Article Text

Statistics from Altmetric.com
Inflammatory bowel disease free papers
001 AMPLIFICATION OF TOLL-LIKE RECEPTOR SENSITIVITY BY MURAMYL DIPEPTIDE IS IMPAIRED IN CROHN’S DISEASE ASSOCIATED NOD2 MUTATIONS
D. A. van Heel1, S. Ghosh1, M. Butler1, K. A. Hunt1, A. Lundberg1, T. Ahmad2, D. P. B. McGovern2, C. Onnie3, K. Negoro2, S. Goldthorpe2, B. M. J. Foxwell1, C. G. Mathew3, A. Forbes1, D. P. Jewell2, R. J. Playford1.1Imperial College; 2University of Oxford; 3GKT School of Medicine
Introduction and Aims: Both NOD2/CARD15 alleles are mutated in about 15% of Crohn’s disease patients, but functional effects remain unclear. Most studies have been performed in transfected cell lines, which may not reflect function in primary human cells, particularly interactions with toll-like receptor (TLR) pathogen recognition pathways.
Methods: Peripheral blood mononuclear cells (PBMC) were cryopreserved from wild type controls (n = 7), NOD2 1007fs/1007fs (n = 4), 908Arg/1007fs (n = 4), 702Trp/1007fs (n = 6), 702Trp/702Trp (n = 5). Cells were stimulated for 22 hours with muramyl dipeptide (MDP, 1–1000 nM) and/or synthetic/ultra pure ligands to TLRs 1/2, 3, 4, 5, 2/6, 7/8, 9. In some cases, cells were further purified by immunomagnetic beads. Cytokines were analysed by ELISA, and by multiplex protein arrays.
Results: In wild type PBMC, MDP induced little TNFα and IL-1β but strong IL-8 secretion (from B cells, T cells, and monocytes), and markedly upregulated TNFα and IL-1β secretion by all TLR ligands. MDP/TLR ligand synergy was also evident for IL-1α, IL-4, 6, 10, 12, and GM-CSF. In all common Crohn’s NOD2 double mutant genotypes, these effects were profoundly impaired at low nanomolar MDP doses.
Conclusion: In human Crohn’s disease, there are defects in cross talk between the NOD2/TLR pathways and NOD2/IL-8 driven neutrophil recruitment. The current human data are in contrast to recent mouse findings (Watanabe et al. Nat Immunol 2004) where micromolar MDP doses downregulated NOD2 knockout splenocyte TLR2 responses. Our data provide the basis for a rapid diagnostic test of NOD2 functional deficiency. NOD2 activation appears to prime the immune system rather than elicit a proinflammatory response. We propose that absence of an “MDP danger signal” in Crohn’s disease may cause failure of early immune pathogen clearance, and lead to the later abnormal adaptive immune responses to bacterial antigens seen in Crohn’s disease patients.
002 RESPONSE OF MONOCYTES TO MDP IN CROHN’S DISEASE: EFFECT OF NOD2 MUTATIONS
T. A. Chalmers-Watson, A. Bromfield, M. Abeya, S. Keshav.Royal Free & University College Medical School, Pond Street, London, UK
Introduction: Crohn’s disease is characterised by an abnormal inflammatory response, potentially triggered by components of enteric bacteria, in genetically susceptible individuals, and mutations in the NOD2 gene are strongly associated with ileal Crohn’s disease. Peripheral blood monocytes, a key component of the innate immune system, express the highest levels of NOD2 and we recently showed that NOD2 is also constitutively expressed by epithelial Paneth cells. Muramyl dipeptide (MDP), a component of bacterial peptidoglycan (PGN), is the putative ligand for NOD2. MDP primes subsequent responses to LPS & PGN in murine and human monocytic cell lines, although this effect has not been well documented in primary monocytes.
Aim: Our aim was to study the effects of inherited mutations in the NOD2 gene on monocytic responses to bacterial components.
Methods: Monocytes from healthy controls, and patients with Crohn’s disease who were wild type, heterozygous, or homozygous with regard to the three common disease-causing mutations in the NOD2 gene were isolated by Ficoll gradient centrifugation. Cells were stimulated with bacterial products in vitro, with and without prior priming with MDP. The transcription of selected cytokines was determined by real time RT-PCR.
Results: TNFα and IL-1β mRNA expression was induced by PGN, MDP, and lipopolysaccharide (LPS) and responses to PGN and MDP were significantly reduced in monocytes from patients with Crohn’s disease carrying NOD2 mutations. The expression of other cytokines, such as TGFβ, was not affected. Although responses to MDP were relatively modest compared with LPS, priming with MDP significantly altered the subsequent cytokine response to stimulation with LPS. This effect could explain how mutations in the NOD2 gene can have profound pathological effects, while MDP, the putative ligand for NOD2, has relatively weak proinflammatory activity by itself.
003 PREVALENCE OF VIRULENCE GENES IS INCREASED IN MUCOSAL POPULATIONS OF ENTEROCOCCUS FAECALIS IN ULCERATIVE COLITIS
E. Furrie, K. Blackett, S. Macfarlane, A. Fite, J. H. Cummings, G. T. Macfarlane.Microbiology and Gut Biology Group, University of Dundee, Ninewells Hospital and Medical School, Dundee DD1 9SY, UK
Introduction: Ulcerative colitis (UC) is a relapsing inflammatory disease of the colon with unknown aetiology. We have previously found greatly increased numbers of culturable enterococci (predominantly Ent faecalis) on mucosal surfaces in UC patients. Fluorescent in situ hybridisation of biopsies by an Ent faecalis 16S rRNA specific probe illustrated mucosal overgrowth in UC. It has been proposed that Ent faecalis in UC expresses surface proteins that allow receptor mediated adhesion to host epithelial cells.
Aims: To determine the prevalence of six Ent faecalis virulence genes in UC mucosa versus healthy controls.
Methods: Quantitative real-time PCR (qrtPCR) assays have been developed for enterococcal specific determination and their virulence/adhesion factor genes, aggregation substance (Agg), enterococcal surface antigen (Esp), Ace, enterococcal stress protein Gls-24, gelatinase (GelE), and SprE. Thirteen UC and 16 normal rectal biopsies were studied. Biopsy size is normalised for all samples by GAPDH levels. Virulence gene prevalence is normalised for numbers of Ent faecalis.
Results: Using qrtPCR to quantitate Ent faecalis colonisation of rectal mucosal surfaces, it was found that the control samples had consistently higher levels of DNA specific for Ent faecalis 16S genes. On further analysis the prevalence of the virulence factors Esp, SprE, and GelE were significantly increased in the enterococci of the rectal mucosa in UC when compared with healthy controls (p = 0.0133, 0.0103, and 0.0133 respectively). Levels of Agg, Ace, and Gls-24 were not significantly different (p = 0.0565, 0.7985, and 0.0565 respectively).
Conclusion: Although numbers of Ent faecalis are reduced in UC mucosa as assessed by a molecular technique, their potential to cause disease is enhanced by a significant increase in virulence factors involved in cell attachment and disruption.
004 MICROBIAL MANNAN SUPPRESSES KILLING OF CROHN’S DISEASE MUCOSA-ASSOCIATED E COLI BY MACROPHAGES: A POSSIBLE PATHOGENIC MECHANISM FOR CROHN’S DISEASE
C. M. Mpofu, J. M. Rhodes, B. J. Campbell, C. A. Hart1, S. W. Edwards2.Department of Medicine, 1Department of Microbiology, and 2School of Biological Sciences, University of Liverpool, Liverpool L69 3BX, UK
Background: Crohn’s disease (CD) patients commonly have serum antibodies (ASCA) to an oligomannan present in baker’s yeast (Saccharomyces cerevisiae) and some other microbial cell walls. We speculated that such mannans might induce a defect in phagocyte bacterial killing similar to that produced by NOD2 mutations. We previously reported that oligomannan inhibits the phagocyte respiratory burst. We have now assessed the effect of mannan on the intracellular killing of CD associated adhesive and invasive Escherichia coli by monocytes and monocyte derived macrophages (MDM).
Methods: Human venous blood mononuclear cells were purified using PolymorphPrep. Monocytes were isolated by adherence to plastic (2 hours). MDM were derived by culturing monocytes for 5–7 days in supplemented RPMI medium. Suspended mononuclear cells (1×106/ml), adherent monocytes, and adherent MDM were cultured with a CD associated adherent and invasive E coli HM605 (
) , control E coli ATCC259222, or Staphylococcus aureus (Oxford strain), in the presence or absence of S cerevesiae mannan (1 mg/ml). Viable bacteria were measured by plate counting after 2 hours’ incubation with cells.
Results: The CD E coli were better able than the control ATCC259222 strain to survive within adherent monocytes: 36% median survival at 2 hours (range 6–57) compared with 1% (0–4; p = 0.03). Addition of mannan had no effect on the control strain but markedly increased survival of the CD E coli at 2 hours (n = 10, mean increase 404.7% +/−SE 217.7, p = 0.01). Mannan similarly increased survival of the CD E coli within MDM (n = 6, mean increase 267.7% +/− SE 115.1, p = 0.001) but had no effect on survival within suspended non-adherent monocytes. Mannan had less effect on survival of S aureus.
Conclusion: Microbial mannan significantly impairs killing of CD associated invasive E coli by adherent monocytes and adherent monocyte derived macrophages. These results are in keeping with Crohn’s disease occurring as the result of either a genetic (NOD2) or acquired (mannan derived) defect in the ability to kill bacteria which enter the cytoplasm of macrophages, such as the mucosa associated invasive E coli.
005 P-GLYCOPROTEIN AND GLUCOCORTICOID RECEPTOR EXPRESSION IN HLA-B27 TRANSGENIC RAT COLON
F. M. Moodie1,2, B. F. Qian3, L. A. Dieleman3, J. R. Seckl2, R. B. Sartor3, J. Satsangi1.1Gastrointestinal and 2Endocrinology Unit, University of Edinburgh, Western General Hospital, Edinburgh, UK; 3Center for Gastrointestinal Biology and Disease, University of North Carolina, Chapel Hill, NC, USA
Introduction: HLA-B27 transgenic (TG) rats develop intestinal inflammation in specific-pathogen free environments (SPF), but not in germ free (GF) conditions. The mdr1a protein (P-glycoprotein (P-gp)) is thought to play a protective role in the intestine and is implicated in the detoxification of xenobiotic compounds from the intestine. GR is involved in the transcription of anti-inflammatory cytokines as well as the inhibition of the proinflammatory transcription factor NFκB, and is widely expressed in the rat colonic epithelium. We studied the effect of bacteria and experimental colitis on expression of P-gp and glucocorticoid receptor (GR) expression.
Methods: Transgenic (TG) and non-transgenic (NT) rats were housed in SPF or GF environments (n = 6/group). Colons were removed and sections from caecum, proximal colon, and rectum were analysed. mRNA levels were studied by in situ hybridisation, and protein levels by western blotting.
Results: All transgenic animals in SPF conditions (TG SPF) developed colonic inflammation. mdr1a mRNA and P-gp expression were significantly reduced in the caecum, proximal colon, and rectum in diseased animals (TG SPF) compared with healthy animals in the same environment (NT SPF) (p<0.001, p<0.01, p<0.05 respectively). GR protein expression was also decreased in diseased animals, in the proximal colon and rectum but not in the caecum (p<0.001). NT animals in GF conditions were associated with reduced P-gp expression in the caecum (but not proximal colon and rectum) (p<0.05), and reduced GR expression in proximal colon and rectum (but not caecum) (p<0.001).
Conclusions: P-gp expression was significantly reduced in the inflamed colon, consistent with observations in ulcerative colitis and other genetic animal models. The reduction in GR protein expression during colitis is novel and requires further investigation. In the non-inflamed colon, the presence of bacteria influences expression of P-gp and GR in a site-specific manner. These data emphasise the complex gene-bacterial interaction within the colon in health and disease.
006 COMPARISON OF DEPSIPHER WITH ANNEXIN-V IN QUANTIFYING APOPTOSIS INDUCED BY INFLIXIMAB, ETANERCEPT, AND ADALIMUMAB IN CD4+ T CELLS AND PERIPHERAL BLOOD MONONUCLEAR CELLS
R. Chaudhary, M. Butler, R. J. Playford, S. Ghosh.Gastroenterology Section, Division of Medicine, Imperial College, London, UK
Background: Infliximab but not etanercept has been reported to induce apoptosis in peripheral blood and lamina propria T lymphocytes in healthy controls and Crohn’s disease patients as detected by annexin-V, which binds exposed phosphatidylserine residues in early apoptosis. More sensitive methods, such as DePsipher, detect a reduction in mitochondrial transmembrane potential following the onset of apoptosis. We compared annexin-V with DePsipher in quantifying apoptosis induced by anti-TNF therapy (infliximab, adalimumab, and etanercept).
Methods: Peripheral blood mononuclear cells (PBMC) were isolated from healthy subjects and CD4+25-T cells were obtained using negative selection. Cells were plated with anti-CD3/28 antibody in solution at 0.001 μg/ml for PBMC and 1 μg/ml for T cells. Following stimulation for 24 hours the test drug was added at a range of concentrations (or control medium). Analysis by flow cytometry was performed at 16 hours after this. 7-AAD was used as a dead cell discriminator with annexin-V and topro-3 with DePsipher.
Results: With stimulated CD4+ T cells the proportion of apoptotic cells with DePsipher was 7.51 to 10.14% compared with 1.65 to 2.74% with annexin-V (p = 0.001). After exposure to infliximab, etanercept, and adalimumab the mean proportion of apoptotic CD4+ T cells were 41.1%, 45.7%, and 45.1% with DePsipher and 23.8%, 24.4%, and 24.0% with annexin-V. PBMC apoptosis rates were between 35.1 and 49.1% with DePsipher and levels of 21.8–28.3% found with annexin-V (p = 0.001). After exposure to infliximab, etanercept, and adalimumab the mean proportion of apoptotic PBMCs was 8.6%, 8.9%, and 8.4% with DePsipher and 2.3%, 2.1%, and 2.0% with annexin-V. With both methods no significant increase in apoptosis induced by anti-TNF therapy was detected compared with stimulated cells alone.
Conclusion: DePsipher detected a greater proportion of apoptotic cells (both stimulated CD4+ T cells and PBMC) than annexin-V. However, we were unable to confirm increased apoptosis after exposure to infliximab, etanercept, or adalimumab over and above that seen after stimulation with anti-CD3/28 antibody, even with the more sensitive DePsipher assay.
007 PARENTAL SMOKING DURING PREGNANCY AND AN ATOPIC BACKGROUND PREDISPOSE TO PAEDIATRIC INFLAMMATORY BOWEL DISEASE
R. K. Russell1,3, R. V. Farhadi1, H. Drummond3, M. Wilson1, J. Satsangi3, D. C. Wilson1,2.1Department of Child life and Health, University of Edinburgh, Royal Hospital for Sick Children, Edinburgh, UK; 2Department of Paediatric Gastroenterology and Nutrition, Royal Hospital for Sick Children, Edinburgh, UK; 3Gastrointestinal Unit, Western General Hospital, Edinburgh, UK
Introduction: Environmental exposures in early life have been implicated in the aetiology of inflammatory bowel disease (IBD). Parental smoking at birth has been linked to risk of later IBD in one previous study (
. We studied various environmental risk factors in a paediatric population based case control study.
Methods: Cases were patients in whom IBD was diagnosed at <16 years and come from a comprehensive regional service. Two age and sex matched controls were recruited from the case’s GP practice. Information on subject demographics was collected, as well as family history of IBD and atopy, personal and parental smoking, breast feeding, surgery, and immunisations.
Results: 113 IBD patients were identified with case control matching in 55% (62 matched pairs). Median age at IBD diagnosis was 10.6 years. Univariate analysis demonstrated parental smoking (mother, father, or both parents) during pregnancy and at birth was more common in the parents of cases than controls 54.1% v 29.2% (p = 0.01, OR 2.87 (1.23–6.66)). Family history of asthma was more common in IBD cases than controls 29% v 13% (p = 0.03, OR = 2.76 (1.01–6.95)). In CD cases, asthma family history (p = 0.02), atopy (p = 0.05), and history of food allergy (p = 0.05) were all more common. Family history of IBD was more common in cases 27% v 9% in controls (p = 0.01, OR = 3.53 (1.28–9.68)). Hepatitis B vaccination was reported by parents to be more common in controls than cases 27.6% v 5.2% (p = 0.01).
Conclusions: This study links passive smoking in pregnancy with development of IBD in children. Passive smoking may also be a risk factor for the development of asthma/atopy or, atopy and IBD may share another common environmental or genetic factor. Modelling is underway to determine the complex interrelationship between smoke exposure, atopy, and IBD.
008 EFFECT OF SMOKING HABIT AND LOAD ON CLINICAL PRESENTATION AND PROGRESSION IN CROHN’S DISEASE AND ULCERATIVE COLITIS
M. C. Aldhous, H. E. Drummond, I. D. R. Arnott, L. Smith, J. Satsangi.Gastrointestinal Unit, Department of Medical Sciences, University of Edinburgh, Western General Hospital, Edinburgh EH4 2XU, UK
Introduction: The differential effects of smoking in IBD are well known—smoking exacerbates Crohn’s disease (CD) but appears to protect patients from developing ulcerative colitis (UC). We asked whether a dose-dependent effect of smoking exists over time and if it affects the phenotype of CD and UC.
Methods: A database of 388 CD and 457 UC patients was analysed with respect to smoking status, anatomical distribution, disease behaviour, and dates of diagnosis and latest follow up. Smoking load was calculated from number of cigarettes/day × years smoked.
Results: In CD, smoking was associated with ileal disease and non-smoking was associated with colonic disease (χ2 = 9.932, p = 0.019). Analysis of smoking load and location showed that the heaviest smokers had upper GI disease, followed by ileal involvement, and lightest smokers had colonic disease (Kruskal-Wallis, p = 0.0003). Smoking was also associated with stricturing/penetrating behaviour and again this was related to smoking load (Kruskal-Wallis, p = 0.0036). Change in disease behaviour from diagnosis to latest follow up showed more smokers developed stricturing disease (χ2 = 7.462, p = 0.024). In UC, ex-smokers at diagnosis were significantly older (median age: ex, 45.83 years; non, 30.38 years; smokers, 30.25 years, p<0.0001). In these, greater smoking load prior to quitting was inversely correlated with time to diagnosis (r2 = 0.1021, p = 0.0002). At follow up colonoscopy, more smokers had a healthy colon than non-smokers (χ2 = 14.736, p = 0.002) and this was also related to smoking load (Kruskal-Wallis, p = 0.0169). Analysis of change in disease extent from diagnosis to follow up showed that disease tended to regress in active smokers (χ2 = 7.137, p = 0.028).
Discussion: This study confirms previous observations of smoking in CD and UC, but also shows a dose-dependent effect with regard to disease location and behaviour in CD and extent in UC. Smoking appears to protect from colonic disease in CD. Common mechanisms may protect the colon from inflammation in CD and UC.
009 MORTALITY IN CROHN’S DISEASE: NO CHANGE IN 34 YEARS
C. Canavan, K. Abrams, J. Mayberry.Leicester General Hospital, Gwendolen Road, Leicester LE5 6ZP, UK
Background: The first study into mortality in Crohn’s disease was published in 1970. Since then there have been numerous studies reporting standardised mortality rates (SMR) that vary from 2.67 to 0.72. This meta-analysis is of the published literature reporting SMR for Crohn’s patients from 1970 to date.
Methods: Medline was searched (using keywords: Crohn’s disease, inflammatory bowel disease, mortality, outcome, prognosis) to identify relevant papers. References from these papers were exploded and no extra papers generated. Papers were excluded if the populations studied were used again to calculate the SMR in later papers, to avoid data replication.
Results: Only three studies report a SMR below 1.0 and only two others had a confidence interval that included 1.0. All other studies report mortality higher than is seen in the general population. Meta-analysis using a random effects model shows that the pooled estimate for SMR for Crohn’s disease patients is 1.5 (p<0.0001). Regression analysis of the data shows that the SMR for these patients has decreased slightly over the past 34 years, but this decrease is not statistically significant (p = 0.08).
Conclusion: Recently it has become accepted that mortality in Crohn’s disease is equal to that of the general population. Reassessing evidence from the original studies and conducting a meta-analysis does not show that this is the case; the mortality risk is 50% greater. The failure of SMR to change significantly for these patients over 34 years suggests that current therapy is no better at reducing mortality risk than treatment methods employed in the 1970s.

Abstract 9
010 EFFICACY AND SAFETY OF MESALAZINE 4.8 G/DAY (800 MG TABLET) COMPARED WITH 2.4 G/DAY (400 MG TABLET) IN TREATING MODERATELY ACTIVE ULCERATIVE COLITIS: ASCEND II STUDY
S. B. Hanauer1, W. J. Sandborn2, S. Katz3, M. A. Safdi4, S. D. Woogen5, L. Law6, C. Yeh6.1Division of Gastroenterology & Hepatology, University of Chicago, IL, US; 2Mayo Clinic, Rochester, MN, US; 3Long Island Clinical Research Association, New York, US; 4Great Cincinnati Gastro Association, OH, US; 5Richmond Gastro Association, VA, US; 6 P&G Pharma, Cincinnati, OH, US
Introduction: Differences exist in the management of acute ulcerative colitis (UC) between the UK and US. The UK practice uses lower daily doses of 5-ASA with a preference for steroid use in patients with active disease. An alternative to managing acute UC, more commonly employed in the US, is the use of higher doses of 5-ASA. This study assessed the efficacy and safety of 4.8 g/day mesalazine (dosed with new formula Procter & Gamble Pharmaceuticals 800 mg tablets) compared with 2.4 g/day mesalazine (dosed with 400 mg tablets of US Asacol) for the treatment of moderately active UC.
Methods: A prospective, double blind, randomised controlled trial. Patients with moderately active UC were randomised to receive either mesalazine 4.8 g/day or mesalazine 2.4 g/day for 6 weeks. The primary endpoint was the percentage of patients who achieved treatment success, defined as complete or partial response based on clinical, endoscopic, and physician assessments.
Results: 268 patients with moderately active UC received either 2.4 g/day (n = 139) or 4.8 g/day (n = 129). 254 patients were eligible for analysis. There were no statistically significant differences for any baseline characteristics between the two treatment groups. At the end of the study, success was achieved in 71.8% (89/124) of patients in the 4.8 g/day group and 59.2% (77/130) of patients in the 2.4 g/day group (p = 0.0357). The higher dose of mesalazine was not associated with an increase in severity or frequency of adverse events or meaningful changes in laboratory results.
Conclusion: In the largest published mesalazine study in acute UC, mesalazine 4.8 g/day (800 mg tablet) was significantly more efficacious than Asacol 2.4 g/day (400 mg tablet) in patients with moderately active disease. Both treatment groups showed comparable safety profiles. The use of a mesalazine 800 mg tablet facilitates treatment with a higher daily dose of 5-ASA without the need for an increased tablet load.
This work was sponsored by P&G Pharmaceuticals.
Small bowel/nutrition free papers
011 THE RELATION BETWEEN ADULT COELIAC DISEASE AND EXOCRINE PANCREATIC INSUFFICIENCY: 12 MONTH FOLLOW UP AND INTERVENTION DATA
J. S. Leeds, A. D. Hopper, S. J. Edwards, D. P. Hurlstone, M. E. McAlindon, S. Morley, D. S. Sanders.Royal Hallamshire Hospital, Sheffield, UK
Introduction: Gluten exposure is the most common reason for continuing gastrointestinal (GI) symptoms in patients with coeliac disease (CD). However we have previously reported that a proportion of patients with CD who still have GI symptoms had underlying exocrine pancreatic insufficiency. This was assessed using faecal elastase-1 (Fel-1).
Aim: To assess whether there is long term symptomatic benefit in patients with CD who have pancreatic exocrine insufficiency identified.
Patients and Method: We recruited patients from the specialist coeliac clinic. Patients were assessed for the following factors: (1) duration of CD, (2) compliance to GFD (based on antibody status), and (3) the presence of continued GI symptoms. All patients attending were invited to produce a stool sample that was assayed for Fel-1 using ELISA. Those patients with Fel-1<200 with significant diarrhoea were offered pancreatic supplementation: Creon (initially 10 000 units b.d).
Results: 209 patients were recruited into the study (55 males, median age 50.8 years) of which 31 patients had a Fel-1<200 (14.8%).
The prevalence of exocrine pancreatic insufficiency was significantly greater in CD patients with ongoing symptoms when compared to the other groups (χ2 p = 0.02). At a minimum of 12 months follow up 18/20 of the patients treated with Creon significantly improved in terms of bowel habit but only 13/46 patients with Fel-1 >200 were improved (χ2 p = <0.01). Mean weight gain 0.9 kg. Two patients found no symptomatic benefit in bowel habit but no patients had side effects with this therapy.
Conclusions: The overall prevalence of exocrine pancreatic insufficiency in CD is 14.8%. In CD patients with persistent GI symptoms, Fel-1 is of value for the assessment of exocrine pancreatic insufficiency. There is a clinical improvement for these individuals in terms of frequency of bowel habit and weight gain.
Abstract 11
012 CAPSULE ENDOSCOPY: INITIAL EXPERIENCE OF 140 CASES
D. Kar, L. Marshall, D. S. Sanders, M. E. McAlindon.Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Background: There are few published data about the use of capsule endoscopy in routine clinical practice and its effect on patient management.
Aim: To describe the clinical experience of 140 consecutive cases and the effect of capsule endoscopy on management.
Methods: Data were collected prospectively over 24 months.
Results: 140 patients (86 females; mean age 52.6 (SD 1.6) years) underwent capsule endoscopy. In five patients delayed gastric emptying meant that the capsule did not leave the stomach during the examination. One patient had the capsule removed endoscopically from the stomach 10 days later. Indications included obscure anaemia (n = 56), overt bleeding (32), suspected Crohn’s disease (28) and functional bowel disorders (14), diagnosis or assessment of coeliac disease (7), and miscellaneous others (3). In the overt bleeders, diagnoses were made in 68% (angioectasia (n = 11), active small bowel bleeding (source unclear) (n = 5), large vascular abnormalities (n = 2) and miscellaneous (n = 3)). Of the anaemia group, 51% had identifiable pathology (angioectasia (n = 14), tumours (n = 5), miscellaneous (n = 10)). Evidence of Crohn’s disease was found in 33% (n = 9) of those suspected of having inflammatory bowel disease. Interestingly, 42% of those suspected of having functional disorders had other diagnoses (Crohn’s disease (n = 2), isolated terminal ileal ulcers (n = 2), and multiple small bowel strictures of uncertain cause (n = 1)). Capsule endoscopy changed management in 36% of cases. This was mostly in the form of further investigation (endoscopy for thermal ablation, obtaining histology, or polyp removal, n = 21), but included treatment of diagnosed Crohn’s disease (n = 12), referral for laparoscopy/laparotomy (n = 9), and the use of other medications (thalidomide for angioectasia and steroids for vasculitis).
Conclusion: Capsule endoscopy has a high diagnostic rate when used to investigate occult or overt obscure gastrointestinal bleeding or suspected Crohn’s disease. The high diagnostic rate in the smaller group with suspected functional disorders may reflect referral bias. Capsule endoscopy has affected management in a third of patients.
013 ILEAL BILE ACID TRANSPORTER EXPRESSION LEVELS IN PATIENTS WITH CHRONIC DIARRHOEA
J. R. F. Walters, K. M. Chavele, V. Taylor, L. Abbott, S. Balesaria, U. Khair, N. F. Barley.Gastroenterology Section, Hammersmith Hospital, Imperial College London, UK
Background: Idiopathic (primary) bile acid malabsorption is an increasingly recognised cause of chronic diarrhoea. Loss of functional ileal tissue following surgical resection or in Crohn’s disease produces a secondary bile acid malabsorption and diarrhoea. Consequently we hypothesised that defective bile acid transporters may be found in patients with chronic diarrhoea and idiopathic bile acid malabsorption. No increase in prevalence of genetic polymorphisms has been found in ileal bile transporters but we now report changes in their levels of expression.
Methods: Ileal biopsies (4–8) were obtained at colonoscopy from patients with chronic diarrhoea and controls without diarrhoea. No patient had macroscopic or histological evidence of ileal disease, or of other causes of diarrhoea. Expression levels of RNA for ileal bile acid binding protein (IBABP) and apical sodium linked bile transporter (ASBT) were measured by Taqman quantitative RT-PCR assays. Results were normalised by comparison with expression of the housekeeping gene GAPDH.
Results: Expression levels of both ASBT and IBABP varied between patients. The median ASBT value in the diarrhoea group (n = 9) was 38% of that in controls (n = 9); median IBABP value was 35% (p<0.05 for both). In general expression of ASBT and IBABP changed in parallel.
Conclusion: These results indicate that ileal expression of these two bile transporters is reduced in many patients with chronic diarrhoea. As the changes occur in parallel, it is possible that changes in transcription factors known to regulate both genes, such as FXR or c-fos, may be implicated.
014 POST INFECTIVE BILE ACID MALABSORPTION: IS IT A LONG TERM CONDITION?
S. Menon, B. J. M. Jones.Russells Hall Hospital, Dudley, West Midlands DY1 2HQ, UK
Introduction: Post infectious bile acid malabsorption comprises a group of patients with a history of an episode of acute gastroenteritis triggering chronic diarrhoea. Terminal ileal dysfunction, which develops as a result, causes bile acid malabsorption. We sought to identify the long term outlook of this group of patients.
Methods: We examined the records of 140 patients with 75SeHCAT results <10% (one week retention). Patients with a diagnosis of post infective bile acid malabsorption were identified. The frequency of diarrhoea and the response to bile acid sequestrants were noted by observations recorded during outpatient visits.
Results: Twenty five patients (13 females, 12 males) had a diagnosis of post infective bile acid malabsorption established after extensive investigations. Three patients had Campylobacter and one patient had Shigella sonnei isolated from stool samples during their original episode of gastroenteritis. Colestyramine was used to treat diarrhoea with the mean frequency of diarrhoea decreasing from 7.8 to 1.9 (95% CI 2.5 to 9.4), p = 0.001; t test. The mean colestyramine dose decreased from 8.2 g/day to 5.4 g/day (95% CI 0.7 to 4.9), p = 0.005; t test. 18/25 (72%) patients had a successful resolution of their diarrhoea on colestyramine and have continued it to date. The mean duration of outpatient follow up was 1.84 years (range 1–5 years). One patient developed ulcerative colitis subsequently. There were no hospital admissions related to diarrhoea and there was no mortality in this group of patients. B12 deficiency did not develop in any patient.
Conclusion: The overall long term outlook of this group of patients is excellent. We have demonstrated the chronic nature of this condition as evidenced by the continued requirement of colestyramine.
015 ANTI-ENDOMYSIAL ANTIBODY SEROCONVERSION PREDICTS MUCOSAL RECOVERY IN TREATED COELIAC DISEASE
S. Sonwalker, A. Clarke, S. M. Kelly.Departments of Gastroenterology and Histopathology, York Hospital, York, UK
Background and Aims: IgA anti-endomysial antibody (EmA) is a useful screening tool for coeliac disease. There is evidence to suggest it can also be used to assess dietary compliance. However, few studies have examined its role as a follow up tool and in particular assessed any correlation between EmA seroconversion to a negative result and mucosal histological recovery.
Methods: We reviewed paired EmA serology and duodenal histology on diagnosis and follow up of coeliac patients. Only patients with initially positve EmA were selected. Endoscopic duodenal biopsies were assessed using the Marsh criteria and the histopathologist (AC) was blinded as to the EmA results.
Results: Complete paired data were available on 47 patients (17 male, average age 53.6 years, range 21–82). Average repeat EmA testing interval was 9.4 months (range 2–22) and average biopsy interval 12.2 months (range 2–24).
Forty three patients (91%) seroconverted to a negative EmA. In 37 of these (86%) the repeat biopsies revealed that the duodenal mucosa had returned to normal or near normal (Marsh grade 0 or 1). The other six patients who seroconverted all showed a definite improvement from the first biopsy, of at least one Marsh grade, but did not return to normal with persistent Marsh grade 2 changes. Most clinicians would, however, accept this as a response, particularly if backed up by a clinical improvement. Four patients remained EmA positive and mucosal histology remained abnormal with persistent grade 3 changes.
Conclusion: These results demonstrate an excellent correlation between EmA seroconversion and histological mucosal response. This study suggests that EmA seroconversion is a useful follow up tool that could replace repeat duodenal biopsies in the routine management of coeliac disease.
016 REPARATIVE PROPERTIES OF A COMMERCIAL FISH PROTEIN HYDROLYSATE PREPARATION
A. J. FitzGerald, P. S. Rai, T. Marchbank, G. W. Taylor1, S. Ghosh, B. Ritz2, R. J. Playford.Department of Gastroenterology and 1Department of Proteomics, Imperial College, Hammersmith Hospital Campus, Du Cane Road, London W12 0NN, UK, 2Department of Bioscience and Biotechnology, Drexel University, Philadelphia, PA, USA
Background: A partially hydrolysed and dried product of pacific whiting fish is currently marketed as a health food supplement to support “intestinal health”. However, there has been only limited scientific study regarding its true biological activity. We therefore tested its efficacy in a variety of models of epithelial injury and repair.
Methods: Effects on proliferation were determined using [3H] thymidine incorporation into epithelial rat intestinal RIE-1 and human colonic HT-29 cells. Effects on restitution (cell migration) were analysed using wounded HT29 monolayers and its ability to influence gastric injury analysed using a rat indomethacin-restraint model. Partial characterisation of bioactive agents was performed using mass spectroscopy, HPLC, and gas chromatography.
Results: Both cell proliferation and cell migration were increased by about threefold when added at 1 mg/ml (p<0.01). Gastric injury was reduced by 59% when gavaged at 25 mg/ml (p<0.05), results similar to using the potent cytoprotective agent; EGF at 12.5 μg/ml. The vast majority of biological activity was soluble in ethanol, with glutamine in its single, di-, and tripeptide forms probably accounting for about 40% of total bioactivity seen. Fatty acid constituents may also have contributed to the cell migratory activity.
Conclusions: Fish protein hydrolysate possesses biological activity when analysed in a variety of models of injury and repair and could provide a novel, inexpensive approach for the prevention and treatment of the injurious effects of non-steroidal anti-inflammatory drugs and other ulcerative conditions of the bowel. Further studies appear justified.
017 KHAT (CATHA EDULIS) SUPPRESSES APPETITE BUT HAS NO EFFECT ON GHRELIN OR PEPTIDE YY LEVELS
C. D. R. Murray1,2, C. Le Roux2, M. Ghatei2, A. V. Emmanuel1,2, I. M. Murray-Lyon2.1St Mark’s Hospital, Harrow; 2Imperial College of Science, Technology and Medicine, London, UK
Background: The leaves of the Khat plant are chewed in the Yemen and parts of East Africa for their pleasurable effects. Chewing releases several sympathomimetic alkaloids, slowing gastric emptying and decreasing appetite, through unknown mechanisms. Plasma ghrelin levels increase with hunger and decrease immediately post-prandially. Peptide YY is released following a meal and exogenous administration decreases appetite. Both these gut derived peptides may have a role in hunger and satiety. It is not known whether the anorexigenic effects of khat are mediated through changes in these gut peptides.
Methods: Six habitual male (median age 40 years, range 36–56) khat chewers attended on two separate occasions for a period of three hours during which they chewed either khat leaves or lettuce after a minimum 6 hour fast. Mean arterial blood pressure (MAP) and pulse rate (PR) were monitored throughout. Blood samples were taken at 0, 30, 60, 120, and 180 minutes and analysed for PYY and ghrelin levels. Subjective assessment of appetite, hunger, and fullness were assessed with standardised description anchored visual analogue scores at the same time as blood testing. Statistical analysis was by ANOVA.
Results: The mean baseline level of ghrelin was 398 pmol/l, and of PYY was 35 pmol/l, compatible with pre-meal levels. Chewing lettuce had no effect on ghrelin or PYY levels and had no effect on subjective feelings of hunger, appetite, and satiety (p>0.05). Chewing khat also had no effect on ghrelin or PYY levels (p>0.05), although it significantly decreased subjective feelings of hunger and appetite and increased fullness (p<0.01). Khat, not lettuce, significantly increased PR and MAP (p<0.05).
Conclusions: Chewing khat decreases subjective feelings of hunger and appetite, increases fullness and results in heightened sympathetic tone. However khat has no effect on ghrelin or PYY levels. This raises the possibility that the anorexigenic effect of khat is mediated through central sympathomimetic mechanisms, independent of these peptides.
018 A DOUBLE BLIND TRIAL OF IMMUNONUTRITION VERSUS ISOCALORIC FEEDS ON SEVERE ACUTE PANCREATITIS
C. B. Pearce1, S. A. Sadek2, A. M. Walters2, S. S. Somers2, S. K. Toh2, T. Johns2, H. D. Duncan1.1Department of Gastroenterology, 2Department of Surgery, Queen Alexandra Hospital, Portsmouth, UK
Introduction: Early enteral feeding is thought to be of benefit in severe acute pancreatitis (SAP). Although immunonutrition in critically ill intensive care patients is clinically promising, there are few trials that investigate the nature and mechanism of benefit in patients with SAP.
Aims: To investigate the benefit of enteral immunonutrition over isocaloric control feeds in patients predicted to develop SAP.
Methods: A double blind trial of a prototype enteral feed containing glutamine, arginine, omega-3 fatty acids, tributyrin, antioxidants, and micronutrients versus an isocaloric isonitrogenous control feed in patients predicted to develop SAP was undertaken. Patients with biochemical and clinical evidence of acute pancreatitis and an APACHE II score ⩾8 were enrolled and fed via nasojejunal tube until oral feeding was possible. Patients were studied over the first 4 days from admission and the C-reactive protein (CRP) and urinary carboxypeptidase B activation peptide (CAPAP) were used as markers of systemic inflammation and pancreatic necrosis respectively.
Results: Thirty one patients were recruited, 15 received study and 16 control feed. There were large differences in baseline CRP and CAPAP values. Mean CRP values increased in the study group in the first 4 days (130.4 to 214.2 mg/l) and decreased in the control group (100.7 to 76.5 mg/l) (p = 0.0357). Over the same period, the mean CAPAP decreased in both the study and control groups (77.4 to 6.6 and 22.4 to 0.34 nmol/l respectively), but decreased significantly more in the study group (p = 0.0084). There were three deaths in the control group and no deaths in the study group (p = NS).
Comments: A significant rise in CRP with a reduction in CAPAP has not previously been described in clinical trials in SAP. This raises the possibility that the systemic inflammatory response in SAP may be protective against pancreatic necrosis, contrary to current dogma. This phenomenon is worthy of further investigation.
019 A ROLE FOR TNF-α IN IRON METABOLISM
A. Laftah, N. Sharma, M. J. Brookes, S. Hughes, T. Iqbal, C. Tselepis.Division of Medical Sciences, University of Birmingham, UK
Background: Iron is essential in a plethora of metabolic processes, catalysing key reactions involving energy metabolism and DNA synthesis. However, an excess of body iron can lead to catastrophic consequences as highlighted by hereditary haemochromatosis and carcinogenesis. Moreover, as iron is required for the growth and virulence of micro-organisms its control is important in maintaining host immunity against bacterial infections. Thus the absorption of iron is a tightly regulated process. We have previously demonstrated that the cytokine TNF-α can modulate iron absorption in small bowel cell line and ex vivo models by modulating both expression and localisation of iron transporter proteins including DMT-1 and IREG-1. In this regard it is the aim of this study to address whether TNF-α can induce similar effects in a whole organism.
Method: Six to eight week old male CD1 mice were injected either with saline (control) or 10.0 ng of recombinant mouse TNF-α. Blood and tissue samples (liver, spleen, and duodenum) were collected either at 3 or 24 hours. mRNA and protein expression for DMT-1, IREG-1, ferritin, and hepcidin was determined by real-time PCR and western blotting respectively. Localisation was determined by immunohistochemistry. Serum iron levels were determined by the Department of Biochemistry, City Hospital, Birmingham.
Results: Consistent with our previous findings TNF-α rapidly (3 hours) induced duodenal mRNA expression of DMT-1, IREG-1, and ferritin with expression returning to baseline by 24 hours. Interestingly liver hepcidin mRNA expression remained unchanged. Prussian staining of the duodenum at 24 hours revealed iron loading within the enterocytes. The serum iron levels were significantly repressed at both 3 and 24 hours in response to TNF-α treatment.
Conclusions: TNF-α can modulate the expression of iron transporters, causing enterocyte iron loading. This in conjunction with TNF-α mediated iron sequestration in the reticuloendothelial system causes a decrease in serum iron levels.
020 PERCUTANEOUS ENDOSCOPIC GASTROSTOMY TUBE REMOVAL AND REPLACEMENT FOLLOWING “BURIED BUMPER SYNDROME”: THE SIMPLE WAY
P. Turner, M. Deakin.University Hospital of North Staffordshire, Stoke on Trent, UK
Many patients have PEGs for long term enteral nutrition and the “Buried Bumper Syndrome” is reported to occur following 2–6% of PEG placements. Various ways have been described of dealing with this including internal incision over the bumper with a needle knife and surgical removal.
We have been using a simple, minimally invasive way of dealing with this problem over the last four years. This method can be used to change a PEG with a buried bumper on a routine endoscopy list under sedation.
-
Initially the PEG tube is cut off approximately 5 cm from the skin after removal of all clips.
-
A pair of ERCP stent grasping or toothed biopsy forceps are inserted via the tube and, despite the bumper not being visible endoscopically, the forceps will always appear through the mucosa.
-
A snare is passed via the scope, caught in the stent grasping forceps and brought out via the PEG tube.
-
The tube is now split with a pair of scissors as deeply as possible into the PEG exit site.
-
The snare is led out through the split tube with the wire of the tube encircling the tube, pushed as far down the tube as possible into the exit site and the snare closed.
-
This last step ensures that gentle traction now applied will be along the PEG tube. Withdrawing the scope will now cause the bumper to concertina and to pop through the mucosa.
-
A PEG can now be replaced at a separate site, although we have successfully used the same tract by including the string of the new PEG within the snare, enabling removal and replacement at the same time.
-
As a track exists this does not have to be pulled tight with the skin, thus preventing further problems.
Liver free papers
021 ENDOSCOPIC LIGATION COMPARED WITH PROPRANOLOL AND COMBINED ISOSORBID MONONITRATES (ISMN) AND PROPRANOLOL TO PREVENT RECURRENT VARICEAL BLEEDING: A PROSPECTIVE RANDOMISED TRIAL
G. Shiha, A. Menesy, S. Seef, A. El Fakhry, E. Abdel Khalek, N. Khalil.Internal medicine department, ElMansoura faculty of medicine, ElMansoura, Egypt
Background: After an attack of bleeding from oesophageal varices, patients are at high risk of recurrent bleeding and death. We compared endoscopic ligation and medical therapy with propranolol ± isosorbid mononitrate (ISMN).
Methods: We randomly assigned 181 patients with cirrhosis who were hospitalised with oesophageal variceal bleeding to receive treatment with endoscopic ligation (61 patients), propranolol (60 patients), and combined ISMN + propranolol (60 patients) during the study period to prevent rebleeding. The primary end points were recurrent bleeding, complications, and death.
Results: After a median follow up period of 12 months, recurrent bleeding developed in 27.8% of patients in the endoscopic ligation group, 41.6% of the combined group, and 51.6% of the propranolol group (p<0.03). Recurrent bleeding from oesophageal varices occurred in 13.1% in the endoscopic ligation group, 35% of the combined group, and 46.7% of propranolol group. Eight patients in the endoscopic ligation group died (13%), nine patients in the combined group (15%), and 11 patients in the propranolol group 18% (p = 0.72).
Complications occurred in 18 patients in the endoscopic ligation group, 22 in the combined group, and 20 patients in the propranolol group. The multivariate Cox analysis indicated that the treatment was the only factor predictive of rebleeding.
Conclusions: Endoscopic band ligation is more effective than propranolol and combined ISMN and propranolol for the prevention of recurrent bleeding from oesophageal varices and is associated with a lower rate of complications.
022 RELATION BETWEEN ALBUMIN SYNTHESIS, SERUM ALBUMIN LEVELS, AND SYSTEMIC INFLAMMATION IN PATIENTS WITH DECOMPENSATED LIVER DISEASE
R. Hamid1, N. Joshi1, D. C. McMillan2, T. Preston3, C. Slater3, A. J. Stanley1.1Department of Gastroenterology and 2University Department of Surgery, Royal Infirmary, Glasgow G31 2ER and SUERC, East Kilbride, Glasgow G75 OQF, UK
Background: The characteristic low serum albumin seen in patients with decompensated liver disease is an important predictor of outcome and is incorporated into the widely used Child-Pugh scoring system for assessment of disease severity. This has traditionally thought to be due to reduced liver synthesis, but recently work has suggested that some of these patients have systemic inflammation with increased catabolism. This suggests that albumin synthesis may be normal or even increased in these patients. The aim of this study was to examine the longitudinal relation between albumin synthesis rate, and circulating concentrations of albumin and C-reactive protein (CRP) in patients with decompensated liver disease during periods of hospitalisation and recovery.
Patients and Methods: Eight patients (median age 48 years; median bilirubin 143 μmol/l) admitted with decompensated alcohol related liver disease and with no evidence of sepsis or GI bleeding were studied. Patients underwent measurement of the albumin fractional synthetic rate (FSR) using a validated phenylalanine flooding dose technique. Routine biochemical parameters of liver function were also measured. Measurements were repeated following clinical improvement (4–6 weeks). The study was approved by the local ethics committee.
Results: Baseline and follow up results are shown in the table.
Abstract 22
Conclusion: During follow up there was a significant improvement in serum albumin concentration and Child-Pugh score, in addition to a reduction in the systemic inflammatory response as evidenced by C-reactive protein concentrations. However, there was no alteration in fractional synthetic rate of albumin over the study period. The results suggest that the low serum albumin concentrations in these patients are secondary to inflammatory related albumin catabolism, not reduced liver synthesis.
023 HCV-SPECIFIC CELLULAR IMMUNE RESPONSES IN SUBJECTS EXPOSED TO BUT UNINFECTED BY HCV
M. Metzner, A. Houldsworth, A. G. Demaine, E. Kaminski, M. E. Cramp.Gastroenterology and Liver Unit, Department of Immunology, Derriford Hospital, Hepatology and Molecular Medicine Research Groups, Peninsula Medical School, Plymouth, UK
Background: Intravenous drug users (IDUs) constitute the UK’s largest group of HCV infected subjects, and it is estimated that around 70% of IDUs are HCV antibody (HCV Ab) positive. IDUs who are uninfected despite years of intravenous drug use may be resistant to HCV infection.
Methods: To identify potential correlates of HCV resistance, we studied HCV-specific T cell responses in four groups: (1) 49 HCV Ab negative and HCV RNA negative IDUs, at high risk of HCV infection; (2) 14 HCV Ab positive, HCV RNA negative patients who had spontaneously cleared HCV infection; (3) 15 HCV Ab positive, HCV RNA positive patients, and (4) 29 healthy volunteers. Peripheral blood mononuclear cells were isolated and tested for HCV-specific cellular responses using recombinant HCV structural and non-structural antigens by direct ex vivo IFNγ ELIspot analysis.
Results: See table.
Abstract 23 Mean (SD) HCV specific IFNγ response per 106 PBMCs
Conclusion: IDUs at high risk of HCV infection who remain HCV seronegative display similar cellular response to those who have spontaneously cleared HCV viraemia. The presence of HCV-specific T cell responses to a range of HCV antigens in the absence of demonstrable infection confirms HCV exposure has occurred and raises the possibility that these responses may protect from chronic infection.
024 TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT FOR PORTAL VEIN THROMBOSIS WITH AND WITHOUT CAVERNOMATOUS TRANSFORMATION
M. Senzolo, J. Tibballs1, E. Cholongitas, C. K. Triantos, A. K. Burroughs, D. Patch.Liver Transplantation and Hepatobiliary Unit, 1Department of Radiology, Royal Free Hospital, London, UK (introduced by A. K. Burroughs)
Introduction: Portal vein thrombosis (PVT) occurs in the context of local and systemic prothrombotic tendencies, as well as in patients with cirrhosis. The major consequence is portal hypertension. Transjugular intrahepatic portosystemic shunt (TIPS) could be an effective treatment for PVT, but its role in cavernomatous transformation is unclear.
Aim: To evaluate feasibility and efficacy of TIPS treatment of PVT with or without cavernomatous transformation.
Material and Methods: All patients referred for TIPS placement who had PVT were evaluated retrospectively for success rate, complications, TIPS patency, and clinical progression.
Results: TIPS was attempted in 23 patients (15 male; 8 female) with PVT between 1994 and 2004. Indications were: acute PVT (3), variceal bleeding (13), refractory ascites (4), portal biliopathy (2), and Budd Chiari disease (1). Ten patients were known to have liver cirrhosis. TIPS was successful in 15 (65%). Eighteen patients had complete PVT in which seven failed TIPS placement. Cavernomatous transformation was seen in eight patients and TIPS was successfully placed in five. Eight patients were treated by additional mechanical thrombectomy, while stents were deployed within the thrombus in the remaining seven, following balloon dilatation. No significant complications occurred during the procedure. The mean follow up was 13.4 months (range 0.3–60). A total of four stent revisions were required in four patients. Of the 15 patients with TIPS, three have undergone liver transplantation, one died, and most showed amelioration of Child-Pugh score. A higher rate of bleeding and death was seen in the group of patients with failed TIPS placement.
Conclusions: TIPS should be considered for selected patients with symptomatic complete PVT with or without cavernomatous transformation, although the success rate is lower in the former.
025 CIPROFLOXACIN REDUCES SMALL INTESTINAL BACTERIAL OVERGROWTH AND PLASMA ETHANOL CONCENTRATION IN PATIENTS WITH NON-ALCOHOLIC STEATOHEPATITIS
A. Sajjad, M. Mottershead, W. Syn, R. Jones, S. Smith, C. U. Nwokolo.Departments of Gastroenterology and Biochemistry, University Hospital, Coventry, UK
Background: Ethanol and other byproducts of small intestinal bacterial activity may be involved in the pathogenesis of non-alcoholic steatohepatitis (NASH). The aim of this prospective study was to compare the effect of a course of ciprofloxacin on small bowel bacterial overgrowth and plasma ethanol concentration in NASH patients and healthy controls.
Methods: Twelve patients with biopsy proven NASH and 11 healthy subjects with normal ultrasound and liver function were studied before and after a five day course of ciprofloxacin 500 mg bd. Bacterial overgrowth was detected by glucose hydrogen breath test and plasma was stored and assayed for ethanol. Glucose tolerance tests were performed to detect occult diabetes. Patients and controls had a detailed medical history taken and physical examination.
Results: Mean BMI for NASH patients and controls was 32 and 25 respectively, Of six NASH patients positive for bacterial overgrowth, one remained positive after ciprofloxacin. In contrast, only one of 11 healthy controls was positive for bacterial overgrowth whose status remained unchanged after ciprofloxacin. Two subjects in each group (who were breath test negative) had detectable plasma ethanol that became immeasurable after ciprofloxacin. Glucose intolerance or non-insulin dependent diabetes was confirmed in eight of 12 NASH patients and two of 11 controls. Five of six NASH patients positive for bacterial overgrowth were either diabetic or glucose intolerant compared with three of six NASH patients who were negative for bacterial overgrowth.
Conclusions: The small bowel in NASH patients is colonised predominantly by ciprofloxacin-sensitive bacteria. Ciprofloxacin resistant bacteria colonise about 10% of normal controls. Small amounts of ethanol are present in the plasma of about 15% of NASH patients and controls, which disappear after ciprofloxacin treatment. These preliminary observations may have implications for the treatment of NASH.
026 INCIDENCE OF CANCERS FOLLOWING ORTHOTOPIC LIVER TRANSPLANTATION IN A SINGLE CENTRE: COMPARISON WITH NATIONAL CANCER INCIDENCE RATES FOR ENGLAND AND WALES
Y. H. Oo1, B. K. Gunson1, R. J. Lancashire2, K. K. Cheng2, J. M. Neuberger1.1The Liver and Hepatobiliary Unit, Queen Elizabeth Hospital, Birmingham; 2Department of Public Health and Epidemiology, University of Birmingham, Edgbaston, Birmingham, UK
Background: Liver transplant recipients may be at higher risk of developing cancers than the normal population. We have compared the incidence of de novo post-transplant tumours in a single centre with national data to determine the extent of increased cancer risk, and also to see whether increased surveillance is needed.
Methodology: 1778 adults (849 male) underwent transplantation (OLT) between January 1982 and March 2004. Patients are followed up closely for life. Observed tumour incidence was compared with expectations based on incidence rates for England and Wales, specified by age, sex, and calendar year.
Results: 141 patients (7.9%) developed new tumours post OLT (60 males). The median age at OLT was 50 years (range 16–73). The table shows observed and expected cancers with significance levels.
Abstract 26
Conclusion: There is an increased incidence of all tumours and skin and lymphoid cancers de novo post-transplant. Increased surveillance for bowel cancer may be particularly important in older patients and those with UC. There should be awareness of the high lung cancer incidence in females. The incidences of breast and cervical cancer are not higher, suggesting that increased screening is not necessary.
027 SERUM TRANSAMINASE INCREASE DURING COMBINATION OF PEGYLATED INTERFERON AND RIBAVARIN TREATMENT FOR CHRONIC HEPATITIS C
P. Thurairajah, D. Thorburn, S. Hubscher, V. Lai, K. O’Donnell, D. Mutimer.Queen Elizabeth Hospital Liver Unit, Birmingham, UK
Background: Antiviral response to pegylated interferon and ribavarin treatment (peg-IFN/riba) is typically associated with a prompt fall in serum transaminases (AST and ALT). For a proportion of patients, serum transaminases rise during treatment. Rarely, clinically significant rises and liver failure may be observed. We examined the serum transaminase response of 169 consecutive peg-IFN/riba treated hepatitis C (HCV) patients.
Methods: Serum transaminase levels recorded at baseline and weeks 1, 2, 4, +4 of treatment for 24 or 48 weeks. Transaminase increases were graded according to WHO criteria: grade 0, no value >baseline; grade 1, maximum value 1–2 × baseline; grade 2, 2–5 × baseline; grade 3, >5 × baseline; grade 4, evidence of liver failure. Pretreatment histology (n = 124) was scored in a blinded manner by SH for Ishak grade and stage and graded for steatosis according to the proportion of hepatocytes involved (grade 1, <30%; grade 2, 30–60%; grade 3, >60%).
Results: Transaminase rise was observed in 52/169 (31%) patients (44 grade 1, six grade 2, one grade 3, one grade 4) and was associated with greater pretreatment body weight (p = 0.007), more advanced histological stage (p = 0.048), and increasing severity of steatosis (p = 0.005). 25/116 (22%) without and 24/50 (48%) with transaminase rise were PCR positive at the end of treatment (p = 0.001). Six of eight (75%) patients with toxicity above grade 1 were PCR negative at the end of treatment. On multivariate analysis, steatosis grade (p = 0.01) and body weight (p = 0.002) were associated with transaminase elevation.
Conclusion: Transaminase increase during peg-IFN/riba is common and sometimes severe. The association with body weight, hepatic steatosis, and histological stage is consistent with IFN mediated induction/exacerbation of steatohepatitis which is independent of antiviral activity.
028 HYPERFIBRINOLYSIS IN CIRRHOSIS: THE ROLE OF RELATIVE PLASMINOGEN-ACTIVATOR-INHIBITOR TYPE 1 DEFICIENCY
J. W. Ferguson1, A. Helmy1, P. Dawson2, C. Ludlam2, D. J. Webb3, D. E. Newby4, P. C. Hayes4.1Departments of Hepatology, 2Haematology, Clinical Pharmacology3, and Cardiology4, University of Edinburgh, Edinburgh, UK
Background and Aims: Fibrin degradation is determined by the endothelial release of tissue plasminogen activator (t-PA) and its subsequent inhibition by plasminogen activator inhibitor type-1 (PAI-1). To maintain normal fibrinolytic balance, increases in baseline plasma t-PA concentrations are associated with compensatory increases in plasma PAI-1 concentrations. Overactivity of the fibrinolytic system (hyperfibrinolysis) occurs in cirrhosis and has been shown to correlate with the risk of variceal haemorrhage. The aims of the study were to assess the influence of basal and stimulated t-PA release in patients with cirrhosis.
Methods: Bilateral forearm blood flow and plasma fibrinolytic variables were measured in eight patients with biopsy proven alcohol induced cirrhosis, ascites, and portal hypertension, and eight age and sex matched healthy controls during infusion of bradykinin (100–900 pmol/min; endothelium dependent vasodilator that releases t-PA) followed by sodium nitroprusside (SNP 2–8 μg/min; a control endothelium independent vasodilator).
Results: Baseline plasma t-PA antigen concentrations were higher in patients (9 v 14 ng/ml; p<0.05) whereas plasma PAI-1 antigen concentrations were similar (55 v 59 ng/ml; p = NS). This resulted in an increased t-PA activity (0 v 3 IU/ml; p<0.05) and reduced PAI-1 activity (21 v 9 AU/ml; p<0.05) indicating a relative deficiency of PAI-1 in patients with cirrhosis. Bradykinin and SNP caused a dose dependent vasodilatation (p<0.001 for both) that did not differ between the two groups. Bradykinin caused a similar release of t-PA antigen (p<0.05 for both) in both patients and controls (23 v 24 ng/100 ml/min; p = NS) without affecting PAI-1 concentrations. Local t-PA activity was increased in patients following acute stimulated t-PA release (1.5 v 5 IU/ml; p<0.05). SNP caused no significant change in fibrinolytic parameters.
Conclusion: We conclude that patients with cirrhosis have a higher basal plasma t-PA activity because of a failure to increase plasma concentrations of its inhibitor, PAI-1. Furthermore, despite releasing normal amounts of t-PA acutely, higher t-PA activity remained due to the relative deficiency of PAI-1. This suggests that the pathogenesis of hyperfibrinolysis in liver cirrhosis is the result of a relative PAI-1 deficiency rather than enhanced t-PA release.
029 THE EXPRESSION OF HEPATIC HEPCIDIN AND DUODENAL DIVALENT METAL TRANSPORTER 1 ARE MODIFIED BY ETHANOL AND ACETALDEHYDE
N. Sharma1, B. Salhan1, M. J. Brookes1, B. T. Cooper2, T. H. Iqbal2, C. Tselepis1.1Department of Medical Sciences, University of Birmingham, Birmingham, UK; 2Gastroenterology Unit, City Hospital, Dudley Road, Birmingham, UK
Background: Increased iron absorption and hepatic haemosiderosis are commonly found in cirrhosis. The divalent metal transport 1 (DMT1) protein, responsible for small bowel iron absorption, is upregulated in cirrhosis. Hepcidin is a liver derived peptide and negative regulator of intestinal iron absorption. Decreased hepcidin leads to tissue iron overload, including hepatic haemosiderosis. The aim of this investigation was to determine the direct effect of alcohol on DMT1 and hepcidin expression.
Methods: Using a human small bowel model (Caco2 cells) and ex vivo culture system stimulated with ethanol and acetaldehyde (the primary metabolic product of alcohol dehydrogenase), DMT1 mRNA and protein expression were measured using real-time PCR and western blotting respectively. A human hepatoma (HepG2) cell line was stimulated with varying concentrations of ethanol and acetaldehyde, and hepcidin mRNA was measured using real time PCR. In addition mRNA was extracted from normal human liver (n = 5) and alcoholic cirrhotic liver (n = 5), and hepcidin expression was compared by real-time PCR.
Results: A significant downregulation in DMT1 mRNA was shown in both small bowel models in response to ethanol and acetaldehyde. Western blotting analysis revealed a significant repression of DMT1 protein in both small bowel models in response to acetaldehyde. Hepcidin mRNA was significantly downregulated in HepG2 cells exposed to ethanol and acetaldehyde and in alcoholic cirrhotic liver.
Conclusion: The expression of DMT1 is downregulated by the direct effect of ethanol and its metabolite acetaldehyde. The downregulation of hepcidin in HepG2 cells exposed to alcohol, and its reduced expression in alcoholic cirrhosis, is likely to account for the iron overload seen in this condition.
030 ALCOHOL DEPENDENCE SEVERITY IN ALCOHOLIC LIVER DISEASE: PREDICTIVE VALUE AND COMPARISON WITH HEAVY DRINKERS WITHOUT LIVER DISEASE
D. Gleeson, R. Francis, C. Gellion, J. Jones, M. P. Bradley, R. J. Peck.Liver Unit, Sheffield Teaching Hospitals, Sheffield, UK
Background: There are limited data on severity of alcohol dependence in patients with alcoholic liver disease (ALD). In one study (Wodak,
) , patients with ALD had relatively low alcohol dependence scores but a formal control group was not included.
Aim: Evaluation of the short alcohol dependence data (SADD) questionnaire questionnaire (
) in heavy drinkers with and without liver disease.
Methods: SADD score calculated (min 0, max 42) from questionnaire administered to two groups of heavy drinkers (>60 U/week (M) or 40 U/week (F) for >5 years) one with decompensated ALD (patients) and one with no clinical, laboratory, or ultrasound evidence of serious liver disease (controls).
Results: SADD score: (A) showed high correlations between repeat estimations in the same subject by the same (r = 0.87, n = 8) or by two (r = 0.97, n = 4) investigator(s). (B) In control subjects, was related to recruitment source: (mean (SD)) 33.5 (5.2) (n = 10) in residents of “dry” houses; 23.5 (9.6) (n = 25) in outpatient attendees at alcohol treatment units; 13.3 (10.6) (n = 36) in acute hospital attendees; 13 (9.3) (n = 19) in primary care attendees, and 9.8 (6.1) (n = 56) in non-healthcare seeking volunteers. (C) <10 and <20 in 36 (30%) and 71 (59%) respectively of 121 patients with decompensated ALD; mean was similar to that in 79 healthcare seeking controls (18.2 (11.7) v 18.6 (11.6)) but was higher in both groups than in non-healthcare seeking volunteers. (D) Correlated positively with mean weekly alcohol intake (r = 0.39 to 0.45 p<0.01) and negatively (r = −0.27 to −0.39 p<0.05) with age and duration of alcohol consumption but did not correlate with severity of liver disease. (E) Did not differ significantly in patients who remained subsequently abstinent from alcohol than in those who continued drinking.
Conclusions: Most patients with severe ALD are not severely alcohol dependent. Although showing expected relations with recruitment source and alcohol consumption, SADD score did not predict subsequent drinking behaviour in ALD patients.
Gastroduodenal free papers
031 LONG TERM STUDY OF RE-INFECTION FOLLOWING SUCCESSFUL ERADICATION OF HELICOBACTER PYLORI INFECTION
E. A. B. Cameron, G. D. Bell, L. Baldwin, K. U. Powell, S. G. J. Williams.Ipswich Hospital, Heath Road, Ipswich, Suffolk, UK
Introduction:H pylori infection is known to cause a number of diseases including peptic ulcer disease and gastric carcinoma. Successful eradication dramatically reduces recurrent ulcer disease. Re-infection rates are likely to be related to the population prevalence of infection. Small, short term studies suggest annual HP re-infection rates in excess of 1%. When we previously attempted to study re-infection rates (
) , the majority of “re-infections” occurred within the first year suggesting recrudescence rather than true re-infection. We now report what are likely to be genuine re-infection rates by studying a large cohort of patients over a much longer period.
Methods: Following eradication, patients were followed up predominantly by means of 13C and 14C urea breath test. Patients were included if at least one test was negative at 1 year or beyond. The rate of re-infection was then calculated in the follow up period beyond 1 year.
Results: Follow up was available for 2676 patients up to a maximum of 13 years post-eradication. After exclusion of patients without at least one negative test at 1 year or greater, 930 remained (mean age 56 (SD 14) years, 614 men) with 2733 years of follow up data available beyond 1 year (mean 3 (SD 2) years). 12 re-infections occurred (seven at 2 years post-eradication, two at 3 years, two at 4 years, and one at 5 years) giving a re-infection rate of 0.44% per year. The mean age of these patients was 50 years (SD 13) and nine were men. No statistically significantly difference was seen for sex or age and all 12 were white.
Discussion: Small, short term studies of H pylori “re-infection” following eradication have probably overestimated the true rate of re-infection, largely as a result of including recrudescence. We have avoided this potential bias by excluding the first year following eradication from analysis. This is the largest study of H pylori re-infection with the longest follow up described to date. Re-infection following successful eradication is a rare phenomenon. Patients clear of infection at 1 year in the UK are very unlikely to re-acquire H pylori.
032 REDUCED GASTRIC AND DUODENAL ULCER INCIDENCE WITH ESOMEPRAZOLE IN AT-RISK PATIENTS TAKING CONTINUOUS NSAID THERAPY
C. Hawkey1, R. Jones2, N. Yeomans3, J. Scheiman4, N. Vakil5, N. Talley6, G. Långström7, J. Næsdal8.1Institute for Clinical Research Trials Unit, University Hospital, Nottingham, UK; 2GKT Department of General Practice, Kings College, London, UK; 3Department of Medicine, University of Melbourne, Footscray, Australia; 4Division of Gastroenterology, University of Michigan, USA; 5University of Wisconsin Medical School, Milwaukee, USA; 6Mayo Clinic College of Medicine, Rochester, USA; 7Biostatistics; 8Med and Sci, AstraZeneca, Mölndal, Sweden
Introduction: Long term non-steroidal anti-inflammatory drug (NSAID) use can lead to gastric and duodenal ulcers (GU/DU).
Methods: 1429 patients with a chronic inflammatory condition at risk of developing ulcers (⩾60 years old and/or with history of GU/DU) were randomised into either of two placebo controlled, parallel group, multicentre studies of similar design. Patients (H pylori negative, ⩾18 years old) received placebo or esomeprazole 20 or 40 mg orally once daily for 6 months, in addition to their NSAID therapy. The primary variable was the proportion of patients without GU/DU throughout 6 months’ treatment (determined by endoscopy at 1, 3, and 6 months).
Results: Esomeprazole 20 and 40 mg significantly reduced the ulcer incidence relative to placebo (see table). The number needed to treat (NNT) to avoid one ulcer case over 6 months for patients taking esomprazole 20 and 40 mg was 9 and 8, respectively. NNTs were similar for patients taking non-selective NSAIDs (10 and 9, respectively (n = 334 and n = 326)) and COX-2-selective NSAIDs (7 and 8, respectively (n = 125 and n = 141)). Both doses were well tolerated.
Abstract 32 Life table estimates of the proportion of patients without GU/DU at 6 months (95% CI)
Conclusion: Esomeprazole prevents GU/DU development in at-risk patients taking long term NSAIDs including COX-2 selective NSAIDs.
033 IL-8–251 PROMOTER POLYMORPHISM AND RISK OF GASTRIC CANCER IN WHITE AND JAPANESE POPULATIONS
M. G. Smith1, G. L. Hold1, C. Rabkin2, W. H. Chow2, J. F. Fraumeni Jr2, N. A. G. Mowat1, T. Ando3, H. Goto3, E. M. El-Omar1.1Department of Medicine and Therapeutics, Aberdeen University, Aberdeen, UK; 2National Cancer Institute, NIH, Rockville, MD, USA; 3Nagoya University Graduate School of Medicine, Nagoya, Japan
Background: Interleukin-8 is of critical importance in the inflammatory response to Helicobacter pylori. It is a powerful chemotactic factor that induces many of the early inflammatory responses to the infection. We have recently shown that a functional promoter polymorphism (IL-8–251 A/T) is associated with an increased risk of developing the pre-malignant changes of hypochlorhydria and gastric atrophy. We have also demonstrated that carriage of the IL-8–251 A allele is associated with higher IL-8 levels and a more pronounced inflammatory response in the gastric mucosa.
Aim: To evaluate the effect of the IL-8–251 (A/T) polymorphism on the risk of developing gastric carcinoma, using case control studies from two populations of differing ethnic backgrounds.
Subjects and Methods: We used a 5′ nuclease assay to genotype the IL-8–251 A/T polymorphism in two gastric cancer case control studies: (1) a White population gastric cancer case control study consisting of 306 gastric cancer cases and 211 controls and (2) a Japanese gastric cancer case control study consisting of 237 gastric cancer cases and 98 controls. Odds ratios and 95% confidence intervals (CI) were calculated and logistic regression was used to adjust for confounding variables.
Results: Carriage of the pro-inflammatory IL-8–251 A allele in the White case control study was not associated with an increased risk of developing gastric carcinoma (OR = 1.006, 95% CI 0.7 to 1.5). No significant differences were observed when the cases were subdivided into cardia (OR = 0.811, 95% CI 0.5 to 1.3) and non-cardia gastric cancers (OR 1.173, 95% CI 0.8 to 1.8). Similarly in the Japanese population carriage of the A allele did not increase the risk of having gastric cancer (OR = 1.166, 95% CI 0.7 to 1.9).
Conclusion: Although carriage of the IL-8–251 A allele is associated with a more pronounced inflammatory response in the gastric mucosa of H pylori infected subjects and an increased risk of developing pre-malignant changes, it does not appear to alter the risk of developing the eventual outcome of gastric cancer. This applies to populations of differing ethnicity. We postulate that this polymorphism is important at an early stage in the inflammatory response to H pylori and may facilitate the action of other mediators in the development of gastric cancer.
034 COX-2 GENE POLYMORPHISMS AND ASSOCIATION WITH PREMALIGNANT CHANGES IN THE STOMACH
M. G. Smith1, G. L. Hold1, M. MacArthur1, M. McLean1, M. E. Hope1, N. A. G. Mowat1, K. E. McColl2, E. M. El-Omar1.1Department of Medicine & Therapeutics, Aberdeen University, Aberdeen, UK; 2Department of Medicine & Therapeutics, Western Infirmary, Glasgow, UK
Background: Cyclooxygenase-2 (COX-2) plays a number of key roles in carcinogenesis including stimulation of cellular proliferation and angiogenesis and inhibition of apoptosis. COX-2 expression is upregulated in gastric premalignant lesions and adenocarcinomas and this increased expression has been correlated with poor clinicopathological variables. Single nucleotide polymorphisms have been described in the COX-2 gene: three promoter polymorphisms (−197 G>C, −765 G>C, and −899 G>C), one exonic (exon 3-8C>G) and one within the 3′- untranslated region (3′ UTR T>C). All polymorphisms are potentially functional and in particular the polymorphism at position −765 affects a putative Sp1 binding site. Carriage of the COX-2–765 G allele is associated with higher COX-2 expression, and individuals with the G/G genotype have an increased risk of myocardial infarction and ischaemic stroke.
Aim: To evaluate the effect of these five described COX-2 polymorphisms on the risk of developing premalignant gastric changes.
Subjects and Methods: We used 5′ nuclease assays or PCR-RFLP to genotype the various COX-2 polymorphisms in a population of 153 healthy first degree relatives of individuals with gastric carcinoma to assess the influence of the polymorphism on pre-malignant gastric abnormalities. Of these, 66 infected subjects had hypochlorhydria/atrophy (HC/ATR), 49 infected subjects did not have the abnormalities and 53 were H pylori negative. All groups were compared with 100 population controls. Odds ratios and 95% confidence intervals (CI) were calculated and logistic regression was used to adjust for confounding variables. Genotyping was confirmed by direct sequencing.
Results: The promoter polymorphisms at positions −197 and −899 were not present in our population. The exon 3 and 3′UTR polymorphisms were present within the study group, but were not associated with an increased risk of pre-malignant changes. Homozygous carriage of the COX-2 −765 G allele was associated with an increased risk of having the pre-malignant abnormalities of hypochlorhydria and gastric atrophy, compared to heterozygotes and subjects homozygotes for the C allele (OR = 5.7, 95% CI 2.3 to 14.1).
Conclusion: The COX-2 −765 G>C polymorphism influences the development of pre-malignant changes in the stomach in H pylori infected subjects, with individuals homozygous for the high expressing G allele having an increased risk of HC/ATR. This polymorphism is a candidate for further study in relation to the inflammatory response to H pylori and the development of gastric cancer and other malignancies.
035 ACUTE EFFECT OF NAPROXEN ON THE INFLAMMATORY CELL INFILTRATE IN H PYLORI INFECTED VOLUNTEERS
M. W. James, A. M. Zaitoun, C. T. Atherton, C. J. Hawkey, J. C. Atherton.Wolfson Digestive Diseases Centre, University Hospital Nottingham, UK
Introduction: The risk of developing distal gastric carcinoma is increased by H pylori infection but reduced by unknown mechanisms with chronic ingestion of NSAIDs (
) . Neutrophils generate reactive oxygen species which may be implicated in carcinogenesis. We have previously shown that NSAIDs reduce H pylori induced interleukin-8 (a neutrophil chemokine) in vitro and animal models of H pylori infection demonstrate a reduction in neutrophils with NSAIDs. We hypothesised that naproxen would reduce H pylori associated neutrophilic infiltration in vivo.
Methods: Sixteen healthy volunteers (12 positive and four negative for H pylori infection) entered a placebo controlled, blinded crossover study of 48 hours naproxen 500 mg bd (a non-selective NSAID) on the acute and chronic inflammatory cell infiltrate in the gastric antral mucosa. Gastric mucosal biopsies taken at baseline endoscopy and 3, 12, and 48 hours after starting treatment were assessed blindly by fully quantitative histopathology. Statistical analysis was by ANOVA using SPSS.
Results: Neutrophils, lymphocytes, eosinophils, and mast cells were significantly higher in subjects infected with H pylori, with or without naproxen therapy, compared with those uninfected (p<0.0001). Mean intra-epithelial and lamina propria neutrophils in H pylori infected subjects were both significantly lower during naproxen therapy compared with placebo by 3 hours, persisting at 48 hours (p<0.05). Naproxen had no significant effect on lymphocytes, eosinophils, or mast cells in H pylori infected subjects, or on any leukocyte cell population in those without H pylori infection.
Conclusions: Acute naproxen ingestion selectively reduces H pylori associated neutrophilic infiltration in the human stomach and this may contribute to a reduction in gastric cancer risk.
Endoscopy free papers
036 MONITORING COLONOSCOPY SUCCESS RATES AND DETECTING CHANGES IN SEDATION PRACTICE USING DATA MINING AND STATISTICAL TECHNIQUES: FIGURES FROM A REGIONAL TRAINING CENTRE
A. P. Reynolds1, B. de la Iglesia1, G. D. Bell2, K. Sheikh2, V. J. Cook2, R. Tighe2.1School of Computing Sciences, UEA, Norwich, UK; 2Endoscopy Unit, Norfolk and Norwich University Hospital, Norwich, UK
Introduction: Anticipating the future needs for CRC screening, the NHS has invested £8.3 million in funding three national and seven regional endoscopy teaching centres for three years. Over the past two years our own regional unit has hosted 10 colonoscopy skills courses and involved many of our own consultant gastroenterologists (n = 7), colorectal surgeons (n = 3), and nurse endoscopists (n = 1) as faculty, as well as local SpRs, nurses, and clinical assistants as trainees. We wondered if (a) some of “what we were preaching” was actually “rubbing off” in terms of our own local practice and, if so, (b) whether this could be reflected in our unit’s colonoscopy success rates and change in sedation/analgesia practice to comply with BSG 2003 guidelines (www.bsg.org.uk).
Methods and Results: Data mining techniques (Gut 2004;Suppl III:A51) were applied to our Endoscribe database to extract the Unit’s monthly crude colonoscopy success rate as well as trends in midazolam and pethidine dosage from February 2002 to May 2004. Trends were examined both graphically (see below) and statistically.
There was a clear improvement in the unit’s caecal intubation rates (p<0.001) while midazolam dosage fell significantly (p<0.001).
Discussion: The significant improvements in our own unit’s performance since starting to run approved colonoscopy skills courses encourages us to believe the same teaching “formula” (which is being rolled out throughout the UK) should reap similar benefits nationally.

Abstract 36
037 COMPUTATIONAL COLOUR TECHNIQUES CAN SPEED UP THE VIEWING OF WIRELESS CAPSULE ENDOSCOPY IMAGES AS WELL AS DETERMINE GASTRIC AND INTESTINAL TRANSIT TIMES
M. Mackiewicz1, J. Berens1, M. Fisher1, G. D. Bell2, C. Jamieson2.1School of Computing Sciences, University of East Anglia, Norwich, UK; 2Endoscopy Unit, Norfolk & Norwich University Hospital, Norwich, UK
Introduction: A wireless capsule endoscopy (WCE) operates for about 8 hours and captures approximately 40 000 images. The images may take a doctor over an hour to assess. To activate red spot detector and localisation features, it is necessary to locate and annotate the relevant GI boundaries. We recently reported (
) building a stomach/intestine classifier. Here, we propose an automatic discriminator of mouth, stomach, intestine, and colon that would significantly reduce video assessment time as well as allow rapid measurement of gastric and intestinal transit times (GTT and ITT).
Aims and Methods: We created a training set by randomly selecting frames from the mouth, stomach, intestine, and colon regions using 12 of 30 videos. We then applied computational colour analysis techniques to the training set to produce an algorithm that classifies frames as mouth, oesophagus/stomach, intestine, or colon. Then, we developed a further algorithm to search for boundaries between adjacent GI regions. Theoretically, this should greatly reduce viewing time and allow determination of GTT and ITT.
Results: We calculated the time difference between the frames manually annotated and those accorded by the algorithm. The median time (30 videos) was 3 seconds and 25 seconds for the stomach/intestine and intestine/colon discriminator respectively (given 20 frames/second watching speed). For mouth/stomach discriminator the median error was only one frame. The mean (standard deviation) ITT computed with our algorithm was 231 (60) minutes: remarkably similar to the 233 (60) minutes derived manually. The figures for GTT are 15.8 (13.7) minutes and 18.37 (13.2) minutes respectively.
Conclusion: We have shown that the mouth/stomach/intestine/colon discriminators are feasible using computational colour techniques and can also be used to determine GTT and ITT. If incorporated into the Rapid Reader, it could significantly reduce the video evaluation time.
038 “SCOPING OUR (ERCP) PRACTICE”: THE GAP BETWEEN CURRENT PRACTICE AND RECOMMENDATIONS FROM THE NATIONAL CONFIDENTIAL ENQUIRY INTO PATIENT OUTCOME AND DEATH
E. J. Williams, the Steering Committee.BSG audit of ERCP, British Society of Gastroenterology, 3 St Andrews Place, London, UK
Introduction and Methods: NCEPOD has recommended that: (1) resuscitation equipment is available in endoscopy rooms; (2) the risks and benefits of therapeutic endoscopy should be explained to patients; (3) protocols for use of sedation should be available, there should be national guidelines on recording vital signs and those responsible for giving sedation should have received formal training/assessment; (4) all endoscopy units should perform regular audit; (5) patients should be reviewed by the consultant endoscopist before therapeutic ERCP. The BSG audit of ERCP is collecting data from five metropolitan regions of England. Preliminary questionnaires on organisation and practice have already been returned by 77/84 (92%) of units and 180/213 (85%) of the non-SpR grade ERCPists identified.
Results: (1) 69/77(90%) of units have a resuscitation trolley in the department and 13/77(17%) in the ERCP room; (2) 77/180(43%) of endoscopists provide written information which includes mention of all substantial risks—that is, bleeding, pancreatitis, cholangitis, and perforation; 72/180 (40%) indicate alternatives to ERCP are usually/always discussed with patients; (3) 43/77 (56%) of units have a sedation policy but only 104/180 endoscopists (58%) are familiar with BSG guidelines (Bell et al 1991). Sedation and monitoring practice varies; 36/180 (20%) of endoscopists report the average dose of midazolam administered during an ERCP is >5 mg. Although all ERCPists use oximetry, only 118/180 (66%) ever supplement this with BP monitoring. When asked what level of saturation should prompt further measures to ensure oxygenation responses range from 82–98%; (4) 88/180 (49%) of endoscopists report that their unit routinely records complications but only 40/180 (22%) indicate this is recorded electronically; (5) Although 57/77 (74%) of units have a process for screening ERCP requests, only 29/180 (16%) of endoscopists personally vet their ERCP referrals.
Conclusion: Major changes in practice will be needed to achieve compliance with the 2004 NCEPOD report’s recommendations.
039 DOES DRINKING A SMALL AMOUNT OF ANTI-FOAM BEFORE UPPER GASTROINTESTINAL ENDOSCOPY IMPROVE THE VIEWS OBTAINED? A DOUBLE BLIND RANDOMISED CONTROLLED STUDY
A. Sreedharan, G. Beech, C. F. Donnellan, C. Flynn, B. J. Rembacken.Department of Gastroenterology, The General Infirmary at Leeds, Great George Street, Leeds LS1 3EX, UK
Background: Administration of oral anti-foam pre-medication before upper gastrointestinal (GI) endoscopy has the potential to improve views, reduce duration of the procedure, and should facilitate detection of early mucosal abnormalities. However, no randomised trial has been conducted to determine its efficacy.
Aim: To determine if drinking an anti-foam preparation prior to endoscopy improves the views of the upper GI tract.
Patients and Methods: 200 patients attending our unit for upper GI endoscopy were randomised to drink either 50 ml of anti-foam preparation (38 ml of water mixed with 0.5 ml of infacol and 1.5 ml of N-acetylcysteine, 10 ml lemonade) or placebo (30 ml tonic water mixed with 10 ml of lemonade and 10 ml water). Patients and endoscopists were blinded to the type of preparation taken. Data collection included the indication, endoscopic findings, proportion of mucosa obscured by mucous or bubbles (between 0–100%) in mid-oesophagus, lower oesophagus, upper greater curve, upper lesser curve, incisura, antrum, cardia, first and second parts of duodenum, duration of procedure, and requirement for additional wash.
Results: Ninety nine patients were randomised to the anti-foam group and 101 patients to the placebo group. 178 patients completed the study, 87 in the anti-foam group and 91 in the placebo group. Baseline patient characteristics, reasons for withdrawal, indication for endoscopy, and endoscopic findings were comparable between the two groups. The median proportion of area obscured by bubbles and mucous was 4% of the upper GI tract in the anti-foam group compared with 12% in the placebo group (Mann-Whitney U, p = 0.0001).
Mean duration of procedure was 7.1 minutes (95% CI 6.3 to 7.9) in the anti-foam group, compared with 8.8 minutes (95% CI 7.7 to 9.8) in the placebo group (independent Student t test, p = 0.01).
The views were regarded as excellent (<5% of mucosa obscured by bubbles) in 55% of the gastroscopies carried out with anti-foam compared with 23% in the placebo group (48/87 v 21/91, p<0.0001 χ2, 19.3). Additional mucosal washes were required in 14 procedures in the anti-foam group compared to 38 in the control group (p = 0.0002, χ2, 13.9). One early gastric cancer was detected in the placebo group.
Conclusion: This is the first randomised, prospective study to confirm that anti-foam pre-medication before upper GI endoscopy provides better views of the mucosa and reduces the duration of the procedure. This type of pre-medication may help in the detection of early GI cancers at endoscopy. However, larger studies are required to determine if this will facilitate better detection of early mucosal abnormalities.
040 ADDITION OF LOCAL ANTISEPTIC SPRAY TO ANTIBIOTIC REGIME REDUCES THE INCIDENCE OF STOMAL INFECTION FOLLOWING PERCUTANEOUS ENDOSCOPIC GASTROSTOMY: A RANDOMISED CONTROLLED TRIAL
N. V. Radhakrishnan, A. H. Shenoy, I. Cartmill, R. K. Sharma, R. George, D. N. Foster, L. J. Quest.Rochdale Infirmary, Acute Pennine Hospitals Trust, Rochdale, OL11 5QA, Lancs, UK
Aim: To study the effectiveness of local antiseptic spray with or without 3 dose parenteral antibiotic in the prevention of stomal infection (SI) following percutaneous endoscopic gastrostomy (PEG).
Methods: Ninety six patients randomised into three groups: group A, intravenous (IV) Cefuroxime 750 mg just before the procedure followed by two further doses 8 hourly; group B, single application of Povidone-Iodine local antiseptic spray (Betadine); group C, combination of A and B. Stomal site examined at midweek (3rd/4th day) and on day 7 for evidence of SI using a scoring system. Fisher’s exact test used for analysis of primary end point (SI at midweek (MW) and end of week (EOW) 1). Logistic regression (LR) models used to consider effects of age, sex, diabetes, acid suppressants, and steroid therapy on outcome.
Results: Total 96 patients. Group A (n = 34) M:F 18:16, mean age 74 years. Group B (n = 28) M:F 15:13, mean age 72 years. Group C (n = 34) M:F 17:17, mean age 74 years. Indications in A, B, C were broadly comparable. SI at MW in A, B, C were 6%, 32%, 9% and at EOW 1 were 32%, 32%, and 3% respectively. SI at MW higher in B (32%) with 6% in A and 9% in C (p = 0.0114) and at EOW 1 lower in C (3%) with 32% each in A and B (p = 0.0013). Cumulative infections (n) at EOW 1 in A, B, C overall were 11, 12, 3 with significant reduction in SI in C (p = 0.003). No significant difference in numbers given antibiotics for other indications between the three groups (p = 0.363). LR showed only diabetes to have a significant effect on SI (OR at MW 33.34, 95% CI 4.33 to 256.7)
Conclusion: Cefuroxime + Betadine spray significantly reduces both midweek and end of week 1 stomal infection following PEG. Betadine spray on its own does not reduce stomal infection at midweek and end of week 1. Prophylaxis with three doses of iv Cefuroxime reduces stomal infection at midweek but not at end of week 1.
041 OUTCOME OF REPEAT OGD TO ENSURE COMPLETE GASTRIC ULCER HEALING
A. N. Hopper, M. R. Stephens, M. C. Allison, W. G. Lewis.Departments of Surgery and Gastroenterology, Royal Gwent Hospital, Newport, UK
Background: Gastric cancer can present as a non-healing gastric ulcer (GU). Current guidelines recommend repeat gastroscopy for patients diagnosed with GU to ensure complete healing after treatment. The value of this practice has been called into question recently.
Aims: The aim of this study was to determine the diagnostic yield of repeat OGD for gastric ulcer, and the subsequent outcomes for patients later diagnosed with gastric cancer.
Methods: Between 1 October 1995 and 30 September 2003, 25 579 OGDs were performed. 544 (2.1%) patients were initially diagnosed with benign GU>3 mm in diameter. Of the 526 patients undergoing OGD to monitor ulcer healing, 12 were diagnosed with gastric cancer (2.3%). The outcomes for these patients were compared with those of the 328 other patients diagnosed with gastric cancer in this time frame.
Results: See table.
Abstract 41
Conclusion: Patients diagnosed with gastric cancer via repeat OGD for GU healing had earlier stage disease than the rest of the gastric cancer cohort. Moreover they were more likely to undergo potentially curative surgery and to survive long term. To identify a gastric cancer patient that will survive five years, 95 patients with an apparently benign GU need to undergo repeat OGD. We believe that this yield justifies a policy of repeat OGD to ensure complete healing of gastric ulcers.
042 HIGH MAGNIFICATION CHROMOSCOPIC COLONOSCOPY OR HIGH FREQUENCY 20 MHZ MINIPROBE EUS STAGING FOR EARLY COLORECTAL NEOPLASIA: A COMPARATIVE PROSPECTIVE ANALYSIS?
D. P. Hurlstone1, M. A. Karajeh1, S. S. Cross2, K. D. Drew1, M. E. McAlindon1, D. S. Sanders1.1Gastroenterology, Royal Hallamshire Hospital, Sheffield; 2Academic Department of Pathology, Royal Hallamshire Hospital, Sheffield, UK
Background: The successful endoscopic management of early colorectal cancer (CRC) using EMR requires the mandatory predication of invasive depth and lymph node metastasis. Previous data have shown high magnification chromoscopic colonoscopy (HMCC) using the Tanaka crypt type Vn(B)/(C) as clinical indicators of T2/N+ disease to show a low specificity (50%) and overall accuracy of 78% with a tendency to over-stage lesions. Conventional 7.5 MHz EUS offers no improved sensitivity and has many technical limitations. Miniprobe EUS “through the scope” permits imaging of lesions proximal to the rectum using direct endoscopic visualisation.
Aim: To compare the staging accuracy of HMCC using the Tanaka crypt type V with miniprobe high frequency 20 MHz EUS.
Methods: Sixty two patients with a possible diagnosis of early CRC were imaged using HMCC followed by 20 MHz EUS by a single endoscopist. Crystal violet staining (0.05%) at 100× magnification permitted Tanaka crypt criteria to be defined (class C: type V crypt disorder non-defined or absent with ulceration). Submucosal deep invasion (sm3+) was defined at EUS by the presence or absence of a disrupted third sonograpohic layer. Predicted T0/1:N0 lesions were resected using EMR with the remaining referred for surgery. The EUS and HMCC staging was then compared to the resected histopathological specimens.
Results: Lesion n = 52 (12 sm1/13 sm2/27 sm3+). 20 MHz EUS was significantly more accurate for invasive depth staging as compared to HMCC (p<0.001) (overall accuracy 93% and 59% respectively). The accuracy for lymph node metastasis detection using EUS and HMCC was 83%/49% respectively (p<0.02). The NPV of EUS for invasive depth was better than that observed using HMCC (94%/56% respectively). The prevalence of nodal disease overall was 19% (10/52) with 80% (8/10) node positive lesions occurring in the sm3+ lesional group (p<0.02, Bonferroni correction applied).
Conclusions: High frequency 20 MHz EUS is superior to HMCC alone when differentiating T1/2 disease with a high PPV for sm3 differentiation. Sm3+ invasion was associated with nodal metastasis.
043 POLYP PREVALENCE IN A COHORT OF 1445 PATIENTS WITH ISOLATED RECTAL BLEEDING: WHAT ARE WE MISSING WITH JUST THE FLEXIBLE SIGMOIDOSCOPE?
R. P. Arasaradnam, S. T. Gopal, M. T. Donnelly, M. M. Skelly.Department of Gastroenterology, Northern General Hospital, Sheffield, UK
Background: The prevalence of colonic polyps (adenomas) is known for selected populations—for example, 27% if personal/family history is present (Hurlestone et al), 12% in a population screened by flexible sigmoidoscope (FS) (UK screening trial). Information about polyp prevalence and distribution in patients who present with isolated rectal bleeding (IRB) is unclear and could direct choice of investigation between flexible sigmoidoscopy and colonoscopy.
Aim: To report polyp type, prevalence and distribution in patients presenting with IRB.
Methods: We conducted a retrospective study with data collected prospectively (March 2001 to April 2004) on 1445 patients (649 men, median age 58 years) who had a colonoscopy (completion rate 82%) for isolated rectal bleeding. Left colon was defined as that proximal to the descending colon.
Results: 368 (26%) patients from a cohort of 1445 had 455 polyps. 236 were adenomas (prevalence of adenomas was 16%). See table.
Abstract 43
Of 212 patients with adenomas, 30 (14%) had polyps with high grade dysplasia. Twenty patients had highly dysplastic adenomas on the left (five <50 years age) and four had highly dysplastic adenomas on both sides. Right colonic highly dysplastic adenomas were found in six patients, only one of whom had a left sided polyp. Clinically significant exclusive right sided polyps (adenoma and in situ carcinoma) were present in 16% of polyps and 4% of all patients while HGD was found in 1% of polyps. In addition, there were 85 cancers, four of which were in patients less than 50 years. The number needed to colonoscope to find a right sided adenoma with no left sided lesion was 22.
Conclusions: This is the largest UK report on polyp prevalence in IRB. As expected, polyp distribution was predominantly in the left colon. Limiting examination of patients with IRB to a FS would have resulted in 126 patients having to return for a colonoscopy. Furthermore, this strategy would have missed 73 adenomas in 67 patients and one colon cancer.
044 ENHANCED MAGNIFICATION ENDOSCOPY IN BARRETT’S OESOPHAGUS
P. Fortun, G. K. Anagnostopoulos, K. Ragunath, P. Kaye, C. Hawkey.WDDC, Queens Medical Centre, Nottingham, UK
Background and Aim: Reliable identification of premalignant change within columnar lined oesophagus (CLO) or Barrett’s oesophagus is a clinically important but practically difficult goal. Enhanced magnification endoscopy (EME) with acetic acid (3%) instillation and targeted biopsy may allow improved detection of intestinal metaplasia (IM) and low or high grade dysplasia (LGD, HGD).
Method: Fifty patients referred to a specialist Barrett’s clinic underwent EME with a high resolution zoom gastroscope. Areas of Barrett’s oesophagus mucosa were classified by pit pattern prior to selective biopsy, targeting pit patterns known to predict a hierarchy of histological abnormality: type I rounded, II linear/tubular, III villous, and IV cerebriform.
Results: The mean length of BO was 4.35 cm, 286 biopsy samples were processed from 50 patients. Histology revealed CLO without IM (6), IM without dysplasia (35), LGD (4), HGD (1), cardiac type (3), and adenocarcinoma (1). Of the 35 patients with IM, the highest grade of pit pattern observed was linear/tubular (14), and villous (21). No cerebriform patterns were seen, while some also contained simple patterns. Of the patients with LGD, HGD, and cancer, the patterns were linear/tubular and villous, villous, and cerebriform respectively. In patients without IM or dysplasia, the whole spectrum of patterns was seen. Looking at yield of IM by length of Barrett’s oesophagus, of those ⩽2 cm, 14/21 (61%) had IM (with one cancer); for >2 cm, 27/29 (93%) had IM (4 LGD, 1 HGD). Ten of the 48 (21%) patients with prior endoscopy and biopsy, had a histological “upgrade” after EME: five from CLO to CLO with IM, three to LGD, one to HGD, and one from IM to cancer, despite a short mean screening interval (5.4 months). We encountered some technical difficulties with blood obscuring target biopsy and limited diagnostic window (4–5 minutes) for acetic acid.
Conclusion: EME allows clear resolution of epithelial pit patterns within Barrett’s oesophagus, and targeted biopsy with a high yield of IM and dysplasia. This may allow a significant histological upgrade. It is a technically challenging procedure with some limitations and will require training and experience to achieve good results.
045 TREATMENT OF HAEMORRHAGIC RADIATION INDUCED PROCTITIS USING TOPICAL FORMALIN INSTILLATION
S. N. Cullen, M. Frenz, A. Mee.Royal Berkshire Hospital, Reading, UK
Background: Between 2% and 5% of patients undergoing pelvic radiotherapy develop chronic radiation proctitis and the problem is becoming more common with the increased use of radiation treatment for pelvic malignancy. There have been no formal trials of treatment for radiation colitis and a variety of methods are currently used including topical steroids, sucralfate enemas, and argon plasma coagulation. Small case series of topical formalin therapy have been reported using a variety of techniques. The use of large volumes of formalin has been associated with some serious side effects. This study aimed to assess the efficacy of small volume topical formalin instillation as a method of controlling bleeding from radiation proctitis.
Method: All patients who had undergone formalin treatment for radiation proctitis at our centre were identified and their notes reviewed. The patients had all received radiotherapy for either prostatic or bladder carcinoma and 13 of the 14 had presented with rectal bleeding. One patient presented with iron deficiency anaemia. Patients were treated by a single operator using 20 ml of a 5% solution of formalin instilled into the rectum via a sigmoidoscope for 2 minutes and then sucked out.
Results: See table.
Abstract 45
Conclusion: Formalin instillation of 20 ml of a 5% solution via a flexible sigmoidoscope appears to be safe in the context of radiation proctitis. A single treatment produced complete resolution of symptoms in half of this group of patients and only two patients reported no benefit. The technique is simple, inexpensive, and quick and requires no sedation. We suggest that it should be considered as a first line for patients presenting with haemorrhagic radiation induced proctitis.
046 MRSA CARRIER STATUS PREDICTS A HIGH RISK OF INFECTION AFTER PEG INSERTION: RESULTS FROM A LARGE PROSPECTIVE AUDIT
A. Cherrington, D. Hill, J. E. Smithson1.Departments of Infection Control and 1Gastroenterology, North Bristol NHS Trust, UK
Background: Percutaneous endoscopic gastrostomy (PEG) is often complicated by infection at the insertion site. A prospective audit has been carried out to identify risk factors within our Trust.
Methods: 100 consecutive patients who had PEGs inserted from September 2003 onwards were studied at both hospitals in North Bristol NHS Trust. Antibiotic prophylaxis was not routinely employed. MRSA (methicillin resistant staphylococcus aureus) status was determined by nose swab at the time of endoscopy. Infective complications which occurred at the insertion site during the next 14 days were monitored prospectively using a standardised scoring system.
Results: Significant PEG site infections occurred in 36/100 (36%) patients. Among MRSA carriers 17/29 (59%) developed infection compared with 19/71 (27%) patients who were MRSA negative (p<0.005, χ2) at the time of PEG insertion. The odds ratio of the likelihood of infection occurring in MRSA positive versus negative patients was 3.65 (95% CI 1.47 to 9.06). MRSA was the commonest cause of infection (15/36) compared with other bacteria and exclusively affected MRSA carriers. No significant associations were found between PEG infection and patients’ initial mouth condition or current antibiotic use. Infection rates did not vary significantly between different endoscopists and were very similar on both hospital sites.
Conclusions: This large prospective audit has identified a high overall infection rate following PEG insertion in our Trust. MRSA carriers are at much greater risk than MRSA negative patients. These findings have important implications for counselling of patients prior to insertion, and will guide future infection control strategy for patients receiving PEGs.
Pancreatic symposium
047 PHOTODYNAMIC THERAPY USING TALAPORFIN SODIUM (LS11) PHOTOSENSITISATION IN THE PANCREAS AND SURROUNDING TISSUES IN THE SYRIAN GOLDEN HAMSTER
J. Wittmann, S. P. Pereira, S. G. Bown.National Medical Laser Centre, Institute of Hepatology, RF & UCL Medical School, London, UK
Aim: To assess the safety of interstitial photodynamic therapy (PDT) using LS11, a novel chlorine derived photosensitiser, in animal studies using the Syrian golden hamster.
Methods: LS11 was administered by direct inferior vena cava (IVC) injection in the anaesthetised hamster at 5 mg/kg. Tissue fluorescence studies in liver, duodenum, colon, and pancreas were performed at 15, 30, 60, 120, and 240 minutes, and 24 hours. To determine the drug-light interval (DLI) producing the largest PDT lesion, 50 J light was delivered to the pancreas, duodenum, liver, colon, spleen, aorta, and IVC at 15, 30, 60, 120, and 240 minutes after 5 mg/kg LS11. The PDT effects on the targeted organ and adjacent structures were assessed by postmortem at 3 and 21 days, or at the time of death.
Results: Fifty hamsters were used during the study (n = 11, tissue fluorescence study; n = 10, liver PDT DLI ranging study; n = 29, PDT safety study (targeting pancreas (n = 11), liver (n = 7), spleen (n = 3), duodenum (n = 2), aorta and IVC (n = 2) and colon (n = 1)). Three animals died from anaesthesia related problems. The largest liver PDT lesions were observed at a DLI of 15 minutes. LS11 produced significant PDT lesions at 5 mg/kg, with concentrations of 1 and 2 mg/kg resulting in smaller volume lesions in keeping with the reciprocity principle of PDT. The pancreas was resistant to direct PDT injury but surrounding organs (stomach, duodenum, and liver) were affected. When the pancreas was treated at 5 mg/kg and 50 J, two hamsters developed localised peritonitis and perforation of the duodenum, requiring culling at 13 days post-PDT. At lesser energies, local adhesions without clinical illness occurred at day 3. At 21 days post-PDT, all animals surviving PDT had recovered completely and were thriving.
Conclusion: LS11 is a safe and predictable agent for use in interstitial PDT. The hamster pancreas has a safe limit of 5 mg/kg and 25 J at a DLI of 15 minutes. Phase I studies in human pancreatic cancer should be feasible.
048 AUTOIMMUNE PANCREATITIS/CHOLANGIOPANCREATOPATHY: EVIDENCE OF MULTISYSTEM INVOLVEMENT
G. J. M. Webster, J. Wittmann, E. Seward, S. P. Pereira, A. R. W. Hatfield.Pancreaticobiliary Unit, Department of Gastroenterology, University College London Hospitals NHS Trust, London, UK
Background: “Autoimmune pancreatitis” (AIP) is a rare condition defined by seven main criteria: pancreatic mass; pancreatic duct stricture; low common bile duct (CBD) stricture; associated autoimmune disease; raised serum IgG4 levels; lymphoplasmacytic infiltrate on biopsy; and therapeutic response to steroids. The usual presentation with obstructive jaundice, pain, and a mass on imaging often leads to a presumptive diagnosis of malignancy. Although well described in Japan, the condition has been rarely reported in Western countries.
Methods: All patients seen in our unit in the 12 months to October 2004, who had clinical features and ERCP findings consistent with AIP, were reviewed and assessed for diagnostic criteria of AIP. Those with additional extra-pancreatic abnormalities were the focus of this work.
Results: Of 984 ERCPs performed, six patients fulfilled criteria for AIP, and four had additional disease (all male, ages 51–55 years). These four met at least six of the seven criteria: pancreatic mass, pancreatic duct stricture, low CBD stricture, lymphocytic infiltrate on biopsy, and pre-existent autoimmune disease in all (diabetes (2), ulcerative colitis (1), Sjogren’s syndrome/sialadenitis (2)); ↑ IgG4 in 3/4 (which normalised on treatment). All four patients showed a clinical response to steroids. Extra-pancreatic abnormalities included: primary sclerosing cholangitis-like intra/extrahepatic disease (4/4); gastric and small bowel thickening (1); bone marrow involvement (1); retroperitoneal mass (1). Renal infiltrates on CT seen in 3/4 patients, with renal impairment in two, and lymphocytic infiltrate and sclerosis on renal biopsy in the one patient biopsied.
Summary: AIP appears to be rare, but does occur in the UK population. The high frequency of intra/extrahepatic biliary abnormalities suggests that “cholangiopancreatopathy” may be a better term than AIP. Moreover, our recent experience suggests that multisystem disease, with clinically significant renal involvement, may be a feature in these patients, posing further questions as to the aetiopathogenesis of the underlying condition.
Oesophageal free papers
049 EFFECT OF ACID SUPPRESSION ON THE PROLIFERATION STATUS OF BARRETT’S OESOPHAGUS
P. Lao-Sirieix1, A. Roy2, R. Fitzgerald1.1MRC Cancer Cell Unit, MRC/Hutchison Research Centre, Cambridge; 2Motility Unit, Addenbrooke’s Hospital, Cambridge, UK
Introduction: Gastro-oesophageal reflux has been advocated as the main risk factor for the development of Barrett’s oesophagus, the precursor of oesophageal adenocarcinoma (AC). Whether or not profound acid suppression has a role in the prevention of AC in patients with Barrett’s oesophagus is not known. Mcm2 is a marker of proliferation. We have previously shown that Mcm2 expression increases, with abnormal expression in the upper crypts and the surface epithelium, during carcinogenesis.
Aim: To determine the effect of acid suppression therapy on proliferation indices in patients with Barrett’s oesophagus.
Materials and Methods: Forty six patients with Barrett’s oesophagus (with or without dysplasia) who underwent pH monitoring were divided into two groups according to their DeMeester score (above or below 14.72). Thirty one patients had a normal score (acid suppressed by their current medication) and 15 had a pathological score (abnormally high acid exposure). Slides from biopsies taken before (3 months), soon after (3.5 months) and long after (1 year) pH monitoring were stained for Mcm2. Mcm2 expression was scored as a percentage of epithelial cells in three compartments: (1) the epithelial surface, (2) the upper crypt, and (3) the lower crypts and glands.
Results: The male to female ratio was 3.5:1 in the acid suppressed group and 1.5:1 in the pathological group. There was no statistical difference between the age, the medication, the dysplasia status, and the levels of Mcm2 expression in the three compartments of the normal and pathological groups before the pH monitoring. The expression levels of Mcm2 decreased with time (long after v before) in the surface (23.5 (SD 3.9) % and 10.8 (SD 3.2) % respectively, p<0.005) and the upper crypt (60.5 (SD 4.8) % and 37.7 (SD 5.9) % respectively, p<0.005) but not in the normal proliferative compartment (lower crypts and glands) of the patients with normal acid exposure. In contrast, there was no alteration in Mcm2 in the pathological group.
Conclusions: Long standing suppression of acid reflux decreases expression of Mcm2 in the surface and the upper crypt of Barrett’s oesophagus patients. This decrease in proliferation might reduce the risk of those patients to progress to AC.
050 ESOMEPRAZOLE AND PANTOPRAZOLE: A COMPARISON FOR MAINTENANCE TREATMENT OF HEALED EROSIVE OESOPHAGITIS
J. Labenz1, D. Armstrong2, P. H. Katelaris3, S. Schmidt4, J. Adler5, S. Eklund6 (introduced by A. J. Morris).1Medical Department, Jung-Stilling-Krankenhaus, Siegen, Germany; 2Division of Gastroenterology, McMaster University Medical Centre, Hamilton, Canada; 3Gastroenterology Department, Concord Hospital, University of Sydney, Sydney, Australia; 4Burnside House, City Medical Chambers, Cape Town, South Africa; 5Biostatistics; 6Med and Sci, AstraZeneca, Mölndal, Sweden
Introduction: The eight week acute phase of the present study showed esomeprazole 40 mg to be more effective than pantoprazole 40 mg for healing erosive oesophagitis (EE) in symptomatic patients. Here we report results of the maintenance phase of the study (SH-NEG-0008).
Methods: Following EE healing and symptom relief in the 4–8 week acute phase, 2766 patients (63% male; mean age 50 years) were randomly allocated to receive esomeprazole 20 mg or pantoprazole 20 mg for 6 months. The primary variable was relapse, defined as endoscopically confirmed EE and/or withdrawal due to symptoms.
Results: The proportion of patients in remission at 6 months was significantly greater with esomeprazole 20 mg than pantoprazole 20 mg.
Conclusion: Esomeprazole 20 mg is more effective than pantoprazole 20 mg for maintenance therapy in patients with healed EE.

Abstract 50 Life table estimates (95% CIs) of 6 month remission rates. ***p<0.001, ****p<0.0001, †p = 0.15.
051 ESOMEPRAZOLE 40 MG COMPARED WITH OMEPRAZOLE 20 MG FOR THE HEALING AND RESOLUTION OF HEARTBURN AMONG PATIENTS WITH MODERATE TO SEVERE REFLUX OESOPHAGITIS: THE PROGRESS STUDY
A. J. Morris1, J-PRosen2, L. Golightly2.1Gastroenterol Department, Glasgow Royal Infirmary, Glasgow, UK; 2ISMO, AstraZeneca, Luton, UK
Introduction: Previous studies show esomeprazole has a greater healing rate and a faster onset of sustained heartburn resolution than omeprazole in patients with reflux oesophagitis (RO). In this study we compared esomeprazole 40 mg (Eso) and omeprazole 20 mg (Ome) for healing of RO, powered specifically to detect a significant difference in patients with severe RO, Los Angeles classification Grades C and D.
Methods: In this double blind, randomised, multicentre study, patients with endoscopically proven moderate/severe RO (Los Angeles Grades C or D) and a history of reflux symptoms were treated with daily Eso 40 mg or Ome 20 mg. Primary variable was endoscopic healing at week 8, assessed by survival estimate. Secondary outcome variables included the frequency of heartburn and acid regurgitation at 4 and 8 weeks (investigator rating of symptoms), and the time to sustained (seven consecutive days/nights) resolution of heartburn (patient diary data).
Results: ITT population included 553 patients. Survival estimates of the proportions healed by week 8 were 89% for Eso and 75% for Ome. The proportion of patients healed by week 4 was also significantly higher with Eso than with Ome (crude rate: 67.4% v 54.2%, p = 0.003). At week 4, a significantly greater proportion of patients on Eso achieved complete resolution of both heartburn and acid regurgitation (62.8% v 51.7%, p = 0.002); complete resolution of heartburn (68.1% v 58.3%, p = 0.005); and relief of heartburn (72.7% v 64.6%, p = 0.014) compared with Ome, respectively. Sustained heartburn resolution was faster with Eso than with Ome (median days: 9 v 14, p = 0.029) and more heartburn free days (70.8% v 63.2%, p0.005) and nights (80.1% v 72.6%, p = 0.003) were achieved with Eso compared with Ome, respectively.
Conclusion: Esomeprazole 40 mg is more effective than omeprazole 20 mg in healing severe RE (Los Angeles Grades C or D) and in providing fast and effective symptom resolution.
052 OPTICAL BIOPSY USING ELASTIC SCATTERING SPECTROSCOPY CAN DETECT DYSPLASIA AND CANCER IN BARRETT’S OESOPHAGUS
G. D. Mackenzie1, K. Johnson1, M. R. Novelli1, M. O’Donovan2, S. Davies2, C. Selvasekar1, S. Thorpe1, I. J. Bigio3, S. G. Bown1, L. B. Lovat1.1National Medical Laser Centre, Middlesex Hospital, London, 2Addenbrookes Hospital, Cambridge, Boston University, Boston, USA3
Background: Elastic scattering spectroscopy (ESS) detects changes in the microscopic physical properties of cells. A pulse of white light is shone through an optical fibre probe, placed in contact with the mucosa through an endoscope, and spectral analysis is undertaken on back scattered light. Results are available in under a second. Light scattering is sensitive to nuclear size and density and other organelles. We present data using this technology to diagnose high grade dysplasia or cancer within Barrett’s oesophagus.
Methods: 890 ESS spectra and matched oesophageal biopsies were taken from 256 sites in 96 patients with Barrett’s. The probe tip was placed in gentle contact with the tissue surface for the sites being interrogated and histology taken from the same site. “Optical biopsies” took under one second to perform. All biopsies were reviewed by three GI pathologists and defined as non-dysplastic or low grade dysplasia (LGD), or high grade dysplasia (HGD) or carcinoma.
Results: Agreement between pathologists for HGD was high (kappa = 0.77). Only biopsies where there was consensus were analysed and histological findings were correlated with the appropriate spectra. For the analysis 2/3 of the data set was used for training the pattern recognition methods, the rest reserved for testing. “Optical biopsy” detected HGD or cancer with a sensitivity 83% and a specificity of 72%. If 20 optical biopsies were taken then only seven (not 20) samples would be required for histology with a negative predictive value >97%.
Conclusions: Preliminary results using ESS show that this technique has potential as a real time diagnostic test for in vivo diagnosis of dysplasia or cancer within Barrett’s mucosa, or as guidance for conventional biopsy to improve sensitivity for HGD over that of random biopsies. Significant histopathology time could be saved by examining up to 65% fewer samples. Additionally, optical biopsy results are immediately available without the need for expert interpretation.
053 PHOTODYNAMIC THERAPY WITH 5 AMINOLEVULINIC ACID FOR HIGH GRADE DYSPLASIA IN BARRETT’S OESOPHAGUS: LONG TERM FOLLOW UP OF 51 PATIENTS
G. D. Mackenzie, B. Clark, C. R. Selvasekar, N. F. Jamieson, M. R. Novelli, S. M. Thorpe, C. A. Mosse, S. G. Bown, L. B. Lovat.National Medical Laser Centre, Department of Surgery, Royal Free & University College School of Medicine, London, UK
Background: Oesophagectomy, the current treatment for high grade dysplasia (HGD) in Barrett’s oesophagus carries 5% mortality and 40% serious morbidity. Photodynamic therapy (PDT), an ablative therapy for HGD in Barrett’s oesophagus, offers a lower risk alternative if proved efficacious. 5-aminolevulinic acid (ALA) has shorter photosensitivity than other agents (<48 hours) and less stricture formation due to selective mucosal uptake. The optimal treatment regimen, however, remains unknown.
Methods: Patients with HGD were treated with PDT with oral ALA at 30 mg/kg (low dose) or 60 mg/kg (high dose) and either low dose (500 or 750 J/cm) or high dose (1000 J/cm) light via diffuser fibre with regular endoscopic follow up. Patients were retreated if clinically indicated.
Results: Fifty one patients had 89 treatments over a six year period. Median follow up is 13.5 months (range 1–68 months). 16/23 patients (70%) who were treated with high dose ALA and high light dose are free of dysplasia. In contrast, remission occurred in 2/12 (17%) after high dose ALA but low light doses and 6/16 (38%) after low dose ALA but high light dose. Eight patients who failed treatment were offered “salvage” PDT with the best regime. Dysplasia was eradicated in 5/8 (63%) of these patients. There were no strictures or cases of skin photosensitivity. Three cases of hypotension after drug administration occurred early in the study but were prevented later by intravenous rehydration and avoidance of psychotropic drugs. One case of upper GI bleeding was seen 2 weeks after PDT requiring a 2 unit transfusion.
Conclusion: High dose ALA/light was significantly better than low dose ALA/high dose light (p = 0.006) or high dose ALA/low dose light (p = 0.008).
054 THE RELATION BETWEEN WORLDWIDE VARIATION IN CAGA+ HELICOBACTER PYLORI INFECTION, HISTOLOGICAL SUBTYPE OF OESOPHAGEAL CANCER, AND SEX
G. Robins1, A. Bailey1, D. Forman2, J. Crabtree1 for the EUROGAST Study Group.1Molecular Medicine Unit, St James’s University Hospital, Leeds; 2Centre for Cancer Research, University of Leeds, Leeds, UK
Background: There has been a dramatic increase in the ratio of adenocarcinomas (AC) to squamous carcinomas (SC) of the distal oesophagus. The incidence of AC in males is higher, with an up to fivefold difference in age standardised rates. Simultaneously, there has been a decrease in the incidence of gastric carcinoma (GCA), which also shows a strong male predominance. GCA is strongly associated with Helicobacter pylori infection, rates of which have declined significantly. Infection with cagA+ Hp is associated with increased inflammation and more severe gastric atrophy (GA). Infection with cagA+H pylori strains has also been negatively associated with oesophageal AC in some studies. The protective effects of H pylori infection may be due to the development of GA. The aims of this study were to examine the effects of sex and H pylori and cagA status on oesophageal AC and SC rates.
Methods: The Eurogast Study Group was comprised of more than 2700 healthy individuals from 13 countries which were selected to provide a representative sample of local populations. Standardised protocols were used to collect and process questionnaire data and serum samples for H pylori and cagA serology. Sex specific population based oesophageal AC and SC rates were used to calculate SC:AC ratios.
Results: Linear regression confirmed a significant correlation between the ratio of SC:AC and serological markers of H pylori infection in males (r = 0.82; p = 0.0035) and females (r = 0.65; p = 0.04). A significant correlation between SC:AC ratio and cagA seropositivity was also seen in males (r = 0.68; p = 0.03), but not in females (r = 0.32; p = 0.37). The association between SC:AC ratio and percentage of serologically confirmed H pylori infected individuals (H pylori +ve) who were also cagA+ve revealed no correlation in males (r = −0.06; p = 0.87) and a significant inverse correlation in females (r = −0.69;p = 0.027).
Conclusions:H pylori +ve individuals have a lower incidence of oesophageal AC. Although negatively associated with AC in males, cagA seropositivity is not so in females, possibly reflecting an effect of an as yet unidentified factor (such as has been proposed for female hormones and development of GCA).
055 SCREENING COMMUNITY SUBJECTS WITH FREQUENT GASTRO-OESOPHAGEAL REFLUX SYMPTOMS FOR RISK OF DEVELOPING OESOPHAGEAL ADENOCARCINOMA: A PILOT STUDY
I. Khan1, I. Mohammed1, J. Gearty2, N. J. Trudgill1.Department of 1Gastroenterology and 2Histopathology, Sandwell General and City Hospitals, West Midlands, UK
Background: Oesophageal adenocarcinoma (OA) frequently presents at a late stage and is associated with a poor five year prognosis. Barrett’s oesophagus is a premalignant condition, potentially offering the opportunity to intervene to prevent OA. Screening community subjects with gastro-oesophageal reflux disease (GORD) symptoms for Barrett’s oesophagus has been proposed but not previously studied.
Methods: We recently conducted a community survey of 4000 subjects stratified by age, sex, and ethnicity to be representative of the population of Sandwell. Subjects with heartburn or acid regurgitation at least once a week, who were <70 years and not previously endoscoped were invited for endoscopy.
Results: 1533 subjects replied to the survey. 325 subjects reported frequent GORD symptoms. 199 met the entry criteria and were invited for endoscopy. 47 agreed: 39 were endoscoped (24 male; mean age 49.1 years; range 26.4–69.2 years), eight did not attend. Endoscopy findings (n): Barrett’s oesophagus (6), oesophagitis (19), hiatus hernia (17), other endoscopic abnormality (10). Only one subject had >3 cm Barrett’s oesophagus but she also had a polypoid carcinoma within her 6 cm Barrett’s oesophagus segment. Of the remaining five subjects with Barrett’s oesophagus, histology revealed specialised intestinal metaplasia in three but no evidence of dysplasia.
Conclusion: In this pilot study of endoscopic screening, the prevalence of Barrett’s oesophagus among community subjects with frequent GORD symptoms was 15%. An asymptomatic OA was diagnosed in one subject. Further study of the role of endoscopic screening for Barrett’s oesophagus is merited.
056 ARE DIET AND PHYSICAL ACTIVITY RISK FACTORS FOR GASTRO-OESOPHAGEAL REFLUX DISEASE SYMPTOMS IN DISCORDANT TWINS?
I. Mohammed, L. Cherkas1, T. D. Spector1, N. J. Trudgill.Sandwell General Hospital, West Midlands and 1Twin Research Unit, St Thomas’ Hospital, London, UK
Background: Meals increase acid reflux in patients with gastro-oesophageal reflux disease (GORD). Obesity is associated with GORD symptoms. We have examined dietary factors and physical activity in discordant twin pairs, in which only one twin has GORD symptoms.
Methods: Eighty three monozygotic (MZ) and 166 dizygotic (DZ) twin pairs, who were discordant in a previous survey of GORD symptoms, were sent questionnaires on GORD symptoms, food frequency, and physical activity (IPAQ). GORD symptoms were defined as at least monthly symptoms of heartburn or acid regurgitation.
Results: Response rate was MZ 84%, DZ 74%. Eligible discordant pairs included 24 MZ (all female, mean age 58 (SD 13) years) and 65 DZ (62 female, age 58 (SD 11) years) pairs. Univariate analysis revealed that increased intake of protein (mean 77 (SD 42) g v 72 +/− 25 g (p = 0.03)), total sugar (119 (SD 72) g v 99 (SD 51) g (p = 0.03)), fat (74 (SD 39) g v 65 (SD 28) g (p = 0.05)), sodium (2511 (SD 959) mg v 2264 (SD 712) mg (p = 0.04)), and potassium (3745 (SD 1210) mg v 3475 (SD 981) mg (p = 0.04)) were associated with GORD symptoms. Body mass index (mean 26 (SD 5) v 25 (SD 4) (p = 0.002)) was also associated with GORD symptoms. However, physical activity, other carbohydrate and fibre intake, and smoking were not associated with GORD symptoms. Multivariate analysis revealed trends for independent associations between intake of protein (p = 0.07), fat (p = 0.09), and sodium (p = 0.06) and GORD symptoms.
Conclusion: Increased intake of protein, fat, sugar, sodium, and potassium and increasing body mass index are associated with GORD symptoms. However, physical activity is not associated.
Endoscopic ultrasound symposium
057 A NOVEL TECHNIQUE OF ENDOSCOPIC ULTRASOUND GUIDED TRUCUT MURAL BIOPSIES IN THE INVESTIGATION OF UNEXPLAINED THICKENING OF OESOPHAGOGASTRIC WALL
G. K. Anagnostopoulos1, P. Kaye2, G. P. Aithal1.1Division of Gastroenterology and 2Pathology, Queen’s Medical Centre, Nottingham, UK
Background: Approaching the patient with CT thickening of oesophagogastric wall and negative endoscopic biopsies is difficult. The aim of this study was to examine whether it is feasible to obtain diagnostic tissue core from the gut wall using endoscopic ultrasound (EUS) guided trucut biopsy technique in this group of patients.
Patients and Methods: During 18 months period, 10 patients (six male) aged 38–87 years (median 66) were identified. They all had diagnostic endoscopy with normal biopsies and thickening of oesophageal/gastric wall on CT. Radial and curvilinear echoendoscopes (GF-UM240, GF-UCT2000-OL5, KeyMed Ltd) were used to identify the area of maximum thickening of gut wall. Under EUS guidance, mucosa was penetrated using 19 gauge trucut needle (Quick-Core, Cook) and 20 mm tissue tray was advanced obliquely through the wall layers to avoid penetration of the serosa. The spring-loaded mechanism built into the handle was triggered to fire the cutting sheath over the tray. The procedure was repeated until a core of tissue was obtained.
Results: All patients had undergone 1–5 (median 1) oesophagogastroduodenoscopies with 2–16 (median 8) biopsies before EUS examination and none had raised a suspicion of malignancy. On EUS, thickening of oesophageal (n = 5) or stomach (n = 5) wall of 5–20 mm (median 11) was noted. EUS guided mural trucut biopsies were performed in all without complications. With 1–5 (median 2.5) passes, 4–20 mm (median 10) tissue cores were obtained. Based on EUS guided trucut biopsies diagnoses of carcinoma were made in five patients (three stomach, two oesophageal). Four others had normal histology and 1 inconclusive. During a follow up of months no false negatives have been identified.
Conclusion: EUS guided trucut mural biopsy technique could yield diagnostic tissue cores in patients with unexplained thickening of oesophagogastric wall. Clinical application of this technique should be evaluated in a larger patient group.
058 SEQUENTIAL SAMPLING: OPTIMISING THE USE OF TWO ENDOSCOPIC ULTRASOUND GUIDED TISSUE SAMPLING TECHNIQUES
G. K. Anagnostopoulos1, A. Zaitoun2, P. Kaye2, K. Ragunath1, G. P. Aithal1.Departments of 1Gastroenterology and 2Pathology, Queens Medical Centre, University Hospital, Nottingham, UK
Background: Each of the two endoscopic ultrasound guided (EUS) guided sampling techniques—fine needle aspiration (FNA) and Tru-cut biopsy—have advantages and limitations when used alone. We have previously shown that combining the two techniques would increase the accuracy of EUS guided sampling, but this involved performing both FNA and Tru-cut biopsies in all the patients.
Aim: To investigate whether performing FNA, only when Tru-cut biopsy samples were inadequate, would be a useful strategy in EUS guided sampling.
Methods: EUS (GF-UCT-240-AL5, KeyMed) guided sampling was performed using 19-gauge needle (Quick-Core, Cook) for Tru-cut biopsies and 22-gauge needles for FNA. Maximum of four passes were made for Tru-cut biopsy and if the samples obtained were inadequate, further FNA was carried out for cytology. We compared the results of this approach (sequential sampling) with 25 previous patients who had undergone both Tru-cut and FNA (dual sampling).
Results: Thirty nine patients (eight females) aged 34–83 (median 66) who underwent “sequential sampling” were compared with 25 (nine female) aged 22–86 years (median 63) who had “dual sampling”. There were no significant difference in the maximum diameter of the lesions sampled in the two groups (0.5–6.0 (mean 2.55 (SD 1.4) cm v 1.5–5.7 (3.38 (SD 1.2) cm) or the route of sampling (oesophagus/stomach/duodenum in 17/18/4 v 6/15/04). The number of passes made were similar (n = 2–7) in both groups (3.54 (SD 1.5) v 4.16 (SD 1.2) and there was no difference in the length of the tissue core (0–2 (1.19 (SD 0.6) v 0.89 (SD 0.5) cm). The diagnosis reached with sequential sampling was accurate in 36/39 (92%) cases compared with 23/25 (92%) in dual sampling group. Six out of 39 in the sequential sampling group needed FNA.
Conclusions: Accurate diagnosis was reached in 92% of cases using “sequential sampling” strategy with 15% of the patients requiring both Tru-cut biopsies and FNA.
059 PREOPERATIVE HIGH FREQUENCY MINIPROBE EUS OF COLORECTAL NEOPLASIA: IS MANAGEMENT MODIFIED?
D. P. Hurlstone1, M. A. Karajeh1, S. S. Cross2, K. D. Drew1, M. E. McAlindon1, D. S. Sanders1.1Gastroenterology, Royal Hallamshire Hospital, Sheffield; 2Academic department of Pathology, Royal Hallamshire Hospital, Sheffield, UK
Background: Miniprobe ultrasound technology permits in vivo luminal staging of colorectal cancer by passing directly through the instrument port of the colonoscope. Conventional EUS techniques have been limited by the requirement for a second endoscopic examination, inability to image stenotic neoplasia, and inaccessibility of tumours proximal to the rectum. As minimally invasive resection techniques such as EMR and laparoscopic resection are now possible, a sensitive preoperative staging tool is required to optimise patient selection.
Aim: To examine the accuracy of miniprobe ultrasound imaging in the preoperative staging of colorectal cancer and address the value of the technique for management decisions.
Methods: 12.5 MHz miniprobe EUS was performed in 130 consecutive patients with adenocarcinoma or broad based polyps of the colorectum by a single endoscopist. Staging criteria for tumour infiltration depth was determined according to the TNM class of the UICC. Metastatic nodal disease was defined as the presence of low echo, round, defined boundary lesion >10 mm in diameter. T0/T1/N0 lesions were resected using EMR with those staged as T2/N+ referred for surgical resection. Imaging results were compared with endoscopic assessment and histopathological finding of the resection specimens.
Results: n = 130. Right colon (n = 55)/left colon (n = 39)/rectum (n = 36) hT = pathology stage/mi-T = EUS stage: Accuracy 98%/NPV 89%/NPV 99% (see table).
Abstract 59
Conclusions: EUS may improve preoperative staging of colon cancer.
Pathology/IBD Symposium
060 DECREASED TELOMERIC REPEAT BINDING FACTOR 2 (TRF2) EXPRESSION IN RESTING PERIPHERAL BLOOD LYMPHOCYTES IN ULCERATIVE COLITIS
K. M. Getliffe, D. Al Dulaimi, C. U. Nwokolo.University Hospital, Coventry, UK
Background: Telomeric repeat binding factor 2 (TRF2) stabilises mammalian telomeres and acts independently of telomerase. Decreased expression results in telomeric fusion and chromosomal instability leading to cell death or carcinogenesis. Such cytogenetic abnormalities are present in peripheral blood lymphocytes (PBLs) of patients with ulcerative colitis (UC) and other inflammatory diseases. In the colonic mucosa in UC, similar changes precede progression to dysplasia and cancer. The mechanism that causes these changes is unknown. Having found no evidence of accelerated telomeric shortening in UC and Crohn’s disease (CD) in previous experiments, our first hypothesis was that underexpression of TRF2 could explain the chromosomal abnormalities present in UC PBLs. TRF2 may also have a role in DNA repair processes, because it is upregulated upon activation of cells with damaged DNA. We also investigated this hypothesis in UC and CD.
Methods: PBLs were obtained from patients with UC (n = 11), CD (n = 10), and healthy controls (n = 11), activated with phytohaemagglutinin and purified with a magnetic cell sorter. Real-time PCR was used to quantitate TRF2 mRNA expression in resting and activated PBLs.
Results: In resting PBLs, mean TRF2 mRNA levels were significantly lower in UC patients compared with controls (9.5 v 12.7, p = 0.013). After activation, mean TRF2 mRNA expression was unchanged in control PBLs (12.7 v 11.5). In contrast, activation increased mean TRF2 mRNA levels in UC patients from 9.5 to 13.2 (p = 0.004) and in CD patients from 10.7 to 16.6, (p = 0.069). Mean TRF2 mRNA expression in activated PBLs in CD patients was also higher than in similar controls cells (16.6 v 11.5, p = 0.037) and a similar trend was seen in UC.
Conclusions: TRF2 mRNA expression is decreased in resting PBLs in UC and could lead to the chromosomal instability observed in this disease. Activation of PBLs led to up regulation of TRF2 mRNA in UC and CD, but not in controls. Since IBD lymphocytes are known to have unstable genomes, TRF2 may be upregulated upon activation in these cells, as part of the DNA damage response. These data provide further evidence of this novel role of TRF2.
061 THE CONTRIBUTION OF BONE MARROW TO COLONIC SUBEPITHELIAL MYOFIBROBLASTS IN INTERLEUKIN-10 KNOCKOUT MICE
S. Bamba, W. R. Otto, C. Y. Lee, M. Brittan, S. L. Preston, N. A. Wright.Histopathology Unit, Cancer Research UK, London
Background: We have previously reported the engraftment of bone marrow-derived stem cells into colonic subepithelial myofibroblasts (SEMFs) in humans and the mouse (Brittan et al. Gut 2002;50:752–7). In the pathogenesis of inflammatory bowel disease (IBD), such as Crohn’s disease and ulcerative colitis, colonic SEMFs are supposed to mediate various kinds of inflammatory responses. We used interleukin (IL)-10 knockout mice as a model of IBD to investigate the contribution of bone marrow derived stem cells in inflamed mucosa.
Method: Whole bone marrow (C57/BL10 and IL-10 knockout mice) was used to perform bone marrow transplantation for IL-10 knockout mice. Tissue samples were evaluated by in situ hybridisation using a Y chromosome-specific probe combined with immunohistochemistry for α-smooth muscle actin to track the donor-derived colonic SEMFs. The mucosal mRNA expression of cytokines was analysed by reverse transcriptase-polymerase chain reaction (RT-PCR).
Results: Body weight and histological scores revealed that knockout mice that received wild type (C57BL10) bone marrow were rescued from colitis. In addition, transplantation of wild type bone marrow decreased the mucosal mRNA expressions of IFN-γ, IL-1β, and IL-6. On the other hand, mice receiving IL-10 knockout bone marrow progressed to marked colitis. Interestingly, Y probe analysis revealed that up to 45% of colonic SEMFs were of bone marrow origin in inflamed mucosa about 3 months after bone marrow transplantation, whereas the contribution among the rescued group was approximately 30%.
Conclusion: (1) IL-10 knockout mice were rescued by wild type bone marrow transplantation. (2) The contribution of bone marrow-derived stem cells into colonic SEMFs was significantly increased in the inflamed mucosa compared to non-inflamed mucosa. These engrafted SEMFs may play an important role in mucosal inflammation.
062 OCTN ASSOCIATED WITH CROHN’S DISEASE AND ULCERATIVE COLITIS BUT DOES IT CAUSE IBD?
S. Waller, M. Tremelling, F. Bredin, E. Padfield, J. Hunter, S. Middleton, J. Woodward, M. Parkes.Department of Gastroenterology, University of Cambridge, UK
Background: A haplotype of genetic markers on chr 5q31 has shown replicable linkage and association with Crohn’s disease (CD) (one report suggested specifically for perianal CD), with conflicting data for ulcerative colitis (UC). The region has blocks of tight linkage disequilibrium (LD), hindering fine mapping. Recently putative functional variants in the positional candidate gene OCTN were shown to be associated with CD. Our aim was to replicate this in a large independent dataset, assess the contribution to UC and CD subphenotypes, and identify whether OCTN is disease causing or it is just an LD effect.
Methods: 1100 IBD subjects (495 CD, 515 UC, 90 indeterminate) from the Cambridge/Eastern panel and 750 healthy controls were genotyped by Taqman for the recently reported OCTN variants 1672C->T and 207G->C together with IGR2230C->T, a non-functional IBD5 marker in the same haploblock as OCTN. Chi-squared statistics were applied (STATA) and stratified analysis was performed by phenotype (CD, UC), CD subphenotype (ileal, colonic, perianal) and Nod2-Card15 status (carriage of ⩾1 of the three common variants SNP8, 12, or 13).
Results: OCTN1672T, 207C, and IGR2230 were associated with both CD and UC (see table). There was tight LD between all three markers (D′>0.94). The effect was equal in perianal, colonic, and ileal CD. In contrast to the report of Peltekova et al no IBD cases carried disease associated OCTN variants if they were homozygous for wild type IGR2230. However if lacking OCTN risk alleles carriage rates of IGR2230 risk alleles were similar in cases (0.197) and controls (0.183).
Abstract 62 Allele frequencies (%) and p value v controls for IBD overall
Conclusion: In this large dataset OCTN variants were associated with both UC and CD and were not CD subphenotype specific. Our data are consistent with an aetiological role for OCTN variants or an LD effect.
063 FECAL POLYMERASE CHAIN REACTION IN DIAGNOSIS OF INTESTINAL TUBERCULOSIS
R. Balamurugan, V. Subramanian, B. S. Ramakrishna.(introduced by Dr Richard Pollok, St George’s Hospital, London). Department of Gastrointestinal Sciences, Christian Medical College, Vellore 632204, Tamil Nadu, India
Objective: To evaluate the utility of fecal polymerase chain reaction (PCR) for Mycobacterium tuberculosis (MTB) in the diagnosis of intestinal tuberculosis (TB).
Subjects: Twelve patients with intestinal tuberculosis and 15 healthy adult controls with functional bowel disease were taken as controls. An additional 10 patients with sputum positive pulmonary TB and six patients with treated intestinal tuberculosis were taken as controls. The diagnosis of intestinal TB was based on histology of ileal or colonic endoscopic mucosal biopsies or resection specimens showing granulomas with caseation, detection of acid fast bacilli by stain or by culture, presence of extraintestinal tuberculosis, or by response to antituberculous treatment.
Methods: DNA was extracted from stools of patients with confirmed intestinal tuberculosis and controls. PCR was carried out using oligonucleotide primers for detection of MTB, selected to amplify a 123 base pair fragment of the IS 6100, previously described that is specific for MTB and contains an internal endonuclease site that allows confirmation of the product by digestion with endonuclease SalI. The sequences of the primers were MTB 1 (20 mer): 5′ CCT GCG AGC GTA GGC GTC GG3′ and MTB 2 (20 mer): 5′ CTC GTC CAG CGC CGC TTC GG 3′. Appropriate positive and negative controls were used.
Results: Eleven of the 12 patients with intestinal TB had a positive fecal PCR while all 15 controls were negative. Fecal PCR for MTb identified more patients than pathology which was positive in eight patients and tissue culture for MTB, which was positive in only two patients. None of the patients with treated intestinal Tb had positive fecal PCR while eight of 10 patients with sputum positive pulmonary TB had positive fecal PCR indicating detection of swallowed bacilli from sputum.
Conclusion: Fecal PCR for MTB is a simple, non-invasive test for the identification of patients with intestinal tuberculosis and is superior to both histopathology and tissue culture for MTB.
Neurogastroenterology/motility free papers
064 CILANSETRON IS EFFICACIOUS IN RELIEVING BOWEL HABIT RELATED SYMPTOMS IN IRRITABLE BOWEL SYNDROME WITH DIARRHOEA PREDOMINANCE
F. Mearin1, P. Whorwell2, F. Carter3, S. Caras3, G. Krause4, C. Steinborn4.1Centro Medico Teknon, Barcelona, Spain; 2University Hospital of South Manchester, Manchester, UK; 3Solvay Pharmaceuticals, Inc, Marietta, GA, USA; 4Solvay Pharmaceuticals GmbH, Hannover, Germany
Introduction: Diarrhoea and abdominal pain/discomfort are key symptoms of irritable bowel syndrome with diarrhea predominance (IBS-D). Cilansetron, a new 5-HT3 receptor antagonist, demonstrated adequate relief of IBS symptoms in a significantly greater proportion of IBS-D patients compared with placebo.1–3
Methods: This double blind, placebo controlled, six month multinational study was designed to assess the efficacy of cilansetron on adequate relief of IBS symptoms in Rome defined IBS-D patients. Here we report on abnormal bowel habit related symptoms in patients who were randomised to receive cilansetron 2 mg TID or placebo. Responders to treatment were defined as patients who reported adequate relief of abnormal bowel habits for ⩾50% of their weekly diary responses. End of Treatment means of daily stool frequency (stools/day), consistency (Bristol stool scale), and urgency (Likert scale, 0 = none to 4 = intolerable) were also assessed.
Results: The intent-to-treat population included 792 subjects: 358 males and 434 females. Cilansetron treatment was associated with statistically significant differences over placebo in the adequate relief of abnormal bowel habits (responders rate: 64% v 46%, p<0.001), decreased stool frequency (−1.60 v −1.18, p<0.001), increased stool firmness (−1.40 v −0.73, p<0.001), and decreased urgency (−0.80 v −0.62, p<0.001). Constipation was the most commonly reported adverse event with cilansetron v placebo (12% v 3%); no complications of constipation were observed. There were three suspected cases of ischaemic colitis in the cilansetron group; all resolved without complications.
Conclusion: In subjects with IBS-D, cilansetron treatment provides significant improvement over placebo in the adequate relief of bowel habit related symptoms.
1
2
3
065 PHENOTYPIC CHANGES TO SOMATIC CHEST WALL AFFERENTS OCCUR FOLLOWING EXPERIMENTAL OESOPHAGEAL ACIDIFICATION
R. P. Willert, C. Delaney, K. Kelly, Q. Aziz, A. R. Hobson.GI Sciences, Hope Hospital, University Of Manchester, UK
Introduction: Increased spinal dorsal horn neuronal excitability—that is, central sensitisation (CS), contributes to the development and maintenance of visceral pain hypersensitivity (VPH). We have previously shown that VPH induces allodynia in the region of viscerosomatic referral reflecting viscerosomatic convergence at the spinal dorsal horn. In somatic pain models, allodynia occurs because of phenotypic changes to somatic A-β fibre afferents allowing these afferents, which normally process innocuous sensations, to encode pain. Such changes may help to explain the clinical observation of chest wall (CW) tenderness in non-cardiac chest pain (NCCP). In this study, we wanted to test the hypothesis that chest wall allodynia induced by oesophageal acidification is mediated by CS.
Aim: To provide objective evidence that experimental oesophageal acidification increases excitability in the spinal dorsal horn resulting in potentiation of the A-β fibre mediated somatosensory evoked potential (SSEP) elicited from the CW region of viscerosomatic referral.
Methods: Eight healthy volunteers were studied in a randomised, double blind, placebo controlled, cross over study. Sensation scores and pain thresholds (PT) to electrical stimulation were determined in the proximal oesophagus (PO), chest wall (CW), and foot (somatic control) before and after a 30 minute distal oesophageal infusion of 0.15 M HCl acid or saline. CW SSEPs were recorded at baseline, 30 minutes post acid, and 90 minutes post acid.
Results: Oesophageal acid infusion resulted in a significant increase in the reported sensory scores and a reduction in PT in the PO and CW (p<0.01) but not in the foot (p = 0.12) when compared with saline. Oesophageal acid caused a reduction in the SSEP latency (p<0.001) but had no effect on amplitude (p = 0.2) compared with saline.
Conclusions: The reduction in CW SSEP latency following oesophageal acidification indicates increased afferent recruitment due to enhanced excitability of spinal dorsal horn neurones. The induced CW allodynia most likely represents phenotypic changes in the stimulation properties of A-β fibre afferents in this region of viscerosomatic referral, providing further objective evidence for the role of CS in our model of VPH. In addition, CW SSEP may provide an objective non-invasive electrophysiological technique for assessing CS in NCCP patients that additionally present with referred CW hypersensitivity.
066 DOES REPEATED DISTAL OEOSPHAGEAL ACID EXPOSURE CAUSE A PROGRESSIVE INCREASE IN PROXIMAL OESOPHAGEAL SENSITIVITY TO ELECTRICAL STIMULATION?
P. J. Matthews, C. M. Delaney, A. R. Hobson, Q. Aziz. Department of GI Sciences, Hope Hospital, University of Manchester, Salford M6 8HD, UK
Background: We have previously shown that distal oesophageal acid infusion in normal healthy subjects causes an increase sensitivity to electrical stimulation in the proximal (non acid exposed) oesophagus. However in GORD patients who demonstrate oesophageal hypersensitivity (OH), acid infusion fails to increase their OH. We hypothesised that repeated oesophageal exposure to acid initially causes oesophageal hypersensitivity but then reaches a maximum level where further acid exposure fails to increase OH
Aims: To determine the effect of hourly 5 minute distal oesophageal infusions on proximal oesophageal hypersensitivity.
Method: Eight normal subjects were recruited and after baseline measurements of proximal oesophageal electrical pain thresholds randomised to four infusions of either 40 ml 0.15NHCL or N Saline (control) given at a rate of 8 ml/hr into the distal oesophagus every hour. A ph catheter was placed in the proximal oesophagus to ensure this was not exposed to acid during oesophageal infusions. Infusions were given in a double blinded manner and experiments were performed two weeks apart. Data were analysed by a method of repeated measurements of analysis of variance (ANOVA).
Results: Distal oesophageal acid exposure caused significant proximal oesophageal hypersensitivity to electrical stimulation (area under the curve measurements were: Nsaline −484.4 (SE 223.7) and 0.15MHCL −2224.7 (SE 317.9) (p<0.001)). The first acid infusion caused the greatest increase in oesophageal sensitivity but a maximum level of oesophageal sensitivity was reached and maintained after the third and fourth acid infusions.
Conclusion: Exposure of the distal oesophagus to short acid infusion causes increased proximal oesophageal sensitivity which is maintained by repeated infusions. Patients with functional heartburn may develop OH after small but frequent distal oesophageal acid reflux episodes; however their OH is likely to reach a maximum level with continued acid exposure.
067 IMAGING THE NEURAL CORRELATES OF VISCERAL AND SOMATIC PAIN IN THE BRAINSTEM
P. Dunckley1, R. Wise1, M. Fairhurst1, P. Hobden1, Q. Aziz2, L. Chang3, I. Tracey1.1Departments of Human Anatomy & Genetics and Clinical Neurology, University of Oxford, Centre for the Functional Magnetic Resonance of the Brain, John Radcliffe Hospital, Oxford, UK; 2Department of GI Science, Clinical Sciences Building, University of Manchester, Hope Hospital, Salford M6 8HD, UK; 3Center for Neurovisceral Sciences and Women’s Health, Division of Digestive Diseases, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA
Background and Aims: Gathering evidence from both humans and animals has shown key roles of brainstem centres in the control of ascending nociceptive input. Nuclei such as the rostral ventromedial medulla (RVM) and periaqueductal grey (PAG) are able to both inhibit and facilitate the nociceptive response. It has been proposed that altered descending modulation may underlie many of the chronic pain syndromes (for example, fibromyalgia and irritable bowel syndrome). Yet, to date, no methods have been available for non-invasively investigating brainstem function. We have used functional magnetic resonance imaging (FMRI) to test the feasibility of imaging the neural correlates of visceral and somatic pain within the brainstem.
Methods: Ten healthy subjects were scanned twice at 3 Tesla during which they received matched, moderately painful electrical stimuli to either the midline lower abdomen or rectum.
Results: Significant activation was observed in regions consistent with the PAG, nucleus cuneiformis (NCF), ventral tegmental area/substantia nigra, parabrachial nuclei, nucleus coeruleus, and red nucleus bilaterally and RVM in both groups. Significantly greater activation of the NCF (left and right sided) was observed in the visceral pain group compared with the somatic group. PAG activity correlated with anxiety during visceral stimulation, but not somatic stimulation.
Conclusions: We propose that these differences observed may represent a divergent nocifensive response between the two sensory modalities along with the greater emotive salience of visceral sensation/pain respectively. Non-invasive investigation of brainstem functioning during pain is essential to further our understanding of the contribution of these nuclei to chronic pain syndromes.
068 EFFECT OF ANXIETY ON THE SENSORY AND PERCEPTUAL CHARACTERISTICS OF VISCERAL AND SOMATIC SENSATION
S. F. Worthen, J. Hanison, Q. Aziz, A. R. Hobson.Section of GI Sciences, University Of Manchester, Hope Hospital, UK
Background: Psychological factors are influential in reports of visceral pain. Anxiety and fear focus attention and once directed towards pain, the experience of it changes. Levels of fear and anxiety vary between individuals and their experience of a situation. This study aimed to investigate the effect of anxiety on the sensory/perceptual characteristics of visceral and somatic sensation in individuals that had previously been involved in similar studies (experienced), and those who had not (naïve). Differences between visceral and somatic sensations and the reproducibility of effects were also investigated.
Methods: Fourteen participants (12 male, age range 18–65 years) were investigated on two occasions. Seven (six male) were experienced and seven (six male) were naïve. Electrical stimulation of the oesophagus and non-dominant hand up to the pain threshold was used as the experimental stimuli. Short form McGill questionnaires, Spielberger state trait anxiety inventories, and anxiety Visual Analogue Descriptor scales were used to quantitatively record the experience.
Results: For the experienced participants, pain thresholds were reproducible over two visits for both visceral (47.7 (SD 21.7) and 47.1 (SD 13.9) mA) and somatic (32.0 (SD 22.5) and 35.3 (SD 16.8) mA) stimulation. For naïve volunteers, only the somatic pain thresholds were reproducible (11.4 (SD 5.5) and 12.4 (SD 3.6) mA) as a significant increase in visceral pain threshold was observed from visit one (23 (SD 8.7) mA) to visit two (28.8 (SD 8.7) mA p<0.05). Differences in anxiety measures were reported between the two groups. On visit one anxiety measures were significantly greater for the naïve (41.6 (SD 12.1)) in comparison to the experienced group (25.7 (SD 4.9), p<0.05). There was also a significant decrease in anxiety measures for this same group between the two visits (41.6 (SD 12.1) and 33.8 (SD 5.5), p<0.05).
Conclusions: Prior experience of the procedures produced lower levels of anxiety and higher pain thresholds. The observed difference in anxiety for naïve volunteers between the two visits has potential implications for patient studies of gastrointestinal dysfunction. It may be that the visceral hypersensitivity observed in patients is not symptom-specific, but rather is simply the effect of anxiety due to the nature of a novel experimental procedure.
Colorectal free papers
069 THE ROLE OF ASPIRIN, NSAID, AND ANTICOAGULANTS IN THE INCREASING INCIDENCE OF ACUTE LOWER GASTROINTESTINAL TRACT BLEEDING OVER 10 YEARS
B. Vijayan, D. L. Armour, A. Fraser, J. Masson, N. A. G. Mowat.Aberdeen Royal Infirmary, Aberdeen, UK
Background: Aspirin, NSAID, and anticoagulants have been associated with both upper and lower gastrointestinal tract bleeding. However, there are no long term prospective studies within well defined communities about the impact of these medications on the natural history of acute lower gastrointestinal bleeding (ALGIB).
Aims: To assess the incidence, severity, complications, and mortality of ALGIB in patients taking aspirin, NSAID, and anticoagulants.
Methods: All patients presenting with ALGIB to the dedicated bleeding unit serving Grampian region from October 1991 to October 2001 were included in the study. Data were collected prospectively and stored on Microsoft Access database for later analysis.
Results: 1472 patients (53% female) had confirmed ALGIB. The mean age was 66 years and 69% were aged over 60. Regular intake of aspirin, NSAID, or anticoagulant on admission was identified in 663 patients (45%). The number of patients not on these drugs remained stable over the study period; however an increase in the number of patients taking the above prescription drugs was noted in the latter half of the study period. Those patients on medications were more likely to have a significant bleed (57%), increased risk of both rebleeding and mortality, but no difference was evident in surgery rates.
Conclusions: The increased use of aspirin, NSAIDs, and anticoagulants in this community has resulted in:
-
Increase in the number of patients admitted with ALGIB.
-
Increase in the number of significant bleeds.
-
Increased rebleeding and mortality rates compared with those not taking any of the above three medications, and therefore requires a review of prescription policy, especially in the elderly.
Abstract 69
070 THE POTENTIAL USE OF FAECAL DIMERIC M2 PYRUVATE KINASE (TUMOUR M2-PK) IN SCREENING FOR COLORECTAL CANCER
K. Koss1, D. Maxton1, J. A. Z. Jankowski2.1Gastroenterology Department, Royal Shrewsbury Hospital, Shrewsbury, UK; 2Digestive Diseases Centre, University Department of Genetics and Molecular Medicine, Leicester Royal Infirmary, Leicester, UK
Background: M2-PK is commonly over expressed in proliferating cells and its dimeric form is mainly predominant in tumour cells. It may therefore be a suitable biomarker for colorectal cancer screening. We conducted a pilot study to see if dimeric M2-PK in faeces enabled us to discriminate between patients with and without colorectal cancer or polyps.
Aim: To assess the sensitivity and specificity of faecal dimeric M2-PK (tumour M2-PK) in patients with colorectal cancer or polyps.
Methods: A prospective study of 45 patients (28 males and 17 females) with a median age of 65 years (range 24–86) undergoing colonoscopy. Stool samples were tested by readily available sandwich ELISA with monoclonal antibodies against dimeric M2-PK.
Results: Thirteen patients underwent normal colonoscopy with a median faecal tumour M2-PK level of 1.85 U/ml (range 0.9–3.41). Eight patients had one or more polyps. Median faecal tumour M2-PK level in five patients with >1 cm polyps was 5.32 U/ml (range 0.9–29.46) and 1.09 U/ml (range 0.9–1.2) in three patients with <1 cm polyps.
Twenty four patients with adenocarcinomas (left colon 20, right colon 4) had increased median faecal tumour M2-PK level of 11.43 U/ml (range 1.71–111.75). At the cut-off level (median +2SD for normal population) of 3.43 U/ml the sensitivity of tumour M2-PK was as follows: colorectal cancer 87.5%, >1 cm polyps 60%, <1 cm polyps 0%. The calculated specificity was 100%.
Conclusion: Faecal tumour M2-PK assay has a high sensitivity and specificity for detecting colorectal cancer and large (>1 cm) colorectal polyps. These results suggest that faecal tumour M2-PK is a new promising, non-invasive screening tool. A larger study is now required.
071 COST COMPARISON BETWEEN STENTING AND SURGERY FOR MALIGNANT COLORECTAL OBSTRUCTION IN ENGLAND
M. C. Parker1, N. Verin2.1Colorectal Surgery, Darent Valley Hospital, Dartford, UK; 2Health Economics, Boston Scientific, Nanterre, France
Aim: Colorectal stents have been developed to treat malignant obstruction of the colon. They have been proved to be a safe and effective treatment for palliation and for colon decompression prior to elective surgery (“bridge to surgery” stenting). Our aim was to compare the hospital costs of stenting versus surgery: palliative stenting versus elective surgery as well as bridge to surgery versus emergency surgery.
Methods: An interactive model was developed to calculate the hospital cost from an NHS Hospital Trust perspective. Hospital resource use (material, staff, procedure time, and length of stay) was derived from a retrospective review of case notes, expert opinion, and Hospital Episode Statistics. Unit costs were taken from the literature and the UK Personal Social Services Research Unit.
Results: For palliative purposes, average hospital cost per patient was £2052 for a stenting procedure and £4704 for an elective surgical procedure. Stenting reduces the cost of palliative treatment by 56% compared with surgery. This difference is mainly explained by the shorter hospital stay (10.8 days v 2.5 days). For resectable patients, average hospital cost per patient was £6847 for a “bridge to surgery” (stenting and one stage resection), and £11 553 for an emergency surgical procedure. The placement of a stent for decompression before an elective surgical intervention reduces the cost of treatment by 41% compared with emergency surgery. This difference is mainly due to a shorter hospital stay (13.5 days v 23 days). Moreover, patients treated electively do not need to stay in intensive care, which diminishes their treatment cost.
Conclusion: The analysis shows that the placement of colorectal stents reduces hospital costs compared with surgical alternatives. In addition to the potential financial savings, the shorter hospital stay allows centres to free up capacity in terms of bed days.
072 PROTEOMICS: A NEW TOOL FOR SCREENING FOR COLON CANCER?
A. M. Lennon1, A. C. Tan1, F. Gleeson2, A. Brannigan3, J. R. Lennon3, J. O’Sullivan4, A. White4, D. keegan4, H. Mulcahy4, J. M. Hyland4, K. Sheahan4, D. P. O’Donoghue4, R. Brown1.1Department of Medical Oncology, Glasgow University, Glasgow, UK; 2Department of Bioinformatics, Glasgow University, Glasgow, UK; 3The Mater Misericordiae Hospital, Dublin, Ireland; 4The Centre for Colorectal Disease, St Vincent’s University Hospital, Dublin, Ireland
Aims: The aim of this pilot study was to determine if protein profiles generated using SELDI-MS could differentiate patients with colorectal cancer, dysplastic polyps, or normal colons.
Methods: 5 ml of plasma was collected from patients with colorectal cancer, dysplastic polyps, and patients who had undergone a normal full colonoscopy. The plasma was fractionated using an anion exchange column and fraction 1 was applied to a CM-10 ProteinChip. Protein profiles were generated using a PBSII ProteinChip Reader Peaks, with protein peaks detected by Biomarker Wizard. A J48 decision analysis tree was developed to identify differentially expressed protein peaks.
Results: The J48 decision analysis tree was able to differentiate normal from polyp/tumour samples with 88.2% sensitivity and 99.2% specificity.
Conclusion: This pilot study provides encouraging results which suggest that protein profiling may have a role to play in screening for colorectal cancer. A larger, prospective study should now be undertaken to confirm these results.
073 DIRECT ACCESS COLONOSCOPY: A COST EFFECTIVE INVESTIGATION FOR TWO WEEK RULE COLORECTAL CANCER REFERRALS
M. Mulchandani1, K. Maruthachalam1, R. K. Jain1, E. Stoker2, A. F. Horgan1.Department of 1Colorectal Surgery and 2Endoscopy, Freeman Hospital, Newcastle upon Tyne, UK
Background: In the Newcastle upon Tyne NHS trust patients are referred under the lower GI two week rule for either a direct access colonoscopy or an outpatient visit at the discretion of the referring general practitioner.
Aim: To calculate the cost of investigating a patient referred under the two week rule for colorectal cancer and compare the cost of direct access colonoscopy v outpatient referrals.
Methods: Retrospective study of data obtained from case notes and endoscopy records of all lower GI two week rule referrals in 2001 and 2002.
Results: 766 patients were referred in two years. 167 patients underwent direct access colonoscopy (DAC) and 599 patients were seen in outpatient clinic. Out of the 599 patients, 495 patients were investigated subsequently by colonoscopy and 17 had a Barium enema. 49 patients did not need further investigations and were discharged from clinic. The average cost of a colonoscopy was £396, a single outpatient visit £128, and that of a barium enema £136. The total cost of investigating patients through DAC was £66 132 and through outpatients was £275 004.
Conclusions: DAC would have resulted in savings of £37 802 if all 766 patients had been referred through this pathway. The projected two week rule referrals for Newcastle in the year 2004 are 800 patients. If the referrals are appropriate, considering the above figures, DAC would result in savings of approximately £70 000.The practice of referring patients for DAC needs to be reviewed. With increasing number of two week rule colorectal referrals DAC will be a cost effective investigation.
Plenary session
074 NATIONAL RESULTS OF AN ENDOSCOPY UNIT GLOBAL RATING SCALE
A. I. Thuraisingam1, V. Tailor2, D. Johnston2, L. Allan2, R. M. Valori1,2.1Gloucestershire Hospitals NHS Trust, Gloucester; 2National Endoscopy Team, NHS Modernisation Agency, St John’s House, East Street, Leicester, UK
Aim: To obtain a national, patient centred view of endoscopy units.
Methods: All endoscopy units in England were requested to complete anonymously a 12 item rating scale for their unit. Items were derived after consultation with those working in the service. Each item was defined by four descriptors (1–4) that described the level achieved, with 4 being best practice. Clinical and nurse leads for the unit were asked to complete the scale. If varying levels of service occurred between clinical teams it was recommended the lowest level score be recorded.
Results: 193 out of 214 endoscopy units responded. The percentage of units scoring for each item is shown in the table.
Abstract 74
Discussion: The results demonstrate considerable variation in practice between units; enable service deficiencies to be highlighted; provide a driver for quality change; and afford a means of unit comparison with Strategic Health Authority and National results. The global rating scale was self-reported but will be repeated (with objective measures to underpin its validity) to allow monitoring longitudinally over time.
075 WHAT IS THE CLINICAL EFFECTIVENESS OF ENDOSCOPY UNDERTAKEN BY NURSES? MULTI-INSTITUTION NURSE ENDOSCOPY TRIAL (MINUET) - ISRCTN 82765705
D. Durai1, J. G. Williams1, I. T. Russell2, W. Y. Cheung1, A. Farrin3 on behalf of MINuET team1University of Wales Swansea, UK; 2University of Wales Bangor, UK; 3York Trials Unit
Introduction: Nurses are increasingly undertaking gastrointestinal (GI) endoscopy, but no randomised trial has been undertaken to confirm the clinical effectiveness of this. This study is a UK multicentre, pragmatic randomised controlled trial designed to evaluate clinical effectiveness of upper and lower GI endoscopy undertaken by nurses.
Methods: Patients >18 years of age referred for investigation of dyspepsia, weight loss, anaemia, change in bowel habit, or bleeding PR were considered for inclusion. Those for a therapeutic procedure were excluded. Randomisation stratified by centre took place before patients were sent for and given an opportunity to request change of endoscopist. 19 centres took part in the flexible sigmoidoscopy subtrial and nine in the OGD subtrial. The primary outcome measure was the Gastrointestinal Symptom Rating Questionnaire (GSRQ). Secondary outcome measures were SF36, STAI, and Gastrointestinal Endoscopy Satisfaction Questionnaire (GESQ). Patients completed questionnaires at baseline, 1 day, 1 month, and 1 year post endoscopy. Primary analysis was by intention to scope. A random sample of OGD video recordings were analysed using a validated objective scale.
Results: 1856 patients were recruited and 914 allocated to a doctor for endoscopy and 942 to a nurse. Five patients requested a change of endoscopist (four from doctor to a nurse, one from nurse to a doctor). There were no significant difference in the GSRQ, SF-36, and STAI scores between the two groups at 1 month and 1 year. Patients in the nurse group were more satisfied (p<0.001). On evaluation of OGD videos nurses scored better in thoroughness of examination of stomach (p<0.0001). There were no significant differences in new GI diagnosis made at one year.
Conclusion: There is no difference in clinical effectiveness of upper and lower GI endoscopies undertaken by doctors and nurses, but patients are more satisfied with nurses. Nurses are more thorough in OGD performance.
076 CROHN’S DISEASE AND COLON CANCER MUCOSA ASSOCIATED ESCHERICHIA COLI STIMULATE COLON EPITHELIAL IL-8 PRODUCTION THROUGH THE EXTRACELLULAR SIGNAL-REGULATED KINASE AND P38 MITOGEN ACTIVATED PROTEIN KINASE PATHWAYS
S. Subramanian, B. Tam, J. M. Rhodes, B. Campbell.Division of Gastroenterology, School of Clinical Sciences, University of Liverpool, Liverpool, L69 3BX, UK
Background: We previously showed increased mucosa-associated E coli below the colonic mucus layer in Crohn’s disease and colon cancer. These E coli induce release of interleukin-8 (IL-8) from HT29 colon epithelial cells (
) but the mechanism for this response was unknown.
Aim: To elucidate the mechanism of the colon epithelial IL-8 response to E coli isolates from Crohn’s disease and colon cancer.
Methods: Confluent HT29 cells were incubated in triplicate for up to 8 hours with E coli isolates at a bacterium:cell ratio of 10:1. E coli were also incubated for 4 hours with HT29 cells pretreated either with U0126, SB203580, or SP600125 (60–90 minutes, at 10 μM), specific inhibitors of activation of extracellular signal-regulated kinase (ERK) 1/2, p38 and Jun N-terminal kinase (JNK) members of the mitogen activated protein kinase (MAPK) family. IL-8 release was measured by ELISA. ERK1/2, p38, and JNK activation were assessed by immunoblotting.
Results: All seven E coli isolates from Crohn’s disease patients provoked IL-8 release, with a median response of 1014 pg/ml at 8 hours (range 640–1900) compared with untreated controls, 143 pg/ml (range 29–242); p<0.025 ANOVA). Similar results were seen with all 14 cancer isolates (p<0.04). Pretreatment of HT29 cells with U0126 resulted in a 69% median reduction (range 39–80) in secreted IL-8 to all E coli isolates tested (n = 21). More specific investigation of two representative isolates from Crohn’s disease and colon cancer showed that following bacterial treatment, ERK1/2 activation (p44/p42) was initiated within 5 minutes, sustained for 1 hour, blocked by U0126 with resultant IL-8 secretion reduced by 89 and 91% (both p<0.001 ANOVA; n = 3). p38 pathway inhibition with SB203580 also resulted in reduced IL-8 secretion to all 21 isolates (median 72%, range 19–98). However, JNK inhibition by SP600125 resulted in low or no reduction of IL-8 release in response to E coli isolates (median 34%; range −12 to 54%, n = 21). Any JNK activation by E coli was seen at 60 minutes.
Conclusions: Crohn’s disease and colon cancer mucosa-associated E coli, although lacking known pathogenicity genes, mediate release of IL-8 from colon epithelial cells through activation of ERK1/2 and p38, thus implicating these host cell-signalling pathways as potential targets for therapeutic intervention.
077 SURVIVAL AT SIX WEEKS OF CIRRHOTIC PATIENTS ADMITTED TO AN INTENSIVE CARE UNIT
E. Cholongitas, M. Senzolo, K. Kwong, D. Patch, V. N. Nikolopoulou, G. Leandro, S. Shaw1, A. K. Burroughs.Liver Transplantation and Hepatobiliary Unit, 1Department of Intensive Care, Royal Free Hospital, London, UK
Background: There is a high mortality rate in cirrhotics admitted to an intensive care unit (ICU). Most ICU scores are derived from populations without many cirrhotics.
Aim: To evaluate the factors associated with 6 week survival in cirrhotics admitted to ICU and to assess established scores.
Patients and Methods: 312 cirrhotics (182 male, mean age 49.6 (SD 11.5) years) were consecutively admitted. At admission, 40 variables, including admission calendar year, were available to derive a multivariable logistic regression model. Child-Pugh (CP), MELD, Apache II, and SOFA scores on admission were evaluated and compared by ROC curves. Complications and therapeutic interventions during ICU stay were recorded.
Results: Cirrhosis was alcoholic in 65%; ventilation needed in 88%, renal failure in 41%. The median length of stay in ICU was 4 (range 1–48) days. The median CP, Apache II, MELD, and SOFA scores were 11, 18, 24, and 11 respectively. Mortality was 65% (n = 203) at 6 weeks. The cause of death was multiple organ failure in 45%. Factors independently associated with 6 week survival on admission were: fewer organs failing (<3 = 51.5%, ⩾3 = 10%) and per unit log, lower FiO2 (OR = 0.04, 95% CI 0.04 to 0.51), lactate (OR = 0.76, 95% CI 0.64 to 0.90), urea (OR = 0.94, 95% CI 0.90 to 0.99) and bilirubin (OR = 0.996, 95% CI 0.992 to 0.999). Predictive value of outcome in terms of ROC was best for SOFA followed by MELD score.
Conclusions: A specific prognostic score for cirrhotics admitted to ICU can be derived in this large cohort as key markers of organ function were prognostic: FiO2 (respiratory), bilirubin (hepatic), urea (renal, hepatic), lactate (hepatic, renal) as well as three or more failing organs (resulting in 90% mortality). The established ICU scores, SOFA and MELD, which contain the above variables, or their surrogates, offered better prediction than Apache II or CP scores.
Gastrointestinal physiology associates group
078 THE EFFECTS OF POSTURE ON GASTRIC EMPTYING: A MAGNETIC RESONANCE IMAGING STUDY
M. Fox1,2, A. Steingötter3, P. Boesinger3, M. Fried2, W. Schwizer2.1St Thomas’ Hospital, London, UK; 2Division of Gastroenterology and 3Institute for Biomedical Engineering, University Zurich, Switzerland
Background: Gastric emptying proceeds despite changes in body position. The effect of position on the rate of gastric emptying and the physiological mechanisms that drive gastric emptying are poorly understood. Specifically it is unclear whether tonic or peristaltic contraction drives gastric emptying. MRI is a non-invasive investigation with which these processes can be studied, providing quantitative assessment of multiple aspects of gastrointestinal structure and function.
Patients and Methods: Twelve volunteers were investigated in the seated position (SP) and the upside-down position (UP) after ingestion of 300 ml non-nutrient liquid meal. Gastric emptying, intragastric distribution, peristaltic and tonic gastric motor function were measured using an open configuration MRI. The contribution of peristalsis and tonic contraction to gastric emptying was assessed.
Results: A marked difference in distal/proximal intragastric distribution between UP and SP was observed (7% v 40%; p<0.01). The rate of gastric emptying was similar in both positions but emptying pattern was linear in UP and exponential in SP (p<0.05). Peristalsis was slower in UP than SP (2.8 v 3.0 min−1; p<0.01). Propagating waves were observed to transport fluid against gravity in UP; however no correlation between peristaltic frequency and gastric emptying was present. Postprandial tonic relaxation of the stomach (“accommodation”) was greater in UP than SP (AUC gastric volume 6196 v 5372 ml/min; p<0.05). A negative correlation between tonic response and the rate of gastric emptying was present in SP (r2 = 0.46; p<0.01). No correlation was present in UP.
Conclusions: The stomach maintains the rate of gastric emptying for a non-nutrient liquid meal despite radical changes in body position and intragastric distribution. Gastric emptying is driven by tonic contraction (“pressure pump”) in SP but not in UP. Peristaltic transport of liquid appears to be important for gastric emptying in UP; however peristaltic frequency does not affect the rate of gastric emptying.
079 DAY TO DAY VARIABILITY OF 48 HOUR OESOPHAGEAL PH MONITORING BY BRAVO CAPSULE
A. Anggiansah, M. Fox, R. Anggiansah, R. C. Mason, T. Wong.Department of Gastroenterology and Oesophageal Laboratory, St Thomas’ Hospital, London, UK
Introduction: The wireless Bravo capsule is an innovative, catheter-free pH monitoring system. Following endoscopic placement the device monitors intraoesophageal pH over 48 hours. This provides an opportunity to examine day to day reproducibility in ambulatory intraoesophageal pH recordings and whether the extended recording period improves reliability/diagnostic yield of the test.
Methods: Eighteen consecutive patients (median age 45 (range 29–67 years)) with reflux symptoms referred for Bravo pH studies. The day to day concordance of pH measurements was assessed over 24 hours, and in the upright and supine positions. In addition, patients were classified as having either abnormal or normal acid exposure on both test days and in both positions (defined as >4.2% pH<4/24 hour (>3.4% supine, >8.3% upright)). Diagnostic reproducibility was calculated by comparing the diagnostic classification on day 1 and 2 (kappa (κ) value). The potential diagnostic yield and accuracy from the 48 hour recording was assessed.
Results: 48 hour pH studies for 16/18 patients were available (deployment failure (n = 1) recording incomplete (n = 1)). 48 hour acid exposure±day to day variance was 7.3±2.6%, variance was higher in the supine position (7.3±1.8% upright, 5.8±5.1% supine, p<0.01) and increased with reflux severity (p<0.01). Day 1 to day 2 acid exposure had 51% concordance, (72% upright, 47% supine). In terms of diagnostic classification, 10/16 patients had abnormal acid exposure day 1 and 13/16 day 2 (κ 0.47). Diagnostic reproducibility was good in the upright (κ 0.71) but poor in the supine (κ 0.41) position. No patient had normal acid exposure on day 2 that had abnormal acid reflux on day 1.
Conclusions: The day 1 to day 2 concordance of Bravo pH measurements was fair, being good in the upright but poor in the supine position. Variability in the supine position also impaired day to day diagnostic reproducibility. These results are similar to earlier reports (Pandolfino 03) and appear less favourable than those reported for conventional systems (Johnsson 88). Acid exposure and diagnostic yield were higher day 2; this may reflect a return to normal daily activity.
080 THE EFFECTS OF LUMINALLY GENERATED NITRIC OXIDE ON THE RESTING TONE OF THE HUMAN LOWER OESOPHAGEAL SPHINCTER IN THE FASTING STATE
J. J. Manning, A. Wirz, K. E. L. McColl.Western Infirmary, Glasgow, UK
Introduction: Nitric oxide (NO) is generated in high concentrations in the upper gastrointestinal tract. Approximately 25% of dietary nitrates are recycled to the salivary glands. This nitrate is then secreted into the mouth and then 25% converted to nitrite by buccal bacteria. NO is generated when the swallowed nitrite encounters a healthy stomach, secreting both hydrochloric and ascorbic acid. This takes place just distal to the pH step-up point at the gastric cardia. Neuronally generated NO plays a key role in the relaxation of the lower oesophageal sphincter (LOS) and clearance of acid from the oesophagus. Our hypothesis is that the high concentrations of NO produced physiologically in the lumen of the LOS will reduce its resting pressure, rendering the patient more susceptible to acid reflux.
Aim: To see if LOS pressure is affected following exposure to physiological concentrations of luminal nitric oxide.
Method: Twelve healthy, H pylori negative volunteers were examined. A water perfused manometry catheter was passed nasogastrically. Following baseline recordings the catheter was re-inserted and taped in position. Two blinded, sequential infusions were perfused through channels on the catheter located at the pH step-up point for 30 minutes each, one a NO generating solution and the other a nitrate based control. Measurements were made after each infusion. The order of infusions was reversed on a separate study day.
Results: There was no statistical difference between the resting LOS pressures of the two groups: nitrate 23.7 mm Hg v nitrite 23.9 mm Hg (p<0.96), taking into account the order of solution delivery. There was also no statistically significant change in total sphincter length, abdominal sphincter length, and position of the sphincter lower border.
Conclusion: Physiological concentrations of NO delivered to the gastric cardia of healthy volunteers do not cause a reduction in the resting LOS pressure while in the fasting state. We postulate that luminal NO may prove to have a greater effect on the LOS when it is under stress, such as in the post-prandial state.
081 IRRITABLE BOWEL SYNDROME IS RARELY ASSOCIATED WITH SMALL INTESTINAL BACTERIAL OVERGROWTH IN THE UK
R. Lea, K. Solanki1, L. Sinha, P. Vales1, J. M. Hebden.Department of Gastroenterology and 1GI Physiology, Manchester Royal Infirmary, Oxford Road, Manchester, UK
Background: Irritable bowel syndrome (IBS) is usually diagnosed when symptom based diagnostic criteria are fulfilled in the absence of any evidence of relevant organic disease. Small intestinal bacterial overgrowth (SIBO) may cause symptoms similar to IBS, and hence lead to diagnostic confusion; however the recent BSG guidelines do not suggest specifically excluding this condition as a possibility in IBS patients.1 Nevertheless, two studies have reported that the majority of IBS patients do indeed have evidence of SIBO when hydrogen breath testing is performed, and that many such patients improve symptomatically following appropriate antibiotic therapy.23
Aim: To prospectively investigate the prevalence of SIBO in IBS patients attending a general gastroenterology clinic in the UK.
Methods: Twenty consecutive outpatients diagnosed with IBS according to Rome II criteria supported by clinically appropriate investigations underwent glucose hydrogen breath tests using standard techniques. A positive test was defined as a rise in breath hydrogen of >20 ppm over baseline.
Results: Eleven patients (55%) aged 26–65 years had diarrhoea predominant IBS (D-IBS) (9F), six patients (30%) aged 25–73 years were constipation predominant (6F), and three patients (15%) aged 44–64 years had alternating type IBS (3F). Only two patients (10%), both with D-IBS, had evidence of SIBO and both of these improved following antibiotic therapy; the remaining 18 (90%) IBS patients had negative breath tests. Neither patient with SIBO had any evidence of a recognised predisposing condition.
Conclusion: Rome II positive IBS patients have a low prevalence of SIBO.
1
2
3
Inflammatory bowel disease symposium
082 INFLIXIMAB FOR THE TREATMENT OF PYODERMA GANGRENOSUM: A RANDOMISED, DOUBLE BLIND PLACEBO CONTROLLED TRIAL
T. N. Brooklyn1, A. Shetty2, J. Bowden3, C. E. Griffiths3, G. Dunnill1, A. Forbes2, R. Greenwood1, C. S. Probert1.1Bristol Royal Infirmary, Bristol, UK; 2St Marks Hospital, Middlesex, UK; 3Hope Hospital, Manchester, UK
Introduction: Pyoderma gangrenosum (PG) is a chronic ulcerating skin condition that often occurs in association with inflammatory bowel disease (IBD). There have been a number of reports of PG responding to infliximab, a monoclonal antibody against tumour necrosis factor alpha (TNFα). In the first randomised placebo controlled trial of any drug for the treatment of PG, we have studied of role of infliximab in this disorder.
Methods: Patients with a clinical diagnosis of PG were randomised to receive an infusion of infliximab at 5 mg/kg or placebo. Patients were assessed at 2 weeks and non-responders were offered open labelled infliximab. Patients were assessed again at week 4 and week 6. The primary end point was clinical improvement at week 2, with secondary end points being remission and improvement at week 6.
Results: Thirty patients were entered into the study. After randomisation, 13 patients received infliximab at a dose of 5 mg per kilogram and 17 patients received placebo. At week 2, significantly more patients in the infliximab group had improved 46% (6/13) compared with the placebo group 6% (1/17), p = 0.025. 23 patients who had not improved by week 2 were offered open label infliximab, all accepted the treatment. Overall, 29 patients received infliximab with 69% (20/29) demonstrating a clinical response. The remission rate at week 6 was 21% (6/29). There was no response in 31% (9/29) of patients.
Conclusion: This short term study has demonstrated that infliximab at a dose of 5 mg/kg is superior to placebo in the treatment of PG. Open label treatment with infliximab also produced promising results. Infliximab treatment should be considered in patients with PG, irrespective of whether they have coexistent IBD or not.
083 MAINTENANCE THERAPY WITH NATALIZUMAB IMPROVES QUALITY OF LIFE IN PATIENTS WITH CROHN’S DISEASE
S. Ghosh1, M. Allison2, C. Nwokolo3, J. Plevris4, J. Sanderson1, J. Shaffer5, S. Schreiber6, P. Rutgeerts7, W. Sandborn8, J-FColombel9.1London, UK; 2Newport Gwent, UK; 3Coventry, UK; 4Edinburgh, UK; 5Manchester, UK; 6Kiel, Germany; 7Leuven, Belgium; 8Minnesota, USA; 9Lille, France
Background and Aim: Maintenance therapy with natalizumab (a humanised monoclonal IgG4 antibody to α4 integrin) in the ENACT trials was associated with significantly higher rates of sustained response and remission in patients with Crohn’s disease (CD) through 15 months compared with placebo (PLC). Additional efficacy analyses included quality of life (QoL) assessments. Data from the European Quality of Life-5D (EQ-5D) Health Questionnaire at month 15 are presented.
Patients and Methods: Adult patients with CD (n = 339) who achieved response (⩾70 point reduction in baseline Crohn’s Disease Activity Index (CDAI) and/or remission CDAI<150) and had a CDAI score <220 after three infusions of natalizumab in ENACT-1 were re-randomised to natalizumab (n = 168, 300 mg) or PLC (n = 171) and received up to 12 additional monthly infusions in ENACT-2. QoL assessments were completed at months 3, 6, 9, 12, and 15.
Results: At month 15, a greater proportion of patients in the natalizumab group reported no problems in each of the five categories of the EQ-5D compared with the PLC group (no mobility problems, 69% v 53%; no self-care problems, 81% v 65%; no problems performing usual activities, 63% v 30%; no pain or discomfort, 33 v 16%; not anxious/depressed, 55% v 35%; formal statistical tests were not performed). At month 15, the mean change (standard deviation) from baseline of ENACT-1 in the visual analog scale (VAS) component of the EQ-5D was 27.3 (SD 24.5) for patients in the natalizumab group compared with 16.8 (SD 26.5) for patients in the PLC group (p<0.001). Scores on this scale range from 0–100. Higher scores represent improved perceptions of health.
Conclusion: Improvements observed in the components of the EQ-5D are consistent with sustained response and remission rates observed in CD patients through 15 months of continuous treatment with natalizumab compared with PLC.
084 NATURAL KILLER CELL NUMBERS ARE INCREASED BY STRESS AND DECREASED BY HYPNOTHERAPY IN PATIENTS WITH ULCERATIVE COLITIS
J. E. Mawdsley, D. G. Jenkins, M. G. Macey, D. S. Rampton.Research Centre for Gastroenterology, Barts and the London, Queen Mary School of Medicine and Dentistry, London, UK
Introduction: Psychological stress is reported to worsen ulcerative colitis (UC). Hypnosis is effective for functional GI disorders. Although claimed by some patients to improve UC, the possible mechanisms are unknown. Natural killer (NK) cells may have a pathogenic role in IBD and changes in their number occur in stress related conditions.
Aim: To compare the effects of psychological stress and hypnotherapy on NK cell numbers in patients with UC.
Method: Three experimental protocols were used:
-
Stress. Patients with inactive UC underwent an acute psychological stress test, performing an IQ test for 50 minutes, while listening to different music in each ear.
-
Hypnotherapy. Patients with active UC (SCCAI ⩾4, Baron score ⩾2) underwent gut-focused hypnotherapy for 50 minutes.
-
Control. Patients with UC listened to relaxing music for 50 minutes.
Blood was taken before, at the end, and 30 minutes after each protocol for flow cytometric analysis of NK cells (% leucocytes CD16, CD56).
Results: See table.
Abstract 84 NK cells (% leucocytes)
Conclusions: Acute psychological stress increases NK cell number, whereas hypnotherapy decreases NK cell number in patients with UC. These changes could play a pathogenic role in the induction of relapse by psychological stress in quiescent UC and explain some of the reported benefits of hypnotherapy in active disease.
085 PREBIOTIC FRUCTO-OLIGOSACCHARIDE AS A THERAPY FOR CROHN’S DISEASE: AN OPEN LABEL TRIAL
J. O. Lindsay1, K. Whelan2, A. Stagg3, P. Gobin2, H. Omar3, M. A. Kamm1, S. C. Knight3, A. Forbes1.1St Mark’s Hospital, London; 2Department of Nutrition and Dietetics, King’s College London; 3Antigen Presentation Research Group, Imperial College London
Introduction: The intestinal microbiota play a pivotal role in the inflammation associated with Crohn’s disease. Individual bacterial species may induce proinflammatory or immunoregulatory responses that are mediated by pattern recognition receptors, such as toll like receptors (TLR), present on mucosal dendritic cells. Bifidobacteria appear immunoregulatory and increase dendritic cell IL-10 production in vitro. Fructo-oligosaccharides (FOS) are bifidogenic in healthy volunteers, although their effect in patients with Crohn’s disease is not known.
Aims: To assess the effect of oral FOS on disease activity, stool bifidobacteria, and mucosal dendritic cell function in patients with moderately active Crohn’s disease.
Methods: Ten patients with active ileocolonic Crohn’s disease received 15 g/day FOS for three weeks. Disease activity was measured using the Harvey Bradshaw Index (HBI). Faecal bifidobacteria were quantified by fluorescent in situ hybridisation. Mucosal dendritic cell IL-10 production and TLR expression were assessed by flow cytometry of dissociated rectal biopsies.
Results: Dietary supplementation with 15 g/day FOS was well tolerated and resulted in a reduction in mean (standard deviation) HBI from 9.8 (SD 3.1) to 6.9 (SD 3.4) (p<0.01). There was an increase in faecal bifidobacteria from 8.8 (SD 0.9) to 9.4 (SD 0.9) log10 cells/g dry faeces (p<0.005). The percentage of IL-10 positive dendritic cells increased from 30 (SD 38) to 53 (SD 33) (p = 0.06). In addition, the percentage of dendritic cells expressing TLR 2 and TLR 4 increased from 1.7 (SD 3.4) to 36.8 (SD 32) (p = 0.08) and 3.6 (SD 7.1) to 75.4 (SD 7.9) (p<0.001), respectively.
Conclusions: Fructo-oligosaccharides increase faecal bifidobacteria concentrations and modify both mucosal dendritic cell IL-10 production and TLR expression. This novel therapeutic strategy decreases Crohn’s disease activity and warrants further investigation in a controlled trial.
Cell/molecular biology free papers
086 CLUSTERS OF PHENOTYPICALLY RELATED HUMAN COLONIC CRYPTS DEVELOP THROUGH CRYPT FISSION: IMPLICATIONS FOR COLORECTAL CARCINOGENESIS
S. L. Preston1, S. A. C. McDonald1, D. Oukrif1, L. Greaves2, D. Turnbull2, P. Tadrous1, P. Sasieni1, J. A. Jankowski1, M. Novelli1, N. A. Wright1.1Cancer Research UK; 2University of Newcastle upon Tyne, UK
Introduction: It has been proposed that colorectal cancer is caused by the accumulation of DNA mutations in colonic stem cells. Crypt fission (a crypt splitting to form two daughter crypts) is a likely method by which these mutations spread through the colon. Crypts within close proximity to each other should therefore be genetically related. Mitochondrial (mt) cytochrome c oxidase subunit I (cox) was used as a marker of crypt clonality, as mtDNA has a relatively high mutation rate compared to nuclear DNA.
Aim: To investigate whether colonic crypts with cox mutations are clustered.
Methods: Immunohistochemistry for cox was performed on en face sections of normal colonic tissue (from 14 patients undergoing resection). In two patients sequencing of the mt genome was performed on laser captured, cox negative crypts as well as their closest cox positive neighbours. In a further experiment, all crypts within images of each section from all patients were labelled as cox negative or cox positive, and a computer program used to identify clusters of negative crypts by comparison to 1000 iterations of a random assignation of these labels. This was repeated on multiple sections per patient by three independent investigators.
Results: In patient 1, all six crypts had the exactly the same mtDNA sequence except that the three neighbouring cox negative crypts had a 6277 G-A transition (which predicts a Gly125Asp amino acid substitution within cox)—this was not present in the three adjacent cox-positive crypts. In patient 2, a 7275 T-C transition predicting a Ser458Pro substitution within cox was found only in the adjoining cox-negative crypts. All 14 patients exhibited clustering of cox-negative crypts with each having a relative prevalence (a negative crypt having a negative neighbour) of greater than 1. When compared with the random iterations this was significant in 12/14 patients (p<0.05). Conclusions: Related colonic crypts are clustered. This supports crypt fission as a mechanism by which DNA mutations spread and has important implications for colorectal tumourigenesis.
087 A ROLE FOR EMT REGULATORS IN OESOPHAGEAL ADENOCARCINOMA
P. Jethwa, D. van Dellen, P. Taniere, R. T. Spychal, C. Tselepis.Division of Medical Sciences, University of Birmingham, UK
Background: Barrett’s metaplasia is a premalignant condition predisposing to oesophageal adenocarcinoma. A number of key molecular aberrations have been identified in the malignant progression of this disease including the induction of oncogenes such as C-myc and Cyclin D and the silencing of the adherens junctional protein E-cadherin. The repression of E-cadherin in epithelial cancers is likely to play a key role in both migration and invasion. E-cadherin can be silenced by a number of mechanisms including promoter hyper-methylation, LOH and by transcription repression involving the EMT regulators SLUG, SNAIL, and Twist. The aim of this study is to determine the expression levels of these repressors and to correlate this with E-cadherin status in the progression of Barrett’s metaplasia.
Methods: Localisation of SLUG, SNAIL, Twist, and E-cadherin was determined by immunohistochemistry. mRNA and protein expression levels were determined by real time PCR and western blotting respectively. Co-localisation of E-cadherin and EMT regulators was addressed by co-immunofluoresence.
Results: Immunolocalisation of EMT regulators demonstrated strong nuclear and cytoplasmic reactivity for SLUG and Twist in all adenocarcinomas studied (n = 30). This correlated with both real time PCR and western blotting data. Snail however, was only weakly expressed in a small portion of adenocarcinomas, and in positive adenocarcinomas less than 10% of epithelial cells were positive. Dual immunofluoresence demonstrated an inverse correlation between E-cadherin and SLUG/Twist immunoreactivity. In areas of adenocarcinoma with preserved E-cadherin immunoreactivity both Slug and Twist were absent. Conversely in E-cadherin negative cells expression of both SLUG and Twist was high.
Conclusion: Both SLUG and Twist are overexpressed n the malignant progression of Barrett’s metaplasia and this may represent a novel mechanism of E-cadherin repression in this disease.
088 BONE MARROW CONTRIBUTES TO FUNCTIONALLY ACTIVE CELLS IN TUMOUR STROMA
N. C. Direkze1,2, R. Jeffery1, K. Hodivala-Dilke1,3, F. Burke1,3, F. T. Hunt1, R. Poulsom1,3, M. R. Alison1,3, F. Balkwill1,3, N. A. Wright1,3.1Cancer Research UK; 2Imperial College London, UK; 3Bart’s and the London School of Medicine and Dentistry, UK
Background: We have previously provided evidence that the bone marrow contributes to myofibroblast populations in multiple organs including the gastrointestinal tract and tumour stroma in a mouse model of insulinoma. However, there has been a call to provide evidence that these cells are not only present but functionally active. Here we report further evidence that the bone marrow contributes to tumour stroma in intraperitoneal tumour stroma. We provide morphological evidence that these cells are functionally active and support this with evidence that these bone marrow derived cells are producing appropriate mRNA, indicating functionality.
Method: Female wild type mice were transplanted with male green fluorescent protein (GFP) positive bone marrow. Subsequently, these mice received an intraperitoneal injection of ID8 cells—an ovarian tumour cell line—to induce the formation of intraperitoneal tumours. After tumour harvest bone marrow-derived myofibroblasts were demonstrated in these tumours by combining in situ hybridisation for the Y chromosome with immunohistochemistry for α-smooth muscle actin, (αSMA). By combining the techniques of in situ hybridisation for DNA and/or RNA with immunohistochemistry for markers of bone marrow derivation (such as GFP) or myofibroblast morphology (αSMA) we have also assessed the functionality of these cells.
Results: Our findings show that the bone marrow contributes to myofibroblast populations in intraperitoneal tumours. We have also found evidence to show that these bone marrow-derived cells express mRNA for pro-collagen1α.
Conclusion: Bone marrow contributes collagen-producing cells to tumour stroma. These functionally active cells provide further evidence that the bone marrow provides part of an important axis in the process of fibrosis which may ultimately lead to the development of new methods of targeting therapy.
089 EPITHELIAL TO MESENCHYMAL TRANSFORMATION IN VITRO INDUCED BY TRANSFORMING GROWTH FACTOR BETA IN OESOPHAGEAL ADENOCARCINOMA
JonathanR. E. Rees, BenA. Onwuegbusi, RebeccaC. Fitzgerald.MRC Cancer Cell Unit, MRC/Hutchison Research Centre, Cambridge, UK
Introduction: Oesophageal adenocarcinoma (AC) presents late, and metastasises early and has less than a 20% five year survival. Epithelial to mesenchymal transition (EMT) has been identified at the invasive front of tumours and the fibroblastic phenotype induced during this process promotes invasion and metastasis. We have previously demonstrated that transforming growth factor beta (TGFβ) has a role in Barrett’s carcinogenesis, but whether this cytokine can promote EMT in AC is not known.
Aim: To determine whether TGFβ can induce EMT in AC cell lines and to assess the functional effects of this treatment.
Materials and Methods: A range of cell lines (TE7, BIC, SEG, OE19, OE33) were cultured under standard conditions in six well plates and treated for 96 hours with TGFβ over a concentration range (0–20 ng/ml). Expression of epithelial markers, E-cadherin, CK18 and mesenchymal markers, vimentin and α smooth muscle actin (αSMA) were determined by RT-PCR and confirmed by western blotting. Functional effects of treatment were assessed using wound healing, two chamber invasion, and slow aggregation assays.
Results: TGFβ led to an alteration in gene expression in TE7 cells, which were significant for TE7. TGFβ treatment had no effect on BIC cells, which we have previously shown to lack SMAD signalling. Hence, BIC was used as a negative control. In TE7 there was TGFβ dependent downregulation of E-cadherin and CK18, whereas αSMA expression was upregulated. The effects on E-cadherin were confirmed by western blotting. Functional assays for TE7, but not BIC, showed significant differences in wound healing, invasion, and aggregation between control and TGFβ treated conditions (p<0.005).
Conclusions: TGFβ can induce molecular changes of EMT in a model system of oesophageal adenocarcinoma. These changes are associated with a significant increase in invasive capacity. As these effects were not observed in SMAD-4 deficient BIC cells this suggests that the induction of EMT in this system is mediated through SMAD signalling.
090 EVOLUTION OF HELICOBACTER PYLORIVACA AND CAGA GENES WITHIN INDIVIDUALS AND FAMILIES IS COMMON AND CHANGES VIRULENCE
R. H. Argent1, R. J. Thomas1, F. Aviles-Jimenez1, D. P. Letley1, E. M. El-Omar2, J. C. Atherton1.1Wolfson Digestive Diseases Centre, and Institute of Infection, Immunity and Inflammation, University Hospital, Nottingham, UK; 2Department of Medicine, Institute of Medical Sciences, University of Aberdeen, Foresterhill, Aberdeen, UK
Background:Helicobacter pylori strains possessing a functional cag pathogenicity island (PaI) and vacuolating (m1) forms of the vacuolating cytotoxin, VacA, are associated with increased virulence. The cag PaI facilitates the translocation of CagA into the cytosol of epithelial cells where it becomes tyrosine phosphorylated within EPIYA motifs (the number of which varies between strains), and causes profound cytoskeletal and proliferative changes.
Methods:H pylori strains were isolated from 45 relatives (siblings or offspring, in 13 families) of gastric cancer patients in Scotland. vacA type and cagA status were determined by PCR amplification and nucleotide sequencing. Similarities between strains were determined by RAPD-PCR.
Results: RAPD-PCR revealed that the same H pylori strain was present in more than one family member in 9/13 families (29 relatives). 18 relatives in 10 families had unique H pylori strains. Only two subjects had demonstrated multiple infections. However, microevolution of strains to alter virulence was common within individuals and families. Five individuals had isolates of the same strain with different cagA alleles, and two with different vacA alleles. Within families with the same strain, eight members had different cagA alleles. Sequencing of cagA variable regions revealed that most differences were due to direct duplication of sequence encoding EPIYA motifs and phenotypic analysis showed that this increased CagA phosphorylation. In one family, variations in cagA were also due to additional recombination between strains, and one isolate had lost cagA. Sequencing of vacA showed that two strains had evolved such that isolates possessing s1/m1 and s1/m2 vacA coexisted. The s1/m2 forms were found to possess stop codons towards the 5′ end and not to express toxin activity.
Conclusions: We show that evolution of cagA and vacA occurs commonly within individual stomachs by recombination (vacA and cagA) and duplication of EPIYA motifs (cagA) which changes activity of these virulence factors. This demonstrates the capacity of H pylori to evolve rapidly to become more or less virulent, which may be important for host adaptation and disease pathogenesis.
Pathology free papers
091 SHEDDING OF HUMAN INTESTINAL EPITHELIAL CELLS RESULTS IN GAPS IN THE EPITHELIAL MONOLAYER
T. F. Bullen1, F. Campbell2, D. M. Pritchard1, M. J. Hershman3, A. J. M. Watson1.1Department of Medicine, Liverpool of University, Department of 2Pathology and 3Surgery, Royal Liverpool University Hospital, UK
Introduction: Epithelial cells (ECs) are known to shed from the surface of the human intestine. ECs that have become detached are known to undergo apoptosis (anoikis), however the mechanism of cell detachment is obscure. Previous studies of living mice using confocal microscopy have demonstrated the presence of gaps associated with EC shedding. These gaps are filled with a non-cellular material that maintains the EC barrier.
Hypothesis: In the human intestine ECs are shed and then undergo apoptosis, sometimes leaving a discontinuity in the remaining epithelium.
Methods: Specimens of human intestine were obtained from five patients undergoing bowel resection. 4 μm sections of human large and small intestine were collected taking special care not to disturb the epithelial layer. Sections were stained with H & E, Alcian Blue, Period Acid-Schiff, and an antibody that detects activated caspase-3.
Results: In both the small and large intestine, ECs could be seen that were in the process of being shed. Apoptotic nuclei could be identified in these shedding ECs. Discontinuities in the EC monolayer were sometimes seen beneath those being shed. The cell position from which the EC was shed was replaced by eosin staining material that does not contain a nucleus and is distinct from goblet cells (n = 44). We termed these nucleus free zones “gaps”. In the small intestine 41 gaps were present in 1072 villous sections, while in the large intestine seven gaps were present in 296 crypts. In the small intestine 24 gaps were caspase-3 negative, six epithelial cells in the monolayer were caspase positive and eight shed cells were caspase positive. In the large intestine 48 gaps were caspase negative, 11 epithelial cells in the monolayer were caspase positive and eight shed cells were caspase positive.
Conclusions: EC discontinuities occur under shedding cells. Apoptosis appears to account for cell detachment in only a minority of cases. Novel mechanisms, analogous to those we have observed in the mouse, account for cell shedding and have important implications for disease pathogenesis.
092 ASSESSING INTEROBSERVER VARIATION IN THE REPORTING OF LOCAL PERITONEAL INVOLVEMENT IN COLON CARCINOMA
S. Littleford, A. Baird, A. Cairns, P. Quirke, O. Rotimi, C. Verbeke, N. Scott.Departments of Histopathology, Leeds General Infirmary and St James’s University, Leeds, UK
Introduction and Aim: Local peritoneal involvement (LPI) has been identified as the strongest independent prognostic factor in Duke’s B colon cancer and has been suggested as a potential means of selecting patients for adjuvant therapy. However, substantial variation in the reporting of LPI has been documented between histopathology departments. A grading system for the reporting of LPI has been proposed by Shepherd et al. This study aimed to validate this grading system by determining the degree of interobserver variation in the reporting of LPI.
Methods: 138 cases of pT3 and pT4 colon carcinomas diagnosed between 2001 and 2004 were identified from a pathology database. Four specialist gastrointestinal pathologists independently assessed representative H&E slides of the closest tumour proximity to the peritoneal surface according to the Shepherd et al grading system. Kappa statistics were performed to assess the degree of interobserver variation.
Results: Interobserver variation ranged from κ = 0.45 (moderate) to κ = 0.64 (substantial) when all four categories of the grading system were analysed separately. Kappa values were improved when the categories were grouped to represent the presence or absence of LPI, with a range of κ = 0.74 (substantial) to κ = 0.89 (almost perfect).
Conclusions: Using the proposed grading system there was excellent agreement between specialist gastrointestinal pathologists in reporting LPI in pT3 and pT4 colon carcinomas. Agreement was better when comparing the presence or absence of LPI as opposed to individual categories. This grading system can be recommended to assess LPI in these patients.
093 THE TFF2/MUC6 SECRETING CELL LINEAGE IN MUCOUS TRANSFORMATION OF THE HUMAN GASTRIC MUCOSA
N. A. Wright1,2, J. R. Vanderbilt3.1Cancer Research UK; 2Barts and the London School of Medicine and Dentistry, UK; 3Vanderbilt University School of Medicine, Nashville, TN, USA
Background: In several experimental and clinical situations, attention has been drawn to the presence of mucous transformation of gastric body glands; such changes are associated with H pylori and H felis infection, and it has been proposed that such a lineage, which expresses TFF2/hSP, and also MUC6, called spasmolytic polypeptide-expressing metaplasia (SPEM), is the precursor of gastric dysplasia and carcinoma.
Methods and Results: Gastric excision specimens were studied in which glands lined with cells of mucous phenotype were present in body mucosa. 23 cases showed H pylori in the antrum, and 10 in the body mucosa. Hyperplasia of the mucous neck cells was a frequent finding, and mucous cell transformation occurred within the lower neck area of the gland, closely associated with MNC hyperplasia. The mucous cells expressed TFF2/hSP, MUC-6, lysozyme, PSTI and PDX-1. It is possible that MNCs proceed to differentiate into the cells seen in mucous transformation, but because MNCs are not seen in fully developed mucous transformation, differentiation may be directly from stem cell progeny. Both MNC hyperplasia and mucous transformation in body glands appear closely associated with the presence of H pylori induced gastritis, suggesting that they represent a mucosal defence reaction to H pylori.
Conclusions: The TTF2/MUC6 secreting lineage (TMUCSL), which includes, inter alia, mucous neck cells, basal antral gland cells, Brunner’s gland cells, PPM, SPEM, and basal UACL gland cells, is an important phenotype which occurs indigenously in the gastrointestinal mucosa and is frequently induced in conditions where damage and regeneration is occurring. The relation between mucous cell lineages, TMUCSL, and the evolution of gastric carcinoma in H pylori infection certainly warrants a great deal more attention.
094 TRANSJUGULAR LIVER BIOPSY: IS IT EFFECTIVE FOR ACCURATE HISTOLOGICAL INTERPRETATION?
E. Cholongitas, A. Quaglia1, D. Samonakis, M. Senzolo, C. K. Triantos, D. Patch, A. P. Dhillon1, G. Leandro, A. K. Burroughs.Liver Transplantation and Hepatobiliary Unit, 1Department of Pathology, Royal Free Hospital, London, UK
Background: Currently an adequate percutaneous liver biopsy (evaluating chronic hepatitis) is defined as ⩾20–25 mm long and/or containing ⩾11 complete portal tracts (CP) based on a selected series of 30 mm or longer biopsies (
) . However, even with 17G needles only 42% of biopsies have ⩾10 CP (
) . These data imply that more than one pass is necessary for adequate samples. In contrast, transjugular liver biopsy (TJLB), despite smaller diameter, allows multiple passes without increasing complications.
Aim: To document length of TJLB and number of portal tracts/biopsy and to evaluate diagnostic efficacy.
Patients and Methods: 326 consecutive TJLB in 274 patients, always using three passes (19G Tru-cut biopsy needle). For each TJLB, the number of fragments, length of each fragment and number of CP contained in each fragment were evaluated in a specific review.
Results: There were no technical failures. Histological diagnosis was possible in 322 (98.8%). The median number of fragments was 5 (range 1–13), with a median total length of 22 (range 3–46) mm with 65% being 20 mm or more. In 132 (40.5%) with severe parenchymal disturbance (cirrhosis and necrosis) the number of CP was not evaluated. In 194 (59.5%) the median number of CP was 8 (range 0–26), with ⩾6 in 146 (76%). Fifty (26%) had ⩾11 CP; these biopsies were significantly longer compared to those with <11 CP (28 mm v 20 mm, p<0.0001). All TJLB with ⩾11 CP were longer than 15 mm and 50% of those ⩾25 mm length had ⩾11 CP.
Conclusions: TJLB with three passes yields adequate biopsy samples for diagnosis and 65% were 20 mm or more in length. However, only 26% had ⩾11 CP. Four passes should increase this. TJLB is an ideal technique to obtain sufficiently longer liver biopsies particularly when multiple biopsies/patient are being evaluated, but the minimum number of passes will need to be at least four to reliably evaluate chronic hepatitis.
095 BAG-1 EXPRESSION IN HUMAN RECTAL CANCER AND THE EFFECT OF NEO-ADJUVANT RADIOTHERAPY
D. G. Glancy1, N. Clemo2, M. G. Thomas1, M. Moorghen2, A. Williams2.1Coloproctology Unit, Bristol Royal Infirmary, UK; 2University of Bristol, UK
Introduction: Bag-1 is a cell survival protein shown to protect against radiation induced cell death in vitro. Bag-1 localises to both nucleus and cytoplasm, and its expression is altered in many different tumours. The significance of Bag-1 in colorectal cancer has not been widely studied, although nuclear expression may correlate with distant metastasis.
Aim: To establish the expression of Bag-1 in human rectal cancer compared to normal mucosa, and determine whether expression is altered by neo-adjuvant radiotherapy (RT)/chemoradiotherapy (C-RT).
Methods: Twenty patients with rectal cancer were recruited. Five patients underwent RT and six C-RT prior to surgery. Pre and post-treatment biopsies were taken from the tumour, together with normal mucosa. Bag-1 was identified using immunohistochemistry and expression scored in terms of intensity (I 0–3) and proportion (p 0–4). An “H” score was calculated (I × P) for each nuclear and cytoplasmic compartment.
Results: 18/20 patients progressed to surgery (one patient from each RT/C-RT group developed metastases). 17/17 normal mucosal samples expressed Bag-1, although the staining was heterogeneous with both positive and negative cells within a colonic crypt. Bag-1 positive cells showed a significantly higher nuclear pattern of staining than cytoplasmic (p = 0.0005). Tumours showed variable Bag-1 expression, although the proportion of positive cells was increased compared with adjacent normal tissue, and there was a significant increase in cytoplasmic Bag-1 staining within the tumours (p = 0.0125). Interestingly, 4/18 tumour samples were negative for Bag-1 (H score 0–1). Bag-1 expression was unaltered in four patients following RT and could not be evaluated following C-RT due to 3/5 patients undergoing near or complete pathological response (Mandard tumour regression grade 1–2).
Conclusions: Bag-1 is expressed in normal rectal mucosa with a heterogeneous nuclear pattern of staining. Bag-1 expression in rectal cancer varies from absent to strongly positive but with higher cytoplasmic expression than normal. Bag-1 expression appeared unaltered following RT but further numbers are required to confirm this.
Service development free papers
096 ARE FINANCIAL CONSTRAINTS LIMITING THE PRESCRIPTION OF INFLIXIMAB IN CROHN’S DISEASE? A SURVEY OF THE INFLAMMATORY BOWEL DISEASE GROUP OF THE BRITISH SOCIETY OF GASTROENTEROLOGY
T. Thomas, J. F. Mayberry.Leicester General Hospital, Gwendoline Road, Leicester, LE4 5PW, UK
Background: Infliximab, a chimeric monoclonal antibody against TNF-α, has been licensed for use in the UK since 1997 for patients with Crohn’s disease. The treatment is recommended for use in a specific group of patients with the disease, as outlined in the National Institute of Clinical Excellence guidelines published in 2002. It remains unclear whether there are any factors preventing or limiting gastroenterologists from prescribing infliximab in these patients.
Aim and Methods: The aim was to identify the factors limiting the prescription of infliximab in patients with Crohn’s disease and to determine any regional variations in the frequency of its prescription. A postal survey of the members of the IBD group (excluding pathologists) was conducted.
Results: After three mailings 453/545 (83% response rate) questionnaires were returned of which 415 responses were included in the final analysis. Seventy nine per cent of consultants had a special interest in IBD. Overall, the drug was not used in the hospital in 4.5% of the cases and in 17% the drug was not available on the hospital formulary. One or more limiting factors for prescribing infliximab was identified in 26% of cases. Limited financial resources accounted for 63% of all limiting factors. There were no significant variations among various regions with respect to the presence of limiting factors compared to the national average. Overall there was no significant difference in prescribing infliximab in the last year when groups with and without limiting factors were compared. (Yates corrected χ2, p = 0.27). However there was a statistically significant difference in the number of times infliximab was prescribed in the last year when limiting factors for prescription were present across the regions (for prescribing 1–3 times for the same patient in the last year, paired t test, 95% confidence intervals, −8.8 to −4.1, p = 0.001). Infliximab was prescribed less frequently when limiting factors were present.
Conclusion: There are one or more limiting factors for prescribing infliximab in patients with Crohn’s disease in all regions in the UK but there are no significant variations between regions. Financial constraint appears to be the predominant limiting factor. The presence of limiting factors has a significant influence on the frequency of prescription of the drug. This may have an impact with respect to the treatment of patients with severe, refractory Crohn’s disease in the UK.
097 MANAGING THE QUEUE FOR IN-HOSPITAL ENDOSCOPY: MUST INPATIENTS BE PATIENT?
S. Hebbar, L. James, P. Clarke, S. Barker, M. C. Allison.Calcraft Suite, Royal Gwent Hospital, Newport NP20 2UB, UK
Introduction: At the last BSG two UK teaching hospitals presented a retrospective audit of their in-hospital endoscopy workload during the month of August 2002. We undertook a prospective survey of inpatient endoscopy in a large district hospital serving 335 000 population during September and October 2004. The aims were to examine (1) the time devoted to inpatients and outpatients in relation to the numbers investigated during 2 months; (2) appropriateness of inpatient OGD requests in relation to recent NICE guidance; (3) impact of vetting and cancelling inappropriate referrals; (4) delays between referral and procedure.
Methods: A proforma was made for each inpatient endoscopy referral form received, and the progress of each referral was tracked. Potentially inappropriate referrals were visited by a GI physician or specialist nurse.
Results: Inpatient referrals totalled a median of 37 per week (range 31–47). 377 inpatients were referred for 385 procedures (208 diagnostic and 30 therapeutic OGD, 70 flexible sigmoidoscopies, 30 colonoscopies, and 47 ERCPs). 43 requests for OGD did not fulfil NICE guidance. Four of these were appropriate (screening for varices, staging cancer), leaving 39 (19%) potentially inappropriate requests. 23 patients were cancelled due to inappropriate referral and/or comorbidity. 31 requests for OGD were rebooked as outpatient. 28 requests for lower GI endoscopy and four for ERCP were either cancelled or booked as outpatient. Despite these measures only 48% of inpatients could be accommodated within 24 hours of referral, 11% had to wait over one week, and a Saturday inpatient initiative list had to be done. During the study period 688 outpatients spent 191 hours in the procedure rooms, while 279 inpatients took 96 hours. Thus during 2 months, 29% of patients were inpatients, and they took 33% of total endoscopy session time.
Conclusions: Despite implementing vetting and an initiative list, over 1000 bed days were taken by inpatients awaiting endoscopy over the two study months. Matching capacity and demand is difficult given the weekly fluctuations in referrals. At least one third of procedure room time should be allocated to inpatient work. Segmentation of inpatient lists would increase endoscopy room downtime but would free up hospital beds.
098 DOES INFORMED CONSENT FOR ENDOSCOPIC PROCEDURES LEAD TO AN INFORMED DECISION?
R. Sidhu, V. Sakellariou, M. Karajeh, P. Layte, A. Soliman.Barnsley District General Hospital, UK
Background and Aim: The process of informed consent is an important part of any medical procedure. This study aimed to assess the impact of postal information on the understanding of consenting for upper and lower GI endoscopy, and on the decision process for accepting the procedure. Patient information packets included a consent form explaining the specific risks, the DOH leaflet “about consent” and leaflets about the procedure.
Methods: An anonymous patients view questionnaire was posted to 1800 patients that had attended and to 314 patients that did not attend (DNA) for GI endoscopy at our Endoscopy Unit. Consent was obtained in the usual way by the endoscopist performing the procedure after ensuring patients had received their postal packs.
Results: 906 of the questionnaires (43%) were returned (DNAs = 60). 6.5% of patients admitted to not having read the information provided on consent and procedure (24 = uppers, 35 = lowers). Most responders felt the information supplied was appropriate. Only 5% felt the information was too much, difficult to understand or too little. The information provided had no impact on decision making for 42% patient, while 2.6% of patients were put off having the test. 44% (n = 396) felt it helped them make an informed decision. The section of risks was only read by 82%. A larger proportion of patients felt reassured for gastroscopy as compared to colonoscopy (n = 146 v 23) however the majority preferred to know the risks (75.6%). 8% of patients were not bothered if the risk was rare—less than 1 in 1000, 8.8% were interested in the complication rate of the endoscopist performing their procedure, while 35% preferred to know the risks in general terms (no numbers).
From the DNA group, a larger number DNA’d gastroscopy compared with colonoscopy. 8.5% that DNA’d were influenced by the information provided.10% felt this was due to being worried about the procedure. The number of DNAs was not large enough to get a statistically significant result about age group and reasons of cancellation.
Conclusion: Although patients prefer to know the risks of GI endoscopy, in our study it failed to help informed consent for nearly half of them while it deterred a small group of patients.
099 A NURSE LED PARACENTESIS SERVICE IS SAFE AND EFFICIENT
P. Rawcliffe, C. Skilbeck, S. M. Kelly.Department of Gastroenterology, York Hospital, York, UK
Background and Aims: Paracentesis is an important part of the management of refractory ascites. With increasing pressures on junior doctors’ time we found patients were waiting unacceptably long periods for their drains to be inserted. Outpatients also faced additional delays for admission related to pressure on beds. We therefore set up a nurse led paracentesis service to try and address this problem.
Methods: Two senior ward nurses were taught the relevant anatomy and pathophysiology including interpretation of blood and ascitic fluid results. Nurses then received practical training in drain insertion. Once competent, nurses performed solo paracentesis on selected patients according to a defined protocol. This included the facility for known outpatients to self-refer for paracentesis.
Results: Over the initial 10 month period of the service nurses performed 100 episodes of paracentesis on 23 patients. There was only one, minor, complication related to bleeding from a superficial vessel, which settled.
There was a substantial improvement in waiting times for both in and outpatients. Outpatients now self-refer and paracentesis is largely done as a daycase procedure in this group. Drain insertion is now much more efficient and access times have improved. Most day cases have a drain inserted within 2 hours of admission facilitating same day discharge. Waiting times for inpatients have also improved dramatically with patients no longer waiting up to 48 hours for a drain as they have done in the past.
Patients have expressed a preference for the service and in particular the improved access times. Patients also perceive that the nurses have more time for the procedure and take more care.
Conclusion: Nurse led paracentesis is safe. It has reduced patient waiting times, is a more efficient use of beds and also frees up junior doctors time. In the future the standardised training package also enables the nurses to train junior doctors in the procedure.
100 MATCHING CAPACITY AND DEMAND FOR ENDOSCOPY: A SIMPLE MATHEMATICAL MODEL
M. C. Allison.Endoscopy Lead, National Leadership and Innovation Agency for Healthcare, Innovation House, Llanharran, Cardiff, UK
Background: The Modernisation Agency’s endoscopy programme has highlighted wide variations in waiting times for colonoscopy, and in numbers of colonoscopies that hospitals perform per 100 000 population (100 k) served. Guidance is available from the BSG on the numbers of each endoscopic procedure needed per year in an “average” district hospital serving 250 000. In “Consultant Physicians Working with Patients” the Royal College of Physicians has also advised on maximum numbers of procedures to be accommodated in an endoscopy session.
Methods: Based on the above guidance, it was calculated that 686 half day endoscopy sessions are needed per year to meet predicted demand for gastroscopy, colonoscopy, flexible sigmoidoscopy, and ERCP for a hospital serving 250 000. Given that an endoscopist doing one session per week will only fulfil 40 sessions per year (due to leave and post-take duties etc), it follows that 17.2 fixed endoscopy sessions per week are needed to meet demand expected from 250 000. Endoscopy units in 18 acute hospitals in Wales (population 2.9 million) were surveyed in 2002, and for each unit the variance between predicted session requirement (from the above model) and actual sessions taking place was calculated. A positive variance suggests that sessions are not being fully utilised. Negative variance suggests too many patients per list and/or insufficient endoscopy provision to meet the needs of the population served.
Results: In Wales as a whole, 194 sessions were taking place per week, a variance of minus 14.8 sessions (that is, an under-capacity of 14.8 sessions per week). Variance for each hospital ranged from −7.8 to +5.1 sessions (median +0.6). Nine hospitals had an under-provision and the other nine had a positive variance.
Conclusions: By this model the predicted sessional requirement proved to be very close to actual capacity in acute hospitals in Wales. Therefore the proposed model has criterion validity, and may facilitate comparison of endoscopy capacity and session utilisation between units. Those with negative variance may find this model helpful in supporting bids for increased capacity.
101 ROLE OF LIVER NURSE SPECIALIST: IMPACT OF AUDIT ON CHANGE IN PRACTICE OF LIVER BIOPSY AT A DISTRICT GENERAL HOSPITAL
A. Saleem, S. Needs, I. Petransky, D. K. George.Torbay District General Hospital, Gastroenterology Department, Torquay TQ2 7AA, UK
Introduction: Two previous audits (February 1999 to February 2000, 94 patients and November 2000 to April 2001, 51 patients) undertaken at the same hospital revealed that BSG liver biopsy guidelines were not adhered to with regard to the timing of imaging and blood tests (INR, platelet count) and number of passes. This resulted in a change in practice with the liver biopsy service coordinated by a specialist nurse.
Aims: To assess impact of this change in practice on adherence to BSG guidelines at Torbay Hospital and to assess patient morbidity and mortality.
Method: Audit proformas collected prospectively and case notes examined retrospectively of 89 patients from January 2003 to December 2003 particularly looking at: timely imaging and blood tests (INR, platelet count), method of biopsy, morbidity, and mortality.
Results: The majority, 91% were performed as a day case procedure. The commonest indication for liver biopsy was chronic hepatitis C infection (40% as compared with 12% and 17% in previous two audits).
99% had ultrasound performed on the same day as biopsy, 94% had INR and platelet count checked within one week of the procedure. 94% had documented informed consent. Two patients had more than one pass, both performed by a consultant. The commonest complication was minor pain (requiring oral analgesia), though this complication was significantly reduced compared to the previous audits (19/89 v 75/145) χ2 = 13.37, p = 0.001. No patient had a serious complication (one patient in the first audit had a pneumothorax) and there were no deaths.
Conclusion: A change in practice has resulted in better adherence to BSG guidelines hence completing the audit cycle. More importantly a significant improvement in morbidity has been achieved.
102 THE 2005 CANCER WAITING TIMES TARGET: WILL WE EVER HIT THE TARGET FOR OESOPHAGOGASTRIC CANCER?
G. Moran, H. Iyer, A. Bailey, J. R. Butterworth (introduced by J M Bateman).Shrewsbury and Telford Hospital NHS Trust, Shrewsbury, SY3 8XQ, UK
Introduction: The Government’s NHS Cancer Plan (2000) sets out strict cancer waiting times targets including a maximum one month (31 days) wait from cancer diagnosis to first treatment by December 2005.
Methods: All oesophagogastric cancers (OGCs) treated with curative intent (that is, neo-adjuvant chemotherapy plus surgery or surgery alone) between January 2002 and October 2004 were retrospectively examined with particular emphasis on the time from diagnosis to first treatment. Date of diagnosis may be considered an arbitrary point—is it the time of the index endoscopy or is it made at the first MDT meeting, when all relevant clinical information is discussed? We assessed time to first treatment from both standpoints.
Results: Between January 2002 and October 2004 a total of 89 OGCs were treated with curative intent (64 male, 25 female); 37 in 2002, 31 in 2003, and 21 in 2004 to October. Of these 64 were oesophageal (56 adenocarcinoma, 8 squamous cell) and 25 gastric carcinomas. Forty seven (52.8%) received neoadjuvant chemotherapy. The mean age was 64.74 years (range 43–83 years). The mean time (days) from endoscopy to treatment in 2002, 2003, and 2004 was 52 (range 18–99), 51.5 (range 16–162) and 67.8 (range 10–184) respectively (p = NS). The mean time (days) from the first MDT meeting to treatment for the years 2002, 2003, and 2004 was 36.8 (range 3–75), 33.1 (range 1–97), and 48.8 (range 9–148); (p<0.05 for 2003 v 2004). Of all the OGCs, only 11/37 (29.7%) during 2002, 14/31 (45.2%) during 2003, and 8/21 (38.1%) during 2004 were treated within one month of the first MDT meeting. Twenty (80%) of the gastric carcinomas remain alive at a median follow up of 12 months (range 1–31), and 41 (64%) of the oesophageal carcinomas are alive at a median of 14.5 months (range 1–34 months).
Conclusions: Less than 40% of our patients with OGCs treated with curative intent are currently meeting the government’s cancer waiting time targets for December 2005 when the first MDT meeting is considered the point of diagnosis. Coordinated and innovative strategies are required to achieve these ambitious targets.
103 A DYSPHAGIA HOTLINE CLINIC: OPTIMISING THE SERVICE
I. A. Murray1, E. Despott1, A. Sanyal1, G. Maskell2, R. Farrow2, C. Bloor2, S. H. Hussaini1, H. R. Dalton1.Departments of 1Gastroenterology and 2Radiology, Royal Cornwall Hospital, Truro, UK
Introduction: Dysphagia is a common reason for referral under the two week pathway for upper GI cancer. In 2003, we introduced a one-stop dysphagia clinic to deal with these referrals. 67% of referrals referred did not have dysphagia, but reflux, odynophagia, or globus. The incidence of significant disease in this cohort is very small. We redesigned our service to reduce inappropriate referrals and fast track patients through appropriate investigations.
Methods: A simple specific fax questionnaire was designed asking the following question: “Does food or drink stick on swallowing?” Referred patients had a 5 minute consultation with a specialist registrar or consultant using a symptom-specific proforma, then underwent either barium swallow or gastroscopy, or both on the same day.
Results: 137 patients were referred over an 8 month period. Of these, 108 had true dysphagia (81.8%) a significant increase from previous referral pattern (p<0.001: χ2). Six had globus (4%), one throat pain (1%), and the remainder were appropriate for referral under the two week pathway, although not primarily with dysphagia, for example, dyspepsia with vomiting, anorexia, or weight loss. Five patients declined to attend. By minor changes within the endoscopy and radiology departments, it was possible to see and investigate all patients within two weeks of referral. 52 patients underwent barium swallow, 84 patients gastroscopy, and six patients both. 11 patients had oesophageal carcinoma, one carcinoma of gastro-oesophageal junction, one had gastric carcinoma, and one gastric lymphoma (that is, malignancy in 10.6%). A further 12 had benign oesophageal strictures, four pharyngeal pouches, 38 dysmotility, 43 reflux disease without stricturing, four minor inflammation (gastritis/duodenitis), three Schatzki rings, six had globus, and one each of pyloric stenosis, gastric volvulus, cricopharyngeal web, oesophageal ulceration, oesophageal diverticulum, extrinsic compression, duodenal ulcer and achalasia. Some patients had more than one pathology.
Discussion: By introducing a three question referral proforma, we increased the appropriateness for referral for the dysphagia clinic from 32.6% to 81.8%. There was a slight, non-significant increase in the number of upper GI malignancies detected (from 8.7% to 10.6%) although oesophageal dysmotility and reflux disease remained the most common final diagnoses.
Radiology symposium
104 A PROTOCOL FOR COLONIC IMAGING IN ELDERLY PATIENTS
R. Taneja, J. Green, H. Adams, G. L. Swift.Llandough Hospital, Cardiff, CF64 2XX, UK
Background: The options available for imaging the colon have expanded from barium enema (BE) and colonoscopy to include CT pneumocolon and minimal preparation CT (MPCT). Although BE and colonoscopy are well established, they are limited in elderly patients by being invasive, requiring patients to be mobile and require bowel prep. CT pneumocolon requires bowel prep but is non-invasive, is well tolerated, and allows examination of extracolonic structures.
Methods: We established a protocol for colonic imaging requests where patients under 40 years were directed to colonoscopy, those over 40 who were fit and mobile underwent barium enema, and those with poor mobility or frail underwent CT pneumocolon or MPCT.
Results: Our experience of the first 96 patients having CT was reviewed. These were performed between May 2002 and February 2004. Indications included one or more of: anaemia (42), change in bowel habit (34), unexplained weight loss (23), lower GI bleed (11), abdominal pain (9), and anorexia (2).
CT findings were normal in 19, showed diverticular disease in 33, colonic strictures in two, significant polyps in two, colonic carcinoma in one. In 40 cases there were extracolonic findings which were considered significant in 13. These included a hypernephroma, appendiceal adenocarcinoma, adrenal secondary, liver metastases, lymphadenopathy in three, intra abdominal collection in two, and aortic aneurysm in four. In two patients CT was inadequate due to poor bowel preparation in one and under distention in the other.
Conclusions: CT provided adequate information in 94 of 96 patients. Significant colonic pathology was found in 38 and extracolonic pathology in 13. The procedure was well tolerated and is a useful alternative to barium enema or colonoscopy in frail, elderly patients.
105 EVALUATION OF “PREPLESS” CT VIRTUAL COLONOSCOPY FOR DETECTION OF COLORECTAL NEOPLASIA IN ELDERLY PATIENTS: A FEASIBILITY STUDY IN A DISTRICT GENERAL HOSPITAL
M. A. Karajeh, V. Sakellariou, K. Kapur, A. Soliman, S. Riley, P. McAndrew.Barnsley DGH, Gawber Road, Barnsley S75 2EP, UK
Background: “Prepless” CT virtual colonoscopy (CTVC) has been shown to be feasible using oral barium for faecal tagging and electronic cleansing with encouraging initial reports. Elimination of bowel preparation would be a major advantage, especially in the elderly.
Aims: To assess the sensitivity and specificity of “prepless” CTVC for detection of colorectal cancer and polyps ⩾1 cm in patients over age 60 years with iron deficiency anaemia.
Methods: A prospective, evaluator blinded, study of 20 patients with iron deficiency anaemia (mean age 71 years, 50% male, mean haemoglobin 9.3 g/dl) comparing “prepless” CTVC to optical colonoscopy. Patients were given four doses of oral barium during the preceding 48 hours, but no bowel cleansing agents. CTVC was performed with a PHILIPS 4 detector row MX-8000 scanner, with slice collimation of 2 mm, using prone and supine acquisitions. Images were analysed on a dedicated workstation (EZEM Innerview) using 2D images cross referenced to the 3D fly through. Electronic cleansing (digital subtraction of tagged stool) was performed using commercially available software. All patients underwent optical colonoscopy within 3 weeks of CTVC.
Results: There were four cancers and three polyps ⩾1 cm identified at optical colonoscopy (caecal intubation rate 95%) in seven patients. “Prepless” CTVC with electronic cleansing correctly identified all four cancers and two of the three polyps giving overall sensitivity of 86%. There was one false positive finding (“possible cancer”) on virtual colonoscopy giving overall specificity 92%.
Conclusion: “Prepless” CT virtual colonoscopy is feasible with good sensitivity and specificity for colorectal cancer and significant polyp lesions.
Neoplasia free papers
106 ZD6474 SIGNIFICANTLY REDUCES POLYP BURDEN IN A MOUSE MODEL OF INTESTINAL CANCER
R. A. Goodlad1, A. J. Watkins1, R. Poulsom1, A. Ryan2, S. R. Wedge2, I. T. Pyrah2, N. Mandir1, R. W. Wilkinson2.1Cancer Research UK, Histopathology Unit, 44 Lincoln’s Inn Fields, London WC2A 3PX, UK; 2Departments of Cancer and Infection Research and Safety Assessment, AstraZeneca Pharmaceuticals, Alderley Park, Macclesfield, Cheshire SK10 4TG, UK
Introduction: ZD6474, an orally active inhibitor of vascular endothelial growth factor receptor-2 (VEGFR-2) and epidermal growth factor receptor (EGFR) tyrosine kinase activity, was used to study the effect of blocking angiogenesis and EGFR signalling in multiple intestinal neoplasia (ApcMin/+) mice. These mice develop numerous benign polyps due to a mutation of the adenomatous polyposis coli (APC) gene, as in familial adenomatous polyposis (FAP) in humans.
Methods: In the first study, ZD6474 (12.5, 25, or 50 mg/kg/day) or vehicle was administered daily by oral gavage to 6 week old C57BL/6J-ApcMin/+ mice (n = 12/group) for 28 days. In the second study, 10 week old ApcMin/+ mice (n = 12/group) were given ZD6474 50 mg/kg/day or vehicle daily for 28 days. Following treatment, the number and size of polyps in the small and large intestines were scored. Immunohistochemical analysis was performed to detect vasculature staining (factor 8) and β-catenin intracellular localisation, and VEGFR-2 mRNA was detected by in situ hybridisation.
Results: In the first study, all doses of ZD6474 reduced polyp number in the small bowel and colon (46% and 76%, respectively, with 50 mg/kg/day; p<0.05). Polyp diameter was also reduced significantly in the small bowel, thus decreasing mean burden by 75%. In the second study, both small bowel polyp number and diameter were reduced, thus decreasing polyp burden by 72% (p<0.01). ZD6474 (50 mg/kg/day) halved the proportion of cells showing nuclear localisation of β-catenin staining (p<0.005), and reduced the number of cells expressing VEGFR-2 from 7.4 (SD 1.3) to 2.8 (SD 0.6) per villus (p<0.001). ZD6474 significantly reduced the number and size of polyps to a similar extent in the two studies.
Conclusion: These results suggest that VEGFR-2/EGFR signalling plays a key role in the development of intestinal adenomas, and that inhibiting this activity can markedly reduce polyp burden at both early and late stages.
107 TUMOR M2-PK: COMPARATIVE STUDY OF THE VALUE OF TUMOUR MARKERS IN THE DIAGNOSIS OF COLORECTAL LIVER METASTASIS
I. Rubio Pinedo, R. Faroq, B. R. Davidson.Royal Free Hospital NHS Trust, Pond Street, London, NW3 2QG, UK
Introduction: Colorectal metastases in liver are found at some stage of their disease in around 56% of patients with colorectal cancer. This study was designed to evaluate a new tumour marker, Tumor M2-PK, in discriminating colorectal liver metastatic patients from healthy controls, and compared it against the conventional tumour markers CEA and CA 19.9.
Patients and Methods: This study includes 28 patients that were worked up for resection of colorectal metastatic liver diseases. All patients had presurgical CEA, CA 19.9, and Tumor M2-PK levels measured. The mean age of these 19 men and nine women was 57 years (range 48–65). Comparisons were made with an historical healthy control group (n = 68; 16 male+52 female, 16–78 years, mean age 38.4).
Results: See table.
Abstract 107
Conclusion: This study has confirmed Tumor M2-PK to be significantly more sensitivity in the diagnosis of colorectal liver metastasis than the other tumour markers, CEA, and CA 19.9.
This study provided some unexpected data. Five of the 28 patients produced levels of Tumor M2-PK below the cut-off point. One of these patients presented three different lesions measuring a total of 420 ml and another had a single tumour that measured 881.2 ml, which raises the possibility of a correlation between Tumor M2-PK and tumour metabolism rather than tumour volume.
108 GASTRIN INDUCES PLEIOMORPHIC CHANGES ASSOCIATED WITH BARRETT’S METAPLASIA: “A WOLF IN SHEEP’S CLOTHING”?
P. A. Atherfold, J. A. Obszynska, (introducedbyJ. A. Jankowski).Digestive Diseases Centre, Leicester Royal Infirmary Leicester, UK
Background: It has been hypothesised that Barrett’s adenocarcinoma derives from a clonally expanded population of cells present within the oesophageal compartment. The contributory role of gastrin as a consequence of proton pump inhibitor therapy, to the clonal selection of malignant epithelium and thus the development of Barrett’s adenocarcinoma remains unclear.
Methods: We examined the presence and functional consequences of gastrin and CCKB receptor in Barrett’s tissue and cell lines. This included biopsy tissue from the body or fundus, and Barrett’s and squamous epithelium. The cells used included OE21, a moderately differentiated oesophageal squamous carcinoma cell line; OE33, a well differentiated oesophageal columnar carcinoma cell line, and OE33GR derived from the OE33, stably transfected with wild type gastrin/CCKB receptor (>10000-fold more CCKB receptor).
Results: Real time and RT-PCR analysis verified the presence of mRNA to the CCKB receptor and gastrin in all tissues, with most expressed in the body/fundus followed by Barrett’s and squamous epithelium. The OE33GR cell line expressed the most CCKB receptor. However, the OE21 expressed more gastrin mRNA, than in OE33GR or OE33.
Using flow cytometry, gastrin had a minor effect on cellular proliferation, significantly reducing G0/G1 phase arrested cells, induced following serum deprivation (p<0.05, Mann-Whitney). This effect was diminished using the CCKB receptor antagonist JB93182. The response was independent of ERK1/2, NF-κB, and β-catenin activity. Gastrin had no significant effect on induction of apoptosis in any of the cell lines. Gastrin significantly increased cellular migration in OE33GR cells (p<0.01) but had no effect in OE33, indicating a requirement for CCKB receptor.
Conclusion: Gastrin plays only a minor role in proliferation. It has however, a major novel role in cellular migration. This has important implications with regards to clonal evolution of Barrett’s and in response to damage and restitution early in the reflux disease.
109 TNFα ACCELERATES CLONAL SELECTION OF BARRETT’S EPITHELIUM
P. A. Atherfold, A. Cerbinskaite, J. A. Obszynska, (introduced byJ. A. Jankowski).Digestive Diseases Centre, Leicester Royal Infirmary, Leicester, UK
Background: Barrett’s oesophagus is associated with an inflammatory response. It is also hypothesised that Barrett’s adenocarcinoma develops as a consequence of the evolution of a clonal population of cells within the oesophagus. These clones may be selected over their neighbouring normal epithelial cells, by various environmental factors that influence cell survival.
Aims: The aim of this study was to characterise the in vitro model of mucosal inflammation to determine the influence of TNFα on cellular proliferation, apoptosis, cadherin biology, and colony formation, in a panel of oesophageal cancer cell lines. Previous work from the group has shown that the OE21 corresponds to a moderately differentiated oesophageal squamous carcinoma, OE33 to a well differentiated oesophageal adenocarcinoma, and SEG-1 to a poorly differentiated oesophageal adenocarcinoma and thus alluding to an in vitro model of squamous to metaplasia to adenocarcinoma sequence.
Methods and Results: Using western blotting, SEG-1 cells were found to express (fivefold) more TNF-receptor 1 compared with OE33 and OE21.
In SEG-1, TNFα was shown to inhibit cellular proliferation by inducing a G0/G1 cell cycle arrest, which was evident at 24 hours (p<0.05, Mann-Whitney). Treatment with TNFα also caused a significant increase in the number of apoptotic cells at 24 and 48 hours, in each of the cell lines examined (p<0.05, Mann-Whitney).
Utilising agarose colony forming assays, identified SEG-1 as the most tumourgenic cell line, followed by OE33 and OE21. This was associated with poor cell-cell cadherin dependent adhesion, relying on cell-extracellular matrix adhesion instead. Following TNFα treatment, there was no significant change in tumourgenicity in OE21 or OE33, but an increase was noted in SEG-1 (p<0.05, Mann-Whitney).
Conclusion: These data provide evidence that TNFα may be involved in tumour invasiveness and alter proliferation and apoptosis, indicating a potential role for augmenting differential clonal selection between squamous cells and metaplastic columnar cells.
110 IN SITU GENERATION OF N-NITROSO COMPOUND FROM DIETARY NITRATE VIA NITRIC OXIDE IN THE HUMAN PROXIMAL STOMACH
J. Winter, S. Paterson, G. Scobie, A. Wirz, T. Preston1, K. E. L. McColl.University Department of Medicine and Therapeutics, Western Infirmary, Glasgow and 1Scottish Universities Environmental Research Centre, East Kilbride, UK
Background: The mutagen responsible for the rising incidence of adenocarcinoma at the gastric cardia and distal oesophagus is unknown. We have previously shown that high luminal levels of nitric oxide are generated from dietary nitrate at the sites of cancer occurrence. Also, using a bench top model of the gastro-oesophageal junction we have demonstrated that nitric oxide diffuses into the adjacent epithelium and within it generates N-nitroso compounds, known powerful carcinogens.
Aim: To ascertain if the luminal nitric oxide derived from dietary nitrate is exerting localised nitrosative stress and generating N-nitroso compounds within the adjacent epithelial compartment in humans.
Methods: A silastic tube containing the secondary amine morpholine was divided longitudinally into 1.5 cm segments and attached to a pH catheter. It was then passed nasogastrically. The tube wall has the permeability properties of an epithelial lipid membrane. Subjects were studied on two separate days, drinking water containing 2 mmols of nitrate on one day and on the other day water only. Blood and saliva samples were collected regularly and analysed for nitrate and nitrite. The tube was removed after 2.5 hours and each segment was drained and nitrite and N-nitrosomorpholine concentrations measured.
Results: Ten healthy volunteers have been studied. Nitrite and N-nitrosomorpholine were generated in situ within the segments exposed to acid pH, with peak concentrations in the second or third segment below the pH step up point. Concentrations of nitrite and N-nitrosomorpholine increase by three- to fivefold following nitrate ingestion.
Conclusion: Ingestion of dietary nitrate leads to in situ N-nitroso compound formation in humans with normal gastric acid secretion, concentrations being maximal in the proximal stomach. This is the first study to demonstrate in situ generation of N-nitroso compounds from endogenously generated nitric oxide derived from dietary nitrate.
111 THE POTENTIAL OF 5-LIPOXYGENASE PRODUCTS IN THE PREVENTION OF COLON CANCER: NSAIDS, LTB4, AND PPARα
A. Shonde, A. J. Bennett, C. J. Hawkey.University of Nottingham Division of Gastroenterology, University Hospital Nottingham, Nottingham NG7 2UH, UK
Background: NSAIDs reduce the risk of colon cancer. More recently peroxisome proliferator activated receptors (PPARs) have been associated with the pathogenesis of colon cancer. We have previously shown a potential role for PPARα in preventing colon cancer.1 A role for Leucotriene B4 is also suggested because LTB4 is a ligand for PPARα. The effect of NSAIDs on colon cancer may be due to substrate diversion from the cyclooxygenase pathway to the lipoxygenase pathway, thus producing excess LTB4.
Aims: (1) To establish if NSAIDs enhance LTB4 synthesis in organ culture of colonic tissue. (2) To assess if LTB4 activates PPARα in HCA7 (colon cancer cell line).
Method: Samples of normal colon and colon cancer were placed in organ culture±indomethacin 10−6 and 10−5M. HCA7 cells were transfected with PPARα expression vector and the peroxisome proliferator response element (PPRE-tk-luc) which drives luciferase gene expression via a three tandem repeat of PPRE. LTB4 10 μM was added 5 hours after transfection. The cells were analysed 48 hours after transfection for luciferase.
Results: Indomethacin caused a concentration dependant enhancement of LTB4 synthesis in organ culture. The mean LTB4 level was 14.6 (SD 3.5) pg/mg in normal colonic tissue compared to 295.6 (SD 110.5) pg/mg in colon cancer. The addition of indomethacin 10−6 and 10−5M resulted in mean LTB4 levels of 50.6 (SD 7.6) and 97.5 (SD 7.5) pg/mg in normal colonic tissue and 323.3 (SD 123.8) and 526.3 (SD 162.3) pg/mg in colon cancer. LTB4 10 μM activated PPRE-tk-luc in cells cotransfected with PPARα. We found a threefold increase in luciferase activity in HCA7 cells transfected with PPARα and PPRE-tk-luc compared with controls.
Conclusion: NSAIDs enhance LTB4 synthesis in colonic tissue. LTB4 activates PPARα in HCA7 cell line. This suggests a potential mechanism by which NSAIDs are chemoprotective in colon cancer.
1
Case presentations
112 AN UNUSUAL CAUSE OF ASCITES IN A PATIENT WITH ALCOHOL LIVER DISEASE
J. Gasem1, F. Mohammed2, B. Rameh1.1Royal Oldham Hospital, 2Wythenshawe Hospital, Manchester, UK
Case report: A 57 year old male who had worked as a thermal insulator engineer, initially presented with abnormal liver function tests and a history of heavy alcohol use. Abdominal U/S showed fatty infiltration of the liver. Blood investigations for causes of chronic liver disease were all negative. He was advised about his alcohol intake but failed to attend follow up appointments. Seven years later he developed ascites, which was exudative. Investigations including CXR, endoscopy, colonoscopy, U/S, and CT abdomen were normal. His ascites was successfully managed with diuretic therapy. Seven months later he was readmitted with abdominal pain and recurrence of ascites. Repeat CT showed dense soft tissue material, just deep to the anterior abdominal wall and primarily related to the peritoneum and mesentery. Occupational history confirmed asbestos exposure. Histology of biopsied omentum at laparotomy showed malignant peritoneal mesothelioma (MPM). The patient demised 5 days after laparotomy.
Discussion: Mesotheliomas are rare mesenchymal tumours derived from the mesothelium of serosal cavities. Solitary peritoneal involvement is encountered in only 10–20% of reported cases, and the annual incidence is less than 1–2 cases per million. An association between asbestos exposure and MPM is recognised and there may be a long delay between exposure and manifestation of disease.
Clinical presentation is non-specific with abdominal pain and distension. The initial diagnosis can be very difficult and laparoscopy may be needed in suspected cases. Prognosis is unfavourable, median survival is only 12–14 months. There is currently no universally accepted treatment. Modalities tried have included surgical resection, irradiation and systemic or intraperitoneal chemotherapy.
This case illustrates the difficulty in early diagnosis of MPM. Persistence in obtaining a diagnosis is essential when one suspects MPM. Increased awareness and appropriate investigations may lead to earlier diagnosis and improve the continued dismal prognosis.
113 WHEN IS CROHN’S NOT CROHN’S?
N. F. S. Watson1, C. Parsons1, A. Jawhari2, C. Maxwell-Armstrong1.Departments of 1General Surgery and 2Gastroenterology, Queens Medical Centre, Nottingham, UK
Case report: In this case report we discuss a 32 year old male who presented to our general surgery outpatient clinic with perianal sepsis. On direct questioning he admitted to a one year history of loose motions, bright red PR bleeding, and intermittent periumbilical pain. Abdominal examination was unremarkable; however PR examination revealed an excoriated moist anus and two distinct external discharging fistulae. Following further investigations the patient was diagnosed and treated for Crohn’s disease.
A short time after his initial presentation, and following review by a consultant gastroenterologist, the patient attended accident and emergency with an episode of acute respiratory distress. As the case evolved further an unusual alternative to the diagnosis of Crohn’s disease was revealed.
We discuss the diagnostic difficulty caused by the overlap in gastrointestinal symptoms between these two conditions, and would welcome dialogue with any clinician who has experience of such cases.
114 AN UNUSUAL FATAL CASE OF “IRRITABLE BOWEL SYNDROME”
J. Gasem, E. Roche.Macclesfield District Hospital, UK
Case report: A 61 year old British White female was referred to clinic with a 6 week history of post-prandial central abdominal pain and weight loss of one stone. Her spouse was from Iraq. She had a past medical history of irritable bowel syndrome (IBS), diagnosed 15 years ago, stable COPD, and a previous pneumothorax. On examination, she was thin with a BMI of 18.5, but no other abnormalities were detected. Initial investigations to exclude malignancy included chest x ray, CT thorax, abdomen and pelvis, and gastroscopy were unremarkable. Her blood results showed Hb 11.1 g/l, platelets 675×109, ESR 22 ml/hr, CRP 14 mg/l, and albumin 22 g/l. On review 3 months later, a repeat CT scan to exclude mesenteric thrombosis or ischaemia showed focal thickening of a segment of small bowel. This was followed by a small bowel meal which showed an irregular 7 cm stricture in the small bowel. Subsequently, at an emergency laparotomy for abdominal pain, she was found to have large multiple constricting lesions of the small bowel, infiltrating the sigmoid colon with mesenteric lymphadenopathy. Histology showed giant cells and granulomata with areas of caseous necrosis. No organisms were found on ZN stain, but tissue PCR proved positive for TB. The patient had a prolonged stay on ITU, involving intensive oral and IV anti-TB treatment. Despite this, she continued to have multiple complications and died 2 months later.
Discussion: Abdominal TB is very rare with an estimated incidence of 0.43 per 100 000 in one British city. It has an insidious onset and symptoms and signs may vary with the site of involvement and type of lesion. A high index of suspicion is therefore needed, especially in groups not traditionally thought to be at risk. Abdominal TB can affect the gastrointestinal tract (GI), the peritoneum, lymph nodes of the small bowel mesentery, or the solid viscera. The GI tract is involved in 66–75% of patients. The most common site is the ileocaecal region. In this case, it involved a long segment of jejunum, infiltrating the sigmoid colon and mesenteric lymph nodes, behaving like a malignant tumour. This case was also unusual in its lack of an inflammatory response with only marginally raised inflammatory markers and no ascites.
115 INTRACTABLE VOMITING DUE TO GASTRIC NEUROPATHY
S. J. Foley, A. Watson, G. Di Nardo1, R. De Giorgio1, T. Bowling, R. S. Spiller.Wolfson Digestive Disease Centre, University Hospital Nottingham NG7 2UH, UK; 1Department of Internal Medicine & Gastroenterology, St Orsola-Malpighi Hospital, Bologna, Italy
Case report: A 29 year old male developed right chest and abdominal discomfort. He described difficulty initiating swallowing then dysphagia. Painless vomiting after meals followed. He suffered an itchy toxic erythema for one week. His symptoms progressed, and he continued to vomit. He was intolerant of feeding via jejunostomy, and after six months commenced TPN. 18 months after presentation he continues to require TPN.
Initial investigations with blood tests including haematological and biochemical markers, auto-antibodies, OGD, colonoscopy, small bowel follow through, abdominal CT scan, and MRI brain scan were all within normal limits. Gastric emptying studies were incomplete owing to vomiting.
Oesophageal manometry demonstrated an increased lower oesophageal sphincter pressure, but clinical response to balloon dilatation was very transient.
Antro-duodenal manometry was normal. Electrogastrography demonstrated reduced (2–4 cpm) power of 38% (>75%) and reduced pre/post-prandial power ratio 1.4 (>2.0).
Full thickness gastric antral biopsies were stained for SP, VIP, bcl-2, and c-kit. There was reduced staining compared with control in the myenteric plexus for all these markers. These suggest neuronal degeneration and loss of intersitial cells of Cajal.
We conclude that this case of idiopathic gastroparesis was due to a gastric neuropathy.
116 RAPIDLY ACCUMULATING ASCITES: AN UNUSUAL CASE
A. H. Shenoy1, A. Turner2, K. Akhtar2, A. N. Khan3, M. Bradgate2, R. George2, P. Sugarbaker4.1Department of Gastroenterology, Gloucestershire Royal Hospital, Gloucester GL1 3NN, UK; 2Department of Gastroenterology, 3Department of Surgery, 4Department of Pathology, Pennine Acute Hospitals NHS Trust, Rochdale, Lancashire OL12 9QB, UK; 5Department of Radiology, North Manchester General Hospital, Manchester, UK; 6Department of Surgical Oncology, Washington Cancer Institute, Washington DC 20010, USA
Case report: A 56 year old man presented with weight loss and ascites of a few weeks duration. He was exposed to asbestos for four years from the age of 19 years. Chest CT in 2002 had shown minor plural plaque disease only. His ESR was 70 mm at 1 hour and CRP 30 mg/l but FBC, U&E, LFT, Ca, CEA and CA 19–9, ECG, echocardiogram, and lung functions were normal. Ascitic fluid: protein of 65 g/l, cells 20×106 cells/l, (lymphocytes and mesothelial cells on cytology). Gram staining and culture negative. Ultrasound and CT demonstrated moderate ascites, normal liver, spleen, kidneys, and patent portal and hepatic veins. A diagnostic laparoscopy showed multiple small peritoneal deposits and focal infiltration of omentum. Primary peritoneal malignant mesothelioma (PPMM) was confirmed on peritoneal histology. He underwent a cytoreductive surgery followed by perioperative intraperitoneal chemotherapy (PIC). Perioperatively heated 1.5% dianeal containing 100 mg cisplatinum and 30 mg of doxorubicin was perfused into abdominal cavity with continuous manipulation of intraperitoneal surfaces during the chemotherapy treatment. Intraperitoneal chemotherapy was continued for five days post operatively with paclitaxel (40 mg/day). He remains well to date.
Discussion: PPMM is rare but is increasing in frequency. About 20% of cases of mesotheliomas have peritoneal lesions. The commonest cause is asbestos exposure. 1/3 present with abdominal distention, 1/3 with abdominal pain, and the remaining third with combined symptoms. PPMM can be classified into three types: (1) “wet type” presenting with malignant ascites, (2) “dry type” presenting with a focal mass seen on computed tomography, and (3) combined type. Diagnosis may be suspected after ultrasound, CT and MRI, but the final diagnosis is confirmed by a laparoscopic biopsy. CT is useful in determining the extent of the tumour. With cytoreductive surgery and PIC, three year disease progression free survival improves to over 60%. Hyperthermic peritoneal chemotherapy using cisplatin and doxorubicin is shown to be safe with low mortality and minimal morbidity. It allows uniform delivery of chemotherapeutic agent and hyperthermia to the residual peritoneal disease post cytoreductive surgery.
117 WHAT IS THE CAUSE OF THIS CHOLESTATIC JAUNDICE?
A. H. Shenoy, J. L. Parker, J. M. Geraghty, H. G. Thomas, G. L. Constable.Musgrove Park Hospital, Taunton TA1 5DA, UK
Case report: A 63 year old man was admitted with a short history of painless jaundice associated with anorexia, weight loss, fatigue, back pain, and symptoms of urinary bladder outflow obstruction. There were no specific risk factors for liver disease and no alcohol or any drug use. There were no stigmata of chronic liver disease. There was deep jaundice with 4 cm hepatomegaly but no splenomegaly or ascites. Rectal examination revealed a large malignant feeling prostatic mass. Blood analysis results: Hb 8.4 g/dl, MCV 91 fl, WBC 12.56×109/l, platelet count 61×109/l, INR 1.0, ferritin 2130 mcg/l; vitamin B12 and red cell folate were normal. Peripheral blood smear showed a leucoerythroblastic picture. CRP 76, bilirubin 74 umol/l, alkaline phosphatase 4405 u/l, alanine transaminase 219 u/l, albumin 25 g/l, gammaglutamyl transferase 2834 u/l. Viral hepatitis serology and the autoimmune profile were normal. Prostate specific antigen was 336 ng/l. Other tumour markers (CEA, CA 19–9, and alfa feto-protein) were normal. Both ultrasound and subsequent CT scans revealed a normal liver and biliary tree with no evidence of metastases. There were a few stones in the gall bladder and the latter also showed an enlarged prostate with right-sided pelvic lymphadenopathy. An isotope bone scan showed extensive disseminated sclerotic metastases. A liver biopsy was undertaken with continued suspicion of malignant liver infiltration. Liver histology showed extensive extramedullary erythropoiesis and cholestasis but no evidence of metastatic disease.
As there was no evidence of biliary dilatation or obstruction on ultrasound or high resolution CT in our patient, further imaging of biliary tree was not undertaken. Cholestatic jaundice without liver metastases or biliary obstruction is an extremely rare presentation of prostate cancer. We identified only three case reports in the literature, which suggest that this is a paraneoplastic phenomenon. The underlying pathophysiology of this phenomenon is not clear. This is the first reported case of cholestatic paraneoplastic syndrome with extramedullary erythropoiesis but no linkage is known between these two pathological processes.
118 BEWARE OF THIS COMPLICATION OF THERAPEUTIC ENDOSCOPY!
N. V. Radhakrishnan, A. H. Shenoy, R. K. Sharma.Department of Gastroenterology, Rochdale Infirmary, Rochdale OL12 0NB, UK
Case report: We report a serious complication of emergency therapeutic endotherapy for acute variceal bleeding. A 67 year old lady was admitted with severe oesophageal variceal bleeding. She was known to have autoimmune cirrhosis (Child B). Banding failed but sclerotherapy with 17 ml of 3% sodium tetradecyl sulphate (Fibro-vein) was successful in achieving haemostasis. Post-procedure chest x ray was normal. On day 12 CXR done in view of right sided pleuritic chest pain and shortness of breath showed a moderate right pleural effusion which grew Klebsiellaoxytoca. Empyema complicating hospital-acquired pneumonia was managed with intercostal chest drain and appropriate antibiotic. She continued to be pyrexial. On day 35 she noted the appearance of blackcurrant soft drink in the chest drain soon after drinking! A gastromiro swallow confirmed a fistula between the lower oesophagus and right pleural cavity above the diaphragm. Oral feeding was stopped and total parenteral nutrition started. At thoracotomy no oesophageal tear/fistula was seen and decortication of the right lung was done. She was fed through a jejunal feeding tube placed at the time of the surgery. Repeat contrast swallows showed continued presence of the fistula but her general condition was poor for further surgery. She died of upper GI bleeding 81 days after admission.
119 AN UNUSUAL CAUSE OF BACK PAIN
S. Keshav, K. P. Basavaraju, C. S. Keeling-Roberts, C. R. Hunt, N. K. Ahluwalia.Stepping Hill Hospital, Stockport, UK
Case report: An 18 year old White male presented with two months’ history of diarrhoea without any associated blood. There was no history of abdominal pain, nausea, vomiting, recent travel abroad, or antibiotic use. He was a non-smoker and had no family history of IBD. Clinical examination was unremarkable. FBC, U&E, LFT, TFT, calcium, haematinics were normal except for low haemoglobin (Hb) 128 g/l and low albumin at 33 g/l. ESR was raised at 79 mm/hour. Anti-endomysial antibody was negative. The upper GI endoscopy and the duodenal biopsies were normal. Pancolonic patchy inflammation and superficial ulcers with intervening normal mucosa was noted on colonoscopy. Histological examination of the colonic biopsy showed cryptitis and epitheloid granulomas favouring the diagnosis of Crohn’s disease. He was started on oral prednisolone and Balsalazide.
On review six weeks later, his bowel action was normal but he complained of disabling low back pain of 3–4 weeks’ duration. On examination, he was apyrexial with no spinal tenderness and bilateral SLR test was within normal limits. X rays of the lumbosacral spine and sacro-iliac joints were normal. ESR was raised at 87 mm/hour, Hb was 123, and WBC count was raised at 15 with a neutrophil count of 13. LFT showed raised GGT at 148, alkaline phosphatase at 164 U/l, and low albumin at 28. Infection screen and hepatitis screen were negative. He was treated with IV antibiotics and steroids.
Abdominal ultrasound showed partially occlusive thrombus in the superior mesenteric vein (SMV) extending into the portal vein. CT abdomen confirmed the SMV thrombus. He was started on tinzaparin and warfarin. His back pain subsided within two weeks and ESR returned to normal in about four weeks. His thrombophilia screen was negative. He has remained symptom free on warfarin for the last four years.
Thromboembolism is a well recognised serious complication in patients with IBD. Portal vein thrombosis should be considered as one of the differential diagnoses in IBD patients presenting with severe back pain.
120 A DIFFICULT CASE OF UPPER GASTROINTESTINAL HAEMORRHAGE
A. Shah, M. P. S. Skander, M. M. Ahmed.Depatment of Gastroenterology, Good Hope Hospital, Rectory Road, Sutton Coldfield, B75 7RR, UK
Introduction: Bleeding from gastric varices poses a therapeutic challenge and treatment remains controversial. We present a case where bleeding from isolated gastric varices (IGV) was successfully treated with injections of n-butyl-2-cyanoacrylate glue (Histoacryl).
Case: A 77 year old lady with various comorbidity (ishaemic heart disease, treated hypothyroidism, arthritis, and obesity) was investigated in 2001 for mild abnormalities in liver biochemistry. Liver auto-antibodies, hepatitis B and C serology, ferritin, and abdominal ultrasound were all normal and a tentative diagnosis of non-alcoholic fatty liver disease was made. In September 2004, she was admitted with a severe upper gastrointestinal bleed (Hb 11.7 g/dl falling to 9 g/dl). Urgent endoscopy revealed bleeding from isolated fundal varices (IGV type1). She was initially treated with blood/FFP transfusion and iv terlipressin. A Sengstaken tube was inserted and the gastric balloon was inflated. Due to a shortage of beds, she was transferred to an ITU in another hospital where resuscitation continued. There was recurrent bleeding when the Sengstaken tube was removed. It was felt that she was unsuitable for a transjugular intrahepatic porto-systemic shunt (TIPSS) due to the ischaemic heart disease. She continued to bleed intermittently and was transferred back to our unit 11 days later. A further endoscopy was undertaken and the gastric varices (which were still bleeding) were injected with a mixture of 0.7 ml lipiodol and 0.5 ml Histoacryl glue taking care not to block the endoscope. The bleeding ceased and a further injection was instituted two weeks later. The patient made a dramatic recovery and was discharged home a month after the original admission. A CT scan before discharge showed evidence of (asymptomatic) pulmonary glue emboli, a known complication of Histoacryl injection.
Discussion: Histoacryl injection for bleeding gastric varices was first used in 1986 and subsequent studies have shown that it is highly effective. However, Histoacryl injection is still regarded as “experimental” in most centres and facility/expertise is often limited. This case illustrates that appropriate use of Histoacryl injection can be life saving especially if TIPSS is not available or is contra-indicated. Endoscopists should be aware of this technique and be versed in its application.
121 TRAUMATIC JAUNDICE FIVE MONTHS ON: A CASE REPORT
A. Ahmed, A. Banfield, G. R. Plant, J. K. Ramage.North Hampshire Hospital, Basingstoke, UK
Case report: We report a patient presenting to his general practitioner with jaundice five months after a road traffic accident and blunt abdominal injury. The initial injury included contusion of his liver, intracapsular haematoma, and laceration of his spleen. He was managed conservatively with regards to his abdominal injury. Repeat CT scan two weeks later did not reveal any new abnormality.
He subsequently was seen in outpatients with obstructive jaundice. Assessment of the cause of his jaundice, management, and outcome is described. The relevant literature is also discussed.
122 HYPERCALCAEMIA AND A PANCREATIC MASS
A. Banfield, A. Ahmed, I. Ilesley, A. Brooks, C. Pearce, J. Ramage.North Hampshire Hospital Basingstoke and Royal Hampshire County Hospital Winchester, UK
Case report: A 44 year old female presented with amenorrhoea, malaise and episodic diarrhoea. Serum calcium was found to be raised at 3.21 mmol/l (2.1–2.6). Subsequent parathyroid imaging and bone scan were negative. Further tests showed PTH surpressed at <0.11 pmol/l (0.5–4.4), Vitamin D 14.8 μg/l (10–41) and PTHrP raised at 7.3 pmol/l (0.7–1.8). A CT showed a mass in the body and tail of the pancreas 10×6×10 cm. The patient received treatment for presumed hypercalcaemia of malignancy but normocalcaemia could not be maintained. Calcium levels were eventually brought into normal range using Lanreotide Autogel. This is the first time this drug has been used specifically for controlling calcium levels in this kind of tumour. PTHrP levels were unchanged hence the mechanism is speculative. Further management options include chemotherapy, surgery, and radionuclide therapy.
Plenary posters
123 REDUCING INAPPROPRIATE USE OF INTRAVENOUS PROTON PUMP INHIBITORS WITH A COST EFFECTIVE GUIDELINE
A. I. Thuraisingam, P. Adams, J. Makhijani, T. Brooklyn, J. T. Anderson.Cheltenham General Hospital, Cheltenham, Gloucester, UK
Background: Hospital intravenous (IV) proton pump inhibitors (PPI) use was unrestricted within licensed indications. Monitoring prescribing trends, pharmacists observed IVI PPI use was increasing. The clinical indications for IVI PPI were reviewed during the development of IVI PPI guidelines.
Methods: A randomised sample retrospective case note review was performed on patients identified by pharmacy as receiving IV PPI in a six month period before IVI PPI guidelines were introduced. The guideline was promoted via the consultant gastroenterology staff (for example, endoscopy reports); memoranda to wards; in ward formularies, and by “policing” from ward pharmacists. Following guideline introduction a prospective audit was performed on all patients issued with IV PPIs.
Results: In the pre-guideline period, IV PPIs were inappropriately prescribed according to indication or route in 18/19 patients reviewed (95%) resulting in 74 out of 77 doses (96%) being inappropriately administered. In one month after the introduction of the guideline 12 patients used IV PPI. Data were incomplete for one patient. IV PPIs were inappropriately prescribed in 5/11 patients (45%) resulting in 14 out of 112 inappropriately administered doses (13%). In the six month period prior to the guidelines the mean monthly usage of PPI was 163 doses per month. In the six month period following guideline introduction the mean monthly usage decreased by 43% to 93 doses per month.
Discussion: The introduction of an IVI PPI guideline has improved the appropriateness of IV PPI use. An increase in the number of doses per patient prescribed IV PPI was observed, mainly as a result of more appropriate continuous IVI PPI infusions. Despite this, the absolute amount of drug used still decreased. The cost reduction from this decreased use of IV PPI is projected to amount to more than £4000 per year for our hospital. Over the same period there has been no increase in the expenditure on oral PPI drugs.
Conclusion: An IVI PPI guideline backed and promoted by all relevant stakeholders was found to be both clinically and cost effective.
124 LONG TERM FOLLOW UP OF PATIENTS WITH COMMON BILE DUCT STONES MANAGED WITH BILIARY STENTING IN A DISTRICT GENERAL HOSPITAL
J. Gasem, A. Quayle, W. Brough, P. Foster.Macclesfield District General Hospital, SK10 3BL, UK
Background: 890 ERCPs were undertaken during a five year period (01/01/1999 to 31/12/2003). Common bile duct (CBD) stones were found in 336 (37.7%). The CBD was cleared at initial ERCP in 74%. 53 (26%) patients were managed with biliary stenting.
Aim: To determine the outcome of patients with CBD stones managed with biliary stenting.
Method: A retrospective audit of 53 case notes in 2004.
Results: The age range was 50–99 years (median 83). The mean ASA grading was 3. Patients were followed up for a median of 7 months (range 1–43). Of the 53 patients, 13 (24.6%) had their ducts cleared at subsequent ERCP (median three procedures, range 2–5) during a median follow up of 7 months (range 1–43). Six patients were referred to a tertiary centre and the duct was cleared in three. 37 patients were managed with biliary stenting long term and were followed up for a median 11 months (range 3–39) They underwent a total of 96 ERCPs with a median of two (range 1–8) per patient. The median interval between ERCPs was 6 months (range 3–12). Procedure related complications occurred in 2.1%. There were 17 episodes (12 patients) of cholangitis and 10 deaths (three related to stone disease and seven unrelated) in the group managed with long term stenting compared with two episodes (two patients) of cholangitis and no deaths in the group who eventually had their ducts cleared. For the patients who died, the median time to death was 6 months (range 3–23).
Conclusion: Procedural related complications were few. Biliary stenting as a bridge to eventual duct clearance was associated with a low rate of cholangitis. However there was a high rate of cholangitis in patients managed with long term stenting and the mortality in this group was 30%. Death occurred early and was mainly from non-biliary causes indicating significant comorbidity. Clearance of stones from the CBD duct remains the goal of management but long term stenting may still be appropriate for some patients.
125 20 MHZ HIGH FREQUENCY ENDOSCOPIC ULTRASOUND ASSISTED ENDOSCOPIC MUCOSAL RESECTION: A PROSPECTIVE ANALYSIS OF COLORECTAL SUBMUCOSAL LESIONS
D. P. Hurlstone1, M. A. Karajeh1, S. S. Cross2, K. D. Drew1, M. E. McAlindon1, D. S. Sanders1.1Gastroenterology, Royal Hallamshire Hospital, Sheffield; 2Academic department of Pathology, Royal Hallamshire Hospital, Sheffield, UK
Background: 20 MHz high frequency mini-probe ultrasound enables in vivo imaging of submucosal colorectal lesions (SMTs). Endoscopic mucosal resection permits extended horizontal and vertical excision margins by cleaving the submucosal layer anterior to the muscularis propria (MP). Using a combined EUS and EMR technique for SMTs may offer an endoscopic therapeutic alternative to surgery in this select patient group.
Aim: To establish the safety and efficacy of high frequency 20 MHz EUS assisted EMR for the management of colorectal submucosal lesions.
Methods: Twenty nine lesions were referred for EUS assisted EMR. A single endoscopist performed all examinations. Endoscopic exclusion criteria were (1) >20 mm diameter; (2) associated mucosal ulceration; (3) poor echo definition of the MP. All SMTs were imaged using 20 MHz EUS with water fill or balloon acoustic coupling. Morphology was defined according to the JCSC. EMR was performed using the Karita 0.18% n-saline lift and cut technique. Histological diagnosis was made in all cases. Endoscopic and EUS follow up was at 3, 6, and 12 months.
Results: Nineteen lesions met inclusion criteria (4 carcinoid, 6 leiomyoma, 4 lipoma, 3 lymphangioma, 2 fibrovascular polyps). Median diameter 8 mm (range 3–20). EUS assisted EMR was successful in 18/19 (95%) lesions. Immediate bleeding occurred in one patient requiring endoclip haemostasis. Resection was histologically verified as complete in 16 (88%) cases. There was no association between the submucosal lesion position (sm1–3) with regard to margin negativity and resection rates (p>0.5). Two patients with rectal carcinoid failed to lift symmetrically at EMR despite adequate EUS visualisation of the third hypoechoic layer. Both were referred for transanal resection. No evidence of local recurrence was identified at a median follow up interval 8 months (range 1–12).
Conclusions: 20 MHz EUS assisted EMR offers an effective alternative to surgery in a select cohort of colorectal SMTs. The combined technique provides an en bloc histopathological specimen permitting resection margin assessment.
126 ENDOSCOPIC ABLATION OF DYSPLASTIC BARRETT’S OESOPHAGUS COMPARING ARGON PLASMA COAGULATION AND PHOTODYNAMIC THERAPY: LONG TERM RESULTS OF A RANDOMISED PROSPECTIVE TRIAL
N. Kapoor1, K. Ragunath1, V. S. V. S. Raman1, M. T. M. T. Haqqani2, N. Krasner1.1Aintree Centre for Gastroenterology and 2Department of Pathology, University Hospital Aintree, Liverpool, UK
Introduction: Endoscopic mucosal ablation with argon plasma coagulation (APC) and photodynamic therapy (PDT) is a promising technique to treat dysplastic Barrett’s oesophagus. A previous randomised prospective study has shown comparable effects at 4/12.1 We aimed to determine the long term effects on dysplasia eradication and malignancy risk.
Methods: Twenty nine patients with dysplastic Barrett’s oesophagus 3–10 cm, (24 LGD, 5 HGD) were randomised to mucosal ablation with either PDT (13) or APC (16). PDT was performed 48 hours after intravenous injection of Photofrin 2 mg/kg with 630 nm red laser light, 200 J/cm through a PDT balloon in one session. APC was performed at power setting of 65W, argon gas flow 1.8 l/min in 1–6 sessions (mean 3). All patients were maintained on high dose proton pump inhibitors. Outcome data were obtained from case note scrutiny and endoscopy/histology database analysis.
Results: Follow up interval from initial treatment to latest OGD is 112–1122 days (average 703). Of 13 PDT treated patients (2 HGD, 11 LGD), one patient developed oesophageal adenocarcinoma (within a 12 month period). No other patients had any degree of dysplasia on their latest histology but all had residual metaplasia on histology. Barrett’s length was reduced by 35% on follow up.
Of 16 APC treated patients (3 HGD, 13 LGD), no patients have developed malignancy. Three patients had LGD and none had HGD on latest histology. 13/16 had residual metaplastic tissue. Residual Barrett’s length was reduced by 42%.
Conclusions: Mucosal ablative strategies may have an important role in the management of patients with dysplasia in Barrett’s oesophagus. Mucosal ablation may downgrade or prevent the progression of dysplasia. APC and PDT have similar efficacies long term. However, the majority of individuals have residual metaplastic tissue on follow up, with potential further malignant potential, and continued surveillance is necessary.
1
127 IDENTIFICATION AND CHARACTERISATION OF PROTEINS INTERACTING WITH EUKARYOTIC DNA TOPOISOMERASE I
A. V. McNamara, A. J. M. Watson, J. R. Jenkins.University of Liverpool, School of Clinical Science, Division of Gastroenterology, First Floor Nuffield Building, Crown Street, Liverpool, L69 3BX, UK
Background: Human topoisomerase I (Top I) is of considerable biomedical importance because it is the target of the camptothecin (CPT) family of anticancer drugs. Derivatives of CPT, irinotecan (IRT) and topotecan (TPT) are routinely used in clinic, primarily in the treatment of metastatic colorectal cancer. The aim of this study is to identify novel proteins interacting with Top I, which may reveal new potential chemotherapeutic targets.
Methods: Proteins that interact with Top I were identified using extracts from the human colon adenoma HCT116 cell line by immunoprecipitation, followed by mass spec (MALDI-TOF) analysis. Interactions were confirmed by counter immunoprecipitation.
Results: Using the above methodology we have identified 18 proteins as physically interacting with Top I. One of these is Hsp70, which is known to be associated with Top I. Seven of these interactions have been confirmed, which include the molecular chaperone Hsp90. This is the target of new up and coming anti cancer therapies. Using the Hsp90 inhibitor geldanamycin (GA) on the HCT116 cell line, we have disrupted the Top I and Hsp90 interaction. When a Topoisomerase I poison is also added we see a synergistic effect on both cell killing and proliferation inhibition. Surprisingly we have also demonstrated that up to 48 hours after GA treatment Top I is not degraded. This is despite the fact that GA binding is thought to promote assembly of a super chaperone machine that favours client protein degradation (Scheider et al, 1996).
Conclusion: We have identified a direct interaction between Top I and Hsp90, and found the combination of GA and Top I poisons act synergistically to both inhibit the growth of and kill colorectal cancer cells.
Continuing work: Elucidation of the mechanism behind the synergistic effect observed when Top I and Hsp90 inhibitors are used in combination.
128 THE INTRINSIC AND EXTRINSIC APOPTOTIC PATHWAYS ARE RAPIDLY ACTIVATED IN RESPONSE TO OXIDATIVE STRESS IN PANCREATIC ACINAR CELLS
H. K. Baumgartner1,2, L. Ashurst1, R. Sutton3, A. Tepikin1, O. H. Petersen1, A. J. M. Watson2, O. V. Gerasimenko1.1Department of Physiology and Divisions of2 Gastroenterology and 3Surgery & Oncology, University of Liverpool, Liverpool, UK
Background: Oxidative stress plays an important role in the pathogenesis of acute pancreatitis. Cytosolic calcium elevations precede both acinar cell necrosis and apoptosis. We have investigated the mechanisms of apoptosis by measuring real time caspase activation induced by oxidative stress in pancreatic acinar cells, examining both the intrinsic (via caspase-9) and extrinsic (via caspase-8) apoptotic pathways.
Methods: Isolated mouse pancreatic acinar cells were loaded with fluorescent substrates (molecular probes) for activated caspase-9, caspase-8, caspase-3, and a general caspase substrate. Using confocal microscopy, fluorescence of cleaved substrate was imaged in real time in response to the oxidant menadione (Gerasimenko et al, 2002). Caspase activity was examined in the presence and absence (BAPTA-AM treated cells) of cytosolic calcium or reduced ER calcium.
Results: Caspase-9 was activated within a few minutes after administration of menadione. Time to ½ max activation (t1/2) was 129±43 s; n = 12. Fluorescence from the general caspase substrate showed a similar time course of activation as caspase-9, suggesting that caspase-9 is the first activated caspase. T1/2 104±48 s; n = 19. Activation of caspase-9 was inhibited in the presence of BAPTA-AM, but not in the presence of TPEN. Caspase-8 was activated (t1/2) within 26±3 minutes after treatment with menadione in 5–15% of cells. Activation of caspase-8 was not effected by the presence of BAPTA-AM or TPEN. We also studied the spatial distribution of caspase-9, 8, and 3 using confocal microscopy. Caspase-9 was activated at or close to mitochondria in response to menadione in pancreatic acinar cells. In contrast caspase-8 distribution was homogeneous in the cytosol.
Conclusions: Both the intrinsic (caspase-9) and extrinsic (caspase-8) apoptotic pathways are rapidly activated in response to oxidative stress in the pancreatic acinar cell. Caspase-9 is activated in a calcium dependent manner close to mitochondria. Caspase-8 is also activated in some cells and this activation is calcium independent and spatially homogeneous.
129 AUTOMATED IDENTIFICATION OF OESOPHAGEAL PERISTALSIS AND CLASSIFICATION OF DISMOTILITY USING A ROLLING CORRELATION METHOD
S. Perring (introduced by J. A. Snook).Poole Hospital NHS Trust, Poole, Dorset, BH15 2JB, UK
Oesophageal manometry is used to classify oesophageal functional disorders. Classification of disorders is based on diversion from normal parameters of lower oesophageal sphincter function and oesophageal peristalsis. However normal oesophageal peristalsis covers a wide range of amplitude and propagation speed, and the limits for abnormality are fairly arbitrary. Assessment is normally performed by visual inspection or by proprietary software based on threshold or peak identification.
An automated system for identification of oesophageal peristalsis and calculation of propagation speed has been developed by calculating a rolling correlation coefficient between a portion of the manometry trace and a representative peristaltic wave template. The initial standard wave template was generated from averaging peristalsis in 10 normal oesophageal studies. A further wave template was then generated from the 10 best peristaltic waves identified in the individual patient data and the rolling correlation recalculated iteratively. Peristaltic waves are identified by a correlation coefficient peak of >0.65 and their exact onset time identified by the position of the peak of the correlation curve.
The performance of this technique was compared with threshold detection and peak identification automated techniques. For 10 normal oesophageal studies the success at automatic identification of peristalsis was compared with expert visual inspection of the manometry traces.
This technique offers the potential for more precise and reliable automated identification of oesophageal peristalsis as well as more consistent measurement of propagation speed. It offers the possibility of more subtle classification of oesophageal motility abnormalities.
Abstract 129
130 SIMPLE NON-INVASIVE CRITERIA PREDICT THE PRESENCE OF OESOPHAGEAL VARICES IN HEPATITIS C CIRRHOSIS
W. J. Griffiths, T. Woodall, A. E. Gimson, G. J. Alexander, M. E. D. Allison.Department of Hepatology, Addenbrooke’s Hospital, Cambridge, CB2 2QQ, UK
Background: Clinical practice guidelines state that patients with cirrhosis should undergo endoscopic screening for oesophageal varices and that non-selective beta blockade is indicated for those with medium to large varices to reduce the risk of variceal haemorrhage. However, fewer than 50% of patients screened will have varices and 13–20% will require primary prophylaxis. Accurate non-invasive prediction could significantly reduce endoscopic requirements resulting in cost savings and improved patient satisfaction.
Methods: A retrospective analysis was performed on hepatitis C patients with severe fibrosis or cirrhosis on biopsy who had undergone screening endoscopy. Platelet count, prothrombin time, and spleen length at the time of each OGD episode were recorded. Patients were excluded if they had a history of splenectomy, or the presence of coexisting liver disease, hepatoma, or portal vein thrombosis.
Results: 133 patient episodes (104 patients: 93 cirrhosis, 11 severe fibrosis) fulfilled criteria for inclusion. Oesophageal varices were present in 44 cases (33%) and grade 2/3 varices in 11 cases (8%). Platelet count <100 and/or spleen length ⩾14 cm had a sensitivity and specificity for the presence of varices of 95% and 67% respectively. 62 OGDs (47%) could have been avoided with a false-negative rate of only 5%. Importantly no medium to large varices would have been missed. In those with a history of ongoing excess alcohol (35 episodes) sensitivity for varices was 100%.
Conclusions: Varices in hepatitis C cirrhosis can be accurately predicted by simple non-invasive markers of portal hypertension. Pre-selection based on the criteria above would obviate the need for endoscopy in nearly half our currently-screened population, without missing those who would require primary prophylaxis. This would clearly be of benefit to both physicians and patients alike. These criteria are currently being validated in a cohort of hepatitis C patients from a separate institution.
131 INCREASING BURDEN OF LIVER DISEASE: HOSPITAL ADMISSION RATES IN ENGLAND, 1989/90–2002/03
M. Fullard1, S. Westlake2, V. Osborne2, A. Majeed3, J. D. Maxwell1, S. Clark1, C. Tibbs1, J. Y. Kang1.1Department of Gastroenterology, St George’s Hospital, 2Office for National Statistics, 3Department of Primary Care & Social Medicine, Imperial College, London, UK
Aim: To investigate time trends for hospital admission rates in England for liver diseases from 1989/90 to 2002/03.
Methods: Data on admission rates for liver diseases (ICD-9 570–573, 070, ICD-10 K70–76, B15–19) were obtained from the Hospital Episodes Statistics (HES) service. Day cases were excluded. Data for hepatitis C were only available from 1995/96 to 2002/03*.
Results: Overall admissions increased by 71% in males, 43% in females. For alcoholic liver disease, the increase was more marked, affecting all age groups and both sexes. Admission rates for hepatitis A fell overall, but rose among males aged 15–44, 65–74, and ⩾85 years. For hepatitis B, admission rates increased overall, but fell in males aged 15–24, 65–74, and ⩾85 years. Admission rates for hepatitis C rose overall, but fell for both men and women aged 25–34, and for men ⩾85 years.
Conclusions: Hospital admission rates for most forms of liver disease increased from 1989/90 to 2002/03, while those for hepatitis A fell. A worrying trend is the large increase in admission rates for alcoholic liver disease in younger subjects as well as older individuals. These data have implications for public education and health care planning, particularly with respect to liver transplantation.
Abstract 131
132 EXAGGERATED POSTPRANDIAL COLONIC MOTILITY IN IRRITABLE BOWEL SYNDROME: A ROLE FOR 5-HYDROXYTRYPTAMINE?
W. Atkinson1, S. J. Lockhart1, B. G. Keevil, P. J. Whorwell, L. A. Houghton.Departments of Medicine & 1Clinical Chemistry, University Hospital of South Manchester, M20 2LR, UK
Background: Colonic motility in many patients with irritable bowel syndrome (IBS) appears to be exaggerated, particularly after meals.12 5-hydroxytryptamine (5-HT) plays an important role in the normal control of motility,3 but its involvement in the motor dysfunction associated with IBS is unclear.
Aims: To investigate the relation between platelet depleted plasma 5-HT (PDP 5-HT) concentrations and the colonic motor response to a standard meal in patients with IBS compared with healthy volunteers.
Methods: PDP 5-HT concentrations were assessed for 5 hours (30 minute intervals) following a standard meal (530 kcal), while simultaneously recording colonic motility in 35 patients with IBS (aged 19–53 years, eight male) and 16 healthy volunteers (18–39 years, six male). Motility was recorded using a 5-channel (spaced 5 cm apart) solid state catheter introduced to a depth of 35 cm by flexible sigmoidoscopy into the unprepared colon. 5-HT concentration was measured by reverse-phase high performance liquid chromatography with fluorimetric detection.
Results: Both colonic motility (activity index (AI): 15.52 mm Hg (median)) and PDP 5-HT concentration (24.53 nmol/l (mean)) were greater in IBS patients compared with healthy volunteers (AI: 8.92 mm Hg, difference from IBS (95% CI), −7.36 mm Hg (−15.22 to 0.74) mm Hg, p = 0.028; PDP 5-HT: 17.64 nmol/l, ratio IBS:HV, 1.39 (0.96 to 2.02), p = 0.079). In addition, the amount of motility directly correlated with PDP 5-HT concentration in patients with IBS (r = 0.435, p = 0.009), but not in healthy volunteers (r = 0.338, p = 0.201).
Conclusions: These data are the first to provide evidence for a possible link between 5-HT and the exaggerated colonic motility response seen following meal ingestion in patients with IBS.
1
2
3
133 INFORMATION NEEDS OF PATIENTS WITH OESOPHAGOGASTRIC CANCER
A. N. Hopper, C. Gent, M. R. Stephens, M. C. Allison, W. G. Lewis.Department of Surgery, Royal Gwent Hospital, Newport, UK
Background: An extraordinary thing about the medical profession is that it has managed to avoid sharing the truth with patients for so many centuries. In 1672 the French physician de Sorbiere considered the idea, but thought that it might seriously jeopardise medical practice and concluded that it would not catch on.
Aims: To assess the information needs of patients diagnosed with oesophagogastric cancer and compare this to the perceived information needs in the opinion of junior doctors.
Methods: Sixty of 68 patients (88%) responded to a postal questionnaire (median age 68 years (range 43–85), 48 male, 37 with a diagnosis of gastric cancer, 23 oesophageal cancer). Thirty one of 50 doctors (62%; 12 PRHOs, 9 SHOs, 10 SpRs) responded to a questionnaire regarding their information sharing practices.
Results: Ninety seven per cent of patients wanted all possible information about their diagnosis, but only 29% of doctors were willing to give all the available information (χ2 53, DF1, p<0.01). Sixty four per cent of patients wanted to receive their diagnosis from a doctor and 24% of patients would have preferred to receive their diagnosis from a clinical nurse specialist. Doctors believed that all patients should receive their diagnoses from doctors (χ2 43, DF1, p<0.01). Eighty one per cent of doctors were willing to communicate a serious illness with a good prognosis, however only 45% would communicate a diagnosis with a poor prognosis (χ2 8, DF1, p<0.01). Of the 26 doctors who had received formal training in breaking bad news, 12 (46%) considered this training to be inadequate.
Conclusion: The majority of patients with a diagnosis of oesophagogastric cancer want a great deal of information concerning their illness. Adequate training in information disclosure may help address this issue.
134 RED LIGHT EXCITATION OF METHYLENE BLUE CAUSES DNA DAMAGE IN OESOPHAGEAL ADENOCARCINOMA CELLS
R. G. Sturmey1, J. R. Olliver1, C. P. Wild1, P. Sahay2, L. J. Hardie1.1Molecular Epidemiology Unit, The LIGHT Laboratories, University of Leeds, Leeds LS2 9JT; 2Endoscopy Department Pontefract General Infirmary, Pontefract, WF11 1PL, UK
Background: Barrett’s oesophagus is a precancerous metaplastic condition which carries an increased risk of progression to oesophageal adenocarcinoma. Endoscopic identification of Barrett’s oesophagus, and targeting of areas for biopsy and subsequent histological analysis can be aided by the use of vital dyes, such as methylene blue (MB); a procedure referred to as chromoendoscopy. MB, when photoexcited, generates reactive oxygen species which can cause mutagenic DNA lesions. We have reported that levels of DNA damage are increased in Barrett’s mucosa following MB chromoendoscopy. It may be possible to minimise DNA damage during chromoendoscopy by varying light wavelength and MB concentration and we have investigated this in an in vitro model.
Methods: Cells from the oesophageal adenocarcinoma line OE33 were challenged with 15 mM MB excited by either full spectrum white light or 633 nm red light (the specific excitation wavelength of MB). In addition, the concentration of MB was varied (0.015–15 mM). DNA damage was measured in treated cells by Comet assay, modified for the detection of oxidised purines such as 8-oxo-deoxyguanosine.
Results: Photoexcited MB caused DNA damage in a concentration dependant manner; the amount of damage was decreased by lower concentrations of MB (1.5 mM p<0.01; 0.15 mM p<0.01 Vs15 mM). Illumination of MB challenged cells with red light caused 1.5-fold higher level of strand breaks in DNA compared with excitation by white light (p<0.001). The proportion of oxidative lesions was relatively similar in both groups.
Conclusions: These data provide further evidence for the potential mutagenic effect of MB when combined with endoscopic light. The results show that the red light portion of the spectrum is responsible for excitation of MB and the majority of DNA damage. Simple modifications to chromo-endoscopy practise, such as filtering out red light from endoscopic white light, or reducing MB concentration may limit DNA damage induced by the procedure.
Funded by Yorkshire Cancer Research Grant #YCRL305.
135 SPECIALIST REGISTRARS IN THE UK HAVE SUBOPTIMAL TRAINING IN CLINICAL NUTRITION
S. C. Cooper, J. M. Colby, K. A. Davidson, C. U. Nwokolo.Walsgrave Hospital, University Hospitals Coventry and Warwickshire, Coventry, UK
Introduction: Up to 40% of hospital admissions are malnourished, delaying recovery from surgery, prolonging rehabilitation, and increasing hospital stay. Knowledge of nutrition has been poor among doctors; thus the government published “A core curriculum for nutrition in the education of health professionals” in 1994. Medical student teaching is reported to have improved since the department of health published “Nutrition for Medical Students” (1995). The Royal College of Physicians have published recommendations for doctors in 2002.
Aims and Methods: We aimed to establish the current level of nutritional education, knowledge and practices of general medicine specialist registrars (SpRs). A two-sided questionnaire was distributed at a regional training day.
Results: Sixty four completed questionnaires were analysed from an attendance of 140, a response rate of 46%. All specialities and years (72% in the first 3 years) were represented. Thirty six per cent (n = 23) of SpRs received nutrition education at medical school, 87% of which was didactic. Only 30% (n = 19) received any postgraduate education. Forty one per cent (n = 26) have never seen a PEG insertion, with 38% (n = 24), understanding the correct procedure of consent for incompetent patients. Only 9% (n = 6) knew to use albumin “rarely or never” as a nutritional marker. Seventy two per cent (n = 46) are able to calculate BMI, while 52% (n = 33) identified the healthy range. The correct advised intake for the average male and female was correctly identified in 34% (n = 22) and 42% (n = 27) respectively. Seventeen per cent (n = 11) quoted the correct number of calories in one litre of 5% dextrose, and 9% (n = 6) correctly indicated that one litre of 0.9% saline contained 154 mmol of sodium.
Conclusions: Knowledge of clinical nutrition is important in day to day medical practice, and steps were taken in the 1990s to improve the training of medical staff in this discipline. This survey of general medical SpRs identifies that although some have acquired good knowledge and practices, many are still lacking the training and skills as set down by the Royal College of Physicians’ report in 2002.
136 PROPHYLACTIC VACCINATION AGAINST Helicobacter pylori in the Mongolian gerbil
A. H. T. Jeremy, Y. Du, M. F. Dixon1, P. A. Robinson, J. E. Crabtree.Molecular Medicine Unit, St. James’s University Hospital, Leeds and 1Department of Pathology, The General Infirmary, Leeds, UK
Introduction: Vaccines against H pylori could circumvent the problem of increasing antibiotic resistance and be particularly useful in developing countries where re-infection rates are high following standard eradication regimes. The Mongolian gerbil is a good model for H pylori infection as the gastric pathology induced by infection mirrors that in the human. Furthermore, the inflammatory response to H pylori infection in gerbils is considerably greater than that observed in murine models. The aim of this study was to determine if gerbils could be prophylactically vaccinated against H pylori.
Methods: Mongolian gerbils were vaccinated orally three times with H pylori whole cell sonicate with cholera toxin (CT) adjuvant. Vaccinated gerbils (Vac) (n = 10), CT adjuvant controls (n = 10), and controls (n = 10) were challenged with H pylori 4 weeks later and sacrificed 6 weeks post-infection. H pylori strain 42GX (a Chinese clinical isolate) was used for both vaccination and challenge. Gastric mucosa was taken for histology, microbiology, urease test and snap frozen for analysis of cytokine transcripts by RT-PCR.
Results: All infection and CT controls (20/20) were H pylori positive by culture and/or urease test. In contrast, only 2/10 vaccinated gerbils were H pylori positive (χ2, p<0.001). Protection was associated with increased serum H pylori IgG antibodies and reduced gastritis. One of the two infected Vac animals had mild chronic inflammation in the antrum, the other infected and all non-infected Vac animals had normal mucosa. In the control groups the degree of inflammation was variable. 25% (5/20) had corpus gastritis and 2/20 had corpus mucous metaplasia. Gastric IL-12p40 and IFNγ transcripts were significantly decreased in vaccinated animals compared with infection and CT controls (p<0.01). Only low levels of gastric IL-10 and TGFβ transcripts were found.
Conclusions: Gerbils can be successfully vaccinated against H pylori. In contrast to mice, no post-immunisation gastritis was evident in the Mongolian gerbil model.
137 MORE RESOURCES TO IMPLEMENTATION OF THE “TWO WEEK RULE” WILL NOT LEAD TO DIAGNOSIS OF COLON CANCER AT AN EARLIER STAGE
R. Shenderey, M. Prince, D. Nylander.Department of Gastroenterology, City Hospitals Sunderland NHS Trust, UK
Introduction and Aims: Part of the rationale for the implementation of the “two week rule” pathway (2WP) for patients with cancer was to improve outcomes by shortening the period from presentation to diagnosis and thus, treatment as it was felt that delays in the pathway at this point led to more advanced disease at diagnosis. The hope was that if specialists see patients with a defined set of symptoms promptly, then cancers would be diagnosed at an earlier stage.
We carried out an audit of our patients with LGI cancer to assess: (1) if all patients with the designated urgent symptoms were referred within the 2WP; (2) if referral via the 2WP led to diagnosis at earlier disease stage; (3) if patients with left sided disease were more likely to present to their general practitioner complaining of symptoms and consequently be referred urgently.
Method: All patients with LGI cancer diagnosed in the 12 month period from 1 January 2003 identified from the hospital database. Their notes were requested. One author (RS) analysed all notes received, extracting all demographic and relevant clinical data, which were entered on to a database
Results: 145 patients had a diagnosis of LGI cancer in the relevant period. 142 notes were retrieved for analysis. 81 were males. Median age was 69 years (range 41–90). See table for further details.
Abstract 137
Discussion and Conclusions: Our audit demonstrates the following:
-
Four years since implementation of the 2WP, the majority of patients with lower GI cancer are still being referred using standard letter despite most having designated high risk symptoms.
-
Patients referred via 2WP do not have earlier stage disease.
-
Patients referred via 2WP do not have significantly more left sided disease (χ2 p = 0.08) than those referred by standard posted letter.
Devoting more resources to making the 2WP more efficient will probably not lead to diagnosis of earlier stage colon cancer. It may be that any additional resources should be directed to screening programmes.
138 FAILURE OF TREFOIL PEPTIDE RESPONSE TO MUCOSAL INJURY IN NEONATAL NECROTISING ENTEROCOLITIS
D. Vieten, A. P. Corfield, D. Carroll, P. Ramani, R. D. Spicer.Mucin Research Group, Department of Paediatric Surgery, Bristol Hospital for Children, Upper Maudlin Street, Bristol BS2 8AE, UK
Background: Necrotising enterocolitis (NEC) is a major cause of morbidity and mortality in neonatal intensive care units. The aetiology is multifactorial and its pathogenesis poorly understood. The trefoil peptides (TFF1–3) and mucins contribute to mucosal protection in the intestine. TFFs play a fundamental role in epithelial protection, repair, and restitution and are upregulated in of mucosal repair. Mucins are major structural components of the supramucosal protective barrier.
Aims: We hypothesise that impaired mucosal regeneration, partly due to failure of TFF upregulation, contributes to the pathogenesis of NEC. This study investigates MUC 1–5AC and TFF 1–3 mRNA and trefoil gene product levels in the GI tract of infants with NEC and normal controls.
Methods: Parents of babies up to 44 weeks’ gestation having laparotomy and bowel resection were approached for consent. Bowel samples were fixed in formalin and then embedded in paraffin. Trefoil and mucin mRNA expression and TFF localisation was determined by in situ hybridisation and immunohistochemistry.
Results: Patient groups were 16 with NEC, eight recovering from NEC, and 20 controls. TFF 1 and 2 mRNA expression was not detected in any of the NEC specimens and there was a downregulation of TFF3 expression in 77% of NEC patients. Immunohistochemistry revealed a decrease in TFF3 in sites adjacent to mucosal damage secondary to NEC. Patterns for TFF1 and 2 matched the in situ results. Mucin gene expression is unchanged in NEC compared to normal controls for both membrane bound and secreted mucins.
Conclusions: While TFF1–3 upregulation occurs in response to gut mucosal injury, our results suggest that there is a lack of TFF expression in response to NEC in the premature gut despite preservation of structural constituents of the supramucosal barrier. This may lead to impaired mucosal restitution and contribute to the cascade of bowel necrosis and generalised sepsis characteristic of the disease.
139 GASTRIC PHENOTYPE ASSOCIATED WITH CARDIA CANCER INDICATES DUAL AETIOLOGY
S. Hansen1, K. Melby1, S. Aase1, E. Jellun1, V. Fyfe2, J. Ferguson2, S. E. Vollset1, K. E. L. McColl2.1Norwegian Cancer Register, Norway; 2Western Infirmary, Glasgow, UK
Background: Non-cardia gastric cancer is positively associated with H pylori induced atrophic gastritis and hypochlorhydria. In contrast, oesophageal adenocarcinoma is negatively associated with H pylori infection occurring in subjects with healthy acid secreting stomachs and reflux. The aetiology of cardia cancer and associated gastric phenotype is unclear and we have studied the latter.
Methods: The study was based on 101 601 individuals from the Norwegian JANUS Cohort Study. To each of 123 non-cardia gastric cancer cases and 41 cardia cancer cases, three controls were matched. Serum from each subject was stored frozen a median of 12.1 years since collection and tested for anti-Hp antibodies and pepsinogen I/II ratio.
Results: Non-cardia gastric cancer was positively associated with H pylori (OR 4.75, 95% CI 2.56 to 8.81) infection whereas cardia cancer was negatively associated with infection (OR 0.27, 95% CI 0.12 to 0.59). Non-cardia cancer was associated with atrophic gastritis with the risk of cancer progressively increasing with each falling quintile of pepsinogen I/II ratio. (1 ref, 1.2, 2.5, 5.3, 11) (p<0.000 for trend). Cardia cancer showed a complex pattern with respect to pepsinogen I/II in that the mean value was similar to the controls but there was a significant over-representation of H pylori associated atrophy (pepsinogen I/II <5) in the cardia cancer group v controls (44% v 19%, p = 0.02).
Summary: Non-cardia cancer is positively associated with H pylori infection and atrophy. In contrast, cardia cancer is negatively associated with H pylori infection but positively associated with atrophy.
Conclusion: These findings are most consistent with cardia cancer being of dual and disparate aetiology. Some cases being similar to oesophageal adenocarcinoma and negatively associated with H pylori infection and others being similar to non-cardia cancer and positively associated with H pylori atrophic gastritis. H pylori infection may therefore both predispose to, and protect from, cardia cancer.
140 A COMMON CTLA4 HAPLOTYPE ASSOCIATED WITH COELIAC DISEASE
K. A. Hunt1, D. P. B. McGovern2, P. J. Kumar3, S. Ghosh1, S. P. L. Travis2, J. R. F. Walters1, D. P. Jewell2, R. J. Playford1, D. A. van Heel1.1Imperial College; 2University of Oxford; 3Barts and the London NHS Trust, UK
Introduction and Aims: Coeliac disease is a common enteropathy with a strong inherited risk characterised by dietary wheat, rye, and barley induced T cell activation. Although there is replicated linkage to 2q33, results are inconsistent from association studies of the most promising candidate genes: the CD28/CTLA4/ICOS cluster. CTLA4 plays a key role in regulating T lymphocyte mediated inflammatory responses, and variants in the 3′ region influence development of diabetes and thyroid disease.
Methods: We genotyped CTLA4 variants (−1722 C/T, −658 T/C, −318 C/T, +49 A/G, +1822 C/T, CT60 A/G) to tag all common haplotypes (>5% frequency) and an ICOS variant (IVS+173 C/T) in 340 white UK coeliac disease cases. Strict ascertainment criteria for coeliac cases required both villous atrophy at diagnosis and positive serology. 973 healthy controls were available for SNP, and 705 for CTLA4 haplotype, based association analyses.
Results: Coeliac disease showed weak association with the CTLA4 +1822 T (p = 0.019) and CT60 G (p = 0.047) alleles. Strong association was seen with a common CTLA4 haplotype (p = 0.00067, odds ratio 1.41), of frequency 32.7% in coeliac disease and 25.5% in healthy controls.
Conclusions: A common CTLA4 haplotype shows strong association with coeliac disease, and contains multiple alleles reported to affect immunological function. Loss of tolerance to dietary antigens in coeliac disease may be mediated in part by heritable variants in co-signalling genes regulating T cell responses.
141 IMPAIRED ACUTE INFLAMMATION IN THE TERMINAL ILEUM OF CROHN’S PATIENTS
D. Marks1, D. Oukrif1, M. Novelli1, A. Forbes2, A. W. Segal1, M. Harbord1,2.1University College London; 2St Mark’s Hospital, Middlesex, UK
Background: The acute inflammatory response is reduced at sites of skin and rectal trauma in quiescent Crohn’s disease (CD).
Hypothesis: Acute inflammation is attenuated in the ileum in CD.
Method: Paired biopsies were taken from the neo-terminal ileum and rectum from patients with CD or non-inflammatory controls with familial adenomatous polyposis (FAP), all of whom had ileorectal anastomoses. Each biopsy margin was re-biopsied 6 hours later. The mean Harvey-Bradshaw index was 2 and mean CRP <4 mg/l. No immunosuppressives were prescribed. The number of cells stained with anti-myeloperoxidase (MPO) and anti-IL-8 were determined in a blind fashion in five randomly selected high power fields (hpf).
Results: Inflammation was minimal in all baseline samples. In FAP, trauma induced substantial neutrophil infiltration and IL-8 production in the ileum and rectum respectively (MPO: 201.5 and 130.0 cells/hpf; IL-8: 219.8 and 141 cells/hpf). The response was significantly weaker in CD (MPO: 86.2 and 60.0 cells/hpf; IL-8: 36.5 and 49.5 cells/hpf). The magnitude of the inflammatory response was highly correlated between each paired post-traumatic ileal and rectal sample (MPO: r2 = 0.9267, IL-8: r2 = 0.9194, p<0.05).
Conclusions: This further indicates that CD may be an immunodeficiency disease.

Abstract 141
142 SPECIFIC HAPLOTYPIC VARIATIONS OF THE MULTIDRUG RESISTANCE 1 (ABCB1/MDR1) GENE ARE ASSOCIATED WITH SUSCEPTIBILITY OR RESISTANCE TO ULCERATIVE COLITIS
G. T. Ho1, N. Soranzo2, E. Nimmo1, A. Tenesa1, D. Goldstein2, J. Satsangi1.1Gastrointestinal Unit and MRC Human Genetics Unit, Western General Hospital, Edinburgh; 2Goldstein Laboratories, University College London, London, UK
Background and Aims: Our previous genetic data suggest a complex contribution of the allelic variants of the multidrug resistance gene (ABCB1/MDR1) in determining susceptibility to UC.1 We have now performed a detailed haplotypic study by selecting informative tagging SNPs (htSNPs) which span the ABCB1/MDR1 gene in a case control association study.
Methods: Six htSNPs representing common haplotypic variations of the ABCB1/MDR1 gene were genotyped in 249 UC, 179 Crohn’s disease (CD) and 260 controls. Haplotypes were inferred using the expectation-maximisation algorithm. Association was tested using log-likelihood ratio and single haplotype analysis using Fisher’s test.
Results: On log-likelihood analysis, a highly significant association was observed with UC, p = 4.22×10−7. On single haplotype analyses, 4 and 1 haplotypes were positive and negatively associated with UC respectively (p values 0.001–0.004). Further analysis revealed three of the six htSNPs (Tag 1-intron 3, Tag 8-C3435T, and Tag 11-intron 27–9) to be critical in the observed associations. Haplotypes composed of these three htSNPs retained a highly significant association with UC (p = 6.8×10−5). Protective haplotypes composed from 6 and 3-locus tSNPs share the same alleles and retain a highly significant negative association with UC (both p<0.0001). No association was seen with CD.
Conclusions: This study shows that specific haplotypic variants of ABCB1/MDR1 gene can increase or decrease susceptibility to UC. The overall contribution extends beyond that of previously studied intragenic SNPs (C3435T and G2677T SNP). Fine localisation of potential variant(s) responsible for this association and functional work are now necessary.
1
Liver posters
143 FATIGUE IN PRIMARY BILIARY CIRRHOSIS IS ASSOCIATED WITH SYMPTOMS OF AUTONOMIC DYSFUNCTION
J. L. Newton, N. Bhala, J. A. Burt, D. E. J. Jones.Centre for Liver Research, University of Newcastle, UK
Background: Fatigue is the severest symptom experienced by those with primary biliary cirrhosis (PBC). The pathogenesis of fatigue is unknown although recent work by our group suggests it is associated with autonomic dysfunction (AD). Previous studies in those with cirrhotic liver disease have shown AD occurs frequently, it is however generally not considered in the clinical management of patients. In a large cohort of well characterised patients with PBC, we investigate whether symptoms commonly described by patients with AD are seen more frequently in patients with the fatigue associated with PBC.
Methods: Patients with definite or probable PBC were recruited via the PBC patients support group. All patients were asked to complete symptom questionnaires to determine the prevalence of postural dizziness, blackouts, and falls. Fatigue was determined using the PBC specific quality of life tool, the PBC-40. In this group, median PBC-40 fatigue domain score was 30. Those with scores >30 were the “fatigued” group, scores ⩽30 were the “non-fatigued” group.
Results: 137 PBC patients completed the questionnaires. 69 patients were non-fatigued (PBC-40 fatigue domain score ⩽30) and 68 fatigued (>30). There were no significant differences between the two groups in age, personal or family history of cardiovascular or cerebrovascular disease, or disease stage. The fatigued group complained of autonomic symptoms of dizziness significantly more frequently than the non-fatigued group (p<0.0001), with 9/10 of the most fatigued complaining of dizziness and 0/10 least fatigued. There was no significant difference between the prevalence of falls or blackouts, but the prevalence of chest pain almost reached significance (p = 0.059).
Conclusion: If AD does play a part in the fatigue of PBC an increased prevalence of symptoms associated with AD would be expected. This study confirms that fatigue in PBC is associated with symptoms characteristic of AD. We would suggest that AD in PBC is not a benign condition and further studies examining the role of AD in fatigue are required.
144 THE PORTAL CIRCULATION HAS THE LOWEST RATIO OF ACYLATED/TOTAL GHRELIN IN HUMANS
M. Mottershead, L. Wong, H. Randeva, C. U. Nwokolo.Department of Gastroenterology, University Hospital, Coventry, UK
Objective: Ghrelin, a polypeptide produced by specialised gastric neuroendocrine cells is present in plasma in acylated (active) and unacylated (inactive) forms. The liver could alter the dynamics of ghrelin as it passes from the portal to the systemic circulation where it is involved in the regulation of body composition.
Methods: Blood was sampled simultaneously from portal, peripheral, central venous, and arterial sites in patients (n = 10) undergoing surgery for colon cancer or inflammatory bowel disease. Aprotonin was added, plasma separated and stored at −20°C. Acylated and total ghrelin were assayed in one batch. Total ghrelin is the sum of acylated and unacylated forms.
Results: Median total ghrelin concentration was 1089 pg/ml in the portal compartment and this was significantly higher than in the peripheral blood (921 pg/ml), p = 0.01 with similar trends observed in the central venous (984 pg/ml) and arterial (886 pg/ml) compartment. In the portal compartment, the ratio of acylated/total ghrelin was 4%. In contrast this ratio was 6% in the other three systemic compartments representing a 50% increase in the acylated form.
Conclusions: The portal circulation has the lowest concentration of unacylated ghrelin and the highest concentration of the total form. It is therefore likely that the liver modifies the dynamics of ghrelin by increasing the proportion of acylated and therefore bioactive ghrelin present in the systemic circulation. Further studies are needed to determine the biological significance of this process and whether it is compromised in liver disease.
145 THE INCIDENCE, CLINCAL PRESENTATION, AND MORTALITY ASSOCIATED WITH SPONTANEOUS BACTERIAL PERITONITIS IN A UK TEACHING HOSPITAL
M. J. Brookes, H. Douis, P. G. Wilson.Gastroenterology Unit, City Hospital, Dudley Road, Birmingham, UK
Background: Spontaneous bacterial peritonitis (SBP) is recognised to be one of the major causes of bacterial infections in patients with liver cirrhosis. Bacterial infection in cirrhosis is associated with a high mortality rate. Early diagnosis and treatment is therefore essential. The aim of this audit was to assess the incidence, diagnosis, and management of SBP and its associated mortality rate in a UK teaching hospital.
Methods: Retrospective review of ascites samples over one year. Demographic data, aetiology of cirrhosis, Child’s classification, and clinical presentation were recorded. Ascites and serum laboratory variables at presentation were reviewed. Mortality rates at 4 weeks and 3 months were calculated.
Results: 106 patients underwent ascitic sampling. 146 ascites samples were analysed, (1.37 per patient; range 1–12). Mean (standard deviation) age at presentation was 57.3 years (SD 14.6), with a male predominance (79.4%). 21% of samples revealed evidence of SBP (in accordance with the international ascites club definition). SBP was associated with high serum CRP (p = 0.002), ascites albumin (p = 0.03), and serum ascites albumin gradient (SAAG) <11 (p = 0.001). Serum bilirubin, prothrombin time, renal function, and white cell count did not significantly differ between patients with SBP and those with no evidence of SBP. The rate of upper gastrointestinal haemorrhage, fever, and abdominal pain were the same for both groups. Four week mortality was 48.4% in the SBP group and 35.6% in those with no evidence SBP (p = 0.001). However 3 month mortality was 58.1% in the SBP group and 53% in those with no evidence of SBP (p = NS)
Conclusions: Spontaneous bacterial peritonitis rates are similar to internationally published data. Spontaneous bacterial peritonitis was associated with high serum CRP, a SAAG of <11, and a higher 4 week mortality rate than patients with no evidence of SBP.
146 LIVER FUNCTION TEST PATTERNS IN OBSTRUCTIVE JAUNDICE
J. O. Hayat, C. J. Loew, K. N. Asrress, A. S. McIntyre, D. A. Gorard.Wycombe Hospital, High Wycombe, HP11 2TT, UK
Background: Obstructive jaundice is believed to cause greater abnormalities of alkaline phosphatase (Alk P) than aspartate transaminase (AST). We have compared liver function test (LFT) patterns in obstructive jaundice patients undergoing ERCP for malignant strictures and stones.
Methods: 207 (105 male) obstructive jaundice patients having ERCP were divided into 69 with a malignant biliary stricture, 97 with a common bile duct (CBD) stone and 41 with a clear cbd but whose recent resolving jaundice, CBD dilatation and gallbladder stones suggested recent stone passage. LFTs and enzyme ratios (value/upper limit of normal) immediately before ERCP, at highest bilirubin and during acute pain bouts (severe enough to warrant hospitalisation) were compared.
Results: See table. The AST ratio/Alk P ratio for stone patients was 1.13 (1.3) and for stricture patients was 0.83 (0.6), p = 0.06. The highest bilirubin recorded in stricture patients, 294 (155), was greater p<0.0001 than the highest bilirubin in patients with cbd stones, 92 (76), and presumed recent passed CBD stones, 108 (75). Severe pain episodes in stone and recent stone patients were accompanied by higher levels of bilirubin 80 (54) v 53 (53), p<0.0001, and AST, 276 (213) v 108 (117), p<0.00001 but similar Alk P levels 292 (190) v 265 (203), compared with levels for the same patients at the time of ERCP.
Abstract 146 Pre-ERCP LFTs, as mean (SD)
In stone and presumed stone patients, when the bilirubin was at its highest, the AST ratio/Alk P ratio of 2.37 (3.2) was much greater than the AST ratio/Alk P ratio of 1.13 (1.3) at the time of ERCP, p<0.001.
Conclusion: Although Alk P rises more than AST in obstructive jaundice due to strictures, the AST rise in cbd stone disease equals the Alk P rise and exceeds it at times of maximum jaundice and during pain.
147 INTRAVENOUS GLYCINE AMELIORATES THE EARLY PHASE OF LIVER WARM ISCHAEMIA REPERFUSION INJURY IN A RABBIT ANIMAL MODEL
H. Sheth, T. Hafez, G. Glantzounis, K. M. Sales, A. Seifalian, B. Fuller, B. R. Davidson.University Department of Surgery, Royal Free and University College Medical School, Royal Free Hospital, London, UK
Background: Liver ischaemia reperfusion injury (IRI) is a major complication of liver transplantation. Cytokine release by activated Kuppfer cells (KC) play a central role in this inflammatory response. Glycine, a non-essential amino acid, may protect against liver IRI by inhibiting KC activity.
Materials and Methods: A rabbit model of hepatic lobar warm ischaemia reperfusion (I/R) was used. Sham group (n = 6) underwent laparotomy alone for 7 hours. I/R group (n = 6) underwent 60 minutes of left and median lobe inflow occlusion and 6 hours of reperfusion. Glycine+I/R group (n = 6) underwent a similar procedure after receiving glycine 5 mg/kg intravenously. Systemic haemodynamics, bile flow, portal flow, hepatic microcirculation (laser Doppler flowmeter), intracellular tissue oxygenation (near infrared spectroscopy), serum TNFα, IL-8, AST, and ALT were measured at 1, 2, 4, and 6 hours post-ischaemia.
Results: Systemic haemodynamic parameters remained stable in all groups throughout. On reperfusion, glycine+I/R group demonstrated increased bile flow (145.0 (11.4) v 108.3 (28.2) μl/min/gm, p<0.05), portal blood flow (95.6 (18.6) v 62.5 (19.3) ml/min, p<0.001), hepatic microcirculation (220.6 (25.0) v 151.6 (46.0) Flux units, p<0.05) and hepatic intracellular tissue oxygenation (−13.8 (6.7) v −25.5 (7.7) Δ units, p<0.05) compared to I/R group. Serum TNFα was significantly reduced in glycine+I/R group as compared to I/R group at 1 (187 (118) pg/ml v 283 (99) pg/ml; p<0.01), 2 (203 (111) pg/ml v 267 (58) pg/ml; p<0.01) and 4 hours (198 (96) pg/ml v 330 (116) pg/ml; p<0.01). Serum AST, ALT, and IL-8 were significantly less at 1, 2, 4, and 6 hours in glycine+I/R group as compared with I/R group (p<0.05).
Conclusions: Glycine improved bile flow, portal blood flow, hepatic microcirculation, and suppressed cytokine expression in this animal model and hence may provide a novel therapeutic modality.
148 DOES PERIOPERATIVE N-ACEYLCYSTEINE PREVENT ISCHAEMIA REPERFUSION INJURY DURING LIVER RESECTION?: A PROSPECTIVELY RANDOMISED DOUBLE BLIND CLINICAL TRIAL
H. Sheth1, G. Glantzounis1, T. Hafez1, A. Quaglia2, J. Duncan3, B. R. Davidson1.1University department of Surgery, 2University Department of Pathology, 3University Department of Anaesthesia, Royal free Hospital, Royal Free and University College Medical School, Pond Street, London NW3 2QG, UK
Introduction: Liver ischemia reperfusion injury (IRI) is a major complication of liver resection and transplantation. Accumulation of toxic oxidative radicals, cytokines, upregulated adhesion molecules and depletion of intracellular glutathione stores affect postoperative hepatocellular function. N-acetylcysteine (NAC), an antioxidant and hepatic glutathione precursor may prevent this injury.
Methods: Forty three patients were randomised to a NAC group (NACG) to receive NAC as an IV infusion (150 mg/kg in 250 ml of 5% dextrose loading dose, followed by 50 mg/kg in 500 ml of 5% dextrose over 4 hours and 50 mg/kg in 500 ml of 5% dextrose over 8 hours) or a placebo group (PG) which received equivalent volume of 5% dextrose. Blood samples for FBC, U/E, and LFT were taken at laparotomy, following liver mobilisation and after parenchymal resection. Trucut liver biopsies were taken before liver mobilisation and after parenchymal resection, stained for ICAM-1 by immunohistochemistry, and assessed semiquantitatively by blinded pathologists.
Results: Twelve patients were excluded due to inoperable tumours at laparotomy. Of the 31 patients, 15 received NAC and 16 were randomised to PG. There were no differences in age, sex, case distribution, and blood loss or transfusion requirements between the groups. ALT was significantly less in the NACG (p = 0.011) after resection while ALP was significantly higher in the NACG (p = 0.042). ICAM-1 expression was upregulated in 6/16 patients (38%) in the PG and in 3/15 patients (20%) in the NACG. ICAM-1 was downregulated in 1/15 patient in the NACG and none in the PG.
Conclusions: Perioperative NAC improved parenchymal liver function and decreased Icam-1 expression following resection.
149 CHOLEDOCHAL CYSTS IN ADULTS
A. T. George, (introduced by Dr K. George, Consultant Gastroenterologist, Torbay Hospital, Torquay, UK), M. Jacob, M. Anandakumar, K. V. Vijayan, A. Kalam, Subhlal, A. P. Kuruvilla.Medical College, Trivandrum, Kerala, India
Introduction: Choledochal cysts are usually a disease of children but can present late in adulthood. Patients may be asymptomatic or may present with repeated infection but the feared complication is the development of malignancy in these cysts.
Methods: A retrospective study of 35 cases of adult choledochal cysts that were treated in our hospital between January 1989 and December 2003 was done. The clinical presentations, investigative findings, management options exercised, and the mortality patterns of those with and without malignancy were assessed.
Results: The various parameters of 31 patients (Group A) who had no evidence of malignancy were compared with those of four patients (Group B) in whom choledochal cysts were complicated by malignancy. Older age of presentation (p = 0.001), significant weight loss (p = 0.008), higher levels of bilirubin (p = 0.044), and absence of calculi in the biliary tree (p = o.017) were found to be associated more with group B than with group A. Complete excision of the cyst and Roux-en-Y hepaticojejunostomy was done in 31 patients—one had a concomitant hemihepatectomy for intrahepatic extension of the cyst. Three patients had an access loop constructed. Of the four patients in group B, two patients were diagnosed preoperatively while the other two were diagnosed only on postoperative histopathological examination. The latter two patients are alive, asymptomatic, and on regular follow up. In a mean follow up of 60 months in groups, three cases of recurrent cholangitis and one case of anastamotic stricture—which required reanastamosis—were observed.
Conclusions: Biliary tract malignancy complicating choledochal cysts should be suspected in those with an older age of presentation, with a history of significant weight loss and increasing levels of bilirubin in spite of imaging showing an absence of calculi in the hepatobiliary system. Complete excision of the cyst with Roux-en-Y hepaticojejunostomy is the present treatment of choice for uncomplicated choledochal cysts and can be done with a low long term complication rate.
150 A TWO YEAR PROSPECTIVE AUDIT OF PERCUTANEOUS LIVER BIOPSIES
S. Sen, H. Dallal, P. S. Phull.Gastrointestinal & Liver Service, Aberdeen Royal Infirmary, Aberdeen, UK
Background: Percutaneous liver biopsy is one of the more important tools used in the diagnosis of hepatic diseases. This audit evaluated the failure rates (inability to obtain sufficient tissue) and complication rates of percutaneous liver biopsies.
Methods: All percutaneous liver biopsies performed in the gastroenterology department at our institution were prospectively audited over a two year period. A standardised proforma was used to collect the data.
Results: A total of 245 biopsies were performed on 232 patients over the audit period. Of these, 144 were blind and 101 were radiologically guided. Forty four biopsies were performed as day cases. The commonest indications for liver biopsies were abnormal liver functions in 87 cases (36%), followed by hepatitis C infection in 61 cases (25%). Mean passes attempted per patient was 1.32 (SD 0.04). Complications occurred in 21 procedures (8.9%), of which only three were serious (1.3%). Sufficient tissue could not be obtained in 18 cases (failure rate 7.3%). A significantly greater number of passes were attempted in radiologically guided (1.49 (SD 0.06)) versus blind procedures (1.22 (SD 0.04)) (p = 0.0002), though complication rates were similar for both (6.9% v 10.4% respectively, p = 0.5). Serious complications occurred in only 1% of radiologically guided and 1.4% of blind biopsies (p = 0.8). Moreover, failure rates were significantly lower with radiologically guided biopsies (3/101, 3%) compared with blind procedures (15/144, 10.4%) (p = 0.04). Of the 44 day-case biopsies, complications occurred in only two cases (4.5%), none being serious. However, the failure rate was higher (7/44, 16%) compared to non-day-case biopsies (9/201, 4.5%) (p = 0.01).
Conclusion: Percutaneous liver biopsy is a safe procedure with a high success rate. Radiologically guided procedures have a higher success rate but a similar complication rate compared to blind procedures. Day case biopsies in selected patients have a similar complication rate but lower success rate compared to non-day-case biopsies.
151 DO WE DRINK MORE THAN OUR PATIENTS?
L. Williams, D. Trivedi, A. Chunfat, R. Ratcliffe, R. Alcolado.Royal Glamorgan Hospital, Ynysymaerdy, Llantrisant CF72 8XR, UK
Introduction: Alcohol excess represents a worldwide health issue. Medical students and doctors are at high risk of alcohol abuse. 20% of medical students drink more than the national recommendations and one in 15 doctors are said to be alcohol dependent.
Methods: The AUDIT questionnaire was used to determine alcohol consumption and risk status. A prospective study was carried out in December 2003 when anonymous questionnaire were given to acute medical patients, and then to medical students and doctors in March 2004.
Results: Fifty two students (mean age 23 years) and 68 doctors (mean age 34 years) were included. 57% of the medics were male. Of the 59 patients included, 63% were male (mean age 59 years).
Female medics had higher AUDIT scores then than male medics (6.9 v 5.99), but female patients scored less than male patients (5.3 v 8.3). 37% of male medics were high risk drinkers compared with 43% of male patients. 37% of female medics were high risk drinkers compared with 2% of female patients. No sex differences in the abstinence rates were evident, when comparing patients and medics. 54% of all students were high risk drinkers, 23% of doctors and 34% of patients. 43% of the high risk drinking medics were female, compared with 20% of patients. AUDIT scores: students 9.2, doctors 4.1, patients 7.2 (but patients <25 years scored 8.5). AUDIT scores fell as age increased. Scores fell as hospital grade increased (from third year students to SpR/consultant). Muslims/Sikhs/Hindus and married medics scored low. Written documentation revealed only 50% of the high risk drinkers.
Conclusion: The AUDIT questionnaire is easy to use and determines those at risk of developing alcohol related illness. Doctors drink less than patients, but medical students drink more. Female medics were more likely to be high risk drinkers than female patients/male medics. Patients at high risk of alcohol abuse were not reliably identified in case notes.
152 A SNAPSHOT OF A&E ATTENDEES IN A DISTRICT GENERAL HOSPITAL: HIGHLIGHTING THE BURDEN OF ALCOHOL ABUSE
L. Williams, J. Hutchinson, D. Moody-Jones, R. Alcolado.Royal Glamorgan Hospital, Ynysymaerdy, Llantrisant CF72 8XR, UK
Introduction: 35% of the A&E budget is spent on alcohol related injuries, 2–40% of all attendances are because of alcohol misuse. In the Royal Glamorgan Hospital 2003, this was recorded as 0.69%.
Method: A prospective study was performed between January and February 2004. A questionnaire was distributed to the “walking wounded” patients in A&E. Alcohol abuse was determined using a 5 shot scoring system (CAGE and AUDIT).
Results: 282 questionnaires were completed—58.5% male, 79% between 18–54 years, 22% unemployed, 13.5% students. 17.7% attendances were attributed to alcohol (alleged assault 36%, accidental trauma 24%, acute intoxication 12%), increasing at weekends. 20% of all male attendances were attributed to alcohol misuse. This was most commonly seen in the unemployed cohort, 35.5% compared with 12.4% in the employed.
A third of all A&E attendees were hazardous drinkers (39.4% of men, 24.8% of women). 31.5% of hazardous drinkers attended for alcohol related reasons compared to 9% of non-hazardous drinkers. 5.3% admitted to drug abuse (most commonly cannabis), 60% of these were hazardous drinkers. 32.6% of attendees smoked (M:F 2:1), increasing in hazardous drinkers to 45.7%.
Only 38% of alcohol related causes were documented. Only 76.6% of hazardous drinkers had alcohol histories in the case notes.
Conclusion: 17.7% of A&E attendances were attributed to alcohol misuse (assault, accidental trauma; male, unemployed). A simple alcohol questionnaire is capable of identifying heavy drinkers. 33.3% of all attendees were heavy drinkers, predominantly men, and attending for alcohol related reasons. An association of alcohol misuse and drug abuse was seen.
153 AUDIT OF ACUTE VARICEAL BLEEDING IN A TERTIARY REFERRAL CENTRE
J. Parr, M. Hudson.Liver Unit, Freeman Hospital, Newcastle upon Tyne, NE3 4EU, UK
Introduction: Acute variceal bleeding (AVB) carries a high mortality. However, there is recent evidence to suggest this mortality is falling.
Aims and Methods: To review the management of AVB in a tertiary referral unit and determine outcome. We conducted a retrospective audit of 59 AVB episodes referred to our unit between 1 January 2001 and 31 January 2002.
Results: 59 consecutive bleeding episodes were identified in 50 patients. The mean age was 55.2 years (range 32–79). Fourteen patients presented with their first AVB, 24 admissions were direct to our unit. Thirty five admissions were tertiary referrals for unstable AVB. The Child’s Grade included 4 A, 26 B, and 20 C cirrhotic patients. The average length of stay was 12.9 days(range 2–36), 93% (55) of patients underwent endoscopy within 24 hours of admission. At endoscopy oesophageal varices (n = 32), gastric varices (n = 8), and both (n = 10) were confirmed. In 36 (61%) of 59 admissions the varices were actively bleeding at endoscopy. 17 (47%) of these patients rebled during that admission. Seven (19%) of these 36 patients died in hospital during that admission. Therapeutic intervention at endoscopy included sclerotherapy (n = 25), banding (n = 5), both (n = 1), histoacryl (n = 3). One patient required surgery. Of the 50 patients admitted, 17 proceded to TIPSS, 15 being alive at 1 year. In 57 of 59 AVB episodes vasoactive agents were used. All patients received antibiotic prophylaxis. Rebleeding complicated 22 (37%) of 59 admissions. The overall in hospital mortality was 22% (n = 11). Of the 11 patients who died, eight (73%) were Child’s C, and three (27%) B. The overall mortality in the 20 Child C patients was 40%.There were no early deaths (within 6 weeks) of discharge.
Conclusions: The improved mortality for AVB is confirmed within the tertiary referral setting. This study emphasises the importance of early therapeutic endoscopy with the option of TIPSS, but highlights the significance of active VB at the time of endoscopy in those with advanced liver disease as a predictor of a poor outcome.
154 VIRAL KINETICS IN PATIENTS TREATED WITH PEGYLATED INTERFERON-α2B FOR RECURRENT HEPATITIS C AFTER ORTHOTOPIC LIVER TRANSPLANTATION
M. Heydtmann, D. A. Freshwater, T. Dudley, S. Palmer, S. Hübscher, D. Mutimer.Liver Unit, Queen Elizabeth Hospital, Birmingham, B15 2TH, UK
Background: Recurrent hepatitis C is universal in patients receiving a liver transplant for chronic hepatitis C and leads to inflammation and cirrhosis in many cases. In this clinical setting viral kinetics are not known and antiviral treatment is still experimental.
Methods: Patients transplanted for chronic hepatitis C who met the inclusion criteria of hepatic fibrosis due to recurrent disease and no major comorbidities were offered treatment with once weekly pegylated interferon-α2b 1.5 μg/kg body weight. Viral genotype was determined and viral load was measured frequently in the first 48 hours of treatment initiation. The half life of the virus after treatment begins which reflects viral clearance rate was calculated using the steepest decline of viral load in the first 48 hours.
Results: Fourteen patients fulfilled the inclusion criteria (six genotype 1, five genotype 3, and three genotype 2). The pretreatment viral load was not significantly different between patients with genotype 1 (mean 1.66×106) v genotypes 2 and 3 (mean 3.85×106).
The viral half life was between 1.13 to over 20 hours for all patients with a median of 2.6 hours for genotypes 2 and 3 patients and 7.8 hours for genotype 1 patients, a statistically significant difference (p = 0.02, Mann-Whitney U). End of treatment response was observed in five patients: three genotype 3 patients and two genotype 1 patients. Sustained virological response was observed in a patient with genotype 1 (viral half life: 5.65 hours) and a patient with genotype 3 (viral half life: 1.41 hours). From this cohort there were no early predictors of end of treatment response or sustained virological response.
Conclusion: In the population of patients with recurrent hepatitis C after liver transplantation antiviral treatment leads to a rapid decline of viral load and the viral clearance rate is comparable to non-transplanted HCV patients. As in non-transplanted patients genotypes non 1 are associated with a shorter viral half life at treatment initiation.
155 HEPATITIS C: A WEIGHTY ECONOMIC PROBLEM?
R. L. Shenderey, R. Harrison, D. A. Burke.Cumberland Infirmary, North Cumbria Acute Hospitals Trust, Carlisle
Introduction: Combination therapy with Pegylated interferon and Ribavarin is currently recommended for the treatment of hepatitis C. Peginterferon α-2a is proposed at a fixed dose regime of 180 μg/week and Peginterferon α-2b as a variable dose dependant on the patient’s weight of 1.5 μg/kg/week. Ribavarin dosing is dependant on patient’s weight and genotype.
Aim: To compare the potential costs of using different Pegylated interferon/Ribavarin regimens based on the proportions of hepatitis C virus genotype and presenting patient weight in the local population.
Method: A retrospective study of PCR positive patients known to our service in North Cumbria, to determine the proportion of different genotypes and patients initial weight. Potential drug costings (list price excluding VAT) were calculated based on 24 weeks combination therapy for genotypes 2 and 3 and 48 weeks for other genotypes. We used an estimated 20% discontinuation rate for those with genotypes 1 and 4 who showed no early virological response at 12 weeks.
Results: Seventy nine hepatitis C PCR positive and genotyped patients attending our service for consideration of treatment were identified: 60 male; 19 female, median age 39 years (range 19–68). Weight 73 kg (median) range 43–163 kg. Thirty two patients were found to be genotype 1 or 4, 47 genotype 2 or 3. Costs of treating: Peginterferon α-2b £407 171 using vials, £447 888 using prefilled pens, Ribavarin (Rebetol) £299 778—total cost £706 949 (vials) or £747 666 (pens). Peginterferon α-2a £345 571 and Ribavarin (Copegus) £242 274—total £587 845
Conclusions: Currently there are no head to head trials of these treatment regimens, but, assuming equal efficacy of the two treatments, significant cost savings could be made in our patient group by adopting a fixed dose Pegylated interferon regimen. Local proportions of genotype and weights should be included in the planning of hepatitis C services. This could have large financial implications if implemented across the UK.
156 DOES COEXISTENT HEPATITIS C INFECTION ALTER THE OUTCOME OF ACUTE ALCOHOLIC HEPATITIS?
M. McMahon, A. J. Stanley, A. J. Morris, E. H. Forrest.Department of Gastroenterology, Glasgow Royal Infirmary, Castle Street, Glasgow G4 OSF, UK
Introduction: Acute alcoholic hepatitis (AAH) remains a frequent cause of admission with a high morbidity and mortality. Hepatitis C (HCV) infection may coexist with alcoholic liver disease. However, previous studies of AAH have excluded those patients with evidence of viral hepatitis and so little is known of the natural history of this combination of pathologies. Our clinical experience led us to believe that these patients may have a worse prognosis.
Aims: We aimed to assess the 28 day outcome of patients with AAH and HCV infection and compare this to the outcome of patients with AAH alone.
Methods: Patients with a clinical diagnosis of AAH and HCV were identified retrospectively. From their medical records clinical and laboratory data were collected and the modified discriminant function (mDF) and Glasgow Alcoholic Hepatitis Score (GAHS) were calculated. These results were then compared with an historical cohort of patients with AAH who had HCV excluded (n = 241).
Results: Data was complete for 34 patients. Patients with a combination of both AAH and HCV were younger (38 years v 48 years, p<0.001). In addition, their transaminases levels were higher (p<0.001 for both AST and ALT). Twenty four patients had a mDF ⩾32, and five patients had a GAHS ⩾9. Overall there were only three deaths in the AAH/HCV group. The table compares the 28 day mortality of AAH with and without HCV.
Abstract 156
Conclusions: Short term mortality in patients with the combination of AAH and HCV infection appears to be no worse than patients with AAH alone. The GAHS appears to be a better predictor of outcome for patients with AAH and coexistent HCV infection, as it is for AAH alone.
157 TUMOUR LYMPHOCYTIC INFILTRATE AND RECURRENCE OF HEPATOCELLULAR CARCINOMA FOLLOWING LIVER TRANSPLANTATION: A RELATION TO PHENOTYPE
E. Unitt1, A. Marshall1, S. Rushbrook1, S. Davies2, S. Vowler3, L. Morris4, N. Coleman4, G. M. Alexander1.Departments of 1Medicine and 2Histopathology, Addenbrooke’s Hospital, Cambridge; 3Centre for Applied Medical Statistics, Department of Public Health and Primary Care, Institute of Public Health, Cambridge; 4MRC Cancer Cell Unit, Hutchinson Building, Cambridge
Background: Hepatocellular carcinoma (HCC) is a common malignancy with a dismal prognosis. Liver transplantation is the most effective treatment for highly selected patients but tumour recurrence remains an important cause of mortality. Vascular invasion, tumour grade and tumour size are independent predictors of HCC recurrence and death following transplantation. Tumour immunity is related to prognosis for certain malignancies, but there are few data on the relation between lymphocytic infiltration in HCC and outcome nor with regard to HCC recurrence following liver transplantation.
Methods: The tumour CD4+, CD8+, and Foxp3+ lymphocyte infiltrate was assessed by immunohistochemistry in explant tissue of 69 patients who underwent liver transplantation for HCC between 1987 and 2001 with a known outcome. The data were analysed according to HCC recurrence and known correlates of outcome, including histology.
Results: Tumour size, vascular invasion, and the “Milan criteria” all predicted tumour recurrence (p = 0.035, p = 0.003, and p = 0.06 respectively). In addition, a CD4: CD8 ratio >1 was associated with a reduced risk of tumour recurrence (p = 0.003). Increased lymphocytic infiltration was associated with lower tumour grade (p = 0.001), but not with tumour recurrence. The presence of Foxp3+ lymphocytes was associated with vascular invasion (p = 0.04).
Conclusion: The data support the hypothesis that immune responses are important in HCC and that the phenotype of infiltrating lymphocytes is informative regarding prognosis. In particular the presence of Foxp3+ T-regulatory lymphocytes was associated with a poor outcome.
158 CD8+ LYMPHOCYTES INFILTRATING HEPATOCELLULAR CARCINOMA ARE IMMATURE AND SUPPRESSED BY CD4+CD25+ REGULATORY T CELLS
E. Unitt1, S. Rushbrook1, N. Coleman2, G. J. M. Alexander1.1Department of Medicine, Addenbrooke’s Hospital, Cambridge; 2MRC Cancer Cell Unit, Hutchinson Building, Cambridge, UK
Introduction: CD8+ T cells are probably important in tumour immunity. Antigen experienced, or memory CD8+ T cells (45RO+) can be categorised as central memory cells (CD27+CD28+CCR7+), early effector cells (CD27+CD28+CCR7-), and late effector cells (CD27-CD28-CCR7-) with cytotoxic capacity and interferon γ production limited to the latter group. We hypothesised that CD8 cells infiltrating HCC would have impaired maturation and/or cytotoxic potential as a result of regulation by CD4+CD25+ T regulatory cells (T-regs).
Methods: Phenotype and cytotoxic potential of infiltrating CD8+ T cells in patients undergoing liver transplantation for HCC were assessed using a combination of flow cytometry and immunohistochemistry. CD25+ T-regs were freshly isolated from HCC and used in proliferation assays with autologous CD8+ T cells. IFN γ ELISPOT was used to assess peripheral CD8 T cell responses to recognised tumour peptides (AFP and MAGE) pre and post depletion of T-regs in HLA-A2+ patients.
Results: Infiltrating CD8+ T cells have a predominantly central memory phenotype with low perforin expression (13% of CD8+ T cells, range 5–21%). On immunohistochemistry, <5% of CD8+ cells infiltrating HCC expressed intracellular perforin and Granzyme B. In co-culture experiments, HCC derived T-regs suppressed both proliferation and perforin expression of autologous circulating CD8+ T-cells upon non-specific stimulation. Prior depletion of circulating CD25+ T-cells enhanced CD8+ tumour specific responses to AFP and MAGE peptides.
Conclusions: CD8+ T-cells infiltrating HCC have reduced cytotoxic capacity. T-regs within HCC have the capacity to inhibit proliferation and perforin expression in CD8 cells. We suggest that infiltrating CD8+ T cells in HCC have an impaired capacity for anti-tumour responses. One explanation for this could be suppression by infiltrating CD4+CD25+ cells. Prior T-reg depletion may enhance the effects of immunotherapy involving CD8+ cells as effectors.
159 ALCOHOLIC LIVER DISEASE: ANOTHER DISEASE OF SOCIAL DEPRIVATION?
C. Welhengama, J. Jones, M. P. Bradley, R. J. Peck1, J. Skinner2, C. Price2, D. Gleeson.Liver Unit and 1Department of Radiology, Sheffield Teaching Hospitals and 2West Sheffield Primary Care Trust, Sheffield, UK
Background: It is unclear why only 10–20% of heavy drinkers develop serious ALD.
Aim: Assessment of association between ALD and social deprivation.
Subjects: (1) Heavy drinking (>60 U/wk (M) or 40 U/wk (F) for >5 years) Sheffield residents (a) presenting to hospital with decompensated ALD (patients) and (b) with no clinical, laboratory, or ultrasound evidence of serious liver disease (controls); these controls divided into healthcare seeking (recruited while presenting to hospital or primary care) and non-healthcare seeking (volunteers recruited by advertisement). (2) Subjects from the Sheffield Health and Exercise (SHEX) Survey of 1686 randomly selected Sheffield residents, who reported consuming >40 U alcohol over the previous week.
Methods: Townsend, Jarman, and Index of Multiple Deprivation (IMD) scores calculated from postcodes of home residences at time of presentation/interview.
Results: See table. Age and lifetime alcohol consumption (unavailable in SHEX subjects) did not differ between the other groups. The patient-control differences remained significant when healthcare seekers with and without other alcohol-related presentations were considered separately.
Abstract 159
Conclusions: Heavy drinkers seeking healthcare constitute a socially deprived group; of these, patients with decompensated ALD are more socially deprived than those without liver disease, thus ALD may itself be associated with social deprivation.
160 CONFOCAL MICROSCOPY FOR CD25 AND MCM-2: A WAY TO DISTINGUISH BETWEEN ACUTE CELLULAR REJECTION AND RECURRENT ALLOGRAFT HEPATITIS C INFECTION (A PILOT STUDY)
E. Unitt1, A. Marshall1, L. Morris2, N. Coleman2, G. J. M. Alexander1.1Department of Medicine, Addenbrooke’s Hospital, Cambridge; 2MRC Cancer Cell Unit, Hutchinson Building, Cambridge, UK
Background: Hepatitis C virus (HCV) infection with cirrhosis is a leading indication for liver transplantation in the UK. Recurrence of infection following liver transplantation is almost universal. Multiple episodes of acute cellular rejection are associated with higher HCV recurrence rates and treatment for acute cellular rejection may itself accelerate HCV infection and severity. However, the histological appearances of acute cellular rejection (AR) and HCV recurrence cannot always be distinguished with confidence. We have previously shown that lymphocytes in the portal tracts of HCV infected liver are hypoproliferative, possibly due to infiltrating CD25+ T regulatory cells. We hypothesised that the lymphocytic infiltrate seen in AR and recurrent allograft infection would differ in the expressions of CD25 (an activation marker and a marker of T regulatory cell) and Mcm-2 (a pan cell-cycle marker, positive in activated lymphocytes, but negative in T regulatory lymphocytes), and may be a useful way to distinguish between them.
Methods: We used confocal microscopy for CD25 and Mcm-2 to assess five patients with a confirmed histological diagnosis of AR (two of whom were transplanted for HCV infection) and five patients with recurrent allograft HCV infection.
Results: Lymphocytes infiltrating the portal tract in AR were positive for both CD25 and Mcm-2 in >80%. In contrast, <5% lymphocytes in recurrent allograft HCV infection coexpressed these markers.
Conclusion: The results of this pilot study suggest that portal tract lymphocytes in acute rejection and recurrent allograft HCV infection comprise different populations. Confocal microscopy for CD25 and Mcm-2 may be useful in diagnosing acute rejection in patients transplanted for HCV. Further prospective studies are necessary to validate our findings.
161 WHOLE BODY ENDOGENOUS NITRIC OXIDE PRODUCTION IN PATIENTS WITH DECOMPENSATED LIVER DISEASE
D. A. Elphick1, E. A. G. Demoncheaux1, M. B. Dürner2, G. E. Higgins2, D. Crowther2, E. J. Williams1, T. W. Higenbottam1, D. Gleeson1.1Royal Hallamshire Hospital, 2Sheffield Hallam University, Sheffield, UK
Background: Increased nitric oxide (NO) production has been implicated in the pathogenesis of the hyperdynamic circulation found in patients with advanced liver disease. This may contribute to complications such as sodium and water retention and portal hypertension. Our aim was to determine nitric oxide synthase (NOS) dependent whole body NO production, by in vivo L-arginine to nitrite and nitrate conversion, in patients with decompensated liver disease.
Subjects and Methods: Ten patients with decompensated liver disease (Child-Pugh class B or C) were compared with 10 age and sex matched healthy controls. All patients had low systemic blood pressure indicating a hyperdynamic circulation (mean (SD) BP 102/65 (10/12)). All patients had ascites and all had varices (eight oesophageal, two at splenic hilum) indicating portal hypertension. Six had biopsy proven cirrhosis (four not biopsied) and alcohol was considered the sole aetiology for liver disease in all. Patients and controls had no evidence of bacterial infection, had no comorbidity, were abstinent from alcohol for at least 4 weeks, did not smoke, had no renal impairment and consumed a standardised low nitrate diet for the duration of the study. NOS dependent whole body NO production was assessed by giving an intravenous infusion of L-[15N]2-arginine (50 μmol/min for 30 minutes) and measuring isotopic urinary enrichment of 15N-nitrite and 15N-nitrate by ion chromatography coupled with mass spectrometry.
Results: There were no differences between patients with liver disease and controls with regard to: (a) 36 hour urinary excretion of 15N-nitrite plus 15N-nitrate (113.4 (38.1) v 118.0 (31.9) nmol/mmol creatinine), (b) 36 hour urinary 14N-nitrite plus 14N-nitrate (42.8 (13.6) v 62.5 (17.0) μmol/mmol creatinine), or (c) blood 14N-nitrite plus 14N-nitrate concentrations (122.6 (18.3) v 136.4 (22.7) μmol/l) (results shown as mean (SEM)).
Conclusions: Our results, in a well characterised set of patients, argue against greater basal NOS dependent whole body NO production in patients with decompensated liver disease.
162 CAUSES OF STEATOSIS IN CHRONIC HEPATITIS C INFECTION AND THE IMPACT OF STEATOSIS ON TREATMENT RESPONSE
C. Meaden1, R. F. McMahon2, T. W. Warnes1.1Department of Gastroenterology, Manchester Royal Infirmary M13 9WL; 2Department of Pathology, Manchester Royal Infirmary M13 9WL, UK
Background: Steatosis is a common finding in liver biopsy specimens from patients with chronic hepatitis C infection, in some studies it is present in up to 65% of cases. The significance of steatosis in chronic hepatitis C infection is that it may be associated with a more aggressive clinical course and worsening liver fibrosis.
Methods: Pretreatment liver biopsies from 102 patients chronically infected with hepatitis C were graded for steatosis by a single histopathologist. Of this group 41.18% (42/102) had no steatosis. Of the 58.82% (60/102) with steatosis 20.59% (21/102) had grade 1 steatosis, 32.35% (33/102) had grade 2, and 5.88% (6/102) had grade 3. 76 of these patients underwent a second liver biopsy immediately following treatment.
Results: In univariate analysis patients with steatosis tended to be older, heavier, have a higher BMI, and a higher viral load, but the only significant predictors of steatosis were a history of excessive alcohol consumption (>50 g/day) before treatment (p = 0.004) and having genotype 3 (p = 0.038). In multivariate analysis a past history of consuming more than 50 g/day of alcohol was the only significant predictor of steatosis on pretreatment biopsy (OR 4.18, p = 0.006). The presence of steatosis per se was not associated with a worse response to treatment (sustained response rate with steatosis and without steatosis was 19.57% and 14.29%, respectively p = 0.477). A striking finding was the difference in behaviour between the genotypes: genotype 3 had a significantly greater amount of steatosis before treatment compared to genotype 1 (genotype 3 v 1, p = 0.038, v 2 p = NS) and lost a significantly greater amount after treatment (genotype 3 v 1, p = 0.020 and v 2, p = 0.040).
Conclusions: The association of genotype 3 with steatosis and reversal of it with treatment suggests a causative role for this genotype in steatosis. The impact of alcohol consumption on steatosis in hepatitis C has not been widely reported and may reflect exclusion of such patients from studies and underestimates of alcohol consumption by patients.
163 DOES SMOKING AFFECT DISEASE PROGRESSION IN PRIMARY BILIARY CIRRHOSIS?
P. Tachtatzis, M. Thyssen, M. Jenkins, P. Gedling, R. Chapman.Department of Gastroenterology, John Radcliffe Hospital, Oxford, UK
Introduction: Primary biliary cirrhosis (PBC) is a disease of unknown aetiology. Current evidence suggests that there is a genetic susceptibility for the disease triggered by a variety of environmental factors. Previous data suggest that smoking is such a factor and that ever-smokers are overrepresented in patients with PBC.
Aim: To investigate whether cigarette smoking affects disease presentation and progression in PBC.
Methods: To study a group of patients with PBC and record disease associations, smoking, and alcohol habits. The severity of the disease at initial presentation was assessed using the Mayo Risk Score as an established predictor of survival. The rate of progression of disease was assessed over a mean of 5 years.
Questionnaires were sent to 105 patients with a diagnosis of PBC. The questionnaire requested details concerning smoking and alcohol habits, occupation, and associated diseases.
Results: Ninety five replies were received (90% response). Women comprised 89% of the group and men 11%. Mean age at presentation for women was 55 years and for men 64 years (p = 0.02). Commonest disease associations were 20% thyroid disease, 28% osteoarthritis, and 11% Sjogren’s syndrome. Twenty two patients (21%) were smokers, 37 patients (35%) were non-smokers, and 30 patients (28%) were ex-smokers. The mean Mayo score at presentation for smokers and non-smokers was similar (4.317, 4.372) and for ex-smokers it was significantly higher at 4.803 (p = 0.012). Over the period of follow up the rate of change of Mayo score was not affected by smoking habit (p = 0.149). Alcohol intake did not have any affect on either the Mayo Risk Score or subsequent survival.
Conclusion: We conclude that past smoking habit may be associated with a worse Mayo score and survival probability at presentation but does not affect rate of progression of disease.
164 IS IT POSSIBLE TO DIFFERENTIATE NON-ALCOHOLIC STEATOHEPATITIS FROM SIMPLE FATTY LIVER WITHOUT A LIVER BIOPSY?
A. H. Shenoy, J. M. Geraghty, D. James, S. Pugh, P. D. Thomas.Taunton and Somerset Hospital, Taunton, UK
Introduction: Liver biopsy is required to distinguish inflammatory/fibrotic liver disease from simple “fatty liver” in patients with non-alcoholic fatty liver disease (NAFLD). Serum markers such as procollagen III (PCIII) and hyaluronic acid (HA) have been used as a non-invasive test for liver fibrosis in patients receiving methotrexate.
Aim: To determine whether serum markers of fibrosis PCIII and HA can distinguish patients with non-alcoholic steatohepatitis/fibrosis from simple steatosis in patients with NAFLD.
Methods: Prospective cohort study. 29 patients presenting between June 2000 and April 2004 with NAFLD on liver histology underwent biometric and clinical assessment and blood assay for conventional liver function tests, ferritin, PCIII, and HA. A single histopathologist blinded to the results of PCIII and HA assays scored the liver biopsies for fatty change, inflammation, and fibrosis using a modified Ishak scoring system. Two groups with and without fibrosis and significant inflammation were identified and the levels of the biochemical markers compared.
Results: There were no significant differences in any of the biometric or biochemical markers between the groups with and without inflammation and/or fibrosis (see table—median (range) given). In particular, PCIII and HA levels did not differ (p>0.5).
Abstract 164
Procollagen III and hyaluronic acid levels significantly correlated (Spearman’s non-parametric correlation 0.59, p = 0.001). Liver fibrosis and total inflammatory scores also significantly correlated (0.63, p<0.01); but neither significantly correlated with PCIII or HA.
Conclusion: This study suggests that PCIII and HA cannot be used to distinguish inflammatory and/or fibrotic liver disease from simple steatosis in patients with NAFLD
165 REACTIVATION OF HERPES SIMPLEX VIRUS AFTER ORTHOTOPIC LIVER TRANSPLANTATION
W. J. H. Griffiths, T. G. Wreghitt1, G. J. Alexander.Department of Hepatology, 1Clinical Microbiology and Public Health Laboratory, Addenbrooke’s Hospital, Cambridge, CB2 2QQ, UK
Background: Reactivation of herpes simplex virus (HSV) after orthotopic liver transplantation has been reported but its incidence and clinical significance are unknown. The aims of this study were to determine whether HSV reactivation occurs during the initial period following liver transplantation, the clinical significance of this, and what predictive risk factors might be identified.
Methods: Twelve consecutive male patients awaiting orthotopic liver transplantation and who were positive for HSV antibody were enrolled after informed consent. HSV PCR was performed on mouth and penile swabs at the pre-transplant stage (all negative) and at days 5 and 10 post-transplant. Data were recorded regarding clinical evidence of HSV infection, degree of immunosuppression (duration of lymphopenia, use of supplemental high dose steroids), length of intensive care stay, and hospital admission and use of antiviral agents.
Results: Five out of twelve patients (42%) had evidence of oral reactivation after transplant. Four had HSV-1 and one HSV-2. Genital reactivation was not seen. Four patients were positive on day 5 with one remaining positive by day 10. The patient who became positive on day 10 had been readmitted to critical care on day 4. One patient had oral herpes (positive day 5) and was treated with aciclovir. Reactivation did not correlate with degree of immunosuppression but intensive care stay was longer in positive patients (mean 5.6 v 2 days, p>0.05). One patient received ganciclovir from day 1 and had HSV reactivation.
Conclusions: Oral HSV reactivation is common after liver transplantation although clinical significance appears low in this preliminary study. Critical care stay may be a risk factor and reactivation may occur despite ganciclovir. A larger study is underway to further clarify the significance of occult HSV reactivation after liver transplantation and determine whether routine testing for HSV infection by simple mouth swab should be advocated.
166 THE INFLUENCE OF CD-14 POLYMORPHISMS ON HEPATIC FIBROSIS IN CHRONIC HEPATITIS C INFECTION
M. L. Cowan1, L. Ang1, C. J. Tibbs1, M. A. Mendall2, J. D. Maxwell1.1St George’s Hospital and 2Mayday University Hospital, London, UK
Introduction: Even accounting for the known risk factors the rate of progression of fibrosis in chronic hepatitis C infection is very varied. Genetic factors have been implicated. We speculated that CD-14, a molecule involved in the immune response to non-specific microbial components including lipopolysaccharide, may be involved in disease progression. A single amino acid change in the promoter region (C(-260)T) is known to increase CD-14 post-transcriptional activity. The CC homozygote state has been associated with increased γGT in the general population and also with non-alcoholic fatty liver disease.
Methods: 172 patients with chronic hepatitis C who had liver biopsies for staging of their disease (fibrosis scored according to Ishak criteria) were assessed. CD-14 polymorphism status was determined by RFLP. Multivariate analysis was performed to determine risk of fibrosis using logistic regression.
Results: See table.
Abstract 166
The unadjusted odds ratio is 4.96 (1.48–16.57; p = 0.009) for severe fibrosis (Ishak 5 or 6) in subjects who are CD-14 CC homozygotes and 2.99 (0.95–9.37; p = 0.06) for CT heterozygotes v TT homozygotes. These findings are more marked when adjusted for age, sex, BMI, ethnicity, and maximum alcohol intake: CC OR 5.49 (1.51–19.9; p = 0.01); CT OR 3.67 (1.1–12.3; p = 0.035). Of these other risk factors only ethnicity was an independent risk for severe fibrosis (Asian subjects OR 3.2 (1.14–8.94; p = 0.027)).
Conclusion: The CD-14 CC state is a significant independent risk factor for the development of severe fibrosis in chronic hepatitis C with an intermediate risk in CD-14 CT heterozygotes. Reduced innate immune activation may play an important role in preventing fibrosis in hepatitis C.
167 THE GLASGOW ALCOHOLIC HEPATITIS SCORE AND THE EFFECT OF PENTOXIFYLLINE IN ALCOHOLIC HEPATITIS
N. C. McAvoy1, E. Forrest2, P. C. Hayes1.1Liver Unit, Royal infirmary of Edinburgh, 2Department of Gastroenterology, Glasgow Royal Infirmary, UK
Background: It has recently been reported that treatment with pentoxifylline, an inhibitor of tumour necrosis factor, improves survival in severe alcoholic hepatitis. The aim of this study was to review retrospective data to validate the Glasgow Alcoholic Hepatitis Score (GAHS) and identify any influence of pentoxifylline treatment.
Method: Single centre retrospective observational study. We identified patients diagnosed with alcoholic hepatitis who were admitted to our unit from August 2000 to August 2004 and reviewed case records in 49 cases. Inclusion criteria were serum bilirubin >80 umol/l on admission and excess alcohol within four weeks of admission. Patients were excluded if they had a primary presentation with gastrointestinal haemorrhage, evidence of obstructive jaundice, viral hepatitis, autoimmune liver disease, hepatocellular carcinoma, or an AST (ALT) >500 IU/l.
Results: Thirty eight of the 49 patients were treated with pentoxifylline. In the non-pentoxifylline treatment group, patients with a Maddrey DF ⩾32 had a 28 and 84 day mortality of 17% whereas there where no deaths in patients with a DF <32. In patients with a GAHS ⩾9 the 28 and 84 day mortality was 50% whereas in those with GAHS <9 there were no deaths.
Pentoxyfylline treatment in those patients with DF ⩾32 and a GAHS<9 did not affect mortality (12.5% (28 days), 37.5% (84 days) pentoxyfylline group v 15% (28 days), 24% (84 days) non-pentoxyfylline group) (p = NS). However, treatment with pentoxyfylline in those with a GAHS ⩾9 significantly reduced mortality (17% (28 days), 29% (84 days) pentoxyfylline group v 47% (28 days), 61% (84 days) non-pentoxyfylline group) (p<0.02) when compared with a large and comparable population (n = 120) from other centres.
Conclusion: The GAHS is a more specific measure for outcome from alcoholic hepatitis than Maddreys DF. Patients with a DF ⩾32 but a GAHS<9 do not benefit from pentoxyfylline. However, patients with a GAHS ⩾9 who received pentoxyfylline treatment show a significant improvement in survival.
168 INCREASED SERUM ALPHAFETOPROTEIN LEVELS IN PATIENTS WITH CHRONIC HEPATITIS C WITHOUT HEPATOCELLULAR CARCINOMA: A 10 YEAR SINGLE CENTRE PROSPECTIVE STUDY
S. Barclay, R. Fox, E. Spence, E. McCruden, C. Frew, J. McAllister, S. Campbell, P. R. Mills.Gastroenterology Unit, Brownlee Centre, Regional Virus Laboratory and Department of Biochemistry, Gartnavel General Hospital, Glasgow, UK
Background: Patients with chronic hepatitis C (HCV) and cirrhosis are at risk of hepatocellular carcinoma (HCC). Many HCV patients do not now undergo routine liver biopsy and selection for HCC screening is difficult.
Methods: A prospective investigation of the value of a baseline serum alphafetoprotein (AFP) level on all new HCV patients was undertaken over a 10 year period (1993–2002) at a single centre. Serum AFP was monitored in those patients with a raised level, together with those with a clinical or biopsy diagnosis of cirrhosis. Further investigation included imaging or targeted liver biopsy as clinically indicated. Patients were followed for a further 18 months. Outcome was collated from case records, hospital databases, and Registrar General for Scotland mortality search.
Results: 690 patients had active HCV (PCR positive) infection, at least one recorded AFP measurement and the absence of hepatitis B or HIV co-infection. Mean age was 41.2 years (SD 10.2), with a male preponderance of 1.9:1. 70 patients (10.1%) had a significantly increased serum AFP (>12 ng/ml) level. In 10 of these an alternative cause was found (seven pregnancy, three germ cell tumour). Seven patients developed HCC and all died. Positive predictive value for HCC was 11.7%. 53 patients (7.7%) had a rise in serum AFP in the absence of HCC. The raised AFP level often persisted in the range 15–171 ng/ml. Multivariate analysis demonstrated raised AFP to be associated independently with increasing age and stage of fibrosis. 38 patients (5.5%) died during the study period.
Conclusion: AFP was poorly predictive of HCC in this study with many HCV patients with active liver disease having persistently raised levels in the absence of HCC. These findings have implications for large scale screening for HCC.
169 REGENERATION OF THE ISCHAEMIC LIVER REMNANT AND EFFECT OF GLYCINE
M. M. Habib1, C. Selden2, H. F. J. Hodgson2, B. R. Davidson1.1University Department of Surgery and Liver Transplantation; 2Centre for Hepatology, Royal Free and University College Medical School, University College London, Royal Free Hospital, London, UK
Introduction: Glycine reduces hepatic ischaemia reperfusion injury (IRI). We studied the effect ischaemia and its modulation by glycine on regeneration of the liver remnant.
Materials and Methods: We studied, in Sprague-Dawley rats, the effects of oral glycine (or isonitrogenous valine as control) on liver regeneration after 70% partial hepatectomy, when the remnant regenerating lobes had or had not been exposed to 30 minutes ischaemia before resection. Regeneration was assessed by liver/body mass ratio, total protein, DNA, and Bromodeoxyuridine (BrdU) incorporation into hepatocytes.
Results: Early regenerative indices (24 hours) were diminished in previously ischaemic remnants of controls, but the glycine supplemented group showed greater regenerative activity (BrdU index). At 24 hours BrdU Index was significantly reduced in ischaemic remnants compared with non-ischaemic remnants, 12.7 (6.29) % v 46.41 (6.6) % (p = 0.0037). Liver mass, total protein, and DNA were also significantly reduced. BrdU index was significantly improved by the administration of glycine, 28.92 (6.5) % (p = 0.04). By 96 hours, regeneration in the previously ischaemic groups was enhanced in all parameters. BrdU index was significantly increased in ischaemic remnants compared with non-ischaemic remnants, 91.5 (1.0) % v 85.4 (2.3) % (p = 0.02). Ischaemic remnants had significantly increased liver/body mass ratio than non-ischaemic remnants, 3.5 (0.04) % v 3.07 (0.04) % (p = 0.0001). This was also confirmed by significantly increased total DNA and protein content, although the enhancing effect of glycine was no longer apparent.
Conclusion: Ischaemia impairs the regenerative response at 24 hours and improves the ultimate recovery at 96 hours. Glycine ameliorates the early negative impact of moderate ischaemia, and may have the potential to improve outcome after resectional liver surgery.
170 TRANSIENT ISCHAEMIA AND REPERFUSION IMPAIRS EARLY REGENERATIVE RESPONSE IN THE HEPATIC REMNANT
M. M. Habib1, C. Selden2, H. F. J. Hodgson2, B. R. Davidson1.1University Department of Surgery and Liver Transplantation; 2Centre for Hepatology, Royal Free and University College Medical School, University College London, Royal Free Hospital, London, UK
Introduction: We have previously shown that moderate ischaemia impairs early regenerative response at 24 hours after partial hepatectomy (PHx), while enhances the recovery of liver weight at 96 hours. Others have suggested that molecular changes after brief ischaemia suggest that it may enhance liver regeneration. Here we studied the effect of short period of ischaemia reperfusion as may occur during hilar dissection or as is used to induce ischaemic preconditioning, on hepatic regenerative response.
Materials and Methods: Male Sprague-Dawley rats (250–275 g) were divided into two groups: group A (n = 6) underwent 70% PHx (median and left lobe) and group B (n = 6) underwent 10 minutes of ischaemia to the right and caudate lobes and 10 minutes of reperfusion, before 70% PHx as in group A. Animals in both groups were recovered for 24 hours. DNA synthesising hepatocytes were labelled by Bromodeoxyuridine 50 mg/kg body weight, given intraperitoneally 4 hours before killing under anaesthesia. BrdU index was determined from the percentage of BrdU labelled nuclei after BrdU immunostaining.
Results: At 24 hours after partial hepatectomy BrdU index was significantly reduced (p = 0.0481) in group B (32.47 (9.9) %) compared with group A (59.35 (6.55) %). Though there was no significant difference (p = 0.459) in the liver weight/body mass ratio between group A (2.10 (0.07) %) and B (2.033 (0.05) %).
Conclusion: Transient periods of ischaemia reperfusion injury before partial hepatectomy, impair the early regenerative response in the liver remnant which has implications for hepatic resections and split liver transplantation.
171 POST ORTHOPTIC LIVER TRANSPLANT COMPLICATIONS IN PRIMARY SCLEROSING CHOLANGITIS
S. Ramakrishnan, M. Hudson.Freeman Hospital, Newcastle upon Tyne, NE7 7DN, UK
Introduction: Previous studies have suggested a higher retransplatation rate and lower survival in primary sclerosing cholangitis (PSC) patients post orthoptic liver transplant (OLT)1; more frequent relapse of IBD has also been reported post OLT.2
Aims and Methods: A retrospective case note based study of complications post OLT in patients with PSC and the impact of OLT on IBD or pouchitis.
Results: Twenty five (M:F 20:5, age range 28–67 years) patients with PSC have received 31 liver grafts. Six (25%) patients have required retransplantation, five (20%) of 25 for hepatic artery thrombosis (HAT); this compares to 9% in our non-PSC transplant population. Biliary complications developed in six (23%) in the PSC patients compared with 9% in non-PSC transplant patients. De novo hepatitis was seen in four (16%) and recurrent PSC in one. The overall mortality in the PSC patients is 24% to date. 40% (9/22) of PSC patients have had significant events related to their IBD after OLT despite immunosuppression. 22% (2/9) developed de novo colitis, 30% (3/9) have undergone colectomy, 33% of those regularly screened have developed significant dysplastic lesions.
Conclusions: As previously described the incidence of HAT and mortality is high in our PSC liver transplant population. To date the incidence of recurrent PSC is lower than previously reported. Our findings confirm significant complications from IBD post OLT with a need for continued colonoscopic surveillance.
1
2
172 CCR7+ memory CD8 T cells in normal and chronic hepatitis C infected liver
M. Heydtmann1, D. Hardie2, S. Hübscher3, M. Salmon, C. D. Buckley2, D. H. Adams1.1The liver Research Laboratories; 2Department of Rheumatology; 3Department of Pathology Birmingham University, Birmingham, B15 2TH, UK
Background: In hepatitis C infection (HCV) failure of T cell mediated viral clearance results in chronic hepatitis and tissue damage. Memory T cells are divided into CCR7+ central (CM) and CCR7− effector (EM) cells. CM cells are thought to be excluded form peripheral tissue and use CCR7 and CD62L to enter lymph nodes from blood whereas EM cells enter non-lymphoid tissue including liver. We performed extensive phenotyping of lymphocytes infiltrating normal and HCV infected liver and analysed the CCR7 ligands in liver tissue.
Methods: Liver infiltrating lymphocytes from HCV transplant patients and normal donors were isolated and analysed by up to 4 colour flowcytometry. Liver sections were stained using immunohistochemistry and 4 colour confocal microscopy.
Results:
-
All CD8 T cells in human liver are CD11ahigh/CD62Llow indicating an absence of naïve cells in the liver.
-
We detected CCR7+/CD62L−/CD11ahigh primed/memory cells in normal and HCV liver. These included both CD45RA+ and CD45RA− cells with the latter subset reduced in HCV compared with normal liver.
-
Immunohistochemistry revealed strong expression of the CCR7 ligands CCL19 and CCL21 on sinusoids and portal vessels in normal and HCV infected liver. CCL19 was detected on both endothelial (CD31+) and lymphatic (LYVE-1+) vessels and CCL21 on some CD31+ vessels. In HCV the expression of both chemokines increased on sinusoids and on neovessels in portal tracts
Conclusion: Expression of CCR7 in the absence of CD62L on subsets of primed liver infiltrating CD8 cells suggests these cells migrate from tissue via lymphatics into lymph node. We term these cells centripetal memory cells and suggest that they traffic between liver and lymph nodes to provide immune surveillance. The relative lack of these cells in HCV infected liver suggests that this pathway is compromised.
173 HCV SPECIFIC T CELL RESPONSE IN SEXUAL PARTNERS OF HCV POSITIVE SUBJECTS
P. T. F. Kennedy1,2, R. Moses1, R. Williams1, G. Dusheiko2, A. Bertoletti1.1Institute of Hepatology and 2Centre of Hepatology, Royal Free and University College Medical School, University College London, UK
Background: Sexual transmission of hepatitis C virus (HCV) is considered a minor risk factor for infection. To investigate whether HCV negative sexual partners of HCV positive subjects are able to mount a protective HCV specific T cell response, their global HCV specific T cell repertoire was analysed. Responses were compared with those present in resolved HCV infection and in HCV negative controls.
Methods: Patients with resolved HCV infection (n = 5), HCV negative sexual partners of HCV+ subjects (n = 5) and HCV negative controls without any HCV risk factors were recruited for the study. HCV specific T cell response was analysed directly ex vivo and after in vitro stimulation with IFN-γ ELI Spot assay using 601 overlapping peptides spanning the entire HCV sequence, genotype 1a. Intracellular cytokine staining was used to differentiate IFN-γ production from a CD4 or CD8 T cell population.
Results: Ex vivo and in vitro analysis of HCV specific T cell response in sexually exposed non-infected subjects demonstrates the presence of peptide specific CD4 and CD8 T cell responses. This T cell response was quantitatively lower and narrowly focused to fewer peptides (3–4 peptides out of 601) in comparison to the broader peptide specific T cell response found in patients with resolved HCV infection (10–25 peptides out of 601). The extent of HCV peptide specific T cell response found in sexually exposed non-infected subjects was similar to the T cell response detected in negative controls without any HCV risk factors. In silico analysis of the amino acid sequence of responsive HCV peptides found in HCV sexually exposed and negative controls reveals extensive sequence homology with proteins present in common human viruses (HSV, HPV, VV). Analysis of T cell cross reactivity between peptides derived from different pathogens and HCV peptides is under way.
Conclusion: HCV peptide specific T cells can be demonstrated in HCV sexually exposed non-infected subjects. Cross reactivity with other common pathogens is the more likely explanation for their presence as opposed to direct HCV priming. The importance of such responses in HCV protection will need further evaluation.
174 DIFFERENT POPULATIONS OF ALCOHOL MISUSERS
J. White, C. Nelson, N. Sheron, K. Tull, S. Smith.Liver Research Group, University of Southampton, Southampton General Hospital, Tremona Road, Southampton SO16 3TN, UK
Introduction: Alcoholic liver disease (ALD) and physical alcohol dependence are both consequences of chronic alcohol misuse. These two consequences however do not go hand-in-hand. Previous studies have suggested that the majority of patients presenting with alcoholic liver disease are not severely dependent on alcohol.
We explored this further by investigating whether there are in fact two separate populations of alcohol misusers and looked into any differences between the two groups which may explain why some of them develop ALD and some develop severe alcohol dependence requiring residential detox.
Methods: Participants were recruited into three cohorts and data were collected using two interview administered questionnaires. The ALD cohort (n = 31) was recruited from liver wards and outpatients at Southampton General Hospital, the alcohol detox cohort were residents from a Southampton alcohol treatment centre, and age matched controls were recruited from other wards at SGH providing their admission was not related to alcohol. Levels of physical alcohol dependency were measured using the well established Severity of Alcohol Dependence Questionnaire (SADQ). The second questionnaire was designed specifically for the study and assessed drinking pattern, reasons for heavy drinking, and the social circumstances of the participants.
Results: 71% of the patients with ALD were not physically dependent on alcohol according to the SADQ questionnaire. See figure.

Abstract 174 Error bar illustrating differences in SADQ scores between cohorts with 95% CI.
Our results also show statistically significant differences between the cohorts in (1) subject age, (2) mean daily alcohol consumption, (3) who subjects drank with and where, (4) reasons for heavy drinking, and (5) social circumstances of subjects.
Discussion: Our results show there are two separate and quite different populations of alcohol misusers and the majority of those who develop ALD are not dependent on alcohol according to the best validated tool for dependency. To tackle the problem of alcohol misuse in this country we will therefore require two different approaches in effective intervention for these two very different sets of people.
175 THE ROLE OF LIVER TRANSPLANTATION IN THE TREATMENT OF WILSON’S DISEASE
C. M. Bates, J. S. Davidson, K. J. Simpson.Scottish Liver Transplant Unit, Royal Infirmary of Edinburgh, Edinburgh, UK
Background: Wilson’s disease is an autosomal recessive defect in cellular copper transport. Liver transplant is a treatment option for those presenting with fulminant hepatic failure, treatment resistant cases, or those with cirrhosis and chronic liver failure.
Methods: A case review was performed of all patients referred to the Scottish liver transplant unit (SLTU) diagnosed with Wilson’s disease, to evaluate the clinical findings at time of referral, treatment commenced, and outcome achieved including requirement for liver transplant.
Results: On review of case records between November 1992 and September 2004, 10 patients were identified as Wilson’s disease. Median age at time of referral was 20 years (range 13–42 years). Three patients known previously to have Wilson’s disease were referred for transplant assessment due to chronic liver failure. Two were listed and subsequently received successful liver transplant (OLT). The third patient was readmitted with acute liver failure and encephalopathy and underwent successful super urgent OLT.
Seven patients were referred urgently for acute severe liver injury. Median age 18 years (range 13–23). One patient developed encephalopathy with fulminant hepatic failure and underwent successful super urgent OLT. Six patients were commenced on copper chelating therapy. One patient deteriorated despite medical therapy and subsequently received successful OLT in a paediatric unit.
Conclusion: Ten patients have been referred to SLTU with Wilson’s disease, five have received successful OLT, two super urgent, and three elective. Five patients referred with acute liver injury without evidence of encephalopathy were successfully treated with copper chelating therapy. This study shows that even patients with severe acute liver injury can be successfully treated with chelation therapy; however, the onset of hepatic encephalopathy or chronic liver failure in patients with known Wilson’s disease are indications for liver transplant.
176 INCREASED PLASMA PROCOLLAGEN PEPTIDE PREDICTS CIRRHOSIS BUT NOT FIBROSIS ON LIVER BIOPSY
P. Moncur, S. M. Kelly.Department of Gastroenterology, York Hospital, York, UK
Aims: Previous work has suggested a correlation between plasma procollagen peptide and the degree of fibrosis/cirrhosis identified at liver biopsy. This correlation may allow the progress of patients with liver disease to be monitored without the need for invasive liver biopsy. We examined the predictive value of procollagen peptide for fibrosis on liver biopsy in routine clinical practice. In particular, we were interested to see if correlated with fibrosis short of cirrhosis.
Materials and Methods: In a prospective study, all liver biopsies performed for assessment of liver parenchymal disease over a two year period had a plasma procollagen peptide level measured at the time of biopsy. Liver histology was classified as demonstrating no fibrosis, fibrosis only and established cirrhosis.
Results: Results were available on 39 patients with a variety of diagnoses—ALD, hep C, fatty liver/NASH, AIH, PSC, PBC, and drug related hepatitis.
Interquartile ranges for each of the three histological groups were calculated and the results analysed using the Mann-Whitney U test. There was no significant difference in procollagen peptide levels obtained from non-cirrhotic livers with (n = 14; 4.7 (2.7) μg/l) or without fibrosis (n = 21; 4.0 (1.0) μg/l: p>0.05).
There was a highly significant correlation between procollagen peptide levels from patients with established cirrhosis on biopsy compared to non-cirrhotic individuals (n = 4; 8.0 (1.2) μg/l: p<0.01).
Conclusions: Procollagen peptide levels appear not to be useful as a reliable predictor of progression to fibrosis alone. However, it may provide a non-invasive method for identifying individuals likely to have developed established cirrhosis.
177 EFFECT OF HEPARINOIDS (GLYCOSAMINOGLYCANS) ON COAGULATION: A THROMBOELASTOGRAPHIC STUDY
M. Senzolo, E. Cholongitas, C. K. Triantos, A. Riddell1, J. Coppell1, A. K. Burroughs.(introduced by A. K. Burroughs). Liver Transplantation and Hepatobiliary Unit, Haemophilia Centre and 1Haemostasis Unit; Royal Free Hospital, London, UK
Introduction: Endogenous heparinoids which are glycosaminoglycans (GAGSs) impair coagulation as assessed by heparinase-modified-thrombelastography (TEG) in infected cirrhotics (Montalto, J Hepatol 2002). However, which heparinoid is responsible is not known.
Aim: To evaluate different GAGs in normal blood using native and heparinase modified TEG.
Material and Methods: Ten healthy volunteers (8 M, F, mean age 36.8 (SD 8) years) were enrolled. Based on Danaparoid concentration, Heparan Sulfate (H) 0.12 mg/ml, Dermatan sulphate (D) 0.83 mg/ml, Chondroitin-4-sulfate (C) 2.5 mg/ml, corresponding to 10 U/ml of GAG were added to volunteers’ whole citrated blood; then diluted obtaining concentrations of: 1.0 U/ml, 0.5 U/ml, 0.1 U/ml, 0.05 U/ml. Native and heparinase-modified-TEG were performed for all GAG concentrations. Following double centrifugation of samples, PT/INR, APTT, thrombin time (TT) anti Xa level (antiXa) and Heparin cofactor II (HCII) levels were measured at all GAG concentrations.
Results: A significant TEG heparin-like effects was seen at the higher concentrations H1.0 U/ml, H0.5 U/ml, D1 U/ml, D0.5 U/ml, as well as at highest of Chondroitin sulphate (C1 U/ml). All were completely reversed by heparinase-modified-TEG. As expected, PT and INR did not detect the heparin-like effect, but PTT was significantly lower in samples with heparin-like effect than in samples without. A significant decrease in HCII values was seen in higher concentration of Derman Sulfate and Chondroitin-4-sulphate, compared with lower concentrations, but not in Heparan Sulfate samples.
Conclusion: Native and heparinase-modified-TEG can detect not only the effect of Heparan, but also of Dermatan and Chondroitin-4 Sulpate on coagulation. Therefore these compounds may be responsible for the endogenous heparin effect in vivo.
178 IS ERCP BENEFICIAL IN PATIENTS WITH MALIGNANT BILIARY STRICTURES PLUS LIVER METASTASES?
P. McConville, A. Murdock, C. Larkin, T. C. K. Tham.Division of Gastroenterology, Ulster Hospital, Dundonald, Belfast, N Ireland, UK
Background: ERCP plus stenting is recognised to be of benefit in the palliation of malignant biliary strictures. However it is not known if patients with concomitant liver metastases will benefit from ERCP. The aims of this study were to see if ERCP plus stenting produced a reduction in bilirubin and symptomatic improvement in patients with malignant biliary obstruction and liver metastases
Methods: Consecutive patients with known malignant biliary strictures and liver metastases were identified from a prospective ERCP database. A chart review of each case was performed to identify basic demographics, pre procedure plus last recorded bilirubin and evidence of symptomatic improvement (reduction in lethargy, nausea and vomiting, abdominal pain, and itch)
Results: A total of 20 patients were identified (eight male, 12 female, mean age 72). Data on symptomatic improvement were incomplete in two patients for bilirubin assessment and seven patients for symptomatic improvement. The diagnoses included liver metastases from non-biliary malignancy in 11 (55%) and pancreatic malignancy nine (45%).
17 out of 20 (85%) had dominant extra-hepatic strictures and three (15%) had intrahepatic strictures without a dominant extrahepatic stricture. Plastic stents were inserted in 11 and metal stents in nine.
Following stent insertion, a reduction in bilirubin was observed in 14 out of 18 (78%) and symptomatic improvement was observed in six out of 13 (46%). 12 out of 15 (80%) with a dominant extrahepatic stricture had a reduction in bilirubin and five out of 10 (50%) improved symptomatically. Two out of three (67%) of those without a dominant extrahepatic stricture had a reduction in bilirubin post-stent and one out of three (33%) improved symptomatically. Mortality data were available on six patients: four out of six (67%) survived more than 30 days and mean survival was 80 days.
Conclusions: The majority of patients with malignant biliary strictures and liver metastases benefited from ERCP and stenting as there was a reduction in bilirubin and symptomatic improvement. Patients with dominant extrahepatic strictures seemed to benefit more than those without extrahepatic strictures.
179 CD81 SEQUENCE AND SUSCEPTIBILITY TO HCV INFECTION
A. Houldsworth, M. Metzner, A. G. Demaine, E. Kaminski, M. E. Cramp.Gastroenterology and Liver Unit, Department of Immunology, Derriford Hospital, Hepatology and Molecular Medicine Research Groups, Peninsula Medical School, Plymouth, UK
Background: Several cell surface molecules have been shown to have hepatitis C virus (HCV) binding properties and may serve as receptors to facilitate viral entry into cells. The large extracellular loop (LEL) of CD81 has been shown to bind the HCV envelope protein E2. Previous studies have demonstrated several critical residues for the CD81-HCV E2 interaction. We hypothesised that sequence variation in the CD81 LEL may result in altered susceptibility to HCV infection.
Methods: Three groups of cases were studied: HCV antibody positive but HCV RNA negative cases with spontaneous viral clearance, HCV antibody and HCV RNA positive chronically infected cases, and also cases with a long history of intravenous drug usage at high risk of HCV infection who were termed HCV exposed but uninfected cases. CD81 sequencing was performed in two ways. Firstly, genomic DNA was extracted from whole blood samples and the exonic sections of the gene encoding the CD81 LEL were amplified in four sections by PCR and subsequently sequenced. Secondly, the whole LEL (≈700 bp) was sequenced from cDNA made following RNA extraction from peripheral blood mononuclear cells.
Results: In total, 61 cases had their genomic DNA sequenced; 21 cases of spontaneous clearance, 15 chronic HCV, and 25 HCV exposed but uninfected cases. Of these 61, 23 also had the whole length LEL sequenced from cDNA—11 spontaneous clearers, five chronically infected, and seven exposed but uninfected. No sequence variation was found in any of the cases studied by either method, including the section of the gene coding the residues most important for CD81-HCV E2 binding.
Conclusions: The large extracellular loop of CD81 is a highly conserved molecule. There are no common differences in genomic sequence that influence susceptibility to, or outcome of, HCV infection.
180 CAUSES OF SIGNIFICANT HYPERTRANSAMINASAEMIA IN AN INPATIENT POPULATION
R. C. Thomas, J. V. Metcalf.University Hospital of North Tees, Stockton, UK
Introduction: Abnormal liver function tests are common in the acute hospital setting. The cause is often multifactorial. In most cases the abnormalities are slight and require little investigation. An ALT (alanine aminotransferase) >350 however, indicates significant liver injury. We proposed to evaluate the causes of significant hypertransaminasaemia in our trust (two district general hospitals) over a 3 month period.
Methods: A search performed on the biochemistry computer revealed 61 suitable patients. Consent from these patients was sought by letter, and obtained from 47 patients (77%). Their notes were then reviewed.
Results: Of the 47 patients five (10.6%) died during their admission. The mean age was 57.7 years and the median was 58 (range 14–89). The majority of patients were under medical care (59.6%), 31.9% under surgical care, 6.3% paediatrics, and 2.1% on ITU.
The commonest causes were gallstone related (27.7%), with cardiovascular causes (congestive cardiac failure and ischaemia) the next most common (14.9%), and then drug related episodes (including paracetamol overdosage) 10.6%. 14 patients had an ALT>1000. Of these 35.7% had viral hepatitis (a, b, c), 28.6% were drug related (including overdosage), and 21.4% were related to ischaemia. 70% of all the cardiovascular related causes were found in those over 70, although gallstone related disease was still more common in this age group. Viral hepatitis (a, b, c) was most common in the under 40s. Alcohol related causes were identified only in patients aged 40–60 years.
Conclusion: Abdominal ultrasound should be performed in all inpatients with hypertransaminasaemia to exclude gallstone related disease. The patient’s age should be accounted for when considering the cause—in the elderly cardiovascular causes should be excluded, and in the young screen for hepatitis
181 THE GLASGOW ALCOHOLIC HEPATITIS SCORE IS NOT SUPERIOR TO THE DISCRIMINANT FUNCTION IN PREDICTING 12 MONTH MORTALITY
B. K. Baburajan, G. L. A. Bird, P. Mills.Department of Gastroenterology, Maidstone Hospital, Maidstone, Kent, UK
Background: Acute alcoholic hepatitis can have a hospital mortality of up to 60% in the first month. Treatment with steroids has been shown to decrease the mortality but their use remains controversial. The Glasgow Alcoholic Hepatitis Score (GAHS) has been proposed to be superior to the conventionally used Maddrey Discriminant function in identifying patients at high risk of mortality
Methods: Sixty two patients with acute alcoholic hepatitis were recruited to a randomised trial into the survival benefit of Amlodipine (Bird GLA, Prach A, Mc Mahon AD, et al. Randomised double blind controlled trial of the calcium antagonist amlodipine in the treatment of acute alcoholic hepatitis.
No differences were shown between the treated and the placebo groups and hence the body of data is taken as a whole. In 36, alcoholic hepatitis was confirmed on liver biopsy. The rest had typical clinical and laboratory criteria. The data were subsequently analysed to compare the reliability of the GAH Score and the Maddrey DF in predicting short term and 1 year mortality.
Results: The required data were available on 48 patients. In this group there were nine deaths over 28 days and 20 deaths over 12 months. 7/20 had a Glasgow acute hepatitis score >9 (35%). 14/20 had a DF of >32 (70%).
Conclusions: The GAHS had a positive predictive value of 0.6 and a negative predictive value of 0.7 for death in 12 months. This was similar to the Maddrey DF in the same group (PPV 0.5 and NPV 0.7). The GAHS had a lower sensitivity than DF (38% v 72%) and a higher specificity than the DF (86% v 60%) in this group. It also had a higher sensitivity and specificity than the Maddrey DF in predicting 28 day survival. Both models are limited by low sensitivity and specificity.
182 THE NATURAL HISTORY OF HEPATIC SARCOID
N. Zakaria, P. T. F. Kennedy, S. Mudawi, A. Papadopoulou, I. Murray-Lyon, R. duBois, J. Devlin, H. J. N. Andreyev.Chelsea & Westminster, Royal Brompton and Kings College Hospitals, London, UK
Background: Sarcoidosis is a multisystem granulomatous disorder of unknown aetiology which variably involves the liver. It is generally thought that sarcoidosis causes severe disease only of the lung. We undertook this study to investigate the natural history of hepatic sarcoid and to investigate its response to treatment.
Patients and Methods: This was a retrospective study of 90 consecutive patients (M:F 47:43) with a diagnosis of liver sarcoid referred to two tertiary liver clinics. Median age was 44 years (range 20–72). Follow up was for a minimum of 2 years. Clinical notes, laboratory, histological, and radiological data for all patients were reviewed.
Results: Twenty six per cent (23/90) had liver sarcoid without lung involvement. 74% (67/90) had both. Liver biopsy was performed in 36/90 patients. Established cirrhosis was present in 14/36. 9/14 were cirrhotic at presentation, the remaining five progressed to cirrhosis. Portal hypertension (PHT) was present in 16 (non-cirrhotic PHT 4/16).
Treatment and Outcome: A total of 63 received corticosteroids. 18/63 had a sustained biochemical response. Two progressed to cirrhosis despite steroid therapy.16/45 received a second-line immunosuppressive agent. 8/16 showed a clear response to treatment augmentation, (4 azathioprine, 3 methotrexate, 1 both). 6/90 patients underwent orthotopic liver transplantation. In 4/6 a diagnosis of sarcoid was made only on examination of the explanted liver. Sarcoid recurred after liver transplantation in one patient.
Conclusion: Sarcoidosis as a cause of chronic liver disease is underestimated. An evidence base for treatment is lacking. The percentage of patients who required OLT is indicative of the potential severity of disease. Diagnosis is sometimes made after examination only of the explanted liver, confirming the elusive nature of the disease. A biochemical response to therapy does not necessarily mirror histopathology. Emphasis on the early introduction of immunosuppressive agents in the treatment of hepatic sarcoid may reduce the numbers of patients requiring liver transplantation in the future.
183 PERIPHERAL HEPATIC AND HAEMATOPOIETIC STEM CELLS AFTER PARTIAL HEPATECTOMY: PRELIMINARY DATA
R. Stigliano, L. Marelli, C. Pang, M. Lowdell, D. Patch, K. Rolles, B. Davidson, N. Rolando, A. K. Burroughs.Department of Surgery, Liver Transplantation and Hepatobiliary Medicine and Department of Haematology, Royal Free Hospital, London, UK
Background: The role of stem cells in liver regeneration after partial hepatectomy is not well documented. Recent studies suggest that haematopoietic stem cells residing in bone marrow may contribute to liver regeneration after injury.
Aim: To determine if hepatocyte progenitor cells can be detected in peripheral blood after partial hepatectomy.
Method: Peripheral blood mononuclear cells (PBMC) were isolated before surgery and then monitored in the postoperative period in patients undergoing liver resection due to neoplastic disease. Peripheral hepatocyte progenitors were defined as mononuclear cells expressing CD117(+), CD34(−), and CD45low,1 were assessed by flow cytometry analysis. RESULTS: 10 patients (M/F 6/4, mean age 60 (SD 14) years) were resected for liver metastases (n = 7) and non-cirrhotic hepatocellular carcinoma (n = 3); four had right hepatectomy, four multisegmentectomy, and two segmentectomy. Median values before and on day 5 post-hepatectomy were ALT 23.5 (17–283) and 149 (14–892) UI/l; AST 28.5 (22–230) and 76.5 (33–850) UI/l; PBMCs 22.2 (2.4–32) and 18.7 (3.2–70) 106/ml; CD117+34–45weak (hepatocyte progenitors) were 0.22 (0–2.33) and 0.19 (0.04–1.08) %; CD117±34+45weak (haematopoietic progenitors) were 0.11 (0.04–0.65) and 0.26 (0.06–2.82) %. The number of bone marrow progenitors was independent of the amount of tissue resected. There was a negative correlation between ALT increase and the percentage of CD117+34–45weak on the fifth day (ALT r = −0.65 p = 0.042, AST r = − 0.71 p = 0.023).
Conclusions: In this study we have documented an increase of haematopoietic progenitors but not of hepatocyte progenitors in peripheral blood following partial hepatectomy. Whether hepatic progenitors contribute to regeneration will require further study
1
184 CIRCULATING PROGENITOR CELLS AFTER VASCULAR INJURY
R. Stigliano, L. Marelli, M. Senzolo, F. Morisco, C. Pang, M. Lowdell, D. Patch, J. Tibballs, N. Davies, K. Rolles B Davidson, N. Rolando, A. K. Burroughs.Liver Transplantion and Hepatobiliary Medicine Unit, Department of Radiology and Haematology, Royal Free Hospital, London, UK
Introduction: Bone marrow has been the source of liver repopulating cells in experimental liver transplantation. Whether liver injury per se is a stimulus is unknown. Transarterial chemoembolisation (TACE) of hepatocellular carcinoma (HCC) is followed by raised transaminases secondary to necrosis.
Aim: To establish if progenitor cells are incresed in peripheral blood after vascular injury in humans.
Method: 20 ml peripheral blood was collected before and 24 hours after embolisation of HCC. Peripheral blood mononuclear cells (PBMCs) were isolated and cryopreserved. Peripheral hepatocyte progenitors were defined as mononuclear cells expressing CD117(+), CD34(−) and CD45low; these were assessed by flow cytometry analysis.
Results: Ten cirrhotics (M/F 9/1; age 65 (SD 10) years) with HCC. The median CP score was 7, CLIP score 2; 70% ⩽3 nodules, 30% >3; 90% right hepatic artery and 10% selective TACE. Before and after TACE, median ALT was 65 (33–137) and 74 (38–172) UI/l; AST 88 (48–575) and 96 (56–625) UI/l; Bilirubin 38 (15–68) and 42 (28–97) μmol/l; PBMC 21 (10–40) and 20 (9–30) 106/ml; CD117+34–45low 0.12% (0.02–1.41) and 0.14 (0.06–5.53); CD 34+total 0.42% (0.08–3.13) and 0.17% (0.04–2.74). The median changes were: ALT 5 UI/l (−13 to 164), AST 0 UI/l (−24 to 625), bilirubin 14.5 (−2 to 32) μmol/L, CD117+34−0.03% (−1.21 to 5.51), CD34+−0.18% (−80 to 0.47). Before TACE, the percentage of CD117+34–45low correlated with ALT (r = 0.683; p = 0.042), while after TACE CD 34+ cells were inversely correlated with ALT (r = −0.940; p = 0.000) and AST (r = −0.770; p = 0.009).
Conclusions: Circulating hepatic progenitor cells can be found in stable cirrhotics with HCC. However there was no significant difference in the proportion of CD34 and CD117+34–45low progenitors cells in peripheral blood following modest vascular injury after TACE. Whether the size of injury, presence of HCC, and/or patient age influence these findings needs further investigation.
185 EPIDEMIOLOGY OF ACUTE LIVER FAILURE IN SINGAPORE
S. G. Lim, K. F. Teoh, C. T. Wai, M. O. Aung, M. Da Costa, H. L. Lee, J. Isaac.Division of Gastroenterology, Department of Medicine, Department of Surgery, Liver Transplant Unit, National University Hospital, Singapore
Background: Acute liver failure (ALF) is a rare but devastating disease but its epidemiology in Asia has not been well studied. Our aim is to review causes and courses of ALF referred to the national liver transplant center in Singapore.
Methods: We retrospectively analysed all cases of adult patients with ALF referred to the Liver Transplant Program in Singapore from 1991–2003. Causes of ALF and course of their illness were reviewed. Eighty five adult patients were referred for consideration of emergency liver transplant for ALF during the 13 year period. Age (mean (SEM), median (range)) was 43 (1), 43 (15–72) years, 65 (77%) Chinese, 48 (57%) male.
Results: The three commonest causes of ALF were: reactivation of chronic hepatitis B in 38 (45%), drug induced liver injury (DILI) in 32 (38%), and Wilson’s disease in four (5%). Overall transplant free survival was 15/85 (18%). Among the 32 patients with DILI, traditional Chinese medicines (TCM) was implicated in eight patients, followed by acetaminophen (n = 6), and antituberculosis drugs (n = 5). Patients with DILI were more likely to be female (20/32 v 17/53, p = 0.007), and had better survival (11/32 v 8/53, p = 0.039) and transplant free survival (9/32 v 6/53, p = 0.049) than those with other diagnosis. At multivariate analysis, age at presentation (p = 0.019) was the only independent factor associated with transplant free survival.
Conclusion: The clinical course of ALF in Singapore is different from those in the West, with a poor transplant free survival at 18%, and reactivation of hepatitis B being the commonest cause. Although transplant free survival for DILI appears better than other causes, it was insignificant at multivariate analysis. TCM is an important cause for ALF in Singapore. Unfortunately, use of TCM is not regulated in most countries so further studies and audit on safety of use of TCM are urgently needed.
186 N-ACETYLCYSTEINE PROTECTS PRIMARY HUMAN HEPATOCYTES FROM FAS-LIGAND BINDING INDUCED APOPTOSIS
R. C. Saich, C. Selden, M. Rees1, H. Hodgson.Centre for Hepatology, Royal Free & University College Medical School, Royal Free Campus, Rowland Hill Street, London, NW3 2PF; 1The North Hampshire Hospital, Aldermaston Road, Basingstoke, RG24 9NA, UK
Introduction: Apoptosis is implicated in the pathogenesis of a number of human liver diseases. Fas, a death receptor of the TNF super-receptor family, is highly expressed in the liver. Binding of Fas by Fas-Ligand (Fas-L) causes activation of a cascade of caspase enzymes resulting in apoptosis and liver injury. Fas-L levels and Fas expression are increased in a number of liver diseases implicating the Fas death receptor pathway in the pathophysiology of these conditions.
N-acetylcysteine (NAC) has been shown to reduce mortality in the treatment of paracetamol toxicity due to its effect as a glutathione donor. In addition NAC has been shown to have anti-oxidant, reducing, and anti-apoptotic effects. The effects of NAC on Fas-L induced apoptosis in hepatocytes have not previously been studied.
Aim: To investigate if NAC protects primary human hepatocytes against Fas-ligand binding induced apoptosis in vitro.
Methods: Primary human hepatocytes isolated from normal human liver were incubated for 12 hours in complete medium±NAC 10 mM, followed by addition of Fas-L 20 ng/ml for 4 hours for apoptosis assessment and 16 hours for cell viability. Apoptosis was quantified by TUNEL staining and microscopy, and Caspase 3 enzyme activation using a luminescence based assay. Cell viability was assessed by measuring tetrazolium reducing ability (MTT) colourmetrically.
Results: Fas-ligand increased apoptosis in hepatocytes (Caspase 3 activation 183%±0.5%, p<0.005, TUNEL cell positivity 212 (6.7) %, p<0.0002). This increase in apoptosis was eliminated by treatment with NAC, (Caspase 3 activatation 104 (5.9) % p = 0.58, TUNEL positivity 103 (7.6) %, p = 0.78). Fas-L decreased cell viability to 76 (6.3) %, p<0.05 and this effect was eliminated by treatment with NAC, cell viability 107 (1.7) %, p = 0.154.
Conclusion: NAC protects primary human hepatocytes from Fas-ligand binding induced apoptosis.
187 MOLECULAR ADSORBENTS RECIRCULATING SYSTEM THERAPY DOES NOT DECREASE THE ABILITY OF LIVER FAILURE PLASMA TO INDUCE APOPTOSIS AND CELL DEATH
R. C. Saich, C. Selden, M. Rees1, H. Hodgson.Centre for Hepatology, Royal Free & University College Medical School, Royal Free Campus, London, NW3 2PF; 1The North Hampshire Hospital, Aldermaston Road, Basingstoke, RG24 9NA, UK
Introduction: Liver failure is associated with accumulation of endogenous toxins capable of inducing apoptosis in hepatocytes which may perpetuate liver failure. Many of these toxins are albumin bound and not efficiently removed by conventional methods. Molecular adsorbents recirculating system (MARS) dialysis against a 20% human albumin solution, improves haemodynamic stability, encephalopathy, renal and liver function.
Aim: To test the hypothesis that treatment with MARS removes toxins that induce hepatocyte cell death and thus improves liver function.
Methods: Eight patients, with acutely decompensated chronic liver disease were treated with two to three 6 hour MARS therapy sessions. Plasma samples taken immediately before and after each treatment session were applied to primary human hepatocytes monolayers for 4 hours. Apoptosis induced was measured using a luminescence based Caspase 3 activity assay in a 96 well format and by TUNEL staining. Effects on hepatocyte viability were assessed by measuring tetrazolium reducing ability (MTT). The effectiveness of each MARS treatment in removing albumin bound toxins was assessed by measuring bilirubin pre- and post-treatment. Data were analysed for statistical significance using a paired student t test.
Results: Significant removal of albumin bound substances was shown by a 29% reduction in Bilirubin (mean pretreatment 369 (53) μmol/l, mean post treatment 263 (34) μmol/l, p<0.005). However MARS therapy did not reduce the ability of liver failure plasma to induce apoptosis in primary human hepatocytes as measured by Caspase 3 activation (pre 5038 (880) LU, post 4985 (802) LU, p = 0.89), or TUNEL positivity (pre 7.2 (0.67) %, post 6.9 (6.2) %, p = 0.44), and did not improve cell viability measured by MTT (pre 0.57 (0.04) AU550, post 0.58 (0.04) AU550, p = 0.26).
Conclusion: These results suggest that improvement in liver function seen after MARS therapy is not due to removal of substances directly toxic to hepatocytes.
188 BUDD-CHIARI IN EDINBURGH: 27 YEARS’ EXPERIENCE
S. P. Griffin, J. Ferguson, P. C. Hayes.Royal Prince Alfred, Sydney, Australia and Royal Infirmary Edinburgh, UK
Background: Budd-Chiari syndrome represents occlusion of the main hepatic veins. Thrombosis, usually due to a haematological or other thrombotic disorder, is the predominant cause. The presentation may be acute with fulminant liver failure or chronic with evolving features over months. Classically pain, ascites, and hepatomegaly are present and prognosis is poor despite the young age of most patients. Accepted algorithms for management have yet to be determined. We report retrospectively on the experience in Edinburgh since 1977.
Methods: Twenty patients with confirmed Budd-Chiari were identified up to 2003. The diagnosis was initially made on ultrasound in all 20 with confirmation made with hepatic venography in 11 and autopsy or surgery in eight. Liver biopsy supported the diagnosis in 50%. 16 of 20 were female with the average age at diagnosis 31 years (n = 19). 60% have died with all but one of these deaths within 20 months of onset of symptoms.
Results: Eleven of the 20 had a definite thrombotic tendency diagnosed; antithrombin III definite in two, PRV in two, PNH in one, ET and pregnancy in one, uncharacterised myeloproliferative disorder in one (on bone marrow biopsy), flare of colitis and PSC in one, pancreatic cancer in one, pericardial rhabdomyosarcoma in one, and clotting on warfarin in one (incomplete screen). One subject had an absent SVC, while five were on the OCP alone. In three no cause was identified or the thrombophilia screen was incomplete.
A TIPSS was attempted in six; one long term success on warfarin, one short term success with repeated procedures, one initial success requiring a surgical shunt, one hepatic infarction, and two failed procedures. A surgical shunt was performed in four with one long term survivor on warfarin. Five patients had a liver transplant with two survivors on warfarin. One patient with ET did well on hydroxyurea with recanalisation of the hepatic veins after a failed TIPSS. A patient with agenesis of the SVC has ascites but survives off warfarin. Two further patients are well on warfarin alone with uncharacterised thrombophilias.
Comment: Budd-Chiari in Scotland is a rare disorder that primarily affects young women, with a poor prognosis despite aggressive intervention. This is despite improved diagnosis, haematological investigations, and intervention.
189 IS INTERFERON ALPHA THERAPY SAFE AND EFFECTIVE FOR PATIENTS WITH CHRONIC HEPATITIS C AND INFLAMMATORY BOWEL DISEASE? A CASE CONTROL STUDY
A. Anderloni, S. Bargiggia, D. Thorburn2, S. Ardizzone, A. Giorgi1, F. Parente.Department of Gastroenterology and 1Infectious Diseases, L. Sacco University Hospital, Milan, Italy; 2The Liver Unit, Queen Elizabeth Hospital, Birmingham, UK
Background: HCV infection is more common in patients with inflammatory bowel disease (IBD) than in general population. Limited data are available so far on the effects of α-interferon (IFN) therapy in chronic active hepatitis (CAH) C in patients with concomitant IBD. The aim of this study has been to evaluate the efficacy and safety of interferon-α monotherapy in patients with CAH C and inactive or mildly active IBD.
Methods: Between 1995 and 2000 we tested anti-HCV Ab in 513 consecutive IBD patients; 21 were anti-HCV Ab and HCV-RNA positive with histologically proved CAH. All these patients, whose IBD was on clinical remission or mildly active, as well as a group of sex and age matched controls with CAH only, were treated with human leucocyte α-interferon (Alfaferone, Alfa-Wassermann, Bologna, Italy), 6 MU tiw for 12 months. The criteria of response to treatment were as follows: persistently normal ALT and viral clearance (HCV-RNA negative) at the end of treatment (complete response = CR), incomplete response (IR) in case of ALT normalisation without viral clearance (HCV-RNA positive), and sustained response (SR) in case of ALT normalisation and HCV clearance 12 months after the end of treatment.
Results: Twenty one patients with CAH and inactive or mildly active IBD (10 with CD and 11 with UC) and 63 sex and age matched controls with CAH only received IFN-α monotherapy. We observed CR in 42% and SR in 24% of IBD patients compared with 35% and 18% in the control group,respectively (p = NS). None of the 21 IBD patients had severe adverse effects and the mild ones observed were comparable to those seen in the control group. No patients developed an IBD relapse during the IFN treatment period or in the 12 months thereafter.
Conclusions: The biochemical and virological response to a 12 month human leucocyte α-IFN treatment in patients with CAH C and IBD is quite comparable to that registered in CAH patients without IBD. Adverse effects are similar in both groups of patients and totally unrelated to the underlying inflammatory bowel condition. This provides the hepatologists with the proof that IFN-α can be started with safety in HCV patients with a concomitant IBD provided that the inflammatory bowel condition is on clinical remission.
Pancreas posters
190 THE PERFORMANCE OF LINEAR EUS, ENDOSCOPIST ASPIRATE ASSESSMENT, FLUID CYTOLOGY, AND FLUID TUMOUR MARKERS IN THE DIAGNOSIS OF PANCREATIC CYSTIC LESIONS
K. Oppong, D. Richardson, M. Egan, D. Manas, B. Jaques, C. O’Sullivan, R. Charnley.Pancreato-Biliary Unit, Freeman Hospital Newcastle upon Tyne, UK
Background: Mucinous cystadenomas (MCA) and intraductal papillary mucinous tumours (IPMT) carry significant malignant potential while serous cystadenomas (SCA) have an extremely low malignant potential. Accurate differentiation between these lesions is important in ensuring appropriate management.
Aims: To assess the clinical utility of linear EUS morphology, aspirate appearance, cytology, and fluid markers in differentiating mucinous from non-mucinous cystic neoplasms.
Methods: A prospective audit of all patients referred for EUS assessment of a pancreatic cystic lesion, during the last 18 months at our Regional Pancreatobiliary Centre. Individuals with significant pretest suspicion of a pseudocyst were excluded. FNA was performed in all lesions with a 22 g or 19 g needle and cyst contents sent for cytology and (where possible) fluid sent for amylase, CEA, CA19/9, and CA-125 assay. Fluid appearance (thin v viscid) was recorded. All procedures were performed as day cases. IV antibiotics were given pre procedure and oral ciprofloxacin for 3 days post procedure.
Results: Thirty six procedures were performed in 34 individuals; 22 females and 11 males. Mean age 61 years (range 33–88). There were no procedural complications. A postulated EUS diagnosis was recorded in 18 patients. Fluid appearance was recorded in 28 procedures. Fluid markers were assayed in 23 patients. A final diagnosis based on surgical histology (9) or clinical outcome (6) is available in 15 cases, surgery is pending in a number of other patients. The diagnoses were MCA 5, IPMT 3, SCA 2, and Pseudocyst 5. The accuracy, sensitivity, and specificity of cytology for mucinous lesions was 91%, 100%, 75%, EUS diagnosis 90%, 100%, 50% and aspirate appearance 92%, 100%, 86%. Amylase >5,000 U/l had 100% accuracy, sensitivity, and specificity for pseudocyst. Tumour markers were assayed in seven of the 15 but only one of the surgically proven mucinous neoplasm. CEA was not elevated in this patient.
Conclusion: Linear EUS, visual aspirate assessment and cytology showed high accuracy and sensitivity for mucinous cyst. Aspiration of sufficient (viscid) cyst contents for biochemical and tumour markers was not always possible. Although numbers are small CEA assay was not found to be useful.
191 DEVELOPMENT OF A DISEASE SPECIFIC QUALITY OF LIFE SCORE QUESTIONNAIRE FOR PATIENTS WITH GASTROINTESTINAL NEUROENDOCRINE TUMOURS
A. H. G. Davies, J. K. Ramage, L. Friend, L. Jones, J. Ardill, G. Larsson, M. Falconi, R. Bettani, M. Koller, O. Sezer, C. Fleissner, B. Taal.Carcinoid Clinic, King’s College, NHH Basingstoke, Royal Liverpool, RVH Belfast, UK, Uppsala University Sweden, Verona, Italy, Marburg, Berlin, Germany, Amsterdam, the Netherlands
Introduction: Quality of life measurements are increasingly being used as an end point in clinical trials especially those involving patients with malignant diseases. Neuroendocrine tumours of gut origin give rise to symptoms not only from the presence of tumour in the liver (pain, ascites, pressure) but also from the output of the various hormones secreted by these tumours. There is therefore the need to develop a disease specific quality of life score questionnaire to supplement the already validated European Organisation for the Research and Treatment of Cancers core questionnaire (QLQ–C30).
Aim: To develop a disease specific quality of life score questionnaire for patients with neuroendocrine tumours of the gut to supplement the EORTC core cancer questionnaire QLQ–C30.
Method: Phase 1–3 of the EORTC quality of life study group guidelines for module development was used.
Results: Forty one relevant issues (questions) were generated after an extensive literature search. After a semistructured interview of 15 healthcare workers and 35 patients operationalisation of the questions was performed resulting in a 35 question provisional questionnaire. This questionnaire was translated into seven European languages and tested in 180 patients with neuroendocrine tumours of the gut. After analysis a final questionnaire of 20 questions was produced and this will be validated and used in clinic trials in the future.
Conclusion: This supplement to the core questionnaire is the only tool available specifically for gut related NETs, reflects patients’ views, and should be sensitive in detecting small changes in quality of life as a result of treatment or disease progression.
192 PRESSURE CHANGE IN THE RAT PANCREAS DURING ACUTE PANCREATITIS
E. W. Seward, M. Reynolds, E. Yazaki, D. F. Evans, C. C. Ainley.Wingate Institute, Barts and the London, Whitechapel E1 2BB, UK
Introduction: Data from models of the pathogenesis of acute pancreatitis (AP) describe the characteristic cellular and biochemical changes as an early occurrence—within a few hours of AP induction. Pancreatic ductal hypertension may play a role in AP, and addition of dietary alcohol is known to make induced AP worse. The time frame of pressure change associated with AP has not been described. We hypothesised that AP would be characterised by a pressure rise within hours and that this rise would be higher in more severe forms of AP.
Methods and Results: All experiments were performed on female rats under terminal anaesthesia with Home Office approval. A perfused manometer was sited in the common pancreatobiliary duct at laparotomy. Bile flow was obstructed completely with a hilar stitch. Pancreatic secretary volume was measured by cannulating the duodenum. AP was induced by two intraperitoneal injections of 50 μg/kg cholecystokinin (CCK) one hour apart and measurements taken for 5 hours in total. Controls were given saline. Experiment 1: saline controls (n = 8) v CCK rats (n = 7). Experiment 2: alcohol fed rats (making 36% of standard calorie requirements over a four week period, n = 7) v pair fed, chow fed controls (n = 8). Both groups had AP induced by CCK as above.
Amylase and histological analysis (graded 0–4 for oedema, necrosis, and vacuolisation) of the pancreas were assessed. Statistical analysis was by Student’s t test or Mann-Whitney U test (see table).
Abstract 192
Conclusions: CCK induced AP produces an early intraductal pressure rise associated with an increased secretary volume. Alcohol feeding produces a histologically more severe AP without these volume and manometric changes, suggesting that increased pancreatic duct pressure is not a necessity for AP under all conditions.
Oesophagus posters
193 RAMAN SPECTROSCOPY: ILLUMINATION OF BIOCHEMICAL CHANGES IN CARCINOGENESIS WITH POTENTIAL ENDOSCOPIC APPLICATION
G. Shetty1,2, C. Kendall1, B. Warren3, K. Geboes4, N. Shepherd5, N. Stone1, H. Barr1,2.1Biophotonics Research Group; 2Department of Surgery, Gloucestershire Royal Hospital, Gloucester, UK; 3Department of Pathology, John Radcliffe Hospital, Oxford, UK; 4Universitaire Ziekenhuizen, Leuven, Belgium; 5Department of Pathology, Gloucestershire Royal Hospital
Background: We have demonstrated the potential of Raman spectroscopy for the identification and classification of malignant changes in oesophagus. However, there is no clear recognition of the biochemical changes that distinguish between the different stages of malignant progression. Our aim is to understand these changes through Raman mapping studies.
Methods: Raman spectroscopy was used to analyse 87 oesophageal biopsies from 44 patients. Spectral results were correlated with the consensus opinion of three pathologists using multivariate statistical analysis. Raman spectral mapping was used to analyse 20 micron sections of tissue, on calcium fluoride slides, from 30 snap frozen oesophageal biopsies taken from 22 patients. Principal component analysis was used to identify the major differences between the spectra across each map.
Results: Raman classification models developed with eight pathology groups demonstrated sensitivity 73–100% and specificity 90–100%. Pseudocolour maps of the principal component scores have been generated and the peaks of the corresponding loads identified enabling visualisation of the biochemical changes associated with malignancy.
Conclusions: Raman spectroscopy is a highly sensitive and specific technique for demonstration of biochemical changes in carcinogenesis of Barrett’s oesophagus. The technique is now being developed into an endoscopic probe for real time endoscopic optical diagnosis.
194 THE EFFECT OF TEGASEROD ON OESOPHAGEAL FUNCTION: A RANDOMISED CONTROL TRIAL IN HEALTHY VOLUNTEERS
M. Fox1, I. Hampele2, B. Stutz3, M. Fried3, W. Schwizer3.1St Thomas’ Hospital, London, UK; 2Novartis, Basel, Switzerland; 3Division of Gastroenterology, University Hospital Zürich, Switzerland
Introduction: Gastro-oesophageal reflux disease (GORD) is characterised by abnormal lower oesophageal sphincter (LOS) function and oesophageal dysmotility; functional abnormalities that increase oesophageal acid exposure. Tegaserod is a 5-HT4 receptor partial agonist with prokinetic effects on gastrointestinal motor function. Tegaserod as an adjunct to acid suppression in GORD reduces postprandial oesophageal acid exposure (Kahrilas APT 2000). The mechanism by which acid exposure was reduced is unknown.
Patients and Method: 18 healthy volunteers entered a randomised, placebo controlled, cross over trial of tegaserod 6 mg twice daily. (Zelmac®, Novartis, Basel, Switzerland). Four hour combined high resolution manometry (HRM) and pH (2 hours fasting and 2 hours postprandial) with continuous recording of oesophageal body and LOS function, gastric and distal oesophageal pH, was performed at the end of each seven day treatment period. Primary outcomes were LOS pressure, peristaltic function, and distal oesophageal acid exposure. Additionally HRM combined with videofluoroscopy examined the effects of tegaserod on oesophageal clearance for liquid and solid bolus.
Results: After the test meal LOS pressure reduced, distal contraction pressure fell and peristaltic duration decreased (all p<0.01). Tegaserod had no effect on LOS pressure, marginally increased contraction pressure (58 v 57 mm Hg, p = 0.048) and significantly increased peristaltic velocity (an 8% rise, p<0.001). In these healthy subjects transient oesophageal LOS relaxations and reflux episodes were very infrequent regardless of treatment. Tegaserod had no effect on bolus transport for liquid barium but reduced the incidence of bolus escape for marshmallow solid bolus (66% v 31%; p<0.01). There was no interaction between prandial phase and treatment.
Conclusion: In healthy volunteers tegaserod (Zelmac®) 6 mg twice daily did not effect LOS function but had prokinetic effects on oesophageal motility, and improved oesophageal clearance for solid bolus.
195 DNA DAMAGE, RISK FACTORS, AND DISEASE PROGRESSION IN BARRETT’S OESOPHAGUS
J. R. Olliver1, L. J. Hardie1, Y. Y. Gong1, S. Dexter2, D. Chalmers3, K. Harris4, M. Cowan5, C. P. Wild1.1Molecular Epidemiology Unit and 2Academic Unit of General Surgery, Medicine and Anaesthesia, University of Leeds, UK; 3Gastroenterology Unit and 4Department of Radiology, Leeds General Infirmary, Leeds LS2 9JT, UK; 5Castle Hill Hospital, Cottingham, Hull HU16 5JQ, UK
Introduction and Aim: Oesophageal adenocarcinoma develops on a background of Barrett’s oesophagus. A number of risk factors have been linked to both conditions, including gastro-oesophageal reflux and smoking. This study investigated if such risk factors generate promutagenic DNA damage in the esophagus.
Method: Following ethical approval, the comet assay was used to measure DNA damage in endoscopic biopsies from control, Barrett’s oesophagus and oesophageal adenocarcinoma patients. Patients completed a questionnaire detailing exposure to some of the known risk factors for and Oesophageal adenocarcinoma.
Results: In Barrett’s oesophagus patients, DNA damage was higher Barrett’s oesophagus (mean % tail DNA, 23.3%; 95% CI, 21.7 to 25.0%) compared with normal oesophageal (15.1%; 95% CI: 13.6 to 16.8%; p<0.001) and gastric mucosa (20.1%; 95% CI: 18.1 to 22.3%; p<0.001). In addition, the highest quartile of DNA damage in Barrett’s mucosa was associated with an increased risk (OR 9.4; 95% CI: 1.1 to 83.4; p = 0.044) of developing adenocarcinoma or high grade dysplasia compared with DNA damage levels in the lowest quartile. Smoking and current reflux symptoms resulted in higher levels of DNA damage whilst anti-inflammatory drug use resulted in lower levels.
Conclusion: Collectively these data are consistent with a continuous genotoxic insult in the Barrett’s mucosa that may, in part, explain the genetic instability in this tissue and its increased risk of disease progression. There is an indication for a role for smoking in inducing DNA damage in oesophageal mucosa but an understanding of the role of reflux requires further investigation, as does the potentially protective role of anti-inflammatory drugs.
This work was supported by Yorkshire Cancer Research (L281).
196 OXIDISED PROTEINS, RISK FACTORS, AND DISEASE PROGRESSION IN BARRETT’S OESOPHAGUS
J. R. Olliver1, C. P. Wild1, S. Dexter2, D. Chalmers3, K. Harris4, M. Cowan5, L. J. Hardie1.1Molecular Epidemiology Unit and 2Academic Unit of General Surgery, Medicine and Anaesthesia, University of Leeds, UK; 3Gastroenterology Unit and 4Department of Radiology, Leeds General Infirmary, Leeds LS2 9JT, UK; 5Castle Hill Hospital, Cottingham, Hull HU16 5JQ, UK
Introduction and Method: Oxidative stress is being increasingly implicated in the pathogenesis of gastro-oesophageal reflux, Barrett’s oesophagus, and oesophageal adenocarcinoma. Following ethical approval, protein oxidation, as measured by protein carbonyl levels, was quantified in biopsies from control, Barrett’s oesophagus, and oesophageal adenocarcinoma patients by ELISA.
Results: Among the Barrett’s oesophagus group the mean level of carbonyl groups was significantly raised in the Barrett’s (0.136 nmols/mg protein; 95% CI: 0.110 to 0.161 nmols) compared with matched gastric (0.113 nmols; 95% CI: 0.092 to 0.135 nmols; p = 0.024) but reduced in comparison to matched squamous mucosa (0.163 nmols; 95% CI: 0.138 to 0.188 nmols; p = 0.056). A similar pattern of oxidation was observed in the oesophageal adenocarcinoma group. In the Barrett’s oesophagus and oesophageal adenocarcinoma groups there were significant positive correlations (p<0.05) in the levels of protein carbonyls measured in matched Barrett’s and squamous, and Barrett’s and gastric mucosa. Comparison across groups revealed increased levels of carbonyl groups in the squamous tissue of the Barrett’s oesophagus and oesophageal adenocarcinoma patient groups compared with the control group. Positive associations were observed between the presence of a hiatus hernia (p<0.05), tobacco smoking (p<0.05), alcohol use (p<0.05), and protein carbonyl level whilst a negative association was observed with current use of proton pump inhibitor medication (p<0.05).
Conclusion: These data support an association between Barrett’s oesophagus and oxidative stress with increased levels of protein carbonyls measured in the squamous mucosa of Barrett’s oesophagus and oesophageal adenocarcinoma patients compared with controls.
This work was supported by Yorkshire Cancer Research (L281)
197 IMPACT OF TREATMENT ON BARRETT’S CANCER INCIDENCE
P. A. C. Gatenby, J. R. Ramus, C. P. J. Caygill, A. Watson.UK National Barrett’s Oesophagus Registry (UKBOR), Department of Surgery, Royal Free and University College Medical School, London NW3 2PF, UK
Introduction: Goals of therapy in Barrett’s columnar lined oesophagus (CLO) include symptom control and prevention of complications. Small uncontrolled series have suggested that fundoplication may confer a protective effect against adenocarcinoma development. This study utilises the large numbers in UKBOR to investigate this hypothesis.
Methods: Medical records of 546 patients from seven UK centres with biopsy proven CLO and ⩾1 year of histological follow up were examined. Patients were grouped into those who had undergone antireflux surgery (n = 32), PPI+/− H2RA therapy (n = 436), and H2RA therapy alone (n = 78). The rates of progression to adenocarcinoma (AC) or high grade dysplasia (HGD) were examined using log linear analysis.
Results: Total follow up was 2977 patient years. Mean follow up >5 years in all treatment groups. A total of 27/546 patients developed incident HGD/AC: 21/436 patients treated with PPI+/− H2RA; 6/78 patients treated with H2RA only; and 0/32 patients treated with antireflux surgery. p = 0.067 for antireflux surgery v medical therapy (see fig).
Conclusions: The apparent protection by antireflux surgery just failed to reach statistical significance over medical therapy. Only a randomised controlled trial could resolve this.

Abstract 197
198 INVESTIGATION OF BACTERIAL COLONISATION OF THE SMALL BOWEL IN PATIENTS WITH BARRETT’S OESOPHAGUS USING 16S RRNA GENE SEQUENCE ANALYSIS
S. Macfarlane1, E. Furrie1, G. T. Macfarlane1, J. F. Dillon2.1Microbiology and Gut Biology Group, and 2Department of Gastroenterology, University of Dundee, Dundee DD1 9SY, UK
Background: Barrett’s oesophagus is a complication of chronic gastroesophageal reflux disease in which patients are at risk of oesophageal dysplasia and adenocarcinoma.
Aims: To characterise bacteria present in small intestinal aspirates and those colonising mucosal surfaces in patients with Barrett’s oesophagus compared with controls with normal or inflamed oesophageal mucosae.
Methods: Biopsies and aspirates were obtained during endoscopy from seven Barrett’s oesophagus patients, seven patients with a normal oesophagus, and three patients with either oesophagitis or reflux. Samples were serially diluted and plated on a range of selective culture media for both anaerobic and aerobic isolation of bacteria, including H pylori. Bacterial isolates were identified by 16S rRNA gene sequencing. Fluorescent in situ hybridisation (FISH) was also used to determine the spatial localisation of these organisms on the mucosal surface.
Results: Mucosal colonisation was detected in six Barrett’s oesophagus patients, in all patients with an inflamed oesophagus, and in four of the normal patients. Both aspirate and biopsy samples from Barrett’s oesophagus were found to contain complex populations of bacteria, with many isolates being common to both sites. These included normal members of the oropharyngeal microflora (streptococci, staphylococci, lactobacilli). Uniquely, high levels of atypical campylobacteria (C mucosalis, C concisus, C rectus) which have been linked to enteritis and periodontal infections were found to colonise 57% of the Barrett’s oesophagus patients (4/7). H pylori was not detected in any of the patients. Microscopy demonstrated that the bacteria were able to colonise the mucosal surface and were not simply the result of passive transfer.
Conclusion: Unusual pathogenic bacteria have been found on mucosal surfaces in patients with Barrett’s oesophagus. These organisms may be involved in either initiation, maintenance, or exacerbation of the disease process.
199 DO PATIENTS WITH REFLUX FOLLOW DOCTOR’S ADVICE? A LONG TERM STUDY OF PATIENTS PROTON PUMP INHIBITOR USAGE FOLLOWING ENDOSCOPY
A. Murdock, G. B. Turner, T. C. K. Tham.Division of Gastroenterology, Ulster Hospital Dundonald, Belfast, N. Ireland, UK
Background: For patients with simple reflux symptoms endoscopy can evaluate the degree of oesophagitis helping to plan long term medical therapy. However there are few studies evaluating whether patients follow the endoscopist’s medical advice post endoscopy.
Methods: 100 consecutive patients underwent a diagnostic endoscopy. Following endoscopic assessment of the degree of oesophagitis, therapy was stepped up, remained unchanged, or stepped down. At contact one year later patients were asked how they were taking their proton pump inhibitors (PPI) and adequacy of symptom control.
Results: 65 (65%), 32 males and 33 females, were contactable. 30 patients were under 55 years old, 35 over 55 years. Overall 39 of the 65 patients (60%) complied with their treatment one year after endoscopy. In the under 55 age group 14 patients (47%) complied with their treatment. In the over 55 age group 25 patients (71%) complied with their treatment. In total, 11 of the 65 patients (17%) remained symptomatic (see table).
Abstract 199
Conclusion: One year after endoscopy for reflux disease 60% of patients contacted have continued to take their PPI as initially recommended after the procedure. The majority of patients (83%) remain symptom free either on or off their PPI.
200 EVALUATION OF TREATMENT FOR ACHALASIA IN A DISTRICT GENERAL HOSPITAL 1990–2004
S. A. Hughes, R. J. Ede.Darent Valley Hospital, Dartford, UK
Background: Achalasia is a primary oesophageal motility disorder, causing dysphagia, regurgitation, vomiting, and chest pain. Few prospective long term comparative trials of therapy exist on which to base recommendations about current treatment.
Aims: To determine patient demographics, patterns of presentation, and effectiveness and complications of various treatment modalities in patients with achalasia.
Patients and Methods: All patients diagnosed with achalasia based on typical manometric and/or radiological findings were included. Severity of symptoms before and after treatment was assessed using a symptom score, based on dysphagia, chest pain, and vomiting.
Results: 24 patients (12 M, 12 F) aged from 18 to 92 years (median 59 years) were studied. Dysphagia was the most common presenting symptom (79%), followed by chest pain/heartburn (54%) and vomiting (50%). Most patients presented with two or three symptoms (66%). 21 patients (88%) underwent pneumatic dilatation (PD) and two (8%) received botulinum toxin injection. There was a positive correlation between basal lower oesophageal sphincter pressure and initial symptom score. There was no difference in initial symptom scores in those aged under and over 50 (p = 0.7). Average symptom scores all improved with the first and subsequent treatments. The symptom score after the first treatment in those under 50 was 2.57/9 v 4/9 in those over 50 (p>0.05). The average number of treatments required was 2.82 in those under 50 v 1.62 in those over 50 (p = 0.15). 67% of those treated first with the 30 mm balloon required more than one procedure v 46% in those treated first with the 35 mm balloon. 55% of patients under 50 complained of post-procedural increase in acid reflux, as compared with 0% in those over 50 (p = 0.001). There was one perforation in a total of 52 procedures over 14 years. One patient was referred for elective Heller’s myotomy after three PD.
Conclusions: Balloon dilatation and botulinum toxin are safe and effective treatments for achalasia in all age groups. Younger patients should be warned of the likelihood of post-procedural increase in acid reflux, and the need for more than one procedure.
201 THE EFFECTS OF AGE ON OESOPHAGEAL MOTILITY AND RELUX SEVERITY
J. T. M. Lee, M. Fox, T. Wong, R. Anggiansah, A. Anggiansah.Department of Gastroenterology and Oesophageal Laboratory, St Thomas’ Hospital, London, UK
Introduction: The effects of increasing age on lower oesophageal sphincter (LOS) function, peristaltic motility, and the severity of gastro-oesophageal reflux (GOR) are uncertain.
Aim: To investigate the association age on oesophageal dysmotility and 24 hours reflux severity (%time pH<4) in patients with reflux symptoms referred for manometry and pH studies.
Method: A retrospective study of 1307 consecutive patients with reflux disease referred to a tertiary referral centre 2000 to 2004. Full data were available for 985 (75%). Manometry assessed LOS pressure, abdominal, and total LOS length by 1 cm stationary pull through, and peristalsis by ten 5 ml water swallows. Hiatus hernia was defined as the absence of an abdominal LOS. Peristaltic dysmotility was classified as hypotensive (<40 mm Hg), non-transmitted (NT) or simultaneous contraction (SC). The pH probe was placed 5 cm above the LOS for 24 hours ambulatory pH studies. Univariate and multivariate regression assessed the association of age with the physiological measurements. Group comparisons were used to identify variation within the age range.
Results: The median age was 49 years (range 15–102). All associations were consistent across the age range. Age had no independent effect on LOS pressure or total LOS length but was associated with decreasing abdominal length (p<0.01)/increasing prevalence of hiatus hernia (p<0.03). Peristaltic dysmotility increased with age (p<0.01), predominantly due to increased prevalence of SC. Reflux severity (%time pH<4/24 h) increased with age (p<0.001) equivalent to an ∼1%/24 h increase in acid exposure every decade, an effect that was more pronounced in the supine position (p<0.01).
Conclusion: Age was associated with an increase in reflux severity, especially in the supine position. These changes were accompanied by a steady decrease in abdominal LOS length/increase in hiatus hernia prevalence and deterioration in peristaltic motility. Increasing oesophageal acid exposure with age may be the consequence of structural changes at the gastro-oesophageal junction/reflux barrier and impaired oesophageal clearance.
202 A SYSTEMATIC REVIEW AND META-ANALYSIS OF THE SEX RATIO FOR BARRETT’S OESOPHAGUS, EROSIVE REFLUX DISEASE AND NON-EROSIVE REFLUX DISEASE
M. B. Cook, C. P. Wild, D. Forman.
Introduction: Barrett’s oesophagus is associated with reflux disease and substantially increases the risk of oesophageal adenocarcinoma. All of these conditions have been reported to be more commonly diagnosed in males. Although the sex ratio of oesophageal adenocarcinoma is routinely documented, there has been no systematic consideration of the sex ratio for Barrett’s oesophagus or reflux disease. We undertook, therefore, a systematic review and meta-analysis of the sex ratio for Barrett’s oesophagus, erosive reflux disease (ERD), and non-erosive reflux disease (NERD) in order to compare these results with the sex ratio for oesophageal adenocarcinoma.
Methods: Medline (1966–2004), Embase (1980–2004), and Medline in Process were searched for relevant citations using a highly sensitive search strategy. Studies to be included required a sample size of ⩾50 patients, consecutive recruitment at an institute accessible by all and no obvious signs of bias in the recruitment process or numbers reported. Authors of papers which met the selection criteria, but were ineligible due to omitted data, were contacted; responses were included in the analysis. Stata 8.2 was used to conduct random effect meta-analyses. Excess heterogeneity was investigated by univariate meta-regression.
Results: The Barrett’s oesophagus meta-analysis included 32 studies and gave an overall pooled male: female sex ratio of 1.96:1 (95% CI 1.77 to 2.17:1). For ERD the pooled sex ratio was 1.57:1 (95% CI 1.40 to 1.76:1) from 28 studies, and for NERD it was 0.72:1 (95% CI 0.62 to 0.84:1) from 14 studies. The variables, study design, study size, and year of study were found not to have a significant effect upon the heterogeneity, whilst definition of Barrett’s oesophagus (columnar lined or specialised intestinal metaplasia) (p = 0.046), and geographical location (p<0.005) were significant effect modifiers.
Discussion: The meta-analysis estimates for ERD and Barrett’s oesophagus, while showing an excess of males, are substantially lower than similar estimates for oesophageal adenocarcinoma. It is important to establish why male Barrett’s oesophagus and ERD patients are at increased risk of malignancy compared with females.
203 OESOPHAGEAL ADHESIVE SOLUTIONS OF ALGINATE PROTECT AGAINST DAMAGE CAUSED BY GASTRIC REFLUX
M. Tang1, P. W. Dettmar2, H. K. Batchelor1.1Medicines Research Unit, Aston University, Birmingham, UK; 2Technostics, The Deep Business Centre, Hull, UK
Previous work has demonstrated that solutions of alginate may adhere to the oesophagus for up to 60 min.1 This work measured their ability to protect the oesophageal epithelial surface from damage caused by refluxed acid and pepsin. The rate of acid and pepsin diffusion through solutions of sodium alginate was measured using in vitro techniques.
Vertical Franz diffusion cells were used to measure the rate of diffusion of acid and pepsin through solutions of sodium alginate of low, medium, and high MW. A set volume of alginate solutions was evenly dispersed at the interface between the donor and receptor of the Franz cell. The donor contained 30 ml of acid or the acidic pepsin solution and the receiver contained distilled water. At set time points a 1.5 ml sample was collected from the receptor and replaced with the same volume to ensure the sink conditions. The concentration of the pepsin in each sample was determined using UV spectrometer according to a calibration curve set up previously. Acid diffusion was monitored directly via a pH meter.
The rate of both acid and pepsin diffusion was significantly reduced (ANOVA analysis; p<0.05) in the presence of an alginate solution compared with the control. A 2% w/v alginate solution in a layer of 0.44 mm depth, demonstrated the greatest reduction in acid diffusion with a permeation coefficient 14% that of a control value. The rate of acid diffusion was linked to the alginate composition rather than the MW with alginates with a high guluronic composition demonstrating the best protection. Pepsin diffusion was also significantly reduced as the depth (38% of control value at 0.22 mm and 18% of control value at 0.88 mm) and concentration (40% of control value at 1% w/v and 12% of control value at 4% w/v) of applied alginate increased. This study demonstrates that an adhesive layer of alginate present within the oesophagus will limit the contact of refluxed acid and pepsin with the epithelial surface.
1
204 AN IN VITRO EXAMINATION OF ADHESIVE ALGINATE SOLUTIONS AS OESOPHAGEAL PROTECTANTS
M. Tang1, P. W. Dettmar2, H. K. Batchelor1.1Medicines Research Unit, Aston University, Birmingham, UK; 2Technostics, The Deep Business Centre, Hull, UK
Introduction and Aim: Previous in vitro work reported by Batchelor et al1 stated that aqueous solutions of alginate adhere to oesophageal epithelium for up to 60 min. These adhesive layers minimise transfer of acid and pepsin, and thus offer protection to the oesophageal epithelium from gastric reflux.2 This study used microscopy to visualise the in vitro injury by acid and pepsin in gastric reflux and the protection offered by liquid sodium alginate.
Method: The upper epithelial layer of porcine oesophagus was isolated via immersion of the whole tissue in saline solution for 1 min at 60°C. The isolated epithelium was placed on a Transwell insert (diameter = 1.5 cm) and 2.5 ml acid or acidified pepsin solution was dispensed on the surface either in the presence or absence of 0.04 ml alginate, paired epithelium sections were used as a control. Acid solutions of pH 1, 2 and 3 were investigated and solutions of 0.1, 0.2 and 0.3% m/v pepsin (at pH 1). After 1 hour, the epithelium was removed, sectioned, and stained (H&E). A ZEISS microscope was used to view the surface damage and capture images. Score assessment criteria were set up (0 = no damage, 2 = slight damage, 4 = moderate damage, 6 = significant damage, 8 = serious damage). The images were randomly numbered. Ten volunteers were asked to assess the score for each photo according to the criteria. The score results were analysed statistically (ANOVA).
Results and Conclusion: The damage at low pH was significantly greater than high pH (Score: 5.5 (SD 0.9) at pH 1 v 1.5 (SD 0.9) at pH 3). In addition, higher concentrations of pepsin increased the epithelium damage (Score: 7.7 (SD 0.5) at 0.3% w/v v 3.7 (SD 0.8) at 0.1% w/v). The presence of alginate on the tissue surface demonstrated lower damage score in all cases including three pHs and three concentration of pepsin and significantly reduced damage compared with the control (p<0.05, ANOVA).
1
2
205 NORMALISATION OF LOWER OESOPHAGEAL PH AN IMPOSSIBLE GOAL IN SOME PATIENTS WITH BARRETT’S OESOPHAGUS?
C. Gordon, P. Sattianayagam, P. Neild, J. D. Maxwell, J. Y. Kang.Department of Gastroenterology, St George’s Hospital, London, UK
Background: The current endpoint in acid suppression treatment of patients with Barrett’s oesophagus is symptom abolition. Some authorities have suggested that Barrett’s oesophagus can be reversed with normalisation of the lower oesophageal pH profile.
Aims: To assess 24 hour lower oesophageal pH profiles in patients with Barrett’s oesophagus, rendered asymptomatic on proton pump inhibitors (PPIs), and to determine if abnormal acid profiles in these patients can be reversed by increasing their acid suppression treatment.
Methods: 24 hour dual lower oesophageal and gastric pH studies were performed on patients with Barrett’s oesophagus who were asymptomatic taking PPIs. Those in whom the acid profile was abnormal were invited to have repeat studies after intensification of their acid suppression regimen. A normal 24 hour oesophageal acid study was defined as 1) total time pH<4 less than 4.1% and 2) DeMeester score <14.75.
Results: 27 patients were recruited (18 M, 9 F, mean age 62): 26/27 (92%) had persistent nocturnal acid breakthrough on the first 24 hour study; 9/27(33%) had a normal oesophageal acid profile at recruitment on: omeprazole 20 mg once daily (1), lansoprazole 15 mg once daily (2), lansoprazole 30 mg once daily (4), lansoprazole 30 mg twice daily (1), esomeprazole 20 mg once daily (1). The remainder had abnormal studies on; omeprazole 20 mg once daily (5), omeprazole 20 mg twice daily (1), lansoprazole 15 mg once daily (2), lansoprazole 30 mg once daily (6), lansoprazole 30 mg twice daily (2), esomeprazole 40 mg once daily (2). Of these, nine had further studies after adjustment to their acid suppression treatment. Lower oesophageal pH profiles were normalised in five but remained abnormal in four patients despite maximal doses of PPI and histamine-2 receptor antagonists (Esomeprazole 40 mg bd ± ranitidine 300 mg at bedtime). All four patients continued to have nocturnal acid breakthrough.
Conclusion: Many patients with Barrett’s oesophagus have abnormal intra-oesophageal acid profiles despite being asymptomatic on treatment. Normalization of the oesophageal acid profile may not be possible despite maximal acid suppression with currently available agents, in up to 30% of patients.
206 RANDOMISED CONTROLLED TRIAL OF PHOTODYNAMIC THERAPY USING LOW DOSE 5 AMINOLEVULINIC ACID ACTIVATED BY RED OR GREEN LIGHT FOR HIGH GRADE DYSPLASIA IN BARRETT’S OESOPHAGUS
C. R. Selvasekar, G. D. Mackenzie, B. R. Clark, M. R. Novelli, S. M. Thorpe, C. A. Mosse, S. G. Bown, L. B. Lovat.National Medical Laser Centre, Department of Surgery, Royal Free and University College School of Medicine, London, W1W 7EJ
Background: Photodynamic therapy (PDT) is an ablative therapy for dysplasia in Barrett’s oesophagus. In our preliminary study using red laser (1000 J/cm diffuser fibre), aminolevulinic acid (ALA)-PDT 60 mg/kg eradicated high grade dysplasia (HGD) in 80% of patients at two year follow up. Others have shown that ALA at 30 mg/kg activated by green laser light can successfully treat low grade dysplasia in Barrett’s oesophagus. We hypothesise that, for HGD, red light is better than green but that 30 mg/kg ALA is as effective as 60 mg/kg. Our RCT compares ALA-PDT activated by red or green light.
Methods: Any dysplastic nodules were removed by EMR and ALA PDT was given if HGD remained. Patients were randomised to green or red laser treatment applied 4 hours after oral ALA administration. Patients received up to three treatments with PDT one month apart, and those who failed were offered ‘salvage’ PDT with 60 mg/kg ALA (red light).
Results: 16 patients with HGD were recruited (8 patients/group). Four underwent EMR. 37 PDT treatments were given (18 red, 19 green) with no major complications. Median follow up is 18.5 months (12–26 months). Dysplasia was eradicated after 5/18 (28%) treatments using red light and 1/19 (5.3%) using green light (p = 0.08 NS). Five patients had salvage PDT with ALA 60 mg/kg. 4/5 (80%) remain free from HGD at median follow up 12 months. The trial was stopped following interim analysis.
Conclusion: PDT with ALA at 30 mg/kg activated with green or red laser is ineffective for eradication of HGD in Barrett’s oesophagus. We recommend only high dose (60 mg/kg) ALA treatment for HGD.
207 CIRCUMFERENTIAL RESECTION MARGIN INVOLVEMENT IS A POOR PROGNOSTIC FACTOR IN OESOPHAGEAL MALIGNANCY
E. A. Griffiths1, Z. Brummell1, S. Pritchard2, I. M. Welch1.1Department of Gastrointestinal Surgery and 2Department of Histopathology, South Manchester University Hospitals NHS Trust, Manchester, UK
Introduction: Involvement of the circumferential resection margin (CRM) is known to be a poor prognostic factor in rectal cancer surgery. However, the results in oesophageal surgery have been conflicting. Our aim was to assess the effect on survival of CRM involvement in patients with resected oesophageal malignancy.
Methods: The cases of 243 patients who underwent a potentially curative oesophagectomy were analysed. Pathological details such as TNM stage, differentiation, CRM status, and overall stage were collected. Univariate and multivariate survival analyses were performed using the Kaplan-Meier method and Cox proportional hazard model.
Results: CRM status was clear in 164 patients and for 79 patients tumour was within 1 mm. Median survival in these groups were 33 and 18 months, respectively (p = 0.002). When stratified by N stage, CRM status was of more prognostic significance in N0 stage (p = 0.015) than N1 stage (p = 0.23). The hazard ratio for risk of death from oesophageal cancer was 1.68 (95% CI 1.2 to 2.3) for those with CRM involvement. Age and overall TNM stage, but not CRM status, were independent prognostic factors on multivariate analysis.
Conclusion: Involvement of the CRM predicts poor prognosis in patients with resected oesophageal malignancy. It has more prognostic significance in patients without lymph node metastases. It should continue to be routine to report this highly prognostic variable.
208 IMPACT OF GOVERNMENT GUIDELINES ON SURVIVAL OF PATIENTS WITH OESOPHAGEAL CARCINOMA
A. Cairns, J. Keating, C. Brown, A. Higham, N. Mapstone, E. Stewart, H. Pratt, B. Teague, C. Ball.Departments of Medicine, Surgery and Histopathology, Morecambe Bay Hospitals NHS Trust, Cumbria, England, UK
Background: Guidelines to fast track patients to dedicated upper gastrointestinal (GI) centres may improve survival of patients with oesophageal malignancy.
Aims: To examine the patients’ journey from GP to surgery or palliative care in patients with suspected oesophageal carcinoma.
Methods: One hundred patients with histologically proven oesophageal malignancy diagnosed from January 2002 to March 2004 were studied. We analysed any delays in the system: from initial symptoms to GP consultation, from GP consultation to seeing a specialist.
Results: 66% of patients were male with a mean age of 69 years, and 34% were female with a mean age of 72 years. Histological type was adenocarcinoma in 84% and squamous carcinoma in 14%. The majority of patients presented with dysphagia (76%). There appeared to be a delay in a significant group of patients seeing their GP: only 33 saw their GP within one month of developing symptoms, of whom 18 (56%) were alive at 6 months, and 9 (27%) were alive at 12 months; for the 50 patients who presented to their GP with symptoms ranging from one to six months, 29 (58%) were alive at 6 months, and 18 (36%) were alive at 12 months (NS). Fifty five patients were seen within the two week cancer wait, of whom 34 (62%) were alive at 6 months and 21 (38%) were alive at 12 months. 37 patients were seen outside the two week cancer deadline of whom 22 (59%) and 14 (41%) were alive at 6 months and 12 months, respectively (NS). Forty patients underwent potentially curative surgery and 18 had a palliative operation. Ninety percent were alive at 6 months and 70% at 12 months (curative surgery).
Conclusion: The delay in patients self-referring to their GP did not adversely affect their survival. Patients seen within the two week cancer wait and those seen after this time deadline had a similar survival outcome. Delays in patients seeing their GP or seeing the specialist do not appear to alter outcome in oesophageal carcinoma.
209 IS TUMOUR LENGTH A PROGNOSTIC FACTOR IN RESECTED OESOPHAGEAL MALIGNANCY?
E. A. Griffiths1, Z. Brummell1, S. Pritchard2, I. M. Welch1.1Department of Gastrointestinal Surgery and 2Department of Histopathology, South Manchester University Hospitals NHS Trust, Manchester, UK
Introduction: Gastrointestinal specialists generally feel that long oesophageal tumours have a poorer prognosis. However the evidence to support this notion is limited. Our aim was to investigate the relationship between histologically determined length and aspects of tumour pathology together with survival for patients with resected oesophageal malignancy.
Methods: Histopathological reports for oesophageal malignancies resected in our unit between 1994 and 2003 were analysed. Pathological details such as TNM stage, differentiation, completeness of surgical resection, and overall stage were collected. Univariate and multivariate survival analyses were performed.
Results: 309 reports were analysed (72% adenocarcinoma, 23% squamous carcinoma, and 4% others). Median tumour length was 3.5 cm (range 0.5 to 14 cm). Tumour length greater than 4 cm was significantly associated with increasing T stage (p = 0.0001), N stage (p = 0.011), overall stage (p = 0.0001), and involvement of the longitudinal resection margin (p = 0.018). Univariate survival analysis found tumour length greater than 4 cm was associated with poor overall survival (p = 0.00001). Tumour length was also an independently poor prognostic factor on multivariate analysis (p = 0.018).
Conclusion: Tumour length greater than 4 cm (as determined histologically) is significantly associated with adverse pathological features and poor overall patient survival.
210 THE TISSUE INHIBITOR OF METALLOPROTEINASE-3 GENE IS METHYLATED DURING OESOPHAGEAL ADENOCARCINOMA DEVELOPMENT: LOSS OF PROTEIN EXPRESSION CORRELATES WITH POOR PROGNOSIS
L. J. Hardie1, S. J. Darnton2, R. S. Muc3, C. P. Wild1, A. G. Casson4. (introduced by Forman D).1Molecular Epidemiology Unit, School of Medicine, University of Leeds, Leeds LS2 9JT, UK; 2Oesophageal Research Laboratory, Department of Thoracic Surgery and 3Department of Histopathology, Birmingham Heartlands Hospital, Birmingham B9 5SS, UK; 4Division of Thoracic Surgery, Dalhousie University and QE II Health Sciences Centre, Halifax, Nova Scotia, B3H 2Y9, Canada
Introduction: Tissue inhibitor of metalloproteinase-3 (TIMP-3) is an inhibitor of several matrix metalloproteases and in vitro studies suggest it can inhibit tumour cell growth and metastasis and induce apoptosis. The TIMP-3 gene may be silenced by methylation during the development of oesophageal adenocarcinoma (OA), but the expression and location of TIMP-3 protein and its association with clinicopathological features have yet to be described in OA.
Method: TIMP-3 gene methylation and mRNA expression were analysed in five oesophageal cell lines and 24 resected OAs. The association between TIMP-3 protein expression and clinicopathological features was assessed in a series of 79 resected OAs.
Results: TIMP-3 methylation was only detected in the OE33 OA cell line. In case matched tissues, 0% of normal mucosa, 72% of Barrett’s mucosa, and 90% of OAs were methylated for TIMP-3. TIMP-3 mRNA was detected in all the cell lines and normal, metaplastic, and tumour tissues. TIMP-3 protein was localised to the cytoplasm in cell lines and tissues. At the invading edge of tumours, protein staining was equal to, or reduced, compared with normal tissues. Reduction of TIMP-3 protein expression was associated with disease stage (p = 0.046) and poor patient survival (OR 2.1, 95% CI 1.2 to 3.5, p = 0.007). Mean survival time was halved in patients with reduced tumour TIMP-3 expression, from 49 to 24 months.
Conclusion: Methylation of the TIMP-3 gene is associated with the development of OA. Reduced expression of TIMP-3 protein in OA is associated with increased tumour invasiveness and reduced patient survival.
Neoplasia posters
211 HELICOBACTER PYLORI STIMULATED EPITHELIAL ERK PHOSPHORYLATION IS REDUCED BY THE SPECIFIC EGFR INHIBITOR EKB-569
Y. Du, K. Danjo, A. H. T. Jeremy, P. A. Robinson, J. E. Crabtree.Molecular Medicine Unit, St James’s University Hospital, UK
Introduction:H pylori activates multiple signalling pathways in gastric epithelial cells, including transactivation of the EGF receptor (EGFR) and activation of MAP kinases, extracellular signal related kinases 1 (ERK1) and ERK2. H pylori activation of the EGFR signalling pathway may be relevant to the epithelial hyperproliferation and increased risk of gastric carcinogenesis associated with infection. The aims of this study were to evaluate whether H pylori induced phosphorylation of ERK (pERK) is via the EGF receptor.
Methods:H pylori (G27, cag PAI+) and a cagM- isogenic mutant (H12-5A) were co-incubated with A431 epithelial cells for 45 min, 1.5 hours, or 3 hours. Cells pre-incubated with the EGFR inhibitor EKB-569 (0.001–1 μM) were co-cultured with H pylori for 3 hours. EGF (25 ng/ml) and untreated/EKB-569 treated cells were used as positive and negative controls, respectively. Total ERK and pERK status was simultaneously quantified in situ using two colour “in cell western blot” analysis.
Results: Both G27 and H12-5A significantly increased pERK in A431 cells compared with unstimulated controls. Maximum pERK was observed at 1.5 hours (G27, 205.1 (SD 10.9) v 100.0 control, n = 12, p<0.001; H12-5A, 210.6 (SD 13.6), n = 12, p<0.001) and similar high levels of pERK were observed at 3 hours with both strains. EKB-569 dose dependently inhibited pERK induced by both strains. Inhibition of H12-5A induced pERK was observed at 10 nM EKB-569 (174.0 (SD 32.5) v 242.4 (SD 21.1) untreated control, n = 3 paired t test, p<0.03) and inhibition increased at 100 nM EKB-569 (145.2 (SD18.4), p<0.003). EKB-569 similarly inhibited H pylori G27 stimulated ERK phosphorylation.
Conclusion: ERK activation was induced by H pylori strains with and without a functional cag PAI, and could be partially blocked by the specific EGFR inhibitor EKB-569. Two colour “in cell western” analysis represents a useful tool to evaluate inhibitors of H pylori cell signalling pathways of relevance to gastric carcinogenesis.
212 PURE ISOMERS OF CONJUGATED LINOLEIC ACID CAN REDUCE COLONIC TUMOUR NUMBER BUT MIXED ISOMERS INCREASE TUMOUR SIZE IN A MOUSE MODEL OF INTESTINAL CANCER
N. Mandir, R. A. Goodlad.Cancer Research UK, Histopathology Unit, 44 Lincoln’s Inn Fields, London
Introduction: Dietary conjugated linoleic acids (CLA) have been implicated in altered fat metabolism and body weight. They may have a role in the prevention of intestinal neoplasia and moderate colitis through the PPARγ receptor. The predominant forms are the cis-9, trans-11 (c9t11) and trans-10, cis-12 isomers (t10c12). The c9t11 isomer, which is present in ruminant meat, has been reported to be the more beneficial. The effects of various forms of CLA were investigated in the multiple intestinal neoplasia (ApcMin/+) mice, which have a mutation of the APC gene, as in FAP in man.
Methods: Five week old ApcMin/+ mice were fed a control diet or diets with 1% of c9t11, t10c12, or a mix of the isomers (n = 20 per group). After 28 days the mice were killed and the intestines opened, spread on filter paper and fixed in Carnoy’s fluid. The number and size of polyps in the small and large intestines was scored as were vincristine arrested metaphases and crypt fission.
Results: The stomach and small intestine were significantly heavier in the t10c12 and mix treated groups (p<0.001). t10c12 and the mix significantly reduced polyp number, in the proximal small intestine (p<0.001). t10c12 and the mixture increased polyp diameter in the mid and distal small intestine (p<0.05 to 0.001) so that the polyp burden was in turn significantly increased (p<0.05 for t10c12 and 0.01 for the mixture). All the CLA’s reduced polyp number in the colon (from 9.1 (SD1.6) to 4.4 (SD 0.7), 3.6 (SD0.8), and 3.0 (SD0.6), p<0.01), but the mixture significantly increased polyp diameter in the colon (38% p<0.05).
Conclusion: All the CLA’s could reduce polyp number, especially in the colon, however t10c12 and the mixture increased polyp diameter and thus tumour burden. It is a cause of concern that the mixture is the version that is generally commercially available. c9t11 did not alter diameter, lending weight to the suggestion that this natural isomer of CLA is beneficial.
213 A MECHANISM FOR CYCLOOXYGENASE-2 MEDIATED REGULATION OF APOPTOSIS IN COLORECTAL CANCER CELLS; THE ROLE OF DRAK2, A DEATH ASSOCIATED PROTEIN KINASE
G. A. Doherty1,2, S. M. Byrne1,2, S. C. Austin1, G. M. Scully1, T. G. Neilan1, E. W. Kay3, F. E. Murray2, D. J. Fitzgerald1.1Department of Molecular Medicine, Conway Institute for Biomolecular and Biomedical Research, University College Dublin; 2Departments of Gastroenterology and 3Histopathology, Beaumont Hospital, Dublin, Ireland
Introduction: Cyclooxygenase-2 (COX-2) is over expressed in the majority of colorectal tumours; a property which renders them resistant to apoptosis. The mechanisms by which COX-2 modulates apoptosis have not been well characterised. We have identified DRAK2, a pro-apoptotic serine threonine kinase, as regulated by COX-2 in cancer cells.
Method and Results: DRAK2, a death associated protein kinase was identified by triplicate oligonucleotide microarrays as consistently upregulated in HCA7 cells following treatment with SC-236, a selective COX-2 inhibitor. Quantitative PCR (qRT-PCR) confirmed this induction of DRAK2 transcription (4.4 fold increase, p = 0.02), an effect that was reversed by co-treatment with PGE2. Upregulation of DRAK2 protein in HCA7 cells was confirmed by immunofluorescence microscopy. DRAK2 mRNA levels are suppressed in human colorectal tumours (n = 10) relative to normal colorectal mucosa (mean decrease of 50%, p = 0.001), and show a negative correlation with COX-2 expression. Treatment of patients with colorectal cancer (n = 5) with a selective COX-2 inhibitor for 5–7 days causes upregulation of DRAK2 transcription in tumour tissue (2.6 fold increase, p = 0.004). Silencing of DRAK2 expression in HT-29 cells (mirroring the effect of COX-2) was achieved by RNA interference (mean reduction in DRAK2 expression of 70%, p = 0.02). DRAK2 silencing renders these cells more resistant to apoptosis induced by SC-236, but not by the apoptosis inducer staurosporine (n = 3).
Conclusion: DRAK2, a novel pro-apoptotic kinase, is regulated in vitro and in vivo by COX-2 and this regulation may explain some of the anti-neoplastic activity of COX-2 inhibitors in colorectal cancer.
214 NEUROENDOCRINE TUMOUR IMAGING: SOMATOSTATIN RECEPTOR SCINTIGRAPHY V 123I-MIBG SCINTIGRAPHY
A. M. Quigley, M. E. Caplin, T. Shah, A. J. W. Hilson, J. R. Buscombe.Neuroendocrine Tumour Unit, Royal Free Hospital, London, UK
Background: It is commonly believed that when scintigraphic imaging of neuroendocrine tumours (NETs) is performed somatostatin receptor scintigraphy, using 111In-pentreotide (SRS), is always superior to 123I-MIBG. However, our experience suggests that the situation may be more complex.
Objectives: To determine the extent of rate of disconcordance between SRS and MIBG scintigraphy in patients with NETs.
Methods: Planar and SPECT SRS and MIBG scintigraphy of 141 patients with histologically proven NETs were assessed retrospectively by a single reviewer to determine the number and site of lesions for each scan in the same patient. Scans were performed between Jan 2000 and May 2004.
Results: In 45/141 patients (32%) there was concordance between both examinations, in both the number and distribution of the lesions identified. In 96/141 (68%) of patients, the scans were discordant. Of these 96 patients: 25 (26%) had more lesions on the SRS; 29 (30%) had lesions demonstrated on the SRS alone; 18 (19%) had more lesions identified on the MIBG scan; and six (6%) had lesions on the MIBG scan alone. In the remaining18 patients (19%) both scans were positive but different lesions were identified on each of the two scans.
Conclusions: The large number of discordant SRS and MIBG scintigraphy in this study serves to highlight the need to perform both scans in patients with NETs, particularly if therapy is being considered. In a small, but clinically significant group of patients, the MIBG scintigraphy may be positive when the SRS is negative. We are currently investigating the NET subtypes and their biological characteristics e.g. proliferation index. The fact that different lesions were identified on each of the two scans in some patients, suggests that NET patients are likely to possess more than one population of tumour cells. The reasons for these differences require further investigation.
215 EGFR EXPRESSION AND ACTIVATION IN NEUROENDOCRINE TUMOURS
T. Shah, R. Frow, A. Quaglia, A. Dhillon, D. Hochhauser, M. Caplin.Neuroendocrine Tumour Unit, Royal Free Hospital, London
Introduction: The epidermal growth factor receptor (EGFR) is abnormally activated in many epithelial tumours. This results in the recruitment and phosphorylation of several intracellular substrates. One such pathway involves extracellular signal regulated kinases ERK1 and ERK2. Another important pathway involves phosphatidylinositol-3 kinase (PI3K) and the downstream protein serine/threonine kinase Akt. The phosphorylation/activation of ERK1/2 and Akt leads to a cascade of responses resulting in cell growth, proliferation, survival, transformation, and motility. EGFR inhibition with anti-EGFR antibody and/or small molecule EGFR-tyrosine kinase inhibitors has shown promise in in vitro, in vivo, and clinical studies. However the expression/activation of EGFR, and its consequences, have not been assessed in neuroendocrine tumours (NETs).
Aims: To determine the role of EGFR in NETs: by demonstrating its expression, its activation, and the subsequent activation of downstream pathways involving ERK1/2 and Akt.
Methods: 3 μm sections of formalin fixed paraffin embedded tumour tissue were obtained from patients with all forms of NETs (foregut, midgut, and hindgut). Immunohistochemical evaluation was performed for the expression of EGFR (n = 85), activated (Tyrosine1068-phosphorylated)-EGFR (n = 37), activated (Serine473-phosphorylated)-Akt (n = 41), and activated (Threonine183 and Tyrosine185- diphosphorylated)-ERK1/2 (n = 46). The antibody binding was visualised by using DAB peroxidase substrate kit. The sections were counterstained with Mayer’s haematoxylin for 5 min. All sections were independently read by one histopathologist.
Results: Of the NET tissue samples assessed: 92% were positive for EGFR expression; 81% were positive for activated EGFR; 78% were positive for activated Akt; and 98% were positive for activated ERK1/2.
Conclusion: We have demonstrated the presence of EGFR in the majority of patients with NETs, as well as the subsequent activation of EGFR and the activation of downstream indicators of tumour survival and progression. We are further investigating the role of EGFR inhibition in the treatment of NETs.
216 GLYCINE-EXTENDED GASTRIN STIMULATES PROLIFERATION AND INHIBITS APOPTOSIS IN COLON CANCER CELLS VIA MULTIPLE PATHWAYS
O. Ogunwobi, I. L. P. Beales.Gastroenterology Unit, Norfolk and Norwich University Hospital and School of Medicine, University of East Anglia, UK
Glycine extended gastrin (G-Gly) is an alternative end product of processing of the progastrin precursor protein. Recent evidence suggests that G-Gly has a different spectrum of biological activities to classical amidated gastrin. G-Gly promotes cell proliferation in normal and malignant colonic epithelium, and is produced by colon cancers suggesting an autocrine action. NSAIDs appear to protect against colon cancer. Several mechanisms are involved in the latter but both inhibition of cyclo-oxygenase and apoptosis induction are important. We have examined the mechanisms of G-Gly induced proliferation, in particular the involvement of cyclo-oxygenase related pathways.
Methods: HT-29 cells were cultured with G-Gly. Cell number and viability were assessed by colormetric assays. Intracellular signalling pathways were examined using specific inhibitors and ELISAs for activated intermediates. Apoptosis was assessed by nucleosome ELISA.
Results: G-Gly caused an increase in cell proliferation (maximum 35% above basal) that was insensitive to inhibition of either COX-1, COX-2 or the epidermal growth factor receptor, but was abolished by inhibition of phosphatidylinositol-3 kinase (PI3 kinase) with LY294002. Higher concentrations of celecoxib reduced cell number by inducing apoptosis. G-Gly reversed the apoptotic effect of serum starvation and ameliorated the effect of celecoxib. Inhibition of PI3 kinase, extracellular signal related kinase (ERK) (with PD98059), p38 MAP kinase (with SB203580), c-Jun-NH2 kinase (with SP600125) or NF-κB (with BAY 11-7082) abolished the protective effect of G-Gly. G-Gly increased nuclear translocation of NF-κB.
Conclusions: Glycine extended gastrin promotes proliferation and survival of colon cancer cells. Production of G-Gly either by normal G-cells or neoplastic tissues might reduce the beneficial chemo-preventative effects of celecoxib. The protective effects of G-Gly involve activation of the ERK, p38, and JNK mitogen activated protein kinase cascades, PI3 kinase, and NF-κB.
217 LARGE SERIES PROSPECTIVE EXPERIENCE WITH EUS FOR POST-CHEMOTHERAPY STAGING OF OESOPHAGEAL CANCER. TIME TO ANSWER THE QUESTION OF CLINICAL VALUE
L. Doig, J. Meenan, C. Vu.Guy’s and St Thomas’ Hospitals, Department of Gastroenterology, Lambeth Palace Road, London SE1 7EH, UK
Background: Neo-adjuvant chemotherapy increasingly is being used in the management of oesophageal cancer. Predicting tumour stage prior to curative resection based on EUS and CT is problematic due to the presence of inflammatory tissue. The detail permitted by EUS may be however superior to CT in predicting local resectability. The clinical value of EUS in this setting has been the subject of several small studies lacking the power to give a definitive answer.
Aim: To prospectively assess the clinical value of EUS in the pre-operative staging of oesophageal cancer post neo-adjuvant chemotherapy.
Methods: Patients with oesophageal cancer were prospectively enrolled in a study comprising initial staging with EUS and CT, followed by neo-adjuvant chemotherapy and subsequent repeat EUS and CT prior to curative surgery. Maximum TNM stages were given.
Results: 119 patients entered the study: 86 had surgery (mean age 62 years; male: 69, female: 17). The comparative accuracy rates of maximal T and N staging were 76.7%, 58.1% for EUS, and 67.4% (p = 0.227), 51.2% (p>0.50) for CT, respectively. The sensitivity, specificity, PPV and NPV of EUS in detecting T4 disease were 25%, 97.4%, 50%, and 92.7%, respectively.
Conclusion: EUS is not significantly better than CT for staging in post-chemotherapy patients. Although specific for detecting T4 disease, the sensitivity of EUS is too low to make it a useful tool in post-chemotherapy staging of oesophageal cancer.
218 THE ROLE OF 99M-TECHNETIUM DEPREOTIDE IN SCANNING NEUROENDOCRINE TUMOURS
T. Shah, J. Buscombe, M. Caplin.Neuroendocrine Tumour Unit, Royal Free Hospital, London, UK
Background: Neuroendocrine tumours (NETs) express somatostatin receptors which can be utilised for tumour imaging as well as for tumour targeted radiotherapy. 111Indium- pentetreotide (OcteoScan®) is widely used for imaging and is associated with 67–95% sensitivity. It may also identify lesions not clinically or radiologically suspected, however, some lesions may not be positive, and other lesions may become negative with time. This is likely due to the absence or loss of somatostatin receptor subtype 2 (sstr2), which octreotide binds with high affinity, and is particularly likely to occur following alterations in tumour phenotype, that is progression from low grade to high grade tumour. Depreotide is a new somatostatin analogue which binds sstr2/3/5 with high affinity and therefore, has a broader sstr subtype binding profile than octreotide. 99m-Technetium depreotide is now available for radio-isotope imaging of tumours and has been found to be useful in diagnosis of small cell and non-small cell lung cancer.
Aim: To assess the usefulness of 99mTc depreotide scintigraphy in patients with negative or weakly positive111In-pentetreotide scans (Krenning scale ⩽1 (range 0–4)).
Study Design: 12 patients, with histologically proven NETs, were recruited to undergo paired 111In-pentetreotide and 99mTc-depreotide scans. The results were also compared with radiological imaging.
Results: Histology confirmed 66% of tumours to be intermediate grade and 44% to be high grade. Six patients were positive for 99mTc depreotide alone. Four patients were positive for both 111In-pentetreotide and 99mTc-depreotide but the two imaging modalities highlighted different lesions and the 111In-pentetreotide scans were weakly positive (Krenning scale 1). Eight patients were negative for 111In-pentetreotide. Of these, two patients were negative for both 111In-octreotide and 99mTc-depreotide but with clear CT evidence of tumour suggesting negativity for sstr subtypes 2, 3, and 5.
Conclusion: 99mTc-depreotide is a significant new imaging modality in NET patients with intermediate/high grade tumours with no or limited uptake using 111In-pentetreotide. It may identify a group of patients amenable to radionucleotide therapy targeting sstr subtypes 3 and 5 as well 2.
219 GENETIC DELETION OF MACROPHAGE MIGRATION INHIBITORY FACTOR HAS NO SIGNIFICANT EFFECT ON INTESTINAL TUMORIGENESIS IN THE APCmin/+ MOUSE
J. M. Wilson1, N. Scott2, P. L. Coletta1, M. A. Hull1.1Molecular Medicine Unit, University of Leeds; 2Department of Histopathology, St James’s University Hospital, Leeds, UK
Introduction and Aim: We have previously demonstrated that expression of macrophage migration inhibitory factor (MIF) is increased in human colorectal adenomas and intestinal adenomas of the ApcMin/+ mouse model of familial adenomatous polyposis. Moreover, exogenous recombinant human (rh) Mif decreases apoptosis and promotes anchorage independent growth of VACO-235 human colorectal adenoma cells in vitro. Therefore, we tested the hypothesis that genetic deletion of Mif would abrogate ApcMin/+ mouse intestinal tumorigenesis.
Methods:Mif ‘knockout’ mice were obtained from John David (Boston, MA). ApcMin/+ x Mif−/− mice were derived on a mixed C57BL6 x 129 background and compared with age matched ApcMin/+ littermates with wild type Mif alleles. Intestinal adenoma multiplicity and size (diameter) were measured with a dissecting microscope at 120 days of age. Analysis was performed blind to the genotype in all cases.
ApcMin/+ mice with wild type Mif alleles (n = 19) had 35.1 (SD 5.4) adenomas in the small intestine (SI) and 1.7 (SD 0.3) adenomas in the colon. There was no significant difference in SI (26.1 (SD 4.3); p = 0.19; Student’s unpaired t-test) or colonic (1.3 (SD 0.3); p = 0.33) adenoma multiplicity in ApcMin/+ x Mif−/− animals (n = 24). Mean adenoma diameter in Mif-/- proximal (n = 60 tumours), middle (182), and distal (350) SI or colon (32) was reduced between 1–7% compared with Mif+/+ adenomas (proximal n = 78; middle 189; distal 434; colon 33). The difference in adenoma size related to genotype reached statistical significance only in the middle SI (p = 0.04).
Conclusion: Genetic deletion of Mif does not have a major effect on the early stages (adenoma initiation and progression) of intestinal tumorigenesis in the ApcMin/+ mouse, despite rhMIF having ‘tumorigenic’ activity on human colorectal adenoma cells in vitro. We hypothesise that MIF may play a more significant role at later stages of tumorigenesis (eg adenoma to carcinoma transition) not observable in the ApcMin/+ mouse model.
220 GASTROINTESTINAL CARCINOID TUMOURS—A FIVE YEAR EXPERIENCE FROM A DISTRICT GENERAL HOSPITAL
A. Shah1, R. Singh2, M. M. Ahmed1.1Departments of Gastroenterology and 2Pathology, Good Hope Hospital, Sutton Coldfield B75 7RR, UK
Introduction: Gastrointestinal carcinoid (GIC) is a relatively uncommon tumour affecting neuroendocrine cells.
Aims: We reviewed our total experience of GIC over a five year period in a district general hospital (DGH) setting.
Methods and Patients: All patients with a histological diagnosis of GIC between January 1999 and January 2004 were identified from our pathology database. Notes and computerised records of these patients were reviewed and demographic, clinical, management, and outcome data were analysed.
Results: 32 patients (16 Male, median age 53.5 years, range 23–73 years) were identified. Modes of presentations were: acute/subacute small bowel obstruction (4), abdominal pain (8), dyspepsia (2), anaemia/microcytosis (12), diarrhoea (3), haemotochezia (1), and others (2). Only one patient had a raised urinary 5-HIAA. The site of the primary tumour was: stomach (6), small bowel (9), appendix (8), ileocaecum (6), colon (1), and rectum (2). Only one patient (with an ileocaecal primary) had liver metastasis at presentation but did not have symptoms of carcinoid syndrome. Treatments instituted were: surgical resection of primary tumour +/− lymph nodes (26), endoscopic mucosal resection of gastric carcinoid (2), medical treatment only with proton pump inhibitors (1), and conservative management (3). Patients were followed up for a median of 34 months (range 7–68 months). The actuarial five year survival using Kaplan-Meier analysis was 89%. Two patients who had resection of small bowel carcinoid died (both 3 years post diagnosis) from unrelated causes (table).
Abstract 220
Conclusion: GIC is a rare tumour with a diverse range of presentations. GIC was managed surgically in the majority and the medium term prognosis is good.
221 CYCLO-OXYGENASE-2 IS A PROGNOSTIC BIOMARKER IN MID-GUT CARCINOID TUMOURS
I. S. Cadden, B. T. Johnston, G. B. Turner, D. R. McCance, J. E. S. Ardill, A. McGinty.Department of Medicine, Queen’s University Belfast, Mulhouse Building, RGH, Grosvenor Rd, Belfast, BT12 6BJ, N. Ireland, UK
Midgut carcinoids (MGC) are the most common and generally most aggressive of the gastrointestinal carcinoid tumours. Since the role of cyclo-oxygenase-2 (Cox-2) in the development of neuroendocrine tumours has not been adequately investigated, the current study evaluated Cox-2 and the Cox-2 dependent gene product Bcl-2 as tissue based prognostic biomarkers in MGC. Tissue from 37 patients was subjected to immunohistochemical detection of Cox-2 and Bcl-2. For Cox-2 intensity of staining was graded using a semi-quantitative scale from (−) indicating negative expression to (+++) indicating intense positivity. Cox-2 expression was demonstrated in 29/36 tumours. Cox regression analysis indicated a trend towards worse survival with increasing intensity of Cox-2 staining (p = 0.1: 1 year Cum Sur, 5 years Cum Sur; [−] 1.00, 0.42; [+] 0.88, 0.88; [++] 0.92, 0.67; [+++] 0.75, 0.25). When Cox-2 positive tumours were considered separately, significantly worse survival was noted with increasing staining intensity (p = 0.01). While, 9/35 tumours were positive for Bcl-2 expression, Kaplan-Meier analysis indicated that tumour associated Bcl-2 expression had no effect on patient survival (p = 0.82). There was no significant association between Cox-2 and Bcl-2 expression (χ2, p = 0.34). This study provides evidence that, in those MGC expressing Cox-2, similar to other solid tumours, high levels of Cox-2 expression are associated with adverse patient outcome.
222 FACTORS ASSOCIATED WITH GREATER LIKELIHOOD OF GASTROINTESTINAL MALIGNANCY IN PATIENTS WITH IRON DEFICIENCY ANAEMIA: RESULTS OF A PROSPECTIVE STUDY
S. Cherian, L. Bowler, N. Singh, M. Rahman, P. Singh.Department of Gastroenterology, Staffordshire General Hospital, Stafford, UK
Introduction: In a significant proportion of patients, iron deficiency anaemia (IDA) may be caused by gastrointestinal malignancy. For purposes of prioritization, it would be useful to identify factors in patients with IDA which are associated with a greater likelihood of gastrointestinal (GI) malignancy.
Methods: A fast track direct access service for investigation of GI tract of patients with IDA was set up in February 2002. A nurse specialist completed a proforma, which included data on patient demography, GI symptoms, and haemoglobin (Hb). IDA was defined as Hb <13 gm/dl for men and <12 gm/dl for women, with at least one of the following: ferritin <20 µg/l, MCV <78 fl, or transferrin saturation index <10%. In asymptomatic patients over the age of 45 years, the initial investigation was colonoscopy while upper GI endoscopy was the first investigation in younger subjects. In symptomatic patients, the nature of the symptoms determined the sequence of investigation. If the initial endoscopic investigation failed to reveal cancer, coeliac disease, or inflammatory bowel disease, the patient went on to have endoscopy of the other end of the GI tract. SPSS programme was used for logistic regression analysis with the diagnosis of cancer being the dependent variable and following putative dichotomous predictor variables: age (⩽45 v >45), sex, GI symptoms, and Hb (⩾10 v <10).
Results: 380 of 546 referrals during a 30 month period were available for analysis (inappropriate = 80, defaulters = 67, being processed = 19). The median age was 68 years with the interquartile range (IR) of 52 to 77. There were 140 men and 240 women. The median Hb was 9.5 (IR = 8.2 to 10.7). 170 patients had no GI symptoms. 58 patients had GI cancer (colorectal = 43, upper GI = 15). Age >45, male sex, and Hb <10 had a statistically significant association with GI cancer (p = 0.031, 0.001 and <0.001, respectively). The corresponding odds ratios were infinity, 2.9, and 4.4 with 95% CI of 2.7 to infinity, 1.6 to 5.1, and 2.1 to 10.2, respectively. Symptoms had no predictive value.
Conclusion: Over 15% of patients with IDA had GI cancer. Age >45, male sex, and Hb <10 were independently predictive of a greater likelihood of GI cancer. Symptoms had little predictive value. Patients with these characteristics should be given greater priority for full GI work up.
223 EXPRESSION OF PARATHYROID HORMONE RELATED PROTEIN AND THE PTH/PTHrP RECEPTOR IN HUMAN PANCREATIC ADENOCARCINOMA
M. McStay, K. Savage, M. Stubbs, K. Khan, A. Dhillon, M. Caplin.Royal Free and University College Medical School, London, UK
Background: Since its discovery as the factor primarily responsible for humoral hypercalcaemia of malignancy, it has become clear that parathyroid hormone related protein (PTHrP) has an important role in the growth and differentiation of neoplastic and non-neoplastic cells. However, little is known about the expression of PTHrP and PTH/PTHrP receptor (PTH1R) in pancreatic adenocarcinoma.
Aim: To assess the expression of PTHrP and PTH1R in human pancreatic adenocarcinoma resection specimens and cell lines.
Methods: Immunocytochemical localisation of PTHrP and PTH1R was performed by the APAAP method on paraffin sections from 18 consecutive, pre-operatively eucalcaemic, patients with well defined pancreatic adenocarcinoma, and on the pancreatic adenocarcinoma cell lines, Panc-1, BxPC3, and AR42J. Murine monoclonal antibodies to PTHrP (1–10) and PTH1R were used, and specificity was demonstrated by pre-absorbance of antibodies with epitope. Western immunoblotting, using anti-PTHrP (1–34), anti-PTHrP (38–64), and anti-PTH1R was used to assess the expression of PTHrP and PTH1R by the cell lines.
Results: There was positive cytoplasmic tumour cell staining for PTHrP and PTH1R in 17/18 and 16/18 of the tumour resection specimens, respectively. In 15/18 cases, there was positive staining for both PTHrP and PTH1R. PTHrP was localised in the cytoplasm of all cell lines. PTH1R was localised to the membrane and cytoplasm in BxPC3 and Panc-1 cells. Nuclear staining for PTHrP and PTH1R was also seen in 1–5% of BxPC3 cells. Cellular PTHrP was detected by western blotting in all of the cell line extracts. Cellular PTH1R was detected in the Panc-1 and BxPC3 lysates only.
Conclusion: PTHrP and PTH1R are expressed in human pancreatic adenocarcinoma. The expression of PTHrP peptide and receptor implies a paracrine/autocrine for PTHrP that may contribute to tumour progression and differentiation. If PTHrP is detectable in the circulation of patients with pancreatic cancer, it could serve as a useful tumour marker for the early detection of pancreatic adenocarcinoma.
224 PREVENTION OF ACID N-NITROSATION REQUIRES BOTH WATER AND LIPID SOLUBLE ANTIOXIDANTS
S. Paterson, T. Preston, G. Scobie, K. E. L. McColl.Western Infirmary, Glasgow, G11 6NT
Introduction: The predominant anatomical site of acid N-nitrosation is the gastro-oesophageal (GO) junction where nitrite and thiocyanate secreted in saliva first encounter acidic gastric pH. Ascorbic acid prevents the nitrosation by converting the nitrosating species to nitric oxide (NO). However, the NO is oxidised back to nitrosative species in the presence of lipid, overriding the protective effect of ascorbic acid.
Aim: To assess the effect of lipid antioxidants on nitrosative chemistry under conditions simulating the GO junction.
Methods: Nitrite (100 μmol), thiocyanate (1 mmol), and ascorbic acid (1 mmol) were added to 50 ml 0.1 M HCl pH 15. 5 ml of the lipid tributyrin was present on its own or with a lipid antioxidant (alpha-tocopherol, beta-carotene or butylated hydroxytoluene (BHT)) present at concentrations of 10 μM, 100 μM, 1 mM, 10 mM or 100 mM. The N-nitrosatable secondary amine morpholine was added to the aqueous and lipid phases at a concentration of 5 mmol. The concentration of N-nitrosomorpholine generated at 15 min was analysed by GCMSMS.
Results: In the absence of lipid antioxidant 4.3 (SD 0.4) μmol/l, N-nitrosomorpholine was detected in the 50 ml aqueous solution despite the presence of ascorbic acid. The addition of any of the three lipid antioxidants was able to completely inhibit N-nitrosation but there was a marked difference in the concentration required to achieve this. On a molar basis alpha-tocopherol was 100 times more effective than beta-carotene and 1000 times more effective than BHT.
Conclusions: Prevention of nitrosative stress occurring from the acidification of salivary nitrite at the GO junction requires the presence of adequate concentrations of both water and lipid soluble antioxidants. Alpha-tocopherol is the most effective lipid antioxidant in preventing N-nitrosation.
Gastroduodenal posters 225–234
225 TIME TRENDS IN HOSPITAL ADMISSION AND MORTALITY DUE TO PEPTIC ULCER IN SCOTLAND 1991–2002
C. Gordon1, A. Elders3, A. Majeed2, K. D. Bardhan4, J. D. Maxwell1, J. Y. Kang1.1Department of Gastroenterology, St Georges Hospital, London, UK; 2Department of Primary Care, Imperial College, London, UK; 3NHS National Services Scotland, Edinburgh; 4Department of Gastroenterology, Rotherham General Hospital, Rotherham, UK
Background: Despite the recent advent of potent acid suppressants and treatment for H pylori infection, time trends in hospital admission rates for peptic ulcer (PU) remain unclear. We have previously shown an increase among older people, especially for haemorrhage, over the 1990s in England, although there was little overall change. In contrast, hospitalization rates for PU fell in the USA over this period, irrespective of age.
Aims: To determine time trends in Scotland for hospital admissions and mortality for duodenal ulcer (DU), gastric ulcer (GU), as well as prescriptions for proton pump inhibitors (PPIs) and low dose aspirin, from 1991 to 2002.
Methods: Data on admissions, mortality, and community prescriptions were obtained from the Information and Statistics Division of the NHS National Services, Scotland.
Results: Between 1992 and 2002 hospital admission rates for GU and DU, whether overall or complicated, generally declined or remained stable in most age groups. However, admission rates for DU haemorrhage increased in those aged ⩾75 age group (males from 97.0 to 132.3/100 000/year, females from 37.6 to 63.4/100 000/year). Mortality rates fell uniformly across all age and diagnostic groups. Community prescriptions for low dose aspirin rose by 547% and those for PPIs by 1327%.
Conclusions: There are divergent trends in hospital admission rates for PU in Scotland for the period from 1991 to2002. While rates for most ages and diagnostic groups fell or remained stable, DU haemorrhage increased in both men and women over the age of 75. These findings are in line with those from England and may be due to an increase in the use of low dose aspirin.
226 DOES JOINT PRESCRIPTION OF ANTIDEPRESSANTS AND NSAIDS SUBSTANTIALLY INCREASE THE RISK OF UPPER GASTROINTESTINAL BLEEDING?
L. J. Tata1, P. J. Fortun2, R. B. Hubbard1, L. Smeeth3, C. J. Hawkey2, C. J. P. Smith4, H. J. Whitaker5, C. P. Farrington5, T. R. Card1, J. West1.1Departments of Epidemiology and Public Health; 2Wolfson Digestive Diseases Centre; 4Respiratory Medicine, University of Nottingham; 3Departments of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine; 5Department of Statistics, The Open University
Background: An over 10 fold risk of gastrointestinal bleeding has been reported with concurrent use of antidepressant and non-steroidal anti-inflammatory drugs (NSAIDS). Recent guidance has advised either caution or avoidance of joint prescription of these drugs, particularly in people aged over 80 years.
Methods: We conducted a case control study of 11 261 cases with upper gastrointestinal bleeding compared with 53 156 controls matched by gender, age and general practice obtained from The Health Improvement Network primary care dataset. We coupled this with a self controlled case series analysis.
Results: A two fold risk of gastrointestinal bleed was associated with both families of drugs (odds ratio (OR) = 2.09, 95% CI 1.91 to 2.28 for antidepressants and OR = 2.15, 95% CI 2.02 to 2.28 for NSAIDs). Concurrent prescription of these drugs was associated with a marginally higher risk (OR = 2.83, 95% CI 2.39 to 3.34). Estimates were no greater in people over 80 years of age and the magnitude of risk decreased with increasing comorbidity, which was not explained by preferential prescribing of gastroprotective drugs. The self controlled analysis showed a greater risk of gastrointestinal bleeding with NSAIDs (incidence rate ratio (IRR) = 2.64, 95% CI 2.46 to 2.84) than with antidepressants (IRR = 1.43, 95% CI 1.29 to 1.59). The risk when both drugs were combined was: IRR = 3.25, 95% CI 2.19 to 4.82.
Conclusions: Antidepressants and NSAIDs are associated with an increased risk of gastrointestinal bleeding. These risks are not substantially increased when both drugs are prescribed together. In contrast to recent advice, our study suggests that joint prescription of these drugs is reasonably safe, particularly in older populations.
227 NICE GUIDANCE WILL DELAY DIAGNOSIS OF CANCER IN PATIENTS OVER 55 WITH NEW ONSET DYSPEPSIA
A. Stokes, A. F. Goddard.Digestive Diseases Centre, Derby City Hospital, Derby DE22 3NE, UK
Background: NICE guidance suggests that patients with dyspepsia alone are at low risk of cancer and endoscopy should be avoided if possible whatever the age. The evidence for this approach in patients over 55 is contradictory. Avoidance of early endoscopy in patients over 55 with cancer will delay diagnosis by over 3 months if NICE guidance is followed.
Aim: To measure the prevalence of cancer in patients with new onset dyspepsia with or without alarm symptoms in patients over 55.
Methods: All referrals of patients over 55 to our trust (population served 400000) with new onset dyspepsia (excluding those with just reflux symptoms) were audited from October 2000 to September 2002. The presence of alarm symptoms and presence of cancer on subsequent investigation were measured (see table).
Abstract 227
Results: 480 patients were referred. 32 (6.7%) of these patients had cancer. Cancer sites were: oesophagus (13), stomach (4), pancreas (6), biliary tract (3), lung (2), ovary (1), colon (1), and unknown primary (2).
Conclusions: New onset dyspepsia in patients over 55 is associated with cancer in a significant percentage of patients and endoscopy must not be delayed by symptomatic treatments.
228 UPPER GASTROINTESTINAL HAEMORRHAGEASSOCIATED WITH LOW DOSE ASPIRIN AND ANTI-THROMBOTIC DRUGS—A SIX YEAR ANALYSIS AND COMPARISON WITH NON-STEROIDAL ANTI-INFLAMMATORY DRUGS
A. S. Taha, W. J. Angerson, S. Mair, R. P. Knill-Jones, O. Blatchford.Departments of Gastroenterology, Crosshouse Hospital – Kilmarnock, Surgery, and Section of Public Health and Health Policy, University of Glasgow, UK; Department of Public Health Medicine, Argyle; Clyde NHS Board, Scotland, UK
Background and Aims: Given the increasing use of low dose aspirin and other anti-thrombotic therapy for vascular protection, we assessed the possibility that the incidence of upper gastrointestinal blood loss has changed in subjects using these agents in comparison with non-steroidal anti-inflammatory drugs (NSAIDs).
Methods: We studied the characteristics of all patients with upper gastrointestinal haemorrhage and attending a single hospital at three points over a six year period: 1996 (n = 204); 1999 (n = 224); and 2002 (n = 252). The χ2 test, Fisher’s exact test, and the Mantel-Haenszel test for trend analysis were used where appropriate.
Results: The incidence of upper gastrointestinal haemorrhage in subjects taking ulcerogenic drugs (1996–2002), is shown in table 1 below (number per 100,000 of the population per annum). The mortality of acute conditions that might be affected by the above drugs is shown in table 2:
Abstract 228 Table 1
Abstract 228 Table 2
Conclusions: The incidence of upper gastrointestinal haemorrhage in users of low dose aspirin and other anti-thrombotic drugs has been steadily rising. It has been paralleled by a fall in cardiac mortality.
229 TEN YEAR FOLLOW-UP OF A COMMUNITY SCREENING AND TREATMENT PROGRAMME FOR H PYLORI
A. C. Ford1, A. G. Bailey1, D. Forman2, A. T. R. Axon1, P. Moayyedi3.1Leeds General Infirmary, Leeds, UK; 2Academic Unit of Epidemiology and Health Services Research, Leeds University, Leeds, UK; 3Gastroenterology Division, Health Sciences Centre, Hamilton, Canada
Introduction: Population screening and treatment of H pylori has been advocated as a means of reducing mortality from gastric cancer. If a reduction in dyspepsia and related health resource use could be demonstrated, it would add further weight to adoption of this strategy. Previous population ‘search and eradicate’ programmes have failed to demonstrate any such effect, but follow up was at one or two years. We have conducted a study to examine these outcomes at 10 years.
Methods:H pylori positive individuals previously enrolled in a community screening programme, and randomised to either eradication therapy or placebo, were contacted via postal questionnaire, and also asked for consent to examine their GP notes. Two people, blinded to original treatment allocation, extracted relevant consultation, referral, prescribing, and investigation data. Utilising UK 2002 reference costs and the BNF allowed a total cost per patient to be obtained.
Results: Of the 2329 original participants, 1864 (80%) were traced and sent questionnaires. Of these, 1086 (58%) responded. 919 (85%) agreed to their GP records being examined. Those symptomatic at baseline, showed a trend towards reduction in symptoms at 10 years with allocation to eradication therapy, but this was not statistically significant (relative risk (RR) = 0.89; 95% CI 0.77 to 1.03). There was a 10 year mean saving in total dyspepsia related costs of £57.06 (95% CI £2.79 to £116.92), and in dyspepsia related prescribing of £40.48 (95% CI £4.92 to £76.04) with allocation to eradication therapy. Those allocated to eradication therapy were significantly less likely to incur any dyspepsia related cost (RR = 0.72; 95% CI 0.66 to 0.80).
Conclusions: There is a significant cost reduction in dyspepsia related prescribing, and a trend towards a reduction in both symptoms of dyspepsia and total dyspepsia related health care cost at 10 years, for H pylori eradication therapy compared with placebo in community screening.
230 TH1 CYTOKINES, BUT NOT GASTRIN INCREASE HELICOBACTER PYLORI INDUCED APOPTOSIS IN SHORT TERM PRIMARY CULTURES OF MURINE GASTRIC GLANDS
S. M. C. Przemeck1, A. J. Watson1, A. Varro2, D. M. Pritchard1.1Division of Gastroenterology and 2Physiological laboratory, University of Liverpool
Background:H pylori induces gastric atrophy in susceptible strains of mice such as C57BL/6 which exhibit a Th1 predominant immune response. This process is accelerated in hypergastrinaemic INS-GAS mice. H pylori induces gastric apoptosis in vivo and it has been proposed that this contributes to the development of atrophic gastritis. We have therefore investigated whether the Th1 cytokines TNFα and interferon-γ, and the antral hormone gastrin modulate H pylori induced apoptosis in primary cultures of murine gastric glands.
Methods: Primary gastric glands were isolated by collagenase A digestion from adult male C57BL/6 mice and allowed to attach and spread in culture for 72 hours. Glands were then exposed to combinations of cytokines, gastrin, and H pylori for up to 48 hours. Apoptosis was detected in paraformaldehyde fixed glands by immunocytochemistry for active caspase 3 and in cultured cells by timelapse fluorescence video microscopy for Annexin V-FITC and propidium iodide. Apoptotic cells were scored and expressed as a percentage of cells within the gland.
Results: At 48 hours, 10–20% of cells in untreated glands stained positively for Annexin V and 5–8% stained positively for active caspase 3. Th1 cytokines at doses in the range from 100 ng/ml to 200 ng/ml increased apoptosis in a concentration dependent manner: interferon-γ up to three fold and TNF-α up to 1.5 fold at 48 hours. H pylori (multiplicity of infection approximately 100/epithelial cell) did not induce apoptosis by 48 hour, but co-treatment with H pylori and 100 ng/ml interferon-γ caused up to 20% of cells to stain positively for active caspase 3. 10 nM gastrin alone or in combination with H pylori did not induce apoptosis.
Conclusions: 1) Primary gastric glands derived from C57BL/6 mice do not undergo apoptosis following exposure to 100:1 H pylori; 2) Th1 cytokines, particularly interferon-γ induce gastric epithelial apoptosis and increase H pylori induced apoptosis; 3) gastrin has no effect upon H pylori induced apoptosis.
231 HELICOBACTER PYLORI REDUCES BIOPSY INDUCED MUCOSAL DAMAGE WITH ACUTE NAPROXEN IN HEALTHY VOLUNTEERS
M. W. James, C. T. Atherton, A. M. Zaitoun, C. J. Hawkey, J. C. Atherton.Wolfson Digestive Diseases Centre, University Hospital Nottingham
Introduction: Conflicting data exist on the acute effect of NSAIDs on mucosal injury in H pylori infection. H pylori infection results in gastric mucosal inflammation, up regulation of COX-2, and increased prostaglandin production. We hypothesized that acute naproxen administration would result in reduced biopsy associated injury in H pylori infected subjects compared with uninfected controls.
Methods: 16 healthy volunteers (12 positive and four negative for H pylori) entered a placebo controlled, blinded crossover study of 48 hours naproxen 500 mg twice daily (a non-selective NSAID) on acute biopsy induced injury in the gastric mucosa. Mapped antral mucosal biopsies were taken at baseline endoscopy and 3, 12 and 48 hours after starting treatment. Before biopsies were taken at each endoscopy, a biopsy site erosion score was recorded by the endoscopist blinded to treatment order for each subject.
Results: In four subjects not infected with H pylori, there were significantly higher median biopsy site erosion scores with naproxen compared with control at 3 hours (1 v 0), 12 hours (2.25 v 1) and 48 hours (2.25 v 1; p<0.01). In 12 subjects with H pylori infection there were also significantly higher median scores with naproxen compared with control at 3 hours (0.5 v 0.17), 12 hours (1 v 0.33) and 48 hours (1.17 v 0.33; p<0.01). However, during naproxen administration, those subjects with H pylori infection had significantly lower scores compared with those uninfected at 3 hours (0.5 v 1), 12 hours (1 v 2.25) and 48 hours (1.17 v 2.25; p = 0.011).
Conclusion: During acute administration of naproxen, there was significantly less biopsy induced mucosal injury in those with H pylori infection compared with those without. We conclude that H pylori infection reduces mucosal damage associated with acute NSAID ingestion and speculate that this may be due to increased mucosal prostaglandin production associated with infection.
232 UPREGULATION OF TISSUE INHIBITORS OF METALLOPROTEINASES-1 AND -3 IN THE GASTRIC MUCOSA IN H PYLORI INFECTION
S. Ahmad1, K. Bodger1,3, L. Pasmany3, A. L. Khan2, G. Dockray4, A. Varro4.1Aintree Centre for Gastroenterology and 2Department of Cellular Pathology, University Hospital Aintree, Liverpool, UK; 3Department of Medicine and 4Physiological Laboratory, University of Liverpool, UK
Background: Tissue inhibitors of metalloproteinases (TIMPs) are a family of protease inhibitors that regulate the activity of matrix metalloproteinases (MMPs) and have roles in inflammatory processes, extracellular matrix (ECM) remodelling, cellular proliferation and (in cancer) invasion and metastasis. We hypothesised that TIMPs may be upregulated in H pylori associated gastritis (either by inflammation or hypergastrinaemia), thereby promoting interstitial fibrosis and tissue remodelling—a key feature of the premalignant process of gastric atrophy.
Methods: Gastric biopsies were obtained at endoscopy. Antral and corpus biopsies were processed for histology, H pylori (HP) status, and Sydney scoring. Abundance of TIMP-1 to -4 (and MMP-8) mRNA and protein was determined in corpus biopsies by quantitative RT-PCR (relative to β-actin) and western blotting, respectively. Cellular sources were examined by indirect immunohistochemistry. Circulating gastrin was measured by RIA.
Results: Compared with uninfected controls (n = 14), mRNAs for TIMPs -1, -3, and -4 were significantly more abundant in the gastric corpus of HP-infected subjects (n = 13) (see table). Results for TIMPs-1 and -3 were supported by the western blot analyses. There were no significant differences in gastric TIMP expression between hyper- and normogastrinaemic subjects within the HP-negative and HP-positive groups. Immunostaining for TIMP-1 and -3: Epithelium: Surface: absent or focal; Glands: strong positive (esp. chief cells in HP+); Stroma: positive; Leucocytes: weak (TIMP-1), positive (TIMP-3).
Abstract 232 Gastric corpus mRNA expression
Conclusions: HP-infection is associated with upregulation of specific TIMPs, notably TIMPs -1 and -3 in glandular epithelium and stroma. Increased TIMP expression in the gastric mucosa may exert a pro-fibrotic influence on ECM remodelling, thereby contributing to the process of glandular atrophy.
233 CLOSING THE COSTS ON HELICOBACTER PYLORI
P. Prasad, K. Manoj, S. G. R. G. Barton.Department of Gastroenterology, Kent and Canterbury Hospital, Canterbury, Kent, UK
Background: Testing for and treating H pylori has proven benefits. Despite the changing incidence of H pylori, CLO biopsies remain a conventional method for identifying it. There are limited data on the resource implications of using disposable biopsy forceps (DBF) instead of reusable biopsy forceps (RuBF).
Aims: To identify the relative cost per positive CLO test between 1996 and 2004, and to assess the national cost of performing a CLO biopsy using DBF.
Methods: The results of 100 consecutive CLO tests were analysed for the years 1996, 1999, and 2004. In 1996 and 1999, CLO tests used RuBF, whereas in 2004 DBF were used. The direct cost of performing a CLO test and the estimated national costs of performing CLO tests were calculated. The relative cost per positive CLO test was compared between these years.
Results:1996: 28 positive CLO tests per 100 CLO tests performed; 1999: 19 positive CLO tests per 100 CLO tests; 2004: 11 positive CLO tests per 100 CLO tests. Assuming a cost of £5.20 per CLO kit, negligible costs for the RuBF and £12 per DBF, the cost per positive CLO test in 1996 was £18.57 compared with £27.37 per positive CLO test in 1999 and £156.36 per positive CLO test in 2004. This represents a cost difference of £137.79 and an 8.4 fold relative rise in the cost (since 1996) to identify a positive CLO test in 2004.
Conclusions: The cost per positive CLO test in 2004 was £156.36 compared with £18.57 in 1996, which represents an 8.4 fold rise attributable to the additional costs of using disposable biopsy forceps and the changing incidence of H pylori. This cost may be offset by the need to perform biopsies for additional pathology. BSG data suggest that the annual requirement for upper GI endoscopy in the general population is 1.5:100. Assuming 50% of the upper GI endoscopies performed in the general population will have a CLO test, the current direct cost per annum of performing CLO tests on the general population is estimated to be £7.7 million. This cost would rise to £15.4 million if a CLO test were performed routinely at every upper GI endoscopy. Further research is required to determine whether it remains cost-effective to perform CLO tests to detect H pylori.
234 CURRENT MORTALITY DATA FOR PATIENTS WITH AN UPPER GI BLEED. HAS ANYTHING CHANGED SINCE ROCKALL?
S. Hillyard, J. D. Linehan.Royal United Hospital, Combe Park, Bath BA1 3NG, UK
Introduction: In 1996 Rockall et al devised a scoring system predicting mortality and likelihood of rebleeding. In Bath a well established consultant led emergency GI bleed service has been established with 24 hours cover, 365 days per year. All patients admitted with a GI bleed are endoscoped within 24 hours and are usually admitted to a specialist GI ward. Our mortality data were compared with the Rockall score data.
Methods: Mortality for all patients with a GI bleed admitted to RUH with a GI bleed between January and November 2003. The Rockall scores for these patients were recorded prospectively. These data were compared with the original Rockall data.
Results: 393 patients were admitted to RUH and compared with Rockall data (n = 2956). Ages were analysed <60 years (RUH 31.6% v 31.2%), 60–79 (RUH 34.4% v 42.3%), and >80 (RUH 34.1% v 26.1%) (see table).
Abstract 234
Conclusion: Although our overall mortality data are comparable with the data from Rockall, it is not as good as some specialised units have been able to obtain in the last few years. A possible explanation for a higher mortality rate could be that a higher proportion of our patients were above 80. Our excess mortality rate was also primarily in patients with a Rockall score of 5 and 6. These patients with moderate GI bleeds were sometimes delayed in getting to the specialist GI ward. This adds weight to the provision of a specialised GI bleed unit with protected beds.
Endoscopy posters
235 TO BE OR NOT TO BE SEDATED? —THE EFFECT OF AGE AND GENDER ON AN INDIVIDUAL PATIENT’S LIKELY DECISION
A. P. Reynolds1, B. de la Iglesia1, G. D. Bell2, V. J. Cook2, R. Tighe2.1School of Computing Sciences, UEA, Norwich NR4 7TJ, UK; 2Endoscopy Unit, Norfolk and Norwich University Hospital, Norwich NR4 7UY, UK
Introduction: Non-sedated patients can usually be rapidly discharged whereas sedated patients require more intensive monitoring and spend a longer period on the endoscopy unit before discharge. In planning an outpatient (OP) list of OGDs or flexible sigmoidoscopys (FSs), there is thus some merit in trying to ensure that the last (as well as, preferably, the penultimate patient) on the list have opted not to be sedated. Patients undergoing OP diagnostic OGD or FS are, however, given a free choice as to whether or not they would prefer to be sedated. We wondered whether the data mining techniques we have employed to look at Endoscribe databases (Gut 2004 Suppl III A51) could help predict patient choice.
Methods and Results: Our endoscopy unit serves a population of 450 000 and carries out about 6500 OGDs and 1700 FSs per year. We took the Endoscribe database records of the last two years’ unit activity and studied the effect of patient age and sex on 1) their decision to be sedated and, if so, 2) the dose of midazolam used. Figures 1 and 2 show that female patients, particularly in the younger age groups, are much more likely to opt for sedation (p<0.001).

Abstract 235 figure 1

Abstract 236 figure 2
Discussion and Conclusions: The results suggest that in planning an OP list of OGDs or FSs, a case could be made for deliberately booking any younger, particularly female, patients relatively early on a list. Conversely, placing any older and particularly male patients nearer the end of the list should enhance efficiency and throughput.
236 CAN NURSE ENDOSCOPISTS SEDATE PATIENTS SAFELY?
V. Cambridge, J. D. Linehan.Royal United Hospital, Combe Park, Bath, BA1 3NG, UK
Introduction: Whether nurse endoscopists (NEs) can sedate patients with midazolam varies widely between NHS trusts. Traditionally NEs have been encouraged to endoscope pre-selected unsedated patients. This leads to administrative difficulties and limits their practice or requires doctors to sedate their patients. To enable our NE to perform colonoscopy and OGDs on all suitable patients, an “in house” training programme, pre-assessment tool, and sedation protocol was developed. If a higher dose of sedation was needed then a doctor would be needed to administer this for the NE.
Aim: To assess the use of sedation by the NE compared with an associate specialist with >10 years of experience.
Methods: Records of patients who had been endoscoped by the NE or by the associate specialist (AS) in a 12 month period were examined. AS was chosen as the endoscopic workload was similar. Midazolam dosage, frequency of fumazenil use, and complications were recorded.
Results: No significant difference in midazolam usage or reversal agents was noted. No serious complications happened in either group. Completion rate for colonoscopy was similar in both groups (85%) (see table).
Abstract 236
Conclusion: With training, and a protocol, NEs can give sedation safely as long as it takes place within a well supported environment, eg with proper monitoring and adequate recovery facilities, and may actually give less sedation. Nationally enabling NEs to sedate patients, it would give NEs the ability to endoscope a wider group of patients.
237 SEDATION FOR ENDOSCOPY: BIGGER SYRINGE, SMALLER DOSE
N. P. Galletly, D. M. Forton, D. S. Bansi, A. V. Thillainayagam.Department of Gastroenterology, Charing Cross Hospital, Fulham Palace Road, London, UK
Background: The majority of endoscopic procedures are performed under conscious sedation with a short acting benzodiazepine such as midazolam. There is increasing emphasis being placed on safe sedation practices, and the 2003 BSG Safety and Sedation During Endoscopic Procedures Guidelines recommend that the “dosage of benzodiazepines … should be kept to a minimum to achieve sedation.” In our endoscopy unit midazolam was previously drawn up for endoscopy in a 2 ml syringe (midazolam concentration 2.5 mg/ml), but in mid-2003 this was changed to a 5 ml syringe (midazolam concentration 1 mg/ml). The aim of this study is to determine whether changing the syringe size resulted in a change in midazolam dose given for endoscopic procedures.
Methods: A retrospective review of endoscopy database records for all gastroscopies (OGDs) and colonoscopies performed with midazolam sedation for a three month period immediately before and a three month period immediately after the change in syringe size was performed.
Results: A total of 316 OGDs and 292 colonoscopies were performed in the 3 months prior to the change in syringe size; 281 OGDs and 253 colonoscopies were performed in the 3 months afterwards. For OGDs, the mean dose of midazolam given for a procedure was reduced from 3.3 mg to 3.0 mg following the change in syringe size (p<0.01); for colonoscopies the mean midazolam dose was reduced from 3.2 mg to 2.9 mg (p<0.01). Sub-group analysis by endoscopist showed a significant reduction in midazolam dose given by SpRs (p<0.02) for OGDs, and by both SpRs and consultants (p<0.01) for colonoscopies.
Conclusion: A larger syringe results in a greater volume of sedative but a lower concentration of midazolam per ml, allowing for greater incremental titration of sedation. We have shown that the use of a larger syringe to draw up midazolam for endoscopy is associated with a significant reduction in the midazolam dose given. This is a simple method of reducing sedation doses and its implementation should be considered by all endoscopy units.
238 A STUDY TO EVALUATE THE ROLE OF SEDATION IN COLONOSCOPY
I. W. Rees, R. Dawood, I. Salam.West Wales General Hospital, Carmarthen, UK
Background: There is an increasing body of evidence demonstrating the acceptance of unsedated colonoscopy. With endoscopy units facing increasing workload, older patients, and patients with significant co-morbidity the role of unsedated colonoscopy merits serious consideration. We have looked at patient acceptance in a district general hospital (DGH) setting in west Wales.
Methods: Patients referred to IS for colonoscopy and who were able to give informed consent were invited to participate in a prospective observational study. Prior to colonoscopy participants were asked if they wished to be sedated or not, those who declined had the option to convert to sedation at any time. Patient acceptability was assessed via a questionnaire.
Results: Over a nine month period a total of 122 patients were recruited ranging from 18 to 84 years. (Male 51% v Female 49%) The analysis was conducted on an intention to treat basis. 33.6% of patients were sedated from the outset. Of the 64% who started without sedation 10 patients opted for sedation during the procedure (data incomplete on 2.4%). Analysis of the patient questionnaires was by the two sample Wilcoxon test. This revealed only one significant difference between the two groups that being the level of discomfort during the procedure in those patients unsedated (p = 0.02). There was however no difference in terms of their overall rating and willingness to undertake the procedure in the future (p = 0.136).
Conclusions: This DGH based study has findings consistent with previous studies. Patients’ colonoscopy experiences did not differ overall between the sedated and non-sedated groups. Therefore non-sedation appears to be an acceptable choice in standard colonoscopy practice.
239 USE OF PROPOFOL SEDATION FOR COLONOSCOPY: A DISTRICT UNIT EXPERIENCE
P. Nixon, K. Poon, A. Safe.Department of Medicine and Gastroenterology, Central Gipland Health Services, Victoria, Australia
Background: Complete examination of the colon is important in the diagnosis of colotrectal caner and full assessment of IBD. The JAG recommend caecal intubation rate 90% or higher. There is an increasing interest in the use of propofol for sedation during endoscopy, because of its rapid recovery profile.
Aim and Methods: To assess the outcome of colonoscopy (results, caecal intubation rate, and complications) performed in a district unit over 12 months using propofol sedation. Data were collected from Endoscribe database for all colonoscopies done by a senior endoscopist between February 2003 and January 2004. Patients’ case notes and sedation records were reviewed. Patients who had previous bowel surgery were excluded. Caecal intubation was documented by a photograph or terminal ileum biopsies and adjusted for failure due to an obstructing mass. Any intra procedural complications were documented.
Results: During the study period 326 colonoscopies were performed (57% females). 21 patients had previous surgery. Adjusted caecal intubation was 98%. The indications for colonoscopy were: abdominal pain 22%, chronic diarrhoea 19%, alternate bowel habits 17%, family history of colon cancer 15%, rectal bleeding 10%, assessment of IBD 1%, and anaemia 1%. 41% of the examinations were normal. The main findings were: diverticular disease 27%, colonic polyps 21%, IBD 11%, and colorectal cancer 3%. 283 patients received propofol for sedation. The mean dose was 147 mg (range 20–400 mg). Of them 86% received midazolam with a mean dose 5.4 mg (range 1–10 mg). Five patients developed hypoxia during the procedure. No other complications particularly perforation were recorded.
Conclusion: The audit demonstrated that propofol provided a safe and effective sedation. Propofol sedation might be considered in selective patients to reduce their discomfort and improve service efficiency.
240 USE OF PROPOFOL SEDATION FOR ERCP IN THE ELDERLY POPULATION: AN AUSTRALIAN DISTRICT UNIT EXPERIENXE
P. DeCruz, R. Kerr, A. Safe.Department of Medicine and Gastroenterology, Central Gipsland Health Services, Victoria, Australia
Background: Adequate patient sedation is essential for diagnostic and therapeutic ERCP. There is an increasing interest in the use of propofol for sedation during endoscopic examination, because of its rapid recovery profile. The data of its use in the elderly are scant.
Aims and Methods: To assess the safety and efficacy of the use of propofol sedation in the elderly population during therapeutic ERCP procedures. Data were collected from Endoscribe database for all therapeutic ERCP procedures carried out in the unit on patients above 70 years of age between March 2003 and September 2004. Patients’ case notes and sedation sheets were reviewed. Patients’ cooperation and satisfaction were assessed objectively.
Results: A total of 70 elderly patients underwent 78 procedures (range 1–3). 62% were female. The most frequent indication for ERCP was suspicion of bile duct stones. 31 patients (40%) were jaundiced and 18 had clinical cholangitis. Urgent ERCP was performed in eight patients for acute gall stone pancreatitis. The common bile duct was cannulated in 70 procedures (89%). Thirteen patients had stents for incomplete duct clearance. Five patients had malignant strictures. 63 patients (90%) received propofol with a mean dose of 162 mg (range 20–400 mg). 93% of the patients had midazolam with a mean dose of 3.6 mg (range 1–8 mg) and 96% received fentanyl (mean dose 54 µg and range 25–100 µg). Three patients developed hypoxia during the procedure. One patient developed a short episode of atrial fibrillation. Three patients developed clinical pancreatitis. None of them required intensive care. No procedure related mortality was reported in this cohort. The patients’ cooperation and satisfaction were excellent.
Conclusion: The audit demonstrates that the use of propofol for ERCP in the elderly is safe and effective with a low complication rate. The therapeutic efficacy is good and the patients tolerate the procedure quite well. Close patient monitoring is recommended with propofol sedation because of its narrow therapeutic window.
241 COULD CAPNOGRAPHY PLAY ANY USEFUL ROLE IN MONITORING SEDATED PATIENTS ON AN ENDOSCOPY UNIT?
J. Hancock1, D. Nylander1, L. Fowler1, R. S. Rowland2, G. D. Bell2.1Gastroenterology Department, Sunderland Royal Hospital, Sunderland, UK; 2School of Computing Sciences, UEA, Norwich NR4 7TJ, UK
Background and Aims: Cardiopulmonary complications are the commonest cause of endoscopic procedure related mortality. Capnography during anaesthesia and IV propofol sedation is routine since it gives a much earlier warning of imminent arterial oxygen desaturation than is possible with pulse oximetry alone. We wished to establish if a portable capnograph might aid the monitoring of light to moderately sedated patients on a busy endoscopy unit.
Methods and Results: 43 patients about to undergo colonoscopy (mean age 51.1 with a range 22–77 years) were attached to a combined portable pulse oximeter/capnogram (Oridion Microcap Plus). The 43 patients received a mean total dose of 4.0 mg of midazolam (range 3–5 mg). Pethidine (25–50 mg) was employed in only 3/43 cases. Patients completed a patient satisfaction questionnaire. All colonoscopies were carried out by DN, all were total and every patient stated they were either very satisfied (84%) or quite satisfied (16%). However 76% experienced some pain and 23.6% wanted to have more sedation if the test ever needed to be repeated. The Microcap Plus data were downloaded onto a PC and analysed using Profox software. The SpO2 falls mainly occurred in the recovery ward after the procedure itself had been completed. Desaturation episodes occurred in 67% of patients (mean lowest SpO2 of 91.2% lasting an average of 53 seconds). In 30% of patients the respiratory rate temporally fell to below six breaths per min.
Discussion: The portable capnograph/pulse oximeter and associated nasal filter line proved easy to use. Despite using modest (and arguable at times suboptimal) doses of IV sedation and analgesia, the patients undergoing colonoscopy had frequent episodes of hypoventilation, changes in ETCO2 and oxygen desaturation especially in the recovery period. A case could be made for using a portable capnograph/pulse oximeter routinely in certain high risk patients groups undergoing endoscopic procedures.
242 THE ROLE OF COGNITIVE FUNCTION IN ASSESSING INFORMED CONSENT FOR ENDOSCOPY
A. D. Yeoman, M. J. Dew, L. Das, S. Rajapaksa.Prince Philip Hospital, Llanelli, Wales, UK
Introduction: Informed consent is the cornerstone of good medical practice. We have previously audited the level of understanding of consent in patients undergoing endoscopy and found deficiencies in their understanding of procedures. We set out to ascertain whether cognitive function impacted on understanding of consent for endoscopic procedures.
Method: We prospectively interviewed 100 patients after obtaining consent but prior to endoscopy. Levels of understanding of the procedure were based on defined criteria and a mini mental test score (MMS) was recorded.
Results: 36% had poor or no understanding of the consent process, yet 92% had a normal MMS. 100% with good understanding and 78% of those with poor or no understanding had a normal MMS. The mean MMS fell progressively from 29.6 in those 21–30 years to 24.4 in those >80 years. An age related fall in the level of understanding was seen only in those over 70 years. Subnormal MMS were seen in virtually all age groups.
Conclusion: Whilst a low MMS precluded a good level of understanding, a normal MMS did not guarantee understanding. Although age >70 years was associated with poorer understanding, young age did not preclude either a low MMS or a poor level of understanding. In summary, normal cognitive function does not predict good understanding of informed consent but cognitive impairment precludes it.
243 ENDOSCOPY AND NCEPOD—A RETROSPECTIVE FIVE YEAR ENDOSCOPY AUDIT
J. Rademaker.Conquest Hospital, Hastings, East Sussex, UK
Background: The recent publication from NCEPOD “Scoping our Practice” has significant implications for all hospitals. Also the recent BMJ editorial “Seriously ill elderly patients are subjected to futile endoscopy” prompted a review of the main endoscopic procedures carried out at the Conquest Hospital. All consultants who recorded their endoscopy results on the clinical information agreed for the audit to be carried out.
Methods: Using the audit tool of the local clinical information system, which records all endoscopy results, an audit of all diagnostic and therapeutic endoscopies—upper (OGD), lower (COLON), and ERCP from January 2000 to September 2004 was performed. The system automatically records readmission and deaths via the hospital patient information data received from register of local births and deaths. Although this is not full proof it gives a simple electronic method to review 30 day mortality.
Results: (see table).
Abstract 243
Conclusion: This audit showed that 30 day mortality outcomes are close to NCEPOD data except for ERCP. Further analysis of outcomes for therapeutic v diagnostic OGD were 10% and 2%, respectively. PEG outcomes varied from 30% to 50%. ERCP outcomes for each year were poor because patients with inoperable cancer were offer palliative stent for obstructive jaundice. However one to two unexpected deaths occurred each year and highlight that ERCP remains a high risk procedure requiring competent trained endoscopist and fully informed patients.
A linked endoscopy reporting and clinical information system with mortality data provides an electronic method of data capture. More detailed analysis of individual endoscopists and procedures performed are required to allow regular feedback and change in clinical practice.
244 HOW SAFE IS UPPER GI ENDOSCOPY?
D. McLernon1, P. T. Donnan1, S. McLeod, A. Crozier, C. Mowat, J. F. Dillon.1Ninewells Hospital and Medical School, University of Dundee, Scotland, UK
Background: The safety of upper GI endoscopy (OGD) remains of interest. The NCEPOD recently reported on the morbidity and mortality of therapeutic procedures in England and Wales. The data were collected by questionnaire, with a response rate of only 66%. The BSG audit in 1995 reported a mortality rate of 1:2000 for diagnostic procedures but was also flawed. Furthermore, the role of endoscopy has changed considerably since then.
Aims: To assess the safety of OGD in the current era.
Methods: We used endoscopy records to identify all patients who had an OGD in the period from 1 July 2000 to 30 June 2003. Patients were record linked to hospital records (SMR01), Carstairs deprivation scores, and the death registry. Patients who died within 30 days of OGD were identified.
Results: 12 925 OGDs were performed on 10 030 patients; median age 62 (IQ range: 48–75), 54% female. 396 deaths occurred within 30 days of the procedure, median age 76 (IQ range: 64–83), giving an all cause patient death rate of 3.95%. For inpatients, this rose to 9.5%, v 0.86% for outpatients. 128 deaths followed a therapeutic OGD, giving a death rate of 1/5 (128/640). 48 of these had a PEG insertion, giving a death rate of 1/6 for this indication alone (48/302). The corresponding rate for diagnostic OGD was approximately 1/35 (268/9390). Analysis is ongoing but thus far 42 deaths have been judged related to or caused by OGD, giving a crude patient death rate of approximately 1/250. 17 of these patients had a PEG insertion giving a crude patient death rate of 1/18 for this indication alone (17/302). 22 of the OGD related deaths followed a therapeutic procedure, giving a causal death rate of approximately 1/29 (22/640). The corresponding rate for diagnostic OGD was approximately 1/470 (20/9390). Logistic regression analysis was performed on the outcome of all cause mortality within 30 days of OGD, adjusting for age, sex, deprivation, co-morbidity, in/outpatient, indications, premedication type, diagnosis etc. The odds of an inpatient dying within 30 days of endoscopy compared with an outpatient is 2.29 (p<0.001). The odds of dying from a therapeutic procedure compared with a diagnostic procedure is 2.99 (p<0.001). Further results will be obtained for endoscopy related deaths.
Conclusions: The safety of OGD is determined by the pre-morbid state of the patient. This suggests that we should be more selective in our use of endoscopy, particularly when there is little likelihood of therapeutic benefit.
245 NURSE LED OPEN ACCESS ENDOSCOPY CAN PROVIDE RAPID ACCESS TO ENDOSCOPY FOR UNITS THAT PLAN TO MODIFY THE NICE DYSPEPSIA GUIDELINES
C. J. Rees, A. Frame, C. Davison, S. Panter, S. Soo, K. Wynne.Department of Gastroenterology, South Tyneside Healthcare Trust, UK
Introduction: Open access endoscopy (OAE) is well established but waiting times are often long. In April 2002 our upper GI OAE became an entirely nurse led service. New NICE guidance recommends only endoscoping dyspeptic patients over the age of 55 after an initial period of treatment. Many clinicians have concerns that this guidance may delay the diagnosis of serious pathology.
Methods: Using a database we reviewed the pathology diagnosed in all patients undergoing OAE from April 2002 to September 2004. Other outcomes measured included waiting times and time to dispatch of results. Patients with alarm features were excluded from OAE.
Results: 1095 patients endoscoped by a single nurse endoscopist in a 30 month period were included in the study. Patients were referred by 73 GPs serving a population of 180 000. Median waiting time was reduced from 20 weeks in 2002 to 3 weeks in September 2004. The median time of results being sent to GPs was reduced from 16 to 3 days. The pathology diagnosed is summarised in the table.
Abstract 245
Conclusions: Nurse led OAE diagnosed significant pathology and improved service efficiency. Cancers picked up by OAE were diagnosed at an earlier stage. A central theme of the NHS plan is earlier diagnosis of cancer. We plan to continue endoscoping patients over the age of 55 with new onset dyspepsia and believe that nurse led OAE is the most effective way of providing this service.
246 PROSPECTIVE ANALYSIS OF 30 DAYS COMPLICATION RATE AFTER OUTPATIENT UPPER GASTROINTESTINAL ENDOSCOPY
S. Ishaq1, I. Mohammed1, C. Lyth2, L. Rowe2, J. Brand2, B. Wallace2, K. Walley2, T. Bowling3.1Gastroenterology Department, Sandwell General Hospitals, West Bromwich, UK; 2University Hospital of North Staffordshire, UK; 3Queen’s Medical Centre Nottingham, UK
Introduction: There is limited literature addressing minor complications associated with upper gastrointestinal endoscopy.
Methods: 375 outpatients undergoing their first diagnostic procedure in a single centre were recruited between January 2000 and July 2002. Patients completed an anxiety questionnaire pre-procedure and two further questionnaires 7 days and 30 days post-procedure. Nurse assistant completed a separate questionnaire during the procedure.
Results:Patient perspective: Minor complications (sore throat/hoarse voice, wind, nausea/vomiting, abdominal/chest pain, and fatigue) affected 16% of the patients and for 5% these lasted longer than seven days. Nine patients called their GP/hospital because of problems following the procedure. There were no hospital admissions. 12% of the patients experienced problems during the procedure including difficult intubations, patient distress, and in one patient procedure could not be completed because of patient distress. Complications were not linked to length of procedure or grade of endoscopist, but patients with midazolam as premedication had a higher incidence of minor complications compared with xylocaine or xylocaine/midazolam combination. Anxiety scores were high at 12%, but there was no correlation with complication rates. 18% felt the procedure was worse than expected and 20% said they would not have it done again. There was a trend to better tolerance of the procedure by lengthening the time between sedation and intubation (median time = 60 seconds).
Conclusions: The minor complications rate in this study was higher than that reported in the limited published literature, as was overall patient intolerance. Complications were not linked to length of procedure or grade of endoscopist, but patients sedated with midazolam as premedication had more minor complications compared with xylocaine or xylocain/midazolam combination. Delaying intubation after sedation for at least 2 min improved procedure tolerance.
247 A PILOT STUDY OF NASAL ENDOSCOPY
K. A. Rye, A. T. Cole, A. Stokes, R. Wilson.Digestive Diseases Centre, Derby City General Hospital, Derby Hospitals Foundation Trust, Uttoxeter Road, Derby DE22 3NE, UK
Introduction: Unsedated nasal intubation for upper gastrointestinal endoscopy is possible because of the development of ultra thin 5 and 6 mm instruments. Per oral endoscopy (OE) may also be undertaken unsedated but typically requires two assistants for the procedure. We hypothesised that nasal endoscopy (NE) can be performed with only one assistant to the endoscopist, as an assistant to care for the mouth is not necessary.
Aims: To test this hypothesis we are prospectively studying 60 patients randomised to unsedated nasal or to conventional endoscopy. We present an interim analysis of the first 51 patients. Procedure duration, completeness of examination, staff requirements, and adverse events were recorded. Patient acceptability was assessed by a post procedure and a one week postal questionnaire.
Results: Available data on 48 patients are analysed (endoscopy was not undertaken in one patient, data outstanding for two patients). 27 patients were randomised to NE (age range 39–76, median 68 years). 23/27 underwent successful nasal endoscopy and in 22 this was a complete examination (one failed duodenal intubation, two required oral intubation, two failed intubation by either route). Mean procedure time was 7 min, and 15/23 found NE easily acceptable. Four patients having NE were helped by both nursing assistants though none required airway care. 21 patients were randomised to OE (age range 25–78, median 62 years). All had complete examinations, and mean procedure time was 4.9 min. 13/21 found the procedure easily acceptable. All had airway care but three did not require a second assistant. No major adverse events occurred. Immediate complications were uncommon and minor, relating to minor nasal trauma (4/27).
Conclusions: Unsedated nasal endoscopy can be safely undertaken without dedicated assistance for airway care. It appears to be as acceptable to patients as oral endoscopy, though procedure times may be slightly longer. Nasal intubation in this study was not possible in 4/22 patients.
248 HIGH RESOLUTION MAGNIFICATION ENDOSCOPY WITH ADAPTIVE INDEX OF HAEMOGLOBIN COLOUR ENHANCEMENT TO EVALUATE THE UGI TRACT
K. Ragunath, G. Anagnostopoulos, P. Fortun, P. Kaye, C. J. Hawkey.Wolfson Digestive Disease Centre, University Hospital Nottingham, UK
Background and Aim: Recently Olympus-Keymed (UK) has launched the Lucera Video Endoscopy processor that has the advanced features of adaptive index of haemoglobin (IHb) colour and structural enhancement features. Combined with a high resolution magnification endoscope it emphasizes subtle chromatic and structural alterations in the mucosa, highlighting the pit patterns and the microvascular architecture. Our aim was to systematically study the UGI tract with the above endoscopy system.
Methods: We report our experience from the observations made in the first 50 patients who underwent UGI endoscopy for a defined clinical indication with a high resolution magnification gastroscope (Olympus, Q240Z) and Olympus Lucera CV 260 video endoscopy processor.
Results: We were able to distinguish in all patients the normal gastric antral and body microvasculature as previously described.1 In gastric body mucosa, microvasculature forms a honeycomb-like subepithelial capillary network (SECN) pattern, while in normal antral mucosa a regular coil shaped SECN pattern was demonstrated. In one patient with endoscopic appearance of a flat reddened antral lesion, we were able to identify the disappearance of the regular SECN pattern, and visualised a demarcation line separating normal from abnormal capillary network. Histology showed high grade dysplasia (HGD). In three patients with fundic gland polyps the appearance was that of body-type mucosa while in two patients with adenomas there was villous pit pattern and increased vascularity. We examined the duodenal villi in all patients and we demonstrated patchy shortening of villi in a patient with coeliac disease on gluten free diet. In 12 patients with Barrett’s oesophagus there was increased vascularity which was more pronounced in two patients. Histology confirmed low grade dysplasia in one and HGD in the other.
Conclusion: High resolution magnification endoscopy with adaptive IHb enhancement can be a powerful tool for the detection of subtle GI pathology. Further experience is needed in order to estimate its true diagnostic efficacy.
1
249 A RETROSPECTIVE REVIEW OF UPPER GI ENDOSCOPY FOLLOWING BONE MARROW TRANSPLANTATION
N. P. Galletly, G. W. H. Stamp, A. V. Thillainayagam.Departments of Gastroenterology and Histopathology, Hammersmith Hospitals NHS Trust, London, UK
Background: Upper GI symptoms are common following BMT and may be attributable to graft versus host disease (GvHD), opportunistic infections or medication side effects. GvHD is a common complication of allogeneic BMT and often involves the GI tract. Hammersmith Hospital is a regional centre for bone marrow transplantation (BMT). We undertook this study to review our experience of upper GI endoscopy following BMT.
Methods: Retrospective review of the medical notes and endoscopy database records of all patients who had upper GI endoscopy following allogeneic BMT during a seven year period between October 1997 and October 2004.
Results: 185 BMT (70% for CML) patients (107 males, 81 females, age range 13–69 years) had 268 upper GI endoscopies, of which 75% were performed within 100 days of transplantation. The most frequent indications for endoscopy were nausea and vomiting (54%), abdominal pain and dyspepsia (29%), and upper GI bleeding (10%). The most common endoscopic findings were gastritis (51%) and duodenitis (35%). In 26% of endoscopies, no abnormality was found. 34% of gastric biopsies from patients with endoscopic gastritis showed changes consistent with GvHD; gastric biopsies from endoscopically normal stomachs showed changes consistent with GvHD in 35%. Duodenal biopsies were positive for GvHD in 34% of patients with duodenitis and 26% of patients with an endoscopically normal duodenum.
Conclusion: Indications for upper GI endoscopy post-BMT include nausea and vomiting, and abdominal discomfort. Changes consistent with GvHD are common in upper GI biopsies of patients following allogeneic BMT. Unfortunately endoscopic findings of both gastritis and duodenitis have poor predictive value for the presence of GvHD. Gastric and duodenal biopsies should be taken irrespective of the presence of endoscopic changes.
250 DO BENIGN LOOKING GASTRIC ULCERS NEED FOLLOW UP ENDOSCOPY AND BIOPSY?
A. Claridge, A. Weidmaan, R. Lea, A. J. Makin, J. M. Hebden.Department of Gastroenterology, Manchester Royal Infirmary, Oxford Road, Manchester, UK
Introduction: It is standard teaching to biopsy gastric ulcers and perform serial gastroscopies until healing is complete, as approximately 1% will be malignant. However, a recent study has cast doubt on this practice.1
Aim: A retrospective review of benign gastric ulcers diagnosed over the last six years at a teaching hospital.
Methods: All benign gastric ulcers on the endoscopy database (April 1998 to August 2004) were identified and associated histology reports retrieved.
Results: 224 benign looking gastric ulcers at index endoscopy were identified. Biopsy samples were taken in 130 (58.0%), demonstrating cancer (1), metaplasia (7), normal histology (13), ulcer (30), and inflammation (75). A follow up endoscopy was performed in 116/223 (52.0%) patients. In 4/116 the appearances were suspicious of a carcinoma, but histology was benign in every case. Adenocarcinoma was however discovered on biopsy at the second endoscopy in two patients both of whom appeared to have benign looking gastric ulcers. One patient had not been biopsied at the index endoscopy; the other patient’s index histology showed metaplasia only. A further patient whose index histology showed inflammatory changes was subsequently found to have a MALToma at follow up gastroscopy and biopsy. Fifty three patients had three or more endoscopies, but no further malignancies were detected.
Conclusions: Endoscopically benign gastric ulcers without histological evidence of malignancy warrant a follow up examination. In our study three malignancies would have been missed unless a second gastroscopy had been performed, although further endoscopic follow up is of questionable value.
1
251 UPPER GI CANCERS—HOW MANY DO WE MISS?
S. Shetty, V. Mudaliar, E. T. Swarbrick, B. C. McKaig.New Cross Hospital, Wolverhampton WV10 0QP
Introduction and Aims: Upper GI cancers carry a poor prognosis and diagnosis at an early pathological stage is associated with longer survival. Our aim was to identify and characterise patients with upper GI cancer whom had previously undergone upper GI endoscopy within three years of diagnosis.
Method: Over a two year period patients with gastric or oesophageal cancer were retrospectively identified via pathology database. Patients were cross referenced with endoscopy database to identify those patients who had undergone upper GI endoscopy within the previous three years.
Results: 96 patients with gastric cancer and 137 patients with oesophageal cancer were identified. Of 96 patients with gastric cancer, eight (8.3%) had undergone gastroscopy within three years (range: 2 weeks to 32 months). All eight patients had varying symptoms of dyspepsia at index gastroscopy. Of these eight patients, five subsequently presented with inoperable cancers, and only one had N0 disease. Index gastroscopy in all eight patients identified significant gastric inflammation however only two patients had biopsies taken, both demonstrating intestinal metaplasia. Three of five patients tested for H Pylori were found to be positive. Of 137 patients with oesophageal cancer, four (2.9%) had undergone an endoscopy within the last three years (range 4 months to 27 months). Three out of the four patients were noted to have Barrett’s oesophagus and two of these patients were in a Barrett’s screening programme.
Conclusion: All patients with gastric cancer who had undergone previous endoscopy were noted to have significant gastric inflammation. Should these patients have more rigorous biopsy protocols, H pylori testing, and endoscopic follow up? Of those patients presenting with oesophageal cancer, two of four patients were in a Barrett’s surveillance programme again fuelling the debate over the benefits of screening in this condition.
252 PREVALENCE OF BARRETTS OESOPHAGUS AT DIAGNOSIS AND AFTER THERAPY OF LA GRADE C AND D REFLUX OESOPHAGITIS
A. J. Morris, J. P. Rosen, L. Golightly.Gastroenterol Department, Glasgow Royal Infirmary, Glasgow, UK; ISMO, Astrazeneca, Luton, UK
Introduction: Identification of patients with Barrett’s oesophagus will allow surveillance for dysplasia and may identify those at high risk of developing adenocarcinoma. No recommendations exist for repeat endoscopy in patients with severe reflux oesophagitis to ensure healing or screen for prevalence of Barrett’s oesophagus.
Methods: As part of a double blind, randomised, and multicentre study, patients with severe reflux oesophagitis (LA grade C/D) and daily heartburn received healing dose proton pump inhibitor therapy for 8 weeks. Endoscopy findings at baseline and at 8 weeks were recorded including severity of reflux disease and presence of Barrett’s oesophagus. All endoscopists received training in the use of the LA classification of reflux oesophagitis. Biopsy confirmation of Barrett’s was not required.
Results: 553 patients were studied: 380 male, 173 female. The mean (SD) age was 54.5 (SD 13.3) years. Baseline LA classification was LA grade C (n = 417 (75.4%)), LA Grade D (n = 136 (24.6%)). At 8 weeks 414 patients (74.8%) studied had achieved mucosal healing. Baseline prevalence of Barrett’s oesophagus was 12.5% (69 patients), and at 8 weeks 24.6% (146 patients) (p<0.05).
Conclusion: In patients with severe reflux oesophagitis (LA grade C/D), baseline endoscopy may underestimate the prevalence of Barrett’s oesophagus since more cases are detectable on mucosal healing. Repeat endoscopy at 8 weeks might ensure healing and identify patients with Barrett’s to allow consideration of entry to a surveillance programme.
253 THE INCIDENCE OF GASTRIC POLYPS IN PATIENTS ATTENDING FOR BARRETT’S SURVEILLANCE
D. C. McCole, C. D. Auld.Department of Surgery, Dumfries and Galloway, Royal Infirmary, Bankend Road, Dumfries DG1 4AP, UK
Introduction and Aim: A prospective endoscopy database (1994–2003) of over 17 000 examinations reveals an overall 3% incidence of gastric polyps but for patients with reflux oesophagitis, the incidence is unchanged. Conversely, the incidence in Barrett’s oesophagus appears greater than oesophagitis per se. A prospective study was undertaken to evaluate the incidence, types of polyps, and to determine any relationship to proton pump inhibitor (PPI) therapy, length of Barrett’s, and helicobacter status.
Patients and Methods: Prospective data were collected in 83 patients on the Barrett’s register by a single endoscopist (DMcC). Age, sex, helicobacter status, length of Barrett’s, number, and types of gastric polyps were recorded. The duration of PPI medication was also noted. The M:F ratio was 51:32 (61.5%:38.5%) and the mean age was 61.7 years (range 32–79 years)
Results: 31 patients (37%) were found to have gastric polyps of which 77.5% were multiple. Fundic gland polyps were noted in 78% and hyperplastic polyps in 22% of patients. There was no relationship with age and sex, but there was a tendency for longer segment Barrett’s to be associated with a higher incidence of polyps (52% when >7 cm). This was not statistically significant when χ2 test of proportions with Yates correction was used (p = 0.1545). 76 of the 83 patients (91.5%) were on regular PPI therapy, but the incidence of polyps was unrelated to the duration of PPI. All except one were helicobacter negative.
Conclusion: Controversy exists as to whether PPI therapy may cause gastric polyps. In this study there appears to be a definite relationship between Barrett’s oesophagus and gastric polyps which is unrelated to duration of PPI therapy. A prospective study is underway to compare reflux oesophagitis (group 1) and Barrett’s oesophagus (group 2) in relation to PPI therapy to address this.
254 SIX MONTH AUDIT OF OESOPHAGEAL DILATATION—CLINICAL PRACTICE AND COMPLICATIONS AT UNIVERSITY COLLEGE LONDON HOSPITALS NHS TRUST
A. Casburn-Jones, S. M. Thorpe, A. Crabb, S. G. Bown, L. B. Lovat.University College Hospital, London, UK
Oesophageal dilatation is a commonly practised technique but there are few controlled studies regarding practice. The BSG guidelines published in February 2004 highlight good practice and promote use of standard protocols in the clinical practice of oesophageal dilatation.
Aims: To assess current practice at UCLH against the new BSG guidelines and to determine the complications and mortality following oesophageal dilatation at UCLH against national standards.
Method: A retrospective case review of all patients undergoing oesophageal dilatation, between July and December 2003, in the department of gastroenterology at UCLH was undertaken. Unisoft endoscopic recording system and patient case notes were reviewed.
Results: 82 oesophageal dilatations were performed in 62 patients (68% male), median age 71 years (range 32–94 years); indications included malignant stricture (73%), peptic stricture (11%), radiotherapy stricture (9%), and achalasia (7%). Prior to dilatation, 91% had undergone previous endoscopic assessment, 79% had a tissue diagnosis, and 53% had recent imaging. All achalasia patients had had manometry. Consent forms included information on expected perforation rate on only 24% of forms. A consultant was present at 82% of dilatations and the rest were done by a final year SpR. Bougienage with Savary-Gillard dilators was the most popular technique (84%), and balloon dilatation was used for all achalasias. Final dilatation diameter was recorded in all cases, but in 46% starting diameter was not. 66% of dilatations included an additional procedure: stent (14), laser (19), EUS (15), other (7). There were two perforations (2.4%) after bougienage for malignant strictures, neither required operative intervention, and both were alive at 1 month. Four dilatations to palliate cancer (5%) were complicated by pneumonia, one by chest pain and vomiting requiring hospital admission. There was no mortality directly related to oesophageal dilatation but all three patients who developed pneumonia died 28, 46, and 57 days post dilatation.
Conclusions: The BSG dilatation standards are achievable in practice.
255 OESOPHAGEAL STENT INSERTION WITHOUT FLUOROSCOPIC OR ENDOSCOPIC CONTROL: A RETROSPECTIVE AUDIT
R. Bhargava, R. Kaja, M. Syed, H. Chatha, S. Cherian, V. Jain, P. Singh.Department of Gastroenterology, Staffordshire General Hospital, Stafford, UK
Introduction: Self expanding metallic stents (SEMS) provide good palliation for malignant dysphagia. Traditionally such stents have been inserted under fluoroscopic control, which has service provision implications in terms of availability of equipment and personnel often resulting in delays. Safe and effective stent placement without need for fluoroscopy would be a significant advance.
Methods: For the past 3.5 years, we have placed Ultraflex oesophageal stents without fluoroscopic or endoscopic control, simply by using the distance markers on the introducer. We have retrospectively reviewed our experience with this technique with regard to efficacy and immediate and late complications.
Results: Thirty-four patients had oesophageal stents placed with this technique. There were 20 men and 14 women. The median age was 77 years (range 35–92). Proximal oesophagus was the site of obstruction in one, mid-oesophagus in 24, and distal oesophagus in nine. Thirty patients had primary oesophageal cancer and four had primary lung cancer with erosion or extrinsic compression. Twelve patients had 10 cm stents inserted while 15 cm stents were placed in 22. Dysphagia was successfully relieved in all patients. One patient died within 24 hours of stent placement because of massive haemetemesis. One patient had early displacement within 72 hours of stent placement which required restenting. Sixteen patients required repeat endoscopy for dysphagia with five needing three or more repeat endoscopies. Only six of the 16 had endoscopic evidence of stent occlusion at 13, 34, 52, 69, 147, and 195 days after initial stent insertion. Food bolus was responsible for stent occlusion in three, which was cleared endoscopically. Tumour overgrowth was the problem in the other three, which was relieved with the placement of a second stent. The median survival after stent insertion was 82 days with the interquartile range of 40 to 239 days.
Conclusion: SEMS can be placed safely and effectively without fluoroscopic control in the vast majority of patients with malignant oesophageal obstruction with excellent palliation and low risk of complications.
256 ENDOSCOPIC LESIONS RELATED TO LOW DOSE ASPIRIN AND ANTI-THROMBOTIC DRUGS IN SUBJECTS WITH UPPER GASTROINTESTINAL BLOOD LOSS
A. S. Taha, W. J. Angerson, S. Mair, R. P. Knill-Jones, O. Blatchford.Departments of Gastroenterology, Crosshouse Hospital – Kilmarnock, Surgery, and Section of Public Health & Health Policy, University of Glasgow, UK; and Department of Public Health Medicine, Argyle and Clyde NHS Board, Scotland, UK
Background: Although upper gastro-intestinal haemorrhage is a recognised complication of low dose aspirin and other anti-thrombotic agents, little is known about the site or nature of the bleeding lesions.
Patients: We, therefore, analysed the endoscopic details of 680 patients with upper gastrointestinal bleeding and presenting over a three year period to a single general centre affiliated to the University of Glasgow: 408 men (60%), 272 women (40%), aged 60 (44–76) years, median (interquartile range). They included 153 patients on low dose aspirin (75 mg daily), 84 on NSAIDs, and 60 on other anti-thrombotic drugs, 29 on warfarin, 16 on dipyridamole, and 15 on clopidogrel.
Results: Erosive oesophagitis was found in 150 patients, gastric ulcers in 52, and duodenal ulcers in 95 patients. The results of the multiple logistic regression analysis of risk factors associated with bleeding endoscopic lesions are as follows (see table): When only a single factor was present, oesophagitis was found in 28 of 98 bleeders (28.6%) on aspirin (p = 0.004), 13 of 29 (44.8%) on other anti-thrombotics (p<0.001), and six of 45 (13.3%) on NSAIDs. Cardiac disease was the major indication for their use with few peptic symptoms.
Abstract 256
Conclusions: Oesophagitis is common in bleeders taking aspirin or anti-thrombotic drugs, and can be confused with coexisting heart disease.
257 UNDER PERFORMING OR UNDER FUNDING? A SURVEY OF PRACTICE IN UPPER GASTROINTESTINAL BLEEDING
S. Hearnshaw, D. A. Burke.Cumberland Infirmary, Carlisle, UK
Introduction: Endoscopic haemostasis in UGI bleeding reduces the risk of rebleeding, transfusion requirement, and improves mortality. Several haemostatic techniques are advocated, but all are dependant on accurate localisation and identification of the bleeding site. Removal of adherent clot is recommended to enable haemostatic treatment. BSG guidelines for UGI bleeding recommend access to endoscopy out of hours.
Aims: To collect data from UK endoscopy units regarding: endoscopic workload related to UGI bleeding, availability of out of hours service, and current lavage and haemostatic techniques.
Methods: An anonymised postal questionnaire requesting details of current practice was sent to 297 UK endoscopy units known to the BSG.
Results: 166/297 (55.8%) units replied reporting a median of 3000 (range 150–7000) UGI endoscopies/year with a median of five endoscopists (range 1–15), 265 endoscopies/year for UGI bleeding, an average of 58 bleeds/endoscopist/year. One unit reported no UGI bleeding service. Only 95/163 (3 non-responders) reported an established out of hours service for UGI bleeding. 57% of departments routinely attempt clot removal at endoscopy for bleeding; 86% use washing techniques to remove clot, 13 using combination techniques with snares and clips. 85% report the use of syringes to clear the field of view, and four units use other pump irrigation techniques. To achieve haemostasis, 86% report adrenaline injection, 25% Argon Plasma Coagulation, and 24% use APC and adrenaline.
Conclusions: The success of haemostatic techniques is reliant on adequate vessel visualisation. The majority of respondents use syringed water to clear the field and remove adherent clot. Although cheap, it can be cumbersome and may not be the most efficient method of lavage. If recommended best practice in managing UGI bleeding includes timely endoscopic assessment, this survey shows a significant deficiency in terms of access to out of hours UGI endoscopy and application of appropriate techniques. The reasons for lack of implementation of best practice needs detailed assessement.
258 GASTROSCOPY NEGATIVE MELAENA: IS FURTHER INVESTIGATION JUSTIFIED? A RETROSPECTIVE REVIEW
S. Halsall, J. Ramesh, A. J. Makin, J. M. Hebden.Department of Gastroenterology, Manchester Royal Infirmary, Oxford Road, Manchester, UK
Introduction: Melaena typically results from significant blood loss from the upper gastrointestinal tract and it is standard practice to investigate with a gastroscopy. It is not clear how much further to investigate if the index gastroscopy is negative.
Aim: To review the presentation, investigations, and outcome of patients referred with melaena alone and a subsequent normal gastroscopy.
Methods: A search of the endoscopy database (April 1998 to December 2003) was undertaken and data were extracted by retrospective case note review.
Results: Seventy four (18.6%) of 397 patients referred with melaena alone had a normal gastroscopy. Sixty three (85%) of the 74 case notes were retrieved and reviewed. Median age was 61 years (range 21–84); 52 (83%) were inpatients and 11 (17%) direct endoscopy referrals by GPs. All inpatients had a gastroscopy within 72 hours; direct endoscopy referrals median 30 days (range 10–150). Seventeen (27%) were taking aspirin, 14 (22%) were on anticoagulants, and 10 (16%) were on NSAIDs. Anaemia was present in 35 (55%), raised urea in 20 (32%), elevated prothrombin time in 11 (18%), and thrombocytopenia in four (6%). A median of two (range 1–8) units transfusion was given to 26/35 anaemic patients. Colonoscopy was offered to 27 (43%) patients: normal in 11 (18%), refused in four (6.3%), right sided carcinoma in three (4.8%), diverticulosis in three (4.8%), right sided colitis, caecal ulcer, and rectal mass each in one (1.6%). Small bowel meals were performed in seven and all normal, enteroscopy in three and all normal, and mesenteric angiography in seven revealing one superior mesenteric artery aneurysm and one angiodysplasia. Ten patients (16%) died during the acute admission and four at follow up. All deceased were >60 years with multiple co-morbidities.
Conclusions: Patients presenting with melaena in whom gastroscopy is normal warrant further investigation with a colonoscopy. In our review, 5/27 (19%) colonoscopies revealed significant right sided pathology to account for melaena, including three cases of colonic carcinoma.
259 TOP OR BOTTOM FIRST OR DO BOTH TOGETHER FOR IRON DEFICIENCY ANAEMIA?
M. Aljabiri, C. Kothari, P. Dubois, S. Mann.Niall van Someren, Kalpesh Besherdas
Introduction: Iron deficiency anaemia (IDA) in UK is mainly caused by dietary insufficiency, malabsorption or gastrointestinal blood loss. Currently the BSG guidelines do not give a clear indication of which part of the GI tract should be investigated first or should both be investigated together.
Aims: To identify any difference in investigation of IDA beginning with examination of foregut or hindgut against examining both foregut and hindgut together.
Methods: A single centre, retrospective analysis of patients undergoing upper/lower gastrointestinal endoscopy for IDA as the primary indication. 118 consecutive patients that were undergoing gastroscopy and colonoscopy for IDA and 83 patients who underwent gastroscopy first followed by colonoscopy were identified.
Results: A cause for IDA was identified in 24 of 118 patients (20%) who underwent gastroscopy and colonoscopy on the same day. In 6/24 (25%) patients an upper GI cause was identified. These included duodenal ulcer (two patients), gastric cancer (one patient), haemorrhagic gastritis (one patient), and severe oesophagitis in two patients. In 18/24 (75%) patients a lower GI cause was identified. The lower GI causes included colonic cancer (eight patients), colonic polyps (one patient), colitis (six patients), angiodysplasia (one patient), and haemorrhoids in two patients.
A cause for IDA was identified in 17 of 83 patients (20%) who underwent gastroscopy first and then at a subsequent date colonoscopy. A lower GI cause was identified in 13/17 patients (76%) with all having a colonic tumour. An upper GI cause in 6/17 (35%), with two patients having a reason for IDA in both upper and lower GI tract. The upper GI causes included duodenal ulcer (two patients), gastric ulcer (one patient), telengectasia (two patients), and portal gastropathy in one patient.
Conclusions: 20% of patients have an identifiable cause of IDA in the upper or lower GI tract on endoscopy. In this study, the prevalence of lower GI causes was significantly greater than upper GI causes. From this study as a large proportion of patients in whom the cause of IDA was colonic cancer it is recommended that investigation of IDA begin with colonoscopy first.
260 ENDOSCOPIC GASTROPLICATION FOR PROTON PUMP INHIBITOR REFRACTORY GASTRO-OESOPHAGEAL REFLUX DISEASE
P. M. Lynch, T. C. K. Tham.Division of Gastroenterology, Ulster Hospital, Dundonald, Belfast
Background: A minority of patients with gastroesophageal reflux disease (GORD) are not controlled with proton pump inhibitors (PPIs). These patients are a management challenge. The aim of this study was to prospectively evaluate if GORD patients unresponsive to PPI therapy will benefit from endoscopic gastroplication (EG).
Patients and Methods: Seven consecutive patients with persisting symptoms of GORD despite high dose PPI or H2RA therapy underwent EG (one patient had a previous laparoscopic fundoplication 11 years previously; another patient had a previous partial gastrectomy). Each patient completed two questionnaires (SF-36 Health Survey and a Reflux/Dyspepsia Symptom Questionnaire employing a visual analogue scale) before and 3 months after undergoing EG, utilising the Bard Endocinch device.
Results: All patients successfully completed EG; median number of plications placed was two (range 1–3). No complications occurred. Five of the seven patients (including one with a previous fundoplication and another with a partial gastrectomy) reported symptom improvement following EG. There was no overall significant improvement in reflux related or dyspeptic related symptom scores, although for the patient subgroup who did benefit from EG (reflux n = 5/7; dyspepsia n = 4/7), the improvement in reflux related symptoms was significant (pre-EG = 24.2; post-EG = 69.7; p = 0.043) and non-significant for dyspepsia symptoms (pre-EG = 64.3; post-EG = 85.7; p = 0.066). PPI usage was reduced in those who reported a symptom improvement. Following EG, there was no difference in median SF-36 Quality of Life scores.
Conclusions: EG may reduce reflux symptoms in 70% of patients with GORD refractory to treatment with PPIs. This may include patients with previous fundoplication and partial gastrectomy. Larger studies are required to confirm our observation.
261 VIDEO CAPSULE ENDOSCOPY WITHOUT PRIOR SMALL BOWEL RADIOLOGY
R. Peiris, S. Dar, G. M. Maskell, S. H. Hussaini, H. R. Dalton.Royal Cornwall Hospital, Truro, UK
Introduction: Video capsule endoscopy (VCE) for the management of suspected small bowel pathology is usually preceded by small bowel enema to exclude stricturing disease.
Aim: To determine the outcome of VCE with and without prior small bowel radiology.
Method: Prospective study of 89 consecutive patients undergoing VCE. Indications included suspected gastrointestinal bleeding (overt n = 11, obscure n = 45), suspected small bowel Crohn’s disease (n = 23), unexplained chronic abdominal pain (n = 7), undiagnosed diarrhoea (n = 2), and refractory coeliac disease (n = 1). Before VCE, all patients had a normal gastroscopy and colonoscopy. 52/89 patients had a non-diagnostic double contrast small bowel study.
Results: Significant pathology was found in 56/89 (62.9%) patients. In 54/89 (60.6%) the VCE findings were of diagnostic significance. The diagnostic pickup rate of VCE in suspected gastrointestinal bleeding was 67.8 (38/56) and in the suspected small bowel Crohn’s group was 52.1% (12/23). A normal small bowel double contrast study was performed in 52/89 patients (58.4%). VCE provided a diagnosis in 29/52(55.7%). 37 patients had VCE without prior small bowel radiology. In 31/37 the indication was recurrent iron deficiency anaemia and 6/37 suspected small bowel Crohn’s disease. The diagnostic pick up rate was 22/37 (59.4%). 4/89(4.49%) patients had capsule impaction. 3/4 of these patients had had normal prior small bowel barium studies.
Conclusion: The diagnostic yield of VCE was in 67.8% in patients with obscure gastrointestinal bleeding and 52.1% in suspected Crohn’s disease, which is comparable with other series published. This study supports the idea that small bowel radiology is of limited value in patients with IDA. VCE is associated with an impaction rate of 4.49% (4/89) despite a normal small bowel study in 3/4 patients. In the light of the above study our current practice is to use VCE as the small bowel imaging modality of first choice in patients with IDA. If the patient has any symptoms of obstruction or raised inflammatory markers, this is preceded by a ‘dummy’ VCE.
262 ANGIOECTASIA OF THE SMALL INTESTINE—NEW INSIGHTS FROM CAPSULE ENDOSCOPY
S. Hughes, P. A. Flower, S. Turner.North Bristol NHS Trust, UK
Introduction: Capsule endoscopy (CE) has proved valuable for investigating obscure GI bleeding (OGIB) and suspected Crohn’s disease. Previously, vascular abnormalities were usually seen as typical angioectatic spots in elderly patients. With CE, vascular lesions not visible with other techniques can be identified and this may contribute to a better understanding of these lesions.
Results: 78 patients were subjected to CE for various indications. Most patients had previously had push enteroscopy. Eighteen were found to have vascular lesions. Most (16) were being investigated for OGIB/recurrent iron deficiency anaemia (RIDA) but two young men being investigated for abdominal pain had typical angioectasias considered to be incidental findings. Two patients with OGIB had unusual vascular abnormalities consisting of tortuous, thin walled, superficial mucosal vessels. Active bleeding was seen in one of these patients who had subsequently been treated at interoperative enteroscopy. In addition to the above typical and atypical vascular abnormalities, discrete ‘red spots’ were identified in six patients and ‘pink spots’ in five patients. Nine of these 10 patients had OGIB/RIDA. No such lesions were seen in the other 68 studies. The significance of these spots remains uncertain. Whether or not they represent early vascular lesions remains to be determined.
Conclusions: CE is a more useful technique for identifying vascular abnormalities in the small intestine than previously available tests. Vascular lesions may have a pattern which differs from the classical angioectatic spots commonly described, and typical lesions may be found incidentally in young people. CE also identified red and pink spots, mainly in those with bleeding or anaemia, which may represent early vascular lesions.
263 THE CLINICAL IMPACT OF WIRELESS CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING: DOES IT MAKE A DIFFERENCE?
K. Sheikh, K. Elamin, C. P. Jamieson.Department of Gastroenterology, Norfolk and Norwich University Hospital, Norwich NR4 7UY, UK
Introduction: Wireless capsule endoscopy (WCE) has become the imaging of choice in the investigation of patients with obscure GI bleeding when gastroscopy and colonoscopy are normal.1 The impact of the procedure on clinical outcome in this group warrants further examination.
Methods and Results: We prospectively studied transfusion dependent patients referred to our unit with obscure bleeding or iron deficiency anaemia. A total of 47 patients were studied over a 28 month period. All patients had a normal gastroscopy and colonoscopy before WCE. The final diagnoses included angioectasia in 19 (40%) patients, ileal ulceration compatible with previously undiagnosed Crohn’s disease in three patients and ileal erosions of undetermined significance in one patient. A duodenal polyp and a Dieu-la-Foy lesion were each found in one patient. WCE was normal in 22 (47%) patients. Referring clinicians were consulted at the end of the study to gain information regarding the patients’ outcomes in subsequent follow up. One patient had surgery, the majority having been managed conservatively. The complications included video capsule entrapment in a pharyngeal pouch in one patient, technical failure of capsule in one patient and failure to pass beyond pylorus in one patient who had a probable diabetic gastric dysmotility.
Conclusions: WCE detected visible lesions in small intestine in 53% of patients. Interestingly, it suggested small bowel Crohn’s as a cause of obscure anaemia in three patients in whom small bowel contrast series had been normal. Only one patient had definitive surgery (for a Dieu-la-Foy lesion) post WCE, but the majority have not required further gastrointestinal investigations. The importance of WCE lies in directing appropriate intervention to bleeding lesions in a few patients, making a diagnosis, and hence avoiding unnecessary further investigation in many and detecting Crohn’s disease causing anaemia in an important minority.
1
264 A BLINDED COMPARISON OF A NURSE AND A DOCTOR IN THE DETECTION OF CAPSULE ENDOSCOPY ABNORMALITIES
D. Kar, L. Marshall, D. S. Sanders, M. E. McAlindon.Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Background: Capsule endoscopy is a first line small bowel investigative procedure and demand is growing rapidly. Performing the procedure is not demanding but viewing the images is time consuming. Screening of the images by readers other than the doctor may increase the flexibility of the service.
Aim: To compare a non-doctor and doctor reader in detection of pathology shown by capsule endoscopy.
Methods: Viewing of 50 consecutive videos by a nurse and a doctor were timed. Both were blinded to the indication and each other’s findings. The nurse had no prior experience or teaching in interpretation of capsule endoscopy images, although she had assisted at fibreoptic endoscopy. Both were asked to save thumbnails of all possible pathology, which was graded as relevant (ulcers, erosions, angioectasia, blood), uncertain (erythema, red dots, oedema), and irrelevant (lymphangiectasia, prominent vessels, lymphoid follicles). A third expert arbitrated.
Results: Of 50 patients, 27 were female, mean age 48 (SD 2.7) years. Indications included anaemia (n = 16), suspected Crohn’s disease (15), overt bleeding (12), suspected functional bowel disorder (4), and others (3). The nurse took longer to read the videos than the doctor (mean 73 and 58 min, respectively; p<0.001). There was no difference in the number of relevant or uncertain pathologies identified (3.8 and 5.2 relevant, and 2.4 and 2.2 uncertain abnormalities per case for nurse and doctor, respectively, p = ns) although the nurse was more likely to record irrelevant findings (4.7 and 2.0 lesions per case, respectively, p<0.01). The doctor missed one small pedunculated terminal ileal polyp in a patient with anaemia, otherwise no important pathology was missed by either reader.
Conclusions: With no specific training, a nurse capsule endoscopy reader was able to reliably detect relevant pathology which allowed the correct diagnosis in all cases. Nurse readers may allow the service to cater for increased demand.
265 CAN NURSE PRACTITIONERS EXAMINE AND REPORT VIDEO CAPSULE ENDOSCOPY AS EFFECTIVELY AS PHYISCIANS?
G. Schofield, C. Fraser, G. Brown, C. Thapar, B. Saunders.Wolfson Unit for Endoscopy, St Mark’s Hospital, Harrow, UK
Background: Video capsule endoscopy (VCE) is a pain free diagnostic procedure which examines the gastrointestinal tract, particularly focusing on the small intestine. Demand for VCE is increasing and it is likely that the service will become nurse practitioner rather than physician led within some national health care services across the United Kingdom. Where gastroenterologists’ time and availability tends to be limited, nurse practitioners already have an important function within specialties such as endoscopy.
Aim: As a specialist intestinal referral centre, St Mark’s Hospital has had a nurse led VCE service for one year. The aim of this study was to examine whether qualitative differences exist in examination and reporting practices between nurses and physicians similarly trained in VCE as this could have potentially adverse implications for a nurse led service.
Methods: A prospective, double blinded study examining the reporting practices of two VCE readers. The two readers were a nurse practitioner (GS) identified as R1, and a senior gastroenterologist (GB) as R2. 20 consecutive patients referred for VCE were included in the study. The Rapid® Workstation Main screen was used for the viewing and reporting of each of the 20 cases and a formulated VCE proforma ensured a standardised reporting method was used by both readers. All results including interreader differences in final diagnoses, and recommendations following VCE were reviewed for accuracy by an independent gastroenterologist (CF).
Results: Significant differences in examination technique and reporting of VCE recordings by R1 and R2 were detected (as shown in Table). R1 consistently used more viewing aids during VCE examinations (zoom function, blood indicator) than R2, and their reviewing duration was longer due to viewing at a slower frame rate. R1 also identified more significant lesions overall than were noted by R2. Each reviewer was requested to identify when the capsule first reached specific sections of the gastrointestinal tract. There was some minor discrepancy between readers for entry times into ileum and caecum. In terms of reporting, the final diagnoses made by each reader were identical (except R1 reported one additional incorrect finding). A similar number of recommendations were made by both readers, all of which were appropriate.
Abstract 265
Conclusions: This study suggests that a nurse practitioner specifically trained in VCE provides an equally effective reporting service as a physician in terms of accurate diagnoses and discharge recommendations. Despite the differences in examination technique, there was ultimately no difference in the quality of the final VCE report made by the nurse practitioner.
266 ENDOSCOPIC ULTRASOUND: A DEVELOPING SERVICE AT CITY HOSPITAL, THE FIRST 100 CASES
S. C. Cooper, P. G. Wilson.Department of Gastroenterology, City Hospital, Dudley Road, Birmingham, UK
Background: Endoscopic ultrasound (EUS) enables the clinician to image many areas of the upper gastrointestinal tract with greater accuracy than transabdominal ultrasound, and visualise pathology of smaller dimensions than other modes of imaging. EUS is now considered complimentary to other forms of staging such as CT and PET scanning. Dr P.G. Wilson set up the service at City Hospital, examining the first patient on the 11th May 2001. We sought to audit the first 100 cases, in order to appraise this new service.
Results: Patients of all ages have been examined (25–92, median 66). Referrals have been received from across the West Midlands. The indication for EUS was predominantly for staging of malignant disease (n = 51), and assessing potential malignancy (n = 36). Areas of examination: oesophagus n = 74, stomach n = 8, pancreato-biliary n = 7, biliary tree n = 6, pancreas alone n = 3, and duodenum n = 2. Only five procedures were abandoned, four due to stricturing. In identifying local disease, EUS was superior to other imaging in 16 cases, and less helpful in seven cases. Use of a linear echoendoscope would have enabled biopsies to be taken and would have been beneficial in 45 patients.
Conclusions: In some cases EUS can more accurately stage local disease compared with more traditional imaging modalities. EUS is thus shown to assist in patient management, especially in staging malignant disease. We aim to continue developing the service.
267 THE REFERRAL PATTERN FOR ENDOSCOPIC ULTRASOUND OF A DISTRICT GENERAL HOSPITAL AND IMPACT ON ERCP
J. S. Fraser, D. Dewar, J. O’Donohue, D. M. Reffitt.Department of Gastroenterology, University Hospital Lewisham, London SE13 6LH, UK
Introduction and Aims: Endoscopic ultrasound (EUS) is predominantly a tertiary referral service with limited access for most district general hospitals (DGH). University Hospital Lewisham is a DGH with a population of 250 000 and has an open endoscopic ultrasound service, unrestricted by access and unbiased in referral pattern. Here, we audit the referral pattern for EUS in Lewisham as a guide to the potential use for EUS in a DGH.
Methods: Sequential patients between March 2003 and September 2004 referred for EUS at Lewisham were audited. We ascertained demographic data, source of referral (Gastroenterologist/Surgeon/Other), and indication for EUS. We assessed the clinical impact of the EUS service by calculating the reduction in number of endoscopic retrograde cholangiopancreatographies (ERCP) required.
Results: 127 EUS examinations were requested. Seven patients did not attend, intubation was unsuccessful in one patient. Of those completed, 115 were radial and four linear. The mean age of patients was 59 (range 19–93): 64 were male. Sixty four patients (50.4%) were referred by surgeons, 61 (48%) were referred by medical gastroenterologists, and two (1.6%) by other physicians. Twenty six (20.5%) were referred for assessment of oesophageal tumours, 12 (9.5%) for assessment of gastric lesions, four (3%) for assessment of duodenal lesions, 30 (23.5%) for further definition of a pancreatic mass, and 55 (43.5%) for definition of the biliary tree. Of these, 50 were completed: 43 (86%) were for visualisation of common bile duct (CBD) microlithiasis, and seven (14%) for assessment of malignancy. Thirty eight (88%) of those for CBD stones were negative, thus avoiding ERCP.
Conclusions: There is a significant need for availability to both oesophagogastric and pancreaticobiliary EUS in a DGH. Although access to EUS is prioritised for tumour staging at tertiary hospitals, it is often more restricted for benign indications and excluding biliary stones, which reduce the need for local ERCP.
268 EUS STAGING OF OESOPHAGEAL CANCER WITHOUT DILATION: OESOPHAGOPROBE AS THE PREFERRED INSTRUMENT
C. Vu, L. Doig, S. Tsang, J. Meenan.Guy’s and St Thomas’ Hospital, London, UK
Background: Stricturing oesophageal cancers prevent complete EUS staging without pre-dilation in one third of cases. Use of the Olympus MH908 slim probe (7.9 mm; 7.5 MHz) may potentially obviate the need for dilation, avoiding the attendant costs and the risks of perforation. Strictured lesions due to late presentation are problematic in developing countries but it is unknown whether the case mix in developed countries justifies the addition of this instrument to standard equipment.
Aim: To compare the ability of the MH 908 slim probe (SP) or standard echoendoscope (SE) to fully stage stricturing oesophageal cancers without initial dilation.
Methods: Data were collected over a five year period (1999–2003), the first two years of which EUS staging was performed only with a SE without dilation. After the introduction of a SP, EUS staging was performed in the subsequent three years with it as the first choice.
Results: Complete staging (94.8% v 77.2%; p<0.001), identification of advanced tumours (T3 or T4) (82.8% v 70.4%; p<0.001), malignant nodes (71.1% v 59.0%; p = 0.002), and distal nodes (23.8% v 16.0%; p = 0.009) were significantly higher in the SP compared with the SE group (349 and 351 patients, respectively). Coeliac adenopathy was not significantly different between the two groups. In a subgroup analysis, the ability of the SE to pass a stricture significantly impacted on the T staging accuracy rate (84% v 40%; p = 0.009).
Conclusion: The oesophagoprobe is significantly more successful than the standard echoendoscope in the complete staging of oesophageal cancer without dilation, the detection of advanced tumours and distal nodes. We propose using the oesophagoprobe as the first choice for EUS staging of oesophageal cancer.
269 DEVELOPMENT OF AN EVIDENCE BASED PROTOCOL FOR TIME TO DISCHARGE FOLLOWING OUTPATIENT ENDOSONOGRAPHY GUIDED FINE NEEDLE ASPIRATE OR TRUCUT BIOPSY
C. Vu, L. Doig, J. Meenan.Guy’s and St Thomas’ Hospital, London, UK
Background: The risks of endoscopic ultrasound (EUS) guided fine needle aspirate (FNA) or trucut biopsy (TCB) are small. However, it is unclear whether patients who undergo such procedures as outpatient should be observed for a longer period than diagnostic EUS.
Aim: Prospective study of the safety of outpatient EUS-FNA and TCB as compared with diagnostic EUS.
Methods: 100 consecutive patients (group A) who underwent outpatient EUS-FNA and/or TCB and another 100 consecutive patients who underwent diagnostic EUS (group B) were analysed prospectively. All cases were performed under conscious sedation. The differences in the mean age, sedation dosages, mean procedure time, and recovery time between the two groups were compared. All patients were assessed for evidence of immediate and late (by phone call within 48 hours) complications after the procedure.
Results: A total of 176 FNA and 36 TCB passes on 109 lesions were performed in 100 patients (81 FNA only, 14 TCB only, and 5 both). FNA/TCB indications: pancreatic 72, intraabdominal 23, and mediastinal 14; diagnostic EUS indications: oesophago-gastric 58, pancreato-biliary diseases 40, others 2. All patients were discharged without any clinically significant immediate complications. One patient with a history of chronic pancreatitis was admitted later on the same day for abdominal pain (normal amylase) after EUS-FNA. Another patient had self limiting mild haematemesis (stable haemoglobin levels) (see table).
Abstract 269
Conclusion: Patients who have undergone outpatient EUS-FNA or EUS-TCB can safely be recovered and discharged using the same post-procedure observation protocol as for diagnostic EUS.
270 THE SAFETY OF ENDOSONOGRAPHY GUIDED FINE NEEDLE ASPIRATION AND/OR TRUCUT BIOPSY IN PATIENTS ON ASPIRIN, NSAIDS OR PROPHYLACTIC LOW MOLECULAR WEIGHT HEPARIN
C. Vu, L. Doig, J. Meenan.Guy’s and St Thomas’ Hospitals, London, UK
Background: Endoscopic ultrasound (EUS) FNA is classified as a high risk procedure for gastrointestinal bleeding under the American Society of Gastrointestinal Endoscopy guidelines. Limited data suggest that aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs) in standard doses do not increase the risk of significant bleeding after EGD or colonoscopy with biopsy, polypectomy or biliary sphincterotomy. Because of the paucity of data, the same recommendation is extrapolated to EUS-FNA.
Aim: To compare the safety of EUS guided FNA or trucut biopsy (TCB) in patients who are taking aspirin, NSAIDs, or prophylactic low molecular weight heparin (LMWH), and those who are not.
Methods: Consecutive patients undergoing EUS FNA or TCB were prospectively analysed for all complications. We exclude patients on non-aspirin antiplatelet drugs from EUS-FNA or TCB because of their profound effect on platelets. Cystic aspirate cases were given routine antibiotic prophylaxis. All patients were assessed for evidence of immediate and late (by a phone call within 48 hours for outpatient or by review as inpatient) complications after the procedure. Bleeding was considered significant if there was: haematemesis, melaena, continuous intraluminal oozing requiring haemostatic procedures, or EUS evidence of an expanding hypoechoic area extraluminally.
Results: 224 patients underwent EUS-FNA or TCB on 243 sites (153 pancreatic, 55 intraabdominal, 34 mediastinal, 1 rectal), of which 194 were solid, 46 cystic, and 3 ascites. One (3.6%) of 28 patients taking potentially risky drugs (23 aspirin/NSAIDs and five LMWH) developed extraluminal bleeding compared with five (2.6%) of the remaining 196 patients (p = 0.263). None of these patients developed any clinically significant sequel. One patient from the low risk group developed intraluminal bleeding requiring injection therapy and haemoclipping. One patient (0.65%) developed pancreatitis. There was no difference in the bleeding complication between the FNA and TCB group (p = 0.246).
Conclusion: EUS-FNA or TCB appears to be safe in patients taking aspirin, NSAIDs, or prophylactic LMWH.
271 LINEAR ENDOSONOGRAPHY GUIDED CYSTGASTROSTOMY OF PANCREATIC PSEUDOCYST
C. Vu, J. Meenan, T. Wong.Department of Gastroenterology, Guy’s and St Thomas’ Hospitals, London, UK
Background: Pancreatic pseudocysts, complicates 10% of patients with acute pancreatitis. Although surgical cystgastrostomy has been the mainstay of treatment historically, the endoscopic techniques in draining bulging pseudocyst provide a less invasive option. Recently, the wider adoption of interventional linear doppler endoscopic ultrasound (EUS) has seen an emerging technique of transmural cystgastrostomy under direct imaging. We present our experience of EUS guided cystgastrostomy.
Aim: The aim of the study is to document the efficacy and safety of linear EUS guided cystgastrostomy.
Patients and Methods: 19 consecutive patients (three patients failed previous cyst drainage attempts (two blind endoscopic and one radiological); three patients had pancreatic abscesses) with symptomatic pancreatic pseudocyst deemed suitable on helical CT scan for endoscopic drainage were referred over a two year period. All patients underwent diagnostic radial EUS before linear EUS guided cystgastrostomy (puncture followed by stent placement) under routine antibiotic prophylaxis.
Results: Of 19 patients, cystgastrostomy was deemed not suitable on radial EUS in nine patients (3 small size pseudocysts, 2 with more than 1 cm gastric pseudocyst distance, 2 with perigastric varices, and 2 with other diagnoses), and one patient had a Zenker’s diverticulum preventing endoscope intervention. Cystgastrostomy was attempted in nine patients with 100% success. Endoscopic “bulge” sign was absent in four (44.4%) patients who underwent cystgastrostomy. There were no immediate or delayed procedure complications. Six patients (66.7%) had complete pseudocyst resolution on a mean follow up of 12.4 (range 3–22) months. One patient had an asymptomatic recurrence of the pseudocyst and two required subsequent operative drainage.
Conclusion: EUS guided cystgastrostomy is safe, effective and a viable alternative in the non-operative management of pseudocyst. EUS is better than CT scan in selecting patients for cystgastrostomy.
272 ROLE OF ENDOSCOPIC ULTRASOUND FOLLOWING NORMAL ULTRASOUND AND/OR MAGNETIC RESONANCE IMAGING IN PATIENTS SUSPECTED OF BILIARY CALCULUS DISEASE
A. Kausar1, V. Y. Kaushik2, D. Chang1, M. Chadwick1.1Dept of Surgery and 2Gastroenterology, Blackburn Royal Infirmary, East Lancashire NHS Trust, Bolton Road, Blackburn, UK
Introduction: Endoscopic ultrasound (EUS) is increasingly becoming an established investigation for evaluation of pancreato-biliary disease. This study was carried out at our DGH to identify its efficacy in diagnosing biliary calculus disease (BCD) in those patients who had normal ultrasound (US) and/or magnetic resonance imaging (MRI).
Methods: A retrospective study of consecutive 38 patients who had EUS for pancreaticobiliary disease assessment. EUS findings were compared with conventional radiology in patients who had suspected BCD. These patients presented with right upper quadrant or typical biliary pain, painful obstructive jaundice, recurrent pancreatitis or abnormal liver tests with right upper quadrant pain.
Results: Of the 38 patients, 29 were identified to have suspected BCD; the remaining nine had pancreatic diseases. All 29 patients had at least one US by an experienced radiologist, and six also had MRI scans. 5/29 (17%) patients had calculi identified by EUS alone and were proven at subsequent surgery or ERCP. Of these five, two had stones in gall bladder, and the remaining three had common bile duct (CBD) stones. EUS also identified those stones seen on US or MRI (3/29). Those patients with normal EUS, 21/29(72%) had their case notes or subsequent admission data reviewed over a period of 8–16 months. No further data refuted the normal findings. One patient had suspicion of a CBD stone at EUS, but subsequent look at EUS pictures failed to confirm the suspicion. Even with this false positive, the specificity of EUS was 95% with sensitivity of 100%. No adverse effects occurred at EUS. Interestingly, majority of patients consistently tolerated the procedure very well. We think this may have been because of lack of air insufflation during EUS.
Conclusion: EUS is a highly specific and sensitive test for diagnosing BCD. In patients with strong suspicion of BCD but negative conventional imaging techniques, EUS should be performed. Adequate patient selection may help reduce the number of true negative tests.
273 DOES TOPICAL GTN ON THE SPHINCTER OF ODDI FACILITATE ERCP?
A. Talwar, C. Dare, J. A. Pain. (introduced by Snook J).Department of Pancreatico-biliary Surgery, Poole General Hospital, Dorset BH15 2JB, UK
Background and Aims: Endoscopic retrograde cholangio-pancreatography (ERCP) is a technically challenging procedure. Glyceryl-trinitrate (GTN) has been shown to reduce tone in the Sphincter of Oddi (SO), cannulation of which is a rate limiting factor. A double blind randomised control trial was performed to assess whether topical GTN on the SO would facilitate cholangiography and/or bile duct cannulation.
Patients and Methods: 104 patients requiring ERCP for biliary symptoms were randomised into two groups, 52 controls pre-treated with 5 ml 0.9% Normal Saline (NS), and 52 pre-treated with 5 ml GTN (concentration 1 mg/ml). Patients were excluded on the basis of 1) previous ERCP, stenting or needle knife papillotomy (NKP); 2) oral or sublingual nitrate use; 3) patient refusal. The time was measured from application of the solution to successful cannulation, successful cholangiography or decision to perform NKP.
Results: There was no statistical difference between the two groups in primary cannulation rate (86.5% v 90.4%; p = 0.76), overall cannulation rate following NKP (96.2% v 96.2%; p = 1.0), time to cholangiography (median time 1.95 min v 1.55 min; p = 0.43), or time to cannulation (median time 3 min v 2.82 min; p = 0.65).
Conclusion: Topically administered GTN to the SO does not aid in obtaining a cholangiogram or cannulation during an ERCP.
274 ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY TRAINING: THE TRAINEES PERSPECTIVE. A REGIONAL SURVEY OF GASTROENTEROLOGY TRAINEES
M. J. Brookes1, N. P. Michell2, P. G. Wilson1.1Department of Gastroenterology, City Hospital, Dudley Road, Birmingham, UK; 2Department of Gastroenterology, Birmingham Heartlands Hospital, Bordesley Green East, Birmingham, UK
Introduction: Improved non-invasive imaging has all but eliminated the need for diagnostic endoscopic retrograde cholangiopancreatography (ERCP). This has potential impact on training opportunities and will reduce the need for ERCP trained gastroenterologists. The purpose of this survey was to determine trainee’s attitudes and exposure to ERCP training compared with the Joint Advisory Group on Gastrointestinal Endoscopy’s (JAG) recommendations.
Design: An anonymous survey of regional trainees in gastroenterology to determine attitudes and exposure to ERCP training.
Results: 82% (28) of trainees responded, of which 89% (25) expressed a desire train in ERCP. Of these trainees only 12% (3) had performed >251 supervised ERCPs, and only 16% (4) of trainees reported performing >100 ERCPs annually. Selective duct cannulation rates were: <50% for 52% (13) of trainees; 51–75% for 24% (6) of trainees; and 75–90% for 24% (6) of trainees. 24% (6) of trainees had attended a JAG approved ERCP training course. ERCP training was considered essential for the CCST in gastroenterology by 46% (13) of trainees, though 82% (23) felt training would improve job prospects.
Conclusions: Most trainees wish to train in ERCP, although this is not essential or necessary. Perceptions about ERCP training need to be addressed in order that the correct number of trainees will be trained (in accordance with JAG guidelines) in order to provide future ERCP services.
275 ONE YEAR PROSPECTIVE AUDIT OF ERCP ACROSS ONE HOSPITAL TRUST
S. Ramakrishnan1, J. Crosbie1, H. Gray2, S. Panter1, S. Mansfield3, R. M. Charnley3, M. Griffin3, N. Hayes3, M. Hudson1, K. Matthewson1, K. Oppong1.1Departments of Gastroenterology, 2Endoscopy, and 3Surgery, Freeman Hospital and Royal Victoria Infirmary, Newcastle upon Tyne NHS Hospitals NHS Trust, Newcastle upon Tyne, UK
Aims: To produce a comprehensive assessment of the practice of ERCP in two units within one acute trust, one of which provides a regional pancreatobiliary service.
Methods: A standard audit proforma was created to record the level of seniority of endoscopist, degree of supervision, indications, immediate and 30 day complications, grade of difficulty, cannulation rate, procedural success rate, sedation practice, antibiotic usage, consent, duration of procedure, and patient monitoring. The 12 month audit was commenced on both sites in May 2002. Procedural difficulty and complications were defined according to published criteria.
Results: 482 procedures were performed in 385 patients during the year. 320 procedures were performed at the Regional centre (Unit 1) and 162 at Unit 2. The procedures were performed on five lists by six consultants, three at Unit 1 and three at the Unit 2. Proformas were completed for 474 (98%) of the procedures. Trainees were involved in 40% of the procedures. In 96% of cases the desired duct for cannulation was the CBD. The crude cannulation rate was 88.5%, adjusted cannulation rate 90.5%. 82% of procedures at Unit 1 and 70% of procedures at Unit 2 were therapeutic. 18% of the procedures at Unit 1 and 7% at Unit 2 were Grade 5.12/474 (2.5%), patients died within 30 days of the procedure, 10 had advanced malignancy. None of the deaths were directly related to the ERCP procedure, 3.0% of patients had pancreatitis. There were four cases of bleeding (0.8%), one patient (0.2%) had a small retroduodenal perforation that settled with conservative management. One patient required a laporotomy for an impacted lithotripter basket.
Conclusion: The majority of ERCP procedures were therapeutic in intent and outcome. Overall acceptable rate of duct cannulation and procedural success were achieved. The results of this audit have provided us with data to review and change our practice.
276 EXPERIENCE AND ASPIRATIONS OF ERCP TRAINEES IN ENGLAND
E. J. Williams.the Steering Committee. BSG audit of ERCP, British Society of Gastroenterology, 3 St Andrews Place, London, UK
Introduction and Methods: It is suggested that completion of 180–200 ERCPs is required for trainees to achieve competence. In 1998 the BSG surveyed GI trainees; 193/236 (83%) of respondents believed ERCP training necessary to compete for specialist posts though 35/163 (22%) of ERCP trainees rated their ERCP training as inadequate. In 2003 to 2004 we performed a repeat survey of ERCP trainees in five regions of England. At the time of writing 92 SpR trainees in ERCP have been identified and 65 (71%) have supplied information regarding training.
Results: Gastroenterology SpRs = 59, Radiology SpRs = 3, Surgical SpRs = 1, Other SpRs = 2. Respondents have been in grade for a mean of 4.3 years (median 4, range 0–8, non-response = 3); 8/65 commenced ERCP training prior to being appointed SpRs,16/65 in year 1 of SpR training, 18/65 in year 2, 6/65 in year 3, and 13/65 thereafter (not specified = 4); 43/65 had performed 300+ OGDs before commencing ERCP training. Respondents had performed their first ERCP a mean of 3.2 years earlier (median 3, range 0–8, non-response = 3). Median number of supervised ERCPs in the preceding year was <50 (range 0 to 200). Of those who were in their 2nd year of ERCP training or higher 21/41 had performed <50 supervised ERCPs in the previous 12 months; 6/21 had supplemented this with <50 independent ERCPs (and in one case >50); 22/65 rated their training as excellent, 31/65 as good, 7/65 as adequate, and 4/65 (6%) as inadequate (non-response = 1); 11/51 of those who had undertaken a total of <200 supervised ERCPs in their career recalled performing at least one independent (unsupervised) ERCP in the preceding 12 months. Of those preferring a teaching hospital career 20/29 definitely intended to perform ERCP as consultants v 13/36 of those who did not; 49/65 (75%) thought that ERCP training was required to ensure future job opportunities were not denied to them, though only 25/49 definitely planned to perform ERCP as a consultant.
Conclusion: Whilst most SpRs training in ERCP believe this to be necessary for career development, not all have a clear intention to perform ERCP as a consultant. Given that the typical trainee has participated in <50 ERCPs in the preceding year future training programmes will need to address trainee selection.
277 INITIAL INSERTION OF A METAL STENT FOR PALLIATION OF DISTAL MALIGNANT BILIARY OBSTRUCTION: A COST CONSEQUENCE ANALYSIS IN THE UK
D. Thorburn1, G. Haydon1, N. Verin2.1The Liver Unit, Queen Elizabeth Hospital, Birmingham, UK; 2Health Economics, Boston Scientific, Nanterre, France
Objective: Biliary drainage by endoscopically placed stent (plastic or metal) is the accepted palliative treatment for malignant distal biliary obstruction. Metallic stents are more expensive but have a lower occlusion rate and consequently require less reinterventions. The aim of this study is to compare the total costs at one year of metal v plastic stent placement as palliation for malignant distal biliary obstruction.
Methods: A Markov model with a time horizon of 12 months and cycle lengths of 1 month was designed to evaluate the cumulative costs over time of plastic and metal stenting. The transitional probabilities of stent occlusion and death were derived from a meta-analysis of all published randomised trials (
) . A national health care perspective was adopted. Unit cost data were obtained from UK public sources (NHS National Schedule of Reference Costs, 2003). Hospital resource use was derived from a survey of four UK physicians.
Results: Initial procedural costs were higher for metal (GBP 1495) compared with plastic (GBP 1038) stent placement. However, follow up costs were substantially reduced for metal stents due to fewer reinterventions for exchange. The break even point, where total costs of metal stenting are lower than total costs of plastic stenting, was after 4 months. When patients survive longer than 4 months, metal stents became cost saving. At 12 months, the cost per patient with a metal stent was GBP 1882 and GBP 2375 for a patient with a plastic stent. The cost difference per patient in favour of metal stents was GBP 493.
Conclusion: This analysis demonstrates that initial metal stent placement is a cost saving strategy when patients survive for more than 4 months. The higher initial procedural cost with a metal stent is offset by a reduction in retreatment costs. In addition, avoiding reinterventions and associated hospitalisation is beneficial to these patients who have a limited life expectancy.
278 CONSENT PRACTICE FOR ERCP—IS ADHERENCE TO BSG GUIDELINES ASSOCIATED WITH A REDUCED EXPERIENCE OF COMPLAINTS PERTAINING TO COMPLICATIONS?
E. J. Williams.the Steering Committee. BSG audit of ERCP, British Society of Gastroenterology, 3 St. Andrews Place, London, UK
Introduction: The BSG recommends endoscopists provide written information to patients prior to ERCP and inform them of 1) alternatives to ERCP, 2) trainee participation, and 3)“substantial risks” (pancreatitis, cholangitis, perforation, and bleeding).
Methods and Results: The BSG audit of ERCP has identified 202 consultant ERCPists in five metropolitan regions of England. At the time of writing 169/202 (84%) of consultants have responded to a questionnaire regarding consent practice. During lifetime practice 50 (30%) have experienced ⩾1 complaint relating to an ERCP complication; 52 (31%) have >10 years experience at consultant grade and 85 (50%) performed >100 ERCPs in the preceding year; 67 (40%) report alternatives to ERCP are usually/always discussed; 111 (66%) usually/always mention participation of trainees; 151 (89%) supply written information to patients; 126 (75%) routinely indicate a risk of pancreatitis in writing, and 155 (92%) do so verbally; 77 (46%) indicate a risk of cholangitis in writing, and 85 (50%) do so verbally; 112 (66%) indicate a risk of perforation in writing, and 141 (83%) do so verbally; 125 (74%) indicate a risk of bleeding in writing, and 154 (91%) do so verbally; 41 (24%) provide no written information on any of the above risks; 13 (8%) provide no verbal information on any of the above risks. Experience of complaints was significantly more likely among those who did not verbally disclose any substantial risks (62% v 27%, p<0.01). There was no significant difference in experience of complaints between those who provided written disclosure of risk and those who did not (28% v 34%). As may be anticipated experience of complaints was more common among those with >10 years experience as consultant (47% v 22%, p<0.02) or a case volume of over 100 procedures/year (38% v 21%, p<0.04). Lack of verbal disclosure was not significantly associated with length of time in grade or annual workload.
Conclusion: : ERCP related complaints are related to time in grade and annual workload but may also be influenced by how verbal information is conveyed.
279 NURSE LED FLEXIBLE SIGMOIDOSCOPY SURVEILLANCE FOR FAMILIAL ADENOMATOUS POLYPOSIS IS SAFE, RELIABLE AND EFFECTIVE
R. F. S. Man, C. Fraser, B. Saunders.Wolfson Unit for Endoscopy, St. Mark’s Hospital, Harrow, UK
Introduction: People with familial adenomatous polyposis (FAP) have a 100% risk of colorectal cancer. This results from the inevitable development of numerous pre-malignant adenomatous polyps throughout the colon and rectum. Prophylatic total colectomy is recommended to minimise this risk but cancer can still develop post-operatively124 if adenomas are not removed from the rectal remnant or the ileal anal pouch.35 Our endoscopy unit provides the only nurse led flexible sigmoidoscopy surveillance service for FAP patients in the UK. Our aim of this study was to determine the surveillance outcomes of this large cohort of FAP patients following total colectomy.
Aims and Methods: This was a prospective analysis of six hundred and twenty consecutive FAP patients with either ileo-rectal anastomosis or ileal pouch anal anastomosis who had undergoing flexible sigmoidoscopy by a single nurse endoscopist (RM) over a period of two years (October 2002 to October 2004).
Results: A total of 725 polyps were resected—583 were snare polypectomies, and 142 polyps were destroyed by argon plasma coagulation. No post-polypectomy bleeds or perforations occurred. Histologically, the resected polyps were ranged from tubular adenomas to villous adenomas with mild to moderate dysplasia. Twenty patients were referred for further endoscopic mucosal resection due to large or board based polyps. A further 12 patients with polyps close to the dentate line were not suitable for endoscopic resection, and were referred for transanal surgical excision. Two patients required removal of the rectal remnant for extensive or severely dysplastic polypoid lesions. No cancers were detected during this period. Importantly, no missed cancers were reported during follow up of this patient group.
Conclusion: FAP patients after colectomy require life long endoscopic surveillance. Nurse led surveillance for removal of adenomas cancer prevention by flexible sigmoidoscopy appears to be safe, reliable, and effective.
1
2
3
4
5
280 RESULTS OF SCREENING COLONOSCOPY IN FAMILIAL COLORECTAL CANCER
P. S. Phull1, H. Gregory2, Z. Miedzybrodska2.1Gastrointestinal and Liver Service, Aberdeen Royal Infirmary; 2Department of Medical Genetics, University of Aberdeen
Introduction: The value of screening colonoscopy in familial colorectal cancer is uncertain. We performed an audit of subjects with a family history of colorectal cancer, referred by the regional genetics service for screening.
Methods: All subjects at risk of familial colorectal cancer reviewed by the regional genetics service over a three year period were identified from the genetics database. As a check, the endoscopy database at our institution was also used to identify such subjects who underwent colonoscopy. Case notes were retrieved and data collected for demographic details, the risk category for familial colorectal cancer (as defined in the SIGN guidelines for colorectal cancer), and colonoscopy findings. Symptomatic patients, subjects with FAP, Peutz-Jeugers syndrome or other rare high risk disorders were excluded.
Results: Of the total of 213 subjects identified, 63 did not meet the inclusion criteria. Of the remaining 150 subjects, 99 (66%) were in the moderate risk group, and 51 (34%) were in the high risk group for familial colorectal cancer. In the moderate risk group, 12 of the 99 (12%) subjects had adenomatous colorectal polyps identified. All cases except one had single polyps; one subject had over 40 polyps, the largest being 2 cm in diameter. Subjects aged >50 years were more likely to have adenomatous polyps (17.5% v 8.5% of those aged <50 years). In the high risk group, 11 of the 51 (22%) of subjects had adenomatous polyps found at colonoscopy (25% of those aged <50 years v 15.8% of those aged >50 years). All subjects had single polyps and only one had a polyp greater than 1 cm in size. There were no cases of high grade dysplasia or carcinoma identified.
Conclusions: Screening colonoscopy in familial colorectal cancer identifies a significant number of subjects with adenomatous polyps. The yield of screening colonoscopy is greater in high risk subjects or moderate risk subjects over the age of 50 years.
281 AUDIT OF NEGATIVE LOWER GI INVESTIGATIONS PRECEDING FINAL DIAGNOSIS OF COLORECTAL CANCER
A. Somasekar, B. M. Stephenson, K. D. Vellacott, I. W. Thompson, L. James, M. C. Allison.Royal Gwent Hospital, Newport, South Wales
Background: Recent studies highlight miss rates for colonoscopy and barium enema (BE). We reviewed records on all patients presenting to our multidisciplinary team (MDT) with colorectal cancer (CRC) from January 2000 to June 2004 to identify those who had previous lower GI investigations that had not found CRC, and to examine possible causes of detection failure. Our colorectal MDT serves a 400 000 population.
Methods: Case ascertainment was done using the clinical, endoscopy, and histopathology databases. Patients with recurrent CRC or second cancers were excluded. For the remaining 585 patients we audited all BEs, flexible sigmoidoscopies (FS), colonoscopies, and colorectal pathology during the 5 years before the eventual diagnosis of CRC.
Results: 31 patients (5%) had undergone lower GI endoscopic investigation during the 6–60 months before their eventual cancer diagnosis. These were subdivided as follows: 1) a relevant abnormality was seen in seven patients, but there was a delay in final characterisation as malignant; 2) seven patients with cancer complicating inflammatory bowel disease were identified at surveillance or presented with interval cancers; 3) six patients had been under polyp follow up of whom two were diagnosed at surveillance and four had been discharged from surveillance; 4) four patients had undergone an incomplete colonoscopy and later developed right sided cancer; 5) two had undergone FS but later presented with proximal cancer; 6) three patients had undergone apparently complete colonoscopy 1, 3 and 4 years before cancer diagnosis—these may be true missed lesions; 7) two patients had undergone a negative FS two years before eventual diagnosis of recto-sigmoid cancer. Adding 6) and 7) gives a true miss rate of only one patient per year. 28 patients (5%) had negative BE a median 3 (1–4) years before diagnosis of rectal (10 patients), sigmoid (10), descending (2), and proximal CRC (6).
Conclusion: These results confirm that complete colonoscopy rarely misses colorectal cancer. The methodology described herein may assist MDTs in surveying their current practice and maintaining the quality of their colonoscopy services.
282 WAITING LIST VALIDATION FOR SCREENING AND SURVEILLANCE COLONOSCOPY
B. H. Hayee, M. Barnden, A. Harris.Kent and Sussex Hospital, Tunbridge Wells, Kent TN4 8AT, UK
Introduction: The waiting time for screening or surveillance colonoscopy (SSC) is between 6 to 18 months at the Kent and Sussex Hospital. In the light of current guidelines1 and recommendations from the NHS Modernisation Agency,23 a recent local audit showed that 10% of patients were ineligible for SSC, while 40% of the remainder were being investigated at an inappropriate interval.4
Methods: 300 consecutive patients were selected from the Endoscopy Database (Metasa, UK): 100 from each consultant waiting list. The study was then extended to include all patients on one consultant waiting list (n = 200). Medical notes were searched to determine indications for SSC and follow up interval. Ineligible patients were contacted by detailed letter and removed from the waiting list with the option to contact the department.
Results: Of the 300 patients (143 male; average age 54), 72 (24%) did not meet BSG guidelines for SSC and could potentially be removed from follow up. Of the remainder, a further 132 patients (58%) could have their follow up interval extended. From 200 patients on a single consultant waiting list, 41 were identified and contacted by letter. Of these six expressed extreme concern at the decision whilst four requested an outpatient appointment to discuss the matter further. The remaining 31 (75%) have not replied (eight weeks later).
Conclusions: Waiting list validation using BSG guidelines results in significant reductions in waiting list length, without increases in resource allocation. This approach must be sensitive to patients’ concerns, but appears acceptable to the majority. The largest gains would be made by strictly applying BSG guidelines to screening for family history and polyp surveillance.
Acknowledgements: Dr R. H. Loke and Mr A. J. Cook.
1
2
3
4
283 SAFETY AND EFFECTIVENESS OF COLONOSCOPY IN THE ELDERLY
M. A. Karajeh, D. S. Sanders, R. Kalla, V. Campbell, D. P. Hurlstone.Royal Hallamshire Hospital, Glossop Road, Sheffield S10 2JF, UK
Background: Optical colonoscopy is the diagnostic gold standard for imaging of the colon and rectum and has the advantage of allowing biopsies and polypectomy. However, there may be reluctance to refer elderly patients for colonoscopy because of a perception of a higher risk of complications and a high rate of incomplete examinations.
Aims: We prospectively assessed whether there are differences in the completion rates, diagnostic yield, complication rates, and 30 day mortality between patients over the age of 65 years and patients under the age of 65 years, undergoing colonoscopy at our centre.
Methods: Data were collected from a prospective database on 2000 colonoscopies performed at a single university teaching hospital over a two year period (January 2002 to January 2004). We compared 1000 colonoscopies in patients over age 65 years with 1000 colonoscopies in patients under age 65 years (control group). Data were collected on sedation, “crude” and “adjusted” completion rate (discounting failures due to obstructive pathology and poor bowel preparation), diagnostic yield, complications, and 30 day mortality.
Results: The median age was 75 years (51% females) for the elderly group and 54 years (59% females) for controls. The proportion of patients who received sedation was similar for both groups (59% v 62%, p = 0.97) but the mean dose of midazolam was lower in the elderly group (3.8 mg v 4.5 mg, p<0.0001). The “crude” completion rate was lower for the elderly group (81.8% v 86.5%, p = 0.004), but the “adjusted” completion rate was similar for both groups (92.3% elderly v 90.5% control, p = 0.18). The overall diagnostic yield was higher in the elderly group (65% v 45%, p<0.0001) with higher rate of carcinoma detected (7.1% v 1.3%, p<0.0001). The complication rate was low with no difference between the two groups (0.2%): 2/1000 cases of transient tachycardia and bradycardia per group. There was one death in the elderly group within 30 days (bronchopneumonia).
Conclusions: Colonoscopy in the elderly is safe and effective with a high diagnostic yield.
284 VARIABLE STIFFNESS COLONOSCOPES ARE A DISADVANTAGE IN MALE PATIENTS IRRESPECTIVE OF THEIR BODY MASS INDEX
J. Hancock1, D. Nylander1, J. Painter1, L. Fowler1, R. Rowland2, G. D. Bell2.1Gastroenterology Department, Sunderland Royal Hospital, Sunderland; 2School of Computing Sciences, UEA, Norwich NR4 7TJ, UK
Background and Aims: Clinical trials of variable stiffness colonoscopies (VSC) v conventional colonoscopies (CC) have been conflicting. Colonoscopy in women takes longer and cause more pain than in men. Patients with a low BMI (irrespective of gender) may similarly take longer due to a greater propensity to looping. We decided to see if gender and BMI should affect an experienced endoscopist’s decision to use either a VSC or CC.
Methods: A total of 49 patients (28 male and 21 female with mean (SD) ages, and BMIs of 55.1 (SD 17.1), 53.1 (SD 15.5), 25.6 (SD 5.0), and 25.7 (SD 6.5), respectively) had their colonoscopies carried out by one of two experienced colonoscopists (DN and JP) using, at random, either an Olympus CF240L (CC) (n = 27) or a CF240AL (VSC) (n = 22). Patients were offered to be sedated or not. Those sedated had relatively small doses of midazolam plus additional analgesis with pethidine or Entonox if necessary. A magnetic endoscope imager and ‘painometer’ (Gut 2000;46(suppl II) A30) was used and the ‘painometer’ pressed whenever the patient indicated significant discomfort.
Results: Female patients experienced more discomfort (p<0.0004) and requested Entonox significantly more frequently then men (p<0.03). Caecal intubation times were shorter in males than females (10.8 (SD 7.9) v s 14.9 (SD 5.6), p<0.001). In both sexes there were highly significant correlations between caecal intubation times and discomfort scores but no correlation between BMI and either variable. In the CC group (both sexes), there was no significant difference from the VSC group for either discomfort score or speed of caecal intubation. However analysis by gender revealed male patients had less pain and a shorter caecal intubation time (mean 3 min, p<0.001) when a CC was used.
Discussion: Even in females, the advantages of a VSC are marginal. In male patients a CC actually performs significantly better than a VSC and is now our preferred instrument in this group. BMI need not influence the decision as to whether or not to use a VSC or CC.
285 THE USEFULNESS OF A PAEDIATRIC SCOPE OR GASTROSCOPE IN DIFFICULT COLONOSCOPY CASES
N. Suzuki, C. Thapar, N. Palmer, C. Williams, B. Saunders.Wolfson Unit for Endoscopy, St Mark’s Hospital, London, UK
Background: Colonoscopies can be difficult in some instances, even when performed by an expert. To tackle these cases, the employment of a paediatric scope was reported to be effective.
Aim: To examine the efficacy of changing instruments during colonoscopy for difficult cases; to determine the capability of using a gastroscope for colonoscopy.
Methods: A retrospective review of consecutive colonoscopy cases between 2001 and 2003 was performed. Data from cases considered as difficult by experts (BPS/CBW/NS) (i.e. requiring more than two instruments for the insertion) was collected. The indication, reason for difficulty, instrument used, and site reached were examined.
Results: In total 4084 colonoscopies were performed by the expert colonoscopists during this period, of which 76 cases (1.9%) required more than two scopes. Difficulties were due to a challenging sigmoid: fixation 36, sigmoid loop/tortuous sigmoid 22, narrowed/stricture 10, or discomfort 2 (not recorded in five). These were secondary to diverticular disease in 34, hysterectomy in 8, cancer in 5, previous radiation therapy in 2, and anastomotic stricture in 1. A standard colonoscope (CF 200 230 or 240) was used as a first scope in 74 of 76 cases. The other two cases were started with a paediatric scope (PCF). As a second scope, a PCF and a gastroscope (GIF) were used in 67 and seven cases, respectively. The other two cases were completed with a variable stiffener or imager scope. The six cases in which the experts could not get through the sigmoid colon with a paediatric scope, a further attempt was undertaken with a GIF (third scope). Total colonoscopy was possible in 66% of the cases, with a challenging sigmoid colon, by changing instruments. In addition, the problematic sigmoid was passable in a further 17%, despite incomplete colonoscopy. When a GIF was used in colonoscopy, the difficult sigmoid was passed in 92.4%, with a total colonoscopy rate of just 54%.
Conclusion: The use of a smaller calibre scope is effective to negotiate challenging sigmoid colons. When using a gastroscope in experts’ hands, total colonoscopy can be achieved in more than half the number of cases.
286 DOES COMPLETING THE AUDIT CYCLE IMPROVE COLONOSCOPY RESULTS?
P. Duane, A. Parcell, T. Brown, S. Caplin, J. Baxter, U. Dave.Morriston Hospital, Swansea, UK
Introduction: Recent UK national colonoscopy audit has shown the caecal intubation rate to be only 77% (Gut 2004;53:277–83). With the proposed colorectal cancer screening programme in the UK, the need for improved caecal intubation rate is crucial. A recently published article has shown that a quality improvement programme (e.g. further colonoscopy training, inpatient bowel preparation, and increased colonoscopy time) using two completed cycles of audit improved colonoscopy completion from 60% to 88% (
) . We believe that the process of audit itself may contribute to the demonstrated improved completion rates.
Method: Retrospective audits of colonoscopy completion were carried out in 1997, 1998, and 2003. No specific measures were introduced between 1997 and 2004 but after each audit cycle results were discussed in the departmental meetings and need of improved colonoscopy completion were stressed. A prospective audit was carried out for 7 months in 2004 where completion and patient discomfort were recorded by the endoscopist and endorsed by the endoscopy nurse.
Results: See table.
Abstract 286 Table
Discussion: Colonoscopy completion rate improved from 55% in 1997 to 85% in 2004. Repeated audits of colonoscopy may contribute to improved completion by making individuals aware if they are not performing satisfactorily.
287 DATA MINING TECHNIQUES CAN BE USED TO RAPIDLY INTERROGATE AN ENDOSCOPY DATABASE AND CALCULATE ‘ADJUSTED’ COLONOSCOPY SUCCESS OR FAILURE RATES—BUT WHAT CRITERIA SHOULD BE USED TO DEFINE SUCH SUCCESS?
K. Sheikh1, A. P. Reynolds2, B. de la Iglesia2, G. D. Bell1, R. Tighe1.1Endoscopy Unit, Norfolk and Norwich University Hospital, Norwich NR4 7UY, UK; 2School of Computing Sciences, UEA, Norwich NR4 7TJ, UK
Introduction: We have studied our unit’s success rates for total colonoscopy and also the various reasons/excuses given by different endoscopists when the caecum (or alternatively surgical anastomosis) was not reached. The results can be presented either as ‘crude’ or some form of ‘adjusted’ intubation rate: but what form should this take?
Methods and Results: We applied various data mining techniques (Gut 2004 (Suppl 3):A51) to interrogate our endoscopy unit’s database (Endoscribe) from February 2002 to May 2004. We identified 4889 colonoscopies performed by 49 different endoscopists. The initially data mining exercise identified possible 649 ‘failures’. One of us (SK) then examined by hand the original endoscopy report (plus where necessary the case notes) of all 649 patients. Only 12/649 (1.9%) were reclassified as being successes. Thus the crude colonoscopy failure rate was 637/4889 or 13.1%. If we serially excluded the following: planned limited colonoscopy (n = 35), obstructing cancer (n = 118), diverticular disease (n = 61), poor bowel prep (n = 180), and finally ‘other reasons’ (n = 38), then the adjusted unit’s colonoscopy failure rate fell to 12.4%, 10.2%, 9.0%, 5.4%, and 4.5%, respectively
Discussion: Using data mining methods, we were relatively easily able to obtain an accurate ‘crude’ colonoscopy success rate: either for the unit as a whole or any individual endoscopist. The same techniques can be used to derive ‘adjusted’ success/failure rates. This begs the question as to which ‘failures’ to exclude from any such ‘adjusted success/failure’ calculation. It would seem reasonable to exclude impassable neoplasms and planned limited examinations but not looping, pain, and intolerance. There remains the ‘grey area’ of whether ‘poor bowel prep’, all/some ‘diverticular disease’ and ‘instrument failure’ should be included in any such ‘adjusted’ success rate figure.
288 THE VALUE OF ROUTINE TERMINAL ILEAL BIOPSY TO DOCUMENT SUCCESSFUL COMPLETION OF COLONOSCOPY
S. Sen1, R. J. C. Steele2, P. S. Phull1 on behalf of the Scottish Colorectal Cancer Screening Pilot1Gastrointestinal and Liver Service, Aberdeen Royal Infirmary, Aberdeen, UK; 2Ninewells Hospital and Medical School, Dundee, UK
Background: Complete visualisation of the colon is an important quality assurance parameter for colonoscopy. The ‘gold standard’ for documenting this remains terminal ileal biopsy after intubating the ileo-caecal valve, but this utilises extra resources. The present study evaluated the usefulness of such biopsies in documenting completion of colonoscopies.
Methods: Data collected prospectively by the Colorectal Cancer Screening Pilot in Scotland were audited to retrieve claimed completion rates of colonoscopy, number of procedures where terminal ileal biopsy was used to document completion, and was correlated with the actual histology.
Results: During the audit period, a total of 4393 colonoscopies were performed, of which 3912 (89%) were documented as having been ‘completed’. Terminal ileal biopsies were used to document completion in 506 procedures (13%). Histology was available from 387 procedures; in 369 cases, terminal ileal biopsies were taken solely to document completion of colonoscopy. Of these 369 biopsies, 362 (98%) proved to be from the terminal ileum on histology. Fourteen colonoscopists performed terminal ileal biopsies for documentation of completion of the procedure. However, 286 of the 369 biopsies (78%) were performed by just two of the colonoscopists. For these two operators, 283 of the 286 biopsies proved to be from the terminal ileum (99%).
Conclusion: In the case of colonoscopists who have a high rate of successful intubation of the ileo-caecal valve, there is a near perfect concordance (99%) between ‘claimed’ colonoscopy completion and histologically proven completion. This suggests that for such colonoscopists, routine terminal ileal biopsy is unnecessary for documentation of completion.
289 90% CAECAL INTUBATION RATE: WHAT HAPPENS TO THE OTHER 10%?
E. A. Johns, D. A. Gorard, A. S. McIntyre.Department of Gastroenterology, Wycombe Hospital, High Wycombe, Bucks HP11 2TT, UK
Aims: JAG guidelines suggest “Caecal intubation rates should exceed 90% in patients without stricturing or marked contamination”. We aim to establish what happens in those patients where caecal intubation is not achieved.
Method: All colonoscopies performed over a three year period (January 1998 to December 2000) were analysed. Examinations were deemed incomplete if the caecum, terminal ileum or surgical anastamosis were reported as not having been reached. Incomplete colonoscopy reports were analysed (demographics, indication, extent, and reason for failure), medical notes retrieved, and GP surgeries contacted to establish what happened next. A minimum follow up period of 36 months was chosen on the basis that any missed malignant pathology would have revealed itself within this time frame.
Results: Of the 1525 colonoscopies performed 1262 (83%) were complete and 263 (17%) incomplete. The adjusted caecal intubation rate (reason: marked contamination 48, strictures 47, other 19) was 90%. Individual operator rates varied between 84% (95% CI 70 to 94) and 98% (95% CI 95 to 100). Of the 1262 completed procedures cancer was identified in 45 patients (3.5%). Of the 263 patients who underwent an incomplete procedure, 46 were excluded as no notes were available, and 18 did not meet the minimum follow up period. Of the remaining 199, there were 79 males, 120 females with a mean age of 62 (18–89) years, and mean follow up of 46 months. 12% had a further colonoscopy, 22% radiological investigations, 57% were assessed in clinic, and 9% no further follow up. New malignant pathology has subsequently been found in only two patients after 48 and 71 months. Neither was likely to have been identifiable at the index procedure had it been complete, because subsequent barium enema and complete colonoscopy were normal within two years of the incomplete test.
Conclusions: The 10% of patients in whom caecal intubation is not achieved have a low risk of malignancy being identified. In our unit only one third of patients were deemed to require further colonic imaging after incomplete colonoscopy, without any adverse effects for those not being further investigated. A proportion of patients referred for colonoscopy probably only require left sided or limited colonoscopy to explain symptoms. Failure to complete a colonoscopy should only lead to further investigation if indicated by the symptomatology.
Radiology posters
290 ARE THE SOPHISTICATED 21ST CENTURY RADIOLOGICAL INVESTIGATIONS RELIABLE IN PREDICTING WHICH PATIENTS SHOULD UNDERGO A LAPAROTOMY?
A. J. Shah, S. Rajagopalan, R. Hargest, S. Ghosh, R. J. Delicata, R. L. Blackett, C. Bransom, D. R. B. Jones.Nevill Hall Hospital, Abergavenny, UK
Aims: To determine if laparotomy based solely on the basis of initial clinical and radiological diagnosis is acceptable in current clinical practice.
Methods: Data were audited on the last 100 consecutive emergency laparotomies performed at a district general hospital over a period of 14 months. Re-Look laparotomies for removal of packs were excluded. The initial clinical diagnosis at admission by a middle grade surgeon and a radiological assisted diagnosis (ultrasound scan (USS)/computerised tomography (CT scan)/magnetic resonance imaging (MRI)/gastrograffin enemas) carried out by a consultant radiologist were documented. These were then compared with the operative findings.
Results: 100 patients underwent an emergency laparotomy. Three of them were laparotomies for either change or removal of packs. 46/97 had a laparotomy on the basis of initial clinical and plain x ray findings only (ruptured abdominal aortic aneurysm, perforated viscus, small bowel obstruction secondary to irreducible hernias). 51/97(53%) had a more advanced radiological investigation prior to surgery. 26 had USS, 19 had a CT scan, two underwent an MRI, two had a barium enema, and two patients a gastrograffin contrast enema.
Out of the 26 USS, only 8 (31%) had a radiological diagnosis that matched the operative findings. Only 4/19 (21%) CT scans had findings confirmed at laparotomy, 1/2 (50%) for MRI, and none in barium enema. However both the gastrograffin studies matched the operative finding. Radiological diagnosis was accurate in only 15/51 (29%) patients. Clinical diagnosis was correct in only in 30 out of 97 patients (38%). Further analysis revealed that in only 22/51 (43%) of patients, combined clinical and radiological diagnosis matched the operative findings.
Conclusion: Neither clinical nor radiological diagnosis alone could achieve an accurate diagnosis. Combining clinical and radiological information did not result in a substantial improvement in the diagnosis. Exploratory laparotomy should still be considered where there is a suspicion of peritonitis or an unsettling acute abdomen as even a CT scan of the abdomen does not have a great diagnostic accuracy.
291 THE NETWORKING CAPABILITIES OF A LAPTOP BASED 3D DICOM VIEWER TO FACILITATE MULTI SITE MDTS
D. J. T. Heatley1, R. S. Rowland2, G. D. Bell2, S. L. Smith3, D. M. Rae4, D. L. Hegarty5, I. H. K. Scott4.1BT Group, Ipswich IP5 3RE; 2School of Computing Sciences, UEA, Norwich NR4 7TJ; Depts of 3Radiology; 4Surgery; 5Business Development, The Ipswich Hospital, Ipswich IP4 5PD, UK
Background: Our group previously presented the development and trials of a laptop based 3D DICOM viewer (www.di-sect.com) for single site MDT cancer meetings where high end viewing facilities are unavailable (Gut 2004;Supp III:A79). We showed that a suitable low cost laptop, running our software, reproduces the image quality and 3D view features of high end workstations used in radiology departments. Our most recent work explores the networking capabilities of this system for multisite MDT meetings within and between different hospital trusts.
Methods and Results: We have demonstrated that diagnostic quality DICOM images can be shared between multiple locations by, (1) transmitting them as video over the hospital LAN or telephone network (ISDN6) using the video conferencing stations available in most hospitals, or (2) deploying our laptop based system at each location, all displaying the same DICOM file, and interconnected via the network. The first approach delivers video and audio commentary to all locations but is limited by the availability of video conferencing stations. The remote image quality is also slightly reduced. However, the second approach can operate almost anywhere, delivers pristine image quality at all locations, although only supports audio commentary.
Conclusions: Broadly, the second configuration affords multisite MDTs the greatest flexibility and best image quality. The absence of a video view of the other location(s) does not hinder interactions within the team. However, the need for duplicate data at each location requires careful attention, and we are exploring ways of auto-deleting the duplicates when the meeting ends. In contrast, the first configuration only requires the DICOM file at the “head end” and so avoids duplication. Ultimately the optimum choice is dependent on several factors. Nevertheless the potential improvement in the efficacy of multisite MDTs is already clear, as are the potential cost savings.
292 EXTRACOLONIC ABNORMALITIES FOUND AT VIRTUAL COLONOSCOPY
M. Bose, J. Bell1, P. Casey, L. Jackson, O. Epstein.Academic Department of Gastroenterology & 1Department of Radiology, Royal Free Hospital, London, UK
Introduction: The Royal Free virtual colonoscopy (VC) study has been designed to explore the possible role of VC in the future of gastroenterology diagnostics. A potential advantage of VC over optical colonoscopy (OC) is the ability of VC to detect extracolonic lesions.
Methods: Outpatients aged >50 years old whose investigation included colonoscopy were invited to participate in a study of VC. This entailed attending for a virtual colonoscopy (V3D Viatronix) on the same day and prior to their OC. A radiologist (JB) skilled in reading 2D and 3D CT reconstruction reported both the VC and extracolonic findings which were added to the study database. This study reports the prevalence and significance of extracolonic findings in 50 patients who underwent VC prior to OC.
Results: Among the 50 patients there were 34 females and 16 males participants with a mean age of 62.6 (SD 8.9) years. In 14 patients (28%) there were no extracolonic findings. The radiologist described extracolonic abnormalities in 36 patients (72%). These included gallstones (4), hiatus hernia (7), liver calcification or cysts (6), renal abnormalities (8), adrenal adenomas (3), vascular calcification (9), gynaecological abnormalities (6), lung disease(4), and bony abnormalities (12). The radiologist advised further investigations in four cases (8%). These were: ultrasound for a mixed liver cyst, pelvic MRI for possible endometriosis, investigations for renal medullary calcinosis, and a further CT to evaluate one of the three adrenal adenomas. Other clinically significant findings that required further action were the presence of a lung nodule and a significant abdominal aortic aneurysm.
Conclusion: In addition to offering a minimally invasive method for examining the colon VC has the additional byproduct of providing extracolonic information some of which might be valuable in the overall assessment of the patient’s abdominal symptoms.
GI physiology posters
293 USE OF OESOPHAGEAL MANOMETRY AS A DIAGNOSTIC TOOL IN SRI LANKA
T. G. H. C. Ferdinandis, K. I. Deen, H. J. De Silva.Faculty of Medicine, University of Kelaniya, Sri Lanka
Background: Oesophageal manometry is a useful investigation in patients with oesophageal symptoms, when endoscopy and radiological findings are negative or equivocal. Though it is widely used as a clinical tool in hospitals in the UK and Europe, the facility is not freely available for patients in South Asia. In Sri Lanka, with a population of 18 million, oesophageal manometry is available only at the Motility Lab of the Teaching Hospital, Ragama, which was established in 1997. Our primary aim is to review the referral patterns and to assess the usefulness of stationary and ambulatory oesophageal manometry as a diagnostic tool in the clinical setup.
Methods: Data obtained from patients referred (first referrals) for static and ambulatory manometry between 1997 and 2003 were reviewed. Oesophageal motility disorders were defined according to previously published literature. Manometry data obtained from healthy Sri Lankan subjects were also used for comparison with patient data.
Results: 156 stationary manometry and two ambulatory manometry studies have been performed during the above period. More than 95% of patients were referred by consultant surgeons and physicians practicing in the country’s capital, Colombo. Referred for oesophageal manometry to exclude oesophageal motility disorders were 82 males and 74 females. The mean duration of symptoms was 2.5 (SD 2.3) years. Reasons for referral were: dysphagia 79 (51%), regurgitation 20 (13%), non-cardiac chest pain 11 (7%), heartburn (with normal pHmetry) 10 (6.5%), connective tissue disease five (3%), atypical symptoms nine (6%), symptoms of non-ulcer dyspepsia 22 (14%). Manometry report was normal in 64 (41%) patients. Achalasia was the diagnosis in 44 (45%) patients. Eleven (25%) of them did not have all typical manometric features of achalasia. There were six (6%) patients with isolated LOS hypertension. Only three (3%) patients had manometry criteria of nut cracker oesophagus and one (1%) with diffuse oesophageal spasm. Ineffective oesophageal motility was seen in 37 (37%) patients and pathological acid reflux was found in 11 (30%) of them. A positive diagnosis was established in 55% of patients presenting with dysphagia, 18% with non cardiac chest pain, 10% with heartburn, 80% with connective tissue disease, 11% with atypical symptoms, and 17% with symptoms of non ulcer dyspepsia.
Conclusions: Stationary oesophageal manometry appears to be a useful diagnostic tool because it helped to establish a diagnosis in 59% of symptomatic patients with negative or equivocal endoscopic and radiological findings. Unfortunately, oesophageal manometry appears to be underutilised as a diagnostic tool by doctors serving in the outstations.
294 AUTOMATIC CLUSTERING AND CLASSIFICATION OF AMBULATORY OESOPHAGEAL MANOMETRY WAVEFORMS
A. Chan, K. R. Haylett, J. Globe1, A. Smythe1, P. Vales, R. F. McCloy2.GI Investigation Unit; 1University Department of Surgery, Royal Hallamshire, Sheffield; 2University Department of Surgery, Manchester Royal Infirmary, Manchester, UK
Introduction: Analysis of ambulatory oesophageal manometry (AOM) can be problematic due to the complexity and amount of data recorded. Although computer analysis is possible, problems are often experienced with the rules based software used to detect peaks and classify patterns. As a result station oesophageal manometry is still the gold standard for motility analysis despite the rarity of symptoms occurring during the investigations short study period.
Aims and Methods: This study aimed to develop a clustering technique to investigate the waves and patterns seen during AOM. The technique developed used a self organising feature map (SOFM) to cluster candidate events from 25 control studies. The only parameters used to select the candidates were a single threshold between the minimum and maximum value and the time in which an event must occur.
Results: This approach successfully clustered events seen during the AOM investigations without a predefined set of rules. Different types of peaks were identified and grouped into a range of different shapes and patterns. Having identified distributions of waves and patterns for asymptomatic controls, the developed SOFM can optimally fit new patient or control data and the rates of occurrence of different peaks and patterns can be found.
Conclusions: The developed technique successfully enabled the clustering and visualisation of waves and patterns of AOM waveforms. Although in its early stages of development, this technique may offer a new approach to the analysis of AOM data. Our current work involves comparing the control and patient data to determine if this technique can be used to routinely analyse AOM data.
295 ASSESSMENT OF A NOVEL SOLID STATE TRANSDUCER BILIARY MANOMETER
L. A. Smith, W. Jackson, K. Wedgwood, H. H. Tsai.Castle Hill Hospital, Hull, UK
Introduction: In the assessment of sphincter of Oddi dysfunction (SOD), biliary manometry is the accepted method for diagnosis. This is usually performed using a triple lumen catheter with a water perfused manometer. We have developed a bespoke solid-state transducer instead of a water perfused system.
Methods: Biliary manometry from 1999–2004 was performed using the solid-state manometer. The manometer is a pressure transducer attached to a 6 Fr catheter. Methods of measurement were as for standard manometry techniques, basal duodenal pressure was taken as zero. The biliary system was cannulated and the transducer withdrawn to the sphincter of Oddi. Pressures greater than 40 mm Hg were deemed abnormal. Sphincterotomy was performed in patients with high basal pressures or where clinically indicated. Cholangiogram was performed in all patients after manometry.
Results: Forty two patients were referred for manometry for recurrent abdominal pain from suspected SOD (40 biliary type and two pancreatic type). Successful cannulation and pressure readings were taken in 34 (81%). One failure was related to the catheter. 16 had abnormal liver function tests and 15 had associated dilated ducts. Two patients were found to have common bile duct strictures on cholangiogram following normal manometry, seven were found to have gallstones—all had normal manometry but underwent sphincterotomy for clinical indications. The 2 patients with pancreatic pain, 1 had SO pressure >40 mm Hg and had sphincterotomy. The 23 remaining patients with SOD, eight had abnormal SOP. 7/8 had a sphincterotomy performed. Only three patients with SOP <40 mm Hg underwent sphincterotomy, all were type II SOD, with recurrent admissions. The remaining 12 patients were a mix of type II and III SOD.
Discussion: There are several advantages that may be conferred by using a solid-state manometer, the transducer is easy to cannulate. There are no water perfusion effects on either biliary pressure or the pancreas seen with traditional manometers.
296 PATIENT SATISFACTION WITH pH STUDIES: BRAVO CAPSULE V NASOESOPHAGEAL CATHETER SYSTEM
J. T. M. Lee, M. Fox, A. Mohsen, R. Anggiansah, A. Anggiansah, T. Wong.Department of Gastroenterology and Oesophageal Laboratory, St Thomas’ Hospital, London, UK
Introduction: Limitations of conventional catheter based, 24 hour oesophageal pH studies are discomfort, inconvenience, interference with daily activity, and oral intake. The Bravo capsule is an innovative, endoscopically placed, catheter-free pH monitoring system that may be more acceptable to patients.
Aims: To evaluate patient satisfaction of naso-oesophageal catheter pH studies (N-pH) and Bravo catheter-free pH studies (B-pH).
Methods: A structured questionnaire assessed patient satisfaction in 18 patients investigated by B-pH (with previous failed N-pH monitoring) and 116 consecutive patients undergoing conventional N-pH. Ten questions assessed overall satisfaction, patient discomfort, and alterations to food intake/daily routine. Patient experience was scored on 5 point Likert scales (higher numbers representing a more positive experience). The responses were compared by χ2 analysis.
Results: Age and sex distribution were similar in both groups (p = NS). There was a strong trend (p = 0.06) to higher overall satisfaction with B-pH than N-pH; 93% of B-pH and 50% of N-pH patients were satisfied with the procedure (4-5/5), none of the B-pH group but 16% of N-pH was dissatisfied (1-2/5). Placement of the device was painful in 16% of B-pH and 17% of N-pH patients (p = NS), throat or nose discomfort was experienced during monitoring by none of the B-pH but 47% of N-pH patients (p<0.01). Swallowing difficulties for solids occurred in 60% of the N-pH v 44% B-pH patients (p = 0.09). Daily activity was restricted in 29% of N-pH but not in B-pH patients, 81% of N-pH v 36% B-pH did not go to work on test days (p = 0.08). 63% of N-pH v 100% of B-pH patients would recommend the test to another patient (p<0.02).
Conclusions: Most patients were satisfied by B-pH and N-pH; however satisfaction with B-pH tended to be higher and patients were more likely to recommend the catheter-free pH monitoring system to others. B-pH was better tolerated and interfered with daily life less than N-pH, although swallowing difficulties were not uncommon. The Bravo capsule is a well tolerated alternative to catheter based pH studies.
297 PROXIMAL OESOPHAGEAL pH MONITORING: SHOULD OESOPHAGEAL LENGTH AFFECT POSITIONING?
R. Anggiansah, M. Fox, A. J. Botha, D. Bartlett, T. Wong, A. Anggiansah.Department of Gastroenterology and Oesophageal Laboratory, St Thomas’ Hospital, London, UK
Introduction: Controversy exists regarding the positioning of the proximal pH probe for the evaluation of suspected reflux related extra-oesophageal symptoms and disease. In clinical practice many laboratories use a single catheter with two pH electrodes spaced at 15 cm. This technique does not account for variability of oesophageal length (OL), upper or lower oesophageal sphincter (UOS/LOS) position.
Aims: To establish whether the position of the proximal pH electrode relative to the UOS, LOS, and oesophageal length has effects on measurements of proximal acid exposure, and to identify relations between oesophageal length and measurements of reflux severity.
Methods: A retrospective study of 178 consecutive patients referred for dual oesophageal pH monitoring (median age 48 years, range 17–79). Manometry assessed LOS and UOS position and oesophageal length (OL: distal UOS to proximal LOS) by 1 cm stationary pull through. For 24 hour ambulatory pH studies a catheter with two pH electrodes spaced at 15 cm was placed with the distal electrode 5 cm above the LOS. Multivariate regression was used to identify any association of catheter position with OL and reflux events or severity (% time pH<4).
Results: Manometry demonstrated mean (SD) UOS length 3.5 (1.0) cm, LOS length 4.4 (0.9) cm, and OL 20.0 (2.3) cm. Seven patients (<4%) had OL ⩽15 cm (that is, less than pH electrode separation). There was no association of age or sex with sphincter or oesophageal length. No association was found between sphincter or oesophageal length with proximal reflux events or severity, and no interaction between proximal (or distal) pH electrode position and reflux parameters was present. Proximal reflux severity increased with age (p<0.03) and was associated with distal reflux severity (p<0.001), an effect that was more important in the upright than supine position (r2 = 0.33 v 0.17, p<0.01); however distal pH measurement alone would have failed to detect 30/178 (17%) patients with increased acid exposure (>1%) in the proximal esophagus.
Conclusions: The positioning of pH electrodes for oesophageal pH studies need not routinely account for UOS position or OL. Although closely associated with distal reflux, proximal pH studies increase sensitivity of pH monitoring for extra-oesophageal symptoms.
298 LUMINAL REGULATION OF INTESTINAL EPITHELIAL STEM CELL FATE
H. Dogra, L. Kruidenier, I. R. Sanderson, N. M. Croft, J. W. Wilson.Research Centre in Gastroenterology, Institute of Cell and Molecular Science, Queen Mary’s School of Medicine and Dentistry, University of London, UK
Background: The stem cell compartment of the gastrointestinal epithelium is important in development and in maintaining a state of homeostasis in the adult epithelium. Localised within the intestinal crypt, stem cells proliferate and differentiate to produce all epithelial cell lineages, tightly controlled by signalling molecular pathways such as Hedgehog and Wnt. Here, we have investigated if bacterial (LPS), inflammatory (IL-1β), or dietary agents (butyrate), which are known to regulate intestinal epithelial cell function, can also cause changes in stem cell number. We analysed the expression of the RNA binding protein Musashi-1 (Msi-1) as a marker for intestinal epithelial stem cells, using RT-PCR, western blotting, and fluorescence microscopy.
Results: Proliferating Caco-2 colonic epithelial cells showed a low basal expression of Msi-1, which decreased with time. Treatment with LPS or IL-1β did not affect Msi-1 expression. Addition of the short chain fatty acid butyrate, however, consistently downregulated the expression of Msi-1. Butyrate did not promote differentiation, as assessed by RT-PCR analysis of the differentiation markers Cdx-2 and NGN3. Furthermore, these changes in Msi-1 expression were independent of the presence of cyclopamine, an inhibitor of the Hedgehog signalling pathway, and the Wnt antagonist Dickkopf-1.
Because Wnt signals from subepithelial myofibroblasts are considered essential in maintaining the epithelial stem cell niche, we then co-cultured Caco-2 cells with CCD-18co colonic myofibroblasts. This caused a dramatic upregulation of Caco-2 Msi-1 expression, which could be diminished not only by Dickkopf-1 but also by butyrate.
Conclusion: Our results suggest that butyrate, a major luminal constituent in the colon, can affect stem cell numbers in the gut. Dietary manipulation of stem cell fate might be a novel strategy to prevent intestinal hyperplasia or to promote tissue repair.
299 THE EFFECTS OF BILE ACIDS ON INTESTINAL ION SECRETION IN THE TRICHINELLA SPIRALIS INFECTED MOUSE MODEL OF IRRITABLE BOWEL SYNDROME
N. Kalia, K. D. Bardhan1, J. Hardcastle, D. Grundy.Department of Biomedical Sciences, University of Sheffield; 1District General Hospital, Rotherham, UK
Background and Aims: The recent finding of disturbed bile acid function in irritable bowel syndrome (
) suggests that alterations in bile acid induced secretion could contribute to IBS associated diarrhoea. Therefore, the secretory response to BAs was examined in vitro in intestinal tissues from a Trichinella spiralis mouse model of post-infectious visceral hypersensitivity and control animals.
Methods:T spiralis infected Swiss mice were sacrificed at 18 and 25 days post infection (PI). Stripped sheets of jejunum and ileum from infected and non-infected control mice were mounted in Ussing chambers. Taurodeoxycholic acid (TDCA; 1 mM) or cholic acid (CA; 1 mM) was added serosally and peak increases in short circuit current (Isc), indicative of active anion secretion, were determined. Results are presented as mean (SEM), with n = 6 animals in each group.
Results: Basal ileal Isc was significantly increased (p<0.001) at 18 (80 (6) μA cm−2) but not 25 days (43 (5) μA cm−2) PI compared to control (46 (4) μA cm−2). However, basal jejunal Isc was unchanged at 18 (72 (5) μA cm−2) or 25 days (82 (10) μA cm−2) PI compared to control (83 (3) μA cm−2). Jejunal and ileal Isc responses to TDCA and CA were enhanced at 18 days PI but significantly so in the ileum. By 25 days PI, however, the augmented secretory response had reversed and was significantly reduced in both jejunum and ileum.
Discussion: Intestinal secretory responses to bile acids were augmented at 18 days PI, particularly in the ileum, but attentuated at 25 days, suggesting a biphasic influence of the PI process on bile acid induced secretion. Thus, increased bile acid induced ileal ion secretion may contribute to the diarrhoea associated with IBS.
Dr Kalia, Postdoctoral Fellow, is supported by The Bardhan Research & Education Trust (Registered Charity No 328452).
Nutrition posters
300 THE BURIED BUMPER SYNDROME
I. Tiwari, M. Roberts, K. Moore.Endoscopy Unit, Broomfield Hospital, Chelmsford CM1 7ET, UK
Introduction: As more and more patients are having feeding through a gastrostomy tube there is increasing number of complication being observed. Buried Bumper Syndrome (BBS) is a condition where the internal bumper of the gastrostomy tube is embedded in the gastric wall causing obstruction to the feeding. We report our experience of BBS over the last 3 years.
Methods: All patients who had BBS between June 2001 and August 2004 were identified from the records in the endoscopy unit. During this period 270 percutaneous endoscopic gastrostomies (PEGs) were performed on 238 patients and amongst them six patients had developed Buried Bumper Syndrome. These patients were studied in detail.
Results: We identified six patients with BBS during this period. There were two males and four females, age range 51–86 years (mean 72 years) with diagnosis of CVA (4), motor neuron disease (1), and mental handicap (1). Three patients had BBS within 4 weeks of PEG, two within 6 months, and one after a year. We had used Freca tubes on nine occasions, Tyco-Entristar tubes on 91 occasions, and Merck-Corflow tubes on 170 patients. All the patients who developed BBS had Tyco-Entristar tubes.
Some patients who developed BBS early after PEG were noted to pull and fiddle with the gastrostomy tubes. Entristar tubes seem to be more prone to cause BBS compared with Corflow tubes, although both are external traction removable. It was possible to pull the tubes out by traction in all the patients who had BBS and new tube was inserted at the same site and long term feeding could be continued following that.
Conclusion: Buried Bumper Syndrome is more common with external-traction removable gastrostomy tubes but they can easily be removed and a new tube inserted at the same site.
301 A NEW ROLE FOR THE NUTRITION NURSE SPECIALIST—FLUOROSCOPIC GUIDED INSERTION OF NASOJEJUNAL TUBES
F. Mohammed, N. Wilson, L. Telfer, J. Mason, C. Summerton.Trafford General Hospital, Manchester, UK
Background: The benefits of enteral nutrition when compared with parenteral nutrition are well established. However, provision of enteral nutrition may not occur because of lack of optimal feeding access. Many hospitalised patients are intolerant to gastric feeding, although they can tolerate small bowel feeding. Most institutions rely on endoscopic methods or fluoroscopy for placing nasojejunal feeding tubes. Placement is frequently delayed because other procedures requiring endoscopic or radiological equipment and staff take precedence. Our aim was to evaluate the effectiveness of a nutrition nurse specialist (NNS) in the fluoroscopic guided insertion of nasojejunal tubes.
Methods: The NNS established a protocol for the fluoroscopic guided insertion of NJ tubes. 8Fr, 150 cm stylet, Merck single lumen tubes were used. A push and pull technique was used to advance the tube into the third part of the duodenum or beyond. Final tube position was confirmed by injecting Omnipaque, followed by an abdominal radiograph, which was reviewed by a consultant radiologist.
Results: Ten tubes were attempted over an 8 month period. Seven (70%) were successfully placed postpylorically with 40% at or beyond D3. Of the three unsuccessful placements, one patient was discovered to have a large hiatus hernia and another had had previous gastric surgery. Indications for jejunal feeding were postoperative feeding (four cases); carcinomatosis with nausea and poor appetite (three cases); pancreatitis (two cases); and aspiration (one case). The average radiological screening time to achieve tube placement was 10.5 minutes (range 1–27). There were no complications of tube insertion or from feeding. Average duration of feeding via the inserted tubes was 10.6 days (range1–20). During the audit period there was a 35% reduction in parenteral feeding.
Conclusions: A NNS can successfully insert nasojejunal tubes using a fluoroscopic method in appropriately selected patients. This could represent a new role for nutrition nurses, leading to timely enteral feeding and a decrease in parenteral feeding.
302 A DOUBLE BLIND TRIAL OF IMMUNONUTRITION V ISOCALORIC FEEDS AFTER MAJOR UPPER GASTRO INTESTINAL SURGERY
C. B. Pearce1, S. S. Somers2, S. K. Toh2, S. A. Sadek2, A. M. Walters2, T. Johns2, H. D. Duncan1.1Department of Gastroenterology; 2Department of Surgery, Queen Alexandra Hospital, Portsmouth, UK
Introduction: The gut-origin-of-sepsis hypothesis identifies the “leaky gut” as an essential factor in developing septic complications with multi-organ failure in post surgical patients. This effect may be ameliorated by enteral nutrition. Although, immunonutrition has shown improved outcomes in some surgical patients, there is a need to investigate its potential role in patients after major upper gastrointestinal surgery (MUGIS) and the mechanisms behind any identifiable benefits.
Aims: To investigate the benefit that enteral immunonutrition has over isocaloric control feeds in MUGIS.
Methods: A double blind trial of a prototype enteral feed containing glutamine, arginine, ω-3 fatty acids, tributyrin, antioxidants, and micronutrients versus an isocaloric isonitrogenous control feed was undertaken. Patients after upper GI surgery requiring tube feeding alone for ⩾5 days were eligible. All patients were fed using needle jejunostomy tubes inserted at operation until oral feeding was possible. The study period was over the first 5 days post surgery with the C-reactive protein (CRP) and retinol binding protein (RBP) used as markers of systemic inflammation and nutrition respectively.
Results: Forty four patients were randomised, 23 received study and 21 control feeds. RBP levels in the study group were significantly higher than in the control group at day 5 (p = 0.0284). There were no significant differences in CRP between the two groups neither at any point nor in adverse events or other outcome measures, including infection rate, length of hospital stay, and time in ITU
Comments: The increase in RBP suggests an improved nutritional status in patients given the prototype feed. As studies of immunonutrition have shown improved outcomes in surgical patients, improved nutritional status and/or RBP may be a factor in these findings and is worthy of further investigation.
303 LIVER TOXICITY IN PARENTERAL NUTRITION: ROLE OF CYCLICAL INFUSION
J. A. Binnie1, L. Linton-Willoughby2, R. J. Harvey1, J. B. Saunders1, W. S. Wassif3.Departments of 1Gastroenterology, 2Pharmacy, and 3Clinical Biochemistry, Bedford Hospital, Kempston Road, Bedford, MK42 9DJ, UK
Background: Liver toxicity is a well recognised complication of parenteral nutrition (PN) thought to result from provision of energy in excess of requirement. Patients with underlying liver disease, those who are septic, and those who have had surgery are at particular risk. The risk of developing liver toxicity is increased in patients unable to tolerate enteral feeding and the pattern of liver damage is one of hepatic steatosis and cholestasis. In the majority of adults liver toxicity is self-limiting and resolution occurs once enteral feeding is established. Deranged alkaline phosphatase (AP) occurs early in therapy, other liver enzymes may increase subsequently. Rarely does the bilirubin rise.
Methods: Forty three sequential adult patients required PN from 1 August 2003 to 31 July 2004. If liver tests were abnormal and no other cause identified nor was there the possibility of introducing enteral feeding then the total calorie content of PN was reduced. After 48 hours of calorie reduction, cyclical infusion was commenced.
Results: AP fell significantly after cyclic PN was initiated (see table). There was no significant difference between the two groups in bilirubin or AST activity or albumin concentrations.
Abstract 303
Conclusion: Cyclic PN appears to prevent further deterioration in liver tests and may reverse abnormalities. Patients with pre-existing liver disease and abnormal liver enzymes at initiation of PN are more likely to require cyclic PN and abnormalities are more likely if duration is prolonged. Cyclic PN should be routinely considered in patients with pre-existing liver disease and increased liver enzymes once they are haemodynamically stable on PN.
304 ENDOSCOPIC V RADIOLOGICAL GASTROSTOMY: AUDIT OF OUTCOMES IN A DISTRICT GENERAL HOSPITAL
R. Wong, M. R. Price, J. Bickerstaff, N. Reading1, E. M. Alstead, L. Langmead.Departments of Gastroenterology and 1Radiology, Whipps Cross University Hospital, London, UK
Background: Feeding gastrostomy is an established method of maintaining long term enteral nutrition. Techniques for insertion are percutaneous endoscopic gastrostomy (PEG), radiologically inserted gastrostomy (RIG), or surgical. The choice of method may be based on availability rather than suitability.
Aim: To review outcomes of PEG and RIG at an 800 bed district general hospital.
Methods: Records of patients who had PEGs and/or RIGs inserted between 1/1/04 and 30/9/04 were reviewed for 7 and 30 day morbidity and mortality. Patients or carers were contacted to provide details of late complications. Other data included patient demographics, indication, time from request to insertion, antibiotic use, and tube failure rate.
Results: Twelve patients (6M, 6F), age 63 years (43–80), (median (range)) had PEGs. 29 patients (16M, 13F), age 66 years (48–93) had RIGs. Stroke was the most frequent indication. Overall, mortality was 18%. There was no difference in 7 or 30 day mortality between the two groups. No deaths were procedure related. Early complications were more frequent after RIG (31%, tube failure = 3, site infection = 2, pneumonia = 1, septicaemia = 1, pain = 1) than PEG (0%) p<0.04). Late complications occurred in 37% of RIGs (tube failure = 4, site infection = 3, pneumonia = 1, UTI = 1, MRSA = 1) and 9% of PEGs (pneumonia = 1) (p<0.05). Comorbidity did not increase complication rate. No PEG tubes failed, 13% of RIGs failed. Median time from request to insertion was greater for PEGs (16 days) than RIGs (9 days) (p<0.0005). Patients under the care of gastroenterologists were more likely to have PEGs inserted than those under the care of non-gastroenterologists (p<0.01).
Conclusion: Complication rates of RIGs were similar to published data but for PEGs were low. Limited access to PEGs means that RIGs are performed preferentially, especially by general physicians, despite a higher complication rate. Additional resources are needed to increase availability of PEG insertion as an effective and safer alternative to RIG.
305 MANGANESE AND CHROMIUM STATUS IN PATIENTS BEFORE, DURING, AND AFTER PARENTERAL NUTRITIONAL SUPPORT
J. E. East1, R. Ramnarace1, L. Linton-Willoughby2, J. Binnie1, S. Enaganti1, K. Davies3, R. J. Harvey1, B. Sampson4, W. S. Wassif5.Departments of 1Gastroenterology, 2Pharmacy, 3Dietetics, 5Clinical Biochemistry, Bedford Hospital; 4Clinical Chemistry, Charing Cross Hospital, UK
Background: Recent reports have emphasised the need to ensure optimal daily amounts of micronutrients particularly when intravenous route is the sole or primary source of nutrition. Micronutrients are important cofactors in metabolism, activating enzymes and coenzymes, and help protect against free radical oxidative damage, but are rarely measured. Amounts administered in parenteral nutrition (PN) for ill patients are “best guess” and based on healthy adult oral requirements.
Aims and Methods: To investigate manganese (Mn) and chromium (Cr) status in patients receiving PN. Samples were collected in trace element free tubes, prior to, and at weekly intervals during PN (Frensius Kabi), with a final sample when enteral nutrition was established. All patients received 10 ml additrace daily (weekdays). Biochemical analysis was performed with ICPMS (Perkins Elmer Elan DRCII).
Results: Twelve patients were studied, 7M:5F, median age 59.5 years (range 18–88). Baseline median Cr and Mn concentrations were within reference range (<10 nmol/l for each). Concentration of Cr and Mn rose significantly after 1 week of PN (p<0.01, p<0.05 respectively). Levels peaked at nearly 3 and 1.5 times above the upper limit of reference range and returned rapidly towards normal after establishment of enteral feeding (p<0.05 for Cr, compared to week 4). Median values shown (see table).
Abstract 305
Conclusions: Mn and Cr levels are not raised in acutely ill patients prior to commencement of PN. Current PN regimens appear to over supplement patients with Cr and Mn. Enteral nutrition reverses this. High levels of both elements have been associated with adverse outcomes. Regular monitoring of Mn and Cr might allow optimal replacement. This is particularly important in long term PN support.
306 SELENIUM AND ALUMINIUM STATUS IN PATIENTS BEFORE, DURING, AND AFTER PARENTERAL NUTRITIONAL SUPPORT
J. E. East1, R. Ramnarace1, S. Henson1, L. Linton-Willoughby2, J. Saunders1, B. Sampson3, W. S. Wassif4.Departments of 1Gastroenterology, 2Pharmacy, 4Clinical Biochemistry, Bedford Hospital; 3Clinical Chemistry, Charing Cross Hospital, UK
Background: Recent reports have emphasised the need to ensure optimal daily amounts of trace metals particularly during parenteral nutrition (PN) but they are rarely measured. Selenium (Se) dependant enzymes are important in redox state regulation and minimising oxidative damage. Aluminium (Al) can potentiate oxidative and inflammatory events and has been linked with neurodegenerative disorders. Al is usually a contaminant and has no known biological role.
Aims and Methods: To investigate Se and Al status in patients receiving parenteral nutrition. Samples were collected in trace element free tubes, prior to, and at weekly intervals during PN (Frensius Kabi), with a final sample when enteral nutrition was established. All patients received 10 ml additrace (Se4+ 0.4 µmol) daily (weekdays). Biochemical analysis was performed with ICPMS (Perkins Elmer Elan DRCII).
Results: Twelve patients were studied, 7M:5F, median age 59.5 years (range 19–88). Median serum values are shown in table. Levels of Se were low before and during PN but started to return towards reference range (RR, 0.8–1.75 μmol/l) after establishing enteral feeding. Concentrations of Al were within RR (<0.3 μmol/l) before, during and after PN. No significant changes detected in all Se (p>0.1) or Al (p>0.1) results.
Abstract 306
Conclusions: Se levels are low in acutely ill patients prior to commencement of PN. Current widely used supplementation in PN regimes does reverse this situation. This may be important for acutely unwell patients as well as those on long term PN support. Consideration should be given to more active monitoring and correction of Se levels acutely. Concentrations of Al remained low throughout PN excluding Al contamination of PN feeding.
307 COPPER AND NICKEL STATUS IN ACUTELY ILL PATIENTS BEFORE AND DURING PARENTERAL NUTRITION
J. E. East1, R. Ramnarace1, A. Deacon2, J. Binnie1, L. Linton-Willoughby3, J. Saunders1, B. Sampson4, W. S. Wassif2.Departments of 1Gastroenterology, 2Clinical Biochemistry, 3Pharmacy, Bedford Hospital; 4Clinical Chemistry, Charing Cross Hospital, UK
Background: Recent reports have emphasised the need to ensure optimal daily amounts of micronutrients particularly when intravenous route is the sole or primary source of nutrition. Micronutrients are important cofactors in metabolism, activating enzymes and coenzymes, and help protect against free radical oxidative damage, but are rarely measured.
Aims and Methods: To investigate copper (Cu) and nickel (Ni) status in patients receiving parenteral nutrition (PN). Samples were collected in trace element free tubes, prior to, and at weekly intervals during PN (Frensius Kabi). Patients received 10 ml additrace daily (weekdays). Biochemical analysis was performed with ICPMS (Perkins Elmer Elan DRCII).
Results: Data are presented as median (range) (see table). 12 patients were studied, 7M:5F, median age 59.5 years (range 18–88). Baseline Cu and Ni concentrations were within reference range (RR, 12–20 and <22; respectively). Concentration of Cu exceeded RR at week 2 but Ni remained within RR throughout. Both pre and during PN levels for some patients exceeded the RR by twice the upper limit of normal and total range varied almost threefold between patients for both elements, although there were no significant (p>0.1) change in any of the values.
Abstract 307
Conclusions: Basal Cu and Ni levels are within RR. Current Ni supplementation is appropriate, but Cu levels exceed the RR by week 2. There is interpatient variation in Cu and Ni levels with some patients greatly exceeding RR. Monitoring of Cu might guide supplementation.
Colorectal posters
308 INTRAVENOUS IMMUNOGLOBULIN IN THE TREATMENT OF SEVERE CLOSTRIDIUM DIFFICILE DIARRHOEA
S. McPherson, C. Rees, S. Soo, R. Ellis1, S. Panter.Department of Gastroenterology and 1Microbiology, South Tyneside District Hospital, South Shields, UK
Background:Clostridium difficile diarrhoea (CDD) is common in frail hospitalised patients. It leads to significant morbidity and mortality, and prolonged hospitalisation. Patients who develop severe, prolonged, or recurrent CDD have a poor antitoxin antibody response leading to low serum antitoxin antibodies. Use of intravenous immunoglobulin (IVIG) has been advocated in these patients.
Aim: To assess the response of patients with recurrent or severe CDD to IVIG in our institution.
Patients and Methods: A retrospective review of 228 CD toxin positive patients revealed 10 patients who were treated with IVIG since November 2003. Eight patients had severe CDD and two had recurrent CDD. The median age was 76 years (range 54–85). All patients had received non-CDD antibiotics (median three courses, range 1–7). The median length of symptoms before IVIG was 30 days (range 7–58). The patients received a median of three courses of vancomycin or metronidazole (range 2–5) before IVIG. Four patients had megacolon and two pancolitis on CT scanning. All patients had hypoalbuminaemia (median 24, range 18–33) and a raised CRP (median 46, range 25–178) at the time of infusion. Total protein was low in eight patients (median 51, range 33–66).
Results: Eight patients responded to IVIG (Flebogamma, Grifols, Barcelona, Spain, dose 150–400 mg/kg) with bowels returning to normal in a median 8 days (range 2–26 days), one patient received two doses. The two patients that failed to respond died (one died 11 days after IVIG of septicaemia and lymphoma and one died 17 days after IVIG of septicaemia). All patients tolerated the infusion with no side effects. Three patients had a recurrence (one had two recurrences) but these patients responded to a 10 day course of vancomycin.
Conclusion: We describe the largest series of patients treated with IVIG for recurrent or severe CDD. IVIG is effective and randomised controlled trials are warranted.
309 EXCISION OF RECTAL ADENOMAS USING THE UROLOGICAL RESECTOSCOPE SHOULD BE CONSIDERED WHEN ENDOSCOPIC POLYPECTOMY FAILS
D. Sankararajah, M. J. Forshaw, G. Maphosa, M. Stewart.(Introduced by R. Ede). Department of Surgery, Darent Valley Hospital, Dartford, UK
Objective: Rectal adenomas are often too large or sessile to be excised by endoscopic polypectomy and present a management dilemma. This study evaluates the results of rectal adenoma excision using the urological resectoscope.
Methods: All patients treated by endoscopic transanal resection using a urological resectoscope (January 1991–October 2004) were prospectively studied. All of the rectal tumours were initially assessed as benign.
Results: Forty patients (50% males; median age 72 years (range 40–88) underwent a total of 80 endoscopic transanal resections (mean two per patient; range 1–9). The tumours treated were predominantly located in the lower two thirds of the rectum (83%) and were greater than 2 cm in maximum dimension (83%): extensive circumferential carpet of tumour was present in five patients. 50% of patients required only a single procedure to obtain clearance. Mean operative time was 26 minutes (range 10–65 minutes). 78% of patients stayed in hospital for less than 24 hours. Postoperative morbidity was 8%; mortality was zero. Histology revealed severe dysplasia in 48% of patients. Foci of adenocarcinoma were present in five patients; only one patient required open resectional surgery. With a median follow up of 47 months (range 2–162 months), local recurrences occurred in 10% of patients: all of these patients were successfully treated by further transanal resection; one elderly patient developed a rectal cancer 5 years after refusing any further local treatments for a severely dysplastic rectal adenoma.
Conclusions: Large sessile rectal adenomas unsuitable for endoscopic polypectomy can be simply and effectively treated by endoscopic transanal resection using a urological resectoscope with an acceptably low local recurrence rate and similar outcomes to transanal endoscopic microsurgery.
310 PELVIC FLOOR SYNDROME: DEFINITION AND ASSESSMENT OF A CLINICAL ENTITY
K. Davis, D. Kumar, R. West.St George’s Hospital, Tooting, London SW17 ORE, UK
Background: Pelvic floor dysfunction (PFD) describes a wide range of clinical problems that rarely occur in isolation. Several studies have shown that pelvic floor disorders commonly coexist or develop sequentially over time although the true incidence of concomitant symptomatology is unknown. PFD is believed to be due to site-specific disorders that emanate from a single pelvic compartment. Since treatment strategies are based on this concept, it is not surprising that the outcome of such treatments is suboptimal.
Objective: To assess by means of a standardised questionnaire how far women presenting with pelvic floor symptoms in one of three domains (UI, FI, or prolapse) have symptoms in another domain.
Design: Cross sectional study. Setting: tertiary colorectal and urogynaecology units.
Participants: 543 patients referred to one of three specialist clinics. Mean age 53.5 years.
Main Outcome Measures: Symptoms relating to pelvic floor dysfunction reported using a written questionnaire.
Results: Scales relating to each of the pelvic floor compartments were constructed and had satisfactory internal coherence (alphas 0.63 to 0.78). Scores on these scales were predictive of overall distress/inconvenience (p<0.001). A total of 304 (55.9%) women reported symptoms related to all three compartments. In the presence of one symptom the odds of reporting a symptom in another domain approximately doubled (UI in FI; OR 2.1, 95% CI 1.37 to 3.21, prolapse in UI; OR 2.5, CI 1.63 to 3.83, FI in prolapse; OR 2.2, CI 1.48 to 3.20) and in the presence of two symptoms the odds of having a third increased almost threefold (FI in UI/prolapse; OR 2.6 95% CI 1.78 to 3.71, prolapse in UI/FI; OR 2.8, CI 1.94 to 4.15, UI in FI/prolapse; OR 2.9, CI 1.92 to 4.42).
Conclusion: This study documents for the first time the extent to which patients presenting with one type of pelvic floor dysfunction also had concomitant symptomatology. The extent of association suggests that pelvic floor dysfunction should be considered as a syndrome. The current strategy of addressing pelvic floor disorders based on a single presenting complaint needs to be reconsidered
311 IS FLEXIBLE SIGMOIDOSCOPY A USEFUL INVESTIGATION IN IRON DEFICIENCY ANAEMIA WITHOUT GI SYMPTOMS?
T. Kitiyakara, A. S. McIntyre, D. A. Gorard.Wycombe Hospital, Queen Alexandra Road, High Wycombe, Bucks, HP11 2TT, UK
Background and Aim: Proximal colonic imaging is important when investigating iron deficiency anaemia without GI symptoms, but the role of flexible sigmoidoscopy (FS) is unclear. Distal colorectal neoplasms might be expected to also cause GI symptoms before anaemia occurs. We have compared the yield from FS for anaemia and other indications.
Methods: The prevalence of colorectal cancers and polyps at FS performed for rectal bleeding (RB), abdominal pain (AP), change in bowel habit (CIBH), and anaemia during a 5 year period (1997–2002) were compared. Case notes of patients with anaemia were scrutinised to ensure that the patients were asymptomatic and the anaemia truly iron deficient. A comparison with findings from the national FS screening trial was also made. In the study’s second part, symptoms of all cancers detected at FS during this period were noted, checking case notes for GI symptoms if anaemia seemed to be the procedure’s sole indication.
Results: There were 1077 RB cases, 901 CIBH cases, 393 AP cases, and 254 anaemia cases. 195 case notes (59 not retrievable) of anaemia patients were scrutinised. 111 cases were patients who truly had iron deficient anaemia and no GI symptoms. Anaemia patients were older, mean age 69.5 years, than patients with AP (55.7 years), RB (60.7 years), CIBH (61.1 years), or FS screening trial participants (55–64 years). Six of 111 anaemia patients had proximal colonic cancers, but cancer was found at FS in just one (0.9%) anaemia patient, and this was in the descending colon. This compares with cancer at FS in 66 (6.1%) RB patients (χ2 = 5.2, p<0.05), 36 (4%) CIBH patients (χ2 = 2.7, p = 0.1, NS), eight (2%) AP patients (NS), and 131 of 40 674 (0.3%) individuals in the UK FS screening trial (NS). Polyp prevalence was similar at 166 (15.4%) RB patients, 89 (9.9%) CIBH patients, 35 (8.9%) AP patients, and 11 (10.1%) anaemia patients. Checking symptoms from 129 cancers detected at FS during this period confirmed the one patient presenting with solely iron deficient anaemia.
Conclusion: FS reveals no more colorectal neoplasia in iron deficiency anaemia without GI symptoms, than in asymptomatic individuals having FS screening. In this setting, FS is not useful and should be abandoned.
312 PROTON PUMP INHIBITORS AS A RISK FACTOR FOR CLOSTRIDIUM DIFFICILE ASSOCIATED DIARRHOEA
K. A. Yearsley, A. V. Ramadas, L. J. Gilby, E. M. Kubiak, M. C. Allison.Departments of Gastroenterology and Microbiology, Royal Gwent Hospital, Newport, South Wales, NP20 2UB, UK
Introduction: Profound inhibition of gastric acid secretion by proton pump inhibitors (PPI) removes a defence against ingested bacteria and spores. This phenomenon increases the risk of developing some forms of bacterial gastroenteritis. Three retrospective studies and one small prospective case control investigation of a possible link between acid suppression therapy and Clostridium difficile associated diarrhoea (CDAD) have reported conflicting results.
Methods: A prospective case control study of consecutive patients with CDAD was undertaken in a large district hospital. We included all patients with new onset CDAD, confirmed by the presence of C difficile toxin A in the faeces. A control for each case was identified by examining the list of patients on the same ward at the same time, and selecting the patient whose date of birth was closest to that of the case. Information on proton pump inhibitor and antibiotic prescriptions was recorded onto a standard proforma.
Results: There were 155 cases and 154 controls (mean age 78.7 years in the CDAD group and 79.1 years in the controls). Of the CDAD group, 143 (92.3%) had received antibiotics during the preceding 3 months, compared with 75 (48.7%) of the controls (OR 12.6, CI 6.2 to 26.0, χ2 = 70.5, p<0.001). Among all those receiving antibiotics, 59 (41.3%) of the CDAD group had also received PPI within the preceding 3 months, compared to 20 (26.7%) of the control group (OR 1.9, CI 1.0 to 3.7, χ2 = 4.5, p = 0.03). Among the entire CDAD group 64 (41.3%) had received PPI therapy compared with 40 (26.0%) of controls (OR 2.0, CI 1.2 to 3.3, χ2 = 8.1, p = 0.004).
Conclusions: The risk of CDAD in hospitalised patients receiving antibiotics may be compounded by exposure to PPI therapy. The possibility that PPI may be an independent risk factor for new and/or relapsing CDAD should be investigated. Meanwhile consideration should be given to suspending or stopping PPI in hospitalised patients needing antibiotics unless there is a clear indication for such therapy.
313 THE LONG TERM FUNCTIONAL OUTCOME OF OVERLAPPING ANAL SPHINCTER REPAIR AND ANTERIOR LEVATORPLASTY
C. Evans, K. Davis, D. Kumar.St George’s Hospital, London, UK
Background: Reconstructive surgery has been shown to give functional improvements in patients with faecal incontinence secondary to anal sphincter damage. However, it is unclear which patients benefit and its long term efficacy has been questioned.
Aim: To assess the functional outcome of a single surgeon series of overlapping anal sphincter repairs with anterior levatorplasty.
Method: A retrospective study of case notes and anorectal physiology of 66 patients combined with an interview to assess their current degree of continence and associated quality of life after surgery.
Results: Sixty six female patients, mean age 62.8 years and (range 32–83), mean follow up 45.2 months and (range 14–78) were assessed. Functional improvement in continence was seen in 77.1% of patients, which mirrored their subjective rating of surgery (62.7% rating the operative results as good/excellent). Complete continence was reported in 14 (21.2%) patients, a further 21 (31.8%) reporting incontinence to flatus only. Continence Grading Scores improved from a mean (SD) 9.71 (4.82) presurgery to 5.55 (4.11) post. Stratification by age (63 years< or ⩾63 years) demonstrated no statistical difference in functional results between patient groups. Similarly stratification by follow up showed no statistically significant differences between long term v short term groups (43–78 months v 14–42 months). Post-surgical physiology data showed no statistically improved results when compared to presurgery.
Conclusions: Overlapping anal sphincter repair with anterior levatorplasty is an effective treatment for faecal incontinence. Patient age does not correlate with outcome and symptoms do not deteriorate over time. Anorectal physiology results do not predict for symptomatic improvement in patients with faecal incontinence secondary to sphincter damage.
314 ENDOSCOPIC ALTERNATIVES TO DILATATION IN THE MANAGEMENT OF ANASTOMOTIC STRICTURES OF THE COLON AND RECTUM
M. J. Forshaw, G. Maphosa, D. Sankararajah, M. Stewart, M. C. Parker.(introduced by R. Ede). Department of Surgery, Darent Valley Hospital, Dartford, UK
Objective: Dilatation is the commonest form of treatment for anastomotic strictures but is often unsuccessful and repeat procedures are required. This study assesses the short and long term results from using self-expanding metallic stents (SEMS) and endoscopic transanal resection of strictures (ETARS) in managing high grade strictures where other treatments have failed.
Methods: Data on all patients with biopsy proven benign anastomotic strictures (luminal diameter <7 mm) following colorectal surgery between April 1995 and October 2004 were prospectively collected.
Results: SEMS and ETARS were performed in 10 patients with high-grade strictures (seven males; median age 71 years (range 50–79). Ten ETARS procedures were performed in six patients. The mean operating time was 42 minutes (range 15–70). The median postoperative hospital stay was 1 day (range 1–18). Early complications occurred in two patients: one patient required re-operation for bleeding; an asymptomatic anastomotic perforation occurred in a second patient. ETARS was technically unsuccessful in an acutely angulated long stricture. SEMS were successfully inserted into five patients (including the failed ETARS) without any early complications. With a median follow up of 16 months (range 1–73), all 10 patients have had satisfactory long term outcomes. Stent migration occurred in one patient at 30 months, who remained asymptomatic. One patient required three ETARS procedures for control.
Conclusions: SEMS and ETARS are simple, safe, and effective methods in treating difficult high grade anastomotic strictures. ETARS is most useful for short tight strictures with good transanal access. The use of stents appears to be associated with a lower rate of subsequent re-intervention.
315 A POTENTIAL ROLE FOR THE CHEMOKINE RECEPTOR CXCR4 AND ITS LIGAND CXCL12 IN THE LOCOREGIONAL SPREAD OF COLORECTAL CANCER
C. Bailey, R. Negus, G. Roberts, R. Goldin, D. Peck, A. Darzi.Academic Department of Surgery, Imperial College of Medicine at St Mary’s, 10th Floor, QEQM, Praed Street, London W2 1NY, UK
Background: Colorectal cancer remains a major cause of cancer mortality with 16 000 deaths per annum in the UK. Although patients with early stage disease have a high survival, only 37% of those with regional lymph node involvement will survive 5 years. The role of chemokine receptors and their ligands in tumour growth and metastatic progression is now becoming apparent. Here we explore the role of the chemokine, CXCL12 and its receptor, CXCR4 in the development of peritoneal metastases.
Methods: A survey of 21 colorectal cancers using ribonuclease protection assay revealed a significantly greater level of CXCR4 receptor expression when compared with normal colonic mucosa. Strikingly, this was seen in all grades of tumour, indicating this to be an early tumorogenic event.
Results: Functional assays based on the colorectal cell lines, SW620, SW480, HT-29 and primary human mesothelial cells, indicated CXCR4 mRNA and protein expression in tumours and expression of its ligand CXCL12 by mesothelium. Both systems were surprisingly refractive to classical proinflammatory stimuli; however hypoxia, a known poor prognostic factor, had a significant effect. Exposure to hypoxic conditions induced an upregulation of CXCR4 protein expression, with a concomitant enhancement of the ability of cells to migrate to CXCL12 and mesothelium supernatant.
Conclusions: These data indicate the possibility of chemokine receptor ligand mediated, directional metastasis, which can play a role in the locoregional spread of colorectal cancer. Taken together with other emerging data, this implies that chemokine networks may provide a common mechanism of metastasis for carcinomas.
316 COLONOSCOPIC AND RADIOLOGICAL MISS RATES FOR COLORECTAL CANCER IN A DISTRICT GENERAL HOSPITAL
S. Barker, T. Thresher, P. A. Kitching, J. D. Linehan.Royal United Hospital, Combe Park, Bath, BA1 3NG, UK
Introduction: It is recognised that both colonoscopic and radiological investigations for colorectal cancer (CRC) have a low but significant miss rate. A recent Canadian study demonstrated a colonoscopic miss rate of 4% for right-sided cancers.1 In the UK, both radiological investigations and colonoscopy are used in the diagnosis of CRC. There have been no recent studies in the UK to assess the miss rate with these modalities.
Aim: To assess the miss rate of CRC with colonoscopic and radiological investigations and to determine if the rates are similar to previous studies.
Methods: All patients with a new diagnosis of CRC in an 18 month period were identified using a histopathological database and records were checked to see if they had received any radiological or colonoscopic investigation in the 3 years before diagnosis. Investigations within the previous 6 months were considered to be diagnostic unless mistakenly called normal.
Results: 332 patients with a new diagnosis of CRC were identified between 1/1/03 and 30/6/04. 158 were female and 174 male. 15 (4.5%) had had a prior investigation, in the last 3 years, by either colonoscopy or radiology—including barium enema and CT imaging—that had not shown any significant lesion. On average there was an 89% colonoscopy completion rate for all endoscopists.
Conclusion: 4.5% is a low but significant miss rate and comparable to other studies. There needs to be larger studies into CRC miss rates for colonoscopic and radiological investigations in the UK and highlights the importance of discussing the potential for “a missed diagnosis” when consenting patients.
Abstract 316
1
317 THE DETERMINANTS OF ANORECTAL SENSATION AND CONTINENCE IN HEALTHY, CONTINENT SUBJECTS
M. Fox1, D. Menne2, M. Fried3, W. Schwizer3.1St Thomas’ Hospital, London; 2Menne Biomed, Tübingen, Germany; 3Division of Gastroenterology, University Hospital Zurich, Switzerland
Aims: To manage continence problems effectively, an understanding of the normal physiology of anorectal sensation and continence in healthy subjects is required. In a sequence of studies we assessed (1) the effects of anorectal sensorimotor function (n = 41) and (2) stool consistency (n = 10), on anorectal filling sensation and continence in continent subjects. (3) To test the initial findings loperamide was administered and the investigations repeated (n = 10).
Methods: Measurements were acquired from healthy, continent subjects in a randomised, double blind, prospective fashion. Rectal function and capacity were assessed by barostat and anal function by manometry. To test anorectal sensation and continence during rectal filling, a viscous stool substitute was infused into the rectum at 60 ml/min to 1500 ml. The volume infused at first awareness, urgency, initial incontinence, and maximum volume retained were recorded.
Results: (1) Covariant analysis revealed no independent associations for age, sex, or weight with retention test measurements. The sensation of first awareness was closely associated with resting pressure whereas faecal urgency was associated with squeeze pressure. The volume at first incontinence was associated with squeeze pressure and rectal compliance. The maximum volume (a stable reservoir volume in the majority) was closely associated with rectal capacity. (2) Continence was better maintained for high viscosity than low viscosity stool substitute during filling. This finding was significant for patients with weaker and less well maintained anal squeeze pressure. (3) Loperamide had effects on anal sphincter pressure that modulated anorectal sensation and fecal continence during rectal filling as predicted by the initial studies.
Conclusion: These findings provide objective evidence that anorectal sensation and continence in health requires a compliant rectal reservoir of adequate capacity, and effective anal sphincter function. Continence for low viscosity stool depends on effective anal sphincter function. The close association between continence, anorectal motor, and sensory function indicates that an adaptive mechanism is present that maintains continence across the “normal range” of anorectal structure and function.
318 TOTAL RECTAL EXCISION AND COLOPLASTY POUCH FOLLOWING NEOADJUVANT THERAPY FOR RECTAL CANCER: DOES IT RESTORE ANORECTAL PHYSIOLOGY?
S. R. E. Wijesuriya, K. I. Deen, G. Ratnayake.Department of Surgery University of Kelaniya, Sri Lanka
Introduction: Neoadjuvant therapy for rectal cancer results impaired threshold and maximum tolerable rectal volumes. The aim of the study was to evaluate whether total rectal excision and coloanal anastomosis with coloplasty pouch restore anorectal physiology following neoadjuvamt therapy for rectal cancer.
Patients and Methods: Eight patients (3 males, median age 55 years, range 46–63) with rectal cancer were subjected to high dose long course neoadjuvant therapy followed by nerve sparing low anterior resection and coloanal anastomosis with coloplasty pouch. Maximum resting anal sphincter pressure (MRP), maximum squeeze pressure (MSP), threshold rectal volume (TV), and maximum tolerable rectal volume (MTV) were assessed before neoadjuvant therapy and 6 months after low anterior resection.
Results: There was no significant difference in maximum resting anal sphincter pressure, maximum squeeze pressure, threshold rectal volume and maximum tolerable rectal volume in patients before NAT and following low anterior resection ((MRP pre NAT v post op: 36 mm Hg v 34 mm Hg, p = 0.82; MSP pre NAT v post op: 98 mm Hg v 116 mm Hg, p = 0.50); TV pre NAT v post op: 55 ml v 63 ml, p = 0.48, MTV pre NAT v post op: 180 ml v 165 ml, p = 0.34; t test).
Conclusions: Anorectal physiology is restored in patients who undergo total rectal excision and coloanal anastomosis with coloplasty pouch following neoadjuvant therapy for rectal cancer. Therefore all patients who are subjected to neoadjuvant therapy for rectal cancer may benefit from total rectal excision irrespective of tumour location.
319 MICROSCOPIC COLITIS IN TAYSIDE: CLINICAL FEATURES, ASSOCIATIONS, AND BEHAVIOUR
T. Heron, S. Walsh1, C. Mowat.Departments of 1Pathology, Gastroenterology, Ninewells Hospital and Medical School, Dundee, UK
Background: Microscopic colitis is a term encompassing collagenous colitis and lymphocytic colitis. The incidence ranges from 4–10 cases/100 000. It can be associated with coeliac disease, rheumatoid arthritis, thyroid dysfunction, and certain drugs. It classically produces watery diarrhoea in elderly patients in whom the colon appears normal. Management can prove difficult. There is little evidence base to support any particular treatments and the natural history is unclear.
Aims: To determine the clinical features, associations, and behaviour of microscopic colitis in Tayside.
Method: All cases from 1999–2004 were identified from pathology records and reviewed by a single pathologist. Their case notes were reviewed to obtain clinical details, associations, and outcomes.
Results: There were 33 confirmed cases of microscopic colitis; 11 lymphocytic colitis, 22 collagenous colitis; male:female ratio 1:2, mean age 64.2 years (range 35–90). The mean annual incidence of microscopic colitis was 1.65/100 000. All patients reported increased bowel frequency and watery diarrhoea. 50% reported weight loss, urgency and abdominal cramps. 30% reported night rising. 54% had associated autoimmune conditions (three had coeliac disease). 11/22 with collagenous colitis were on a proton pump inhibitor. Follow up data were available on 31/33 patients over a mean of 26.8 months (range 1–60). Therapeutic strategies used alone or in combination in 27 patients included mesalazine, loperamide, steroids, and PPI withdrawal/switch. 25/31 (81%) patients reported complete resolution of symptoms. Of these, only four patients remained on therapy. Five patients reported partial resolution. In total, nine patients received steroids; of these, three patients with lymphocytic colitis reported only partial response.
Conclusions: The incidence of microscopic colitis in Tayside is lower than expected. It should be suspected in elderly patients attending with watery diarrhoea. Patients frequently have coexisting autoimmune disease. Although symptoms are disabling, they respond to a variety of therapies and resolve in the vast majority within 12 months. Steroids are required in the minority.
320 IDENTIFYING PATIENTS WITH IRRITABLE BOWEL SYNDROME VIA A POPULATION SURVEY
N. Rousseau1, E. McColl1, G. Rubin2, C. May1 (introduced by A.P.S. Hungin).1CHSR, 21 Claremont Place, University of Newcastle, Newcastle upon Tyne, NE2 4AA; 2University of Sunderland, Benedict Building, St George’s Way, Sunderland, SR2 7BW, UK
Objective: To identify patients with irritable bowel syndrome (IBS) via a random population survey.
Background: Various criteria have been used to identify patients with IBS in clinical practice and research. Currently the “gold standard” is Rome II but some still view IBS as a diagnosis of exclusion.
Design: Self-completion postal questionnaire using Rome II criteria.
Setting: Seventeen general practices in the north of England; including rural, urban, affluent, and economically deprived areas.
Participants: A random sample of approximately 190 adult patients from each practice list (a total of 3171 patients).
Results: The overall response rate was 46.9%. Response rate varied by GP practice from 37.4% to 61.7%. Overall, 8% of patients who responded had Rome II IBS. Over 60% of patients identified as having IBS under the Rome II criteria reported that they had or thought they might have the condition, but 17% did not think they had the condition. 10% of those meeting criteria for Rome II IBS self-reported an organic bowel disease (36% of those reporting organic bowel disease met Rome II criteria for IBS).
Rome II IBS varied by practice to an unexpected degree (prevalence rates varying from 1.9% to 15.3%). There was a strong relation with response rate (Pearson correlation −0.67 p<0.01) with lower prevalence in practices where response rate is higher. However, response rate (0.74, p<0.01) and prevalence of Rome IBS (0.67, p<0.01) were both also highly correlated with measures of affluence.
Conclusions: The Rome II criteria are useful in identifying a sample of patients with IBS in the population but the relation with self-reported disease is not straightforward. The link between prevalence, response, and affluence merits further investigation.
Pathology posters
321 ASSESMENT OF DICLOFENAC INDUCED SMALL BOWEL DAMAGE BY CAPSULE ENTEROSCOPY
L. Maiden1, B. Thjodleifsson2, I. Bjarnason1.1Department of Medicine, Guy’s, King’s, St Thomas’ Medical School, London, UK; 2Department of Medicine University Hospital of Iceland, Reykjavik, Iceland
Background: Conventional acidic non-steroidal anti-inflammatory drugs (NSAIDs) frequently cause small bowel inflammation. Diagnosis is largely based on assay of surrogate markers of inflammation in stool such as faecal calprotectin. However stool markers are not widely available and the precise nature of this inflammation is uncertain. We used wireless capsule enteroscopy to quantitate and assess the nature of the small bowel damage caused by NSAIDs when taken short term.
Methods: Forty healthy volunteers underwent a baseline capsule enteroscopy and faecal calprotectin test. After taking diclofenac slow release 75 mg twice a day (with omeprazole 20 mg twice a day for gastroprotection) for a total of 14 days both investigations were repeated.
Results: Seventy five per cent of subjects had repeat faecal calprotectin concentrations above the upper limit of normal. Capsule enteroscopy demonstrated new pathology in 27 (68%) of subjects. The commonest lesions were mucosal breaks without haemorrhage, seen in 15 (38%), reddened folds in 14 (35%); petichiae or red spots in 13 (33%); denuded mucosa in eight (20%); blood in the lumen without a visualised source in three (8%) and a mucosal break with haemorrhage in 2 (5%) subjects. Fifteen of the 27 subjects had more than one lesion concurrently.
Conclusion: Capsule enteroscopy demonstrates a range of small bowel lesions after 2 weeks of diclofenac ingestion with erosions and ulcers being evident in over a third of the volunteers.
322 HUMAN ANTIBODY RESPONSE AGAINST THE p58 SUBUNIT OF THE HELICOBACTER PYLORI CYTOTOXIN: SEROTYPING VACA
F. Avilés1, D. P. Letley1, E. El-Omar2, J. Torres3, J. C. Atherton1.1Wolfson Digestive Diseases Centre. University of Nottingham, Nottingham, UK; 2Department of Medicine and Therapeutics, Aberdeen University, Aberdeen, UK; 3Instituto Mexicano del Seguro Social, Mexico City, Mexico
Background: The vacuolating cytotoxin (VacA) of Helicobacter pylori is a major virulence factor. Toxin activity differs among isolates due to polymorphism in the signal and mid regions of the vacA gene. For the mid region, type m1 VacA binds more extensively to cells and has been more closely associated in USA and Western Europe with peptic ulcer disease and gastric cancer than type m2. As VacA typing is an important tool for identifying patients at higher risk of severe gastroduodenal diseases, we aimed to develop a serological test for this marker.
Methods: 119 matched strains and serum samples were obtained from infected individuals in three locales, 31 from Nottingham, 43 from Glasgow, and 45 from Mexico. A control group of 31 non-infected individuals was also used. For the strains, the vacA gene was typed by PCR. To test for specific anti-VacA antibodies, recombinant p58 subunit from strains 60190 (m1) and Tx30a (m2) was prepared. Following initial characterization using immunoblotting, recognition of these proteins by serum antibodies was evaluated by an ELISA method.
Results: Of the 119 serum samples from infected individuals, 103 recognised at least one of the two p58 subunits. Antibodies from 31 subjects reacted with both proteins at similar levels and antibodies from 72, reacted principally with only one type. From the last group, 81% of the sera were specific to the mid region type of the infecting strain.
Discussion: Results indicate that in 87% of patients the toxin was expressed in vivo. A lack of response might be explained by: (a) no VacA expression or (b) failure of an immune response to the toxin. Presence of similar levels of antibodies against both proteins may imply colonisation with both VacA m1 and m2 strains. Finally, it is possible to predict the VacA mid region type in 81% of patients exposed to only one form of the toxin. This may be useful to identify patients or populations at high risk of gastric cancer.
323 P27 IS DOWNREGULATED IN GASTRIC PRECANCEROUS LESIONS AND CORRELATES WITH SURVIVAL ON GASTRIC CARCINOMA PATIENTS
G. K. Anagnostopoulos1, D. Stefanou1, E. Arkoumani1, K. Paraskeva3, K. Lekaniti1, E. Tsianos2, N. J. Agnantis1 (introduced by K. Ragunath).1Pathology and 2Gastroenterology Department, University of Ioannina, Medical School, 3Gastroenterology Department, Agia Olga Hospital, Athens, Greece
Background: Cell cycle control is important in carcinogenesis and cancer progression. P27 is a member of the Cip/Kip family of cyclin dependent kinase inhibitors, and acts as a negative regulator of G1 progression. Thus p27 has been proposed to be a putative tumour suppressor. The aim of our study was to examine the expression of p27 in gastric cancer and precancerous lesions and to evaluate its prognostic implications.
Methods: P27 protein was studied by immunohistochemistry, using monoclonal antibodies (IB4, Novocastra, dilution 1:20), in paraffin specimens of gastric cancer and surrounding mucosa of 98 patients who underwent resection for gastric adenocarcinoma. P27 immunoreactivity was considered as high if the percentage of positive cells was over 30%, low if the percentage of positive cells was 5–30% or negative if the percentage of positive cells was less than 5%.1
Results: The average staining score for p27 in chronic gastritis, atrophic gastritis, intestinal metaplasia, and gastric dysplasia were 2/2, 1.80/2, 1.52/2, and 1.19/2 respectively. Low or loss of p27 immunoreactivity was observed in 59 (60%) of 98 stained tumours. There was no significant correlation between p27 expression and age, sex, grade of differentiation, or Lauren classification. Reduced expression of p27 was associated with depth of invasion and nodal metastasis. Kaplan-Meier plots of survival showed tumors with low p27 were associated with poorer survival than those with high p27 expression (p<0.01). In multivariate analysis stage of the disease was the only independent factor associated with poor prognosis.
Conclusion: P27 protein is downregulated in gastric precancerous lesions. Gastric cancer with low expression of p27 is associated with aggressive characteristics and poorer outcome.
324 AUDIT OF PATHOLOGIST PERFORMANCE IN COLORECTAL CANCER REPORTING FOLLOWING IMPLEMENTATION OF A SPECIALISED GI PATHOLOGY SERVICE IN THE DGH SETTING
S. K. Gurusamy, R. A. Carr, D. S. A. Sanders (on behalf of GI Services, Warwick Hospital).Department of Pathology, Warwick Hospital, Warwick, UK
Introduction and Aim: There is an ongoing national debate about the merits and feasibility of specialist reporting in histopathology in the district general hospital (DGH) setting. We report the impact of specialised reporting for colorectal cancer in our department with regard to pathologist performance.
Methods: An Access based colorectal cancer database was designed based on the RCPath Colorectal Cancer Minimum Dataset. Before August 2003 colorectal cancer excisions were reported by any of five consultant pathologists in the department. Subsequently a single gastrointestinal pathologist reported the majority of colorectal cancer excisions. A total of 200 cases were audited, of which 100 cases were entered prospectively and 100 cases retrospectively.
Results: The following parameters of pathologist performance were assessed pre and post specialist reporting (see table).
Abstract 324
Conclusion: There was a significant improvement in pathologist performance in the post-specialist period with respect to (a) report turnaround times, (b) mean lymph node harvest, (c) adequate sampling of tumour, and (d) the pick up rate of extramural vascular invasion. Additional measures of good practice initiated included total mesorectal excision assessment for rectal cancers, and specimen photography for surgical resection margin and radiology audit.
325 INCREASED CIRCULATING ANTI- AND PRO-INFLAMMATORY CYTOKINES DURING ACTIVE DISEASE IN PATIENTS WITH ULCERATIVE COLITIS, NORMALISED FOLLOWING ADSORPTIVE GRANULOCYTE AND MONOCYTE APHERESIS
H. Hanai1, T. Iida1, F. Watanabe2, M. Yamada3, K. Takeuchi1, T. Tanaka1, K. Kondo1, M. Kikuyama4, Y. Maruyama2, Y. Iwaoka3, K. Hirayama5, A. R. Saniabadi6.1Department of Medicine, Hamamatsu University; 2Fujueda General Hospital; 3Hamamatsu Medical Centre; 4Hamamatsu Rosai Hospital; 5Hamamatsu Insurance Hospital; 6Japan Immunoresearch Laboratories, Japan
Background: IL-6 is known to activate leucocytes and promote leucocyte extravasation while IL-18 is known to induce interferon-gamma and chemokine release and invoke Th1-like actions. In contrast, IL-10 is known to induce Th2-like actions and IL-1 receptor antagonist (IL-1ra) counteracts the actions of IL-1β. We have investigated the relationships between UC clinical activity index (CAI) and circulating levels of IL-1ra, IL-10, IL-6, and IL-18.
Methods: IL-1ra, IL-10, IL-6, and IL-18 were measured in 31 patients with active UC; mean CAI 11.1, range 5–25 and 12 healthy controls. Patients were given granulocyte and monocyte adsorptive apheresis (GMA) with Adacolumn. Leucocytes which bear the FcγR and complement receptors adsorb to the column leucocytapheresis carriers. Each patient could receive up to 11 GMA sessions over 8 weeks.
Results: We found strong correlations between CAI and IL-10 (r = 0.827, p<0.001), IL-6 (r = 0.785, p<0.001), and IL-18 (r = 0.791, p<0.001). IL-1ra did not show correlation with CAI. Following GMA therapy, 24 of 31 patients achieved remission and the levels of all 4 cytokines fell to the levels in healthy controls. Further, blood levels of IL-1ra and IL-10 increased at the column outflow and inflow at 60 minutes suggesting release from leucocytes that adhered to the carriers.
Conclusions: Increased blood levels of IL-6 and IL-18 together with peripheral blood granulocytes and monocytes/macrophages which in patients with active UC show activation behaviour and increased survival time can be pro-inflammatory and should be targets of therapy by GMA.
326 INVESTIGATING THE LINK BETWEEN MAST CELL DENSITY AND SEVERITY OF HELICOBACTER PYLORI GASTRITIS IN THE CORPUS AND ANTRIUM
C. Osonnaya, K. Osonnaya, P. Swain.Epidemiology and Education Unit, Centre for Adult and Paediatric Gastroenterology, Institute of Cell and Molecular Science, Barts and The London, Queen Mary’s School of Medicine and Dentistry, University of London, Turner Street, London E1 2AD, UK
Objective: To investigate the link between mast cell density, Helicobacter pylori intensity, and histopathological severity of gastritis in the corpus and antrum mucosa.
Methods: The study included 68 H pylori positive and 22 H pylori negative patients. All case underwent endoscopy, and biopsies were obtained for the evaluation of H pylori and histopathological examination. All biopsies were evaluated according to the Sydney system and mast cell density in both the corpus and antrum mucosa was analysed by modified Giemsa stain, Spearman’s correlation test was used to determine the relation between mast cell density and other histopathological parameters. The comparison of mast cell density between H pylori positive and negative group was analysed by Mann Whitney U test.
Results: Mast cell density was significantly higher in the H pylori positive group than in the H pylori negative group (p<0.001) both in the antrum and corpus. The higher mast cell distribution was correlated with increased inflammation, activity, and H pylori in the antrum and corpus (p<0.001). No relation was found between mast cell distribution and intestinal metaplasia or atrophy.
Conclusion: The results of this study suggest that mast cells may play a role in the development of H pylori gastritis.
Cell/molecular biology posters
327 DETECTION AND CHARACTERISATION OF TP53 MUTATIONS IN TUMOURS OF THE OESOPHAGUS AND CARDIA FROM AN AREA OF HIGH INCIDENCE (LOWER NORMANDY, FRANCE)
J. Breton1,2, F. Sichel2, J. Marnay3, D. Arsene4, M. Lechevrel2.(introduced by D. Forman). 1Molecular Epidemiology Unit, Leeds Institute for Genetics, Health and Therapeutics, University of Leeds, UK; 2GRECAN, François Baclesse Centre and University of Caen, France; 3Department of Pathology, François Baclesse Centre, Caen; 4Department of Gastro-Enterology, Caen Teaching Hospital, Caen, France
Background and Aim: The p53 protein is a transcription factor involved in key processes such as cell cycle control, apoptosis, and DNA repair. Alterations to the TP53 gene are considered one of the most common genetic alterations in cancers. Screening for and identifying TP53 mutations in tumours could be of use clinically to improve prognosis and therapy for digestive cancers. Our aim was to compare the sensitivity and specificity of denaturing high performance liquid chromatography (DHPLC) with conventional TP53 mutation detection by denaturing gradient gel electrophoresis (DGGE). The former technique has advantages of minimal sample handling and a throughput suitable for clinical applications. In addition, this study allowed the collection of data regarding TP53 mutation patterns in distinct histological subtypes of oesophageal and gastric tumours.
Methods: DNA was extracted from tumoural samples from the oesophagus (n = 46) and cardia (n = 8) and screened for TP53 mutations using both techniques. Mutations were confirmed and characterised by sequencing.
Results: Ninety seven per cent (33/34) of oesophageal squamous cell carcinomas had a TP53 mutation or polymorphism. We found a high proportion of mutations at A:T base pairs which could be attributed to heavy alcohol consumption. In adenocarcinomas (cardia and oesophagus), the mutation frequency was 69% (11/16). Frequent transitions at CpG sites in these samples could be related to endogenous and inflammatory processes. DHPLC gave comparable results to DGGE in terms of sensitivity and specificity.
Conclusion: We have therefore demonstrated that DHPLC can be considered a reliable TP53 mutation screening method, and is more compatible than electrophoretic approaches for studies involving large numbers of clinical samples.
328 HEPATIC STELLATE CELLS MODULATE THE SWITCH FROM ACUTE TO CHRONIC INFLAMMATION BY PROMOTING LYMPHOCYTE RECRUITMENT, RETENTION, AND SURVIVAL
A. P. Holt, A. Filer*, P. F. Lalor, C. D. Buckley1, D. H. Adams.Liver Research Laboratory and 1Department of Rheumatology, University of Birmingham, UK
Background: We sought to determine whether hepatic stellate cells (HSC) maintain the chronic inflammatory cellular infiltrate associated with liver fibrosis.
Methods: HSC were isolated from human liver tissue obtained through the transplantation programme in Birmingham using established techniques. Secretion of cytokines and chemokines was analysed with multiplex bead based assays and confirmed with sandwich ELISA. Real-time studies of lymphocyte chemotaxis to HSC and HSC supernatants were made using modified invasion chambers. Adhesion studies were performed on HSC, skin, and spleen fibroblast monolayers, and blocking mAB used to identify the pathways involved. Lymphocyte survival on fibroblast monolayers was also measured using fixed volume live cell counting, and apoptosis by expression of Caspase-3.
Results: (1) HSC secrete a wide repertoire of chemokines and cytokines which are upregulated following stimulation with TNFα or IL1b. Rapid lymphocyte chemotaxis occurs in response to TNFα stimulated HSC and HSC conditioned serum. (2) Unstimulated HSC and spleen fibroblasts support adhesion of lymphocytes and promote greater lymphocyte motility and transmigration than skin FB. Stimulation with TNFα, IL1b and IFγ increases lymphocyte adhesion and transmigration, which was significantly reduced following ICAM-1 or VCAM-1 blockade. (3) CD4+ T cell survival is significantly increased by co-culture with liver HSC relative to skin and spleen controls, and is associated with reduced numbers of Caspase-3 positive T cells.
Discussion: Cytokine activated HSC promote rapid recruitment and retention of lymphocytes through integrin and chemokine dependent pathways. By maintaining survival of terminally differentiated lymphocytes, HSC can modify the liver microenvironment to modulate the switch from acute resolving to chronic persistent inflammation.
329 COMH: PURIFICATION OF A UNIQUE H PYLORI PROTEIN
K. Kostidis, P. Thackray, K. D. Bardhan1, C. W. Potter, J. R. Sayers.Division of Genomic Medicine, Medical School, University of Sheffield; 1District General Hospital, Rotherham, UK
Introduction: Many organisms, including H pylori, take up DNA from their environment (competence), using it as an energy source and occasionally for genetic transformation. This is enabled by a complex network of ComB proteins, located close to and within the bacterial cell membrane. H pylori alone possesses the comH gene, which when deleted results in loss of competence.1
Aim: To identify the putative protein produced by comH and to determine if it is a nuclease.
Methods: The H pylori laboratory strain 26695 was cultured & DNA isolated. The comH gene was then amplified by PCR and cloned in several expression vectors (pJONEX-4, pET21, pTOPO, and pGEX-KG). Nuclease activity of the expressed protein was assessed by its capacity to fragment DNA (change in optical density) and to cleave it on DNA agarose gels.
Results: (1) The optimum conditions for expression were achieved with the pGEX-KG system. The comH is expressed as a protein fused with Glutathione S-transferase (GST). (2) GST-Com H fusion protein was expressed at high levels, particularly in E coli RIPL cells (which provide for the rare codons missing in standard E coli). (3) Cells were harvested and lysed. The GST-ComH fusion was found in the insoluble fraction so was solubilised in urea. (4) The protein was purified by affinity and ion-exchange chromatography. (5) Nuclease activity was not observed.
Discussion: The comH gene produces a protein with no homology to any protein known. Against expectation, it is not a nuclease. Its function remains unknown but we presume is in some way essential in making H pylori competent.
Conclusion: This is the first time the ComH protein, the product of the unique H pylori competence gene comH, has been expressed and purified.
Acknowledgment: K Kostidis is a Research Fellow of The Bardhan Research & Education Trust (Registered Charity No 328452).
1
330 DEPLETION OF SCAR ASSOCIATED MACROPHAGES REMOVES THE KEY SOURCE OF COLLAGENOLYTIC MMP-13 AND CRITICALLY AFFECTS SPONTANEOUS RECOVERY OF LIVER FIBROSIS
J. A. Fallowfield1, J. S. Duffield2, C. M. Constandinou1, R. Lang3, R. C. Benyon1, J. P. Iredale1.1Division of Infection Inflammation and Repair, University of Southampton, UK; 2Renal Division, Brigham & Women’s Hospital, Harvard Institute of Medicine, Boston, MA, USA; 3Division of Developmental Biology and Department of Opthalmology, Children’s Hospital Research Foundation, OH, USA
Background: Clinical studies and experimental models show the potentially reversible nature of even advanced hepatic fibrosis. However, the molecular and cellular events which mediate resolution of scar remain unclear. In particular, the role of macrophages in both fibrogenesis and spontaneous recovery requires investigation.
Methods: Rats were treated for 4 weeks or 12 weeks with intraperitoneal carbon tetrachloride to induce a reversible fibrosis or incompletely reversible cirrhosis respectively. We have shown using immunohistochemistry that both models are characterised by abundant scar associated macrophages which express matrix metalloproteinase-13 (MMP-13) and may thus be the major source of this key collagenolytic enzyme in rodents. Quantitation of MMP-13 mRNA by real-time PCR and protein by western analysis demonstrated upregulation of MMP-13 at peak fibrosis and also during early recovery when the numbers of activated stellate cells are decreasing, but macrophages are still present and associated with areas of fibrosis. Moreover, laser microdissection was used to localise gene expression within fibrotic liver and demonstrated that MMP-13 message is confined to areas of scarring.
To investigate macrophage function mechanistically, we used a transgenic mouse (CD11b-DTR) in which macrophages were selectively depleted by administration of diphtheria toxin. Macrophage depletion during early recovery inhibited the degradation of liver scar with persistence of perisinusoidal collagen and attenuated resorption of elastin. In contrast, ablation of scar associated macrophages during liver injury diminished fibrosis.
Discussion: We suggest that scar associated macrophages may contribute to the initiation of matrix degradation by perisinusoidal expression of MMP-13. In addition, the strikingly diverse effects of macrophage depletion serve to highlight their critical role in regulation of both fibrogenesis and spontaneous resolution.
331 NF-κB ACTIVATION BY BILE ACIDS: THE INFLUENCE OF ACIDITY
G. J. S. Jenkins, J. Cronin, A. Alhamdani, S. H. Doak, A. P. Griffiths, J. M. Parry, J. N. Baxter.Swansea Clinical School, University of Wales Swansea, Swansea SA2 8PP, UK
We have recently shown that the bile acids DCA and CDCA can induce transcriptional activation of NF-κB in oesophageal cell lines and ex vivo biopsies. We have also shown that NF-κB activation is increasingly observed during the metaplasia-dysplasia-adenocarcinoma sequence. Hence bile induced NF-κB activation may represent an important molecular event in oesophageal carcinogenesis.
Subsequent to activation by bile, NF-κB translocates to the nucleus and induces transcription of a set of genes including IL-8 and I-κB. Our initial studies suggested that acidity could abrogate the bile induced transactivation of NF-κB (as measured by upregulation of genes such as IL-8), but acidity alone was not sufficient to induce transactivation by NF-κB. In contrast, other groups have shown, using band-shift assays, that acidity alone can activate NF-κB (that is, cause nuclear translocation). We now show, using transcription factor assays of nuclear extracts of bile/acid treated cells, that acidity alone can indeed cause nuclear translocation of NF-κB. However, this activation falls short of inducing transcription, as measured by real-time PCR of IL-8 and I-κB. Chromatin immunoprecipitation (ChIP) assays to assess whether acidity alone causes IL-8/I-κB promoter binding, are currently in progress.
Furthermore, when cells are exposed to a combination of bile and acid, the acidity indeed modulates NF-κB dependent transcription. For example, in OE33 cells, DCA at pH7 causes upregulation of I-κB, DCA at acid pH caused far greater upregulation of I-κB, which peaked at pH6, the pKa of DCA. Furthermore, DCA at pH6 causes this increased upregulation of I-κB independently of NF-κB, as determined by including an inhibitor of NF-κB (PDTC). Therefore, another signalling pathway appears to be involved in I-κB expression and hence may interact with NF-κB signalling following acidic bile exposure.
332 REGULATION OF THE MYC NETWORK IN THE PROGRESSION TO OESOPHAGEAL ADENOCARCINOMA
J. K. R. Boult1, J. P. Bury3, A. J. Bullock4, M. J. Campbell1, P. Taniere2, S. MacNeil4, C. Tselepis1.1Division of Medical Sciences and 2Department of Clinical Pathology University of Birmingham, Birmingham, B15 2TT, UK; 3Department of Pathology and 4Division of Clinical Sciences, University of Sheffield, Sheffield, UK
Background: Barrett’s metaplasia is a premalignant lesion predisposing to oesophageal adenocarcinoma. Progression of Barrett’s metaplasia to adenocarcinoma is characterised by sequential molecular and genetic events, driven partly by components of the gastro-oesophageal refluxate. Supporting this hypothesis, it has been demonstrated that bile acids and cytokines can induce c-myc expression, consistent with the reported over expression of this oncogene during the malignant progression of BM. However, the ability of c-myc to act as a transcription factor and to influence cell fate is partly governed by levels of the related Mad family proteins, including Mad-1 and Mxi-1. This study aims to characterise the levels of c-myc, Mad1, and Mxi1 in the progression to oesophageal adenocarcinoma.
Methods: Using real-time PCR, we demonstrated a significant induction of c-myc in 6/11 and 12/19 samples of reflux oesophagitis and oesophageal adenocarcinoma, respectively. In these c-myc positive samples, there was a parallel induction in Mxi1. In the majority of samples that failed to show an elevation in c-myc or Mxi1 there was instead a dramatic induction in Mad1. Immunohistochemical staining demonstrated that c-myc was localised to the basal layer of the native squamous oesophagus whilst Mxi1 and Mad1 were expressed in the parabasal layers. C-myc and Mxi1 were localised in areas of intense inflammation in specimens of oesophagitis and expression became more widespread in Barrett’s Metaplasia and adenocarcinoma. In this regard we have established an ex vivo oesophageal raft culture system to determine the functionality of the Myc network in the oesophagus.
Conclusion: In summary, the Myc network is dysregulated in the malignant progression of Barrett’s metaplasia and may be useful in the design of therapeutic agents and as a diagnostic indicator of malignant potential.
333 THE MOLECULAR EVOLUTION OF BARRETT’S METAPLASIA
D. van Dellen, P. Jethwa, P. Taniere, S. Pelengaris, J. W. Fielding, M. T. Hallissey, C. Tselepis.Department of Medicine, University of Birmingham, Edgbaston, Birmingham, UK
Background: Barrett’s metaplasia is a premalignant lesion, which is strongly associated with gastro-oesophageal reflux disease (GORD) and predisposes to oesophageal adenocarcinoma. How GORD induces Barrett’s metaplasia however remains uncertain, though clearly components of the refluxate can induce molecular changes including c-myc expression, an oncogene over-expressed in the malignant progression of Barrett’s metaplasia. It is our hypothesis that in reflux oesophagitis, components of the refluxate can mediate c-myc leading to squamous cell apoptosis and that this event is a precursor to intestinal clonal expansion.
Methods: (1) C-myc, Bcl-2, Bcl-xl, and Bax expression in normal oesophagus, reflux oesophagitis, and Barrett’s metaplasia specimens were identified by immunohistochemistry and western blotting. (2) Levels of apoptotic activity in normal oesophagus, reflux oesophagitis, and Barrett’s metaplasia were examined by Tunel and PARP cleavage. (3) Exogenous C-myc was expressed in the suprabasal layer of oesophagus in a transgenic c-mycER murine model.
Results: (1) Western blotting revealed an increased expression of c-myc and pro-apoptotic protein (Bax) expression (18/29 and 15/22 respectively). This was confirmed by immunohistochemistry which revealed increased cytoplasmic expression in areas of high grade oesophagitis. (2) Tunel revealed increased apoptotic activity in areas of c-myc activition. (3) Two weeks of exogenous c-myc expression failed to induce a phenotypical change in the c-mycER murine model.
Conclusions: C-myc is a candidate molecule for the initiation of BM. We have demonstrated an upregulation in c-myc and Bax expression which correlates with increased apoptosis in RO. It is our hypothesis that c-myc directs apoptosis of the squamous mucosa predisposing to the formation of Barrett’s metaplasia. Future work includes transgenic basal layer over expression and oesophageal raft cultures
334 GASTRIN INDUCES MDM-2 AND SUPPRESSES P53 EXPRESSION IN AGSGR CELLS, RESULTING IN RESISTANCE TO DNA DAMAGE INDUCED APOPTOSIS
S. M. C. Przemeck1, A. J. Watson1, A. Varro2, D. M. Pritchard1.Division of 1Gastroenterology and 2Physiological Laboratory, University of Liverpool, UK
Background: In addition to regulating gastric acid secretion, the antral hormone gastrin exerts well described morphogenic and mitogenic effects upon gastric epithelium. Studies involving a number of cell lines have also suggested that gastrin can inhibit apoptosis. The mechanisms responsible for the anti-apoptotic action of gastrin are currently not fully understood.
Methods: AGSGR cells, a human gastric carcinoma cell line expressing wild type p53 and stably transfected with the gastrin-CCKB receptor were used. Expression of p53 and mdm-2 were assessed by western blotting following treatment with gastrin-17. After pretreatment with gastrin-17 for 6 hours or 24 hours, DNA damage was induced by the chemotherapeutic drug, etoposide. Apoptosis was assessed by cell counting according to morphological criteria and by flow cytometry for active caspase-3 positive cells. Cell survival was assessed by clonogenic assay.
Results: Administration of 10 nM gastrin to AGSGR cells caused increased mdm-2 protein expression at 1–2 hours and decreased p53 protein expression at 4–6 hours. Six hour treatment with 50 μM etoposide caused increased p53 expression and a 7–8 fold increase in apoptosis in AGSGR cells. Treatment of AGSGR cells for 6 hours or 24 hours with 10 nM gastrin prior to 50 μM etoposide caused significantly less p53 induction and resulted in a less than twofold increase in apoptotic cells (p<0.05). Clonogenic assays demonstrated significantly increased cell survival when AGSGR cells were pretreated for 6 hours with 1 nM or 10 nM gastrin prior to 1 hour incubation with 2–12 μM etoposide. These responses were not observed in parental AGS cells and were inhibited in AGSGR cells by the gastrin-CCKB receptor antagonists L740, 093, and YM022.
Conclusions: (1) Gastrin induces mdm-2 protein expression in AGSGR cells prior to decreased expression of p53 protein. (2) Gastrin pretreatment of AGSGR cells inhibits apoptosis and results in increased cell survival following treatment with the DNA damaging agent, etoposide.
335 RADIATION INDUCES GASTRIN-CCKB RECEPTOR EXPRESSION IN IEC-6 AND IEC-18 INTESTINAL EPITHELIAL CELLS
P. D. Ottewell1, A. J. Watson1, A. Varro2, D. M. Pritchard1.Division of 1Gastroenterology and 2Physiological Laboratory, University of Liverpool, UK
Background: We have previously demonstrated increased crypt survival in hypergastrinaemic INS-GAS mice following γ radiation and have demonstrated increased expression of the gastrin-CCKB receptor in murine intestinal epithelium following 14Gy γ radiation. In order to investigate the regulation of gastrin-CCKB receptor expression further we have now established a cell line model of this phenomenon. IEC-6 and IEC-18 cells are non-transformed pluripotent rat small intestinal cell lines which do not normally express the gastrin-CCKB receptor but do respond mitogenically to gastrin.
Methods: IEC-6 and IEC-18 cells were treated with 2Gy or 4Gy γ radiation. Gastrin-CCKB receptor mRNA was detected by nested RT-PCR. Radioligand binding studies were performed using 125I-gastrin-17 in irradiated IEC-6 cells. The effects of gastrin-17 upon cell proliferation were assessed by cell counting and 3H-thymidine incorporation in serum free and 10% serum supplemented conditions.
Results: Gastrin-CCKB receptor mRNA could not be detected in unirradiated serum treated cells. Transient expression of gastrin-CCKB receptor mRNA was observed 24 hours after serum starvation of both IEC-6 and IEC-18 cells. Gastrin-CCKB transcripts were detected in IEC-6 and IEC-18 cells 24–96 hours after 4Gy but not 2Gy γ radiation. Radioligand binding experiments confirmed specific binding of gastrin to IEC-6 cells 24 hours after 4Gy γ-radiation and the absence of binding in unirradiated cells. 10 nM gastrin had no effect upon cells cultured in serum supplemented media, but caused increased proliferation of IEC-6 and IEC-18 cells in serum free media, particularly after 4Gy γ radiation.
Conclusions: Expression of the gastrin-CCKB receptor is induced in non-transformed intestinal epithelial cells following γ radiation. This results in specific gastrin receptor binding and leads to increased proliferation following treatment with 10 nM gastrin. This suggests that induction of hypergastrinaemia may have a role in the treatment of radiation induced enteritis.
336 RADIATION INDUCES P53 DEPENDENT APOPTOSIS IN THE PROLIFERATIVE ZONE OF MOUSE GASTRIC EPITHELIUM
S. M. C. Przemeck, P. D. Ottewell, A. J. M. Watson, D. M. Pritchard.Division of Gastroenterology, University of Liverpool, UK
Background and Aims: The apoptosis induced by γ-radiation in the distal murine intestine has been extensively investigated, but the apoptotic response of gastric epithelium to γ radiation has not been well characterised. We have assessed different methods for the detection of apoptosis in mouse stomach and have then investigated the kinetics of radiation-induced gastric apoptosis, the cell types undergoing apoptosis and the genetic regulation of this response by p53.
Methods: 10–12 week old male CD1 mice were exposed to 0–14 Gy γ radiation and sacrificed at 0–72 hours. Apoptosis was assessed on a cell positional basis by light microscopy of formalin fixed gastric antrum and corpus processed for H and E, caspase 3 immunohistochemistry, or TUNEL. The cell types undergoing apoptosis were identified using immunohistochemical markers for parietal, mucous neck, and proliferating cells. Genetic regulation of this process was assessed by comparing three inbred strains and p53 wild type (+/+) and null (−/−) mice.
Results: Apoptosis was maximally induced in gastric antrum (4.4%) and corpus (1.1%) 48 hours after 12Gy radiation. Much less apoptosis was observed compared to small intestinal and colonic epithelia. H and E, caspase 3 immunohistochemistry, and TUNEL detected similar numbers and distributions of apoptotic cells. Apoptosis occurred most frequently at cell positions 5–6 in the antrum and cell positions 15–18 in the corpus, coinciding with the distribution of PCNA labelled proliferating cells, but not with H+/K+/ATPase labelled parietal cells or TFF2 labelled mucous neck cells. Inbred mouse strains showed differential sensitivities to apoptosis induction, with C57BL/6 being most and Balb/c least sensitive. Two- to threefold less apoptosis was observed in p53−/− antrum and corpus compared with p53+/+ 48 hours after 12Gy γ radiation.
Conclusions: (1) H and E, caspase 3 immunohistochemistry and TUNEL are equivalent for detection of gastric apoptosis; (2) radiation induced gastric apoptosis is p53 dependent and occurs maximally in the proliferative zone of both antrum and corpus.
337 APPLICATION OF COMPETITIVE MICROARRAYS TO ASSESS GENE EXPRESSION IN AN OESOPHAGEAL CELL LINE AFTER ACID EXPOSURE: HIGHLIGHTING QUALITY CONTROL ISSUES
C. F. Donnellan1,2, C. P. Wild1, L. J. Hardie1, S. Rollinson3, S. M. Everett2.1Molecular Epidemiology Unit, 3Academic Unit of Haematology and Oncology, University of Leeds; 2Department of Gastroenterology, Leeds General Infirmary, Leeds, LS2 9JT, UK
Background: Detection of molecular biomarkers that identify Barrett’s oesophagus patients at greatest risk of oesophageal adenocarcinoma (EA) may help to rationalise surveillance programmes. Acid reflux is an accepted risk factor for both Barrett’s oesophagus and EA, but the biological processes involved are poorly defined. Microarrays may provide a route to identifying novel biomarkers linked to reflux exposure and disease risk.
Methods: The Barrett’s oesophagus EA cell line, Flo-1, was challenged with acidified media (pH4) for 15 minutes. RNA was extracted from acid treated and control cells 6 hours later. RNA was reverse transcribed to cDNA and labelled with either green Cy3 or red Cy5 fluorescent cyanine dyes. cDNA from acid treated and control cells was competitively hybridised to oligonucleotide arrays (Human Genome Mapping Project). Both biological (RNA from separate acid treatments) and technical (the same RNA hybridised to separate arrays) replicates were conducted. Self-self (the same RNA labelled with both dyes) and dye-flip (reversing the dye labelling of samples) hybridisations were also performed.
Results: Altered expression (>twofold change in expression) of 122 genes was observed following acid challenge. However, parallel analysis of self-self arrays revealed that only 62 of these genes were not false positives. Only two genes (nuclear factor of activated T cells, cytoplasmic, calcineurin-dependent 2, and Ras-related with diabetes) exhibited dye-flipping (that is, were upregulated in the acid treated sample, whether labelled with Cy3 or Cy5 dyes). Only 17 genes were consistent across technical replicates and 1 gene between biological replicates.
Conclusions: The results show that competitive oligonucleotide arrays demonstrate Cy3 dye bias and stringent controls are needed to avoid false data interpretation. However, application of strict criteria to array data has yielded potential genes of interest that respond to acid exposure, including those that interact with c-myc and upregulate COX-II.
338 A ROLE FOR DISCS LARGE TUMOUR SUPPRESSOR PROTEIN IN BARRETT’S METAPLASIA
P. Jethwa, D. Van Dellen, P. Taniere, S. Roberts, R. T. Spychal, C. Tselepis.Division of Medical Sciences, University of Birmingham, UK
Background: Discs large (Dlg), a member of the membrane associated guanylate kinase (MAGUK) family, is essential for the maintenance of epithelial cytoarchitecture and cell proliferation in response to cell-cell contact. Dlg perturbation results in increased cell proliferation and neoplastic growth suggesting a role for Dlg as a tumour suppressor. In this regard repression of Dlg has been shown in cervical neoplasia and mammary ductal carcinomas. The aim of this study was to (1) determine the expression levels of Dlg in the progression of Barrett’s metaplasia to oesophageal adenocarcinoma and (2) examine whether Dlg expression was crucial for adherens junctional integrity.
Methods: mRNA and protein expression for Dlg and E-cadherin was determined by real-time PCR and western blotting respectively. Localisation of Dlg was determined by Immunohistochemistry. Co-localisation of Dlg and E-cadherin was determined by immunofluoresence.
Results: Dlg was repressed in 49% of oesophageal adenocarcinomas matched with normal mucosa (n = 35) of which 53% showed a concomitant repression in E-cadherin. In normal squamous oesophagus Dlg was localised to a perinuclear location in basal cells while in the differentiated layers Dlg was cytoplasmic with evidence also of immunoreactivity at cell borders. In Barrett’s metaplasia Dlg was predominantly cytoplasmic and membranous while in the progression to oesophageal adenocarcinoma Dlg immunoreactivity was markedly reduced with only cytoplasmic reactivity observed. In addition in E-cadherin positive adenocarcinoma cells Dlg was co-localised with E-cadherin at cell borders. Conversely in cells which had a loss of E-cadherin, Dlg was either absent or cytoplasmic.
Conclusions: We provide evidence that Dlg is lost in the malignant progression of Barrett’s metaplasia to oesophageal adenocarcinoma and that this may in part mediate the repression observed in E-cadherin.
339 ADIPONECTIN STIMULATES PROLIFERATION AND INTERLEUKIN-8 SECRETION BY COLONIC EPITHELIAL CELLS
O. Ogunwobi, I. L. P. Beales.Gastroenterology Unit, Norfolk and Norwich University Hospital and School of Medicine, University of East Anglia, UK
Background: Obesity is an important risk factor for many significant conditions. It has recently become apparent that fat has important immunological and endocrine functions. Factors produced by adipocytes, termed adipokines (of which leptin is the best known), regulate the function of a variety of cell types including the GI epithelium. Adiponectin is a recently discovered adiopokine. Two distinct forms of adiponectin have been described: a full length form (fAd) and a truncated form containing only the globular portion (gAd). The full functions of adiponectin remain to be determined but it appears to have anti-diabetic activity and agonists may prove therapeutically beneficial in this regard. We have examined the effects of adiponectin on human colon epithelial cells.
Methods: HT-29 cells were cultured in the presence of increasing concentrations of recombinant human adiponectin. Cell proliferation was assessed by a colormetric assay, IL-8 protein, IL-8 mRNA and activated nuclear localised transcription factors by specific ELISAs.
Results: Both forms of adiponectin produced identical enhancement of proliferation. Maximal effect was 35% above control; the EC50 was 0.01 μg/ml for both fAd and gAd. Globular adiponectin significantly enhanced IL-8 secretion to 87% above basal but was synergistic in combination with IL-1β (609% increased to 1254% above basal). Full length adiponectin had no effect alone but significantly enhanced the effect of IL-1β, although much less potently than gAd. Globular adiponectin significantly increased both IL-8 mRNA expression and nuclear translocation of NF-κB. The IL-8 stimulatory activity of gAD was abolished by the ERK inhibitor PD98059, the p38 MAP kinase inhibitor SB203580, and the NF-κB inhibitor BAY 11-7082. The growth promoting effect was unaffected by PD98059 and SB203580.
Conclusions: Adiponectin enhances proliferation of colonic cancer cells and stimulates IL-8 secretion by different intracellular pathways. Further studies into the effects of adiponectin on colonic physiology are warranted with particular regard to different nutritional situations.
340 DIFFERENTIAL EXPRESSION OF HEDGEHOG SIGNALLING COMPONENTS (SHH, IHH, PTC1, GLI1) ALONG THE LENGTH OF THE HEALTHY ADULT COLON
C. W. Lees, A. Grant, J. F. Loane, S. E. Howie, J. Satsangi.GI Unit & Centre for Inflammation Research, University of Edinburgh, UK
Introduction: Strong evidence now exists that the Hh signalling pathway is critical in the development of the adult GI tract, maintenance of epithelial stem cell populations and cellular differentiation. Dysregulation of Hh signalling in colonic neoplasia and inflammation may lead to the identification of novel therapeutic targets. However, key questions regarding the localisation of Hh homologues (Shh, Ihh), ligands (Ptc1) and downstream transcriptional regulators (Gli1) remain.
Methods: Protein expression of Shh, Ihh, Ptc1, and Gli1 were analysed by immunohistochemistry along the length of 10 healthy colons. Negative controls were included and antibody specificity determined. mRNA was detected in the same tissue by RT-PCR.
Results: Shh protein is expressed throughout the length of the healthy adult colon, in the epithelium. A clear gradient of expression is present from proximal (caecum) to distal colon, with maximal expression in the rectum. Consistent variation is present within the longitudinal axis of individual crypts, with strong luminal expression extending into the upper two thirds of crypts. Ihh protein is strongly expressed in occasional crypt cells (CD3 positive, CD56 negative cells that are also strongly positive for Ptc1), but only weakly positive in some surface epithelial cells. Ptc1 protein is strongly expressed in interstitial cells, including CD3 positive cells, and throughout the epithelium. There is no differential expression of Ptc1 in various regions of the colon.
Conclusions: There is a clear gradient of increasing expression of Shh throughout the normal colon. The transmembrane receptor, Ptc1, is present throughout the length of the colon, indicating that all areas retain the capacity to receive and process a Shh or Ihh signal. This may represent a process by which injured gut epithelium signals to the immune system. These data have clear implications for the study of up/downregulation of Hh signalling components in different disease states and interpretation of recently published data. Such gradients may also exist for other signalling pathways, and influence disease location.
341 DEVELOPMENT OF A MODEL TO INVESTIGATE THE ROLE OF TOLL-LIKE RECEPTORS IN H PYLORI INDUCED APOPTOSIS OF GASTRIC CANCER CELLS
G. Maharaj, J. B. Elder, M. Deakin, G. T. Williams.Post-grad Medicine, Keele University, UK
Background:Helicobacter pylori was classified as a class 1 carcinogen by the IARC in 1994, due to its association with gastric cancers. It has been reported to induce apoptosis in several gastric cancer cell lines, but the mechanism remains unclear. We are testing the hypothesis that apoptosis may be induced through the toll-like receptors (TLRs), some of which have recently been linked to apoptosis in other model systems. We propose that H pylori can bind the relevant TLRs, and that this engages the apoptotic machinery of the cell, possibly signaling via MyD88.
Methods: By using two gastric cancer cell lines, AGS and KATO-111, an oesophagogastric cell line OE-19, and a sonicated ultracentrifuged sample of H pylori, we have investigated the effects of this bacterium on apoptosis in these cell lines. We have monitored the expression of toll-like receptors 2, 4, 5 and 9 on these cell lines, using various techniques, for example, immunohistochemistry. Blocking experiments to elucidate their functional role in the apoptotic pathway are in progress.
Results: We have confirmed that this preparation of H pylori, induces apoptosis in AGS and KATO-111 cell lines, and report that OE-19 cells also undergo apoptosis. Apoptosis induction was time dependent, for example, by using 10 μg/ml of the sonicate, apoptotic rates at 12 hours were 10.5, 13.3, and 8.3% for AGS, Kato-111, and OE-19 respectively, whereas they increased to 20.1, 19.4, and 16.1% respectively, at 72 hours. Apoptosis induction was also dose dependent, at least up to 100 μg/ml. Preliminary data indicate that these cell lines show varying expression of the different TLRs, for example, AGS and KATO-111 appear positive for TLR4, but OE-19 does not. H pylori appears to induce the expression of some of the receptors—for example, AGS does not appear to express TLR2, but can be induced by H pylori to express it.
Conclusions: Further development of this model, by blocking the expressed TLRs, by different blocking techniques, will help determine if these receptors are involved in apoptosis. We plan to use this model system to investigate the molecular mechanisms by which H pylori affects apoptosis, a process which is central to H pylori induced pathology.
Inflammatory bowel disease posters
342 FAECAL CALPROTECTIN IN THE MANAGEMENT OF IBD AND IN THE ASSESSMENT OF PATIENTS WITH IBS
D. Parker, S. Bharathi, I. B. Holbrook, S. M. Kelly.Departments of Gastroenterology and Biochemistry, York Hospital, York, UK
Background and Aims: Calprotectin is a neutrophil derived protein that is stable in stool. It shows promise as a non-invasive marker of intestinal inflammation but as yet it is not widely employed. We reviewed our experience of calprotectin in the evaluation of patients with known IBD (quiescent and active) and in the assessment of new patients with possible IBS.
Methods: A retrospective analysis of calprotectin results, diagnosis, and outcomes was carried out. Faecal calprotectin was measured by an ELISA method (PhiCal) with a normal range of 0–60 μg/g.
Results: 118 results were available for analysis. 59 patients were known to have IBD. Calprotectin was normal in 19 of these (18 Crohn’s, 1 ulcerative colitis) correlating with the clinical impression of quiescent disease in 16 patients. Three other patients went onto further investigations that revealed no evidence of disease activity, again correlating with the normal calprotectin. Levels were elevated in 40 IBD patients (33 Crohn’s, 7 ulcerative colitis). This correlated with the clinical impression of active disease and helped guide treatment and investigation in these patients. 11 of these patients had further investigations that confirmed active disease. In 59 patients with possible IBS calprotectin was normal in 48. After appropriate investigations the final diagnosis was that of IBS in 38 of these patients. In the other 10 the final diagnosis was that of diverticulosis (2) or non-intestinal pathology (8). None had IBD. 11 of these 59 patients had an elevated calprotectin but were subsequently found not to have intestinal pathology. In 4 of these the result was very borderline (61–85 μg/g) and the final diagnosis was IBS. Two were on NSAIDs. In the 5 others the final diagnosis was IBS (3) and miscellaneous (2).
Comment: This suggests that faecal calprotectin correlates well with IBD disease activity and is a useful adjunct in the management of these patients. Calprotectin has a good negative discriminant value in the assessment of IBS and may replace invasive investigations of young patients with this possible diagnosis.
343 FAECAL CALPROTECTIN: A NON-INVASIVE, SENSITIVE, AND OBJECTIVE METHOD IN THE ASSESSMENT OF CROHN’S DISEASE ACTIVITY
D. R. Gaya1, A. Duncan2, T. D. B. Lyon2, J. B. Neilly3, S. Han3, J. Howell3, C. Liddell1, A. J. Stanley1, A. J. Morris1, J. F. MacKenzie1.1Department of Gastroenterology; 2Department of Biochemistry; 3Department of Nuclear Medicine, Glasgow Royal Infirmary, Glasgow G4 0SF, UK
Introduction: Clinical and laboratory assessment of activity in Crohn’s disease correlate poorly with endoscopic findings. However, the invasive nature of repeated endoscopic examinations and the fact that active Crohn’s disease may be beyond the reach of an endoscope has fuelled the search for faecal markers of intestinal inflammation. Calprotectin is a calcium binding protein abundant in neutrophil cytosol and is extremely stable in faeces. Studies to date have shown faecal calprotectin to be an excellent surrogate marker of neutrophil influx into the bowel lumen.
Aim: To assess whether a one-off faecal calprotectin concentration from a spot stool sample reliably detects active inflammation in patients with Crohn’s disease when compared with radiolabelled white cell scanning (WCS) and the Crohn’s disease activity index (CDAI).
Methods: Subjects were chosen if they had a previously confirmed diagnosis of Crohn’s disease and were suspected on clinical grounds to be in the midst of a relapse. 35 patients entered the study and underwent WCS and had a stool sample collected for faecal calprotectin on the same day. A CDAI was also calculated for each subject. WCS was scored by three experienced nuclear physicians who were blinded to each other, as well as the faecal calprotectin and CDAI results. Inflammation was scored at six standard sites on WCS to give a mean total severity, extent, and combined severity and extent score. Patients were excluded if they were receiving oral prednisolone, PPIs, or NSAIDs, if they had only distal/perianal disease documented, or if they had a stoma. Aminosalicylate, azathoprine, 6-mercaptopurine, or methotrexate were continued at a similar dose but no new drugs were commenced until the CDAI was completed.
Results: There was significant positive correlation between faecal calprotectin and mean total WCS score (r = 0.73, p<0.001), severity WCS score (r = 0.64, p<0.001), extent WCS score (r = 0.71, p<0.001), and the combined extent and severity WCS score (r = 0.71, p<0.001). A cut off of faecal calprotectin >100 μg/g gave a sensitivity of 80%, specificity of 67%, positive predictive value of 87%, and a negative predictive value of 64% in identifying those with and without any inflammation on a WCS. There was, however, no significant correlation between CDAI and mean total WCS score (r = 0.21, p = 0.24) nor was there significant correlation between CDAI and faecal calprotectin (r = 0.33, p = 0.06).
Conclusions: These results indicate that although CDAI does not accurately reflect inflammatory activity in Crohn’s disease, a one-off faecal calprotectin can reliably detects the presence or absence of intestinal inflammation in adults with Crohn’s disease, when compared to WCS. Furthermore, the faecal calprotectin concentration reflects the severity and/or extent of that inflammation. In the future, a spot stool sample test for faecal calprotectin may replace more invasive tests in the assessment of those with known Crohn’s disease.
344 REPEAT FAECAL AND SERUM CALPROTECTIN TO MONITOR THERAPY OF ACTIVE IBD: COMPARISON WITH CLINICAL SCORES AND PLANAR RADIO-LABELLED WHITE CELL SCANS (WCS)
A. Poullis1, A. G. Irwin1, C. Gordon1, J. Gane1, A. J. Britten1, S. Heenan1, M. A. Mendall2, W. Vennart3.1Maxwell JD St George’s Hospital, London, SW17, UK; 2Mayday University Hospital, UK; 3Thornton Heath and Pfizer, UK
Introduction: WCS provide non-invasive and accurate quantification of IBD activity. Faecal and serum calprotectin may provide novel measures of inflammation in IBD.
Aims: To compare paired faecal calprotectin and serum calprotectin levels with clinical scores and WCS in the treatment of active IBD.
Patients: 10 subjects with active ulcerative colitis (5 mild, 4 moderate, 1 severe) and 13 subjects with active Crohn’s disease (7 mild, 5 moderate, 1 severe).
Methods: Serum calprotectin, faecal calprotectin serum CRP were measured and 99mTc-HMPAO WCS were carried out before and after 2 weeks treatment of active IBD. Prior to each measure activity scores for ulcerative colitis (Powell-Tuck index (PTI) and Mayo clinic score (MCS)) or Crohn’s disease (Crohn’s disease activity index (CDAI), Harvey Bradshaw Index (HBI), and van Hees activity index (VHAI)) were calculated. Comparisons were made between static data, absolute, and percentage change of measured variables over the study period.
Results: When analysed as static values faecal calprotectin was significantly correlated to CDAI (r = 0.47, p = 0.03), VHAI (r = 0.57, p = 0.009), CRP (r = 0.34, p = 0.016), and WCS score (r = 0.57, p = 0.003). Serum calprotectin was not correlated to any other measured variables. Absolute changes in faecal calprotectin levels were not correlated to absolute changes in other variables. Absolute changes in serum calprotectin were significantly correlated to absolute changes in the PTI (r = 0.64, p = 0.05) and WCS score (r = 0.45, p = 0.05). Percentage change in faecal calprotectin was significantly correlated to percentage change in MCS only (r = 0.7, p = 0.037). Percentage change in PC was significantly correlated to percentage change in PTI (r = 0.84, p = 0.012) and MCS (R = 0.67, p = 0.04).
Conclusion: Faecal but not serum calprotectin is a useful non-invasive marker of gastrointestinal inflammation, reflecting the total inflammatory burden of the gastrointestinal tract particularly in Crohn’s disease. Changes in faecal calprotectin levels are less useful than changes in serum calprotectin levels in monitoring response to treatment particularly in ulcerative colitis.
345 PREVALENCE OF HELICOBACTER PYLORI INFECTION IN WHITE CAUCASIAN AND SOUTH ASIAN PATIENTS WITH IBD
J. D. Arnold, A. Sivagnanaratnam, A. Sangwaiya, F. Ahmad, P. Holloway, N. I. McNeil.Ealing Hospital, Southall, London, UK
Introduction: The significance of the inverse relationship suggested in previous studies between Helicobacter pylori infection and IBD is unclear. No study has been reported, to our knowledge, of H pylori infection in South Asian populations with IBD.
Aim and Methodology: Our study was designed to compare H pylori infection in patients with IBD and with healthy controls matched for ethnicity, age, and sex. Prior or current usage of sulphasalazine was an exclusion criterion. 151 consecutive IBD patients (age range 17–90, 84 females) seen in our outpatient clinics (95 ulcerative colitis, 41 Crohn’s disease, 11 indeterminate colitis) had IgG H pylori antibody titres measured for this study. All the IBD patients were diagnosed by endoscopic findings, histology, or imaging. The control group consisted of 210 people (age range 10–92, 132 females): one 111 white Caucasian and 99 South Asian people living in west London.
Results: The seroprevalence of H pylori infection was 42% (n = 151) in IBD patients compared with 40% (n = 210) in the control group. The seroprevalence was lower (34%) in Crohn’s disease (n = 41) compared with ulcerative colitis (44%), patients (n = 95) p>0.05. The seroprevalence of H pylori was similar in both Caucasian (n = 84, age range 18–85, mean age 47) and South Asian patients (n = 66, age range 17–90, mean age 46) with IBD (42%). The seroprevalence of H pylori in the control group was 37% (n = 111, age range 14–92, mean age 51) in Caucasians compared with 42% (n = 99, age range 10–83, mean age 44) in South Asians (p>0.05).
Conclusion: In our study, there were no significant differences in the prevalence of H pylori between IBD patients and the healthy controls in white Caucasian and South Asian populations, as shown by the H pylori antibody test. Differences shown in previous studies may be attributable to sulphasalazine therapy.
346 VALUE OF SERUM TRANSFERRIN RECEPTOR LEVELS IN ASSESSING IRON STATUS IN PATIENTS WITH IBD
J. D. Arnold, A. Sangwaiya, A. Sivagnanaratnam, N. I. McNeil, P. Holloway.Ealing Hospital, Southall, Middlesex, UK
Introduction: It is difficult to assess iron status in patients with chronic inflammatory conditions such as IBD. Currently available tests such as serum ferritin have limitations in differentiating iron deficiency anaemia (IDA) from anaemia of chronic disease (ACD). Serum transferrin receptor (STfR) level has been proposed as a potential tool to identify iron deficiency in patients with chronic inflammation. Ferritin levels may be raised in inflammatory disorders in spite of iron deficiency. STfR levels are not influenced by inflammation and high levels are thought to represent iron deficiency.
Patients and Methods: The aim of our study was to examine the value of STfR in the assessment of iron status in the patients with IBD in a west London population. The study comprised 154 patients with IBD between the age range 17–90 years, diagnosed on clinical, endoscopic, histological, and/or radiological findings. They were compared with age and sex matched healthy controls (n = 209) from the same local community. All patients and controls underwent blood investigations comprising haemoglobin, serum B12, red cell folate, ferritin, transferrin, serum iron, and STfR. Anaemia was defined in these patients as a haemoglobin level of less than 11.5 in females and 13.5 in males. Iron deficiency was considered to be present if the ferritin was less than 7 ng/ml or the serum iron was low less than 10 µm/l.
Results: Of the 154 patients, 61 patients were found to be anaemic based on the haemoglobin thresholds as described above. A subgroup of 44 patients was classified as IDA based on low ferrritin or iron. Seventeen of the 61 anaemic patients were found to have a normal ferritin and serum iron. STfR levels were not significantly different in the patients in the IDA group (n = 44; 2.55 (SD1.39) mg/l) compared with either patients in the ACD group (with normal ferritin and serum iron) (n = 17; 1.67 (0.77) mg/l; p>0.05) or with IBD patients without anaemia (n = 93; 1.62 (0.78) mg/l; p>0.05). These results were also not significantly different to healthy controls (n = 209; 1.55 (0.60) mg/l).
Conclusion: Anaemia is common in patients with IBD. There were no significant differences in the STfR levels in patients with IBD irrespective of iron status compared with healthy controls. The early promise of STfR as a useful tool in differentiating IDA from ACD has not been confirmed.
347 SERUM INSULIN LIKE GROWTH FACTOR-II (IGF-II) IS DECREASED IN ADULTS WITH ACTIVE COLITIS INDEPENDENT OF BODY MASS INDEX
R. J. Makins1, J. E. D. Mawdsley1, P. M. Irving1, A. B. Ballinger2.1Centre for Gastroenterology, Barts and The London, Queen Mary’s School of Medicine and Dentistry, Turner Street, London E1 2AD, UK; 2Academic Department of Medical and Surgical Gastroenterology, Homerton University Hospital, London E9 6SR, UK
Introduction: Increased serum IGF-II levels have been shown to be associated with an increased risk of sporadic colorectal cancer. We have previously demonstrated that IGF-II is up regulated in the inflamed mucosa in active colitis and in dysplasia and cancer arising on a background of colitis.1 Serum IGF-II levels in adults with colitis has not previously been investigated.
Aims: To determine whether serum IGF-II levels differ in adult patients with active colitis compared to patients with colitis in remission and with healthy controls.
Methods: Twenty patients (10 inactive, 10 active colitis) were recruited. Ten healthy volunteers acted as controls. Patients’ disease activity was assessed by sigmoidoscopy, graded by Baron’s score and by clinical assessment via the simple colitis activity index. 5 ml venous blood sample was collected from each subject centrifuged at 2000 g for 10 min with separation of serum. Serum was analysed for IGF-II using a commercially available IGF-II ELISA kit. Patients’ body mass index (BMI) was also recorded.
Results: Subject details were: 10 controls (5 female) median age 32 (range 21–36); 10 inactive patients (7 female) median age 47 (30–72); 10 active (5 females) median age 42 (32–60). Serum IGF-II was 16% lower in patients with active disease compared to controls (727 (SD37), 865 (26) respectively; p = 0.0072). No difference between controls and inactive patients or actives and inactive patients (p = 0.075). No difference in BMI between groups and no correlation between BMI and serum IGF-II levels.
Conclusions: Serum IGF-II is decreased in active colitis independent of BMI. This is in contrast to the observation that mucosal IGF-II expression is increased in active colitis and in dysplasia and cancer associated with colitis. Serum IGF-II can not, therefore, be utilised to assess cancer risk in patients with colitis as it does not reflect mucosal levels.
1
348 ACUTE PSYCHOLOGICAL STRESS INCREASES PLATELET ACTIVATION AND PLATELET–LEUCOCYTE AGGREGATE FORMATION IN PATIENTS WITH INACTIVE ULCERATIVE COLITIS
J. E. Mawdsley, M. G. Macey, D. S. Rampton.Research Centre for Gastroenterology, Barts and the London, Queen Mary School of Medicine and Dentistry, London, UK
Introduction: Acute psychological stress is reported anecdotally to worsen ulcerative colitis. Platelet activation and platelet–leucocyte aggregate (PLA) formation are increased in ulcerative colitis and may be pathogenic.12
Aim: To assess the effects of acute psychological stress on platelet activation and PLA formation in patients with inactive ulcerative colitis.
Methods: 12 patients with inactive ulcerative colitis (SCCAI<4, Baron score <2) underwent an acute psychological stress test involving an IQ test for 50 min, while listening to different music (folk and rock) in either ear. Five patients with inactive ulcerative colitis underwent a control procedure, listening to relaxing music for 50 min. Levels of stress were assessed by recording pulse and blood pressure every 15 min. Blood was taken before, at the end of, and 30 min after the protocol for analysis by flow cytometry of platelet activation (percentage platelets expressing CD62p) and percentage leucocytes forming PLAs (CD45, CD42a).
Results: The stress test increased pulse rate by an average of 5 bpm (p = 0.002). Platelet activation and PLA formation was increased by the stress test and remained elevated 30 min later (see table 1).
Abstract 348
Conclusion: Acute psychological stress increases platelet activation and formation of platelet–leucocyte aggregates in patients with inactive ulcerative colitis. These changes could play a pathogenic role in the induction of relapse by psychological stress in quiescent ulcerative colitis.
1
2
349 INFLIXIMAB IS NOT AN EFFECTIVE TREATMENT IN PATIENTS WITH CROHN’S DISEASE AND INTERNAL FISTULAE
G. Kouklakis1, J. Moschos1, A. Mpoumponaris1, S. Kadis2, G. Minopoulos1.1Endoscopy unit, Democrition University of Thrace, Greece; 2Queen Elizabeth Hospital, Gateshead, UK
Introduction: Infliximab is one of the most effective treatments in patients suffering from Crohn’s disease with internal fistulae. Not enough evidence exists to support whether it is an effective maintenance treatment for the same type of patients.
Patient Selection and Method: The study included 7 patients (4 males, 3 females) median age 24 years. They were all patients with Crohn’s disease and had internal fistulae at their initial assessment. Among the male patients with internal fistulae, the first had 2 enteroenteric, 1 enterosigmoid, and 1 enterovesical fistulae, the second had 1 enteroenteric and 1 enterosigmoid fistulae, the third one had 1 enterogluteal and 1 enterocolic fistulae, and the fourth had 1 enteroenteric fistula. Among the female patients, the first had 1 enterovaginal fistula, the second had 1 enteroenteric fistula, and the third had 1 enteroenteric and 1 enterosigmoid fistulae. All patients received infliximab 5 mg/kg intravenous at weeks 0–2 and 6 and every 8 weeks thereafter.
Results: The patient with the enterovesical fistula had an incomplete closure and suffered from repeated urinary tract infections and finally underwent surgical closure of the fistula. The patient with the enterovaginal fistula suffered from repeated infections and underwent surgical closure of the fistula. The female patient with just 1 enteroenteric fistula suffered from small bowel obstruction and had emergency surgery and the patient with the enterosigmoid fistula suffered from perforation of the sigmoid colon just after the third infusion and also had emergency surgery. In the remaining patients, although partially closed, their fistulae didn’t close completely until the 52nd week.
Conclusion: Crohn’s disease patients with internal fistulae may partially respond to infliximab during maintenance treatment, but may also develop serious complications while on treatment that can lead to surgical intervention.
350 METHOTREXATE THERAPY FOR IBD—DO TRIAL DATA TRANSLATE INTO CLINICAL PRACTICE?
A. Dahele, J. Fennel, A. Shand, J. Satsangi.Gastrointestinal Unit, Western General Hospital, Edinburgh, UK
Introduction: A remission rate of 39.4% in Crohn’s disease patients treated with 25 mg/week intramuscular methotrexate has been reported.1 65% of patients treated with this protocol were maintained in remission with 15 mg/week methotrexate orally.2 In practice, methotrexate is often used only after purine analogues have failed to control symptoms in IBD patients. The efficacy of this methotrexate protocol use in the induction and maintenance of remission in refractory IBD patients was evaluated in a retrospective case note review.
Results: Data were available for 26 patients (13 females: 13 males) aged 17–66 years (median 31). 22 patients had Crohn’s disease, 2 ulcerative colitis, and 2 indeterminate colitis. The duration of IBD ranged 0.6–28 years (median 7.5). Azathioprine had been tried in 25/26 (96%) patients, but was ineffective in 10 (40%) or poorly tolerated in 15 (60%) patients. At the start of intramuscular methotrexate, 17 (65%) patients were on oral prednisolone at a dosage ranging 0–40 (median 15) mg/day. The duration of steroid therapy ranged from 1 month to 15 years (median 7 months). Of the 25 patients treated with intramuscular methotrexate (1 patient was started on oral methotrexate), 21 (84%) reported improved symptoms after a median duration of 2 months (range 3 weeks to 4 months). Steroids were reduced in 6 (38%) patients and withdrawn in 3 (19%) patients. One man was able to stop steroids for the first time in 12 years. Prior steroid dosage and pre-treatment with infliximab did not influence the response rate. Nine patients (35%) relapsed during the intramuscular methotrexate course after a median duration of 7 weeks (range 4–17 weeks). Of the 18 patients converted to oral methotrexate, 13 (72%) relapsed after a median duration of 2 months (range 2 weeks to 9 months). All patients who had relapsed during intramuscular therapy relapsed again after conversion to oral methotrexate. Five patients (28%) did not relapse during intramuscular or oral therapy. 11/26 (42%) patients ultimately required surgery. The most common adverse events recorded were nausea in 7 (27%) and abnormal LFTs in 9 (35%) patients.
Conclusion: Using the published protocol, methotrexate therapy is efficacious in inducing remission in a proportion of refractory IBD patients, but does not maintain long term remission. An alternative maintenance regime of continued parenteral methotrexate or higher dosage oral therapy need to be evaluated.
1
2
3
351 RESCUE METHOTREXATE THERAPY IN CHRONIC ACTIVE ULCERATIVE COLITIS PATIENTS INTOLERANT OF THIOPURINES
L. Rook, S. M. Kelly.Department of Gastroenterology, York Hospital, York, UK
Background and Aims: Therapeutic options for patients with steroid dependant chronic active ulcerative colitis intolerant of thiopurines are limited. Methotrexate is employed in Crohn’s disease but its value in ulcerative colitis remains unclear. We evaluated our experience of methotrexate in this group of patients.
Methods: Patients with steroid dependant chronic active ulcerative colitis intolerant of thiopurines and reluctant to consider colectomy were offered methotrexate therapy after a full, informed discussion. Patients were treated as per our established protocol for Crohn’s disease. They received subcutaneous methotrexate 25 mg weekly for 12 weeks followed by oral methotrexate 15 mg/week thereafter. All patients also received standard folic acid therapy. If patients improved steroids were slowly reduced and stopped.
Results: Eight patients (4 male, mean age 45 years, range 23–57) intolerant to thiopurines (azathioprine and or 6-mercaptopurine) were started on methotrexate. Six responded with a clinical remission and all were able to fully withdraw steroid therapy. Currently they remain well on oral methotrexate after a mean follow up period of 10 months (range 4–18). Two patients failed to respond and went on to colectomy. Response rate in this small group was therefore 75%. Methotrexate was well tolerated. One patient reduced the dose because of nausea but remains well on 7.5 mg/week. No other adverse events were recorded.
Conclusions: Methotrexate is worth considering in this group of patients and our results are encouraging. Clearly further studies are required to evaluate the place of methotrexate in patients with chronic active ulcerative colitis who are intolerant of thiopurines.
352 REGIONAL VARIATION OF mRNA OF HYDROGEN SULPHIDE DETOXIFICATION ENZYMES IN THE COLON MAY PREDISPOSE TO ULCERATIVE COLITIS
S. C. Kong, E. Furrie, G. T. Macfarlane, J. H. Cummings.Division of Pathology and Neuroscience, Ninewells Hospital and Medical School, Dundee, UK
Background: Ulcerative colitis starts in the rectum and spreads proximally. The exact mechanism for this is not known. This pathogenesis may be due to the inability of certain parts of the colon to detoxify the toxin hydrogen sulphide (H2S). This study looks at the distribution of mRNA of H2S detoxification enzymes rhodanese (RH), mercaptopyruvate sulphurtransferase (MST), and sulphite oxidase (SO) in ulcerative colitis and normal colon.
Methods: Colonic biopsies were taken from the rectum, descending colon, transverse colon, and ascending colon of 10 ulcerative colitis patients and 10 patients without IBD. mRNA for each of the H2S detoxification enzyme was quantitated using enzyme specific primers and real time PCR (iCycler). GAPDH was used as housekeeping gene to normalise the result.
Results: Table shows result for ulcerative colitis colon. The Wilcoxon signed rank test showed that the ascending colon has statistically more mRNA of RH than the rectum or descending colon (p = 0.005 and p = 0.017, respectively). Ascending colon also has statistically more mRNA of MST than decending colon (p = 0.028). There was no statistical difference in the mRNA of H2S detoxification enzyme levels between ascending colon and the rectum/descending colon in the normal colon of the non-IBD patients.
Conclusion: This study suggests that the ability of the rectum and descending colon in ulcerative colitis to detoxify H2S may be impaired and thus possibly explaining why ulcerative colitis starts in the distal colon and tends to affect the left colon.
Abstract 352
353 MODE OF DELIVERY AND RISK OF FAECAL INCONTINENCE IN WOMEN WITH OR WITHOUT IBD: QUESTIONNAIRE SURVEY
J. Ong, G. Edwards, M. C. Allison.Departments of Gastroenterology, Obstetrics and Gynaecology, Royal Gwent Hospital, Newport NP20 2UB, UK
Introduction: Elective caesarean section may be recommended for patients with Crohn’s disease and perineal involvement. Many patients with ulcerative colitis and proctitis develop urgency and fear of incontinence while their disease is active. Little is known about caesarean section rates in parous women with IBD, nor the possible long term impact of vaginal delivery and episiotomy on continence in women with IBD.
Methods: Questionnaires were sent to all 467 members of the south east Wales branch of the National Association for Colitis and Crohn’s Disease. Male members were asked to request their unaffected female spouse/partner to complete the forms in order to give a control group.
Results: Completed forms were returned by 301 members (response rate 65%). Forms from seven single males were excluded. Caesarean section had been undertaken for 25 of the 142 parous women with IBD (18%) v 9 of the 69 without IBD (13%; χ2 = 0.52, p = ns). Only one woman had undergone caesarean section due to IBD. Of the parous women with IBD 36 (25%) had persisting problems with faecal incontinence, of whom 8 (22%) dated this back to the time of vaginal delivery. Only one of the parous control group had suffered persisting faecal incontinence following vaginal delivery. Subjective attributions as to onset of faecal incontinence in each group are summarised in the table.
Abstract 353
Conclusions: Persisting faecal incontinence is reported by a significant minority of parous women with IBD, and nearly 25% date this back to vaginal delivery. Caesarean section is rarely recommended due to IBD alone. If our findings are confirmed in prospective studies the threshold for recommending caesarean section may need to be lowered for patients with IBD.
354 A STUDY OF ADVERSE EVENTS ARISING FROM AZATHIOPRINE AND 5-AMINOSALICYLATE CO-PRESCRIPTION IN IBD
J. H. Makhijani, C. S. Probert.Department of Gastroenterology, Bristol Royal Infirmary, Bristol, UK
Introduction: There is an alleged interaction between azathioprine and 5-aminosalicylate that has caused increased anxiety regarding co-prescription among gastroenterologists and it is not clear whether this interaction is real.
Aims: To assess the effect of combination treatment of 5-aminosalicylate and azathioprine in patients with IBD.
Methods: Retrospective analysis of 100 patients prescribed azathioprine in IBD clinic between January 2002 and January 2004 was performed. Review of case notes identified 31 patients receiving azathioprine (group I) and 69 patients who were receiving azathioprine with 5-aminosalicylate (Group II). Data were collected from both groups on drug tolerance, withdrawal, side effects, and thiopurine-S-methyl transferase (TPMT) level if measured.
Results: It was observed that the incidence of withdrawal of azathioprine due to adverse effects in group II was 49% (34/69) compared with 32% (10/31) in group I. In 76% (19/25) of patients in group II, azathioprine had to be withdrawn despite being on a low dose as compared to only 27% (3/11) in group I. TPMT level was measured in 50% of the patients and was normal in 42%. Reasons for withdrawal of azathioprine due to adverse effects were as follows: abdominal symptoms (4 in group I, 8 in group II), infection (2 in each group). In group II, 5 patients had myelosuppression, 2 developed pancreatitis, 1 had abnormal liver function tests, and in 7 patients azathioprine was withdrawn due to miscellaneous causes like fever, joint pain, and malaise; however, none of these was encountered in group I. Poor disease control accounted for withdrawal in 2 patients in group I and 3 patients in group II. In 3 patients azathioprine was withdrawn on request of the patients (pregnancy).
Conclusion: Adverse effects appeared more common in the group with combination treatment. There was no evidence of nephrotoxicity in this series. A significant number of patients in the co-prescription group were unable to tolerate even a low dose of azathioprine. TPMT levels did not predict those patients who were intolerant to azathioprine or combination of azathioprine and 5-aminosalicylate.
355 PHASE I/II TRIAL OF TREFOIL FACTOR FAMILY 3 (TFF3) ENEMA THERAPY WITH ORAL MESALAZINE FOR MILD TO MODERATE LEFT-SIDED COLITIS
A. Mahmood, L. Melley, A. J. Fitzgerald, S. Ghosh, R. J. Playford.Department of Gastroenterology, Imperial College, London W12 0NN, UK
Introduction and Aims: Current treatment of ulcerative colitis is imperfect. Trefoil peptides are known to stimulate repair in many models of injury, including animal models of colitis. We have now assessed the efficacy of TFF3 enema treatment in a clinical trial.
Methods: Patients with mild to moderate left sided ulcerative colitis were recruited into a double blind randomised placebo-controlled study. Patients taking steroids or with proctitis only were excluded. Patients received 75 ml enema containing either TFF3 (10 mg/ml) or saline alone once a day for 14 days. All patients also received an oral dose increment of 1.2 g mesalazine daily above their normal usage. Patients were assessed at 0, 2, 4, and 12 weeks. Remission was defined as UCDAI of 0 or 1 with no blood in stool. Individual clinical improvement was defined as a UCDAI reduction of >3. Results are expressed as median (IQR). Data were analysed using χ2 and ANOVA. If a patients condition deteriorated, requiring withdrawal, subsequent visit data were not included.
Results: See table. Analysed on an intention to treat basis, only 1 patient went into remission (in TFF3 group at day 28). UCDAI significantly reduced over time in both groups (p<0.05). Clinical improvement was seen in 2 TFF3 and 3 placebo patients on day 14 and 2 patients in each group on day 28. In the ANOVA, no interaction due to the use of TFF3 was seen.
Abstract 355
Conclusion: Increasing the dose of 5ASA was moderately effective in reducing UCDAI but was insufficient to induce remission. TFF3 enema was well tolerated but did not provide additional benefit above that of adding additional 5ASA alone.
356 TOPICAL 5-AMINOSALICYLATE CAN BE ADDED TO HIGH DOSE (4 G) ORAL THERAPY WITHOUT SIGNIFICANT CHANGES TO URINARY CONCENTRATIONS OF 5-AMINOSALICYLATE AND ACETYL-5-AMINOSALICYLATE OR EVIDENCE OF RENAL ADVERSE EFFECTS
C. Probert1, P. Marteau2, J. Ford3, J. Rademaker4, M. Parkes5, A. Forbes6, S. Riley7, D. Burke8, T. C. K. Tham9, M. Foldager10.1Gastroenterology, Bristol Royal Infirmary, Bristol, UK; 2Paris, France; 3Bristol, UK; 4Hastings, UK; 5Cambridge, UK; 6London, UK; 7Sheffield, UK; 8Carlisle, UK; 9Belfast, N. Ireland; 10Ferring, Denmark
Background: A recent multi-national study included 127 mild-moderate ulcerative colitis patients, treated with Pentasa 4 g oral 5-aminosalicylate daily, for 8 weeks and randomised to receive a Pentasa enema containing 1 g 5-aminosalicylate or placebo, for weeks 1–4 (PINCE study1). In view of the high 5-aminosalicylate dose, an additional safety evaluation was performed in patients recruited in the UK.
Methods: Serum creatinine, urine protein, and urine haemoglobin were measured at inclusion and after 4 weeks and 8 weeks. For UK patients, at week 4 and 8 visits, levels of 5-aminosalicylate and Ac-5-aminosalicylate were determined from urine samples collected after the previous bedtime dose.
Results: For serum creatinine, urine protein, and urine haemoglobin findings, there were no distinct changes during the study, nor were there obvious differences between the treatment groups. For UK patients, there were no significant differences in urinary excretion of 5-aminosalicylate or Ac-5-aminosalicylate between the two groups as shown in the table. Full data were available at all time points for 14 patients and there were no differences within each group comparing levels at week 4 and week 8.
Abstract 356
Conclusion: The addition of topical treatment to oral therapy did not appear to increase the amount of drug processed by the kidneys and did not cause any renal adverse effects. These data add reassurance to the successful outcome of the PINCE study.
1
357 CAREFUL PATIENT SELECTION MAY IMPROVE RESPONSE RATES TO INFLIXIMAB IN IBD
C. B. Pearce, C. W. Siah, D. J. E. Cullen, I. C. Lawrance.Fremantle Hospital, Western Australia
Introduction: The use of infliximab in Crohn’s disease is well known, but controversial in ulcerative colitis. Patient driven usage of infliximab for Crohn’s disease is common in the USA and may lead to its use for non-Crohn’s disease symptoms, thus reducing the response rates. Careful selection of truly active, refractory Crohn’s disease patients may thus improve the clinical effectiveness of infliximab.
Aims: To determine whether careful patient selection can improve response rates and if infliximab is of use in ulcerative colitis.
Method: Patients receiving infliximab for IBD were considered for treatment only after failure of disease control with conventional therapy, that is 5-aminosalicylate, steroids, immunomodulation, and antibiotics and after confirmation of active disease by endoscopy or the presence of active fistulae. Patients were classified as Crohn’s disease or non-Crohn’s disease IBD. Side effects were analysed for any patient receiving infliximab.
Results: 190 infusions were given to 63 patients (35 Crohn’s disease, 14 non-Crohn’s disease IBD, 14 other). In Crohn’s disease, 107 infusions were given with 83% (29/35) of patients treated for severe inflammatory disease (2.9 infusions/patient) and 37% (13/35) treated for fistulising disease (3.6 infusions/patient). For inflammatory disease, 90% responded (26/29) and 62% attained remission (18/29). 11 patients with fistulising disease (85%) responded and 46% (6/13) resolved their fistulae. In non-Crohn’s disease IBD, 21 infusions were given (1.5 infusions/patient), 64% of patients (9/14) responded, and the remission rate was 50% (7/14). Ten per cent (6/58) of all patients experienced adverse events. Three per cent (2/58) had serious adverse events. There was one death secondary to alcoholic hepatitis not thought to be infliximab related.
Summary: Our results in non-Crohn’s disease IBD suggest clinical efficacy and encourage consideration in this condition. Our response and remission rates in IBD appear better than the standard published results, while side effect rates are similar. The practice of careful patient selection may therefore improve the effectiveness of infliximab and its cost-effectiveness.
358 CAN BOWEL ULTRASOUND REPLACE COLONOSCOPY IN DIAGNOSING ULCERATIVE COLITIS FLARE-UP AND MONITORING ITS RESPONSE TO MEDICAL THERAPY? A PROSPECTIVE, ENDOSCOPIC CONTROLLED STUDY
F. Parente1, S. Greco1, M. Molteni1, A. Anderloni1, L. Pastore1, S. Ardizzone1, G. M. Sampietro2.1Department of Gastroenterology, L Sacco University Hospital, Milan, Italy; 2Digestive Surgery, L Sacco University Hospital, Milan, Italy
Background and Aim: Although bowel ultrasound has proved to be an important diagnostic tool in IBD, especially in Crohn’s disease, its usefulness as primary imaging procedure in patients with ulcerative colitis is still unclear. We therefore undertook a prospective endoscopic controlled study to assess the accuracy of bowel ultrasound in defining the extension, the severity, and the response to medical treatment of ulcerative colitis.
Material and Methods: 85 patients with already proven extensive ulcerative colitis consecutively seen in the outpatient IBD clinic or admitted to our unit for the suspicion of disease flare-up entered the study. All patients underwent bowel ultrasound and total colonoscopy as well as routine laboratory tests. Patients with active ulcerative colitis were re-studied on two more different occasions (8 and 24 weeks after treatment with steroids, respectively) by colonoscopy and ultrasound. The clinical (Truelove) and endoscopic activity (Baron) indices of the disease were assessed on each occasion. At bowel ultrasound the presence and the degree of colonic wall thickening, the echopattern, the vascularity, as well as the loss of haustra coli were considered and taken into account in calculating an ultrasound activity index.
Results: 78 out of 85 patients had ulcerative colitis flare-up. The accuracy of bowel ultrasound in detecting active ulcerative colitis was 91%. The extension of active ulcerative colitis was correctly defined at ultrasound in 87% of patients. The ultrasound activity index strongly correlated with clinical and endoscopic activity before treatment (ultrasound index/endoscopic index r = 0.78; ultrasound index/clinical index r = 0.69). Moreover, ultrasound index decreased significantly in patients who experienced clinical improvement with steroids paralleling the behaviour of the clinical and endoscopic indices, whereas it did not change in those unresponsive to medical therapy.
Conclusions: Bowel ultrasound is highly predictive of disease flare-up in patients with an already known extensive ulcerative colitis and is also very useful in evaluating the anatomical localisation of disease. In addition, colonic ultrasound appearance correlates well with the clinical and endoscopic activity of ulcerative colitis, thus supporting the use of bowel ultrasound as a reliable alternative to coloscopy in evaluating patients’ response to medical therapy.
359 FACTORS AFFECTING THE TIME TO IBD DIAGNOSIS IN CHILDREN: IMPLICATIONS FOR PRACTICE
R. K. Russell1,3, J. R. Read1, P. Rogers2, P. M. Gillett2, J. Satsangi3, D. C. Wilson1,2.1Department of Child life and Health, University of Edinburgh, Royal Hospital for Sick Children, Edinburgh, UK; 2Department of Paediatric Gastroenterology and Nutrition, Royal Hospital for Sick Children, Edinburgh, UK; 3Gastrointestinal Unit, Western General Hospital, Edinburgh, UK
Introduction: This study investigated the various medical factors that may contribute to the diagnostic delay in IBD, namely: type of IBD, the referral pathway, and investigations performed.
Methods: A retrospective case note review in a tertiary paediatric gastroenterology centre from 1996–2004.
Results: 142 patients were studied: 61% had Crohn’s disease, 23% ulcerative colitis, and 16% IC. Median age at diagnosis was 11 years. Median time from symptom onset to diagnosis was 27 weeks. Median time from hospital referral to diagnosis was faster in medical paediatrics compared with paediatric surgery (8.5 v 20 weeks, p = 0.02). Children with failure to thrive at diagnosis took longer to diagnose (32 v 11.5 weeks, p = 0.001). Patients presenting with classical symptoms of Crohn’s disease were diagnosed faster (11 v 31 weeks; p = 0.001). Diarrhoea in IBD patients resulted in faster diagnosis than those without (11 v 20 weeks; p = 0.001). 96% of patients had raised inflammatory markers at diagnosis. Colonoscopy with upper endoscopy (UGIE) was most likely to diagnose IBD in 95% of cases. It was superior in IBD diagnosis compared with sigmoidoscopy which was diagnostic in 50% of cases (p = 0.04).
Conclusions: Median time from symptom onset to diagnosis in this series is 27 weeks. The diagnosis was made faster by referral to paediatric medical services. Classical Crohn’s disease symptoms and diarrhoea decreased time to diagnosis. Most children had abnormal blood tests at diagnosis. UGIE combined with colonoscopy is the endoscopic investigation of choice when investigating children with suspected IBD.
360 GENOTYPE-PHENOTYPE ANALYSES OF THE IBD SUSCEPTIBILITY GENE DLG5
J. R. F. Cummings1,2, K. R. Herrlinger1, T. Ahmad1, D. P. Jewell1.1Department of Gastroenterology, Gibson Laboratories, University of Oxford, Radcliffe Infirmary, Oxford OX2 6HE, UK; 2IBD Group, Wellcome Trust Centre for Human Genetics, Roosevelt Drive, Oxford OX3 7BN, UK
Background and Aims: A recent study mapped an IBD linkage region on chromosome 10 IBD to the DLG5 gene. This gene is expressed in the colon and small intestine where it encodes a scaffolding protein important in maintaining epithelial cell integrity. A modest association was reported with variants of this gene in a German cohort of IBD patients, with the strongest association seen with Crohn’s disease. No data regarding the contribution of polymorphisms within this gene to clinical phenotype currently exists. In this case-control study we attempt to replicate these findings and to explore the contribution of variation in this gene to disease heterogeneity of IBD.
Patients and Methods: We studied 699 rigorously phenotyped IBD patients (359 Crohn’s disease and 340 ulcerative colitis) and 360 healthy controls recruited from a single UK centre. Six informative SNPs were genotyped by Sequenom and gene haplotypes constructed using the PHASE software.
Results: There were no significant SNP or haplotype associations demonstrated with susceptibility to Crohn’s disease or ulcerative colitis. Analyses by phenotype showed no association with disease location, behaviour, or the presence of extra-intestinal manifestations. Analyses were repeated following stratification by the presence or absence of the three common Crohn’s disease associated NOD2/CARD15 variant alleles but again no associations were identified.
Conclusions: In this ethnically homogenous cohort of IBD patients from Oxford we were unable to demonstrate association between either disease susceptibility, or phenotype, and DLG5 polymorphisms. Larger studies may be required to replicate this previously described association.
361 MULTIPLE SNPs AT THE IBD5 LOCUS CONTRIBUTE TO THE RISK OF CROHN’S DISEASE
C. Onnie1, S. Fisher1, J. Hampe2, M. Mirza1, A. Forbes3, J. Mansfield4, J. Sanderson1, C. Lewis1, S. Schreiber2, C. Mathew1.1GKT School of Medicine, KCL, London, UK; 2University of Kiel, Germany; 3St Marks Hospital, London, UK; 4Royal Victoria Infirmary, Newcastle, UK
Aims: We investigated the report that two SNPs in the SLC22A4 and SLC22A5 genes (L503F and G-207C) are causal alleles for susceptibility to Crohn’s disease at the IBD5 locus on chromosome 5q31.1
Methods: L503F, G-207C, and six other SNPs from the 250 kb risk haplotype at IBD5 were genotyped in two large case control samples from Britain and Germany. SNP genotypes were analysed for pairwise linkage disequilibrium (LD) and association with Crohn’s disease, and a regression based haplotype method used to analyse the contribution of individual alleles or haplotypes to disease risk using the WHAP program.
Results: Strong LD was observed across the region (0.70<D′<0.98). The frequency of the risk allele was significantly increased for seven out of the eight SNPs the most significant association being found with L503F (p = 2.4×10−9). Using a conditional modelling approach with forward SNP selection (WHAP), L503F produced the most significant single SNP effect (p = 3.1×10−8). Addition of SNPs Gx100A and C2063G to the null model containing only L503F significantly improved the model fit (p = 0.0083). Forward SNP selection of G-207C did not significantly improve the fit of the regression model (p>0.5).
Conclusions: L503F, a variant shown to affect the function of the OCTN1 cation transporter encoded by SLC22A4 is likely to be a major contributor to disease risk. The other functional variant in the promoter of the adjacent SLC22A5 gene, C-207G, which is in strong LD with L503F (D′ = 0.98), did not refine a haplotype with L503F and is therefore unlikely to represent an independent risk allele. However, the inclusion of two other SNPs (Gx100A and C2063G) into a three-SNP risk haplotype significantly improved the fit of the regression model, indicating that L503F itself does not fully explain the association in the region and that other genes within the region may contribute towards disease risk.
1
362 REPLICATION OF ASSOCIATION BETWEEN IBD AND TNF-857 BUT NOT DLG5, NFKB, KERATIN 8 OR TUCAN/CARD8
S. Waller, M. Tremelling, F. Bredin, S. Greenfield, M. Parkes.Department of Gastroenterology, University of Cambridge, UK
Background: A number of positional candidate gene variants have recently been reported to show evidence of genetic association with IBD overall (TNF-857, DLG5, NFkB, Keratin 8) or Crohn’s disease (TUCAN/CARD8, TNF-1031). Replication of these findings in independent datasets is key to verifying them due to the large number of candidate gene studies undertaken globally and a tendency to use non-conservative statistical thresholds. Our aim was to attempt replication of these findings in a large well characterised IBD panel.
Methods: 1100 IBD subjects (495 Crohn’s disease, 515 ulcerative colitis, 90 indeterminate) from the Cambridge/Eastern panel and 750 healthy controls were genotyped by Taqman for the reportedly associated genetic variants listed (see table). χ2statistics were applied and association sought for Crohn’s disease and ulcerative colitis separately and IBD overall. Crohn’s disease subphenotype analysis (ileal, colonic, perianal) was undertaken for markers showing evidence of association in the primary analysis or those specifically associated with Crohn’s disease previously.
Abstracts 362, Allele frequencies (%) for the markers studied
Results: See table. TNF-857 shows modest but significant association between its common allele and IBD (p = 0.02), with equal contribution from Crohn’s disease and ulcerative colitis. No specific Crohn’s disease subphenotype associations were seen. The recently reported associations with DLG5 and TUCAN were not replicated.
363 HAPLOTYPE TAGGING SNPS IN THE VITAMIN D RECEPTOR GENE ARE NOT ASSOCIATED WITH IBD
M. Tremelling, S. Waller, F. Bredin, E. Padfield, J. Hunter, S. Middleton, J. Woodward, M. Parkes.Department of Gastroenterology, University of Cambridge
Background: Vitamin D is immunoactive and its receptor (VDR) gene maps within the IBD2 locus on chromosome 12. VDR variants have been associated with IBD but data have been weak and inconsistent. VDR gene haplotype structure has recently been elucidated: it has three blocks of strong linkage disequilibrium and typing a single “haplotype-tagging” (ht) SNP from each block provides data representative of most variation in the gene. Our aim was to study these htSNPs with previously associated VDR variants and undertake a definitive assessment of the role of this gene in IBD susceptibility.
Methods: 1100 IBD subjects (495 Crohn’s disease, 515 ulcerative colitis, 90 indeterminate) from the Cambridge/Eastern panel and 750 healthy controls (EPIC) were genotyped by Taqman for the previously associated −1739A promoter and Taq1 polymorphisms (the latter is an htSNP for haplo-block B) with two additional htSNPs dil_1450 and dil_4856 necessary for VDR gene coverage. χ2statistics were applied and stratified analysis was performed by phenotype (Crohn’s disease, ulcerative colitis), Crohn’s disease sub-phenotype (ileal, colonic, perianal) and NOD2/CARD15 status (carriage of ⩾1 of the three common variants SNP8, 12 or 13).
Results: No VDR polymorphism showed association to IBD overall, ulcerative colitis/Crohn’s disease (see table), or Crohn’s disease sub-phenotypes. For Taq1 85/495 Crohn’s disease subjects were homozygous TT v 114/748 controls (p = 0.32). The allele frequency of Taq1 in NOD2 carrying Crohn’s disease affected was 41.6% (p = 0.8).
Abstract 363, Allele frequencies (%) for the four VDR polymorphisms genotyped
Conclusion: In this large dataset no evidence of association between VDR, htSNPs, and IBD or its sub-phenotypes was observed. This study rules out anything but a minor contribution of this gene to IBD.
364 DO NOD2/CARD15 VARIANTS EXPLAIN THE HIGH PREVALENCE OF EARLY-ONSET CROHN’S DISEASE IN SCOTLAND?
R. K. Russell1, H. Drummond1, L. Smith1, N. Anderson2, E. R. Nimmo1, D. C. Wilson3,4, P. M. Gillett3, P. McGrogan5, K. Hassan5, L. T. Weaver6, M. Bisset7, G. Mahdi7, J. Satsangi1.1Gastrointestinal Unit, Western General Hospital, Edinburgh, UK; 2Public Health Sciences, Edinburgh University, UK; 3Department of Paediatric Gastroenterology and Nutrition, Royal Hospital for Sick Children, Edinburgh, UK; 4Department of Child life and Health, University of Edinburgh, UK; 5Department of Paediatric Gastroenterology, Yorkhill Hospital, Glasgow, UK; 6Department of Child Health, University of Glasgow, UK; 7Department of Paediatric Gastroenterology, Royal Aberdeen Children’s Hospital, Aberdeen, UK
Introduction: The incidence of early-onset Crohn’s disease in Scotland is one of the highest recorded worldwide. Three single nucleotide polymorphisms R702W, G908R, and Leu1007finsC in the CARD15 (formerly NOD2) gene have been implicated in susceptibility to Crohn’s disease. We have investigated whether these CARD15 variants are important in the Scottish early-onset population.
Patients and Methods: 247 IBD (167 Crohn’s disease, 60 ulcerative colitis and 20 IC) patients aged less than 16 years at IBD diagnosis were recruited. 414 parents were also recruited. PCR-based genotyping for the R702W, G908R, and Leu1007finsC mutations was performed. Transmission disequilibrium testing (TDT) was used to assess linkage and association within the parent-child trios. Detailed genotype-phenotype analysis was undertaken.
Results: Allele frequencies in Crohn’s disease were 6.4%, 2.8%, and 4.5% for R702W, G908R, and Leu1007finsC, respectively. The results are similar to the Scottish adult Crohn’s disease population, (Genes + Immunity 2004; 5:417–25), higher than controls (p = 0.007) but markedly lower than index populations studied in Europe (p<0.00001).1 19.7% of Crohn’s disease patients carried at least 1 CARD15 mutation. The population attributable risk (PAR) for the 3 CARD15 mutations was only 7.7%. TDT demonstrated preferential transmission of Leu1007finsC mutation (p = 0.006). Univariate analysis demonstrated CARD15 carriers were more likely to need surgery (p = 0.0001) and were less likely to form granulomas (p = 0.0002). At Crohn’s disease diagnosis carriers were less likely to have inflammatory disease behaviour (p = 0.02) and more likely to have stricturing disease (p = 0.02). Multivariate analysis demonstrated CARD15 carrier status was an independent risk factor for IBD surgery (p = 0.001, OR 4.5 (1.8–11.3)).
Conclusions: This is the first UK early onset NOD2/CARD15 study. The 3 CARD15 variants described have a definite, but relatively small contribution to Crohn’s disease susceptibility and behaviour, similar to the Scottish adult Crohn’s disease population. Priority should now be given to identifying novel genetic determinants within this high risk, high incidence population.
1
365 OCTN 1 AND 2 POLYMORPHISMS WITHIN THE IBD5 LOCUS PREDICT SUSCEPTIBILITY AND SEVERITY IN CROHN’S DISEASE
C. L. Noble, E. R. Nimmo, H. Drummond, L. Smith, I. D. R. Arnott, J. Satsangi.Gastrointestinal Unit, Western General Hospital, Edinburgh, UK
Introduction: Recent data have suggested that polymorphisms in the organic cation transport genes OCTN1 (a missense substitution in exon 9) and OCTN2 (a G→C transversion in the promoter) may represent disease causing mutations which account for the genetic contribution of the IBD5 locus on chromosome 5q31.1 We have assessed the contribution of IBD5, OCTN1, and OCTN2 polymorphisms in determining genetic susceptibility and disease phenotype in Crohn’s disease and ulcerative colitis.
Patients and Methods: 252 Crohn’s disease, 305 ulcerative colitis, and 294 healthy controls were studied. Genotyping for IBD5 SNPs IGR2096, IGR2198, IGR2230, OCTN1 rs1050152, and OCTN2 rs26313667 was carried out using the Taqman system. Association with disease susceptibility and genotype-phenotype relationships was investigated.
Results: The IBD5, OCTN1, and OCTN2 polymorphisms were in strong LD (D prime>0.959), so IGR2198 was used as a risk haplotype marker for IBD5. IBD5 was associated with Crohn’s disease IGR2198 variant allele frequency (49% v 41%, p = 0.007) and homozygosity (24% v 15%, p = 0.009) when compared to healthy controls. IBD5 was also associated with stricturing/penetrating disease at follow up (p = 0.015) and disease progression (p = 0.025) on univariate analysis and with the need for surgery on multivariate analysis (p = 0.006). No association was seen with peri-anal disease (p = 0.59). Variant allelic frequency of OCTN1 (53% v 43%, p = 0.0015), OCTN2 (56% v 48%, p = 0.015) and homozygosity for the transverse colon haplotype of OCTN1/OCTN2 (28.4% v 16%, p = 0.0012) were associated with Crohn’s disease v healthy controls. On multivariate analysis the transverse colon haplotype was associated with need for surgery in Crohn’s disease (p = 0.004). In the absence of the IBD5 risk haplotype an association of OCTN1/2 variants and Crohn’s disease was not observed (18.6% Crohn’s disease v 27.1% healthy controls). No associations were seen with ulcerative colitis.
Conclusions: The IBD5 locus influences susceptibility in Crohn’s disease, disease behaviour, progression and need for surgery in Crohn’s disease. No associations were seen with ulcerative colitis. The contribution of the OCTN1/2 variants was not independent of the IBD5 haplotype, and detailed genetic, functional and expression studies will be needed to confirm the precise identity of the genes within this locus.
1
366 CARD15, SMOKING, AND TIME TO SECOND OPERATION IN ILEAL CROHN’S DISEASE
J. Barbour, C. E. Todhunter, M. Price, A. Sutherland-Craggs, P. T. Donaldson, D. Dwarakarnath, W. Cunliffe, S. Kadis, C. Onnie, C. G. Mathew, J. C. Mansfield.School of Clinical Medical Sciences, University of Newcastle upon Tyne and Department of Medical and Molecular Genetics, Guy’s, King’s and St Thomas’s School of Medicine, London, UK
Background: Over 50% of patients with Crohn’s disease will require surgery. Relapse after surgery is common and unpredictable and second operations are frequent. Smoking cessation reduces relapse rate. Mutations in the CARD15 gene influence age at onset and disease location.
Aim: To investigate the interaction between smoking and CARD15 genotype and their effects on post-operative recurrence and time to second operation.
Method: Patients who had had ileal resections for Crohn’s disease were recruited from three centres and genotyped for the three common CARD15 mutations: R702W, G908R and L1007fs. Results were expressed as CARD15+ve (one or more mutant allele) or CARD15-ve (no mutant alleles). Age at first operation was analysed with respect to CARD15 genotype. The influence of post-operative smoking and CARD15 status on mean time to second operation was investigated using Kaplan-Meier survival curves.
Results: 124 patients who had had terminal ileal resections were included; 29% CARD15+ve, 71% CARD15-ve. Mean age at first operation 36.5 years (range 12–71 years), 44% post-operative non-smokers, 56% post-operative smokers. CARD15+ve patients had a significantly younger age at first operation than CARD15-ve patients, 31 years v 38 years, p = 0.0025. Smokers had significantly reduced time to second operation than non-smokers, 100 months (95% CI 84 to 116) v 160 months (95% CI 132 to 188). Smoking shortened time to second operation by 36% in CARD15+ve v 38% in CARD15-ve patients.
Conclusion: Smoking influences time to second operation in both CARD15+ve and CARD15-ve patients with Crohn’s disease.
367 THE THALIDOMIDE DERIVATIVE CC-10004 INHIBITS MMP-3 PRODUCTION FROM LAMINA PROPRIA CELLS ISOLATED FROM SUBJECTS WITH IBD
J. N. Gordon, A. R. Bremner, S. L. Pender, P. M. Goggin, T. T. MacDonald.Division of Infection, Inflammation and Repair, University of Southampton School of Medicine, UK
Introduction: We have previously shown that one of the major pathways through which pro-inflammatory cytokines such as TNFα cause tissue injury in the gut is by stimulating mucosal myofibroblasts to produce stromelysin (MMP-3) and that this can be inhibited by a p55TNFR fusion protein in a foetal gut explant model. Thalidomide has recently been reported to be effective in the treatment of steroid resistant Crohn’s disease. We decided to investigate the effect of thalidomide and three of its analogues on stromelysin production in an ex-vivo cell culture model.
Methods: Lamina propria monuclear cells (LPMCs) were isolated from colonic biopsies of subjects with IBD or uninflamed controls by dithiothreitol-EDTA-collagenase. Mucosal myofibroblasts were isolated by sequential passaging of adherent cells with purity confirmed as >95% by immunohistochemistry prior to use. TNFα was determined by ELISA, and MMP-3 and TIMP-1 by western blotting.
Results: TNFα production by PWM stimulated normal LPMCs was significantly reduced by CC-10004 (10 μg/ml) compared with vehicle control. MMP-3 production was also significantly reduced by CC-10004 (10 μg/ml) compared with vehicle control. CC-10004 was shown to cause a dose-dependent reduction in MMP-3 protein production. Neither thalidomide nor the other two analogues (CC-4047 and CC-5013) caused a significant reduction in TNFα or MMP-3 production from lamina propria monuclear cells. CC-10004 had no effect on MMP-3 production by TNFα and IL-1β stimulated gut myofibroblasts.
Conclusion: Thalidomide does not inhibit TNFα or MMP-3 from gut lamina propria mononuclear cells. However, one of its analogues, CC-10004 is effective and may represent a potential therapy for the treatment of IBD. Its efficacy is due to TNFα inhibition preventing the induction of MMPs by mucosal myofibroblasts, rather than a direct effect on MMP production.
368 LONG LIVED IgG PLASMA CELLS IN THE GUT OF PATIENTS WITH IBD
J. N. Gordon, P. M. Goggin, T. T. Macdonald.Division of Infection, Inflammation and Repair, University of Southampton School of Medicine, UK
Introduction: One of the most striking features of ulcerative colitis is the massive and uniform presence of IgG plasma cells along the diseased mucosa which recent evidence suggests may be of primary pathogenic significance. However, to date, little work has been done on gut plasma cells since they are difficult to isolate and are reported to die quickly ex vivo. We have developed a novel method of isolating functional gut plasma cells as a tool to investigating their role in IBD.
Methods: Biopsy and resection tissue specimens were obtained from patients with active IBD and from normal controls. Lamina propria mononuclear cells were isolated and immunomagnetic selection using Crohn’s disease 138, CD38, and CD54 was then undertaken to positively select various plasma cell populations. Purity of plasma cells was assessed using FACS and imunohistochemistry, functional status by IgA ELISA, and life-span using ELISPOT.
Results: Immunomagnetic selection using the plasma cell marker Crohn’s disease 138 gave the best results with a high yield of >95% pure plasma cells. Over 95% of these cells isolated from normal mucosa expressed cytoplasmic IgA. Functional activity was confirmed by the active secretion of IgA into culture supernatant over 10 days as measured by ELISA. Plasma cells from patients with ulcerative colitis contained a higher proportion which expressed cytoplasmic IgG. In culture, IgA plasma cells from both normal and ulcerative colitis patients died rapidly, however IgG plasma cells from ulcerative colitis patients persisted in culture for at least 2 weeks without exogenous stimulation and probably represent a long lived population.
Conclusion: We have developed a novel method of isolating gut plasma cells as a tool to investigate their role in IBD. IgA plasma cells die rapidly in culture but IgG plasma cells remain viable for at least 2 weeks. Since previous studies have suggested that these IgG plasma cells secrete autoantibodies of pathogenic significance, our results suggest that these long lived plasma cells contribute to tissue injury.
369 NICOTINE INHIBITS TNF-α INDUCED INTERLEUKIN-8 (IL-8) PRODUCTION BY HT29 COLONIC EPITHELIAL CELL LINE
K. M. Khatab, B. Hudspith, J. Wilson, D. S. Rampton.Centre for Gastroenterology, Institute of Cell and Molecular Science, Barts and The London Queen Mary School of Medicine and Dentistry, London, E1 2AD, UK
Background: While smoking and nicotine patches are beneficial in ulcerative colitis, smoking has a deleterious effect in Crohn’s; the reason for this paradox is unknown. IL-8 is a potent colonocyte-derived chemokine which promotes recruitment of neutrophils. The effect of nicotine on IL-8 production by colonocytes is not clear.
Hypothesis: We hypothesised that nicotine downregulates IL-8 production by epithelial cells with a colonic phenotype (HT29), but has a stimulatory effect on those with small intestinal phenotype (Caco2).
Methods: HT29 and Caco2 cells were grown in 24 well plates in DMEM until confluent. After washing with PBS and culture in serum free medium, they were stimulated with TNF-α (0–100 ng/ml) in the presence of nicotine (10−9–10−5 M). After 24 h, supernatants were collected and IL-8 assayed by ELISA.
Results: TNF-α dose dependently stimulated IL-8 production by HT29 and Caco2 cells. In HT29 cells, nicotine (in concentrations resembling those found in the serum) significantly inhibited IL-8 production (shown as pg/ml, mean (SD); see table). In contrast, nicotine had no effect on IL-8 production by Caco2 cells (results not shown).
Abstract 369
Conclusions: Nicotine had no effect on TNF-α-induced IL-8 production by cells with small intestinal phenotype (Caco2). In contrast, the results in HT29 cells suggest that nicotine’s beneficial actions in ulcerative colitis may be due in part to its inhibition of IL-8 production by colonocytes.
370 THE −174 G/C INTERLEUKIN-6 POLYMORPHISM DETERMINES GROWTH FAILURE IN PAEDIATRIC ONSET CROHN’S DISEASE
A. Sawczenko1, M. Idestrom2, A. B. Ballinger1, N. M. Croft1, I. R. Sanderson1.1Adult and Paediatric Gastroenterology, Institute of Cell and Molecular Science, Barts and The London, Queen Mary, University of London, UK; 2Department Child Health, Karolinska Institute, Stockholm, Sweden
Background: Growth impairment is a significant clinical problem for a proportion of patients whose Crohn’s disease starts in childhood. The illness is characterised by raised levels of interleukin-6 (IL-6). In a rodent colitis model, we have previously shown that IL-6 mediates growth failure, with reversal by an anti-IL-6 antibody. The IL-6 −174 G>C polymorphism is reported to affect IL-6 transcription. We therefore hypothesised that the IL-6 GG genotype would induce growth failure in children with Crohn’s disease, as this genotype is associated with increased IL-6 transcription compared to GC and CC genotypes.
Patients and Methods: The IL-6 −174 genotype was typed in 153 Northern European Caucasian children with Crohn’s disease and height and clinical data abstracted from case records. Height at diagnosis was available in all cases and for a subset of 66 that had finished growing. Plasma C reactive protein (CRP) level, at diagnosis, was used as an indirect measure of circulating IL-6 activity. Genotypes of the cases were compared to 351 controls without Crohn’s disease.
Results: At diagnosis children were significantly growth impaired (p = 0.012). However, children with the IL-6 GG genotype were more growth retarded (height standard deviation score −0.51 v −0.1; p = 0.031) and had higher CRP levels (36 v 18 mg/dl; p = 0.037) than the GC or CC genotypes. Final adult height of the GG genotype cases was also less than the GC or CC cases (p = 0.053). The frequency of the IL-6 genotypes in the cases was the same as in controls (p = 0.7).
Conclusion: These data suggest that the IL-6 −174 genotype determines growth failure, but it is not associated with a risk of developing the disease. These findings, if replicated in a distinct population, will target which children require growth sparing therapy.
371 IL-6, COL1a1, AND VDR GENE POLYMORPHISMS AND BONE MINERAL DENSITY IN CROHN’S DISEASE
C. E. Todhunter, A. Sutherland-Craggs, S. Bartram, C. G. Mathew, P. T. Donaldson, A. K. Daly, R. M. Francis, J. C. Mansfield, N. P. Thompson.School of Clinical Medical Sciences, University of Newcastle upon Tyne, UK; Department of Medical and Molecular Genetics, Guy’s, King’s and St. Thomas’s School of Medicine, UK; Department of Medicine and Musculoskeletal Unit, Newcastle upon Tyne Hospitals NHS Trust, UK
Background: Osteoporosis is an important cause of morbidity in patients with Crohn’s disease. The pathogenesis of reduced bone mineral density is multi-factorial. A range of genetic factors have been implicated in other populations of patients with osteoporosis.
Aim: To investigate the influence of IL-6, COL1a1, and VDR genotype on bone mineral density in patients with Crohn’s disease.
Method: Patients were genotyped for IL-6 NIaIII promoter SNP, C = NIaIII site present and G = NIaIII site absent, COL1a1 Sp1 transcription factor SNP, G/T transition, S = G present, s = T present, and VDR Taq1, C/T transition, and Fok1 (F/f) SNPs. Bone mineral density (BMD) was measured at the lumbar spine (LSP) and total hip using DEXA.
Results: 158 female, 87 male patients aged 24 to 70 years (mean 44 years). There were no significant differences between any genotypes and age, BMI, pre/post-menopausal status, smoking, or steroid use. 213 patients were genotyped for IL-6 SNP. LSP and total hip BMD was significantly lower in patients with GG genotype (48%) than CC genotype (15%). BMD LSP: GG 0.95 g/cm2, CC 1.03 g/cm2 (95% CI difference 0.003 to 0.15), BMD total hip: GG 0.84 g/cm2, CC 0.93 g/cm2 (95% CI difference 0.019 to 0.16). 180 patients were genotyped for COL1a1 SNP. There was no significant difference in BMD at LSP. Total hip BMD was significantly lower in patients with Ss genotype (27%) than SS genotype (53%). BMD total hip: Ss 0.81 g/cm2, SS 0.88 g/cm2 (95% CI difference 0.005 to 0.13). There were no significant differences in BMD between VDR genotypes.
Conclusion: IL-6 and COL1a1 gene polymorphisms influence bone mineral density in patients with Crohn’s disease.
372 SENSORI-NEURAL HEARING LOSS (SNHL): AN UNDER RECOGNISED EXTRA INTESTINAL MANIFESTATION OF ULCERATIVE COLITIS
S. Rao1, S. Basu1, J. Mathews1, G. K. B. Rao2, P. Bliss2, Y. S. Ang2, B. N. Kumar1.1Department of ENT and Head and Neck Surgery, Royal Albert Edward Infirmary, Wigan, UK; 2Department of Gastroenterology, Royal Albert Edward Infirmary, Wigan, UK
Background: Extra intestinal manifestations are common in ulcerative colitis but hearing loss has only been reported sporadically. Presence of sub clinical hearing loss has been described in ulcerative colitis but the ototoxic effect of salicylates has been implicated previously.
Aim: Aim of this study is to verify the hypothesis suggesting that sensori-neural hearing loss is a true extra intestinal manifestation of ulcerative colitis due to autoimmune mechanisms rather than due to ototoxicity.
Methods: Seventy six patients with ulcerative colitis were recruited in this study. Full otologic examination followed by pure tone audiometry was performed, and their hearing thresholds were compared with normal age and sex controls of the British population. Sera from the patients who had acute exacerbation in the last 12 months was compared with normal controls by immunocytochemical techniques. Nineteen patients who were not on 5-aminosalicylate were analysed separately.
Results: Statistical analysis of the audiological data showed significant sub clinical hearing loss in low to mid frequencies compared to normal population in the sub group not on 5-aminosalicylate (p<0.01). At high frequencies (8 kHz) presbyacusis negated the effect of ulcerative colitis. Sera of the patients exposed to guinea pig’s cochlea exhibited more immunoflourescence in the outer hair cell region than controls.
Conclusion: The statistical analysis and immunological tests suggests that there may be direct effect on the cochlea causing sub clinical hearing loss. This further confirmation of hearing loss attributed to the extra intestinal manifestation of ulcerative colitis.
373 HYPERGASTRINAEMIA REDUCES THE SEVERITY OF DEXTRAN SULPHATE SODIUM INDUCED COLITIS AND 5-FLUOROURACIL INDUCED MUCOSITIS IN MICE
C. A. Duckworth1, P. D. Ottewell1, R. Dimaline2, A. Varro2, D. M. Pritchard1.1Division of Gastroenterology, University of Liverpool, UK; 2Physiological laboratory, University of Liverpool, UK
Background: The role of amidated gastrin in the small intestine and colon remains unclear, especially as the gastrin/CCKB receptor is not normally expressed at these sites. We have previously demonstrated increased expression of the gastrin/CCKB receptor in murine intestine following γ-radiation and that INS-GAS mice (a transgenic strain expressing elevated serum concentrations of amidated gastrin) exhibit significantly increased small intestinal and colonic crypt survival following γ-radiation compared to their wild-type (FVB/N) counterparts. Increased crypt survival following γ-radiation was also demonstrated in FVB/N mice rendered hypergastrinaemic using omeprazole. We have now investigated whether hypergastrinaemia alters the severity of inflammatory conditions of the intestine.
Methods: Colitis was induced in adult INS-GAS and FVB/N mice by administration of 3% dextran sulphate sodium (DSS) for 5 days in the drinking water. Intestinal mucositis was induced in the same strains by administration of two intra-peritoneal injections of 400 mg/kg 5-fluorouracil (5-FU) 6 h apart. Mouse weight and stool consistency were monitored. Histological changes were assessed in H and E stained sections using the crypt survival assay and by counting cell number per hemicrypt.
Results: INS-GAS mice showed less weight loss (0.2%) and less diarrhoea 3 days following completion of DSS than FVB/N mice (14.7% weight loss) (p<0.05). Colonic crypt survival was significantly increased in INS-GAS mice (73%) 3 days after completion of DSS compared with FVB/N (44%) (p<0.05). Cell number per hemicrypt was significantly greater in small intestinal and colonic epithelia of INS-GAS mice relative to FVB/N 72 h and 96 h after 5-FU (p<0.05).
Conclusions: The severity of DSS induced colitis and 5-FU induced mucositis is reduced in hypergastrinaemic INS-GAS mice. Induction of hypergastrinaemia may be useful for treating inflammatory conditions of the intestine.
374 ISOLATED TERMINAL ILEAL ULCERATION (ITiU)—IS IT ALWAYS CROHN’S?
R. P. Arasaradnam, S. Jalil, M. E. McAlindon.Department of Gastroenterology, Northern General Hospital and The Gastroenterology and Liver Unit, Royal Hallamshire Hospital, Sheffield Teaching Hospitals, Sheffield, UK
Background: The natural history of isolated terminal ileal ulcers (ITiU) remains unknown. Although usually associated with a diagnosis of Crohn’s, this is not always confirmed on histology. A vascular hypothesis has been suggested as a possible mechanism but often in such patients, NSAID consumption is a confounding factor.
Aim: To determine the clinical relevance of isolated terminal ileal ulceration (ITiU).
Methods: We performed a retrospective analysis within two teaching hospitals in Sheffield. Case note analysis was undertaken of all patients whose colonoscopy report indicated terminal ileal ulcers in the absence of any evidence of colonic disease.
Results: See table.
Abstract 374
A clinical suspicion of Crohn’s disease was the indication for colonoscopies in the majority of patients. Only 12 (17%) had a co-existant history of NSAID consumption, 6 of whom had normal histology. Histological confirmation of Crohn’s was achieved in only 44% and a further 3 patients with CIIBD. In 21%, histology was normal. Almost half had a final diagnosis of Crohn’s. Of the remaining 36 (51%) patients, NSAID use might explain 6 (9%) of these. This still leaves 30 (41%) with an uncertain cause of their TI ulcers in whom no diagnosis was reached.
Conclusions: For patients with ITiU, almost half had histological confirmation of Crohn’s leading to a final diagnosis. 50% of NSAID users had ITiU with negative histology. No definitive diagnosis was given in 41%. Possibilities include Crohn’s or other primary small bowel disease which might become overt with time, occult NSAID use, or that ITiU are a manifestation of normal small intestine immune response. Further long term studies are required to determine this.
375 INHIBITION OF PROLIFERATION OF STIMULATED PERIPHERAL BLOOD MONONUCLEAR CELLS BY DIFFERENT ANTI-TNF THERAPIES
R. Chaudhary, M. Butler, R. Playford, S. Ghosh.Gastroenterology section, Division of Medicine, Imperial College London, UK
Background: In Crohn’s disease there is increased proliferation of immune cells associated with a resistance to apoptosis of lymphocytes. The mechanism of action of infliximab is thought to involve apoptosis of immune cells, antibody dependent cell mediated cytotoxicity (ADCC), and complement dependent cytoxicity (CDC). We report the effect of different anti-TNF monoclonal antibodies on proliferation of peripheral blood mononuclear cells.
Methods: Peripheral blood mononuclear cells (PBMC) from healthy individuals were isolated using a density gradient separation technique. Cells were stimulated using anti-CD3/28 antibodies at (0.001 ug/ml) in solution and incubated with medium containing the test anti-TNF drug (infliximab, etanercept, adalimumab) at a range of concentrations. Proliferation was assessed at day 5 using tritiated thymidine incorporation. Flow cytometry using annexin-V was performed on PBMC exposed to infliximab to assess apoptosis.
Results: The fig 1–3 represent the summary of experiments (x-axis = concentration of drug; y-axis = proliferation at day 5). Infliximab, etanercept, and adalimumab strongly inhibit proliferation of stimulated PBMC in a dose dependant fashion. Out of the three anti-TNF agents infliximab appears to be the most potent at suppressing proliferation (ANOVA p = 0.001). No increase in apoptosis was found on flow cytometry to account for this reduction in proliferation.

Abstract 375, figure 1

Abstract 375, figure 2

Abstract 375, figure 3
Conclusion: All anti-TNF antibodies suppress proliferation of stimulated PBMC but infliximab appears to be the most potent. Serum levels of anti-TNF agents would be important in suppressing immune cell proliferation in inflammation.
376 THE EPIDEMIOLOGY AND CLINICAL FEATURES OF COLLAGENOUS COLITIS IN LOTHIAN
J. N. Rajan1, C. Noble1, C. Anderson2, J. Satsangi1, A. M. Lessels2, I. D. R. Arnott1.1Gastrointestinal Unit, University of Edinburgh Department of Medical Sciences, School of Clinical and Molecular Medicine, UK; 2Department of Pathology, Western General Hospital, Edinburgh, UK
Introduction: Collagenous colitis has previously been regarded as an uncommon cause of a diarrhoeal illness. However, recent Scandinavian data have suggested a rising incidence, approaching that of Crohn’s disease. Notable similarities exist between Scotland and Scandinavia in the incidence and genetics of Crohn’s disease. The incidence of collagenous colitis in the UK is unknown. We aimed to assess the incidence and clinical features of collagenous colitis in Lothian over two 3 year cohorts and compare to existing data.
Methods: All diagnoses of collagenous colitis in Lothian are made in two pathology departments. Case ascertainment was performed by searching pathology department databases and cross-referenced with Lothian surgical audit, clinical and endoscopy databases. Diagnoses were sought for years 1998–2000 and 2001–2003. Pathological slides were reviewed to confirm a diagnosis of collagenous colitis. Clinical information was obtained by case note review and discussion with patients GP.
Results: 37 patients with a confirmed diagnosis of collagenous colitis were identified in the time period 1998–2003. There were 28 females and 9 males (ratio 3:1) with a median age at diagnosis of 64.5 years (interquartile range 44.0–74.75 years). The mean annual incidence of collagenous colitis was 0.8/100 000 population and this did not vary between the two time cohorts. A non-significant peak of incidence occurred in November with no other seasonal variations. We confirm that the principal symptom of collagenous colitis is watery diarrhoea (100%) and the commonest accompanying symptoms were weight loss (38%), abdominal pain (32%), faecal incontinence (32%), and fatigue (8%). Disease course followed a chronic continuous course in 8% of patients, a chronic intermittent course in 73% with a single attack occurring in 19% of patients. Associated autoimmune conditions occurred in 38% of patients with coeliac disease present in 14% of cases. Nine patients used lanzoprazole and NSAIDs use was present in two thirds of cases.
Conclusions: The annual incidence of collagenous colitis in Lothian is comparable to that of France but lower than reported figures from Sweden. This may reflect a low case frequency but may also be due to low clinical suspicion of the condition or the availability of endoscopic as opposed to radiological services in this region. The clinical characteristics of the identified patients reveal similar patterns to those identified in other studies.
377 THE RELATIONSHIP BETWEEN CROHN’S DISEASE ACTIVITY AND WHOLE-BODY RNA METABOLISM IN ADULT PATIENTS
I. Ladeira1, S. M. Gabe2, A. Forbes2, G. K. Grimble1.1Roehampton University, West Hill, London SW15 3SN, UK; 2St Marks Hospital, Watford Road, Harrow HA1 3UJ, UK
Aim: Early studies showed that active Crohn’s disease perturbed protein and energy metabolism. Modern treatments may mitigate this. We have, therefore, compared the relationship between disease activity and whole-body RNA turnover, which is a proxy for protein metabolism. This can be calculated from urinary excretion of the modified nucleosides and nucleobase, N2, N2-dimethylguanosine (DMG), pseudouridine and 7-methyl guanine (7MG), respectively.1
Methods: 60 adult male volunteers (37 M: 23 F) were recruited, of whom 21 were controls (healthy students) and 39 had a confirmed diagnosis of Crohn’s disease (active: n = 20, CDAI 150–400; inactive: n = 19, CDAI <150). Spot urine samples were collected between 9am and 2pm, excluding the first voiding of the morning. RNA metabolites and creatinine were determined by HPLC and automated chemistry, respectively. Excretion is expressed as μmol/mmol creatinine, RNA turnover was calculated as g/kg muscle/day assuming that 1 g creatinine is excreted by 20 kg muscle/day. Values are expressed as mean (standard deviation; SD).
Results: Disease significantly increased excretion of pseudouridine (active: 53.60 (SD 7.55), inactive: 46.14 (7.98), controls: 25.16 (1.80), p<0.05), and 7MG (active, 1.01 (0.13), controls, 0.69 (0.06), p<0.05). Calculated tRNA turnover was increased by active and inactive disease (0.23 (0.03) g/kg muscle/day and 0.21 (0.03) g/kg muscle/day, respectively, compared with controls, 0.143 (0.05) g/kg muscle/day, p<0.05) whereas rRNA breakdown compared to controls (0.19 (0.13)) was significantly increased by active disease (0.70 (0.62), p<0.05), and not by inactive disease (0.48 (0.83), p>0.05).
Conclusion: In summary, with current treatments, Crohn’s disease has a significant impact on turnover of RNA (the machinery of protein synthesis) even in patients who are in remission. We infer that protein turnover is also affected, and propose that this technique be used to investigate the effectiveness of nutrition support in these patients.
1
378 CORTICOSTEROID RESISTANCE AND DEPENDENCE IN IBD: ANALYSIS OF 5 YEAR INCEPTION COHORT
P. S. Chiam, G. T. Ho, J. Loane, H. Drummond, J. Satsangi.Gastrointestinal Unit and Department of Pathology, Western General Hospital, Edinburgh, UK
Aim and Background: Corticosteroid therapy remains the most frequently used first line therapy in the management of active IBD despite its known limitations. We aim to determine the outcome of corticosteroid therapy in a hospital based inception cohort.
Methods: All newly diagnosed patients with IBD at the Western General Hospital, Edinburgh, between January 1998 and August 2003 were identified. The outcomes were assessed at 30 day and 1 year following corticosteroid therapy. At 30 days, patients were classified as being in complete remission, partial remission, or no response. At 1 year, they were classified into prolonged response, corticosteroid dependent or requiring surgery.
Results: 136 ulcerative colitis and 80 Crohn’s disease newly diagnosed patients were identified and followed up. 86 (63%) ulcerative colitis and 60 (75%) Crohn’s disease patients required treatment with corticosteroid. At 30 days, 69 (51%) ulcerative colitis were in complete remission, 42 (31%) in partial remission and 25 patients (18%) had no response, respectively. For Crohn’s disease, 32 (40%), were in complete remission, 28 (35%) were in partial remission, and 20 (25%) patients had no response, respectively. Outcomes after 1 year in ulcerative colitis patients were prolonged response in 75 (55%), corticosteroid dependence in 23 (17%), surgery in 29 (21%), and 9 patients were lost to follow up (7%), respectively. Outcomes for Crohn’s disease patients after 1 year were prolonged response in 30 (38%), corticosteroid dependence in 19 (24%), and surgery in (35%), respectively.
Conclusion: Although corticosteroid is effective in inducing remission in IBD in the short term (79%), corticosteroid dependence (29%) and surgery (39%) are common within 1 year of follow up. The rates of corticosteroid dependence and resistance remain remarkably similar to older published series.
379 LONGITUDINAL STUDY OF BONE DENSITY CHANGES IN CROHN’S DISEASE
R. C. Rakshit, F. Al-Azzawi, K. Abrams, S. J. Iqbal, J. F. Mayberry, R. J. Robinson.University Hospitals of Leicester NHS Trust, UK
Background and Aims: Osteoporosis is an important complication of Crohn’s disease. Few longitudinal studies are available and these give conflicting results regarding long term bone density changes. This study aims to evaluate the predictive value of clinical factors and biochemical bone turnover markers for bone density changes in patients with Crohn’s disease.
Methods: Data were available for 27 patients (11 male) with Crohn’s disease followed up for 8 years. Clinical details, physical measurements, and bone mineral density (measured by Dual x ray Absorptiometry Scan (DEXA scan)) at the spine and the hip were measured at baseline and after 8 years. Biochemical markers of bone turnover (osteocalcin (BGP), bone specific alkaline phosphatase (BALP), pro-carboxyterminal propeptide (PICP), and urinary deoxypyridinoline (DPD)) were measured at baseline. SPSS (v11.5) was used for statistical analysis.
Results and Conclusion: The mean percentage bone density change in the spine was 4.4% (SD 7.8%) and −0.7% (SD 6.1%) in the hip. Seven patients were on treatment with hormone replacement therapy, calcium, and bisphosphonates. Treatment did not correlate significantly with bone mineral density changes. Baseline bone turnover markers did not correlate significantly with bone density changes in the spine (BGP r = 0.31, p = 0.12; BALP r = 0.33, p = 0.08; PICP r = 0.03, p = 0.87; DPD r = −0.002, p = 0.99) or the hip (BGP r = 0.03, p = 0.87; BALP r = 0.08, p = 0.67; PICP r = 0.18, p = 0.37; DPD r = −0.33, p = 0.86)).
A linear regression model using sex, age, body mass index, previous surgery, site of disease, duration of disease, cumulative oral steroid usage treatment with HRT/calcium, and bone turnover markers could predict 50% of bone change at the spine and 30% at the hip. Bone density change in Crohn’s disease has a multifactorial causation. Bone turnover markers do not help to predict it in the long term.
380 COST OF ILLNESS OF PAEDIATRIC IBD
A. Bassi1, Z. Bassi2, A. M. Dalzell2, D. Casson2, K. Bodger1.1Aintree Centre for Gastroenterology, University Hospital Aintree, Liverpool, UK; 2Royal Liverpool Children’s NHS Trust, Liverpool, UK
Background: Ulcerative colitis and Crohn’s disease are chronic disorders that may require repeated medical interventions. We have reported cost of illness data for adult IBD in the UK (Gut 2004), but there are no similar reports of the scale and profile of cost of illness for IBD in paediatric populations. The present study aimed to describe secondary care resource use and direct costs for IBD patients managed at a single tertiary children’s centre.
Methods: Children receiving any form of care for IBD at the centre over a 1 year time frame were identified. Case note audit of all confirmed cases was undertaken and resource use during the study time frame was abstracted. Item costs were taken from local and/or national sources.
Results: Data relating to 150 paediatric IBD patients were analysed (ulcerative colitis: n = 59, Crohn’s disease: n = 82, indeterminate colitis: n = 9). Mean age (SD) and mean duration of disease were: ulcerative colitis: 12.6 (3.7) years and 2.4 years; Crohn’s disease 13.7 (2.8) years and 2.4 years. Mean age at diagnosis (ulcerative colitis; Crohn’s disease): 10; 11 years. Seven Crohn’s disease patients (8.5%) had perianal disease/fistulating complications, 11 patients (7%) had evidence of extraintestinal manifestations (sclerosing cholangitis (1), arthritis (1), sacroilitis (1), uveitis (2), and erythema nodusum (5)). For ulcerative colitis versus Crohn’s disease: acute flare needing immunosuppressants/elemental diet 47% v 40%; hospitalisation rate 19% v 44%; surgery 6% v 7%. Costs are summarised in the table.
Abstract 380 Direct medical costs in UK sterling (£): total cost (median/patient/year; range)
Conclusions: Inpatient care accounts for 63% and 71% of overall direct costs respectively for paediatric ulcerative colitis and Crohn’s disease. This contribution of inpatient costs to total economic burden of illness is even greater than that observed in adult IBD populations.
381 HYDROGEN SULPHIDE DETOXIFICATION ENZYMES: REGULATION OF EXPRESSION BY BUTYRATE AND SULPHIDE IN HUMAN COLON
S. Ramasamy1, M. J. S. Langman1, S. Singh2, M. C. Eggo1.Division of Medical Sciences, The Medical School, Univeristy of Birminghom, UK
Introduction: In human colon, the predominant sulphur containing gas produced by sulphate reducing bacteria (SRB) is hydrogen sulphide (H2S). H2S is highly toxic and selectively inhibits butyrate oxidation. Butyrate is not only an important energy source for colonocytes but also induces differentiation. Ineffective detoxification may damage the colonic mucosal barrier resulting in IBD. The enzyme rhodanese can detoxify H2S. Rhodanese is comprised of 2 isoenzymes; thiosulphate sulphurtransferase (TST) and mercaptopyruvate sulphurtransferase (MST).
Aim: To examine the localisation of TST and MST in paraffin embedded sections of colonic crypts and investigate the regulation of their expression and activity in a human colonic cancer cell line (HT-29) by butyrate and sulphide.
Methods: HT-29 cells were treated with 2 mM butyrate and varying doses of NaHS for 24 h or 48 h. Cells were lysed in 0.1% Triton X-100 and aliquots used to assay enzyme activities. For TST the substrate was sodium thiosulphate and for MST the substrate was sodium mercaptopyruvate and the rate of thiocyanate formation was determined. Specific antisera to TST and MST were used with western blotting to examine regulation of protein expression. MST and TST expression in colonic sections was assayed by immunohistochemistry.
Results: TST activity was significantly increased by butyrate at 24 h and 48 h (62% p<0.05). Sulphide at low concentrations (0.2 mM) also increased TST activity at 24 h (21% p<0.05). Western blotting showed increased expression of TST protein. Higher concentrations of sulphide (1 mM to 3 mM) reduced enzyme activity significantly and degradation of MST and TST was seen on western blots. In sections of normal colon, TST and MST expression was found at the top of the colonic crypts where differentiation is highest and the bases of the crypts were unstained.
Conclusions: Butyrate increases the activities of isoenzymes of rhodanese. This increased expression may protect colonocytes from the toxic effects of H2S. In IBD, failure of colonocytes to differentiate may contribute to the disease process.
382 WHICH PATIENTS UNDERGO COLECTOMY FOR IBD?
M. Lang-Lenton, C. S. Waddington, R. F. A. Logan.University of Nottingham, University Hospital, Nottingham NG7 2UH, UK
Introduction: Severe ulcerative colitis is potentially life threatening, with cyclosporine being the main alternative to surgery in severe steroid refractory disease. While the outcome of colectomy is generally good with an almost zero mortality it nevertheless indicates a failure of medical therapy. The purpose of this study was to examine the circumstances preceding colectomy in our area with a view to identifying opportunities to improve our medical management.
Methods: Case record review of all patients undergoing emergency or elective colectomy for IBD between Jan 2002 and Dec 2003 and identified from a database maintained by the stoma nurses.
Results: 86 patients (46 M:40 F) (median age 48.3) having a colectomy for IBD were identified. 14 patients (16%) underwent emergency (out of hours) or urgent surgery in their first presentation. In 5 patients (35%) the disease was fulminant. In 9 patients (64%) the duration of symptoms prior to surgery was <12 weeks, steroids were used in 11 patients (78%) and cyclosporine in only 4 patients (28%). Of the remainder all (n = 69) had previously diagnosed IBD, 38 patients had elective surgery for failure of outpatient treatment, 28 had non-elective surgery for failure of inpatient treatment and 3 surgery for cancer control. In this group the mean duration of symptoms was 8.5 years (median 5.6 years). Six patients (9%) had more than five hospital admissions prior to surgery, 25 patients (36%) had 2–5 admissions, 16 patients (23%) had one admission, 17 patients (24%) had no previous admissions and 4 patients (6%) had unknown number of admissions. Medical management immediately prior to surgery consisted of steroids in 58 patients (84%), immunosupressants in 22 patients (32%), cyclosporine in 16 patients (23%).
Conclusions: In the Nottingham area most colectomies are performed in patients with previously diagnosed IBD. About half are performed electively after failure of outpatient IBD management. Of those having non-elective surgery only 12/28 (43%) had had treatment with cyclosporin and 17/28 (60%) had been tried on immunosuppressants.
383 THIOPURINE METHYLTRANSFERASE ACTIVITY IN RECTAL MUCOSA AND ERYTHROCYTES IN IBD
S. Ramasamy1, R. Picton1, M. J. S. Langman1, S. Singh2, M. C. Eggo1.Division of Medical Sciences, The Medical School, Univeristy of Birminghom, UK
Introduction: TPMT is a key enzyme in determining response to treatment with azathiopurine or 6-mercaptopurine and development of potential serious side effects. In vivo azathiopurine is metabolised to 6-MP which is further catabolised via the enzyme xanthine oxidase and methylation catalysed by thiopurine methyltransferase (TPMT).
Aim: To determine factors that influence TPMT activity in rectal mucosa and erythrocytes. We sought to determine the effects of IBD per se, patient sex, age, smoking habit, and disease activity.
Patients and Methods: Rectal biopsy samples were taken from patients with IBD and from controls during investigation of lower gastrointestinal symptoms. Blood was also collected from patients attending either endoscopic examination or gastrointestinal clinics. Control samples were predominantly patients with IBS or dyspepsia. In addition, blood was taken from laboratory colleagues to comprise a community control group.
Results: There were no significant differences between controls and the ulcerative colitis and Crohn’s disease groups in rectal TPMT activity. In erythrocytes, TPMT activity in ulcerative colitis and Crohn’s disease patients was significantly higher than community controls. In contrast, there was no significant difference among the ulcerative colitis, Crohn’s disease, and hospital control groups. Community control activity was lower than that in the hospital control group. TPMT activity was significantly lower in the 11 patients with active disease in the ulcerative colitis group compared with the 37 in remission, 0.65 (SD 0.07) pmoles/mg/minute v 0.80 (0.04), respectively, p = 0.04. Smokers in the community control group were found to have a significantly higher TPMT activity than non-smokers.
Conclusions: TPMT activity is influenced in erythrocytes by disease activity in ulcerative colitis and by smoking which may have a bearing on dosing of patients.
384 LOOP ILEOSTOMY FOR CROHN’S DISEASE: MOLECULAR CLUES TO DISEASE PATHOGENESIS
T. Ahmad1, K. Maillard2, M. Allen2, S. Goldthorpe1, M. Daperno1, F. Cummings1, B. Warren1, S. Travis1, K. Welsh3, S. Marshall3, D. P. Jewell1.1University of Oxford, UK; 2Oxagen Ltd, Abingdon, UK; 3Imperial College, London, UK
Background: Crohn’s disease is characterised by an inappropriate response of the mucosal immune system to unidentified antigens in the faecal stream. Several genomic regions are believed to harbour susceptibility genes, but positional cloning strategies have been limited by the extent of linkage disequilibrium across these gene dense regions.
Aim: To identify genes involved in susceptibility to colonic Crohn’s disease by combining positional information with changes in gene expression in early disease activation.
Methods: Five patients with a defunctioning ileostomy for refractory colonic Crohn’s disease, who were in clinical remission for at least 3 months, were studied. Patients were challenged on three consecutive days with autologous ileal effluent, instilled down the efferent ileostomy limb. Mucosal biopsies were taken from the ascending colon prior to and on day 3 of faecal challenge. Four individuals who had undergone loop ileostomy for rectal cancer acted as controls, allowing the discrimination of changes specific to Crohn’s disease. Gene expression was studied using a customised oligonucleotide array (Nimblegen) designed to include genes encoded in extended regions of replicated Crohn’s disease linkage (7396 probe sets representing ⩾3500 known genes from chromosomes 1p22–1p36, 3p24–3q12, 5q22–5q35, 6p, 14p13–14q22, 16p13–16q22, 17q12–17q25, and 19p). Hybridisations were carried out in duplicate. Genstat was used to normalise the data and test statistical models. Differential expression of selected genes is being confirmed by Q-PCR.
Results: Four of five patients exhibited a rise in CRP, of whom three had clinical and histological evidence of disease activation. No response was seen in controls. Prior to challenge significant differences in gene expression were observed between Crohn’s disease and controls. Upon challenge significant changes in expression were seen in both groups, and for 100 genes this response was significantly different (p<0.01) between Crohn’s disease and controls. Interestingly, the vast majority of these demonstrated reduced expression on challenge in Crohn’s disease, compared with controls.
Discussion: The loop ileostomy provides a unique model to study the complex pattern of gene expression characterising the initiation and amplification of the aberrant immune response in Crohn’s disease. Combined with positional information these data may help identify susceptibility genes involved in Crohn’s disease pathogenesis.
385 TARGETING MYELOID LEUCOCYTES AS SPECIFIC IMMUNE CELLS IN THE TREATMENT OF IBD: DOES THIS MEAN “TREATMENT WITH NO DRUG?”
A. Saniabadi1, H. Hanai2, Y. Suzuki3, N. Yoshimura4, Y. Saito4, K. Takeuchi5, I. Bjarnason5, R. Lofberg6.1Japan Immunoresearch Laboratories; 2Hamamatsu University; 3Sakura Hospital, Toho University; 4Chiba University; 5GKT Medical School, London; 6Karolinska Institute at Sophiahemmet, Stockholm
Background: Ulcerative colitis and Crohn’s disease are debilitating IBD that poorly respond to pharmacological interventions with salicylates, immunosuppressants, corticosteroid, or novel biologicals. Further, these agents have adverse effects that add to the disease complications. The current thinking is that IBD reflects an over exuberant immune activation driven by excessive generation of inflammatory cytokines like TNFα, IL-1β, and IL-6. However, major sources of these cytokines include myeloid cells (granulocytes and monocytes/macrophages) which in IBD are elevated with activation behaviour, prolonged survival, and are found in vast numbers within the inflamed intestinal mucosa. Accordingly, myeloid cells might be appropriate targets of therapy.
Methods: This report is based on the Adacolumn, which can selectively deplete excess and activated myeloid leucocytes. Adacolumn is filled with cellulose acetate beads that selectively adsorb myeloid cells and a small fraction of lymphocytes (Fc-gamma-R and complement receptors bearing cells). Twenty steroid naive patients with moderate (n = 14) or severe (n = 6) ulcerative colitis as measured by the Colitis Activity Index and Endoscopic Index of Rachmilewitz despite 1.5–2.25 g/day of 5-aminosalicylic acid, but none on corticosteroids, received 6 to 10 myeloid cell adsorption sessions at two sessions/week. Efficacy was assessed 1 week after the last session.
Results: All 20 patients completed their intended sessions; the majority responded to six sessions. Seventeen patients (85%) achieved remission which was maintained in 60% at 8 months. The three non-responders had deep colonic ulcers on endoscopy at study initiation. Decreases were seen in total leucocytes (9.7 (SD 1.0) to 7.0 (0.6)×103/μL, p = 0.003), percentage neutrophils (p = 0.003), percentage monocytes (p = 0.004), an increase in lymphocytes (p = 0.001), decreases in CRP (p = 0.0002), and a rise in blood levels of soluble TNFα receptors I (p = 0.0007) and II (P = 0.0045). In a separate study of 39 patients with severe ulcerative colitis who received up to 11 sessions, the remission rate was 81% in steroid refractory and 88% in steroid naive. Further, myeloid cell purging with Adacolumn has been associated with the release of IL-1 receptor antagonist, suppression of TNFα, IL-1β, IL-6, IL-8, down-regulation of trafficking and adhesion molecules, L-selectin, and the chemokine receptor CXCR3.
Conclusions: Selective depletion of myeloid cells appears to be anti-inflammatory and an effective non-pharmacological treatment for patients with active IBD. Changes in blood levels of inflammatory factors are thought to contribute to the efficacy of this procedure. The treatment has a clear drug-sparing role and potentially should reduce colectomy rate. However, this strategy warrants large controlled studies to fully evaluate its therapeutic efficacy in IBD.
386 ALTERED SERUM ANTIOXIDANTS AFTER ILEAL POUCH SURGERY: A COMPARATIVE STUDY
M. S. Muhtaseb, A. K. Foulis, D. K. Talwar, D. S. T. J. O’Reilly, R. F. Mckee, J. H. Anserson, I. G. Finlay.Lister Surgical Unit, Glasgow Royal Infirmary, Glasgow G31 2ER, UK
Introduction: Pan-proctocolectomy and ileal pouch-anal anastomosis (IPAA) is the operation of choice for patients with ulcerative colitis and familial polyposis. The aim of this study was to assess the circulating antioxidant vitamins, inflammatory status, and lipid peroxidation product (Malondiladehyde, MDA) in patients with ileal pouch-anal anastomosis and compare that with the level in healthy controls. In addition, the level of these elements was correlated with the degree of inflammation in the mucosa of the ileal pouch.
Methods: Fifty IPPA patients (16 females) with a median follow up of 10 years (2–15) and 46 age matched controls were included in the study. After overnight fasting blood was obtained for antioxidants vitamins, C-reactive protein, and Malondiladehyde. The degree of pouch inflammation was assessed according to previously described criteria, a score was given for each biopsy for acute and chronic inflammation.
Results: The patients and controls subjects had no evidence of systemic inflammatory response as measured by C-reactive protein (CRP<10).Compared with the controls the IPAA group had significant lower levels of β carotene (mean:80 v 183 μg/L, p<0.001), α carotene (mean: 17.3 v 25 μg/L, p<0.002), and lycopene (mean: 141.3 v 217.1 μg/L, p<0.001).In contrast, the IPAA group had higher levels of vitamin E cholesterol ratio (median:6.6 v 5, p<0.001).There was no difference in the plasma concentration of lutein, MDA, and vitamin A and C between the IPAA and control group. There was a positive correlation between the degree of inflammation and the level of α and beta carotene, p: 0.05 and 0.01, respectively.
Conclusion: The results of this study show evidence of reduced level of serum antioxidants in ileal pouch patients. This is either due to reduced intake, impaired absorption, or increased consumption as a result of chronic inflammation in the pouch. In contrast, vitamin E levels were significantly raised in comparison with controls, the aetiology of this is not clear. The positive correlation between the level of β carotene and the degree of inflammation in the pouch mucosa raises a question about the level these antioxidants at the mucosa level, this need to be explored in future studies.
387 SIMVASTATIN AND INFLAMMATION
T. Algladi, E. Campbell, J. A. Smith and CJ Hawkey.University of Nottingham, Division of Gastroenterology, University Hospital Nottingham, Nottingham NG7 2UH, UK
Background: Laboratory and clinical data suggest that statins reduce expression of inflammatory cytokines and adhesion molecules to an extent that is clinically useful in rheumatoid arthritis. Equally, statins commonly cause diarrhoea but mechanisms are unclear. We therefore evaluated whether the effects of simvastatins on inflammatory mechanisms had potentially anti-inflammatory effects in human colon mucosa.
Method: We used cell and organ culture and immunoassay to investigate the effect of simvastatin on release of interleukin (IL) 1β and tumour necrosis factor (TNF) α from inflamed or lipopolysaccharide (LPS) stimulated human colonic mucosa, peripheral blood and lamina propria mononuclear cells (PBMCs and LPMCs), and from microvascular human colonic endothelial (HuCE) cells isolated from operation specimens, using anti-Crohn’s disease 34 coated magnetic beads.
Results: Unexpectedly, simvastatin (10−5–3×10−3 M) caused concentration dependent (p = 0.052) increases in release of IL 1β from human colonic mucosa in organ culture, overall by 4.27 (SD 1.24) fold (n = 18). Values for TNFα were 2.48 (1.13) fold (NS). Similarly simvastatin (10−6–3×10−5 M) appeared to stimulate IL 1β secretion in HuCE, overall by 11.6 (SD 0.90) fold (1 experiment). Conversely, simvastatin (5×10−7–3×10−5 M) showed the previously recognised inhibition of IL 1 release from LPS stimulated human PBMNCs (overall by 79.7 (6.5%)) and LPMNCs (overall by 70.9 (10.1).
Conclusion: Simvastatin had potentially pro-inflammatory effects on human colonic mucosa in organ culture. The possibility that this could mediate simvastatin diarrhoea warrants investigation. The effects of simvastatin appears complex and may require understanding of different signalling pathways in endothelial and mononuclear cells.
Small bowel posters
388 EFFECT OF ISCHAEMIC PRECONDITIONING ON THE INTESTINAL INTRACELLULAR TISSUE OXYGENATION DURING ISCHAEMIA REPERFUSION INJURY OF THE INTESTINE
I. H. Mallick, W. Yang, M. C. Winslet, A. M. Seifalian.University Department of Surgery, Royal Free and University College Medical School, London, UK
Ischaemia reperfusion injury frequently occurs following abdominal surgery. Ischaemic preconditioning provides a way of protecting the intestine from damage inflicted by ischaemia reperfusion injury. The effect of ischaemic preconditioning on the intestinal intracellular tissue oxygenation following ischaemia reperfusion injury is unclear. Rats (250–300 g) were allocated into 3 groups (n = 6/group): (a) sham laparotomy; (b) ischaemia reperfusion, 30 min of superior mesenteric artery occlusion followed by 2 h of reperfusion; (c) ischaemic preconditioning, as in group B, but preceded by 10 min ischaemia and 10 min of reperfusion. Heart rate, oxygen saturation (SaO2), and mean arterial pressure (MAP) was monitored throughout the experiment. Intestinal intracellular tissue oxygenation (cytochrome oxidase) was monitored continuously by near infrared spectroscopy. At the end of the reperfusion, blood samples for lactate dehydrogenase (LDH) levels and biopsies of ileum for histological evaluation were obtained. Heart rate and SaO2 were stable in all the animals. Ischaemia of the small intestine induced transient increase in MAP (p⩽0.01). At the end of the reperfusion, ischaemia reperfusion was associated with a significant decrease in cytochrome oxidase values (p<0.05 v sham). Where as ischaemic preconditioning improved the cytochrome oxidase values significantly (p⩽0.01 v ischaemia reperfusion) at the end of reperfusion. Serum LDH was significantly reduced in ischaemic preconditioning compared with ischaemia reperfusion group (p<0.001). Histological examination showed that ischaemic preconditioning attenuated the mucosal injury. This study demonstrates the beneficial effect of ischaemic preconditioning on the intestinal intracellular tissue oxygenation after ischaemia reperfusion injury.
389 THE LIFE EXPECTANCY OF PEOPLE WITH COELIAC DISEASE IN THE UK USING LIFE TABLE METHODOLOGY
J. West, R. F. A. Logan, R. Hubbard, T. R. Card.Division of Epidemiology and Public Health, University of Nottingham, UK
Background: There may be a small increase in risk of death in people with coeliac disease when compared with the general population.1 To aid communication of this risk we present a life table analysis.
Methods: We selected people with coeliac disease from the GPRD and up to five matched controls for each. We calculated the mortality rate per 1000 years within five year age bands. We then derived life tables to enable the calculation of life expectancy.
Results: We included 4728 people with coeliac disease and 23 609 controls. The abridged life table is shown.
Abstract 389
Conclusions: People with coeliac disease do have a slightly reduced life expectancy that decreases with increasing age. Indeed, in people with coeliac disease of older ages there may even be an associated increase in life expectancy. The loss of life expectancy in people with coeliac disease is less than the difference seen between people living in Salford (73.2 years) and Salisbury (78.2 years).2
1
2
390 SMALL BOWEL BACTERIAL OVERGROWTH IN SYMPTOMATIC OLDER PEOPLE: IS EMPIRICAL ANTIBIOTIC TREATMENT JUSTIFIED?
D. A. Elphick, T. S. Chew, S. E. Higham, N. Bird, A. K. Ahmed, S. Ahmad, D. S. Sanders.Royal Hallamshire Hospital, Sheffield S10 2JF, UK
Background: In older people, small bowel bacterial overgrowth syndrome may be a common cause of diarrhoea and nutrient malabsorption. Historically, culture of jejunal aspirates was considered the gold standard investigation for this condition, but this test is invasive, costly, and often yields positive results in asymptomatic individuals. Breath tests are the preferred investigation in clinical practice. Of these the glucose breath test (GBT) is the most commonly used. We aim to determine which clinical features and baseline laboratory investigations indicate a high likelihood of small bowel bacterial overgrowth as defined by a positive GBT.
Methods: A retrospective analysis of hospital, computer, and general practitioner records for all patients referred for GBT over a 6 year period in a teaching hospital. A standard pro forma was filled out for all patient records found.
Results: Out of 197 referrals, 168 patient records were located and analysed (62 male, 106 female; median age 65), making this the largest UK based study reported. Patient characteristics predictive of a positive GBT were: increasing age (p<0.01), low serum B12 (p = 0.02), low serum albumin (p = 0.03), previous partial gastrectomy (p<0.01), previous right hemicolectomy (p<0.01), presence of small bowel diverticulae (p = 0.01), and concurrent use of a proton pump inhibitor (p<0.01). 52.5% (n = 21/40) of patients studied who were over 75 years v 21.8% (n = 28/128) of those under 75 years had a positive GBT (p<0.01). The median time to diagnosis of small bowel bacterial overgrowth from first hospital visit to positive GBT was 39 weeks.
Conclusions: As there is often a significant delay in the diagnosis of small bowel bacterial overgrowth, we would suggest that older patients with indicative symptoms and a predisposing factor (including previous partial gastrectomy, previous right hemicolectomy, small bowel diverticulae, or use of a proton pump inhibitor) or concurring laboratory indices (low B12 or albumin) could receive empirical antibiotic treatment for bacterial overgrowth without unnecessary delay in order to relieve symptoms and limit the effects of malabsorption.
391 IMMUNOLOCALISATION OF THE HUMAN DUODENAL FERRIC REDUCTASE DCYTB AND ITS RELATIONSHIP TO IRON STATUS IN SUBJECTS WITH MILD IRON DEFICIENCY
A. C. Y. Li1, A. Warley1, V. Thoree1, R. Simpson2, A. Mckie2, K. Kodjabashia1, R. P. H. Thompson1, J. J. Powell1.1Gastrointestinal Laboratory, St Thomas’ Hospital, London UK; 2Department of Life Sciences, King’s College London, London, UK
Background: The ferric reductase Dcytb plays a critical role in the absorption of dietary iron and appears to be expressed on the duodenal enterocyte brush border. Evidence suggests that Dcytb expression is increased in severe iron deficiency, especially with anaemia, but the situation in more typical mild iron deficiency is unclear.
Aims: To determine the site and extent of expression of Dcytb in patients with normal iron status or mild iron deficiency (Hb >9 g/dl and ferritin <20 ng/ml or iron saturation <20%) and also to evaluate its relationship with body and enterocyte iron status.
Methods: Duodenal biopsies and blood were obtained from 35 patients attending for routine upper gastrointestinal endoscopy. 24 (7 iron deficient and 17 iron replete) biopsies were processed for light microscopy and immunohistochemistry was performed with antibodies against Dcytb and heavy and light chain ferritin subunits. Immunolabelling was semi-quantified with image analysis software. The 11 remaining biopsies (3 iron deficient and 8 iron replete) were processed for electron microscopy. Immunolocalisation of Dcytb and intracellular ferritin was performed with appropriate primary antibodies followed by 10 nm gold conjugate labels. Labelling densities for each antibody were expressed as gold labels per micron square on duodenal enterocyte images.
Results: With light microscopy, brush border Dcytb immunolabelling intensity was strongly negatively correlated with serum iron saturation (p<0.001) but only weakly negatively with haemoglobin (p<0.08) and serum ferritin (p<0.4). Electron microscopy confirmed preferential labelling of Dcytb for microvilli rather than enterocyte cytoplasm (p = 0.001) and ferritin labels for cytoplasm (p<0.02). There was no correlation between cytoplasmic ferritin labelling and blood markers for iron status with either light microscopy or electron microscopy.
Conclusions: Dcytb expression is increased even in mild iron deficiency and is independent of duodenal enterocyte cytoplasmic ferritin expression.
392 A RANDOMISED CONTROLLED TRIAL OF NITAZOXANIDE FOR THE SYNDROMIC TREATMENT OF AIDS RELATED PERSISTENT DIARRHOEA
I. Zulu1, P. Kelly2, L. Njobvu1, S. Sainongo1, J. Mwansa1, K. Kanonga1, D. Mwenya1, V. McDonald3, M. J. G. Farthing2, R. C. G. Pollok2.1Dig. Dis. Research Project, University of Zambia School of Medicine, Lusaka, Zambia; 2Department of Adult and Paediatric Gastroenterology, Queen Mary’s School of Medcine, London UK; 3Department of Gastroenterology, St Georges’ Hospital Medical School, London, UK
Background: The majority of adults with AIDS and the persistent diarrhoea malnutrition syndrome in Zambia have protozoal intestinal infection. In an attempt to develop effective treatment, which can be offered using a syndromic approach, we carried out a double blind, randomised controlled trial of nitazoxanide in patients with this syndrome.
Methods: Patients with diarrhoea of one month duration or longer attending the University Teaching Hospital, Lusaka, were randomised to receive nitazoxanide (1000 mg twice daily) or matching placebo for two weeks and then followed up for 6 weeks. Endpoints were clinical response, parasitological clearance, and mortality.
Results: 207 adult patients were randomised; 42 died during the study. The primary assessment of efficacy was made after 17 days. Clinical response was observed in 56 (76%) of 74 patients receiving nitazoxanide and 45 (61%) of 74 patients receiving placebo (p = 0.052). However, after adjustment for CD4 count below 50/μl, the Mantel-Haenszel adjusted odds ratio for response was 2.3 (95% CI 1.1 to 5.0; p = 0.02). The rate of improvement in diarrhoea was markedly higher in patients with CD4 counts under 50 cells/μl receiving nitazoxanide while they were taking the medication (p = 0.007). Neither differences between the two groups in parasitological clearance nor mortality at 4 weeks (19%) were observed.
Conclusion: Nitazoxanide given orally for 14 days was associated with clinical improvement in AIDS patients with diarrhoea in Zambia with low CD4 counts, but the benefit was largely restricted to the period when the drug was being administered.
393 DO GLUTAMIC ACID DECARBOXYLASE ANTIBODIES PREDICT DEVELOPMENT OF OTHER AUTOIMMUNE DISEASES IN PATIENTS WITH COELIAC DISEASE?
J. S. Leeds, R. C. Bunn, M. Hadjivassiliou, D. S. Sanders.Royal Hallamshire Hospital, Sheffield, UK
Introduction: Patients with coeliac disease have been found to have a higher prevalence of other organ specific autoantibodies and autoimmune conditions such as thyroid disease. One previous paediatric report (n = 90) suggested that elevated glutamic acid decarboxylase (GAD) antibodies may be implicated in the pathogenesis of coeliac disease with specific reference to the development of other autoimmune diseases.
Aims: To assess the relationship between GAD antibodies and the prevalence of autoimmune disease in adult patients with coeliac disease.
Patients and Methods: Patients were recruited from the specialist coeliac clinic. In addition to demographic information an assessment was made of the following factors: a) duration of coeliac disease; b) compliance to gluten free diet (GFD); and c) the presence and duration of other autoimmune conditions. Endomysial antibodies, tissue transglutaminase, and IgG and IgA gliadins were checked as markers of compliance. Finally, GAD antibodies were assessed. A GAD antibody titre of 1.0 U/ml or less is considered normal.
Results: 219 patients with coeliac disease (61 males, mean age 51.6 years) were recruited. 118 patients had GAD <1.0 of which 28 (23.7%) had other autoimmune diseases and 101 patients had GAD >1.0 of which 35 (34.7%) had other autoimmune diseases (relative risk = 1.5). The most common associated autoimmune condition was thyroid disease. 60 coeliac disease patients were newly diagnosed (⩽6 months), 107 were compliant with their GFD and 52 patients were deemed non-compliant (based on history and antibody profile). Median GAD titres when subdividing according to these 3 groups were 0.9, 1.0 and 1.8, respectively (Mann-Whitney U test p = 0.024).
Conclusions: Raised GAD antibodies were significantly higher in both coeliac disease patients with ongoing gluten exposure and those coeliac disease patients with other autoimmune diseases. These data support the assertion that on-going gluten exposure increases the risk of developing other autoimmune disease. In addition, GAD antibodies may be implicated in this pathogenesis.
394 MEASUREMENT OF BONE MINERAL DENSITY IN COELIAC DISEASE: ARE THE BSG GUIDELINES ADEQUATE?
P. M. Lynch, R. Donaghy, S. D. Johnston.Department of Gastroenterology, Belfast City Hospital, Belfast, Northern Ireland
Background: A reduction in bone mineral density is associated with untreated coeliac disease. The aim of this study was to evaluate if DEXA screening of coeliac patients detected osteopaenia or osteoporosis in patients who were not identified as high risk coeliacs, according to the BSG Guidelines.
Methods: Demographic, clinical, and DEXA scan results were collected on all newly diagnosed coeliac patients over a two year period. T score <−2.5 on DEXA scan was accepted as a diagnosis of osteoporosis. Postmenopausal women, men aged >55 years, and all patients with fragility fractures were regarded as high risk coeliacs. The remainder were regarded as low risk.
Results: Forty one (13 male; mean age 43.4 years) patients diagnosed with coeliac disease were included. DEXA scan was requested in 35 (85%) patients, performed in 26 (63%) patients with a result documented in 24 (59%) patients. Of 10 high risk patients, 1 (10%) had osteoporosis, 5 (50%) had osteopaenia, and 4 (40%) were normal. Of 14 low risk patients, 1 (7%) had osteoporosis, 5 (36%) had osteopaenia, and 8 (57%) were normal.
Conclusions: Out of 24 patients with coeliac disease two (8%) patients had osteoporosis and 10 (42%) had osteopaenia. If the BSG Guidelines were to be strictly adhered to, 50% of patients with osteoporosis or osteopenia would have been missed. This small study would suggest that performing DEXA scans on all newly diagnosed coeliacs is probably worthwhile.
395 IS THERE CLINICAL RELEVANCE IN TESTING PATIENTS WITH ADULT COELIAC DISEASE FOR THYROID DYSFUNCTION?
J. S. Leeds, R. C. Bunn, D. S. Sanders.Royal Hallamshire Hospital, Sheffield, UK
Introduction: An association between coeliac disease and autoimmune thyroid disease is well described. Thyroid disease is usually identified first. It has been shown that unidentified coeliac disease may lead to poor control of both hypo- and hyper-thyroidism. There are conflicting results with respect to the role of a gluten free diet (GFD) and the reversibility of biochemical thyroid dysfunction.
Aims: To assess the clinical value of routine testing for thyroid disease in patients with adult coeliac disease.
Patients and Methods: Patients were recruited from the specialist coeliac clinic when attending for their annual review. In addition to demographic details information was collected on duration of coeliac disease and compliance to the GFD. All patients had their thyroid function checked (Free T4 and TSH initially). Patients are specifically questioned about tiredness and weight loss (weight is also measured).
Results: 207 patients were included in the study. 36 patients (17.4%) had known thyroid disease (23 with hypothyroidism and 13 with hyperthyroidism). Over the period of study (Nov 2003–Oct 2004) 13 patients (6.3%) were found to have newly identified biochemical thyroid abnormalities. Four of the 13 were new patients of whom three had a raised TSH with normal free T4 and one patient had a low TSH with a normal free T4. Six of nine follow up patients developed new biochemical thyroid abnormalities; four had a raised TSH with low normal T4 and two had low TSH with normal T4. In three follow up patients there was a change in management as a result of checking the thyroid function. One patient had T3 toxicosis (complained of weight loss) and the other two patients had new hypothyroidism (complained of tiredness). Two percent (3/147) of follow up patients with coeliac disease had clinically relevant thyroid dysfunction.
Conclusions: Concurrent thyroid disease is highly prevalent in adult coeliac disease (24.2%). We identified 2% who had clinically unrecognised thyroid disease despite a GFD. However, these individuals were all symptomatic. Directed questioning with specific testing may help identify patients early with thyroid disease allowing treatment or referral to an endocrinologist if relevant.
396 THE DIAGNOSTIC ACCURACY OF CAPSULE ENDOSCOPY IN COELIAC DISEASE: A BLINDED PILOT STUDY
A. D. Hopper, D. S. Sanders, M. E. McAlindon.Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Macroscopic changes in the duodenum due to villous atrophy can be seen at oesophagogastroduodenoscopy (OGD). Endoscopic signs of coeliac disease have a reported specificity from 87–100%. OGD and duodenal biopsy (D2Bx) remains the gold standard but some patients will refuse to have this invasive procedure.
Aim: A blinded pilot study to assess the use of capsule endoscopy in recognising small bowel features of coeliac disease.
Methods: 20 consecutive patients prospectively referred for capsule endoscopy from Dec 2003 to June 2004. All referrals were for iron deficiency anaemia of unknown cause or diarrhoea. All patients had routine OGD and D2Bx. A capsule endoscopy was performed with visualisation of the small bowel. The data from every capsule endoscopy was reported by a single investigator who was blind to the result of the D2Bx.
Results: Of the 20 patients recruited 14 were found to have normal D2Bx. This group was subsequently categorised as controls. The other six patients had biopsy proven coeliac disease. The demographics of the two groups were comparable: controls (n = 14, age 28–73, 8 female) and coeliac disease (n = 6, age 36–80, 3 female). The villi were reported as abnormal in 5/6 patients with coeliac disease and abnormal in 0/14 control patients. The validity of capsule endoscopy for diagnosing coeliac disease is shown in the table. The five patients that had abnormal villi reported at capsule endoscopy also had duodenal macroscopic changes reported at their OGD. The patient with coeliac disease that had normal villi noted at capsule endoscopy had a normal duodenum reported at OGD. The duodenal biopsies of this patient were consistent with marsh criteria 3b (SVA).
Abstract 396
Conclusion: The capsule endoscopy has a similar specificity to endoscopic signs of coeliac disease. However, the capsule endoscopy is not invasive and may be an acceptable investigation in patients with positive antibodies who refuse OGD. Larger sample sizes are required to validate our initial observations.
397 IS ROUTINE DUODENAL BIOPSY ESSENTIAL TO STOP COELIAC DISEASE BEING MISSED AT CASTROSCOPY?
A. D. Hopper, J. S. Leeds, A. Lewis, D. P. Hurlstone, M. E. McAlindon, D. S. Sanders.Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Introduction: Duodenal biopsy (D2Bx) is recommended in patients with anaemia. However, coeliac disease may present with many other subtle gastrointestinal symptoms that are also indications for OGD. We recently described that 13.6% of our patients with newly diagnosed coeliac disease had a previous OGD (prior to their diagnosis of coeliac disease) but did not have a D2Bx.
Aims and Methods: We assessed whether routine D2Bx increased the rate of diagnosis of coeliac disease. An audit was carried out examining total number of OGD and D2Bx per year from July 1999 to July 2004 using case note review and Endoscribe database. Rates of D2Bx overall (table 1) and in the specific indication of anaemia were noted (table 2). Table 2 also shows sub-division by specialty of the endoscopist. Patients in the anaemia group were excluded if they had a previous D2bx, evidence of carcinoma or on anticoagulation. D2Bx evidence of new coeliac disease cases was cross referenced with the histopathology database.
Abstract 397, table 1: D2Bx with new coeliac disease
Abstract 397, table 2: D2Bx in anaemia
Results: See tables.
There was a significant increase in the rate of D2Bx from 16.7 to 26% over 5 years (χ2 p<0.001). There was a strong relationship between the rate of D2Bx and diagnosis of new cases of coeliac disease (r = 0.894; p<0.05). Nurse endoscopists have the highest rate of D2Bx in anaemia.
Conclusion: Increased rates of D2Bx at OGD lead to an increased diagnosis of coeliac disease. However, overall rates of D2Bx are still low even when D2Bx is recommended. There may be a case for routine D2Bx.
398 PERCUTANEOUS ANGIOPLASTY AND STENT PLACEMENT IN CHRONIC MESENTERIC ISCHAEMIA
A. Akbar, J. E. Jackson, J. Walters, R. J. Playford, S. Ghosh.Hammersmith Hospital, London, UK
Background and Aim: Chronic mesenteric ischaemia (CMI) is generally treated by surgical revascularisation, but percutaneous angioplasty and stenting is emerging as an alternative. Angioplasty alone may be associated with a significant re-stenosis rate. We report the long term results of percutaneous transluminal angioplasty (PTA) and stent placement in CMI.
Methods: Retrospective data collection for 5 years (1999–2004) to identify patients with significant CMI who had been treated by coeliac and/or superior mesenteric artery (SMA) and/or inferior mesenteric artery (IMA) stenting by a single expert operator (JEJ). Technical success, defined as a post intervention stenosis of less than or equal to 30%, and post procedure complications resulting in delayed stay of more than 48 h, were noted. Follow up data collected included mortality, recurrent stenosis, and recurrent symptoms.
Results: Eight patients (7F, 1M) aged 44–78 years (mean 62 years) were identified. Patients presented with chronic abdominal pain (n = 6), weight loss (n = 4), and acute intestinal ischaemia (n = 2). Aetiology was arteriopathy in 7, and diaphragm median arcuate ligament (MAL) compression in 1 patient. Number of major vessels involved ranged from 2 (n = 2) to 3 (n = 6). Technical success was obtained in all 8 with 7 coeliac and 1 IMA stents inserted following angioplasty. No post procedure complications occurred. Follow up ranged 10–75 months (median 35 months). Significant late stenoses occurred in 4 patients. Of these, 1 patient with continued compression by the MAL had a 3 months. post stent laparotomy; repeat angiogram at 66 months. post stent showed wide stent patency. The second patient had ongoing symptoms after the initial coeliac stent and 1 months. later had IMA stent insertion. At 32 months. she remains well; follow up angiogram at 24 months. revealed a patent stent. The third patient with recurrence at 19 months. required a SMA stent insertion (initial coeliac stent); she is asymptomatic at 21 months. The fourth patient with recurrence at 66 months. received a second coeliac stent. There was no mortality.
Conclusion: Our experience confirms high technical success with no mortality or post-procedure complications. Further stent insertion was required for recurrent symptoms in 3/8 patients. In CMI patients who are often elderly with significant cardiovascular morbidity, angioplasty followed by mesenteric stenting offers a minimally invasive alternative to surgery.
399 SMALL BOWEL IRON ABSORPTION IS INHIBITED BY TNF-α
N. Sharma1, M. Brookes1, B. T. Cooper2, T. H. Iqbal2, C. Tselepis1.1Division of Medical Sciences, University of Birmingham UK, 2City Hospital, Birmingham, UK
Background: Chronic inflammation effects iron metabolism causing anaemia. Iron is initially taken into duodenal and jejunal enterocytes by the apical metal transporter DMT1. It is then either stored by ferrtin or exported out of the cell by the basal iron transporter IREG1. In this study we demonstrate a modulation of iron absorption by TNF-α and describe the molecular mechanisms underlying this.
Methods: Caco-2 cells in transwell plates were stimulated with TNF-α (5 ng/ml) for up to 24 h. Iron transport across the cell monolayer was determined by the use of 55Fe scintillation. Utilising a Caco-2 cell line model and human ex vivo small bowel (EVSB) culture system, changes in the mRNA and protein expression of DMT1, IREG1, and ferritin were measured by means of real time PCR and western blotting, respectively. Changes in localisation of all three proteins were demonstrated by immunflouresence and immunohistochemistry. EVSB iron uptake in response to TNF-α was determined by Perls stain.
Results: TNF-α treated Caco-2 cells showed an initial significant increase in both iron uptake and export. However, by 24 h both parameters were significantly repressed. This was consistent with expression data showing an initial increase in DMT1 and IREG1 followed by a fall to baseline levels by 24 h in Caco-2 cells and 6 h in EVSB. In addition there was a late and sustained increase in ferritin expression in both models. TNF-α treatment of Caco-2 cells and EVSB caused a relocalisation of IREG1 away from the basolateral membrane with little effect on DMT1 and ferritin. Enterocytes in EVSB became significantly iron loaded with TNF-α.
Conclusions: Ultimately TNF-α appears to cause a block on iron absorption and iron trapping within the enterocyte. This occurs by consistent changes in the expression of DMT-1, IREG1, and ferritin coupled with the relocalisation of IREG1. This study highlights a mechanism whereby TNF-α can inhibit iron absorption and so contribute to the anaemia of chronic inflammation.
400 THE NATURAL HISTORY OF BILE ACID MALABSORPTION (BAM)
P. Basumani, M. Smith, B. Dawson, B. Mason, C. Royston, P. J. Willemse, K. D. Bardhan.District General Hospital, Rotherham, UK
Introduction and Aim: The SeHCAT retention test has simplified diagnosing diarrhoea due to BAM (retention <10%). We assessed the long term outcome of BAM, of which little is known.
Methods: Changes in BAM in patients with diarrhoea predominant IBS (D-IBS) and structural disease were compared, based on those in whom the SeHCAT test was repeated. Most with troublesome diarrhoea and BAM were treated with the bile acid sequestrants (BAS) colestipol (or cholestyramine) and their response to treatment assessed.
Results: 89 patients had paired SeHCAT tests (mean: interval 4 years; total follow up 8 years), comprising: D-IBS n = 35, ileal Crohn’s disease 17; coeliac disease + ileal resection 10; cholecystectomy 12; mixed surgery (⩾ 2 of cholecystectomy, gastric surgery, ileal coeliac disease) 6; and miscellaneous 9. SeHCAT when initially abnormal remained so in most. In D-IBS, SeHCAT increased to ⩾10% (that is, normal) in one quarter of patients, mainly to levels of 11–20%. In contrast it remained abnormal in all with structural disease. Response to treatment: 56 were treated with BAS. Nine could not tolerate treatment. Treatment was fully effective (return to normal) in 20, partially so in 22 but ineffective in five. The clinical response did not correlate with either the cause of BAM or with initial or subsequent SeHCAT retention values.
Discussion and Conclusions: Abnormal SeHCAT retention remains unchanged in the majority, particularly in those with structural disease. Treatment with colestipol (or cholestyramine) results in improvement or resolution of symptoms in 80%. The clinical response does not correlate with either the cause of BAM or with the initial or subsequent SeHCAT retention.
Abstract 400
401 HIGH PREVALENCE OF ABNORMAL DUODENAL HISTOLOGY IN ASYMPTOMATIC COELIAC PATIENTS
D. H. Dewar, J. S. Fraser, M. W. Johnson, P. J. Ciclitira.Department of Gastroenterology, The Rayne Institute, St Thomas’ Hospital, London, UK
Background: Histological recovery in coeliac disease has been shown to be delayed or incomplete after treatment with a gluten free diet (GFD). Performing routine duodenal biopsy is not indicated in follow up of patients with coeliac disease, in the absence of persisting symptoms or other clinical manifestations.
Methods: We performed repeat duodenal biopsy in asymptomatic coeliac patients in addition to their routine follow up. Only those on a GFD for longer than 1 year and with no symptoms were included. Patient demographics and the duration of GFD diet were noted. Anti-endomysium IgA antibodies (AEA) were also measured in each patient. The biopsies were examined and categorised as to whether they displayed normal histology, intra-epithelial lymphocytosis (>30 per 100 enterocytes), or villous atrophy. All individuals were under active follow up in our centre and indicated that they were complying with a GFD.
Results: We performed duodenal biopsy in 90 asymptomatic adults with coeliac disease, age range 18–82 (mean 50.1 years), 69% were female. The average duration of GFD was 4.1 years (1–32 years). Thirty six biopsies (40%) were normal and 54 (60%) were abnormal. Seventeen biopsies (18.9%) showed an isolated increase in intra-epithelial lymphocyte count. The remaining 37 biopsies (41%) displayed villous atrophy, which was severe or subtotal in 12 cases (13.3%). Six patients (6.7%) were positive for AEA, and all six had significant villous atrophy. All patients with normal biopsies or an isolated lymphocytosis were negative for AEA. However, 31/37 patients (83.8%) with villous atrophy were also negative for AEA.
Conclusions: Poor compliance is often blamed for persisting symptoms and abnormal duodenal histology in coeliac disease. It is not common practice to biopsy asymptomatic patients. In our study 60% of apparently healthy patients with coeliac disease have abnormal small bowel histology, with 41% displaying degrees of villous atrophy. The implication of this finding is unclear although it may suggest predisposition to disease complications.
402 LONG TERM FOLLOW UP OF COELIAC DISEASE: A PATIENT QUESTIONNAIRE STUDY
J. R. Bebb1, A. Lawson1, K. Blount2, J. Lewis2, T. Knight3, W. P. Goddard1, K. Teahon1, R. G. Long1.1Department of Gastroenterology; 2Department of Dietetics and Nutrition; 3Governance Team; Nottingham City Hospital, Hucknall Road, Nottingham NG5 1PB, UK
Introduction: Coeliac disease may affect up to 1% of the population and the BSG recommends long term follow up of these patients, although the absolute risk of complications such as malignancy and osteoporotic fracture is probably small.
Aim: To determine what proportion of patients with diagnosed coeliac disease remain under specialist follow up and to examine patients’ perspectives on the long term management of coeliac disease.
Methods: Patients who had a duodenal biopsy between July 1994 and July 2004 consistent with coeliac disease were identified from the histopathology database of a single teaching hospital. A questionnaire was sent to 183 patients whose medical records confirmed a clinical diagnosis of coeliac disease.
Results: 103 (56%) patients with a mean age of 55 (17–92) returned their questionnaire. Patients had on average been diagnosed with coeliac disease 4.5 years earlier. 88% were trying to follow a strict gluten free diet. 60% of patients were under some kind of follow up although this varied between hospital doctor/dietitian (77%) and GP (23%). 40% of respondents were under no active follow up. Of those attending a hospital outpatient clinic 69% found it useful or very useful. When asked for preferred method of coeliac disease follow up the most popular option was to see a dietician with a doctor being available if required. No follow up was the least preferred option.
Conclusion: Respondents to this study showed great variation in follow up of their coeliac disease—40% were under no active follow up. Most attenders to hospital outpatients found this useful. Most patients would prefer to see a dietitian rather than a doctor, the reasons for this may be more than for dietary advice alone. This may have implications for the way in which services for coeliac disease patients are planned.
Service development posters
403 IMPACT OF A MULTIDISCIPLINARY IBD CLINIC IN A DISTRICT GENERAL HOSPITAL
S. Maitra, J. Vasani, B. K. Chaudhury, M. Kurmani, A. Lee, K. D. Bhattacharya, C. Berthou, A. Agarwal.University Hospital Hartlepool; Holdforth Road, TS24 9AH, UK
Introduction: The BSG emphasises the role of multidisciplinary approach in the treatment of IBD.1A monthly IBD clinic, ran jointly by a colorectal surgeon, a gastroenterologist, and a IBD support nurse, was therefore set up to integrate the management of a definite group of IBD patients, identified to have a complicated course of the disease.
Materials and Methods: The correspondence letters for all the patients attending the clinic over a 18 months period were reviewed according to a standard proforma.
Results: 53 patients (24 male; 29 female) attended the clinic. All of them were seen within a month’s time from referral. 19 (35.8%) had ulcerative colitis and 34 (64%) had Crohn’s disease. Major causes of referral for ulcerative colitis were recurrent flare ups (7 (36.8%)); dysplasia (2 (10.5%)), and one was a non responder; for coeliac disease 10 (29.4%) had symptomatic stricture and 9 (26%) had perianal/fistulising disease, respectively. Surgery was advised for 17 (32%); 12 (22%) of them in the first visit; 3 refused, 8 (15%) had proctocolectomies, 2 (3.7%) each had ileal resection and hemicolectomy, and 1 (1.8%) each had balloon dilatation and stricturoplasty. Infliximab was given to 4 (11.7%) with severe coeliac disease and all but one had sustained response. All patients were counselled by the IBD nurse. Other important inputs included smoking ceasation advice to all coeliac disease patients and surveillance decision for patients with longstanding ulcerative colitis.
Conclusion: The combined input from the gastroenterologist, the surgeon, and the IBD support nurse in a joint clinic proves to be useful in integrating the decision making in a select group of complicated IBD patients and hastening the whole treatment process by saving time taken up in exchange of correspondence.
1
404 THE PATIENT’S EXPERIENCE OF CENTRALISATION OF CANCER CARE AND THE ROLE OF THE SPECIALIST NURSE: RESULTS OF A PRELIMINARY SURVEY
C. Lock, A. H. Gibbons, I. Dunkley, P. J. Roberts, R. J. Dickinson.Hinchingbrooke Hospital, Huntingdon PE 29 6NT, UK
Background: The West Anglia Cancer Network was established in February 2000 and covers a population of 1.6 million. Patients with upper gastrointestinal (GI) cancers are managed by a multidisciplinary team with patient care being shared between the units and the centre in Cambridge. Most patients will have to travel from home to both the unit and the centre, meeting many different personnel. This process needs to be seamless; to facilitate this we appointed a nurse specialist.
Aim: To gain insight into the patients’ experience of the referral pathway and to evaluate the role of the nurse specialist.
Methods: A postal questionnaire was sent to suitable consecutive patients seen between December 2002 and December 2003.
Results: 52 patients were diagnosed with upper GI cancer and of these 33 were sent a questionnaire. The results can be summarised as follows. The process: Patients perceived that improvement was needed between initial referral to the unit (35%) and in the time between diagnosis and treatment at the centre (25%). Information given: 55% were satisfied with the information given and the majority (68%) regarded the specialist nurse as the prime source of further information and advice. Travel arrangements: Of the patients needing to travel to the centre for further treatment 30% experienced travel difficulties and 15% found the journey distressing.
Conclusion: The study highlighted the parts of the patient pathway that needed attention. Despite difficulties regarding travel to the centre most patients were satisfied with the care they received. The patients greatly appreciated the co-ordinating role of the upper GI specialist nurse and saw her as the primary source of information.
405 GUIDED PRIMARY CARE MANAGEMENT OF IBD
B. H. Hayee, S. Basavarajaiah, A. W. Harris.Kent & Sussex Hospital, Tunbridge Wells, Kent TN4 8AT, UK
Introduction: Stable patients with IBD are usually reviewed regularly in secondary care,1 often duplicating activity from primary care,2 using an estimated 15 million outpatient appointments (OPAs) in the UK each year.3 An alternative approach, guided primary care management (GPCM), uses a combination of detailed clinic letters (copied to patient and GP), telephone advice, and patient self-referral to clinic. Outpatient appointments are then made available for new referrals, and relapsing patients can be seen quickly—in line with current guidelines.4 GPCM has been used in the Kent & Sussex Hospital since 1997 (and has been validated with retrospective data5).
Methods: A prospective study was undertaken to follow stable IBD patients for a 6 month period, as they were discharged from clinic. All events relating to IBD were then recorded, including GP visits, phone advice, outpatient appointments attendances, hospital admissions, and blood results.
Results: 57 patients were in GPCM for a minimum of 6 months (range 6–9 months, mean 7.4), 25 with Crohn’s disease and 32 with ulcerative colitis. Three were discharged to the intramuscular methotrexate clinic. Of 12 patients discharged on 6-mercaptopurine, 11 had blood tests at the correct interval with one event of leucopenia detected. GPCM was attempted in six of nine disease relapses, with three responding to suggested management. Eight outpatient appointments were generated. There were no cases of serious drug side effects, emergency admissions, unplanned surgery, or deaths.
Conclusions: GCPM for IBD in this population appears safe and reduces outpatient follow up. Eight outpatient appointments were requested either by GPs or patients—compared with an expected 57 (one per patient in a 6 month period), leading to a net gain of 49 appointments in a 6 month period.
1
2
3
4
5
406 IMPACT OF THE EUROPEAN WORKING TIME DIRECTIVE ON SPECIALIST TRAINING AND EXPERIENCE
B. H. Hayee, A. W. Harris.Kent & Sussex Hospital, Tunbridge Wells, UK
Introduction: The European Working Time Directive (EWTD) on junior doctors’ working hours has been in place since 1 August 2004, limiting working hours to 58 hours per week, with entitlements to daily and weekly rest breaks.1 There are currently a total of eight specialist registrars (SpRs) participating in a compliant rota at the Kent & Sussex Hospital. Statements from the Royal College of Physicians (RCP) demonstrate that a cell of at least eight SpRs will minimise the impact on specialist training,2 with a total of 35 h/week available for continuity, clinics, or procedures. However, SpR trainees have fixed training sessions that may coincide with on-call commitments or mandatory rest breaks. For this reason, it is postulated that time spent in specialist training may be significantly reduced.
Aims and Methods: To determine the impact of the EWTD on actual time spent in specialist training in fixed sessions by comparing the (non-compliant) rota prior to 1 August 2004 with the compliant rota afterward, over an 8 week period.
Results: In an 8 week period prior to 1 August 2004, all speciality sessions were attended, regardless of on-call commitments. The EWTD compliant rota from 1 August 2004 led to the loss of eight endoscopy sessions, two specialist clinics, and three consultant wardrounds.
Discussion: Extrapolated to 1 year, the EWTD changes would result in the loss of approximately 25 of a maximum of 120 elective and emergency endoscopy sessions and 10 of 100 outpatient clinics. This estimate does not take into account consultant leave and SpR annual or study leave as these values are presumed to be similar for periods before and after 1 August.
Conclusion: This study demonstrates that, excluding consultant and SpR annual or study leave, the new EWTD compliant rota will result in the loss of approximately 20% of endoscopy sessions and 10% of outpatient clinics over one year at the Kent & Sussex Hospital.
1
2
407 GASTROENTEROLOGY OUTREACH: A NOVEL WAY OF DELIVERING GASTROENTEROLOGY SERVICES
S. A. Weaver, M. Hattersley, W. Cato-Addison, H. Vargas, D. Sivapathasuntharam, D. R. Fine.Department of Gastroenterology, Southampton General Hospital, Tremona Road, Southampton SO16 6YD, UK
Introduction: One aim of a gastroenterology service is to provide high quality specialist advice and management throughout an acute general hospital. Providing this service is challenging in the face of ward based care, reduction of junior doctors hours, shift systems, and the demands of the acute medical take. In Southampton teaching hospitals a novel gastroenterology outreach service has been developed to deliver acute specialist gastroenterology services throughout the hospital.
Method: A consultant led team of specialist registrar, senior house officer, and house officer is now assigned as the gastroenterology outreach team. They are responsible for managing all gastroenterology patients not on a gastroenterology ward, taking all requests for specialist advice and taking over patient care if appropriate, as well as reviewing all patients with upper gastrointestinal haemorrhage not on a gastroenterology ward. Consultants and juniors rotate through the service.
Results: In setting up this novel outreach service we assessed the nature of our workload and the satisfaction of those referring patients. There was a consistent pattern of diagnoses as typified by 133 consecutive referrals in a two month period: 48 (36%) GI haemorrhage, 14 (11%) IBD, 13 (10%) dysphagia, 12 (9%) obstructive jaundice, 12 (9%) diarrhoea of which two thirds were recurrent Clostridium difficile related, and 7 (5%) GI maligancy. Questionnaires to assess the service were sent to 69 consultants and 39 replied (57%). 24/39 were aware and 22/39 had used the service. 19/22 (86%) felt that the patient had benefited and received better care. All 22 would use the service again.
Conclusion: A novel outreach method of providing gastroenterology services to a teaching hospital is possible and provides better care for patients.
408 AUDIT OF OUTCOME OF OUTPATIENT REFERRALS OF ASYMPTOMATIC PATIENTS WITH MILDLY ABNORMAL ALANINE AMINOTRANSFERASE LEVELS
K. Damodharan, G. I. Leontiadis, A. Saeed, S. Kadis (introduced by Louizou LA).Department of Gastroenterology, Queen Elizabeth Hospital, Gateshead, UK
Background: Although there are guidelines for the management of patients with grossly abnormal liver function tests (LFTs), there are no clear ones for managing patients with mildly abnormal tests.
Aim: To analyse the outcomes of asymptomatic patients referred with mildly abnormal ALT levels, by GPs, and also to determine if such patients need a specialist referral.
Methods: Retrospective review of case notes and laboratory results of all patients who were referred by GPs to the gastroenterology outpatient clinic of a district general hospital in UK, with raised alanine aminotransferase (ALT) levels less than twice the upper normal limit, between August 2001 and August 2002. LFTs of these patients were monitored for a follow up period of 1–2 years.
Results: 82 patients were referred with the above criteria during this period and investigated. A definite cause was identified in 52 patients (63.41%): alcoholic liver disease in 18 patients, non-alcoholic fatty liver disease in 28 patients, primary biliary cirrhosis in one patient, partial alpha 1 antitrypsin deficiency in one, drug induced in two, cholelithiasis in one, and liver metastases in one. No cause was identified in 30 patients. Overall two patients (2.4%) had pathology requiring intervention; one with liver metastases and one with primary biliary cirrhosis. The rest of the patients who were followed up by the hospital or GP had either spontaneous resolution (in 13 patients) or persistently mildly abnormal ALT levels.
Conclusion: Investigation and follow up of asymptomatic patients with mildly abnormal ALT levels alone has a very low yield of significant pathology. This suggests that these patients might be investigated by a non-invasive liver screen and followed up at primary care level and referred to a specialist for management, only if pathology is identified with the initial liver screen or the ALT rises above twice the upper normal limit during follow up.
409 IMPACT OF A SPECIALIST CLINIC IN THE MANAGEMENT OF PATIENTS WITH BARRETT’S OESOPHAGUS
G. K. Anagnostopoulos, B. Pick, K. Ragunath.Wolfson Digestive Disease Centre, University Hospital Nottingham, UK
Background and Aim: Barrett’s oesophagus is a common premalignant condition in the Western world. A high number of patients were undergoing surveillance endoscopy in our unit without adequate assessment in an unstructured approach. In order to streamline this process, a specialist Barrett’s clinic was set up with a specialist nurse, registrar, and consultant. Our aim was to assess the impact of a specialist clinic on the management of this chronic condition.
Methods: Barrett’s oesophagus diagnosis and surveillance guideline was introduced modelling the American College of Gastroenterology Guidelines. Data were collected prospectively, August 03 to September 04. All patients attending Barrett’s surveillance endoscopy and all newly diagnosed patients were seen in the specialist clinic. After confirming the diagnosis based on endoscopy and histology report, patients were assessed based on their comorbidity and willingness to undergo surveillance. Reflux symptom control and acid suppression was addressed. Verbal and written information was given before a fully informed management plan was agreed. A repeat endoscopy with zoom endoscope and dye spray with targeted biopsy was done when there was disparity between endoscopic and histological diagnosis or if there was a clinical need.
Results: 143 patients (51 women) aged 26–88 (median 62) were examined. This resulted in reducing the endoscopy waiting list and converting a gastroscopy list to a much needed colonoscopy list. In 16 patients surveillance was stopped (13, comorbidity, 3 no evidence of Barrett’s). In 25 patients treatment was altered to relieve reflux symptoms. Forty eight patients (34%) underwent repeat endoscopy, 8 (17%) had a histological upgrade, 4 changed from columnar lined oesophagus (CLO) to CLO with intestinal metaplasia (IM), 1 from CLO to LGD, 1 from IM to LGD, 1 from IM to HGD, and 1 from intestinal metaplasia to cancer.
Conclusion: A specialist Barrett’s clinic can provide a systematic individualised approach to patients with this chronic condition and may prove cost effective to the health service.
410 COLONOSCOPY AND ANAEMIA: AUDIT OF APPROPRIATENESS OF COLONOSCOPY FOR A SINGLE INDICATION
M. Rashid, S. Thomas, D. Morris, S. Greenfield, P. McIntyre, M. Wright.Department of Gastroenterology, QE2 Hospital, Welwyn Garden City, Herts, UK
Introduction: All endoscopies should be performed for appropriate indications. If iron deficiency anaemia (IDA) is the indication for colonoscopy then there should be evidence of this. The aim of this audit was to establish how many patients undergoing colonoscopy actually had IDA.
Methods: All colonoscopies performed with anaemia as an indication during 6 months from 1 September 2003 to 28 February 2004 were identified by endoscopy computer database search. Patient notes and pathology database records were then searched for evidence of a recent full blood count and or ferritin prior to the colonoscopy.
Results: 78 colonoscopies were performed. 13 patients had additional indications for colonoscopy and six patients did not have any blood results available and were excluded from the audit. Of the remaining 59 patients only 45 had either microcytic anaemia or/and a low ferritin.
Conclusions: If anaemia was the sole indication for colonoscopy, 23.7% of procedures done were inappropriate. This has implications for risks to patients as well as resource use. As a result of this audit we have introduced a vetting system including a requirement to give details of red cell and iron indices on the request card.
411 THE EFFECT OF KENT AND MEDWAY DYSPEPSIA GUIDELINES ON THE DEMAND FOR OPEN ACCESS ENDOSCOPY
S. D. McLaughlin, A. W. Harris.Kent & Sussex Hospital, Tunbridge Wells, Kent, UK
Background: More than 1000 OGDs are performed on open access endoscopy (OAE) lists/year in our unit. Most are normal. The NICE guidelines1 aim to reduce this by under a third. Similar guidance for patients with dyspepsia were prepared and distributed to all GPs in Kent and Medway in March 2004.
Aim: To determine the impact that the guidelines have made on the demand for OAE.
Methods: Demand data were collected from the trust IT department on the number of requests for OAE from local GPs between: 1/4–30/9/03 and 1/4–30/9/04. Data were assessed by χ2, where p <0.05 is significant.
Results: See fig 1 and table 1.
Abstract 411

{kind=link}
{kind=link}
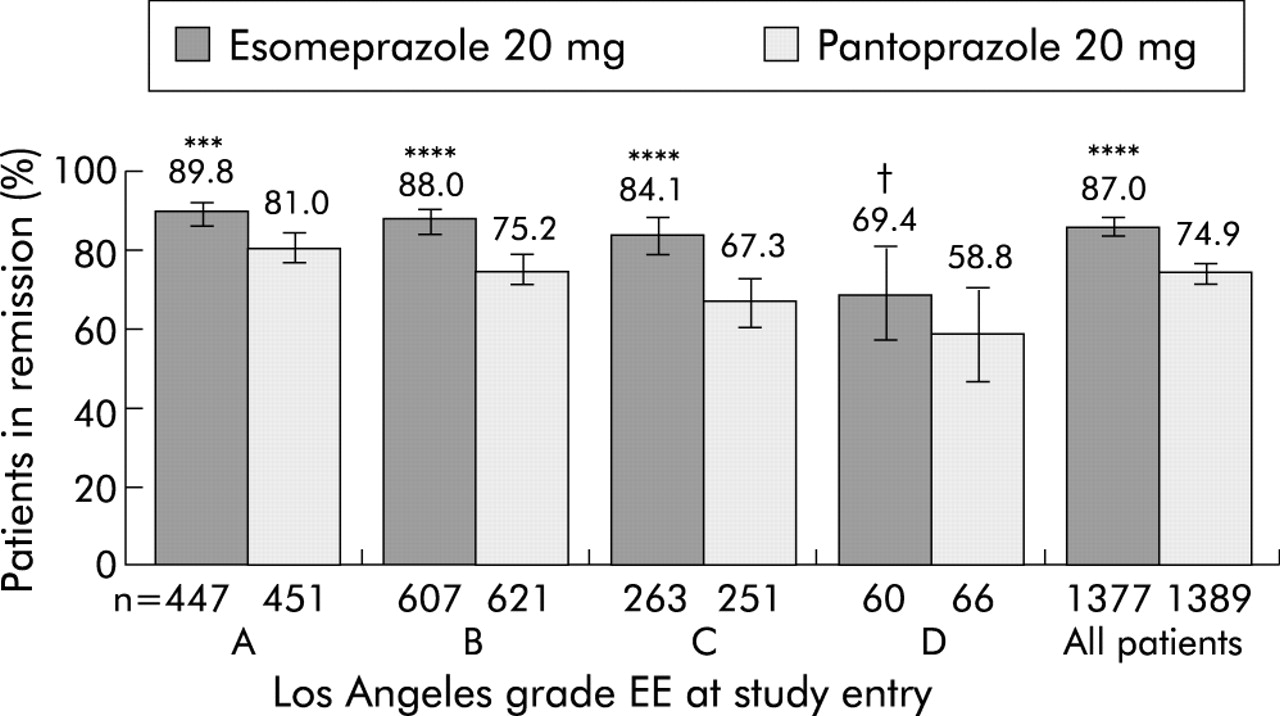{kind=link}
{kind=link}
{kind=link}
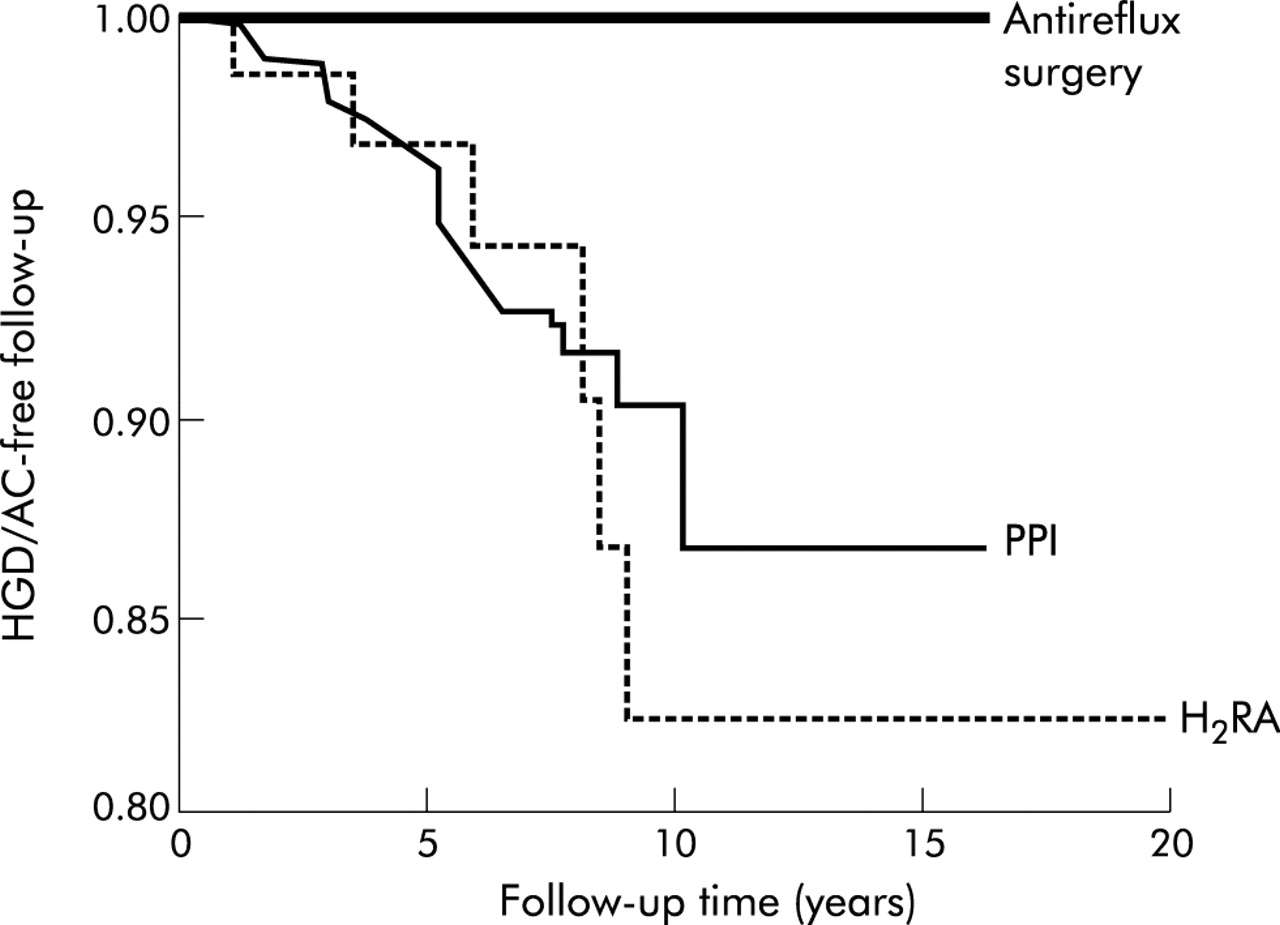{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract 411, figure 1.
Conclusion: Distribution of Kent and Medway dyspepsia guidelines has had a significant impact on the endoscopy service leading to a 17% decrease in demand for OAE. We expect a further decrease in demand following launch of national guidance from NICE.
1
412 USE OF INFLIXIMAB IN CROHN’S DISEASE: A DISTRICT GENERAL HOSPITAL AUDIT
R. Goel, D. Milligan, C. B. Summerton.Department of Gastroenterology, Trafford General Hospital, Moorside Road, Davyhulme, Manchester M41 5SL, UK
In April 2002, NICE issued guidance on the use of infliximab in Crohn’s disease. However, since then clinical practice has been shaped by the publication of the ACCENT I and ACCENT II trials. In the light of the changing practice, we decided to audit the use of infliximab in a UK district general hospital setting, to see if patients were still being treated in accordance with NICE guidance.
Objectives: To identify all patients with Crohn’s disease who were started on treatment with infliximab between June 2002 and March 2004 in Trafford General Hospital. To audit the decision to start and maintain treatment against the criteria published in NICE guidance.
Methods: Retrospective analysis of patient case notes, using an objective audit questionnaire.
Results: 18 individuals received infliximab for Crohn’s disease during this period. In 69% of these patients, infliximab was started in accordance with NICE guidance. 31% of patients did not fit the strict criteria of the NICE guidance, largely because there was no record in the case notes that surgery had been considered as a treatment option. However, patients in both groups showed considerable clinical benefit. 83% of patients received maintenance therapy, of who 40% were on 12 weekly maintenance, 53.3% on 8 weekly, and 6.6% on more frequently than 8 weekly. NICE guidance would suggest that maintenance therapy should only be given if there is evidence of relapse after initial therapy. However, we found from our audit that the decision to give maintenance therapy was usually made at the same time as the decision to initiate therapy, reflecting the influence of the ACCENT trials.
Conclusion: Our audit highlights that a number of patients are now receiving maintenance therapy outside of the scope of the NICE guidance published in 2002. This guidance is due to be reviewed in May 2005. However, this 3 year delay is arguably too long, when there have been significant changes in evidence engendered by new trials. It is confusing for commissioners when expensive new treatments are being administered outside of national guidelines. We would welcome a rapid response facility from NICE for situations such as this.
413 INVESTIGATION OF PATIENTS WITH UNINTENTIONAL ABNORMAL WEIGHT LOSS PRESENTING TO GASTROENTEROLOY SERVICES
A. H. Shenoy, P. D. Thomas.Taunton and Somerset Hospital, Taunton, UK
Introduction: Weight loss is a criterion for referral to secondary care under 2 week cancer rule in the UK. The underlying pathology, yield of investigations, and outcome in this patient cohort is poorly understood.
Aims: To determine the optimum investigation strategy for unintentional abnormal weight loss.
Methods: Retrospective audit. 159 patients referred to GI services with weight loss (+ other symptoms) between June 2001 and July 2003 who were investigated and followed for at least 1 year from the date of referral to case note review. Those with a pathological cause of weight loss (group 1) were compared with those for which no pathological cause was found (group 2) to assess for factors at presentation that predicted organic disease.
Results: See table.
Abstract 413, table 1
39 patients (24.5%) had malignancies; 28 of which were GI and 11 non-GI. 15 (9.4%) had non-malignant diagnoses (GI in 7 and non-GI in 8). There was no difference in presenting symptoms (for example, dysphagia, abdominal pain, vomiting, and rectal bleeding) except diarrhoea was more common in group 2. Organic disease was found in 44% (14/32) of USS/CT, 19% (12/63) gastroscopies, 11% (12/114) lower GI investigations, and 6% (4/67) CXR. Logistic regression analysis showed that the hypoalbuminaemia alone is a good predictor of the presence of the diagnosis but it was not very sensitive.
Discussion: A third of patients referred with unintentional abnormal weight loss had organic disease (25% malignant). The chance of detecting significant disease is high in those who are older, have anaemia, abnormal LFT, or hypoalbumenaemia, the latter being the strongest predictor. Symptoms are of little value in distinguishing organic disease. Investigation should include CXR, TFT, and an upper or lower GI endoscopy or barium enema (depending on symptoms), followed by abdominal USS or CT. In younger patients (<55 years) without abnormalities in baseline blood tests, dietetic review and ‘watch and wait’ is a reasonable strategy.
414 FEASIBILITY OF NON-PHYSICIAN EUS STAGING OF OESOPHAGEAL CANCER AND ITS IMPACT ON THE WIDER EUS SERVICE
J. Meenan, C. Vu, S. Anderson, L. A. Doig.Department of Gastroenterology, Guy’s and St Thomas’ Hospital, London, UK
Background: Opportunities to acquire the breadth of training needed to meet the demands of EUS are few, hindering expansion of services. The natural division between diagnostic and therapeutic EUS raises the question of whether sub-specialisation is feasible and whether there might be a role for the non-physician endoscopist.
Aim: A prospective study to assess the potential for a non-physician endoscopist to stage oesophageal cancer with radial EUS and to determine the impact that this approach would have on the wider EUS service.
Methods: 100 patients underwent radial EUS staging of oesophageal cancer. The studies were performed by a non-physician endoscopist whom had received prior hands on training in EUS (125 cases). Cases were observed by an experienced endosonographer. Both independently reported in writing a TNM stage.
Results: The non-physician endoscopist completed the full EUS procedure in 98 cases, requiring assistance to pass tightly strictured lesions in two cases. Assessing the accuracy of T-staging over 98 cases, there was very good agreement (k = 0.834) between both observers. When the first and second 50 cases were compared, agreement rose from good (k = 0.79) to very good (k = 0.89). Agreement for N-staging was very good (k = 0.858). The introduction of a non-physician endoscopist performed service accounted for 22% of procedures performed with a parallel rise in the number of complex cases performed by physicians.
Conclusion: Extending the role of the non-physician endoscopist to include radial EUS for oesophageal cancer staging is feasible. Such an approach would allow medically trained endoscopists to focus on more complex EUS.
415 ARE DYSPEPSIA GUIDELINES BEING FOLLOWED IN PRIMARY CARE?
M. R. Aljabiri, D. Ramdass, P. Dubois, S. Mann, N vanSomeren, K. Besherdas.Chase Farm Hospital, London, UK
Background:H pylori testing in young patients with uncomplicated dyspepsia has been recommended. A test and treat strategy for dyspeptics positive for H pylori is recommended by many gastroenterology bodies including the AGA and reassurance/symptomatic treatment in those who test negative.
Aim: To assess whether dyspepsia guidelines of a test and treat strategy are implemented in primary care prior to referral to secondary care.
Methods: A prospective study of 56 consecutive patients under 55 years without alarm symptoms whom were referred to secondary care (a district general hospital) for further management of dyspepsia was performed. The patients were assessed for prior prescription of empirical therapy with acid suppression, and also for prior testing/eradication of H pylori.
Results: General practitioners checked for presence of H pylori in 30/56 patients (53.5%) prior to referral. Of these, 17 patients were offered eradication prior to referral to secondary care. Of the 26/56 patients (46.4%) not tested for H pylori, two received eradication therapy empirically prior to referral and 13 of these 26 (50%) were prescribed empirical therapy with acid suppression. 33/56 patients (57.1%) were prescribed empirical therapy with 27/32 receiving a proton pump inhibitor and 6/32 having had ranitidine. Only 11 of 56 (19.6%) patients were judged to follow the current test and treat strategy of dyspepsia management. Thirteen of 56 patients (23%) referred did not have H pylori tested nor were they prescribed empirical therapy.
Conclusions: Despite widespread dissemination of dyspepsia guidelines, only 19% of patients referred to secondary care have followed the current test and treat dyspepsia management strategy. 23% of patients referred for further management of simple dyspepsia did not follow the test and treat or empirical therapy strategy within our hospital. Implementation of dyspepsia guidelines remains poorly practiced despite widespread dissemination of these guidelines.
416 HIDDEN DEMAND: UNINVESTIGATED IRON DEFICIENCY ANAEMIA IN PRIMARY CARE
T. Syed, A. Dar, A. MacWhannel, E. T. Swarbrick, A. M. Veitch.Departments of Gastroenterology and Haematology, New Cross Hospital Wolverhampton, UK
Introduction and Aims: Iron deficiency anaemia may indicate gastrointestinal malignancy, and a fast track 2 week wait service has been available for 5 years. BSG guidelines recommend investigation with gastroscopy and colonoscopy/barium enema. We serve a population of 300 000 and undertake approximately 3200 gastroscopies and 900 colonoscopies per year. We aimed to determine the number of patients identified with iron deficiency in primary care in Wolverhampton, to assess subsequent investigation, and to estimate additional demand upon the service if full compliance was met.
Methods: Blood samples from primary care indicating iron deficiency anaemia (Hb<11.5 g/dl + MCV<80fl) in patients >50 years of age were identified for January to March 2003. These were cross referenced with endoscopy, pathology, and fast track databases to determine subsequent referral for investigation.
Results: 177 cases were identified with microcytic anaemia. Only 32 (18.1%) were referred via fast track (21 for anaemia, 11 for symptoms). The mean delay to referral was 85.6 days (range 7–260). Twenty cases underwent gastroscopy, 8 colonoscopy. One case of stomach cancer and three cases of colon cancer were identified. Subsequently three additional cases of cancer were diagnosed in patients not initially referred (one disseminated adenocarcinoma, one colon cancer, and one cholangiocarcinoma).
Conclusions: The majority of cases of iron deficiency in primary care are not being referred for investigation. A small number of cancers are therefore being diagnosed at an unnecessarily late stage. If current guidelines were applied rigorously then up to 155 additional patients per 3 months would require investigation. This equates to between 620 units of endoscopic activity (OGD+/− barium enema) to 1860 units (OGD + colonoscopy) per year, that is 62 to 186 additional lists per year (at 10 units/list).
417 THE 2 WEEK WAIT AND UPPER GASTROINTESTINAL CANCER: ON TARGET BUT MISSING THE POINT?
S. C. Ng, M. C. L. Pitcher.Department of Gastroenterology, Northwick Park Hospital, Harrow, Middlesex, UK
Objective: To assess the effectiveness in clinical practice of the Department of Health’s 2 week referral guidelines to secondary care for patients with suspected upper gastrointestinal (GI) cancer 4 years from launch.
Methods: Six months retrospective audit of case notes of all patients with upper GI cancer referred to a district general hospital serving a population of 400 000 from October 2003 to March 2004.
Results: 53 cancers were diagnosed in the 6 months audit period. 125 patients were referred for investigation via the 2 week pathway, of which eight were diagnosed with upper GI cancer (diagnostic yield 6%). 95% (119/125) of patients were seen within 2 weeks and 78% (97/125) fulfilled clinical criteria for referral. The time to cancer diagnosis was <1 week in 88%. Other final diagnoses within this group included 43% functional gut disorders, 42% benign (mainly upper GI) pathology and 2% non-upper GI cancer. 7% of patients failed to attend. At least one “alarm” symptom was present in 88% (7/8) of patients with upper GI cancer and 76% (80/105) in the non-cancer group. Of 45 upper GI cancer patients diagnosed during the audit period but not referred via the 2 week pathway, 13 (25%) were seen in traditional gastroenterological outpatient clinics and 32 (60%) presented on acute take, of which 20 (63%) were hepatopancreatobiliary cancers.
Conclusions: A disproportionate number (43%) of patients with functional gut disorders were referred via the 2 week pathway whereas the majority (85%) of patients with upper GI cancer presented via other routes. The presence of alarm symptoms was not a discriminatory predictor of upper GI cancer. More education and communication is needed for GPs to appropriately use the 2 week service and hospital clinicians should be included in reviewing referral pro formas to avoid inappropriate endoscopic investigation of patients. Twenty one patients were referred each month via the 2 week pathway for urgent review. This has implications for workload as well as a potential to delay an initial assessment of the majority of patients with upper GI cancer referred via more traditional routes to secondary care.
418 MULTIDISCIPLINARY TEAM MANAGEMENT IS ASSOCIATED WITH IMPROVED OUTCOMES AFTER SURGERY FOR GASTRIC CANCER
M. R. Stephens1, A. N. Hopper1, G. Blackshaw1, J. D. Barry1, P. Edwards1, I. Hodzovic1, G. V. Thomas1, C. Gent1, M. C. Allison2, W. G. Lewis1.1Departments of Surgery and 2Gastroenterology, Royal Gwent Hospital, Newport, UK
Aims: To compare outcomes following modified D2 R0 gastrectomy for gastric cancer patients treated by a multidisciplinary team with outcomes for patients treated prior to the inception of the multidisciplinary team.
Patients and Methods: Ninety five consecutive patients undergoing R0 gastrectomy for gastric adenocarcinoma in a single large UK cancer unit between 1 January 1996 and 31 December 2003 were studied prospectively. The outcomes for 50 control patients (34 male, median age 71 years (range 46–86)) treated prior to the introduction of the multidisciplinary team were compared with the outcomes for the 45 patients (31 male, median age 68 years (range 27–83)) treated by the multidisciplinary team.
Results: The proportion of patients referred for a surgical opinion increased from 59% prior to the introduction of the multidisciplinary team to 75% following the multidisciplinary team inception (χ2 12.383, DF 1, p<0.001). The operative mortality fell from 12% in control patients to 2.2% in MDT patients (χ2 3.317, DF 1, p 0.07). Corrected cumulative 5 year survival increased from 35% in control patients to 71% in multidisciplinary team patients (log rank 8.09, DF 1, p 0.004). Multivariate analysis using Cox’s proportion hazards model revealed the presence of lymph node metastases (hazard ratio 2.62, 95% CI 1.72 to 4.00, p<0.001), and multidisciplinary team management (hazard ratio 0.46, 95% CI 0.23 to 0.92, p<0.029) to be the most important predictors of survival.
Conclusion: These results highlight the impact of harnessing the diverse but allied talents of specialist MDT members to optimise the outcomes of surgery for patients with gastric cancer.
419 DIETICIAN LED FOLLOW UP FOR ADULT COELIAC DISEASE: IS IT SAFE?
J. S. Leeds, M. Deakin, R. Bolton, G. James, J. M. Sayer.Department of Gastroenterology, Doncaster Royal Infirmary, UK
Introduction: The most common cause of continuing symptoms in patients with coeliac disease is ingestion of gluten, whether intentional or accidental. Patients with coeliac disease are followed up in very different ways: in general gastroenterology clinics, in specific coeliac clinics, or follow up based in primary care. We developed an alternative method of follow up using a dedicated dietician to review the patients. We have audited our 2 year experience with reference to safety and patient satisfaction.
Aims: To assess the effectiveness and safety of a dietician led coeliac clinic and to assess this service from a patient’s perspective.
Patients and Methods: The dietician uses a standardised pro forma to identify new clinical problems, discusses updates in the gluten free diet, and completes a thorough assessment of compliance. The pro forma identifies unintentional weight loss or continued gastrointestinal symptoms (despite rigorous dietetic assessment). There is also assessment of dietary calcium intake and osteoporosis risk. The completed pro forma is then reviewed by the referring consultant, together with the blood results and a letter sent to the patients’ GP. Any new clinical problems are referred back to the gastroenterology clinic which runs parallel to the dietician led clinic. All patients were mailed a patient satisfaction questionnaire covering all aspects of the management of their coeliac disease.
Results: 118 patients with coeliac disease have attended the dietician led clinic. During the period of audit only three patients had been referred back from the dietician led clinic to the gastroenterologist for further assessment, one with weight loss, two with persisting diarrhoea. 66 patients (22 males) returned the patient satisfaction survey. 58 patients wishing continued follow up and 40 patients preferring dietician led follow up. Only 30 patients had been tested for osteoporosis in the past. Patients indicated that dietician appointments were more relevant.
Conclusions: Dietician led follow up of patients with coeliac disease appears to be effective, safe and the majority prefer the dietician led service as long as they could see a gastroenterologist if necessary.
420 A PROSPECTIVE AUDIT TO ESTABLISH IF INFLIXIMAB IS SAFE TO BE ADMINISTERED BY A NURSE SPECIALIST IN A DISTRICT GENERAL HOSPITAL
A. Thomson, A. Muthumala, R. Malik, D. Suri, F. R. Vicary, V. S. Wong.Department of Gastroenterology, Whittington Hospital, London N19, UK
Background: The induction and maintenance of remission in patients with Crohn’s disease using infliximab has now been well established in controlled trials. The patients participating in these multi-centre clinical trials have been recruited mainly from teaching/academic hospitals rather than district generals. The multidisciplinary team including GI physicians and surgeons at our hospital developed an agreed protocol to utilise a clinical nurse specialist to coordinate the treatment of selected coeliac disease patients with infliximab.
Aim: A prospective audit to assess the safety and feasibility of treating Crohn’s with infliximab utilising a clinical nurse specialist in a district general hospital.
Method: Patients with severe coeliac disease (CDAI>250), having failed to respond to steroids+/− azathioprine, were recruited to receive infliximab between June 2000 and June 2004. The consultant gastroenterologists assessed patients and referred those who fulfilled the treatment criteria to the CNS. All the patients underwent pre-dose counselling, routine blood tests, routine CXR, and Heaf test. If satisfactory, patients were admitted for the infusion, monitored, and discharged as a day case by the clinical nurse specialist. Patients were followed up regularly in the nurse led clinic and 24 h GI helpline using an agreed protocol.
Results: A total of 16 patients with severe coeliac disease (12 female: 4 male between ages18–56) received treatment (4 colitis, 5 anastomotic, 4 terminal ileal, 2 perianal and fistula, and 1 duodenal). There was complete response in 6 patients (37%) as shown by a reduction in the CDAI scores from 403 (SD 86) to 140 (33) (p<0.05). There was a partial response in 3 patients (19%) and no response in 7 patients (44%) who went to surgery between 1 and 8 months after the last infusion. The side effects were two infusion reactions only which resolved. However, the duodenal Crohn’s patient died of unknown cause 3 months after the last infusion.
Conclusion: Infliximab can be used safely within a district general hospital setting. The clinical nurse specialist plays an essential part in treatment from start to finish, forming the linchpin from which multidisciplinary care is delivered.
421 EFFECT OF 2 WEEK WAIT GUIDELINES ON WAITING TIMES FOR COLONOSCOPY
R. Sidhu, B. S. Höroldt, M. Fogg, M. T. Donnelly.Departments of Gastroenterology, Northern General Hospital (NGH), Sheffield, UK
Background and Aim: Since the introduction of the 2 week wait, the number of patients referred for evaluation of suspected lower gastrointestinal malignancies has steadily increased. Our aim was to assess the impact of the 2 week rule on waiting times for routine appointments and the difference it made to the yield of cancer diagnoses. We audited all patients referred for lower GI endoscopy to NGH between Jan–June 03, including patients referred via 2 week wait.
Findings: 861 patients were referred and underwent lower GI endoscopy—the average age of the patients was 61 years (median age 63 years).122 patients (64 male, 57 female) were 2 week wait referrals, their average age was 64.7 years, median age 67 years. The presenting complaints of all patients (TWW patients) were: rectal bleeding 41% (51%), change in bowel habit 35.7% (54%), abdominal pain 24% (23%), anaemia 18% (20%), weight loss 10% (18%), and abdominal mass 2% (8%). The main endoscopic findings of non-2 week wait patients (2 week wait patients) were: colorectal carcinoma (CRC) 5% (11%), polyps 26% (21%), haemorhoids 14% (15%), diverticular disease, 14% (23%), inflammation 16% (10%), and other 4% (4%). Waiting times shown in the table. Of 49 patients with cancer, 13 patients were referred on the 2 week wait (26.5%) and 36 were referred along other routes (73.5%). Only 13 patients (11%) referred via the 2 week wait proved to have a diagnosis of cancer compared with 5% referred along other routes. The commonest symptom cancer patients had was rectal bleeding; the commonest diagnosis found in 2 week wait group was diverticular disease.
Abstract 421, table 1
Conclusions: The majority of patients found to have CRC were not referred under the 2 week wait rule. Overall, time taken for lower GI endoscopy in both groups was reasonable. This ensures patients presenting with cancer via other routes do not face excessive delays.
422 ACCEPTABILITY AND USEFULNESS OF ENDOSCOPY TRAINING ASSESSMENT SHEETS
A. I. Thuraisingam, A. I. Morris.Royal Liverpool University Hospital, Prescot Steet, Liverpool L7 8XP, UK
Introduction: Assessment of endoscopy training is important; however standardised endoscopy assessment tools are lacking.
Methods: An endoscopy assessment sheet was introduced in our unit, a national training centre, to standardise assessment. The sheets aim to assess all aspects of endoscopy training, provide a record that training occurred, and help focus training on any particular areas of weakness. An anonymised questionnaire was sent to all trainers and trainees to assess the sheets. Eight trainers, including gastroenterologists, surgeons and a radiologist, and eight trainees, all gastroenterology SpRs took part. Respondents were asked to grade statements 1 to 5. 1 = strongly disagree; 2 = disagree; 3 = no opinion; 4 = agree; 5 = strongly agree.
Results: The percentage agreeing or strongly agreeing with each statement is shown. The forms are simple to complete and acceptable to use (88%); the forms are consistently used (63%); they effectively document the quantity of the procedures performed (81%); they effectively document the quality of the procedures performed (75%); they provide a reasonable overall assessment of trainees (100%); they are useful at highlighting which aspects of a trainee’s performance could be improved (81%); they are useful at highlighting which aspects of a trainer’s performance could be improved (27%); their use encourages a more complete assessment of endoscopy training (88%); they aid training in endoscopic procedures (81%); their use has directly focussed your training in/teaching of endoscopy (63%); they provide no useful information (6%); and their use should become more widespread (88%).
Discussion: Endoscopy training sheets have standardised and broadened assessment outside procedural competence alone. They are viewed positively, felt to be practical and effective at documenting procedures by the majority. Although this is a small, single site study, there was a 100% response rate and by assessing trainers and trainees both groups actually involved in endoscopy training are addressed. A standardised sheet is acceptable to both groups and appears to be an improvement on recording quantity of procedures alone. It also provides firm, documentary evidence that training and assessment has occurred.
423 DIRECT ACCESS COLONOSCOPY: A COST EFFECTIVE INVESTIGATION FOR 2 WEEK RULE COLORECTAL CANCER REFERRALS
M. Mulchandani1, K. Maruthachalam1, R. K. Jain1, E. Stoker2, A. F. Horgan1.1Department of Colorectal Surgery1 Freeman Hospital, Newcastle upon Tyne, UK; 2Department of Endoscopy, Freeman Hospital, Newcastle upon Tyne, UK
Background: In the Newcastle upon Tyne NHS Trust patients are referred under the lower GI 2 week rule for either a direct access colonoscopy or an outpatient visit at the discretion of the referring GP.
Aim: To calculate the cost of investigating a patient referred under the 2 week rule for colorectal cancer and compare the cost of direct access colonoscopy v outpatient referrals.
Methods: Retrospective study of data obtained from case notes and endoscopy records of all lower GI 2 week rule referrals in 2001 and 2002.
Results: 766 patients were referred in 2 years. 167 patients underwent direct access colonoscopy (DAC) and 599 patients were seen in outpatient clinic. Out of the 599 patients, 495 patients were investigated subsequently by colonoscopy and 17 had a barium enema. 49 patients did not need further investigations and were discharged from clinic. The average cost of a colonoscopy was £396, a single outpatient visit £128, and that of a barium enema £136. The total cost of investigating patients through DAC was £66 132 and through outpatients was £275 004.
Conclusions: DAC would have resulted in savings of £37 802 if all 766 patients had been referred through this pathway. The projected 2 week rule referrals for Newcastle in the year 2004 are 800 patients. If the referrals are appropriate, considering the above figures, DAC would result in savings of approximately £70 000. The practice of referring patients for DAC needs to be reviewed. With increasing number of 2 week rule colorectal referrals DAC will be a cost effective investigation.
424 NURSE LED INVESTIGATION OF IRON DEFICIENT ANAEMIA IMPROVES ACCESS TIMES, RELEASES CLINIC SLOTS, AND PICKS UP SIGNIFICANT PATHOLOGY
M. Shores, E. Potrykus, S. M. Kelly.Department of Gastroenterology, York Hospital, York UK
Aims: We set up a nurse led pathway for the investigation of iron deficient anaemia. The aim was to reduce access times and free up valuable outpatient slots.
Methods: Letters referring patients with iron deficiency are triaged by a consultant according to an agreed protocol. Patients seen via the nurse led pathway attend the endoscopy unit, are assessed by the nurses, and undergo further blood tests, OGD with duodenal biopsies, flexible sigmoidoscopy, and, unless initial findings dictate otherwise, subsequently a barium enema. Results are returned to the responsible consultant who decides on further follow up or discharge.
Results: In the first 12 months 91 patients have been through the service. Access times are improved and all patients are seen within 4 weeks of referral. Significant pathology (excluding oesophagitis and Barrett’s) was found in 35 patients (38.4%), with six peptic ulcers, six coeliac disease, one oesophageal cancer, one gastric cancer, six colorectal cancers, 14 with colonic polyps, and one further patient with HGD in gastric biopsies. Malignancy pick up rate was therefore 8.8%. After review of results 56 patients (61.6%) were thought not to need review in clinic and were discharged.
Conclusions: A nurse led pathway for the investigation of iron deficient anaemia improves access times. Significant pathology is picked up in a substantial number, who may benefit from the reduced access times. Most other patients can then be discharged back to their GP without further follow up so releasing valuable outpatient clinic slots for other patients.
425 UPPER GASTROINTESTINAL ENDOSCOPY PATIENT SATISFACTION SURVEY
S. Gupta, L. Grellier, K. Thompson.Department of Gastroenterology, Worthing Hospital, UK
Introduction: Patient satisfaction has become an important tool in measuring performance and planning optimal health care delivery. We conducted a postal patient satisfaction survey for patients who had oesophagogastroduodenoscopy (OGD) at our unit.
Aims and Methods: All patients having outpatient OGD during a 6 week period in 2002 were sent a postal Patient Satisfaction Questionnaire. This questionnaire included six core items of the modified Group Health Association of America-9 (mGHAA-9) survey. The patients were asked to rank items from 1–14 (most to least) in order of importance. Non-responders were sent a second reminder by post.
Results: Of 119 patients, 80 (67.8%) responded. Of these 27 were included, the main reason for exclusion being uninterpretable rankings. The mean age of patients was 58.2 (SD 20.7) years (see table).
Abstract 425
Conclusion: Technical skill of endoscopist and personal manner of nursing and other staff scored highest in the factors influencing patient satisfaction while noise level, privacy in the examination or recovery room, and staff explanation for reasons of delay were the least important.
426 2 WEEK WAIT FOR UPPER GI CANCER: ARE GPS GETTING THE MESSAGE?
E. Carty1, H. Barrett1, A. M. Sawyerr1, R. R. Greaves1, C. Britt2, E. M. Alstead1.1Whipps Cross University Hospital, Leytonstone, London, UK; 2Waltham Forest Primary Care Trust, UK
Introduction: Twenty out of 21 abstracts reported to the BSG on the 2 week wait referral scheme for patients with upper GI cancer presented negative data.1 We report positive data on the appropriateness of GP referrals via the 2 week wait referral scheme and time from referral to diagnosis.
Method: A comparison of data from an Outer London District General Hospital in 2001 with that from 2004 on: (i) number of patients referred via the 2 week wait scheme for upper GI cancer; (ii) proportion of those referrals subsequently diagnosed as upper GI cancer; (iii) number of patients with upper GI cancer presenting outside the scheme; and (iv) for cancer patients, the time from referral to diagnosis of upper GI cancer.
Results: In 2001, 191 patients were referred via the 2 week wait scheme; only 2% of those were subsequently diagnosed with upper GI cancer. 75% of patients diagnosed with upper GI cancer presented outside the scheme. In the first 8 months of 2004, 175 patients were referred via the 2 week wait scheme, 9% (n = 16) of those patients were subsequently diagnosed with upper GI cancer. 48% (n = 15) of patients diagnosed with upper GI cancer presented outside the scheme. Meanwhile the mean time from GP referral to histological diagnosis in 2001 was 62 days and in 2 week wait scheme patients in 2004 was 26 days (p 0.01).
Conclusion: The proportion of patients with upper GI cancer referred via the 2 week wait scheme has improved without a significant increase in the number of referrals. Over the same period the time from referral to diagnosis has halved.
1
427 FACTORS AFFECTING NON-ATTENDANCE IN NEW GASTROENTEROLOGY OUTPATIENT REFERRALS
S. Gupta, D. J. Maxwell, J. Y. Kang.Department of Gastroenterology, St George’s Hospital, London, UK
Aims: A prospective analysis of factors affecting non-attendance in new gastroenterology outpatient referrals.
Methods: Referral letters and electronic patient records were used to determine the demographics, source and urgency of referral and symptoms of non-attenders and attenders.
Results: 222 patient records from 34 clinics during a 6 week period in 2004 were studied. Information regarding smoking, alcohol consumption, employment, and marital status were not always available. Symptoms leading to referral whether upper or lower gastrointestinal, liver related, or anaemia did not affect the chances of non-attendance.
Conclusion: 20% of new gastroenterology referrals failed to attend their outpatient appointments. Mention of alcohol use in the referral letter and not being married were independently associated with non- attendance. Whether a patient attended or not was not influenced by the source or urgency of referral, type or duration of symptoms, and the interval between referral and appointment date. Shortening the time from referral to clinic appointment may not solve the problem of non-attendance at gastroenterology clinics (see table).
Abstract 427
428 AN AUDIT OF ACUTE UPPER GASTROINTESTINAL HAEMORRHAGE. CAN BLATCHFORD AND ROCKALL SCORES AID IN THE MANAGEMENT?
M. Musa, C. E. F. Grimley.Burnley General Hospital, Casterton Avenue, UK
Introduction: Acute upper gastrointestinal haemorrhage is the commonest GI emergency. Clinical risk stratification is important in the treatment, timing of investigation and safe discharge of patients.
Aims: Whether the Blatchford score can aid in identifying patients with significant risk of needing treatment. Wether the Rockall score can be utilised in identifying patients at low risk of rebleeding and death.
Methods: A retrospective audit of 48 case notes with requests for urgent inpatient endoscopy to investigate acute upper gastrointestinal haemorrhage. High risk patients were identified as those needing therapeutic treatment at endoscopy. Blatchford scores were calculated to ascertain whether these scores could have been used in the clinical risk stratification pre-endoscopically. In the Blatchford study, a score of ≥6 correlated with a 50% or greater risk of needing treatment. Rockall scores of less than 3 were considered low risk of rebleeding or death.
Results: 15 high risk patients were identified. 14 of these 15 patients had Blatchford scores of ≥6. However, only 8 of 15 (53%) had endoscopy within 24 h. If the Blatchford score was used 14 of 15 (93%) high risk patients could have had urgent endoscopy within 24 h. 23 patients had endoscopic findings which were normal or showed mild-moderate oesophagitis and were deemed low brisk. 19 of these 23 cases had Blatchford scores of <6. All 15 high risk cases had significant Rockall scores above 2. 13 of 23 low risk cases had Rockall scores <3 and could possibly have been discharged early. There were no rebleeding or deaths in patients with Rockall scores <3.
Conclusion: The Blatchford score can aid in the clinical risk stratification of patients with acute upper gastrointestinal haemorrhage, and would help to prioritise those patients requiring urgent endoscopy. The Rockall score can be used to aid in early discharge of patients at low risk of rebleeding and death with healthcare costs benefits. As a result of this audit, we have introduced a new acute upper gastrointestinal haemorrhage endoscopy request form and guidelines that incorporate the Blatchford and Rockall scores.
429 GENETIC HAEMOCHROMATOSIS: DIAGNOSTIC ACCURACY OF A DISTRICT GENERAL HOSPITAL CODING
V. Mohan, A. Vaishnavi.Withybush Hospital, Haverfordwest SA61 2PZ, UK
Introduction: Genetic haemochromatosis has a genotype prevalence of 1/200 in Caucasians. As a result of incomplete penetrance, its phenotype is less common. Accurate diagnosis and early, regular phlebotomies of confirmed cases to reduce tissue iron overload is crucial for successful management. Epidemiological data on prevalence and national disease burden depends largely on hospital coding statistics. We present an audit of diagnostic accuracy of patients coded as genetic haemochromatosis in our hospital database.
Methods: We identified all patients clinically coded as genetic haemochromatosis from 1995–2003. The standard for correct diagnosis was a raised ferritin and transferrin saturation supplemented by any one of the following criteria: homozygous or compound heterozygous HFE gene mutation liver biopsy confirming tissue iron overload; therapeutic response to iron depletion with regular phlebotomies. We also looked at data on HFE gene mutations in confirmed cases.
Results: 16 patients were coded as haemochromatosis, but only 11 (69%) met the above standards for diagnosis. In the five who were wrongly coded, genetic haemochromatosis was only considered as a differential due to raised ferritin. Nevertheless, it got transcribed and coded as a diagnosis in the inpatient database. The erroneous coding persisted even after the diagnosis was excluded at outpatient review since the latter visits are not coded. Hyperferritinaemia was usually due to an acute phase response or alcoholic liver disease though in one it was related to multiple previous transfusions. Among 11 patients with confirmed genetic haemochromatosis, HFE gene test was done in 7; the others had their diagnosis confirmed before 1996. 4/7 had homozygous Cys282Tyr mutation, 2/7 were compound heterozygotes, and 1/7 had a non-HFE mutation.
Conclusion: 31% of cases were wrongly coded as genetic haemochromatosis. The current hospital system does not code outpatient visits and therefore cannot rectify any previous errors. Clinicians therefore need reminding that they must only transcribe definite (not probable) diagnosis for coding purposes. There is an urgent need to update our information systems to include OPD visits so that accurate epidemiological data is sent to the Patient Episode Database Wales. (PEDW)
430 THE NURSE LED DYSPEPSIA CLINIC: DOES IT WORK?
J. C. Dearden, I. Mason, O. Epstein.The Royal Free Hospital, Pond Street, Hampstead, London, UK
Background and Aims: Forty percent of all new patient referrals to our unit have dyspepsia or gastroeosphageal reflux. There is delay for routing GI outpatient appointments and concern that this might adversely affect patient outcome. A nurse led dyspepsia clinic was developed to ensure prompt review of patients with arrangements for onward referral of those needing further investigation and treatment.
Methods: We conducted a retrospective audit of patients attending the nurse led clinic. Assessment included the outcome of guideline based triage, investigations, and eventual patient outcome. In addition, patient satisfaction was assessed using a validated questionnaire.
Results: 478 patients attended over the 11 month period. The average waiting time to clinic review was 33 days. GP indications for referral were alarm symptoms or dysphagia in 39.4%. Waiting times for investigations were: 10.6 weeks for urgent oesophagoduodenoscopy (OGD), 23.5 weeks for routine OGD, and 3.6 weeks for barium swallow. Patients with alarm symptoms had either an OGD (80%) or a barium swallow (20%). In this group, two had oesophageal carcinoma, four benign peptic ulcers, and there was a single case of coeliac disease. In the satisfaction survey, 93% of patients understood the aetiology of their symptoms and the reasons for the subsequent investigations. No patient expressed dissatisfaction at being assessed by a nurse specialist. Review of all patient records 8 months after initial management revealed only one patient was been re-referred to the gastroenterology department.
Discussion: All patients were seen within a month of GP referral. While the initial contact was quick, waiting times for endoscopy remained a bottleneck. This did not result in delayed cancer diagnosis as both patients with oesophageal carcinoma had alarm symptoms and were fast tracked by the nurse specialist with investigations complete within 10 days. With these exceptions no patient labelled with alarm symptoms had malignant disease. The nurse led dyspepsia clinic involves short waiting times and permits prompt detection of patients in need of urgent investigation. Patient satisfaction levels are high and re-referral within an 8 month follow up period is unusual.
431 THE SUSTAINED BENEFITS OF A DEDICATED ENDOSCOPY REFERRAL FORM FOR UPPER GI HAEMORRHAGE
S. E. Levison, G. S. Banait (Introduced by Lynch DAF).Department of Gastroenterology, Blackburn Royal Infirmary, UK
Background: Last year we demonstrated the benefits of introducing a dedicated endoscopy referral form incorporating the Rockall score. It reduced time to endoscopy and the length of inpatient stay, without any adverse effects.1 We now ask if these benefits are sustained.
Aims: Evaluate the impact of the referral form 12 months after introduction. Compare outcomes immediately before, immediately following, and 12 months following introduction of the referral form.
Method: The case notes of 40 randomly selected patients admitted with upper GI haemorrhage in the 4 months prior to the introduction of the new acute referral form were compared with 20 similar patients admitted 12 months later. Differences were analysed using χ2 and t tests. The 12 month outcomes were then compared with 40 patient admitted immediately after the new acute referral form’s introduction.
Results: There were no significant differences between any of the groups in terms of age, gender, endoscopic diagnoses, or Rockall scores. Comparing 12 month and pre-referral form, there was a trend towards earlier endoscopy for patients referred on the new form. 90% v 62.5% were endoscoped within 36 h (p<0.10). Average hospital stay for patients with a simple GI bleed was reduced (2.6 v 4.0 days, p = 0.04). Average stay for all patients was reduced (5.0 v 8.8 days, p = 0.05). Total mortality was unaltered at 10%. Comparison of 12 month and immediate post-introduction data demonstrated no significant difference in any outcome. The initial benefits had not decayed.
Conclusion: Use of a dedicated endoscopy referral form continues to have a favourable effect on highly desirable outcomes. This audit demonstrates that a sustained impact is achievable by the introduction of a form harbouring a number of key characteristics; availability at the time of assessment, incorporation of the Rockall score, and guidance on post-endoscopy management. The new form has become an integral part of patient management and benefits patients, clinicians, and the hospital trust. Such effective interventions must be actively promoted.
1
432 DAY CASE LIVER BIOPSIES ARE SAFE IN PATIENTS WITH SUSPECTED MALIGNANT DISEASE
A. S. Dias, S. Lean, M. Farrugia, M. Smith.Oldchurch Hospital, Waterloo Road, Romford, Essex RM7 0BE, UK
Introduction: Liver biopsy is an invaluable tool for the investigation of patients with hepatic disease. Haemorrhage is a major complication and in non-malignant disease has been estimated to occur in 0.2% of cases (0.04% fatal). In cancer patients this risk is increased to 0.97%.1 BSG guidelines recommend that patients with a strong suspicion of malignancy should not have day case biopsies.2
Methods and Results: We looked at liver biopsies performed from September 2000 to March 2004 and compared the complication rates between patients with suspected malignant disease and non-malignant disease. All biopsies were ultrasound guided using an 18G core biopsy needle and performed by the same consultant radiologist. Post biopsy, day case patients were observed in a dedicated recovery area for at least 6 h; inpatients were transferred back to the ward for further observations. Of a total of 189 patients 67 had malignant disease and 122 had liver disease due to other causes. Day case liver biopsies were performed in 14 patients with cancer and 88 patients with non-malignant disease. No complications occurred in the cancer group but in the non-cancer group, six patients (4.9%) developed post biopsy bleeding: two required blood transfusion with angiography and embolisation while one patient required an emergency laparotomy for intraperitoneal bleeding. There were no fatalities. Overall 97.1% of all day case biopsies had documentation of post biopsy observations conforming to BSG guidelines; in contrast only 51.7% of inpatient biopsies complied with BSG guidelines.
Conclusions: In contrast to previous studies patients with cancer in our study population did not have an increased risk of bleeding post liver biopsy. While a greater proportion of these individuals had their biopsies as inpatients, observations in day case patients may be in fact superior. Day case liver biopsies are a safe option in patients with malignancy.
1
2
433 WHAT DOES AN ADULT COELIAC PATIENT WANT FROM MEDICAL GASTROENTEROLOGY OUTPATIENT SERVICES?
L. K. Murray1, A. Sanyal2, I. A. Murray2.1Open University; 2Department of Gastroenterology; Royal Cornwall Hospital
Introduction: The optimum delivery of outpatient gastroenterology services is a thorny issue. Routine annual follow up of coeliac patients often results in little change to management, and is costly both to the health service, and to patients in the time spent travelling to and waiting in clinics for often short appointments. Non-medical practitioners can check routine blood tests, give advice and book tests where appropriate, following protocols. Hence, specialist nurse led clinics are relatively common, dietitian led clinics are functioning, or in many cases, patients are simply discharged back to primary care. We aimed to determine patient preferences with respect to their follow up.
Methods: A self-reported postal questionnaire was sent to over 100 adult coeliac patients attending medical gastroenterology outpatients.
Results: 51 patients responded to the questionnaire (38%). Only one thought they were asked to attend clinic too often, although 24% stated they had to wait too long in clinic to be seen and 53% saw a different doctor at each visit. 12% found that their questions were not always answered. 20% found that seeing a dietitian helped them stick to their diet, and 28% thought that they did not see a dietitian often enough. Although 56% would prefer to be seen in a specialist coeliac clinic, only 10% would be happy to attend a clinic run by a dietitian and 14% a clinic run by a specialist nurse rather than doctor, 66% preferring to continue in the normal clinic. 75% would prefer to have their blood tests taken prior to clinic so that the result was available, and 42% thought the service to coeliac patients “could be better”. Only 8% did not stick to a strict gluten free diet although 20% found difficulty knowing which foods were gluten free or getting information about coeliac disease. 14% felt that they received little help managing their coeliac disease.
Discussion: In this self-selected cohort of coeliac patients, with self-reported strict adherence to a gluten free diet, there was still a relatively high percentage that struggled to determine if foodstuffs were gluten free and to obtain information about coeliac disease. There was a strong reluctance to consider “novel” clinic solutions although standard problems with medical clinics were identified (different doctors, long waiting times in clinic). A specialised coeliac clinic (presumably medically led) and one where results were available at clinic rather than afterwards were key factors identified to improve patient satisfaction. Greater dietitian availability was also requested.
Neurogastroenterology/nutrition posters
434 POST-INFECTIOUS IBS OCCURS AFTER NON-GASTROINTESTINAL AS WELL AS INTESTINAL INFECTION
E. S. McKeown, S. D. Parry, R. Stansfield, J. R. Barton, M. R. Welfare.University of Newcastle Faculty of Medicine, North Tyneside Hospital, Rake Lane, North Shields, Tyne and Wear NE29 8NH, UK
Objectives: Functional GI disorders may follow bacterial gastroenteritis. It is not known whether post-infectious functional GI disorders are specific to GI infections. The primary aim of this study was to determine the frequency of IBS, functional dyspepsia or functional diarrhoea at 3 and 6 months after a non-GI infection.
Methods: This was a prospective, case-control study of people with non-gastointestinal bacterial infection, gastroenteritis, and healthy controls. Functional GI disorders were diagnosed with the use of self-completed Rome II modular questionnaires administered at baseline, 3, and 6 months.
Results: 45 eligible cases were identified and 36 (75%) consented. There was no difference in the incidence of all or any specific functional GI disorder between the GI and non-GI infections. Any functional GI disorder was more frequent in people who had a non-GI infection than in controls at both 3 months (odds ratio 4.34 (95% confidence interval 3.60 to 16.45)) and 6 months (4.76 (4.42 to 27.92)). IBS alone was more frequent in people with non-GI infections at 3 months (6.12 (1.30 to 29.12)) but did not quite reach statistical significance at 6 months (4.58 (0.79 to 26.46)).
Conclusions: There is no difference in the frequency of functional GI disorders following non-GI bacterial infection compared with bacterial gastroenteritis. Functional GI disorders occur more frequently in people after non-gastrointestinal bacterial infection compared with controls. No study has previously investigated the influence of non-GI infections on the development of functional GI disorders. Our findings suggest that non-GI infections may be an aetiological factor in the development of functional gastrointestinal disorders. Further studies are now needed to explore the underlying immune and inflammatory mechanisms.
435 MODULATION OF GASTRIC EMPTYING USING HYPNOTIC SUGGESTION IN HEALTHY VOLUNTEERS
H. P. Jones1, H. F. Kemp2, W. Meier-Augenstein2, P. Cooper1, A. Fryer1, P. J. Whorwell1, L. A. Houghton1.1Academic Department of Medicine, University Hospital of South Manchester, UK; 2Environmental Engineering Research Centre, Queen’s University, Belfast
Introduction: Both visceral sensation12 and orocaecal transit3 are amenable to alteration by hypnosis. The aim of the present study was to determine whether gastric emptying can also be modified using hypnosis.
Methods: Gastric emptying was measured, using the 13C breath test in 18 healthy volunteers (20–53 years; 3 male); once while the subject received hypnotic suggestions that their stomach was emptying its contents slowly (active) and once while listening to relaxing music (control). Each test condition (active and control) was applied for 30 min, 30 min after ingestion of a flapjack meal (231 kcal) containing 150 mg of stable isotope [13C-1] -sodium acetate. The order of studies was randomised, and the intensity of the symptoms of nausea, bloating, distension, fullness, discomfort, and indigestion scored on a scale of 0–5 (5 = very severe) at the end of each test condition.
Results: Gastric emptying was significantly delayed by the hypnotic suggestion that the stomach was emptying its contents slowly (time for half of the meal to empty, T1/2: 148.1 min (mean)) compared with control conditions (T1/2: 135.9 min; mean difference from active (95% CI): −12.2 min (−24.1 to −0.38) min; p = 0.04). This was associated with significantly worse symptomatology under active (mean overall symptom score: 0.31) compared with control conditions (0.05; mean difference from active −0.26 (−0.54 to 0.01); p = 0.01).
Conclusions: These data show that gastric emptying can be modified by hypnotic suggestion, and may help to explain how gut directed hypnotherapy improves symptoms in patients with functional dyspepsia.4
1
2
3
4
436 POST-INFECTIOUS IBS: PROGNOSTIC DATA AT 3 YEARS
E. S. McKeown, S. D. Parry, J. R. Barton, M. R. Welfare.University of Newcastle Faculty of Medicine, North Tyneside Hospital, Rake Lane, North Shields, Tyne and Wear NE29 8NH, UK
Objectives: Up to a quarter of all people with infectious gastroenteritis go on to develop a post-infectious functional gastrointestinal disorder including IBS. However, little data exists on the prognosis of post-infectious IBS with one recent study estimating a recovery in just under half of cases at 6 years.1 This study’s aim was to assess the persistence of gut dysfunction in a cohort of patients with a previous diagnosis of post-infectious functional gastrointestinal disorder just 3 years on from their proven bacterial enteric infection.
Methods: A follow up study inviting 26 from 27 possible individuals with a diagnosis of a post-infectious functional gastrointestinal disorder, including 18 with post-infection IBS, 6 -months after gastroenteritis. Consented cases resubmitted the IBS, functional dyspepsia and functional diarrhoea components of the Rome II Modular Questionnaire at 3 years.
Results: Twenty one subjects completed the 3 year follow up questionnaire. In over half (n = 12, 57%), gut symptoms had resolved completely. Nine subjects (43%) were still symptomatic. Of the 18 cases with post-infection IBS at 6 months, 13 completed the 3 year questionnaire. Six (46%) reported complete resolution of IBS with five reporting persistence (38%). Symptoms had changed from IBS at 6 months to functional dyspepsia at 3 years in the remaining two subjects.
Conclusions: About half (46%) of post-infection IBS cases have recovered at 3 years. This is a similar figure to the 43% seen in the 6 year follow up study published.1 People with post-infection IBS may recover earlier than 3 years but to determine whether recovery from post-infection IBS persists over time much larger prognostic studies are required. This study adds further important data on post-infection IBS prognosis.
1
437 CILANSETRON DEMONSTRATED RELIEF FROM ABDOMINAL PAIN/DISCOMFORT IN IBS WITH DIARRHOEA PREDOMINANCE
H. Monnikes1, L. A. Houghton2, F. Carter3, S. Caras3, G. Krause4, C. Steinborn4.1Charité-University Hospital & Medical School, Berlin, Germany; 2University Hospital of South Manchester, UK; 3Solvay Pharmaceuticals, Inc., Marietta, GA, USA; 4Solvay Pharmaceuticals GmbH, Hannover, Germany
Introduction: In two double blind, placebo controlled studies, a 3 month US study (S1) and a 6 month multinational study (S2) cilansetron, a new 5HT3 receptor antagonist, demonstrated relief of abdominal pain/discomfort in a significantly greater proportion of IBS with diarrhoea predominance (IBS-D) patients compared with placebo.12
Methods: A post-hoc analysis of males and females was performed on the mean change in mean daily abdominal pain/discomfort scores from baseline to end of treatment. Patients with Rome-defined IBS-D were randomised to receive either cilansetron 2 mg TID or placebo. Abdominal pain/discomfort was measured daily using a validated interactive voice response system (Likert scale, 0 = no pain to 4 = intolerable pain). Responders to treatment were defined as subjects who reported adequate relief for >50% of their weekly diary responses.
Results: The intent-to-treat populations were 692 in S1 (205 men, 487 women) and 792 in S2 (358 men, 434 women). Results from the S1 and S2 trials indicated significantly more responders in the cilansetron groups v the placebo groups for the relief of abdominal pain/discomfort; 52% v 37%, p<0.001 over 3 months and 61% v 46%, p<0.001 over 6 months. Mean baseline abdominal pain/discomfort scores for both studies ranged 1.72–1.89 for cilansetron and 1.71–1.86 for placebo. In males, cilansetron improved abdominal pain/discomfort v placebo in mean reduction in mean scores from baseline (S1: −0.55 v −0.44, p = 0.083; S2: −0.90 v −0.67; p = 0.023). In females, abdominal pain/discomfort improvement was similar and significant (S1: −0.75 v −0.49; p = 0.002, S2: −0.94 v −0.74; p = 0.005). Constipation was the most commonly reported adverse event in both studies. There were four suspected cases of ischemic colitis, one in S1 and three in S2; all were transient and resolved without sequelae.
Conclusion: Cilansetron provides significant relief from abdominal pain/discomfort in both males and females with IBS-D for at least 6 months.
1
2
438 THE ILEO-CAECAL VALVE: MORPHOLOGY AND MANOMETRY SUGGEST A COMBINED FLAP VALVE AND PHYSIOLOGICAL SPHINCTER
E. D. P. S. Fernando, K. I. Deen.Faculty of Medicine, University of Kelaniya, Sri Lanka
Introduction: The nature of the ileo-caecal valve remains controversial. It is believed to function chiefly as a flap valve. We undertook manometric evaluation combined with videography of the ileo-caecal valve to further ascertain its nature.
Patients and Method: Twenty one individuals (9 males, median age 49 years, range 24–77 years) undergoing colonoscopy were studied. A water filled balloon of maximum diameter 10 mm attached to a non-distensible plastic catheter was introduced into the terminal ileum via the colonoscope with minimal air insufflation. The balloon-catheter device was attached to a pressure transducer connected to a single channel chart recorder. Pressure within the terminal ileum, ileo-caecal valve and the caecum was recorded for 1 min at each station after a period of stabilisation. Mean pressure was defined as the area under the curve/duration. Simultaneously, videography of the ileo-caecal valve was performed in thirteen of 21 individuals to observe the passage of the effluent through this valve.
Results: In 20 (95%) of 21 individuals, intra-ileal pressure exceeded intra-caecal pressure (ileal pressure (mean 40.98, SD 44.73) cm H2O v caecal pressure (mean 17.77, SD 46.27) cm H2O). An ante-grade pressure gradient was observed from the terminal ileum to caecum in 15 (71%) of these 20 individuals. The five (24%) of 20, we observed a high-pressure zone within the ileo-caecal valve. In one person (5%) a reverse pressure gradient was seen where caecal pressure exceeded terminal ileal pressure. Videography revealed a typical flap valve with a longer superior flap in 11 (85%) of 13.
Conclusions: The manometry of the ileo-caecal valve revealed a flap valve with an ante-grade pressure gradient in the majority. A reverse gradient was seen in one. This may explain ileo-caecal valve incompetence. The ileo-caecal valve is a flap, which also has a demonstrable physiological sphincter.
439 GASTROINTESTINAL SYMPTOMS IN PATIENTS UNDERGOING CONTINUOUS AMBULATORY PERITONEAL DIALYSIS TREATMENT
A. K. Neil1, A. Barnabas1, J. B. Eastwood2, I. C. R. Hartley3, J. D. Maxwell1, J. Y. Kang1.1Departments of Gastroenterology and 2Renal Medicine, St Georges Hospital, London, UK; 3Pepys Road Surgery, London, UK
Background: Uraemic patients have been said to have a high frequency of gastrointestinal symptoms including nausea, vomiting and constipation, but this hypothesis has not been tested rigorously.
Aims: To determine the prevalence of gastrointestinal symptoms in patients with end-stage renal failure on continuous ambulatory peritoneal dialysis treatment, and to compare them to sex- and age-matched general medical outpatients without renal failure as well as community subjects.
Methods: Patients and hospital controls completed a locally validated Rome II questionnaire, usually face-to-face but in a few instances over the telephone. Community controls received and returned their questionnaires through the post.
Results: Of 58 patients on continuous ambulatory peritoneal dialysis treatment in our department 54 (93%) completed the study. No patient had frequent vomiting. The prevalence of various gastrointestinal symptoms, IBS and unspecified functional bowel disorders was compared with that of 48 outpatients and 94 community controls (see table).
Abstracts 439, table 1
Conclusions: Patients on continuous ambulatory peritoneal dialysis have an increased prevalence of several gastrointestinal symptoms compared with community controls. They use more laxatives than both control groups suggesting that a tendency to constipation is being adequately managed.
440 RISK OF OESOPHAGEAL CANCER IN ACHALASIA CARDIA: A META-ANALYSIS
C. L. Gillies1, K. R. Abrams1, J. F. Mayberry2.1Department of Health Sciences, University of Leicester, 22–28 Princess Road West, LE1 6TP, UK; 2Leicester General Hospital, Gwendoline Road, Leicester, LE4 5PW, UK
Background: Following the initial report of oesophageal cancer in achalasia cardia by Fagge et al in 1862 various reports have supported this association. The risk of oesophageal cancer is estimated to be between 3–30% in various studies. Despite this there are currently no guidelines regarding surveillance in these patients.
Aims and Methods: The aim of this meta-analysis was to establish the magnitude of risk of oesophageal cancer in achalasia cardia and to determine how this changes with time. A literature search using MEDLINE was done. Data were collected on duration of achalasia, length of follow up, and number of oesophageal cancers both in the first year after diagnosis of achalasia and subsequent years. Overall pooled estimates, with 95% confidence intervals (CI), of cancer incidence were obtained using a Bayesian-Poisson regression model.
Results: Of the 28 studies identified 16 met the inclusion criteria and were included in the meta-analysis. This covered a time period of 1932–92. Most studies were from Europe, USA, South America, or Australia. The overall incidence of oesophageal cancers based on 16 studies was estimated to be 1.36 (95% CI 0.56 to 2.51) per 1000 patient years. Thirteen of the 16 studies could be divided into those where oesophageal cancer occurred during the first year of diagnosis and those, which occurred during the subsequent years. When the results were time stratified by the year of diagnosis the incidence rated were 0.71 (95% CI 0.00 to 4.71) in the first year after diagnosis compared to incidence rates of 1.55 (95% CI 0.60 to 2.53) in the subsequent years. The population incidence rates were lower than the pooled incidence rates.
Conclusion: Achalasia cardia is a risk factor for oesophageal cancer. The risk of oesophageal cancer increases with time as evidenced from the time-stratified analysis. There may a case for surveillance in these patients.
441 OBESITY AS AN INDEPENDANT RISK FACTOR FOR FUNCTIONAL GUT DISORDERS
Z. Philipose1, M. A. Mendall1, A. Poullis2.1Department of Gastroenterology, Mayday University Hospital; 2Department of Gastroenterology, St George’s Hospital, London, United Kingdom
Introduction: Obesity has been associated with significant morbidity mainly cardiovascular illnesses. It has also been shown to be associated with gut inflammation in previous studies.1 Low grade bowel inflammation has been noted in diarrhoea predominant IBS.
Aims and Methods: To assess if obesity or increased body mass index (BMI) is a risk factor for functional gut disorders independant of female sex status, history of gut infection, and psychological morbidity. This entailed a study of 349 subjects (aged between 50 to 70 years) with almost equal proportion of males and females from a general population. A standardised dietary, bowel habit questionnaire and SF-36 was filled in and their BMI was calculated. The data were analysed using multiple logistic regression in SPSS.
Results: Out of the total, 44 subjects fulfilled the ROME II diarrhoea predominant criteria for functional gut disorders.2 The BMI quartile 1 was 11/90 (12%); quartile 2 was 9/95 (9.5%); quartile 3 was 10/89 (11%); and quartile 4 was 14/75 (19%). The risk of association of per kg/m2 increase in BMI was 1.087 (OR) with p = 0.037 (95% CI 1.005 to 1.176). There was no association with relation to age or sex status.
Conclusion: Following adjustment for the different features of SF-36 (namely vitality, social functioning, bodily pain, and general health perceptions) which individually accounted for females with diarrhoea predominant IBS but there was no attenuation of the association of BMI. This suggests that the pathogenesis of diarrhoea predominant IBS associated with obesity may have a physical basis but that associated with the female sex may have a different basis.
1
2
Supplementary materials
In supplement II, April 2005, abstract 420 (A prospective audit to establish if infliximab is safe to be administered by a nurse specialist in a district general hospital. A Thomson et al, p A111) of the BSG Annual Meeting is incorrect. The two letter abbreviation of CD was mistakenly changed to Coeliac disease rather than Crohn's disease.
Linked Articles
- Abstracts
- CORRECTION
- Corrections