
Abstract
Background
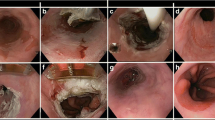
Barrett’s esophagus–related high-grade dysplasia or mucosal cancer can be treated by endoscopic mucosal resection (EMR), but the adjacent metaplastic epithelium remains at risk for developing further lesions. Our objective was to evaluate the results of the circumferential EMR in removing not only the neoplastic lesion but also the remaining Barrett’s epithelium.
Methods
Forty-one consecutive patients (mean age: 66 years) with Barrett’s esophagus were submitted to 63 EMR sessions in one single-referral endoscopic unit. All patients had high-grade dysplasia, and cancer was detected in 23 of these cases, most of them classified as T1N0 (20 patients) by endosonography. Mucosectomy after saline submucosal injection was performed for the neoplastic lesions and, if necessary, the residual Barrett’s epithelium was removed by the same technique one month later.
Results
A retrospective evaluation showed that, during a mean follow-up of 31.6 months, Barrett’s epithelium was completely replaced by squamous epithelium in 31 (75.6%) cases. There were 10 complications, all of which were managed endoscopically: 8 cases of bleeding and two perforations occurred in 9 (14.3%) patients. One patient developed an esophageal stricture. Barrett’s epithelium recurred in 10 (24.4%) patients and recurrent or metachronous early cancer was detected in 5 (12.2%), all but one of which were treated again by EMR; the fifth patient was referred to surgery. Argon plasma coagulation was used in 6 cases to treat Barrett’s epithelium, and two patients received concomitant chemoradiotherapy as adjuvant therapy.
Conclusions
Circumferential EMR provides an effective endoscopic approach to the management of Barrett’s esophagus-related high-grade dysplasia and mucosal cancer. Additional studies are necessary to evaluate the long-term results.
Similar content being viewed by others


References
Buttar NS, Wang KK, Lutzke LS, Krishnadath KK, Anderson MA (2001) Combined endoscopic mucosal resection and photodynamic therapy for esophageal neoplasia within Barrett’s esophagus. Gastrointest Endosc 54: 682–688
Ell C, May A, Gossner L, Pech O, Gunter E, Mayer G, Henrich R, Vieth M, Muller H, Seitz G, Stolte M (2000) Endoscopic mucosal resection of early cancer and high-grade dysplasia in Barrett’s esophagus. Gastroenterology 118: 670–677
Fleischer D (2000) Endoscopic mucosal resection: (not) made in the USA (so commonly): A dissection of the definition, technique, use, and controversies. Gastrointest Endosc 52: 440–444
Giovannini M, Bories E, Pesenti C, Moutardier V, Monges G, Danisi C, Lelong B, Delpero JR (2004) Circumferential endoscopic mucosal resection in Barrett’s esophagus with high-grade intraepithelial neoplasia or mucosal cancer. Preliminary results in 21 patients. Endoscopy 36: 782–787
Heitmiller RF, Redmond M, Hamilton SR (1996) Barrett’s esophagus with high grade dysplasia: An indication for prophylactic esophagectomy. Ann Surg 224: 66–71
Holscher AH, Bollschweiler E, Schroder W, Gutschow C, Siewert J (1997) Prognostic differences between early squamous-cell and adenocarcinoma of the esophagus. Dis Esophagus 10:179–184
Lightdale CJ (1999) Esophageal cancer. Am J Gastroenterol 94:20–29
May A, Gunter E, Roth F, Gossner L, Stolte M, Vieth M, Ell C (2004) Accuracy of staging in early oesophageal cancer using high resolution endoscopy and high resolution endosonography: A comparative, prospective, and blinded trial. Gut 53:634–640
May A, Gossner L, Pech O, Muller H, Vieth M, Stolte M, Ell C (2002) Intraepithelial high-grade neoplasia and early adenocarcinoma in short-segment Barrett’s esophagus: Curative treatment using local endoscopic treatment techniques. Endoscopy 34: 604–610
Mino-Kenudson M, Brugge WR, Puricelli WP, Nakatsuka LN, Nishioka NS, Zukerberg LR, Misdraji J, Lauwers GY (2005) Management of superficial Barrett’s epithelium-related neoplasms by endoscopic mucosal resection: Clinicopathologic analysis of 27 cases. Am J Surg Pathol 29: 680–686
Nigro JJ, Hagen JA, DeMeester TR, DeMeester SR, Theisen J, Peters JH, Kiyabu M (1999) Occult esophageal adenocarcinoma: Extent of disease and implications for effective therapy. Ann Surg 230: 433–438
Nijhawan PK, Wang KK (2000) Endoscopic mucosal resection for lesions with endoscopic features suggestive of malignancy and high-grade dysplasia within Barrett’s esophagus. Gastrointest Endosc 52: 328–332
Ormsby AH, Petras RE, Henricks WH, Rice TW, Rybicki LA, Richter JE, Goldblum JR (2002) Observer variation in the diagnosis of superficial oesophageal adenocarcinoma. Gut 51: 671–676
Pellegrini CA, Pohl D (2000) High-grade dysplasia in Barrett’s esophagus: Surveillance or operation? J Gastrointest Surg 4: 131–134
Sampliner RE (2002) Practice Parameters Committee of the American College of Gastroenterology. Updated guidelines for the diagnosis, surveillance, and therapy of Barrett’s esophagus. Am J Gastroenterol 97: 1888–1895
Satodate H, Inoue H, Yoshida T, Usui S, Iwashita M, Fukami N, Shiokawa A, Kudo SE (2003) Circumferential EMR of carcinoma arising in Barrett’s esophagus: Case report. Gastrointest Endosc 58: 288–292
Savoy AD, Wallace MB (2005) EUS in the management of the patient with dysplasia in Barrett’s esophagus. J Clin Gastroenterol 39: 263–267
Scotiniotis IA, Kochman ML, Lewis JD, Furth EE, Rosato EF, Ginsberg GG (2001) Accuracy of EUS in the evaluation of Barrett’s esophagus and high-grade dysplasia or intramucosal carcinoma. Gastrointest Endosc 54: 689–696
Seewald S, Akaraviputh T, Seitz U, Brand B, Groth S, Mendoza G, He X, Thonke F, Stolte M, Schroeder S, Soehendra N (2003) Circumferential EMR and complete removal of Barrett’s epithelium: A new approach to management of Barrett’s esophagus containing high-grade intraepithelial neoplasia and intramucosal carcinoma. Gastrointest Endosc 57: 854–859
The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon (2003). Gastrointest Endosc 58: S3–S43
Vieth M, Rosch T (2006) Endoscopic mucosal resection and the risk of lymph-node metastases: Indications revisited? Endoscopy 38: 175–179
Vieth M, Ell C, Gossner L, May A, Stolte M (2004) Histological analysis of endoscopic resection specimens from 326 patients with Barrett’s esophagus and early neoplasia. Endoscopy 36: 776–781
Weston AP, Badr AS, Hassanein RS (1999) Prospective multivariate analysis of clinical, endoscopic, and histological factors predictive of the development of Barrett’s multifocal high-grade dysplasia or adenocarcinoma. Am J Gastroenterol 94: 3413–3419
Acknowledgments
Doctor Lopes is financed by grants from CNPq-Brazil.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lopes, C.V., Hela, M., Pesenti, C. et al. Circumferential endoscopic resection of Barrett’s esophagus with high-grade dysplasia or early adenocarcinoma. Surg Endosc 21, 820–824 (2007). https://doi.org/10.1007/s00464-006-9187-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-006-9187-3