Article Text

Statistics from Altmetric.com
Since December 2019, a novel coronavirus referred to as SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2)1 was identified as the causative agent of a respiratory syndrome named COVID-19.2 Since February 2020, an outbreak of COVID-19 has developed in Lombardy, in northern Italy, posing serious challenges to healthcare system. As reported, COVID-19 severity directly correlates with patient’s age and several comorbidities,3 but no data are currently available regarding clinical outcome in inflammatory bowel diseases (IBD). Recently, the International Organization for the Study of Inflammatory Bowel Disease (IOIBD) recommended a reduction of corticosteroid therapy in IBD patients, while maintaining thiopurines and biologics,4 even if Authors recognised that specific IBD research on COVID-19 is lacking.
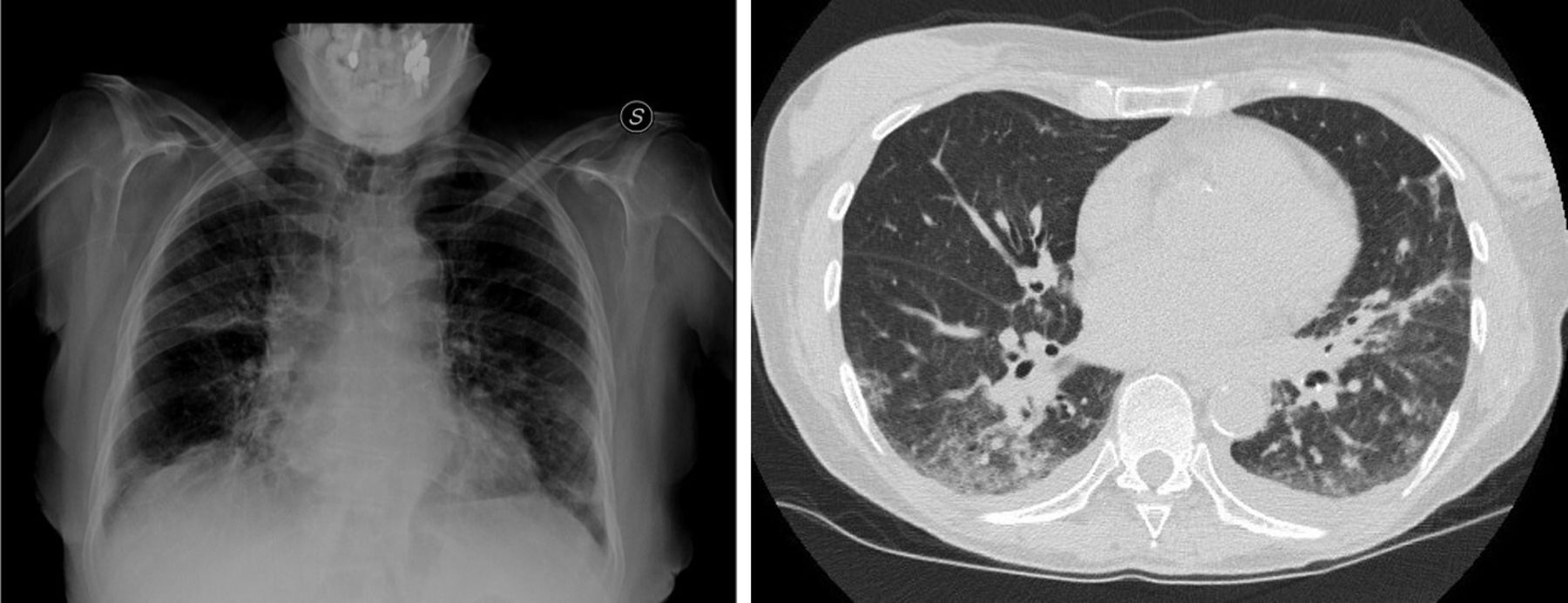
On 12 February 2020, days before this outbreak was recognised, an 80-year-old female with a 3-year history of left-sided ulcerative colitis (UC), in maintenance with mesalamine, presented to our clinic with a 7-day history of fever and bloody diarrhoea. On admission, the patient reported four bowel movements per day with blood and fever up to 38.5°C. Laboratory tests documented severe anaemia (haemoglobin 7 g/dL) and increased C-reactive protein (CRP) (6 mg/dL). A sigmoidoscopy showed large and deep ulcers in sigmoid colon and rectum (figure 1). Stool cultures were negative, including tests for Clostridium difficile. The patient was therefore diagnosed with a severe UC relapse and intravenous corticosteroid therapy (methylprednisolone 40 mg/day) was started. During the next 3 days, the frequency of bowel movements decreased, fever resolved and CRP returned into normal range. On the fourth day, fever up to 39°C developed, followed by dry cough. On the basis of the evolving knowledge regarding SARS-CoV-2 outbreak, including data relative to hospital-acquired infections, a case of COVID-19 was suspected. Chest radiography showed bilateral pneumonia, confirmed by chest CT scan (figure 2). The nasopharyngeal swab sample confirmed the presence of SARS-CoV-2 and a diagnosis of COVID-19 pneumonia was made. The patient was treated with non-invasive ventilation, and a combination of lopinavir/ritonavir and hydroxychloroquine. Intravenous corticosteroid was rapidly switched to oral prednisone, and an accelerated tapering was initiated. Despite an initial improvement, the patient’s condition subsequently worsened and the patient died after 14 days of hospitalisation. Prednisone dosage at the time of patient’s death was 25 mg daily.

Endoscopic image of the sigmoid colon showing severe inflammation with large and deep ulcers.
{kind=link}
{kind=link}
On the left, a plain chest X-ray showing bilateral pulmonary infiltrates; on the right, a chest CT scan showing multiple bilateral pulmonary ground-glass opacities.
Corticosteroids administration showed no effect on mortality but delayed lower respiratory tract clearance of the coronavirus in both SARS and Middle East respiratory syndrome.5 In a recent retrospective study, corticosteroids were more frequently administered in patients with poor outcome,6 although another study showed potential benefit for patients who develop acuterespiratory distress syndrome.7 Current WHO recommendations suggest that routine corticosteroids should be avoided in COVID-19, unless they are indicated for another reason.5 According to recent reports, >75% of patients with COVID-19 received antiviral drugs, including lopinavir/ritonavir. Lopinavir/ritonavir has shown anti-coronavirus activity in vitro and was associated with a reduced mortality in SARS,8 however a recent clinical trial demonstrated no benefit in hospitalised patients with severe COVID-19.9 Chloroquine is a cheap and a safe drug widely used for malaria and autoimmune diseases, and has recently been reported as a potential broad-spectrum antiviral drug. A recent study revealed that chloroquine was highly effective in the control of SARS-CoV-2 in vitro.10 Finally, we hereby report the first case of a COVID-19 pneumonia in an elderly patient with severe acute UC treated with corticosteroids. Considering a COVID-19 incubation time of up to 14 days, it is possible that the patient was already harbouring SARS-CoV-2 when corticosteroids were initiated; as a consequence, it would be advisable to test for the virus before systemic steroid initiation in highly epidemic areas. Nevertheless, further evidences are required to define the best treatment strategy in IBD patients.
Footnotes
Contributors SM and FC wrote the letter; AS, FP and MV critically reviewed the letter and made adjustments to the text.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.