Article Text

Statistics from Altmetric.com
Introduction
The global epidemic of obesity continues to escalate despite the substantial rise in medical, governmental and public awareness of weight gain. Obesity is a multifactorial disorder of behaviour, genetics and environment. Many obese individuals suffer from several comorbidities, including type 2 diabetes mellitus, cardiovascular disease and cancer. Recently, the World Health Organization predicted that the global population in 2015 will comprise approximately 2.3 billion overweight adults and more than 700 million obese adults.1 The UK government predicts that according to current trends, 60% of all males and half of all females will be obese by 2050.2 As a result, the treatment of an expanding obese population carries a heavy burden on healthcare resources aimed at weight loss therapies, but also the associated comorbidities that also require additional costs.
Although a fundamental need for disease prevention is universally acknowledged, the increased prevalence of obesity now mandates the widespread application of disease treatments and interventions. Numerous medical treatments have been developed to promote weight loss although the majority have not demonstrated long term efficacy or safety, particularly for the morbidly obese population.3 Surgical strategies for weight loss have been in place for over half a century and are being considered with increased favour due to consistent success in providing sustained weight loss for the complex morbidly obese population. These operations that were initially titled as bariatric surgery have also demonstrated considerable benefits to cardiovascular outcomes, cancer risk and the systemic metabolism such that they can resolve type 2 diabetes mellitus in approximately 75% of morbidly obese patients so that now they are also termed as metabolic procedures.4,–,7 As a result, national and international healthcare associations such as the UK's National Institute for Health and Clinical Excellence (NICE), National Institutes of Health in the USA and the International Federation for the Surgery of Obesity advise surgery for patients with a body mass index (BMI) greater than 40 kg/m2, or a BMI >35 kg/m2 in addition to an associated comorbidity such as diabetes or hypertension which could be improved by weight loss.8 These international guidelines are continually reassessed to consider increasing evidence relating to performing these operations at lower weight categories,9 aimed at treating metabolic dysfunction in addition to excess weight. Currently, NICE also stipulates that: (1) all appropriate non-surgical measures have been tried but have failed to achieve or maintain adequate, clinically beneficial weight loss for at least 6 months; (2) the person has been receiving or will receive intensive management in a specialist obesity service; (3) the person is generally fit for anaesthesia and surgery; (4) the person commits to the need for long term follow-up; and (5) bariatric surgery is also recommended as a firstline option (instead of lifestyle interventions or drug treatment) for adults with a BMI of >50 kg/m2 in whom surgical intervention is considered appropriate.8
Annually, over 344 000 procedures are performed worldwide: 220 000 of these take place in the USA/Canada and 6000 are performed in the UK, with over 90% being performed laparoscopically.10 Of the multitude of surgical operations available, three are most widely accepted by the majority of bariatric/metabolic surgeons. These include: (1) Roux-en-Y gastric bypass; (2) adjustable gastric band; and (3) sleeve gastrectomy (a newer operation that can be performed as a standalone procedure or combined simultaneously, or prior to, a duodenal switch procedure). Each procedure offers distinctive effects on the resolution of obesity but also carries healthcare costs that reflect both the expected operative expenses on obese patients (with their unique geometry and increased thrombotic risk) and also the long term follow-up of these cases. Although some units report a 1 year mortality of 4.6%,11 a meta-analysis of 361 studies on 85 048 patients undergoing a wide spectrum of bariatric procedures revealed a perioperative (≤30 days) mortality of 0.28% and a 2 year postoperative mortality of 0.35%,12 which is further corroborated by a recent multicentre prospective study focusing on the perioperative safety of bariatric surgery.13
It has recently been demonstrated that only 2.5–33% of patients eligible for surgery receive bariatric procedures.2 The question therefore arises whether healthcare providers such as the National Health Service or private insurers can afford such a treatment strategy in the current climate of rigorous financial accountability and societal responsibility.
The financial cost of obesity
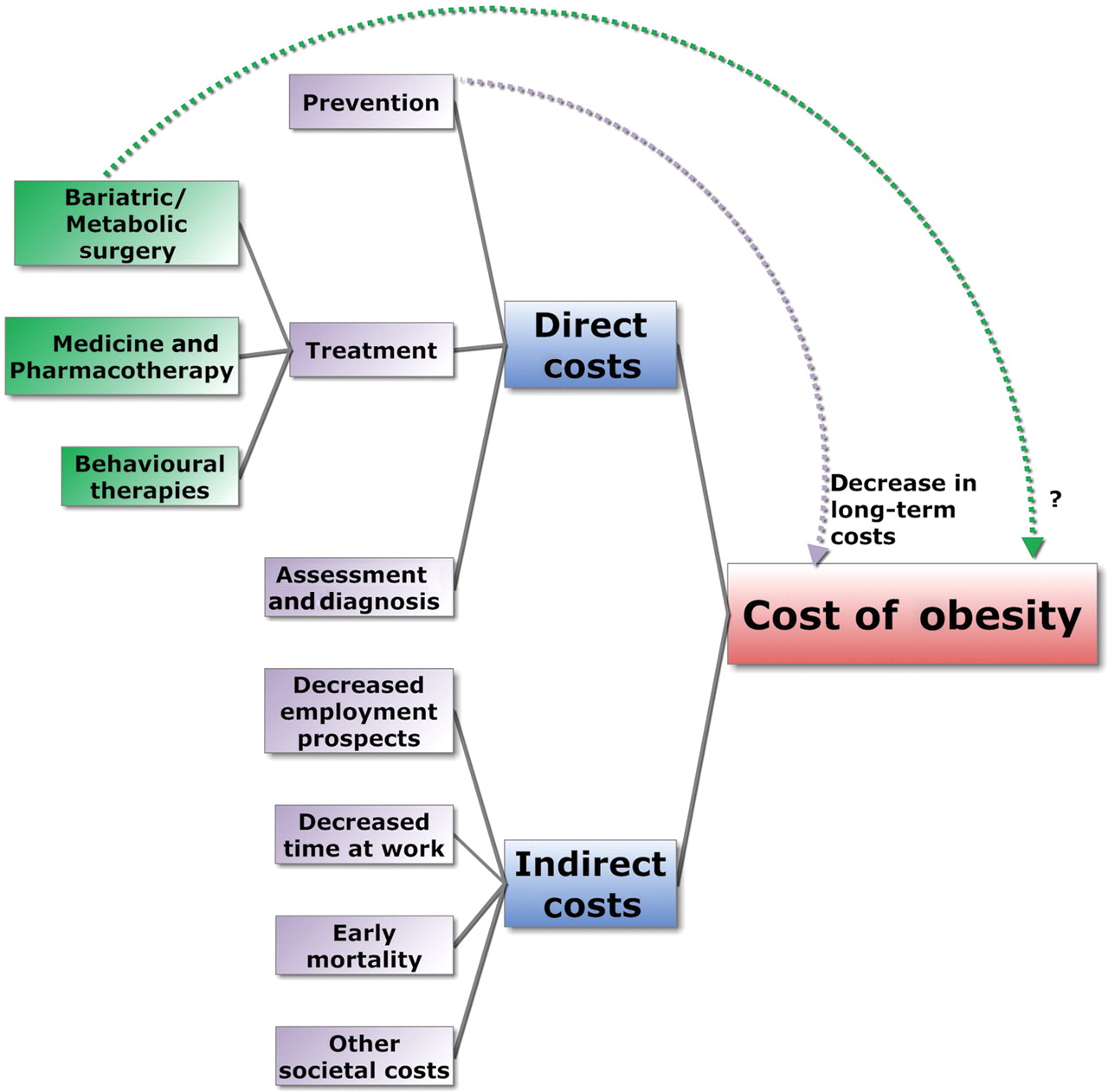
The cost of obesity can be evaluated through its direct and indirect effects on expenditure (figure 1). Direct costs include those of disease prevention, assessment, diagnosis and treatment. These include the cost of treating comorbidities such as diabetes, heart disease, hypertension, metabolic syndrome, sleep apnoea, cancer and joint degeneration. Indirect costs include lower economic output as a result of early mortality, decreased employment prospects and decreased time at work (due to illness). Furthermore, there are the added indirect expenses of larger public seating, reinforced wheelchairs and hospital beds, and even broader airplane seats.

The cost of obesity.
In the UK, the direct costs of obesity have been estimated at £4.3 billion2 compared with £2.6 billion calculated from 1998 at the National Audit Office. The broader costs across 15 European Union (EU) states have been calculated at £28 billion,14 and for 25 EU states as £34 billion per year. The addition of overweight individuals to this calculation results in an overall cost of £68 billion pounds in the EU as a result of both the obese and overweight population.15 In the USA, the direct healthcare costs of obesity have been quoted as approximately £48 billion (US$75 billion) based on the 1998 Medical Expenditure Panel Survey model. This cost focused on the direct costs of obesity and is considered an underestimate as it does not include the indirect cost of obesity or the overheads associated with the pre-obese overweight population.16
It has been estimated that the direct cost of obesity can be as high as 2.6% of all healthcare costs in the EU17 (and up to 7% worldwide),18 corresponding to 0.9% of total gross domestic product in the EU and up to 1.2–1.4% of total gross domestic product in the USA.17
The direct costs of obesity represent the ‘tip of the iceberg’ as the indirect costs of obesity also carry a considerable burden. In England alone, the National Audit Office has estimated that national obesity has resulted in 18 million sick days and 31 000 deaths each year. This corresponds to approximately 40 000 lost years of working life associated with a decreased lifespan of approximately 9 years in the obese population.14
Direct and indirect costs of bariatric surgery
Offering patients bariatric surgery requires the establishment of specialist bariatric centres with inhouse multidisciplinary expertise. This includes metabolic physicians, gastroenterologists, endocrinologists and radiologists with an interest in obesity, dieticians, psychiatrists and psychologists, respiratory physicians with an interest in sleep apnoea, specialist nurses, bariatric surgeons and anaesthetists. These tertiary clinical units integrate services with primary and secondary care to achieve a cohesive treatment system for obese patients.
Many of the clinical facilities for bariatric patients can be offered through established hospital facilities and protocols; however, obese patients have some unique needs that can incur extra healthcare costs. These include specialist equipment such as longer operating instruments, and large hospital and operating beds. Furthermore, there are the added costs of potential reoperations and revisional surgery (including the problems of surgery for loose skin).
Different health systems have different costing pathways. The start-up costs for setting up a hypothetical bariatric practice in the US utilising Medicare reimbursement for 300 cases has been quoted to be as much as £285 000 ($444 592). The total reimbursement for such a practice would be £330 500 ($516 158), resulting in £45 500 pay for surgical expertise and subsequent practice investment.19 This is one example of financial expense in a private bariatric service and does not take into account variation of operations or clinical practice. For example, the gastric bypass procedure is considered more invasive than an adjustable gastric band in view of the requirement for operative enterotomies and anastomoses. Conversely, however, the gastric band has been demonstrated as more expensive in view of the larger number of necessary postoperative follow-ups to adjust band tightness.20
In the UK, funding bodies (the outgoing primary care trusts and likely the forthcoming NHS commissioning board and General Practice Consortia) pay for each patient to undergo surgery. Although they adhere to NICE guidelines, in view of funding considerations, they focus on more stringent criteria such as NORCOM (North Derbyshire County primary care trusts, South Yorkshire and Bassetlaw Commissioning Consortium), often only supporting surgery if the BMI is >45 with comorbidities, or >50 alone. The overall treatment cost paid to each hospital trust is approximately £5000–£10 000. The operative costs in the USA and UK have decreased by approximately 25%.10 21 This may have resulted from a switch in open operative practice towards laparoscopic surgery so that there are lower overall hospital costs (through decreased patient stay and complications) although the cost of disposable instruments is now conversely higher than open surgery. There is also a significant variation in disposable costs between different laparoscopic techniques.
Several studies have listed the cost comparisons of performing bariatric surgery versus the cost of treating patients medically (table 1). Although many of these studies were cohort studies without randomisation, the majority demonstrate a clear trend in decreasing the direct costs of clinical utilisation and medication expenditure. The financial recuperation of the initial payment for surgery would occur within 1–4 years in health systems within the USA, Canada and the UK. After this time, both the cumulative cost and annual cost of postsurgical patients is lower than the treatment costs for controls. One economic model predicted that if 25% of eligible UK patients were to undergo bariatric surgery, then the national cost saving could be as high as £1295 million. The studies assessing a surgical reversal of indirect costs of obesity such as a decrease in sick days and increased working potential did not universally demonstrate a significant improvement in costs but offered a positive trend in employment related attributes.
Cost comparison of patients undergoing bariatric procedures compared with controls
Cost effectiveness of bariatric surgery
The analysis of pure financial cost advantage in relation to patient outcome does not always reflect the goal of healthcare strategies, which are ultimately aimed to preserve and improve the quality of life (QoL). There is now increasing evidence that bariatric surgery offers profound benefits not only to patient outcomes, but also QoL.34 35 Economic techniques that assess cost value in terms of particular outcomes are known as cost effectiveness analyses. A subgroup of these known as cost utility analyses consider QoL in their methodology. The outcome of a cost utility analysis is measured in terms of cost per quality adjusted life year (QALY). Traditionally, there has been a general consensus that the decisions to accept treatment modalities depend on whether the intervention offers a threshold of £20 000–£30 000/QALY36 (or $50 000 in the USA). Several studies using deterministic decision models have provided evidence that bariatric operations offer a cost per QALYS of between £2000 and £22 500 (table 2). There have been calls to increase the threshold range for national costs per QALY although the majority of bariatric economic models already offer a cost utility well within nationally agreed guidelines.37 Although surgery offers a consistent cost effectiveness, this has not yet been based on the highest levels of evidence set in the context of large scale randomised trials. As a result, the improved QoL and cost utility reported for these operations may have been derived from the selected subgroup of patients who have personally favoured or been offered surgery. Clearly there is an increased need for larger scale, better designed robust trials to formulate economic cost effectiveness models. These should include enhanced evidence regarding the cost effectiveness of these procedures on decreasing the risk of obesity associated comorbidities such as those for diabetes, cardiovascular disease, sleep apnoea and even cancer.4,–,7 38 39
Economic analysis of bariatric procedures
Limitations of current studies
Although many of the current economic models offer some important information regarding bariatric operations, they also carry several limitations. These derive from the absence of experimental evidence, the lack of like-with-like comparisons and the high level of heterogeneity and variation in current studies. Future studies will require increased precision to enhance the robustness of current models in order to decrease the uncertainty of current economic predictions. Calculating the surgical risk and costs of bariatric surgery are not dissimilar to that performed for screening in vascular disease or the risk of cerebrovascular accident/death after carotid surgery.49 50 In such cases, prospect economic models should define cost per QALY in relation to an acceptable postoperative mortality or morbidity.
Furthermore, there is an ongoing argument by obesity specialists that the existing economic analyses of obesity and bariatric surgery represent an example of a tendency to ‘medicalise’ society and its problems and challenges. Obesity is considered in an unquestioning way to be a disease that requires assessment, diagnosis and treatment, and that this conceptualisation of obesity does not give sufficient ‘front end’ analysis to the nature of obesity, related causal pathways and potential solutions. Future economic models require an increased depth of analysis to consider obesity in its broadest sense.
Conclusion
The progressing avalanche of global obesity will continue to challenge healthcare systems despite the worldwide necessity to reduce healthcare costs. Bariatric surgery is a successful intervention in the arsenal of obesity treatments, offering successful weight loss, decreased healthcare risks and in some cases bionic effects.38 Based on longitudinal trials and case series, bariatric surgery demonstrates powerful cost savings through direct cost comparisons and cost effectiveness studies. There is however a clear requirement to formulate economic models based on the highest levels of evidence, including well designed multicentre randomised control trials. Future studies should also incorporate high precision cost–benefit analyses to equip policy makers and clinicians with advanced decision making guidance that should increasingly incorporate patient focused outcomes such as patient reported outcome measures. The future for the management of obesity will continually require a strong preventive element; nevertheless, bariatric surgery can increasingly offer successful disease resolution and cost–benefit for an increasing proportion of obese, overweight and metabolically disordered patients. This will most likely increase in view of the continual evolution of operative techniques that currently include single incision laparoscopic surgery, endoscopic bypass procedures (such as the EndoBarrier system), transoral gastroplasty (such as the TOGA System) and the newer intragastric balloons. The cost effectiveness of bariatric surgery can result in an increased number of cases with commensurate cost savings (figure 2). The length of time for which bariatric procedures can be favoured will however depend on our ability to develop safer, cheaper and more efficacious antiobesity alternatives.

{kind=link}
{kind=link}
Hypothetical projection of the cost–benefit of bariatric surgery to UK society over 20 years.
References
Footnotes
-
Funding The authors are grateful for support from the Wellcome Trust and the NIHR Biomedical Research Centre Funding Scheme.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.