Article Text

Abstract
Objective Magnetic resonance imaging (MRI) enables accurate assessment of inflammatory bowel diseases (IBD), but its main limitation is the need for bowel preparation. Diffusion-weighted imaging is feasible in Crohn's disease. We evaluated the accuracy of MRI in combination with diffusion-weighted imaging (DWI-MRI) without oral or rectal preparation in assessing colonic inflammation in both ulcerative colitis and Crohn's disease.
Design This was an observational study of a single-centre cohort.
Patients All patients who underwent DWI-MRI-colonography without bowel preparation between January 2008 and February 2010 in our centre were analysed.
Results Among the 96 patients (ulcerative colitis=35; Crohn's disease=61) who had DWI-MRI-colonography, 68 had concomitant endoscopy. In ulcerative colitis a segmental magnetic resonance score (MR-score-S) >1 detected endoscopic inflammation with a sensitivity and specificity of 89.47% and 86.67%, respectively (AUROC=0.920, p=0.0001). In the Crohn's disease group, a MR-score-S >2 detected endoscopic inflammation in the colon with a sensitivity and specificity of 58.33% and 84.48%, respectively (AUROC=0.779, p=0.0001). The MR-score-S demonstrated better accuracy for the detection of endoscopic inflammation in the ulcerative colitis group than in the Crohn's disease group (p=0.003). In ulcerative colitis, the proposed total magnetic resonance score (MR-score-T) correlated with the total modified Baron score (r=0.813, p=0.0001) and the Walmsley index (r=0.678, p<0.0001). In Crohn's disease, the MR-score-T correlated with the simplified endoscopic activity score for Crohn's disease (r=0.539, p=0.001) and the Crohn's disease activity index (r=0.367, p=0.004). The DWI hyperintensity was a predictor of colonic endoscopic inflammation in ulcerative colitis (OR=13.26, 95% CI 3.6 to 48.93; AUROC=0.854, p=0.0001) and Crohn's disease (OR=2.67, 95% CI 1.25 to 5.72; AUROC=0.702, p=0.0001). The accuracy of the DWI hyperintensity for detecting colonic inflammation was greater in ulcerative colitis than in Crohn's disease (p=0.004).
Conclusions DWI-MRI-colonography without bowel preparation is a reliable tool for detecting colonic inflammation in ulcerative colitis.
- Ulcerative colitis
- Crohn's disease
- magnetic resonance colonography
- diffusion-weighted imaging
- colonic inflammation
- abdominal MRI
- Crohn's colitis
- inflammation
- MRI
Statistics from Altmetric.com
- Ulcerative colitis
- Crohn's disease
- magnetic resonance colonography
- diffusion-weighted imaging
- colonic inflammation
- abdominal MRI
- Crohn's colitis
- inflammation
- MRI
Significance of this study
What is already known about this subject?
MRI colonography enables accurate assessment of inflammatory bowel diseases
The main limitation of MRI colonography is the need for bowel preparation
Diffusion-weighted imaging is feasible in Crohn's disease for the detection of colonic inflammation
What are the new findings?
Diffusion-weighted imaging magnetic resonance colonography (MRI-DWI-colonography) without oral or rectal preparation is a reliable tool for detecting colonic inflammation in ulcerative colitis
This imaging technique does not require fasting, is non-invasive, non-irradiating, does not require any bowel preparation, and is of short duration
Diffusion-weighted imaging hyperintesnity exhibited the same accuracy as ‘rapid gadolinium enhancement after intravenous contrast medium administration’ for the detection of endoscopic inflammation in both ulcerative colitis and Crohn's disease
How might it impact on clinical practice in the foreseeable future?
MRI-DWI-colonography, a modality combining MRI and diffusion-weighted imaging, without oral or rectal preparation might be used in clinical practice to assess colonic inflammation in ulcerative colitis
Diffusion-weighted imaging sequence may replace gadolinium injection for detecting inflammatory colonic segments in ulcerative colitis
Introduction
Inflammatory bowel diseases (IBD) primarily comprise two disorders, ulcerative colitis, which affects only the colon, and Crohn's disease, which can affect the entire gastrointestinal tract. Currently, conventional colonoscopy (CC) represents the ‘gold standard’ for assessing disease activity and extent in ulcerative colitis1 and Crohn's disease.2 Its main drawbacks are the need for colonic preparation, its invasiveness and the risk of complications related to general anaesthesia. Several reports have highlighted the increased risk of ionising radiation associated with CT scanning in patients with IBD.3 MRI has the advantage of avoiding the risks related to ionising radiation, particularly because the population is made up of young patients who will undergo several morphological explorations throughout the course of their disease. Using endoscopy as the reference standard Rimola et al prospectively evaluated the accuracy of MRI for assessment of disease extent and severity in 50 patients with Crohn's disease.4 The authors demonstrated that MRI may represent an alternative to CC in the evaluation of ileocolonic Crohn's disease.4
However, the main limitation of this imaging method is the need for colonic preparation similarly to CC.4–6 In our daily practice and in the literature, oral or rectal preparations are usually poorly tolerated.7 This may limit the use of MRI in clinical practice.
Diffusion-weighted imaging (DWI) derives its image contrast from differences in the motion of water molecules between tissues.8 Two pilot studies assessed the feasibility of DWI in Crohn's disease, but no definite conclusions can be drawn from these studies because colonoscopy was not used as the reference test9 or because the sample size was small.10 In addition, DWI has not been evaluated in ulcerative colitis.
In our centre, MRI is routinely used to assess disease activity in patients with IBD. Because in some IBD patients our aim was only to detect the presence of colonic inflammation, we did not administer bowel cleansing, but diffusion-weighted (DW) sequences were added to MR colonography.
Here, we report our experience with a simple non-invasive imaging technique, namely MR colonography in combination with DWI (MRI-DWI-colonography) without any oral or rectal preparation, in both ulcerative colitis and Crohn's disease.
The aims of this observational study were: (1) to assess the accuracy of MR-DWI-colonography without oral or rectal preparation in the detection of colonic inflammation, evaluated by CC; and (2) to correlate findings on MR-DWI-colonography without oral or rectal preparation with clinical and biological IBD activity indices.
Patients and methods
Population studied
We performed an observational study of a single-centre cohort in which a prospectively designed, standardised evaluation was used by experienced clinicians for all patients. Data were retrieved from a prospectively maintained database. Between 15 January 2008 and 9 February 2010, 96 patients with a diagnosis of IBD based on clinical, biological, endoscopic, histological and/or radiological evidence underwent MR-DWI-colonography without oral or rectal preparation and with or without concomitant colonoscopy. Colonoscopy was considered concomitant to MR-DWI-colonography if it was performed within 48 h after the radiological examination, without any therapeutic intervention during this interval. Colonoscopy and MR-DWI-colonography were performed during a flare or to rule out active disease. In our centre the diffusion-weighted sequence is added routinely on MRI. The Ethics Committee of the University Hospital of Nancy approved this practice as it does not generate particular risk to the patient and produces no extra charge on the imaging procedure. Our cohort of IBD patients is reported to The Commission Nationale de l'Informatique et des Libertés (N°1404720) which supervises the implementation of the 6 January 1978 Act on data processing, data files, and individual liberties as amended by the 6 August 2004 Act relating to protection of individuals with regard to the processing of personal data.
Clinical and biological markers of disease activity
In our centre, all patients are followed according to a standardised follow-up protocol and clinical data were retrieved from a prospectively maintained database. Clinical disease activity scores were calculated using data collected on the day of MR-DWI-colonography: the simple clinical colitis activity index (Walmsley index)11 in ulcerative colitis patients, and the Crohn's disease activity index (CDAI)12 in patients with Crohn's disease. The following biological parameters were collected from the patients' electronic records: C-reactive protein, haemoglobin, haematocrit, leucocytes, platelets, serum iron, and albumin. Only examinations performed in the 48 h after the MR-DWI-colonography were regarded as concomitant examinations and included in the analyses.
Endoscopy
Colonoscopy was considered the ‘gold standard’ for assessing colonic lesions. Patients followed a bowel cleansing protocol via oral ingestion of 3000–4000 ml of an iso-osmotic polyethylene glycol and electrolyte solution (COLOPEG; Bayer Family Health, Gaillard, France) on the evening before examination, as routinely performed in our department. Endoscopy was performed under anaesthesia with propofol (PROPOFOL DAKOTA PHARM; Sanofi-Aventis, Paris, France). All colonoscopies were performed by two experienced endoscopists (MAB, LPB) using column video colonoscopy (QFC L 140; Olympus, Tokyo, Japan). All colonic lesions were rated according to standardised scoring systems for ulcerative colitis and Crohn's disease as routinely used in the department.
Ulcerative colitis
The severity and extent of endoscopic lesions were assessed by the modified Baron score (MBS).13 To correlate endoscopic lesions with findings on MRI-DWI-colonography, five endoscopic segments were defined: rectum, sigmoid, left colon, transverse colon, and right colon. The MBS was applied to each segment to obtain a segmental MBS (MBS-S). A total score was calculated from the sum of the segmental scores to obtain the total MBS (MBS-T). Endoscopic inflammation in the colon was considered ‘present’ in a given segment if MBS-S ≥ 1.
Crohn's disease
The severity and extent of endoscopic lesions were assessed by the simplified endoscopic activity score for Crohn's disease (SES-CD).14 To correlate the MRI-DWI findings with colonoscopy, six endoscopic segments were defined: rectum, sigmoid, left colon, transverse colon, right colon, and ileum. The SES-CD was applied to each segment to obtain a segmental SES-CD (SES-CD-S). Endoscopic colonic inflammation was considered ‘present’ when the following lesions were reported by the endoscopist: erythema, oedema, pseudo-polyps, aphthoid ulcers, and ulceration.
Magnetic resonance colonography acquisition protocol
No bowel cleansing was proposed to the patient the day before the examination. On the day of MRI-DWI-colonography, patients were not fasting and had not received an oral or rectal preparation. MRI examinations were performed using a 1.5 T GE Signa HDx scanner (General Electric HealthCare, Waukesha, Wisconsin, USA). The protocol comprised a two-dimensional (2D) SS FSE short Te (single shot fast spin echo short Te) sequence in the axial and coronal planes, a 2D SS FP (steady state free precession) with fat saturation in the coronal plane, a diffusion-weighted sequence in the axial plane, a 3D gradient echo (GE) T1 sequence after intravenous administration 0.2 ml/kg body weight of gadoteric acid (DOTAREM, 0.5 mmol/ml; Guerbet, Villepinte, France) at a rate of 3 ml/s for dynamic study in the axial plane (arterial phase (25 s after injection), portal phase (70 s after injection), and post-equilibrium phase (2 min after injection)), and a 2D gradient echo with fat saturation at 3 min and 5 min after injection in the axial and coronal planes. The diffusion-weighted sequence employed a diffusion factor b fixed at 600 s/mm2 and provided two sets of images, one for the expected b value and another for b=0.The acquisition was performed in the axial plane using a 36 cm field of view and a 7 mm slice thickness with no gap, with a 3×5 mm2 in-plane resolution. Two stations were needed to cover the abdomen and the pelvis. The b factor was fixed at 600 s/mm2 because this value constituted the best compromise between SNR (signal to noise ratio) and lesion detection sensitivity on our MRI system. All sequences were performed in respiratory triggering except for the dynamic study with 3D gradient echo T1 after intravenous injection of contrast medium, 2D gradient echo T1, and the SS FP sequences, which were done with the breath held. Concerning the instrumental aspect, a 12-element phase-array coil was systematically used with a parallel imaging technique (SENSE: Sensitivity Encoding, factor 2). The gradient amplitude was 33 mT/m. The duration of the entire examination was about 20 min. Technical characteristics of diffusion-weighted imaging sequence and 3D acquisition gradient echo sequence are available as online supplementary material.
Magnetic resonance score
For MRI-DWI-colonography analysis, six segments were identified: rectum, sigmoid, left colon, transverse colon, right colon, and ileum. Based on a comprehensive review of the literature, six radiological signs were studied: (1) DWI hyperintensity (DWI-HI), (2) rapid gadolinium enhancement after intravenous contrast medium administration (GADO), (3) differentiation between the mucosa–submucosa complex and the muscularis propria, (4) bowel wall thickening, (5) parietal oedema, and (6) the presence of ulceration(s). The definition of each radiological sign is provided in table 1.
Definition of the six components of the magnetic resonance (MR) score
The presence and absence of a radiological sign in a given segment were rated ‘1’ and ‘0’, respectively. The segmental MR-score (MR-score-S) was calculated as the sum of the numerical values obtained for the six radiological signs for a given segment. The total MR-score (MR-score-T) was calculated as the sum of the MR-score-S in a patient, with values ranging from 0 to 30 in the case of ulcerative colitis and from 0 to 36 in the case of Crohn's disease. For each patient, two MR-scores were established by two experienced radiologists (VL, OB).
Statistical analyses
Quantitative variables are described as means±SD (SD) or as medians and percentiles (IQR: 25% and 75%) in the case of an abnormal distribution. Proportions are expressed as percentages and 95% CIs. All correlations were studied using Spearman's nonparametric correlation coefficients (r and p value, respectively).
Correlation between the MR-score and endoscopic findings
Only patients who had undergone a lower gastrointestinal endoscopy considered concomitant with the MRI-DWI-colonography were included in the analysis. In the ulcerative colitis group, the following parameters have been studied for correlation: (1) MR-score-S versus MBS-S and (2) MR-score-T versus MBS-T. In the Crohn's disease group, the following parameters have been studied for correlation: (1) MR-score-S versus SES-CD-S and (2) MR-score-T versus SES-CD.
Accuracy of the MR-score-S and its six components for detection of endoscopic inflammation
The MR-score-S and its six components were analysed to assess their accuracy in the detection of endoscopic colonic inflammation in the corresponding intestinal segment. The analysis was performed using the receiver operating characteristic (ROC) method to calculate the sensitivity, specificity, and area under the receiver operating characteristic curve (AUROC) with the associated p value. In a second step, the AUROC of the six MR-score components were compared to identify the one that best detects endoscopic colonic inflammation. These AUROC comparisons were carried out using the procedure proposed by Delong et al.15
Identifying predictive factors for endoscopic inflammation among the MR-score items
To search for independent variables predictive of the presence of endoscopic colonic inflammation, the six items composing the MR-score were integrated into a binary logistic regression model. The forward method was used. All variables with p<0.1 were included in the model, and the variables with p<0.05 were retained in the model. Results were shown as ORs and 95% CIs.
Correlation of MR-score-T or endoscopic scores with clinical and biological markers of disease activity
All patients who had undergone a MRI-DWI-colonography were included in the analysis of correlation between the MR-score and the IBD activity markers. Only patients who had undergone endoscopic evaluation were included in the analysis of correlation between endoscopic scores and IBD activity markers. In a second step, for each IBD activity marker, the correlation coefficient of the MR-score was compared with that of endoscopic scores. Comparisons of correlation coefficients were performed using the correlation coefficients comparison test.16
Interobserver agreement for MR-score calculation
Interobserver agreement between two independent radiologists (VL, OB) for the MR-score-T, the MR-score-S, and the six MR-score components, was evaluated through κ statistics. Interpretation of the κ coefficient was carried out according to Altman.17
All reported p values were two-sided, and p<0.05 was considered statistically significant. Statistical analyses were performed using MedCalc® software version 11.2.
Results
Baseline characteristics of the 96 patients
A total of 96 patients were analysed, including 35 patients with ulcerative colitis and 61 patients with Crohn's disease. The baseline characteristics of the two groups are shown in tables 2 and 3.
Baseline characteristics of patients in the ulcerative colitis group (n=35)
Baseline characteristics of patients in the Crohn's disease group (n=61)
As indicated above, MRI-DWI-colonography was performed in all patients. In the ulcerative colitis group, 28 patients (80%) underwent endoscopic evaluation, including 16 patients (57%) with complete colonoscopy, two patients (7%) with endoscopy up to the splenic flexure, nine patients (32%) with sigmoidoscopy, and one patient (4%) with proctoscopy. A total of 105 segments were analysed in the ulcerative colitis group. In the Crohn's disease group, 40 patients (66%) underwent endoscopic evaluation, including 27 patients (68%) with ileocolonoscopy, six patients (15%) with colonoscopy without ileum visualisation, three patient (8%) with endoscopy up to the hepatic flexure, and four patients (10%) with sigmoidoscopy. Of note, one patient had a history of right hemicolectomy for IBD. A total of 211 segments in the Crohn's disease group were analysed (figure 1).
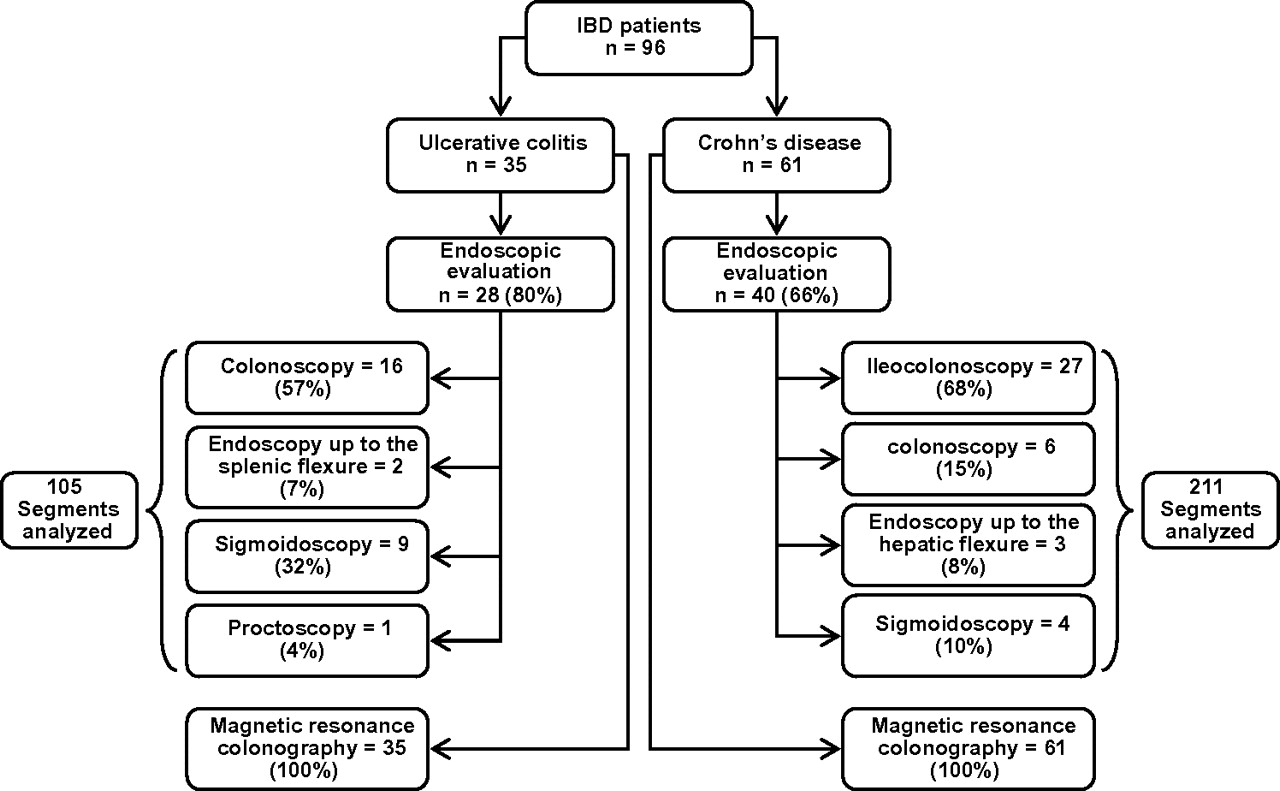
Flow chart of the 96 patients with inflammatory bowel disease included in the study.
Correlation between the MR-score and endoscopic scores in ulcerative colitis and Crohn's disease
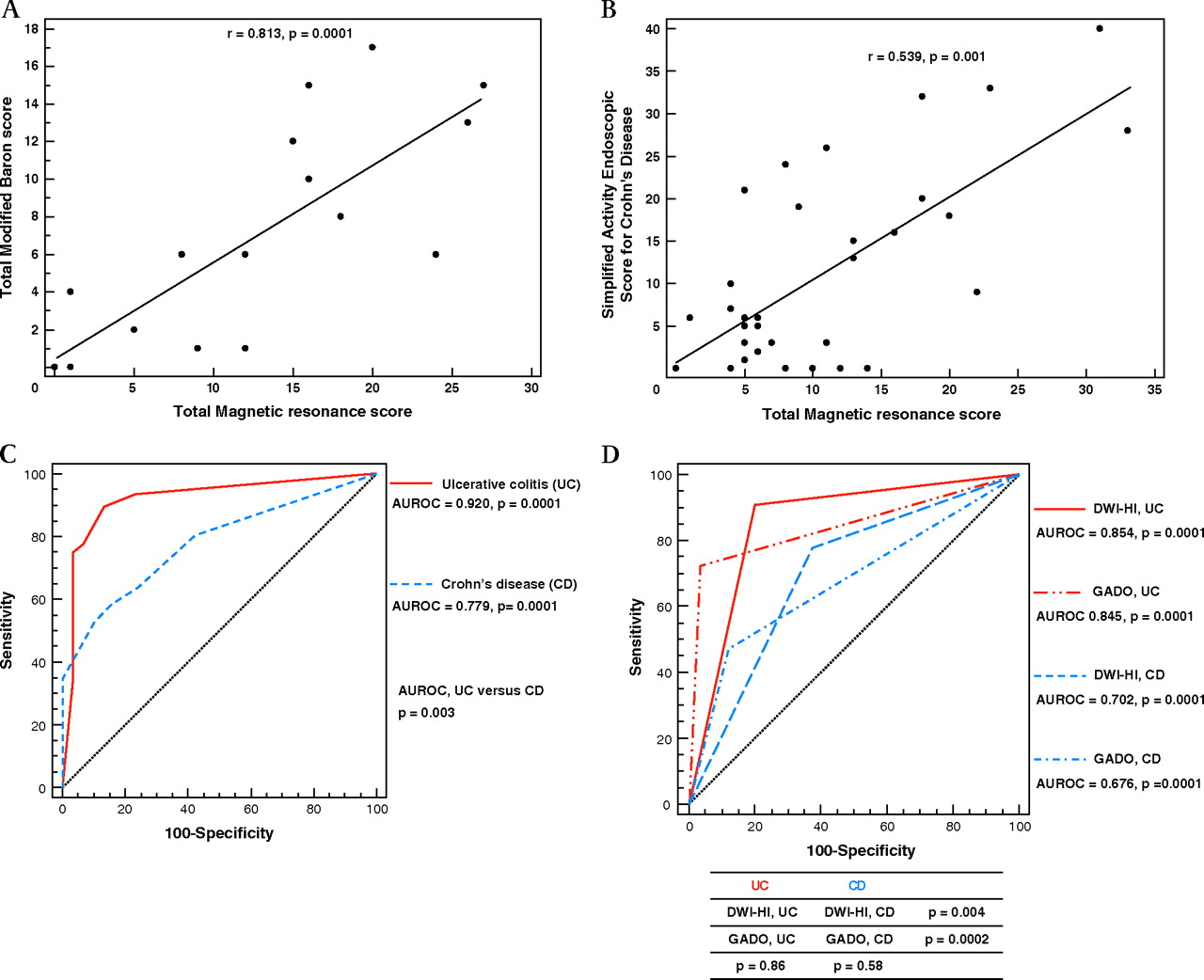
In segmental analysis, the MR-score-S was correlated with the MBS-S (r=0.659, p<0.0001) and SES-CD-S (r=0.565, p<0.0001). The MR-score-T was also correlated with the MBS-T (r=0.813, p=0.0001) and SES-CD (r=0.539, p=0.001) (figure 2A,B).

Accuracy of the magnetic resonance score (MR-score) for evaluation of endoscopic inflammation in the colon in ulcerative colitis and in Crohn's disease. (A) Correlation between the total MR-score (MR-score-T) and the total modified Baron score in the ulcerative colitis group. (B) Correlation between the MR-score-T and the simplified endoscopic activity score for Crohn's Disease (SES-CD) in the Crohn's disease group. (C) Accuracy of the segmental MR-score for detecting endoscopic inflammation in the colon in the ulcerative colitis and Crohn's disease groups. (D) Accuracy of diffusion-weighted imaging hyperintensity (DWI-HI) and rapid gadolinium enhancement after intravenous contrast medium administration (GADO) for detecting endoscopic inflammation in the colon in ulcerative colitis and in Crohn's disease (AUROC, area under the receiver operating characteristic curve; ulcerative colitis, ulcerative colitis; CD, Crohn's disease).
Accuracy of the MR-score for endoscopic inflammation detection in ulcerative colitis and Crohn's disease
Segmental MR-score, DWI-HI, and GADO
Sensitivity, specificity, and AUROC of the MR-score-S and its six components for the detection of colonic inflammation in patients with ulcerative colitis and Crohn's disease are shown in table 4. The comparisons of AUROCs of the MR-score-S and its six components between ulcerative colitis and Crohn's disease are displayed in the supplementary figure 1. In the ulcerative colitis group, a MR-score-S >1 detected endoscopic inflammation with a sensitivity and specificity of 89.47% and 86.67%, respectively, with an AUROC of 0.920 (p=0.0001). In the Crohn's disease group, a MR-score-S >2 detected endoscopic inflammation in the colon with a sensitivity and specificity of 58.33% and 84.48%, respectively, with an AUROC of 0.779 (p=0.0001). The MR-score-S demonstrated better accuracy for the detection of endoscopic inflammation in the ulcerative colitis group than in the Crohn's disease group (p=0.003) (figure 2C). In the ulcerative colitis group, the presence of a DWI-HI demonstrated a sensitivity and a specificity of 90.79% and 80%, respectively, for the detection of endoscopic inflammation, with an AUROC of 0.854 (p=0.0001). DWI-HI was more effective for the detection of endoscopic colonic inflammation in ulcerative colitis than in Crohn's disease (p=0.004) (figure 2D). In the ulcerative colitis group, GADO detected endoscopic inflammation in the colon with a sensitivity and specificity of 72.37% and 96.67%, respectively, with an AUROC of 0.845 (p=0.0001). GADO was more effective for the detection of endoscopic inflammation in ulcerative colitis than in Crohn's disease (p=0.0002) (figure 2D).
Accuracy of the segmental magnetic resonance score (MR-score-S) and its six components for the detection of colonic endoscopic inflammation in ulcerative colitis and in Crohn's disease
Four other parameters of the MR-score
In ulcerative colitis, ROC analyses for the four remaining parameters of the MR-score (differentiation between the mucosa–submucosa complex and the muscularis propria, bowel wall thickening, parietal oedema, and ulceration) for the detection of endoscopic inflammation demonstrated a good sensitivity (88.16%) and specificity (83.33%) for the ‘differentiation between the mucosa–submucosa complex and the muscularis propria’. For the three other items the sensitivity was low, ranging from 38.16% to 67.11%, with excellent specificities ranging from 93.33% to 96.67%. In Crohn's disease, ROC analyses for the same four parameters revealed low sensitivities ranging from 36.11% to 62.5% and good to excellent specificities ranging from 75% to 100%.
Among these four parameters, the ‘differentiation between the mucosa–submucosa complex and the muscularis propria’ and ‘ulcerations’ exhibited better accuracy for the detection of endoscopic inflammation in ulcerative colitis than in Crohn's disease. The accuracy was similar for the other two items in both ulcerative colitis and Crohn's disease (table 4) (supplementary figure 1).
MRI findings in patients with ulcerative colitis or Crohn's disease with severely active disease or in clinical remission are shown in figures 3 and 4 and supplementary figures 2 and 3.

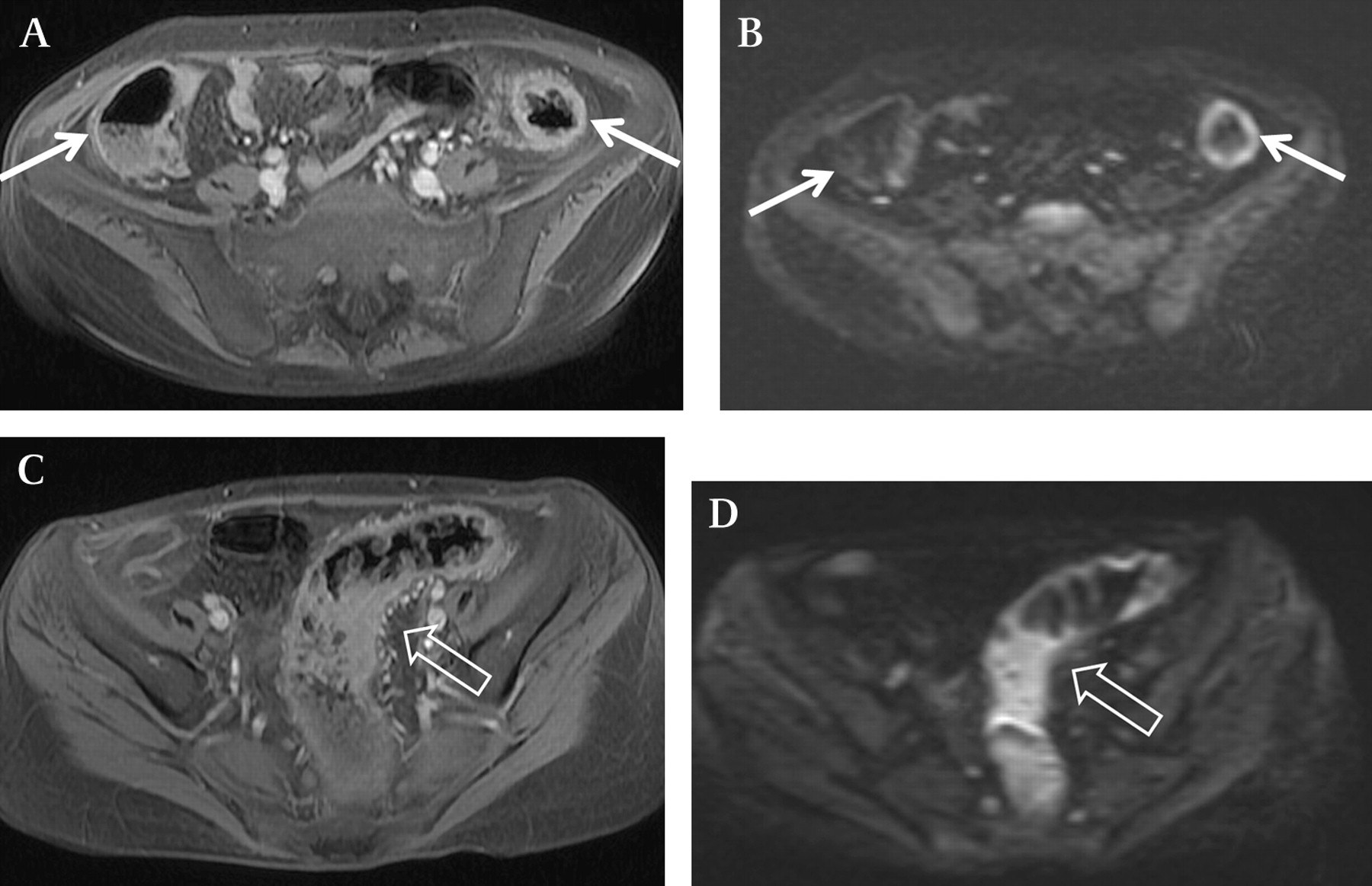
A 22-year-old woman with a severe attack of ulcerative colitis (pancolitis); Walmsley index=10; Total modified Baron score=13; Total magnetic resonance score=26/30; (A) Rapid gadolinium enhancement in the right and left colons (full arrows); (B) diffusion-weighted hyperintensity in the right and the left colons (full arrows); (C) rapid gadolinium enhancement in the sigmoid (hollow arrow); (D) diffusion-weighted hyperintensity in the sigmoid (hollow arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A 22-year-old woman with severely active colonic Crohn's disease; Crohn's disease activity index (CDAI) = 403; simplified activity endoscopic score for Crohn's disease = 15; total magnetic resonance score = 33/36. (A) Rapid gadolinium enhancement in the right and left colons (full arrows); (B) diffusion-weighted hyperintensity in the right and left colons (full arrows); (C) rapid gadolinium enhancement in the sigmoid in the gradient echo T1-weighted sequence after contrast enhancement (hollow arrow); (D) diffusion-weighted hyperintensity in the sigmoid (hollow arrow).
Comparison among the six MR-score items for endoscopic inflammation detection in ulcerative colitis or in Crohn's disease
Ulcerative colitis
When comparing the accuracy of the six MR-score items for the detection of endoscopic inflammation in patients with ulcerative colitis, one item displayed decreased accuracy, namely parietal oedema (supplementary table 1). Of note, there was no significant difference in accuracy between DWI-HI and GADO AUROC (p=0.86) (figure 2D).
Crohn's disease
In Crohn's disease, all six MR-score items displayed broadly similar accuracy in detecting endoscopic inflammation (supplementary table 2). Of note, there was no significant difference in accuracy between DWI-HI and GADO AUROC (p=0.58) (figure 2D).
Predictive factors for endoscopic inflammation among MR-score items in ulcerative colitis and Crohn's disease
In ulcerative colitis, binary logistic regression revealed two items in the MR-score that were independent predictors of the presence of endoscopic colonic inflammation: the presence of a DWI-HI (OR=13.26, p=0.0001) and the presence of GADO (OR=25.6, p=0.003). In Crohn's disease, the presence of a DWI-HI (OR=2.67, p=0.01) and the presence of bowel wall thickening (OR=10.03, p<0.0001) were independent predictors of the presence of endoscopic inflammation in the colon (table 5).
Binary logistic regression analysis presenting factors independently associated with endoscopic inflammation in ulcerative colitis and in Crohn's disease
Correlation of the MR-score-T with clinical and biological markers of disease activity in ulcerative colitis and Crohn's disease
Ulcerative colitis
In ulcerative colitis, the MR-score-T correlated strongly with the Walmsley index (r=0.678, p<0.0001). The MR-score-T correlated with all biological parameters studied: CRP, haemoglobin, haematocrit, platelet count, serum iron, and albumin. The correlation coefficients between the MR-score-T and all clinical and biological markers of disease activity were broadly similar to the corresponding correlation coefficients between MBS-T and the same disease activity markers (table 6).
Correlation of total magnetic resonance score or endoscopic scores with clinical and biological markers of disease activity in ulcerative colitis and Crohn's disease
Crohn's disease
Similar to ulcerative colitis, the MR-score-T correlated with CDAI (r=0.367, p=0.004). The MR-score-T correlated with all biological parameters studied except platelet count. The correlation coefficients between the MR-score-T and all clinical and biological markers of disease activity were broadly similar to the corresponding correlation coefficients between SES-CD and the same disease activity markers. Of note, the SES-CD correlated significantly with CDAI and all biological parameters studied (CRP, haemoglobin, haematocrit, platelet count, serum iron, and albumin) (table 6).
Interobserver agreement for MR-score calculation
Interobserver agreement was very good in the evaluation of MR-score-T (κ coefficient (K)=0.85) and good in the evaluation of MR-score-S (K=0.807). Concerning each of six components of the MR-score, the interobserver agreements were good with κ coefficients ranging from 0.64 to 0.803 (table 7).
Interobserver agreement for MR-score calculation
Discussion
Our results indicate that MRI-DWI-colonography, a modality combining MRI and DWI, without oral or rectal preparation may represent a non invasive tool in assessing colonic inflammation in ulcerative colitis.
Over the past 20 years, more than 20 studies have reported the accuracy of MRI in Crohn's disease, and three studies included patients with ulcerative colitis.6 18 19 Endoscopy was used as a reference standard test in most studies.4 6 18–31 Rimola et al recently evaluated the value of MRI for assessing disease activity in comparison with CC in a prospective study involving 50 patients with Crohn's disease. MRI findings were predictive of the presence of endoscopic lesions, as reported by CC. The authors developed a composite MRI score derived from logistic regression, which demonstrated a good diagnostic accuracy for detecting the endoscopic activity of Crohn's disease (AUROC = 0.891, sensitivity 0.81, specificity 0.89).4 None of the patients included in this study had ulcerative colitis.4
MRI was performed after bowel cleansing with at least 1000 ml polyethylene glycol solution.4 In addition, 45 min before the MR each patient had to drink 1500 ml of polyethylene glycol solution for adequate distension of the distal ileum. Finally, a volume of warm water ranging from 1000 to 2000 ml was administered to the patient using a flexible rectal balloon catheter.4 In the literature and in our daily practice, it should be emphasised that oral and rectal bowel cleansing preparations are often poorly tolerated by patients.32 As stated by Rimola et al4 these data underscore the need to develop imaging techniques that do not require bowel preparation.
DWI derives its image contrast from differences in the motion of water molecules between tissues.8 Such imaging can be performed quickly, without the need for the administration of exogenous contrast medium.8 33 Only two studies have reported the feasibility of this technique in Crohn's disease. In the study performed by Kiryu et al, barium contrast radiography and/or the pathology of surgically resected specimens was used as reference examinations. No CC was performed in this work.9 Oto et al employed CC or the surgically removed bowel as the reference tests, but only 11 patients could be analysed. In addition, patients had received an oral preparation (1350 ml over 45 min) with intramuscular administration of glucagon at a dose of 1 mg.10 In both studies, patients had fasted 2 or 6 h prior to the examination.9 10
The technique of MRI-DWI-colonography used in our study has several advantages: (1) neither oral nor rectal preparation is required, (2) no fasting is needed, and (3) the duration of the procedure is relatively short (about 20 min for the overall process).
Overall, our results indicate that MRI-DWI-colonography without oral or rectal preparation allows the detection of endoscopic inflammation in IBD, especially in ulcerative colitis. The aim of the present study was to evaluate the accuracy of MRI-DWI-colonography without oral or rectal preparation for the detection of colonic inflammation in IBD. From a pathological standpoint, it is well known that colonic inflammation in ulcerative colitis is continuous and diffuse, which may allow better detection of colonic inflammation by diffusion-weighted MRI. By contrast, the colonic inflammation in Crohn's disease is usually segmental. This might explain the lower accuracy of diffusion-weighted sequences for the detection of colonic inflammation in Crohn's disease when compared to ulcerative colitis. Furthermore, our results indicate that bowel wall thickening was a better predictor of the presence of endoscopic inflammation in the colon of patients with Crohn's disease (OR=10.03, p<0.0001) when compared to DWI-HI (OR=2.67, p=0.01). This result supports the view that bowel wall thickening better reflects inflammation in Crohn's disease because of its transmural pattern. Consistently, several studies have demonstrated the accuracy of the bowel wall thickening as an independent predictor of inflammation during Crohn's disease, as measured by ultrasonography,20 CT,34 or MRI.29 Whether luminal contrast may improve the diagnostic accuracy of our technique remain to be investigated. Our data indicate that MRI-DWI-colonography without oral or rectal preparation cannot be recommended for detecting colonic inflammation in Crohn's disease.
All available studies utilised gadolinium-enhanced T1- and T2-weighted sequences.4 6 18 20 22–26 28 29 35 Since the publication of the first cases of gadolinium-induced nephrogenic systemic fibrosis, interest in finding an alternative method of extracellular contrast enhancement has arisen. The diffusion-weighted sequence for MRI avoids the use of gadolinium injection. Interestingly, DWI-HI exhibited the same accuracy as GADO for the detection of endoscopic inflammation in both ulcerative colitis and Crohn's disease, suggesting that the DWI sequence may replace gadolinium injection for detecting inflammatory colonic segments in IBD. Logistic regression analysis showed that a DWI-HI was predictive of the presence of endoscopic inflammation in both the ulcerative colitis and the Crohn's disease groups (OR=13.26 and 2.67, respectively).
Even though data collection was prospective and standardised, our study was observational. Therefore, our results remain to be confirmed in an independent validation cohort. Pending validation studies, colonoscopy remains the ‘gold standard’ to assess disease activity and severity in IBD. In addition, colonoscopy allows evaluation of mucosal lesions at the histological level and is usually well tolerated.
The number of patients in the ulcerative colitis group was relatively low compared with the Crohn's disease group, but the results remained significant, confirming the superiority of DWI-HI and GADO in the detection of endoscopic inflammation in the ulcerative colitis compared with the Crohn's disease group.
In conclusion, MRI-DWI-colonography without oral or rectal preparation could represent a non-invasive tool in assessing colonic inflammation in IBD, especially in ulcerative colitis. This technique is non-invasive, non-irradiating, does not require any bowel preparation, and is of short duration. The MR score appears to be easy to calculate, reproducible, and well correlated with disease activity in both ulcerative colitis and Crohn's disease. Our results also indicate that gadolinium contrast medium may be replaced by the diffusion-weighted sequence for the detection of endoscopic inflammation, which has the advantage of eliminating any risk of gadolinium-induced nephrogenic systemic fibrosis.
References
Supplementary materials
Web only data gut.2009.197665
Files in this Data Supplement:
Footnotes
AO and VL contributed equally to this study.
Competing interests None.
Ethics approval This study was conducted with the approval of the University Hospital of Nancy.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Digest