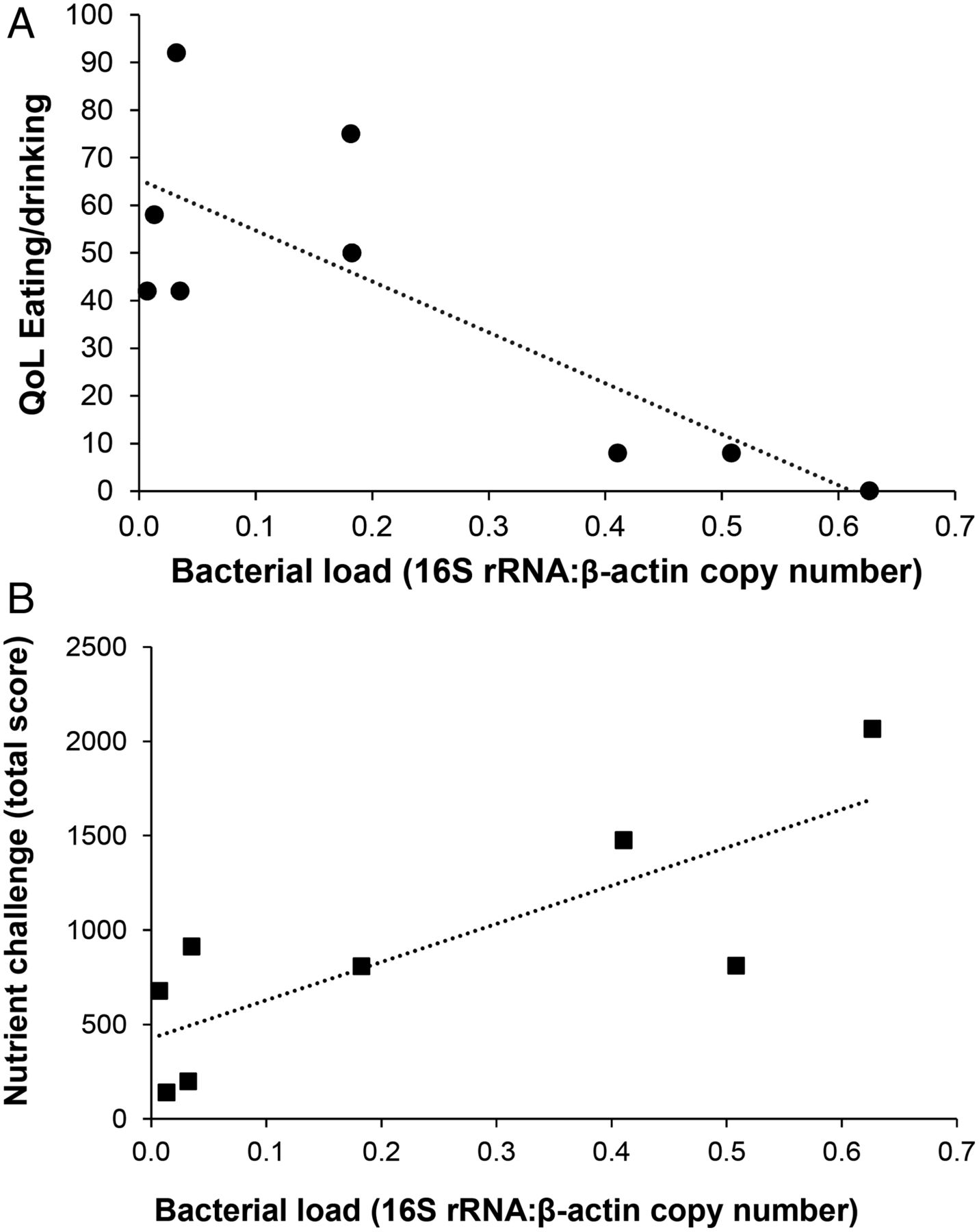
In the patients with FD, we also assessed quality of life (Nepean Dyspepsia Index8), symptom responses to a meal (standardised nutrient challenge9) and total bacterial load (quantitative PCR). Strikingly, we observed a negative correlation between duodenal mucosal bacterial load and reported quality of life (figure 2, p=0.01). In addition, more severe symptom responses to the standardised meal positively correlated with mucosal bacterial load (figure 2, p=0.02). Furthermore, as the total bacterial load increased, bacterial diversity decreased.
{kind=link}
{kind=link}
Duodenal mucosal bacterial load is linked to symptoms in functional dyspepsia (FD). (A) Reported Quality of life (QoL) (Nepean Dyspepsia Index) in patients with FD was negatively correlated with bacterial load (r=−0.8, p=0.01). (B) Total meal-related symptoms reported by patients (nutrient challenge total score) following a standardised test meal positively correlated with bacterial load (r=0.8, p=0.02). Bacterial load was assessed using qPCR and reported as the ratio between copies of the bacterial 16S rRNA and human β-actin genes. Correlations were assessed using a Spearman correlation (r).
These results highlight a new paradigm for symptom generation in FD, and suggest the importance of mucosal bacteria in the small intestine. While these organisms are ‘oral like’, they are present in the duodenal mucosa, and are linked to symptoms. This is particularly interesting to consider in the context of PPI use as a treatment for FD, with varying efficacy.10
Thus, to more fully understand both the interesting results obtained by Jackson et al,1 and Imhann et al,2 as well as those we have presented above, a more substantial research effort into understanding the microbiome of the small intestine, akin to the large intestine, is needed.
Acknowledgments
We thank all patients for their participation in this study. We also appreciate the contributions of the nursing and administrative staff of the Department of Gastroenterology and Hepatology, Princess Alexandra Hospital; with particular acknowledgement Teressa Hansen for her contribution to patient recruitment. Sequencing was performed at the Australian Centre for Ecogenomics, The University of Queensland.
References
Footnotes
Contributors LZ and ERS: data acquisition and analysis, writing and editing of manuscript. AR: data acquisition and patient recruitment. NAK: ethics and patient recruitment. LF: data acquisition and supervision. MM: study design, obtained funding, critical review of manuscript. MMW, NJT and GH: study concept and design, obtained funding, critical review of manuscript.
Funding We would like to acknowledge the project support of the Princess Alexandra Hospital (PA) Research Foundation and the NHMRC (APP1084544).
Competing interests None declared.
Ethics approval Metro South Health Human Research Ethics Committee; The University of Queensland Medical Research Ethics Committee. Written consent was obtained from all participants.
Provenance and peer review Not commissioned; internally peer reviewed.